Ηπατοκυτταρικός Καρκίνος Συστηματική Θεραπεία. Θωμάς Μακατσώρης Επίκ. Καθ. Παθολογίας-Ογκολογίας Ιατρική Σχολή Πανεπιστημίου Πατρών 11/5/2018
|
|
|
- Jonah Francis
- 5 years ago
- Views:
Transcription
1 Ηπατοκυτταρικός Καρκίνος Συστηματική Θεραπεία Θωμάς Μακατσώρης Επίκ. Καθ. Παθολογίας-Ογκολογίας Ιατρική Σχολή Πανεπιστημίου Πατρών 11/5/2018
2 Advisory Board Disclosures Roche, Boeringer, Sanofi, Astra Zeneca, Genesis Honoraria Roche, Sanofi, Amgen, Merck, BMS, Gilead
3
4
5
6
7
8
9 Phase III SHARP Study: Sorafenib vs Placebo in Advanced HCC Stratified by macroscopic vascular invasion and/or extrahepatic spread; ECOG PS; geographical region Pts with advanced HCC, Child-Pugh A, at least 1 untreated lesion, ECOG PS 2, no previous systemic treatment, life expectancy 12 wks (N = 602) Sorafenib 400 mg PO BID, continuous dosing (n = 299) Placebo 2 tablets PO BID, continuous dosing (n = 303) Primary endpoints: OS, time to symptomatic progression Secondary endpoint: TTP (independent review), disease control rate, safety Llovet JM, et al. N Engl J Med. 2008;359: Kane RC, et al. Oncologist. 2009;14:
10 Probability of Survival SHARP: OS, TTP OS P < Mos Since Randomization Llovet JM, et al. N Engl J Med. 2008;359: Sorafenib Placebo Probability of No Symptomatic Progression Probability of Radiologic Progression Time to Symptomatic Progression P = Time to Radiologic Progression P < Mos Since Randomization Slide credit: clinicaloptions.com
11 SHARP: Efficacy Outcome Llovet JM, et al. N Engl J Med. 2008;359: Sorafenib (n = 299) Placebo (n = 303) HR (95% CI) P Value Median OS, mos ( ) < % CI yr OS, % Median TTP (symptomatic), mos 95% CI ( ).77 Median TTP (radiologic), mos ( ) < % CI Level of response, % CR 0 0 NA PR SD Disease-control rate, %
12
13 Sorafenib in Advanced HCC (GIDEON): OS by Child-Pugh Status at Study Entry Survival Distribution Function Median OS, Mos (95% CI) Child-Pugh A (< 7) (n = 726): 10.3 ( days) Child-Pugh B (7-9) (n = 219): 4.8 ( days) Child-Pugh C (> 9) (n = 12): 2.0 (46-94 days) Days Since Start of Treatment Daniele B, et al. ASCO Abstract Slide credit: clinicaloptions.com
14 Phase III STORM: OS With Adjuvant Sorafenib for HCC After Resection or Ablation Sorafenib (n = 556) Placebo (n = 558) OS (%) Pts at Risk, n Placebo Sorafenib Bruix J, et al. Lancet Oncol. 2015;16: HR: (95% CI: ; 1-sided P =.48) Mos Slide credit: clinicaloptions.com
15
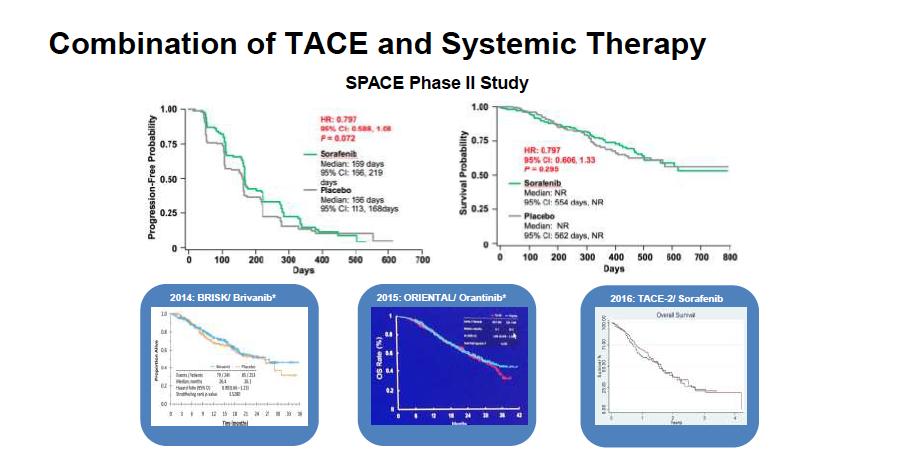
16 TACE With Doxorubicin Beads ± Sorafenib in Intermediate-Stage HCC (Phase III SPACE) Progression Probability MVI/EHS Probability TTP (Central Review) HR: P =.072 Sorafenib Median: 169 days Placebo Median: 166 days Days 1.00 Time to MVI/EHS Sorafenib Median: NR Placebo Median: NR HR: P = Days Lencioni R, et al. J Hepatol. 2016;64: Survival Probability UnTACEable Progression Probability Sorafenib Median: NR OS 0.25 Placebo HR: Median: NR P = Days 1.00 Time to UnTACEable Progression HR: P =.999 Sorafenib Median: 95 days Placebo Median: 224 days Sorafenib (n = 154) Placebo (n = 153) Days Slide credit: clinicaloptions.com
17
18 Lenvatinib: Mechanism of Action Multitargeted, oral small molecular TKI Potent against VEGFR2 and VEGFR3 Also targets VEGFR1, FGFR1-3, PDGFRα, RET, and KIT O N O CI H N O H N VEGFR Lenvatinib RAS RAF MEK T202/Y204 P ERK1/2 P T421/S424 S235/S236 FGFR X PI3K AKT mtor P S6K P S6 T389 H 2 N O Angiogenesis Finn RS, et al. ASCO Abstract TPS4153.
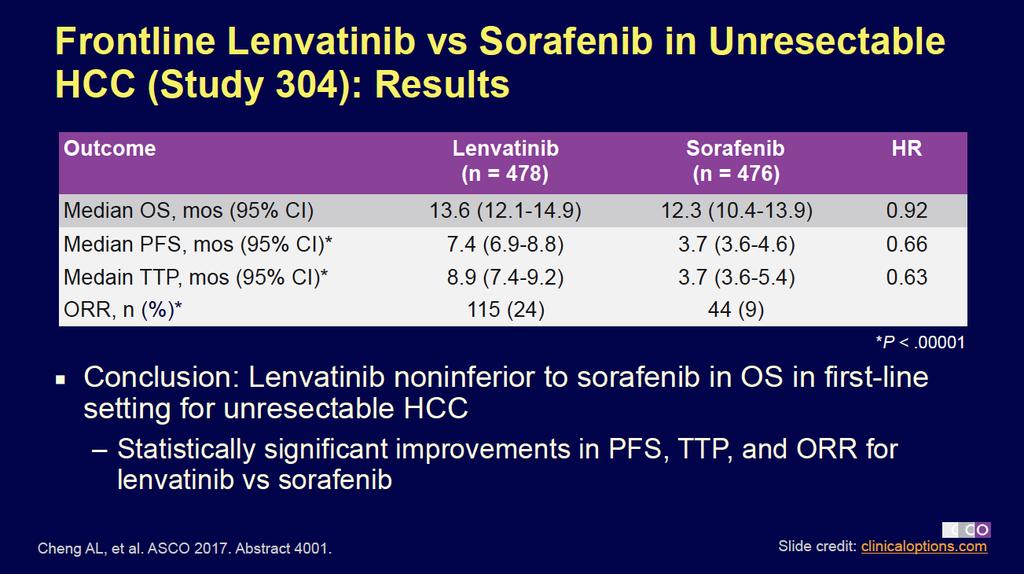
19 Phase III Study 304: Frontline Lenvatinib vs Sorafenib in Unresectable HCC Randomized, open-label noninferiority phase III trial Pts with unresectable, previously untreated HCC, Child-Pugh A, ECOG PS 0-1 (N = 954) Lenvatinib 8 mg or 12 mg* QD (n = 478) Sorafenib 400 mg PO BID (n = 476) *Based on body weight. Treat until progression or toxicity Primary endpoint: OS Secondary endpoints: PFS, TTP, ORR, PK, QoL ClinicalTrials.gov. NCT Cheng AL, et al. ASCO Abstract 4001.
