Proton Therapy for Ependymoma and Craniopharyngioma at the University of Florida: Lessons Learned About Efficacy and Toxicity
|
|
|
- Polly Atkins
- 5 years ago
- Views:
Transcription

1 Proton Therapy for Ependymoma and Craniopharyngioma at the University of Florida: Lessons Learned About Efficacy and Toxicity Danny Indelicato, MD Mendenhall Chair of Pediatric Radiotherapy University of Florida
2 Disclosure I will not be discussing any specific pharmaceutical or hardware company
3 Lesson #1 Proton therapy is broadly accepted and widely utilized in the treatment of ependymoma and craniopharyngioma in the United States and Europe



4 Participants responses to the question: What is the treatment of choice for the following pediatric tumors? Participants could answer proton therapy, photon therapy, or both, depending on circumstances. 2016
5 2016 Worldwide Proton Therapy Delivery Top 10 diagnoses (75% of patients) All countries USA EUR ASIA Rhabdomyosarcoma 244 (13.4) 162 (13.4) 52 (12.0) 30 (16.8) Medulloblastoma 230 (12.7) 149 (12.4) 59 (13.7) 22 (12.3) Ependymoma 205 (11.3) 131 (10.9) 62 (14.4) 12 (6.7) Low-grade glioma 129 (7.1) 93 (7.7) 25 (5.8) 11 (6.1) Ewing sarcoma 125 (6.9) 91 (7.6) 27 (6.3) 7 (3.9) Neuroblastoma 103 (5.7) 57 (4.7) 13 (3.0) 33 (18.4) Craniopharyngioma 100 (5.5) 61 (5.1) 34 (7.9) 5 (2.8) Intracranial pure germinoma 86 (4.7) 52 (4.3) 19 (4.4) 15 (8.4) Hodgkin lymphoma 80 (4.4) 77 (6.4) 1 (0.2) 2 (1.1) Other bone/soft tissues sarcoma 73 (4.0) 46 (3.8) 23 (5.3) 4 (2.2) Journy N, Indelicato DJ, Klinerman R, Withrow D, de Gonzalez

6 children treated at UF since Over 200 ependymomas and craniopharyngiomas
 or ependymoma (13) proton radiation outcome : 23 craniopharyngioma (4) or ependymoma (4) IMRT radiation : 8 Both the largest series describing the outcome of radiotherapy for pediatric")
7 Pubmed accessed on August 30, 2018 Articles involving craniopharyngioma (42) or ependymoma (67) proton radiation : 109 craniopharyngioma (14) or ependymoma (18) IMRT radiation : 32 craniopharyngioma (10) or ependymoma (13) proton radiation outcome : 23 craniopharyngioma (4) or ependymoma (4) IMRT radiation : 8 Both the largest series describing the outcome of radiotherapy for pediatric ependymomas and craniopharyngiomas were carried out with protons


8 Lesson #2 In ependymoma, proton therapy and limited CTV margins reduce the radiation dose to developing neural tissue without compromising disease control Proton plan IMRT plan
9 Patient Characteristics 179 pediatric patients with non-metastatic intracranial ependymoma treated between on prospective outcome study 98 patients (55%) were 3 years old 103 patients (58%) were male 119 patients (65%) had posterior fossa tumors 120 patients (67%) had grade 3 tumors
10 Pre-radiation treatment 152 patients (85%) had total or near total resection prior to RT 48 patients (27%) required more than 1 resection 59 patients (33%) received pre-rt chemotherapy 36 patients (20%) with methotrexate-based regimen Median duration between definitive surgery and radiation was 55 days in patients who did not receive chemotherapy

11 University of Florida Ependymoma Treatment Guidelines GTV = Tumor bed and any residual disease



12 University of Florida Ependymoma Treatment Guidelines GTV = Tumor bed and any residual disease CTV1 = GTV + 5 mm

13 University of Florida Ependymoma Treatment Guidelines GTV = Tumor bed and any residual disease CTV1 = GTV + 5 mm PTV1 = CTV1 + 3 mm


14 University of Florida Ependymoma Treatment Guidelines GTV = Tumor bed and any residual disease CTV1 = GTV + 5 mm PTV1 = CTV1 + 3 mm CTV2 = GTV


15 University of Florida Ependymoma Treatment Guidelines GTV = Tumor bed and any residual disease CTV1 = GTV + 5 mm PTV1 = CTV1 + 3 mm CTV2 = GTV PTV2 = CTV2 + 3 mm

16 Prescription Dose University of Florida Ependymoma Treatment Guidelines * If 3 y/o with a gross total resection, no PTV2 boost PTV2 = 59.4 Gy PTV1 = 54 Gy
17
18 100 Median follow-up: 3.2 years Patients lost to follow-up: 2 Freedom from event (%) Overall survival (3 yr: 90.4%) Local control (3 yr: 85.4%) Progression-free survival (3 yr: 75.9%) Years
19 Literature Review: Pediatric Ependymoma Group Author (year) N 3 yr LC 3 yr PFS 3 yr OS Current Study Indelicato (2017) % 76% 90% Historic UF Swanson (2011) 25 31%* 25%* 35%* *10 year
20 Literature Review: Pediatric Ependymoma Group Author (year) N 3 yr LC 3 yr PFS 3 yr OS Current Study Indelicato (2017) % 76% 90% Historic UF Swanson (2011) 25 31% 25% 35% CHOP Kuo (2007) 49 NR 41%* 66%* WashU** Mansur (2005) 40 NR 58%* 71%* Taiwan Jiang (2004) 31 NR 52%* 58%* Iowa Paulino (2002) 28 65%* NR 86%* Kyoto** Oya (2002) 48 NR 42%* 62%* Rotterdam Van Veelen-Vincent (2002) 44 NR 64%* 80%* ** includes adult patients * 5 year
21 Literature Review: Pediatric Ependymoma Group Author (year) N 3 yr LC 3 yr PFS 3 yr OS Current Study Indelicato (2017) % 76% 90% Historic UF Swanson (2011) 25 31%* 25%* 35%* CHOP Kuo (2007) 49 NR 41%* 66%* WashU** Mansur (2005) 40 NR 58%* 71%* Taiwan Jiang (2004) 31 NR 52%* 58%* Iowa Paulino (2002) 28 65%* NR 86%* Kyoto** Oya (2002) 48 NR 42%* 62%* Rotterdam Van Veelen-Vincent (2002) 44 NR 64%* 80%* Historic Average Various % 25-64% 35-86% ** includes adult patients * 5 year
22 Literature Review: Pediatric Ependymoma Group Author (year) N 3 yr LC 3 yr PFS 3 yr OS Current Study Indelicato (2017) % 76% 90% Historic Average Various % 25-64% 35-86% St Jude Merchant (2007) %** 69%** 81%** ** 7 year
23 Literature Review: Pediatric Ependymoma Group Author (year) N 3 yr LC 3 yr PFS 3 yr OS Current Study Indelicato (2017) % 76% 90% Historic Average Various % 25-64% 35-86% St Jude Merchant (2007) % 69% 81% PSI Ares (2016) 50 86% NR 88% MGH MacDonald (2013) 70 83% 76% 95%
24 Literature Review: Pediatric Ependymoma Group Author (year) N 3 yr LC 3 yr PFS 3 yr OS Current Study Indelicato (2017) % 76% 90% Historic Average Various % 25-64% 35-86% St Jude Merchant (2007) % 69% 81% PSI Ares (2016) 50 86% NR 88% MGH MacDonald (2013) 70 83% 76% 95% AIEOP Massimino (2016) %* 65%* 81%* French Child s Cancer Society Ducassou (2015) % 53-62% 77-86% CCG/COG Garvin (2012) 84 NR 57%* 71%* * 5 year

25 Lesson #3 Treatment technique and risk factors impact ependymoma control these are applicable beyond particle therapy
26 Variable Age at RT Age at first surgery Gender Grade Recurrent prior to RT Race Chemotherapy prior to RT GTR/NTR at time of radiation 3 Year Disease Control Estimates on Univariate Analysis N Local Control (%) P= Progression- Free Survival (%) P= Overall Survival (%) % 77% 91% > % 74% 90% % > % 78% 72% 90% 91% Female 76 92% 87% 99% <0.05 Male % 67% 84% % 81% 90% % 73% 91% Yes 18 93% 84% 100% No % 75% 89% White/Asian % 78% 92% Black/Hispanic 26 80% 64% 81% Yes 59 87% 75% 87% No % 76% 92% Yes % 79% 93% <0.01 <0.05 No 27 67% 59% 77% P= <0.01 <0.05
27 Variable Age at RT Age at first surgery Gender Grade Recurrent prior to RT Race Chemotherapy prior to RT GTR/NTR at time of radiation 3 Year Disease Control Estimates on Univariate Analysis N Local Control (%) P= Progression- Free Survival (%) P= Overall Survival (%) % 77% 91% > % 74% 90% % > % 78% 72% 90% 91% Female 76 92% 87% 99% <0.05 Male % 67% 84% % 81% 90% % 73% 91% Yes 18 93% 84% 100% No % 75% 89% White/Asian % 78% 92% Black/Hispanic 26 80% 64% 81% Yes 59 87% 75% 87% No % 76% 92% Yes % 79% 93% <0.01 <0.05 No 27 67% 59% 77% P= <0.01 <0.05
28 Variable Age at RT Age at first surgery Gender Grade Recurrent prior to RT Race Chemotherapy prior to RT GTR/NTR at time of radiation 3 Year Disease Control Estimates on Univariate Analysis N Local Control (%) P= Progression- Free Survival (%) P= Overall Survival (%) % 77% 91% > % 74% 90% % > % 78% 72% 90% 91% Female 76 92% 87% 99% <0.05 Male % 67% 84% % 81% 90% % 73% 91% Yes 18 93% 84% 100% No % 75% 89% White/Asian % 78% 92% Black/Hispanic 26 80% 64% 81% Yes 59 87% 75% 87% No % 76% 92% Yes % 79% 93% <0.01 <0.05 No 27 67% 59% 77% P= <0.01 <0.05
29 Variable Age at RT Age at first surgery Gender Grade Recurrent prior to RT Race Chemotherapy prior to RT GTR/NTR at time of radiation 3 Year Disease Control Estimates on Univariate Analysis N Local Control (%) P= Progression- Free Survival (%) P= Overall Survival (%) % 77% 91% > % 74% 90% % > % 78% 72% 90% 91% Female 76 92% 87% 99% <0.05 Male % 67% 84% % 81% 90% % 73% 91% Yes 18 93% 84% 100% No % 75% 89% White/Asian % 78% 92% Black/Hispanic 26 80% 64% 81% Yes 59 87% 75% 87% No % 76% 92% Yes % 79% 93% <0.01 <0.05 No 27 67% 59% 77% P= <0.01 <0.05
30 Variable 3 Year Disease Control Estimates on Univariate Analysis N Local Control (%) P= Progression- Free Survival (%) P= Overall Survival (%) P= Location Posterior fossa % 72.0% 86.5% Supratentorial % 83.4% 98.2% Duration between last surgery and start of RT* 56 days 63 84% >56 days 57 85% 73% 95% 79% 90% Total Dose Total Dose in patients who had GTR/NTR Total Dose in patients who had STR 54 Gy 70 89% 78% 94% >55.8 Gy % 74% 88% 54 Gy 60 91% 80% 97% >55.8 Gy 92 87% 77% 90% 54 Gy 10 76% 65% 76% >55.8 Gy 17 61% 56% 78% * Non-chemo patients
31 Variable 3 Year Disease Control Estimates on Univariate Analysis N Local Control (%) P= Progression- Free Survival (%) P= Overall Survival (%) P= Location Posterior fossa % 72.0% 86.5% Supratentorial % 83.4% 98.2% Duration between last surgery and start of RT* 56 days 63 84% >56 days 57 85% 73% 95% 79% 90% Total Dose Total Dose in patients who had GTR/NTR Total Dose in patients who had STR 54 Gy 70 89% 78% 94% >55.8 Gy % 74% 88% 54 Gy 60 91% 80% 97% >55.8 Gy 92 87% 77% 90% 54 Gy 10 76% 65% 76% >55.8 Gy 17 61% 56% 78% * Non-chemo patients
32 Variable 3 Year Disease Control Estimates on Univariate Analysis N Local Control (%) P= Progression- Free Survival (%) P= Overall Survival (%) P= Location Posterior fossa % 72.0% 86.5% Supratentorial % 83.4% 98.2% Duration between last surgery and start of RT* 56 days 63 84% >56 days 57 85% 73% 95% 79% 90% Total Dose Total Dose in patients who had GTR/NTR Total Dose in patients who had STR 54 Gy 70 89% 78% 94% >55.8 Gy % 74% 88% 54 Gy 60 91% 80% 97% >55.8 Gy 92 87% 77% 90% 54 Gy 10 76% 65% 76% >55.8 Gy 17 61% 56% 78% * Non-chemo patients
33 Variable Location Duration between last surgery and start of RT* Total Dose Total Dose in patients who had GTR/NTR Total Dose in patients who had STR 3 Year Disease Control Estimates on Univariate Analysis Local Progression- Overall N Control P= Free Survival P= Survival (%) (%) (%) Posterior fossa % 72.0% 86.5% Supratentorial % 83.4% 98.2% 56 days 63 84% >56 days 57 85% 73% 95% 79% 90% 54 Gy 70 89% 78% 94% >55.8 Gy % 74% 88% 54 Gy 60 91% 80% 97% >55.8 Gy 92 87% 77% 90% 54 Gy 10 76% 65% 76% >55.8 Gy 17 61% 56% 78% P= On multivariate analysis, extent of resection maintained significance for improved local control and disease free survival, with borderline association with overall survival (p = 0.057) female gender maintained significance for better overall survival
34 SJYC07 Multi-institutional trial using riskadapted therapy to treat children <3 years old with malignant brain tumors including ependymoma Sought, for the first time, a prospective validation of retrospective data on the impact of molecular subgroup on outcomes in ependymoma ASCO 2018, Upadhyaya et al
35 Schema Maximum safe surgical resection Induction chemotherapy MTX/VCR/CTX/cisplatin Residual disease + second-look surgery 54 Gy radiation (CTV = 5 mm) 6 cycles of oral maintenance chemotherapy with cyclophosphamide, topotecan alternating with erlotibib
36 Patients Between 2008 and 2016, 54 children with ependymoma (median age, 1.6 years; range, ) All M0 based on imaging DNA methylation-based tumor subgroups: PF-A: 42 (78%) ST-RELA: 8 (15%) ST-YAP: 4 (7%) Similar patient age, tumor grade, and extent of resection across subgroups Median follow-up: 3.6 years
37 PFS and OS of Entire Cohort PFS by Subgroups 91% OS at 4 years Recurrence was distant (n = 7), local (n = 6), or combined (n = 1) p = 0.4 PFS by Extent of Resection PFS for PF-A with and without 1q gain p < 0.05 p = 0.15
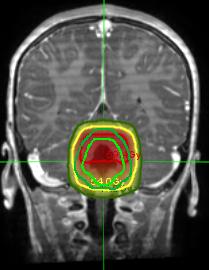
38 Lesson #4 In craniopharyngioma, proton therapy with limited CTV margins reduces the radiation dose to developing neural tissue without compromising disease control Proton plan IMRT plan

39 University of Florida Craniopharyngioma Treatment Guidelines GTV = Gross disease
40 University of Florida Craniopharyngioma Treatment Guidelines GTV = Gross disease CTV = GTV + 5 mm, encompassing ventricle surfaces in contact with cyst



41 University of Florida Craniopharyngioma Treatment Guidelines GTV = Gross disease CTV = GTV + 5 mm, encompassing ventricle surfaces in contact with cyst PTV = CTV + 3 mm
42 University of Florida Craniopharyngioma Treatment Guidelines Prescription Dose PTV = 54 Gy

43
44 RT2CR Phase II trial for children with craniopharyngioma treated with proton therapy using 5 mm CTV Comparison cohort Phase II trial of conformal or intensity-modulated photon therapy using 5 mm CTV margin Trial Modality Patients Dose CTV Margin RT2CR Proton Gy 5 mm RT1 Photon Gy 5 mm PI: T. Merchant
45 RT2CR Treatment at the University of Florida Follow-up testing at St. Jude Imaging Time Points Year 1 every 3 months Year 2 every 6 months Year 3 every 6 months Year 4 every 6 months Year 5 every 6 months Evaluations/Schedule Protocol-based Assessments Months after RT Start Imaging Diagnostic MR X X X X X X X X X X X X X Investigational MR X X X X PET-FDG X X X PET-methionine X X X Clinical-Standard Assessment/Triage X X X X X X X X X X X X X Lab: CBC X X X X X X X X X X X X X Lab: Chemistry X X X X X X X X X X X X X Lab: Endocrine Screen X X X X X X X X X X X X X Audiometry X X X X X X Endocrine Clinic X X X X X X Neurology Clinic X X X Ophthalmology X X X X X X Physical Exam X X X X X X X X X X X X X Clinical-Investigational Endocrine/Provocative X X X Sleep/Fatigue Research Questionnaires X X X X X X X X X X X X X Actigraphy X X X X X X Melatonin/Core Temp X X X X X X Function Laboratory X X X X X X X Sleep Evaluation X X X Psychology X X X X X X Questionnaires/QOL X X X X X X Laboratory- Investigational Genomics X X Cytokines X X X X X X X

46 Merchant et al, ASTRO 2017 Comparative Results Progression-Free Survival Probability Months Since Initiation of Irradiation RT1 RT2CR Proton cohort median follow-up 36.5 months (range months)
47 Merchant et al, ASTRO 2017 Comparative Results Overall Survival Probability Months Since Initiation of Irradiation RT1 RT2CR
48 Merchant et al, SIOP 2017 Academic Achievement Scores: Proton vs Photon Reading Scores Math Scores Baseline 36 months 92 Baseline 36 months Proton Photon Proton Photon p= p=0.0263
49 Conclusions Progression-free survival estimates for proton therapy were comparable to those reported for children treated using photons Cognitive testing results from two prospective trials comparing proton and photon cohorts showed preservation of academic achievement for those treated with proton therapy compared to conformal radiation therapy using photons Final analysis will be performed 3 years after the last patient has been treated (early 2019)
50 Lesson #5 Treatment technique and risk factors impact craniopharyngioma tumor control these are applicable beyond particle therapy


51 University of Florida Craniopharyngioma Treatment Guidelines GTV = Gross disease CTV1 = GTV + 5 mm, encompassing ventricle surfaces in contact with cyst PTV1 = CTV1 + 3 mm CTV2 = GTV


52 University of Florida Craniopharyngioma Treatment Guidelines GTV = Gross disease CTV1 = GTV + 5 mm, encompassing ventricle surfaces in contact with cyst PTV1 = CTV1 + 3 mm CTV2 = GTV PTV1 = CTV2 + 3 mm
53 University of Florida Craniopharyngioma Treatment Guidelines Prescription Dose PTV1 = 45 Gy PTV2 = 54 Gy







54 Active Cyst Monitoring Week 2: GTV (red) Week 3: Cyst drained via ommaya Week 4: Cyst reaccumulating Week 5: Cyst needs repeat drainage Of the 94 children on RT2CR, we observed cyst expansion required replanning (n=8), drainage (n=4), or both (n=2)


55 Additional Research
56 Lesson #6 Proton therapy is not associated with unexpected toxicity ependymoma and craniopharyngioma



