Parenchyma saving resectionsfictions. (Colorectal liver metastasis)
|
|
|
- Sibyl Gray
- 5 years ago
- Views:
Transcription
 Bjørn Edwin, professor, MD, PhD Section manager, Clinical Research The Interventional")
1 Parenchyma saving resectionsfictions or facts? (Colorectal liver metastasis) Bjørn Edwin, professor, MD, PhD Section manager, Clinical Research The Interventional Center and HPB-Department Oslo University Hospital, Rikshospitalet Oslo, Norway
 N =643 643 pat.")
 approx.")
2 Lap. liver resections Total laparoscopic experience (1998- Aug.2014) N = pat., 713 procedures Re-resections: 101 procedures (31 afteropensurgeryand 70 procedures after laparoscopy) approx. 60% colorectal metastases 35 HCC patients 2


3 Whatis parenchyma/parenchymal sparing/savingresection/technique (PST) Definition: A technique sparsely described in the literature A resection that removes the metastasis without compromising cancer-related outcome, sparing as much healthy parenchyma as possible What is gold standard in 2014 formal or parenchyma sparing? Differs from surgeon, country, culture, disease
 Painter Pieter Paul Rubens 530")
4 Minimal invasiv surgery, Re-generation Parenchyma sparing technique was described very early Zevseagle eating a part of Prometheus liver every day but during the night it re-generated (Greek Mythology) Painter Pieter Paul Rubens 530 BC
5 PST Resection Reduce numbers of segments e.g. seg. 6/7 instead of formal right side hemihepatectomy Atypical, local, wedge resection What about local ablations: Cryo, RF, Nanoknife, Microwave, HIFU etc.
6 Why Parenchymasavingresections?
7 Short introduction: Treatmentof liver metastasis from colorectal cancer
8 Resectability 10-30%of all pat.withliver metastasis from colorectal cancer is potential candidates for curative liver resections 1,2 1 McArterMD/ Fong Y. SemSurgOncol2000; 19: Scheele J. Br J Surg1993; 80:
9 Survival without operation metastasis from colorectal cancer Chemotherapy (overall survival) FOLFIRI/FO LFOX FOLFOX/FOL FIRI median survival of months Median (month) Events/patie nts [ ] [ ] 65/109 67/111 Median followup 18.6 months
10 Survival 5 years Open / Laparoscopic liver resection First authors, year Country No. of patients 3-year overall survival, % 5-year overall survival, % First authors, year Country Number of patients 3-year overall survival, % 5-year overall survival, % Ito et al, 2008 USA 1, Nguyen et al, 2009 Multicentre study: USA, France Blazer et al, 2008 USA Kazaryan et al, 2010 Norway Adam et al, 2008 France, Netherla nds Casting et al, 2009 Twocentre study: France Zakaria et al, 2007 USA Vibertet al, 2006 Sasaki et al, 2009 France Japan
11 Open/Laparoscopic re-resections Publication Fong et al, 1994 Nordlinger et al, 1994 No of patients Perioperat ive mortality (%) Survival 5 years (%) Survival 10 years (%) (mean) ,9-33 Fernandez Trigo et al, 1995 Scheele et al, 1996 Adam et al, 1997 Yamamolo et al, 1997 Petrowsky et al, 2002 Shaw et al, , First authors, year Shafaee et al, 2011 Country Tricentre study: France, Norway, USA No. of pts 3-year overall surviva l, % 5-year overall surviva l, % 55 * Is Laparoscopic Repeat Hepatectomy Feasible? A Tri-institutional Analysis Zahra Shafaee 1, AirazatM. Kazaryan 2, M. Marvin 3,K. Ravindra 3, Joseph F. Buell 3, BjørnEdwin 2, Brice Gayet 1. J Am Coll Surg Feb;212(2):171-9.


12 Treatment have changed to a more aggressive approach
13 Multimodal vs. classic approach "Classical" approach Multimodal treatment (more aggressive approach) Colorectal liver metastases Colorectal liver metastases Neoadjuvant chemotherapy (downstaging)? Conventional resection, Formal hepatectomy Portal vein embolisation? Two stage hepatectomy? Resection and/or ablation Parenchymal sparing surgery Repeated resection? Adjuvant chemotherapy? Lung / adrenal metastases - resection? Re-resection/ ablation Palliative chemotherapy Chemotherapy Re-evaluation if responce
14 Multimodal treatment in patients with colorectal metastasis. Change a the situation from a disease with a relatively short life expectancy, to a chronic disease with the possibility to live many years extra (B.Edwin)---personal opinion
15
16 Planning both before and during the operation
17
18
19 19
20
21 Parenchyma sparing techniques Decreased morbidity Increased possibility for re-resections Recent studies: No difference in survival between non-anatomic and anatomic resection. No randomised studies 21
22 Parenchyma sparing technique Factors that are important to know more about. Influence of resection margins on survival What about repeated resections? Howrecurrent metastasis occurs in the liver remnant Vascular anatomy ---pre and per operative planning Out and inflow Size of segments
23 Other important parameters Influence of Chemotherapy (neoadj./adj.) on the disease Tumor biology
24 Resection margins influence on survival and recurrence