20
21

22
23 Regorafenib: Oral Multikinase Inhibitor Targeting Multiple Tumor Pathways Cl F F F N H O N H F O N O Regorafenib N H Biochemical Activity Mean Regorafenib IC 50, nmol/l ± SD Tests, n VEGFR1 13 ± Murine VEGFR2 4.2 ± Murine VEGFR3 46 ± 10 4 TIE2 311 ± 46 4 PDGFR-β 22 ± 3 2 Inhibition of proliferation KIT PDGFR RET Inhibition of tumor microenvironment signaling PDGFR-β FGFR Inhibition of neoangiogenesis VEGFR1-3 TIE2 1. Wilhelm SM, et al. Int J Cancer. 2011;129: Mross K, et al. Clin Cancer Res. 2012;18: Strumberg D, et al. Expert Opin Investig Drugs. 2012;21: FGFR1 202 ± 18 6 KIT 7 ± 2 4 RET 1.5 ± RAF ± B-RAF 28 ± 10 6 B-RAF V600E 19 ± 6 6 Slide credit: clinicaloptions.com
24 Sorafenib vs Regorafenib: Key Molecular Difference Sorafenib H 3 C H N O N O H N O H N CF 3 CI Regorafenib H 3 C H N O N O F H N O H N CF 3 CI Slide credit: clinicaloptions.com
25
26
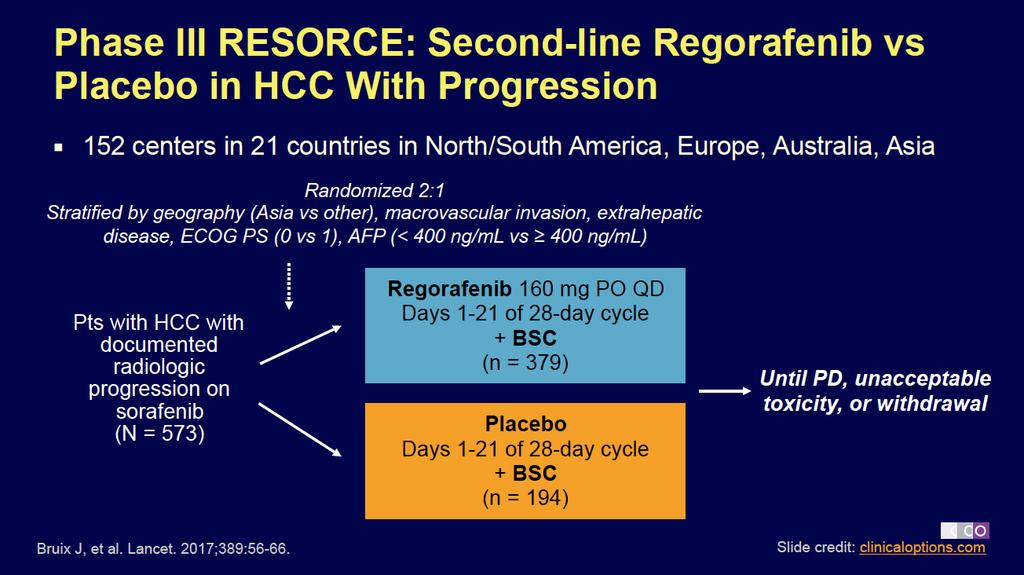
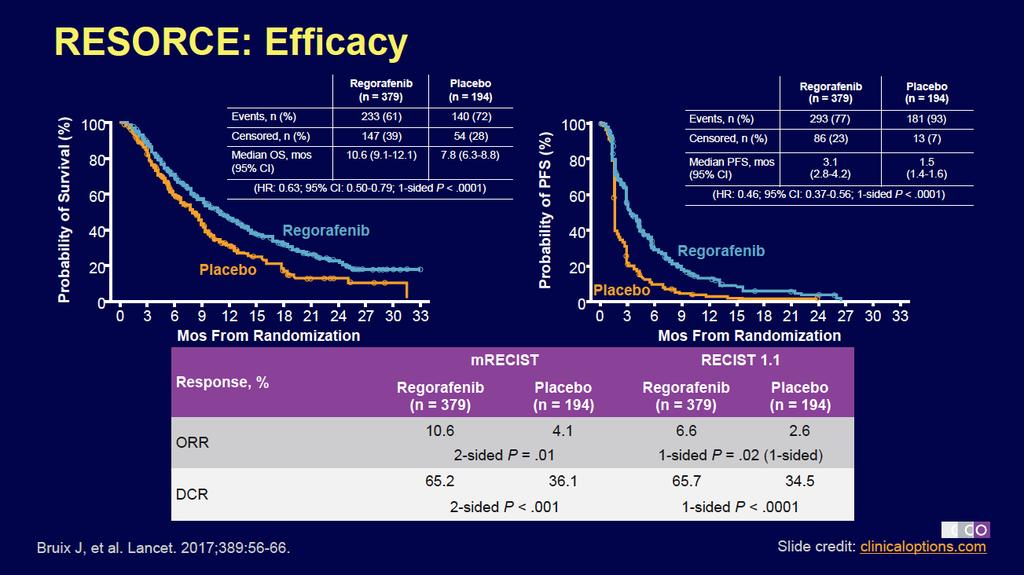
27 Regorafenib: Dosage and Administration Approved by the FDA in April 2017 for pts with HCC previously treated with sorafenib [1] Recommended dose: 160 mg PO QD x 3 wks Q4W [1] 2-wk washout period recommended after discontinuing sorafenib [2,3] Allows for elimination of sorafenib and metabolites Demonstrated safety with this approach in RESORCE trial 1. Regorafenib [package insert]. 2. Bruix J, et al. Lancet. 2017;389: Jordi Bruix, MD, personal communication Slide credit: clinicaloptions.com
28
29
30
31
32
33 Phase I/II CheckMate 040: Nivolumab in Advanced HCC Phase I/II Without viral hepatitis 0.1 mg/kg (n = 1) Dose Escalation (n = 48) design n = 6 n = 9 n = 10 n = 10 n = mg/kg (n = 3) 1.0 mg/kg (n = 3) 3.0 mg/kg (n = 3) 10 mg/kg (n = 13) Dose Expansion (n = 214) 3 mg/kg Sorafenib untreated or intolerant (n = 56) Sorafenib progressor (n = 57) HCV infected 0.3 mg/kg (n = 3) 1.0 mg/kg (n = 4) 3.0 mg/kg (n = 3) HCV infected (n = 50) HBV infected 0.1 mg/kg (n = 5) 0.3 mg/kg (n = 3) 1.0 mg/kg (n = 3) 3.0 mg/kg (n = 4) HBV infected (n = 51) El-Khoueiry AB, et al. Lancet. 2017;[Epub ahead of print].
34
35
36
37

38

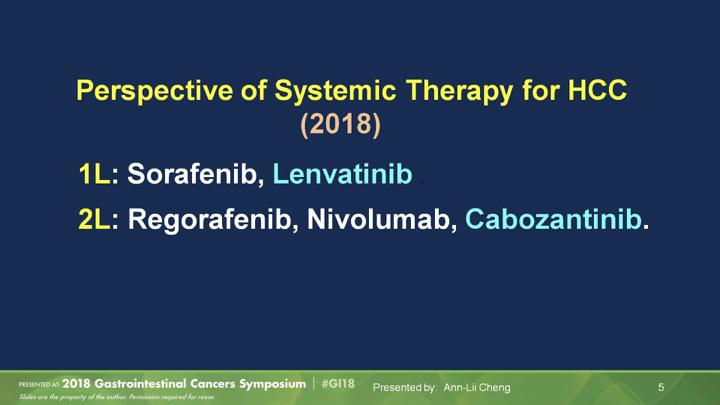
39 Conclusions<br />(2018 perspective of systemic tx for HCC)
40 Συμπερασματα
41
42
43
44 The Challenge: First-line Randomized Phase III Trials in HCC Phase III Trial Target(s) Median TTP, Mos Median OS, Mos Sunitinib vs sorafenib [1] VEGFRs, PDGFRs, c-kit, Flt3, RET 4.1 vs 3.8 HR: 1.13 (95% CI: ; P =.83) 7.9 vs sided P =.0014 Brivanib vs sorafenib (BRISK-FL) [2] VEGFR2, FGFR 4.2 vs 4.1 HR: 1.01 (95% CI: ) 9.5 vs 9.9 HR: 1.07 (95% CI: ; P =.3116) Linifanib vs sorafenib [3] VEGFR and PDGFR 5.4 vs. 4.0 HR: 0.76 (95% CI: ; P =.001) 9.1 vs. 9.8 HR: 1.04 (95% CI: ; P = NS) Sorafenib + erlotinib vs sorafenib + placebo [4] VEGFR1,2,3, Ras, Raf, EGFR 3.2 vs 4.0 HR: 1.13 (95% CI: ; P =.18) 9.5 vs. 8.5 HR: 0.93 (95% CI: ; P =.41) Doxorubicin + sorafenib vs References sorafenib in (CALGB slidenotes ) [5] VEGFR1,2, PDGFR, Ras, Raf 4.0 vs 3.9 HR: 0.90 (95% CI: ) 8.9 vs 10.5 HR: 1.06 (95% Slide CI: credit: ) clinicaloptions.com
45
46
47 Phase III SARAH: SIRT vs Sorafenib in Locally Advanced, Inoperable HCC After 2 Rounds of TACE Probability of Survival ITT Population (N = 459) SIRT Sorafenib Median 8.0 mos 9.9 mos HR: 1.15 (95% CI: ; log-rank P =.18) Pts at Risk, n Mos Since Randomization SIRT Sorafenib Probability of Survival Pts at Risk, n SIRT Sorafenib Per Protocol Population (n = 380) SIRT Sorafenib Median 9.9 mos 9.9 mos HR: 0.99 (95% CI: ; log-rank P =.92) Mos Since Randomization Vilgrain V, et al. EASL Abstract GS-02 Slide credit: clinicaloptions.com
48 Liver Embolotherapy Techniques Technique Mechanism Pros Cons TAE Induction of ischemic necrosis at arteriolar level using permanent embolic (eg, small particles) Low cost, no chemotherapy adverse events Postembolization syndrome; may cause PEs Conventional TACE (ctace) Intrahepatic chemotherapy combined with embolization from ethiodized oil Strongest evidence for benefit based on RCT data Technical variation between operators (ctace) Systemic release of chemotherapy (ctace) Postembolization syndrome DEB-TACE Intrahepatic chemotherapy + embolization with slowrelease drug-eluting beads More standardized than ctace, lower systemic release of chemotherapy More expensive than ctace Postembolization syndrome Kishore S, et al. Curr Oncol Rep. 2017;19:40. May improve TTP Fewer sessions required No postembolization syndrome Cost: 2-3x more expensive Requires Slide credit: multidisciplinary clinicaloptions.com
49 Conclusion: How to treat pts with advanced disease? First line Second line Third line Sorafenib Lenvatinib? Immunotherapy? Ongoing phase III trial of nivolumab vs sorafenib Regorafenib Cabozantinib? Ongoing phase III study vs placebo Immunotherapy? Ongoing phase III study of pembrolizumab vs BSC Slide credit: clinicaloptions.com
50 Treatment Options for Pts With HCC Stage of Disease Treatment Option Survival Rate Early Surgery/transplantation, PEI/RFA ~ 50% to 75% at 5 yrs ~ 40% to 50% at 5 yrs *Monotherapy or combination chemotherapy, immunotherapy, internal radiation, tamoxifen, antiandrogen agents failed to Intermediate demonstrate survival benefit. TACE ~ 40% to 60% at 2 yrs Advanced (first line) Sorafenib/clinical trials < 30% at 1 yr* Llovet JM. J Gastroenterol. 2005;40:
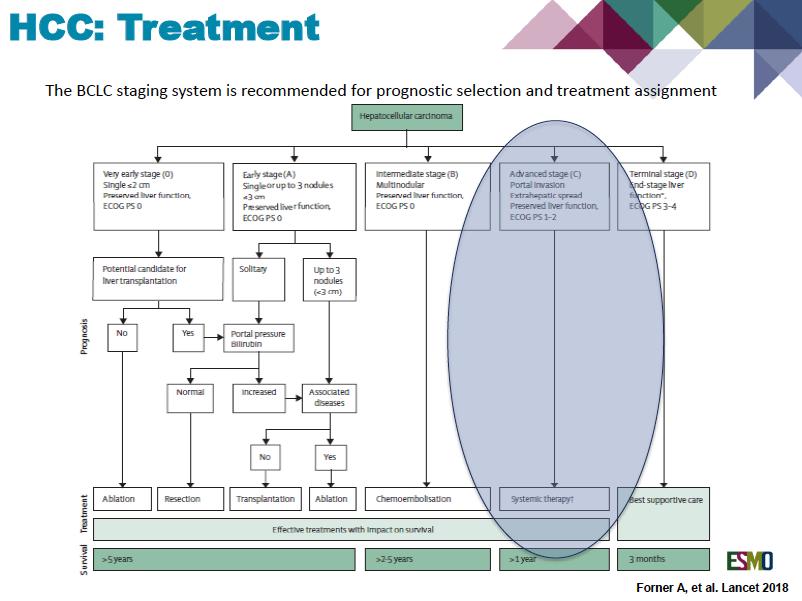
51 Tumor Burden, Liver Function, and Performance Status Influence Prognosis First-line treatment options for each stage of HCC Therapy is decided according to tumor burden, liver function, and PS Pts: Child-Pugh A-B, preserved ECOG PS, absence of severe comorbidities Diagnosis BCLC 0 BCLC A BCLC B BCLC C BCLC D Surgery ablation TACE Sorafenib Best Death supportive care Bruix J, et al. Gastroenterology. 2016;150: Slide credit: clinicaloptions.com
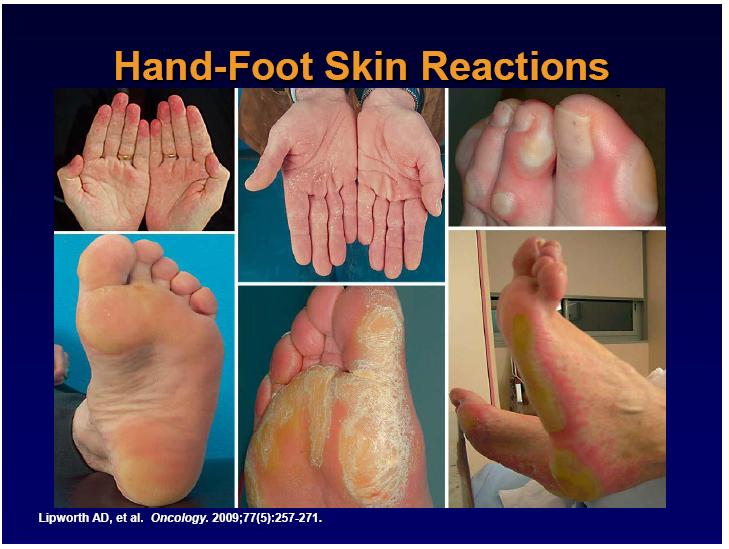
52 SHARP: Drug-Related Adverse Events Adverse Event Reported in 10% of Pts, % Any Grade Llovet JM, et al. N Engl J Med. 2008;359: Sorafenib (n = 297) Placebo (n = 302) P Value Grade 3 Grade 4 Any Grade Overall incidence Grade 3 Grade 4 Any Grade Grade 3/4 Fatigue < Alopecia <.001 NA Hand foot skin reaction Rash/desquamati on < 1 0 <.001 < Anorexia 14 < < Diarrhea <.001 <.001 Nausea 11 <
53 Treatment of Advanced HCC: Probability of Survival Sorafenib Outcomes in Western Pts [1] P < Mos Since Randomization Best Response (RECIST), % Sorafenib (n = 299) Placebo (n = 303) CR 0 0 PR SD PD Progression-free rate at 4 mos Probability of Survival Sorafenib Outcomes in Asian Pts [2] Mos Response, n (%) Sorafenib (n = 150) Sorafenib Placebo Placebo (n = 76) CR 0 0 PR 5 (3.3) 1 (1.3) SD 81 (54.0) 21 (27.6) PD 46 (30.7) 41 (54.0) Not assessable 18 (12.0) 13 (17.1) 1. Llovet JM, et al. N Engl J Med. 2008;359: Cheng AL, et al. Lancet Oncol. 2009;10:25-34.
54
55
56
The Current Champion: Angiogenesis inhibitors
 The Current Champion: Angiogenesis inhibitors Baek-Yeol RYOO University of Ulsan College of Medicine ASAN Medical Center Dept. of Oncology Seoul, Korea Survival probability Sorafenib: Overall Survival
The Current Champion: Angiogenesis inhibitors Baek-Yeol RYOO University of Ulsan College of Medicine ASAN Medical Center Dept. of Oncology Seoul, Korea Survival probability Sorafenib: Overall Survival
Current Standards of Care of Hepatocellular Carcinoma? Prof. Mohsen Mokhtar M.D Cairo Univ.
 Current Standards of Care of Hepatocellular Carcinoma? Prof. Mohsen Mokhtar M.D Cairo Univ. Disclosures Honoraria Received : Amgen, Astra Zeneca, Bohrengier, Hikma,Hospira, GSK, Lilly, Merck, MSD, Novartis,
Current Standards of Care of Hepatocellular Carcinoma? Prof. Mohsen Mokhtar M.D Cairo Univ. Disclosures Honoraria Received : Amgen, Astra Zeneca, Bohrengier, Hikma,Hospira, GSK, Lilly, Merck, MSD, Novartis,
Riunione Monotematica A.I.S.F The future of liver diseases. HEPATIC NEOPLASMS The challenge for new drugs
 Riunione Monotematica A.I.S.F. 2016 The future of liver diseases Milan 13 th -15 th October 2016 Centro Congressi Fondazione Cariplo HEPATIC NEOPLASMS The challenge for new drugs Massimo Iavarone Gastroenterology
Riunione Monotematica A.I.S.F. 2016 The future of liver diseases Milan 13 th -15 th October 2016 Centro Congressi Fondazione Cariplo HEPATIC NEOPLASMS The challenge for new drugs Massimo Iavarone Gastroenterology
12 AISF Special Conference Sorafenib: magnitude of benefit, side effects and stopping rules 9 years after approval
 12 AISF Special Conference Sorafenib: magnitude of benefit, side effects and stopping rules 9 years after approval ARMANDO SANTORO Roma 10-6-2016 SORAFENIB APPROVAL 29 OCTOBER 2007 Marketing authorization
12 AISF Special Conference Sorafenib: magnitude of benefit, side effects and stopping rules 9 years after approval ARMANDO SANTORO Roma 10-6-2016 SORAFENIB APPROVAL 29 OCTOBER 2007 Marketing authorization
Advances in Systemic Therapy Hepatocellular Carcinoma (HCC) Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016
 Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016") Advances in Systemic Therapy for Hepatocellular Carcinoma (HCC) Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016 Scope Background Staging and treatment strategies Current systemic therapy
Advances in Systemic Therapy for Hepatocellular Carcinoma (HCC) Dr ZEE Ying Kiat HASLD Conference Ho Chi Minh City, 18 December 2016 Scope Background Staging and treatment strategies Current systemic therapy
New Therapies in HCC Bruno Sangro Clínica Universidad de Navarra. IdISNA. CIBERehd. Pamplona, Spain
 New Therapies in HCC Bruno Sangro Clínica Universidad de Navarra. IdISNA. CIBERehd. Pamplona, Spain PHC 2018 - www.aphc.info EASL-EORTC Guidelines EASL EORTC Guidelines. J Hepatol. 2012;56:908-43. Systemic
New Therapies in HCC Bruno Sangro Clínica Universidad de Navarra. IdISNA. CIBERehd. Pamplona, Spain PHC 2018 - www.aphc.info EASL-EORTC Guidelines EASL EORTC Guidelines. J Hepatol. 2012;56:908-43. Systemic
Il treatment plan nella terapia sistemica dell epatocarcinoma
 Il treatment plan nella terapia sistemica dell epatocarcinoma M. Iavarone, MD PhD CRC A.M. e A. Migliavacca Center for the Study of Liver Disease Division of Gastroenterology and Hepatology Fondazione
Il treatment plan nella terapia sistemica dell epatocarcinoma M. Iavarone, MD PhD CRC A.M. e A. Migliavacca Center for the Study of Liver Disease Division of Gastroenterology and Hepatology Fondazione
Il Tumore del Fegato Prospettive Future nel Trattamento dei Tumori Gastrointestinali
 Il Tumore del Fegato Prospettive Future nel Trattamento dei Tumori Gastrointestinali Lorenza Rimassa Medical Oncology Unit Humanitas Cancer Center Humanitas Research Hospital Rozzano (Milano) Disclosures
Il Tumore del Fegato Prospettive Future nel Trattamento dei Tumori Gastrointestinali Lorenza Rimassa Medical Oncology Unit Humanitas Cancer Center Humanitas Research Hospital Rozzano (Milano) Disclosures
First-line therapy for unresectable HCC:
 ESMO GI Cancer Preceptorship 15 November 2017 Singapore First-line therapy for unresectable HCC: an oncologist s viewpoint Chiun Hsu, MD, PhD G raduate I n stitute of Oncology, National Taiwan Univers
ESMO GI Cancer Preceptorship 15 November 2017 Singapore First-line therapy for unresectable HCC: an oncologist s viewpoint Chiun Hsu, MD, PhD G raduate I n stitute of Oncology, National Taiwan Univers
蕾莎瓦 Nexavar 臨床試驗資料 (HCC 肝細胞癌 )
") 蕾莎瓦 Nexavar 臨床試驗資料 (HCC 肝細胞癌 ) 1 Sorafenib Improves Survival in Hepatocellular Carcinoma: Results of a Phase III Randomized, -Controlled Trial Josep M. Llovet, Sergio Ricci, Vincenzo Mazzaferro, Philip
蕾莎瓦 Nexavar 臨床試驗資料 (HCC 肝細胞癌 ) 1 Sorafenib Improves Survival in Hepatocellular Carcinoma: Results of a Phase III Randomized, -Controlled Trial Josep M. Llovet, Sergio Ricci, Vincenzo Mazzaferro, Philip
Advances in percutaneous ablation and systemic therapies for hepatocellular carcinoma
 Advances in percutaneous ablation and systemic therapies for hepatocellular carcinoma Paris Hepatology Congress 2019 Pierre Nahon Service d Hépatologie Hôpital Jean Verdier Bondy Université Paris 13 INSERM
Advances in percutaneous ablation and systemic therapies for hepatocellular carcinoma Paris Hepatology Congress 2019 Pierre Nahon Service d Hépatologie Hôpital Jean Verdier Bondy Université Paris 13 INSERM
Latest Developments in the Treatment of Hepatocellular Carcinoma
 Latest Developments in the Treatment of Hepatocellular Carcinoma Roniel Cabrera, MD MS Associate Professor of Medicine Director of Hepatology and Medical Director of Liver Transplantation Division of Gastroenterology,
Latest Developments in the Treatment of Hepatocellular Carcinoma Roniel Cabrera, MD MS Associate Professor of Medicine Director of Hepatology and Medical Director of Liver Transplantation Division of Gastroenterology,
A) PUBLIC HEALTH B) PRESENTATION & DIAGNOSIS
 PUBLIC HEALTH B) PRESENTATION & DIAGNOSIS") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary), April 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Centre, BC Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary), April 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Centre, BC Cancer
Nexavar in advanced HCC: a paradigm shift in clinical practice
 Nexavar in advanced HCC: a paradigm shift in clinical practice Tim Greten Hanover Medical School, Germany Histopathological progression and molecular features of HCC Chronic liver disease Liver cirrhosis
Nexavar in advanced HCC: a paradigm shift in clinical practice Tim Greten Hanover Medical School, Germany Histopathological progression and molecular features of HCC Chronic liver disease Liver cirrhosis
A New Era of Systemic Therapy for Hepatocellular Carcinoma with Regorafenib and Lenvatinib
 Published online: March 9, 2017 Editorial A New Era of Systemic Therapy for Hepatocellular Carcinoma with Prof. M. Kudo Editor Liver Cancer Introduction The SHARP study in 2007 [1] and the Asia Pacific
Published online: March 9, 2017 Editorial A New Era of Systemic Therapy for Hepatocellular Carcinoma with Prof. M. Kudo Editor Liver Cancer Introduction The SHARP study in 2007 [1] and the Asia Pacific
Novel Molecular Molecular Therapies In Hepatocarcinoma Prof Eric
 Novel Molecular Therapies In Hepatocarcinoma Prof. Eric Raymond Department of Médical Oncology Hôpital Beaujon, Clichy Université Paris 7 Denis Diderot INSERM-U728 eric.raymond@bjn.aphp.fr HCC is a highly
Novel Molecular Therapies In Hepatocarcinoma Prof. Eric Raymond Department of Médical Oncology Hôpital Beaujon, Clichy Université Paris 7 Denis Diderot INSERM-U728 eric.raymond@bjn.aphp.fr HCC is a highly
Study Objective and Design
 Randomized, Open Label, Multicenter, Phase II Trial of Transcatheter Arterial Chemoembolization (TACE) Therapy in Combination with Sorafenib as Compared With TACE Alone in Patients with Hepatocellular
Randomized, Open Label, Multicenter, Phase II Trial of Transcatheter Arterial Chemoembolization (TACE) Therapy in Combination with Sorafenib as Compared With TACE Alone in Patients with Hepatocellular
Management of advanced Hepatocellular carcinoma
 Management of advanced Hepatocellular carcinoma V Di Martino* Acknowledgements to T Thevenot *Advisory board/lectures/travel facilities: Case report (1) Mr T. Philippe 55 yrs old Past IV drug user (1985)
Management of advanced Hepatocellular carcinoma V Di Martino* Acknowledgements to T Thevenot *Advisory board/lectures/travel facilities: Case report (1) Mr T. Philippe 55 yrs old Past IV drug user (1985)
New Insights: Systemic Therapy for Advanced Hepatocellular Carcinoma (HCC)
") New Insights: Systemic Therapy for Advanced Hepatocellular Carcinoma (HCC) Thomas W.T. Leung Associate Director and Honorary Consultant Comprehensive Oncology Centre Hong Kong Sanatorium and Hospital Hong
New Insights: Systemic Therapy for Advanced Hepatocellular Carcinoma (HCC) Thomas W.T. Leung Associate Director and Honorary Consultant Comprehensive Oncology Centre Hong Kong Sanatorium and Hospital Hong
WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC?
 WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC? Dr. Alexander Kim Chief, Vascular and Interventional Radiology, Medstar Georgetown University Hospital, USA DISCLAIMER Please note: The views
WHAT IS THE BEST APPROACH FOR TRANS-ARTERIAL THERAPY IN HCC? Dr. Alexander Kim Chief, Vascular and Interventional Radiology, Medstar Georgetown University Hospital, USA DISCLAIMER Please note: The views
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary)
") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Liver and Biliary Tract Cancers Critical Review
 Liver and Biliary Tract Cancers Critical Review Lorenza Rimassa Oncologia Medica e Ematologia Humanitas Cancer Center Humanitas Research Hospital Rozzano (Milano) Critical review Oral presentations Melero
Liver and Biliary Tract Cancers Critical Review Lorenza Rimassa Oncologia Medica e Ematologia Humanitas Cancer Center Humanitas Research Hospital Rozzano (Milano) Critical review Oral presentations Melero
Jon Trent, MD, PhD. Associate Professor Dept. of Sarcoma Medical Oncology The University of Texas, M. D. Anderson Cancer Center
 Gastrointestinal Stromal Tumor GISTS 2010: After Standard of Care Jon Trent, MD, PhD Associate Professor Dept. of Sarcoma Medical Oncology The University of Texas, M. D. Anderson Cancer Center jtrent@mdanderson.org
Gastrointestinal Stromal Tumor GISTS 2010: After Standard of Care Jon Trent, MD, PhD Associate Professor Dept. of Sarcoma Medical Oncology The University of Texas, M. D. Anderson Cancer Center jtrent@mdanderson.org
HCC: Epidemiology. Update on treatment of advanced hepatocellular carcinoma. Incidence of HCC is increasing
 Update on treatment of advanced hepatocellular carcinoma Jean-Luc Raoul Centre E Marquis Rennes, Brittany France HCC: Epidemiology Europe - USA: C virus, alcohol obesity, iron Europe: 4 deaths / year 6
Update on treatment of advanced hepatocellular carcinoma Jean-Luc Raoul Centre E Marquis Rennes, Brittany France HCC: Epidemiology Europe - USA: C virus, alcohol obesity, iron Europe: 4 deaths / year 6
Cisplatin plus Gemcitabine versus Gemcitabine for Biliary Tract Cancer. Valle J et al. N Engl J Med 2010;362(14):
:") Cisplatin plus Gemcitabine versus Gemcitabine for Biliary Tract Cancer Valle J et al. N Engl J Med 2010;362(14):1273-81. Introduction > Biliary tract cancers (BTC: cholangiocarcinoma, gall bladder cancer,
Cisplatin plus Gemcitabine versus Gemcitabine for Biliary Tract Cancer Valle J et al. N Engl J Med 2010;362(14):1273-81. Introduction > Biliary tract cancers (BTC: cholangiocarcinoma, gall bladder cancer,
Unmet Needs in the Treatment of Advanced Hepatocellular Carcinoma
 Unmet Needs in the Treatment of Advanced Hepatocellular Carcinoma Joong-Won Park Center for Liver Cancer National Cancer Center, Korea Advanced HCC Definition - An abtract concept, Not clear, No consensus
Unmet Needs in the Treatment of Advanced Hepatocellular Carcinoma Joong-Won Park Center for Liver Cancer National Cancer Center, Korea Advanced HCC Definition - An abtract concept, Not clear, No consensus
Optimal management of HCC: in Asia
 Optimal management of HCC: in Asia Kwang-Hyub Han, MD Department of Internal Medicine, Institute of Gastroenterology, Yonsei University College of Medicine, Seoul, Korea Newly diagnosed HCC : > 70% occur
Optimal management of HCC: in Asia Kwang-Hyub Han, MD Department of Internal Medicine, Institute of Gastroenterology, Yonsei University College of Medicine, Seoul, Korea Newly diagnosed HCC : > 70% occur
SEQUENCING OF HCC TREATMENT. Dr. Amit G. Singal Medical Director, UT Southwestern Medical Center, USA
 SEQUENCING OF HCC TREATMENT Dr. Amit G. Singal Medical Director, UT Southwestern Medical Center, USA February 2018 DISCLAIMER Please note: The views expressed within this presentation are the personal
SEQUENCING OF HCC TREATMENT Dr. Amit G. Singal Medical Director, UT Southwestern Medical Center, USA February 2018 DISCLAIMER Please note: The views expressed within this presentation are the personal
David N. Robinson, MD
 David N. Robinson, MD Background and Treatment of mrcc Background ~ 64,770 new cases of kidney/renal pelvis cancers will be diagnosed in the US in 2012 with an estimated 13,570 deaths [1] ~ 75% are clear-cell
David N. Robinson, MD Background and Treatment of mrcc Background ~ 64,770 new cases of kidney/renal pelvis cancers will be diagnosed in the US in 2012 with an estimated 13,570 deaths [1] ~ 75% are clear-cell
Malignant pleural Mesothelioma: A Year In Review
 Malignant pleural Mesothelioma: A Year In Review Rabab Gaafar,MD Prof. Medical Oncology NCI Cairo University National Cancer Institute Conference 2015 ASCO news in Mesothelioma Introduction ASCO news second
Malignant pleural Mesothelioma: A Year In Review Rabab Gaafar,MD Prof. Medical Oncology NCI Cairo University National Cancer Institute Conference 2015 ASCO news in Mesothelioma Introduction ASCO news second
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better?
 Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Sorafenib in HCC. Discussion points
 Discussion points in Andrew X. Zhu, MD, PhD 214 CASL Meeting-Consensus, Controversies and Future Directions in -data from phase III trials ptimal Dosing Side effects and management strategies use in Child-Pugh
Discussion points in Andrew X. Zhu, MD, PhD 214 CASL Meeting-Consensus, Controversies and Future Directions in -data from phase III trials ptimal Dosing Side effects and management strategies use in Child-Pugh
Hepatocellular Carcinoma: A major global health problem. David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center
 Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
Karcinom dojke. PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski
 Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
When patients fail on molecular targeted therapy: what to do in 2013
 When patients fail on molecular targeted therapy: what to do in 2013 For 3 rd APASAL HCC conference on 23 Nov 2013 Dr. Stephen L. Chan Department of Clinical Oncology The Chinese University of Hong Kong
When patients fail on molecular targeted therapy: what to do in 2013 For 3 rd APASAL HCC conference on 23 Nov 2013 Dr. Stephen L. Chan Department of Clinical Oncology The Chinese University of Hong Kong
Immunotherapy for Melanoma. Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center
 Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Antiangiogenic therapy in GI cancer: current status and future directions
 Riccardo Giampieri, MD, PhD Università Politecnica delle Marche Ospedali Riuniti diancona Antiangiogenic therapy in GI cancer: current status and future directions Before starting Summary - Antiangiogenesis
Riccardo Giampieri, MD, PhD Università Politecnica delle Marche Ospedali Riuniti diancona Antiangiogenic therapy in GI cancer: current status and future directions Before starting Summary - Antiangiogenesis
9th Paris Hepatitis Conference
 9th Paris Hepatitis Conference Paris, 12 January 2016 Treatment of hepatocellular carcinoma: beyond international guidelines Massimo Colombo Chairman Department of Liver, Kidney, Lung and Bone Marrow Units
9th Paris Hepatitis Conference Paris, 12 January 2016 Treatment of hepatocellular carcinoma: beyond international guidelines Massimo Colombo Chairman Department of Liver, Kidney, Lung and Bone Marrow Units
2 nd line Therapy and Beyond NSCLC. Alan Sandler, M.D. Oregon Health & Science University
 2 nd line Therapy and Beyond NSCLC Alan Sandler, M.D. Oregon Health & Science University Treatment options for advanced or metastatic (stage IIIb/IV) NSCLC Suitable for chemotherapy Diagnosis Unsuitable/unwilling
2 nd line Therapy and Beyond NSCLC Alan Sandler, M.D. Oregon Health & Science University Treatment options for advanced or metastatic (stage IIIb/IV) NSCLC Suitable for chemotherapy Diagnosis Unsuitable/unwilling
HCC with Intrahepatic Portal vein Tumour Should Be Treated by Systemic Therapy Rather Than Transarterial Therapy (Pros)
") HCC with Intrahepatic Portal vein Tumour Should Be Treated by Systemic Therapy Rather Than Transarterial Therapy (Pros) Yi-Hsiang Huang, MD, Ph.D. Professor, Division of Gastroenterology & Hepatology,
HCC with Intrahepatic Portal vein Tumour Should Be Treated by Systemic Therapy Rather Than Transarterial Therapy (Pros) Yi-Hsiang Huang, MD, Ph.D. Professor, Division of Gastroenterology & Hepatology,
Current experience in immunotherapy for metastatic renal cell carcinoma
 Current experience in immunotherapy for metastatic renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute FOIU, Tel Aviv, 3 July 2018 Financial and Other Disclosures Off-label use of drugs,
Current experience in immunotherapy for metastatic renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute FOIU, Tel Aviv, 3 July 2018 Financial and Other Disclosures Off-label use of drugs,
Incorporating Immunotherapy into the treatment of NSCLC
 Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
HCC: Is it an oncological disease? - No
 June 13-15, 2013 Berlin, Germany Prof. Oren Shibolet Head of the Liver Unit, Department of Gastroenterology Tel-Aviv Sourasky Medical Center and Tel-Aviv University HCC: Is it an oncological disease? -
June 13-15, 2013 Berlin, Germany Prof. Oren Shibolet Head of the Liver Unit, Department of Gastroenterology Tel-Aviv Sourasky Medical Center and Tel-Aviv University HCC: Is it an oncological disease? -
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist
 Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Update on the Management of HER2+ Breast Cancer. Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany
 Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Developping the next generation of studies in RCC
 Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Developping the next generation of studies in RCC Bernard Escudier Institut Gustave Roussy Villejuif, France Disclosure Information Advisory/Consultancy Role Pfizer, Exelixis, Novartis, BMS, Bayer, Roche,
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy
 Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Current Concepts in the Treatment of HCC
 Falk Symposium 167 Current Concepts in the Treatment of HCC Peter R. Galle I. Medical Department Johannes Gutenberg-University Mainz Germany Liver cancer: sixth most common cancer worldwide Most common
Falk Symposium 167 Current Concepts in the Treatment of HCC Peter R. Galle I. Medical Department Johannes Gutenberg-University Mainz Germany Liver cancer: sixth most common cancer worldwide Most common
Practice changing studies in lung cancer 2017
 1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Paul Martin MD FACG. University of Miami
 Paul Martin MD FACG University of Miami 1 Liver cirrhosis of any cause Chronic C o c hepatitis epat t s B Risk increases with Male gender Age Diabetes Smoking ~5% increase in HCV-related HCC between 1991-28
Paul Martin MD FACG University of Miami 1 Liver cirrhosis of any cause Chronic C o c hepatitis epat t s B Risk increases with Male gender Age Diabetes Smoking ~5% increase in HCV-related HCC between 1991-28
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Personalized Management of HCC
 Personalized Management of HCC Josep M. Llovet, MD, FAASLD Professor of Medicine. Director, Liver Cancer Program, ISM at Mount Sinai, NYC. Professor of Research-ICREA. BCLC Group-IDIBAPS. Liver Unit. Hospital
Personalized Management of HCC Josep M. Llovet, MD, FAASLD Professor of Medicine. Director, Liver Cancer Program, ISM at Mount Sinai, NYC. Professor of Research-ICREA. BCLC Group-IDIBAPS. Liver Unit. Hospital
3/22/2017. I will be discussing off label/investigational use of tivantinib for hepatocellular carcinoma.
 Grant/Research Support - AbbVie, Conatus, Hologic, Intercept, Genfit, Gilead, Mallinckrodt, Merck, Salix, Shire, Vital Therapies Consultant AbbVie, Gilead, Merck Member, Scientific Advisory Board Vital
Grant/Research Support - AbbVie, Conatus, Hologic, Intercept, Genfit, Gilead, Mallinckrodt, Merck, Salix, Shire, Vital Therapies Consultant AbbVie, Gilead, Merck Member, Scientific Advisory Board Vital
Addictive Benefit of Transarterial Chemoembolization and Sorafenib in Treating Advanced Stage Hepatocelluar Carcinoma: Propensity Analysis
 Addictive Benefit of Transarterial Chemoembolization and Sorafenib in Treating Advanced Stage Hepatocelluar Carcinoma: Propensity Analysis Gwang Hyeon Choi, Ju Hyun Shim*, Min-Joo Kim, Min-Hee Ryu, Baek-Yeol
Addictive Benefit of Transarterial Chemoembolization and Sorafenib in Treating Advanced Stage Hepatocelluar Carcinoma: Propensity Analysis Gwang Hyeon Choi, Ju Hyun Shim*, Min-Joo Kim, Min-Hee Ryu, Baek-Yeol
pan-canadian Oncology Drug Review Final Clinical Guidance Report Nivolumab (Opdivo) for Hepatocellular Carcinoma November 29, 2018
 for Hepatocellular Carcinoma November 29, 2018") pan-canadian Oncology Drug Review Final Clinical Guidance Report Nivolumab (Opdivo) for Hepatocellular Carcinoma November 29, 2018 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Nivolumab (Opdivo) for Hepatocellular Carcinoma November 29, 2018 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
Unmet Need Mucosal and Uveal Melanoma
 Unmet Need Mucosal and Uveal Melanoma Matteo Carlino Crown Princess Mary Cancer Centre Westmead and Blacktown Hospitals Melanoma Institute Australia The University of Sydney. Cutaneous Overall Survival
Unmet Need Mucosal and Uveal Melanoma Matteo Carlino Crown Princess Mary Cancer Centre Westmead and Blacktown Hospitals Melanoma Institute Australia The University of Sydney. Cutaneous Overall Survival
Regorafenib from Bayer Submitted to Health Authorities Seeking Approval in Second-Line Treatment of Liver Cancer
 News Release Not intended for U.S. and UK Media Bayer AG Communications, Government Relations & Corporate Brand 51368 Leverkusen Germany Tel. +49 214 30-0 www.news.bayer.com Regorafenib from Bayer Submitted
News Release Not intended for U.S. and UK Media Bayer AG Communications, Government Relations & Corporate Brand 51368 Leverkusen Germany Tel. +49 214 30-0 www.news.bayer.com Regorafenib from Bayer Submitted
SIRT for Intermediate and Advanced HCC
 Pamplona, junio de 2008 SIRT for Intermediate and Advanced HCC Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain 90 Y-RE MRI SPECT FUSION 90 Y-RE = Yttrium-90 radioembolization Sangro
Pamplona, junio de 2008 SIRT for Intermediate and Advanced HCC Bruno Sangro Clínica Universidad de Navarra. CIBERehd. Pamplona, Spain 90 Y-RE MRI SPECT FUSION 90 Y-RE = Yttrium-90 radioembolization Sangro
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors?
 Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Hepatocellular Carcinoma
 Hepatocellular Carcinoma Ghassan K. Abou-Alfa Memorial Sloan Kettering Cancer Center Great Debates & Updates in GI Malignancies New York, NY March 28, 2015 Epidemiology Scoring and staging Agenda Curative
Hepatocellular Carcinoma Ghassan K. Abou-Alfa Memorial Sloan Kettering Cancer Center Great Debates & Updates in GI Malignancies New York, NY March 28, 2015 Epidemiology Scoring and staging Agenda Curative
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute
 Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Angiogenesis and tumor growth
 Anti-angiogenic agents: where we are? Martin Reck Department of Thoracic Oncology Hospital Grosshansdorf Germany Angiogenesis and tumor growth Journal of experimental Medicine 1972; 133: 275-88 1 Angiogenesis
Anti-angiogenic agents: where we are? Martin Reck Department of Thoracic Oncology Hospital Grosshansdorf Germany Angiogenesis and tumor growth Journal of experimental Medicine 1972; 133: 275-88 1 Angiogenesis
100% pure beta emitter Decays to zirconium-90 Physical half-life of 64.1 hours (2.67 days) 94% of radiation delivered within 11 days
 94% of radiation delivered within 11 days") 100% pure beta emitter Decays to zirconium-90 Physical half-life of 64.1 hours (2.67 days) 94% of radiation delivered within 11 days TheraSphere [US package insert]. Surrey, UK: Biocompatibles UK Ltd,
100% pure beta emitter Decays to zirconium-90 Physical half-life of 64.1 hours (2.67 days) 94% of radiation delivered within 11 days TheraSphere [US package insert]. Surrey, UK: Biocompatibles UK Ltd,
Surveillance for Hepatocellular Carcinoma
 Surveillance for Hepatocellular Carcinoma Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded on April
Surveillance for Hepatocellular Carcinoma Marion G. Peters, MD John V. Carbone, MD, Endowed Chair Professor of Medicine Chief of Hepatology Research University of California San Francisco Recorded on April
EGFR Mutation-Positive Acquired Resistance: Dominance of T790M
 Treatment of EGFR Mutation-Positive Acquired Resistance: T790M+ or T790M- H. Jack West, MD Swedish Cancer Institute, Seattle, WA EGFR Mutation-Positive Acquired Resistance: Dominance of T790M Yu, Clin
Treatment of EGFR Mutation-Positive Acquired Resistance: T790M+ or T790M- H. Jack West, MD Swedish Cancer Institute, Seattle, WA EGFR Mutation-Positive Acquired Resistance: Dominance of T790M Yu, Clin
NSCLC 2 nd and further line therapies. Egbert F. Smit MD PhD. Dept. Thoracic Oncology, Netherlands Cancer Institute
 NSCLC 2 nd and further line therapies Egbert F. Smit MD PhD. Dept. Thoracic Oncology, Netherlands Cancer Institute e.smit@nki.nl ESMO Guidelines 2016: Treatment of Stage IV nonsquamous NSCLC at progression
NSCLC 2 nd and further line therapies Egbert F. Smit MD PhD. Dept. Thoracic Oncology, Netherlands Cancer Institute e.smit@nki.nl ESMO Guidelines 2016: Treatment of Stage IV nonsquamous NSCLC at progression
An Update on Hepatocellular Carcinoma. Ed Gane NZ Liver Transplant Unit
 An Update on Hepatocellular Carcinoma Ed Gane NZ Liver Transplant Unit Hepatocellular Carcinoma has a High Burden of Disease APSCVIR March 2018 Lung Liver Colon/Rectal Stomach Breast Cervix Uteri Esophagus
An Update on Hepatocellular Carcinoma Ed Gane NZ Liver Transplant Unit Hepatocellular Carcinoma has a High Burden of Disease APSCVIR March 2018 Lung Liver Colon/Rectal Stomach Breast Cervix Uteri Esophagus
Liver resection for HCC
 8 th LIVER INTEREST GROUP Annual Meeting Cape Town 2017 Liver resection for HCC Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre The liver is almost unique in that treatment of the
8 th LIVER INTEREST GROUP Annual Meeting Cape Town 2017 Liver resection for HCC Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre The liver is almost unique in that treatment of the
Lung Cancer Case. Since the patient was symptomatic, a targeted panel was sent. ALK FISH returned in 2 days and was positive.
 Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
RETHINKING OUR APPROACH TO INTERMEDIATE-SIZE HCC
 SATELLITE SYMPOSIUM Emerging Horizons in HCC: From Palliation to Cure RETHINKING OUR APPROACH TO INTERMEDIATE-SIZE HCC Professor Riccardo Lencioni, MD, FSIR, EBIR University of Pisa School of Medicine,
SATELLITE SYMPOSIUM Emerging Horizons in HCC: From Palliation to Cure RETHINKING OUR APPROACH TO INTERMEDIATE-SIZE HCC Professor Riccardo Lencioni, MD, FSIR, EBIR University of Pisa School of Medicine,
Second - Line Debate: Axitinib
 Second - Line Debate: Axitinib Alain Ravaud, MD PhD Bordeaux, France DISCLOSURES Member of Global, European and/or French advisory board in RCC and/or GU tumors for Pfizer, Novartis, GSK, Roche, BMS, Merck.
Second - Line Debate: Axitinib Alain Ravaud, MD PhD Bordeaux, France DISCLOSURES Member of Global, European and/or French advisory board in RCC and/or GU tumors for Pfizer, Novartis, GSK, Roche, BMS, Merck.
Liver and Biliary Tract Cancers Highlights
 Liver and Biliary Tract Cancers Highlights A cura di Lorenza Rimassa, MD Medical Oncology Unit, Humanitas Research Hospital IRCCS, Rozzano (Milano) Disclosures Consulting or Advisory Role: Lilly, Bayer,
Liver and Biliary Tract Cancers Highlights A cura di Lorenza Rimassa, MD Medical Oncology Unit, Humanitas Research Hospital IRCCS, Rozzano (Milano) Disclosures Consulting or Advisory Role: Lilly, Bayer,
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy. What every patient needs to know. James Larkin
 Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Opzioni terapeutiche nel paziente ALK-traslocato
 Opzioni terapeutiche nel paziente ALK-traslocato Giulio Metro S.C. Oncologia Medica Ospedale Santa Maria della Misericordia, Azienda Ospedaliera di Perugia Carcinoma del polmone non microcitoma: quali
Opzioni terapeutiche nel paziente ALK-traslocato Giulio Metro S.C. Oncologia Medica Ospedale Santa Maria della Misericordia, Azienda Ospedaliera di Perugia Carcinoma del polmone non microcitoma: quali
Background. Capdevila J, et al. Ann Oncol. 2018;29(Suppl 8): Abstract 1307O. 1. Dasari A, et al. JAMA Oncol. 2017;3(10):
: Abstract 1307O. 1. Dasari A, et al. JAMA Oncol. 2017;3(10):") Efficacy of Lenvatinib in Patients With Advanced Pancreatic (pannets) and Gastrointestinal (ginets) WHO Grade 1/2 (G1/G2) Neuroendocrine Tumors: Results of the International Phase II TALENT Trial (GETNE
Efficacy of Lenvatinib in Patients With Advanced Pancreatic (pannets) and Gastrointestinal (ginets) WHO Grade 1/2 (G1/G2) Neuroendocrine Tumors: Results of the International Phase II TALENT Trial (GETNE
Unmet needs in intermediate HCC. Korea University Guro Hospital Ji Hoon Kim
 Unmet needs in intermediate HCC Korea University Guro Hospital Ji Hoon Kim BCLC HCC Stage 0 PST 0, Child Pugh A Stage A C PST 0 2, Child Pugh A B Stage D PST > 2, Child Pugh C Very early stage (0) 1 HCC
Unmet needs in intermediate HCC Korea University Guro Hospital Ji Hoon Kim BCLC HCC Stage 0 PST 0, Child Pugh A Stage A C PST 0 2, Child Pugh A B Stage D PST > 2, Child Pugh C Very early stage (0) 1 HCC
Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging
 Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Hepatobiliary and Pancreatic Surgery Chief of Hepatobiliary and Pancreatic Surgery
Celsion Symposium New Paradigms in HCC Staging: HKLC vs. BCLC Staging Ronnie T.P. Poon, MBBS, MS, PhD Chair Professor of Hepatobiliary and Pancreatic Surgery Chief of Hepatobiliary and Pancreatic Surgery
Treatment of Hepatocellular Carcinoma. Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center
 Treatment of Hepatocellular Carcinoma Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center Epidemiology of HCC: world The 5 th most common cancer worldwide > 500, 000 new
Treatment of Hepatocellular Carcinoma Andrew J. Muir, MD MHS Division of Gastroenterology Duke University Medical Center Epidemiology of HCC: world The 5 th most common cancer worldwide > 500, 000 new
Dr Shankara Paneesha. ASH Highlights Department of Haematology & Stem cell Transplantation
 ASH Highlights 2015 Themes of ASH 2015 Novel therapies - Myeloma AML Lymphoma Pd-L1 & PD-l inhibitors Emerging concepts in biology HIF-1a pathway Cautionary tales ASH Choosing Wisely list IFM/DFCI
ASH Highlights 2015 Themes of ASH 2015 Novel therapies - Myeloma AML Lymphoma Pd-L1 & PD-l inhibitors Emerging concepts in biology HIF-1a pathway Cautionary tales ASH Choosing Wisely list IFM/DFCI
The Management of Advanced Stage Hepatocellular Carcinoma
 The Management of Advanced Stage Hepatocellular Carcinoma Pierce K.H Chow MD PhD Professor, Duke-NUS Graduate Medical School Singapore Senior Consultant Surgeon, National Cancer Center Singapore Senior
The Management of Advanced Stage Hepatocellular Carcinoma Pierce K.H Chow MD PhD Professor, Duke-NUS Graduate Medical School Singapore Senior Consultant Surgeon, National Cancer Center Singapore Senior
III Sessione I risultati clinici
 10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
Timing of targeted therapy in patients with low volume mrcc. Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital
 1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
Hepatocellular Carcinoma (HCC)
") Hepatocellular Carcinoma (HCC) Matthias Pinter Div. Gastroenterology & Hepatology Medical University of Vienna Agenda Epidemiology Screening & Diagnosis Staging & Treatment Early stage Intermediate stage
Hepatocellular Carcinoma (HCC) Matthias Pinter Div. Gastroenterology & Hepatology Medical University of Vienna Agenda Epidemiology Screening & Diagnosis Staging & Treatment Early stage Intermediate stage
An Open-Label Phase Ib/II Study of Sulfatinib in Patients with Advanced Neuroendocrine Tumors (NCT )
") An Open-Label Phase Ib/II Study of Sulfatinib in Patients with Advanced Neuroendocrine Tumors (NCT02267967) J.M. Xu a, J. Li b, C.M. Bai c, N. Xu d, Z.W. Zhou e, Z.P. Li f, C.C. Zhou g, W. Wang h, J. Li
An Open-Label Phase Ib/II Study of Sulfatinib in Patients with Advanced Neuroendocrine Tumors (NCT02267967) J.M. Xu a, J. Li b, C.M. Bai c, N. Xu d, Z.W. Zhou e, Z.P. Li f, C.C. Zhou g, W. Wang h, J. Li
QUANDO LA TERAPIA MEDICA
 IL NODULO EATICO dalla diagnosi.. alla terapia Sala Conferenze, Biblioteca "Rosanna Benzi" Genova Voltri 21 Settembre 2013 QUANDO LA TERAIA MEDICA Dott. Gianfranco ercario U.O.S. di Gastroenterologia OEI
IL NODULO EATICO dalla diagnosi.. alla terapia Sala Conferenze, Biblioteca "Rosanna Benzi" Genova Voltri 21 Settembre 2013 QUANDO LA TERAIA MEDICA Dott. Gianfranco ercario U.O.S. di Gastroenterologia OEI
Immunotherapy for NSCLC: Current State of the Art and Future Directions. H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States
 Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Clinical Roundtable Monograph
 Clinical Roundtable Monograph Clinical Advances in Hematology & Oncology August 2017 The Treatment Path in Hepatocellular Carcinoma Faculty Hashem B. El-Serag, MD, MPH Margaret M. and Albert B. Alkek Professor
Clinical Roundtable Monograph Clinical Advances in Hematology & Oncology August 2017 The Treatment Path in Hepatocellular Carcinoma Faculty Hashem B. El-Serag, MD, MPH Margaret M. and Albert B. Alkek Professor
ASCO 2011 Genitourinary Cancer
 ASCO 2011 Genitourinary Cancer Expanding Options for Chronic Diseases? Walter Stadler, MD, FACP University of Chicago Disclosures (All Non-University &/or Financial Dealings with Potential, Real, or Perceived
ASCO 2011 Genitourinary Cancer Expanding Options for Chronic Diseases? Walter Stadler, MD, FACP University of Chicago Disclosures (All Non-University &/or Financial Dealings with Potential, Real, or Perceived
Special situations: Patients with liver metastasis or liver primary tumor. Erika Martinelli, MD PhD Medical Oncologist
 Special situations: Patients with liver metastasis or liver primary tumor Erika Martinelli, MD PhD Medical Oncologist Outline: Liver (anatomy, basic functions) Liver Immuno-landscape Immuno-landscape in
Special situations: Patients with liver metastasis or liver primary tumor Erika Martinelli, MD PhD Medical Oncologist Outline: Liver (anatomy, basic functions) Liver Immuno-landscape Immuno-landscape in
Carcinoma de Tiroide: Teràpies Diana
 Carcinoma de Tiroide: Teràpies Diana Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology THYROID CANCER:
Carcinoma de Tiroide: Teràpies Diana Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology THYROID CANCER:
Will All Adjuvant Therapy Trials Be Negative in RCC?
 Will All Adjuvant Therapy Trials Be Negative in RCC? Tim Eisen Eleventh European International Kidney Cancer Symposium 29-30 April 2016 Crowne Plaza Barcelona Fira Center, Barcelona, Spain Tim Eisen -
Will All Adjuvant Therapy Trials Be Negative in RCC? Tim Eisen Eleventh European International Kidney Cancer Symposium 29-30 April 2016 Crowne Plaza Barcelona Fira Center, Barcelona, Spain Tim Eisen -
Overview: Immunotherapy in CNS Metastases
 Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
UPDATE OF EASL CLINICAL PRACTICE GUIDELINES: MANAGEMENT OF HEPATOCELLULAR CARCINOMA*
 UPDATE OF EASL CLINICAL PRACTICE GUIDELINES: MANAGEMENT OF HEPATOCELLULAR CARCINOMA* Dr. Catherine Frenette Medical Director of Liver Transplantation, Scripps Green Hospital, La Jolla, CA, USA May 2018
UPDATE OF EASL CLINICAL PRACTICE GUIDELINES: MANAGEMENT OF HEPATOCELLULAR CARCINOMA* Dr. Catherine Frenette Medical Director of Liver Transplantation, Scripps Green Hospital, La Jolla, CA, USA May 2018
Immunotherapy for the Treatment of Head and Neck Cancers. Barbara Burtness, MD Yale University
 Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
II sessione. Immunoterapia oltre la prima linea. Alessandro Tuzi ASST Sette Laghi, Varese
 II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy