Upper Gastrointestinal Cancers in the Elderly. Choo Su Pin Senior Consultant Medical Oncology National Cancer Centre Singapore
|
|
|
- Reynard Walters
- 5 years ago
- Views:
Transcription

1 Upper Gastrointestinal Cancers in the Elderly Choo Su Pin Senior Consultant Medical Oncology National Cancer Centre Singapore

2 Gastric Cancer --High Global Burden Global Cancer Deaths % of all cancer (2008) deaths Lung Cancer 1,400, % Stomach Cancer 740, % Liver Cancer 700, % Colorectal Cancer 610, % Breast Cancer 460, % Jemal et al. CA Cancer J Clin 2011;61:69 90

3 OesophagealCancers Among top 10 causes of cancer deaths worldwide More common in males Affects developing countries more esp Africa and East Asia Squamous cell carcinoma predominant in these countries In Singapore 80% are squamous cell carcinoma, the rest mostly adenocarcinoma GLOBOCAN 2008
4 Gastro-oesophagealCancer is a disease of the elderly 60.9% of oesophagealand 64.6% of gastric cancers occur in those aged 65years

5 Curative Surgery is mainstay of care in Gastric Cancer (GC) D2 Gastrectomy is a standard of care here European studies have not shown better outcomes with D2 vs D1 dissection and have higher postop mortality: Dutch postop mortality 4% vs Japanese postop mortality 0.8% D2 dissection includes removal of: 7, left gastric artery; 8, common hepatic artery; 9, celiac artery; 10, splenic hilus; 11, splenic artery Sasako 2008, Hatgrink 2004
6 Are surgical outcomes in elderly the same for GC? (Takeshita 2013) N=1193 gastrectomiesfor GC, of which n=104 aged 80 years and above Postopmortality 1.9% in 80yrs vs 0.7% in younger But no differences in disease-specific survival between those 80yrs vs those < 80yrs even when D2 gastrectomy done
7 More postop complications in the elderly Hayashi 2012
8 E-PASS score predicts for postop N=414 pts who had gastrectomies + LND for GC: 38.4% 75yrs 61.6% < 75yrs Comprehensive Risk Score ( CRS) predicted for survival outcome after surgery and death from comorbid disease CRS calculated from Pre-op Risk Score ( Age, severity of IHD and lung disease, DM, ECOG and ASA physiological status) and Surgical Stress Score ( blood loss/weight; operation time; extent of skin incision) complications Ariake2014

9 ROLE of ADJUVANT THERAPY in GASTRIC CANCER Practice differs between regions: Gastric Cancer amenable to surgery Should we be offering adjuvant therapy to elderly patients? Is this benefit worth the potential side Curative Surgery followed by Adjuvant Chemotherapy +/-RT Prevent Relapse Cure Prolong Survival effects? Absolute benefit of Adjuvant Therapy after curative surgery is about 10-15%
10 Adjuvant Chemotherapy in GC our practice Options are: 1) Oral TS-1 x 1 year ACTS-GC trial (Sakuramoto 2007) N=1059 Aged 20-80yrs, all had D2 gastrectomy 2) Oral Xeloda+ iv Oxaliplatin( XELOX) x 6 months CLASSIC trial ( Bang 2012, 2013) N=1035, D2 gastrectomy, R0 68% HR for death=0.68; p= y DFS 53% P< S1 post-op Surgery XELOX post-op Surgery 3-year OS 80.1% 70.1% 3-year RFS 72.2% 59.6% 5-year DFS 68% 53% 5-year OS 78% 69%

11 Adjuvant TS-1 in resectedgc ( ACTS-GC trial) Patients aged > 80yrs were not included in this trial NEJM 2007; 357:
12 Classic study Subgroups and toxicity Bang Lancet 2012 G3/4 AE XELOX (%) Neutropenia 22 PLT 8 Nausea 8 Vomiting 7 Neuropathy 2 DFS benefit appears to be less in N0. Stat sig in N1 and N2. However only 10% of pt N0. 12


13 MAGIC trial N= 503 from Centers from UK, Holland, Germany, Brazil, Singapore, NZ About 20% were 70 yrs and above 14% lower oes 11% EGJ Cunningham 2006
14 Adjuvant Chemo in Elderly with D2 Gastrectomy Retrospective series, n=360 GC patients aged >65years All had D2 gastrectomy 34.7% received adjuvant chemotherapy Findings: Adjuvant chemotherapy increased OS, HR0.60, p0.003 Stage 3 GC benefited from chemo, not Stage I & II Benefit was seen with fluropyrimidine chemotherapy Jin 2013
15 Adjuvant Therapy in Elderly with ResectedGC Most of the trials included elderly patients Benefit of adjuvant therapy shown across all age groups Whether or not adjuvant therapy should be given should be discussed with each patient: Balance benefit with potential toxicities
16 Curative Approaches to Oesophageal Cancers-our practice Surgery alone Definitive ChemoRT(cervical oesophageal) Pre-operative ChemoRTfollowed by surgery
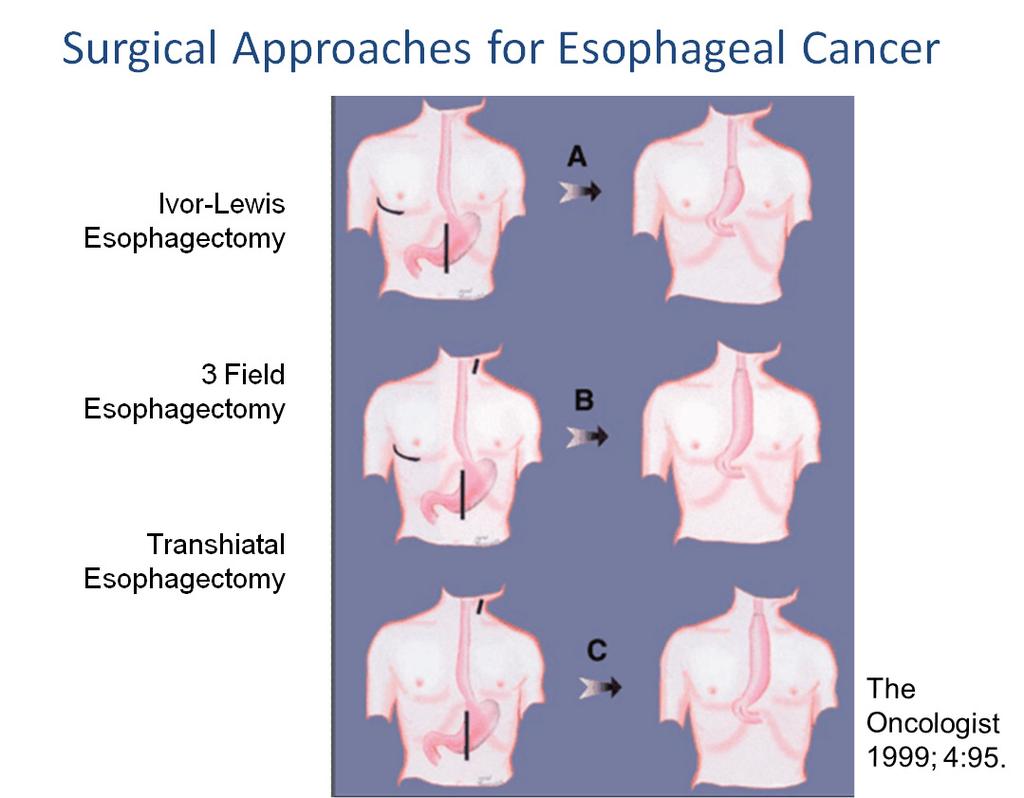
17 Surgical Approaches for Oesophageal Ca
18 Outcomes of oesophagealresection in elderly-retrospective series
19 Definitive ChemoRT for oesophageal cancer: RTOG T3N0-1 thoracic eso SCF LN allowed 90% SqCC, 10% adeno N=123 R CF cisplatin75mg/m2 D1 and 5-FU 1000mg/m2 for 4 days on D1 and D29 with RT 50Gy/25# > 2 cycles CF q3wk RT 64Gy CRT RT Median OS 14.1m 9.3m 5yr OS 27% 0% Local failure 47% 66% P<0.001 More than 20% in each arm were aged 70y and above CRT is toxic 64% G3/4 toxicity > 50% myelosuppresion, 8% N&V No toxicity analysis in relation to age Herskovic A et al. NEJM 1992 Al-SaraffM et al. JCO 1997
20 Definitive ChemoRT in Elderly with OC Study Patients Treatment Outcomes Toxicities Tougeron 2008 Single institution series Anderson 2007 Single institution series Servagi Vemat 2009 Phase II N=109, 70y and above with OC (70.6% SCC) N=25, Pts > 65y with stage II or III OC N=22 aged 75y stage II & III ( 68% SCC) Concurrent RT with Cisplatin + 5FU ( 89.9%) or Irinotecan + Cisplatin (9.2%) Concurrent RT with5fu + Mitomycin-C Concurrent RT with cisplatin Median OS 15.2m DFS 8.3m 5Y 0S 12.8% Median OS 35m 2y OS 64% 56.9% grade 2 AE 36% grade 3-4 haem toxicity 1y OS 62.4% Only grade 2 vomiting 53.2% had dose reductions No differences in outcomes between Charlson comorbid score 2 or >2.
21 Neoadjuvant Chemo RT followed by surgery: CROSS trial Thoracic oeso+ GOJ (<2cm invasion stomach) adenoca, SqCC, large cell T1N1 or T2/3 N0-1 No M1a/b ds N=366 Pts aged 36-79yrs 75% adenoca; 23% SCC 80% T3; 65% N1 80% lower oeso (58%) / GEJ (22%) 5x Weekly carboauc2 5x Weekly taxol 50mg/m2 RT 41.4Gy in 25# + Surgery Surgery CRT-- Surgery Surgery Median OS 49.4m 24m R0 resection 92% 69% Local recurrence 14% 34% Peritoneal mets 4% 14% Less than 13% grade 3 toxicities No analysis on relationship between age and outcomes or toxicities Van Hagen et al. NEJM 2012
22 Palliative chemotherapy in the Elderly with Gastro-oesophageal cancers
23 Management of Advanced Gastric Cancer; Chemotherapy improves OS compared to BSC Survival with best supportive care (BSC) alone: 3 months Chemotherapy improves OS compared to BSC: Benefit about 6 months Quality of life isalso improved. (HR 0.39, 95% Cl , p< ) Wagner et al., JCO 2006
24 Is combination chemo better than single agent? Combination chemo superior to single agent [HR 0.83, 95%CI , p=0.001] Wagner A D et al. JCO 2006;24:
25 Which combination is better? New generation regimen since 2000 Study Treatment No.Pt RR (%) TTP (month) OS (month) p - value Van Cutsem (V325) Dank (V306) Cunningham (REAL-2) Kang Boku (JCOG9912) Narahara (SPIRITS) Ajani (FLAGS) CDDP+5FU Doce+CDDP+5FU CDDP+5FU Irinotecan+5FU/LV ECF EOF ECX EOX CDDP+5FU CDDP+capecitabine FU CDDP+irinotecan S S CDDP+S CDDP+5-FU CDDP+S NS 0.02 NS NS
26 Studies on chemotherapy in Elderly GC Catalona 2012 No. of pts Regimen Response PFS OS Gd3 Toxicities 43 mfolfox 1 st line Liu mfolfox 1 st line Kim Frail or elderly; Kim aged 70yrs Tsushima aged 70yrs mfolfiri salvage 77% received doublet or triplet chemo S-1+ cisplatin (n=21) vs S-1 (n=37) 34.9% 6.8m 10.5m <10% 52.5% 6.5m 10m <8% 12.5% 2m 5.4m 20% 26% m 19.7% - 5m vs 5.2m 14.4m vs 10.9m Haem toxicities 57% vs 35%
 advanced vs metastatic GC vs GEJ measurable vs non-measurable ECOG PS 0-1 vs 2 capecitabine vs 5-FU R 5-FU or capecitabine +")
27 Trastuzumabimproves survival when added onto Chemo for HER2 + GC: ToGAtrial Phase III, randomised, open-label, international, multicentre study 3807 patients screened 1,2 810 HER2-positive* Primary endpoint: OS Stratification factors HER2-positive advanced GC (n=584) advanced vs metastatic GC vs GEJ measurable vs non-measurable ECOG PS 0-1 vs 2 capecitabine vs 5-FU R 5-FU or capecitabine + cisplatin (n=290) 5-FU or capecitabine + cisplatin + trastuzumab (n=294) *as defined in the protocol (IHC 3+ and/or FISH+) Chosen at investigator s discretion 1. Bang et al. ASCO 2009; Abstract Chung et al. ECCO-ESMO 2009; Abstract
28 Efficacy: OS subgroup analysis Category Subgroup N HR 95% CI All All , 0.91 Primary site GEJ , 1.08 Stomach , 0.96 ECOG PS , , 1.79 Fluoropyrimidine 5-FU , 1.23 Capecitabine , 0.95 Age group < , 1.14 > , 0.88 Region Asia , 1.11 C/S America Europe , , 0.89 Other , 3.08 GC type Diffuse Intestinal , , 0.88 Mixed , 1.46 Prior gastrectomy No 451 Yes , , 1.34 No. metastatic sites , 1.26 > , Favours T Risk ratio Favours no T
29 ToGatrial:Safety: cardiac AEs Cardiac event, n (%) F+C n=290 F+C + trastuzumab n=294 All Grade 3/4 All Grade 3/4 Cardiac AEs, total 18 (6) 9 (3) 17 (6) 4 (1) Cardiac failure 2 (<1) 2 (<1) 1 (<1) 1 (<1) LVEF drops* <50% 2 (1.1) 14 (5.9) <50% and by 10% 2 (1.1) 11 (4.6) Cardiac AEs leading to death 2 (<1) Cardiac arrest; cardio-respiratory arrest 2 (<1) Acute MI; cardiac failure Would recommend careful systolic dysfunction monitoring in elderly *Measured at baseline and every 12 weeks; MI, myocardial infarction
30 Palliative Chemotherapy in Elderly Multiple clinical trials have shown that there are a variety of effective chemotherapy options for GOC Current data shows that chemotherapy in elderly is as effective However, toxicities can be more common We have to tailor treatment to particular needs of each elderly patient
31 Concluding thoughts There is underrepresentation of elderly patients in clinical trials partly due to strict selection criteria Thus applying what we know as best treatment to elderly patients has to be balanced against known risks of the treatment itself Regardless, chronological age should not be a limiting factor in determining best treatment but the biological age and fitness of the patient should be considered first Any treatment decisions in the elderly must take into consideration ECOG, nutritional status, comorbidity and future QOL Several tools exist ( geriatric assessment scores etc) to help us make these decisions. While running elderly specific trials may be difficult, more such trials are needed in order to answer our questions. In meantime, other trials should be designed to incorporate age in relation to outcomes
32 Thank you
Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy
 Anna Dorothea Wagner, PD & MER Department of Oncology University of Lausanne Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy Structure 1. Background and overview 2. Adjuvant chemotherapy:
Anna Dorothea Wagner, PD & MER Department of Oncology University of Lausanne Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy Structure 1. Background and overview 2. Adjuvant chemotherapy:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
 Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy
 Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy Joseph Chao, M.D. Assistant Clinical Professor Department of Medical Oncology & Therapeutics
Which Treatment Approach is Most Appropriate for Primary Therapy of Gastric Cancer: Neoadjuvant Chemotherapy Joseph Chao, M.D. Assistant Clinical Professor Department of Medical Oncology & Therapeutics
Updated Apr 2017 by Dr. Ko (Medical Oncologist, Abbotsford Cancer Centre)
") Metastatic Esophagogastric Cancer Summary Updated Apr 2017 by Dr. Ko (Medical Oncologist, Abbotsford Cancer Centre) Reviewed by Dr. Yoo-Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer Centre, University
Metastatic Esophagogastric Cancer Summary Updated Apr 2017 by Dr. Ko (Medical Oncologist, Abbotsford Cancer Centre) Reviewed by Dr. Yoo-Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer Centre, University
CHEMOTHERAPY FOR METASTATIC GASTRIC CANCER
 CHEMOTHERAPY FOR METASTATIC GASTRIC CANCER Dr Elizabeth Smyth Royal Marsden, UK ESMO Gastric Cancer Preceptorship Valencia 2017 IMPORTANT CONSIDERATIONS WHEN TREATING ADVANCED GASTRIC CANCER Short OS Pain
CHEMOTHERAPY FOR METASTATIC GASTRIC CANCER Dr Elizabeth Smyth Royal Marsden, UK ESMO Gastric Cancer Preceptorship Valencia 2017 IMPORTANT CONSIDERATIONS WHEN TREATING ADVANCED GASTRIC CANCER Short OS Pain
Chemotherapy for Advanced Gastric Cancer
 Chemotherapy for Advanced Gastric Cancer Andrés Cervantes Professor of Medicine DISCLOSURE OF INTEREST Employment: None Consultant or Advisory Role: Merck Serono, Roche, Beigene, Bayer, Servier, Lilly,
Chemotherapy for Advanced Gastric Cancer Andrés Cervantes Professor of Medicine DISCLOSURE OF INTEREST Employment: None Consultant or Advisory Role: Merck Serono, Roche, Beigene, Bayer, Servier, Lilly,
Perioperative chemotherapy: individualized therapy or same treatment for all? Prof. Dr. med. Salah-Eddin Al-Batran
 Perioperative chemotherapy: individualized therapy or same treatment for all? Prof. Dr. med. Salah-Eddin Al-Batran Institute of Clinical Cancer Research Krankenhaus Nordwest UCT - University Cancer Center
Perioperative chemotherapy: individualized therapy or same treatment for all? Prof. Dr. med. Salah-Eddin Al-Batran Institute of Clinical Cancer Research Krankenhaus Nordwest UCT - University Cancer Center
GASTRIC & PANCREATIC CANCER
 GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
Perioperative versus adjuvant management of gastric cancer, update 2013
 Perioperative versus adjuvant management of gastric cancer, update 2013 Cornelis J.H. van de Velde, MD, PhD,FRCPS and FACS,Hon. Professor of Surgery President ECCO - the European Cancer Organization Past-President
Perioperative versus adjuvant management of gastric cancer, update 2013 Cornelis J.H. van de Velde, MD, PhD,FRCPS and FACS,Hon. Professor of Surgery President ECCO - the European Cancer Organization Past-President
NEOADJUVANT THERAPY IN CARCINOMA STOMACH. Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah
 NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
NEOADJUVANT THERAPY IN CARCINOMA STOMACH Dr Jyotirup Goswami Consultant Radiation Oncologist Narayana Superspeciality Hospital, Howrah NEOADJUVANT THERAPY?! Few believers Limited evidence Many surgeons
Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT
 Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT David H. Ilson, MD, PhD Gastrointestinal Oncology Service Memorial Sloan Kettering Cancer Center Disclosure Consulting
Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT David H. Ilson, MD, PhD Gastrointestinal Oncology Service Memorial Sloan Kettering Cancer Center Disclosure Consulting
Advances in gastric cancer: How to approach localised disease?
 Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
Advances in gastric cancer: How to approach localised disease? Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation
(Neo-) adjuvant Treatment of Gastric Cancer. - The European View
 adjuvant Treatment of Gastric Cancer. - The European View") (Neo-) adjuvant Treatment of Gastric Cancer - The European View Florian Lordick, MD Professor of Oncology Director of the University Cancer Center Leipzig (UCCL) University of Leipzig, Germany My Conflict
(Neo-) adjuvant Treatment of Gastric Cancer - The European View Florian Lordick, MD Professor of Oncology Director of the University Cancer Center Leipzig (UCCL) University of Leipzig, Germany My Conflict
Gastroesophag Gastroesopha eal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. G. H addock Haddock M.D.
 Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
Current standards of care in gastric cancer
 Current standards of care in gastric cancer Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Outline Resectable gastric cancer: the role of neoadjuvant and adjuvant
Current standards of care in gastric cancer Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Outline Resectable gastric cancer: the role of neoadjuvant and adjuvant
2015 EUROPEAN CANCER CONGRESS
 2015 EUROPEAN CANCER CONGRESS 25-29 September 2015 Vienna, Austria SUMMARY The European Cancer Congress (ECC 2015) combined the 40th European Society for Medical Oncology (ESMO) congress with the 18th
2015 EUROPEAN CANCER CONGRESS 25-29 September 2015 Vienna, Austria SUMMARY The European Cancer Congress (ECC 2015) combined the 40th European Society for Medical Oncology (ESMO) congress with the 18th
Esophageal and GEJ Adenocarcinoma: Chemo + RT is the Preferred Treatment
 Esophageal and GEJ Adenocarcinoma: Chemo + RT is the Preferred Treatment David H. Ilson, MD, PhD Gastrointestinal Oncology Service Memorial Sloan-Kettering Cancer Center Preop Therapy in Esophageal and
Esophageal and GEJ Adenocarcinoma: Chemo + RT is the Preferred Treatment David H. Ilson, MD, PhD Gastrointestinal Oncology Service Memorial Sloan-Kettering Cancer Center Preop Therapy in Esophageal and
ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT
 ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT DOCETAXEL, OXALIPLATIN AND FLUOROURACIL/LEUCOVORIN (FLOT) FOR RESECTABLE
ESMO 2017, Madrid, Spain Dr. Loredana Vecchione Charite Comprehensive Cancer Center, Berlin HIGHLIGHTS ON CANCERS OF THE UPPER GI TRACT DOCETAXEL, OXALIPLATIN AND FLUOROURACIL/LEUCOVORIN (FLOT) FOR RESECTABLE
Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy
 Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy Priv. Doz. Dr. Dr. med. T.O. Götze Institute of Clinical Cancer Research Director: Prof. Dr. S.-E. Al- Batran University Cancer
Neo- and adjuvant treatment for gastric cancer: The role of chemotherapy Priv. Doz. Dr. Dr. med. T.O. Götze Institute of Clinical Cancer Research Director: Prof. Dr. S.-E. Al- Batran University Cancer
ONCOLOGY LETTERS 2: , 2011
 ONCOLOGY LETTERS 2: 241-245, 2011 Irinotecan monotherapy offers advantage over combination therapy with irinotecan plus cisplatin in second-line setting for treatment of advanced gastric cancer following
ONCOLOGY LETTERS 2: 241-245, 2011 Irinotecan monotherapy offers advantage over combination therapy with irinotecan plus cisplatin in second-line setting for treatment of advanced gastric cancer following
Resectable locally advanced oesophagogastric cancer
 Resectable locally advanced oesophagogastric cancer Clinical Case Discussion Florian Lordick University Cancer Center Leipzig University Clinic Leipzig Leipzig, Germany esmo.org DISCLOSURES Honoraria for
Resectable locally advanced oesophagogastric cancer Clinical Case Discussion Florian Lordick University Cancer Center Leipzig University Clinic Leipzig Leipzig, Germany esmo.org DISCLOSURES Honoraria for
Newly Diagnosed Cases Cancer Related Death NCI 2006 Data
 Multi-Disciplinary Management of Esophageal Cancer: Surgical and Medical Steps Forward Alarming Thoracic Twin Towers 200000 150000 UCSF UCD Thoracic Oncology Conference November 21, 2009 100000 50000 0
Multi-Disciplinary Management of Esophageal Cancer: Surgical and Medical Steps Forward Alarming Thoracic Twin Towers 200000 150000 UCSF UCD Thoracic Oncology Conference November 21, 2009 100000 50000 0
Jonathan Dickinson, LCL Xeloda
 Xeloda A blockbuster in the making Jonathan Dickinson, LCL Xeloda Xeloda unique tumor-activated mechanism Delivering more cancer-killing agent straight into cancer Highly effective comparable efficacy
Xeloda A blockbuster in the making Jonathan Dickinson, LCL Xeloda Xeloda unique tumor-activated mechanism Delivering more cancer-killing agent straight into cancer Highly effective comparable efficacy
Getting to the Bottom of Treatment: An Update in the Management of Esophagogastric Cancers
 Getting to the Bottom of Treatment: An Update in the Management of Esophagogastric Cancers Disclosures None Cindy L. O Bryant, PharmD, BCOP, FCCP, FHOPA Professor, University of Colorado Skaggs School
Getting to the Bottom of Treatment: An Update in the Management of Esophagogastric Cancers Disclosures None Cindy L. O Bryant, PharmD, BCOP, FCCP, FHOPA Professor, University of Colorado Skaggs School
The role of chemoradiotherapy in GE junction and gastric cancer. Karin Haustermans
 The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
Adjuvant Chemotherapy
 State-of-the-art: standard of care for resectable NSCLC Adjuvant Chemotherapy JY DOUILLARD MD PhD Professor of Medical Oncology Integrated Centers of Oncology R Gauducheau University of Nantes France Adjuvant
State-of-the-art: standard of care for resectable NSCLC Adjuvant Chemotherapy JY DOUILLARD MD PhD Professor of Medical Oncology Integrated Centers of Oncology R Gauducheau University of Nantes France Adjuvant
Lung Cancer Epidemiology. AJCC Staging 6 th edition
 Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Tegafur, gimeracil, and oteracil (known as S1) for first-line palliative treatment of advanced gastric cancer
