Modern Aspects in Lymphoma Diagnostics Prognosis and Prediction. Alexandar Tzankov
|
|
|
- Ernest Mills
- 5 years ago
- Views:
Transcription
1 Modern Aspects in Lymphoma Diagnostics Prognosis and Prediction Alexandar Tzankov
2 Introduction Prognostic and predictive markers Conclusions
3 Introduction Prognostic and predictive markers Conclusions
4 Quiz for clinicians In my daily routine I ask the diagnostic disciplines for prognostic/predictive markers in lymphomas 1. No, I am not aware of such markers 2. No, they do not influence my decision 3. Sometimes, after reading a paper 4. Yes 5. Only in relapsed or treatment-resistant cases
5 Quiz for diagnosticians In my daily routine I test lymphomas for prognostic/predictive markers 1. No, I am not aware of such markers 2. No, nobody is interested in such markers 3. Sometimes, after reading a paper 4. Yes 5. Only if required by the physician



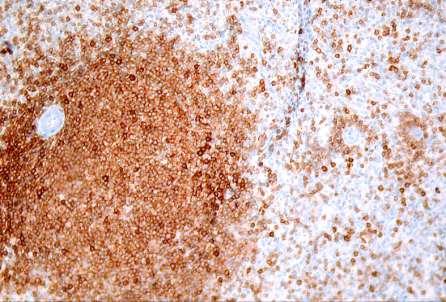
6 55 y, male, diagnostic splenectomy CD20 TRAP


7 52 y, female, diagnostic splenectomy CD5 Cyclin D1
8 Exact diagnosis - the best prognostic and predictive factor Splenic marginal zone lymphoma Good prognosis after splenectomy 50% probability of not needing further therapy Chance to be HBV or HCV+ (needing therapy) Splenic mantle cell lymphoma Poorer prognosis Need of staging Need of adjuvant chemotherapy
9 Mitterlchener 2006
10 Introduction Prognostic and predictive markers Conclusions
11 Prognostic markers Help to stratify patients for treatment by identifying patients with different risks of outcome and thus may improve their chance of survival fate May have medical economical aspects
12 Prognostic markers - requirements Categorize patients Reproducibly measurable Readily available assessment technology
13 WHO categorization prognostic value Lymphoma entities Sir Thomas Hodgkin Virchow ARP Gall/Mallory Rappaport Lukes/Collins IWF updated Kiel REAL/WHO WHO
14 Prognosis of T-cell lymphomas Savage 2008
15 Predictive markers Indicate sensitivity or resistance to a specific therapy Allow better identification of patients, who will positively respond to the therapy Minimizing unnecessary suffering from side effects Reducing cost to both the patient and the wider health community
16 Predictive markers - requirements Indicate specific response to a certain drug Reproducibly measurable Readily available assessment technology

17 WHO categorization predictive value Lymphoma entities Sir Thomas Hodgkin Virchow ARP Gall/Mallory Rappaport Lukes/Collins IWF updated Kiel REAL/WHO WHO
18 Cladribine is that efficient only in HCL Saven 1998


19 MZL of MALT are curable with antibiotics
20 Interactions between therapy and prognostic markers ABVD Van Spronsen 1996 COPP
21 Interaction between therapy and prognostic markers with R no R Canioni 2008

22 Prognosis and prediction in lymphomas, beyond WHO DLBCL Hodgkin lymphoma FL and MCL T-cell lymphomas
23 Diffuse large B-cell lymphoma (DLBCL)

24 Therapy - the main prognosticator
25 Quiz In my daily routine I rely on DLBCL prognosis and treatment choice on 1. Gut feeling 2. IPI 4. Stage 5. Specific disease subtypes 6. All above




26 DLBCL heterogeneity
27 IPI challenges to the gold standard In R-CHOP treated cases IPI can not identify patients with <50% chance of survival (Sehn 2007) IPI 3-5 have similar outcomes under R-CHOP, but not IPI 0-2 (Ziepert 2010) In low IPI patients, tumor bulk is a risk factor (Pfreundschuh 2006) In relapsing patients time to relapse is of more significant prognostic value than IPI (Gisselbrecht 2010)
28 Does morphology further matter? DLBCL, NOS Centroblastic Immunoblastic Anaplastic Plasmablastic T-cell-/histiocyte-rich Lymphomatoid granulomatosis (Grade 3)
29 Immunoblastic vs centroblastic 1997 centroblastic immunoblastic Engelhard 1997

30 Immunoblastic vs centroblastic 2010 Ott 2010
31 Ott 2010

32 Plasmablastic DLBCL Tzankov 2004



33 T-cell-/histiocyte-rich LBCL



34 T-cell-/histiocyte-rich LBCL




35 THRBCL are not NPLHL
36 THRBCL are not NPLHL Biasoli 2009 & Bouabdallah 2003


37 Lymphomatoid granulomatosis
38 Predictive importance of the morphological variants of DLBCL Poorer response of immunoblastic DLBCL to R-CHOP Lacking Rituximab target in plasmablastic DLBCL A role for immune modulation (EBV specific CTC) in plasmablastic DLBCL and lymphomatoid granulomatosis?

39 Genetic heterogeneity of DLBCL Monti 2005

40 Genetic heterogeneity of DLBCL Alizadeh 2000
41 Event-free survival of DLBCL

42 ABC - a predictive factor Dunleavy 2009
43
44 Predictive importance of the gene expression profile variants Selective sensitivity to Bortezomib (ABC > GCB) Lenalidomide (ABC > GCB) Temsirolimus (GCB, PTEN loss of function) Enzastaurin (PKC ABC without NF- B mutations) Fostematinib (Syk, ABC dependent on BCR signaling) Hampered by unavailability of detection technology for mass analyses and poor reproducibility
45 Immunohistochemistry as a surrogate for gene expression profiling Meyer 2011
46 Reproducibility of semiquantitative immunohistochemical stainings of the Choi algorythm between observers and institutions

47 Basel Oxford Bcl-6 GCET1

48 Results Lawrie 2012
49 Gutierrez-Garcia 2011
50 Why are phenotypic markers less robust? Tissue preservation bias Subjective evaluation Poorly working antibodies Poor choice of markers Fail to consider +/- controls Poor choice of cut-offs Dependence on the applied therapy

51 Cut-off scores of prognostic phenotypic markers in DLBCL Tzankov 2008
52 ROC analysis as a powerful tool to choose proper prognostic cut-offs Tzankov 2010
53 ROC analysis as a powerful tool chose proper prognostic cut-offs Tzankov 2010
54 Prognostic markers with Rituximab Rituximab abolished the prognostic effect of Bcl-2 expression in DLBCL (Mounier 2003) Rituximab abolished the prognostic effect of Bcl-6 rearrangements/expression (Winter 2006) HIF1 correlates with better PFS in DLBCL with R-CHOP, but not CHOP, since HIF can regulate CD20 expression (Ahmed 2009)
55 BCL6 breaks and prognosis
56 DLBCL, topographically-defined entities Primary DLBCL of the CNS (of testis) Primary mediastinal B-cell lymphoma Primary cutaneous DLBCL, leg-type




57 Primary DLBCL of CNS, decreased efficacy of Rituximab Pharmacokinetic effects of the blood-brain barrier
58 Quiz When choosing Rituximab treatment I 1. Apply it to all B-cell lymphomas 2. Always ask the diagnostician about CD20 expression 3. Ask the diagnostician about CD20 expression only in relapses 4. Apply it especially in MZL 5. Perform a HBV screening

59 CD20 expression in B-cell lymphomas



60 -cell markers in MZL differentiation


61 -cell markers Genetic reporgramming e.g. c-myc abnormalities Hoeller 2008

62 ALK1+ DLBCL

63 -cell markers, -cell markers Genuine negativity for the respective marker EBV Tzankov 2004


