Paediatric Ophthalmology (in 120 minutes!)
|
|
|
- Clara Armstrong
- 6 years ago
- Views:
Transcription
1 Paediatric Ophthalmology (in 120 minutes!) FRACP Trainees 4 July 2016 James Elder Department of Ophthalmology, RCH
2 Outline of Lecture Examination Techniques Vision Ocular motility & Binocular Vision Neuro-ophthalmology Assessment of globe Specific Conditions FRACP

3 What is vision? Simple Acuity, colour, contrast, field, depth perception, motion Complex Extracting meaning FRACP
4 Examination Techniques


5 Assessment Objective Subjective FRACP
6 Normal Visual Expectations Birth Brief fixation on face object light FRACP
7 Normal Visual Expectations Six weeks Maintain fixation on face, object or light and follow through 90 degrees Smiling and visual responsive (especially to a face) FRACP
8 Normal Visual Expectations Six months Reach for small object Actively follow object FRACP
9 Normal Visual Expectations One year Reach for tiny objects (eg 100 s & 1000 s) FRACP
10 Normal Visual Expectations 2-3 years Picture matching (Kay picture test) 3-4 years Letter matching (Sheridan Gardiner test) 5 years Snellen acuity logmar tests FRACP
11 How to assess an infant s vision History Ask the parents Family history of eye problems Observation Watch child s visual behaviour Tests Elicit visual behaviour FRACP


12 Visual Acuity Tests FRACP
13 When to refer? Suspect poor or sub-normal vision Visual acuity of 6/12 or worse FRACP
14 Special tests of visual function Colour vision Visual field Stereoacuity Contrast sensitivity FRACP



15 Colour Vision FRACP

16 Visual Field Perimetry FRACP
17 Visual Field Confrontation FRACP

18 Stereoacuity FRACP

19 Ocular Motility Duction = movement of one eye Version = movement of both eyes Duction Version FRACP
20 Ocular Motility Ductions Versions Abduction Adduction Sursumduction (Elevation) Infraduction (Depression) (Cycloduction) Dextroversion Laevoversion Elevation Depression Convergence Divergence Cycloversion FRACP



21 Ocular Motility FRACP

22 Classification of squint - simplified FRACP
23 Binocular Vision Aim: stereoscopic depth perception Downsides: Diplopia Amblyopia FRACP
24 Binocular Vision Phoria vs Tropia Phoria = latent misaligment of eyes Tropia = manifest misaligment of eyes = more significant problem FRACP
25 Detection of Squint Observation Cover test Eye movements FRACP

26 Detection of Squint Observation Cover test Eye movements FRACP

27 Detection of Squint Observation Cover test Eye movements FRACP

28 Detection of Squint Observation Cover test Eye movements FRACP

29 Detection of Squint Observation Cover test Eye movements FRACP

30 Cover test FRACP

31 Detection of Squint Observation Cover test Eye movements FRACP
32 Additional examination Visual acuity Red reflex (children) General examination FRACP

33 Red reflex FRACP
34 Neuro-ophthalmology Pupil reactions Optic nerve function Examination of optic disc Visual field defects Nystagmus & odd eye mevements FRACP
35 Neuro-ophthalmology Pupil reactions Direct Consensual Near reflex Relative afferent defect Beware of neonatal & pharmacological miosis FRACP
36 Neuro-ophthalmology Anatomy of Pupil Response FRACP


37 Neuro-ophthalmology RAPD = relative afferent pupil defect Sensitive measure of retinal and/or optic nerve dysfunction Compares afferent input to pupillary response of the two eyes FRACP
38 Neuro-ophthalmology Optic nerve function RAPD Colour vision Red desaturation Visual acuity Visual field FRACP
39 Examination of Optic Nerve Direct ophthalmoscope Dilated pupil helps enormously (tropicamide 1% very safe) Dim room lighting Child fixes on distant target Approach o from visual axis Your right eye for child s right eye, etc FRACP

40 Normal Optic Disc FRACP


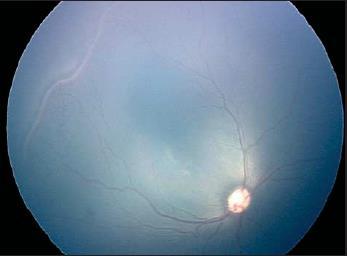
41 Papilloedema FRACP


42 Optic disc hypoplasia FRACP



43 Optic Disc Drusen FRACP

44 Optic Atrophy FRACP


45 Neuro-ophthalmology Visual field defects Horizontal cut off think optic nerve FRACP

46 Neuro-ophthalmology Visual field defects Vertical cut off think chiasmal & retro-chiasmal FRACP

47 Confrontation field FRACP
48 Neuro-ophthalmology Nystagmus & odd eye movements Will cover later FRACP




49 Globe Detection of Extra bits Clouldy bits Missing bits Most can be done with simple light source (direct ophthalmoscope) FRACP


50 Globe Red reflex Direct ophthalmoscope m from child FRACP
51 Strabismus

52 Childhood squint - comitant FRACP

53 Adult squint - incomitant FRACP
54 Consequences of squint - I Children Adults Amblyopia Diplopia Loss of binocular depth perception FRACP
55 Causes of squint - children Primary failure of binocular control Abnormality of convergence or divergence Refractive error Loss of vision in one eye Genetic tendency FRACP

56 Accommodative esotropia FRACP
 FRACP 2016")
57 Consequences of squint - II In both adults & children the head may be turned to maximise binocular function (abnormal or compensatory head posture) FRACP
58 Management of squint Confirm presence of squint Measure vision (including stereoacuity) Document diplopia Measure deviation Measure refractive error Examine for other disease (ocular & nonocular) Determine need for special investigations FRACP
59 Management of squint Prescribe glasses Treatment of amblyopia Surgery FRACP
60 Aims of treatment Treat any associated amblyopia Minimise/overcome any diplopia Maximise binocular depth perception Improve binocular visual field (convergent squints only) Improve cosmesis FRACP
61 When to refer Squint definitely present Squint cannot be excluded Large angle squint before 6 months of age Any squint after 6 months (even if intermittent) Urgent referral if red reflex is abnormal FRACP
62 Watery Eyes
 FRACP 2016")
63 Watery (& Sticky Eyes) FRACP


64 Watery eyes Epiphoria is the result of Excess tear production Deficient tear drainage FRACP

65 Corneal foreign body FRACP

66 Corneal abrasion FRACP

67 Subtarsal foreign body FRACP

68 An approach to watery eyes in children FRACP
69 Sticky Eyes & Infections
70 Sticky eyes Discharge consists of mucus & inflammatory cells +/- pathogens Does not always indicate infection FRACP
 FRACP")
71 Gonococcal conjunctivitis (Ophthalmia neonatorum) FRACP

72 Sac Abscess FRACP

73 Pre-septal cellulitis FRACP

74 Orbital cellulitis FRACP

75 Pre-septal vs orbital cellulitis FRACP
76 Pre-septal vs orbital cellulitis Pre-septal Sick Swollen lids Normal vision Normal pupil reaction Normal eye position Normal eye movements Orbital Very sick Lids red +/- swollen Vision may be down May have RAPD Proptosis Restricted eye movements +/- pain FRACP
77 Trauma
78 Trauma to child s eye Physical Blunt Sharp/penetrating Chemical Electromagnetic Thermal Radiotherapy Light FRACP

79 Hyphema - blunt trauma FRACP

80 Blow-out fracture - blunt trauma FRACP




81 Penetrating injuries FRACP

82 Chemical trauma! FRACP


83 Non-Accidental Injury FRACP
84 What causes haemorrhage? Loss of integrity of vascular system! Disruption of vessel Cut or tear vessel Burst /rupture vessel Failure of clotting mechanisms Abnormal vessel fragility FRACP
85 Potential causes of retinal haemorrhage in infants Direct trauma to globe Clotting abnormalities Transmitted pressure FRACP
86 Potential causes of retinal haemorrhage in infants Leukaemia Haemorrhagic disease of the newborn Sickle Cell retinopathy ECMO treatment Retinopathy of prematurity As part of disease (frequent) As result of handling with neck flexion & extension (uncertain) As the result of Retcam examination (rare) Galactosemia Henoch-Schonlein purpura Thrombocytopaenic purpura Maternal ingestion of Cocaine Meningitis Intracranial vascular malformation Optic disc drusen Retinal astrocytoma in tuberous sclerosis X-linked retinoschisis Intraocular surgery Severe hypertensiongalactosemia Homocystinuria Glutaric aciduria* Osteogenesis Imperfecta Osteoporosis- pseudoglioma syndrome Incontinentia Pigmenti Central retinal vein occlusion Infections Cytomegalovirus Herpes simplex type 6 Herpes simplex type 1 Malaria Meningococcal septicaemia* Streptococcus pyogenes meningitis* Strep. Pneumoniae meningitis* Congenital toxoplasmosis Fibromuscular dysplasia Terson s syndrome** Asphyxia FRACP
87 Potential causes of retinal haemorrhage in infants with abusive head trauma Direct concussive force applied to the eye resulting in vessels disruption (this mechanism may be a subset of the vitreo-retinal traction mechanism below) Increased venous pressure transmitted from intracranial cavity or central venous drainage in the chest Increased intracranial pressure resulting in localized venous obstruction, either within the distal optic nerve or at the level of the optic disc Direct spread of intracranial bleeding along the optic nerve (subdural or subarachnoid spaces) into the eye Vitreo-retinal traction leading to rupture of retinal vessels and splitting or elevation of the retina and rarely retinal dialysis or detachment. FRACP

