Radiotherapy In-vivo Treatment Verification: Multi-center analysis for more than 6 million fractions delivered
|
|
|
- Peter Carr
- 5 years ago
- Views:
Transcription
1 Radiotherapy In-vivo Treatment Verification: Multi-center analysis for more than 6 million fractions delivered Gustavo Olivera, Daniel Galmarini, Xiaohu Mo, Donald Parnell, Stephanie Key, Yu Chen, Daniel Dosoretz, Eduardo Fernandez, Constantine Mantz, Steven Finlkelstein 21 st Century Oncology Abstract Context: Verification and safety are always a main concern in external beam radiotherapy. Even when significant time and resources are expended to guarantee quality of treatment, incidents still may happen. QA was usually performed before treatment. Verify what happen during the actual treatment may help to find undetected possible issues. With the introduction of portal dosimetry verification of behavior during treatment for every patient every fraction is clinically feasible. Objective: Present the results of an in-vivo verification technique. Observe in-vivo deliveries and show improvements that can be achieved on the treatment consistency over time. Analyze the number of times that in-vivo verification trigger action levels and evaluate the extra workload involved. Design, Settings and Patients: An in-vivo verification program was implemented in 84 clinics over a period of 3 years. More than 6 million daily fractions were recorded and analyze. The data cover most of the external radiotherapy manufacturers equipment (Varian, Siemens, Elekta and TomoTherapy). For every patient every fraction the calibrated portal exit dosimetry panel collected the exit beam dosimetry. An average of five-day fraction exit dosimetry panel was compared against a reference fraction using the gamma metric. A troubleshoot procedure was in place to evaluate when action level was triggered. Results: The use of in-vivo verification allows improving the dosimetric treatment consistency as the treatment. In a period of 1 year results improved passing criteria by 6% for linacs and 7% for TomoTherapy and were maintained to those levels since then. The level of intervention was dependent on the anatomical site. Head and neck, lung and breast approximately 20% of the weekly portal triggered and action level that require verification during treatment. For pelvis 13% and less than 10% for prostate. On average between one or two average weekly exit dosimetry portals per patient need to be verified because of trigger of an action level. Conclusions: In-vivo verification had been used to trigger lack of consistency on the exit dosimetry in more than 6 millions fractions and 84 clinics. Significant Improvements on treatment consistency are obtained and maintained by performing in vivo verification on daily basis. The number of flags detected for the more common treat anatomical site is
2 significant and require to be verified to clear up possible issues. Based on these numbers and difficulty in predict what patients will have flags in vivo verification should be considered for every patient every fraction. This will imply and extra work load of at least the same amount of time and sometimes even double than the time that is spend verifying pre-treatment QA (even having automatic procedures).
3 1- Introduction External beam radiotherapy is a commonly used technique to treat cancer. During the last 20 years radiotherapy had rapidly evolved from three-dimensional conformal radiotherapy (3D) [1], to intensity modulated radiotherapy (IMRT)[2, 3] and many forms of image-guided radiotherapy (IGRT)[3]. These technologies aim to minimize the radiation deposited to normal tissues and in many cases allow increasing the dose delivered to the tumor. All of these techniques have comprehensive quality assurance procedures (QA) in place that had been evolving as the technology evolves[4-10]. Even with such comprehensive QA programs still incidents may happen during treatment delivery [11-23]. In IMRT the typical QA involves in phantom measurements that act as patient surrogate or by delivering the plan to a portal imager[9]. Both of them are typically performed before treatment. The IGRT portion in the majority of cases is performed by getting a portal image or a CT from the different possible on board CT capabilities available. This image capabilities aid in patient setup but also the can help during the in-vivo verification. Verification of what happen during the time that treatment is actually delivered (in-vivo verification) may provide significant insight to evaluate the actual course of treatment. Possible issues that may be undetected with QA before treatment could be found using in-vivo verification techniques[24-26]. Countries like France[27] and UK[28, 29] have government recommendations for in-vivo dosimetry techniques. The evolution on portal dosimetry in modern machines allows to perform in vivo dosimetry in clinical routine in an efficient fashion[24, 30-38]. However, still this type of in-vivo verification may not be widely used for every patient every day, and sometimes is not even available on the treatment machines. A lot of resources, time and equipment are invested on QA programs that in general look into what is happen before treatment. However, not always what happened during treatment is evaluated. Techniques to efficiently perform in-vivo verification increase the current workload, but also provide valuable information to evaluate and adapt (if necessary) the course of treatment. The current manuscript presents the results from an in-vivo verification program implemented in 84 clinics where more than 6 million fractions were delivered. The in-vivo verification covers most of the machines manufactures available (Varian, Siemens, Elekta and TomoTherapy). The number of times that an intervention is flagged due to violation of an action level that triggered review during the course of treatment is analyzed for the more common anatomical sites. The intervention may correspond to possible setup, machine or anatomical changes. The number of flags decreases as function of time when in-vivo
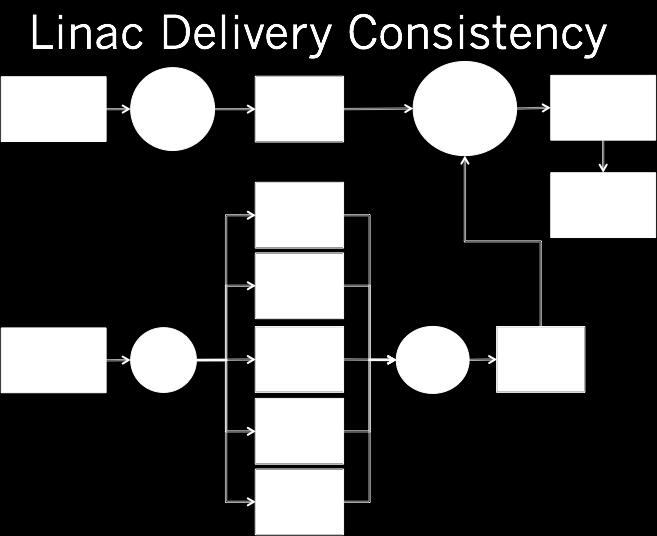
4 verification was used. The verification of possible flags during treatment is a necessary condition to evaluate normal course of treatment. 2- Materials and Methods 2.1- In vivo verification technique In order to analyze the delivery during treatment a delivery consistency procedure was implemented. Figure 1 is a workflow diagram of the implemented procedure. For each patient and each fraction a portal image of the exit dose impinging the exit detector by the transmitted treatment beam is acquired during treatment. It is worth to remark that this procedure does not imply any extra dose to the patient. The technique only collects radiation that is going through the patient. The exit detectors for the linacs had been calibrated following manufacturer procedures in order to have their reading in Calibrated Units (CU)[35, 39, 40]. For the TomoTherapy machines the projection average raw data of the exit detector was used. Patient setup for all deliveries was image guided, either with portals, CBCT or MVCT. In particular in TomoTherapy machines all patients where guided with daily MVCT. On the first implementation that we use, and for most of the results presented on this manuscript, the user selects a particular portal as reference fraction. This approach will be valid provided that the setup for that reference fraction is adequate and that the anatomical changes between the plan and actual fraction are small. After a detailed verification of the registration at the time of treatment for those two fractions, and the similarity of the anatomy between the planning CT and daily CT is checked (when CT available), one of those fractions is chosen as reference fraction if the information is consistent. If the first two fractions are not consistent, there are procedures to evaluate possible causes of the inconsistency to continue the process of selecting a reference fraction. Once the reference fraction is selected it is compared against a computed five days average of the daily portals. To compare the consistency between the reference fraction respect to the weekly average the Gamma metric is used[41]. Each clinic was allowed to choose their action levels for review on between 3% 3mm and 5% 5mm for the linacs. In TomoTherapy was always 3%3mm. If the action level is violated an investigation was needed to identify and clear up the possible issues. Figure 2 is the table used during the troubleshoot procedure that includes a system review and a place to indicate possible cause of failures
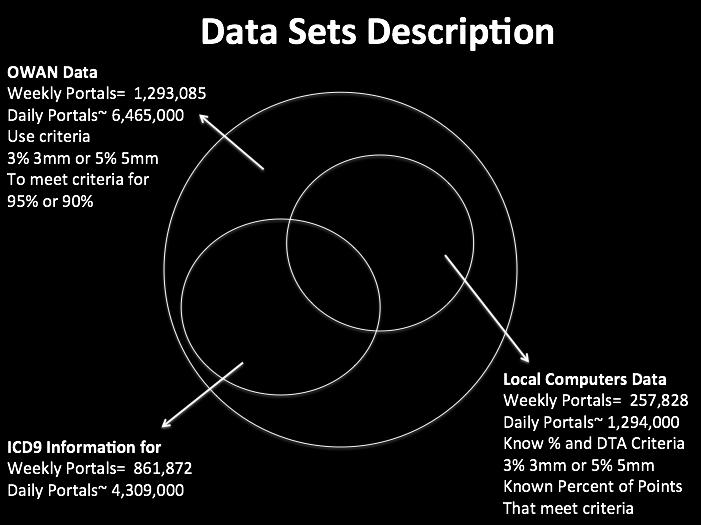
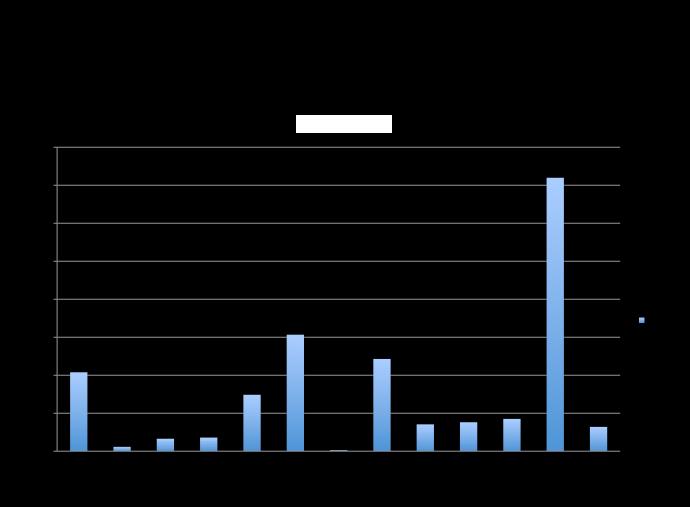
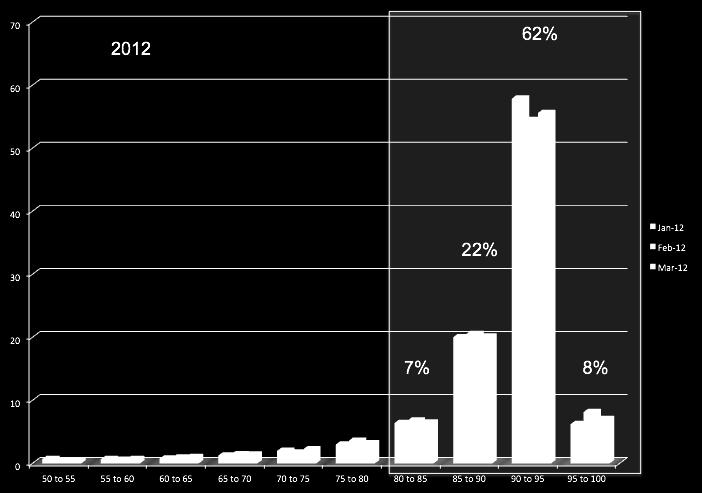
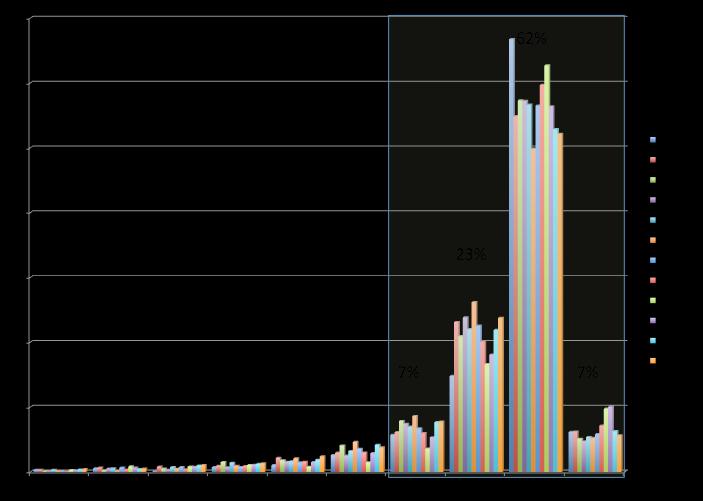
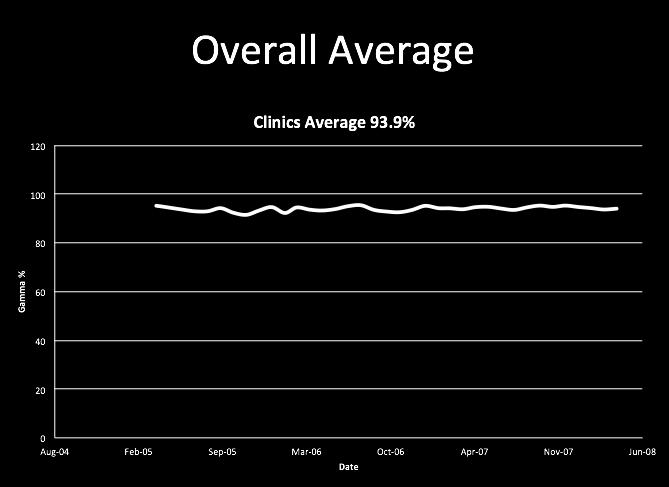
5 determined after investigation. Also it is indicated if physics or physician action is required Data sets Data had being collected for 84 clinics and for a period of 3 years. Due to the large number of clinics and the length that data had being collected not all of the data contains the same amount of detail. The number of data for linacs is described in Figure 3. Approximately 6,465,085 daily portals had being analyzed. They correspond to 1,293,085 weekly portals. For this data set it is known if they use 3% 3mm or 5% 5mm criteria and if the number of portal points passing that gamma criteria was over 95% or 90 % respectively. For approximately 4,309,000 daily portals that correspond to 861,872 weekly portals ICD9 information was available to determine anatomical location. For approximately 1,294,000 fractions that correspond to 257,858 weekly portals it is known if 3% 3mm or 5% 5mm criteria was used and the exact percentage of points of the portal imager that pass the corresponding Gamma criteria. The data set for TomoTherapy contains 42,866 daily portals. 3- Results and Discussions Figure 4a shows the distribution of anatomical cases analyzed for linacs. Prostate, head and neck, breast, pelvis and lung encompass the main core of the portals analyzed. As mentioned earlier clinics where allowed to choose their action level for review. Some of the clinics use gamma criteria 3% 3mm and others 5% 5mm. Also, sometimes the clinics that use the 3% 3mm, as the treatment evolved if properly justified switch the criteria for the last part of the treatment to 5% 5mm. Example for this correspond to patients with significant anatomical changes and/or weight loss that may difficult the daily setup. To shed some light on the impact of using 3% 3mm or 5% 5mm as action level we analyzed the distribution of the percentage of points passing each criteria. At first glance two distinctive regions can be observed in Figure 4b. The first region (under 80 % threshold) corresponds to systematic issues such as incomplete image capture, couch bar on the exit beam, incomplete delivery, etc. The region associated to deviations link to the clinical evolution of the treatment is the region with percentage pass over 80%. For this region the distribution of points passing the criteria 3% 3mm and 5% 5mm is very similar. Also the number of cases under the 80% pass criteria is very small and decrease very rapidly. This seems to indicate that even when may be desirable to improve quality to work with the tighter criteria 3 % 3mm, still clinical relevant issues will be flag with both criteria. Figure 5 analyze the improvements that using the in-vivo verification procedure had provided on the percentage of points passing the action level criteria from 2009 to The percentage of pass month by month is displayed for each year in each plot. It can be observed that a significant shift toward higher level of
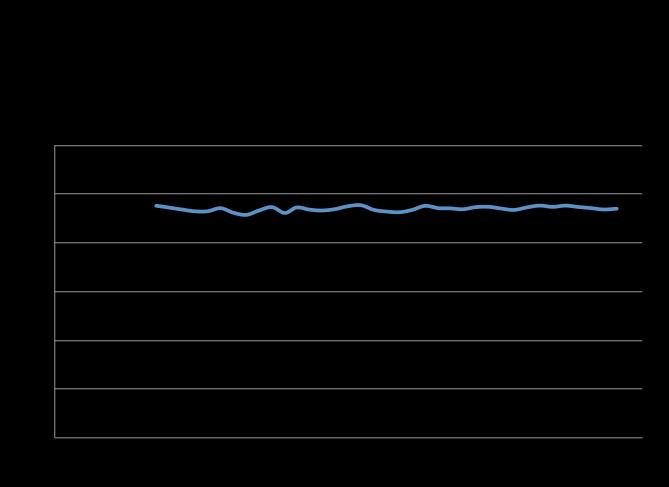
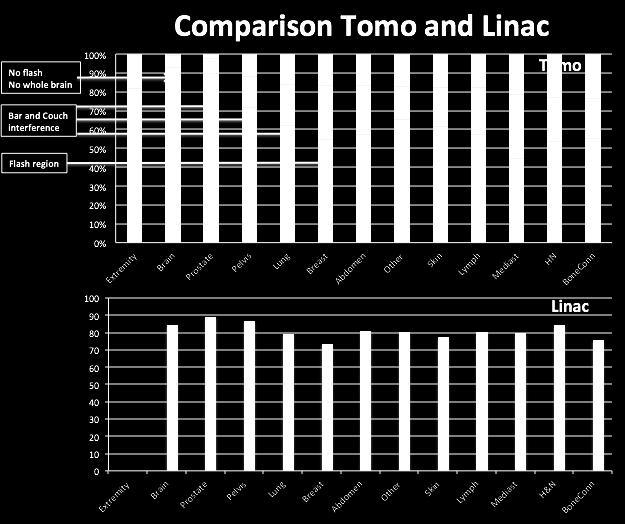
6 pass (on the order of 6% on average for bins between 80 to 95%). For the subsequent years the improvements had been small and reach a plato. The use of the in vivo-verification had improve noticeable the consistency of the plan delivery and is able to keep it over time. Figure 6 displays for each one of the anatomical sites considered the percentage of average weekly portals that pass the action level criteria. The data was analyzed separately for linacs (Figure 6a) and TomoTherapy (Figure 6b). For the linacs some cases were daily aligned by portal imagers and some other with cone beam CT. By the contrary in TomoTherapy 100 percent of the cases where CT guided and all of them with 3% 3mm tolerances. For head and neck cases 18% of the weekly in-vivo verification gamma in linacs and 22% of the weekly gamma for TomoTherapy triggered action levels for review. This means on average for head and neck cases one or may be two weeks of treatment will require a physics review to verify the adequacy of the treatment. For pelvis the percentage of weekly portal that need review is 13% for linac and TomoTherapy; for breast 26% in linacs and 16% in TomoTherapy; in lung 21% in linacs 16 % in TomoTherapy; for Prostate 11% in linacs and 4% in TomoTherapy. By no means the lower trigger percentage in TomoTherapy is associated to better treatments in TomoTherapy. For breast cases the differences are associated to the flash region. TomoTherapy does not have a flash region and linacs do. If the breast is in a different spot of the flash region for a linac may trigger action level but does not correlate to a clinical relevant issue. Also, in some few cases the retractable arms interfere in different fashions the exit beam in linacs that also is not relevant clinically. For prostate, lung and pelvis the difference between TomoTherapy and linacs is associated to interference from the couch and moveable arms at the exit beam that is not clinically relevant. Perhaps in the future threshold for flagging should become anatomically dependent. From this figures can be inferred that on average for prostate a weekly portal every two patients will need to be reviewed. For head and neck, pelvis, breast and lung at least one and may be two weekly portals per patient will trigger action for review. Clearly different anatomical sites will need different level of controls during treatment. However, it is very important to notice that unless we measure all of them we are not able to predict what patients and when they will need review. So every patient every fraction will need to be measured and analyzed to verify at least treatment consistency. Figure 6c shows the average number of interventions needed as function of time for all of the anatomical cases analyzed. The number is around 6 % that is clearly shifted to those levels due to be prostate the majority of cases evaluated (see Figure 2). The load of review had been approximately constant over time. Typically by just a QA before treatment many of these inconsistencies may go undetected. They will arise from possible machine, setup and/or anatomical changes. Sometimes they correspond to the normal course of treatment but sometimes no. In any case once detected and they need to be analyzed and solve if deem necessary. The role of a technique like this is to provide flags due
7 to lack if consistency. The clinical impact of this flags will need more ancillary process to be able to evaluate them. For instance, to be able to reconstruct the dose that was deposited on the patient is highly desirable tool to evaluate possible clinical impact of cases that triggered action levels. In the TomoTherapy machines where 100% of the cases are CT guided we now have implemented such a tool to measure clinical impact that performs adaptive dose recalculation. The program is completely automatic and gathers the information from the same archives that the in-vivo verification does. The program extracts the daily MVCT creating a merge CT at the location where the patient was treated taking into account the image registration used for treatment. A merge image is a CT that contains the complete MV CT that was imaged with the planning kv CT filling in the rest of the image. This merge CT is used to compute the fraction dose. The dose calculator is a convolution superposition[42-44] dose calculator. To be more efficient, our implementation is GPU based. A deformable registration algorithm based on morphons[45, 46] was used to generate daily contours and analyze daily and cumulative DVHs. The deformable registration also provides deformation maps that allow mapping back the daily doses to the planning CT in order to compare planned dose respect to cumulative actual delivery. A GUI allows the user to analyze the registration, contours, daily and cumulative doses. We have implemented adaptive dose recalculation on five linacs also. As part of a future work we will also evaluate the clinical relevance of the flags provided by in vivo verification based on portals. It is interesting to notice that the behavior per anatomical site for TomoTherapy and Linacs is very similar even when in TomoTherapy daily CT guidance is used in all cases. From the results presented can be inferred that the implementation of a program such as the one described here, can validate consistency during treatment and also flag for verification is an action level is violated. The workload per patient (even if the process are automatic) may increase by 100 to 200 percent respect to the time that typically is expended validating pre-treatment QA. Additional work will need to be performed if an adaptive dose recalculation process is implemented to gauge clinical impact. Even when this will be and extra use of resources in a radiotherapy department, by doing this many possible issues could be detected at the more critical moment that is the treatment time. 4-Conclusions Results from an in-vivo verification program with more than 6 millions fractions from 84 clinics were presented. The data cover most of the external radiotherapy manufacturers equipment (Varian, Siemens, Elekta and TomoTherapy).