25 Resection margin 2 publications 2013 and 2014: 1 mm resection margin is enough for CRLM 25
26 Resection margin This supports the theory about Parenchyma Sparing Technique (PST), indirectly, in the way that a big amount of liver tissue around the tumor does not need to be resected. 26
27 WhataboutRe-resection---safe? J GastrointestSurg.2009 Dec;13(12): doi: /s Epub2009 Oct 1. Repeat curative intent liver surgery is safe and effective for recurrent colorectal liver metastasis: results from an international multi-institutional analysis. de JongMC, Mayo SC, PulitanoC, LanellaS, RiberoD, StrubJ, Hubert C, Gigot JF, SchulickRD, Choti MA, Aldrighetti L, Mentha G, Capussotti L, Pawlik TM. Ann Surg Sep;250(3): doi: /SLA.0b013e3181b4539b. Rates and patterns of recurrence following curative intent surgery for colorectal liver metastasis: an international multiinstitutional analysis of 1669 patients. de JongMC, PulitanoC, RiberoD, StrubJ, MenthaG, SchulickRD, ChotiMA, AldrighettiL, CapussottiL, PawlikTM. Repeat curative intent surgery (CIS) for recurrent colorectal liver metastasis can be performed with low morbidity and near-zero mortality Patients with no extra-hepatic disease are best candidates for repeat CIS. In these patients, repeat CIS can offer the chance of long-term survival.
28 Re-resection ---open Publication Fong et al, 1994 Nordlinger et al, 1994 No of patients Perioperat ive mortality (%) Survival 5 years (%) Survival 10 years (%) (mean) ,9-33 Fernandez Trigo et al, 1995 Scheele et al, 1996 Adam et al, 1997 Yamamolo et al, 1997 Petrowsky et al, 2002 Shaw et al, N ,
29 Dia 28 N2 Obs: Perioperative mortality 1.6% (2 patients) in Petrowsky study Norstein; 30/09/2014
30 Re-resection --- Laparoscopic Result-CRLM First authors, year Shafaee et al, 2011 Country Tricentre study: France, Norway, USA No. of pts 3-year overall surviva l, % 5-year overall surviva l, % 55 * Is Laparoscopic Repeat Hepatectomy Feasible? A Tri-institutional Analysis Zahra Shafaee 1, AirazatM. Kazaryan 2, M. Marvin 3,K. Ravindra 3, Joseph F. Buell 3, BjørnEdwin 2, Brice Gayet 1. J Am Coll Surg Feb;212(2): Laparoscopic repeat hepatic resections can be performed safely and with good results, particularly in patients with earlier laparoscopic resections.
31 Whylaparoscopy Theoretical advantages J Hepatobiliary Pancreat Sci Oct;21(10): doi: /jhbp.139. Epub 2014 Aug 5. Laparoscopic hepatectomy is theoretically better than open hepatectomy: preparing for the 2nd International Consensus Conference on Laparoscopic Liver Resection. Wakabayashi G, Cherqui D, Geller DA, Han HS, Kaneko H, Buell JF. Six years have passed since the first International Consensus Conference on Laparoscopic Liver Resection was held. This comparatively new surgical technique has evolved since then and is rapidly being adopted worldwide. We compared the theoretical differences between open and laparoscopic liver resection, using right hepatectomy as an example. We also searched the Cochrane Library using the keyword "laparoscopic liver resection." The papers retrieved through the search were reviewed, categorized, and applied to the clinical questions that will be discussed at the 2nd Consensus Conference. The laparoscopic hepatectomyprocedure is more difficult to master than the open hepatectomyprocedure because of the movement restrictions imposed upon us when we operate from outside the body cavity. However, good visibility of the operative field around the liver, which is located beneath the costal arch, and the magnifying provide for neat transectionof the hepatic parenchyma. Another theoretical advantage is that pneumoperitoneumpressure reduces hemorrhage from the hepatic vein. The literature search turned up 67 papers, 23 of which we excluded, leaving only 44. Two randomized controlled trials (RCTs) are underway, but their results are yet to be published. Most of the studies (n = 15) concerned short-term results, with some addressing long-term results (n = 7), cost (n = 6), energy devices (n = 4), and so on. Laparoscopic hepatectomy is theoretically superior to open hepatectomy in terms of good visibility of the operative field due to the magnifying effect and reduced hemorrhage from the hepatic vein due to pneumoperitoneum pressure. However, there is as yet no evidence from previous studies to back this up in terms of short-term and long-term results. The 2nd International Consensus Conference on Laparoscopic Liver Resection will arrive at a consensus on the basis of the best available evidence, with video presentations focusing on surgical techniques and the publication of guidelines for the standardization of procedures based on the experience of experts. 30
32 31
33 Whylaparoscopy? Less adhesions, easier to perform repeated resections Laurent et al, J Hepatobiliary pancreat surg 2009: Laparoscopic liver resection facilitates salvage liver transplantation for hepatocellular carcinoma. Personal experience 32
34 How metastasis occurs in the liver remnant Aim: To determine if recurrent liver metastases recur in the same liver lobe as initial metastases, or in the contralateral lobe. 85 patients were found eligible for the study: -only patients with repeated metastasesafter primary liver surgery for colorectal metastases were included Patients divided into three groups: Group I initial metastases in the left lobe (n= 25) Group II initial metastases in the right lobe (n= 40) Group III initial metastases in both lobes (n= 20)
35 So what.. More then 50% of recurrent liver metastases appear in the contralateral lobe or bi-lobar This means After formal resections compared with parenchyma sparing technique, the patients have less chance of further surgical treatment
36 Parenchyma sparing technique Pre and per operative planning --- 3D map Vascular Anatomy In- and outflow, size of segments Important knowledge
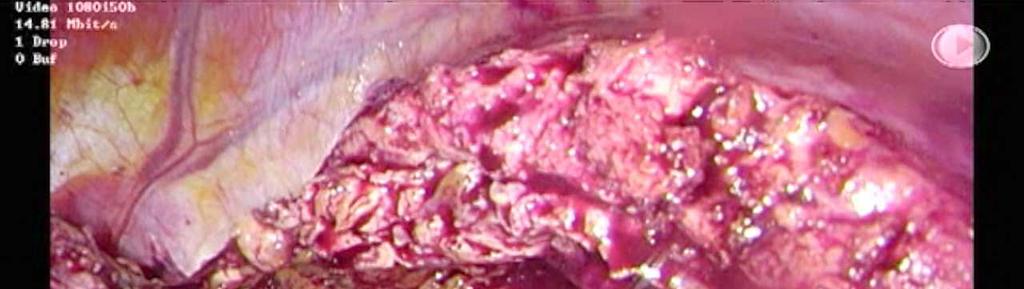
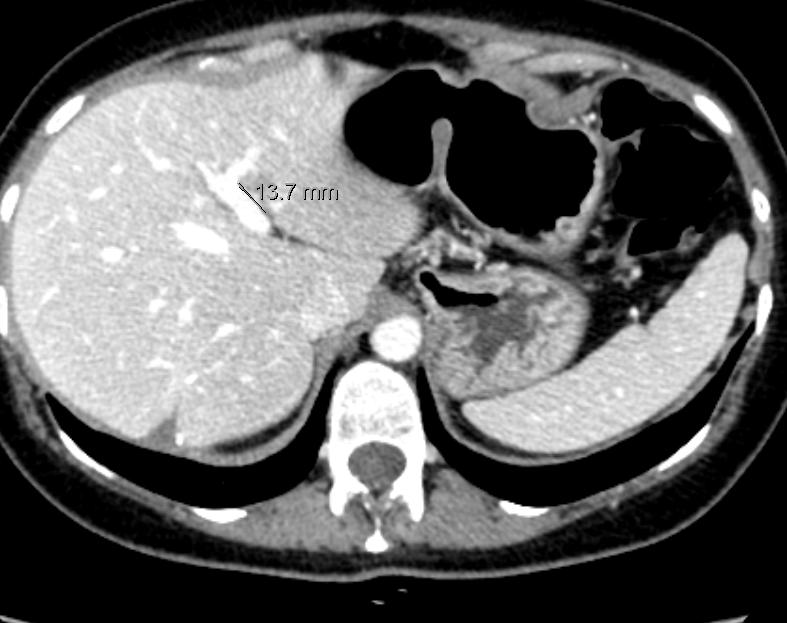
37 Case report: Major resection or Parenchymasparing: Patient E. female 48 years old; Sigmoideumresection in Jan. 2012, Dukes D cancer Syncronliver metastasis in S7, 17 mm


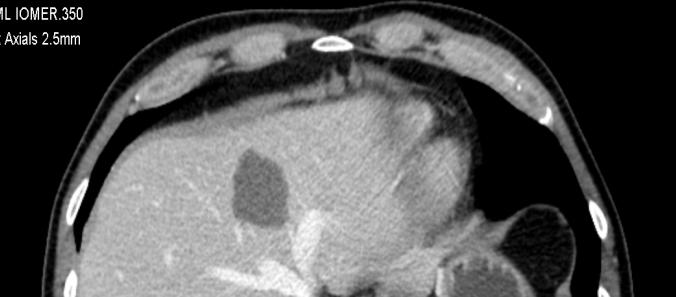
38 CT-scan, initial met in S7
39 Op. 3 month after sigm. res. Local resection S specimen 70*50*20 mm Tumor 25 mm free resection margin


