Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy
|
|
|
- Trevor Horton
- 6 years ago
- Views:
Transcription

, Duke-NUS Medical")
1 Resection of liver limited resectable metastases Upfront, neoadjuvant and repeat hepatectomy Dr Chan Chung Yip MBBS, M.Med(Surgery), MD, FAMS, FRCSEd Senior Consultant and Head Department of Hepatopancreatobiliary and Transplant Surgery Singapore General Hospital Associate Professor (Adj), Duke-NUS Medical School ESMO Preceptorship Programme GI Tumours Singapore November 2017

2

3
4 Introduction Resection of colorectal liver metastasis (CRLM) is required for long term survival 15-25% will present with synchronous CRLM 40-50% will develop CRLM within 3 years of resection of primary tumour 25% of patients with CRLM are eligible for surgical extirpation

5 Chronology of chemotherapy for mcrc
6
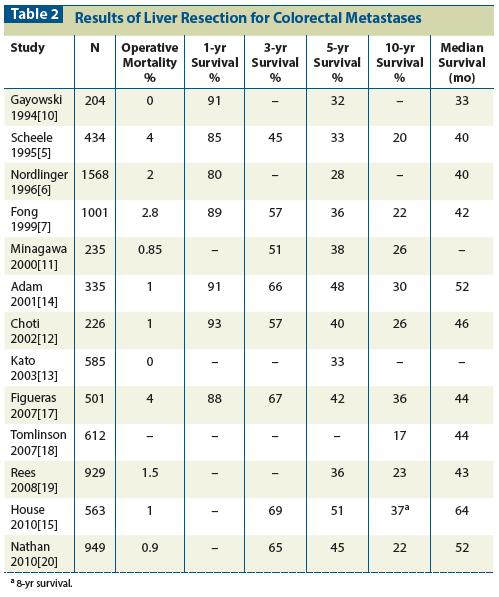
7 Surgical resection of colorectal liver metastasis in patients with expanded indications: a single-center experience with 501 patients. Figueras J et al. Dis Colon Rectum, patients with 545 liver resections over 15 year period comparing classic with expanded indications Expanded indications: lesions > 10cm (n=14), bilateral deposits (n=194), 4 metastasis (n=140), extra-hepatic disease (n=73) 52% of patients 5 year survival: 45% vs 34%, 10 year survival: 36 vs 24% (p=0.0009) 4 metastases and extra-hepatic disease predict poor outcome
8 Can we improve survival with chemotherapy?
9 Role of adjuvant chemotherapy in resectable CRLM Robust data on role of systemic chemotherapy for resected stage III and unresectable stage IV cancer Data on role of adjuvant chemotherapy for resected CRLM is scant 4 randomized trials, 2 published Langer B et al. Proc Amer Soc Clin Oncol 2002 Portier G et al. J Clin Oncol 2006 Both did not show difference in overall survival, Portier et al trial showed disease free survival benefit Poor accrural, small sample size
10 Role of adjuvant chemotherapy in resectable CRLM Several large retrospective studies Parks R et al. J Am Coll Surg 2007 Figueras J et al. Dis Colon Rectum 2007 Wang X et al. Br J Cancer 2007 All reported overall and DF survival benefit for adjuvant 5-FU A randomized phase II study comparing adjuvant 5-FU/folinic acid with FOLFIRI in patients following complete resection of liver metastases from colorectal cancer. Ychou M et al. Ann Oncol No difference in overall or DF survival
11 Peri-operative and Neoadjuvant Chemotherapy Survival benefits from pre-hepatectomy chemotherapy have not been established Retrospective studies show improved survival with adjuvant therapy but not with neoadjuvant therapy. Increased post operative complications Adam R et al. Ann Surg Reddy SK et al. Ann Surg Oncol Only 1 randomized trial (EORTC Intergroup trial 40983) Norlinger B et al. Lancet Norlinger B et al. Lancet Oncol 2013
12 EORTC Intergroup Trial patients randomized to surgery alone or surgery with perioperative FOLFOX 4 chemotherapy Median follow-up 8.5yrs Non-statistically significant trend in 5yr PFS favouring chemotherapy group (38% vs 30%, HR 0.81, p=0.068) 5yr OS similar: 51% vs 48% (HR 0.88, 95% CI )
13 Peri-operative and Neoadjuvant Chemotherapy Early treatment of systemic disease Allow biology of disease to declare itself In vivo assessment of response to chemotherapy While already resectable, lesions treated with neoadjuvant chemotherapy may benefit from further downsizing to facilitate increased rates of margin negative as well as parenchymal sparing resections
14 Progression on chemotherapy Marker for aggressive tumour biology Uncommon, 5-15% of patients Development of new lesions strongest predictor of poor post-hepatectomy outcome 5 yr survival in pts with >3 mets that progressed 8% Prognostic impact of progression in form of growth of pre-existing lesion less clear Allen et al. J Gastrointest Surg 2003 Adam et al. Ann Surg 2004
15 Can prehepatectomy chemotherapy identify pts who will unlikely benefit from hepatectomy? Relatively few patients experience disease progression while receiving short duration of contemporary chemotherapy 11/171 pts (7%) exhibited progressive disease in response to FOLFOX (EORTC Intergroup Trial Lancet 2008) Does neoadjuvant chemotherapy reveal disease precluding surgical treatment of initially resectable CRLM? Reddy SK, Tsung A, Marsh JM, Geller D. JSO 2012 Median progression-free survival for metastatic unresectable cancer exceeds 6 months in most phase III trials Extended durations of chemotherapy treatment would be required to identify those patients with interval disease progression
16 How useful is prehepatectomy chemotherapy an invivo test of response? Response to chemotherapy before hepatic resection will help determine optimal post hepatectomy chemotherapy 14% and 9% of patients whose disease was downsized from unresectable to resectable CLM responded to second and third lines of treatment when first-line chemotherapy failed. Adam R et al. Ann Surg 2004
17 Disease progression on pre-hepatectomy chemotherapy may render previously resectable CLM unresectable, thereby preventing opportunity for long term survival? EORTC 40983: 364 pts 4 mets assigned to liver resection with or without perioperative chemotherapy 67/182 pts assigned to chemo had objective response 11 progressed, 8 of whom no longer resectable 83% resected vs 84% in surgery alone group
18
19 Chemotherapy induced liver injury Irinotecan Steatosis, Chemotherapy Associated SteatoHepatitis (CASH) Oxaliplatin: Sinosoidal injury (Sinusoidal Obstruction Syndrome- SOS, blue liver syndrome ) Bevacizumab: Impairment of liver regeneration (anti-vegf)
20 Does preoperative chemotherapy increase the morbidity and mortality after surgery? EORTC Intergroup trial 40983, overall complication increased from 16-25%, rate of hepatic complications from 9-15%. No change in mortality. Norlinger et al, Lancet 2008 Multicentric cohort study showing significantly higher complication rate 24% vs 37% in patients subjected to neoadjuvant chemotherapy for resectable lesions. Adam R et al. Ann Surg 2010 In the setting of extended surgical resection, may contribute to development of small for size syndrome and fatal liver failure
21 Can neoadjuvant chemotherapy help select patient for type of surgical resection? Recurrence following liver resection is expected Shift from anatomical resection to parenchymal sparing strategies to improve subsequent resectability Trade off: Higher risk of margin positive resection

22 Margin status remains an important determinant of survival after surgical resection of colorectal liver metastases in the era of modern chemotherapy. Vauthey JN et al. Ann Surg 2013 Optimal morphological response
23 Margin status remains an important determinant of survival after surgical resection of colorectal liver metastases in the era of modern chemotherapy. Vauthey JN et al. Ann Surg 2013 Pathological response: Area of residual viable tumour cells within each metastatic lesion as percentage of total tumour surface area Minor response: 0-49% Major response: 50% Multiple nodules: Mean of response in each individual nodule
24 Margin status remains an important determinant of survival after surgical resection of colorectal liver metastases in the era of modern chemotherapy. Vauthey JN et al. Ann Surg of 378 resections (14%) R1 resections. 246 (65%) synchronous lesions. No of mets median=2, mean=3 5yr OS R0 vs R1 resection: 55% and 26% Survival benefit a/w negative margins greater in patients with suboptimal morphological response (5yr OS: 62% vs 11%, P=0.007); patients with optimal response (3yr OS rate: 92% vs 88%, P=0.917) Greater in patients with minor pathological response (5yr OS: 46% vs 0%, P=0.002); patients with major response (5yr OS: 63% vs 67%, P=0.587)
25 Margin status remains an important determinant of survival after surgical resection of colorectal liver metastases in the era of modern chemotherapy. Vauthey JN et al. Ann Surg 2013 Optimal radiological response : Multiple wedge resections (parenchymal sparing) Suboptimal radiological response : Anatomical resections



26 Dilemma - The disappearing metastasis Nov 2011 Feb 2012
27 The disappearing metastases Complete clinical response from chemotherapy to sites of CLM obviates the need for surgical extirpation of these sites? Benoist S et al reported the recurrence of disease at site of unresected disappearing lesions in 23 of 31 lesions (74%). J Clin Oncol Tanaka et al reported similar findings with recurrence in 11 of 27 lesions (41%) at median of 14 months f/u. Ann Surg 2009.