8 Significant improvements on treatment consistency over time can be achieved by monitoring the behavior during treatment. It was shown that the number of verifications that was needed due to action levels that trigger a flag was anatomy dependent. For head and neck, breast and lung approximately 20 % of the weekly verification portals trigger action level. For pelvis 13% of the weekly portals required verification and prostate less than 10%. These numbers are significant to show the need to verify treatments invivo. Verification during treatment may detect possible issues that may go undetected otherwise. It should be observed that the level of flagging for each anatomical site was on similar levels for linacs and TomoTherapy. By one side linacs use flagging criteria of 3% 3mm and 5%5mm and the IGRT portion was either 2D portal or cone beam CT. On the other hand TomoTherapy always used 3%3mm and every fraction was CT guided. On average between one or two weekly portals per patient trigger actions levels during the course of a patient treatment and require to be verified. The workload to do this task is considerable but we should keep in mind that may provide valuable information to QA patients. It typically will take per patient at least the same amount of time and sometimes-even double than the time that is spending verifying pre-treatment QA (even having automatic procedures).
9 Figure 1: Workflow diagram for the in-vivo verification technique used. Figure 2: Table used duirng the troubleshooting procedure when action levels are flag. Figure 3 : Description of the linac data sets available for analysis. Figure 4: a) Description of the case mix used on this analysis. The cases were used using ICD9 information. b) Histogram of percentage of passing points for weekly portals for the 3% 3mm and 5%5mm criterias. Figure 5: Histogram of percentage of passing points for weekly portals for each month a) 2009, b) 2010, c) 2011, a) Figure 6: Percentace weekly portals passing in-vivo verification criteria for different anatomical sites. a) Linacs, b) TomoTherapy, c) Overall passing percentage as function of time.
10 Bibliography 1. Khan, F.M. and B. Gerbi, Treatment Planning in Radiation Oncology. 2012: Wolters Kluwer Health, Lippincott Williams & Wilkins. 2. Webb, S., Intensity-Modulated Radiation Therapy, ed. C.S. orton, J; Webster, J. 2001: IOP. 3. Bortfeld, T., Image-guided IMRT. 2006, Berlin: Springer. xii, 460 p. 4. Murphy, M.J., et al., The management of imaging dose during image-guided radiotherapy: report of the AAPM Task Group 75. Med Phys, (10): p Ezzell, G.A., et al., IMRT commissioning: multiple institution planning and dosimetry comparisons, a report from AAPM Task Group 119. Med Phys, (11): p Klein, E.E., et al., Task Group 142 report: quality assurance of medical accelerators. Med Phys, (9): p Langen, K.M., et al., QA for helical tomotherapy: report of the AAPM Task Group 148. Med Phys, (9): p Gregoire, V. and T.R. Mackie, State of the art on dose prescription, reporting and recording in Intensity-Modulated Radiation Therapy (ICRU report No. 83). Cancer Radiother, (6-7): p Low, D.A., et al., Dosimetry tools and techniques for IMRT. Med Phys, (3): p Bissonnette, J.P., et al., Quality assurance for image-guided radiation therapy utilizing CT-based technologies: a report of the AAPM TG-179. Med Phys, (4): p Yeung, T.K., et al., Quality assurance in radiotherapy: evaluation of errors and incidents recorded over a 10 year period. Radiother Oncol, (3): p Ash, D., Lessons from Epinal. Clin Oncol (R Coll Radiol), (8): p Peiffert, D., J.M. Simon, and F. Eschwege, [Epinal radiotherapy accident: passed, present, future]. Cancer Radiother, (6-7): p Williams, M.V., Radiotherapy near misses, incidents and errors: radiotherapy incident at Glasgow. Clin Oncol (R Coll Radiol), (1): p Williams, M.V., Improving patient safety in radiotherapy by learning from near misses, incidents and errors. Br J Radiol, (953): p Ortiz Lopez, P., J. M. Cosset, P. Dunscombe, O. Holmberg, J. C. Rosenwald, L. Pinillos Ashton, J. J. Vilaragut Llanes and S. Vatnitsky ICRP publication 112. A report of preventing accidental exposures from new external beam radiation therapy technologies. Ann ICRP, (4): p Shafiq, J., et al., An international review of patient safety measures in radiotherapy practice. Radiother Oncol, (1): p Bissonnette, J.P. and G. Medlam, Trend analysis of radiation therapy incidents over seven years. Radiother Oncol, (1): p Bogdanich, W., Radiation Offers New Cures, and Ways to Do Harm, in New York Times
11 20. Abdel-Wahab, M., et al., Safety in radiation oncology: the role of international initiatives by the International Atomic Energy Agency. J Am Coll Radiol, (11): p Dunscombe, P., Recommendations for safer radiotherapy: what's the message? Front Oncol, : p Kim, J., Categorizing accident sequences in the external radiotherapy for risk analysis. Radiat Oncol J, (2): p Mazeron, R., N. Aguini, and E. Deutsch, [Risk analysis in radiation therapy: state of the art]. Cancer Radiother, (4): p , quiz Fiorino, C., et al., Quality assurance by systematic in vivo dosimetry: results on a large cohort of patients. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology, (1): p Mans, A., et al., Catching errors with in vivo EPID dosimetry. Medical physics, (6): p Lu, W., et al., Validation of a simple portal dose calculator calculation model for plan QA and in-vivo dosimetry. Medical Physics, (6): p Derreumaux, S., et al., Lessons from recent accidents in radiation therapy in France. Radiat Prot Dosimetry, (1): p Edwards, C.R., et al., An update survey of UK in vivo radiotherapy dosimetry practice. The British journal of radiology, (960): p Edwards, C.R. and P.J. Mountford, Characteristics of in vivo radiotherapy dosimetry. The British journal of radiology, (983): p Heukelom, S., J.H. Lanson, and B.J. Mijnheer, In vivo dosimetry during pelvic treatment. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology, (2): p Heukelom, S., et al., In vivo dosimetry during tangential breast treatment. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology, (4): p Essers, M., J.H. Lanson, and B.J. Mijnheer, In vivo dosimetry during conformal therapy of prostatic cancer. Radiotherapy and oncology : journal of the European Society for Therapeutic Radiology and Oncology, (2): p McDermott, L.N., et al., Replacing pretreatment verification with in vivo EPID dosimetry for prostate IMRT. International journal of radiation oncology, biology, physics, (5): p Williams, M.V. and A. McKenzie, Can we afford not to implement in vivo dosimetry? The British journal of radiology, (969): p Wendling, M., et al., A simple backprojection algorithm for 3D in vivo EPID dosimetry of IMRT treatments. Medical physics, (7): p Fidanzio, A., et al., Breast in vivo dosimetry by EPID. Journal of applied clinical medical physics / American College of Medical Physics, (4): p Chen, Q., et al., TomoTherapy MLC verification using exit detector data. Med Phys, (1): p Wendling, M., et al., In aqua vivo EPID dosimetry. Medical physics, (1): p Fidanzio, A., et al., Generalized EPID calibration for in vivo transit dosimetry. Phys Med, (1): p
12 40. Van Esch, A., T. Depuydt, and D.P. Huyskens, The use of an asi-based EPID for routine absolute dosimetric pre-treatment verification of dynamic IMRT fields. Radiother Oncol, (2): p Low, D.A. and J.F. Dempsey, Evaluation of the gamma dose distribution comparison method. Medical Physics, (9): p Mackie, T.R., J.W. Scrimger, and J.J. Batista, A convolution method of calculating dose from 15 MeV x-rays. Med. Phys., : p Ahnesjö, A., Collapsed cone convolution of radiant energy for photon dose calculation in heterogeneous media. Med Phys, : p Lu, W., et al., Accurate convolution/superposition for multi-resolution dose calculation using cumulative tabulated kernels. Phys Med Biol, (4): p Castadot, P., et al., Comparison of 12 deformable registration strategies in adaptive radiation therapy for the treatment of head and neck tumors. Radiother Oncol, (1): p Castadot, P., et al., Adaptive radiotherapy of head and neck cancer. Semin Radiat Oncol, (2): p
13
14
15
16 a b
17

18 a b c
SunCHECK Patient Comprehensive Patient QA
 The SunCHECK Platform SunCHECK Patient Comprehensive Patient QA SunCHECK Patient // Comprehensive Patient QA Automate Your Patient QA SunCHECK Patient automates all your Patient QA needs from Secondary
The SunCHECK Platform SunCHECK Patient Comprehensive Patient QA SunCHECK Patient // Comprehensive Patient QA Automate Your Patient QA SunCHECK Patient automates all your Patient QA needs from Secondary
Evaluation of Dosimetry Check software for IMRT patient-specific quality assurance
 JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 16, NUMBER 3, 2015 Evaluation of Dosimetry Check software for IMRT patient-specific quality assurance Ganesh Narayanasamy, Travis Zalman, Chul S. Ha,
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 16, NUMBER 3, 2015 Evaluation of Dosimetry Check software for IMRT patient-specific quality assurance Ganesh Narayanasamy, Travis Zalman, Chul S. Ha,
DELIVERED PATIENT DOSE
 SOFTWARE DELIVERED PATIENT DOSE The only software that provides a true picture of patient and dose at each stage of treatment. Adaptivo patient dosimetry software does something other patient dosimetry
SOFTWARE DELIVERED PATIENT DOSE The only software that provides a true picture of patient and dose at each stage of treatment. Adaptivo patient dosimetry software does something other patient dosimetry
iviewdose Confidence and assurance in dose delivery
 iviewdose Confidence and assurance in dose delivery As radiotherapy techniques advance and treatment plans become more complex, involving escalated doses and increasingly conformal deliveries, the need
iviewdose Confidence and assurance in dose delivery As radiotherapy techniques advance and treatment plans become more complex, involving escalated doses and increasingly conformal deliveries, the need
Are Transmission Detectors a Necessary Tool for a Safe Patient Radiation Therapy Program?