64 -cell markers Oncogenic loss of B-cell identity Adams 2008




65 DLBCL of the testis CD20 Ki67 FOXP1
66 DLBCL of immune-privileged sites Booman 2008
67 DLBCL of immune-privileged sites More aggressive than most DLBCL Frequent relapses at other immuneprivileged sites


68 Rosenwald 2003 Primary mediastinal B-cell lymphoma
 gains at 2p16 (REL locus) Meier 2009")
69 HL and PMBL closely related Clinically Mediastinal mass, young adults, F > M Morphologically Sclerosis, Reed-Sternberg-like cells Phenotypically CD30, no surface immunoglobulins decreased expression of OCT.2, BOB-1 Genotypically gains at 9p24 (JAK2 and PD1L locus) gains at 2p16 (REL locus) Meier 2009

70 CD20 CD30 CD15 Traverse-Glehen 2005

71 CD30 OCT-2 Traverse-Glehen 2005
72 Definition - B-cell lymphoma with overlapping features of HL/DLBCL clinical, morphological, phenotypic - Transitional phenotype, usually CD45+ Preserved B-cell signature (CD79a, BOB-1, OCT.2) Expression of CD30 and CD15 True grey zone cases Composite synchronous cases Sequential cases

73 Histopathological diagnosis most important predictive marker Hodgkin lymphoma Risk-adapted ABVD- or BEACOPP with or without irradiation Primary mediastinal B-cell lymphoma (R-)CHOP, (R-)MACOP-B, R-EPOCH Adjuvant radiotherapy does not offer survival benefit 10 CR/11 grey zone patients, 44% required radiation for CR OS and PFS at 4 years 86% and 57%, respectively Only 3 CR/12 HL patients treated with CHOP Dunleavy 2009 Miller 1983
 Irreproducible category Kappa among 7 experts = 0.")
74 Problematic issues Very problematic for treating physicians Seductive category (basket for difficult cases) Irreproducible category Kappa among 7 experts = 0.35

75 Hoeller 2010
76 Take home messages HL and PMBLC are closely related clinically, morphologically, pheno- and genotypically But Are treated in different ways Grey zones should be kept as few as possible Detailed phenotypic examination may help to classify most cases properly CD79a, BOB1, p63, CD45, CD23 and LMO2 (+ in PMBL) Cyclin E, MUM1, CD15 and LMP/EBER (+ in chl)
77 Some more grey zone issues Grey zones HL/DLBCL are not limited to the mediastinum and not limited to the differential of PMBL Classical HL/TCRBCL Classical HL/EBV+ DLBCL of elderly and EBV+ LPL NLPHL/TCRBCL
78 Lymphomas with special clinical context Paediatric type FL Paediatric type NMZL EBV+ T-cell LPD of childhood EBV+ DLBCL of the elderly


79 EBV+ DLBCL of the elderly EBNA 2 EBV+ >50J No immune deficiency or previous lymphoma Exclusion of LyG, PBL, PEL, HL, IM Poor prognosis 8% of DLBCL in Asia, 2.5% in Europe Hoeller 2010




80 Chronic inflammation associated DLBCL Pyothorax-associated DLBCL DLBCL associated with infected vascular prostheses DLBCL in arthritic joints can be diagnosed only integratively in >70% associated with EBV and CD20-negative
81 Predictive importance of lymphomas with special clinical context Modulation of immune defects is a treatment option EBV-antiviral therapy in latency type III (EBNA 2+) EBV-specific CTC in all EBV-associated cases Explant of prostheses in analogy to ALCL with breast implants
82 Quiz When treating/diagnosing DLBCL I 1. Always ask for the MYC status 2. Knowledge of the MYC status does not influence my therapy decision 3. Ask for the MYC status only in young patients 4. Perform a CNS prophylaxis in MYC rearranged cases 5. Analyze MYC only in high Ki-67 instances

 poor prognosis with CHOP very poor if accompanied by")
83 DLBCL, C-MYC and Burkitt DLBCL 20 x more common than Burkitt in adults Burkitt 3 x more common than DLBCL in children C-MYC rearrangements in 5-9% of DLBCL unpredictable by morphology (Obermann 2009) poor prognosis with CHOP very poor if accompanied by additional aberrations

84




85 DLBCL vs Burkitt mbl index >.95 mbl index <.05
86 DLBCL vs Burkitt Hummel 2006
87 Open questions Is there still a prognostic role of the C-MYC gene status in R-CHOP treated DLBCL? Does the type of C-MYC gene aberrations play a distinct prognostic role?
88 Study design 601 patients with de novo DLBCL treated with R-CHOP and 332 patients treated with CHOP all with clinical follow-up and GEP data Interphase FISH for C-MYC gene abnormalities C-MYC break-apart probe (BAP) IgH/C-MYC double-fusion probe (DFP)
89 Results CHOP 217/332 evaluable (65%) R-CHOP 455/601 evaluable (76%)

90

91

92

93
94 Results
95 Results
96 Discussion kb ebl Exon 1 Exon 2 Exon 3 sbl HIV BL alternative
97 Conclusions C-MYC aberrations are detectable in 10% of DLBCL more commonly in GCB Alternative C-MYC rearrangements account for 3% C-MYC aberrations detected by BAP add independent prognostic information for individual DLBCL risk estimation in R-CHOP treated cases
98 Courtesy of Prof. Klapper
99 Predictive importance of MYC aberrations in DLBCL Lessons from children MYC translocations in molecular Burkitt and nonmolecular Burkitt are not of negative prognostic value if treated like Burkitt MYC rearranged DLBCL are often GCB and R-CHOP resistant DA-EPOCH-R or Burkitt-therapies in adults?
100
101 DLBCL, progress through differentiation? We are the best prognostic and predictive factors Right diagnoses Proper therapies Different DLBCL variants and subtypes associated With distinct outcomes Distinct genetical background Differentiated treatment modalities no Rituximab in CD20-negative cases PBL, ALK+ DLBCL, PEL Smart small drugs? Immunomodulation? EBV-specific therapy? - MYC rearranged cases?
102 Follicular lymphoma (FL)
103 FL, prognostic/predictive factors FLIPI sustained its role in the R era (Hiddemann 2005, Buske 2006) In stage I and II FLIPI does not identify patients at risk, but PET does 90% of PET+ progress within 2 years compared to 20% of PET- (Zinzani 2007) BM involvement - contraindication for radiolabeled anti-cd20 approaches

104 Dave 2004


105 High FOXP3 cell numbers better outcome Tzankov 2008
106 Prognostic importance of PD1+ T-cells Carreras 2009

107 Muenst 2010
108 Rituximab abolishes the prognostic significance of macrophages Canioni 2008

109 Relander 2010
110 Mantle cell lymphoma (MCL)
111 GEP risk groups are reflected by Ki-67
112 Hodgkin lymphoma (HL)
113 Quiz When treating/diagnosing Hodgkin lymphoma I 1. Not interested in subtyping since treatment is the same 2. Treat classical and NLPHL in a different manner 3. Treat classical and NLPHL in a different manner only in stage I & II 4. Interested in subtyping only for prognosis


114 Classical HL or nodular paragranuloma? Reed-Sternberg cell


115 Classical HL or nodular paragranuloma? Reed-Sternberg cell
116 Best predictor in stage I & II Classical HL chemotherapy (ABVD) +/- radiation Nodular paragranuloma chirurgical excision +/- Rituximab +/- radiation (+)/- chemotherapy Fong 2009
117 HL, prognostic/predictive factors Stage, B-symptoms IPS identifies only patients at very high risk (Hasenclever 1998) For low risk patients - low serum albumin and extranodal site of prognostic value (Franklin 2000) PET Post-therapy - prognostic with 90% specificity and sensitivity (Zijlstra 2006) Interim - reliable to identify poor responders
118 HL, tumor-related prognostic factors - it is all in the background! Eosinophils better prognosis (Wassliewski 2000) Mast cells - worse prognossi (Canioni 2009) Macrophages worse prognosis (Steidl 2010) Granzyme B - worse prognosis (Oudejans 1997) FOXP3 + - better prognosis (Tzankov 2008) B-cells - better prognosis (Chetaille 2009)

