Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies
|
|
|
- Nathaniel Lewis
- 5 years ago
- Views:
Transcription
1 Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018
2 Objectives To understand how the trend toward less invasive lymph node biopsies impacts the practice of hematopathology To learn how to triage small specimens to maximize diagnostic utility To understand the application of ancillary tests to lymph node core biopsies To raise awareness of common pitfalls in diagnosing lymphoma on core biopsies 2


3 Core Needle Lymph Node Biopsy 3
4 Evolution of the core needle biopsy University of Michigan Experience Increase FNA % CNB % Excision 140 (40% of total LN Bx) 170 (20% of total LN Bx) Current state Dramatic increase in FNA and core needle biopsies for suspected lymphoma 4
5 Why? Ultrasound guided approaches for LN located in deep, inaccessible sites Better ancillary techniques Improved diagnostic criteria Better yield of diagnosis Increased opportunity for disease monitoring 5
6 The Problem Is The WHO classification system based on histologic findings from excisional biopsies. 6
7 Core needle biopsies (CNB)in lymphoma diagnosis Multi-institutional study Determine the diagnostic approach most likely to yield a definitive and accurate diagnosis Total 532 patients with CNB of LN evaluated Czader M et al., USCAP abstract
8 Core needle biopsies (CNB)in lymphoma diagnosis Multi-institutional study RESULTS 23% no definitive diagnosis 83% specific WHO diagnosis made; longer CNB and larger needle gauge IHC performed on 72% FCM performed on 69% FNA yielded better material for FCM than tissue cores Czader M et al., USCAP abstract
9 Core needle biopsies (CNB)in lymphoma diagnosis Multi-institutional study RESULTS 128 CNB diagnosis was confirmed in 40% of LN excision biopsies 50% cases showed minor changes in diagnosis 9% cases showed major changes in diagnosis 77% of diagnosed as lymphoma were treated based on CNB diagnosis Czader M et al., USCAP abstract
10 Core needle biopsies (CNB)in lymphoma diagnosis Multi-institutional study Conclusions Definitive WHO diagnosis is rendered in the majority of CNB cases Significant number are treated based on CNB diagnosis 23% of CNB cases are non-diagnostic 10% with significant diagnostic discrepancies on LNEx Aggregate core lengths improves diagnostic accuracy Czader M et al., USCAP abstract

11 Core needle biopsies are here to stay! 11
12 Pearls and pitfalls in the diagnostic workup of small lymph node biopsies I. Nodular lymphoid proliferations II. Assessment of transformation in CNB III. Polymorphous lymphoid proliferations IV. Lymphoid proliferations with Reed- Sternberg-like cells V. Lymphoid infiltrates with extensive sclerosis VI. Diffuse large cell proliferations 12
13 Pearls and pitfalls in the diagnostic workup of small lymph node biopsies I. Nodular lymphoid proliferations II. Assessment of transformation in CNB III. Polymorphous lymphoid proliferations IV. Lymphoid proliferations with Reed- Sternberg-like cells V. Lymphoid infiltrates with extensive sclerosis VI. Diffuse large cell proliferations 13

14 Nodular lymphoid proliferations Reactive Follicular hyperplasia PTGC Castleman disease B-cell Non-Hodgkin lymphoma Follicular lymphoma Chronic lymphocytic leukemia/ small lymphocytic lymphoma Mantle cell lymphoma Marginal zone lymphoma Mantle cell lymphoma Neoplastic Hodgkin lymphoma NLP Hodgkin lymphoma Classical Hodgkin lymphoma T-cell Follicular T-cell lymphoma Nodal PTL with TFH phenotype Angioimmunoblastic T cell lymphoma 14


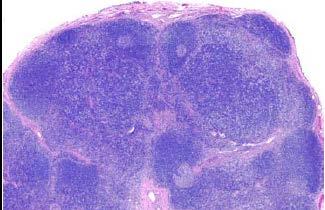
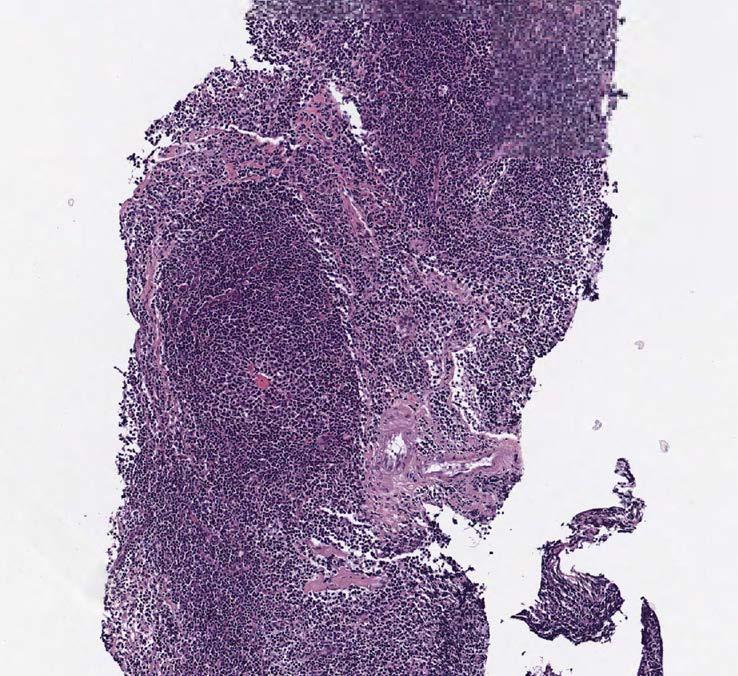
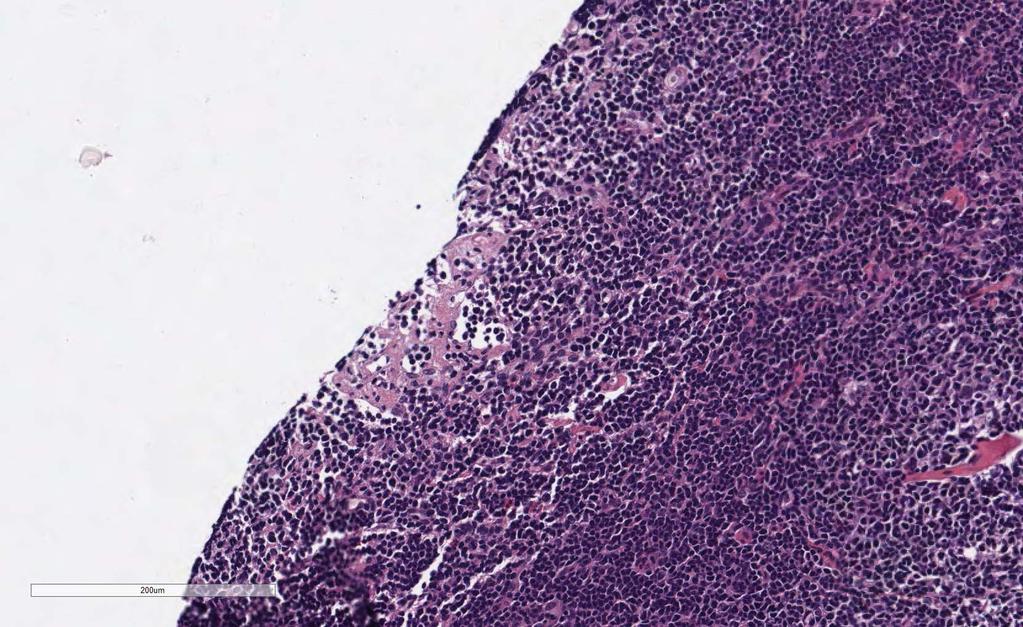
15 CNB: left neck mass of 55 year old man 15

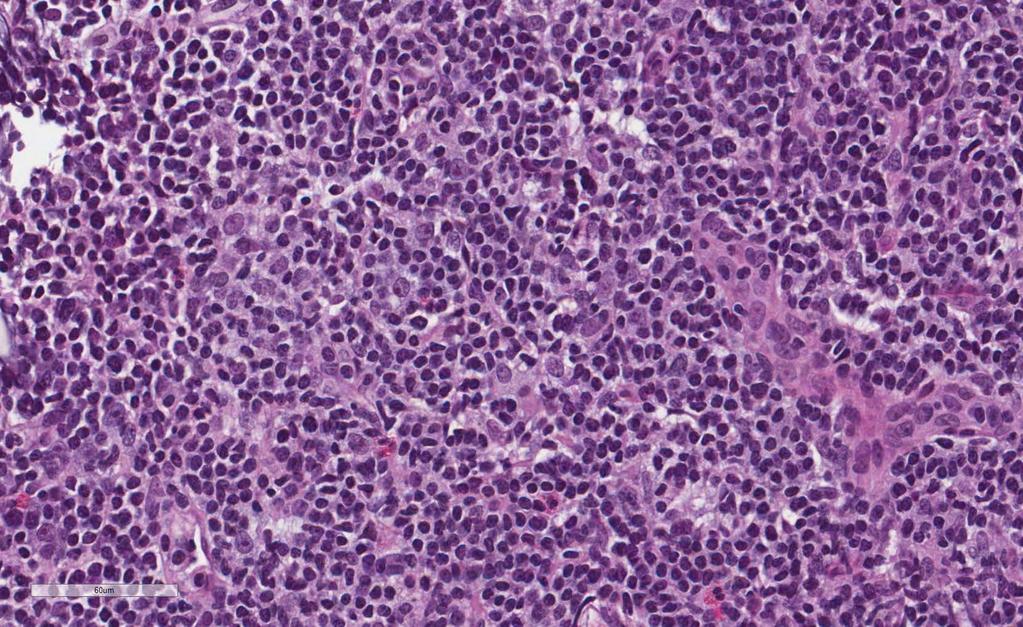
16 Cytologic features 16
17 Differential Diagnoses Reactive Small B cell lymphomas T cell lymphoma of small T cells Precursor lymphoid neoplasms 17


18 Proliferation centers in CLL/SLL 18
19 Immunophenotyping All suspected lymphoma samples should have basic immunohistochemistry and / or FCM Flow cytometry if there is viable tissue IHC if there is sufficient tissue even if necrotic 19
20 What will FCM tell us? Exclude lymphoblastic lymphoma/leukemia Determine if there is a clonal B cell population Determine the presence of CD5, CD10 + B cells or clonal plasma cells Ten-color flow cytometry can distinguish many subtypes of B-cell lymphoma Determine the presence of T cell antigen aberrancies 20
21 FCM is not very good at identifying: The presence of NLPHL or CHL Identifying and characterizing large B-cell neoplasms The presence of a clonal T cell population 21
22 Association between length of tissue core and cell number for FCM and diagnostic concordance Chi, P et al., Cytometry Part B
23 Concordance between morphology and flow cytometry Chi, P et al., Cytometry Part B

24 Back to our case 24

25 CD10 BCL6 25
26 CD5 26

27 Cyclin D1 Cyclin D1 27
28 Diagnosis Mantle cell lymphoma Other CD5+ B-cell lymphomas CLL/SLL (beware of BTKi that downregulate CD5,CD43) De novo CD5+ DLBCL Marginal zone lymphoma (rare) 28
29 Can we assess transformation in small biopsies? can be helpful in evaluating suspected transformation to higher grade disease but should not be definitive 29

30 CNB of inguinal node of 69 year old man with history of FCL 30
31 31
32 32
33 33

34 CD20 highlights nodules and diffuse areas 34

35 CD3 highlights nodules and diffuse areas 35

36 BCL-6 highlights nodules and diffuse areas 36

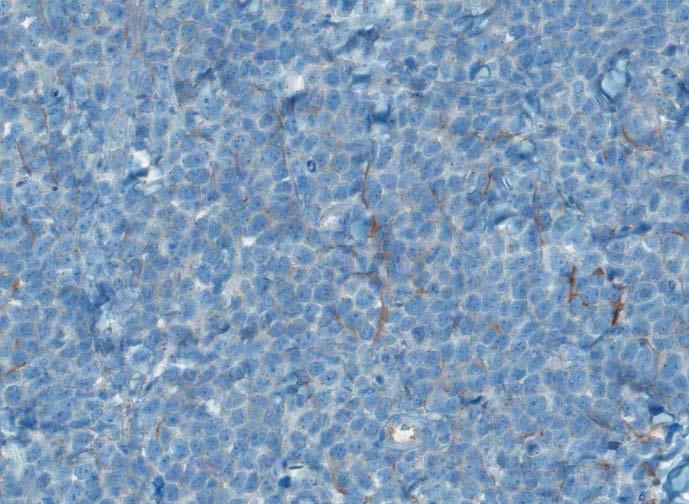
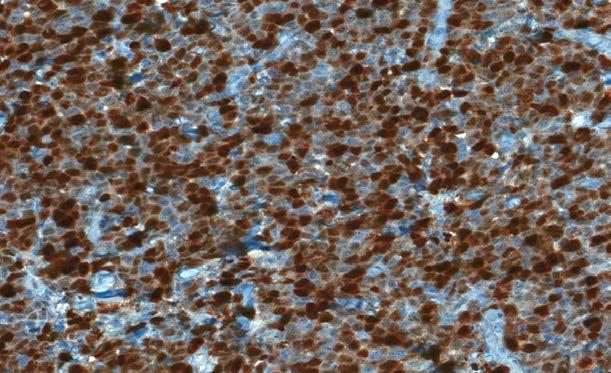
37 Ki67 demonstrates 2 different populations Ki % Ki % 37
38 Diagnosis B-cell lymphoma of germinal center origin Definitive subclassification cannot be made Raise concern for: FCL and possible DLBCL FCL grade 3 Low grade FCL with high proliferation index 38

39 Be aware of FCL with high proliferation index 39



40 FCL with high proliferation index CD20 CD3 Ki67 Flow cytometry: CD10+, CD19+, CD20+, FMC7+, lambda+, CD5-, CD23-40
41 Pearls and pitfalls in the diagnostic workup of small lymph node biopsies I. Nodular lymphoid proliferations II. Assessment of transformation in CNB III. Polymorphous lymphoid proliferations IV. Lymphoid proliferations with Reed- Sternberg-like cells V. Lymphoid infiltrates with extensive sclerosis VI. Diffuse large cell proliferations 41

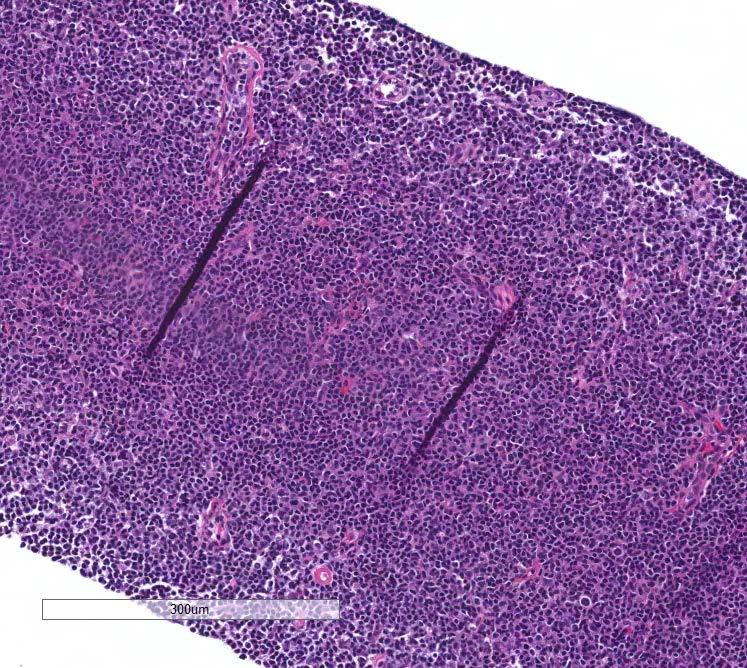
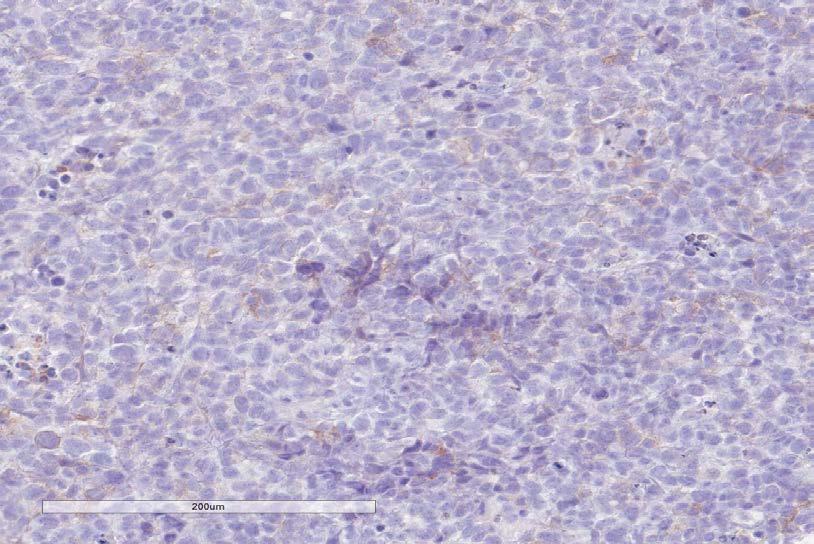
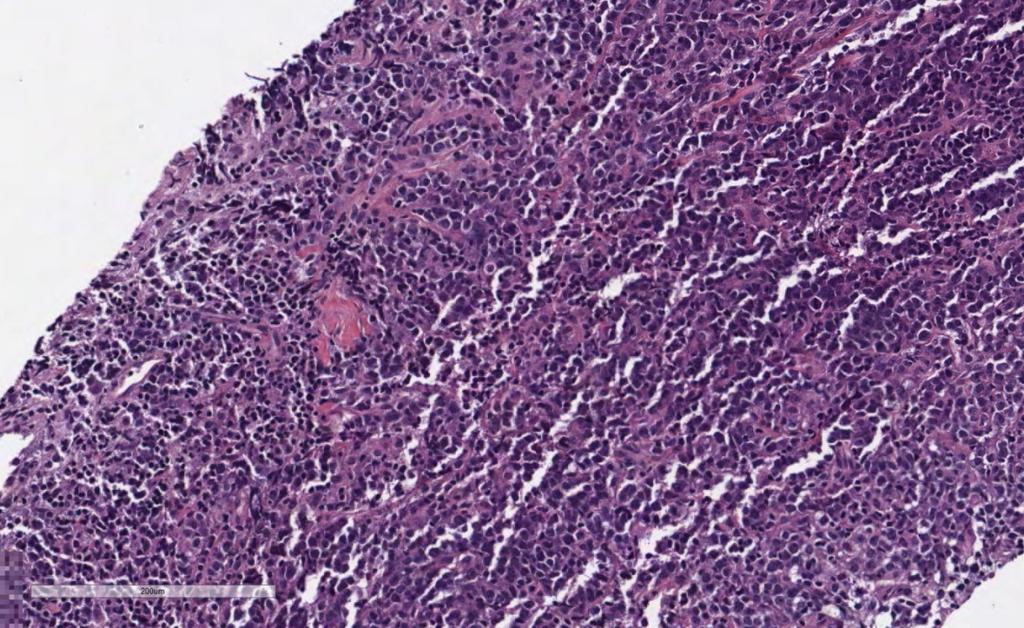
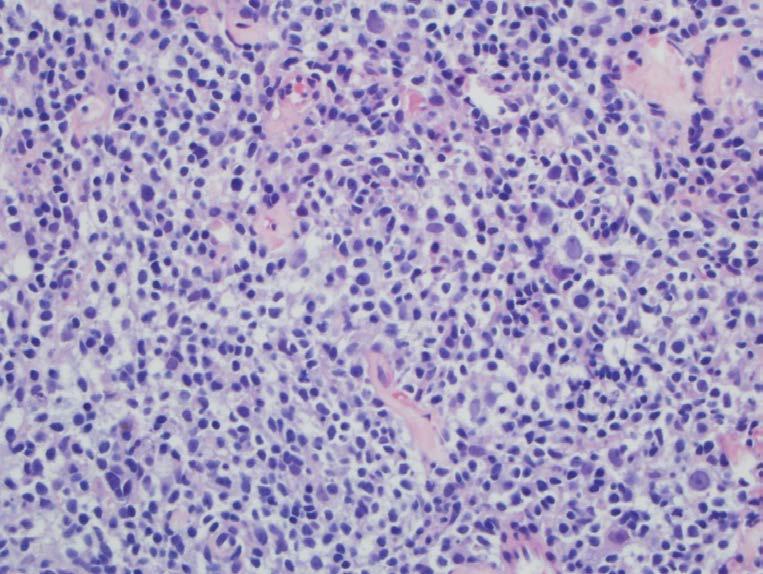
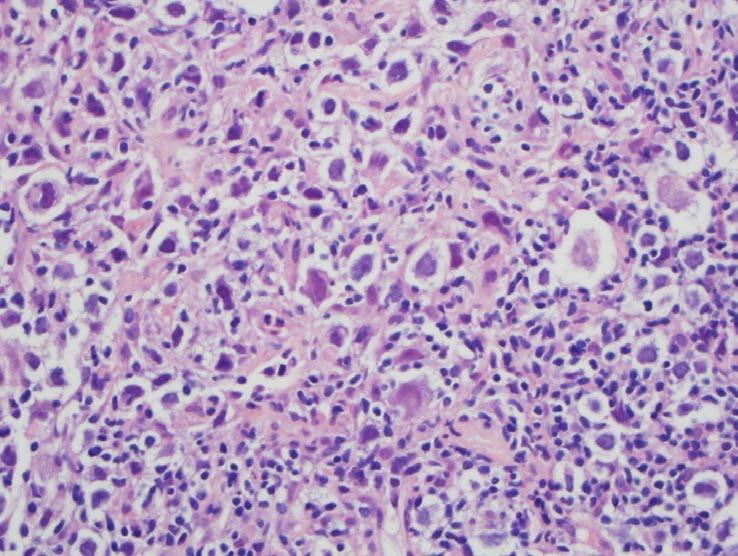
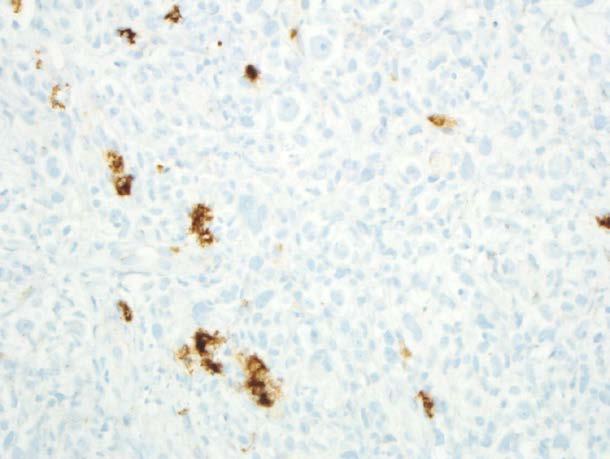
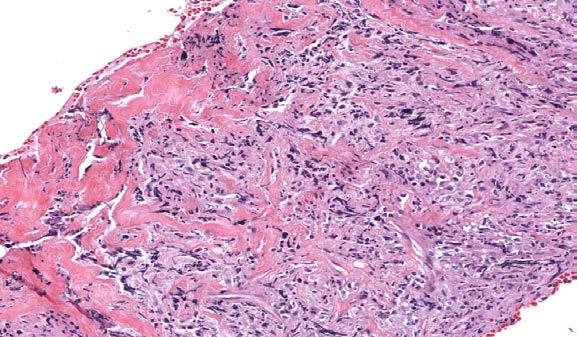
42 60 year old woman with nasopharyngeal No previous medical history presented to the primary care physician lesion Diffuse, destructive submucosal infiltrate Significant necrosis of the superficial mucosa 42