 Are Transmission Detectors a Necessary Tool for a Safe Patient Radiation Therapy Program? Can you currently use direct documentation and measurement of delivered dose to ensure you did not underdose or
Are Transmission Detectors a Necessary Tool for a Safe Patient Radiation Therapy Program? Can you currently use direct documentation and measurement of delivered dose to ensure you did not underdose or
Leila E. A. Nichol Royal Surrey County Hospital
 2 nd UK and Ireland Dosimetry Check User Meeting Symposium Clatterbridge Cancer Centre, 24 th October 2012 Leila E. A. Nichol Royal Surrey County Hospital Leila.Nichol@nhs.net *My experience with Dosimetry
2 nd UK and Ireland Dosimetry Check User Meeting Symposium Clatterbridge Cancer Centre, 24 th October 2012 Leila E. A. Nichol Royal Surrey County Hospital Leila.Nichol@nhs.net *My experience with Dosimetry
Use of Electronic Portal Image Detectors for Quality Assurance of Advanced Treatments
 Use of Electronic Portal Image Detectors for Quality Assurance of Advanced Treatments Jean M. Moran, Ph.D. Department of Radiation Therapy, University of Michigan, 1500 E. Medical Center Drive, Ann Arbor
Use of Electronic Portal Image Detectors for Quality Assurance of Advanced Treatments Jean M. Moran, Ph.D. Department of Radiation Therapy, University of Michigan, 1500 E. Medical Center Drive, Ann Arbor
Overview of Advanced Techniques in Radiation Therapy
 Overview of Advanced Techniques in Radiation Therapy Jacob (Jake) Van Dyk Manager, Physics & Engineering, LRCP Professor, UWO University of Western Ontario Acknowledgements Glenn Bauman Jerry Battista
Overview of Advanced Techniques in Radiation Therapy Jacob (Jake) Van Dyk Manager, Physics & Engineering, LRCP Professor, UWO University of Western Ontario Acknowledgements Glenn Bauman Jerry Battista
Dose rate response of Digital Megavolt Imager detector for flattening filter-free beams
 Received: 12 May 2017 Revised: 23 October 2017 Accepted: 10 April 2018 DOI: 10.1002/acm2.12358 RADIATION ONCOLOGY PHYSICS Dose rate response of Digital Megavolt Imager detector for flattening filter-free
Received: 12 May 2017 Revised: 23 October 2017 Accepted: 10 April 2018 DOI: 10.1002/acm2.12358 RADIATION ONCOLOGY PHYSICS Dose rate response of Digital Megavolt Imager detector for flattening filter-free
8/3/2016. The EPID Strikes Back! - EPID In-Vivo Dosimetry. EPID Research Number of Publications. Why EPID in-vivo? Detectable errors: patient
 Number of Publications Number of publications 8/3/2016 The Strikes Back! - In-Vivo Dosimetry AAPM, Washington D.C, USA, 2016 Peter Greer 1,2 (1) University of Newcastle, Australia, (2) Calvary Mater Newcastle,
Number of Publications Number of publications 8/3/2016 The Strikes Back! - In-Vivo Dosimetry AAPM, Washington D.C, USA, 2016 Peter Greer 1,2 (1) University of Newcastle, Australia, (2) Calvary Mater Newcastle,
Quality assurance in external radiotherapy
 Quality assurance in external radiotherapy dr. Marius Laurikaitis medical physicist Oncological Hospital of Kaunas Medical University Hospital Kaunas, 2010-10-14 Acceptance and Commissioning Acceptance
Quality assurance in external radiotherapy dr. Marius Laurikaitis medical physicist Oncological Hospital of Kaunas Medical University Hospital Kaunas, 2010-10-14 Acceptance and Commissioning Acceptance
Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR
 Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR PhD, FAAPM, FACR, FASTRO Department of Radiation Oncology Indiana University School of Medicine Indianapolis, IN, USA Indra J. Das,
Linac or Non-Linac Demystifying And Decoding The Physics Of SBRT/SABR PhD, FAAPM, FACR, FASTRO Department of Radiation Oncology Indiana University School of Medicine Indianapolis, IN, USA Indra J. Das,
AAPM Task Group 180 Image Guidance Doses Delivered During Radiotherapy: Quantification, Management, and Reduction
 AAPM Task Group 180 Image Guidance Doses Delivered During Radiotherapy: Quantification, Management, and Reduction Parham Alaei, Ph.D. Department of Radiation Oncology University of Minnesota NCCAAPM Fall
AAPM Task Group 180 Image Guidance Doses Delivered During Radiotherapy: Quantification, Management, and Reduction Parham Alaei, Ph.D. Department of Radiation Oncology University of Minnesota NCCAAPM Fall
Introduction. Modalities used in imaging guidance. Flat panel detector. X-ray Imaging Dose to Patients in the Era of Image-Guided Radiation Therapy
 X-ray Imaging Dose to Patients in the Era of Image-Guided Radiation Therapy George Ding, Ron Price, Charles Coffey Vanderbilt-Ingram Cancer Center Vanderbilt University Medical Center, Nashville, TN Introduction
X-ray Imaging Dose to Patients in the Era of Image-Guided Radiation Therapy George Ding, Ron Price, Charles Coffey Vanderbilt-Ingram Cancer Center Vanderbilt University Medical Center, Nashville, TN Introduction
SBRT fundamentals. Outline 8/2/2012. Stereotactic Body Radiation Therapy Quality Assurance Educational Session
 Stereotactic Body Radiation Therapy Quality Assurance Educational Session J Perks PhD, UC Davis Medical Center, Sacramento CA SBRT fundamentals Extra-cranial treatments Single or small number (2-5) of
Stereotactic Body Radiation Therapy Quality Assurance Educational Session J Perks PhD, UC Davis Medical Center, Sacramento CA SBRT fundamentals Extra-cranial treatments Single or small number (2-5) of
MVCT Image. Robert Staton, PhD DABR. MD Anderson Cancer Center Orlando. ACMP Annual Meeting 2011
 MVCT Image Guidance and QA Robert Staton, PhD DABR MD Anderson Cancer Center Orlando ACMP Annual Meeting 2011 Disclosures MDACCO has received grant funding from TomoTherapy, Inc. Overview TomoTherapy MVCT
MVCT Image Guidance and QA Robert Staton, PhD DABR MD Anderson Cancer Center Orlando ACMP Annual Meeting 2011 Disclosures MDACCO has received grant funding from TomoTherapy, Inc. Overview TomoTherapy MVCT
Normal tissue doses from MV image-guided radiation therapy (IGRT) using orthogonal MV and MV-CBCT
 using orthogonal MV and MV-CBCT") Received: 28 September 2017 Revised: 17 November 2017 Accepted: 28 December 2017 DOI: 10.1002/acm2.12276 RADIATION ONCOLOGY PHYSICS Normal tissue doses from MV image-guided radiation therapy (IGRT) using
Received: 28 September 2017 Revised: 17 November 2017 Accepted: 28 December 2017 DOI: 10.1002/acm2.12276 RADIATION ONCOLOGY PHYSICS Normal tissue doses from MV image-guided radiation therapy (IGRT) using
Comparison of high and low energy treatment plans by evaluating the dose on the surrounding normal structures in conventional radiotherapy
 Turkish Journal of Cancer Volume 37, No. 2, 2007 59 Comparison of high and low energy treatment plans by evaluating the dose on the surrounding normal structures in conventional radiotherapy MUHAMMAD BASIM
Turkish Journal of Cancer Volume 37, No. 2, 2007 59 Comparison of high and low energy treatment plans by evaluating the dose on the surrounding normal structures in conventional radiotherapy MUHAMMAD BASIM
S. Derreumaux (IRSN) Accidents in radiation therapy in France: causes, consequences and lessons learned
 Accidents in radiation therapy in France: causes, consequences and lessons learned") S. Derreumaux (IRSN) Accidents in radiation therapy in France: causes, consequences and lessons learned MEDICAL LINEAR ACCELERATORS Electron beam (MeV) Photon beam (MV) PRECISION REQUIRED IN RADIOTHERAPY
S. Derreumaux (IRSN) Accidents in radiation therapy in France: causes, consequences and lessons learned MEDICAL LINEAR ACCELERATORS Electron beam (MeV) Photon beam (MV) PRECISION REQUIRED IN RADIOTHERAPY
Pre-treatment and in-vivo dosimetry of Helical Tomotherapy treatment plans using the Dosimetry Check system
 Pre-treatment and in-vivo dosimetry of Helical Tomotherapy treatment plans using the Dosimetry Check system E. Mezzenga, * E. Cagni, A. Botti, M. Orlandi and M. Iori Medical Physics Unit, IRCCS Arcispedale
Pre-treatment and in-vivo dosimetry of Helical Tomotherapy treatment plans using the Dosimetry Check system E. Mezzenga, * E. Cagni, A. Botti, M. Orlandi and M. Iori Medical Physics Unit, IRCCS Arcispedale
Independent corroboration of monitor unit calculations performed by a 3D computerized planning system
 JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 1, NUMBER 4, FALL 2000 Independent corroboration of monitor unit calculations performed by a 3D computerized planning system Konrad W. Leszczynski* and
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 1, NUMBER 4, FALL 2000 Independent corroboration of monitor unit calculations performed by a 3D computerized planning system Konrad W. Leszczynski* and
biij Initial experience in treating lung cancer with helical tomotherapy
 Available online at http://www.biij.org/2007/1/e2 doi: 10.2349/biij.3.1.e2 biij Biomedical Imaging and Intervention Journal CASE REPORT Initial experience in treating lung cancer with helical tomotherapy
Available online at http://www.biij.org/2007/1/e2 doi: 10.2349/biij.3.1.e2 biij Biomedical Imaging and Intervention Journal CASE REPORT Initial experience in treating lung cancer with helical tomotherapy
Feasibility study on the verification of actual beam delivery in a treatment room using EPID transit dosimetry
 Baek et al. Radiation Oncology 2014, 9:273 RESEARCH Open Access Feasibility study on the verification of actual beam delivery in a treatment room using EPID transit dosimetry Tae Seong Baek 1,2, Eun Ji
Baek et al. Radiation Oncology 2014, 9:273 RESEARCH Open Access Feasibility study on the verification of actual beam delivery in a treatment room using EPID transit dosimetry Tae Seong Baek 1,2, Eun Ji
D DAVID PUBLISHING. Uncertainties of in vivo Dosimetry Using Semiconductors. I. Introduction. 2. Methodology
 Journal of Life Sciences 9 (2015) 120-126 doi: 10.17265/1934-7391/2015.03.005 D DAVID PUBLISHING Uncertainties of in vivo Dosimetry Using Semiconductors Zeina Al Kattar, Hanna El Balaa and Saeed Zahran
Journal of Life Sciences 9 (2015) 120-126 doi: 10.17265/1934-7391/2015.03.005 D DAVID PUBLISHING Uncertainties of in vivo Dosimetry Using Semiconductors Zeina Al Kattar, Hanna El Balaa and Saeed Zahran
Guidelines for the use of inversely planned treatment techniques in Clinical Trials: IMRT, VMAT, TomoTherapy
 Guidelines for the use of inversely planned treatment techniques in Clinical Trials: IMRT, VMAT, TomoTherapy VERSION 2.1 April 2015 Table of Contents Abbreviations & Glossary... 3 Executive Summary...
Guidelines for the use of inversely planned treatment techniques in Clinical Trials: IMRT, VMAT, TomoTherapy VERSION 2.1 April 2015 Table of Contents Abbreviations & Glossary... 3 Executive Summary...
Data Collected During Audits for Clinical Trials. July 21, 2010 Geoffrey S. Ibbott, Ph.D. and RPC Staff
 Data Collected During Audits for Clinical Trials July 21, 2010 Geoffrey S. Ibbott, Ph.D. and RPC Staff RPC Programs Assure... Constancy of basic machine calibration (TLD/OSLD Audits) Validity of treatment
Data Collected During Audits for Clinical Trials July 21, 2010 Geoffrey S. Ibbott, Ph.D. and RPC Staff RPC Programs Assure... Constancy of basic machine calibration (TLD/OSLD Audits) Validity of treatment
Concept for quantifying the dose from image guided radiotherapy
 Schneider et al. Radiation Oncology (2015) 10:188 DOI 10.1186/s13014-015-0492-7 RESEARCH Open Access Concept for quantifying the dose from image guided radiotherapy Uwe Schneider 1,2*, Roger Hälg 1,2 and
Schneider et al. Radiation Oncology (2015) 10:188 DOI 10.1186/s13014-015-0492-7 RESEARCH Open Access Concept for quantifying the dose from image guided radiotherapy Uwe Schneider 1,2*, Roger Hälg 1,2 and
Collapsed Cone Convolution 2D illustration
 Collapsed Cone Convolution 2D illustration 8 cones Energy desposition decreases very quickly with distance Energy is absorber in blue pixels only. IGRT1 technologies Paweł Kukołowicz Warsaw, Poland IGRT
Collapsed Cone Convolution 2D illustration 8 cones Energy desposition decreases very quickly with distance Energy is absorber in blue pixels only. IGRT1 technologies Paweł Kukołowicz Warsaw, Poland IGRT
Eric E. Klein, Ph.D. Chair of TG-142
 Eric E. Klein, Ph.D. Chair of TG-142 Professor of Radiation Oncology Washington University St. Louis, MO 2010 AAPM Annual Meeting Med. Phys. 21(4) 1994 Performance-based, comprehensive guidelines for preventing
Eric E. Klein, Ph.D. Chair of TG-142 Professor of Radiation Oncology Washington University St. Louis, MO 2010 AAPM Annual Meeting Med. Phys. 21(4) 1994 Performance-based, comprehensive guidelines for preventing
EORTC Member Facility Questionnaire
 Page 1 of 9 EORTC Member Facility Questionnaire I. Administrative Data Name of person submitting this questionnaire Email address Function Phone Institution Address City Post code Country EORTC No Enter
Page 1 of 9 EORTC Member Facility Questionnaire I. Administrative Data Name of person submitting this questionnaire Email address Function Phone Institution Address City Post code Country EORTC No Enter
Accuracy Requirements and Uncertainty Considerations in Radiation Therapy
 Departments of Oncology and Medical Biophysics Accuracy Requirements and Uncertainty Considerations in Radiation Therapy Introduction and Overview 6 August 2013 Jacob (Jake) Van Dyk Conformality 18 16
Departments of Oncology and Medical Biophysics Accuracy Requirements and Uncertainty Considerations in Radiation Therapy Introduction and Overview 6 August 2013 Jacob (Jake) Van Dyk Conformality 18 16
1. Murphy, Martin J., et al. "The management of imaging dose during image-guided radiotherapy: report of the AAPM Task Group 75.
 1 2 1. Murphy, Martin J., et al. "The management of imaging dose during image-guided radiotherapy: report of the AAPM Task Group 75." Medical physics 34.10 (2007): 4041-4063. 3 1. Murphy, Martin J., et
1 2 1. Murphy, Martin J., et al. "The management of imaging dose during image-guided radiotherapy: report of the AAPM Task Group 75." Medical physics 34.10 (2007): 4041-4063. 3 1. Murphy, Martin J., et
Learning objective. Outline. Acknowledgements. KV CBCT Imaging Part I. R Hammoud AAPM 2008 CE-Therapy (SAM) 1
 1") 1 2 KV CBCT Imaging Part I Rabih Hammoud, MS, DABR Henry Ford Health System Detroit, Michigan Acknowledgements Indrin Chetty, PhD Teamour Nurushev, PhD Harrison Guan, PhD Jinkoo Kim, PhD JianYue Jin, PhD
1 2 KV CBCT Imaging Part I Rabih Hammoud, MS, DABR Henry Ford Health System Detroit, Michigan Acknowledgements Indrin Chetty, PhD Teamour Nurushev, PhD Harrison Guan, PhD Jinkoo Kim, PhD JianYue Jin, PhD
8/2/2018. Disclosure. Online MR-IG-ART Dosimetry and Dose Accumulation
 Online MR-IG-ART Dosimetry and Dose Accumulation Deshan Yang, PhD, Associate Professor Department of Radiation Oncology, School of Medicine Washington University in Saint Louis 1 Disclosure Received research
Online MR-IG-ART Dosimetry and Dose Accumulation Deshan Yang, PhD, Associate Professor Department of Radiation Oncology, School of Medicine Washington University in Saint Louis 1 Disclosure Received research
IGRT1 technologies. Paweł Kukołowicz Warsaw, Poland
 IGRT1 technologies Paweł Kukołowicz Warsaw, Poland Minimal prerequisite for good, efficient radiotherapy ICTP 2015 Paweł Kukołowicz 2/29 Minimal prerequisite for good, efficient radiotherapy Well trained
IGRT1 technologies Paweł Kukołowicz Warsaw, Poland Minimal prerequisite for good, efficient radiotherapy ICTP 2015 Paweł Kukołowicz 2/29 Minimal prerequisite for good, efficient radiotherapy Well trained
Adaptive planning in the context of adaptive radiotherapy
 in the context of adaptive radiotherapy Danilo Pasini Radiotherapy Department Università Cattolica del Sacro Cuore - Rome Zagreb 6/8 November Knowledge Based Oncology Individualizing Modelling Adaptive
in the context of adaptive radiotherapy Danilo Pasini Radiotherapy Department Università Cattolica del Sacro Cuore - Rome Zagreb 6/8 November Knowledge Based Oncology Individualizing Modelling Adaptive
Image Guided in Radiation Therapy (IGRT) Chumpot Kakanaporn Med Phys Radiation Oncology Siriraj Hospital
 Chumpot Kakanaporn Med Phys Radiation Oncology Siriraj Hospital") Image Guided in Radiation Therapy (IGRT) Chumpot Kakanaporn Med Phys Radiation Oncology Siriraj Hospital EBT Process Diagnosis Simulation Tx Planning Tx Verification Tx Delivery X-ray CT MRI NM Patho Process
Image Guided in Radiation Therapy (IGRT) Chumpot Kakanaporn Med Phys Radiation Oncology Siriraj Hospital EBT Process Diagnosis Simulation Tx Planning Tx Verification Tx Delivery X-ray CT MRI NM Patho Process
IMRT QA: Point Dose Measurements or 2D Array?
 QA for IMRT IMRT QA: Point Dose Measurements or D Array? General Linac QA for IMRT MLC checks Dose linearity at low MU Patient-specific measurements Performed using various methods Purpose is to verify
QA for IMRT IMRT QA: Point Dose Measurements or D Array? General Linac QA for IMRT MLC checks Dose linearity at low MU Patient-specific measurements Performed using various methods Purpose is to verify
Feasibility of portal dosimetry for flattening filter-free radiotherapy
 JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 17, NUMBER 1, 2016 Feasibility of portal dosimetry for flattening filter-free radiotherapy Robert W. Chuter, a Philip A. Rixham, Steve J. Weston and
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 17, NUMBER 1, 2016 Feasibility of portal dosimetry for flattening filter-free radiotherapy Robert W. Chuter, a Philip A. Rixham, Steve J. Weston and
Albert Lisbona Medical Physics Department CLCC Nantes Atlantique a
 The Equipment : safety, commissioning, re commissioning calibration : Equipements : sûreté, recette, modification calibration A medical physicist point of view. Albert Lisbona Medical Physics Department
The Equipment : safety, commissioning, re commissioning calibration : Equipements : sûreté, recette, modification calibration A medical physicist point of view. Albert Lisbona Medical Physics Department
An anthropomorphic head phantom with a BANG polymer gel insert for dosimetric evaluation of IMRT treatment delivery
 An anthropomorphic head phantom with a BANG polymer gel insert for dosimetric evaluation of IMRT treatment delivery G. Ibbott a, M. Beach a, M. Maryanski b a M.D. Anderson Cancer Center, Houston, Texas,
An anthropomorphic head phantom with a BANG polymer gel insert for dosimetric evaluation of IMRT treatment delivery G. Ibbott a, M. Beach a, M. Maryanski b a M.D. Anderson Cancer Center, Houston, Texas,
I. Equipments for external beam radiotherapy
 I. Equipments for external beam radiotherapy 5 linear accelerators (LINACs): Varian TrueBeam 6, 10 & 18 MV photons, 6-18 MeV electrons, image-guided (IGRT) and intensity modulated radiotherapy (IMRT),
I. Equipments for external beam radiotherapy 5 linear accelerators (LINACs): Varian TrueBeam 6, 10 & 18 MV photons, 6-18 MeV electrons, image-guided (IGRT) and intensity modulated radiotherapy (IMRT),
What do we Know About Adaptive Radiotherapy? Lei Dong, Ph.D. Scripps Proton Therapy Center San Diego, California
 What do we Know About Adaptive Radiotherapy? Lei Dong, Ph.D. Scripps Proton Therapy Center San Diego, California AAMD Region II Meeting Houston, Texas September 13-14, 2012 Learning Objectives To gain
What do we Know About Adaptive Radiotherapy? Lei Dong, Ph.D. Scripps Proton Therapy Center San Diego, California AAMD Region II Meeting Houston, Texas September 13-14, 2012 Learning Objectives To gain
The RPC s Evaluation of Advanced Technologies. AAPM Refresher Course July 29, 2008 Geoffrey S. Ibbott, Ph.D. and RPC Staff
 The RPC s Evaluation of Advanced Technologies AAPM Refresher Course July 29, 2008 Geoffrey S. Ibbott, Ph.D. and RPC Staff 1 http://rpc.mdanderson.org Supported by: NCI grants CA10953 and CA81647, and an
The RPC s Evaluation of Advanced Technologies AAPM Refresher Course July 29, 2008 Geoffrey S. Ibbott, Ph.D. and RPC Staff 1 http://rpc.mdanderson.org Supported by: NCI grants CA10953 and CA81647, and an
PHYS 383: Applications of physics in medicine (offered at the University of Waterloo from Jan 2015)
") PHYS 383: Applications of physics in medicine (offered at the University of Waterloo from Jan 2015) Course Description: This course is an introduction to physics in medicine and is intended to introduce
PHYS 383: Applications of physics in medicine (offered at the University of Waterloo from Jan 2015) Course Description: This course is an introduction to physics in medicine and is intended to introduce
CURRICULUM OUTLINE FOR TRANSITIONING FROM 2-D RT TO 3-D CRT AND IMRT
 CURRICULUM OUTLINE FOR TRANSITIONING FROM 2-D RT TO 3-D CRT AND IMRT Purpose The purpose of this curriculum outline is to provide a framework for multidisciplinary training for radiation oncologists, medical
CURRICULUM OUTLINE FOR TRANSITIONING FROM 2-D RT TO 3-D CRT AND IMRT Purpose The purpose of this curriculum outline is to provide a framework for multidisciplinary training for radiation oncologists, medical
IMRT/IGRT Patient Treatment: A Community Hospital Experience. Charles M. Able, Assistant Professor
 IMRT/IGRT Patient Treatment: A Community Hospital Experience Charles M. Able, Assistant Professor Disclosures I have no research support or financial interest to disclose. Learning Objectives 1. Review
IMRT/IGRT Patient Treatment: A Community Hospital Experience Charles M. Able, Assistant Professor Disclosures I have no research support or financial interest to disclose. Learning Objectives 1. Review
EXACTRAC HIGHLY ACCURATE PATIENT MONITORING
 EXACTRAC HIGHLY ACCURATE PATIENT MONITORING PATIENT POSITION MONITORING ExacTrac is an in-room based monitoring system that detects intrafractional motion during treatment delivery. Two kv X-Ray units
EXACTRAC HIGHLY ACCURATE PATIENT MONITORING PATIENT POSITION MONITORING ExacTrac is an in-room based monitoring system that detects intrafractional motion during treatment delivery. Two kv X-Ray units
Verification of treatment planning system parameters in tomotherapy using EBT Radiochromic Film
 Verification of treatment planning system parameters in tomotherapy using EBT Radiochromic Film E.B.Rajmohan¹, Pratik Kumar¹, Bhudatt Paliwal,² David Westerly², N.Gopishankar³, R.K.Bisht³, D.Tewatia²,
Verification of treatment planning system parameters in tomotherapy using EBT Radiochromic Film E.B.Rajmohan¹, Pratik Kumar¹, Bhudatt Paliwal,² David Westerly², N.Gopishankar³, R.K.Bisht³, D.Tewatia²,
CHAPTER 5. STUDY OF ANGULAR RESPONSE OF asi 1000 EPID AND IMATRIXX 2-D ARRAY SYSTEM FOR IMRT PATIENT SPECIFIC QA
 CHAPTER 5 STUDY OF ANGULAR RESPONSE OF asi 1000 EPID AND IMATRIXX 2-D ARRAY SYSTEM FOR IMRT PATIENT SPECIFIC QA 5.1 Introduction With the advent of new techniques like intensity modulated radiotherapy
CHAPTER 5 STUDY OF ANGULAR RESPONSE OF asi 1000 EPID AND IMATRIXX 2-D ARRAY SYSTEM FOR IMRT PATIENT SPECIFIC QA 5.1 Introduction With the advent of new techniques like intensity modulated radiotherapy
Feasibility study on effect and stability of adaptive radiotherapy on kilovoltage cone beam CT
 220 research article Feasibility study on effect and stability of adaptive radiotherapy on kilovoltage cone beam CT Poonam Yadav 1,2,3, Velayudham Ramasubramanian 3, Bhudatt R. Paliwal 1,2 1 Department
220 research article Feasibility study on effect and stability of adaptive radiotherapy on kilovoltage cone beam CT Poonam Yadav 1,2,3, Velayudham Ramasubramanian 3, Bhudatt R. Paliwal 1,2 1 Department
Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer?
 Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer? Dimos Baltas Dept. of Medical Physics & Engineering, Strahlenklinik, Klinikum Offenbach GmbH 63069 Offenbach, Germany
Can we deliver the dose distribution we plan in HDR-Brachytherapy of Prostate Cancer? Dimos Baltas Dept. of Medical Physics & Engineering, Strahlenklinik, Klinikum Offenbach GmbH 63069 Offenbach, Germany
THE TRANSITION FROM 2D TO 3D AND TO IMRT - RATIONALE AND CRITICAL ELEMENTS
 THE TRANSITION FROM 2D TO 3D AND TO IMRT - RATIONALE AND CRITICAL ELEMENTS ICTP SCHOOL ON MEDICAL PHYSICS FOR RADIATION THERAPY DOSIMETRY AND TREATMENT PLANNING FOR BASIC AND ADVANCED APPLICATIONS March
THE TRANSITION FROM 2D TO 3D AND TO IMRT - RATIONALE AND CRITICAL ELEMENTS ICTP SCHOOL ON MEDICAL PHYSICS FOR RADIATION THERAPY DOSIMETRY AND TREATMENT PLANNING FOR BASIC AND ADVANCED APPLICATIONS March
The Radixact System Experience at Miami Cancer Institute. Tino Romaguera, D.Sc. Senior Physicist
 The Radixact System Experience at Miami Cancer Institute Tino Romaguera, D.Sc. Senior Physicist Disclosure An honorarium is provided by Accuray for this presentation The views expressed in this presentation
The Radixact System Experience at Miami Cancer Institute Tino Romaguera, D.Sc. Senior Physicist Disclosure An honorarium is provided by Accuray for this presentation The views expressed in this presentation
Managing the imaging dose during image-guided radiation therapy
 Managing the imaging dose during image-guided radiation therapy Martin J Murphy PhD Department of Radiation Oncology Virginia Commonwealth University Richmond VA Imaging during radiotherapy Radiographic
Managing the imaging dose during image-guided radiation therapy Martin J Murphy PhD Department of Radiation Oncology Virginia Commonwealth University Richmond VA Imaging during radiotherapy Radiographic
Abstract: A National Project for the in-vivo dosimetry in radiotherapy: first results
 Abstract: A National Project for the in-vivo dosimetry in radiotherapy: first results A.Piermattei 1, L. Azario 1, S. Cilla 2, A.Fidanzio 1, F.Greco 1, M.T.Russo 3, S. Zucca 4 1 Istituto di Fisica e Unità
Abstract: A National Project for the in-vivo dosimetry in radiotherapy: first results A.Piermattei 1, L. Azario 1, S. Cilla 2, A.Fidanzio 1, F.Greco 1, M.T.Russo 3, S. Zucca 4 1 Istituto di Fisica e Unità
Quality assurance and credentialing requirements for sites using inverse planned IMRT Techniques
 TROG 08.03 RAVES Quality assurance and credentialing requirements for sites using inverse planned IMRT Techniques Introduction Commissioning and quality assurance of planning systems and treatment delivery
TROG 08.03 RAVES Quality assurance and credentialing requirements for sites using inverse planned IMRT Techniques Introduction Commissioning and quality assurance of planning systems and treatment delivery
Margins in SBRT. Mischa Hoogeman
 Margins in SBRT Mischa Hoogeman MARGIN CONCEPTS Why do we use margins? Target / tumor To a-priori compensate for (unknown) deviations between the intended target position and the real target position during
Margins in SBRT Mischa Hoogeman MARGIN CONCEPTS Why do we use margins? Target / tumor To a-priori compensate for (unknown) deviations between the intended target position and the real target position during
SRS Uncertainty: Linac and CyberKnife Uncertainties
 SRS Uncertainty: Linac and CyberKnife Uncertainties Sonja Dieterich, PhD Linac/CyberKnife Technological Uncertainties 1 Linac Mechanical/Radiation Isocenters Depuydt, Tom, et al. "Computer aided analysis
SRS Uncertainty: Linac and CyberKnife Uncertainties Sonja Dieterich, PhD Linac/CyberKnife Technological Uncertainties 1 Linac Mechanical/Radiation Isocenters Depuydt, Tom, et al. "Computer aided analysis
Implementation of advanced RT Techniques
 Implementation of advanced RT Techniques Tibor Major, PhD National Institute of Oncology Budapest, Hungary 2. Kongres radiološke tehnologije, Vukovar, 23-25. September 2016. Current RT equipments at NIO,
Implementation of advanced RT Techniques Tibor Major, PhD National Institute of Oncology Budapest, Hungary 2. Kongres radiološke tehnologije, Vukovar, 23-25. September 2016. Current RT equipments at NIO,
Evaluating Pre-Treatment IMRT & VMAT QA Techniques Using Receiver Operating. Characteristic (ROC) Analysis. Allison Lorraine Mitchell
 Analysis. Allison Lorraine Mitchell") Evaluating Pre-Treatment IMRT & VMAT QA Techniques Using Receiver Operating Characteristic (ROC) Analysis by Allison Lorraine Mitchell Graduate Program in Medical Physics Duke University Date: Approved:
Evaluating Pre-Treatment IMRT & VMAT QA Techniques Using Receiver Operating Characteristic (ROC) Analysis by Allison Lorraine Mitchell Graduate Program in Medical Physics Duke University Date: Approved:
Intensity Modulated Radiation Therapy: Dosimetric Aspects & Commissioning Strategies
 Intensity Modulated Radiation Therapy: Dosimetric Aspects & Commissioning Strategies ICPT School on Medical Physics for Radiation Therapy Justus Adamson PhD Assistant Professor Department of Radiation
Intensity Modulated Radiation Therapy: Dosimetric Aspects & Commissioning Strategies ICPT School on Medical Physics for Radiation Therapy Justus Adamson PhD Assistant Professor Department of Radiation
SBRT Credentialing: Understanding the Process from Inquiry to Approval
 SBRT Credentialing: Understanding the Process from Inquiry to Approval David Followill, Ph.D. (presented by Andrea Molineu, M.S.) IROC Houston QA Center July 15, 2015 What is credentialing? Verification
SBRT Credentialing: Understanding the Process from Inquiry to Approval David Followill, Ph.D. (presented by Andrea Molineu, M.S.) IROC Houston QA Center July 15, 2015 What is credentialing? Verification
A Dosimetric study of different MLC expansion aperture For the radiotherapy of pancreas cancer
 IOSR Journal of Applied Physics (IOSR-JAP) e-issn: 2278-861.Volume 6, Issue Ver. II (May-Jun. 201), PP 2- A Dosimetric study of different MLC expansion aperture For the radiotherapy of pancreas cancer
IOSR Journal of Applied Physics (IOSR-JAP) e-issn: 2278-861.Volume 6, Issue Ver. II (May-Jun. 201), PP 2- A Dosimetric study of different MLC expansion aperture For the radiotherapy of pancreas cancer
Dosisverifikation mit Delta 4 Discover während der Behandlung
 Dosisverifikation mit Delta 4 Discover während der Behandlung Anders Adolfson, Regional Sales Manager at Scandidos AK IMRT 2015 in Erlangen, March 19 th 2015 Agenda Which problem does Delta 4 Discover
Dosisverifikation mit Delta 4 Discover während der Behandlung Anders Adolfson, Regional Sales Manager at Scandidos AK IMRT 2015 in Erlangen, March 19 th 2015 Agenda Which problem does Delta 4 Discover
Overview of TG225 - Medical Physics Practice Guideline #1
 Overview of TG225 - Medical Physics Practice Guideline #1 Evaluation and quality assurance of x-ray based image guided radiotherapy systems Jonas Fontenot, Ph.D. MPPG #1 Evaluation and Quality Assurance
Overview of TG225 - Medical Physics Practice Guideline #1 Evaluation and quality assurance of x-ray based image guided radiotherapy systems Jonas Fontenot, Ph.D. MPPG #1 Evaluation and Quality Assurance
WHOLE-BRAIN RADIOTHERAPY WITH SIMULTANEOUS INTEGRATED BOOST TO MULTIPLE BRAIN METASTASES USING VOLUMETRIC MODULATED ARC THERAPY
 doi:10.1016/j.ijrobp.2009.03.029 Int. J. Radiation Oncology Biol. Phys., Vol. 75, No. 1, pp. 253 259, 2009 Copyright Ó 2009 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/09/$ see front
doi:10.1016/j.ijrobp.2009.03.029 Int. J. Radiation Oncology Biol. Phys., Vol. 75, No. 1, pp. 253 259, 2009 Copyright Ó 2009 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/09/$ see front
In-Room Radiographic Imaging for Localization
 In-Room Radiographic Imaging for Localization Fang-Fang Yin, Zhiheng Wang, Sua Yoo, Devon Godfrey, Q.-R. Jackie Wu Department of Radiation Oncology Duke University Medical Center Durham, North Carolina
In-Room Radiographic Imaging for Localization Fang-Fang Yin, Zhiheng Wang, Sua Yoo, Devon Godfrey, Q.-R. Jackie Wu Department of Radiation Oncology Duke University Medical Center Durham, North Carolina
Implementing New Technologies for Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy
 Implementing New Technologies for Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy Implementation of radiosurgery and SBRT requires a fundamentally sound approach Errors don t blur out
Implementing New Technologies for Stereotactic Radiosurgery and Stereotactic Body Radiation Therapy Implementation of radiosurgery and SBRT requires a fundamentally sound approach Errors don t blur out
Measure the Errors of Treatment Set-Ups of Prostate Cancer Patient Using Electronic Portal Imaging Device (EPID)
") IOSR Journal of Applied Physics (IOSR-JAP) e-issn: 2278-4861.Volume 10, Issue 2 Ver. I (Mar. Apr. 2018), PP 55-59 www.iosrjournals.org Measure the Errors of Treatment Set-Ups of Prostate Cancer Patient
IOSR Journal of Applied Physics (IOSR-JAP) e-issn: 2278-4861.Volume 10, Issue 2 Ver. I (Mar. Apr. 2018), PP 55-59 www.iosrjournals.org Measure the Errors of Treatment Set-Ups of Prostate Cancer Patient
REPLACING PRETREATMENT VERIFICATION WITH IN VIVO EPID DOSIMETRY FOR PROSTATE IMRT
 doi:10.1016/j.ijrobp.2006.11.047 Int. J. Radiation Oncology Biol. Phys., Vol. 67, No. 5, pp. 1568 1577, 2007 Copyright 2007 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/07/$ see front
doi:10.1016/j.ijrobp.2006.11.047 Int. J. Radiation Oncology Biol. Phys., Vol. 67, No. 5, pp. 1568 1577, 2007 Copyright 2007 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/07/$ see front
Clinical Implications Of Dose Summation And Adaptation
 Clinical Implications Of Dose Summation And Adaptation Patrick Kupelian, M.D. Professor and Vice Chair University of California Los Angeles Department of Radiation Oncology pkupelian@mednet.ucla.edu August
Clinical Implications Of Dose Summation And Adaptation Patrick Kupelian, M.D. Professor and Vice Chair University of California Los Angeles Department of Radiation Oncology pkupelian@mednet.ucla.edu August
7/10/2015. Acknowledgments. Institution-specific TG-142? AAPM:Task Group-142. Failure-Mode & Effects Analysis
 Acknowledgments Thanks to Saiful Huq for an illuminating conversation about the application of TG-100 Jennifer O Daniel, Ph.D. & Fang-Fang Yin, Ph.D. Duke University Medical Center Annual AAPM Meeting,
Acknowledgments Thanks to Saiful Huq for an illuminating conversation about the application of TG-100 Jennifer O Daniel, Ph.D. & Fang-Fang Yin, Ph.D. Duke University Medical Center Annual AAPM Meeting,
Objective. Evaluation of Linear Accelerator Performance Standards using an Outcome Oriented Approach. Linac performance standards*
 Quality in Radiation Therapy: what is it and how do you achieve it?. Overview of definitions and approaches to Quality Pawlicki. ROSIS Knöö öös. Peer Review Quality Audits Halvorsen. The Regulator s s
Quality in Radiation Therapy: what is it and how do you achieve it?. Overview of definitions and approaches to Quality Pawlicki. ROSIS Knöö öös. Peer Review Quality Audits Halvorsen. The Regulator s s
IGRT Protocol Design and Informed Margins. Conflict of Interest. Outline 7/7/2017. DJ Vile, PhD. I have no conflict of interest to disclose
 IGRT Protocol Design and Informed Margins DJ Vile, PhD Conflict of Interest I have no conflict of interest to disclose Outline Overview and definitions Quantification of motion Influences on margin selection
IGRT Protocol Design and Informed Margins DJ Vile, PhD Conflict of Interest I have no conflict of interest to disclose Outline Overview and definitions Quantification of motion Influences on margin selection
Varian Edge Experience. Jinkoo Kim, Ph.D Henry Ford Health System
 Varian Edge Experience Jinkoo Kim, Ph.D Henry Ford Health System Disclosures I participate in research funded by Varian Medical Systems. Outline of Presentation Review advanced imaging in Varian Edge Linear
Varian Edge Experience Jinkoo Kim, Ph.D Henry Ford Health System Disclosures I participate in research funded by Varian Medical Systems. Outline of Presentation Review advanced imaging in Varian Edge Linear
Clinical evaluation of interfractional variations for whole breast radiotherapy using 3-dimensional surface imaging
 Practical Radiation Oncology (2013) 3, 16 25 www.practicalradonc.org Original Report Clinical evaluation of interfractional variations for whole breast radiotherapy using 3-dimensional surface imaging
Practical Radiation Oncology (2013) 3, 16 25 www.practicalradonc.org Original Report Clinical evaluation of interfractional variations for whole breast radiotherapy using 3-dimensional surface imaging
QA for Clinical Dosimetry with Emphasis on Clinical Trials
 QA for Clinical Dosimetry with Emphasis on Clinical Trials Geoffrey S. Ibbott, Ph.D. and RPC Staff G. Ibbott, AAPM Summer School, June 24, 2009 1 QA Infrastructure for Clinical Trials Participating Institutions
QA for Clinical Dosimetry with Emphasis on Clinical Trials Geoffrey S. Ibbott, Ph.D. and RPC Staff G. Ibbott, AAPM Summer School, June 24, 2009 1 QA Infrastructure for Clinical Trials Participating Institutions
Helical Tomotherapy Experience. TomoTherapy Whole Brain Head & Neck Prostate Lung Summary. HI-ART TomoTherapy System. HI-ART TomoTherapy System
 The Challenges Associated with Differential Dose Delivery using IMRT Chester Ramsey, Ph.D. Director of Medical Physics Thompson Cancer Center Knoxville, Tennessee, U.S.A Collaborators Chester Ramsey, Ph.D.
The Challenges Associated with Differential Dose Delivery using IMRT Chester Ramsey, Ph.D. Director of Medical Physics Thompson Cancer Center Knoxville, Tennessee, U.S.A Collaborators Chester Ramsey, Ph.D.