40 CT-scan 3 month after operation


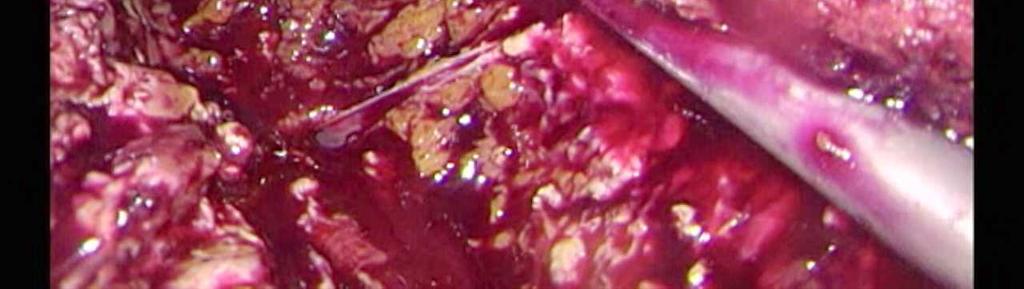
41 Recurrence 14 month after liver resection, seg 6/7
42 Op.14 month after 1st liver resection Local resection of segment 6/7 Tumor 25 mm Specimen 110*80*40 mm, 117 g Free resection margin


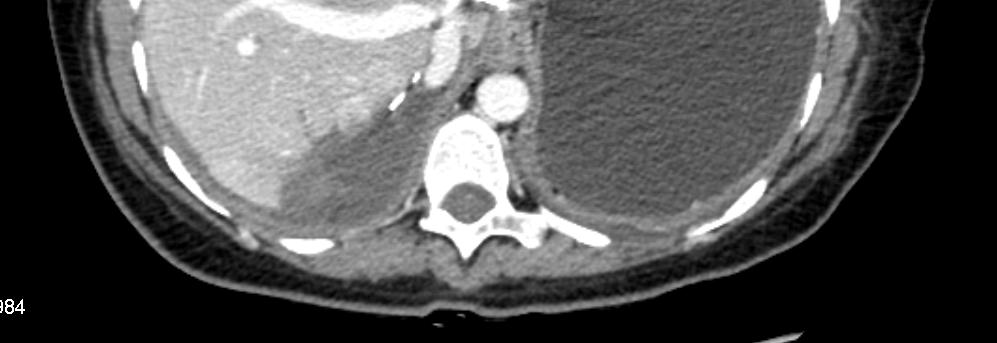
43 After 6 month recurrence S5, S7, S2

44
45 Operated 6 month after 2 nd liver resection and 2 years after colon resection local resection S7 specimen 60*55*20 mm, 64 g, tumor 28 mm local resection S5 specimen 35*28*18, 12 g, tumor 14 mm left lateral resection, extended to seg 4 specimen 100*70*25, 127 g, tumor 22 mm free margins

46 CT-scan 1 day after operation

47 Whatis nextstep? Oslo CoMet study OSlo Laparoscopic vs. Open resection of COlorectal METastasesstudy. Clinicaltrials.gov id: NCT Regional ethical approval after dedicated meeting with committee Is randomization really necessary? Yes, and it s now or never 46
48 The Comet-story so far From Feb 15 th 2012 to Oct 1 st 2014: 186 Patients included Most patients accept Patients demand laparotomy (n=3) 47
49 Immunology: There is a difference in the inflammatory response! 48
50 There is a difference in Quality of Life! 49
51 Whylaparoscopy? Better for the patient Less pain, faster back to activity, cosmetic Easier re-resections/transplant Less immune response Better QoL But we need randomized data! 50
52 Whatto discuss? In our opinion, the discussion is now Parenchyma sparing resections How to avoid formal resections How to do them laparoscopicallywhen needed 51
53 52
54 It is not thestrongest, nor the most intelligent whosurvive, butthosemost responsiveto change. Charles Darwin ( )



55 Thank you very much for your attention!



56 Formal right hemi hepatectomy? Vascular anatomy





57 NO! Segm.II and III too small Canweremovethetumor? N4 Vascular anatomy --- Important!!!
58 Dia 56 N4 "What about segment 4? Norstein; 30/09/2014