119 Steidl 2011


120 A possible prognostic role of macrophages
121 Steidl 2010

122 CD68 low CD68 high Cut off: >1% with respect to OS prognostic sensitivity: 75% prognostic specificity: 65% Tzankov 2010
123 Prognostic significance of CD68- positive tumor macrophages in HL Tzankov 2010

124 FOXP3 Tzankov 2008

125 Prognostic significance of PD1-positive tumor-infiltrating lymphocytes in HL Muenst 2009
126 Prognosis of chl with respect to the cellular background composition Muenst 2009


127 Predictive importance for differential immunomodulation? Steroids, Rapamycin, allo-sctx
128 Do we need tumor-cell related prognostic/predictive factors in HL? Fong 2009

129

130 Problems with the specificity of HDI due to omnipresence of targets Adams 2010

131 Survival of HL after relapse



132 Every fifth relapse is clonally unrelated Obermann 2011
133 T-cell lymphomas (TCL)
134 Prognosis of T-cell lymphomas Savage 2008
135 TCL IPI is valid in T-NHL Prognostic index for PTLC (PIT) bone marrow involvement, age, ECOG and LDH (Gallamini 2004) Prognostic index for NK cell lymphomas non-nasal location, stage and ECOG (Suzuki 2010)
136 TCL, tumor related prognostic markers Ki-67 >80%, EBV and CD15: worse prognosis in PTCL (Went 2006) >70% blasts, Ki-67 >25%, CD56, CD30, EBV: worse prognosis (Rudiger 2002) Cytotoxic phenotype in PTCL worse prognosis (Asano 2009)

137 PTCL, adverse role of cytotoxic phenotype Iqbal 2010
138 Predictive markers in TCL ALK1+: from molecular subtype to Crizotinib PTCL high PDGFR Imatinib (Piccaluga 2007) AITL high VEGF Bevacizumab (Piccaluga 2007, Bruns 2005) CD30-negative TCL express CD52 Alemtuzumab (Enblad 2004) CD30 a therapeutic target for Iratumumab, SGN-30 & 35 (Ansell 2008, Younes 2010) R-CHOP in AITL with lots of EBV-infected B-cells? (Skugor 2010) Nasal NK lymphomas low asparagin synthetase L-asplaraginase (Jaccard 2011)


139 PDGFR and VEGF in PTCL and AITL PDGFR VEGF VEGFR2 Piccaluga 2007
140 Introduction Prognostic and predictive markers Conclusions
141 Prognosis and prediction in lymphomas Precise diagnosis - best prognosticator and predictor Lots of potential tumor- and micromilieu-related prognostic markers Rational molecular targets identified prospective targeted molecular trials
142 Quiz The presentation 1. Was informative but would not change my management strategy 2. Was bad 3. Would somehow influence my management strategy 4. Forces me to look at the recent literature