57 Brainstem Tolerance in Pediatric Radiotherapy




58 Murmurs Among the Zealots

59 Fooled by Randomness? No matter how sophisticated the person, abstract statistical information does not sway us as much as the anecdote. - Nassim Talib
60 Symptomatic brainstem toxicity in ependymoma patients Photon series Rate % Merchant (Lancet 2009) 3/ % Sato (Cancer 2017) 3/38 7.9% Nanda (IJROBP 2017) 5/ % Total 11/ %
61 Symptomatic brainstem toxicity in ependymoma patients Photon series Rate % Merchant (Lancet 2009) 3/ % Sato (Cancer 2017) 3/38 7.9% Nanda (IJROBP 2017) 5/ % Total 11/ % Proton series MacDonald (Neurooncology 2013) Ares (Journal of Neurooncology 2016) 0/70 0 1/50 2% Sato (Cancer 2017) 3/41 7.3% Indelicato (Acta Oncologica 2017) 10/ % Total 14/ %
62 Limitations to current literature 1. Era bias related to imaging technology - Progression vs toxicity 2. Inconsistent toxicity classification and grading - CTCAE is ambiguous and non-specific 3. Existing data sets are disease-specific and include non-relevant patients - Ex: supratentorial ependymomas, S-PNETs 4. Studies report nominal prescribed dose, not brainstem dose 5. Inconsistent/crude definition of brainstem OAR 6. Rare events preclude robust multivariate analyses
63 Potential Risk Factors for Pediatric Patients Dose to brainstem Gender Tumor size Co-morbidity Extent of resection Surgical toxicity Systemic therapy Age Race Target volume Hydrocephalus Number of operations CSF shunting Interval to radiation







64
65 Brainstem necrosis was defined by new or progressive symptoms following radiation involving motor weakness or cranial nerve V-VII or IX-XII corresponding radiographic abnormality within the brainstem in the absence of local disease progression Inclusion criteria: Patients 21 years old with a posterior fossa tumor Exclusion criteria: Intrinsic brainstem tumors (eg. brainstem glioma) Prior radiation to the brain or skull base Photon therapy component >5% Non-standard fractionation (not 1.8 Gy/fx) Less than 6 weeks of followup from the completion of radiation Absence of follow-up MRI
66 Grading Scale Global Characterization Brainstem Symptoms Cranial Nerve Deficits Grade 2 Grade 3 Grade 4 Grade 5 Life-threatening; inability to perform basic age-appropriate self-care functions Minor; interferes to some extent with patient's usual functioning Minor loss of strength Minor deficit Major; incapacitating, significantly interferes with patient's usual functioning Major loss of strength requiring functional aid Moderate deficit Complete paralysis, respiratory failure Complete loss of function in multiple cranial nerves Intervention HBO; steroids Multiagent Prolonged inpatient management of vital function Death
67 Reported Proton Outcomes Median f/u Total Patients With Necrosis Overall Rate %
68 Reported Proton Outcomes Median f/u Total Patients With Necrosis Overall Rate Grade % 1.3%

69 Reported Proton Outcomes Median f/u Total Patients With Necrosis Overall Rate Grade 3+ Grade % 1.3% 0.4%
70 Reported Photon Outcomes Total Patients With Necrosis Overall Rate Grade 3+ Grade % 1.3% 0.4% % 3.3% 1.7%
71 Dose Specifics With brainstem necrosis Without brainstem necrosis Prescription Dose (Gy) Brainstem (Gy) D50% D10% Max (0.1 cc) Proton Photon Proton Photon
 D50% D10% Max (0.1 cc) 55.7 54.7 56.8 58.0 54.6 51.")
72 Dose Specifics With brainstem necrosis Without brainstem necrosis Brainstem (Gy) Prescription Dose (Gy) D50% D10% Max (0.1 cc)
73 119 pediatric patients with non-metastatic posterior fossa ependymoma treated between June February 2017 University of Florida Ependymoma Treatment Guidelines CTV1 CTV1 Dose CTV2 CTV2 Dose GTV + 5 mm 54 Gy GTV 59.4 Gy* * If 3 y/o with a GTR/NTR, no CTV2 boost In cohort of 119 subjects, Median radiation dose in children 3 years old: 54 Gy 93% of children over 3 years old received 59.4 Gy
74 Goal Dose: D50% 61 Gy D10% 63 Gy D90% 44 Gy University of Florida Brainstem Dose Constraints Before October 1, 2013 Per Children s Oncology Group AC0831 Max Dose: D50% 62 Gy D10% 64 Gy D90% 59 Gy

75 Goal Dose: D50% <52.4 Gy D10% <55.4 Gy 0.1cc Max <56.6 Gy University of Florida Brainstem Dose Constraints After October 1, 2013 Per Indelicato et al, 2014 No plan should exceed any Max Dose metric No plan should exceed more than 1 Goal Dose metric Max Dose: D50% <54 Gy D10% <56 Gy 0.1cc Max <58 Gy Exception: Plans for kids <5 y/o should not exceed any Goal Dose metric Brainstem (Gy) With brainstem necrosis Without brainstem necrosis D50% D10% Max (0.1 cc)
76 Freedom from grade 2+ necrosis (%) Median follow-up: 3.1 years overall 4.4 years in 63 patients treated before October 1, years in 56 patients treated after October 1, 2013 Treated prior to October 1, 2013 (1.5 yr: 87%) Treated after October 1, 2013 (1.5 yr: 100%) * Significantly more patients in the pre-2013 cohort received chemotherapy before radiation Years
77 University of Florida Brainstem Dose Constraints After October 1, 2013 Goal Dose: D50% <52.4 Gy D10% <55.4 Gy 0.1cc Max <56.6 Gy Max Dose: D50% <54 Gy D10% <56 Gy 0.1cc Max <58 Gy No plan should exceed any Max Dose metric No plan should exceed more than 1 Goal Dose metric Exception: Plans for kids <5 y/o should not exceed any Goal Dose metric
78 100 Local control (%) Treated prior to October 1, 2013 (1.5 yr: 93.6%) Treated after October 1, 2013 (1.5 yr: 92.4%) p= Years
79 Conclusions Modern radiotherapy techniques result in a 0-10% risk of brainstem toxicity Need more data on interplay of dose and clinical factors UF Brainstem Guidelines offer a starting point for double-scattered proton therapy and IMRT


80 Vasculopathy Following Cranial Radiation


81 2007 Reviewed 345 survivors of cranial radiation Median f/u 54 months Risk factors for moyamoya: Dose to the optic chiasm NF-1 Younger age Optic pathway tumors
 Risk factors for stroke: 1. Increased dose to the Circle of Willis 2.")
82 2017 2,202 French survivors of childhood cancer (treated ) Dosimetry to Circle of Willis estimated using phantom reconstruction in scalable phantoms Median f/u: 26 years 54 pts found to have a stroke (72% ischemic) Risk factors for stroke: 1. Increased dose to the Circle of Willis 2. Male gender (for ischemic stroke)

83 El-Fayech et al, 2017

84 15 July 2018 Objectives: To estimate the rate of vasculopathy following proton therapy in pediatric patients with C/Skull Base tumors To identify risk factors for developing vasculopathy
85 Methods pediatric patients treated with proton therapy for C/skull base tumors at UF All enrolled on prospective outcomes tracking study Recommend imaging: MRI q3-4 months for 3 years, q6 months for 5 years, then annually MRA every 1-2 years for sellar/suprasellar, brainstem, and skull base tumors
86 Methods Endpoints: Vasculopathy Any asymptomatic vessel narrowing identified by imaging, transient ischemic attacks (TIAs), and cerebrovascular accidents (CVAs) Serious Vasculopathy Events resulting in permanent neurological complications or requiring revascularization surgery
87 Methods Multivariate logistic regression used to identify factors associated with toxicity Variables Age, NF, extent of surgical resection, history of postoperative stroke, chemotherapy, total prescribed dose, and dose to the optic chiasm, optic nerves, and hypothalamus Median follow-up: 3.0 years ( )
88 Patient Characteristics Median Age [Range] 7.6 years [ ] Median Prescribed Dose [Range] 54 Gy RBE [ ] Sex Male 357 (55%) Female 294 (45%) Histology Craniopharyngioma 140 (22%) Ependymoma 135 (21%) Low-grade glioma 132 (20%) Medulloblastoma/PNET 80 (12%) Ewing/RMS/NRSTS 74 (11%) Other 90 (14%) Extent of Surgical Resection GTR/NTR 251 (39%) STR/Biopsy 370 (57%) None 30 (4%) Tumor Location Sellar/Suprasellar 276 (42%) Thalamic/Basal Ganglia 70 (11%) Hemispheric/Lateral Venticles 127 (20%) Posterior Fossa 178 (27%)
89 100 Freedom from event (%) year risk of any vasculopathy = 6.4% 3 year risk of serious vasculopathy = 2.6% Years
90 Results Multivariate Analysis Asymptomatic Events Thirty patients developed asymptomatic vessel narrowing on imaging during the study period Serious Events Seven patients (1.2%) developed CVA with permanent neurological deficits (CTCAE Grade 4 toxicity) Four patients had revascularization surgery Any Vasculopathy Factor 3-yr Rate Age <5 y.o. Dmax Optic Chiasm ( 54 CGE) 8.4% vs. 5.4% (p<0.01) 13.1% vs. 2.2% (p<0.001)
91 Results Multivariate Analysis Asymptomatic Events Thirty patients developed asymptomatic vessel narrowing on imaging during the study period Serious Events Seven patients (1.2%) developed CVA with permanent neurological deficits (CTCAE Grade 4 toxicity) Four patients had revascularization surgery Any Vasculopathy Serious Vasculopathy Factor 3-yr Rate 3-yr Rate Age <5 y.o. 8.4% vs. 5.4% (p<0.01) Dmax Optic Chiasm ( 54 CGE) 13.1% vs. 2.2% (p<0.001) 3.8% vs. 1.7% (p<0.05) Gender, tumor histology, tumor location, chemotherapy, extent of surgery, and co-morbidities were not associated with increased risk
92 Conclusions Childhood cancer survivors are at high risk for radiation-related vasculopathy Young children and those receiving 54 Gy to the optic chiasm were at highest risk Incidence of serious vasculopathy following proton therapy similar to historical photon data
93 Comparative Toxicity on RT2CR Trial Modality Patients Dose CTV Margin RT2CR Proton Gy 5 mm RT1 Photon Gy 5 mm Median age of craniopharyngioma patients Photon cohort: 9 years Proton cohort: 9.4 years Severe complications after irradiation were defined as: brain or brainstem necrosis clinically significant vasculopathy resulting in permanent neurological complications or requiring revascularization surgery permanent neurological deficits not related to necrosis or vasculopathy
94 Comparative Toxicity on RT2CR The cumulative incidence of severe complications were similar to those observed in patients treated using photon therapy Merchant et al, ASTRO 2016
95 Lesson #7: Recommendations for limiting toxicity Regardless of radiation modality, If goal is to keep brainstem toxicity <5%, apply UF brainstem dosimetric guidelines based on age and extent of resection If estimated dose the Circle of Willis is >10 Gy, obtain baseline MRA and integrate with followup imaging * * This position does not encompass pencil beam proton therapy