59 YES! Segm. V and VIII drainsto themhv, segm. VI and VII canbe removedwiththetumor and the RHV



60 Post operative result.
HEPATECTOMY. Surgical Potpourri Session. ACS NSQIP National Conference Salt Lake City 2012
 HEPATECTOMY Surgical Potpourri Session ACS NSQIP National Conference Salt Lake City 2012 Pascal Fuchshuber, MD, PhD, FACS Kaiser Permanente Medical Center Walnut Creek - California Hepatic Resection Is
HEPATECTOMY Surgical Potpourri Session ACS NSQIP National Conference Salt Lake City 2012 Pascal Fuchshuber, MD, PhD, FACS Kaiser Permanente Medical Center Walnut Creek - California Hepatic Resection Is
The Surgical Management of Colorectal Metastases
 11th July 2017 Bowel Cancer UK The Surgical Management of Colorectal Metastases Ben Cresswell MD(Res) FRCS Consultant HPB Surgeon The Basingstoke Hepatobiliary Unit United Kingdom Surgical Management of
11th July 2017 Bowel Cancer UK The Surgical Management of Colorectal Metastases Ben Cresswell MD(Res) FRCS Consultant HPB Surgeon The Basingstoke Hepatobiliary Unit United Kingdom Surgical Management of
Surgical management of HCC. Evangelos Prassas Hepatobiliary and Pancreatic Surgery / Liver Transplantation Kings College Hospital / London
 Surgical management of HCC Evangelos Prassas Hepatobiliary and Pancreatic Surgery / Liver Transplantation Kings College Hospital / London Global distribution of HCC and staging systems WEST 1. Italy (Milan,
Surgical management of HCC Evangelos Prassas Hepatobiliary and Pancreatic Surgery / Liver Transplantation Kings College Hospital / London Global distribution of HCC and staging systems WEST 1. Italy (Milan,
MANAGEMENT OF COLORECTAL METASTASES. Robert Warren, MD. The Postgraduate Course in General Surgery March 22, /22/2011
 MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
Colorectal Liver Metastases Metachronous
 Colorectal Liver Metastases Metachronous Professor Rowan Parks Professor of Surgical Sciences University of Edinburgh No disclosures Natural History of Unresected Untreated Colorectal Metastases Year N
Colorectal Liver Metastases Metachronous Professor Rowan Parks Professor of Surgical Sciences University of Edinburgh No disclosures Natural History of Unresected Untreated Colorectal Metastases Year N
Dr Adam Bartlett. General Surgeon Senior Lecturer University of Auckland Auckland City Hospital
 Dr Adam Bartlett General Surgeon Senior Lecturer University of Auckland Auckland City Hospital 11:05-11:15 Hepatic Metastectomy is Associated with Improved Survival Where is everyone? Hepatic Metastectomy
Dr Adam Bartlett General Surgeon Senior Lecturer University of Auckland Auckland City Hospital 11:05-11:15 Hepatic Metastectomy is Associated with Improved Survival Where is everyone? Hepatic Metastectomy
Multidisciplinary Treatment Strategies for Primary and Metastatic Liver Cancers
 Multidisciplinary Treatment Strategies for Primary and Metastatic Liver Cancers Ching-Wei D. Tzeng, M.D. Assistant Professor Surgical Oncology University of Kentucky Markey Cancer Center Affiliate Network
Multidisciplinary Treatment Strategies for Primary and Metastatic Liver Cancers Ching-Wei D. Tzeng, M.D. Assistant Professor Surgical Oncology University of Kentucky Markey Cancer Center Affiliate Network
Liver surgery for colorectal liver metastases. Keith Roberts, Consultant Liver Transplant and Liver/Pancreas Surgeon University Hospitals Birmingham
 Liver surgery for colorectal liver metastases Keith Roberts, Consultant Liver Transplant and Liver/Pancreas Surgeon University Hospitals Birmingham Introduction: what do we do? UHB Liver Unit: Liver resections
Liver surgery for colorectal liver metastases Keith Roberts, Consultant Liver Transplant and Liver/Pancreas Surgeon University Hospitals Birmingham Introduction: what do we do? UHB Liver Unit: Liver resections
Management of Stage IV Colorectal Cancer: Expanding the Horizon
 Management of Stage IV Colorectal Cancer: Expanding the Horizon May Tee, MD, MPH and Jan Franko, MD, PhD MercyOne Surgical Group (Mercy Surgical Affiliates) GI Oncology Conference 2019 March 1, 2019 Disclosures
Management of Stage IV Colorectal Cancer: Expanding the Horizon May Tee, MD, MPH and Jan Franko, MD, PhD MercyOne Surgical Group (Mercy Surgical Affiliates) GI Oncology Conference 2019 March 1, 2019 Disclosures
Treatment strategy of metastatic rectal cancer
 35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
Primary tumor with synchronous metastases
 Metastatic colorectal cancer: special clinical situations Primary tumor with synchronous metastases Stefan Heinrich & Hauke Lang Department of General, Visceral and Transplantation Surgery University Hospital
Metastatic colorectal cancer: special clinical situations Primary tumor with synchronous metastases Stefan Heinrich & Hauke Lang Department of General, Visceral and Transplantation Surgery University Hospital
Treatment of Colorectal Liver Metastases State of the Art
 Treatment of Colorectal Liver Metastases State of the Art Eddie K. Abdalla, MD, FACS Professor and Chairman of Surgery Chief of Hepatobiliary Surgery Hilton Metropolitan Palace Hotel Beirut 16 November,
Treatment of Colorectal Liver Metastases State of the Art Eddie K. Abdalla, MD, FACS Professor and Chairman of Surgery Chief of Hepatobiliary Surgery Hilton Metropolitan Palace Hotel Beirut 16 November,
Management of Colorectal Liver Metastases
 Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
Jose Ramos. Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma
 Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy
 Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy Dr Chan Chung Yip MBBS, M.Med(Surgery), MD, FAMS, FRCSEd Senior Consultant and Head Department of Hepatopancreatobiliary
Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy Dr Chan Chung Yip MBBS, M.Med(Surgery), MD, FAMS, FRCSEd Senior Consultant and Head Department of Hepatopancreatobiliary
Carcinoma del colon-retto: La Chirurgia Robotica nella Malattia Avanzata
 Carcinoma del colon-retto: La Chirurgia Robotica nella Malattia Avanzata Alberto Patriti SSD Chirurgia Robotica Multidisciplinare ASL 2 Umbria Ospedale San Matteo degli Infermi Spoleto - Why MIS for Advanced
Carcinoma del colon-retto: La Chirurgia Robotica nella Malattia Avanzata Alberto Patriti SSD Chirurgia Robotica Multidisciplinare ASL 2 Umbria Ospedale San Matteo degli Infermi Spoleto - Why MIS for Advanced
Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D.
 Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D. Department of Surgery Grand Rounds University of Kentucky January 15, 2014 Metastatic Colorectal Cancer (CRC)
Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D. Department of Surgery Grand Rounds University of Kentucky January 15, 2014 Metastatic Colorectal Cancer (CRC)
How to deal with synchronous primary and liver metastases
 How to deal with synchronous primary and liver metastases Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB) Department of Surgery.
How to deal with synchronous primary and liver metastases Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB) Department of Surgery.
Hepatobiliary Malignancies Retrospective Study at Truman Medical Center
 Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
Trattamento chirurgico delle lesioni epatiche secondarie difficili. Adelmo Antonucci Chirurgia Oncologica e Epato-bilio-pancreatica
 Trattamento chirurgico delle lesioni epatiche secondarie difficili Adelmo Antonucci Chirurgia Oncologica e Epato-bilio-pancreatica What does it mean difficult lesions? Diagnosis Treatment Small size Unfit
Trattamento chirurgico delle lesioni epatiche secondarie difficili Adelmo Antonucci Chirurgia Oncologica e Epato-bilio-pancreatica What does it mean difficult lesions? Diagnosis Treatment Small size Unfit
Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age. Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010
 Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010 Molecular mechanisms for cancer Prevention and screening Molecular
Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010 Molecular mechanisms for cancer Prevention and screening Molecular
Management of colorectal cancer liver metastases
 Management of colorectal cancer liver metastases Aliakbarian M. M.D. Assistant professor of surgery Organ Transplant & Hepatopancreatobiliary Surgeon SUBJECTS The importance of surgical resection in colorectal
Management of colorectal cancer liver metastases Aliakbarian M. M.D. Assistant professor of surgery Organ Transplant & Hepatopancreatobiliary Surgeon SUBJECTS The importance of surgical resection in colorectal
Liver metastases: treatment planning. PJ Valette
 Liver metastases: treatment planning PJ Valette Liver metastases removal December 2010 April 2011 : after chemotherapy June 2011 : after resection of left lobe mets & portal embol. Sept 2011 : 1 year after
Liver metastases: treatment planning PJ Valette Liver metastases removal December 2010 April 2011 : after chemotherapy June 2011 : after resection of left lobe mets & portal embol. Sept 2011 : 1 year after
E importante t che il chirurgo conosca il profilo molecolare del carcinoma del colon?
 E importante t che il chirurgo conosca il profilo molecolare del carcinoma del colon? Giuseppe Aprile Dipartimento di Oncologia Dipartimento di Oncologia Azienda Ospedaliero-Universitaria - Udine Dr. Giuseppe
E importante t che il chirurgo conosca il profilo molecolare del carcinoma del colon? Giuseppe Aprile Dipartimento di Oncologia Dipartimento di Oncologia Azienda Ospedaliero-Universitaria - Udine Dr. Giuseppe
Margin status in liver resections for colorectal metastases Orlando Jorge M. Torres MD, PhD
 Margin status in liver resections for colorectal metastases Orlando Jorge M. Torres MD, PhD Full Professor and Chairman Department of Gastrointestinal Surgery Hepatopancreatobiliary Unit Universidade Federal
Margin status in liver resections for colorectal metastases Orlando Jorge M. Torres MD, PhD Full Professor and Chairman Department of Gastrointestinal Surgery Hepatopancreatobiliary Unit Universidade Federal
How to integrate surgery in the treatment of patients with liver-only metastatic disease
 How to integrate surgery in the treatment of patients with liver-only metastatic disease Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB)
How to integrate surgery in the treatment of patients with liver-only metastatic disease Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB)
Laparoscopic Liver Resection for Hepatocellular Carcinoma
 Original Article Laparoscopic Liver Resection for Hepatocellular Carcinoma Carmen D. Chung, Lydia L. Lau, Kwan Lung Ko, Andrew C. Wong, Shezam Wong, Albert C. Chan, Ronnie T. Poon, Chung Mau Lo and Sheung
Original Article Laparoscopic Liver Resection for Hepatocellular Carcinoma Carmen D. Chung, Lydia L. Lau, Kwan Lung Ko, Andrew C. Wong, Shezam Wong, Albert C. Chan, Ronnie T. Poon, Chung Mau Lo and Sheung
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options
 State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
Liver surgery, acute GI tract bleeding
 Semmelweis University, Faculty of Medicine, 1 st Department of Surgery Liver surgery, acute GI tract bleeding Oszkár HAHN M.D. LIVER CYST US, CT, MRI Parasite (ELISA, eosinophil, anaphylaxy) Echinococcus
Semmelweis University, Faculty of Medicine, 1 st Department of Surgery Liver surgery, acute GI tract bleeding Oszkár HAHN M.D. LIVER CYST US, CT, MRI Parasite (ELISA, eosinophil, anaphylaxy) Echinococcus
Laparoscopic liver resections in surgical treatment of HCC
 Laparoscopic liver resections in surgical treatment of HCC Dr Evgeny Solomonov, MD Department of Organ transplantation HPB surgery Unit Beilinson Hospital Petah Tiqva, Israel 0 HCC The sixth most common
Laparoscopic liver resections in surgical treatment of HCC Dr Evgeny Solomonov, MD Department of Organ transplantation HPB surgery Unit Beilinson Hospital Petah Tiqva, Israel 0 HCC The sixth most common
TREATMENT FOR HCC AND CHOLANGIOCARCINOMA. Shawn Pelletier, MD
 TREATMENT FOR HCC AND CHOLANGIOCARCINOMA Shawn Pelletier, MD Treatment for HCC Treatment strategies Curative first line therapy Thermal ablation vs Resection vs Transplant Other first line therapies TACE
TREATMENT FOR HCC AND CHOLANGIOCARCINOMA Shawn Pelletier, MD Treatment for HCC Treatment strategies Curative first line therapy Thermal ablation vs Resection vs Transplant Other first line therapies TACE
Radiation Therapy for Liver Malignancies
 Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
SECONDARIES: A PRELIMINARY REPORT
 HPB Surgery, 1990, Vol. 2, pp. 69-72 Reprints available directly from the publisher Photocopying permitted by license only 1990 Harwood Academic Publishers GmbH Printed in the United Kingdom CASE REPORTS
HPB Surgery, 1990, Vol. 2, pp. 69-72 Reprints available directly from the publisher Photocopying permitted by license only 1990 Harwood Academic Publishers GmbH Printed in the United Kingdom CASE REPORTS
Colon Cancer Liver Metastases: Liver-Directed Therapy
 Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
HOW I DO IT Feasibility of Bisegmentectomy 7 8 is Independent of the Presence of a Large Inferior Right Hepatic Vein
 Journal of Surgical Oncology 2006;93:338 342 HOW I DO IT Feasibility of Bisegmentectomy 7 8 is Independent of the Presence of a Large Inferior Right Hepatic Vein MARCEL AUTRAN C. MACHADO, MD, 1,2 * PAULO
Journal of Surgical Oncology 2006;93:338 342 HOW I DO IT Feasibility of Bisegmentectomy 7 8 is Independent of the Presence of a Large Inferior Right Hepatic Vein MARCEL AUTRAN C. MACHADO, MD, 1,2 * PAULO
Aintree University Hospital
 Aintree University Hospital Liverpool, UK Evolving role of DEBIRI with DC Bead - TACE in mcrc Hassan Z Malik MD FRCS Consultant Hepatobiliary Surgeon Hassan Z Malik is a consultant to Biocompatibles UK
Aintree University Hospital Liverpool, UK Evolving role of DEBIRI with DC Bead - TACE in mcrc Hassan Z Malik MD FRCS Consultant Hepatobiliary Surgeon Hassan Z Malik is a consultant to Biocompatibles UK
Treatment of oligometastatic NSCLC
 Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Note: Page numbers of article titles are in boldface type. A Adenocarcinoma, pancreatic ductal, laparoscopic distal pancreatectomy for, 61 Adrenal cortical carcinoma, laparoscopic adrenalectomy for, 114
Locoregional Treatments for HCC Applications in Transplant Candidates. Locoregional Treatments for HCC Applications in Transplant Candidates
 Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
Locoregional Treatments for HCC Applications in Transplant Candidates Matthew Casey, MD March 31, 2016 Locoregional Treatments for HCC Applications in Transplant Candidates *No disclosures *Off-label uses
Aggressive surgery in the multimodality treatment of liver metastases from colorectal cancer
 Journal of BUON 12: 209-213, 2007 2007 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Aggressive surgery in the multimodality treatment of liver metastases from colorectal cancer N.
Journal of BUON 12: 209-213, 2007 2007 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Aggressive surgery in the multimodality treatment of liver metastases from colorectal cancer N.
Current Treatment of Colorectal Metastases. Dr. Thavanathan Surgical Grand Rounds February 1, 2005
 Current Treatment of Colorectal Metastases Dr. Thavanathan Surgical Grand Rounds February 1, 2005 25% will have metastases at initial presentation 25-50% 50% will develop metastases later 40% of potentially
Current Treatment of Colorectal Metastases Dr. Thavanathan Surgical Grand Rounds February 1, 2005 25% will have metastases at initial presentation 25-50% 50% will develop metastases later 40% of potentially