28 Predictors of patient with at least one metastases that disappears Small size <3cm Multiple lesions > 3 Longer duration of chemotherapy Benoist S et al. J Clin Oncol 2006 Van Vledder MG et al. J Gastrointest Surg 2010.
29 The disappearing metastases PET does not reliably predict pathological response 34 lesions in 14 patients had resolution of PET positivity after prehepatectomy chemotherapy. 29 (85%) had viable tumour on microscopic examination Tan MCB et al. J Gastrointest Surg % of complete pathological response have radiologically evident lesions
30 The disappearing metastases Good quality MRI to identify missing metastases <10% of pts have complete radiological response of all liver metastases, hence most patients will undergo surgery for residual disease IOUS identifies additional lesions that alter surgical planning in a substantial number of patients Extended prehepatectomy chemotherapy induces pathological changes in surrounding non-tumour bearing liver that reduces sensitivity of both IOUS and visual examination to detect small lesions
31 Fong Clinical Risk Score Ann Surg 1999 Nodal status of primary DFI from primary to discovery of liver mets <12mths Number of tumours >1 Preop CEA > 200ng/ml Largest tumor > 5cm
32 Effect of neoadjuvant chemotherapy in patients with resectable colorectal liver metastases Zhu DX et al. PlosOne 2014 Retrospective analysis of 466pts between 2000 and 2010 Pts divided into pts who received neoadj chemo (n=121) and pts who had adj chemo (n=345) No diff in morbidity, 30-day mortality and 5yr survival (52% vs 48%) Risk factors: Primary tumour T4, 4 mets, largest met 5cm, serum CEA 5ng/ml Low risk 0-2 factors, high risk 3-4 factors Low risk group no survival benefit from neoadjuvant chemo, high risk group survival benefit (5yr 39% vs 33%, p=0.028)
33 Liver resection for multiple colorectal liver metastases with surgery upfront approach: Bi-institutional analysis of 736 cases. Saiura A et al. World J Surg resectable pts and 111 initially unresectable (ie converted) 1993 to 2008 Upfront resectable pts did not receive any preop-chemotherapy and few had adjuvant chemotherapy Patients divided into 3 groups: Group A 1-3 tumours (n=493), Group B 4-7 tumours (n=141), Group C 8 or more tumours (n=102) 5 year overall and recurrence free survival: Group A: 51% and 21%, Group B: 56% and 29%, Group C: 33% and 1.7% Prognostic factors for DFS: Extrahepatic disease, positive surgical margin, nodal involvement of primary, tumour number 4, size >5cm, CEA>200ng/mL, primary site (rectum) Prognostic factors for OS: Node positive primary tumour, EHD, size 5cm, positive margin
34 Should neoadjuvant chemotherapy be given in resectable colorectal liver metastases? Are there sufficient risks of possible poor tumor biology such that addition of one additional factor (ie progression on chemotherapy) would be sufficient to not offer resection? Does the patient have diabetes, obesity of other factors that compromise liver health, such that any degree of liver injury from preoperative chemotherapy might be significantly deleterious? Though resectable, will a minor response make the operation significantly less difficult (eg more easily achieving negative margins, avoid a critical vein, or lessen likelihood of conversion of laparoscopic resection)?