96 Thank you Acknowledgements Tom Merchant Santosh Upadhyaya Julie Bradley Ronny Rotondo Matt Hall
Effectiveness and Safety of Spot Scanning Proton Radiation Therapy for Skull Base Tumors: First Long Term Report of the PSI Experience
 Effectiveness and Safety of Spot Scanning Proton Radiation Therapy for Skull Base Tumors: First Long Term Report of the PSI Experience Carmen Ares, Antony J Lomax, Eugen B Hug, Alessandra Bolsi, Beate
Effectiveness and Safety of Spot Scanning Proton Radiation Therapy for Skull Base Tumors: First Long Term Report of the PSI Experience Carmen Ares, Antony J Lomax, Eugen B Hug, Alessandra Bolsi, Beate
State of the Art Radiotherapy for Pediatric Tumors. Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center
 State of the Art Radiotherapy for Pediatric Tumors Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center Introduction Progress and success in pediatric oncology Examples of low-tech and high-tech
State of the Art Radiotherapy for Pediatric Tumors Suzanne L. Wolden, MD Memorial Sloan-Kettering Cancer Center Introduction Progress and success in pediatric oncology Examples of low-tech and high-tech
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) BONE (Version , 03/28/18)
 BONE (Version , 03/28/18)") BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
BONE (Version 2.2018, 03/28/18) NCCN GUIDELINES ON PROTON THERAPY (AS OF 4/23/18) Radiation Therapy Specialized techniques such as intensity-modulated RT (IMRT); particle beam RT with protons, carbon ions,
11/27/2017. Proton Therapy for Brain Tumors: Hope or Hype? Financial Disclosures. Objectives. None
 Proton Therapy for Brain Tumors: Hope or Hype? 1 Financial Disclosures None 2 Objectives Discuss the rationale and evidence for proton therapy in children and adults Discuss the late effects that can be
Proton Therapy for Brain Tumors: Hope or Hype? 1 Financial Disclosures None 2 Objectives Discuss the rationale and evidence for proton therapy in children and adults Discuss the late effects that can be
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES
 DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
Exploring the potential for clinical introduction of hippocampal-sparing IMPT of pediatric medulloblastoma - Past present and future
 Exploring the potential for clinical introduction of hippocampal-sparing IMPT of pediatric medulloblastoma - Past present and future Daniel Gasic Disclosure Nothing to disclose Introduction Background
Exploring the potential for clinical introduction of hippocampal-sparing IMPT of pediatric medulloblastoma - Past present and future Daniel Gasic Disclosure Nothing to disclose Introduction Background
Sacral Chordoma: The Loma Linda University Radiation Medicine Experience. Kevin Yiee MD, MPH Resident Physician
 Sacral Chordoma: The Loma Linda University Radiation Medicine Experience Kevin Yiee MD, MPH Resident Physician What is a chordoma? 1 st chordoma discovered in clivus by Virchow and Luschka 1856 Rare tumor
Sacral Chordoma: The Loma Linda University Radiation Medicine Experience Kevin Yiee MD, MPH Resident Physician What is a chordoma? 1 st chordoma discovered in clivus by Virchow and Luschka 1856 Rare tumor
THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA. TIMUR MITIN, MD, PhD
 THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA TIMUR MITIN, MD, PhD RESECTABLE DISEASE MANAGEMENT: RESECTABLE DISEASE Resection offers the only possibility of long term survival
THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA TIMUR MITIN, MD, PhD RESECTABLE DISEASE MANAGEMENT: RESECTABLE DISEASE Resection offers the only possibility of long term survival
Protons for Head and Neck Cancer. William M Mendenhall, M.D.
 Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
Protons for Head and Neck Cancer William M Mendenhall, M.D. Protons for Head and Neck Cancer Potential Advantages: Reduce late complications via more conformal dose distributions Likely to be the major
Carbon Ion Radiotherapy for Skull Base and Paracervical Chordomas
 Carbon Ion Radiotherapy for Skull Base and Paracervical Chordomas Azusa Hasegawa, Jun-etsu Mizoe and Hirohiko Tsujii Research Center Hospital for Charged Particle Therapy National Institute of Radiological
Carbon Ion Radiotherapy for Skull Base and Paracervical Chordomas Azusa Hasegawa, Jun-etsu Mizoe and Hirohiko Tsujii Research Center Hospital for Charged Particle Therapy National Institute of Radiological
-Proton Beam Therapy in Paediatric Radiation Oncology -
 -Proton Beam Therapy in Paediatric Radiation Oncology - Beate Timmermann, M.D. West German Proton Therapy Centre Essen Germany Preview Survival Toxicity Why protons? (theoretically) Experiences so far
-Proton Beam Therapy in Paediatric Radiation Oncology - Beate Timmermann, M.D. West German Proton Therapy Centre Essen Germany Preview Survival Toxicity Why protons? (theoretically) Experiences so far
Proton-Radiotherapy for Tumors of the Skull Base: Indications, Advantages, Limitations
 Proton-Radiotherapy for Tumors of the Skull Base: Indications, Advantages, Limitations Eugen B. Hug, MD Director, Center for Proton-Radiotherapy, Paul Scherrer Institut, Villigen and Chair of Proton-Radiotherapy.
Proton-Radiotherapy for Tumors of the Skull Base: Indications, Advantages, Limitations Eugen B. Hug, MD Director, Center for Proton-Radiotherapy, Paul Scherrer Institut, Villigen and Chair of Proton-Radiotherapy.
Pediatr Blood Cancer 2014
 Low grade Glioma! 40% of pediatric brain tumors Pathologically, anatomically, clinically and biologically heterogeneous Leptomeningeal metastases in 5% Frequently protracted clinical course Long-Term Outcome
Low grade Glioma! 40% of pediatric brain tumors Pathologically, anatomically, clinically and biologically heterogeneous Leptomeningeal metastases in 5% Frequently protracted clinical course Long-Term Outcome
Proton Therapy for tumors of the skull base - RESULTS. Eugen B. Hug, MD Medical Director, ProCure Proton Therapy Centers, NY
 Proton Therapy for tumors of the skull base - RESULTS Eugen B. Hug, MD Medical Director, ProCure Proton Therapy Centers, NY Petroclival Chondrosarcoma: 68 72 Gy(RBE) at 1.8 or 2.0 Gy(RBE) GTV: 70.2 Gy(RBE)
Proton Therapy for tumors of the skull base - RESULTS Eugen B. Hug, MD Medical Director, ProCure Proton Therapy Centers, NY Petroclival Chondrosarcoma: 68 72 Gy(RBE) at 1.8 or 2.0 Gy(RBE) GTV: 70.2 Gy(RBE)
Proton Radiation Therapy for Osteosarcomas, Chondrogenic Tumors and Soft Tissue Sarcomas
 Proton Radiation Therapy for Osteosarcomas, Chondrogenic Tumors and Soft Tissue Sarcomas Eugen B. Hug Center for Proton Radiation Therapy Paul Scherrer Institute Histologies Osteogenic Tumors Osteogenic
Proton Radiation Therapy for Osteosarcomas, Chondrogenic Tumors and Soft Tissue Sarcomas Eugen B. Hug Center for Proton Radiation Therapy Paul Scherrer Institute Histologies Osteogenic Tumors Osteogenic
Radiation Technology, Hyogo Ion Beam Medical Center, Tatsuno, Hyogo, JAPAN
 Analysis of Visual Loss Due to Radiation- Induced Optic Neuropathy After Particle Therapy for Head and Neck and Skull Base Tumors Adjacent to Optic Nerves Y. Demizu 1, M. Murakami 1, D. Miyawaki 1, Y.
Analysis of Visual Loss Due to Radiation- Induced Optic Neuropathy After Particle Therapy for Head and Neck and Skull Base Tumors Adjacent to Optic Nerves Y. Demizu 1, M. Murakami 1, D. Miyawaki 1, Y.
Proton Radiation Therapy for Osteosarcomas, Chondrogenic Tumors and Soft Tissue Sarcomas
 Proton Radiation Therapy for Osteosarcomas, Chondrogenic Tumors and Soft Tissue Sarcomas Eugen B. Hug Center for Proton Radiation Therapy Paul Scherrer Institute Is there a place for Proton/Particle Radiotherapy
Proton Radiation Therapy for Osteosarcomas, Chondrogenic Tumors and Soft Tissue Sarcomas Eugen B. Hug Center for Proton Radiation Therapy Paul Scherrer Institute Is there a place for Proton/Particle Radiotherapy
Review of Workflow NRG (RTOG) 1308: Phase III Randomized Trial Comparing Overall Survival after Photon versus Proton Chemoradiation Therapy for
 1308: Phase III Randomized Trial Comparing Overall Survival after Photon versus Proton Chemoradiation Therapy for") Review of Workflow NRG (RTOG) 1308: Phase III Randomized Trial Comparing Overall Survival after Photon versus Proton Chemoradiation Therapy for Inoperable Stage II-IIIB NSCLC 1 Co-Chairs Study Chair: Zhongxing
Review of Workflow NRG (RTOG) 1308: Phase III Randomized Trial Comparing Overall Survival after Photon versus Proton Chemoradiation Therapy for Inoperable Stage II-IIIB NSCLC 1 Co-Chairs Study Chair: Zhongxing
Clinical Trials of Proton Therapy for Breast Cancer. Andrew L. Chang, MD 張維安 Study Chair
 Clinical Trials of Proton Therapy for Breast Cancer Andrew L. Chang, MD 張維安 Study Chair AndrewLChangMD@gmail.com Disclosure Proton Center Development Corporation Scripps San Diego Proton Therapy Center
Clinical Trials of Proton Therapy for Breast Cancer Andrew L. Chang, MD 張維安 Study Chair AndrewLChangMD@gmail.com Disclosure Proton Center Development Corporation Scripps San Diego Proton Therapy Center
Radiation Therapy for Soft Tissue Sarcomas
 Radiation Therapy for Soft Tissue Sarcomas Alexander R. Gottschalk, MD, PhD Assistant Professor, Radiation Oncology University of California, San Francisco 1/25/08 NCI: limb salvage vs. amputation 43 patients
Radiation Therapy for Soft Tissue Sarcomas Alexander R. Gottschalk, MD, PhD Assistant Professor, Radiation Oncology University of California, San Francisco 1/25/08 NCI: limb salvage vs. amputation 43 patients
PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING
 PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING ANATOMY ANATOMY CONT ANATOMY CONT. ANATOMY CONT. EYE OF A CHILD Normal tissue tolerance doses (in conventional #) TD 5/5 TD 50/5 Endpoint Gy Gy Optic nerve
PEDIATRIC ORBITAL TUMORS RADIOTHERAPY PLANNING ANATOMY ANATOMY CONT ANATOMY CONT. ANATOMY CONT. EYE OF A CHILD Normal tissue tolerance doses (in conventional #) TD 5/5 TD 50/5 Endpoint Gy Gy Optic nerve
Pediatric Oncology. Vlad Radulescu, MD
 Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
Pediatric Oncology Vlad Radulescu, MD Objectives Review the epidemiology of childhood cancer Discuss the presenting signs and symptoms, general treatment principles and overall prognosis of the most common
Otolaryngologist s Perspective of Stereotactic Radiosurgery
 Otolaryngologist s Perspective of Stereotactic Radiosurgery Douglas E. Mattox, M.D. 25 th Alexandria International Combined ORL Conference April 18-20, 2007 Acoustic Neuroma Benign tumor of the schwann
Otolaryngologist s Perspective of Stereotactic Radiosurgery Douglas E. Mattox, M.D. 25 th Alexandria International Combined ORL Conference April 18-20, 2007 Acoustic Neuroma Benign tumor of the schwann
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM EPENDYMOMA Last Revision Date July 2015 1 CNS Site Group Ependymoma Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2.
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM EPENDYMOMA Last Revision Date July 2015 1 CNS Site Group Ependymoma Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2.
Pediatric Brain Tumors: Updates in Treatment and Care
 Pediatric Brain Tumors: Updates in Treatment and Care Writer Classroom Rishi R. Lulla, MD MS Objectives Introduce the common pediatric brain tumors Discuss current treatment strategies for pediatric brain
Pediatric Brain Tumors: Updates in Treatment and Care Writer Classroom Rishi R. Lulla, MD MS Objectives Introduce the common pediatric brain tumors Discuss current treatment strategies for pediatric brain
The Role of Radiation Therapy in the Treatment of Brain Metastases. Matthew Cavey, M.D.
 The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
Hot topics in Radiation Oncology for the Primary Care Providers
 Hot topics in Radiation Oncology for the Primary Care Providers Steven Feigenberg, MD Professor Chief, Thoracic Oncology Vice Chair of Clinical Research April 19, 2018 Disclosures NONE 2 Early Stage Disease
Hot topics in Radiation Oncology for the Primary Care Providers Steven Feigenberg, MD Professor Chief, Thoracic Oncology Vice Chair of Clinical Research April 19, 2018 Disclosures NONE 2 Early Stage Disease
Reducing excess radiation from portal imaging of pediatric brain tumors
 JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 14, NUMBER 5, 2013 Reducing excess radiation from portal imaging of pediatric brain tumors Moses Tam, 1 Maya Mathew, 1 Christine J. Hitchen, 1 Ashwatha
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 14, NUMBER 5, 2013 Reducing excess radiation from portal imaging of pediatric brain tumors Moses Tam, 1 Maya Mathew, 1 Christine J. Hitchen, 1 Ashwatha
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MENINGIOMA CNS Site Group Meningioma Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION 3 2. PREVENTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MENINGIOMA CNS Site Group Meningioma Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION 3 2. PREVENTION
Journal of Pediatric Sciences
 Journal of Pediatric Sciences Role of post-operative radiation therapy in single brain metastasis from clear cell sarcoma in children: a case report with systemic review Fadoua Rais, Naoual Benhmidou,
Journal of Pediatric Sciences Role of post-operative radiation therapy in single brain metastasis from clear cell sarcoma in children: a case report with systemic review Fadoua Rais, Naoual Benhmidou,
Radiation Therapy for Liver Malignancies
 Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Dose escalation for NSCLC using conformal RT: 3D and IMRT. Hasan Murshed
 Dose escalation for NSCLC using conformal RT: 3D and IMRT. Hasan Murshed Take home message Preliminary data shows CRT technique in NSCLC allows dose escalation to an unprecedented level maintaining cancer
Dose escalation for NSCLC using conformal RT: 3D and IMRT. Hasan Murshed Take home message Preliminary data shows CRT technique in NSCLC allows dose escalation to an unprecedented level maintaining cancer
Clinical considerations of RBE in proton therapy
 Clinical considerations of RBE in proton therapy H. Paganetti PhD Professor, Harvard Medical School Director of Physics Research, Massachusetts General Hospital, Radiation Oncology Why do we need the RBE
Clinical considerations of RBE in proton therapy H. Paganetti PhD Professor, Harvard Medical School Director of Physics Research, Massachusetts General Hospital, Radiation Oncology Why do we need the RBE
PTCOG 46. Educational Workshop Session IV. Head & Neck CLINICAL. J. Mizoe (NIRS, Japan)
") PTCOG 46 Educational Workshop Session IV CLINICAL Head & Neck J. Mizoe (NIRS, Japan) Photon X-Ray γ-ray Fast Neutron Non-Charged Radiation Electron Proton Helium Light Ion Heavy Particle Carbon Neon Argon
PTCOG 46 Educational Workshop Session IV CLINICAL Head & Neck J. Mizoe (NIRS, Japan) Photon X-Ray γ-ray Fast Neutron Non-Charged Radiation Electron Proton Helium Light Ion Heavy Particle Carbon Neon Argon
Proton- Radiotherapy:
 Proton- Radiotherapy: Future of Medical Indications and Treatment Concepts Eugen B. Hug and Ralf A. Schneider HUG 11/07 The emerging role of Proton Radiotherapy in the framework of modern Photon-RT 2000
Proton- Radiotherapy: Future of Medical Indications and Treatment Concepts Eugen B. Hug and Ralf A. Schneider HUG 11/07 The emerging role of Proton Radiotherapy in the framework of modern Photon-RT 2000
7/1/2015. Objectives. Host Factors LATE EFFECTS OF RADIOTHERAPY IN CHILDHOOD CANCER. Chronic Conditions in Adult Survivors
 LATE EFFECTS OF RADIOTHERAPY IN CHILDHOOD CANCER ARNOLD C. PAULINO, M.D. PROFESSOR DEPARTMENT OF RADIATION ONCOLOGY MD ANDERSON CANCER CENTER Objectives At the end of the presentation, the participant
LATE EFFECTS OF RADIOTHERAPY IN CHILDHOOD CANCER ARNOLD C. PAULINO, M.D. PROFESSOR DEPARTMENT OF RADIATION ONCOLOGY MD ANDERSON CANCER CENTER Objectives At the end of the presentation, the participant
Treatment Planning Evaluation of Volumetric Modulated Arc Therapy (VMAT) for Craniospinal Irradiation (CSI)
 for Craniospinal Irradiation (CSI)") Treatment Planning Evaluation of Volumetric Modulated Arc Therapy (VMAT) for Craniospinal Irradiation (CSI) Tagreed AL-ALAWI Medical Physicist King Abdullah Medical City- Jeddah Aim 1. Simplify and standardize
Treatment Planning Evaluation of Volumetric Modulated Arc Therapy (VMAT) for Craniospinal Irradiation (CSI) Tagreed AL-ALAWI Medical Physicist King Abdullah Medical City- Jeddah Aim 1. Simplify and standardize
Where are we with radiotherapy for biliary tract cancers?
 Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
ARRO Case: Diffuse Intrinsic Pontine Glioma
 ARRO Case: Diffuse Intrinsic Pontine Glioma Nicholas DeNunzio, MD, PhD (PGY-3) Faculty Advisor: Louis S. Constine, MD, FASTRO Department of Radiation Oncology University of Rochester Case Presentation
ARRO Case: Diffuse Intrinsic Pontine Glioma Nicholas DeNunzio, MD, PhD (PGY-3) Faculty Advisor: Louis S. Constine, MD, FASTRO Department of Radiation Oncology University of Rochester Case Presentation
Charged-Particle (Proton or Helium Ion) Radiotherapy for Neoplastic Conditions
 Radiotherapy for Neoplastic Conditions") Charged-Particle (Proton or Helium Ion) Radiotherapy for Neoplastic Conditions Policy Number: 8.01.10 Last Review: 11/2017 Origination: 11/2006 Next Review: 11/2018 Policy Blue Cross and Blue Shield of
Charged-Particle (Proton or Helium Ion) Radiotherapy for Neoplastic Conditions Policy Number: 8.01.10 Last Review: 11/2017 Origination: 11/2006 Next Review: 11/2018 Policy Blue Cross and Blue Shield of
ASTRO econtouring for Lymphoma. Stephanie Terezakis, MD
 ASTRO econtouring for Lymphoma Stephanie Terezakis, MD Disclosures No conflicts to disclose 1970 Total Lymphoid Irradiation (TLI) 1995 Involved-Field Radiotherapy (IFRT) 2008 Involved Node Radiotherapy