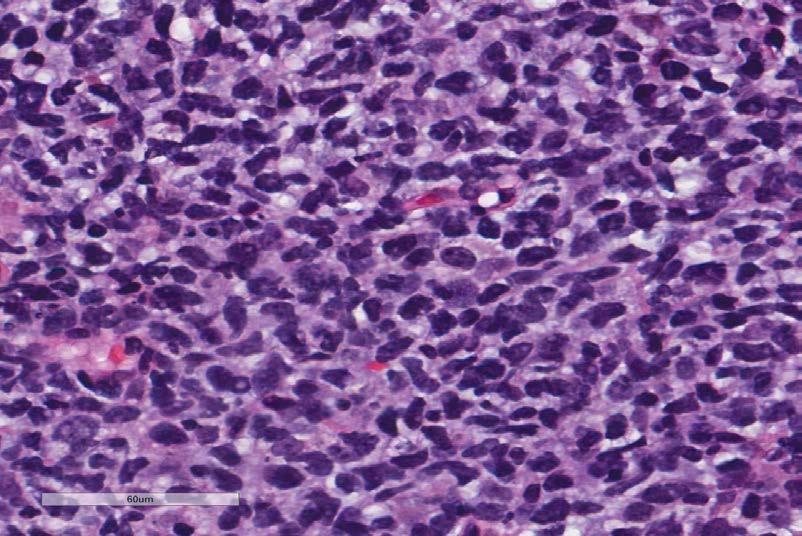
43 Histologic features Large pleomorphic cells with variably prominent nucleoli Numerous mitotic figures and numerous apoptoses with occasional Reed- Sternberg-like cells 43

44 occasional Reed-Sternberg-like cells 44
45 Polymorphous lymphoid proliferations Reactive Paracortical hyperplasia Infectious mononucleosis Wegener s Granulomatous lymphadenitis Neoplastic Hodgkin lymphoma NLP Hodgkin lymphoma Classical Hodgkin lymphoma Non-Hodgkin lymphoma B-cell T cell rich histiocyte rich B cell lymphoma EBV+ polymorphic lymphoma FCL with RS-like cells Composite lymphomas T-cell Peripheral T cell lymphoma,nos Anaplastic large cell lymphoma NK/T cell lymphoma Angioimmunoblastic T cell lymphoma
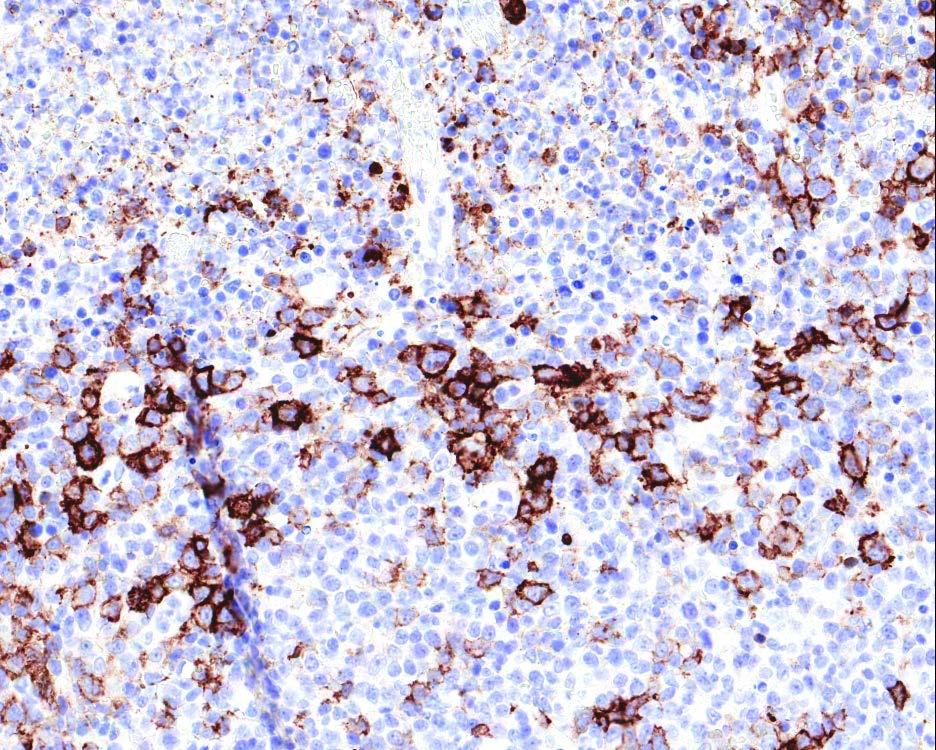
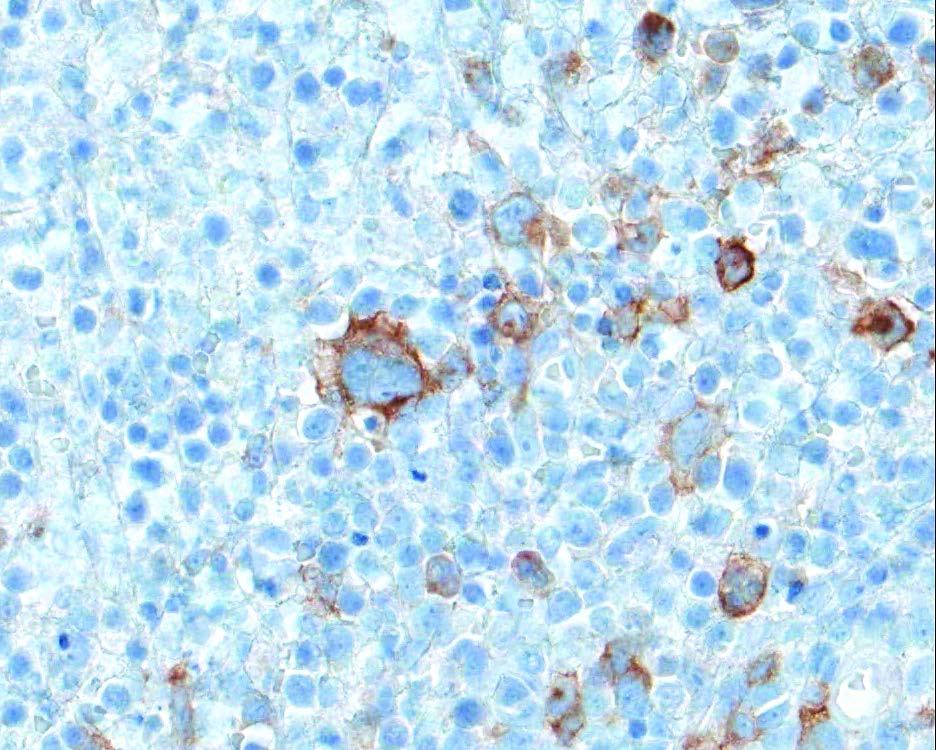
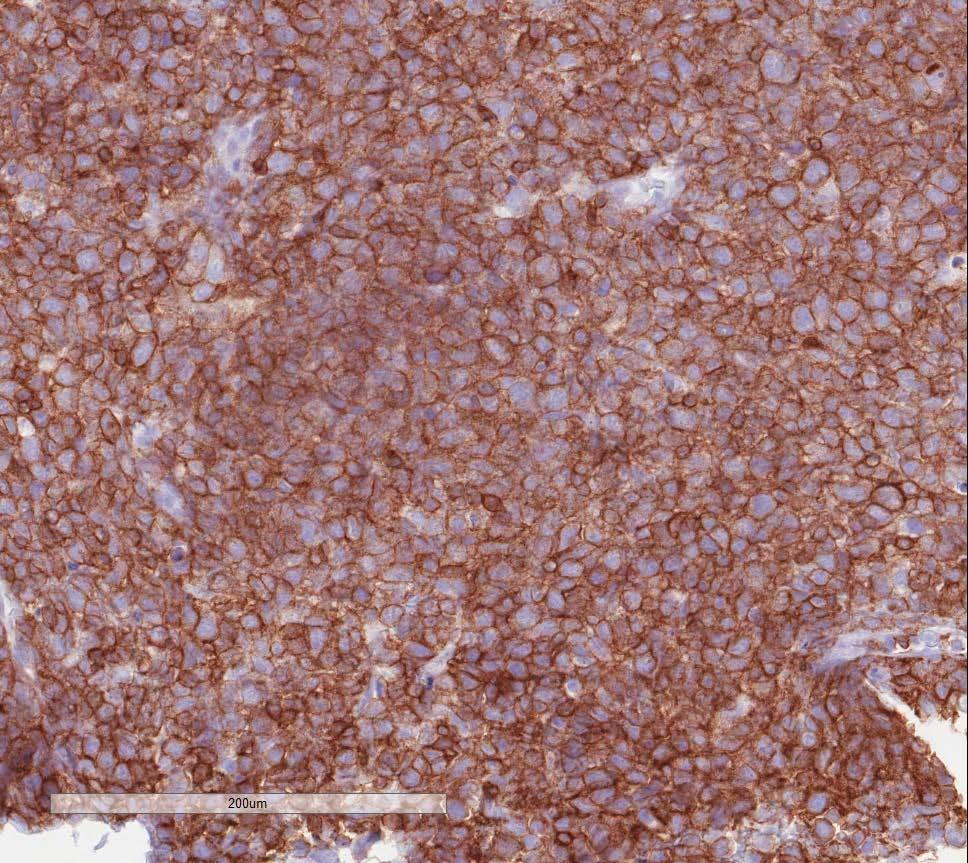
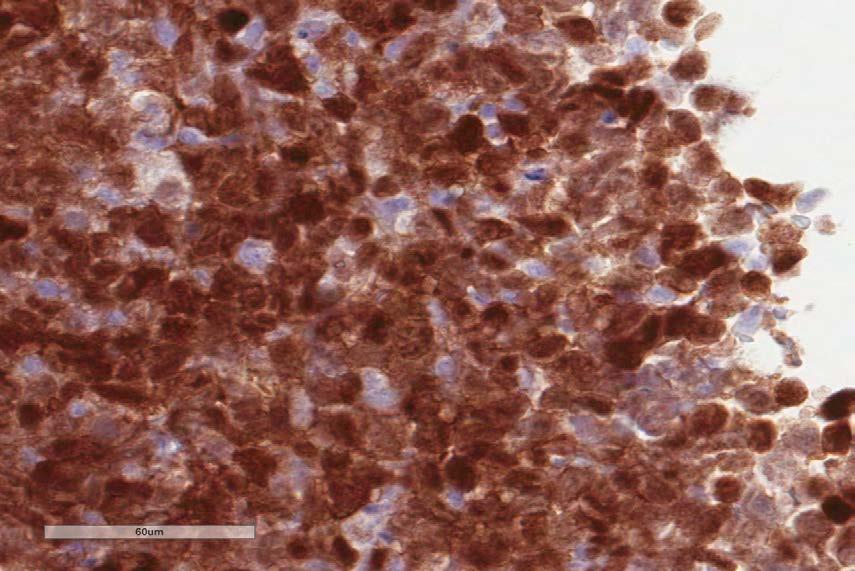
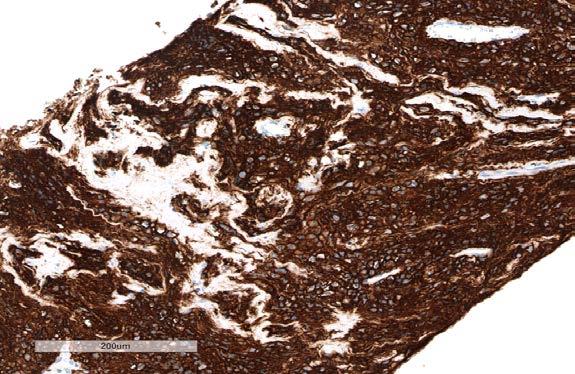
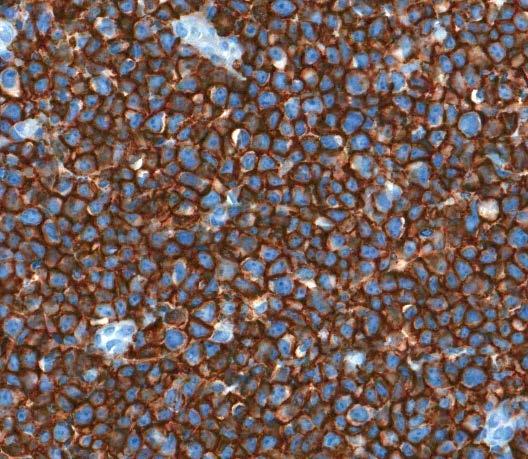
46 CD20 Immunohistochemical studies CD30 46
47 Immunohistochemical studies Antibody Results Antibody Results CD15 Negative CD20 Var Positive EMA Negative CD19 Positive, weak CD10 Negative CD138 Positive, weak T cell antigens CD56 TIA1 Negative Negative Negative PAX5 CD45 CD30 Var Positive Var Positive Large cells HHV8 Negative 47

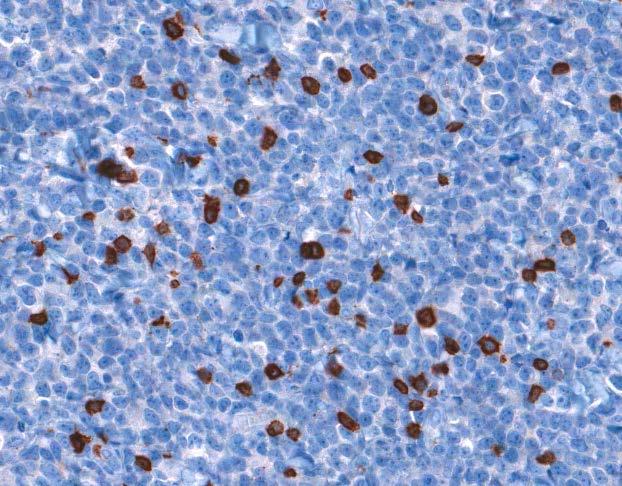
48 EBER-1 Diagnosis EBV-positive diffuse large B-cell lymphoma 48
49 Other EBV+ Large Cell Lymphoma Plasmablastic lymphoma Primary effusion lymphoma Lymphomatoid granulomatosis Pyothorax associated lymphoma T/NK cell lymphoma AITL Classical Hodgkin lymphoma 49
50 Pearls and pitfalls in the diagnostic workup of small lymph node biopsies I. Nodular lymphoid proliferations II. Assessment of transformation in CNB III. Polymorphous lymphoid proliferations IV. Lymphoid proliferations with Reed-Sternberg-like cells V. Lymphoid infiltrates with extensive sclerosis VI. Diffuse large cell proliferations 50

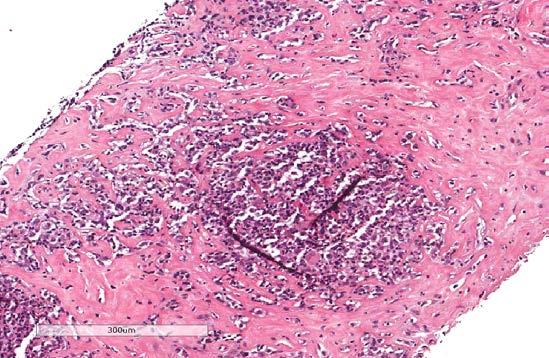
51 71-year-old woman with retroperitoneal mass 51
52 52
53 Differential Diagnosis Reactive Retroperitoneal fibrosis Chronic inflammation Neoplastic Classical Hodgkin lymphoma B-cell non-hodgkin lymphoma Peripheral T-cell lymphoma 53


54 CD20 CD3 54

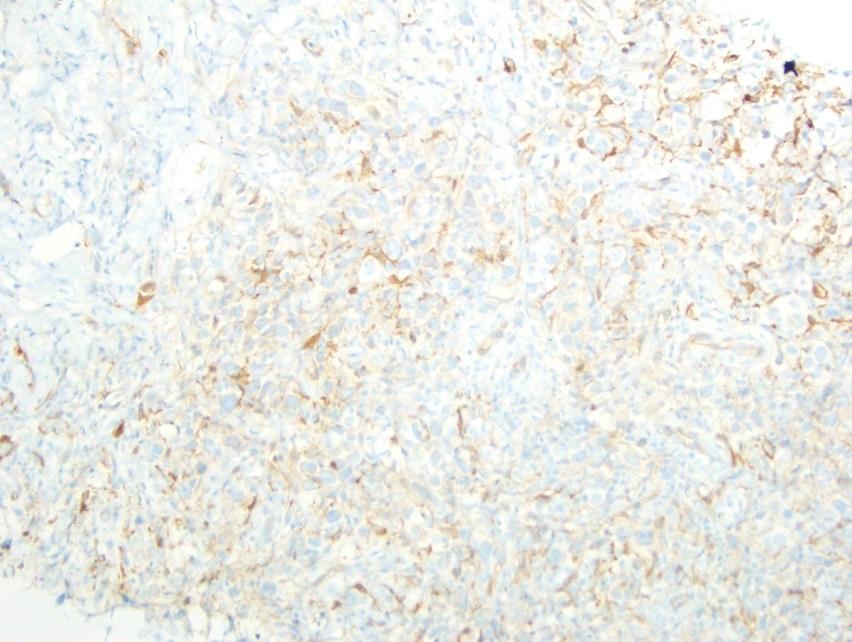
55 CD30 CD15 FASCIN 55

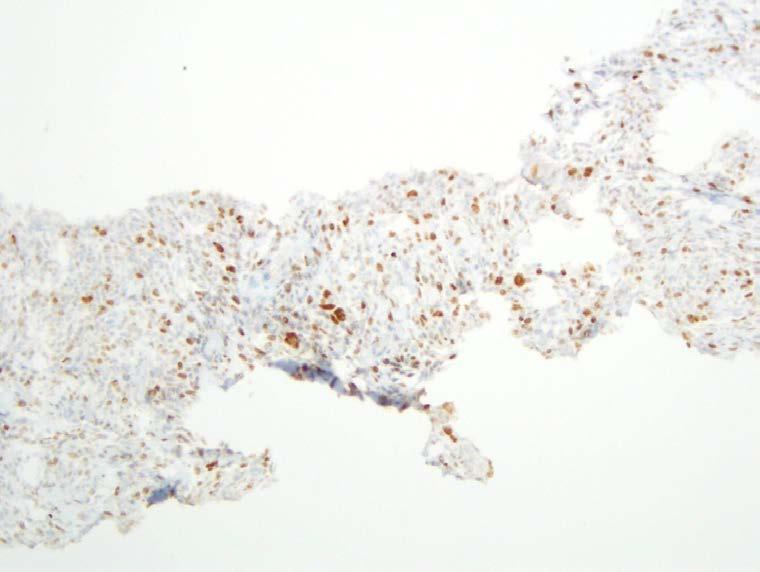
56 LCA BCL6 56
57 Immunophenotype Immunostain Result CD20 + small and large cells CD30 + large cells CD15 - Fascin - BCL6 + small and large cells CD10 - LCA + small and large cells PAX-5 + small and large cells 57
58 Differential Diagnosis Reactive Peripheral T-cell lymphoma B-cell non-hodgkin lymphoma Classical Hodgkin lymphoma Composite lymphoma 58
59 Immunophenotype CHL B-cell NHL Morphology of large cells Sheets of small B-cells Sclerosis BCL6 + CD30 + LCA + 59
60 Reed-Sternberg cells--chl? No inflammatory background CD20 should not be stronger than CD30 on R-S cells in CHL R-S cells are negative for LCA & BCL6 Fascin should be positive on R-S cells Good evidence against CHL if negative Can be positive on other lymphomas (DLBCL) 60
61 Additional information about this case Small paratrabecular lymphoid aggregate in core biopsy Monoclonal CD10 positive B-cell population by FCM 61
62 Diagnosis Follicular lymphoma (grade 1-2) Focal transformation? R-S cells counted as centroblasts (area of grade 3 or DLBCL?) Very small area with >15 R-S cells/hpf 62
63 Features supporting FCL Sclerosis FCL in retroperitoneum OFTEN sclerotic Immunophenotype BCL6 + CD10 + in marrow 63
64 NHL with R-S-like cells Low grade B-NHL Follicular lymphoma CLL with HRS cells Marginal zone lymphoma Mantle cell lymphoma DLBCL Primary mediastinal B-cell lymphoma T-cell rich histiocyterich B-cell lymphoma 64
65 T-NHL with R-S-like cells Anaplastic large cell lymphoma Angioimmunoblastic T-cell lymphoma Peripheral T-cell lymphoma, NOS CD30+ CD15+ 65
66 Other CD30+ Large Cell Lymphoma Diffuse large B-cell lymphoma, anaplastic variant Classical Hodgkin lymphoma (MC, LD) Plasmablastic lymphoma Primary effusion lymphoma Pyothorax associated lymphoma NK/T cell lymphoma 66
67 Pearls and pitfalls in the diagnostic workup of small lymph node biopsies I. Nodular lymphoid proliferations II. Assessment of transformation in CNB III. Polymorphous lymphoid proliferations IV. Lymphoid proliferations with Reed- Sternberg-like cells V. Lymphoid infiltrates with extensive sclerosis VI. Diffuse large cell proliferations 67


68 FCL with extensive sclerosis 68


69 Diffuse large B-cell lymphoma with sclerosis are germinal center derived CD20 FCM: CD10 positive lamda restricted B cells without CD5, CD23 and CD38. 69

70 Primary mediastinal B-cell lymphoma CD20 70


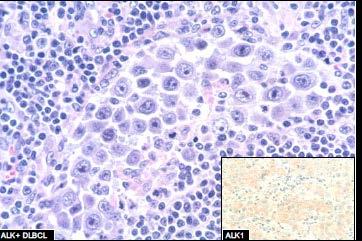
71 ALK+ anaplastic large cell lymphoma presenting with retroperitoneal fibrosis ALK1 71
72 Pearls and pitfalls in the diagnostic workup of small lymph node biopsies I. Nodular lymphoid proliferations II. Assessment of transformation in CNB III. Polymorphous lymphoid proliferations IV. Lymphoid proliferations with Reed- Sternberg-like cells V. Lymphoid infiltrates with extensive sclerosis VI. Diffuse large cell proliferations 72


73 45 year old man with lesion in oral pharynx 73
74 Differential Diagnoses Reactive Infectious Viral Neoplastic Hematopoietic Non-Hodgkin lymphoma diffuse large B-cell lymphomas with anaplastic features, Anaplastic large cell lymphoma (ALK-positive and ALK-negative) Extramedullary myeloid tumor Hodgkin lymphoma Anaplastic myeloma Non-hematopoietic Melanoma Carcinoma (anaplastic variants) Inflammatory myofibroblastic tumor 74
75 Diffuse large B-cell lymphoma CD20 CD3 75
76 Subclassification of DLBCL is possible on small lymph node biopsies DLBCL GC type DLBCL Non-GC type Prognostic information Therapeutic implications 76
77 DLBCL, non-germinal center type CD20 CD3 CD10 MUM1 77


78 Synctitial variant of classical Hodgkin lymphoma CD30 78
79 Differential Diagnoses Diffuse large cell infiltrate DLBCL Double hit lymphoma B-cell lymphoma intermediate Blastoid mantle cell lymphoma Marginal zone lymphoma Anaplastic large cell lymphoma Histiocytic proliferations (Sinus histiocytosis, LCH, histiocytic sarcoma) Flow cytometry has low sensitivity in the diagnosis of Diffuse large B cell lymphoma 79
80 Take home points 80

81 Lymphoma work-up for small biopsies FNA: can be helpful and also submitted for FCM Tiny cores only: submit entire specimen for permanent sections Larger or multiple cores or fragments: attempt complete lymphoma work up, priority is permanent sections for histology 81
82 CNB in lymphoma diagnosis Definitive WHO diagnosis is rendered in the majority of CNB cases Significant number are treated based on CNB diagnosis 23% of CNB cases are non-diagnostic 10% with significant diagnostic discrepancies on LNEx Aggregate core lengths improves diagnostic accuracy Czader M et al., USCAP abstract
83 Core biopsy is useful Inaccessible tumours such as those in the retroperitoneum Do allow a minimal assessment of architecture and immunophenotyping Allows definitive diagnosis and subclassification if IHC/FCM is incorporated appropriately Remember the utility and caveats about antibodies against tumor-specific proteins (ALK, IDH1, and BRAF VE1) 83
84 Core Biopsy Is Not useful Where much of the lymphoid infiltrate is reactive T-cell rich B-cell lymphoma MALT Angioimmunoblastic-type peripheral T-cell lymphoma Classical Hodgkin lymphoma Nodular lymphocyte predominant Hodgkin lymphoma Tumors where the architecture is important Low grade non-hodgkin lymphoma Nodular lymphocyte predominant Hodgkin lymphoma 84
85 When to ask for more tissue? Inadequate tissue: tiny, crushed, necrotic Flow is negative but there are lots of B cells or T cells by IHC Flow is negative but there is a polymorphous infiltrate DDX of CHL vs PTCL FCL with high proliferation index 85
86 Role of Cytogenetic and Molecular Genetic Analysis of SLN Biopsies FISH can be performed on touch preps Cytogenetic evidence is essential for the diagnosis of Burkitt lymphoma FISH should be used as adjuncts to diagnosis and not requested as a routine investigation on all samples PCR results should not form the sole basis for a diagnosis 86
87 Be cautious in interpretation of molecular data: unexpected findings Clonal populations or chromosomal translocations can be observed in non-neoplastic conditions Low level disease or pre-neoplastic conditions Multiple clonal populations can be present in one lesion Double hits in morphologically low grade B-cell lymphomas 87


88 Histopathology Thin sections, 4 um More Testing with Less Tissue Cell suspension Aspirate Cell Block Aspirate Smear Diff-Quik Stained Morphologic analysis Immunohistochemistry Fluorescent in situ hybridization Core needle biopsy Imprints for Wright stain Immunocytochemistry Fluorescent in situ hybridization 10-color flow cytometry Cytogenetics Cytogenomics NGS



89 Thank you for your attention! 89
Contents. vii. Preface... Acknowledgments... v xiii
 Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
Approach to Core Biopsy Specimens
 BDIAP 108th Symposium on Haematopathology Joint Meeting of the BDIAP and BLPG at-bristol, Anchor Road, Harbourside, Bristol BS1 5DB 15th - 17th May 2014 Approach to Core Biopsy Specimens Dr Stefan Dojcinov
BDIAP 108th Symposium on Haematopathology Joint Meeting of the BDIAP and BLPG at-bristol, Anchor Road, Harbourside, Bristol BS1 5DB 15th - 17th May 2014 Approach to Core Biopsy Specimens Dr Stefan Dojcinov
Immunopathology of Lymphoma
 Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Hepatic Lymphoma Diagnosis An Algorithmic Approach
 Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
A Practical Guide To Diagnose B-Cell Lymphomas on FNAs. Nancy P. Caraway, M.D.
 A Practical Guide To Diagnose B-Cell Lymphomas on FNAs Nancy P. Caraway, M.D. Major Factors Impacting Dx Lymphomas on Small Bxs Classification systems Immunophenotyping by multiprobe flow cytometry and
A Practical Guide To Diagnose B-Cell Lymphomas on FNAs Nancy P. Caraway, M.D. Major Factors Impacting Dx Lymphomas on Small Bxs Classification systems Immunophenotyping by multiprobe flow cytometry and
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO
 HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO HODGKIN LYMPHOMA CLASSIFICATION Lukes & Butler Rye WHO-2016 Linphocytic and/or histiocytic Nodular & diffuse Nodular Sclerosis Lymphocyte
HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO HODGKIN LYMPHOMA CLASSIFICATION Lukes & Butler Rye WHO-2016 Linphocytic and/or histiocytic Nodular & diffuse Nodular Sclerosis Lymphocyte
DETERMINATION OF A LYMPHOID PROCESS
 Chapter 2 Applications of Touch Preparation Cytology to Intraoperative Consultations: Lymph Nodes and Extranodal Tissues for Evaluation of Hematolymphoid Disorders INTRODUCTION As discussed in Chap. 1,
Chapter 2 Applications of Touch Preparation Cytology to Intraoperative Consultations: Lymph Nodes and Extranodal Tissues for Evaluation of Hematolymphoid Disorders INTRODUCTION As discussed in Chap. 1,
Mimics of Lymphoma in Routine Biopsies. I have nothing to disclose regarding the information to be reported in this talk.
 Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco I have nothing to disclose regarding the information to be reported in this
Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco I have nothing to disclose regarding the information to be reported in this
Methods used to diagnose lymphomas
 Institut für Pathologie Institut für Pathologie Methods used to diagnose lymphomas Prof. Dr.Med. Leticia Quintanilla-Fend Molecular techniques NGS histology Cytology AS-PCR Sanger seq. MYC Immunohistochemistry
Institut für Pathologie Institut für Pathologie Methods used to diagnose lymphomas Prof. Dr.Med. Leticia Quintanilla-Fend Molecular techniques NGS histology Cytology AS-PCR Sanger seq. MYC Immunohistochemistry
Mimics of Lymphoma in Routine Biopsies. Mixed follicular and paracortical hyperplasia. Types of Lymphoid Hyperplasia
 Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco Types of Lymphoid Hyperplasia Follicular hyperplasia (B-cells) Paracortical
Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco Types of Lymphoid Hyperplasia Follicular hyperplasia (B-cells) Paracortical
Incidence. Bimodal age incidence 15-40, >55 years Childhood form (0-14) more common in developing countries M:F=1.5:1; in all subtypes except NS
 more common in developing countries M:F=1.5:1; in all subtypes except NS") Hodgkin Lymphoma Hodgkin Lymphoma 30% of all lymphomas Absolute incidence unchanged Arise in lymph node, cervical region Neoplastic tissues usually contain a small number of tumor cells Incidence Bimodal
Hodgkin Lymphoma Hodgkin Lymphoma 30% of all lymphomas Absolute incidence unchanged Arise in lymph node, cervical region Neoplastic tissues usually contain a small number of tumor cells Incidence Bimodal
Many of the hematolymphoid disorders are derived
 REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
Lymph node cytopathology : A practical approach to lymphoproliferative disorders
 Lymph node cytopathology : A practical approach to lymphoproliferative disorders Koray Ceyhan, M.D Department of Pathology Faculty of Medicine Ankara University Ankara, Turkey Diagnostic use of FNA in
Lymph node cytopathology : A practical approach to lymphoproliferative disorders Koray Ceyhan, M.D Department of Pathology Faculty of Medicine Ankara University Ankara, Turkey Diagnostic use of FNA in
Aggressive B-Cell Lymphomas
 Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Small B-cell (Histologically Low Grade) Lymphoma
 Lymphoma") Frequency of Lymphoid Neoplasms Small B-cell (Histologically Low Grade) Lymphoma Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital B-cell neoplasms 88% Diffuse large B-cell lymphoma
Frequency of Lymphoid Neoplasms Small B-cell (Histologically Low Grade) Lymphoma Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital B-cell neoplasms 88% Diffuse large B-cell lymphoma
Aggressive B-cell Lymphomas
 Neoplastic Hematopathology Update 2018 Aggressive B-cell Lymphomas Raju K. Pillai City of Hope National Medical Center I do not have any disclosures Disclosures Outline New entities and changes in WHO
Neoplastic Hematopathology Update 2018 Aggressive B-cell Lymphomas Raju K. Pillai City of Hope National Medical Center I do not have any disclosures Disclosures Outline New entities and changes in WHO
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
11/8/2018 DISCLOSURES. I have NO Conflicts of Interest to Disclose. UTILTY OF DETECTING PATTERNS
 Bharat N. Nathwani, M.D. City of Hope Medical Center Professor, Director of Pathology Consultation Services, 1500 East Duarte Road, Duarte, California, 91010 DISCLOSURES -------------------------------------------------------
Bharat N. Nathwani, M.D. City of Hope Medical Center Professor, Director of Pathology Consultation Services, 1500 East Duarte Road, Duarte, California, 91010 DISCLOSURES -------------------------------------------------------
HEMATOPATHOLOGY (SHANDS HOSPITAL AT THE UNIVERSITY OF FLORIDA): Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor
: Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor") HEMATOPATHOLOGY (SHANDS HOSPITAL AT THE UNIVERSITY OF FLORIDA): Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor I. Description of the rotation: During this rotation, the resident will gain
HEMATOPATHOLOGY (SHANDS HOSPITAL AT THE UNIVERSITY OF FLORIDA): Rotation Director: Ying Li, M.D., Ph.D., Assistant Professor I. Description of the rotation: During this rotation, the resident will gain
Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent
 Int J Clin Exp Med 2014;7(1):307-311 www.ijcem.com /ISSN:1940-5901/IJCEM1311029 Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent Qilin Ao 2, Ying Wang 1, Sanpeng Xu 2,
Int J Clin Exp Med 2014;7(1):307-311 www.ijcem.com /ISSN:1940-5901/IJCEM1311029 Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent Qilin Ao 2, Ying Wang 1, Sanpeng Xu 2,
The spectrum of flow cytometry of the bone marrow
 The spectrum of flow cytometry of the bone marrow Anna Porwit Lund University Faculty of Medicine Dept. of Clinical Sciences Div. Oncology and Pathology anna.porwit@med.lu.se Disclosure of speaker s interests
The spectrum of flow cytometry of the bone marrow Anna Porwit Lund University Faculty of Medicine Dept. of Clinical Sciences Div. Oncology and Pathology anna.porwit@med.lu.se Disclosure of speaker s interests