143
144 Entity Factor Importance ALCL Expression of ALK1 Better prognosis, response to Crizotinib B-NHL CD20 Target of monoclonal antibodies like Rituximab DLBCL FL HL ABC subtype MYC-gene rearrangement Increased regulatory and follicular T-cells Increased regulatory T-cells Increased cytotoxic T-cells Increased macrophages MCL High proliferation Worse prognosis Worse prognosis, response to smart drugs Worse prognosis, poor response to R- CHOP, potential for Burkitt therapy protocols Better prognosis, better response to Rituximab Better prognosis Worse prognosis Worse prognosis, poorer response to HD- ASCT when relapsed MZL t(11;18) Resistance to Helicobacter pylori eradication (Liu, 2001)
Aggressive B-cell lymphomas and gene expression profiling towards individualized therapy?
 Aggressive B-cell lymphomas and gene expression profiling towards individualized therapy? Andreas Rosenwald Institute of Pathology, University of Würzburg, Germany Barcelona, June 18, 2010 NEW WHO CLASSIFICATION
Aggressive B-cell lymphomas and gene expression profiling towards individualized therapy? Andreas Rosenwald Institute of Pathology, University of Würzburg, Germany Barcelona, June 18, 2010 NEW WHO CLASSIFICATION
Defined lymphoma entities in the current WHO classification
 Defined lymphoma entities in the current WHO classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno Bellinzona, January 29-31, 2016 Evolution of lymphoma classification Rappaport Lukes
Defined lymphoma entities in the current WHO classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno Bellinzona, January 29-31, 2016 Evolution of lymphoma classification Rappaport Lukes
Aggressive B-Cell Lymphomas
 Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
Aggressive B-cell Lymphoma 2013
 Aggressive B-cell Lymphoma 2013 Diffuse Large B-Cell Lymphoma Burkitt Lymphoblastic lymphoma Gray zone Intermediate DLBCL/HL Intermediate BL/DLBCL Diffuse Large B-cell lymphoma Common morphology: diffuse
Aggressive B-cell Lymphoma 2013 Diffuse Large B-Cell Lymphoma Burkitt Lymphoblastic lymphoma Gray zone Intermediate DLBCL/HL Intermediate BL/DLBCL Diffuse Large B-cell lymphoma Common morphology: diffuse
Aggressive B-cell Lymphomas
 Neoplastic Hematopathology Update 2018 Aggressive B-cell Lymphomas Raju K. Pillai City of Hope National Medical Center I do not have any disclosures Disclosures Outline New entities and changes in WHO
Neoplastic Hematopathology Update 2018 Aggressive B-cell Lymphomas Raju K. Pillai City of Hope National Medical Center I do not have any disclosures Disclosures Outline New entities and changes in WHO
Immunopathology of Lymphoma
 Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Pathology of aggressive lymphomas
 Institute of Pathology Pathology of aggressive lymphomas Leticia Quintanilla-Martinez Changes in the new 2016 WHO Aggressive B-cell lymphoid neoplasms Major changes that impact how cases should be evaludated
Institute of Pathology Pathology of aggressive lymphomas Leticia Quintanilla-Martinez Changes in the new 2016 WHO Aggressive B-cell lymphoid neoplasms Major changes that impact how cases should be evaludated
Aggressive B cell Lymphomas
 Aggressive B cell Lymphomas I have nothing to disclose. Disclosures Raju K. Pillai City of Hope National Medical Center Outline WHO 2016 Classification Large B cell Lymphomas New entities and changes in
Aggressive B cell Lymphomas I have nothing to disclose. Disclosures Raju K. Pillai City of Hope National Medical Center Outline WHO 2016 Classification Large B cell Lymphomas New entities and changes in
The next lymphoma classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno
 Evolution of classification The next classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno The Lymphoma Forum of Excellence, Bellinzona, January 2011 Rappaport Lukes and Collins (immunophenotype)
Evolution of classification The next classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno The Lymphoma Forum of Excellence, Bellinzona, January 2011 Rappaport Lukes and Collins (immunophenotype)
NEW ENTITIES IN AGGRESSIVE B CELL LYMPHOMA. Joon Seong Park, M.D. Dept. of Hematology-Oncology Ajou University School of Medicine
 NEW ENTITIES IN AGGRESSIVE B CELL LYMPHOMA Joon Seong Park, M.D. Dept. of Hematology-Oncology Ajou University School of Medicine Historical background of Lymphoma classification Rappaport classification
NEW ENTITIES IN AGGRESSIVE B CELL LYMPHOMA Joon Seong Park, M.D. Dept. of Hematology-Oncology Ajou University School of Medicine Historical background of Lymphoma classification Rappaport classification
High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li,
: Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li,") High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li, M.D., Ph.D. Fudan University Shanghai Cancer Center
High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li, M.D., Ph.D. Fudan University Shanghai Cancer Center
Pathology of aggressive lymphomas
 Institute of Pathology Pathology of aggressive lymphomas Leticia Quintanilla-Martinez Changes in the new 2016 WHO Aggressive B-cell lymphoid neoplasms Major changes that impact how cases should be evaludated
Institute of Pathology Pathology of aggressive lymphomas Leticia Quintanilla-Martinez Changes in the new 2016 WHO Aggressive B-cell lymphoid neoplasms Major changes that impact how cases should be evaludated
Conflict of Interest Disclosure Form NAME :James O. Armitage, M.D AFFILIATION: University of Nebraska Medical Center
 What Is Personalized Medicine For Patients With Lymphoma? Conflict of Interest Disclosure Form NAME :James O. Armitage, M.D AFFILIATION: University of Nebraska Medical Center DISCLOSURE I have no potential
What Is Personalized Medicine For Patients With Lymphoma? Conflict of Interest Disclosure Form NAME :James O. Armitage, M.D AFFILIATION: University of Nebraska Medical Center DISCLOSURE I have no potential
Aggressive B cell Lymphomas
 Aggressive B cell Lymphomas Raju K. Pillai City of Hope National Medical Center I have no disclosures Outline What is new in the WHO 2016 classification Insights from genomic studies Double Hit Lymphoma
Aggressive B cell Lymphomas Raju K. Pillai City of Hope National Medical Center I have no disclosures Outline What is new in the WHO 2016 classification Insights from genomic studies Double Hit Lymphoma
Aggressive B-cell Lymphomas Updated WHO classification Elias Campo
 Aggressive B-cell Lymphomas Updated WHO classification Elias Campo Hospital Clinic, University of Barcelona Diffuse Large B-cell Lymphoma A Heterogeneous Category Subtypes with differing: Histology and
Aggressive B-cell Lymphomas Updated WHO classification Elias Campo Hospital Clinic, University of Barcelona Diffuse Large B-cell Lymphoma A Heterogeneous Category Subtypes with differing: Histology and
Large cell immunoblastic Diffuse histiocytic (DHL) Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s
 Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s") Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Update on the Classification of Aggressive B-cell Lymphomas and Hodgkin Lymphoma
 Update on the Classification of Aggressive B-cell Lymphomas and Hodgkin Lymphoma Nancy Lee Harris, M. D. Massachusetts General Hospital Harvard Medical School Aggressive B-cell Lymphomas WHO 4 th Edition
Update on the Classification of Aggressive B-cell Lymphomas and Hodgkin Lymphoma Nancy Lee Harris, M. D. Massachusetts General Hospital Harvard Medical School Aggressive B-cell Lymphomas WHO 4 th Edition
Common Problem Areas. WHO Classification. Defines separate diseases (entities) with their CLINICAL AGGRESSIVENESS LOW GRADE / HIGH GRADE
 with their CLINICAL AGGRESSIVENESS LOW GRADE / HIGH GRADE") WHO Classification Defines separate diseases (entities) with their CLINICAL AGGRESSIVENESS REVIEW OF MOST COMMON LYMPHOMA ENTITIES Dr Stefan Dojcinov LOW GRADE / HIGH GRADE (June 2014) The Non-Hodgkin
WHO Classification Defines separate diseases (entities) with their CLINICAL AGGRESSIVENESS REVIEW OF MOST COMMON LYMPHOMA ENTITIES Dr Stefan Dojcinov LOW GRADE / HIGH GRADE (June 2014) The Non-Hodgkin