88 FRACP
. J AAPOS 13(4): 364-369 FRACP 2016 89")
89 Finite element analysis Rangarajan, N., et al. (2009). J AAPOS 13(4): FRACP
90 Globe deformation with vitreous traction FRACP
91 Globe deformation with vitreous traction FRACP
92 Anisocoria (Unequal Pupils)
93 Unequal Pupils Simple anisocoria Pharmacological Third nerve palsy Horner s syndrome FRACP
94 Approach to Anisocoria FRACP
95 Horner Syndrome Clinical Features Anisocoria (miosis) Ptosis (upper & lower eyelids) Anhidrosis Conjunctival hyperaemia (transient) Dilation lag 5 sec 15 sec) Iris heterochromia Harlequin sign (reduced facial flushing) FRACP

96 Anatomy of the oculosympathetic Mughal and Longmuir Curr Neurol Neurosci Rep 2009; 9:384-9 pathway 1 st order neurons Hypothalmus to lower cervical/upper thoracic cord 2 nd order neurons Cord to superior cervical ganglion 3 rd order neurons SCG to eye FRACP
97 Clinical Assessment Confounders Essential (physiological) anisocoria Unrelated ptosis Local ocular causes of miotic pupil FRACP
98 Diagnostic confirmation Cocaine (Apraclonidine) FRACP

99 Mechanism of Action of Diagnostic Agents NE = norepinephrine a = apraclonidine α1 = alpha 1 receptor α2 = alpha 2 receptor Martin TJ Current Neurology and Neuroscience Reports 2007, 7: FRACP
100 Comparison of Agents Agent Action Observation Use Cocaine 4-10% Blocks noradrenaline reuptake Miotic pupil does not dilate Confirms Diagnosis Gold Standard Apraclonidine 0.5-1% (α2>> α1 agonist) α1 agonist de-innervation hypersensitivity Miotic pupil dilates more than normal (reversal of anisocoria) Confirms Diagnosis FRACP
101 Comparison of Agents Agent Cocaine 4-10% Apraclonidine 0.5-1% Hydroxyamphetamine 1% Difficulties Availability Stability? Sedation and cardiovascular SE in young children Not commercially available False +ve with trans-synaptic degeneration FRACP


102 Cocaine test FRACP
103 Possible causes of Horner s syndrome (!) First-order neurons Pathology involving the hypothalamus, brainstem, and spinal cord Infarction Haemorrhage Neoplasm Syringohydromyelia Second-order neurons Bronchogenic carcinoma Sympathetic schwannoma Neuroblastic tumors Enlarged thyroid Neck and upper thoracic surgery or other trauma Primary spinal nerve root tumours Osteophytes Second-order neurons (continued!!) Jugular venous ectasia Subclavian artery aneurysm Other neck lesions causing compression of the cervical sympathetic chain Third-order neurons Internal carotid artery dissection Fibromuscular dysplasia Skull base lesions Cluster or migraine headaches Agenesis or arteritis of the internal carotid artery Aneurysm of the petrous portion of the internal carotid artery Cavernous sinus infl ammation, infection, or neoplasm Rarely, orbital pathology: trauma or neoplasm after surgery FRACP
104 When to investigate? Acquired - all require thorough investigation if no pre-existing diagnosis or history of iatrogenic injury Clinical examination Urinary catecholamine assay Imaging head & neck & chest (MRI > CT)? MIBG scan (meta-iodobenzlguanidine) FRACP
105 When to investigate? Congenital Often clinical uncertainty about time of onset Question: How likely is an isolated Horner s syndrome in an infant to be due to something sinister? FRACP
106 Pediatric Horner s with no known diagnosis at presentation (CHOP, Philadelphia ) Number Comment Patients 28 Further 28 with known diagnosis Age years 2 Range Idiopathic 21 1/56 birth trauma Reactive lymph node 1? Age? Acquired or not Neuroblastoma 4 3 acquired Age 5 & 6 mths & 3 years 1 congenital Age 6 months JXG 1 15 months - acquired Ewings sarcoma 1 3 years - acquired FRACP 2016 AJO 2006; 142: Mahoney NR et al
107 Horner s syndrome < 1 year (Single practice CS Hoyt) Number 23 Idiopathic 16 Birth trauma 4 Known neuroblastoma 1 Ganglioneuroma 1 Acquired Horner s Neuroblastoma 1 History unclear Follow-up (years) Mean 9.3 & median 9 No new diagnoses made BJO 1998; 82:51-4 George et al FRACP
108 Demonstrable Horner s syndrome within the first 4 weeks of life confirmed by photographs or examination (HSC, Toronto & Wilmer, Baltimore 10 year period) +ve obstetric history -ve obstetric history Number No other diagnosis Developmental delay 1 - Congenital varicella - 2 Neuroblastoma - 1 (prior stridor & neck mass) Lymph node (? Reactive) - 2 Follow-up (median/mean) 29 & 35 months 58 & 64 months J AAPOS 1998; 2: FRACP 2016 Jeffery AR et al 108
109 Neuroblastoma & the Eye Ophthalmic features 80/405 60/80 orbital secondary 14/80 Horner s syndrome 9/14 presented with Horner s (2.2% overall) 11/405 presented with opsoclonus Musarella MA et al Ophthalmology 1984; 91: FRACP
110 Investigation of Horner s syndrome presenting < 1 year Acquired INVESTIGATE THOROUGHLY Not obviously acquired +ve obstetric trauma -? Need to investigate -ve obstetric trauma Offer investigation: CXR & Uninary catecholamines Clinical review More extensive investigation (MRI, CT or MIBG) questionable FRACP
111 Leukocoria
112 White Pupil (= leukocoria) Anything within the eye that is pale will result in a white or absent reflex and not a red reflex Cataract Retinoblastoma Chorioretinal coloboma FRACP
 Investigate if other abnormalities FRACP")
113 Cataract If suspect cataract refer Many causes Most due to isolated lens protein gene mutations (AD > XL > AR) Investigate if other abnormalities FRACP



114 Retinoblastoma FRACP
115 Retinoblastoma Present with leukocoria, squint, reduced vision or family history Sporadic (one-off or new mutation) Inherited (autosomal dominant) Unilateral or bilateral Fatal if untreated, 98% survival with treatment Early diagnosis increases chance of preserving vision FRACP

116 Retinoblastoma Two Hit Hypothesis FRACP
117 Surgery Enucleation Irradiation EBR, brachytherapy, proton beam Chemotherapy Retinoblastoma Potential Treatments Systemic, local (subconjunctival / intra-arterial / intravitreal) Cryotherapy Transcleral (may require fornix incision) Laser Thermotherapy / photocoagulation FRACP
118 Principles of Rb Treatment If small a local treatment If larger areduce tumour mass & then local treatment (SALT) If massive a often remove eye (consider reduction especially if bilateral) May be different for bilateral disease FRACP


119 Chorioretinal Coloboma FRACP
120 Congenital Glaucoma

121 Big eyes FRACP
122 Primary congenital glaucoma Raised pressure in eye Stretches the young eye (<2 years) May damage the optic nerve and cornea FRACP
123 Primary congenital glaucoma Watery eye (epiphoria) Light sensitive (photophobia) Corneal haze or cloudiness (corneal oedema) Corneal enlargement (buphthalmos = ox eye ) FRACP
124 Primary congenital glaucoma Treatment Medical Sometimes Be aware of systemic side effects β blockers α agonists Surgical Often FRACP
125 Eyelids



126 Droopy Eyelids FRACP



127 Lumpy lids FRACP
128 Wobbly Eyes
129 Wobbly Eyes (most is nystagmus) Motor Congenital nystagmus Variably reduced vision Null point with compensatory head position Sensory Anything that reduces vision significantly in the first 4 months Albinism Untreated bilateral cataract Retinal abnormality FRACP

130 Nystagmus - Examples FRACP

131 Nystagmus - Examples FRACP

132 Not Nystagmus - Examples FRACP

133 Not Nystagmus - Examples FRACP

134 Not Nystagmus - Examples FRACP
135 Infant with poor vision Nystagmus Yes Anterior segment pathology No Consider 4 options Yes No CVI or DVD COMA High ammetropia CNS pathology Cataract Aniridia Albinism Cornea Posterior segment pathology Yes No Aniridia ON hypoplasia Coloboma ROP Abnormal Retinal Function Rarely CNS Pathology FRACP ? ERG? MRI
136 Systemic Disease & Children s Eyes (This could involve a series of lectures for several months)
137 Systemic Disease & Children s Eyes Down syndrome (any of the previously described eye problems) Prematurity (retinopathy of prematurity) Juvenile chronic arthritis (uveitis) FRACP
138 Retinopathy of Prematurity = ROP Disorder of retinal angiogenesis Seen in some premature infants <500 g.. 30% g.. 10% g.. 3% g.. <1% >1250 g.. never FRACP
139 International Classification of ROP (ICROP) 1983 (revised 2005) Enable uniform description & collaboration Key elements Location Extent Stage Severity FRACP
140 ROP Location & Extent FRACP





141 ROP Stage FRACP



142 ROP -Severity Plus Disease Pre-Plus Disease FRACP

143 ROP disaster = RLF FRACP
144 Aetiology of ROP Unclear Low birth weight Gestational age Supplementary oxygen FRACP
145 Management of ROP Screening to identify those at risk of progressing to retinal detachment Laser treatment for type 1 ROP to prevent progression Long term follow-up to check for sequelae FRACP
146 RCT CRYO ROP 1988 Threshold = severe stage three for 5 continuous of 8 non-continuous clock hours in zone 1 or 2 with plus disease Conclusion Treating ROP of value (!) Cryotherapy % unfavourable No treatment - 43% unfavourable FRACP
147 ETROP 2003 Type 1 ROP Zone I, any stage ROP with plus disease Zone I, stage 3 ROP with or without plus disease Zone II, stage 2 or 3 ROP with plus disease Type 2 ROP Zone I, stage 1 or 2 ROP without plus disease Zone II, stage 3 ROP without plus disease FRACP
 ROP")

148 ROP Treatment Type 1 (Stage III) ROP before & after laser treatment FRACP
149 RCTs & ROP CRYO-ROP (1988) - treatment works Light-ROP (1997) - not caused by light STOP-ROP (2003) - extra O 2 does not turn off ROP ET-ROP (2003) - earlier treatment better STOP-ROP (2010) - O 2 sats of little help BEAT-ROP (2011) - anti-vegf turns off bad ROP BOOST (2013) - aiming for lower target O 2 sats increases mortality & only reduces ROP slightly FRACP
150 ROP sequelae Refractive errors Strabismus Amblyopia Visual loss if retinal scarring or detachment FRACP
151 Juvenile Chronic Arthritis Some children with JCA develop anterior uveitis (iritis) Risk of cataract and glaucoma as complications Beware the PANAFY (= Pauciarticular, ANA positive, Female, Young) FRACP

152 Juvenile Chronic Arthritis FRACP

153 Juvenile Chronic Arthritis FRACP
154 Learning Difficulties & Vision Little convincing evidence of connection between vision defects & learning problems Parents often try unproven treatments (burden of guilt) Educational approach (with appropriate psychological testing) of greatest benefit FRACP
155 Support Services for Children with Reduced Vision Pre-school Early childhood educators from Vision Australia School age Visiting teacher service (EVAC Clinic) Vision Australia School Vision Australia Low Vision Clinic Low vision aides Guide Dogs Association Mobility & occupational therapy FRACP
Ocular warning signs in GP practice: Paediatric Eye Pointers
 Ocular warning signs in GP practice: Paediatric Eye Pointers Dr Benjamin Chang MB, BCh, BAO, MMedSci, FRCS(Irel), FRCS(Edin), FRCOphth(Lond) Senior Consultant Ophthalmology and Visual Sciences Khoo Teck
Ocular warning signs in GP practice: Paediatric Eye Pointers Dr Benjamin Chang MB, BCh, BAO, MMedSci, FRCS(Irel), FRCS(Edin), FRCOphth(Lond) Senior Consultant Ophthalmology and Visual Sciences Khoo Teck
KPA PFIZER EDUCATION GRANT
 KPA PFIZER EDUCATION GRANT What every Paediatrician needs to know in Paediatric Ophthalmology Dr. Njambi Ombaba Paediatricians knowledge in ophthalmology Outline Visual development in a child Amblyopia
KPA PFIZER EDUCATION GRANT What every Paediatrician needs to know in Paediatric Ophthalmology Dr. Njambi Ombaba Paediatricians knowledge in ophthalmology Outline Visual development in a child Amblyopia
Dr Casey Ung. Ophthalmologist Dunedin Hospital Eye Clinic Marinoto Clinic & Specialists Dunedin
 Dr Casey Ung Ophthalmologist Dunedin Hospital Eye Clinic Marinoto Clinic & Specialists Dunedin 8:30-9:25 WS #140: Paediatric Ophthalmology 9:35-10:30 WS #150: Paediatric Ophthalmology (Repeated) Paediatric
Dr Casey Ung Ophthalmologist Dunedin Hospital Eye Clinic Marinoto Clinic & Specialists Dunedin 8:30-9:25 WS #140: Paediatric Ophthalmology 9:35-10:30 WS #150: Paediatric Ophthalmology (Repeated) Paediatric
Paediatric acute ophthalmology. Harry Bradshaw
 Paediatric acute ophthalmology Harry Bradshaw Approach Red eye Leukocoria Neurological Trauma Visual loss Red eye Orbital Eyelid Conjunctiva Cornea Uvea Orbital Orbit fixed volume Contiguous with sinuses,
Paediatric acute ophthalmology Harry Bradshaw Approach Red eye Leukocoria Neurological Trauma Visual loss Red eye Orbital Eyelid Conjunctiva Cornea Uvea Orbital Orbit fixed volume Contiguous with sinuses,
2. The clinician will know how to manage common pediatric ocular diseases
 Ida Chung, OD, MSHE, FCOVD, FAAO Western University College of Optometry Associate Professor/Assistant Dean of Learning 309 E. Second Street, Pomona, CA 91766 Office: 909 938 4140 Email: ichung@westernu.edu
Ida Chung, OD, MSHE, FCOVD, FAAO Western University College of Optometry Associate Professor/Assistant Dean of Learning 309 E. Second Street, Pomona, CA 91766 Office: 909 938 4140 Email: ichung@westernu.edu
Visual Conditions in Infants and Toddlers
 Visual Conditions and Functional Vision: Early Intervention Issues Visual Conditions in Infants and Toddlers Brief Overview of Childhood Visual Disorders Hatton, D.D. (2003). Brief overview of childhood
Visual Conditions and Functional Vision: Early Intervention Issues Visual Conditions in Infants and Toddlers Brief Overview of Childhood Visual Disorders Hatton, D.D. (2003). Brief overview of childhood
Clinical Pearls: Infant vision examination Deborah Orel-Bixler, PhD, OD University of California, Berkeley School of Optometry
 Clinical Pearls: Infant vision examination Deborah Orel-Bixler, PhD, OD University of California, Berkeley School of Optometry Recommended ages for examinations Recommended populations Recommendations
Clinical Pearls: Infant vision examination Deborah Orel-Bixler, PhD, OD University of California, Berkeley School of Optometry Recommended ages for examinations Recommended populations Recommendations
MD (Ophthalmology) May 2007 Examination Paper I MD (Ophthalmology) May 2007 Examination Paper II
 May 2007 Examination Paper I MD (Ophthalmology) May 2007 Examination Paper II") All India Institute of Medical Science MD Ophthalmology Time: 3 hours Max. Marks: 100 Attempt all the questions briefly with labeled diagrams wherever possible Q1. Discuss the mechanisms of accommodation
All India Institute of Medical Science MD Ophthalmology Time: 3 hours Max. Marks: 100 Attempt all the questions briefly with labeled diagrams wherever possible Q1. Discuss the mechanisms of accommodation
Examining Children s Eyes
 Paediatric Ophthalmology What to refer & when? Aims Tips for assessing a child s eyes in general practice Common paediatric ophthalmology symptoms and signs What needs to be referred and when? MISS FARIHA
Paediatric Ophthalmology What to refer & when? Aims Tips for assessing a child s eyes in general practice Common paediatric ophthalmology symptoms and signs What needs to be referred and when? MISS FARIHA
Children's Eye Assessment
 Children's Eye Assessment Dr Antony Bedggood, Children s Specialist Centre Paediatric Ophthalmologist, Cataract & Strabismus Surgeon Why kids need early referral Children s eye problems are often subtle:
Children's Eye Assessment Dr Antony Bedggood, Children s Specialist Centre Paediatric Ophthalmologist, Cataract & Strabismus Surgeon Why kids need early referral Children s eye problems are often subtle:
A Case of Carotid-Cavernous Fistula
 A Case of Carotid-Cavernous Fistula By : Mohamed Elkhawaga 2 nd Year Resident of Ophthalmology Alexandria University A 19 year old male patient came to our outpatient clinic, complaining of : -Severe conjunctival
A Case of Carotid-Cavernous Fistula By : Mohamed Elkhawaga 2 nd Year Resident of Ophthalmology Alexandria University A 19 year old male patient came to our outpatient clinic, complaining of : -Severe conjunctival
OPHTHALMOLOGY REFERRAL GUIDE FOR GPS
 OPHTHALMOLOGY REFERRAL GUIDE FOR GPS A guidebook to support general practitioners in the management and referral of a range of common eye problems. Contents 3 Introduction 4 Ophthalmic Workup 6 Acute Visual
OPHTHALMOLOGY REFERRAL GUIDE FOR GPS A guidebook to support general practitioners in the management and referral of a range of common eye problems. Contents 3 Introduction 4 Ophthalmic Workup 6 Acute Visual
3/16/2018. Optic Nerve Examination. Hassan Eisa Swify FRCS Ed (Ophthalmology) Air Force Hospital
 Air Force Hospital") Optic Nerve Examination Hassan Eisa Swify FRCS Ed (Ophthalmology) Air Force Hospital 1 Examination Structure ( optic disc) Function Examination of the optic disc The only cranial nerve (brain tract) which
Optic Nerve Examination Hassan Eisa Swify FRCS Ed (Ophthalmology) Air Force Hospital 1 Examination Structure ( optic disc) Function Examination of the optic disc The only cranial nerve (brain tract) which
MRI masterfile Part 5 WM Heme Strokes.ppt 1
 Ocular and Orbital Trauma Eye Trauma: Incidence 1.3 million eye injuries in the US per year. 40,000 of these injuries lead to blindness in the US. Patrick Sibony, MD March 23, 2013 Ophthalmic Emergencies
Ocular and Orbital Trauma Eye Trauma: Incidence 1.3 million eye injuries in the US per year. 40,000 of these injuries lead to blindness in the US. Patrick Sibony, MD March 23, 2013 Ophthalmic Emergencies
Shedding Light on Pediatric Cataracts. Kimberly G. Yen, MD Associate Professor of Ophthalmology Texas Children s Hospital
 Shedding Light on Pediatric Cataracts Kimberly G. Yen, MD Associate Professor of Ophthalmology Texas Children s Hospital A newborn infant presents with bilateral white cataracts. What is the best age to
Shedding Light on Pediatric Cataracts Kimberly G. Yen, MD Associate Professor of Ophthalmology Texas Children s Hospital A newborn infant presents with bilateral white cataracts. What is the best age to
EYE TRAUMA: INCIDENCE
 Introduction EYE TRAUMA: INCIDENCE 2.5 million eye injuries per year in U.S. 40,000 60,000 of eye injuries lead to visual loss Introduction Final visual outcome of many ocular emergencies depends on prompt,
Introduction EYE TRAUMA: INCIDENCE 2.5 million eye injuries per year in U.S. 40,000 60,000 of eye injuries lead to visual loss Introduction Final visual outcome of many ocular emergencies depends on prompt,
Acute Eyes for ED. Enis Kocak. The Alfred Ophthalmology
 Acute Eyes for ED Enis Kocak The Alfred Ophthalmology The problem with eyes Things to cover Ocular anatomy Basic assessment Common presentations Eye first aid and procedures Ophthalmic emergencies What
Acute Eyes for ED Enis Kocak The Alfred Ophthalmology The problem with eyes Things to cover Ocular anatomy Basic assessment Common presentations Eye first aid and procedures Ophthalmic emergencies What
UC SF. g h. Eye Trauma. Martha Neighbor, MD Emergency Services San Francisco General Hospital University of California
 UC SF Eye Trauma sf g h Martha Neighbor, MD Emergency Services San Francisco General Hospital University of California Goals Recognize vision threatening eye emergencies Treat them when we can Know when
UC SF Eye Trauma sf g h Martha Neighbor, MD Emergency Services San Francisco General Hospital University of California Goals Recognize vision threatening eye emergencies Treat them when we can Know when
Mom, There s Something Wrong With My Eye
 Mom, There s Something Wrong With My Eye Veeral Shah MD, PHD Texas Children's Hospital Most Common Issues Seen by the Pediatrician Emergent Ocular Issues Seen by the Pediatrician 1 What does this baby
Mom, There s Something Wrong With My Eye Veeral Shah MD, PHD Texas Children's Hospital Most Common Issues Seen by the Pediatrician Emergent Ocular Issues Seen by the Pediatrician 1 What does this baby
C19. Pediatric Neuro-ophthalmology: Dilemmas in clinical practice. 12 June, :15 15:45. Room 115 HAND-OUTS
 C19 Pediatric Neuro-ophthalmology: Dilemmas in clinical practice 12 June, 2017 14:15 15:45 Room 115 HAND-OUTS Is this strabismus really harmful? Karl Golnik, MD, MEd University of Cincinnati, USA Childhood
C19 Pediatric Neuro-ophthalmology: Dilemmas in clinical practice 12 June, 2017 14:15 15:45 Room 115 HAND-OUTS Is this strabismus really harmful? Karl Golnik, MD, MEd University of Cincinnati, USA Childhood
LECTURE # 7 EYECARE REVIEW: PART III
 LECTURE # 7 EYECARE REVIEW: PART III HOW TO TRIAGE EYE EMERGENCIES STEVE BUTZON, O.D. EYECARE REVIEW: HOW TO TRIAGE EYE EMERGENCIES FOR PRIMARY CARE PHYSICIANS Steve Butzon, O.D. Member Director IDOC President
LECTURE # 7 EYECARE REVIEW: PART III HOW TO TRIAGE EYE EMERGENCIES STEVE BUTZON, O.D. EYECARE REVIEW: HOW TO TRIAGE EYE EMERGENCIES FOR PRIMARY CARE PHYSICIANS Steve Butzon, O.D. Member Director IDOC President
Examination Report. September 2012 Diploma Examination. Contents:
 Examination Report September 2012 Diploma Examination Contents: MCQ paper Content page 2 Statistics page 2 Distribution of scores page 3 Standard setting page 3 Summary page 4 CRQ paper Content page 4
Examination Report September 2012 Diploma Examination Contents: MCQ paper Content page 2 Statistics page 2 Distribution of scores page 3 Standard setting page 3 Summary page 4 CRQ paper Content page 4
Normal Pupil. The normal pupil is 2 mm to 6 mm in diameter. In ordinary ambient light the pupils are usually 3 mm to 4 mm in diameter.
 Normal Pupil The normal pupil is 2 mm to 6 mm in diameter. In ordinary ambient light the pupils are usually 3 mm to 4 mm in diameter. Normal Pupil The pupils are small and poorly reactive at birth and
Normal Pupil The normal pupil is 2 mm to 6 mm in diameter. In ordinary ambient light the pupils are usually 3 mm to 4 mm in diameter. Normal Pupil The pupils are small and poorly reactive at birth and
Paediatric Ophthalmology Assessment. Justin Mora 2017
 Paediatric Ophthalmology Assessment Justin Mora 2017 History Visual developmental milestones Aware of people in the room, reaching for objects, following toys, alignment should be central and stable
Paediatric Ophthalmology Assessment Justin Mora 2017 History Visual developmental milestones Aware of people in the room, reaching for objects, following toys, alignment should be central and stable
OPHTHALMOLOGIC PEARLS FOR THE NON- OPHTHALMOLOGIST. David G. Gross D.O. Deen-Gross Eye Centers Merrillville-Hobart Deengrosseye.
 OPHTHALMOLOGIC PEARLS FOR THE NON- OPHTHALMOLOGIST David G. Gross D.O. Deen-Gross Eye Centers Merrillville-Hobart Deengrosseye.com A FEW OF THE AREAS WE WILL DISCUSS Red Eye Glaucoma Neuro ophthalmic tid
OPHTHALMOLOGIC PEARLS FOR THE NON- OPHTHALMOLOGIST David G. Gross D.O. Deen-Gross Eye Centers Merrillville-Hobart Deengrosseye.com A FEW OF THE AREAS WE WILL DISCUSS Red Eye Glaucoma Neuro ophthalmic tid
THE 35 GOLDEN EYE RULES
 THE 35 GOLDEN EYE RULES The Sense of Sight, from La Dame a la Licorne, The Lady and the Unicorn Tapestries, Late 15th Century Flemish Tapestry in wool and silk, Musée Nationale du Moyen Age, Paris. 1.
THE 35 GOLDEN EYE RULES The Sense of Sight, from La Dame a la Licorne, The Lady and the Unicorn Tapestries, Late 15th Century Flemish Tapestry in wool and silk, Musée Nationale du Moyen Age, Paris. 1.
Dr. Litwak is on the speaker bureau and advisory panel for Alcon and Zeiss Meditek
 My Favorite Cases Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker bureau and advisory panel for Alcon and Zeiss Meditek Case LA 62 yobf +HTN, + DM POH told
My Favorite Cases Anthony B. Litwak,OD, FAAO VA Medical Center Baltimore, Maryland Dr. Litwak is on the speaker bureau and advisory panel for Alcon and Zeiss Meditek Case LA 62 yobf +HTN, + DM POH told
Aristotle University Thessaloniki Medical School I. & II. Departments of Ophthalmology 90 DIAGNOSTIC & THERAPEUTIC APPROACHES IN OPHTHALMOLOGY
 Aristotle University Thessaloniki Medical School I. & II. Departments of Ophthalmology 90 DIAGNOSTIC & THERAPEUTIC APPROACHES IN OPHTHALMOLOGY The medical student should be able to... I. Pathophysiology
Aristotle University Thessaloniki Medical School I. & II. Departments of Ophthalmology 90 DIAGNOSTIC & THERAPEUTIC APPROACHES IN OPHTHALMOLOGY The medical student should be able to... I. Pathophysiology
NANOS Patient Brochure
 NANOS Patient Brochure Anisocoria Copyright 2016. North American Neuro-Ophthalmology Society. All rights reserved. These brochures are produced and made available as is without warranty and for informational
NANOS Patient Brochure Anisocoria Copyright 2016. North American Neuro-Ophthalmology Society. All rights reserved. These brochures are produced and made available as is without warranty and for informational
Eye diseases in infancy and early childhood
 Eye diseases in infancy and early childhood Contents: a. Visual development and assessment of vision in infancy and childhood. b. The infant with whitish pupil. c. The infant with watery eye. d. Prematurity
Eye diseases in infancy and early childhood Contents: a. Visual development and assessment of vision in infancy and childhood. b. The infant with whitish pupil. c. The infant with watery eye. d. Prematurity
Ophthalmology Unit Referral Guidelines
 Ophthalmology Unit Referral Guidelines Austin Health Ophthalmology Unit holds sub-specialty sessions to discuss and plan the treatment of patients with specific ocular conditions. General including cataract
Ophthalmology Unit Referral Guidelines Austin Health Ophthalmology Unit holds sub-specialty sessions to discuss and plan the treatment of patients with specific ocular conditions. General including cataract
OPHTHALMOLOGY DEPARTMENT Primary care referral guidelines
 OPHTHALMOLOGY DEPARTMENT Primary care referral guidelines Contents REFERRAL CATEGIES... 2 Emergency... 2 Urgent... 2 Semi urgent/routine... 2 Not accepted... 2 OPHTHALMOLOGY CONDITIONS NOT ACCEPTED...
OPHTHALMOLOGY DEPARTMENT Primary care referral guidelines Contents REFERRAL CATEGIES... 2 Emergency... 2 Urgent... 2 Semi urgent/routine... 2 Not accepted... 2 OPHTHALMOLOGY CONDITIONS NOT ACCEPTED...
Sepideh Tara Rousta, MD FAAO Robert Wood Johnson University Hospital Saint Peter s University Hospital Wills Eye Hospital
 Sepideh Tara Rousta, MD FAAO Robert Wood Johnson University Hospital Saint Peter s University Hospital Wills Eye Hospital 14 mo old w R eye cross (parents) 9 mo old R eye crossing getting worse for past
Sepideh Tara Rousta, MD FAAO Robert Wood Johnson University Hospital Saint Peter s University Hospital Wills Eye Hospital 14 mo old w R eye cross (parents) 9 mo old R eye crossing getting worse for past
Ocular Urgencies and Emergencies
 Ocular Urgencies and Emergencies Pam Boyce, O.D., F.A.A.O. Boyce Family Eye Care, Ltd. 528 Devon Ave. Park Ridge, IL 60068 847-518-0303 Somebody s going to lose an eye Epidemiology 2.4 million ocular and
Ocular Urgencies and Emergencies Pam Boyce, O.D., F.A.A.O. Boyce Family Eye Care, Ltd. 528 Devon Ave. Park Ridge, IL 60068 847-518-0303 Somebody s going to lose an eye Epidemiology 2.4 million ocular and
NEW YORK UNIVERSITY SCHOOL OF MEDICINE DEPARTMENT OF OPHTHALMOLOGY EDUCATIONAL OBJECTIVES AND GOALS
 NEW YORK UNIVERSITY SCHOOL OF MEDICINE DEPARTMENT OF OPHTHALMOLOGY EDUCATIONAL OBJECTIVES AND GOALS Revision Date: 6/30/06 Distribution Date: 7/6/06 The Department of Ophthalmology at the NYU Medical Center
NEW YORK UNIVERSITY SCHOOL OF MEDICINE DEPARTMENT OF OPHTHALMOLOGY EDUCATIONAL OBJECTIVES AND GOALS Revision Date: 6/30/06 Distribution Date: 7/6/06 The Department of Ophthalmology at the NYU Medical Center
Help! My Baby s Eyes Are Crossed (or Something!)
") Help! My Baby s Eyes Are Crossed (or Something!) Madhuri Chilakapati, MD Ophthalmology Chief Complaint My baby has a lazy eye The eyes move funny The eyes don t move together The eyes get stuck The eyes
Help! My Baby s Eyes Are Crossed (or Something!) Madhuri Chilakapati, MD Ophthalmology Chief Complaint My baby has a lazy eye The eyes move funny The eyes don t move together The eyes get stuck The eyes
JINNAH SINDH MEDICAL UNIVERSITY STUDY GUIDE- OPHTHALMOLOGY YEAR 4,
 INTRODUCTION Pakistan, the 7th most populous country in the world, has an urban population of 38.8% and rural dwellers of 61.2%. The country has faced challenges with vision impairment and blindness as
INTRODUCTION Pakistan, the 7th most populous country in the world, has an urban population of 38.8% and rural dwellers of 61.2%. The country has faced challenges with vision impairment and blindness as
Vision Care for Connecticut Children
 Vision Care for Connecticut Children EXECUTIVE SUMMARY November 2003 Prepared by: Judith Solomon, JD Mary Alice Lee, PhD Children s Health Council With funding from: Children s Fund of Connecticut, Inc.
Vision Care for Connecticut Children EXECUTIVE SUMMARY November 2003 Prepared by: Judith Solomon, JD Mary Alice Lee, PhD Children s Health Council With funding from: Children s Fund of Connecticut, Inc.
Carotid Cavernous Fistula
 Chief Complaint: Double vision. Carotid Cavernous Fistula Alex W. Cohen, MD, PhD; Richard Allen, MD, PhD May 14, 2010 History of Present Illness: A 46 year old female patient presented to the Oculoplastics
Chief Complaint: Double vision. Carotid Cavernous Fistula Alex W. Cohen, MD, PhD; Richard Allen, MD, PhD May 14, 2010 History of Present Illness: A 46 year old female patient presented to the Oculoplastics
Department of Ophthalmology
 Period : 03/July/17 to 07/September/17 Semester : 7 th Semester Department of Ophthalmology Lecture Lesson Plan Sr 1 03.07.17 Uvea-Anatomy, Uvea-Anatomy, Classification of Uveitis Dr R Paranjpe Classification
Period : 03/July/17 to 07/September/17 Semester : 7 th Semester Department of Ophthalmology Lecture Lesson Plan Sr 1 03.07.17 Uvea-Anatomy, Uvea-Anatomy, Classification of Uveitis Dr R Paranjpe Classification
Ophthalmic Trauma Update
 Ophthalmic Trauma Update Richard S. Davidson, M.D. Professor of Ophthalmology Vice Chair for Quality and Clinical Affairs UCHealth Eye Center University of Colorado School of Medicine August 5, 2017 Financial
Ophthalmic Trauma Update Richard S. Davidson, M.D. Professor of Ophthalmology Vice Chair for Quality and Clinical Affairs UCHealth Eye Center University of Colorado School of Medicine August 5, 2017 Financial
Dr. D. Y. Patil Medical College, Pimpri, Pune
 Dr. D. Y. Patil Medical College, Pimpri, Pune - 411 018 Period : 04/July/16 to 22/September/16 Semester : 7 th Semester Department : Ophthalmology Lecture Lesson Plan Sr No Date Topic Learning objectives
Dr. D. Y. Patil Medical College, Pimpri, Pune - 411 018 Period : 04/July/16 to 22/September/16 Semester : 7 th Semester Department : Ophthalmology Lecture Lesson Plan Sr No Date Topic Learning objectives
Eyes, ears, teeth and everything in between
 Eyes, ears, teeth and everything in between E M E R G E N C Y D E P A R T M E N T J U N I O R T E A C H created 14/11/10 by S.R. Bruijns, version 1.0 Objectives Eyes Ears Teeth Maxilla- facial EYES Approaching
Eyes, ears, teeth and everything in between E M E R G E N C Y D E P A R T M E N T J U N I O R T E A C H created 14/11/10 by S.R. Bruijns, version 1.0 Objectives Eyes Ears Teeth Maxilla- facial EYES Approaching
Neuro-ophthalmologyophthalmology. Marek Michalec, MD.
 Neuro-ophthalmologyophthalmology Marek Michalec, MD. Neuro-ophthalmology Study integrating ophthalmology and neurology Disorders affecting parts of CNS devoted to vision or eye: Afferent system (visual
Neuro-ophthalmologyophthalmology Marek Michalec, MD. Neuro-ophthalmology Study integrating ophthalmology and neurology Disorders affecting parts of CNS devoted to vision or eye: Afferent system (visual
Pediatric Ocular Sonography
 Pediatric Ocular Sonography Cicero J Torres A Silva, MD Associate Professor of Radiology 2016 SPR Pediatric Ultrasound Course Yale University School of Medicine None Disclosures Objectives of Presentation
Pediatric Ocular Sonography Cicero J Torres A Silva, MD Associate Professor of Radiology 2016 SPR Pediatric Ultrasound Course Yale University School of Medicine None Disclosures Objectives of Presentation
Paola Diaz, O.D. Ocular Disease Resident University of Houston College of Optometry
 Paola Diaz, O.D. Ocular Disease Resident University of Houston College of Optometry Cedar Springs Eye Clinic Abnormal Pupils Why? Test the neurological integrity Aid in the determination for vision loss
Paola Diaz, O.D. Ocular Disease Resident University of Houston College of Optometry Cedar Springs Eye Clinic Abnormal Pupils Why? Test the neurological integrity Aid in the determination for vision loss
DNB Question Paper. December 1
 DNB Question Paper December 1 December,2013 DNB Examination 2013 (December) IMPORTANT INSTRUCTIONS: This question paper consists of 10 questions divided into Part A and Part B, each part containing 5 questions.
DNB Question Paper December 1 December,2013 DNB Examination 2013 (December) IMPORTANT INSTRUCTIONS: This question paper consists of 10 questions divided into Part A and Part B, each part containing 5 questions.
Management of Diplopia Indiana Optometric Association Annual Convention April 2018 Kristine B. Hopkins, OD, MSPH, FAAO
 Management of Diplopia Indiana Optometric Association Annual Convention April 2018 Kristine B. Hopkins, OD, MSPH, FAAO For patients with diplopia, the clinician must differentiate monocular from binocular
Management of Diplopia Indiana Optometric Association Annual Convention April 2018 Kristine B. Hopkins, OD, MSPH, FAAO For patients with diplopia, the clinician must differentiate monocular from binocular
Hong Kong College of Surgical Nursing
 Hong Kong College of Surgical Nursing Surgical Nursing Training: Part B Specialty - Ophthalmological Nursing Curriculum 1 TABLE OF CONTENTS No. Contents Page 1. Introduction 3 2. Aims 3 3. Programme Intended
Hong Kong College of Surgical Nursing Surgical Nursing Training: Part B Specialty - Ophthalmological Nursing Curriculum 1 TABLE OF CONTENTS No. Contents Page 1. Introduction 3 2. Aims 3 3. Programme Intended
Jacqueline Theis, O.D., F.A.A.O.
 Neuro-Ophthalmological Emergencies Presenting in Primary Care Optometry Describes the symptoms, signs, and management of neuro-ophthalmological emergencies. Signs/Symptoms to be Concerned about (especially
Neuro-Ophthalmological Emergencies Presenting in Primary Care Optometry Describes the symptoms, signs, and management of neuro-ophthalmological emergencies. Signs/Symptoms to be Concerned about (especially
A RESOURCE MANUAL MANAGEMENT RETINOBLASTOMA LOW & MIDDLE RESOURCE SETTINGS
 A RESOURCE MANUAL FOR THE MANAGEMENT OF RETINOBLASTOMA IN LOW & MIDDLE RESOURCE SETTINGS UPDATED SEPTEMBER 2017 1 CONTENTS PAGE INTRODUCTION 3 SERVICE LEVEL for Rb MANAGEMENT 4 SCREENING 5 EARLY DIAGNOSIS
A RESOURCE MANUAL FOR THE MANAGEMENT OF RETINOBLASTOMA IN LOW & MIDDLE RESOURCE SETTINGS UPDATED SEPTEMBER 2017 1 CONTENTS PAGE INTRODUCTION 3 SERVICE LEVEL for Rb MANAGEMENT 4 SCREENING 5 EARLY DIAGNOSIS
Department of Ophthalmology
 Department of Ophthalmology Period : 02/July/18 to 30/August/18 Semester : 7 th Semester Lecture Lesson Plan Sr. Date Topic Lesson plan Name of Faculty No. 1 02.07.18 Lens- Lens-Anatomy, Classification
Department of Ophthalmology Period : 02/July/18 to 30/August/18 Semester : 7 th Semester Lecture Lesson Plan Sr. Date Topic Lesson plan Name of Faculty No. 1 02.07.18 Lens- Lens-Anatomy, Classification
Mild NPDR. Moderate NPDR. Severe NPDR
 Diabetic retinopathy Diabetic retinopathy is the most common cause of blindness in adults aged 35-65 years-old. Hyperglycaemia is thought to cause increased retinal blood flow and abnormal metabolism in
Diabetic retinopathy Diabetic retinopathy is the most common cause of blindness in adults aged 35-65 years-old. Hyperglycaemia is thought to cause increased retinal blood flow and abnormal metabolism in
EYE INJURIES OBJECTIVES COMMON EYE EMERGENCIES 7/19/2017 IMPROVE ASSESSMENT OF EYE INJURIES
 EYE INJURIES BRITTA ANDERSON D.O. DMC PRIMARY CARE SPORTS MEDICINE ASSOCIATE TEAM PHYSICIAN DETROIT TIGERS OBJECTIVES IMPROVE ASSESSMENT OF EYE INJURIES UNDERSTAND WHAT IS CONSIDERED AN EMERGENCY DEVELOP
EYE INJURIES BRITTA ANDERSON D.O. DMC PRIMARY CARE SPORTS MEDICINE ASSOCIATE TEAM PHYSICIAN DETROIT TIGERS OBJECTIVES IMPROVE ASSESSMENT OF EYE INJURIES UNDERSTAND WHAT IS CONSIDERED AN EMERGENCY DEVELOP
GNK485 The eye and related structures. Prof MC Bosman 2012
 GNK485 The eye and related structures Prof MC Bosman 2012 Surface anatomy Bony orbit Eyeball and Lacrimal apparatus Extra-ocular muscles Movements of the eye Innervation Arterial supply and venous drainage
GNK485 The eye and related structures Prof MC Bosman 2012 Surface anatomy Bony orbit Eyeball and Lacrimal apparatus Extra-ocular muscles Movements of the eye Innervation Arterial supply and venous drainage
Paediatric Ophthalmology
 Paediatric Ophthalmology Erika Maka MD SEMMELWEIS UNIVERSITY, FACULTY OF MEDICINE DEPARTMENT OF OPHTHALMOLOGY, BUDAPEST DIRECTOR: PROF. DR. ZOLTÁN ZSOLT NAGY Why? When? How?.?.?.?. without problem - Screening
Paediatric Ophthalmology Erika Maka MD SEMMELWEIS UNIVERSITY, FACULTY OF MEDICINE DEPARTMENT OF OPHTHALMOLOGY, BUDAPEST DIRECTOR: PROF. DR. ZOLTÁN ZSOLT NAGY Why? When? How?.?.?.?. without problem - Screening
Tiffany L. Kruger, D.O. Children s Hospital of Michigan Wayne State University/Kresge Eye Institute
 Pediatric Cases Nt Not To Be Missed Tiffany L. Kruger, D.O. Pediatric Ophthalmology Fellow Children s Hospital of Michigan Wayne State University/Kresge Eye Institute Case Presentation CC: Left eye turns
Pediatric Cases Nt Not To Be Missed Tiffany L. Kruger, D.O. Pediatric Ophthalmology Fellow Children s Hospital of Michigan Wayne State University/Kresge Eye Institute Case Presentation CC: Left eye turns
REFERRAL GUIDELINES: OPHTHALMOLOGY
 Outpatient Referral Guidelines Page 1 1 REFERRAL GUIDELINES: OPHTHALMOLOGY Date of birth Demographic Contact details (including mobile phone) Clinical Reason for referral Duration of symptoms Essential
Outpatient Referral Guidelines Page 1 1 REFERRAL GUIDELINES: OPHTHALMOLOGY Date of birth Demographic Contact details (including mobile phone) Clinical Reason for referral Duration of symptoms Essential
Year 2 MBChB Clinical Skills Session Ophthalmoscopy. Reviewed & ratified by: Mr M Batterbury Consultant Ophthalmologist
 Year 2 MBChB Clinical Skills Session Ophthalmoscopy Reviewed & ratified by: o Mr M Batterbury Consultant Ophthalmologist Learning objectives o To understand the anatomy and physiology of the external and
Year 2 MBChB Clinical Skills Session Ophthalmoscopy Reviewed & ratified by: o Mr M Batterbury Consultant Ophthalmologist Learning objectives o To understand the anatomy and physiology of the external and
OCCLUSIVE VASCULAR DISORDERS OF THE RETINA
 OCCLUSIVE VASCULAR DISORDERS OF THE RETINA Learning outcomes By the end of this lecture the students would be able to Classify occlusive vascular disorders (OVD) of the retina. Correlate the clinical features
OCCLUSIVE VASCULAR DISORDERS OF THE RETINA Learning outcomes By the end of this lecture the students would be able to Classify occlusive vascular disorders (OVD) of the retina. Correlate the clinical features
Patient Symptoms- What They Might Mean. Sarah Dougherty Wood, OD, MS, FAAO Heart of America, February 2011 Paraoptometric Lecture
 Patient Symptoms- What They Might Mean Sarah Dougherty Wood, OD, MS, FAAO Heart of America, February 2011 Paraoptometric Lecture Basic ocular anatomy and physiology Movie projector analogy Blur at near/eye
Patient Symptoms- What They Might Mean Sarah Dougherty Wood, OD, MS, FAAO Heart of America, February 2011 Paraoptometric Lecture Basic ocular anatomy and physiology Movie projector analogy Blur at near/eye
Faculty Financial Disclosure. Learning Objectives: Office Ophthalmology. Basic Eye Exam: What s in your pocket/office? Office Ophthalmology
 Faculty Financial Disclosure Office Ophthalmology Lynn K. Gordon, MD, PhD, has no financial relationships to disclose. Lynn K. Gordon, MD, PhD Professor and Vernon O Underwood Family Chair Department of
Faculty Financial Disclosure Office Ophthalmology Lynn K. Gordon, MD, PhD, has no financial relationships to disclose. Lynn K. Gordon, MD, PhD Professor and Vernon O Underwood Family Chair Department of
Southampton Eye Unit. Orthoptic Induction Pack
 Southampton Eye Unit Orthoptic Induction Pack 1 Orthoptics Orthoptics is an Allied Health Profession. It is a graduate profession with a 3 year degree course offered at Liverpool and Sheffield Universities,
Southampton Eye Unit Orthoptic Induction Pack 1 Orthoptics Orthoptics is an Allied Health Profession. It is a graduate profession with a 3 year degree course offered at Liverpool and Sheffield Universities,
ICD -10 -CM Pediatric/Strabismus
 ICD -10 -CM Pediatric/Strabismus Amblyopia Deprivation H53.011 H53.012 H53.013 H53.019 Refractive H53.021 H53.022 H53.023 H53.029 Strabismic H53.031 H53.032 H53.033 H53.039 Suspect H53.041 H53.042 H43.043
ICD -10 -CM Pediatric/Strabismus Amblyopia Deprivation H53.011 H53.012 H53.013 H53.019 Refractive H53.021 H53.022 H53.023 H53.029 Strabismic H53.031 H53.032 H53.033 H53.039 Suspect H53.041 H53.042 H43.043
FRANZCO, MD, MBBS. Royal Darwin Hospital
 Diabetes and Eye By Dr. Nishantha Wijesinghe FRANZCO, MD, MBBS Consultant Ophthalmologist Royal Darwin Hospital 98% of Diabetics do not need to suffer from severe visual loss Yet Diabetic eye disease is
Diabetes and Eye By Dr. Nishantha Wijesinghe FRANZCO, MD, MBBS Consultant Ophthalmologist Royal Darwin Hospital 98% of Diabetics do not need to suffer from severe visual loss Yet Diabetic eye disease is
IMAGE OF THE MOMENT PRACTICAL NEUROLOGY
 178 PRACTICAL NEUROLOGY IMAGE OF THE MOMENT Gawn G. McIlwaine*, James H. Vallance* and Christian J. Lueck *Princess Alexandra Eye Pavilion, Chalmers Street, Edinburgh UK; The Canberra Hospital, P.O. Box
178 PRACTICAL NEUROLOGY IMAGE OF THE MOMENT Gawn G. McIlwaine*, James H. Vallance* and Christian J. Lueck *Princess Alexandra Eye Pavilion, Chalmers Street, Edinburgh UK; The Canberra Hospital, P.O. Box
Abstracts. R Bhola. Visual Fields. K Golnik. C List different methods of assessing peripheral. C Describe relevant anatomy leading to different
 Abstracts Wednesday, July 8, 2015 Infection ontrol in Ophthalmology This course reviews infection control processes for the ophthalmic nurse and technician. Standard precautions, universal precautions,
Abstracts Wednesday, July 8, 2015 Infection ontrol in Ophthalmology This course reviews infection control processes for the ophthalmic nurse and technician. Standard precautions, universal precautions,
TITLE. A 10-year retrospective review of retinopathy of prematurity screening and treatment in Western Romania
 TITLE A 10-year retrospective review of retinopathy of prematurity screening and treatment in Western Romania A 6 year review on preseptal and orbital cellulitis in patients under 18 years old and the
TITLE A 10-year retrospective review of retinopathy of prematurity screening and treatment in Western Romania A 6 year review on preseptal and orbital cellulitis in patients under 18 years old and the
Rapid Visual Loss. Dr Michael Johnson PhD FCOptom DipOrth DipGlauc DipTp(IP) Independent Prescribing Optometrist
 Independent Prescribing Optometrist") Rapid Visual Loss Dr Michael Johnson PhD FCOptom DipOrth DipGlauc DipTp(IP) Independent Prescribing Optometrist Outline Pathophysiology Differential diagnosis. Patient scenarios in community practice:
Rapid Visual Loss Dr Michael Johnson PhD FCOptom DipOrth DipGlauc DipTp(IP) Independent Prescribing Optometrist Outline Pathophysiology Differential diagnosis. Patient scenarios in community practice:
Approach to Strabismus:
 Approach to Strabismus: By John Hilhorst 1. Definitions Strabismus is an anomaly of ocular alignment that can occur in any direction. It is characterized by a misalignment of one or both eyes that may
Approach to Strabismus: By John Hilhorst 1. Definitions Strabismus is an anomaly of ocular alignment that can occur in any direction. It is characterized by a misalignment of one or both eyes that may
They have a lazy eye. Be Specific!! 4/24/2018. Esotropia vs. Pseudoesotropia
 They have a lazy eye Be Specific!! Esotropia vs. Pseudoesotropia Eyes crossing (esotropia) Eyes drifting (exotropia) Head turn Droopy eyelid Vision concerns 1 www.aapos.org/terms/conditions/49 Vertical
They have a lazy eye Be Specific!! Esotropia vs. Pseudoesotropia Eyes crossing (esotropia) Eyes drifting (exotropia) Head turn Droopy eyelid Vision concerns 1 www.aapos.org/terms/conditions/49 Vertical
INFANTILE EXOTROPIA. Lionel Kowal
 INFANTILE EXOTROPIA Lionel Kowal INFANTILE XT Usage often imprecise Variation in definitions number of investigators? onset day 1 of life? constant / intermittent Any / large angle? Associated systemic
INFANTILE EXOTROPIA Lionel Kowal INFANTILE XT Usage often imprecise Variation in definitions number of investigators? onset day 1 of life? constant / intermittent Any / large angle? Associated systemic
Ocular and periocular trauma
 Ocular and periocular trauma No financial disclosures. Tina Rutar M.D. Assistant Professor of Clinical Ophthalmology and Pediatrics Director, Visual Center for the Child University of California San Francisco
Ocular and periocular trauma No financial disclosures. Tina Rutar M.D. Assistant Professor of Clinical Ophthalmology and Pediatrics Director, Visual Center for the Child University of California San Francisco
HKU Department of Ophthalmology Seminar and Workshop 2017 Emergencies in Eye Care for Frontline Healthcare Professionals
 HKU Department of Ophthalmology Seminar and Workshop 2017 Emergencies in Eye Care for Frontline Healthcare Professionals Course Directors and Faculty Professor Jimmy Shiu-Ming Lai MBBS M.Med MD DO FRCOphth
HKU Department of Ophthalmology Seminar and Workshop 2017 Emergencies in Eye Care for Frontline Healthcare Professionals Course Directors and Faculty Professor Jimmy Shiu-Ming Lai MBBS M.Med MD DO FRCOphth
PRECISION PROGRAM. Injection Technique Quick-Reference Guide. Companion booklet for the Video Guide to Injection Technique
 Injection Technique Quick-Reference Guide PRECISION PROGRAM Companion booklet for the Video Guide to Injection Technique Available at www.ozurdexprecisionprogram.com Provides step-by-step directions with
Injection Technique Quick-Reference Guide PRECISION PROGRAM Companion booklet for the Video Guide to Injection Technique Available at www.ozurdexprecisionprogram.com Provides step-by-step directions with
Recurrent intraocular hemorrhage secondary to cataract wound neovascularization (Swan Syndrome)
") Recurrent intraocular hemorrhage secondary to cataract wound neovascularization (Swan Syndrome) John J. Chen MD, PhD; Young H. Kwon MD, PhD August 6, 2012 Chief complaint: Recurrent vitreous hemorrhage,
Recurrent intraocular hemorrhage secondary to cataract wound neovascularization (Swan Syndrome) John J. Chen MD, PhD; Young H. Kwon MD, PhD August 6, 2012 Chief complaint: Recurrent vitreous hemorrhage,
Work Sheet And Course Hand Out
 Work Sheet And Course Hand Out This course provides the primary care health professional with a basic understanding of the eye, its function and the assessment of common sight- and non-sight threatening
Work Sheet And Course Hand Out This course provides the primary care health professional with a basic understanding of the eye, its function and the assessment of common sight- and non-sight threatening
Cairo University Faculty of Medicine. Course Specifications Course title: Ophthalmology (Code): OPH-409. Department of Ophthalmology
: OPH-409. Department of Ophthalmology") Cairo University Faculty of Medicine Department of Ophthalmology Course Specifications Course title: Ophthalmology (Code): OPH-409 Department of Ophthalmology Fourth academic year of M.B.B.Ch. program
Cairo University Faculty of Medicine Department of Ophthalmology Course Specifications Course title: Ophthalmology (Code): OPH-409 Department of Ophthalmology Fourth academic year of M.B.B.Ch. program
TOP 5 EYE CONDITIONS NOT TO BE MISSED
 TOP 5 EYE CONDITIONS NOT TO BE MISSED Dr Kolin Foo Consultant Ophthalmologist Senior Lecturer in Ophthalmology Wellington Hospital Terrace Eye Centre Financial disclosure No financial interest in the products
TOP 5 EYE CONDITIONS NOT TO BE MISSED Dr Kolin Foo Consultant Ophthalmologist Senior Lecturer in Ophthalmology Wellington Hospital Terrace Eye Centre Financial disclosure No financial interest in the products
Test Bank for Medical Surgical Nursing An Integrated Approach 3rd Edition by White
 Test Bank for Medical Surgical Nursing An Integrated Approach 3rd Edition by White Link full download : http://testbankair.com/download/test-bank-for-medical-surgical-nursing-anintegrated-approach-3rd-edition-by-white/
Test Bank for Medical Surgical Nursing An Integrated Approach 3rd Edition by White Link full download : http://testbankair.com/download/test-bank-for-medical-surgical-nursing-anintegrated-approach-3rd-edition-by-white/
OCT : retinal layers. Extraocular muscles. History. Central vs Peripheral vision. History: Temporal course. Optical Coherence Tomography (OCT)
") Optical Coherence Tomography (OCT) OCT : retinal layers 7 Central vs Peripheral vision Extraocular muscles RPE E Peripheral Vision: Rods (95 million) 30% Ganglion cells Central Vision: Cones (5 million)
Optical Coherence Tomography (OCT) OCT : retinal layers 7 Central vs Peripheral vision Extraocular muscles RPE E Peripheral Vision: Rods (95 million) 30% Ganglion cells Central Vision: Cones (5 million)
MRI masterfile Part 5 WM Heme Strokes.ppt 2
 Imaging of Orbital Trauma Corneal Abrasion CT scan is preferable to MRI Bone, Rapid, Easy to monitor patient Foreign bodies, air, hemorrhage Fractures Cost Needed for an MRI MRI Globe and intraocular injuries
Imaging of Orbital Trauma Corneal Abrasion CT scan is preferable to MRI Bone, Rapid, Easy to monitor patient Foreign bodies, air, hemorrhage Fractures Cost Needed for an MRI MRI Globe and intraocular injuries
By Darlene Jones, Nurse. May 2017
 By Darlene Jones, Nurse May 2017 Disclosure of potential conflict of interest Darlene Jones, Nurse I have no conflict of interest Course objectives Become familiar with the different pathologies in ophthalmology
By Darlene Jones, Nurse May 2017 Disclosure of potential conflict of interest Darlene Jones, Nurse I have no conflict of interest Course objectives Become familiar with the different pathologies in ophthalmology
VISUAL REFLEXES. B. The oculomotor nucleus, Edinger-Westphal nucleus, and oculomotor nerve at level of the superior colliculus.
 Neuroanatomy Suzanne Stensaas February 24, 2011, 10:00-12:00 p.m. Reading: Waxman Ch. 15 HyperBrain: Ch 7 with quizzes and or Lab 7 videotape http://www-medlib.med.utah.edu/kw/hyperbrain/anim/reflex.html
Neuroanatomy Suzanne Stensaas February 24, 2011, 10:00-12:00 p.m. Reading: Waxman Ch. 15 HyperBrain: Ch 7 with quizzes and or Lab 7 videotape http://www-medlib.med.utah.edu/kw/hyperbrain/anim/reflex.html
SCIENTIFIC PROGRAM. Pediatric ophthalmology- Optometry challenges (max 20 attendees)
") FRIDAY, 22 SEPTEMBER 2017 WORKSHOPS (OPHTHALMICA Eye Institute) 08:30-09:00 Registration-Welcome 09:00-11:30 Workshops SCIENTIFIC PROGRAM I. Cornea & Refractive surgery (max 30 attendees) - Clinical examination
FRIDAY, 22 SEPTEMBER 2017 WORKSHOPS (OPHTHALMICA Eye Institute) 08:30-09:00 Registration-Welcome 09:00-11:30 Workshops SCIENTIFIC PROGRAM I. Cornea & Refractive surgery (max 30 attendees) - Clinical examination
Index. C Canalicular system, 4 Carbonic anhydrase inhibitors, 29 30
 A Acanthamoeba keratitis (AK), 82, 83 Acute angle-closure crisis, 156 Acute angle-closure glaucoma (AACG), 121, 141, 284 causes of, 122 clinical presentation, 153 evaluation, 156 157 management/treatment,
A Acanthamoeba keratitis (AK), 82, 83 Acute angle-closure crisis, 156 Acute angle-closure glaucoma (AACG), 121, 141, 284 causes of, 122 clinical presentation, 153 evaluation, 156 157 management/treatment,
Scrub In. What is the function of vitreous humor? What does the pupil do when exposed to bright light? a. Maintain eye shape and provide color vision
 Scrub In What is the function of vitreous humor? a. Maintain eye shape and provide color vision b. Maintain eye shape and refract light rays c. Provide night vision and color vision d. Provide night vision
Scrub In What is the function of vitreous humor? a. Maintain eye shape and provide color vision b. Maintain eye shape and refract light rays c. Provide night vision and color vision d. Provide night vision
Lecture Content. Disorders of optic nerve and retina Chiasmal and retrochiasmal disorders Pupil disorders Motility disorders
 Neuro-Ophthalmology Celia H. Chang MD Department of Neurology MIND Institute University of California, Davis, Health System celia.chang@ucdmc.ucdavis.edu Lecture Content Disorders of optic nerve and retina
Neuro-Ophthalmology Celia H. Chang MD Department of Neurology MIND Institute University of California, Davis, Health System celia.chang@ucdmc.ucdavis.edu Lecture Content Disorders of optic nerve and retina
02/03/2014. Average Length: 23mm (Infant ~16mm) Approximately the size of a quarter Volume: ~5mL
 Approximately the size of a quarter Volume: ~5mL") Identify the anatomy of the eye. Explain the basic physiology of the parts of the eye. Briefly discuss various surgeries related to different parts of the anatomy. Average Length: 23mm (Infant ~16mm) Approximately
Identify the anatomy of the eye. Explain the basic physiology of the parts of the eye. Briefly discuss various surgeries related to different parts of the anatomy. Average Length: 23mm (Infant ~16mm) Approximately
Ophthalmoplegia in carotid cavernous sinus fistula
 British Journal of Ophthalmology, 1984, 68, 128-134 Ophthalmoplegia in carotid cavernous sinus fistula T. J. K. LEONARD, I. F. MOSELEY, AND M. D. SANDERS From the Departments ofneuro-ophthalmology and
British Journal of Ophthalmology, 1984, 68, 128-134 Ophthalmoplegia in carotid cavernous sinus fistula T. J. K. LEONARD, I. F. MOSELEY, AND M. D. SANDERS From the Departments ofneuro-ophthalmology and
Ocular Lecture. Sue Bednar NP Ali Atwater PA-C
 Ocular Lecture Sue Bednar NP Ali Atwater PA-C Triaging Ocular Complaints Painful Eye/Red eye +/-blurry vision +/-visual loss +/-floaters +/-fevers If any of the above findings exist, pt is likely to have
Ocular Lecture Sue Bednar NP Ali Atwater PA-C Triaging Ocular Complaints Painful Eye/Red eye +/-blurry vision +/-visual loss +/-floaters +/-fevers If any of the above findings exist, pt is likely to have
DNB QUESTIONS 2014 PAPER 1. b) What are the Clinical Conditions in Which Nystagmus is Seen? c) Management of Nystagmus.
 What are the Clinical Conditions in Which Nystagmus is Seen? c) Management of Nystagmus.") DNB QUESTIONS 2014 PAPER 1 1. a) How Will you investigate a case of Nystagmus? b) What are the Clinical Conditions in Which Nystagmus is Seen? c) Management of Nystagmus. 2. a) What is the Principle of
DNB QUESTIONS 2014 PAPER 1 1. a) How Will you investigate a case of Nystagmus? b) What are the Clinical Conditions in Which Nystagmus is Seen? c) Management of Nystagmus. 2. a) What is the Principle of
Identify the choice that best completes the statement or answers the question.
 Chapter 5. The Eye Multiple Choice Identify the choice that best completes the statement or answers the question. 1. The most common type of eye disorder is: A. Refractive errors B. Macular conditions
Chapter 5. The Eye Multiple Choice Identify the choice that best completes the statement or answers the question. 1. The most common type of eye disorder is: A. Refractive errors B. Macular conditions
PedsCases Podcast Scripts
 PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Approach to Childhood Glaucoma. These podcasts are designed to give medical students an overview of key topics in pediatrics.
PedsCases Podcast Scripts This is a text version of a podcast from Pedscases.com on Approach to Childhood Glaucoma. These podcasts are designed to give medical students an overview of key topics in pediatrics.
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Acetazolamide, in idiopathic intracranial hypertension, 49 52, 60 Angiography, computed tomography, in cranial nerve palsy, 103 107 digital
Index Note: Page numbers of article titles are in boldface type. A Acetazolamide, in idiopathic intracranial hypertension, 49 52, 60 Angiography, computed tomography, in cranial nerve palsy, 103 107 digital
Grand Rounds. Jenny Temnogorod SUNY Downstate Medical Center Department of Ophthalmology September 19, 2013
 Grand Rounds Jenny Temnogorod SUNY Downstate Medical Center Department of Ophthalmology September 19, 2013 History and Examination HPI: 2 day old SGA (small for gestational age, 37 weeks, BWt. 1760g) with
Grand Rounds Jenny Temnogorod SUNY Downstate Medical Center Department of Ophthalmology September 19, 2013 History and Examination HPI: 2 day old SGA (small for gestational age, 37 weeks, BWt. 1760g) with
Strabismus. A.Medghalchi,M.D Assistant professor of ophthalmology Gilan medical science university
 Strabismus A.Medghalchi,M.D Assistant professor of ophthalmology Gilan medical science university ۳ Anatomy Of The EOM s Six Extraocular muscles surround eye: Medial Rectus Lateral Rectus Superior Rectus
Strabismus A.Medghalchi,M.D Assistant professor of ophthalmology Gilan medical science university ۳ Anatomy Of The EOM s Six Extraocular muscles surround eye: Medial Rectus Lateral Rectus Superior Rectus
REVIEW OF HEAD AND NECK CRANIAL NERVES AND EVERYTHING ELSE
 REVIEW OF HEAD AND NECK CRANIAL NERVES AND EVERYTHING ELSE OLFACTORY NERVE CN I ANTERIOR CRANIAL FOSSA CRISTA GALLI OF ETHMOID OLFACTORY FORAMINA IN CRIBIFORM PLATE OF ETHMOID BONE CN I OLFACTORY NERVE
REVIEW OF HEAD AND NECK CRANIAL NERVES AND EVERYTHING ELSE OLFACTORY NERVE CN I ANTERIOR CRANIAL FOSSA CRISTA GALLI OF ETHMOID OLFACTORY FORAMINA IN CRIBIFORM PLATE OF ETHMOID BONE CN I OLFACTORY NERVE