35 Recommendations based on available evidence Surgery upfront followed by adjuvant chemotherapy If need be, limit chemotherapy to 2-4 cycles before performing surgery Avoid pre-operative chemotherapy altogether in cases of small limited lesions (<3cm), else use fiduciary or consider ablation of small lesions prechemotherapy
36 Pattern of recurrence following hepatectomy Most patients with multiple, bilobar disease will ultimately recur Half will recur within 3 years, half of these recurrences isolated to the liver Extra-hepatic metastases most common form of disease recurrence among patients with multiple metastases, liver recurrence most common in patients with small number of mets More extrahepatic than intrahepatic recurrence for initially unresectable metastases downstaged by chemotherapy


37 BJS 2013 Total = 650 hepatectomies

38 Repeat hepatectomy Tumour characteristics Wicherts et al. BJS 2013

39 Repeat hepatectomy - Histopathology Wicherts et al. BJS 2013
40 Overall survival Wicherts et al. BJS 2013 Similar postoperative morbidity and mortality P= and 5yr OS: 76% and 54% with repeat hepatectomy 58% and 45% with one hepatectomy
41 Survival benefit of repeat resection of successive recurrences after the initial hepatic resection for colorectal liver metastases Oba M, Makuuchi M, Kokudo N et al. Surgery : 336 pts upfront liver resection Adjuvant chemotherapy not standard of care; 77 pts receiving chemotherapy excluded Surgical management: Upfront resection regardless of number, distribution or extent
42 Survival benefit of repeat resection of successive recurrences after the initial hepatic resection for colorectal liver metastases. Oba M, Makuuchi M, Kokudo N et al. Surgery 2016 Overall survival Recurrence free survival
43 Survival benefit of repeat resection of successive recurrences after the initial hepatic resection for colorectal liver metastases. Oba M, Makuuchi M, Kokudo N et al. Surgery 2016 At each repeat resection, approx 1/3 recurrence free Of those recurred, approx half suitable for further resection Survival benefit of repeat resections maintained regardless of number of previous resections Sequential repeat resections offer possibility of cure
44 BJS 2016
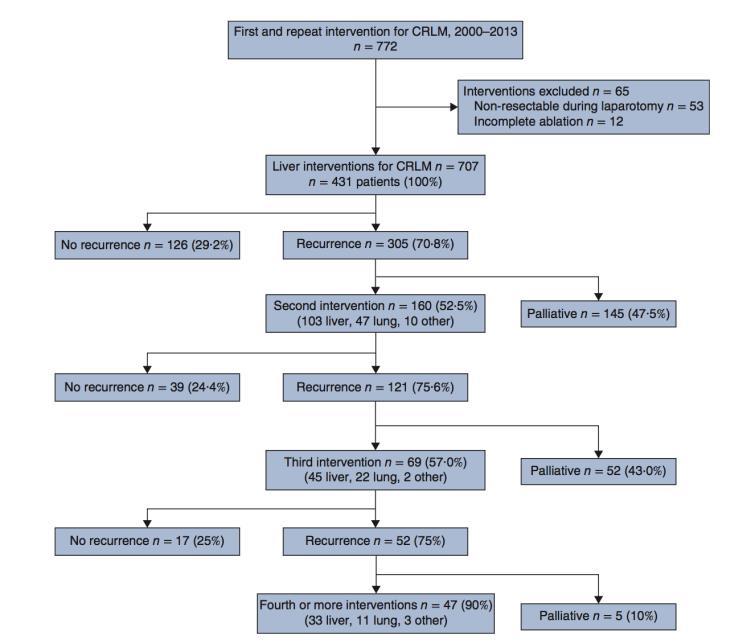
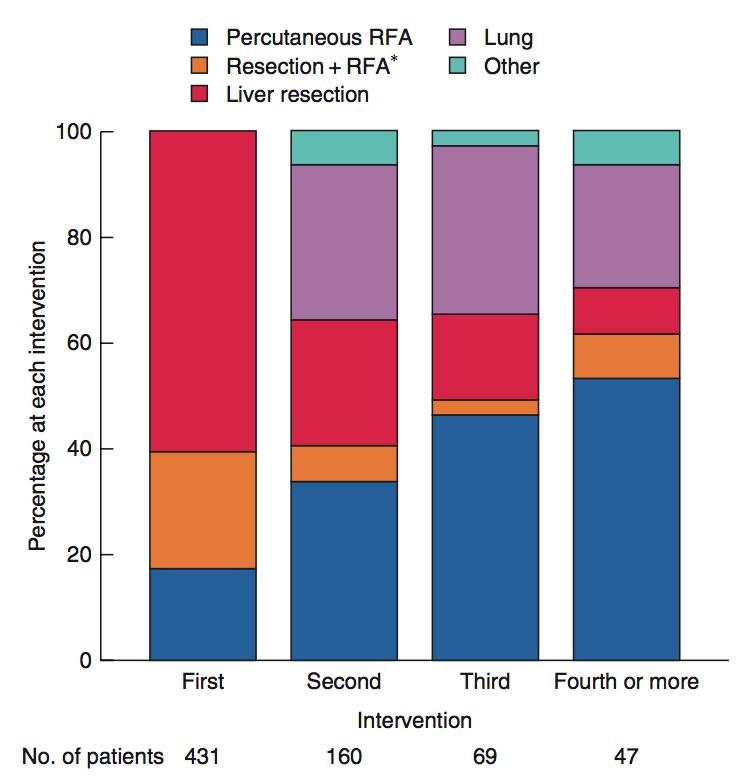
45 Overall recurrence rate 83.5% (152/182) for percutaneous RFA cf 66.6% (201/302) for liver resection (P<0.001) Intra-hepatic recurrence 59.9% in RFA vs 23.9% in liver resection (P<0.001) Risk of ablation-site recurrence after RFA 26.9% (50/186pts, 250 lesions) 92% (46/50) of ablation site recurrence treated with curative intent (41 repeat RFA, 5 resection)
46
47 Selecting patients for a second hepatectomy for colorectal metastases: A systemic review and meta-analysis. Luo LX et al. EJSO pts from 27 studies Recurrent CRLM mote likely solitary, unilobar and smaller Better survival after second hepatectomy in high quality studies Predictors of better survival after second hepatectomy: DFI>1yr, solitary met, unilobar, size 5cm, lack of EHD and R0 resection
48 Conclusion repeat hepatectomy Morbidity and mortality similar to first time hepatectomy Progression free survival maintained with each hepatectomy Possible better survival Increasing indication for ablative approaches
49 Evaluating agreement regarding the resectability of colorectal liver metastases: a national case-based survey of hepatic surgeons. Mohammad WM et al. HPB 2012 Investigates contemporary hepatic surgeon perceptions of resectability of CLM 10 scenarios ranging from a solitary, peripheral lesion to extensive bilobar involvement Evaluate CT images to determine if amenable to resection with or without adjunctive therapies such as radiofrequency ablation, PVE and staged resection
50 Evaluating agreement regarding the resectability of colorectal liver metastases: a national case-based survey of hepatic surgeons Mohammad WM et al. HPB 2012 Consensus only in 2 scenarios with clearly resectable and unresectable disease Marked divergence in opinion on the remainder of cases Little agreement on type and number of non-resectional adjuncts to surgery
51
52 Conclusions Significant heterogeneity in approaches to patient with CLM Lack of randomized trials Rapidly changing management paradigms Imperative CLM patients to be evaluated in multidisciplinary setting by all surgical and oncologic specialties


53 Thank You
Treatment of Colorectal Liver Metastases State of the Art
 Treatment of Colorectal Liver Metastases State of the Art Eddie K. Abdalla, MD, FACS Professor and Chairman of Surgery Chief of Hepatobiliary Surgery Hilton Metropolitan Palace Hotel Beirut 16 November,
Treatment of Colorectal Liver Metastases State of the Art Eddie K. Abdalla, MD, FACS Professor and Chairman of Surgery Chief of Hepatobiliary Surgery Hilton Metropolitan Palace Hotel Beirut 16 November,
Colon Cancer Liver Metastases: Liver-Directed Therapy
 Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
Colorectal Liver Metastases Metachronous
 Colorectal Liver Metastases Metachronous Professor Rowan Parks Professor of Surgical Sciences University of Edinburgh No disclosures Natural History of Unresected Untreated Colorectal Metastases Year N
Colorectal Liver Metastases Metachronous Professor Rowan Parks Professor of Surgical Sciences University of Edinburgh No disclosures Natural History of Unresected Untreated Colorectal Metastases Year N
MANAGEMENT OF COLORECTAL METASTASES. Robert Warren, MD. The Postgraduate Course in General Surgery March 22, /22/2011
 MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D.
 Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D. Department of Surgery Grand Rounds University of Kentucky January 15, 2014 Metastatic Colorectal Cancer (CRC)
Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D. Department of Surgery Grand Rounds University of Kentucky January 15, 2014 Metastatic Colorectal Cancer (CRC)
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options
 State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
Management of colorectal cancer liver metastases
 Management of colorectal cancer liver metastases Aliakbarian M. M.D. Assistant professor of surgery Organ Transplant & Hepatopancreatobiliary Surgeon SUBJECTS The importance of surgical resection in colorectal
Management of colorectal cancer liver metastases Aliakbarian M. M.D. Assistant professor of surgery Organ Transplant & Hepatopancreatobiliary Surgeon SUBJECTS The importance of surgical resection in colorectal
Trattamento chirurgico delle lesioni epatiche secondarie difficili. Adelmo Antonucci Chirurgia Oncologica e Epato-bilio-pancreatica
 Trattamento chirurgico delle lesioni epatiche secondarie difficili Adelmo Antonucci Chirurgia Oncologica e Epato-bilio-pancreatica What does it mean difficult lesions? Diagnosis Treatment Small size Unfit
Trattamento chirurgico delle lesioni epatiche secondarie difficili Adelmo Antonucci Chirurgia Oncologica e Epato-bilio-pancreatica What does it mean difficult lesions? Diagnosis Treatment Small size Unfit
Multidisciplinary Treatment Strategies for Primary and Metastatic Liver Cancers
 Multidisciplinary Treatment Strategies for Primary and Metastatic Liver Cancers Ching-Wei D. Tzeng, M.D. Assistant Professor Surgical Oncology University of Kentucky Markey Cancer Center Affiliate Network
Multidisciplinary Treatment Strategies for Primary and Metastatic Liver Cancers Ching-Wei D. Tzeng, M.D. Assistant Professor Surgical Oncology University of Kentucky Markey Cancer Center Affiliate Network
The Surgical Management of Colorectal Metastases
 11th July 2017 Bowel Cancer UK The Surgical Management of Colorectal Metastases Ben Cresswell MD(Res) FRCS Consultant HPB Surgeon The Basingstoke Hepatobiliary Unit United Kingdom Surgical Management of
11th July 2017 Bowel Cancer UK The Surgical Management of Colorectal Metastases Ben Cresswell MD(Res) FRCS Consultant HPB Surgeon The Basingstoke Hepatobiliary Unit United Kingdom Surgical Management of
Management of Colorectal Liver Metastases
 Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
Management of Colorectal Liver Metastases MM Bernon, JEJ Krige HPB Surgical Unit, Groote Schuur Hospital Department of Surgery, University of Cape Town 50% of patients with colorectal cancer develop liver
Treatment strategy of metastatic rectal cancer
 35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
Surgical Management of Advanced Stage Colon Cancer. Nathan Huber, MD 6/11/14
 Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan
 State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
Chemotherapy for resectable liver mets: Options and Issues. Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA
 Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
8 Giornata Onco-ematologica Varesina
 Azienda Ospedaliera Sant Antonio Abate di Gallarate 8 Giornata Onco-ematologica Varesina Le esperienze di eccellenza del DIPO di Varese Metastasi epatiche da tumore del colon-retto: terapia medica in funzione
Azienda Ospedaliera Sant Antonio Abate di Gallarate 8 Giornata Onco-ematologica Varesina Le esperienze di eccellenza del DIPO di Varese Metastasi epatiche da tumore del colon-retto: terapia medica in funzione
Margin status in liver resections for colorectal metastases Orlando Jorge M. Torres MD, PhD
 Margin status in liver resections for colorectal metastases Orlando Jorge M. Torres MD, PhD Full Professor and Chairman Department of Gastrointestinal Surgery Hepatopancreatobiliary Unit Universidade Federal
Margin status in liver resections for colorectal metastases Orlando Jorge M. Torres MD, PhD Full Professor and Chairman Department of Gastrointestinal Surgery Hepatopancreatobiliary Unit Universidade Federal
Unresectable or boarderline resectable disease
 ESMO Preceptorship Colorectal Cancer Nov 2016 Barcelona Unresectable or boarderline resectable disease Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West German Cancer Center (NWTZ) Learning
ESMO Preceptorship Colorectal Cancer Nov 2016 Barcelona Unresectable or boarderline resectable disease Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West German Cancer Center (NWTZ) Learning
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS
 Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
Management of Stage IV Colorectal Cancer: Expanding the Horizon
 Management of Stage IV Colorectal Cancer: Expanding the Horizon May Tee, MD, MPH and Jan Franko, MD, PhD MercyOne Surgical Group (Mercy Surgical Affiliates) GI Oncology Conference 2019 March 1, 2019 Disclosures
Management of Stage IV Colorectal Cancer: Expanding the Horizon May Tee, MD, MPH and Jan Franko, MD, PhD MercyOne Surgical Group (Mercy Surgical Affiliates) GI Oncology Conference 2019 March 1, 2019 Disclosures
How to deal with synchronous primary and liver metastases
 How to deal with synchronous primary and liver metastases Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB) Department of Surgery.
How to deal with synchronous primary and liver metastases Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB) Department of Surgery.
Aintree University Hospital
 Aintree University Hospital Liverpool, UK Evolving role of DEBIRI with DC Bead - TACE in mcrc Hassan Z Malik MD FRCS Consultant Hepatobiliary Surgeon Hassan Z Malik is a consultant to Biocompatibles UK
Aintree University Hospital Liverpool, UK Evolving role of DEBIRI with DC Bead - TACE in mcrc Hassan Z Malik MD FRCS Consultant Hepatobiliary Surgeon Hassan Z Malik is a consultant to Biocompatibles UK
E importante t che il chirurgo conosca il profilo molecolare del carcinoma del colon?