Non-Hodgkin s Lymphomas Version
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
Diffuse large B-cell lymphomas. G. Verhoef, MD, PhD University Hospital Leuven BHS, March 9, 2013
 Diffuse large B-cell lymphomas G. Verhoef, MD, PhD University Hospital Leuven BHS, March 9, 2013 Case A 72-year-old previously healthy man presented with acute abdominal pain and a 15 kg weight loss. Positron
Diffuse large B-cell lymphomas G. Verhoef, MD, PhD University Hospital Leuven BHS, March 9, 2013 Case A 72-year-old previously healthy man presented with acute abdominal pain and a 15 kg weight loss. Positron
Recent advances in the genetics & biology of lymphoma
 Recent advances in the genetics & biology of lymphoma Chris Bacon Northern Institute for Cancer Research Newcastle University & Newcastle Upon Tyne Hospitals NHS Foundation Trust Lymphoma Rate per 100,000
Recent advances in the genetics & biology of lymphoma Chris Bacon Northern Institute for Cancer Research Newcastle University & Newcastle Upon Tyne Hospitals NHS Foundation Trust Lymphoma Rate per 100,000
Aggressive NHL and Hodgkin Lymphoma. Dr. Carolyn Faught November 10, 2017
 Aggressive NHL and Hodgkin Lymphoma Dr. Carolyn Faught November 10, 2017 What does aggressive mean? Shorter duration of symptoms Generally need treatment at time of diagnosis Immediate, few days, few weeks
Aggressive NHL and Hodgkin Lymphoma Dr. Carolyn Faught November 10, 2017 What does aggressive mean? Shorter duration of symptoms Generally need treatment at time of diagnosis Immediate, few days, few weeks
Exploring the Borderlands between Diffuse Large B-cell Lymphoma and Classical Hodgkin s Lymphoma
 Exploring the Borderlands between Diffuse Large B-cell Lymphoma and Classical Hodgkin s Lymphoma Elaine S. Jaffe National Cancer Institute Bethesda, MD, USA On the Pathological Changes In Hodgkin s Disease
Exploring the Borderlands between Diffuse Large B-cell Lymphoma and Classical Hodgkin s Lymphoma Elaine S. Jaffe National Cancer Institute Bethesda, MD, USA On the Pathological Changes In Hodgkin s Disease
2012 by American Society of Hematology
 2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
Aggressive lymphomas ASH Dr. A. Van Hoof A.Z. St.Jan, Brugge-Oostende AV
 Aggressive lymphomas ASH 2015 Dr. A. Van Hoof A.Z. St.Jan, Brugge-Oostende AV CHOP 1992 2002 R-CHOP For DLBCL High dose chemo With PBSCT Aggressive lymphomas 1.DLBCL 2.Primary Mediastinal Lymphoma 3.CNS
Aggressive lymphomas ASH 2015 Dr. A. Van Hoof A.Z. St.Jan, Brugge-Oostende AV CHOP 1992 2002 R-CHOP For DLBCL High dose chemo With PBSCT Aggressive lymphomas 1.DLBCL 2.Primary Mediastinal Lymphoma 3.CNS
Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009
 Treatment of DLBCL Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009 Non-hodgkin lymphomas DLBCL Most common NHL subtype throughout the world many other types of lymphoma with striking geographic variations
Treatment of DLBCL Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009 Non-hodgkin lymphomas DLBCL Most common NHL subtype throughout the world many other types of lymphoma with striking geographic variations
IX. Is it only about MYC? How to approach the diagnosis of diffuse large B-cell lymphomas
 Hematological Oncology Hematol Oncol 2015; 33: 50 55 Published online in Wiley Online Library (wileyonlinelibrary.com).2217 Supplement Article IX. Is it only about MYC? How to approach the diagnosis of
Hematological Oncology Hematol Oncol 2015; 33: 50 55 Published online in Wiley Online Library (wileyonlinelibrary.com).2217 Supplement Article IX. Is it only about MYC? How to approach the diagnosis of
Immunohistochemical classification of haematolymphoid tumours. Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital
 Immunohistochemical classification of haematolymphoid tumours Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital Malignant lymphoproliferative diseases What are they? Haematolymphoid
Immunohistochemical classification of haematolymphoid tumours Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital Malignant lymphoproliferative diseases What are they? Haematolymphoid
3/23/2017. Disclosure of Relevant Financial Relationships. Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?!
 Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?! Judith A. Ferry Massachusetts General Hospital Disclosure of Relevant Financial Relationships USCAP requires that all
Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?! Judith A. Ferry Massachusetts General Hospital Disclosure of Relevant Financial Relationships USCAP requires that all
Methods used to diagnose lymphomas
 Institut für Pathologie Institut für Pathologie Methods used to diagnose lymphomas Prof. Dr.Med. Leticia Quintanilla-Fend Molecular techniques NGS histology Cytology AS-PCR Sanger seq. MYC Immunohistochemistry
Institut für Pathologie Institut für Pathologie Methods used to diagnose lymphomas Prof. Dr.Med. Leticia Quintanilla-Fend Molecular techniques NGS histology Cytology AS-PCR Sanger seq. MYC Immunohistochemistry
EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH
 EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH CASE E1 M: 68 yrs Left destructive sinonasal lesion.?lymphoma?adenocarcinoma CD20 CD10 BCL6 MIB1 Answers Diffuse large B cell
EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH CASE E1 M: 68 yrs Left destructive sinonasal lesion.?lymphoma?adenocarcinoma CD20 CD10 BCL6 MIB1 Answers Diffuse large B cell
Lymphoma Update: Lymphoma Update: What s Likely to be New in the New WHO. Patrick Treseler, MD, PhD University of California San Francisco
 Lymphoma Update: What s Likely to be New in the New WHO Blood 127:2375; 2016 Patrick Treseler, MD, PhD University of California San Francisco Lymphoma Update: What IS New in the New WHO! Patrick Treseler,
Lymphoma Update: What s Likely to be New in the New WHO Blood 127:2375; 2016 Patrick Treseler, MD, PhD University of California San Francisco Lymphoma Update: What IS New in the New WHO! Patrick Treseler,
Prognostic Factors for PTCL. Julie M. Vose, M.D., M.B.A. University of Nebraska Medical Center
 Prognostic Factors for PTCL Julie M. Vose, M.D., M.B.A. University of Nebraska Medical Center jmvose@unmc.edu Distribution of 1314 Cases by Consensus Diagnosis International T-Cell Lymphoma Project Vose
Prognostic Factors for PTCL Julie M. Vose, M.D., M.B.A. University of Nebraska Medical Center jmvose@unmc.edu Distribution of 1314 Cases by Consensus Diagnosis International T-Cell Lymphoma Project Vose
Aggressive Lymphomas - Current. Dr Kevin Imrie Physician-in-Chief, Sunnybrook Health Sciences Centre
 Aggressive Lymphomas - Current Dr Kevin Imrie Physician-in-Chief, Sunnybrook Health Sciences Centre Conflicts of interest I have no conflicts of interest to declare Outline What does aggressive lymphoma
Aggressive Lymphomas - Current Dr Kevin Imrie Physician-in-Chief, Sunnybrook Health Sciences Centre Conflicts of interest I have no conflicts of interest to declare Outline What does aggressive lymphoma
Many of the hematolymphoid disorders are derived
 REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
WHO 4th ED Classification of Mature B-cell Neoplasms
 WHO 4th ED Classification of Mature B-cell Neoplasms Chronic lymphocytic leukemia /Small lymphocytic lymphoma B-cell prolymphocytic leukaemia Splenic marginal zone lymphoma Hairy cell leukemia Splenic
WHO 4th ED Classification of Mature B-cell Neoplasms Chronic lymphocytic leukemia /Small lymphocytic lymphoma B-cell prolymphocytic leukaemia Splenic marginal zone lymphoma Hairy cell leukemia Splenic
Use of MYC, BCL2 and BCL6 FISH for investigations of high grade B cell lymphoma
 Use of MYC, BCL2 and BCL6 FISH for investigations of high grade B cell lymphoma Dr Anthony Bench Haematopathology and Oncology Diagnostic Service Cambrıdge Unıversıty Hospitals NHS Foundatıon Trust Cambridge
Use of MYC, BCL2 and BCL6 FISH for investigations of high grade B cell lymphoma Dr Anthony Bench Haematopathology and Oncology Diagnostic Service Cambrıdge Unıversıty Hospitals NHS Foundatıon Trust Cambridge
Mediastinal B-cell Lymphomas
