Risk Assessment and Reduction
|
|
|
- Magdalen Stevenson
- 5 years ago
- Views:
Transcription

1 Risk Assessment and Reduction Carol J. Fabian, M.D. Breast Cancer Prevention Program University of Kansas Medical Center Kansas City, KS School of Breast Oncology Atlanta, GA 2013
2 Outline Major and Minor Risk Factors Risk Models and Counseling Biomarkers for Risk Stratification Standard Risk Reduction Strategies Interventions Under Study
3 Risk Factors
4 Major Risk Factors Increase Risk >2 fold Minor Risk Factors Up to 2 Fold Major (>2 fold increase) Minor (>1<2 fold) Mutations associated hereditary cancer 1 st degree < age 60 Chest radiation <30 Pre-cancer (DCIS LCIS, AH) Prior breast or Ovarian Cancer Age >60 Early menarche Nullparity/ Late childbirth No lactation Late menopause 2 nd & 3 rd degree relatives Serum Sex Hormones/SHGB 5 years combined E+ P HRT Obesity Inactivity Serum Insulin/Growth Factors Alcohol

5 Variable Risk with Hormone Replacement
6 Breast Cancer Risk Hormone & Replacement 1. If oophorectomy no excess risk to age After 50 E+P HRT > Risk than E alone 2. E+ Progestins > Risk E+ Natural Progesterone 3. Risk Higher in Lean women 4. Risk Higher if start first 5-10 yrs after Menopause WHI no risk E alone vs inc Million Women 5. Excess risk dissipates within few years of stopping 6. No excess risk vaginal hormones Minimal Excess Risk to Age 60

7 What about HRT High Risk Women Who Undergo Oophorectomy < Age 45 ERT or combined HRT does not attenuate reduction in breast cancer risk in premenopausal women from hereditary breast cancer families undergoing oophorectomy. ERT/ HRT reduces risk of premature CVD oophorectomy < 45 Rebbeck JCO 2005; 23:7804 Domchek et al ASCO 2011 Abstract 1501
 Oophorectomy 35-45 : 2")


8 HRT Reduces Premature CVD Risk from Early Surgical Menopause (<45 ) Oophorectomy : 2 X increase CV death 2X Increase Parkinson s CVD risk? higher BRCA1 mutation carriers. HRT to age reduces excess CVD risk Nelson JAMA 2004;291:1610 Rivera 2009, Rocca 2007, Singh J Thoracic, CV Surg 2013
9 Risk Models and Counseling
10 Risk Assessment and Prevention Consultation Estimate long and short term risk of breast cancer Need for genetic testing Suggest surveillance based on risk Discuss benefits and side effects standard prevention approaches Discuss clinical trials
11 Gail Model (II) Considers Current age Age at menarche Age at first live birth Number of 1st degree relatives Number of biopsies Presence of Atypical Hyperplasia Race Good calibration and Validated in Screening Populations, but discriminatory accuracy is suboptimal ( C statistic ~.63) Rockhill JNCI 93:358, 2001 Tice Breast Cancer Res Treat 94:115, 2005 Gail et al. JNCI 81:1879, 1989, Costantino et al JNCI 91: 1541, 1999.
12 Problems with the Gail Model Cannot use to estimate risk women < age 35 Cannot use if woman has LCIS Does not consider 2 nd or 3 rd degree relatives Underestimates risk if + Paternal FH. Does not estimate risk of BRCA1/2 mutation Does not consider age at diagnosis. Does not consider ovarian cancer Does not consider BMI, age at menopause. Does not take into account preventive Rx

13 Tyrer Cuzick Model IBIS Risk Evaluator Tool
14 Tyrer Cuzick (IBIS) Pros and Cons Pros Estimates Risk if < 35 Estimates risk of BRCA1/2 Considers Factors Gail II Does Not. LCIS Height and Weight 2 nd and some 3 rd degree relatives Age of relatives diagnosis HRT use Ovarian Ca & Oophorectomy Age at menopause Cons Overestimates risk if patient has a dx of Atypical hyperplasia or LCIS and a + FH Does not take into account alcohol, physical activity Does not take into account SERM or AI use Tyrer et al Stat Med ; 23 : 1111 Boughey J CO 2010;28: 3591
15 Printout for Patient



16 We Still Have a Way to Go in the Area of Risk Prediction


17 Adding Biomarkers for Better Risk Prediction Breast Density RR=1 RR 4-5X SNPs and Germline Mutations
18
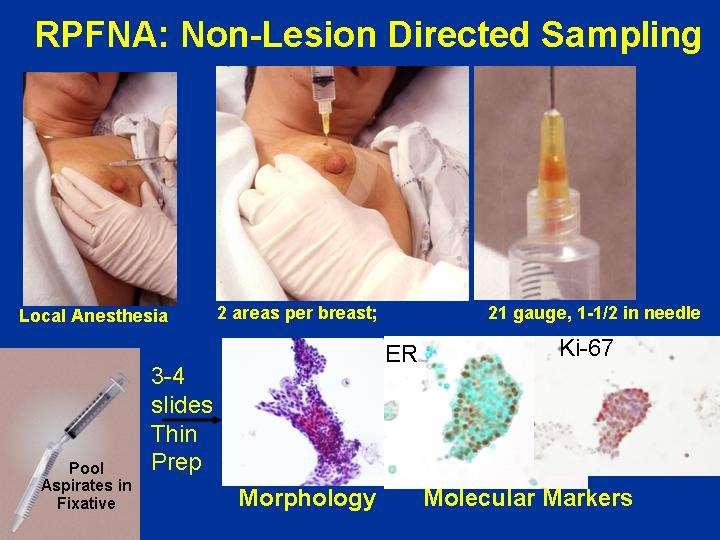
19 Cumulative Frequency, Percent RPFNA Atypia Increases Relative Risk of Breast Cancer by 5-Fold FNA Atypia (N=102) P< Total High Risk Cohort (N=480) 0 No FNA Atypia (N=378) Time from Entry on Study, months Fabian et al. J Natl Cancer Inst 92:1217, 2000.
20 Risk Reduction: Standard Approaches
21 Type of Prevention Intervention Should Vary With Risk Level 1) Prophylactic Surgery: Very High Risk 2) Anti-Hormones: High Risk 3) Lifestyle: Average to Moderate Risk
22 Surgical Risk Reduction Strategies For Very High Risk Women (BRCA1/2) Oophorectomy < age 45 risk by 50-70% even when women are given add back HRT Mastectomy ( risk by ~90%) Cost effective and likely to provide survival advantage Rebbeck et al. NEJM 346:1616, 2002; JCO 23:7804, 2005 Hartmann et al. NEJM 340:77, Warner et al J Clin Oncol. 2011;29: Grann et al Breast Cancer Res Treat :837
23 Decision Tool For BRCA1 and 2 Carriers Determines risk of development of breast cancer and ovarian cancer and death from those cancers by choice and timing of Breast imaging Mammography Breast MRI Prophylactic Oophorectomy Prophylactic Mastectomy Kurian JCO 2012;30:497
24 Relative Risk Reduction in Randomized Trials in Which Eligibility: 5 yr Gail Risk >1.6 or AH or LCIS Pre-menopausal Women (age 35 and over) Tamoxifen ( 50%) Postmenopausal Women Raloxifene (40%),Tamoxifen (50%),Exemestane (65%) Reduction after: AH 85%, LCIS 66%, DCIS ~ 40% Reduction ER+ but not ER- Cancer No Survival Advantage Fisher J NCI 1998; 90: 1371 Fisher Lancet. 1999;353:1993 Vogel Cancer Prev Res :681 Cuzick Lancet 2003; 361:296 Goss NEJM :2381
25 Meta Analysis SERMs for Prevention Individual patient data meta analysis suggest 38% reduction risk for breast cancer (Tamoxifen 33%) SERMs no effect on CV disease Continued effect 5-10 years Only reduces ER+ Cuzick et al Lancet 2013
26 Side Effects Of Preventive Agents Tamoxifen Hot Flashes, Vaginal Discharge Uterine surgery & cancer DVT, PE, Cataracts Raloxifene Hot Flashes, Vaginal Dryness DVT, PE Fisher J Natl Cancer Inst 90:1371,1998 Cuzick. Lancet 361:296, 2003 Vogel JAMA 295:2727,2006 Exemestane Hot Flashes Vaginal Dryness Joint & Muscle pain Bone Density Loss Fatigue Goss NEJM :2381