 E importante t che il chirurgo conosca il profilo molecolare del carcinoma del colon? Giuseppe Aprile Dipartimento di Oncologia Dipartimento di Oncologia Azienda Ospedaliero-Universitaria - Udine Dr. Giuseppe
E importante t che il chirurgo conosca il profilo molecolare del carcinoma del colon? Giuseppe Aprile Dipartimento di Oncologia Dipartimento di Oncologia Azienda Ospedaliero-Universitaria - Udine Dr. Giuseppe
Jose Ramos. Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma
 Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Primary tumor with synchronous metastases
 Metastatic colorectal cancer: special clinical situations Primary tumor with synchronous metastases Stefan Heinrich & Hauke Lang Department of General, Visceral and Transplantation Surgery University Hospital
Metastatic colorectal cancer: special clinical situations Primary tumor with synchronous metastases Stefan Heinrich & Hauke Lang Department of General, Visceral and Transplantation Surgery University Hospital
Introduction. Case Report
 Case Report A patient who showed a pathologically complete response after undergoing treatment with XELOX plus bevacizumab for synchronous liver metastasis of grade H2 from sigmoid colon cancer Yasuhito
Case Report A patient who showed a pathologically complete response after undergoing treatment with XELOX plus bevacizumab for synchronous liver metastasis of grade H2 from sigmoid colon cancer Yasuhito
Behandeling van colorectale levermetastasen. Rol van beeldvorming van de lever bij colorectaal carcinoom
 Behandeling van colorectale levermetastasen Rol van beeldvorming van de lever bij colorectaal carcinoom B. Op de Beeck Universitair Ziekenhuis Antwerpen bart.op.de.beeck@uza.be 10.12.2016 AZ Turnhout campus
Behandeling van colorectale levermetastasen Rol van beeldvorming van de lever bij colorectaal carcinoom B. Op de Beeck Universitair Ziekenhuis Antwerpen bart.op.de.beeck@uza.be 10.12.2016 AZ Turnhout campus
Liver surgery for colorectal liver metastases. Keith Roberts, Consultant Liver Transplant and Liver/Pancreas Surgeon University Hospitals Birmingham
 Liver surgery for colorectal liver metastases Keith Roberts, Consultant Liver Transplant and Liver/Pancreas Surgeon University Hospitals Birmingham Introduction: what do we do? UHB Liver Unit: Liver resections
Liver surgery for colorectal liver metastases Keith Roberts, Consultant Liver Transplant and Liver/Pancreas Surgeon University Hospitals Birmingham Introduction: what do we do? UHB Liver Unit: Liver resections
ADJUVANT CHEMOTHERAPY FOR RECTAL CANCER
 ESMO Preceptorship Programme Colorectal Cancer Barcelona November, 25-26, 2016 ADJUVANT CHEMOTHERAPY FOR RECTAL CANCER Andrés Cervantes Professor of Medicine OLD APPROACH TO RECTAL CANCER Surgical resection
ESMO Preceptorship Programme Colorectal Cancer Barcelona November, 25-26, 2016 ADJUVANT CHEMOTHERAPY FOR RECTAL CANCER Andrés Cervantes Professor of Medicine OLD APPROACH TO RECTAL CANCER Surgical resection
Dr Adam Bartlett. General Surgeon Senior Lecturer University of Auckland Auckland City Hospital
 Dr Adam Bartlett General Surgeon Senior Lecturer University of Auckland Auckland City Hospital 11:05-11:15 Hepatic Metastectomy is Associated with Improved Survival Where is everyone? Hepatic Metastectomy
Dr Adam Bartlett General Surgeon Senior Lecturer University of Auckland Auckland City Hospital 11:05-11:15 Hepatic Metastectomy is Associated with Improved Survival Where is everyone? Hepatic Metastectomy
Dr. Iain Tan. Senior Consultant GI Medical Oncologist National Cancer Centre Singapore
 ESMO-ASIA 2017 Preceptorship (GI cancers) Session: Metastatic colorectal cancer, liver limited metastases Topic: Unresectable or borderline resectable : chemotherapy +/- targeted agents Dr. Iain Tan Senior
ESMO-ASIA 2017 Preceptorship (GI cancers) Session: Metastatic colorectal cancer, liver limited metastases Topic: Unresectable or borderline resectable : chemotherapy +/- targeted agents Dr. Iain Tan Senior
Advances in gastric cancer: How to approach localised disease?
 Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
How to integrate surgery in the treatment of patients with liver-only metastatic disease
 How to integrate surgery in the treatment of patients with liver-only metastatic disease Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB)
How to integrate surgery in the treatment of patients with liver-only metastatic disease Luis Sabater Ortí MD, PhD Associate Professor University of Valencia European Board Surgical Qualification HBP (EBSQ-HPB)
Survival Outcomes of Liver Metastasectomy in Colorectal Cancer Cases: A Single-Center Analysis in Turkey
 DOI:http://dx.doi.org/10.7314/APJCP.2014.15.13.5195 Survival after Liver Metastasectomy in Colorectal Cancer Cases in Turkey RESEARCH ARTICLE Survival Outcomes of Liver Metastasectomy in Colorectal Cancer
DOI:http://dx.doi.org/10.7314/APJCP.2014.15.13.5195 Survival after Liver Metastasectomy in Colorectal Cancer Cases in Turkey RESEARCH ARTICLE Survival Outcomes of Liver Metastasectomy in Colorectal Cancer
ITALIAN SURGICAL SOCIETY ENDOCRINE SURGERY SCHOOL LIVER METASTASIS FROM NEUROENDOCRINE TUMORS
 ITALIAN SURGICAL SOCIETY ENDOCRINE SURGERY SCHOOL LIVER METASTASIS FROM NEUROENDOCRINE TUMORS Gennaro Favia Liver metastasis from NETs Incidence 75% in NETs Knox CD, J Gastroint Surg 2006 .but 28-45% cases
ITALIAN SURGICAL SOCIETY ENDOCRINE SURGERY SCHOOL LIVER METASTASIS FROM NEUROENDOCRINE TUMORS Gennaro Favia Liver metastasis from NETs Incidence 75% in NETs Knox CD, J Gastroint Surg 2006 .but 28-45% cases
Current Treatment of Colorectal Metastases. Dr. Thavanathan Surgical Grand Rounds February 1, 2005
 Current Treatment of Colorectal Metastases Dr. Thavanathan Surgical Grand Rounds February 1, 2005 25% will have metastases at initial presentation 25-50% 50% will develop metastases later 40% of potentially
Current Treatment of Colorectal Metastases Dr. Thavanathan Surgical Grand Rounds February 1, 2005 25% will have metastases at initial presentation 25-50% 50% will develop metastases later 40% of potentially
Predictors of a True Complete Response Among Disappearing Liver Metastases From Colorectal Cancer After Chemotherapy
 Original Article Predictors of a True Complete Response Among Disappearing Liver Metastases From Colorectal Cancer After Chemotherapy Rebecca C. Auer, MD 1 ; Rebekah R. White, MD 2 ; Nancy E. Kemeny, MD
Original Article Predictors of a True Complete Response Among Disappearing Liver Metastases From Colorectal Cancer After Chemotherapy Rebecca C. Auer, MD 1 ; Rebekah R. White, MD 2 ; Nancy E. Kemeny, MD
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Risk factors for cancer recurrence or death within 6 months after liver resection in patients with colorectal cancer liver metastasis
 ORIGINAL ARTICLE pissn 2288-6575 eissn 2288-6796 http://dx.doi.org/10.4174/astr.2016.90.5.257 Annals of Surgical Treatment and Research Risk factors for cancer recurrence or death within 6 months after
ORIGINAL ARTICLE pissn 2288-6575 eissn 2288-6796 http://dx.doi.org/10.4174/astr.2016.90.5.257 Annals of Surgical Treatment and Research Risk factors for cancer recurrence or death within 6 months after
Unresectable or boarderline resectable (Groupp 1) chemotherpy +/- targeted agents
 chemotherpy +/- targeted agents") ESMO Preceptorship Program 27.-28. March Singapore Unresectable or boarderline resectable (Groupp 1) chemotherpy +/- targeted agents Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West
ESMO Preceptorship Program 27.-28. March Singapore Unresectable or boarderline resectable (Groupp 1) chemotherpy +/- targeted agents Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West
Radiation Therapy for Liver Malignancies
 Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Perioperative chemotherapy for colorectal cancer livermetastases: what is the optimal strategy?
 Perioperative chemotherapy for colorectal cancer livermetastases: what is the optimal strategy? Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be A classical case
Perioperative chemotherapy for colorectal cancer livermetastases: what is the optimal strategy? Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be A classical case
LIVER SURGERY 2. Case 1. Med 5 Refresher Course (Surgery) 2013/14. Dr Sunny Cheung
 2013/14. Dr Sunny Cheung") LIVER SURGERY 2 Med 5 Refresher Course (Surgery) 2013/14 24 Jun 2013 Dr Sunny Cheung Case 1 50/M Sudden onset of epigastric pain Abdominal distension Confused HR 120 BP 80/50 Haemocue = 8 What should you
LIVER SURGERY 2 Med 5 Refresher Course (Surgery) 2013/14 24 Jun 2013 Dr Sunny Cheung Case 1 50/M Sudden onset of epigastric pain Abdominal distension Confused HR 120 BP 80/50 Haemocue = 8 What should you
BACKGROUND: STUDY DESIGN: RESULTS: CONCLUSIONS:
 Improved Survival after Resection of Liver and Lung Colorectal Metastases Compared with Liver-Only Metastases: A Study of 112 Patients with Limited Lung Metastatic Disease Antoine Brouquet, MD, Jean Nicolas
Improved Survival after Resection of Liver and Lung Colorectal Metastases Compared with Liver-Only Metastases: A Study of 112 Patients with Limited Lung Metastatic Disease Antoine Brouquet, MD, Jean Nicolas
Treatment of oligometastatic NSCLC
 Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
Treatment of oligometastatic NSCLC Jarosław Kużdżał Department of Thoracic Surgery Jagiellonian University Collegium Medicum, John Paul II Hospital, Cracow New idea? 14 NSCLC patients with solitary extrathoracic
Surgical management of HCC. Evangelos Prassas Hepatobiliary and Pancreatic Surgery / Liver Transplantation Kings College Hospital / London
 Surgical management of HCC Evangelos Prassas Hepatobiliary and Pancreatic Surgery / Liver Transplantation Kings College Hospital / London Global distribution of HCC and staging systems WEST 1. Italy (Milan,
Surgical management of HCC Evangelos Prassas Hepatobiliary and Pancreatic Surgery / Liver Transplantation Kings College Hospital / London Global distribution of HCC and staging systems WEST 1. Italy (Milan,
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Staging Colorectal Cancer
 Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Staging Colorectal Cancer CT is recommended as the initial staging scan for colorectal cancer to assess local extent of the disease and to look for metastases to the liver and/or lung Further imaging for
Efficacy of Neoadjuvant Chemotherapy Regimens Prior to Resection of Colorectal Liver Metastases
 Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine 2-11-2008 Efficacy of Neoadjuvant Chemotherapy Regimens Prior to Resection
Yale University EliScholar A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine 2-11-2008 Efficacy of Neoadjuvant Chemotherapy Regimens Prior to Resection
CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION
 CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION PROVIDED AS AN EDUCATIONAL SERVICE BY THE INSTITUTE FOR CONTINUING HEALTHCARE EDUCATION SUPPORTED BY AN EDUCATIONAL GRANT FROM GENENTECH LEARNING
CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION PROVIDED AS AN EDUCATIONAL SERVICE BY THE INSTITUTE FOR CONTINUING HEALTHCARE EDUCATION SUPPORTED BY AN EDUCATIONAL GRANT FROM GENENTECH LEARNING
Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age. Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010
 Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010 Molecular mechanisms for cancer Prevention and screening Molecular
Evolution of Surgery: Role of the Surgeon in the Molecular and Technology Age Yuman Fong, MD Memorial Sloan-Kettering Cancer Center Rio 2010 Molecular mechanisms for cancer Prevention and screening Molecular
Treating Liver Limited or Oligometastatic CRC
 ESMO Preceptorship Colorectal Cancer Nov 2016 Barcelona Treating Liver Limited or Oligometastatic CRC Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West German Cancer Center (NWTZ) Learning
ESMO Preceptorship Colorectal Cancer Nov 2016 Barcelona Treating Liver Limited or Oligometastatic CRC Claus-Henning Köhne Klinik für Onkologie und Hämatologie North West German Cancer Center (NWTZ) Learning
Radiofrequency Ablation of Primary or Metastatic Liver Tumors
 Radiofrequency Ablation of Primary or Metastatic Liver Tumors Policy Number: 7.01.91 Last Review: 9/2018 Origination: 2/1996 Next Review: 9/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Radiofrequency Ablation of Primary or Metastatic Liver Tumors Policy Number: 7.01.91 Last Review: 9/2018 Origination: 2/1996 Next Review: 9/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC)
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases
 Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
Manchester Cancer Colorectal Pathway Board: Guidelines for management of colorectal hepatic metastases Date: April 2015 Date for review: April 2018 1. Principles The recognised specialist HPB MDT for Greater
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh
 Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Surgical Therapy of GEP-NET: An Overview
 Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 Interventional radiology and stereotactic radiotherapy Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
ESMO Preceptorship Programme Colorectal Cancer Barcelona October 2017 Interventional radiology and stereotactic radiotherapy Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures: last 5 years Speaker:
COLORECTAL CANCER CASES
 COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
COLORECTAL CANCER CASES Case #1 Case #2 Colorectal Cancer Case 1 A 52 year-old female attends her family physician for her yearly complete physical examination. Her past medical history is significant
Management of Liver Metastasis from Colorectal Carcinoma. Aisha White, M.D. SUNY Downstate Division of Transplantation
 Management of Liver Metastasis from Colorectal Carcinoma Aisha White, M.D. SUNY Downstate Division of Transplantation Management of Colorectal Liver Metastasis Epidemiology 25% of patients diagnosed
Management of Liver Metastasis from Colorectal Carcinoma Aisha White, M.D. SUNY Downstate Division of Transplantation Management of Colorectal Liver Metastasis Epidemiology 25% of patients diagnosed
Carcinoma del retto: Highlights
 Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
COLON CANCER PERITONEAL CARCINOMATOSIS TREATMENT Prof. Annibale Donini
 UNIVERSITY OF PERUGIA Department of General and Emergency Surgery Chief: Prof. Annibale Donini COLON CANCER PERITONEAL CARCINOMATOSIS TREATMENT Prof. Annibale Donini COLON CANCER IS A HIGHLY FREQUENT NEOPLASIA
UNIVERSITY OF PERUGIA Department of General and Emergency Surgery Chief: Prof. Annibale Donini COLON CANCER PERITONEAL CARCINOMATOSIS TREATMENT Prof. Annibale Donini COLON CANCER IS A HIGHLY FREQUENT NEOPLASIA
TIMOTHY M. PAWLIK, RICHARD D. SCHULICK, MICHAEL A. CHOTI
 The Oncologist Hepatobiliary Expanding Criteria for Resectability of Colorectal Liver Metastases TIMOTHY M. PAWLIK,RICHARD D. SCHULICK,MICHAEL A. CHOTI Department of Surgery, Johns Hopkins University School
The Oncologist Hepatobiliary Expanding Criteria for Resectability of Colorectal Liver Metastases TIMOTHY M. PAWLIK,RICHARD D. SCHULICK,MICHAEL A. CHOTI Department of Surgery, Johns Hopkins University School
Aggressive surgery in the multimodality treatment of liver metastases from colorectal cancer
 Journal of BUON 12: 209-213, 2007 2007 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Aggressive surgery in the multimodality treatment of liver metastases from colorectal cancer N.
Journal of BUON 12: 209-213, 2007 2007 Zerbinis Medical Publications. Printed in Greece ORIGINAL ARTICLE Aggressive surgery in the multimodality treatment of liver metastases from colorectal cancer N.
Hepatobiliary Malignancies Retrospective Study at Truman Medical Center
 Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
Disclosure. Nothing to Disclose Will not be discussing off label use of any of the medications
 Disclosure Nothing to Disclose Will not be discussing off label use of any of the medications Where s Cranbrook? Follow Up of Colorectal Cancer Stage 0 (in-situ disease) and Stage I (T1-2 N0) Follow up
Disclosure Nothing to Disclose Will not be discussing off label use of any of the medications Where s Cranbrook? Follow Up of Colorectal Cancer Stage 0 (in-situ disease) and Stage I (T1-2 N0) Follow up
How to deal with patients with isolated peritoneal metastases
 ESMO Preceptorship Programme Colorectal Valencia 18-19 May 2018 Michel DUCREUX, MD, PhD Gustave Roussy Cancer Centre, Grand Paris, FRANCE How to deal with patients with isolated peritoneal metastases DISCLOSURE
ESMO Preceptorship Programme Colorectal Valencia 18-19 May 2018 Michel DUCREUX, MD, PhD Gustave Roussy Cancer Centre, Grand Paris, FRANCE How to deal with patients with isolated peritoneal metastases DISCLOSURE
Are we making progress? Marked reduction in operative morbidity and mortality
 Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 5
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 5 Contents 5. Assessment & Management of Liver Metastases 42 5.1. Metachronous
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 5 Contents 5. Assessment & Management of Liver Metastases 42 5.1. Metachronous
Title: What is the role of pre-operative PET/PET-CT in the management of patients with
 Title: What is the role of pre-operative PET/PET-CT in the management of patients with potentially resectable colorectal cancer liver metastasis? Pablo E. Serrano, Julian F. Daza, Natalie M. Solis June
Title: What is the role of pre-operative PET/PET-CT in the management of patients with potentially resectable colorectal cancer liver metastasis? Pablo E. Serrano, Julian F. Daza, Natalie M. Solis June
Treatment of Locally Advanced Rectal Cancer: Current Concepts
 Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Regional Therapy for Management of Peritoneal Carcinomatosis from Gastrointestinal Malignancies
 Regional Therapy for Management of Peritoneal Carcinomatosis from Gastrointestinal Malignancies Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service City of Hope Division of Surgical Oncology September
Regional Therapy for Management of Peritoneal Carcinomatosis from Gastrointestinal Malignancies Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service City of Hope Division of Surgical Oncology September
Parenchyma saving resectionsfictions. (Colorectal liver metastasis)
") Parenchyma saving resectionsfictions or facts? (Colorectal liver metastasis) Bjørn Edwin, professor, MD, PhD Section manager, Clinical Research The Interventional Center and HPB-Department Oslo University
Parenchyma saving resectionsfictions or facts? (Colorectal liver metastasis) Bjørn Edwin, professor, MD, PhD Section manager, Clinical Research The Interventional Center and HPB-Department Oslo University
MEETING SUMMARY ESMO 2018, Munich, Germany. Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER
 MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
Trends and Comparative Effectiveness in Treatment of Stage IV Colorectal Adenocarcinoma
 Trends and Comparative Effectiveness in Treatment of Stage IV Colorectal Adenocarcinoma Taylor S. Riall, MD, PhD CERCIT Workshop October 19, 2012 Department of Surgery Center for Comparative Effectiveness
Trends and Comparative Effectiveness in Treatment of Stage IV Colorectal Adenocarcinoma Taylor S. Riall, MD, PhD CERCIT Workshop October 19, 2012 Department of Surgery Center for Comparative Effectiveness
Adjuvant/neoadjuvant systemic treatment of colorectal cancer
 5th ESO-ESMO Eastern Europe and Balkan Region Masterclass in Medical Oncology Belgrade, June 19 th 2018 Adjuvant/neoadjuvant systemic treatment of colorectal cancer Carlotta Antoniotti Polo Oncologico
5th ESO-ESMO Eastern Europe and Balkan Region Masterclass in Medical Oncology Belgrade, June 19 th 2018 Adjuvant/neoadjuvant systemic treatment of colorectal cancer Carlotta Antoniotti Polo Oncologico
What s New in Colon Cancer? Therapy over the last decade
 What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
Disclosures. Preoperative Treatment: Chemotherapy or ChemoRT? Adjuvant chemotherapy helps. so what about chemo first?
 Disclosures Preoperative Treatment: Chemotherapy or ChemoRT? Advisory boards Genentech (travel only), Pfizer Salary support for clinical trials Celgene, Merck, Merrimack Matthew Gubens, MD, MS Assistant
Disclosures Preoperative Treatment: Chemotherapy or ChemoRT? Advisory boards Genentech (travel only), Pfizer Salary support for clinical trials Celgene, Merck, Merrimack Matthew Gubens, MD, MS Assistant
Management of early rectal cancer: Any role for adjuvant chemotherapy
 Management of early rectal cancer: Any role for adjuvant chemotherapy Andrés Cervantes Professor of Medicine CURRENTS CONCEPTS IN RECTAL CANCER DIAGNOSIS AND THERAPY TME surgery Optimal staging by MRI
Management of early rectal cancer: Any role for adjuvant chemotherapy Andrés Cervantes Professor of Medicine CURRENTS CONCEPTS IN RECTAL CANCER DIAGNOSIS AND THERAPY TME surgery Optimal staging by MRI
Colorectal Liver Metastases
 J Gastrointest Surg (2013) 17:195 202 DOI 10.1007/s11605-012-2022-3 EVIDENCE-BASED CURRENT SURGICAL PRACTICE Colorectal Liver Metastases Ching-Wei D. Tzeng & Thomas A. Aloia Received: 22 July 2012 /Accepted:
J Gastrointest Surg (2013) 17:195 202 DOI 10.1007/s11605-012-2022-3 EVIDENCE-BASED CURRENT SURGICAL PRACTICE Colorectal Liver Metastases Ching-Wei D. Tzeng & Thomas A. Aloia Received: 22 July 2012 /Accepted:
The Role of Adjuvant Chemotherapy for Colorectal Liver Metastasectomy after Pre-Operative Chemotherapy: Is the Treatment Worthwhile?
 1179 Ivyspring International Publisher Research Paper Journal of Cancer 2017; 8(7): 1179-1186. doi: 10.7150/jca.18091 The Role of Adjuvant Chemotherapy for Colorectal Liver Metastasectomy after Pre-Operative
1179 Ivyspring International Publisher Research Paper Journal of Cancer 2017; 8(7): 1179-1186. doi: 10.7150/jca.18091 The Role of Adjuvant Chemotherapy for Colorectal Liver Metastasectomy after Pre-Operative
SUMMARY OF THE SIRFLOX RESULTS
 SUMMARY OF THE SIRFLOX RESULTS The SIRFLOX study results on the combination of SIR-Spheres Y-90 resin microspheres with first-line chemotherapy were published in Journal of Oncology in early 2016. 1 There
SUMMARY OF THE SIRFLOX RESULTS The SIRFLOX study results on the combination of SIR-Spheres Y-90 resin microspheres with first-line chemotherapy were published in Journal of Oncology in early 2016. 1 There
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
Clinical guideline Published: 1 November 2011 nice.org.uk/guidance/cg131
 Colorectal cancer: diagnosis and management Clinical guideline Published: 1 November 2011 nice.org.uk/guidance/cg131 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Colorectal cancer: diagnosis and management Clinical guideline Published: 1 November 2011 nice.org.uk/guidance/cg131 NICE 2017. All rights reserved. Subject to Notice of rights (https://www.nice.org.uk/terms-and-conditions#notice-ofrights).
Regional Therapy for Management of Peritoneal Carcinomatosis from Gastrointestinal Malignancies
 Regional Therapy for Management of Peritoneal Carcinomatosis from Gastrointestinal Malignancies Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service City of Hope Division of Surgical Oncology September
Regional Therapy for Management of Peritoneal Carcinomatosis from Gastrointestinal Malignancies Byrne Lee, MD FACS Chief, Mixed Tumor Surgery Service City of Hope Division of Surgical Oncology September
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Valencia May 2018 State of the art: Standards of care in preoperative treatment for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures:
ESMO Preceptorship Programme Colorectal Cancer Valencia May 2018 State of the art: Standards of care in preoperative treatment for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures:
Ghosts in the Machine: Jonathan B. Koea MD; FRACS. Department of Surgery Auckland Hospital Auckland New Zealand
 Ghosts in the Machine: Patient Journeys Through Cancer Treatment Jonathan B. Koea MD; FRACS. Department of Surgery Auckland Hospital Auckland New Zealand Age-Standardised Cancer Incidence (100,000 population)
Ghosts in the Machine: Patient Journeys Through Cancer Treatment Jonathan B. Koea MD; FRACS. Department of Surgery Auckland Hospital Auckland New Zealand Age-Standardised Cancer Incidence (100,000 population)
Tumor Marker Evolution: Comparison with Imaging for Assessment of Response to Chemotherapy in Patients with Colorectal Liver Metastases
 Ann Surg Oncol DOI 1.1245/s1434-9-887-5 ORIGINAL ARTICLE HEPATOBILIARY TUMORS Tumor Marker Evolution: Comparison with Imaging for Assessment of Response to Chemotherapy in with Colorectal Liver Metastases
Ann Surg Oncol DOI 1.1245/s1434-9-887-5 ORIGINAL ARTICLE HEPATOBILIARY TUMORS Tumor Marker Evolution: Comparison with Imaging for Assessment of Response to Chemotherapy in with Colorectal Liver Metastases
Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging
 Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Hepatobiliary and Pancreatic Surgery Chief of Hepatobiliary and Pancreatic Surgery
Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Hepatobiliary and Pancreatic Surgery Chief of Hepatobiliary and Pancreatic Surgery
INTRAARTERIAL TREATMENT OF COLORECTAL LIVER METASTASES. Dr. Joan Falcó Interventional Radiology UDIAT. Hospital Universitari Parc Taulí
 INTRAARTERIAL TREATMENT OF COLORECTAL LIVER METASTASES Dr. Joan Falcó Interventional Radiology UDIAT. Hospital Universitari Parc Taulí STRATEGIES FOR CRLM LIVER METASTASES Extended indications Resectable
INTRAARTERIAL TREATMENT OF COLORECTAL LIVER METASTASES Dr. Joan Falcó Interventional Radiology UDIAT. Hospital Universitari Parc Taulí STRATEGIES FOR CRLM LIVER METASTASES Extended indications Resectable
Carcinoma del colon-retto: La Chirurgia Robotica nella Malattia Avanzata
 Carcinoma del colon-retto: La Chirurgia Robotica nella Malattia Avanzata Alberto Patriti SSD Chirurgia Robotica Multidisciplinare ASL 2 Umbria Ospedale San Matteo degli Infermi Spoleto - Why MIS for Advanced
Carcinoma del colon-retto: La Chirurgia Robotica nella Malattia Avanzata Alberto Patriti SSD Chirurgia Robotica Multidisciplinare ASL 2 Umbria Ospedale San Matteo degli Infermi Spoleto - Why MIS for Advanced
Embolotherapy for Cholangiocarcinoma: 2016 Update
 Embolotherapy for Cholangiocarcinoma: 2016 Update Igor Lobko,MD Chief, Division Vascular and Interventional Radiology Long Island Jewish Medical Center GEST 2016 Igor Lobko, M.D. No relevant financial
Embolotherapy for Cholangiocarcinoma: 2016 Update Igor Lobko,MD Chief, Division Vascular and Interventional Radiology Long Island Jewish Medical Center GEST 2016 Igor Lobko, M.D. No relevant financial
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease
 Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
Planned relaparotomy following curative resection of a locally advanced gastrointestinal cancer
 Planned relaparotomy following curative resection of a locally advanced gastrointestinal cancer PD Dr. med. Michel Adamina, MSc Department of Surgery Agenda Prerequisite for successful CRS HIPEC Planned
Planned relaparotomy following curative resection of a locally advanced gastrointestinal cancer PD Dr. med. Michel Adamina, MSc Department of Surgery Agenda Prerequisite for successful CRS HIPEC Planned
Case Report Management of a Patient with Metastatic Colorectal Cancer and Liver Metastases
 Case Reports in Oncological Medicine, Article ID 790192, 4 pages http://dx.doi.org/10.1155/2014/790192 Case Report Management of a Patient with Metastatic Colorectal Cancer and Liver Metastases Muhammad
Case Reports in Oncological Medicine, Article ID 790192, 4 pages http://dx.doi.org/10.1155/2014/790192 Case Report Management of a Patient with Metastatic Colorectal Cancer and Liver Metastases Muhammad
Winship Cancer Institute of Emory University Neoadjuvant Systemic Therapy in Metastatic Renal Cell Carcinoma Patients
 Winship Cancer Institute of Emory University Neoadjuvant Systemic Therapy in Metastatic Renal Cell Carcinoma Patients Bradley Carthon, MD, PhD Assistant Professor, Genitourinary Medical Oncology Winship
Winship Cancer Institute of Emory University Neoadjuvant Systemic Therapy in Metastatic Renal Cell Carcinoma Patients Bradley Carthon, MD, PhD Assistant Professor, Genitourinary Medical Oncology Winship
TREATMENT OF PERITONEAL COLORECTAL CARCINOMATOSIS
 TREATMENT OF PERITONEAL COLORECTAL CARCINOMATOSIS Anna Lepistö, MD, PhD Department of Colorectal Surgery, Abdominal Center, Helsinki University Hospital Incidence, prevalence and risk factors for peritoneal
TREATMENT OF PERITONEAL COLORECTAL CARCINOMATOSIS Anna Lepistö, MD, PhD Department of Colorectal Surgery, Abdominal Center, Helsinki University Hospital Incidence, prevalence and risk factors for peritoneal
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
JY Douillard MD, PhD Professor of Medical Oncology
 ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Vienna 26-27 Program October 2015 Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer
ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Vienna 26-27 Program October 2015 Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer
Perioperative Chemotherapy With or Without Bevacizumab in Patients With Metastatic Colorectal Cancer Undergoing Liver Resection
 Original Study Perioperative With or Without Bevacizumab in Patients With Metastatic Colorectal Cancer Undergoing Liver Resection Anastasia Constantinidou, 1 David Cunningham, 1 Fatima Shurmahi, 1 Uzma
Original Study Perioperative With or Without Bevacizumab in Patients With Metastatic Colorectal Cancer Undergoing Liver Resection Anastasia Constantinidou, 1 David Cunningham, 1 Fatima Shurmahi, 1 Uzma