 Mediastinal B-cell Lymphomas A Spectrum of Diseases Wyndham H. Wilson, MD, PhD Mediastinal B-cell Lymphomas Nodular sclerosis Hodgkin Lymphoma Mediastinal grey zone lymphoma Primary mediastinal B-cell
Mediastinal B-cell Lymphomas A Spectrum of Diseases Wyndham H. Wilson, MD, PhD Mediastinal B-cell Lymphomas Nodular sclerosis Hodgkin Lymphoma Mediastinal grey zone lymphoma Primary mediastinal B-cell
Hepatic Lymphoma Diagnosis An Algorithmic Approach
 Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
HIV ASSOCIATED LYMPHOMA. Dr N Rapiti
 HIV ASSOCIATED LYMPHOMA Dr N Rapiti HIV ASSOCIATED LYMPHOMA: OVERVIEW Classification Pathogenesis Prognosis cart Chemotherapy/Radiotherapy/SCT Supportive CASE 40 yr old male, Mr BM, p/w Symptomatic anemia
HIV ASSOCIATED LYMPHOMA Dr N Rapiti HIV ASSOCIATED LYMPHOMA: OVERVIEW Classification Pathogenesis Prognosis cart Chemotherapy/Radiotherapy/SCT Supportive CASE 40 yr old male, Mr BM, p/w Symptomatic anemia
10/31/2017. Immunodeficiencies. Outline. Discuss EBV. Non-destructive Polymorphic Monomorphic Therapies Challenges
 I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Outline Transplant Congenital Autoimmunity T-cell/immune
I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Outline Transplant Congenital Autoimmunity T-cell/immune
11/2/2017. Immunodeficiencies. Joo Y. Song, MD Assistant Professor of Clinical Pathology. I have no financial disclosures.
 I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Transplant Autoimmunity Drugs T-cell dysfunction (Age,
I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Transplant Autoimmunity Drugs T-cell dysfunction (Age,
Incidence. Bimodal age incidence 15-40, >55 years Childhood form (0-14) more common in developing countries M:F=1.5:1; in all subtypes except NS
 more common in developing countries M:F=1.5:1; in all subtypes except NS") Hodgkin Lymphoma Hodgkin Lymphoma 30% of all lymphomas Absolute incidence unchanged Arise in lymph node, cervical region Neoplastic tissues usually contain a small number of tumor cells Incidence Bimodal
Hodgkin Lymphoma Hodgkin Lymphoma 30% of all lymphomas Absolute incidence unchanged Arise in lymph node, cervical region Neoplastic tissues usually contain a small number of tumor cells Incidence Bimodal
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies
 Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Diffuse large B-cell lymphoma (DLBCL) is one of the
 is one of the") Practical Applications in Immunohistochemistry Evaluation of Diffuse Large B-Cell Lymphoma and Related Large B-Cell Lymphomas Dennis P. O Malley, MD; Aaron Auerbach, MD; Lawrence M. Weiss, MD Context.
Practical Applications in Immunohistochemistry Evaluation of Diffuse Large B-Cell Lymphoma and Related Large B-Cell Lymphomas Dennis P. O Malley, MD; Aaron Auerbach, MD; Lawrence M. Weiss, MD Context.
MANAGEMENT OF LYMPHOMAS
 MANAGEMENT OF LYMPHOMAS Challenges & Recommendations F. Chite Asirwa, MD. Internal Medicine Physician Medical Oncologist & Hematologist Director-AMPATH Oncology & Hematology @Kenya Physicians Association
MANAGEMENT OF LYMPHOMAS Challenges & Recommendations F. Chite Asirwa, MD. Internal Medicine Physician Medical Oncologist & Hematologist Director-AMPATH Oncology & Hematology @Kenya Physicians Association
The History of Lymphoma Classification and the 2017 Revision
 The History of Lymphoma Classification and the 2017 Revision ESMO Perceptorship on Lymphoma, Lugano 2018 German Ott Department of Clinical Pathology, Robert-Bosch-Krankenhaus and Dr. Margarete Fischer-Bosch
The History of Lymphoma Classification and the 2017 Revision ESMO Perceptorship on Lymphoma, Lugano 2018 German Ott Department of Clinical Pathology, Robert-Bosch-Krankenhaus and Dr. Margarete Fischer-Bosch
Change Summary - Form 2018 (R3) 1 of 12
 1 of 12") Summary - Form 2018 (R3) 1 of 12 Form Question Number (r3) Type Description New Text Previous Text Today's date was removed 2018 N/A Today's Date Removed from Key Fields 2018 N/A HCT Type 2018 N/A Product
Summary - Form 2018 (R3) 1 of 12 Form Question Number (r3) Type Description New Text Previous Text Today's date was removed 2018 N/A Today's Date Removed from Key Fields 2018 N/A HCT Type 2018 N/A Product
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Diffuse Large B-Cell Lymphoma (DLBCL)
") Diffuse Large B-Cell Lymphoma (DLBCL) DLBCL/MCL Dr. Anthea Peters, MD, FRCPC University of Alberta/Cross Cancer Institute Disclosures Honoraria from Janssen, Abbvie, Roche, Lundbeck, Seattle Genetics Objectives
Diffuse Large B-Cell Lymphoma (DLBCL) DLBCL/MCL Dr. Anthea Peters, MD, FRCPC University of Alberta/Cross Cancer Institute Disclosures Honoraria from Janssen, Abbvie, Roche, Lundbeck, Seattle Genetics Objectives
Hodgkin Lymphomas: An Update
 Hodgkin Lymphomas: An Update Roberto N. Miranda, M.D. Professor UT MD Anderson Cancer Center November 10 th, 2018 Disclosures Scientific Advisory Board, Allergan Inc, 2018 Hodgkin Lymphomas Classical Hodgkin
Hodgkin Lymphomas: An Update Roberto N. Miranda, M.D. Professor UT MD Anderson Cancer Center November 10 th, 2018 Disclosures Scientific Advisory Board, Allergan Inc, 2018 Hodgkin Lymphomas Classical Hodgkin
Lymphoma: The Basics. Dr. Douglas Stewart
 Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
Contents. vii. Preface... Acknowledgments... v xiii
 Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
OSCO/OU ASH-SABC Review. Lymphoma Update. Mohamad Cherry, MD
 OSCO/OU ASH-SABC Review Lymphoma Update Mohamad Cherry, MD Outline Diffuse Large B Cell Lymphoma Double Hit Lymphoma Follicular and Indolent B Cell Lymphomas Mantle Cell Lymphoma T Cell Lymphoma Hodgkin
OSCO/OU ASH-SABC Review Lymphoma Update Mohamad Cherry, MD Outline Diffuse Large B Cell Lymphoma Double Hit Lymphoma Follicular and Indolent B Cell Lymphomas Mantle Cell Lymphoma T Cell Lymphoma Hodgkin
Diagnostic Molecular Pathology of Lymphoid Neoplasms
 Diagnostic Molecular Pathology of Lymphoid Neoplasms (Part II) Rational use of molecular testing in lymphomas Beirut, Lebanon Friday December 2, 2011: Hematopathology Session Adam Bagg University of Pennsylvania
Diagnostic Molecular Pathology of Lymphoid Neoplasms (Part II) Rational use of molecular testing in lymphomas Beirut, Lebanon Friday December 2, 2011: Hematopathology Session Adam Bagg University of Pennsylvania
Highlights of ICML 2015
 Highlights of ICML 2015 Jonathan W. Friedberg M.D. Director, James P. Wilmot Cancer Center Statistics, ICML 2015: a global meeting Almost 3700 participants. 90 countries represented. Attendees: USA 465
Highlights of ICML 2015 Jonathan W. Friedberg M.D. Director, James P. Wilmot Cancer Center Statistics, ICML 2015: a global meeting Almost 3700 participants. 90 countries represented. Attendees: USA 465
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Prevalent lymphomas in Africa
 Prevalent lymphomas in Africa Dr Zainab Mohamed Clinical Oncologist GSH/UCT Groote Schuur Hospital Disclaimer I declare that I have no conflict of interest Groote Schuur Hospital Denis Burkitt 1911-1993
Prevalent lymphomas in Africa Dr Zainab Mohamed Clinical Oncologist GSH/UCT Groote Schuur Hospital Disclaimer I declare that I have no conflict of interest Groote Schuur Hospital Denis Burkitt 1911-1993
Classification! Immunohistochemical classification of haematolymphoid tumours. Malignant lymphoproliferative diseases
 Immunohistochemical classification of haematolymphoid tumours Haematolymphoid Neoplasias: Leukaemia vs Lymphoma C L O N A L M A L I G N A N C I E S Stephen Hamilton-Dutoit Institute of Pathology Aarhus
Immunohistochemical classification of haematolymphoid tumours Haematolymphoid Neoplasias: Leukaemia vs Lymphoma C L O N A L M A L I G N A N C I E S Stephen Hamilton-Dutoit Institute of Pathology Aarhus
Non-Hodgkin lymphoma
 Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
Non-Hodgkin lymphoma Non-Hodgkin s lymphoma Definition: - clonal tumours of mature and immature B cells, T cells or NK cells - highly heterogeneous, both histologically and clinically Non-Hodgkin lymphoma
Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge. ASH 2012 Atlanta
 Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge ASH 2012 Atlanta DLBCL How to improve on R-CHOP What at relapse Mantle cell lymphoma Do we cure patients Treatment at relapse Follicular lymphoma Watch and
Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge ASH 2012 Atlanta DLBCL How to improve on R-CHOP What at relapse Mantle cell lymphoma Do we cure patients Treatment at relapse Follicular lymphoma Watch and
5003 Immunohistochemistry in hematopathology, what's in, what's out, what's useful
 www.ascp.org/ascp2014 5003 Immunohistochemistry in hematopathology, what's in, what's out, what's useful Kathryn Rizzo, DO, PhD VIRGINIA COMMONWEALTH UNIVERSITY Department of Pathology School of Medicine
www.ascp.org/ascp2014 5003 Immunohistochemistry in hematopathology, what's in, what's out, what's useful Kathryn Rizzo, DO, PhD VIRGINIA COMMONWEALTH UNIVERSITY Department of Pathology School of Medicine
Small B-cell (Histologically Low Grade) Lymphoma
 Lymphoma") Frequency of Lymphoid Neoplasms Small B-cell (Histologically Low Grade) Lymphoma Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital B-cell neoplasms 88% Diffuse large B-cell lymphoma
Frequency of Lymphoid Neoplasms Small B-cell (Histologically Low Grade) Lymphoma Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital B-cell neoplasms 88% Diffuse large B-cell lymphoma
ESMO DOUBLE-HIT LYMPHOMAS
 ESMO DOUBLE-HIT LYMPHOMAS Professor Dr. med. Georg Lenz Director Department of Hematology and Oncology Universitätsklinikum Münster, Germany OVERVIEW Definition of double-hit lymphomas Introduction in
ESMO DOUBLE-HIT LYMPHOMAS Professor Dr. med. Georg Lenz Director Department of Hematology and Oncology Universitätsklinikum Münster, Germany OVERVIEW Definition of double-hit lymphomas Introduction in
Robert Carswell Cancer cerebriformis of the lymphatic glands and spleen
 Hodgkin s Lymphoma 1828 Robert Carswell Cancer cerebriformis of the lymphatic glands and spleen Hodgkin s Disease Historical Background 1832 T. Hodgkin On some morbid appearances of the absorbent glands
Hodgkin s Lymphoma 1828 Robert Carswell Cancer cerebriformis of the lymphatic glands and spleen Hodgkin s Disease Historical Background 1832 T. Hodgkin On some morbid appearances of the absorbent glands
Approach to Core Biopsy Specimens
 BDIAP 108th Symposium on Haematopathology Joint Meeting of the BDIAP and BLPG at-bristol, Anchor Road, Harbourside, Bristol BS1 5DB 15th - 17th May 2014 Approach to Core Biopsy Specimens Dr Stefan Dojcinov
BDIAP 108th Symposium on Haematopathology Joint Meeting of the BDIAP and BLPG at-bristol, Anchor Road, Harbourside, Bristol BS1 5DB 15th - 17th May 2014 Approach to Core Biopsy Specimens Dr Stefan Dojcinov
GENETIC MARKERS IN LYMPHOMA a practical overview. P. Heimann Dpt of Medical Genetics Erasme Hospital - Bordet Institute
 GENETIC MARKERS IN LYMPHOMA a practical overview P. Heimann Dpt of Medical Genetics Erasme Hospital - Bordet Institute B and T cell monoclonalities Rearrangement of immunoglobin and TCR genes may help
GENETIC MARKERS IN LYMPHOMA a practical overview P. Heimann Dpt of Medical Genetics Erasme Hospital - Bordet Institute B and T cell monoclonalities Rearrangement of immunoglobin and TCR genes may help
HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO
 HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO HODGKIN LYMPHOMA CLASSIFICATION Lukes & Butler Rye WHO-2016 Linphocytic and/or histiocytic Nodular & diffuse Nodular Sclerosis Lymphocyte
HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO HODGKIN LYMPHOMA CLASSIFICATION Lukes & Butler Rye WHO-2016 Linphocytic and/or histiocytic Nodular & diffuse Nodular Sclerosis Lymphocyte
Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège. 14 th post-ash meeting, January 6 th 2011, Brussels
 Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège 14 th post-ash meeting, January 6 th 2011, Brussels Hodgkin s lymphoma Follicular lymphoma Diffuse large B-cell lymphoma Mantle cell
Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège 14 th post-ash meeting, January 6 th 2011, Brussels Hodgkin s lymphoma Follicular lymphoma Diffuse large B-cell lymphoma Mantle cell
Low-grade B-cell lymphoma
 Low-grade B-cell lymphoma Patho-Basic 11. September 2018 Stephan Dirnhofer Pathology Outline Definition LPL, MBL/CLL/SLL, MCL FL Subtypes & variants Diagnosis including Grading Transformation Summary Be
Low-grade B-cell lymphoma Patho-Basic 11. September 2018 Stephan Dirnhofer Pathology Outline Definition LPL, MBL/CLL/SLL, MCL FL Subtypes & variants Diagnosis including Grading Transformation Summary Be
Chronic Lymphocytic Leukemia Mantle Cell Lymphoma Elias Campo
 Chronic Lymphocytic Leukemia Mantle Cell Lymphoma Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas NAIVE -B LYMPHOCYTE MEMORY CELL CLL MCL FL MZL Small cell size Low proliferation
Chronic Lymphocytic Leukemia Mantle Cell Lymphoma Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas NAIVE -B LYMPHOCYTE MEMORY CELL CLL MCL FL MZL Small cell size Low proliferation
Pathology of the indolent B-cell lymphomas Elias Campo
 Pathology of the indolent B-cell lymphomas Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas Antigen selection NAIVE -B LYMPHOCYTE MEMORY B-CELL MCL FL LPL MZL CLL Small cell
Pathology of the indolent B-cell lymphomas Elias Campo Hospital Clinic, University of Barcelona Small B-cell lymphomas Antigen selection NAIVE -B LYMPHOCYTE MEMORY B-CELL MCL FL LPL MZL CLL Small cell
LINFOMA B (INCLASIFICABLE) CON RASGOS INTERMEDIOS ENTRE LINFOMA DE BURKITT Y LINFOMA B DIFUSO DE CÉLULAS GRANDES.
 CON RASGOS INTERMEDIOS ENTRE LINFOMA DE BURKITT Y LINFOMA B DIFUSO DE CÉLULAS GRANDES.") Congreso Nacional SEAP 2013. LINFOMA B (INCLASIFICABLE) CON RASGOS INTERMEDIOS ENTRE LINFOMA DE BURKITT Y LINFOMA B DIFUSO DE CÉLULAS GRANDES. Santiago Montes Moreno Servicio de Anatomía Patológica, HUMV
Congreso Nacional SEAP 2013. LINFOMA B (INCLASIFICABLE) CON RASGOS INTERMEDIOS ENTRE LINFOMA DE BURKITT Y LINFOMA B DIFUSO DE CÉLULAS GRANDES. Santiago Montes Moreno Servicio de Anatomía Patológica, HUMV
LYMPHOMAS an overview of some subtypes of NHLs
 One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
Understanding your diagnosis. Dr Graham Collins Consultant Haemtologist Oxford University Hospitals
 Understanding your diagnosis Dr Graham Collins Consultant Haemtologist Oxford University Hospitals Common questions I get asked What is lymphoma? What subtype do I have and what does that mean? What are
Understanding your diagnosis Dr Graham Collins Consultant Haemtologist Oxford University Hospitals Common questions I get asked What is lymphoma? What subtype do I have and what does that mean? What are
NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary)
") NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and
NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and
FOLLICULARITY in LYMPHOMA
 FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
Post-ESMO Berne
 Post-ESMO Berne 23.10.2015 Lymphoma Update Panagiotis Samaras Department of Oncology Hemato-Oncology Center University Hospital Zurich Diffuse Large B-Cell Lymphoma (DLBCL) PCNSL Hodgkin s Lymphoma Mantle
Post-ESMO Berne 23.10.2015 Lymphoma Update Panagiotis Samaras Department of Oncology Hemato-Oncology Center University Hospital Zurich Diffuse Large B-Cell Lymphoma (DLBCL) PCNSL Hodgkin s Lymphoma Mantle
Monoclonal B-cell Lymphocytosis
 Entity Centred Approach Lymphoma Classification: WHO and Beyond Clinically meaningful categories Dr Stefan Dojcinov University Hospital of Wales, Cardiff WHO UPDATE - NEW ENTITIES Early lesions lymphoma
Entity Centred Approach Lymphoma Classification: WHO and Beyond Clinically meaningful categories Dr Stefan Dojcinov University Hospital of Wales, Cardiff WHO UPDATE - NEW ENTITIES Early lesions lymphoma
Hodgkin Lymphoma: Outline. HL: Definition. Roberto N. Miranda, M.D. Professor UT MD Anderson Cancer Center. disclose. DISCLOSURES
 Hodgkin Lymphoma: An Update DISCLOSURES I do not have anything to disclose. Roberto N. Miranda, M.D. Professor UT MD Anderson Cancer Center November 3, 2017 Outline Clinical, histopathology, immunophenotype
Hodgkin Lymphoma: An Update DISCLOSURES I do not have anything to disclose. Roberto N. Miranda, M.D. Professor UT MD Anderson Cancer Center November 3, 2017 Outline Clinical, histopathology, immunophenotype
A Practical Guide To Diagnose B-Cell Lymphomas on FNAs. Nancy P. Caraway, M.D.
 A Practical Guide To Diagnose B-Cell Lymphomas on FNAs Nancy P. Caraway, M.D. Major Factors Impacting Dx Lymphomas on Small Bxs Classification systems Immunophenotyping by multiprobe flow cytometry and
A Practical Guide To Diagnose B-Cell Lymphomas on FNAs Nancy P. Caraway, M.D. Major Factors Impacting Dx Lymphomas on Small Bxs Classification systems Immunophenotyping by multiprobe flow cytometry and
Pivotal Genetic Pathways Influencing Treatment in Lymphoma. Philip J. Bierman, M.D. April 24, 2015
 Pivotal Genetic Pathways Influencing Treatment in Lymphoma Philip J. Bierman, M.D. April 24, 2015 Personalized Treatment in Lymphoma What is Personalized Therapy? Customized therapy Individualized therapy
Pivotal Genetic Pathways Influencing Treatment in Lymphoma Philip J. Bierman, M.D. April 24, 2015 Personalized Treatment in Lymphoma What is Personalized Therapy? Customized therapy Individualized therapy
Non-Hodgkin Lymphoma in Clinically Difficult Situations
 Winship Cancer Institute of Emory University Non-Hodgkin Lymphoma in Clinically Difficult Situations James Armitage, MD Professor, Department of Internal Medicine Joe Shapiro Distinguished Chair of Oncology
Winship Cancer Institute of Emory University Non-Hodgkin Lymphoma in Clinically Difficult Situations James Armitage, MD Professor, Department of Internal Medicine Joe Shapiro Distinguished Chair of Oncology
T-cell Lymphomas Biology and Management
 T-cell Lymphomas Biology and Management March-27-2017 Outline Epidemiology Initial Work-up International Prognostic Index Treatment of Diffuse Large B-cell Lymphoma: -Limited Stage -Advanced Stage Frontline:
T-cell Lymphomas Biology and Management March-27-2017 Outline Epidemiology Initial Work-up International Prognostic Index Treatment of Diffuse Large B-cell Lymphoma: -Limited Stage -Advanced Stage Frontline:
Lymphomas in Prof Paul Ruff Division of Medical Oncology
 Lymphomas in 2010 Prof Paul Ruff Division of Medical Oncology Most Common Lymphomas: ~90% B-cell and ~10% T-cell T lymphoblastic: 2% Marginal zone, nodal: 2% Other: 9% Burkitt: 2% Anaplastic large cell:
Lymphomas in 2010 Prof Paul Ruff Division of Medical Oncology Most Common Lymphomas: ~90% B-cell and ~10% T-cell T lymphoblastic: 2% Marginal zone, nodal: 2% Other: 9% Burkitt: 2% Anaplastic large cell:
WHO UPDATE ON LYMPHOMAS. Dr Priya Mary Jacob Asst Professor, Pathology.
 WHO UPDATE ON LYMPHOMAS Dr Priya Mary Jacob Asst Professor, Pathology 3 rd 4 th 4 th revised 2001 2008 2017 The Change The Significance of the Change- Diagnostic, Prognostic The Rationale behind the change.
WHO UPDATE ON LYMPHOMAS Dr Priya Mary Jacob Asst Professor, Pathology 3 rd 4 th 4 th revised 2001 2008 2017 The Change The Significance of the Change- Diagnostic, Prognostic The Rationale behind the change.
Case year old male with abdominal lymphadenopathy Treated with 8 cycles of R-CHOP One year later B-symptoms and progressive disease
 Codirectors Tsieh Sun, M.D., FASCP Francisco Vega, M.D., Ph.D. Department of Hematopathology UT MD Anderson Cancer Center Houston Texas There is no conflict of interest involved in the content and presentation
Codirectors Tsieh Sun, M.D., FASCP Francisco Vega, M.D., Ph.D. Department of Hematopathology UT MD Anderson Cancer Center Houston Texas There is no conflict of interest involved in the content and presentation
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders
 Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Treatment Landscape in R/R DLBCL Novel Targets and Strategies. Wyndham H. Wilson, M.D., Ph.D. Senior Investigator
 Treatment Landscape in R/R DLBCL Novel Targets and Strategies Wyndham H. Wilson, M.D., Ph.D. Senior Investigator Gene-expression profiling of DLBCL subtypes Roschewski, M. et al. (2013) Nat. Rev. Clin.
Treatment Landscape in R/R DLBCL Novel Targets and Strategies Wyndham H. Wilson, M.D., Ph.D. Senior Investigator Gene-expression profiling of DLBCL subtypes Roschewski, M. et al. (2013) Nat. Rev. Clin.
WHO 2016 update lymphoid neoplasms. Dr Sue Morgan Alfred Hospital, Melbourne
 WHO 2016 update lymphoid neoplasms Dr Sue Morgan Alfred Hospital, Melbourne WHO 4 th edition 2008 Established guideline worldwide for diagnosis of haematological malignancy for the last 9 years Significant
WHO 2016 update lymphoid neoplasms Dr Sue Morgan Alfred Hospital, Melbourne WHO 4 th edition 2008 Established guideline worldwide for diagnosis of haematological malignancy for the last 9 years Significant
Radiotherapy in aggressive lymphomas. Umberto Ricardi
 Radiotherapy in aggressive lymphomas Umberto Ricardi Is there (still) a role for Radiation Therapy in DLCL? NHL: A Heterogeneous Disease ALCL PMLBCL (2%) Burkitt s MCL (6%) Other DLBCL (31%) - 75% of aggressive
Radiotherapy in aggressive lymphomas Umberto Ricardi Is there (still) a role for Radiation Therapy in DLCL? NHL: A Heterogeneous Disease ALCL PMLBCL (2%) Burkitt s MCL (6%) Other DLBCL (31%) - 75% of aggressive
Policy for Central Nervous System [CNS] Prophylaxis in Lymphoid Malignancies
![Policy for Central Nervous System [CNS] Prophylaxis in Lymphoid Malignancies](/thumbs/90/104309591.jpg "Policy for Central Nervous System [CNS] Prophylaxis in Lymphoid Malignancies") Policy for Central Nervous System [CNS] Prophylaxis in Lymphoid Malignancies UNCONTROLLED WHEN PRINTED Note: NOSCAN Haematology MCN has approved the information contained within this document to guide
Policy for Central Nervous System [CNS] Prophylaxis in Lymphoid Malignancies UNCONTROLLED WHEN PRINTED Note: NOSCAN Haematology MCN has approved the information contained within this document to guide
Commentary on the WHO Classification of Tumors of Lymphoid Tissues (2008): Aggressive B-cell Lymphomas
: Aggressive B-cell Lymphomas") Commentary on the WHO Classification of Tumors of Lymphoid Tissues (2008): Aggressive B-cell Lymphomas The Harvard community has made this article openly available. Please share how this access benefits
Commentary on the WHO Classification of Tumors of Lymphoid Tissues (2008): Aggressive B-cell Lymphomas The Harvard community has made this article openly available. Please share how this access benefits
Rituximab and Combination Chemotherapy in Treating Patients With Non- Hodgkin's Lymphoma
 Page 1 of 5 Home Search Study Topics Glossary Search Full Text View Tabular View No Study Results Posted Related Studies Rituximab and Combination Chemotherapy in Treating Patients With Non- Hodgkin's
Page 1 of 5 Home Search Study Topics Glossary Search Full Text View Tabular View No Study Results Posted Related Studies Rituximab and Combination Chemotherapy in Treating Patients With Non- Hodgkin's
T cell lymphoma diagnostics and differential diagnosis to Hodgkin lymphoma
 T cell lymphoma diagnostics and differential diagnosis to Hodgkin lymphoma Sylvia Hartmann Dr. Senckenberg Institute of Pathology Goethe University Frankfurt Overview Borderline ALCL classical HL Borderline
T cell lymphoma diagnostics and differential diagnosis to Hodgkin lymphoma Sylvia Hartmann Dr. Senckenberg Institute of Pathology Goethe University Frankfurt Overview Borderline ALCL classical HL Borderline
Nodular lymphocyte predominant Hodgkin lymphoma. Lymphoma Tumor Board. January 5, 2018
 Nodular lymphocyte predominant Hodgkin lymphoma Lymphoma Tumor Board January 5, 2018 Etiology Subtypes of Classical Hodgkin Lymphoma (chl)* Nodular sclerosing HL Most common subtype Composed of large tumor
Nodular lymphocyte predominant Hodgkin lymphoma Lymphoma Tumor Board January 5, 2018 Etiology Subtypes of Classical Hodgkin Lymphoma (chl)* Nodular sclerosing HL Most common subtype Composed of large tumor
Burkitt lymphoma. Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8
 Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology