Editorial Manager(tm) for Neurosurgery Manuscript Draft. Manuscript Number:
|
|
|
- Daisy Hawkins
- 5 years ago
- Views:
Transcription
1 Editorial Manager(tm) for Neurosurgery Manuscript Draft Manuscript Number: Title: Evaluation of variation in the course of the facial nerve, nerve adhesion to tumors, and postoperative facial palsy in acoustic neuroma: A retrospective study of 356 cases Short Title: Course of the facial nerve Article Type: Research - Human - Clinical Studies Section/Category: Tumor Keywords: Acoustic neuromas, Facial nerve, Retrosigmoid approach Corresponding Author: Tetsuro Sameshima, M.D., Ph.D. Corresponding Author's Institution: NTT Medical Center Tokyo First Author: Tetsuro Sameshima, M.D., Ph.D. Order of Authors: Tetsuro Sameshima, M.D., Ph.D.;Akio Morita, M.D., Ph.D.;Rokuya Tanikawa, M.D.;Takanori Fukushima, M.D., D.M.Sc.;Allan H. Friedman, M.D.;Francesco Zenga, M.D.;Alessandro Ducati, M.D.;Luciano Mastronardi, M.D., Ph.D. Manuscript Region of Origin: JAPAN Abstract: Background: Preserving the facial nerve (FN) in patients undergoing acoustic neuroma (AN) surgery requires confirmation of its anatomical location and course. Objective: To investigate the variation in the course of the FN, its adhesion to tumors, and the relationship between such adhesions and postoperative facial palsy. Methods: Subjects were 356 patients who underwent AN surgery for whom the course of the FN could be confirmed. Patients were classified into six groups according to the FN course: (1) ventro-central surface of the tumor (VCe); (2) ventro-rostral (VR); (3) ventro-caudal (VCa); (4) rostral (R); (5) caudal (C); and (6) dorsal (D). The relationship between the course and tumor size, nerve adhesion to tumors, and postoperative FN function was investigated. Results: The FN course was VCe in 185 cases, VR in 137, VCa in 19, R in 10, C in 4, and D in one. proportion of VR increased, and in tumors >3 cm, an increased proportion of patients had severely distorted courses. No significant difference was observed between course patterns of the FN in terms adhere strongly to the tumor capsule, and postoperative facial palsy was more severe in patients with stronger adhesions. Conclusions: The VCe pattern was most common for small tumors. Adhesion to the tumor capsule was most strongly associated with postoperative FN palsy. Suggested Reviewers: Helmut Bertalanffy M.D., Ph.D. Director, Neurosurgery, International Neuroscience Institute Hannover bertalanffy@ini-hannover.de
2 Ketan R. Bulsara M.D. Professor, Neurosurgery, Yale University School of Medicine Opposed Reviewers:
3 Cover Letter May 13, 2011 Nelson M. Oyesiku, MD, PhD, FACS Editor-in-Chief Neurosurgery Dear Dr. Oyesiku: Enclosed please find a copy of our manuscript entitled, Evaluation of variations in the course of the facial nerve, nerve adhesion to tumors, and postoperative facial palsy in acoustic neuroma: A retrospective study of 356 cases which we would like to submit for publication in Neurosurgery. In this study, we present the results of an investigation of the relationship between course of the facial nerve and adhesion of this nerve to tumors, and that between such adhesions and postoperative facial palsy in patients undergoing acoustic neuroma surgery. We believe that our study would be of interest to the readers of your journal because when performing acoustic neuroma surgery, attempts should be made to preserve hearing acuity and to accurately identify the course of the facial nerve in order to preserve its function. The work presented herein is original, has not been previously published in whole or in part, and is not under consideration for publication at any other journal. Each author has contributed significantly to the research presented herein, has reviewed the final version of the manuscript and approved this submission. We would like to thank you in advance for considering this manuscript. Please feel free to contact me if you have any questions or require further information.
4 Sincerely, Tetsuro Sameshima, M.D., Ph.D. Department of Neurosurgery NTT Medical Center Tokyo , Higashi-Gotanda, Shinagawa-ku, Tokyo, , Japan Phone: 81(3) , FAX: 81(3) , Cell: 81(90)
5 *Title Page Evaluation of variation in the course of the facial nerve, nerve adhesion to tumors, and postoperative facial palsy in acoustic neuroma: A retrospective study of 356 cases Tetsuro Sameshima, M.D., Ph.D. 1, Akio Morita, M.D., Ph.D. 1, Rokuya Tanikawa, M.D. 2, Takanori Fukushima, M.D., D.M.Sc. 3,4, Allan H. Friedman, M.D. 4, Francesco Zenga, M.D. 5, Alessandro Ducati, M.D. 6, and Luciano Mastronardi, M.D., Ph.D. 7 1 Department of Neurosurgery, NTT Medical Center Tokyo, Tokyo, Japan, 2 Department of Neurosurgery, Abashiri Neurosurgical Hospital, Abashiri, Japan, 3 Carolina Neuroscience Institute, Raleigh, NC, USA 4 Department of Neurosurgery, Duke University Medical Center, Durham, NC, USA, 5 Department of Neurosurgery, University of Torino, Torino, Italy. 6 Department of Neurosurgery, San Filippo Neri Hospitsal, Roma, Italy Corresponding author contact information Tetsuro Sameshima, M.D., Ph.D. Department of Neurosurgery NTT Medical Center Tokyo , Higashi-Gotanda, Shinagawa-ku, Tokyo, , Japan Phone: 81(3) , FAX: 81(3) , Cell: 81(90) tetsurosameshima@gmail.com
6 *Manuscript Abstract Background: Preserving the facial nerve (FN) in patients undergoing acoustic neuroma (AN) surgery requires confirmation of its anatomical location and course. Objective: To investigate the variation in the course of the FN, its adhesion to tumors, and the relationship between such adhesions and postoperative facial palsy. Methods: Subjects were 356 patients who underwent AN surgery for whom the course of the FN could be confirmed. Patients were classified into six groups according to the FN course: (1) ventro-central surface of the tumor (VCe); (2) ventro-rostral (VR); (3) ventro-caudal (VCa); (4) rostral (R); (5) caudal (C); and (6) dorsal (D). The relationship between the course and tumor size, nerve adhesion to tumors, and postoperative FN function was investigated. Results: The FN course was VCe in 185 cases, VR in 137, VCa in 19, R in 10, C in 4, and D in one. Regarding tumor size, for tumors 1.5 cm the VCe pattern was most common. For tumors 1.5 cm, the proportion of VR increased, and in tumors >3 cm, an increased proportion of patients had severely distorted courses. No significant difference was observed between course patterns of the FN in terms of postoperative FN function, but for tumors 3 cm there was an increasing tendency for the FN to adhere strongly to the tumor capsule, and postoperative facial palsy was more severe in patients with stronger adhesions. Conclusions: The VCe pattern was most common for small tumors. Adhesion to the tumor capsule was most strongly associated with postoperative FN palsy.
7 Key Words: Acoustic neuromas, Facial nerve, Retrosigmoid approach Running title: Course of the facial nerve Introduction The goals of acoustic neuroma surgery are safe tumor resection, hearing preservation, and preservation of facial nerve function. In recent years, operative results reported by expert skull base teams working with innovative microsurgical instruments have improved markedly, with the incidence of facial nerve palsy being only a few percent. In general, during acoustic neuroma surgery, surgeons proceed with removal while confirming the position of the facial nerve, the course of which is known to vary according to factors such as tumor size, site of origin, and degree of adhesion. As accurate preoperative assessment of the anatomical location and course of the facial nerve is difficult even with current advances in imaging technology, the only method currently available is confirmation under a microscope with repeated intraoperative facial nerve stimulation. In this study, we investigated the association between facial nerve course patterns in acoustic neuroma, adhesion to tumors, and postoperative facial palsy. Material and Methods
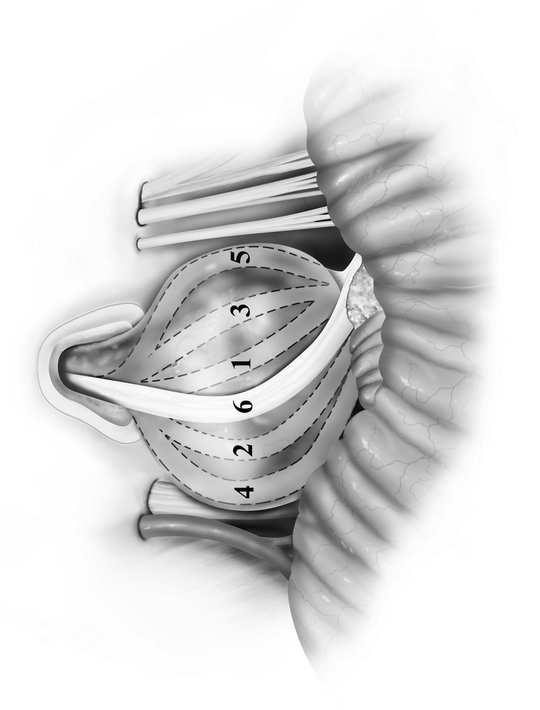
8 Subjects were 356 patients undergoing surgery for acoustic neuroma via the retrosigmoid approach between April 2002 and December 2010 (160 women and 196 men; mean age, 59.1 years; mean tumor size, 19.8 mm). In all cases, we attempted total or near-total removal of the tumor, and facial nerves were anatomically preserved. All procedures were performed by expert neurosurgical teams with intraoperative facial nerve monitoring and intraoperative auditory brain stem response monitoring for hearing preservation. The data obtained included patient age, tumor size (evaluated as the largest transverse diameter on enhanced magnetic resonance images), pre- and postoperative facial nerve function, and extent of adhesions between the facial nerve and the tumor. We classified the course of the facial nerve into 6 patterns according to its path on the surface of the tumor: ventro-central (VCe), ventro-rostral (VR), ventro-caudal (VCa), rostral (R), caudal (C), and dorsal (D) patterns (Figure 1). All 356 patients exhibited normal (grade 1) facial function preoperatively. In addition, the facial nerve was anatomically preserved after surgery in all cases. Facial nerve outcome was reported on the House-Brackmann scale, 1 and the results are recorded as early (approximately 2 weeks after surgery) and late (8 to 12 months after surgery). Adhesion between the tumor and the facial nerve was evaluated during the procedure by the operating surgeon. In patients with severe adhesion, it was difficult to separate the facial nerve from the tumor capsule with blunt dissection, and sharp dissection with scissors was required.
9 Results The course of the facial nerve The VCe pattern, i.e., that in which the facial nerve ran ventrally and centrally over the tumor surface, accounted for 185/356 cases (52.0%), the largest proportion of cases overall, followed by VR in 137 cases (38.5%), VCa in 19 (5.3%), R in 10 (2.8%), C in 4 (1.1%), and D in 1 (0.3%) (Table 1). Categorized by tumor size, for tumors 1.5 cm the pattern was VCe in 77/98 cases (78.6%) and VR in 21 (21.4%); for tumors of cm the pattern was VCe in 90/195 cases (46.2%), VR in 89 (45.6%), VCa in 11 (5.6%), R in 3 (1.5%), C in 1 (0.5%), and D in 1 (0.5%), while for tumors 3.0 cm the pattern was VCe in 18/63 cases (28.6%), VR in 27 (42.9%), VCa in 8 (12.7%), R in 7 (11.1%), and C in 3 (4.8%). That is, for tumors 1.5 cm the VCe pattern was most common, accounting for nearly 80% of cases. For tumors 1.5 cm the proportion of VR rose, and once tumor size exceeded 3 cm, there was an increase in the proportion of patients with severely distorted courses, such as the R pattern in which the nerve runs across the upper peak of the tumor or the VCa and C patterns in which it runs along the caudal side. In one patient (tumor size 2.4 cm), the course ran entirely along the dorsal side. Facial nerve outcome (late) according to the House-Brackmann scale Table 2 shows facial nerve function according to the House-Brackmann scale 1 for
10 each facial nerve course pattern at late follow-up examination (8-12 months). Grade 1 patients comprised 131 cases (70.8%) of VCe, 99 (72.3%) of VR, 15 (78.9%) of VCa, 8 (80.0%) of R, and 2 (50.0%) of C; Grade 2 patients comprised 40 cases (21.6%) of VCe, 31 (22.6%) of VR, 1 (5.3%) of VCa, 1 and (10.0%) of R; Grade 3 patients comprised 9 cases (4.9%) of VCe, 5 (3.6%) of VR, 2 (10.5%) of VCa, 1 (10.0%) of R, 2 (50.0%) of C, and 1 (100%) of D; and Grade 4 patients comprised 5 cases (2.7%) of VCe, 2 (1.5%) of VR, and 1 (5.3%) of VCa. If we exclude patterns C and D, which were seen in only small numbers of patients, there were no major differences in outcome for different facial nerve course patterns in terms of postoperative facial nerve function. Adhesion between the tumor and the facial nerve Table 3 shows the presence or absence of adhesion between the tumor capsule and the facial nerve in terms of course pattern and tumor size. Adhesion was present in 22 cases (28.6%) of VCe and 8 (38.1%) of VR for tumors 1.5 cm; 49 cases (54.4%) of VCe, 49 (55.1%) of VR, 3 (27.3%) of VCa, 2 (66.7%) of R, 1 (100%) of C, and 1 (100%) of D for tumors cm; and 14 cases (77.8%) of VCe, 22 (81.5%) of VR, 5 (62.5%) of VCa, 6 (85.7%) of R, and 2 (66.7%) of C for tumors 3.0 cm. There were no major differences between VCe, VR, and VCa in terms of extent of adhesion, but adhesion was frequent in cases of R, C, and D, courses that ran in an extremely distorted pattern. Adhesion was more frequent for larger tumors in all course patterns. The site of strongest adhesion was in the region of the entrance to the internal auditory canal in all course patterns.
11 Postoperative facial nerve function and tumor adhesion to the facial nerve A comparison of postoperative facial nerve function in relation to the presence or absence of tumor adhesion showed that adhesion had a significant effect on facial nerve preservation outcomes (Table 4). In some cases, the facial nerve was embedded within the tumor capsule, resulting in a higher rate of postoperative facial palsy. Changes in facial nerve morphology When the tumor was larger than 3.0 cm, the facial nerve tended to become thinned and flattened, and to adhere to the tumor capsule more strongly. Discussion The goals of acoustic neuroma surgery are safe, accurate, and complete tumor resection, hearing preservation, and facial nerve preservation. 2-8 In order to accomplish microsurgical total tumor resection with curative intent in patients without any complications, surgeons must have a detailed understanding of temporal bone and cerebellopontine angle anatomy and employ precise and sophisticated micro-technical skills, as well as abundant clinical experience In recent years, operative results reported by expert skull base teams working with innovative microsurgical instruments have improved markedly, with the incidence of facial nerve palsy being only a few percent. 12,13 Normally, hearing impairment
12 is the primary complaint in acoustic neuroma, with preoperative facial nerve palsy hardly ever present, meaning that preservation of this function requires the most care. In general, during acoustic neuroma surgery, resection proceeds while confirming the position of the facial nerve, the course of which is known to vary according to factors such as tumor size, site of origin, and degree of adhesion. Accurate preoperative assessment of the anatomical location and course of the facial nerve is difficult even with the current rapid development of imaging technologies such as MRI. Particularly with large tumors the facial nerve can be compressed and flattened into a thin structure that adheres strongly to the tumor capsule, and sometimes even becomes infiltrated or enfolded into the tumor. Because this makes it difficult to confirm the course accurately, even under a microscope, the only method currently available is cautious confirmation of its course with repeated intraoperative facial nerve stimulation while removing the tumor. We performed frequent intraoperative facial nerve stimulation, 14 identifying the root exit zone of the facial nerve at the earliest possible stage and placing the electrode for continuous stimulation monitoring at that point during tumor removal surgery. With respect to facial nerve course patterns, in our series, courses crossing the ventro-central surface accounted for around 80% of cases for small acoustic neuromas of 1.5 cm. In contrast, for tumors measuring between cm, the frequency of VCe was very similar to that of VR (46.2% vs. VR in 45.6%), and for tumors 3.0 cm the course had shifted to the ventro-rostral surface in many cases, with VCe accounting for 28.6% of cases and VR for 42.9%. In this series, a course across the dorsal portion of the tumor was seen in only one patient (0.3%).
13 Sampath et al. 15 analyzed microanatomical variations in the location of the facial nerves for 1006 cases of acoustic neuromas categorized by size but with measurements 1.0 cm larger than our classification (Group I: smaller than 2.5 cm; Group II: between 2.5 cm and 4.0 cm; and Group III: larger than 4.0 cm). In their patients, the facial nerve most commonly ran across the anterior middle third of the tumor (corresponding to VCe in our classification); this pattern was seen in 40.0% of cases in Group I, 40.2% in Group II, and 39.8% in Group III, followed by the anterior superior third (corresponding to VR) in 33.5% of cases in Group I, 33.2% in Group II, and 32.7% in Group III, and the posterior location (corresponding to D) in 1.6% of cases in Group I, 2.5% in Group II, and 2.6% in Group III. There were no differences in course frequency between different sizes of tumor. In a study of 163 cases of acoustic neuroma, Bae et al. 16 categorized facial nerve course patterns into four groups: (1) the ventral and superior surface of the tumor (corresponding to VR in our classification), (2) the ventral and central surface (corresponding to VCe), (3) the ventral and inferior surface (corresponding to VCa), and (4) the dorsal surface (corresponding to D). They found that the course ran across the ventral and superior surface in 55.8% of cases, the ventral and central surface in 35.0%, the ventral and inferior surface in 8.6%, and the dorsal surface in 0.6%. For tumors of 2 cm diameter, the ventral and central surface pattern was most common, occurring in 65.2% of cases, whereas for tumors of diameter 2 cm the ventral and superior surface was most common, occurring in 59.3%. As in our series, the course increasingly shifted to the rostral side with increasing tumor size. With the retrosigmoid approach, Rand et al. 17,18 reported that the dorsal pattern with the nerve running on the operator s side of the tumor was present in 7-9% of cases.
14 However, for this type of pattern, Sampath et al. 15 reported a frequency of % and Bae et al. 16 noted one of 0.6%, and this pattern was also extremely rare in our series, seen in only one case (0.3%). If the small number of cases with patterns C and D is excluded, there was no difference with respect to postoperative facial nerve function between VCe, VR, VCa, and R, and around 90% of patients were Grade 2 on the House-Brackmann scale after 8-12 months. When the facial nerve is located on the dorsal aspect of the tumor, however, tumor resection is performed across the facial nerve from the start, meaning that postoperative palsy (Grade 3) occurs more easily due to excessive manipulation of the nerve. With respect to adhesion of the facial nerve to the tumor, there were no major differences between VCe, VR, and VCa in terms of course pattern, but adhesion was frequent in cases of R, C, and D, courses that ran in an extremely distorted pattern. Adhesion was more frequent for larger tumors in all course patterns, with stronger pressure from the tumor on the nerve resulting in it becoming morphologically stretched and flattened, with a higher chance of adhering strongly to the tumor capsule and even becoming incorporated within the tumor in some cases. Sampath et al. 15 reported that the facial nerve passed through the tumor itself (infiltrating tumor or enfolded by tumor) in around 3% of cases, but unlike our series, this was not related to tumor size. The site of strongest adhesion was in the region of the internal acoustic foramen in all course patterns, and as there was a tendency for longer latency and smaller amplitude during continuous stimulation monitoring for resections in this area, this location is regarded as having the highest risk of causing facial nerve damage. Accordingly, in recent cases, we have been
15 performing subtotal removal if there is severe adhesion between the facial nerve and the tumor, leaving part of the tumor capsule along the course of the facial nerve, with the goal of facial nerve preservation. Conclusions When performing acoustic neuroma surgery, attempts should be made to preserve hearing acuity and to accurately identify the course of the facial nerve in order to preserve its function. Since it remains difficult to accurately identify the course of the facial nerve on preoperative images, surgical manipulation must be performed carefully and precisely, using appropriate measures as such frequent intraoperative nerve stimulation and continuous stimulation monitoring. References 1) House JW, Brackmann DE. Facial nerve grading system. Otolayngol Head Neck Surg. 1985;93: ) Fischer G, Fischer C, Remond J. Hearing preservation in acoustic neuroma surgery. J Neurosurg. 1992;76: ) Glasscock ME III, Hays JW, Minor LB, Haynes DS, Carrasco VN. Preservation of
16 hearing in surgery for acoustic neuroma. J Neurosurg. 1993;78: ) House WF. Monograph II. Acoustic neuroma. Arch Otolaryngol. 1968;88: ) Ojemann RG. Management of acoustic neuromas (vestibular schwannomas). Clin Neurosurg. 1993;40: ) Samii M, Matthies C. Management of 1000 vestibular scwannomas (acoustic neuromas): the facial nerve-preservation and restitution of function. Neurosurg. 1997;40: ) Samii M, Matthies C. Management of 1000 vestibular scwannomas (acoustic neuromas): surgical management and results with an emphasis on complication and how to avoid them. Neurosurg. 1997;40: ) Samii M, Gerganov V, Samii A. Improved preservation of hearing and facial nerve function in vestibular schwannoma surgery via the retrosigmoid approach in a series of 200 patients. J Neurosurg. 2006;105: ) Ransohoff J. Microsurgical anatomy of the brainstem surface facing an acoustic neuroma. Surgical Neurol. 1986;26:598. (Letter) 10) Rhoton AL Jr. Microsurgical anatomy of the brainstem surface facing an acoustic neuroma. Surgical Neurol. 1986;25; (Letter) 11) Rhoton AL Jr, Tedeschi H. Microsurgical anatomy of acoustic neuroma. Otolaryngol Clin North Am. 1992;25: ) Moriyama T, Fukushima T, Asaoka K, Roche PH, Barrs DM, McElveen JT. Hearing preservation in acoustic neuroma surgery: importance of adhesion between the cochlear nerve and the tumor. J Neurosurg. 2002;97: ) Sameshima T, Fukushima T, McElveen JT, Friedman AH. Critical assessment of
17 operative approaches for hearing preservation in small acoustic neuroma surgery: Retrosigmoid vs middle fossa approach. Neurosurg. 2010;67: ) Benecke JE Jr, Calder HB, Chadwick G. Facial nerve monitoring during acoustic neuroma removal. Laryngoscope. 1987;97: ) Sampath P, Rini D, Long DM. Microanatomical variations in the cerebellopontine angle associated with vestibular schwannomas (acoustic neuromas): a retrospective study of 1006 consecutive cases. J Neurosurg. 2000;92: ) Bae CW, Cho YH, Hong SH, Kim JH, Lee JK, Kim CJ. The anatomical location and course of the facial nerve in vestibular schwannomas: A study of 163 surgically treasted cases. J Korean Neurosurg Soc. 2007;42: ) Rand RW. Microneurosurgery, ed 3. St Louis: Mosby, 1985, 18) Rand RW. Microsurgical anatomy of the brainstem surface facing an acoustic neuroma. Surgical Neurol. 1987;27:403. (Letter) Legends to Figure and Tables Figure 1 Illustration showing our classification of facial nerve course patterns in acoustic neuroma. (1) ventro-central surface of the tumor (VCe); (2) ventro-rostral surface (VR); (3) ventro-caudal surface (VCa); (4) rostral surface (R); (5) caudal surface (C); and (6) dorsal surface (D).
18 Table 1 Facial nerve course patterns by tumor size. Table 2 Postoperative facial nerve outcome (late) according to the House-Brackmann scale for each facial nerve course pattern. Table 3 Presence of adhesions and postoperative facial nerve palsy in relation to tumor size and facial nerve course patterns. Table 4 Presence of adhesions and postoperative facial nerve palsy.
19 Figure
20 Table1 TABLE 1 Facial nerve course patterns by tumor size. No. of Course of facial nerve Tumor size (cm) patients VCe VR VCa R C D < (78.6%) 21(21.4%) (46.2%) 89(45.6%) 11(5.6%) 3(1.5%) 1(0.5%) 1(0.5%) > (28.6%) 27(42.9%) 8(12.7%) 7(11.1%) 3(4.8%) 0 Total (52.0%) 137(38.5%) 19(5.3%) 10(2.8%) 4(1.1%) 1(0.3%) *VCe: ventro-central pattern, VR: ventro-rostral pattern, VCa: ventro-caudal pattern, C: caudal pattern, R: rostral pattern, D: dorsal pattern
21 Table2 TABLE 2 Postoperative facial nerve outcome (late) according to the House-Brackmann scale for each facial nerve course pattern. Course of facial nerve Grade VCe VR VCa R C D 1 131(70.8%) 99(72.3%) 15(78.9%) 8(80.0%) 2(50.0%) (21.6%) 31(22.6%) 1(5.3%) 1(10.0%) (4.9%) 5(3.6%) 2(10.5%) 1(10.0%) 2(50.0%) 1(100%) 4 5(2.7%) 2(1.5%) 1(5.3%) Total
22 Table3 TABLE 3 Presence of adhesions and postoperative facial nerve palsy in relation to tumor size and facial nerve course patterns. Course of facial nerve Tumor size VCe VR VCa R C D (cm) < /77(28.6%) 8/21(38.1%) /90(54.4%) 49/89(55.1%) 3/11(27.3%) 2/3(66.7%) 1/1(100%) 1/1(100%) > /18(77.8%) 22/27(81.5%) 5/8(62.5%) 6/7(85.7%) 2/3(66.7%) 0 Total 85/185(45.9%) 79/137(57.7%) 8/19(42.1%) 8/10(80.0%) 3/4(75.0%) 1/1(100%)
23 Table4 TABLE 4 Presence of adhesions and postoperative facial nerve palsy. Postop Grade Adhesion (+) 113(44.3%) 47(64.4%) 16(80.0%) 8(100.0%) 0 Adhesion (-) 142(55.7%) 26(35.6%) 4(20.0%) 0 0 Total *According to the House-Brackmann grading system
Evaluation of Variation in the Course of the Facial Nerve, Nerve Adhesion to Tumors, and Postoperative Facial Palsy in Acoustic Neuroma
 Original Article 39 Evaluation of Variation in the Course of the Facial Nerve, Nerve Adhesion to Tumors, and Postoperative Facial Palsy in Acoustic Neuroma Tetsuro Sameshima 1 Akio Morita 1 Rokuya Tanikawa
Original Article 39 Evaluation of Variation in the Course of the Facial Nerve, Nerve Adhesion to Tumors, and Postoperative Facial Palsy in Acoustic Neuroma Tetsuro Sameshima 1 Akio Morita 1 Rokuya Tanikawa
Internal Auditory Canal Involvement of Acoustic Neuromas: Surgical Correlates to Magnetic Resonance Imaging Findings
 Otology & Neurotology 22:92 96 200, Otology & Neurotology, Inc. Internal Auditory Canal Involvement of Acoustic Neuromas: Surgical Correlates to Magnetic Resonance Imaging Findings * Samuel H. Selesnick,
Otology & Neurotology 22:92 96 200, Otology & Neurotology, Inc. Internal Auditory Canal Involvement of Acoustic Neuromas: Surgical Correlates to Magnetic Resonance Imaging Findings * Samuel H. Selesnick,
Spatial Relationship between Vestibular Schwannoma and Facial Nerve on Three-dimensional T2-weighted Fast Spin-echo MR Images
 AJNR Am J Neuroradiol 21:810 816, May 2000 Spatial Relationship between Vestibular Schwannoma and Facial Nerve on Three-dimensional T2-weighted Fast Spin-echo MR Images Sabine Sartoretti-Schefer, Spyros
AJNR Am J Neuroradiol 21:810 816, May 2000 Spatial Relationship between Vestibular Schwannoma and Facial Nerve on Three-dimensional T2-weighted Fast Spin-echo MR Images Sabine Sartoretti-Schefer, Spyros
Neurosurgical Review. CE-Chirp ABR in cerebellopontine angle surgery neuromonitoring: technical assessment in four cases.
 CE-Chirp ABR in cerebellopontine angle surgery neuromonitoring: technical assessment in four cases. Journal: Neurosurgical Review Manuscript ID: Draft Manuscript Type: Case Report Date Submitted by the
CE-Chirp ABR in cerebellopontine angle surgery neuromonitoring: technical assessment in four cases. Journal: Neurosurgical Review Manuscript ID: Draft Manuscript Type: Case Report Date Submitted by the
Pichayen Duangthongpon MD*, Chaiwit Thanapaisal MD*, Amnat Kitkhuandee MD*, Kowit Chaiciwamongkol MD**, Vilaiwan Morthong MD**
 The Relationships between Asterion, the Transverse-Sigmoid Junction, the Superior Nuchal Line and the Transverse Sinus in Thai Cadavers: Surgical Relevance Pichayen Duangthongpon MD*, Chaiwit Thanapaisal
The Relationships between Asterion, the Transverse-Sigmoid Junction, the Superior Nuchal Line and the Transverse Sinus in Thai Cadavers: Surgical Relevance Pichayen Duangthongpon MD*, Chaiwit Thanapaisal
Schwannoma of the intermediate nerve
 J Neurosurg 109:144 148, 2008 Schwannoma of the intermediate nerve Case report CHRISTIAN SCHELLER, M.D., 1 JENS RACHINGER, M.D., 1 JULIAN PRELL, M.D., 1 MALTE KORNHUBER, M.D., 2 AND CHRISTIAN STRAUSS,
J Neurosurg 109:144 148, 2008 Schwannoma of the intermediate nerve Case report CHRISTIAN SCHELLER, M.D., 1 JENS RACHINGER, M.D., 1 JULIAN PRELL, M.D., 1 MALTE KORNHUBER, M.D., 2 AND CHRISTIAN STRAUSS,
SPECIAL PAPER IN CELEBRATION OF PROF. YANG'S 50 YEARS CAREER IN MEDICINE
 JOURNAL OF OTOLOGY SPECIAL PAPER IN CELEBRATION OF PROF. YANG'S 50 YEARS CAREER IN MEDICINE ADVANCES IN SURGICAL TREATMENT OF ACOUSTIC NEUROMA HAN Dongyi,CAI Chaochan Acoustic Neuroma (AN) arises from
JOURNAL OF OTOLOGY SPECIAL PAPER IN CELEBRATION OF PROF. YANG'S 50 YEARS CAREER IN MEDICINE ADVANCES IN SURGICAL TREATMENT OF ACOUSTIC NEUROMA HAN Dongyi,CAI Chaochan Acoustic Neuroma (AN) arises from
Results of Surgery of Cerebellopontine angle Tumors
 Original Article Iranian Journal of Otorhinolaryngology, Vol. 27(1), Serial No.78, Jan 2015 Abstract Results of Surgery of Cerebellopontine angle Tumors Faramarz Memari 1, * Fatemeh Hassannia 1, Seyed
Original Article Iranian Journal of Otorhinolaryngology, Vol. 27(1), Serial No.78, Jan 2015 Abstract Results of Surgery of Cerebellopontine angle Tumors Faramarz Memari 1, * Fatemeh Hassannia 1, Seyed
Acoustic Neuroma. Presenting Signs and Symptoms of an Acoustic Neuroma:
 Acoustic Neuroma An acoustic neuroma is a benign tumor which arises from the nerves behind the inner ear and which may affect hearing and balance. The incidence of symptomatic acoustic neuroma is estimated
Acoustic Neuroma An acoustic neuroma is a benign tumor which arises from the nerves behind the inner ear and which may affect hearing and balance. The incidence of symptomatic acoustic neuroma is estimated
For most large acoustic neuromas that bulge into the
 clinical article J Neurosurg 125:787 794, 2016 In vivo visualization of the facial nerve in patients with acoustic neuroma using diffusion tensor imaging based fiber tracking *Fei Song, MM, 1 Yuanzheng
clinical article J Neurosurg 125:787 794, 2016 In vivo visualization of the facial nerve in patients with acoustic neuroma using diffusion tensor imaging based fiber tracking *Fei Song, MM, 1 Yuanzheng
Facial nerve injury in acoustic neuroma (vestibular schwannoma) surgery: etiology and prevention
 surgery: etiology and prevention") Neurosurg Focus 5 (3):Article 4, 1998 Facial nerve injury in acoustic neuroma (vestibular schwannoma) surgery: etiology and prevention Prakash Sampath, M.D., Michael J. Holliday M.D., Henry Brem, M.D.,
Neurosurg Focus 5 (3):Article 4, 1998 Facial nerve injury in acoustic neuroma (vestibular schwannoma) surgery: etiology and prevention Prakash Sampath, M.D., Michael J. Holliday M.D., Henry Brem, M.D.,
Neurosurgery 72[ONS Suppl 2]:ons103 ons115, 2013
![Neurosurgery 72[ONS Suppl 2]:ons103 ons115, 2013](/thumbs/96/127295777.jpg "Neurosurgery 72[ONS Suppl 2]:ons103 ons115, 2013") TUMOR Operative Nuances Contemporary Surgical Management of Vestibular Schwannomas: Analysis of Complications and Lessons Learned Over the Past Decade Yoichi Nonaka, MD, PhD* Takanori Fukushima, MD, DMSc*
TUMOR Operative Nuances Contemporary Surgical Management of Vestibular Schwannomas: Analysis of Complications and Lessons Learned Over the Past Decade Yoichi Nonaka, MD, PhD* Takanori Fukushima, MD, DMSc*
Injury to the facial nerve is a common complication. Efficacy of facial nerve sparing approach in patients with vestibular schwannomas
 See the corresponding editorial in this issue, pp 915 916. J Neurosurg 115:917 923, 2011 Efficacy of facial nerve sparing approach in patients with vestibular schwannomas Clinical article Raqeeb Haque,
See the corresponding editorial in this issue, pp 915 916. J Neurosurg 115:917 923, 2011 Efficacy of facial nerve sparing approach in patients with vestibular schwannomas Clinical article Raqeeb Haque,
Revision Surgery for Vestibular Schwannomas
 528 Original Article Kevin A. Peng 1 Brian S. Chen 3 Mark B. Lorenz 2 Gregory P. Lekovic 1 Marc S. Schwartz 1 William H. Slattery 1 Eric P. Wilkinson 1 1 House Clinic, Los Angeles, California, United States
528 Original Article Kevin A. Peng 1 Brian S. Chen 3 Mark B. Lorenz 2 Gregory P. Lekovic 1 Marc S. Schwartz 1 William H. Slattery 1 Eric P. Wilkinson 1 1 House Clinic, Los Angeles, California, United States
What cranial nerves can we monitor?
 What cranial nerves can we monitor? Laura Hemmer, M.D. SNACC Neuromonitoring Subcommittee Linda Aglio, M.D., M.S. Laura Hemmer, M.D. Antoun Koht, M.D. David L. Schreibman, M.D. What cranial nerve (CN)
What cranial nerves can we monitor? Laura Hemmer, M.D. SNACC Neuromonitoring Subcommittee Linda Aglio, M.D., M.S. Laura Hemmer, M.D. Antoun Koht, M.D. David L. Schreibman, M.D. What cranial nerve (CN)
Introduction to Neurosurgical Subspecialties:
 Introduction to Neurosurgical Subspecialties: Tumor and Skull Base Neurosurgery Brian L. Hoh, MD 1 and Gregory J. Zipfel, MD 2 1 University of Florida, 2 Washington University Tumor / Skull Base Neurosurgery
Introduction to Neurosurgical Subspecialties: Tumor and Skull Base Neurosurgery Brian L. Hoh, MD 1 and Gregory J. Zipfel, MD 2 1 University of Florida, 2 Washington University Tumor / Skull Base Neurosurgery
Management of Cerebrospinal Fluid Leaks After Vestibular Schwannoma Surgery
 Otology & Neurotology 32:1525Y1529 Ó 2011, Otology & Neurotology, Inc. Management of Cerebrospinal Fluid Leaks After Vestibular Schwannoma Surgery *Brannon D. Mangus, *Alejandro Rivas, Mi Jin Yoo, JoAnn
Otology & Neurotology 32:1525Y1529 Ó 2011, Otology & Neurotology, Inc. Management of Cerebrospinal Fluid Leaks After Vestibular Schwannoma Surgery *Brannon D. Mangus, *Alejandro Rivas, Mi Jin Yoo, JoAnn
Removal of vestibular schwannoma and facial nerve preservation using small suboccipital retrosigmoid craniotomy
 274 Original article Removal of vestibular schwannoma and facial nerve preservation using small suboccipital retrosigmoid craniotomy CHEN Ling, CHEN Li-hua, LING Feng, LIU Yun-sheng, Madjid Samii and Amir
274 Original article Removal of vestibular schwannoma and facial nerve preservation using small suboccipital retrosigmoid craniotomy CHEN Ling, CHEN Li-hua, LING Feng, LIU Yun-sheng, Madjid Samii and Amir
Vestibular schwannomas (VSs) account for 6% 8%
 account for 6% 8%") clinical article J Neurosurg 125:1277 1282, 2016 Stability of hearing preservation and regeneration capacity of the cochlear nerve following vestibular schwannoma surgery via a retrosigmoid approach Christian
clinical article J Neurosurg 125:1277 1282, 2016 Stability of hearing preservation and regeneration capacity of the cochlear nerve following vestibular schwannoma surgery via a retrosigmoid approach Christian
The Best Candidates for Nerve-Sparing Stripping Surgery for Facial Nerve Schwannoma
 The Laryngoscope VC 2014 The American Laryngological, Rhinological and Otological Society, Inc. The Best Candidates for Nerve-Sparing Stripping Surgery for Facial Nerve Schwannoma Soon H. Park, MD; Jin
The Laryngoscope VC 2014 The American Laryngological, Rhinological and Otological Society, Inc. The Best Candidates for Nerve-Sparing Stripping Surgery for Facial Nerve Schwannoma Soon H. Park, MD; Jin
Title. Author(s) Takahashi, Haruo. Issue Date Right.
 Takahashi, Haruo. Issue Date Right.") NAOSITE: Nagasaki University's Ac Title Author(s) Citation A case with posterior fossa epiderm symptoms caused by insufficiency of usefulness of free DICOM image view Takasaki, Kenji; Kumagami, Hidetaka
NAOSITE: Nagasaki University's Ac Title Author(s) Citation A case with posterior fossa epiderm symptoms caused by insufficiency of usefulness of free DICOM image view Takasaki, Kenji; Kumagami, Hidetaka
Temporal Lobe Cystic Collection and Associated Oedema: A Rare Complication of Translabyrinthine Resection of Vestibular Schwannoma
 Open Access Case Report DOI: 10.7759/cureus.2217 Temporal Lobe Cystic Collection and Associated Oedema: A Rare Complication of Translabyrinthine Resection of Vestibular Schwannoma Abdurrahman Raeiq 1 1.
Open Access Case Report DOI: 10.7759/cureus.2217 Temporal Lobe Cystic Collection and Associated Oedema: A Rare Complication of Translabyrinthine Resection of Vestibular Schwannoma Abdurrahman Raeiq 1 1.
EDUCATIONAL COURSE «SKULL BASE SURGERY: MICROSURGICAL AND ENDOSCOPIC APPROACHES» October 8-12, 2015
 EDUCATIONAL COURSE under the auspices of Neuroendoscopy committee World Federation of Neurosurgical Societies (WFNS) «SKULL BASE SURGERY: MICROSURGICAL AND ENDOSCOPIC APPROACHES» October 8-12, 2015 Course
EDUCATIONAL COURSE under the auspices of Neuroendoscopy committee World Federation of Neurosurgical Societies (WFNS) «SKULL BASE SURGERY: MICROSURGICAL AND ENDOSCOPIC APPROACHES» October 8-12, 2015 Course
Perforating branches from ovending arteries in hemifacial spasm: anatomical correlation with vertebrobasilar configuration
 J Neurol Neurosurg Psychiatry 1999;67:73 77 73 Department of Neurosurgery, Nagoya University School of Medicine, Nagoya, Japan T Nagatani S Inao Y Suzuki J Yoshida Correspondence to: Dr T Nagatani, Department
J Neurol Neurosurg Psychiatry 1999;67:73 77 73 Department of Neurosurgery, Nagoya University School of Medicine, Nagoya, Japan T Nagatani S Inao Y Suzuki J Yoshida Correspondence to: Dr T Nagatani, Department
With advances in microsurgical techniques and the. Staged resection of large vestibular schwannomas. Clinical article
 J Neurosurg 116:1126 1133, 2012 Staged resection of large vestibular schwannomas Clinical article Ahmed M. Raslan, M.D., 1 James K. Liu, M.D., 3 Sean O. McMenomey, M.D., 1,2 and Johnny B. Delashaw Jr.,
J Neurosurg 116:1126 1133, 2012 Staged resection of large vestibular schwannomas Clinical article Ahmed M. Raslan, M.D., 1 James K. Liu, M.D., 3 Sean O. McMenomey, M.D., 1,2 and Johnny B. Delashaw Jr.,
LONG-TERM FOLLOW-UP OF ACOUSTIC SCHWANNOMA RADIOSURGERY WITH MARGINAL TUMOR DOSES OF 12 TO 13 Gy
 doi:10.1016/j.ijrobp.2007.01.001 Int. J. Radiation Oncology Biol. Phys., Vol. 68, No. 3, pp. 845 851, 2007 Copyright 2007 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/07/$ see front
doi:10.1016/j.ijrobp.2007.01.001 Int. J. Radiation Oncology Biol. Phys., Vol. 68, No. 3, pp. 845 851, 2007 Copyright 2007 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/07/$ see front
Subtotal resection of vestibular schwannoma: Evaluation with Ki-67 measurement, magnetic resonance imaging, and long-term observation
 Clinical Report Subtotal resection of vestibular schwannoma: Evaluation with Ki-67 measurement, magnetic resonance imaging, and long-term observation Journal of International Medical Research 2017, Vol.
Clinical Report Subtotal resection of vestibular schwannoma: Evaluation with Ki-67 measurement, magnetic resonance imaging, and long-term observation Journal of International Medical Research 2017, Vol.
Unilateral Vestibular Schwannomas in Childhood without Evidence of Neurofibromatosis: Experience of 10 Patients at a Single Institute
 DOI: 10.5137/1019-5149.JTN.16283-15.1 Received: 06.10.2015 / Accepted: 28.12.2015 Published Online: 27.05.2016 Original Investigation Unilateral Vestibular Schwannomas in Childhood without Evidence of
DOI: 10.5137/1019-5149.JTN.16283-15.1 Received: 06.10.2015 / Accepted: 28.12.2015 Published Online: 27.05.2016 Original Investigation Unilateral Vestibular Schwannomas in Childhood without Evidence of
 Intracanalicular (0 mm) 10 mm 20 mm 30 mm Translabyrinthine approach Retrosigmoid approach Middle Fossa Approach Otology & Neurotology 24:473 477 2003, Otology & Neurotology, Inc. The Effect of Age on
Intracanalicular (0 mm) 10 mm 20 mm 30 mm Translabyrinthine approach Retrosigmoid approach Middle Fossa Approach Otology & Neurotology 24:473 477 2003, Otology & Neurotology, Inc. The Effect of Age on
Temporal Bone Magnetic Resonance Imaging Study in Hemifacial Spasm
 Temporal Bone Magnetic Resonance Imaging Study in Hemifacial Spasm Sun Kon Kim, M.D., Jin Ho Kim, M.D., Jin Woo Yang, M.D., Hyun Jeong Lee, M.D., Tae Sub Cheong, M.D.*, Young Ho Sohn, M.D., Jin-Soo Kim,
Temporal Bone Magnetic Resonance Imaging Study in Hemifacial Spasm Sun Kon Kim, M.D., Jin Ho Kim, M.D., Jin Woo Yang, M.D., Hyun Jeong Lee, M.D., Tae Sub Cheong, M.D.*, Young Ho Sohn, M.D., Jin-Soo Kim,
QUANTITATIVE ANALYSIS AND COMPUTER AIDED SIMULATION OF MINIMALLY INVASIVE APPROACHES FOR INTRACRANIAL VASCULAR LESIONS
 QUANTITATIVE ANALYSIS AND COMPUTER AIDED SIMULATION OF MINIMALLY INVASIVE APPROACHES FOR INTRACRANIAL VASCULAR LESIONS Alberto Prats Galino Facultat de Medicina UB 1. Project Summary The main goal of this
QUANTITATIVE ANALYSIS AND COMPUTER AIDED SIMULATION OF MINIMALLY INVASIVE APPROACHES FOR INTRACRANIAL VASCULAR LESIONS Alberto Prats Galino Facultat de Medicina UB 1. Project Summary The main goal of this
Otolaryngologist s Perspective of Stereotactic Radiosurgery
 Otolaryngologist s Perspective of Stereotactic Radiosurgery Douglas E. Mattox, M.D. 25 th Alexandria International Combined ORL Conference April 18-20, 2007 Acoustic Neuroma Benign tumor of the schwann
Otolaryngologist s Perspective of Stereotactic Radiosurgery Douglas E. Mattox, M.D. 25 th Alexandria International Combined ORL Conference April 18-20, 2007 Acoustic Neuroma Benign tumor of the schwann
Recently, GKS has been regarded as a major therapeutic. Nervus intermedius dysfunction following Gamma Knife surgery for vestibular schwannoma
 J Neurosurg 118:566 570, 2013 AANS, 2013 Nervus intermedius dysfunction following Gamma Knife surgery for vestibular schwannoma Clinical article Seong-Hyun Park, M.D., 1 Kyu-Yup Lee, M.D., 2 and Sung-Kyoo
J Neurosurg 118:566 570, 2013 AANS, 2013 Nervus intermedius dysfunction following Gamma Knife surgery for vestibular schwannoma Clinical article Seong-Hyun Park, M.D., 1 Kyu-Yup Lee, M.D., 2 and Sung-Kyoo
Indications and contra-indications of auditory brainstem implants. Systematic review and illustrative cases
 Manuscript: Authors: Journal: Indications and contra-indications of auditory brainstem implants. Systematic review and illustrative cases Merkus P (p.merkus@vumc.nl), Di Lella F, Di Trapani G, Pasanisi
Manuscript: Authors: Journal: Indications and contra-indications of auditory brainstem implants. Systematic review and illustrative cases Merkus P (p.merkus@vumc.nl), Di Lella F, Di Trapani G, Pasanisi
CASE REPORTS. Surgical Treatment of Cerebellopontine Angle Trigeminal Schwannoma Via a Retrosigmoid Intradural Approach: A Case Report
 CASE REPORTS Surgical Treatment of Cerebellopontine Angle Trigeminal Schwannoma Via a Retrosigmoid Intradural Approach: A Case Report Cédric Porret MD.,Christian Dubreuil MD. From the Otoneurosurgery Department,
CASE REPORTS Surgical Treatment of Cerebellopontine Angle Trigeminal Schwannoma Via a Retrosigmoid Intradural Approach: A Case Report Cédric Porret MD.,Christian Dubreuil MD. From the Otoneurosurgery Department,
The Classification of Posterior Petrous Meningiomas and Its Clinical Significance
 The Journal of International Medical Research 2009; 37: 949 957 [first published online as 37(3) 13] The Classification of Posterior Petrous Meningiomas and Its Clinical Significance FJ QU 1 *, XD ZHOU
The Journal of International Medical Research 2009; 37: 949 957 [first published online as 37(3) 13] The Classification of Posterior Petrous Meningiomas and Its Clinical Significance FJ QU 1 *, XD ZHOU
Submitted: Revised: Published:
 ORIGINAL ARTICLE ASIAN JOURNAL OF MEDICAL SCIENCES A study assessing the post operative outcome in patients of acoustic schwannoma operated through retrosigmoid approach at tertiary care institutions-
ORIGINAL ARTICLE ASIAN JOURNAL OF MEDICAL SCIENCES A study assessing the post operative outcome in patients of acoustic schwannoma operated through retrosigmoid approach at tertiary care institutions-
Posterior surgical procedures are those procedures
 9 Cervical Posterior surgical procedures are those procedures that have been in use for a long time with established efficacy in the treatment of radiculopathy and myelopathy caused by pathologies including
9 Cervical Posterior surgical procedures are those procedures that have been in use for a long time with established efficacy in the treatment of radiculopathy and myelopathy caused by pathologies including
Intracanalicular acoustic neuroma: early surgery for preservation of hearing STEPHEN J. HAINES, M.D., AND SAMUEL C. LEVINE, M.D.
 J Neurosnrg 79:55-50, 99 Intracanalicular acoustic neuroma: early surgery for preservation of hearing STEPHEN J. HAINES, M.D., AND SAMUEL C. LEVINE, M.D. Center for Craniofacial and Skull Base Surgery,
J Neurosnrg 79:55-50, 99 Intracanalicular acoustic neuroma: early surgery for preservation of hearing STEPHEN J. HAINES, M.D., AND SAMUEL C. LEVINE, M.D. Center for Craniofacial and Skull Base Surgery,
January 25-26, Annual Spetzler Microneurosurgery Course Barrow Neurological Institute
 2018 Annual Spetzler Microneurosurgery Course Microneurosurgery of the Skull Base: Lateral Approaches, Anatomy & Techniques January 25-26, 2018 Phoenix, Arizona For more information: www.barrowneuro.org/education/find-a-conference-or-cme-course/
2018 Annual Spetzler Microneurosurgery Course Microneurosurgery of the Skull Base: Lateral Approaches, Anatomy & Techniques January 25-26, 2018 Phoenix, Arizona For more information: www.barrowneuro.org/education/find-a-conference-or-cme-course/
Retro-odontoid pseudotumors are mass lesions formed
 SURGICAL TECHNIQUE Microscopic Posterior Transdural Resection of Cervical Retro-Odontoid Pseudotumors Yasushi Fujiwara, MD, PhD,* Hideki Manabe,* Tadayoshi Sumida,w Nobuhiro Tanaka,z and Takahiko Hamasakiy
SURGICAL TECHNIQUE Microscopic Posterior Transdural Resection of Cervical Retro-Odontoid Pseudotumors Yasushi Fujiwara, MD, PhD,* Hideki Manabe,* Tadayoshi Sumida,w Nobuhiro Tanaka,z and Takahiko Hamasakiy
Audit and Compliance Department 1
 Introduction to Intraoperative Neuromonitoring An intro to those squiggly lines Kunal Patel MS, CNIM None Disclosures Learning Objectives History of Intraoperative Monitoring What is Intraoperative Monitoring
Introduction to Intraoperative Neuromonitoring An intro to those squiggly lines Kunal Patel MS, CNIM None Disclosures Learning Objectives History of Intraoperative Monitoring What is Intraoperative Monitoring
FRACTIONATED STEREOTACTIC RADIOTHERAPY FOR ACOUSTIC NEUROMAS
 PII S0360-3016(02)02763-3 Int. J. Radiation Oncology Biol. Phys., Vol. 54, No. 2, pp. 500 504, 2002 Copyright 2002 Elsevier Science Inc. Printed in the USA. All rights reserved 0360-3016/02/$ see front
PII S0360-3016(02)02763-3 Int. J. Radiation Oncology Biol. Phys., Vol. 54, No. 2, pp. 500 504, 2002 Copyright 2002 Elsevier Science Inc. Printed in the USA. All rights reserved 0360-3016/02/$ see front
The New England Journal of Medicine LONG-TERM OUTCOMES AFTER RADIOSURGERY FOR ACOUSTIC NEUROMAS
 LONG-TERM OUTCOMES AFTER RADIOSURGERY FOR ACOUSTIC NEUROMAS DOUGLAS KONDZIOLKA, M.D., L. DADE LUNSFORD, M.D., MARK R. MCLAUGHLIN, M.D., AND JOHN C. FLICKINGER, M.D. ABSTRACT Background Stereotactic radiosurgery
LONG-TERM OUTCOMES AFTER RADIOSURGERY FOR ACOUSTIC NEUROMAS DOUGLAS KONDZIOLKA, M.D., L. DADE LUNSFORD, M.D., MARK R. MCLAUGHLIN, M.D., AND JOHN C. FLICKINGER, M.D. ABSTRACT Background Stereotactic radiosurgery
Acoustic Neuroma (vestibular schwannoma) basic level
 basic level") Acoustic Neuroma (vestibular schwannoma) basic level Overview An acoustic neuroma is a tumor that grows from the nerves responsible for balance and hearing. More accurately called vestibular schwannoma,
Acoustic Neuroma (vestibular schwannoma) basic level Overview An acoustic neuroma is a tumor that grows from the nerves responsible for balance and hearing. More accurately called vestibular schwannoma,
Research Journal of Pharmaceutical, Biological and Chemical Sciences
 Research Journal of Pharmaceutical, Biological and Chemical Sciences Morphometric Analysis of Internal Acoustic Meatus and Its Surgically Relevant Relations in Human Temporal Bones. Rajanigandha Vadagaonkar
Research Journal of Pharmaceutical, Biological and Chemical Sciences Morphometric Analysis of Internal Acoustic Meatus and Its Surgically Relevant Relations in Human Temporal Bones. Rajanigandha Vadagaonkar
Acoustic Neuroma (vestibular schwannoma)
") 1 2 Acoustic Neuroma (vestibular schwannoma) Overview An acoustic neuroma is a tumor that grows from the nerves responsible for balance and hearing. These tumors grow from the sheath covering the vestibulocochlear
1 2 Acoustic Neuroma (vestibular schwannoma) Overview An acoustic neuroma is a tumor that grows from the nerves responsible for balance and hearing. These tumors grow from the sheath covering the vestibulocochlear
Impact of video-endoscopy on the results of retrosigmoidtransmeatal microsurgery of vestibular schwannoma: prospective study
 Eur Arch Otorhinolaryngol (2013) 270:1277 1284 DOI 10.1007/s00405-012-2112-6 OTOLOGY Impact of video-endoscopy on the results of retrosigmoidtransmeatal microsurgery of vestibular schwannoma: prospective
Eur Arch Otorhinolaryngol (2013) 270:1277 1284 DOI 10.1007/s00405-012-2112-6 OTOLOGY Impact of video-endoscopy on the results of retrosigmoidtransmeatal microsurgery of vestibular schwannoma: prospective
The human brainstem, roughly the size of the thumb,
 TECHNICAL NOTE J Neurosurg 127:1134 1138, 2017 The superior fovea triangle approach: a novel safe entry zone to the brainstem *Kaan Yagmurlu, MD, M. Yashar S. Kalani, MD, PhD, Mark C. Preul, MD, and Robert
TECHNICAL NOTE J Neurosurg 127:1134 1138, 2017 The superior fovea triangle approach: a novel safe entry zone to the brainstem *Kaan Yagmurlu, MD, M. Yashar S. Kalani, MD, PhD, Mark C. Preul, MD, and Robert
Microneurosurgical and Endoscopic Approaches to the Skull Base
 Microneurosurgical and Endoscopic Approaches to the Skull Base December 11-13, 2014 Phoenix, Arizona Registration form: www.thebarrow.org/conferences_and_symposia/index.htm Course Description Microneurosurgical
Microneurosurgical and Endoscopic Approaches to the Skull Base December 11-13, 2014 Phoenix, Arizona Registration form: www.thebarrow.org/conferences_and_symposia/index.htm Course Description Microneurosurgical
Stereotactic radiosurgery in the management of acoustic neuromas associated with neurofibromatosis Type 2
 Stereotactic radiosurgery in the management of acoustic neuromas associated with neurofibromatosis Type 2 Brian R. Subach, M.D., Douglas Kondziolka, M.D., M. Sc., F.R.C.S.(C), L. Dade Lunsford, M.D., F.A.C.S.,
Stereotactic radiosurgery in the management of acoustic neuromas associated with neurofibromatosis Type 2 Brian R. Subach, M.D., Douglas Kondziolka, M.D., M. Sc., F.R.C.S.(C), L. Dade Lunsford, M.D., F.A.C.S.,
Risk Factors for Hinge Fracture Associated with Surgery Following Cervical Open-Door Laminoplasty
 CLINICAL ARTICLE Korean J Neurotrauma 18;14(2):118-122 pissn 2234-8999 / eissn 2288-2243 https://doi.org/1.134/kjnt.18.14.2.118 Risk Factors for Hinge Fracture Associated with Surgery Following Cervical
CLINICAL ARTICLE Korean J Neurotrauma 18;14(2):118-122 pissn 2234-8999 / eissn 2288-2243 https://doi.org/1.134/kjnt.18.14.2.118 Risk Factors for Hinge Fracture Associated with Surgery Following Cervical
Via Transmastoid Approach. Mitul Chaitan Bhatt. Maharashtra University Miraj India
 ISSN: 2250-0359 Volume 6 Issue 1 2016 Evaluation Of Patients Of Traumatic Facial Palsy Treated By Facial Nerve Decompression Via Transmastoid Approach Mitul Chaitan Bhatt Maharashtra University Miraj India
ISSN: 2250-0359 Volume 6 Issue 1 2016 Evaluation Of Patients Of Traumatic Facial Palsy Treated By Facial Nerve Decompression Via Transmastoid Approach Mitul Chaitan Bhatt Maharashtra University Miraj India
Cervical Sympathetic Chain Schwannomas
 Showa Univ J Med Sci 27 2, 117 123, June 2015 Case Report Shunya EGAWA 1 3, Toshikazu SHIMANE 1 2 3, Kenichiro IKEDA 1 3, Yukiomi KUSHIHASHI 1 3, Yoichi IKENOYA 1 3, Manabu KITANO 3, Yuya KURASAWA 1 2,
Showa Univ J Med Sci 27 2, 117 123, June 2015 Case Report Shunya EGAWA 1 3, Toshikazu SHIMANE 1 2 3, Kenichiro IKEDA 1 3, Yukiomi KUSHIHASHI 1 3, Yoichi IKENOYA 1 3, Manabu KITANO 3, Yuya KURASAWA 1 2,
Neuroscience. Journal. Management of acoustic neuromas. P A L M E T T O H E A L T H Vol. 4 Issue 3 Summer 2018
 Neuroscience P A L M E T T O H E A L T H Vol. 4 Issue 3 Summer 2018 Journal Management of acoustic neuromas pg. 5 Palmetto Health-USC Huntington s Disease Clinic designated HDSA Center of Excellence pg.
Neuroscience P A L M E T T O H E A L T H Vol. 4 Issue 3 Summer 2018 Journal Management of acoustic neuromas pg. 5 Palmetto Health-USC Huntington s Disease Clinic designated HDSA Center of Excellence pg.
S urgical removal is the sole treatment for large acoustic
 453 PAPER Removal of large acoustic neurinomas (vestibular schwannomas) by the retrosigmoid approach with no mortality and minimal morbidity I Yamakami, Y Uchino, E Kobayashi, A Yamaura, N Oka... See end
453 PAPER Removal of large acoustic neurinomas (vestibular schwannomas) by the retrosigmoid approach with no mortality and minimal morbidity I Yamakami, Y Uchino, E Kobayashi, A Yamaura, N Oka... See end
Grading Facial Nerve Function Following Combined Static and Mimetic Surgical Techniques
 416 Original Article Grading Facial Nerve Function Following Combined Static and Mimetic Surgical Techniques John P. Leonetti 1 Sam J. Marzo 1 Douglas A. Anderson 2 Joshua M. Sappington 1 1 Department
416 Original Article Grading Facial Nerve Function Following Combined Static and Mimetic Surgical Techniques John P. Leonetti 1 Sam J. Marzo 1 Douglas A. Anderson 2 Joshua M. Sappington 1 1 Department
Surgical anatomy of the juxtadural ring area
 Surgical anatomy of the juxtadural ring area Susumu Oikawa, M.D., Kazuhiko Kyoshima, M.D., and Shigeaki Kobayashi, M.D. Department of Neurosurgery, Shinshu University School of Medicine, Matsumoto, Japan
Surgical anatomy of the juxtadural ring area Susumu Oikawa, M.D., Kazuhiko Kyoshima, M.D., and Shigeaki Kobayashi, M.D. Department of Neurosurgery, Shinshu University School of Medicine, Matsumoto, Japan
Rebecca J. Clark-Bash, R. EEG\EP T., CNIMeKnowledgePlus.net Page 1
 Navigating the Auditory Pathway: Technical & Physiological Impact on IOM Rebecca Clark-Bash, R. EEG\EP T, CLTM, CNIM, F.ASET, FASNM Faculty Rebecca Clark-Bash R. EEG\EP T., CLTM, CNIM, F.ASNM, F.ASET ASNM
Navigating the Auditory Pathway: Technical & Physiological Impact on IOM Rebecca Clark-Bash, R. EEG\EP T, CLTM, CNIM, F.ASET, FASNM Faculty Rebecca Clark-Bash R. EEG\EP T., CLTM, CNIM, F.ASNM, F.ASET ASNM
Conservative Management of Acoustic Neuroma
 ORIGINAL ARTICLE Conservative Management of Acoustic Neuroma Abdulrahman Al Sanosi, M.D., 1 Paul A. Fagan, M.D., F.R.C.S., F.R.A.C.S., 2 and Nigel D.W. Biggs, M.D., F.R.A.C.S. 2 ABSTRACT Aim of study:
ORIGINAL ARTICLE Conservative Management of Acoustic Neuroma Abdulrahman Al Sanosi, M.D., 1 Paul A. Fagan, M.D., F.R.C.S., F.R.A.C.S., 2 and Nigel D.W. Biggs, M.D., F.R.A.C.S. 2 ABSTRACT Aim of study:
Unilateral extended suboccipital approach for a C1 dumbbell schwanoma
 38 Gorgan et al Unilateral extended suboccipital approach for a C1 dumbbell schwanoma Unilateral extended suboccipital approach for a C1 dumbbell schwanoma R.M. Gorgan, Angela Neacşu, A. Giovani Clinical
38 Gorgan et al Unilateral extended suboccipital approach for a C1 dumbbell schwanoma Unilateral extended suboccipital approach for a C1 dumbbell schwanoma R.M. Gorgan, Angela Neacşu, A. Giovani Clinical
OTOLOGY. 1. BRIEF DESCRIPTION OF OTOLOGIC TRAINING Rotations that include otologic training are a component of each of the four years of training.
 OTOLOGY 1. BRIEF DESCRIPTION OF OTOLOGIC TRAINING Rotations that include otologic training are a component of each of the four years of training. Longwood Rotation PGY-2 through PGY-5 years o Clinic experience
OTOLOGY 1. BRIEF DESCRIPTION OF OTOLOGIC TRAINING Rotations that include otologic training are a component of each of the four years of training. Longwood Rotation PGY-2 through PGY-5 years o Clinic experience
Title. CitationInternational Cancer Conference Journal, 4(1): Issue Date Doc URL. Rights. Type. File Information
: Issue Date Doc URL. Rights. Type. File Information") Title Lymph node metastasis in the suprasternal space from Homma, Akihiro; Hatakeyama, Hiromitsu; Mizumachi, Ta Author(s) Tomohiro; Fukuda, Satoshi CitationInternational Cancer Conference Journal, 4(1):
Title Lymph node metastasis in the suprasternal space from Homma, Akihiro; Hatakeyama, Hiromitsu; Mizumachi, Ta Author(s) Tomohiro; Fukuda, Satoshi CitationInternational Cancer Conference Journal, 4(1):
Use of intraoperative auditory evoked potentials to preserve hearing in unilateral acoustic neuroma removal
 J Neurosurg 61:938-948, 1984 Use of intraoperative auditory evoked potentials to preserve hearing in unilateral acoustic neuroma removal ROBERT G. OJEMANN, M.D., ROBERT A. LEVINE, M.D., WILLIAM M. MONTGOMERY,
J Neurosurg 61:938-948, 1984 Use of intraoperative auditory evoked potentials to preserve hearing in unilateral acoustic neuroma removal ROBERT G. OJEMANN, M.D., ROBERT A. LEVINE, M.D., WILLIAM M. MONTGOMERY,
Radiologic Evaluation of Petrous Apex Masses. Pavan Kavali, MS-IV Morehouse School of Medicine November 16, 2009
 Radiologic Evaluation of Petrous Apex Masses Pavan Kavali, MS-IV Morehouse School of Medicine November 16, 2009 Roadmap Petrous Apex Anatomy Patient D.S.: Clinical Presentation Differential diagnosis of
Radiologic Evaluation of Petrous Apex Masses Pavan Kavali, MS-IV Morehouse School of Medicine November 16, 2009 Roadmap Petrous Apex Anatomy Patient D.S.: Clinical Presentation Differential diagnosis of
Hemifacial spasm is due to neurovascular compression
 Neurosurg Focus 34 (3):E6, 2013 AANS, 2013 Analysis of interpeak latencies of brainstem auditory evoked potential waveforms during microvascular decompression of cranial nerve VII for hemifacial spasm
Neurosurg Focus 34 (3):E6, 2013 AANS, 2013 Analysis of interpeak latencies of brainstem auditory evoked potential waveforms during microvascular decompression of cranial nerve VII for hemifacial spasm
Cystic VSs are described as behaving more aggressively. Fluid-fluid level in cystic vestibular schwannoma: a predictor of peritumoral adhesion
 J Neurosurg 120:197 206, 2014 AANS, 2014 Fluid-fluid level in cystic vestibular schwannoma: a predictor of peritumoral adhesion Clinical article Lei Xia, M.D., Ph.D., 1 Hongwei Zhang, M.D., Ph.D., 1 Chunjiang
J Neurosurg 120:197 206, 2014 AANS, 2014 Fluid-fluid level in cystic vestibular schwannoma: a predictor of peritumoral adhesion Clinical article Lei Xia, M.D., Ph.D., 1 Hongwei Zhang, M.D., Ph.D., 1 Chunjiang
ORIGINAL ARTICLE. Hearing Loss and Changes in Transient Evoked Otoacoustic Emissions After Gamma Knife Radiosurgery for Acoustic Neurinomas
 ORIGINAL ARTICLE Hearing Loss and Changes in Transient Evoked Otoacoustic Emissions After Gamma Knife Radiosurgery for Acoustic Neurinomas Francesco Ottaviani, MD; Cesare Bartolomeo Neglia, MD; Laura Ventrella,
ORIGINAL ARTICLE Hearing Loss and Changes in Transient Evoked Otoacoustic Emissions After Gamma Knife Radiosurgery for Acoustic Neurinomas Francesco Ottaviani, MD; Cesare Bartolomeo Neglia, MD; Laura Ventrella,
Impact of Gamma Knife Radiosurgery on the neurosurgical management of skull-base lesions: The Combined Approach
 Radiosurgery as part of the neurosurgical armamentarium: Educational Symposium November 24 th 2011 Impact of Gamma Knife Radiosurgery on the neurosurgical management of skull-base lesions: The Combined
Radiosurgery as part of the neurosurgical armamentarium: Educational Symposium November 24 th 2011 Impact of Gamma Knife Radiosurgery on the neurosurgical management of skull-base lesions: The Combined
Selected radiosurgery cases from the Rotating Gamma Institute Debrecen, Hungary
 Selected radiosurgery cases from the Rotating Gamma Institute Debrecen, Hungary László Bognár M.D., Ph.D., József G. Dobai M.D., Gábor Csiky and Imre Fedorcsák M.D., Ph.D. Department of Neurosurgery, Medical
Selected radiosurgery cases from the Rotating Gamma Institute Debrecen, Hungary László Bognár M.D., Ph.D., József G. Dobai M.D., Gábor Csiky and Imre Fedorcsák M.D., Ph.D. Department of Neurosurgery, Medical
Morphological study of the foramen magnum and occipital condyle and its surgical implications in transcondylar approach
 Morphological study of the foramen magnum and occipital condyle and its surgical implications in transcondylar approach Joseph Naiem.S Aziz 1 and Ahmed Khaled Al-Hrabi2 1 Deparment of Anatomy, Faculty
Morphological study of the foramen magnum and occipital condyle and its surgical implications in transcondylar approach Joseph Naiem.S Aziz 1 and Ahmed Khaled Al-Hrabi2 1 Deparment of Anatomy, Faculty
A Brief Introduction to Stacked ABR and Cochlear Hydrops Analysis Masking Procedure (CHAMP)
") A Brief Introduction to Stacked ABR and Cochlear Hydrops Analysis Masking Procedure (CHAMP) Prepared for Bio-logic Systems Corp. by Manuel Don, Ph.D. / Betty Kwong, M.S. Electrophysiology Department House
A Brief Introduction to Stacked ABR and Cochlear Hydrops Analysis Masking Procedure (CHAMP) Prepared for Bio-logic Systems Corp. by Manuel Don, Ph.D. / Betty Kwong, M.S. Electrophysiology Department House
S tereotactic radiosurgery, whether delivered by a gamma
 1536 PAPER Gamma knife stereotactic radiosurgery for unilateral acoustic neuromas J G Rowe, M W R Radatz, L Walton, A Hampshire, S Seaman, A A Kemeny... See end of article for authors affiliations... Correspondence
1536 PAPER Gamma knife stereotactic radiosurgery for unilateral acoustic neuromas J G Rowe, M W R Radatz, L Walton, A Hampshire, S Seaman, A A Kemeny... See end of article for authors affiliations... Correspondence
Postoperative Nerve Injury and Recurrence in Surgical Treatment of Head and Neck Schwannomas
 Postoperative Nerve Injury and Recurrence in Surgical Treatment of Head and Neck Schwannomas SHU-HSIEN CHEN 1, PEI-YIEN TSAI 2, YEN-HUI 3 TSAI * AND CHIH-YING LIN 4 1 Institute of Health Industry Management
Postoperative Nerve Injury and Recurrence in Surgical Treatment of Head and Neck Schwannomas SHU-HSIEN CHEN 1, PEI-YIEN TSAI 2, YEN-HUI 3 TSAI * AND CHIH-YING LIN 4 1 Institute of Health Industry Management
Original Policy Date
 MP 7.01.66 Auditory Brainstem Implant Medical Policy Section Surgery Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013 Return to Medical Policy
MP 7.01.66 Auditory Brainstem Implant Medical Policy Section Surgery Issue 12/2013 Original Policy Date 12/2013 Last Review Status/Date Reviewed with literature search/12/2013 Return to Medical Policy
Letter to the Editor: test occlusion under monitoring of motor-evoked potentials for giant distal
 Letter to the Editor: test occlusion under monitoring of motor-evoked potentials for giant distal anterior cerebral artery aneurysm Acta Neurochirurgica Kampei Shimizu, Shoichi Tani, Hirotoshi Imamura,
Letter to the Editor: test occlusion under monitoring of motor-evoked potentials for giant distal anterior cerebral artery aneurysm Acta Neurochirurgica Kampei Shimizu, Shoichi Tani, Hirotoshi Imamura,
In some patients with pituitary macroadenoma, visual acuity
 ORIGINAL RESEARCH A.M. Tokumaru I. Sakata H. Terada S. Kosuda H. Nawashiro M. Yoshii Optic Nerve Hyperintensity on T2-Weighted Images among Patients with Pituitary Macroadenoma: Correlation with Visual
ORIGINAL RESEARCH A.M. Tokumaru I. Sakata H. Terada S. Kosuda H. Nawashiro M. Yoshii Optic Nerve Hyperintensity on T2-Weighted Images among Patients with Pituitary Macroadenoma: Correlation with Visual
Application of neuronavigation in Neurosurgery at King Hussein Medical Center, Jordan
 Keeping up with technology Application of neuronavigation in Neurosurgery at King Hussein Medical Center, Jordan Abdullah al-akayleh Department of Neuosurgery, King Hussean Medical Center, Jordan. ABSTRACT
Keeping up with technology Application of neuronavigation in Neurosurgery at King Hussein Medical Center, Jordan Abdullah al-akayleh Department of Neuosurgery, King Hussean Medical Center, Jordan. ABSTRACT
57. Trajectory o f Primary Vestibular Fibers Originating f rom the Lateral, Anterior, and Posterior Semicircular Canals in the Cat
 No. 7] Proc. Japan Acad., 58, Ser. B (1982) 237 57. Trajectory o f Primary Vestibular Fibers Originating f rom the Lateral, Anterior, and Posterior Semicircular Canals in the Cat By Haj ime MANNEN, Sei-ichi
No. 7] Proc. Japan Acad., 58, Ser. B (1982) 237 57. Trajectory o f Primary Vestibular Fibers Originating f rom the Lateral, Anterior, and Posterior Semicircular Canals in the Cat By Haj ime MANNEN, Sei-ichi
Ve s t i b u l a r schwannomas are benign tumors that. Sporadic unilateral vestibular schwannoma in the pediatric population.
 J Neurosurg Pediatrics 4:000 000, 4:125 129, 2009 Sporadic unilateral vestibular schwannoma in the pediatric population Clinical article Br i a n P. Wa l c o t t, M.D., 1,2 Ga n e s h Si va r a ja n, B.S.,
J Neurosurg Pediatrics 4:000 000, 4:125 129, 2009 Sporadic unilateral vestibular schwannoma in the pediatric population Clinical article Br i a n P. Wa l c o t t, M.D., 1,2 Ga n e s h Si va r a ja n, B.S.,
Comparison of Growth Patterns of Acoustic Neuromas With and Without Radiosurgery
 Otology & Neurotology 27:705 Y 712 Ó 2006, Otology & Neurotology, Inc. Comparison of Growth Patterns of Acoustic Neuromas With and Without Radiosurgery *Alex Battaglia, Bill Mastrodimos, and *Roberto Cueva
Otology & Neurotology 27:705 Y 712 Ó 2006, Otology & Neurotology, Inc. Comparison of Growth Patterns of Acoustic Neuromas With and Without Radiosurgery *Alex Battaglia, Bill Mastrodimos, and *Roberto Cueva
Antonio De la Cruz, MD 27th Alexandria International Combined ORL Congress Alexandria, Egypt April 8, 2009
 ACOUSTIC NEUROMA TREATMENT OPTIONS 2009 27 th Alexandria International Combined ORL Congress Alexandria, Egypt April 10, 2009 AntonioDelaCruz Cruz, MD House Ear Institute Los Angeles, California Antonio
ACOUSTIC NEUROMA TREATMENT OPTIONS 2009 27 th Alexandria International Combined ORL Congress Alexandria, Egypt April 10, 2009 AntonioDelaCruz Cruz, MD House Ear Institute Los Angeles, California Antonio
DIRECT SURGERY FOR INTRA-AXIAL
 Kitakanto Med. J. (S1) : 23 `28, 1998 23 DIRECT SURGERY FOR INTRA-AXIAL BRAINSTEM LESIONS Kazuhiko Kyoshima, Susumu Oikawa, Shigeaki Kobayashi Department of Neurosurgery, Shinshu University School of Medicine,
Kitakanto Med. J. (S1) : 23 `28, 1998 23 DIRECT SURGERY FOR INTRA-AXIAL BRAINSTEM LESIONS Kazuhiko Kyoshima, Susumu Oikawa, Shigeaki Kobayashi Department of Neurosurgery, Shinshu University School of Medicine,
Acoustic Neuroma (vestibular schwannoma)
") Acoustic Neuroma (vestibular schwannoma) Overview An acoustic neuroma is a tumor that grows from the nerves responsible for balance and hearing. These tumors grow from the sheath covering the vestibulocochlear
Acoustic Neuroma (vestibular schwannoma) Overview An acoustic neuroma is a tumor that grows from the nerves responsible for balance and hearing. These tumors grow from the sheath covering the vestibulocochlear
ORIGINAL ARTICLE. The Cochlear-Carotid Interval: Preoperative Assessment for Cochlear Implant
 ORIGINAL ARTICLE The Cochlear-Carotid Interval: Preoperative Assessment for Cochlear Implant Eshrak Hassanein MD; Eman Geneidi MD; and Mohamed Taha MD From the Departments of Radiology (E.Hassanein), Otorhinolaryngology
ORIGINAL ARTICLE The Cochlear-Carotid Interval: Preoperative Assessment for Cochlear Implant Eshrak Hassanein MD; Eman Geneidi MD; and Mohamed Taha MD From the Departments of Radiology (E.Hassanein), Otorhinolaryngology
Vasoactive treatment for hearing preservation in acoustic neuroma surgery
 J Neurosurg 95:771 777, 2001 Vasoactive treatment for hearing preservation in acoustic neuroma surgery CHRISTIAN STRAUSS, M.D., BARBARA BISCHOFF, CAND.MED., MANDANA NEU, M.D., MICHAEL BERG, PH.D., RUDOLF
J Neurosurg 95:771 777, 2001 Vasoactive treatment for hearing preservation in acoustic neuroma surgery CHRISTIAN STRAUSS, M.D., BARBARA BISCHOFF, CAND.MED., MANDANA NEU, M.D., MICHAEL BERG, PH.D., RUDOLF
DEVELOPMENT OF BRAIN
 Ahmed Fathalla OBJECTIVES At the end of the lecture, students should: List the components of brain stem. Describe the site of brain stem. Describe the relations between components of brain stem & their
Ahmed Fathalla OBJECTIVES At the end of the lecture, students should: List the components of brain stem. Describe the site of brain stem. Describe the relations between components of brain stem & their
Air CT Cisternography in the Diagnosis of Vascular Loop Causing Vestibular Nerve Dysfunction
 1045 Air CT Cisternography in the Diagnosis of Vascular Loop Causing Vestibular Nerve Dysfunction Fraydoon Esfahani 1 2 Kenneth D. Dolan 1 Considerable interest has developed in otology concerning the
1045 Air CT Cisternography in the Diagnosis of Vascular Loop Causing Vestibular Nerve Dysfunction Fraydoon Esfahani 1 2 Kenneth D. Dolan 1 Considerable interest has developed in otology concerning the
Hemorrhagic vestibular schwannoma: an unusual clinical entity Case report
 Neurosurg Focus 5 (3):Article 9, 1998 Hemorrhagic vestibular schwannoma: an unusual clinical entity Case report Dean Chou, M.D., Prakash Sampath, M.D., and Henry Brem, M.D. Departments of Neurological
Neurosurg Focus 5 (3):Article 9, 1998 Hemorrhagic vestibular schwannoma: an unusual clinical entity Case report Dean Chou, M.D., Prakash Sampath, M.D., and Henry Brem, M.D. Departments of Neurological
Year 2003 Paper two: Questions supplied by Tricia
 question 43 A 42-year-old man presents with a two-year history of increasing right facial numbness. He has a history of intermittent unsteadiness, mild hearing loss and vertigo but has otherwise been well.
question 43 A 42-year-old man presents with a two-year history of increasing right facial numbness. He has a history of intermittent unsteadiness, mild hearing loss and vertigo but has otherwise been well.
Clinical features of intracranial vestibular schwannomas
 ONCOLOGY LETTERS 5: 57-62, 2013 Clinical features of intracranial vestibular schwannomas XIANG HUANG *, JIAN XU *, MING XU, LIANG FU ZHOU, RONG ZHANG, LIQIN LANG, QIWU XU, PING ZHONG, MINGYU CHEN, YING
ONCOLOGY LETTERS 5: 57-62, 2013 Clinical features of intracranial vestibular schwannomas XIANG HUANG *, JIAN XU *, MING XU, LIANG FU ZHOU, RONG ZHANG, LIQIN LANG, QIWU XU, PING ZHONG, MINGYU CHEN, YING
ACOUSTIC NEUROMAS. University of Florida ENT Clinic Patrick J. Antonelli, MD Matthew R. O Malley, MD
 ACOUSTIC NEUROMAS University of Florida ENT Clinic Patrick J. Antonelli, MD Matthew R. O Malley, MD Rev. 10.31.2011 ACOUSTIC TUMORS Acoustic tumors are non-malignant fibrous growths, originating from the
ACOUSTIC NEUROMAS University of Florida ENT Clinic Patrick J. Antonelli, MD Matthew R. O Malley, MD Rev. 10.31.2011 ACOUSTIC TUMORS Acoustic tumors are non-malignant fibrous growths, originating from the
Incidence and Risk Factors for Late Neurologic Deterioration after C3-6 Laminoplasty in Patients with Cervical Spondylotic Myelopathy
 Incidence and Risk Factors for Late Neurologic Deterioration after C3-6 Laminoplasty in Patients with Cervical Spondylotic Myelopathy Sakaura H, Miwa T, Kuroda Y, Ohwada T Dept. of Orthop. Surg., Kansai
Incidence and Risk Factors for Late Neurologic Deterioration after C3-6 Laminoplasty in Patients with Cervical Spondylotic Myelopathy Sakaura H, Miwa T, Kuroda Y, Ohwada T Dept. of Orthop. Surg., Kansai
Endoscopic Endonasal Surgery for Subdiaphragmatic Type Craniopharyngiomas
 Original Article doi: 10.2176/nmc.oa.2018-0028 Neurol Med Chir (Tokyo) 58, 260 265, 2018 Endoscopic Endonasal Surgery for Subdiaphragmatic Type Craniopharyngiomas Hiroshi NISHIOKA, 1,2 Yuichi NAGATA, 1
Original Article doi: 10.2176/nmc.oa.2018-0028 Neurol Med Chir (Tokyo) 58, 260 265, 2018 Endoscopic Endonasal Surgery for Subdiaphragmatic Type Craniopharyngiomas Hiroshi NISHIOKA, 1,2 Yuichi NAGATA, 1
External carotid blood supply to acoustic neurinomas
 External carotid blood supply to acoustic neurinomas Report of two cases HARVEY L. LEVINE, M.D., ERNEST J. FERmS, M.D., AND EDWARD L. SPATZ, M.D. Departments of Radiology, Neurology, and Neurosurgery,
External carotid blood supply to acoustic neurinomas Report of two cases HARVEY L. LEVINE, M.D., ERNEST J. FERmS, M.D., AND EDWARD L. SPATZ, M.D. Departments of Radiology, Neurology, and Neurosurgery,
Functional outcome after gamma knife surgery or microsurgery for vestibular schwannomas
 J Neurosurg 97:1091 1100, 2002 Functional outcome after gamma knife surgery or microsurgery for vestibular schwannomas JEAN RÉGIS, M.D., WILLIAM PELLET, M.D., CHRISTINE DELSANTI, M.D., HENRY DUFOUR, M.D.,
J Neurosurg 97:1091 1100, 2002 Functional outcome after gamma knife surgery or microsurgery for vestibular schwannomas JEAN RÉGIS, M.D., WILLIAM PELLET, M.D., CHRISTINE DELSANTI, M.D., HENRY DUFOUR, M.D.,
Inner ear patency after retrosigmoid vestibular schwannoma resection
 Original Article Page 1 of 8 Inner ear patency after retrosigmoid vestibular schwannoma resection Alasdair Grenness 1, Fiona C. E. Hill 2, Shannon Withers 2, Claire Iseli 1,2, Robert Briggs 1,2 1 Department
Original Article Page 1 of 8 Inner ear patency after retrosigmoid vestibular schwannoma resection Alasdair Grenness 1, Fiona C. E. Hill 2, Shannon Withers 2, Claire Iseli 1,2, Robert Briggs 1,2 1 Department
Surgical anatomy of the juxta dural ring area
 J Neurosurg 89:250 254, 1998 Surgical anatomy of the juxta dural ring area SUSUMU OIKAWA, M.D., KAZUHIKO KYOSHIMA, M.D., AND SHIGEAKI KOBAYASHI, M.D. Department of Neurosurgery, Shinshu University School
J Neurosurg 89:250 254, 1998 Surgical anatomy of the juxta dural ring area SUSUMU OIKAWA, M.D., KAZUHIKO KYOSHIMA, M.D., AND SHIGEAKI KOBAYASHI, M.D. Department of Neurosurgery, Shinshu University School
INNOVATIVE PERSPECTIVES IN ACOUSTIC NEUROMA SURGERY. VERONA, Italy APRIl 2018 INTERNATIONAL MEETING. program. Hands on and Live Surgery
 Azienda Ospedaliera Universitaria Integrata Verona Scuola triveneta di discipline Otorinolaringoiatriche program INTERNATIONAL MEETING INNOVATIVE PERSPECTIVES IN ACOUSTIC NEUROMA SURGERY Hands on and Live
Azienda Ospedaliera Universitaria Integrata Verona Scuola triveneta di discipline Otorinolaringoiatriche program INTERNATIONAL MEETING INNOVATIVE PERSPECTIVES IN ACOUSTIC NEUROMA SURGERY Hands on and Live
Considerations 3/9/2018. Asheesh Bedi, MD. I have no disclosures or conflicts of interest related to the content of this presentation.
 Radiological Assessment of the Rotator Cuff What predicts outcomes? Asheesh Bedi, MD Harold and Helen W. Gehring Professor Chief, Sports Medicine & Shoulder Surgery MedSport, Department of Orthopedic Surgery
Radiological Assessment of the Rotator Cuff What predicts outcomes? Asheesh Bedi, MD Harold and Helen W. Gehring Professor Chief, Sports Medicine & Shoulder Surgery MedSport, Department of Orthopedic Surgery