ASTRO econtouring for Lymphoma Stephanie Terezakis, MD Disclosures No conflicts to disclose 1970 Total Lymphoid Irradiation (TLI) 1995 Involved-Field Radiotherapy (IFRT) 2008 Involved Node Radiotherapy
The Economic Club of Florida Tallahassee August 13, 2018 Nancy P Mendenhall, MD. The Promise of Protons
 The Economic Club of Florida Tallahassee August 13, 2018 Nancy P Mendenhall, MD The Promise of Protons The Promise of Protons Cancer and radiation therapy The promise of protons UFHPTI: missions and operation
The Economic Club of Florida Tallahassee August 13, 2018 Nancy P Mendenhall, MD The Promise of Protons The Promise of Protons Cancer and radiation therapy The promise of protons UFHPTI: missions and operation
7/1/2015. Radiotherapy in Infant Brain Tumors. Goals and Objectives. Primary Brain and CNS Tumors (0-14 years) Brain Tumors (1 to 4 years)
 Brain Tumors (1 to 4 years)") Radiotherapy in Infant Brain Tumors ARNOLD C. PAULINO, M.D. PROFESSOR OF RADIATION ONCOLOGY MD ANDERSON CANCER CENTER AND TEXAS CHILDREN S HOSPITAL Radiotherapy in Infant Brain Tumors 1. Try to Avoid Irradiation
Radiotherapy in Infant Brain Tumors ARNOLD C. PAULINO, M.D. PROFESSOR OF RADIATION ONCOLOGY MD ANDERSON CANCER CENTER AND TEXAS CHILDREN S HOSPITAL Radiotherapy in Infant Brain Tumors 1. Try to Avoid Irradiation
INTRAOPERATIVE RADIATION THERAPY FOR RETROPERITONEAL SARCOMA
 INTRAOPERATIVE RADIATION THERAPY FOR RETROPERITONEAL SARCOMA ISIORT 2014 Ivy A Petersen, MD Mayo Clinic Rochester, MN NOTHING TO DISCLOSE SOFT TISSUE SARCOMAS 2014 Estimated cases in the USA 12,020 diagnosed
INTRAOPERATIVE RADIATION THERAPY FOR RETROPERITONEAL SARCOMA ISIORT 2014 Ivy A Petersen, MD Mayo Clinic Rochester, MN NOTHING TO DISCLOSE SOFT TISSUE SARCOMAS 2014 Estimated cases in the USA 12,020 diagnosed
Intracranial AT RT / radiotherapy. Therapeutic dilemma / radiotherapy
 Therapeutic dilemma / radiotherapy Agressive tumour, poor outcome Past treatments based on MB concepts (RT CSA) MB Overall survival Mean age : 6.52 years n=36, 5 year 75% 1. Tumour occurs in the very young
Therapeutic dilemma / radiotherapy Agressive tumour, poor outcome Past treatments based on MB concepts (RT CSA) MB Overall survival Mean age : 6.52 years n=36, 5 year 75% 1. Tumour occurs in the very young
Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer
 Techniques in Head and Neck Cancer") 1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
1 Charles Poole April Case Study April 30, 2012 Evaluation of Whole-Field and Split-Field Intensity Modulation Radiation Therapy (IMRT) Techniques in Head and Neck Cancer Abstract: Introduction: This study
NRG Oncology Lung Cancer Portfolio 2016
 NRG Oncology Lung Cancer Portfolio 2016 Roy Decker, MD PhD Yale Cancer Center Walter J Curran, Jr, MD Winship Cancer Institute of Emory University NRG Oncology Lung Cancer Selected Discussion Stage III
NRG Oncology Lung Cancer Portfolio 2016 Roy Decker, MD PhD Yale Cancer Center Walter J Curran, Jr, MD Winship Cancer Institute of Emory University NRG Oncology Lung Cancer Selected Discussion Stage III
7/31/2018. Research Activities: Imaging for RT Image Guidance for Pediatric Radiotherapy. Chia-ho Hua, PhD. Outline
 Research Activities: Imaging for RT Image Guidance for Pediatric Radiotherapy Chia-ho Hua, PhD Chia-ho Associate Hua, Member PhD St. Jude Children s Research Hospital AAPM-COG Joint Session, 60 th Annual
Research Activities: Imaging for RT Image Guidance for Pediatric Radiotherapy Chia-ho Hua, PhD Chia-ho Associate Hua, Member PhD St. Jude Children s Research Hospital AAPM-COG Joint Session, 60 th Annual
Oncological Management of Brain Tumours. Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013
 Oncological Management of Brain Tumours Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013 Outline General considerations of Primary Brain Tumours: epidemiology, pathology, presentation. Diagnosis
Oncological Management of Brain Tumours Anna Maria Shiarli SpR in Clinical Oncology 15 th July 2013 Outline General considerations of Primary Brain Tumours: epidemiology, pathology, presentation. Diagnosis
Reirradiazione. La radioterapia stereotassica ablativa: torace. Pierluigi Bonomo Firenze
 Reirradiazione La radioterapia stereotassica ablativa: torace Pierluigi Bonomo Firenze Background Stage III NSCLC isolated locoregional recurrence in 25% of pts mostly unresectable; low RR with 2 nd line
Reirradiazione La radioterapia stereotassica ablativa: torace Pierluigi Bonomo Firenze Background Stage III NSCLC isolated locoregional recurrence in 25% of pts mostly unresectable; low RR with 2 nd line
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2
 Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Case Conference: SBRT for spinal metastases D A N I E L S I M P S O N M D 3 / 2 7 / 1 2 Case 79 yo M with hx of T3N0 colon cancer diagnosed in 2008 metastatic liver disease s/p liver segmentectomy 2009
Conventional (2D) Versus Conformal (3D) Techniques in Radiotherapy for Malignant Pediatric Tumors: Dosimetric Perspectives
 Versus Conformal (3D) Techniques in Radiotherapy for Malignant Pediatric Tumors: Dosimetric Perspectives") Journal of the Egyptian Nat. Cancer Inst., Vol. 2,. 3, December: 39-34, 29 Conventional (2D) Versus Conformal (3D) Techniques in Radiotherapy for Malignant Pediatric Tumors: Dosimetric Perspectives NESREEN
Journal of the Egyptian Nat. Cancer Inst., Vol. 2,. 3, December: 39-34, 29 Conventional (2D) Versus Conformal (3D) Techniques in Radiotherapy for Malignant Pediatric Tumors: Dosimetric Perspectives NESREEN
Pediatrics -Proton Beam Therapy in Children -
 Pediatrics -Proton Beam Therapy in Children - Beate Timmermann, M.D. West German Proton Therapy Centre Essen Germany Preview Survival Toxicity Why protons? (theoretically) Experiences so far (clinically)
Pediatrics -Proton Beam Therapy in Children - Beate Timmermann, M.D. West German Proton Therapy Centre Essen Germany Preview Survival Toxicity Why protons? (theoretically) Experiences so far (clinically)
The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology
 The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology (specifically, lung cancer) 2/10/18 Jeffrey Kittel, MD Radiation Oncology, Aurora St. Luke s Medical Center Outline The history
The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology (specifically, lung cancer) 2/10/18 Jeffrey Kittel, MD Radiation Oncology, Aurora St. Luke s Medical Center Outline The history
What s New in Radiotherapy For STS of The Extremity? Kaled M. Alektiar, MD, FASTRO Dept of Rad Onc Memorial Sloan Kettering Cancer Center
 What s New in Radiotherapy For STS of The Extremity? Kaled M. Alektiar, MD, FASTRO Dept of Rad Onc Memorial Sloan Kettering Cancer Center Topics Predictive tools for risk assessment Reassessment of dose/volume
What s New in Radiotherapy For STS of The Extremity? Kaled M. Alektiar, MD, FASTRO Dept of Rad Onc Memorial Sloan Kettering Cancer Center Topics Predictive tools for risk assessment Reassessment of dose/volume
NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA
 NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA Roberta Rudà Department of Neuro-Oncology University and City of Health and Science Hospital of Turin, Italy EORTC EANO ESMO Conference 2015 Istanbul, March 27-28
NON-SURGICAL STRATEGY FOR ADULT EPENDYMOMA Roberta Rudà Department of Neuro-Oncology University and City of Health and Science Hospital of Turin, Italy EORTC EANO ESMO Conference 2015 Istanbul, March 27-28
Role of radiotherapy in the treatment of lymphoma in Lena Specht MD DMSc Professor of Oncology Rigshospitalet, University of Copenhagen Denmark
 Role of radiotherapy in the treatment of lymphoma in 2017 Lena Specht MD DMSc Professor of Oncology Rigshospitalet, University of Copenhagen Denmark Disclosures Member of Advisory Board and Principal Investigator,
Role of radiotherapy in the treatment of lymphoma in 2017 Lena Specht MD DMSc Professor of Oncology Rigshospitalet, University of Copenhagen Denmark Disclosures Member of Advisory Board and Principal Investigator,
ES-SCLC Joint Case Conference. Anthony Paravati Adam Yock
 ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
Role of adaptive radiation therapy for pediatric patients with diffuse pontine glioma
 JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 12, NUMBER 2, spring 2011 Role of adaptive radiation therapy for pediatric patients with diffuse pontine glioma Chris Beltran, a Saumya Sharma, and Thomas
JOURNAL OF APPLIED CLINICAL MEDICAL PHYSICS, VOLUME 12, NUMBER 2, spring 2011 Role of adaptive radiation therapy for pediatric patients with diffuse pontine glioma Chris Beltran, a Saumya Sharma, and Thomas
Protocol Abstract and Schema
 Protocol Abstract and Schema Phase II study of Peginterferon alfa-2b (PEGIntron) for pediatric patients with unresectable or recurrent craniopharyngioma. Description and Rationale: Craniopharyngiomas account
Protocol Abstract and Schema Phase II study of Peginterferon alfa-2b (PEGIntron) for pediatric patients with unresectable or recurrent craniopharyngioma. Description and Rationale: Craniopharyngiomas account
Ependymoma Programme Synopsis
 Ependymoma Programme Synopsis TITLE SPONSOR PROTOCOL NUMBER EUDRACT NUMBER NATIONAL INVESTIGATOR- COORDINATOR SIOP Ependymoma program II: An International Clinical Program for the diagnosis and treatment
Ependymoma Programme Synopsis TITLE SPONSOR PROTOCOL NUMBER EUDRACT NUMBER NATIONAL INVESTIGATOR- COORDINATOR SIOP Ependymoma program II: An International Clinical Program for the diagnosis and treatment
Adjuvant Radiotherapy for completely resected NSCLC
 Adjuvant Radiotherapy for completely resected NSCLC ESMO Preceptorship on lung Cancer Manchester February 2017 Cécile Le Péchoux Radiation Oncology Department IOT Institut d Oncologie Thoracique Local
Adjuvant Radiotherapy for completely resected NSCLC ESMO Preceptorship on lung Cancer Manchester February 2017 Cécile Le Péchoux Radiation Oncology Department IOT Institut d Oncologie Thoracique Local
Charged-Particle (Proton or Helium Ion) Radiotherapy for Neoplastic Conditions
 Radiotherapy for Neoplastic Conditions") Charged-Particle (Proton or Helium Ion) Radiotherapy for Neoplastic Conditions Policy Number: Original Effective Date: MM.05.005 07/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST
Charged-Particle (Proton or Helium Ion) Radiotherapy for Neoplastic Conditions Policy Number: Original Effective Date: MM.05.005 07/01/2009 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST
Radio-chemo-immunotherapy using the IDO-inhibitor indoximod for childhood brain cancer (NCT )
") Radio-chemo-immunotherapy using the IDO-inhibitor indoximod for childhood brain cancer (NCT02502708) Theodore S. Johnson, M.D., Ph.D. Pediatric Immunotherapy Program Medical College of Georgia (MCG) Georgia
Radio-chemo-immunotherapy using the IDO-inhibitor indoximod for childhood brain cancer (NCT02502708) Theodore S. Johnson, M.D., Ph.D. Pediatric Immunotherapy Program Medical College of Georgia (MCG) Georgia
Insights into Thymic Epithelial Tumors: Radiation Therapy
 Insights into Thymic Epithelial Tumors: Radiation Therapy Charles R. Thomas, MD Professor and Chairman, Department of Radiation Medicine Professor, Department of Medicine, Division of Hematology/Medical
Insights into Thymic Epithelial Tumors: Radiation Therapy Charles R. Thomas, MD Professor and Chairman, Department of Radiation Medicine Professor, Department of Medicine, Division of Hematology/Medical
Particle Therapy for CNS Tumors Anita Mahajan MD MD Anderson Cancer Center PTCOG, Shanghai June 10, 2014
 Particle Therapy for CNS Tumors Anita Mahajan MD MD Anderson Cancer Center PTCOG, Shanghai June 10, 2014 TCP/NTCP (%) The Potential for Protons in the CNS 10 0 Increase Tumor Control Increase TCP increased
Particle Therapy for CNS Tumors Anita Mahajan MD MD Anderson Cancer Center PTCOG, Shanghai June 10, 2014 TCP/NTCP (%) The Potential for Protons in the CNS 10 0 Increase Tumor Control Increase TCP increased
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MEDULLOBLASTOMA AND PNET CNS Site Group Medulloblastoma and PNET Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM MEDULLOBLASTOMA AND PNET CNS Site Group Medulloblastoma and PNET Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION
Pediatric Brain Tumors Pre, Intra & Post Op Evaluation and Management. Timothy M. George, MD, FACS, FAAP
 Pediatric Brain Tumors Pre, Intra & Post Op Evaluation and Management Timothy M. George, MD, FACS, FAAP PEDIATRIC BRAIN TUMORS BACKGROUND: Incidence: Third most common pediatric tumor type (leukemia, neuroblastoma,
Pediatric Brain Tumors Pre, Intra & Post Op Evaluation and Management Timothy M. George, MD, FACS, FAAP PEDIATRIC BRAIN TUMORS BACKGROUND: Incidence: Third most common pediatric tumor type (leukemia, neuroblastoma,
8/2/2017. Improving Dose Prescriptions for Safety, Reporting, and Clinical Guideline Consistency. Part III
 Improving Dose Prescriptions for Safety, Reporting, and Clinical Guideline Consistency Part III I Das, J Moran, M Langer Keeping Guidelines On Track: The Effect On Clinical Practice of Neglecting Guidelines
Improving Dose Prescriptions for Safety, Reporting, and Clinical Guideline Consistency Part III I Das, J Moran, M Langer Keeping Guidelines On Track: The Effect On Clinical Practice of Neglecting Guidelines
Radioterapia no Tratamento dos Gliomas de Baixo Grau
 Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
Radioterapia no Tratamento dos Gliomas de Baixo Grau Dr. Luis Souhami University Montreal - Canada Low Grade Gliomas Relatively rare Heterogeneous, slow growing tumors WHO Classification Grade I Pilocytic
Protocol of Radiotherapy for Small Cell Lung Cancer
 107 年 12 月修訂 Protocol of Radiotherapy for Small Cell Lung Cancer Indication of radiotherapy Limited stage: AJCC (8th edition) stage I-III (T any, N any, M0) that can be safely treated with definitive RT
107 年 12 月修訂 Protocol of Radiotherapy for Small Cell Lung Cancer Indication of radiotherapy Limited stage: AJCC (8th edition) stage I-III (T any, N any, M0) that can be safely treated with definitive RT
Ependymomas: Prognostic Factors and Outcome Analysis in a Retrospective Series of 33 Patients
 ORIGINAL ARTICLE Brain Tumor Res Treat 2017;5(2):70-76 / pissn 2288-2405 / eissn 2288-2413 https://doi.org/10.14791/btrt.2017.5.2.70 Ependymomas: Prognostic Factors and Outcome Analysis in a Retrospective
ORIGINAL ARTICLE Brain Tumor Res Treat 2017;5(2):70-76 / pissn 2288-2405 / eissn 2288-2413 https://doi.org/10.14791/btrt.2017.5.2.70 Ependymomas: Prognostic Factors and Outcome Analysis in a Retrospective
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM LOW GRADE GLIOMAS CNS Site Group Low Grade Gliomas Author: Dr. Norm Laperriere 1. INTRODUCTION 3 2. PREVENTION 3 3. SCREENING
Feasibility Trial of Optune for Children with Recurrent or Progressive Supratentorial High-Grade Glioma and Ependymoma
 Feasibility Trial of Optune for Children with Recurrent or Progressive Supratentorial High-Grade Glioma and Ependymoma ABSTRACT Recurrent or progressive pediatric CNS tumors generally have a poor prognosis
Feasibility Trial of Optune for Children with Recurrent or Progressive Supratentorial High-Grade Glioma and Ependymoma ABSTRACT Recurrent or progressive pediatric CNS tumors generally have a poor prognosis
Role of protons, heavy ions and BNCT in brain tumors
 Role of protons, heavy ions and BNCT in brain tumors Prof G K Rath Head, NCI (AIIMS-2) Chief, Dr. BRA IRCH, Professor Radiation Oncology All India Institute of Medical Sciences, New Delhi 1 Overview of
Role of protons, heavy ions and BNCT in brain tumors Prof G K Rath Head, NCI (AIIMS-2) Chief, Dr. BRA IRCH, Professor Radiation Oncology All India Institute of Medical Sciences, New Delhi 1 Overview of
JAMES EWING, Endothelial origin. 14 yr Girl
 JAMES EWING, 1921 Endothelial origin 14 yr Girl SPECTRUM OF ESFT NEURAL DIFFERENTIATION Least Well EWING S SARCOMA ATYPICAL EWING S SARCOMA PNET Peripheral Neuroepithelioma ASKIN TUMOR (thoraco-pulmonary)
JAMES EWING, 1921 Endothelial origin 14 yr Girl SPECTRUM OF ESFT NEURAL DIFFERENTIATION Least Well EWING S SARCOMA ATYPICAL EWING S SARCOMA PNET Peripheral Neuroepithelioma ASKIN TUMOR (thoraco-pulmonary)
Gamma knife radiosurgery for Koos grade 4 vestibular schwannomas
 Gamma knife radiosurgery for Koos grade 4 vestibular schwannomas David Mathieu MD FRCSC, Christian Iorio-Morin MD PhD, Fahd Al Subaie MD MSc FRCSC Division of neurosurgery, Université de Sherbrooke, Centre
Gamma knife radiosurgery for Koos grade 4 vestibular schwannomas David Mathieu MD FRCSC, Christian Iorio-Morin MD PhD, Fahd Al Subaie MD MSc FRCSC Division of neurosurgery, Université de Sherbrooke, Centre
ACR TXIT TM EXAM OUTLINE
 ACR TXIT TM EXAM OUTLINE Major Domain Sub-Domain 1 Statistics 1.1 Study design 1.2 Definitions of statistical terms 1.3 General interpretation & analysis 1.4 Survival curves 1.5 Specificity/sensitivity
ACR TXIT TM EXAM OUTLINE Major Domain Sub-Domain 1 Statistics 1.1 Study design 1.2 Definitions of statistical terms 1.3 General interpretation & analysis 1.4 Survival curves 1.5 Specificity/sensitivity
Refresher Course EAR TUMOR. Sasikarn Chamchod, MD Chulabhorn Hospital
 Refresher Course EAR TUMOR Sasikarn Chamchod, MD Chulabhorn Hospital Reference: Perez and Brady s Principles and Practice of radiation oncology sixth edition Outlines Anatomy Epidemiology Clinical presentations
Refresher Course EAR TUMOR Sasikarn Chamchod, MD Chulabhorn Hospital Reference: Perez and Brady s Principles and Practice of radiation oncology sixth edition Outlines Anatomy Epidemiology Clinical presentations
Marco Trovò CRO-Aviano
 From pre-clinical research to clinical practice in radiation therapy: new predictive factors and biological markers to predict normal tissue toxicity after radiation therapy of the lung. Marco Trovò CRO-Aviano
From pre-clinical research to clinical practice in radiation therapy: new predictive factors and biological markers to predict normal tissue toxicity after radiation therapy of the lung. Marco Trovò CRO-Aviano
Clinical Results of Carbon Ion Radiotherapy: The Heidelberg Experience
 Clinical Results of Carbon Ion Radiotherapy: The Heidelberg Experience Stephanie E. Combs, MD Department of Radiation Oncology University of Heidelberg, Germany Carbon ion RT at GSI Active beam delivery
Clinical Results of Carbon Ion Radiotherapy: The Heidelberg Experience Stephanie E. Combs, MD Department of Radiation Oncology University of Heidelberg, Germany Carbon ion RT at GSI Active beam delivery
Childhood Cancer Survivor Study Analysis Concept Proposal
 Childhood Cancer Survivor Study Analysis Concept Proposal Title: Long-Term Outcomes of Childhood Central Nervous System Tumor Survivors: A Report from the Childhood Cancer Survivor Study Working Group
Childhood Cancer Survivor Study Analysis Concept Proposal Title: Long-Term Outcomes of Childhood Central Nervous System Tumor Survivors: A Report from the Childhood Cancer Survivor Study Working Group
Update on Pediatric Brain Tumors
 Update on Pediatric Brain Tumors David I. Sandberg, M.D. Director of Pediatric Neurosurgery & Associate Professor Dr. Marnie Rose Professorship in Pediatric Neurosurgery Pre-talk Questions for Audience
Update on Pediatric Brain Tumors David I. Sandberg, M.D. Director of Pediatric Neurosurgery & Associate Professor Dr. Marnie Rose Professorship in Pediatric Neurosurgery Pre-talk Questions for Audience
Overview of MLC-based Linac Radiosurgery
 SRT I: Comparison of SRT Techniques 1 Overview of MLC-based Linac Radiosurgery Grace Gwe-Ya Kim, Ph.D. DABR 2 MLC based Linac SRS Better conformity for irregular target Improved dose homogeneity inside
SRT I: Comparison of SRT Techniques 1 Overview of MLC-based Linac Radiosurgery Grace Gwe-Ya Kim, Ph.D. DABR 2 MLC based Linac SRS Better conformity for irregular target Improved dose homogeneity inside
National System for Incident Reporting in Radiation Therapy (NSIR-RT) Taxonomy
 Taxonomy") Canadian Partnership for Quality Radiotherapy (CPQR) National System for Incident Reporting in Radiation Therapy (NSIR-RT) National System for Incident Reporting in Radiation Therapy (NSIR-RT) Taxonomy
Canadian Partnership for Quality Radiotherapy (CPQR) National System for Incident Reporting in Radiation Therapy (NSIR-RT) National System for Incident Reporting in Radiation Therapy (NSIR-RT) Taxonomy
A Dosimetric Comparison of Whole-Lung Treatment Techniques. in the Pediatric Population
 A Dosimetric Comparison of Whole-Lung Treatment Techniques in the Pediatric Population Corresponding Author: Christina L. Bosarge, B.S., R.T. (R) (T) Indiana University School of Medicine Department of
A Dosimetric Comparison of Whole-Lung Treatment Techniques in the Pediatric Population Corresponding Author: Christina L. Bosarge, B.S., R.T. (R) (T) Indiana University School of Medicine Department of
SCIENTIFIC PROGRAMME SNOLA THE STATE OF THE ART ON NEURO-ONCOLOGY th March
 SCIENTIFIC PROGRAMME SNOLA THE STATE OF THE ART ON NEURO-ONCOLOGY 2018 15th March 13h 13h45 ROOM 1 ROOM 2 ROOM 3 Imaging and pathology case discussion Lymphomas case discussion- Meningeomas Moderator:
SCIENTIFIC PROGRAMME SNOLA THE STATE OF THE ART ON NEURO-ONCOLOGY 2018 15th March 13h 13h45 ROOM 1 ROOM 2 ROOM 3 Imaging and pathology case discussion Lymphomas case discussion- Meningeomas Moderator:
Disclosures. Overview 8/3/2016. SRS: Cranial and Spine
 SRS: Cranial and Spine Brian Winey, Ph.D. Department of Radiation Oncology Massachusetts General Hospital Harvard Medical School Disclosures Travel and research funds from Elekta Travel funds from IBA
SRS: Cranial and Spine Brian Winey, Ph.D. Department of Radiation Oncology Massachusetts General Hospital Harvard Medical School Disclosures Travel and research funds from Elekta Travel funds from IBA
Small and Big Operations: New Tools of the Trade for Brain Tumors. Disclosure. Incidence of Childhood Cancer
 Small and Big Operations: New Tools of the Trade for Brain Tumors Nalin Gupta MD PhD Chief, Division of Pediatric Neurosurgery Departments of Neurosurgery and Pediatrics University of California San Francisco
Small and Big Operations: New Tools of the Trade for Brain Tumors Nalin Gupta MD PhD Chief, Division of Pediatric Neurosurgery Departments of Neurosurgery and Pediatrics University of California San Francisco
Report on Radiation Disaster Recovery Studies
 Report on Radiation Disaster Recovery Studies Course: Radiation Disaster Medicine Name: Uranchimeg Tsegmed Radiation Disaster Recovery Studies Nowadays, applications of nuclear technology in different
Report on Radiation Disaster Recovery Studies Course: Radiation Disaster Medicine Name: Uranchimeg Tsegmed Radiation Disaster Recovery Studies Nowadays, applications of nuclear technology in different
Advances in external beam radiotherapy
 International Conference on Modern Radiotherapy: Advances and Challenges in Radiation Protection of Patients Advances in external beam radiotherapy New techniques, new benefits and new risks Michael Brada
International Conference on Modern Radiotherapy: Advances and Challenges in Radiation Protection of Patients Advances in external beam radiotherapy New techniques, new benefits and new risks Michael Brada
11/28/2018. Proton Therapy for Liver Cancer: Who, Why, and How. Disclosures. Michael Chuong, MD. None
 Proton Therapy for Liver Cancer: Who, Why, and How Michael Chuong, MD Disclosures None 1 Rationale for proton therapy Hepatic toxicity Biliary toxicity GI toxicity Potentially significant benefit especially
Proton Therapy for Liver Cancer: Who, Why, and How Michael Chuong, MD Disclosures None 1 Rationale for proton therapy Hepatic toxicity Biliary toxicity GI toxicity Potentially significant benefit especially
Particle (proton) Therapy Randomized trials vs. Prospective registry. Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology
 Therapy Randomized trials vs. Prospective registry. Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology") Particle (proton) Therapy Randomized trials vs. Prospective registry Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Should we do randomized trials? Are randomized trials needed
Particle (proton) Therapy Randomized trials vs. Prospective registry Andrew K. Lee, MD, MPH Associate Professor Department of Radiation Oncology Should we do randomized trials? Are randomized trials needed
Might Adaptive Radiotherapy in NSCLC be feasible in clinical practice?
 Might Adaptive Radiotherapy in NSCLC be feasible in clinical practice? E.Molfese, P.Matteucci, A.Iurato, L.E.Trodella, A.Sicilia, B.Floreno, S.Ramella, L.Trodella Radioterapia Oncologica, Università Campus
Might Adaptive Radiotherapy in NSCLC be feasible in clinical practice? E.Molfese, P.Matteucci, A.Iurato, L.E.Trodella, A.Sicilia, B.Floreno, S.Ramella, L.Trodella Radioterapia Oncologica, Università Campus
Specifics of treatment planning for active scanning and IMPT
 Specifics of treatment planning for active scanning and IMPT SFUD IMPT Tony Lomax, Centre for Proton Radiotherapy, Paul Scherrer Institute, Switzerland Treatment planning for scanning 1. Single Field,
Specifics of treatment planning for active scanning and IMPT SFUD IMPT Tony Lomax, Centre for Proton Radiotherapy, Paul Scherrer Institute, Switzerland Treatment planning for scanning 1. Single Field,
Optic Pathway Gliomas, Germinomas, Spinal Cord Tumours. Colin Kennedy March 2015
 Optic Pathway Gliomas, Germinomas, Spinal Cord Tumours Colin Kennedy March 2015 Glioma of the optic chiasm. T1-weighted MRI with gadolinium enhancement, showing intense irregular uptake of contrast. The
Optic Pathway Gliomas, Germinomas, Spinal Cord Tumours Colin Kennedy March 2015 Glioma of the optic chiasm. T1-weighted MRI with gadolinium enhancement, showing intense irregular uptake of contrast. The
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM GERM CELL TUMOURS CNS Site Group Germ Cell Tumours Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM GERM CELL TUMOURS CNS Site Group Germ Cell Tumours Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
Pediatric electron intraoperative radiotherapy: results and innovations
 Pediatric electron intraoperative radiotherapy: results and innovations Felipe A. Calvo ESTRO Hospital General Universitario Gregorio Marañon Madrid, Spain 2017 IOeRT in pediatric cancer: results and innovations
Pediatric electron intraoperative radiotherapy: results and innovations Felipe A. Calvo ESTRO Hospital General Universitario Gregorio Marañon Madrid, Spain 2017 IOeRT in pediatric cancer: results and innovations
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES CENTRAL NERVOUS SYSTEM ANAPLASTIC GLIOMAS CNS Site Group Anaplastic Gliomas Author: Dr. Norm Laperriere Date: February 20, 2018 1. INTRODUCTION