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases
 Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh
 Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Surgical Management of Advanced Stage Colon Cancer. Nathan Huber, MD 6/11/14
 Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Tissue Management With Tri-Staple Technology in Major and Minor Laparoscopic Liver Resections
 Int Surg 2014;99:606 611 DOI: 10.9738/INTSURG-D-13-00101.1 Tissue Management With Tri-Staple Technology in Major and Minor Laparoscopic Liver Resections Vincenzo Scuderi, Roberto I. Troisi Department of
Int Surg 2014;99:606 611 DOI: 10.9738/INTSURG-D-13-00101.1 Tissue Management With Tri-Staple Technology in Major and Minor Laparoscopic Liver Resections Vincenzo Scuderi, Roberto I. Troisi Department of
HEPATIC METASTASES. We can state 3 types of metastases depending on their treatment options:
 HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
Management of HepatoCellular Carcinoma
 9th Symposium GIC St Louis - 2010 Management of HepatoCellular Carcinoma Overview Pierre A. Clavien, MD, PhD Department of Surgery University Hospital Zurich Zurich, Switzerland Hepatocellular carcinoma
9th Symposium GIC St Louis - 2010 Management of HepatoCellular Carcinoma Overview Pierre A. Clavien, MD, PhD Department of Surgery University Hospital Zurich Zurich, Switzerland Hepatocellular carcinoma
Colorectal cancer (CRC)
") Colorectal cancer (CRC) Epidemiology. The 3 rd most common malignancy worldwide 1 Second leading cause of cancer-related death in Western world 2 20-25% of all patients are presented with synchronous colorectal
Colorectal cancer (CRC) Epidemiology. The 3 rd most common malignancy worldwide 1 Second leading cause of cancer-related death in Western world 2 20-25% of all patients are presented with synchronous colorectal
Treatment of Locally Advanced Rectal Cancer: Current Concepts
 Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Hepatobiliary and Pancreatic Malignancies
 Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Pioneers in Laparoscopic HBP Surgery
 East meets west Pioneers in Laparoscopic HBP Surgery Yoshihiro Miyasaka 1, Masafumi Nakamura 1 and Go Wakabayashi 2 1 Department of Surgery and Oncology, Graduate School of Medical Sciences, Kyushu University
East meets west Pioneers in Laparoscopic HBP Surgery Yoshihiro Miyasaka 1, Masafumi Nakamura 1 and Go Wakabayashi 2 1 Department of Surgery and Oncology, Graduate School of Medical Sciences, Kyushu University
Management of Rare Liver Tumours
 Gian Luca Grazi Hepato-Biliary-Pancreatic Surgery National Cancer Institute Regina Elena Rome Fibrolamellar Carcinoma Mixed Hepato Cholangiocellular Carcinoma Hepatoblastoma Carcinosarcoma Primary Hepatic
Gian Luca Grazi Hepato-Biliary-Pancreatic Surgery National Cancer Institute Regina Elena Rome Fibrolamellar Carcinoma Mixed Hepato Cholangiocellular Carcinoma Hepatoblastoma Carcinosarcoma Primary Hepatic
LIVER SURGERY 2. Case 1. Med 5 Refresher Course (Surgery) 2013/14. Dr Sunny Cheung
 2013/14. Dr Sunny Cheung") LIVER SURGERY 2 Med 5 Refresher Course (Surgery) 2013/14 24 Jun 2013 Dr Sunny Cheung Case 1 50/M Sudden onset of epigastric pain Abdominal distension Confused HR 120 BP 80/50 Haemocue = 8 What should you
LIVER SURGERY 2 Med 5 Refresher Course (Surgery) 2013/14 24 Jun 2013 Dr Sunny Cheung Case 1 50/M Sudden onset of epigastric pain Abdominal distension Confused HR 120 BP 80/50 Haemocue = 8 What should you
Liver resection for HCC
 8 th LIVER INTEREST GROUP Annual Meeting Cape Town 2017 Liver resection for HCC Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre The liver is almost unique in that treatment of the
8 th LIVER INTEREST GROUP Annual Meeting Cape Town 2017 Liver resection for HCC Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre The liver is almost unique in that treatment of the
ORIGINAL ARTICLE. A Second Liver Resection Due to Recurrent Colorectal Liver Metastases. accepted as the only curative
 ORIGINAL ARTICLE A Second Liver Resection Due to Recurrent Colorectal Liver Metastases Antonio Sa Cunha, MD; Christophe Laurent, MD; Alexandre Rault, MD; Philippe Couderc, MD; Eric Rullier, MD; Jean Saric,
ORIGINAL ARTICLE A Second Liver Resection Due to Recurrent Colorectal Liver Metastases Antonio Sa Cunha, MD; Christophe Laurent, MD; Alexandre Rault, MD; Philippe Couderc, MD; Eric Rullier, MD; Jean Saric,
Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging
 Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Hepatobiliary and Pancreatic Surgery Chief of Hepatobiliary and Pancreatic Surgery
Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Hepatobiliary and Pancreatic Surgery Chief of Hepatobiliary and Pancreatic Surgery
Correspondence should be addressed to Roland Andersson,
 Gastroenterology Research and Practice Volume 2012, Article ID 568214, 4 pages doi:10.1155/2012/568214 Research Article Repeated Liver Resection for Colorectal Liver Metastases: A Comparison with Primary
Gastroenterology Research and Practice Volume 2012, Article ID 568214, 4 pages doi:10.1155/2012/568214 Research Article Repeated Liver Resection for Colorectal Liver Metastases: A Comparison with Primary
Where are we with radiotherapy for biliary tract cancers?
 Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
6/16/2016. Treating Hepatocellular Carcinoma: Deciphering the Clinical Data. Liver Regeneration. Liver Regeneration
 Treating : Deciphering the Clinical Data Derek DuBay, MD Associate Professor of Surgery Director of Liver Transplant Liver Transplant and Hepatobiliary Surgery UAB Department of Surgery Liver Regeneration
Treating : Deciphering the Clinical Data Derek DuBay, MD Associate Professor of Surgery Director of Liver Transplant Liver Transplant and Hepatobiliary Surgery UAB Department of Surgery Liver Regeneration
Risk factors for cancer recurrence or death within 6 months after liver resection in patients with colorectal cancer liver metastasis
 ORIGINAL ARTICLE pissn 2288-6575 eissn 2288-6796 http://dx.doi.org/10.4174/astr.2016.90.5.257 Annals of Surgical Treatment and Research Risk factors for cancer recurrence or death within 6 months after
ORIGINAL ARTICLE pissn 2288-6575 eissn 2288-6796 http://dx.doi.org/10.4174/astr.2016.90.5.257 Annals of Surgical Treatment and Research Risk factors for cancer recurrence or death within 6 months after
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan
 State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
Laparoscopic liver resection for malignant liver tumors, why not more?
 J Korean Surg Soc 2012;83:30-35 http://dx.doi.org/10.4174/jkss.2012.83.1.30 ORIGINAL ARTICLE JKSS Journal of the Korean Surgical Society pissn 2233-7903 ㆍ eissn 2093-0488 Laparoscopic liver resection for
J Korean Surg Soc 2012;83:30-35 http://dx.doi.org/10.4174/jkss.2012.83.1.30 ORIGINAL ARTICLE JKSS Journal of the Korean Surgical Society pissn 2233-7903 ㆍ eissn 2093-0488 Laparoscopic liver resection for
Adult-to-adult living donor liver transplantation Triumphs and challenges
 Falk Symposium No. 163 on Chronic Inflammation of Liver and Gut Adult-to-adult living donor liver transplantation Triumphs and challenges ST Fan, MS, MD, PhD, DSc Professor Sun CY Chair of Hepatobiliary
Falk Symposium No. 163 on Chronic Inflammation of Liver and Gut Adult-to-adult living donor liver transplantation Triumphs and challenges ST Fan, MS, MD, PhD, DSc Professor Sun CY Chair of Hepatobiliary
TIMOTHY M. PAWLIK, RICHARD D. SCHULICK, MICHAEL A. CHOTI
 The Oncologist Hepatobiliary Expanding Criteria for Resectability of Colorectal Liver Metastases TIMOTHY M. PAWLIK,RICHARD D. SCHULICK,MICHAEL A. CHOTI Department of Surgery, Johns Hopkins University School
The Oncologist Hepatobiliary Expanding Criteria for Resectability of Colorectal Liver Metastases TIMOTHY M. PAWLIK,RICHARD D. SCHULICK,MICHAEL A. CHOTI Department of Surgery, Johns Hopkins University School
Indications for sublobar resection for localized NSCLC
 Indications for sublobar resection for localized NSCLC David H Harpole Jr, MD Professor of Surgery Associate Professor in Pathology Vice Chief, Division of Surgical Services Duke University School of Medicine
Indications for sublobar resection for localized NSCLC David H Harpole Jr, MD Professor of Surgery Associate Professor in Pathology Vice Chief, Division of Surgical Services Duke University School of Medicine
Laparoscopic Resection Of Colon & Rectal Cancers. R Sim Centre for Advanced Laparoscopic Surgery, TTSH
 Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
Laparoscopic Resection Of Colon & Rectal Cancers R Sim Centre for Advanced Laparoscopic Surgery, TTSH Feasibility and safety Adequacy - same radical surgery as open op. Efficacy short term benefits and
HPB ORIGINAL ARTICLE. Abstract. Correspondence. Introduction
 DOI:10.1111/hpb.12204 HPB ORIGINAL ARTICLE Margin status after laparoscopic resection of colorectal liver metastases: does a narrow resection margin have an influence on survival and local recurrence?
DOI:10.1111/hpb.12204 HPB ORIGINAL ARTICLE Margin status after laparoscopic resection of colorectal liver metastases: does a narrow resection margin have an influence on survival and local recurrence?
Embolotherapy for Cholangiocarcinoma: 2016 Update
 Embolotherapy for Cholangiocarcinoma: 2016 Update Igor Lobko,MD Chief, Division Vascular and Interventional Radiology Long Island Jewish Medical Center GEST 2016 Igor Lobko, M.D. No relevant financial
Embolotherapy for Cholangiocarcinoma: 2016 Update Igor Lobko,MD Chief, Division Vascular and Interventional Radiology Long Island Jewish Medical Center GEST 2016 Igor Lobko, M.D. No relevant financial
Surgical Management of Pancreatic Cancer
 I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
8 Giornata Onco-ematologica Varesina
 Azienda Ospedaliera Sant Antonio Abate di Gallarate 8 Giornata Onco-ematologica Varesina Le esperienze di eccellenza del DIPO di Varese Metastasi epatiche da tumore del colon-retto: terapia medica in funzione
Azienda Ospedaliera Sant Antonio Abate di Gallarate 8 Giornata Onco-ematologica Varesina Le esperienze di eccellenza del DIPO di Varese Metastasi epatiche da tumore del colon-retto: terapia medica in funzione
CHIRURGIA EPATOBILIARE IN WEEK SURGERY?
 U.O.C. di Chirurgia Epatobiliare e dei Trapianti Epatici Università degli Studi di Padova CHIRURGIA EPATOBILIARE IN WEEK SURGERY? Umberto Cillo, MD, PhD, FEBS cillo@unipd.it Quali sono gli ingredienti
U.O.C. di Chirurgia Epatobiliare e dei Trapianti Epatici Università degli Studi di Padova CHIRURGIA EPATOBILIARE IN WEEK SURGERY? Umberto Cillo, MD, PhD, FEBS cillo@unipd.it Quali sono gli ingredienti
Image Guidance Improves Localization of Sonographically Occult Colorectal Liver Metastases
 Image Guidance Improves Localization of Sonographically Occult Colorectal Liver Metastases Universe Leung a, Amber L. Simpson a,b, Lauryn B. Adams a, William R. Jarnagin a, Michael I. Miga b, and T. Peter
Image Guidance Improves Localization of Sonographically Occult Colorectal Liver Metastases Universe Leung a, Amber L. Simpson a,b, Lauryn B. Adams a, William R. Jarnagin a, Michael I. Miga b, and T. Peter
Surgery for hilar cholangiocirconoma
 Department of Surgery University Hospital RWTH Aachen Surgery for hilar cholangiocirconoma Ulf Peter Neumann Agenda Operating on the most complex tumor in HBP Surgery Preoperative management Does the patient
Department of Surgery University Hospital RWTH Aachen Surgery for hilar cholangiocirconoma Ulf Peter Neumann Agenda Operating on the most complex tumor in HBP Surgery Preoperative management Does the patient
INTRAARTERIAL TREATMENT OF COLORECTAL LIVER METASTASES. Dr. Joan Falcó Interventional Radiology UDIAT. Hospital Universitari Parc Taulí
 INTRAARTERIAL TREATMENT OF COLORECTAL LIVER METASTASES Dr. Joan Falcó Interventional Radiology UDIAT. Hospital Universitari Parc Taulí STRATEGIES FOR CRLM LIVER METASTASES Extended indications Resectable
INTRAARTERIAL TREATMENT OF COLORECTAL LIVER METASTASES Dr. Joan Falcó Interventional Radiology UDIAT. Hospital Universitari Parc Taulí STRATEGIES FOR CRLM LIVER METASTASES Extended indications Resectable
General summary GENERAL SUMMARY
 General summary GENERAL SUMMARY In Chapter 2.1 the long-term results and prognostic factors of radiofrequency ablation (RFA) for unresectable colorectal liver metastases (CRLM) in a single center with
General summary GENERAL SUMMARY In Chapter 2.1 the long-term results and prognostic factors of radiofrequency ablation (RFA) for unresectable colorectal liver metastases (CRLM) in a single center with
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 5
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 5 Contents 5. Assessment & Management of Liver Metastases 42 5.1. Metachronous
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 5 Contents 5. Assessment & Management of Liver Metastases 42 5.1. Metachronous
How much colon should be resected?
 Colon Cancer Surgical Standard of Care and Operative Techniques Madhulika G. Varma MD Professor and Chief Section of Colorectal Surgery University of California, San Francisco How much colon should be
Colon Cancer Surgical Standard of Care and Operative Techniques Madhulika G. Varma MD Professor and Chief Section of Colorectal Surgery University of California, San Francisco How much colon should be
PATHOLOGIC FACTORS PROGNOSTIC OF SURVIVAL IN PATIENTS WITH GI TRACT AND PANCREATIC CARCINOMA TREATED WITH NEOADJUVANT THERAPY
 PATHOLOGIC FACTORS PROGNOSTIC OF SURVIVAL IN PATIENTS WITH GI TRACT AND PANCREATIC CARCINOMA TREATED WITH NEOADJUVANT THERAPY Jeannelyn S. Estrella, MD Department of Pathology The UT MD Anderson Cancer
PATHOLOGIC FACTORS PROGNOSTIC OF SURVIVAL IN PATIENTS WITH GI TRACT AND PANCREATIC CARCINOMA TREATED WITH NEOADJUVANT THERAPY Jeannelyn S. Estrella, MD Department of Pathology The UT MD Anderson Cancer
Repeated Liver Resection for Colorectal Liver Metastases: A Comparison with Primary Liver Resections concerning Perioperative and Long-Term Outcome.
 Repeated Liver Resection for Colorectal Liver Metastases: A Comparison with Primary Liver Resections concerning Perioperative and Long-Term Outcome. Jönsson, Kristoffer; Gröndahl, Gerd; Salö, Martin; Tingstedt,
Repeated Liver Resection for Colorectal Liver Metastases: A Comparison with Primary Liver Resections concerning Perioperative and Long-Term Outcome. Jönsson, Kristoffer; Gröndahl, Gerd; Salö, Martin; Tingstedt,
Intraoperative staging of GIT cancer using Intraoperative Ultrasound
 Intraoperative staging of GIT cancer using Intraoperative Ultrasound Thesis For Fulfillment of MSc Degree In Surgical Oncology By Abdelhalim Salah Abdelhalim Moursi M.B.B.Ch (Cairo University ) Supervisors
Intraoperative staging of GIT cancer using Intraoperative Ultrasound Thesis For Fulfillment of MSc Degree In Surgical Oncology By Abdelhalim Salah Abdelhalim Moursi M.B.B.Ch (Cairo University ) Supervisors
RF Ablation: indication, technique and imaging follow-up
 RF Ablation: indication, technique and imaging follow-up Trongtum Tongdee, M.D. Radiology Department, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand Objective Basic knowledge
RF Ablation: indication, technique and imaging follow-up Trongtum Tongdee, M.D. Radiology Department, Faculty of Medicine, Siriraj Hospital, Mahidol University, Bangkok, Thailand Objective Basic knowledge
VATS Segmentectomy. Duke Masters Course Sept 2015
 VATS Segmentectomy Duke Masters Course Sept 2015 Scott J. Swanson, M.D. Director, Minimally Invasive Thoracic Surgery Brigham and Women s Hospital Chief Surgical Officer Dana Farber Cancer Institute Professor
VATS Segmentectomy Duke Masters Course Sept 2015 Scott J. Swanson, M.D. Director, Minimally Invasive Thoracic Surgery Brigham and Women s Hospital Chief Surgical Officer Dana Farber Cancer Institute Professor
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers
 Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Epidemiology, aetiology and the patient pathway in oesophageal and pancreatic cancers Dr Ian Chau Consultant Medical Oncologist Women's cancers Breast cancer introduction 3 What profession are you in?
Metastatic Liver Cancer
 4 Metastatic Liver Cancer ANDREW J. SMITH, MD, FRCSC RONALD P. DEMATTEO, MD YUMAN FONG, MD, FACS LESLIE H. BLUMGART, MD, FACS, FRCS (ENG, EDIN, GLAS) The management of hepatic metastases has become more
4 Metastatic Liver Cancer ANDREW J. SMITH, MD, FRCSC RONALD P. DEMATTEO, MD YUMAN FONG, MD, FACS LESLIE H. BLUMGART, MD, FACS, FRCS (ENG, EDIN, GLAS) The management of hepatic metastases has become more
Original article: new surgical approaches to the Klatskin tumour
 Alimentary Pharmacology & Therapeutics Original article: new surgical approaches to the Klatskin tumour T. M. VAN GULIK*, S. DINANT*, O. R. C. BUSCH*, E. A. J. RAUWS, H. OBERTOP* & D. J. GOUMA Departments
Alimentary Pharmacology & Therapeutics Original article: new surgical approaches to the Klatskin tumour T. M. VAN GULIK*, S. DINANT*, O. R. C. BUSCH*, E. A. J. RAUWS, H. OBERTOP* & D. J. GOUMA Departments
Citation for published version (APA): Hompes, D. N. M. (2013). Advanced colorectal cancer: Exploring treatment boundaries.
: Hompes, D. N. M. (2013). Advanced colorectal cancer: Exploring treatment boundaries.") UvA-DARE (Digital Academic Repository) Advanced colorectal cancer: Exploring treatment boundaries Hompes, Daphne Link to publication Citation for published version (APA): Hompes, D. N. M. (2013). Advanced
UvA-DARE (Digital Academic Repository) Advanced colorectal cancer: Exploring treatment boundaries Hompes, Daphne Link to publication Citation for published version (APA): Hompes, D. N. M. (2013). Advanced
Corporate Medical Policy
 Corporate Medical Policy Cryosurgical Ablation of Primary or Metastatic Liver Tumors File Name: Origination: Last CAP Review: Next CAP Review: Last Review: cryosurgical_ablation_of_primary_or_metastatic_liver_tumors
Corporate Medical Policy Cryosurgical Ablation of Primary or Metastatic Liver Tumors File Name: Origination: Last CAP Review: Next CAP Review: Last Review: cryosurgical_ablation_of_primary_or_metastatic_liver_tumors
HIPEC Controversies in the Indications and Application of Regional Chemotherapy for Peritoneal Surface Malignancies
 HIPEC Controversies in the Indications and Application of Regional Chemotherapy for Peritoneal Surface Malignancies Crescent City Cancer Update: GI and HPB Saturday September 24, 2016 George M. Fuhrman,
HIPEC Controversies in the Indications and Application of Regional Chemotherapy for Peritoneal Surface Malignancies Crescent City Cancer Update: GI and HPB Saturday September 24, 2016 George M. Fuhrman,
Chemotherapy for resectable liver mets: Options and Issues. Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA
 Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
4th ESSO Advanced Course on the Management of Colorectal Liver Metastases
 4th ESSO Advanced Course on the Management of Colorectal Liver Metastases 10-11 October 2016 BORDEAUX (FR) 4 th ESSO Advanced Course on the Management of Colorectal Liver Metastases Chairs Serge Evrard,
4th ESSO Advanced Course on the Management of Colorectal Liver Metastases 10-11 October 2016 BORDEAUX (FR) 4 th ESSO Advanced Course on the Management of Colorectal Liver Metastases Chairs Serge Evrard,
Predictors of a True Complete Response Among Disappearing Liver Metastases From Colorectal Cancer After Chemotherapy
 Original Article Predictors of a True Complete Response Among Disappearing Liver Metastases From Colorectal Cancer After Chemotherapy Rebecca C. Auer, MD 1 ; Rebekah R. White, MD 2 ; Nancy E. Kemeny, MD
Original Article Predictors of a True Complete Response Among Disappearing Liver Metastases From Colorectal Cancer After Chemotherapy Rebecca C. Auer, MD 1 ; Rebekah R. White, MD 2 ; Nancy E. Kemeny, MD
is time consuming and expensive. An intra-operative assessment is not going to be helpful if there is no more tissue that can be taken to improve the
 My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
My name is Barry Feig. I am a Professor of Surgical Oncology at The University of Texas MD Anderson Cancer Center in Houston, Texas. I am going to talk to you today about the role for surgery in the treatment
Case Report In Situ Split of the Liver When Portal Venous Embolization Fails to Induce Hypertrophy: A Report of Two Cases
 Case Reports in Surgery Volume 2013, Article ID 238675, 4 pages http://dx.doi.org/10.1155/2013/238675 Case Report In Situ Split of the Liver When Portal Venous Embolization Fails to Induce Hypertrophy:
Case Reports in Surgery Volume 2013, Article ID 238675, 4 pages http://dx.doi.org/10.1155/2013/238675 Case Report In Situ Split of the Liver When Portal Venous Embolization Fails to Induce Hypertrophy:
Radiofrequency Ablation of Primary or Metastatic Liver Tumors
 Radiofrequency Ablation of Primary or Metastatic Liver Tumors Policy Number: 7.01.91 Last Review: 9/2018 Origination: 2/1996 Next Review: 9/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Radiofrequency Ablation of Primary or Metastatic Liver Tumors Policy Number: 7.01.91 Last Review: 9/2018 Origination: 2/1996 Next Review: 9/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Staging & Current treatment of HCC
 Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
MDT IMPROVEMENT PROJECT. Professor Muntzer Mughal, UCLH
 MDT IMPROVEMENT PROJECT Professor Muntzer Mughal, UCLH 1995..assessment and management of rare cancers in multidisciplinary teams.. 2000 the care of all patients with cancer should be formally reviewed
MDT IMPROVEMENT PROJECT Professor Muntzer Mughal, UCLH 1995..assessment and management of rare cancers in multidisciplinary teams.. 2000 the care of all patients with cancer should be formally reviewed
Minimally Invasive Esophagectomy- Valuable. Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006
 Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
Minimally Invasive Esophagectomy- Valuable Jayer Chung, MD University of Colorado Health Sciences Center December 11, 2006 Overview Esophageal carcinoma What is minimally invasive esophagectomy (MIE)?
Unresectable or boarderline resectable disease
 ESMO Preceptorship Colorectal Cancer Nov 2016 Barcelona Unresectable or boarderline resectable disease Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West German Cancer Center (NWTZ) Learning
ESMO Preceptorship Colorectal Cancer Nov 2016 Barcelona Unresectable or boarderline resectable disease Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West German Cancer Center (NWTZ) Learning
Management of Cholangiocarcinoma. Roseanna Lee, MD PGY-5 Kings County Hospital
 Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
Management of Cholangiocarcinoma Roseanna Lee, MD PGY-5 Kings County Hospital Case Presentation 37 year old male from Yemen presented with 2 week history of epigastric pain, anorexia, jaundice and puritis.
Workup of a Solid Liver Lesion
 Workup of a Solid Liver Lesion Joseph B. Cofer MD FACS Chief Quality Officer Erlanger Health System Affiliate Professor of Surgery UTHSC-Chattanooga I have no financial or other relationships with any
Workup of a Solid Liver Lesion Joseph B. Cofer MD FACS Chief Quality Officer Erlanger Health System Affiliate Professor of Surgery UTHSC-Chattanooga I have no financial or other relationships with any