27 What Do We Know About Tamoxifen in Young Women BRCA Mutation Carriers 70% BRCA2 ER+ 30% BRCA1 ER+ Increases Ovarian Cysts Increases Estrogen Levels Decreases Bone Density Not Used Prevention < age 35 Very Little: Few BRCA mutation carriers in Primary Prevention trials Reduces contralateral ca adjuvant
28 Although Tamoxifen > Efficacy Than Raloxifene in the STAR Trial Raloxifene Often Drug of Choice in Postmenopausal Women With A Uterus Because of Fewer Side Effects. Tool Available to Help Define Benefits Freedman et al JCO 2011; 29: 2327
29 Tamoxifen or Raloxifene Contraindicated if Prior Deep Venous Thrombosis Prior Stroke Inherited Clotting Disorder
30 ASCO Guidelines Risk Reduction Counseling Update 2013 Tamoxifen should be discussed with a premenopausal or postmenopausal woman at increased risk for Breast Cancer with a 5 year Gail model or equivalent risk of >1.66 %. Do not monitor with pelvic sonos. Raloxifene or exemestane should be discussed in a postmenopausal woman with a 5 year Gail model or equivalent risk of >1.66 %. < 5% of risk eligible take any of the above Visvanathan et al JCO 2013
31 Hot Flash Free Interventions Under Study Weight Loss Metformin ASA Lignans Omega-3 FA Vitamin D Letrozole for Women on HRT Curcumin Polyphenols
 reduce risk?")
32 How Much Does Weight Loss Does it take to Reduce Breast Cancer Risk? Don t Know NHBL goal 10% general health although 5 % may benefit. Bariatric Surgery 20-30% loss reduces risk Does 5-10 % loss (usual with behavioral wt loss) reduce risk? Observational studies suggest 10% if maintained Sjostrom Lancet Oncol 2009 Teras Cancer Causes Control 2011, Byers Diabetes Obes Metab 2011 Sjostrom Arch Intern Med 1998

33 Phase II Prevention Trials With Tissue Biomarkers as Primary Endpoint Atypia No Atypia Intervention vs Placebo Ki- 67 >2% Ki-67<1%

34 Obesity Leads to Infiltration with macrophages Less adiponectin, more leptin Insulin Resistance More cytokines and inflammatory cell infiltration : TNF alpha, IL6, PAI1, HGF Activation mtor Survival Path motility, angiogenesis, apoptosis Elevated free hormones via aromatase & SHBG Increased Activation of Estrogen Receptor Crown Structures Khandskar Nat Ca Rev 2011, Subbaramaiah Cancer Prev Res 2011
35 Phase II Weight Loss Pilot Trial Design Supported by NCI R21 High Risk Women BMI >25 Kg/m 2 No HRT N=24 Screen for Serum and Tissue Risk Biomarkers RPFNA 6 Months Intervention Tissue Changes Decrease estrogen signaling ( ps2) Decrease tissue proliferation; Ki-67, Cyclin B1 Decrease mtor signaling (S6K) Increase Adiponectin: leptin ratio Fabian Breast Cancer Res Treat 2013 Median 11% Weight Loss Repeat Biomarkers RPFNA
36 Relative Difference, percent Biomarker Change Greater with >10% Weight Loss Adiponectin: Leptin Ratio * * * <10% BW Loss >10% BW Loss Significant change within group Adiponectin * * Leptin * IGF1:IGFBP3 Leptin Ratio * ** * * * * Insulin CRP HGF PAI-1 SHBG * Free E2 & Test -200
37 Reinforces Goal of 10% Loss for Cancer Risk Reduction Expense of Definitive Phase III Primary Prevention Trial May Prevent Ever Being Done

38 Key Components of Successful Behavioral Weight Loss Interventions Goal 10% Loss over 6 months Portion Control with Calorie Restriction Behavioral Modification Exercise Maintenance Encouragement by Physician

39 Metformin Reduces Insulin Resistance and is Associated with Modest Weight Loss Metformin Reduced Breast Cancer risk type II Diabetes ~ 5 % weight loss in diabetics, insulin resistance Being studied in adjuvant setting. Reduces Insulin and mtor Signaling
40 Biomarker Trial Metformin Only Effective in Women with Insulin Resistance 200 T1 3a Invasive BC Core Needle Biopsy R A N D O M I Z E Metformin 850 mg po daily for 3 and bid X 25 days Placebo daily for 3 and bid X 25 days S U R G E R Y Primary Outcome: Secondary Outcome: Change in Cancer/ADH Ki-67 Change in Ki-67 by HOMA Ki-67 No Change Overall Ki67 Lower HOMA>2.8 Higher HOMA<2.8 DeCensi et al Abstract # 519, Bonanni et al JCO 2012

41 Cohort Studies with ASA Suggest Benefit but not Randomized Trial Aspirin Iowa and Minnesota Cohort ( 26,000) 20-30% reduction regular use WHI observational same in higher risk women if dose >100 mg Randomized WHI 100 mg qod negative Bardia 2011, Harris 2003, Cook 2005
 Mammalian Lignans SDG Gut Bacteria")
 Used in Canada to treat")
42 Lignans Function as Natural Selective Estrogen Receptor Modulators Plant Lignan Secoisolariciresinol (SDG) Mammalian Lignans SDG Gut Bacteria Enterolactone Enterodiol Buffer effects of ER alpha Flaxseed Most Concentrated Source of SDG (100x other plants) Used in Canada to treat cylic mastalgia

43 12 Month Pilot Study in Premenopausal Women High Risk Women Low or undetectable baseline lignan levels with 10 fold increase at 6,12 mos Minimal to no side effects. Decrease in Ki-67 over 12 months in majority. Significant decrease in proportion of women with Atypia Placebo Controlled multicenter trial ongoing Pre-Study Change Ki-67 Ki67 p=.0001 P<.0001 Post-Study Fabian et al. Cancer Prevention Res 2010
44 Omega-3 Fatty Acids Replace Pro-inflammatory Omega 6 Fatty Acids in Cell Membranes Being Studied Phase II mg EPA + DHA/day recommended for heart health Animal and correlative studies reduced breast cancer risk but probably at higher doses ( ~3.5 grams) Brasky Ca Epi Biomarkers Prev 2010; 19:1696.
45 Incidence of Atypia, percent 6 Months of DHA + EPA 3.4 g/d Improved Cytomorphology & Proliferation Premenopausal Reduction in % with RPFNA Atypia N=34 77% p= % Reduction in Follicular Phase Ki-67 (%) Ki-67 % N= P=.021 p= Pre-Study Post-Study 0 Pre-omega Pre-Study Post- Post-Study omega Pre-omega Post- omega Favorably modulated proteins associated with MAPK, PI3K, mtor Fabian et al Abstract 1515 ASCO 2013





46 Sun Vitamin D: Important Autocrine Role in Breast Homeostasis Vitamin D Sequestered in FAT Liver Prohormone 25(OH)D Breast 1-α hydroxylase Active hormone 1,25(OH) 2 D Ca++ transport-lactation, Buffers Action Hormones Growth Factors
47 Phase III Studies of Vitamin D for Prevention in Postmenopausal Women Study Type Prevention Menopause Status Vitamin D 3 Dose/day WHI negative Primary Post 400 IU (+ Calcium 1000) Lappe Positive Vital Ongoing Primary Post 1000 IU (+ Calcium 1000) Primary Post > IU + 1gm Omega-3 FA Chlebowski JNCI 2008; 100:1581, Lappe Am J Clin Nutr 2007; 85:1586, Chlebowski JNCI 2008; 100:1581, Lappe Am J Clin Nutr 2007; 85:1586

48 Optimal 25OH D Levels for Breast Health may be Higher than the 32 ng/ml for Bone 50% reduction at 52 ng/ml vs 6ng/ml Quintile Median Values Modified from Garland et al. Steroid Biochem Molec Biol, 2007.

49 Future Prevention: Personalized Medicine Risk and Biology Based Recommendations Biomarkers: Risk, Type of Intervention Likely to Work and Response Increased Emphasis on Healthy behaviors and Natural Products Save Strong Antihormonal agents for Higher Risk
50 END
51 The Million Women Study, Lancet 2003, J NCI 2011, E3N Fournier 2008 Nurses Health Study NEJM 1997, WHI Health Consequences HRT after 50 Large Cohort Studies (50s) Breast Cancer Risk Estrogen Alone; up to 30% relative increase at 10 yrs Estrogen + Progestin; up to 2X relative increase at 10 yrs Higher in lean women and 1 st 5 years after menopause Excess gone after stop 4 years Cardiovascular Risk 20-30% decrease CV deaths ERT starting 40s-50s WHI Randomized Trial (60s) Breast Cancer Risk Estrogen ( CEE) alone no increase /decrease risk 8 years Estrogen + Progestin ~ 25% increase in risk at 5 years Risk higher in women starting within first 10 yrs of menopause Excess gone after stop 2-3 years Cardiovascular Risk Decrease CV ERT starting in 50s. Increased CV events starting oral E or E+P HRT in 60s

52 Excess Breast Ca Risk with HRT for Woman in her 50s Woman in her 60s WHI: None if ERT or 5yrs E+P HRT and no prior E+P HRT. No increase CV events Million Women: ERT 1.5 extra breast ca/ extra breast ca /1000 women 5 yrs E+P HRT WHI: None if 8 yrs ERT but increase if 5 yrs E+P Increase CV events Million Women: ERT1.5 extra breast ca/ extra breast ca/1000 women 5 yrs E+P HRT.