Limits of Precision and Accuracy of Radiation Delivery Systems
 Limits of Precision and Accuracy of Radiation Delivery Systems Jean M. Moran, Ph.D. 1 and Timothy Ritter, Ph.D. 2 1 University of Michigan, Ann Arbor, Michigan 2 Ann Arbor Veterans Affairs Hospital, Ann
Limits of Precision and Accuracy of Radiation Delivery Systems Jean M. Moran, Ph.D. 1 and Timothy Ritter, Ph.D. 2 1 University of Michigan, Ann Arbor, Michigan 2 Ann Arbor Veterans Affairs Hospital, Ann
Risk-based QM for Incorrect Isocenter at Day 1 Setup. TG 100 risk based QM development Process Mapping
 Risk-based QM for Incorrect Isocenter at Day 1 Setup Ellen Yorke Memorial Sloan Kettering Cancer Center TG 100 risk based QM development Process Mapping Failure Modes and Effects Detect Fault Tree Analysis
Risk-based QM for Incorrect Isocenter at Day 1 Setup Ellen Yorke Memorial Sloan Kettering Cancer Center TG 100 risk based QM development Process Mapping Failure Modes and Effects Detect Fault Tree Analysis
MEDICAL PHYSICS INTERNATIONAL Journal, vol.3, No.2, 2015 HOW TO
 HOW TO QUALITY CONTROL AND PRE-TREATMENT QUALITY ASSURANCE APPLICATION OF EPID (as1000) FOR FF AND FFF BEAM VMAT PLANS Y. Mekuria 1, M. Bjorkqvist 1, J. Kulmala 1 1 Turku University Hospital/Radiotherapy
HOW TO QUALITY CONTROL AND PRE-TREATMENT QUALITY ASSURANCE APPLICATION OF EPID (as1000) FOR FF AND FFF BEAM VMAT PLANS Y. Mekuria 1, M. Bjorkqvist 1, J. Kulmala 1 1 Turku University Hospital/Radiotherapy
Work partially supported by VisionRT
 Work partially supported by VisionRT Background of frameless intracranial stereotactic radiosurgery UCSD SRS/SRT procedure Clinical Results Summary Total prescribed doses : order of 10 50 Gy Planning targets
Work partially supported by VisionRT Background of frameless intracranial stereotactic radiosurgery UCSD SRS/SRT procedure Clinical Results Summary Total prescribed doses : order of 10 50 Gy Planning targets
Patient and Linac QA - present and the future
 Patient and Linac QA - present and the future IBA Dosimetry Sandra Kos Service Department Customer Support Specialist sandra.kos@iba-group.com 1 IBA Dosimetry Part of IBA Group OUR MISSION At IBA we dare
Patient and Linac QA - present and the future IBA Dosimetry Sandra Kos Service Department Customer Support Specialist sandra.kos@iba-group.com 1 IBA Dosimetry Part of IBA Group OUR MISSION At IBA we dare
Contributors to this Talk
 Tomotherapy Thomas Rockwell Mackie Tomotherapy Research Group Depts. Of Medical Physics, Human Oncology and Biomedical Engineering University of Wisconsin Madison WI 53706 Phone: (608) 262-7358 Email:
Tomotherapy Thomas Rockwell Mackie Tomotherapy Research Group Depts. Of Medical Physics, Human Oncology and Biomedical Engineering University of Wisconsin Madison WI 53706 Phone: (608) 262-7358 Email:
In-Room Radiographic Imaging for Localization
 In-Room Radiographic Imaging for Localization Fang-Fang Yin, Zhiheng Wang, Sua Yoo, Devon Godfrey, Q.-R. Jackie Wu Department of Radiation Oncology Duke University Medical Center Durham, North Carolina
In-Room Radiographic Imaging for Localization Fang-Fang Yin, Zhiheng Wang, Sua Yoo, Devon Godfrey, Q.-R. Jackie Wu Department of Radiation Oncology Duke University Medical Center Durham, North Carolina
Image Registration for Radiation Therapy Applications: Part 2: In-room Volumetric Imaging
 Image Registration for Radiation Therapy Applications: Part 2: In-room Volumetric Imaging Peter Balter Ph.D University of Texas M.D. Anderson Cancer Center Houston, TX, USA Disclosure Information Peter
Image Registration for Radiation Therapy Applications: Part 2: In-room Volumetric Imaging Peter Balter Ph.D University of Texas M.D. Anderson Cancer Center Houston, TX, USA Disclosure Information Peter
Clinical Implementation of a New Ultrasound Guidance System. Vikren Sarkar Bill Salter Martin Szegedi
 Clinical Implementation of a New Ultrasound Guidance System Vikren Sarkar Bill Salter Martin Szegedi Disclosure The University of Utah has research agreements with Elekta Agenda Historical Review Trans-Abdominal
Clinical Implementation of a New Ultrasound Guidance System Vikren Sarkar Bill Salter Martin Szegedi Disclosure The University of Utah has research agreements with Elekta Agenda Historical Review Trans-Abdominal
Horizon Scanning Technology Briefing National Helical Tomotherapy Horizon Hi-ART System for Scanning external cancer Centre radiotherapy August 2006
 Horizon Scanning Technology Briefing National Horizon Scanning Centre Helical Tomotherapy Hi-ART System for external cancer radiotherapy August 2006 This technology briefing is based on information available
Horizon Scanning Technology Briefing National Horizon Scanning Centre Helical Tomotherapy Hi-ART System for external cancer radiotherapy August 2006 This technology briefing is based on information available
Use of Bubble Detectors to Characterize Neutron Dose Distribution in a Radiotherapy Treatment Room used for IMRT treatments
 Use of Bubble Detectors to Characterize Neutron Dose Distribution in a Radiotherapy Treatment Room used for IMRT treatments Alana Hudson *1 1 Tom Baker Cancer Centre, Department of Medical Physics, 1331
Use of Bubble Detectors to Characterize Neutron Dose Distribution in a Radiotherapy Treatment Room used for IMRT treatments Alana Hudson *1 1 Tom Baker Cancer Centre, Department of Medical Physics, 1331
A VMAT PLANNING SOLUTION FOR NECK CANCER PATIENTS USING THE PINNACLE 3 PLANNING SYSTEM *
 Romanian Reports in Physics, Vol. 66, No. 2, P. 401 410, 2014 A VMAT PLANNING SOLUTION FOR NECK CANCER PATIENTS USING THE PINNACLE 3 PLANNING SYSTEM * M. D. SUDITU 1,2, D. ADAM 1,2, R. POPA 1,2, V. CIOCALTEI
Romanian Reports in Physics, Vol. 66, No. 2, P. 401 410, 2014 A VMAT PLANNING SOLUTION FOR NECK CANCER PATIENTS USING THE PINNACLE 3 PLANNING SYSTEM * M. D. SUDITU 1,2, D. ADAM 1,2, R. POPA 1,2, V. CIOCALTEI
Portal dosimetry in wedged beams
 JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 16, NUMBER 3, 2015 Portal dosimetry in wedged beams Hanno Spreeuw, 1 Roel Rozendaal, 1 Priscilla Camargo, 1,2 Anton Mans, 1 Markus Wendling, 1,3 Igor
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 16, NUMBER 3, 2015 Portal dosimetry in wedged beams Hanno Spreeuw, 1 Roel Rozendaal, 1 Priscilla Camargo, 1,2 Anton Mans, 1 Markus Wendling, 1,3 Igor
Radiosurgery. Most Important! 8/2/2012. Stereotactic Radiosurgery: State of the Art Technology and Implementation Linear Accelerator Radiosurgery
 Therapy SAM Symposium: WE-A-BRCD-1 Stereotactic Radiosurgery: State of the Art Technology and Implementation Linear Accelerator Radiosurgery Kamil M. Yenice, PhD Associate Professor Chief of Clinical Physics
Therapy SAM Symposium: WE-A-BRCD-1 Stereotactic Radiosurgery: State of the Art Technology and Implementation Linear Accelerator Radiosurgery Kamil M. Yenice, PhD Associate Professor Chief of Clinical Physics
The MapCHECK Measurement Uncertainty function and its effect on planar dose pass rates
 JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 17, NUMBER 2, 2016 The MapCHECK Measurement Uncertainty function and its effect on planar dose pass rates Daniel W. Bailey, 1,2 a Jason D. Spaans, 2
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 17, NUMBER 2, 2016 The MapCHECK Measurement Uncertainty function and its effect on planar dose pass rates Daniel W. Bailey, 1,2 a Jason D. Spaans, 2
Assessing Heterogeneity Correction Algorithms Using the Radiological Physics Center Anthropomorphic Thorax Phantom
 Assessing Heterogeneity Correction Algorithms Using the Radiological Physics Center Anthropomorphic Thorax Phantom David Followill, Ph.D. Associate Director Radiological Physics Center RPC History Lesson
Assessing Heterogeneity Correction Algorithms Using the Radiological Physics Center Anthropomorphic Thorax Phantom David Followill, Ph.D. Associate Director Radiological Physics Center RPC History Lesson
UCLA UCLA UCLA 7/10/2015. The need for MRI in radiotherapy. Multiparametric MRI reflects a more complete picture of the tumor biology
 Ke Sheng, Ph.D., DABR Professor of Radiation Oncology University of California, Los Angeles The need for MRI in radiotherapy T1 FSE CT Tumor and normal tissues in brain, breast, head and neck, liver, prostate,
Ke Sheng, Ph.D., DABR Professor of Radiation Oncology University of California, Los Angeles The need for MRI in radiotherapy T1 FSE CT Tumor and normal tissues in brain, breast, head and neck, liver, prostate,
Feasibility of improving cone-beam CT number consistency using a scatter correction algorithm.
 Thomas Jefferson University Jefferson Digital Commons Department of Medicine Faculty Papers Department of Medicine 11-4-2013 Feasibility of improving cone-beam CT number consistency using a scatter correction
Thomas Jefferson University Jefferson Digital Commons Department of Medicine Faculty Papers Department of Medicine 11-4-2013 Feasibility of improving cone-beam CT number consistency using a scatter correction
ADVANCES IN RADIATION TECHNOLOGIES IN THE TREATMENT OF CANCER
 ADVANCES IN RADIATION TECHNOLOGIES IN THE TREATMENT OF CANCER Bro. Dr. Collie Miller IARC/WHO Based on trends in the incidence of cancer, the International Agency for Research on Cancer (IARC) and WHO
ADVANCES IN RADIATION TECHNOLOGIES IN THE TREATMENT OF CANCER Bro. Dr. Collie Miller IARC/WHO Based on trends in the incidence of cancer, the International Agency for Research on Cancer (IARC) and WHO
Gamma analysis dependence on specified low-dose thresholds for VMAT QA
 JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 16, NUMBER 6, 2015 Gamma analysis dependence on specified low-dose thresholds for VMAT QA Ji-Hye Song, 1 Min-Joo Kim, 1 So-Hyun Park, 1,2 Seu-Ran Lee,
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 16, NUMBER 6, 2015 Gamma analysis dependence on specified low-dose thresholds for VMAT QA Ji-Hye Song, 1 Min-Joo Kim, 1 So-Hyun Park, 1,2 Seu-Ran Lee,
Application of asi-kvcbct for Volume Assessment and Dose Estimation: An Offline Adaptive Study for Prostate Radiotherapy
 DOI:10.31557/APJCP.2019.20.1.229 Volume and Dose Assessment on Adapted CT RESEARCH ARTICLE Editorial Process: Submission:08/10/2018 Acceptance:01/05/2019 Application of asi-kvcbct for Volume Assessment
DOI:10.31557/APJCP.2019.20.1.229 Volume and Dose Assessment on Adapted CT RESEARCH ARTICLE Editorial Process: Submission:08/10/2018 Acceptance:01/05/2019 Application of asi-kvcbct for Volume Assessment