 for first-line palliative treatment of advanced gastric cancer") LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Tegafur, gimeracil, and oteracil (known as S1) for first-line palliative treatment of advanced gastric cancer Tegafur, gimeracil, and oteracil (known as S1) in
LONDON CANCER NEW DRUGS GROUP RAPID REVIEW Tegafur, gimeracil, and oteracil (known as S1) for first-line palliative treatment of advanced gastric cancer Tegafur, gimeracil, and oteracil (known as S1) in
Systemic treatment in early and advanced gastric cancer
 Systemic treatment in early and advanced gastric cancer Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer n Surgical resection n Pathology assessment and estimation
Systemic treatment in early and advanced gastric cancer Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer n Surgical resection n Pathology assessment and estimation
Targeted Therapies in Gastric Cancer : Where Do We Stand Today. Yoon-Koo Kang Asan Medical Center, University of Ulsan Seoul, Korea
 Targeted Therapies in Gastric Cancer : Where Do We Stand Today Yoon-Koo Kang Asan Medical Center, University of Ulsan Seoul, Korea Chemotherapy is the standard of care in advanced gastric cancer Median
Targeted Therapies in Gastric Cancer : Where Do We Stand Today Yoon-Koo Kang Asan Medical Center, University of Ulsan Seoul, Korea Chemotherapy is the standard of care in advanced gastric cancer Median
PCPA Advanced Trainee Program Upper GI Cancers. Dr N Singhal Medical Oncologist Royal Adelaide Hospital
 Upper GI Cancers Dr N Singhal Medical Oncologist Royal Adelaide Hospital Localised disease PCPA Advanced Trainee Program 2018 Submucosal PCPA Advanced Trainee Program 2018 Work up EUS- 90% sensitivity
Upper GI Cancers Dr N Singhal Medical Oncologist Royal Adelaide Hospital Localised disease PCPA Advanced Trainee Program 2018 Submucosal PCPA Advanced Trainee Program 2018 Work up EUS- 90% sensitivity
Two Cycles of Chemoradiation: 2 Cycles is Enough. Concurrent Chemotherapy / RT Regimens
 1 Two Cycles of Chemoradiation: 2 Cycles is Enough Heather Wakelee, M.D. Assistant Professor of Medicine, Oncology Stanford University Concurrent Chemotherapy / RT Regimens Cisplatin 50 mg/m 2 on days
1 Two Cycles of Chemoradiation: 2 Cycles is Enough Heather Wakelee, M.D. Assistant Professor of Medicine, Oncology Stanford University Concurrent Chemotherapy / RT Regimens Cisplatin 50 mg/m 2 on days
Updates and best practices in the management of gastric cancer
 Updates and best practices in the management of gastric cancer Olatunji B. Alese, MD Gastrointestinal Oncology, Winship Cancer Institute of Emory University July 28, 2017 1 Incidence 3rd leading cause
Updates and best practices in the management of gastric cancer Olatunji B. Alese, MD Gastrointestinal Oncology, Winship Cancer Institute of Emory University July 28, 2017 1 Incidence 3rd leading cause
3/8/2014. Case Presentation. Primary Treatment of Anal Cancer. Anatomy. Overview. March 6, 2014
 Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Prague July 2016 State of the art: Standard of care for anal squamous cancer Rob Glynne-Jones Mount Vernon Cancer Centre Aim to discuss Background The trials
ESMO Preceptorship Programme Colorectal Cancer Prague July 2016 State of the art: Standard of care for anal squamous cancer Rob Glynne-Jones Mount Vernon Cancer Centre Aim to discuss Background The trials
Neodjuvant chemotherapy
 Neodjuvant chemotherapy Dr Robert Huddart Senior Lecturer and Honorary Consultant in Clinical Oncology Royal Marsden Hospital and Institute of Cancer Research Why consider neo-adjuvant chemotherapy? Loco-regional
Neodjuvant chemotherapy Dr Robert Huddart Senior Lecturer and Honorary Consultant in Clinical Oncology Royal Marsden Hospital and Institute of Cancer Research Why consider neo-adjuvant chemotherapy? Loco-regional
Chemotherapy for resectable liver mets: Options and Issues. Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA
 Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Gastric: 16% 18% 27% Esophageal: 5% 10% 19%
 2.5% of all cancers Median age 68 years Decline in gastric cancer incidence Increase in esophageal, GEJ, cardia adenocarcinoma OS improvement, 1975-77, 1984-86, 1999-2006 Gastric: 16% 18% 27% Esophageal:
2.5% of all cancers Median age 68 years Decline in gastric cancer incidence Increase in esophageal, GEJ, cardia adenocarcinoma OS improvement, 1975-77, 1984-86, 1999-2006 Gastric: 16% 18% 27% Esophageal:
Are we making progress? Marked reduction in operative morbidity and mortality
 Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER
 UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER Susan Davidson, MD Professor Department of Obstetrics and Gynecology Division of Gynecologic Oncology University of Colorado- Denver Anatomy Review
UPDATE IN THE MANAGEMENT OF INVASIVE CERVICAL CANCER Susan Davidson, MD Professor Department of Obstetrics and Gynecology Division of Gynecologic Oncology University of Colorado- Denver Anatomy Review
Chemotherapy of colon cancers
 Chemotherapy of colon cancers Stage distribution Stage I : 15% T 1,2 NO Stage IV: 20 25% M+ Stage II : 20 30% T3,4 NO Stage III N+: 30 40% clinical stages I, II, or III colon cancer are at risk for having
Chemotherapy of colon cancers Stage distribution Stage I : 15% T 1,2 NO Stage IV: 20 25% M+ Stage II : 20 30% T3,4 NO Stage III N+: 30 40% clinical stages I, II, or III colon cancer are at risk for having
Targeted Therapies in Metastatic Colorectal Cancer: An Update
 Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Adjuvant treatment Colon Cancer
 ESMO Preceptorship Colorectal Cancer, October 2016 Singapore Adjuvant treatment Colon Cancer Claus-Henning Köhne University Clinic for Onkology und Haematology Oldenburg, Germany Aim of the lecture Adjuvant
ESMO Preceptorship Colorectal Cancer, October 2016 Singapore Adjuvant treatment Colon Cancer Claus-Henning Köhne University Clinic for Onkology und Haematology Oldenburg, Germany Aim of the lecture Adjuvant
intent treatment be in the elderly?
 Gastric cancer: How strong can curative intent treatment be in the elderly? Caio Max S. Rocha Lima, M.D. Professor of Medicine University of Miami & Sylvester Cancer Center Gastric cancer: epidemiology
Gastric cancer: How strong can curative intent treatment be in the elderly? Caio Max S. Rocha Lima, M.D. Professor of Medicine University of Miami & Sylvester Cancer Center Gastric cancer: epidemiology
Lung Cancer Non-small Cell Local, Regional, Small Cell, Other Thoracic Cancers: The Question Isn t Can We, but Should We
 Lung Cancer Non-small Cell Local, Regional, Small Cell, Other Thoracic Cancers: The Question Isn t Can We, but Should We Edward Garon, MD, MS Associate Professor Director- Thoracic Oncology Program David
Lung Cancer Non-small Cell Local, Regional, Small Cell, Other Thoracic Cancers: The Question Isn t Can We, but Should We Edward Garon, MD, MS Associate Professor Director- Thoracic Oncology Program David
Updated Apr 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Cancer Centre)
") Local Esophageal Cancer Summary Updated Apr 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Cancer Centre) Reviewed by Dr. Yoo-Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer Centre, University
Local Esophageal Cancer Summary Updated Apr 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Cancer Centre) Reviewed by Dr. Yoo-Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer Centre, University
stage III gastric cancer after D2 gastrectomy.
 RESEARCH ARTICLE Comparison of capecitabine and oxaliplatin with S-1 as adjuvant chemotherapy in stage III gastric cancer after D2 gastrectomy Jang Ho Cho, Jae Yun Lim, Jae Yong Cho* Division of Medical
RESEARCH ARTICLE Comparison of capecitabine and oxaliplatin with S-1 as adjuvant chemotherapy in stage III gastric cancer after D2 gastrectomy Jang Ho Cho, Jae Yun Lim, Jae Yong Cho* Division of Medical
Radiotherapy for rectal cancer. Karin Haustermans Department of Radiation Oncology
 Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
Adjuvant/neoadjuvant systemic treatment of colorectal cancer
 5th ESO-ESMO Eastern Europe and Balkan Region Masterclass in Medical Oncology Belgrade, June 19 th 2018 Adjuvant/neoadjuvant systemic treatment of colorectal cancer Carlotta Antoniotti Polo Oncologico
5th ESO-ESMO Eastern Europe and Balkan Region Masterclass in Medical Oncology Belgrade, June 19 th 2018 Adjuvant/neoadjuvant systemic treatment of colorectal cancer Carlotta Antoniotti Polo Oncologico
Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First?
 Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First? Marc Peeters, MD, PhD Head of the Oncology Department Antwerp University Hospital Antwerp, Belgium marc.peeters@uza.be 71-year-old
Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First? Marc Peeters, MD, PhD Head of the Oncology Department Antwerp University Hospital Antwerp, Belgium marc.peeters@uza.be 71-year-old
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Upper GI. Oesophageal & Gastric Cancer. Tumour Group: Regimen name / acronym Cisplatin/5-FU with concomitant RT. Place in therapy
 Tumour Group: Upper GI Tumour Type: Oesophageal & Gastric Cancer Primary Cisplatin/5-FU with concomitant RT Alternative Regimen: Oxaliplatin/ 5FU with concomitant RT (FOLFOX6-RT) Cisplatin Carboplatin
Tumour Group: Upper GI Tumour Type: Oesophageal & Gastric Cancer Primary Cisplatin/5-FU with concomitant RT Alternative Regimen: Oxaliplatin/ 5FU with concomitant RT (FOLFOX6-RT) Cisplatin Carboplatin
Adjuvant chemotherapy in older breast cancer patients: how to decide?
 Adjuvant chemotherapy in older breast cancer patients: how to decide? H. Wildiers University Hospitals Leuven Belgium Wildiers H, Kunkler I, Lancet Oncol 2007 Biganzoli L, Wildiers H, Lancet Oncol. 2012
Adjuvant chemotherapy in older breast cancer patients: how to decide? H. Wildiers University Hospitals Leuven Belgium Wildiers H, Kunkler I, Lancet Oncol 2007 Biganzoli L, Wildiers H, Lancet Oncol. 2012
Systemic Cytotoxic Therapy in advanced HCC
 Systemic Cytotoxic Therapy in advanced HCC Yeul Hong Kim Korea University Anam Hospital Cancer Center Hepatocellular Carcinoma : Overview Epidemiology Current Guideline : advanced HCC Cytotoxic Chemotherapy
Systemic Cytotoxic Therapy in advanced HCC Yeul Hong Kim Korea University Anam Hospital Cancer Center Hepatocellular Carcinoma : Overview Epidemiology Current Guideline : advanced HCC Cytotoxic Chemotherapy
Il paziente anziano con malattia oncologica avanzata: il tumore del colon-retto
 Milano 05.10.2018 Il paziente anziano con malattia oncologica avanzata: il tumore del colon-retto Salvatore Corallo U.O.C. Oncologia Medica IRCCS Istituto Nazionale dei Tumori Milano CRC in elderly patients
Milano 05.10.2018 Il paziente anziano con malattia oncologica avanzata: il tumore del colon-retto Salvatore Corallo U.O.C. Oncologia Medica IRCCS Istituto Nazionale dei Tumori Milano CRC in elderly patients
Pancreatic Adenocarcinoma
 Pancreatic Adenocarcinoma AProf Lara Lipton 28 April 2018 Percentage alive 5 years after diagnosis for men and women Epidemiology 6% of cancer related deaths worldwide 4 th highest cause of cancer death
Pancreatic Adenocarcinoma AProf Lara Lipton 28 April 2018 Percentage alive 5 years after diagnosis for men and women Epidemiology 6% of cancer related deaths worldwide 4 th highest cause of cancer death
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS
 IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
MEETING SUMMARY ESMO 2018, Munich, Germany. Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER
 MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective
 Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
سرطان المعدة. Gastric Cancer حمود حامد
 سرطان المعدة Gastric Cancer ا أ لستاذ الدك تور حمود حامد عميد كلية الطب البشري بجامعة دمشق Epidemiology second leading cause of cancer death and fourth most common cancer worldwide Overall declining Histologic
سرطان المعدة Gastric Cancer ا أ لستاذ الدك تور حمود حامد عميد كلية الطب البشري بجامعة دمشق Epidemiology second leading cause of cancer death and fourth most common cancer worldwide Overall declining Histologic
Adjuvant therapy in pancreatic cancer Monotherapy for whom? JL VAN LAETHEM, MD,PhD
 Adjuvant therapy in pancreatic cancer Monotherapy for whom? JL VAN LAETHEM, MD,PhD Efficacy Parameters in adjuvant monochemotherapy Randomized studies in resectable PDAC Regimen DFS HR (p) OS HR (p) 5-yr-OS
Adjuvant therapy in pancreatic cancer Monotherapy for whom? JL VAN LAETHEM, MD,PhD Efficacy Parameters in adjuvant monochemotherapy Randomized studies in resectable PDAC Regimen DFS HR (p) OS HR (p) 5-yr-OS
What Is The Optimal Adjuvant Therapy in Pancreatic Adenoca: Intensified Chemotherapy March 28 th, 2015
 What Is The Optimal Adjuvant Therapy in Pancreatic Adenoca: Intensified Chemotherapy March 28 th, 2015 Eileen M. O Reilly, M.D. Associate Director David M. Rubenstein Center Pancreatic Cancer Research
What Is The Optimal Adjuvant Therapy in Pancreatic Adenoca: Intensified Chemotherapy March 28 th, 2015 Eileen M. O Reilly, M.D. Associate Director David M. Rubenstein Center Pancreatic Cancer Research
De-Escalate Trial for the Head and neck NSSG. Dr Eleanor Aynsley Consultant Clinical Oncologist
 De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
Triple Negative Breast cancer New treatment options arenowhere?
 Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
ASCO Highlights Lung Cancer
 ASCO Highlights Lung Cancer Anne S. Tsao, M.D. Director, Mesothelioma Program Assistant Professor July 11, 2009 The University of Texas MD ANDERSON CANCER CENTER Department of Thoracic/Head & Neck Medical
ASCO Highlights Lung Cancer Anne S. Tsao, M.D. Director, Mesothelioma Program Assistant Professor July 11, 2009 The University of Texas MD ANDERSON CANCER CENTER Department of Thoracic/Head & Neck Medical
Esophageal Cancer. Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care. David Demos MD Thoracic Surgery Aurora Cancer Care
 Esophageal Cancer Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care David Demos MD Thoracic Surgery Aurora Cancer Care No Disclosures Learning Objectives Review the classification scheme
Esophageal Cancer Wesley A. Papenfuss MD FACS Surgical Oncology Aurora Cancer Care David Demos MD Thoracic Surgery Aurora Cancer Care No Disclosures Learning Objectives Review the classification scheme
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer
 Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Reference No: Author(s) 12/05/16. Approval date: committee. June Operational Date: Review:
 12/05/16. Approval date: committee. June Operational Date: Review:") Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Adenocarcinoma Dr Colin Purcell, Consultant Medical Oncologist & on behalf of the GI Oncologists Group, Cancer
Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Adenocarcinoma Dr Colin Purcell, Consultant Medical Oncologist & on behalf of the GI Oncologists Group, Cancer
Metronomic chemotherapy for breast cancer
 Metronomic chemotherapy for breast cancer M. Colleoni International Breast Cancer Study Group (IBCSG), Division of Medical Senology, European Institute of Oncology Metronomic Scheduling and Inhibition
Metronomic chemotherapy for breast cancer M. Colleoni International Breast Cancer Study Group (IBCSG), Division of Medical Senology, European Institute of Oncology Metronomic Scheduling and Inhibition
Surgical Management of Advanced Stage Colon Cancer. Nathan Huber, MD 6/11/14
 Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Recent advances in the management of metastatic breast cancer in older adults
 Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan
 State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Emerging Role of Immunotherapy in Head and Neck Cancer
 Emerging Role of Immunotherapy in Head and Neck Cancer Jared Weiss, MD Associate Professor of Medicine and Section Chief of Thoracic and Head/Neck Oncology UNC Lineberger Comprehensive Cancer Center Copyright
Emerging Role of Immunotherapy in Head and Neck Cancer Jared Weiss, MD Associate Professor of Medicine and Section Chief of Thoracic and Head/Neck Oncology UNC Lineberger Comprehensive Cancer Center Copyright
Combined Modality Therapy State of the Art. Everett E. Vokes The University of Chicago
 Combined Modality Therapy State of the Art Everett E. Vokes The University of Chicago What we Know Some patients are cured (20%) Induction and concurrent chemoradiotherapy are each superior to radiotherapy
Combined Modality Therapy State of the Art Everett E. Vokes The University of Chicago What we Know Some patients are cured (20%) Induction and concurrent chemoradiotherapy are each superior to radiotherapy
Immunotherapy in head and neck cancer and MSI in solid tumors
 Immunotherapy in head and neck cancer and MSI in solid tumors Brian Hunis, MD, MBA Associate Medical Director, Memorial Cancer Institute. Hollywood, FL »No disclosures Objectives»Discuss the role of immunology
Immunotherapy in head and neck cancer and MSI in solid tumors Brian Hunis, MD, MBA Associate Medical Director, Memorial Cancer Institute. Hollywood, FL »No disclosures Objectives»Discuss the role of immunology
S u p p o r t e d b y a n i n d e p e n d e n t E d u c a t i o n a l G r a n t f r o m B a y e r
 EXPERTS KNOWLEDGE SHARE with Prof. Köhne, Dr. Modest and Dr. Vecchione Madrid (Spain) Sunday September 10 th 2017 S u p p o r t e d b y a n i n d e p e n d e n t E d u c a t i o n a l G r a n t f r o m
EXPERTS KNOWLEDGE SHARE with Prof. Köhne, Dr. Modest and Dr. Vecchione Madrid (Spain) Sunday September 10 th 2017 S u p p o r t e d b y a n i n d e p e n d e n t E d u c a t i o n a l G r a n t f r o m
Current role of chemotherapy in hormone-naïve patients Elena Castro
 Current role of chemotherapy in hormone-naïve patients Elena Castro Spanish National Cancer Research Centre Lugano, 17 October 2017 Siegel, Ca Cancer J Clin,2017 Buzzoni, Eur Urol, 2015 -Aprox 15-20% of
Current role of chemotherapy in hormone-naïve patients Elena Castro Spanish National Cancer Research Centre Lugano, 17 October 2017 Siegel, Ca Cancer J Clin,2017 Buzzoni, Eur Urol, 2015 -Aprox 15-20% of
Current Standard of Care of Gastric Cancer:
 Current Standard of Care of Gastric Cancer: Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation of risk Treatment
Current Standard of Care of Gastric Cancer: Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation of risk Treatment
BRAF Testing In The Elderly: Same As in Younger Patients?
 EGFR, K-RAS, K BRAF Testing In The Elderly: Same As in Younger Patients? Nadine Jackson McCleary MD MPH Gastrointestinal Oncology Dana-Farber/Harvard Cancer Care Boston, MA, USA Outline Colorectal cancer
EGFR, K-RAS, K BRAF Testing In The Elderly: Same As in Younger Patients? Nadine Jackson McCleary MD MPH Gastrointestinal Oncology Dana-Farber/Harvard Cancer Care Boston, MA, USA Outline Colorectal cancer
The next wave of successful drug therapy strategies in HER2-positive breast cancer. Hans Wildiers University Hospitals Leuven Belgium
 The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the clinical
abcd Clinical Study for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the clinical
Is the Neo-adjuvant Approach Better than Adjuvant Approach? Comparative Levels of Evidence: Randomized Trials
 Is the Neo-adjuvant Approach Better than Approach? Virginie Westeel University Hospital Besançon, France Perspectives in Lung Cancer Amsterdam, 5-6 March 2010 Comparative Levels of Evidence: Randomized
Is the Neo-adjuvant Approach Better than Approach? Virginie Westeel University Hospital Besançon, France Perspectives in Lung Cancer Amsterdam, 5-6 March 2010 Comparative Levels of Evidence: Randomized
Hot Topic in tema di neoplasie del Colon: Durata ottimale della chemioterapia adiuvante nei tumori del Colon
 Convegno Nazionale AIOM Giovani 2018 News in Oncology Hot Topic in tema di neoplasie del Colon: Durata ottimale della chemioterapia adiuvante nei tumori del Colon Daniele Rossini U.O. di Oncologia Medica
Convegno Nazionale AIOM Giovani 2018 News in Oncology Hot Topic in tema di neoplasie del Colon: Durata ottimale della chemioterapia adiuvante nei tumori del Colon Daniele Rossini U.O. di Oncologia Medica
Chemoradiotherapy Versus Chemotherapy for Localized Gastric Cancer: A Mini Review
 www.rarediseasesjournal.com Journal of Rare Diseases Research & Treatment Mini-review Open Access Chemoradiotherapy Versus Chemotherapy for Localized Gastric Cancer: A Mini Review Daniel da Motta Girardi
www.rarediseasesjournal.com Journal of Rare Diseases Research & Treatment Mini-review Open Access Chemoradiotherapy Versus Chemotherapy for Localized Gastric Cancer: A Mini Review Daniel da Motta Girardi
Adjuvant therapy in older adults: controversies and challenges - Colorectal cancer -
 International Society of Geriatric Oncology Lisbon October 23 rd 25t h 2014 Adjuvant therapy in older adults: controversies and challenges - Colorectal cancer - Claus-Henning Köhne Klinik für Onkologie
International Society of Geriatric Oncology Lisbon October 23 rd 25t h 2014 Adjuvant therapy in older adults: controversies and challenges - Colorectal cancer - Claus-Henning Köhne Klinik für Onkologie
Esophageal and GEJ Cancers. Case Presentations
 Esophageal and GEJ Cancers Case Presentations Locally Advanced GEJ Cancer (Case 1) A 55 year old man with longstanding GERD presents with increasing solid food dysphagia. EGD reveals a 3 cm mass in the
Esophageal and GEJ Cancers Case Presentations Locally Advanced GEJ Cancer (Case 1) A 55 year old man with longstanding GERD presents with increasing solid food dysphagia. EGD reveals a 3 cm mass in the
Pre- Versus Post-operative Radiotherapy
 Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: James RD, Glynne-Jones R, Meadows HM, et al.
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: James RD, Glynne-Jones R, Meadows HM, et al.
DALLA CAPECITABINA AL TAS 102
 DALLA CAPECITABINA AL TAS 102 Milano 29 settembre 2016 LE PROSPETTIVE NELLA RICERCA Armando Santoro Humanitas Cancer Center THE 1,2.AND 3 LINE CHEMOTHERAPY IN CRC M BEVACIZUMAB AFLIBERCET RAS wt RAS mu
DALLA CAPECITABINA AL TAS 102 Milano 29 settembre 2016 LE PROSPETTIVE NELLA RICERCA Armando Santoro Humanitas Cancer Center THE 1,2.AND 3 LINE CHEMOTHERAPY IN CRC M BEVACIZUMAB AFLIBERCET RAS wt RAS mu
Incorporating biologics in the management of older patients with metastatic colorectal cancer
 Incorporating biologics in the management of older patients with metastatic colorectal cancer D Papamichael MB BS MD FRCP Cyprus Oncology Centre GSK Satellite Symposium SIOG APAC Singapore 12-13 July 2014
Incorporating biologics in the management of older patients with metastatic colorectal cancer D Papamichael MB BS MD FRCP Cyprus Oncology Centre GSK Satellite Symposium SIOG APAC Singapore 12-13 July 2014
Current Standard of Care of Gastro- Esophageal Cancer
 Current Standard of Care of Gastro- Esophageal Cancer Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation of risk
Current Standard of Care of Gastro- Esophageal Cancer Andrés Cervantes Professor of Medicine Classical approach to localised gastric cancer Surgical resection Pathology assessment and estimation of risk
Advances in Chemotherapy of Colorectal Cancer
 Advances in Chemotherapy of Colorectal Cancer Richard M. Goldberg Lineberger Comprehensive Cancer Center University of North Carolina at Chapel Hill Disease Settings Adjuvant Therapy MOSAIC, FOLFOX Andre
Advances in Chemotherapy of Colorectal Cancer Richard M. Goldberg Lineberger Comprehensive Cancer Center University of North Carolina at Chapel Hill Disease Settings Adjuvant Therapy MOSAIC, FOLFOX Andre
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221. Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS
 Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
Clinical Trials. Ovarian Cancer
 1.0 0.8 0.6 0.4 0.2 0.0 < 65 years old 65 years old Events Censored Total 128 56 184 73 35 108 0 12 24 36 48 60 72 84 27-10-2012 Ovarian Cancer Stuart M. Lichtman, MD Attending Physician 65+ Clinical Geriatric
1.0 0.8 0.6 0.4 0.2 0.0 < 65 years old 65 years old Events Censored Total 128 56 184 73 35 108 0 12 24 36 48 60 72 84 27-10-2012 Ovarian Cancer Stuart M. Lichtman, MD Attending Physician 65+ Clinical Geriatric