53 Low Dose Vaginal Hormones No Increased Risk for Breast Cancer Testosterone 1-2 % + Estriol 2 mg every other day. Estrogen rings, creams or inserts Beral Million Women Study Lancet 2003
54 Breast Cancer and Health Risks in Average Risk Women Starting HRT after 50
55 Transdermal Estradiol less CV risk than Cardiovascular Less risk probable with transdermal formulations because less likely than oral to cause blood clots. Breast Cancer Oral CEE alone no increased risk WHI. Transdermal estradiol ~ 30 % excess 10 yrs continuous use in Million Women study. Oral CEE? Fournier Breast Ca Res & Treat 2008; 107: 103, Beral Million Women Study

56 Relative Risk Associated with FH (Compared to those without FH) By Age 1 st degree DX Under 40: tripling of relative risk 40-50: doubling of relative risk 50-65: increase by 1.5 (50%) > 65: little increase Cuzick Breast Cancer 2008; 10 :S13
57 Minor Risk Lifestyle Factors : < 2 Fold Relative Risk but Important For Population Risk Alcohol: Increase relative risk (RR) by 10%/drink/day Estrogen +Progestin Replacement therapy: Increase in RR by 5% per yr of current use (1.25 after five years) Estrogen Alone Replacement Therapy 0-2% increase in RR per year of current use Postmenopausal Obesity:30% increase in RR BMI >30 vs BMI < 25 kg/m 2 Sedentary Lifestyle:25-30% increase in RR no exercise vs 3 hours per week.
58 Major Factors Absolute & Relative Risk Per Year BRCA 1/2 > 30 DCIS Breast XRT<30 LCIS AH + Family HX AH Prior Inv Cancer Age > 60 (vs 30) 2% 2% 2% 1% 1% 0.5% 0.75% 0.33% 20 x 20x 20x 10x 8-10x 4-5x 5-8x 10x

59 Natural Progesterone with Estradiol (E2) May Be Less Risky than Progestins + E2 Estrogen and Progestins > breast tissue proliferation than estrogen + natural progesterone. Baseline Transdermal E2 + MPA French Cohort Study: estradiol + natural progesterone did not increase risk of breast cancer Baseline Transdermal E2 + Progesterone Murkes Fertility and Sterility : Fournier Breast Ca Res & Treat 2008; 107: 103



60 Ongoing Lignan Randomized Phase II Clinical Trial Integrated with Phase II-III Animal Trial Fabian, MD Premenopausal Women SDG 50 mg/d or Placebo 1 yr Biomarkers in Benign Breast Tissue/Blood 1. Response: Ki-67, cytomorphology 2. Mechanism: qrtpcr estrogen response genes, Proteomics: activated MAPK, mtor, Cytokines 3. Follicular reserve Petroff, DVM, PhD Hursting, PhD ER+ Rat/Ovarian SDG or Placebo ER- WNT transgenic mouse Change in Biomarkers 3 mos Cancer Incidence Komen for the Cure Promise Grant KG101039

61 Less than 5 % of Risk Eligible Women Take Tamoxifen for Primary Prevention Perceived education problem Those with the most counseling least likely to take. Concerns: QOL/ side effects Since no survival advantage still very much a patient choice. Waters CEBP 2010 ; Ropka JCO 2010; 28: 3090
62 Phase II Prevention Trials To Test for Risk Biomarker Effect Screen for Risk Biomarker to be Primary Endpoint for trial R A N D O M I Z E Placebo* vs Study Agent 6-12 Months * For Pilots Placebo arm is deleted Repeat Biomarkers




63 Change in Proliferation, ER & Activation, Cytomorphology Normal Hyperplasia Atypia In Situ Cancer Ki-67 Ki-67 <1% 2-15% Relative Risk 2X 5X 10X 100 ER



64 Need IU Vitamin D/ Day to Maintain Serum 25OH D in the ng/ml optimal range. Phase II Trials Ongoing 8oz Milk =100IU Salmon= 400 IU Total body sun exposure to minimal erythema = 10,000 IU
Increased Risk of Breast Cancer: Screening and Prevention. Elizabeth Pritchard, MD 4/5/2017
 Increased Risk of Breast Cancer: Screening and Prevention Elizabeth Pritchard, MD 4/5/2017 No disclosures Defining Risk Risk Factors Modifiable Lifestyle obesity physical activity alcohol consumption breast
Increased Risk of Breast Cancer: Screening and Prevention Elizabeth Pritchard, MD 4/5/2017 No disclosures Defining Risk Risk Factors Modifiable Lifestyle obesity physical activity alcohol consumption breast
Chemo-endocrine prevention of breast cancer
 Chemo-endocrine prevention of breast cancer Andrea DeCensi, MD Division of Medical Oncology Ospedali Galliera, Genova; Division of Cancer Prevention and Genetics, European Institute of Oncology, Milano;
Chemo-endocrine prevention of breast cancer Andrea DeCensi, MD Division of Medical Oncology Ospedali Galliera, Genova; Division of Cancer Prevention and Genetics, European Institute of Oncology, Milano;
Risk Assessment, Genetics, and Prevention
 Risk Assessment, Genetics, and Prevention Katherine D. Crew, MD MS Director, Clinical Breast Cancer Prevention Program Columbia University Medical Center 1 Outline Breast cancer risk factors Hereditary
Risk Assessment, Genetics, and Prevention Katherine D. Crew, MD MS Director, Clinical Breast Cancer Prevention Program Columbia University Medical Center 1 Outline Breast cancer risk factors Hereditary
Breast Cancer Prevention for the Population at Large
 Breast Cancer Prevention for the Population at Large Jack Cuzick Centre for Cancer Prevention Wolfson Institute of Preventive Medicine St Bartholomew s Medical School Queen Mary University of London London,
Breast Cancer Prevention for the Population at Large Jack Cuzick Centre for Cancer Prevention Wolfson Institute of Preventive Medicine St Bartholomew s Medical School Queen Mary University of London London,
Breast Cancer Risk Assessment and Prevention
 Breast Cancer Risk Assessment and Prevention Katherine B. Lee, MD, FACP October 4, 2017 STATISTICS More than 252,000 cases of breast cancer will be diagnosed this year alone. About 40,000 women will die
Breast Cancer Risk Assessment and Prevention Katherine B. Lee, MD, FACP October 4, 2017 STATISTICS More than 252,000 cases of breast cancer will be diagnosed this year alone. About 40,000 women will die
RALOXIFENE Generic Brand HICL GCN Exception/Other RALOXIFENE EVISTA Is the request for the prevention (risk reduction) of breast cancer?
 of breast cancer?") Generic Brand HICL GCN Exception/Other RALOXIFENE EVISTA 16917 GUIDELINES FOR USE 1. Is the request for the prevention (risk reduction) of breast cancer? If yes, continue to #2. If no, approve by HICL
Generic Brand HICL GCN Exception/Other RALOXIFENE EVISTA 16917 GUIDELINES FOR USE 1. Is the request for the prevention (risk reduction) of breast cancer? If yes, continue to #2. If no, approve by HICL
Breast Cancer. Dr. Andres Wiernik 2017
 Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Breast Cancer Prevention Studies. Key Points. Breast cancer prevention studies are clinical trials (research studies conducted with
 CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Breast Cancer Prevention
CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s Breast Cancer Prevention
Spectrum of Care Options for Women at High Risk for Breast and Ovarian Cancer
 Spectrum of Care Options for Women at High Risk for Breast and Ovarian Cancer Sheryl G.A. Gabram, MD, MBA, FACS Professor of Surgery, Emory University Director, High Risk Assessment Program Winship Cancer
Spectrum of Care Options for Women at High Risk for Breast and Ovarian Cancer Sheryl G.A. Gabram, MD, MBA, FACS Professor of Surgery, Emory University Director, High Risk Assessment Program Winship Cancer
POSITION PAPER FOR HEALTH CARE PROVIDERS Use of Pharmacologic Intervention for Breast Cancer Risk Reduction
 P.O. Box 30195 Lansing, MI 48909 Phone: 877-588-6224 FAX: 517-335-9397 www.michigancancer.org Introduction POSITION PAPER FOR HEALTH CARE PROVIDERS Use of Pharmacologic Intervention for Breast Cancer Risk
P.O. Box 30195 Lansing, MI 48909 Phone: 877-588-6224 FAX: 517-335-9397 www.michigancancer.org Introduction POSITION PAPER FOR HEALTH CARE PROVIDERS Use of Pharmacologic Intervention for Breast Cancer Risk
HBOC Syndrome A review of BRCA 1/2 testing, Cancer Risk Assessment, Counseling and Beyond.
 HBOC Syndrome A review of BRCA 1/2 testing, Cancer Risk Assessment, Counseling and Beyond. Conni Murphy, ARNP Cancer Risk Assessment and Genetics Program Jupiter Medical Center Learning Objectives Identify
HBOC Syndrome A review of BRCA 1/2 testing, Cancer Risk Assessment, Counseling and Beyond. Conni Murphy, ARNP Cancer Risk Assessment and Genetics Program Jupiter Medical Center Learning Objectives Identify
Prophylactic Mastectomy State of the Art
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 6 th Brazilian Breast Cancer Conference Sao Paulo, Brazil 9 March 2012 Prophylactic Mastectomy State of the Art Monica Morrow
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 6 th Brazilian Breast Cancer Conference Sao Paulo, Brazil 9 March 2012 Prophylactic Mastectomy State of the Art Monica Morrow
Breast Cancer: Selected Topics for the Primary Care Clinician
 Breast Cancer: Selected Topics for the Primary Care Clinician Leah Karliner, MD MAS October 2009 Primary Care Medicine: Principles and Practice OUTLINE Incidence and Mortality Risk Factors and Risk Reduction/Prevention
Breast Cancer: Selected Topics for the Primary Care Clinician Leah Karliner, MD MAS October 2009 Primary Care Medicine: Principles and Practice OUTLINE Incidence and Mortality Risk Factors and Risk Reduction/Prevention
So, Who are the appropriate individuals that should consider genetic counseling and genetic testing?
 Hello, I m Banu Arun, Professor of Breast Medical Oncology and Co-Director of Clinical Cancer Genetics at the University of Texas MD Anderson Cancer Center. Today I will be discussing with you Hereditary
Hello, I m Banu Arun, Professor of Breast Medical Oncology and Co-Director of Clinical Cancer Genetics at the University of Texas MD Anderson Cancer Center. Today I will be discussing with you Hereditary
OBJECTIVES 8/25/2017. An attempt to organize the chaos
 High Risk for Breast Cancer and Genetics: Who? What? Where? When? An attempt to organize the chaos Presented at Winds of Change Conference November 3, 2017 by Carol Hager, MSN, CRNP and Allison Haener,
High Risk for Breast Cancer and Genetics: Who? What? Where? When? An attempt to organize the chaos Presented at Winds of Change Conference November 3, 2017 by Carol Hager, MSN, CRNP and Allison Haener,
Breast Cancer: Key Issues for the Non-Oncologist
 Breast Cancer: Key Issues for the Non-Oncologist I have no financial disclosures I developed and validated one of the models that will be discussed. I hold no patents and derive no financial benefit from
Breast Cancer: Key Issues for the Non-Oncologist I have no financial disclosures I developed and validated one of the models that will be discussed. I hold no patents and derive no financial benefit from
Patient Education. Breast Cancer Prevention. Cancer Center
 Patient Education Breast cancer affects one in nine women in the US by the time they reach their 80 s. It is the result of several mutations or alterations in the genes found in the DNA of normal breast
Patient Education Breast cancer affects one in nine women in the US by the time they reach their 80 s. It is the result of several mutations or alterations in the genes found in the DNA of normal breast
Host Factors that Increase Breast Cancer Risk
 Host Factors that Increase Breast Cancer Risk 30 th Annual Miami Breast Cancer Conference March 7-10, 2013 Debu Tripathy, MD Professor of Medicine University of Southern California Norris Comprehensive
Host Factors that Increase Breast Cancer Risk 30 th Annual Miami Breast Cancer Conference March 7-10, 2013 Debu Tripathy, MD Professor of Medicine University of Southern California Norris Comprehensive
Lifestyle Factors and Cancer Survivorship: Observational Findings of Weight, Physical Activity, and Diet on Survival
 Lifestyle Factors and Cancer Survivorship: Observational Findings of Weight, Physical Activity, and Diet on Survival Melinda L. Irwin, PhD, MPH Associate Professor of Epidemiology Yale School of Medicine
Lifestyle Factors and Cancer Survivorship: Observational Findings of Weight, Physical Activity, and Diet on Survival Melinda L. Irwin, PhD, MPH Associate Professor of Epidemiology Yale School of Medicine
Case 1. BREAST CANCER From Diagnosis to Treatment: The Role of Primary Care
 BREAST CANCER From Diagnosis to Treatment: The Role of Primary Care Leah Karliner, MD MAS University of California San Francisco Primary Care Medicine Update 2009 April 2009 Case 1 AR, a 60 year old African
BREAST CANCER From Diagnosis to Treatment: The Role of Primary Care Leah Karliner, MD MAS University of California San Francisco Primary Care Medicine Update 2009 April 2009 Case 1 AR, a 60 year old African
Breast density: imaging, risks and recommendations
 Breast density: imaging, risks and recommendations Maureen Baxter, MD Radiologist Director of Ruth J. Spear Breast Center Providence St. Vincent Medical Center Alison Conlin, MD/MPH Medical Oncologist
Breast density: imaging, risks and recommendations Maureen Baxter, MD Radiologist Director of Ruth J. Spear Breast Center Providence St. Vincent Medical Center Alison Conlin, MD/MPH Medical Oncologist
Breast Cancer. Breast Cancer. Established breast cancer risk factors. Established breast cancer risk factors. Cancer incidence.
 Breast Cancer A buffet of breast cancer topics Wendy Y. Chen, MD MPH Dana-Farber Cancer Institute Brigham and Women s Hospital Disclosures: none Not related to anything presented in this lecture Wendy
Breast Cancer A buffet of breast cancer topics Wendy Y. Chen, MD MPH Dana-Farber Cancer Institute Brigham and Women s Hospital Disclosures: none Not related to anything presented in this lecture Wendy
Effective Health Care Program
 Comparative Effectiveness Review Number 17 Effective Health Care Program Comparative Effectiveness of Medications To Reduce Risk of Primary Breast Cancer in Women Executive Summary Background Breast cancer
Comparative Effectiveness Review Number 17 Effective Health Care Program Comparative Effectiveness of Medications To Reduce Risk of Primary Breast Cancer in Women Executive Summary Background Breast cancer
New Insights into Breast Cancer Risk Reduction
 New Insights into Breast Cancer Risk Reduction November 10, 2013 Rowan T. Chlebowski Professor of Medicine David Geffen School of Medicine at UCLA Chief, Division of Medical Oncology and Hematology Harbor-UCLA
New Insights into Breast Cancer Risk Reduction November 10, 2013 Rowan T. Chlebowski Professor of Medicine David Geffen School of Medicine at UCLA Chief, Division of Medical Oncology and Hematology Harbor-UCLA
BSO, HRT, and ERT. No relevant financial disclosures
 BSO, HRT, and ERT Jubilee Brown, MD Professor & Associate Director, Gynecologic Oncology Levine Cancer Institute at the Carolinas HealthCare System Charlotte, North Carolina No relevant financial disclosures
BSO, HRT, and ERT Jubilee Brown, MD Professor & Associate Director, Gynecologic Oncology Levine Cancer Institute at the Carolinas HealthCare System Charlotte, North Carolina No relevant financial disclosures
Disclosure Information Relationships Relevant to this Session
 Disclosure Information Relationships Relevant to this Session DeCensi, Andrea No relevant relationships to disclose. Please note, all disclosures are reported as submitted to ASCO, and are always available
Disclosure Information Relationships Relevant to this Session DeCensi, Andrea No relevant relationships to disclose. Please note, all disclosures are reported as submitted to ASCO, and are always available
BREAST CANCER RISK REDUCTION
 BREAST CANCER RISK REDUCTION Clinical Practice Guideline Update Introduction ASCO published its first breast cancer risk reduction (BCRR) guideline in 1999 ASCO Guidelines are updated at intervals by an
BREAST CANCER RISK REDUCTION Clinical Practice Guideline Update Introduction ASCO published its first breast cancer risk reduction (BCRR) guideline in 1999 ASCO Guidelines are updated at intervals by an
BREAST CANCER. Dawn Hershman, MD MS. Medicine and Epidemiology Co-Director, Breast Program HICCC Columbia University Medical Center.
 BREAST CANCER Dawn Hershman, MD MS Florence Irving Assistant Professor of Medicine and Epidemiology Co-Director, Breast Program HICCC Columbia University Medical Center Background Breast cancer is the
BREAST CANCER Dawn Hershman, MD MS Florence Irving Assistant Professor of Medicine and Epidemiology Co-Director, Breast Program HICCC Columbia University Medical Center Background Breast cancer is the
Current Strategies in the Detection of Breast Cancer. Karla Kerlikowske, M.D. Professor of Medicine & Epidemiology and Biostatistics, UCSF
 Current Strategies in the Detection of Breast Cancer Karla Kerlikowske, M.D. Professor of Medicine & Epidemiology and Biostatistics, UCSF Outline ν Screening Film Mammography ν Film ν Digital ν Screening
Current Strategies in the Detection of Breast Cancer Karla Kerlikowske, M.D. Professor of Medicine & Epidemiology and Biostatistics, UCSF Outline ν Screening Film Mammography ν Film ν Digital ν Screening
Ms. Y. Outline. Updates of SERMs and Estrogen
 Ms. Y Updates of SERMs and Estrogen Steven R. Cummings, MD, FACP San Francisco Coordinating Center CPMC Research Institute and UCSF Support from Lilly, Pfizer, Berlex 55 y.o. woman with mild hypertension
Ms. Y Updates of SERMs and Estrogen Steven R. Cummings, MD, FACP San Francisco Coordinating Center CPMC Research Institute and UCSF Support from Lilly, Pfizer, Berlex 55 y.o. woman with mild hypertension
Breast Cancer Screening and High Risk
 Breast Cancer Screening and High Risk Mary Freyvogel, DO Breast Surgeon Clinical Assistant Professor of Surgery University Hospitals Case Medical Center St. John Medical Center / Elyria Medical Center
Breast Cancer Screening and High Risk Mary Freyvogel, DO Breast Surgeon Clinical Assistant Professor of Surgery University Hospitals Case Medical Center St. John Medical Center / Elyria Medical Center
Qamar J. Khan Bruce F. Kimler Pavan S. Reddy Priyanka Sharma Jennifer R. Klemp Carol J. Fabian
 The VITAL trial Randomized trial of vitamin D3 to prevent worsening of musculoskeletal symptoms and fatigue in women with breast cancer starting adjuvant letrozole. Qamar J. Khan Bruce F. Kimler Pavan
The VITAL trial Randomized trial of vitamin D3 to prevent worsening of musculoskeletal symptoms and fatigue in women with breast cancer starting adjuvant letrozole. Qamar J. Khan Bruce F. Kimler Pavan
Hereditary breast cancer who to refer to a cancer genetics clinic and how to counsel patients with
 Hereditary breast cancer who to refer to a cancer genetics clinic and how to counsel patients with positive and negative results? SAMO Workshop Luzern 3./4.10.2014 Dr. med. Barbara Bolliger TumorTumor-
Hereditary breast cancer who to refer to a cancer genetics clinic and how to counsel patients with positive and negative results? SAMO Workshop Luzern 3./4.10.2014 Dr. med. Barbara Bolliger TumorTumor-
Gynecologic Care for Breast Cancer Survivors. Case
 Gynecologic Care for Breast Cancer Survivors Mindy Goldman, MD Clinical Professor Dept. of Ob/Gyn and Reproductive Sciences Director, Women s Cancer Care Program, UCSF Breast Care Center and Women s Health
Gynecologic Care for Breast Cancer Survivors Mindy Goldman, MD Clinical Professor Dept. of Ob/Gyn and Reproductive Sciences Director, Women s Cancer Care Program, UCSF Breast Care Center and Women s Health
LOBULAR CARCINOMA IN SITU: WHAT DOES IT MEAN? THE SURGEON'S PERSPECTIVE
 : WHAT DOES IT MEAN? THE SURGEON'S PERSPECTIVE Benjamin O. Anderson, M.D. Director, Breast Health Clinic Professor of Surgery and Global Health, University of Washington Joint Member, Fred Hutchinson Cancer
: WHAT DOES IT MEAN? THE SURGEON'S PERSPECTIVE Benjamin O. Anderson, M.D. Director, Breast Health Clinic Professor of Surgery and Global Health, University of Washington Joint Member, Fred Hutchinson Cancer
Post-menopausal hormone replacement therapy. Evan Klass, MD May 17, 2018
 Post-menopausal hormone replacement therapy Evan Klass, MD May 17, 2018 Are we really still talking about this? Are we really still talking about this? 1960-1975- estrogen prescriptions doubled. Pharma
Post-menopausal hormone replacement therapy Evan Klass, MD May 17, 2018 Are we really still talking about this? Are we really still talking about this? 1960-1975- estrogen prescriptions doubled. Pharma
Development, validation and application of risk prediction models
 Development, validation and application of risk prediction models G. Colditz, E. Liu, M. Olsen, & others (Ying Liu, TA) 3/28/2012 Risk Prediction Models 1 Goals Through examples, class discussion, and
Development, validation and application of risk prediction models G. Colditz, E. Liu, M. Olsen, & others (Ying Liu, TA) 3/28/2012 Risk Prediction Models 1 Goals Through examples, class discussion, and
Inherited Breast and Ovarian Cancer: 20 Years of Progress and Future Directions
 Inherited Breast and Ovarian Cancer: 20 Years of Progress and Future Directions Noah D. Kauff, MD, FACOG Director, Clinical Cancer Genetics Duke Cancer Institute / Duke University Health System Disclosures
Inherited Breast and Ovarian Cancer: 20 Years of Progress and Future Directions Noah D. Kauff, MD, FACOG Director, Clinical Cancer Genetics Duke Cancer Institute / Duke University Health System Disclosures
Breast cancer is the most frequently
 Charmaine Kim-Sing, MBChB, FRCPC, Lorna Weir, MD, FRCPC, and Urve Kuusk, MD, FRCPC Breast cancer risk management for moderaterisk and high-risk women An accurate assessment of breast cancer risk can help
Charmaine Kim-Sing, MBChB, FRCPC, Lorna Weir, MD, FRCPC, and Urve Kuusk, MD, FRCPC Breast cancer risk management for moderaterisk and high-risk women An accurate assessment of breast cancer risk can help
A Slow Starvation: Adjuvant Endocrine Therapy of Breast Cancer
 A Slow Starvation: Adjuvant Endocrine Therapy of Breast Cancer Dr. Susan Ellard Surgical Oncology Update October 24, 2009 Disclosure slide Participant in various meetings or advisory boards sponsored by
A Slow Starvation: Adjuvant Endocrine Therapy of Breast Cancer Dr. Susan Ellard Surgical Oncology Update October 24, 2009 Disclosure slide Participant in various meetings or advisory boards sponsored by
Extended Hormonal Therapy
 Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
Evaluations & CE Credits
 Evaluations & CE Credits Nursing Contact Hours, CME and CHES credits are available. Please visit www.phlive.org to fill out your evaluation and complete the post-test. 1 Breast Density and Breast Cancer
Evaluations & CE Credits Nursing Contact Hours, CME and CHES credits are available. Please visit www.phlive.org to fill out your evaluation and complete the post-test. 1 Breast Density and Breast Cancer
Breast Cancer Prevention
 Breast Cancer Prevention TREVOR J. POWLES Royal Marsden NHS Trust, and Institute of Cancer Research, London, United Kingdom Key Words. Breast cancer Chemoprevention Tamoxifen Raloxifene ABSTRACT Epidemiological,
Breast Cancer Prevention TREVOR J. POWLES Royal Marsden NHS Trust, and Institute of Cancer Research, London, United Kingdom Key Words. Breast cancer Chemoprevention Tamoxifen Raloxifene ABSTRACT Epidemiological,
Evaluation & Management of PowerPoint Cover Title. the High Risk Population. High Risk Clinic
 Evaluation & Management of PowerPoint Cover Title the High Risk Population High Risk Clinic Subtitle Joanna Would Springman, Go Here PA-C Assessment Genetics Known genetic mutation Family history with
Evaluation & Management of PowerPoint Cover Title the High Risk Population High Risk Clinic Subtitle Joanna Would Springman, Go Here PA-C Assessment Genetics Known genetic mutation Family history with
BREAST CANCER AND BONE HEALTH
 BREAST CANCER AND BONE HEALTH Rowena Ridout, MD, FRCPC Toronto Western Hospital Osteoporosis Program University Health Network / Mount Sinai Hospital rowena.ridout@uhn.ca None to declare Conflicts of Interest
BREAST CANCER AND BONE HEALTH Rowena Ridout, MD, FRCPC Toronto Western Hospital Osteoporosis Program University Health Network / Mount Sinai Hospital rowena.ridout@uhn.ca None to declare Conflicts of Interest
WEIGHING UP THE RISKS OF HRT. Department of Endocrinology Chris Hani Baragwanath Academic Hospital
 WEIGHING UP THE RISKS OF HRT V. Nicolaou Department of Endocrinology Chris Hani Baragwanath Academic Hospital Background Issues surrounding post menopausal hormonal therapy (PMHT) are complex given: Increased
WEIGHING UP THE RISKS OF HRT V. Nicolaou Department of Endocrinology Chris Hani Baragwanath Academic Hospital Background Issues surrounding post menopausal hormonal therapy (PMHT) are complex given: Increased
Chemoprevention for Breast Cancer
 Ann Surg Oncol (2015) 22:3230 3235 DOI 10.1245/s10434-015-4715-9 ORIGINAL ARTICLE BREAST ONCOLOGY Chemoprevention for Breast Cancer Sandhya Pruthi, MD 1, Ruth E. Heisey, MD 2, and Therese B. Bevers, MD
Ann Surg Oncol (2015) 22:3230 3235 DOI 10.1245/s10434-015-4715-9 ORIGINAL ARTICLE BREAST ONCOLOGY Chemoprevention for Breast Cancer Sandhya Pruthi, MD 1, Ruth E. Heisey, MD 2, and Therese B. Bevers, MD
SOFTly: The Long Natural History of [Trials for] [premenopausal] ER+ Breast Cancer
![SOFTly: The Long Natural History of [Trials for] [premenopausal] ER+ Breast Cancer](/thumbs/95/125806264.jpg "SOFTly: The Long Natural History of [Trials for] [premenopausal] ER+ Breast Cancer") SOFTly: The Long Natural History of [Trials for] [premenopausal] ER+ Breast Cancer Charles Moertel Lecture May 12, 2017 Gini Fleming Charles Moertel Founder of NCCTG Dedication to high quality clinical
SOFTly: The Long Natural History of [Trials for] [premenopausal] ER+ Breast Cancer Charles Moertel Lecture May 12, 2017 Gini Fleming Charles Moertel Founder of NCCTG Dedication to high quality clinical
Extended Adjuvant Endocrine Therapy
 Extended Adjuvant Endocrine Therapy After all, 5 years Tamoxifen works.. For women with ER+ primary breast cancer, previous studies have shown that treatment with tamoxifen for 5 years has a carry-over
Extended Adjuvant Endocrine Therapy After all, 5 years Tamoxifen works.. For women with ER+ primary breast cancer, previous studies have shown that treatment with tamoxifen for 5 years has a carry-over
High Risk or High Reward: Breast Cancer Prevention and Screening in Primary Care: New Challenges and Opportunities
 High Risk or High Reward: Breast Cancer Prevention and Screening in Primary Care: New Challenges and Opportunities Section 1 Jamie Stern, MD, MPH: Mammography in the 40s and 50s: the Data and the Controversy
High Risk or High Reward: Breast Cancer Prevention and Screening in Primary Care: New Challenges and Opportunities Section 1 Jamie Stern, MD, MPH: Mammography in the 40s and 50s: the Data and the Controversy
Research. Breast cancer represents a major
 Research GENERAL GYNECOLOGY Gynecologic conditions in participants in the NSABP breast cancer prevention study of tamoxifen and raloxifene (STAR) Carolyn D. Runowicz, MD; Joseph P. Costantino, DrPH; D.
Research GENERAL GYNECOLOGY Gynecologic conditions in participants in the NSABP breast cancer prevention study of tamoxifen and raloxifene (STAR) Carolyn D. Runowicz, MD; Joseph P. Costantino, DrPH; D.
Outline. Estrogens and SERMS The forgotten few! How Does Estrogen Work in Bone? Its Complex!!! 6/14/2013
 Outline Estrogens and SERMS The forgotten few! Clifford J Rosen MD rosenc@mmc.org Physiology of Estrogen and estrogen receptors Actions of estrogen on bone BMD, fracture, other off target effects Cohort
Outline Estrogens and SERMS The forgotten few! Clifford J Rosen MD rosenc@mmc.org Physiology of Estrogen and estrogen receptors Actions of estrogen on bone BMD, fracture, other off target effects Cohort
HORMONE THERAPY A BALANCED VIEW?? Prof Greta Dreyer
 HORMONE THERAPY A BALANCED VIEW?? Prof Greta Dreyer -- PART 1 -- Definitions HRT hormone replacement therapy HT genome therapy ERT estrogen replacement therapy ET estrogen EPT estrogen progesterone therapy
HORMONE THERAPY A BALANCED VIEW?? Prof Greta Dreyer -- PART 1 -- Definitions HRT hormone replacement therapy HT genome therapy ERT estrogen replacement therapy ET estrogen EPT estrogen progesterone therapy
Prevention of Breast Cancer in Postmenopausal Women: Approaches to Estimating and Reducing Risk
 ARTICLE Prevention of Breast Cancer in Postmenopausal Women: Approaches to Estimating and Reducing Risk Steven R. Cummings, Jeffrey A. Tice, Scott Bauer, Warren S. Browner, Jack Cuzick, Elad Ziv, Victor
ARTICLE Prevention of Breast Cancer in Postmenopausal Women: Approaches to Estimating and Reducing Risk Steven R. Cummings, Jeffrey A. Tice, Scott Bauer, Warren S. Browner, Jack Cuzick, Elad Ziv, Victor
Manejo do câncer de mama RH+ na adjuvância: o que há de novo?
 II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico Manejo do câncer de mama RH+ na adjuvância: o que há de novo? INGRID A. MAYER, MD, MSCI Assistant Professor of Medicine Director,
II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico Manejo do câncer de mama RH+ na adjuvância: o que há de novo? INGRID A. MAYER, MD, MSCI Assistant Professor of Medicine Director,
Low-Fat Dietary Pattern Intervention Trials for the Prevention of Breast and Other Cancers
 Low-Fat Dietary Pattern Intervention Trials for the Prevention of Breast and Other Cancers Ross Prentice Fred Hutchinson Cancer Research Center and University of Washington AICR, November 5, 2009 Outline
Low-Fat Dietary Pattern Intervention Trials for the Prevention of Breast and Other Cancers Ross Prentice Fred Hutchinson Cancer Research Center and University of Washington AICR, November 5, 2009 Outline
Update in Breast Cancer Screening
 Disclosure information: Update in Breast Cancer Screening Karla Kerlikowske, MDDis Update in Breast Cancer Screening Grant/Research support from: National Cancer Institute - and - Karla Kerlikowske, MD
Disclosure information: Update in Breast Cancer Screening Karla Kerlikowske, MDDis Update in Breast Cancer Screening Grant/Research support from: National Cancer Institute - and - Karla Kerlikowske, MD
The Study of Tamoxifen and Raloxifene (STAR): Questions and Answers. Key Points
: Questions and Answers. Key Points") CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s The Study of Tamoxifen
CANCER FACTS N a t i o n a l C a n c e r I n s t i t u t e N a t i o n a l I n s t i t u t e s o f H e a l t h D e p a r t m e n t o f H e a l t h a n d H u m a n S e r v i c e s The Study of Tamoxifen
SERMS, Hormone Therapy and Calcitonin
 SERMS, Hormone Therapy and Calcitonin Tiffany Kim, MD Clinical Fellow VA Advanced Women s Health UCSF Endocrinology and Metabolism I have nothing to disclose Thanks to Clifford Rosen and Steven Cummings
SERMS, Hormone Therapy and Calcitonin Tiffany Kim, MD Clinical Fellow VA Advanced Women s Health UCSF Endocrinology and Metabolism I have nothing to disclose Thanks to Clifford Rosen and Steven Cummings
Lifestyle Risk Factors and Cancer Prevention
 February 3-5, 2016 Lansdowne Resort, Leesburg, VA Lifestyle Risk Factors and Cancer Prevention Melinda L. Irwin, PhD, MPH Professor of Epidemiology, Yale School of Public Health, Associate Director (Population
February 3-5, 2016 Lansdowne Resort, Leesburg, VA Lifestyle Risk Factors and Cancer Prevention Melinda L. Irwin, PhD, MPH Professor of Epidemiology, Yale School of Public Health, Associate Director (Population
J Clin Oncol 29: by American Society of Clinical Oncology INTRODUCTION
 VOLUME 29 NUMBER 17 JUNE 10 2011 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Benefit/Risk Assessment for Breast Cancer Chemoprevention With Raloxifene or Tamoxifen for Women Age 50 Years or
VOLUME 29 NUMBER 17 JUNE 10 2011 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Benefit/Risk Assessment for Breast Cancer Chemoprevention With Raloxifene or Tamoxifen for Women Age 50 Years or
Radiation and DCIS. The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging
 Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
Physical Activity & Cancer What We Know, What We Don t Know. Anne McTiernan, MD, PhD Fred Hutchinson Cancer Research Center Seattle, WA
 Physical Activity & Cancer What We Know, What We Don t Know Anne McTiernan, MD, PhD Fred Hutchinson Cancer Research Center Seattle, WA What We Know Extensive epidemiologic research on relationship between
Physical Activity & Cancer What We Know, What We Don t Know Anne McTiernan, MD, PhD Fred Hutchinson Cancer Research Center Seattle, WA What We Know Extensive epidemiologic research on relationship between
Karen degenevieve MSN, FNP, BC
 Karen degenevieve MSN, FNP, BC Become more comfortable treating common breast complaints. Discuss recent controversial screening recommendations. Discuss oral medications used in breast cancer prevention
Karen degenevieve MSN, FNP, BC Become more comfortable treating common breast complaints. Discuss recent controversial screening recommendations. Discuss oral medications used in breast cancer prevention
Emerging Approaches for (Neo)Adjuvant Therapy for ER+ Breast Cancer
Adjuvant Therapy for ER+ Breast Cancer") Emerging Approaches for (Neo)Adjuvant Therapy for E+ Breast Cancer Cynthia X. Ma, M.D., Ph.D. Associate Professor of Medicine Washington University in St. Louis Outline Current status of adjuvant endocrine
Emerging Approaches for (Neo)Adjuvant Therapy for E+ Breast Cancer Cynthia X. Ma, M.D., Ph.D. Associate Professor of Medicine Washington University in St. Louis Outline Current status of adjuvant endocrine
Kathryn M. Rexrode, MD, MPH. Assistant Professor. Division of Preventive Medicine Brigham and Women s s Hospital Harvard Medical School
 Update: Hormones and Cardiovascular Disease in Women Kathryn M. Rexrode, MD, MPH Assistant Professor Division of Preventive Medicine Brigham and Women s s Hospital Harvard Medical School Overview Review
Update: Hormones and Cardiovascular Disease in Women Kathryn M. Rexrode, MD, MPH Assistant Professor Division of Preventive Medicine Brigham and Women s s Hospital Harvard Medical School Overview Review
FAQ-Protocol 3. BRCA mutation carrier guidelines Frequently asked questions
 ULast updated: 09/02/2015 Protocol 3 BRCA mutation carrier guidelines Frequently asked questions UQ: How accurate are the remaining lifetime and 5 year breast cancer risks in the table? These figures are
ULast updated: 09/02/2015 Protocol 3 BRCA mutation carrier guidelines Frequently asked questions UQ: How accurate are the remaining lifetime and 5 year breast cancer risks in the table? These figures are
Breast Cancer Risk Assessment: Genetics, Risk Models, and Screening. Amie Hass, MSN, ARNP, FNP-BC Hall-Perrine Cancer Center
 Breast Cancer Risk Assessment: Genetics, Risk Models, and Screening Amie Hass, MSN, ARNP, FNP-BC Hall-Perrine Cancer Center Disclosure- I DO NOT HAVE any relevant financial interest with any entity producing,
Breast Cancer Risk Assessment: Genetics, Risk Models, and Screening Amie Hass, MSN, ARNP, FNP-BC Hall-Perrine Cancer Center Disclosure- I DO NOT HAVE any relevant financial interest with any entity producing,
Breast Cancer: Weight and Exercise. Anne McTiernan, MD, PhD. Fred Hutchinson Cancer Research Center Seattle, WA
 Breast Cancer: Weight and Exercise Anne McTiernan, MD, PhD Fred Hutchinson Cancer Research Center Seattle, WA Associations of Obesity with Overall & Breast Cancer Specific Survival Survival Obese vs. Non-obese
Breast Cancer: Weight and Exercise Anne McTiernan, MD, PhD Fred Hutchinson Cancer Research Center Seattle, WA Associations of Obesity with Overall & Breast Cancer Specific Survival Survival Obese vs. Non-obese
MENOPAUSE. I have no disclosures 10/11/18 OBJECTIVES WHAT S NEW? WHAT S SAFE?
 MENOPAUSE WHAT S NEW? WHAT S SAFE? I have no disclosures Sara Whetstone, MD, MHS OBJECTIVES To describe risks of HT by age and menopause onset To recommend specific HT regimen for women who undergo early
MENOPAUSE WHAT S NEW? WHAT S SAFE? I have no disclosures Sara Whetstone, MD, MHS OBJECTIVES To describe risks of HT by age and menopause onset To recommend specific HT regimen for women who undergo early
Learning Objectives. Peri menopause. Menopause Overview. Recommendation grading categories
 Learning Objectives Identify common symptoms of the menopause transition Understand the risks and benefits of hormone replacement therapy (HRT) Be able to choose an appropriate hormone replacement regimen
Learning Objectives Identify common symptoms of the menopause transition Understand the risks and benefits of hormone replacement therapy (HRT) Be able to choose an appropriate hormone replacement regimen
Endocrine Therapy in Premenopausal Breast Cancer. Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology, PA US Oncology
 Endocrine Therapy in Premenopausal Breast Cancer Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology, PA US Oncology Ovarian Ablation or Suppression vs. Not in ER + or ER UK Breast Cancer
Endocrine Therapy in Premenopausal Breast Cancer Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology, PA US Oncology Ovarian Ablation or Suppression vs. Not in ER + or ER UK Breast Cancer
4/13/2010. Silverman, Buchanan Breast, 2003
 Tailoring Breast Cancer Treatment: Has Personalized Medicine Arrived? Judith Luce, M.D. San Francisco General Hospital Avon Comprehensive Breast Care Center Outline First, treatment of DCIS Sorting risk
Tailoring Breast Cancer Treatment: Has Personalized Medicine Arrived? Judith Luce, M.D. San Francisco General Hospital Avon Comprehensive Breast Care Center Outline First, treatment of DCIS Sorting risk
Metastatic Breast Cancer What is new? Subtypes and variation?
 Metastatic Breast Cancer What is new? Subtypes and variation? Anne Blaes, MD, MS University of Minnesota, Division of Hematology/Oncology Director, Adult Cancer Survivor Program Current estimates for metastatic
Metastatic Breast Cancer What is new? Subtypes and variation? Anne Blaes, MD, MS University of Minnesota, Division of Hematology/Oncology Director, Adult Cancer Survivor Program Current estimates for metastatic
The Latest Research: Hormonal Therapies
 The Latest Research: Hormonal Therapies Sameer Gupta, M.D., M.P.H 9/29/2018 Attending Physician, Hematology/Oncology Bryn Mawr Hospital Clinical Assistant Professor, Jefferson Medical College Disclosures
The Latest Research: Hormonal Therapies Sameer Gupta, M.D., M.P.H 9/29/2018 Attending Physician, Hematology/Oncology Bryn Mawr Hospital Clinical Assistant Professor, Jefferson Medical College Disclosures
W3C Life Sciences: Clinical Observations Interoperability: EMR + Clinical Trials Use-case for EMR + Clinical Trials Interoperability
 W3C Life Sciences: Clinical Observations Interoperability: EMR + Clinical Trials Use-case for EMR + Clinical Trials Interoperability Background: The key issue is to investigate whether some of the data
W3C Life Sciences: Clinical Observations Interoperability: EMR + Clinical Trials Use-case for EMR + Clinical Trials Interoperability Background: The key issue is to investigate whether some of the data
Breast Cancer Treatment, Outcomes and Recent Advances. Ogori N Kalu, MD, MS Director Breast Surgery-UH Asst. Prof of Surgery Rutgers NJ Med School
 Breast Cancer Treatment, Outcomes and Recent Advances Ogori N Kalu, MD, MS Director Breast Surgery-UH Asst. Prof of Surgery Rutgers NJ Med School National Statistics 1 in 8 women in the U.S. (12-13%) will
Breast Cancer Treatment, Outcomes and Recent Advances Ogori N Kalu, MD, MS Director Breast Surgery-UH Asst. Prof of Surgery Rutgers NJ Med School National Statistics 1 in 8 women in the U.S. (12-13%) will
Update in Breast Cancer Screening
 Disclosure information: Update in Breast Cancer Screening Karla Kerlikowske, MDDis Update in Breast Cancer Screening Grant/Research support from: National Cancer Institute and Grail - and - Karla Kerlikowske,
Disclosure information: Update in Breast Cancer Screening Karla Kerlikowske, MDDis Update in Breast Cancer Screening Grant/Research support from: National Cancer Institute and Grail - and - Karla Kerlikowske,
Follow-up Issues for Early Stage Breast Cancer: The Role of Surveillance and Long-Term Care
 Follow-up Issues for Early Stage Breast Cancer: The Role of Surveillance and Long-Term Care Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of
Follow-up Issues for Early Stage Breast Cancer: The Role of Surveillance and Long-Term Care Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of
MANAGEMENT OF HIGH RISK BREAST PATIENTS DR PAMELA THOMPSON BREAST PHYSICIAN, FSH
 MANAGEMENT OF HIGH RISK BREAST PATIENTS DR PAMELA THOMPSON BREAST PHYSICIAN, FSH HIGH RISK MANAGEMENT OBJECTIVES Be alert to FHx Breast and/or Ovarian cancer Know how to perform a risk assessment Be aware
MANAGEMENT OF HIGH RISK BREAST PATIENTS DR PAMELA THOMPSON BREAST PHYSICIAN, FSH HIGH RISK MANAGEMENT OBJECTIVES Be alert to FHx Breast and/or Ovarian cancer Know how to perform a risk assessment Be aware
LET S START WITH (AND REMEMBER WE ARE TALKING ABOUT LOCAL E2) THERAPUTIC AGENTS: ARE THEY SAFE? Systemic HT/ET. Ospemifene. Local Estrogen Therapy
 THERAPUTIC AGENTS: ARE THEY SAFE? Systemic HT/ET. Ospemifene. Local Estrogen Therapy") THERAPUTIC AGENTS: ARE THEY SAFE? Steven R. Goldstein, M.D. Professor of Obstetrics & Gynecology New York University School of Medicine Director of Gynecologic Ultrasound Co-Director of Bone Densitometry
THERAPUTIC AGENTS: ARE THEY SAFE? Steven R. Goldstein, M.D. Professor of Obstetrics & Gynecology New York University School of Medicine Director of Gynecologic Ultrasound Co-Director of Bone Densitometry
AN EXAMINATION OF CANADIAN FAMILY PHYSICIANS KNOWLEDGE AND PRACTICE PATTERNS REGARDING BREAST CANCER PREVENTION
 AN EXAMINATION OF CANADIAN FAMILY PHYSICIANS KNOWLEDGE AND PRACTICE PATTERNS REGARDING BREAST CANCER PREVENTION by Mary-Kathryn Tighe A thesis submitted to the Department of Community Health and Epidemiology
AN EXAMINATION OF CANADIAN FAMILY PHYSICIANS KNOWLEDGE AND PRACTICE PATTERNS REGARDING BREAST CANCER PREVENTION by Mary-Kathryn Tighe A thesis submitted to the Department of Community Health and Epidemiology
Victoria Seewaldt, M.D. Duke University
 A211102 Testing for Atypia in Random Periareolar Fine Needle Aspiration (RPFNA) Cytology after 12 months Metformin Chemoprevention versus Placebo Control Victoria Seewaldt, M.D. Duke University Pre-registration
A211102 Testing for Atypia in Random Periareolar Fine Needle Aspiration (RPFNA) Cytology after 12 months Metformin Chemoprevention versus Placebo Control Victoria Seewaldt, M.D. Duke University Pre-registration
Chemoprevention of breast cancer for women at hgh risk
 Thomas Jefferson University Jefferson Digital Commons Department of Medicine Faculty Papers Department of Medicine December 2006 Chemoprevention of breast cancer for women at hgh risk Kathryn Chan Thomas
Thomas Jefferson University Jefferson Digital Commons Department of Medicine Faculty Papers Department of Medicine December 2006 Chemoprevention of breast cancer for women at hgh risk Kathryn Chan Thomas
Hereditary Breast and Ovarian Cancer Rebecca Sutphen, MD, FACMG
 Hereditary Breast and Ovarian Cancer 2015 Rebecca Sutphen, MD, FACMG Among a consecutive series of 11,159 women requesting BRCA testing over one year, 3874 responded to a mailed survey. Most respondents
Hereditary Breast and Ovarian Cancer 2015 Rebecca Sutphen, MD, FACMG Among a consecutive series of 11,159 women requesting BRCA testing over one year, 3874 responded to a mailed survey. Most respondents
Jill Stopfer, MS, CGC Abramson Cancer Center University of Pennsylvania
 Jill Stopfer, MS, CGC Abramson Cancer Center University of Pennsylvania Aging Family history Early menarche Late menopause Nulliparity Estrogen / Progesterone use after menopause More than two alcoholic
Jill Stopfer, MS, CGC Abramson Cancer Center University of Pennsylvania Aging Family history Early menarche Late menopause Nulliparity Estrogen / Progesterone use after menopause More than two alcoholic
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, for early-stage triple-negative breast cancer, 740 742 in older early-stage breast cancer patients, 790 795 anti-her2-directed
Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, for early-stage triple-negative breast cancer, 740 742 in older early-stage breast cancer patients, 790 795 anti-her2-directed
Women s Health: Managing Menopause. Jane S. Sillman, MD Assistant Professor of Medicine Harvard Medical School
 Women s Health: Managing Menopause Jane S. Sillman, MD Assistant Professor of Medicine Harvard Medical School Disclosures I have no conflicts of interest. Learning Objectives 1. Apply strategies to help
Women s Health: Managing Menopause Jane S. Sillman, MD Assistant Professor of Medicine Harvard Medical School Disclosures I have no conflicts of interest. Learning Objectives 1. Apply strategies to help
Breast Disease: What PCPs Need to Know. Eunice Cho MD FACS
 Breast Disease: What PCPs Need to Know Eunice Cho MD FACS New Breast Cancer Screening Guideline for women with average risk Every other year AGE 40 AGE 45 AGE 55 AGE 55 + Talk with your doctor about when
Breast Disease: What PCPs Need to Know Eunice Cho MD FACS New Breast Cancer Screening Guideline for women with average risk Every other year AGE 40 AGE 45 AGE 55 AGE 55 + Talk with your doctor about when
Hormonal Therapies for Breast Cancer. Westmead Breast Cancer Institute
 Hormonal Therapies for Breast Cancer Westmead Breast Cancer Institute Hormonal (endocrine) therapies for breast cancer (also called anti-hormone treatment ) Hormonal therapy is used to treat breast cancers
Hormonal Therapies for Breast Cancer Westmead Breast Cancer Institute Hormonal (endocrine) therapies for breast cancer (also called anti-hormone treatment ) Hormonal therapy is used to treat breast cancers
UPDATE: Women s Health Issues
 UPDATE: Women s Health Issues Renee B. Alexis, MD, MBA, MPH, FACOG Associate Professor Department of OBGYN Kiran C. Patel College of Osteopathic Medicine Disclosure of Conflicts of Interest I have no financial
UPDATE: Women s Health Issues Renee B. Alexis, MD, MBA, MPH, FACOG Associate Professor Department of OBGYN Kiran C. Patel College of Osteopathic Medicine Disclosure of Conflicts of Interest I have no financial
FATTORI DI RISCHIO e STILI DI VITA. Alessandra Modena Oncologia Medica Ospedale Sacro Cuore Don Calabria, Negrar Direttore: Dott. S.
 FATTORI DI RISCHIO e STILI DI VITA Alessandra Modena Oncologia Medica Ospedale Sacro Cuore Don Calabria, Negrar Direttore: Dott. S. Gori Risk factors for breast cancer Singletary SE et al., Ann Surg 2003
FATTORI DI RISCHIO e STILI DI VITA Alessandra Modena Oncologia Medica Ospedale Sacro Cuore Don Calabria, Negrar Direttore: Dott. S. Gori Risk factors for breast cancer Singletary SE et al., Ann Surg 2003
SAMPLE REPORT. Order Number: PATIENT. Age: 40 Sex: F MRN:
 Patient: Age: 40 Sex: F MRN: SAMPLE PATIENT Order Number: Completed: Received: Collected: SAMPLE REPORT Progesterone ng/ml 0.34 0.95 21.00 DHEA-S mcg/dl Testosterone ng/ml 48 35 0.10 0.54 0.80 430 Sex
Patient: Age: 40 Sex: F MRN: SAMPLE PATIENT Order Number: Completed: Received: Collected: SAMPLE REPORT Progesterone ng/ml 0.34 0.95 21.00 DHEA-S mcg/dl Testosterone ng/ml 48 35 0.10 0.54 0.80 430 Sex
Breast Cancer Risk Reduction
 Clinical in Oncology Breast Cancer Risk Reduction V.1.2008 Continue www.nccn.org Panel Members * Therese B. Bevers, MD/Chair Þ The University of Texas M.D. Anderson Cancer Center Mary Gemignani, MD Memorial
Clinical in Oncology Breast Cancer Risk Reduction V.1.2008 Continue www.nccn.org Panel Members * Therese B. Bevers, MD/Chair Þ The University of Texas M.D. Anderson Cancer Center Mary Gemignani, MD Memorial
MANAGEMENT OF DENSE BREASTS. Nichole K Ingalls, MD, MPH NW Surgical Specialists September 25, 2015
 MANAGEMENT OF DENSE BREASTS Nichole K Ingalls, MD, MPH NW Surgical Specialists September 25, 2015 No financial disclosures National Cancer Institute National Cancer Institute Increased Cancer Risk... DENSITY
MANAGEMENT OF DENSE BREASTS Nichole K Ingalls, MD, MPH NW Surgical Specialists September 25, 2015 No financial disclosures National Cancer Institute National Cancer Institute Increased Cancer Risk... DENSITY
Follow-up Care of Breast Cancer Patients
 Follow-up Care of Breast Cancer Patients Dr. Simon D. Baxter, MD, FRCPC Medical Oncologist BC Cancer Kelowna Clinical Instructor, Dept of Medicine University of British Columbia 24 November 2018 Disclosures
Follow-up Care of Breast Cancer Patients Dr. Simon D. Baxter, MD, FRCPC Medical Oncologist BC Cancer Kelowna Clinical Instructor, Dept of Medicine University of British Columbia 24 November 2018 Disclosures
Outline of the presentation
 Outline of the presentation Breast cancer subtypes and classification Clinical need in estrogen-positive (ER+) metastatic breast cancer (mbc) Sulforaphane and SFX-01: the preclinical evidence STEM Phase
Outline of the presentation Breast cancer subtypes and classification Clinical need in estrogen-positive (ER+) metastatic breast cancer (mbc) Sulforaphane and SFX-01: the preclinical evidence STEM Phase
Breast Cancer Risk Assessment among Bahraini Women. Majida Fikree, MD, MSc* Randah R Hamadeh, BSc, MSc, D Phil (Oxon)**
**") Bahrain Medical Bulletin, Vol. 35, No.1, March 2013 Breast Cancer Risk Assessment among Bahraini Women Majida Fikree, MD, MSc* Randah R Hamadeh, BSc, MSc, D Phil (Oxon)** Objective: To estimate breast
Bahrain Medical Bulletin, Vol. 35, No.1, March 2013 Breast Cancer Risk Assessment among Bahraini Women Majida Fikree, MD, MSc* Randah R Hamadeh, BSc, MSc, D Phil (Oxon)** Objective: To estimate breast
Hormone. Free Androgen Index. 2-Hydroxyestrone. Reference Range. Hormone. Estrone Ratio. Free Androgen Index
 Hormonal Health PATIENT: Sample Report TEST REF: TST-12345 Hormonal Health 0.61 0.30-1.13 ng/ml DHEA-S 91 35-430 mcg/dl tient: SAMPLE TIENT e: x: N: Sex Binding Globulin 80 18-114 nmol/l Testosterone 0.34
Hormonal Health PATIENT: Sample Report TEST REF: TST-12345 Hormonal Health 0.61 0.30-1.13 ng/ml DHEA-S 91 35-430 mcg/dl tient: SAMPLE TIENT e: x: N: Sex Binding Globulin 80 18-114 nmol/l Testosterone 0.34