, , 2011 HODGKIN LYMPHOMA
 European Federation of Cytology Societies 4tu Annual Tutorial in Cytopathology Trieste, June 6-10, 2011 HODGKIN LYMPHOMA Classification The World Health Organization Classification of Lymphomas (2001)
European Federation of Cytology Societies 4tu Annual Tutorial in Cytopathology Trieste, June 6-10, 2011 HODGKIN LYMPHOMA Classification The World Health Organization Classification of Lymphomas (2001)
Lymphoma Update: Lymphoma Update: What s Likely to be New in the New WHO. Patrick Treseler, MD, PhD University of California San Francisco
 Lymphoma Update: What s Likely to be New in the New WHO Blood 127:2375; 2016 Patrick Treseler, MD, PhD University of California San Francisco Lymphoma Update: What IS New in the New WHO! Patrick Treseler,
Lymphoma Update: What s Likely to be New in the New WHO Blood 127:2375; 2016 Patrick Treseler, MD, PhD University of California San Francisco Lymphoma Update: What IS New in the New WHO! Patrick Treseler,
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Immunohistochemical classification of haematolymphoid tumours. Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital
 Immunohistochemical classification of haematolymphoid tumours Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital Malignant lymphoproliferative diseases What are they? Haematolymphoid
Immunohistochemical classification of haematolymphoid tumours Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital Malignant lymphoproliferative diseases What are they? Haematolymphoid
Aggressive B-cell Lymphomas Updated WHO classification Elias Campo
 Aggressive B-cell Lymphomas Updated WHO classification Elias Campo Hospital Clinic, University of Barcelona Diffuse Large B-cell Lymphoma A Heterogeneous Category Subtypes with differing: Histology and
Aggressive B-cell Lymphomas Updated WHO classification Elias Campo Hospital Clinic, University of Barcelona Diffuse Large B-cell Lymphoma A Heterogeneous Category Subtypes with differing: Histology and
Classification of Hematologic Malignancies. Patricia Aoun MD MPH
 Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Non-Hodgkin s Lymphomas Version
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
WHO Classification. B-cell chronic lymphocytic leukemia/small T-cell granular lymphocytic leukemia
 Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
T cell lymphoma diagnostics and differential diagnosis to Hodgkin lymphoma
 T cell lymphoma diagnostics and differential diagnosis to Hodgkin lymphoma Sylvia Hartmann Dr. Senckenberg Institute of Pathology Goethe University Frankfurt Overview Borderline ALCL classical HL Borderline
T cell lymphoma diagnostics and differential diagnosis to Hodgkin lymphoma Sylvia Hartmann Dr. Senckenberg Institute of Pathology Goethe University Frankfurt Overview Borderline ALCL classical HL Borderline
FOLLICULARITY in LYMPHOMA
 FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
Common Problem Areas. WHO Classification. Defines separate diseases (entities) with their CLINICAL AGGRESSIVENESS LOW GRADE / HIGH GRADE
 with their CLINICAL AGGRESSIVENESS LOW GRADE / HIGH GRADE") WHO Classification Defines separate diseases (entities) with their CLINICAL AGGRESSIVENESS REVIEW OF MOST COMMON LYMPHOMA ENTITIES Dr Stefan Dojcinov LOW GRADE / HIGH GRADE (June 2014) The Non-Hodgkin
WHO Classification Defines separate diseases (entities) with their CLINICAL AGGRESSIVENESS REVIEW OF MOST COMMON LYMPHOMA ENTITIES Dr Stefan Dojcinov LOW GRADE / HIGH GRADE (June 2014) The Non-Hodgkin
Burkitt lymphoma. Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8
 Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH
 EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH CASE E1 M: 68 yrs Left destructive sinonasal lesion.?lymphoma?adenocarcinoma CD20 CD10 BCL6 MIB1 Answers Diffuse large B cell
EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH CASE E1 M: 68 yrs Left destructive sinonasal lesion.?lymphoma?adenocarcinoma CD20 CD10 BCL6 MIB1 Answers Diffuse large B cell
Integrated Hematopathology. Morphology and FCI with IHC
 Integrated Hematopathology Morphology and FCI with IHC FrontMatter.indd i 9/6/2009 9:30:12 PM FrontMatter.indd ii 9/6/2009 9:30:18 PM Integrated Hematopathology Morphology and FCI with IHC Cherie H Dunphy,
Integrated Hematopathology Morphology and FCI with IHC FrontMatter.indd i 9/6/2009 9:30:12 PM FrontMatter.indd ii 9/6/2009 9:30:18 PM Integrated Hematopathology Morphology and FCI with IHC Cherie H Dunphy,
PhenoPath. Diagnoses you can count on B CELL NON-HODGKIN LYMPHOMA
 PhenoPath Diagnoses you can count on B CELL NON-HODGKIN LYMPHOMA C urrent diagnosis of B cell non-hodgkin lymphoma (B-NHL) is based on the 2008 WHO Classification of Tumours of Haematopoietic and Lymphoid
PhenoPath Diagnoses you can count on B CELL NON-HODGKIN LYMPHOMA C urrent diagnosis of B cell non-hodgkin lymphoma (B-NHL) is based on the 2008 WHO Classification of Tumours of Haematopoietic and Lymphoid
3/23/2017. Disclosure of Relevant Financial Relationships. Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?!
 Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?! Judith A. Ferry Massachusetts General Hospital Disclosure of Relevant Financial Relationships USCAP requires that all
Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?! Judith A. Ferry Massachusetts General Hospital Disclosure of Relevant Financial Relationships USCAP requires that all
Large cell immunoblastic Diffuse histiocytic (DHL) Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s
 Lymphoblastic lymphoma Diffuse lymphoblastic Small non cleaved cell Burkitt s Non- Burkitt s") Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Non Hodgkin s Lymphoma Introduction 6th most common cause of cancer death in United States. Increasing in incidence and mortality. Since 1970, the incidence of has almost doubled. Overview The types of
Dispersed Cell Population & Lymphoglandular Bodies: Features of lymphoid aspirates FNA OF LYMPH NODES OF THE HEAD AND NECK
 William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital FNA OF LYMPH NODES OF THE HEAD AND
William C. Faquin, MD, PhD Professor of Pathology Harvard Medical School Director of Head and Neck Pathology Massachusetts Eye and Ear Massachusetts General Hospital FNA OF LYMPH NODES OF THE HEAD AND
Plasma cell myeloma (multiple myeloma)
") Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Plasma cell myeloma (multiple myeloma) Common lymphoid neoplasm, present at old age (70 years average) Remember: plasma cells are terminally differentiated B-lymphocytes that produces antibodies. B-cells
Thomas Hodgkin and Hodgkin lymphoma
 J Hematopathol (2014) 7:123 138 DOI 10.1007/s12308-014-0214-3 REVIEW ARTICLE Thomas Hodgkin and Hodgkin lymphoma Judith A. Ferry Received: 26 June 2014 /Accepted: 31 July 2014 /Published online: 12 August
J Hematopathol (2014) 7:123 138 DOI 10.1007/s12308-014-0214-3 REVIEW ARTICLE Thomas Hodgkin and Hodgkin lymphoma Judith A. Ferry Received: 26 June 2014 /Accepted: 31 July 2014 /Published online: 12 August
Defined lymphoma entities in the current WHO classification
 Defined lymphoma entities in the current WHO classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno Bellinzona, January 29-31, 2016 Evolution of lymphoma classification Rappaport Lukes
Defined lymphoma entities in the current WHO classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno Bellinzona, January 29-31, 2016 Evolution of lymphoma classification Rappaport Lukes
EQA 015 for the Nov 2018 workshops. Analysis of the responses received with final diagnoses
 EQA 015 for the Nov 2018 workshops Analysis of the responses received with final diagnoses Case 1: Chest biopsy from 52 year old woman with multiple nodular swellings on the body for 6 yrs. Mostly on the
EQA 015 for the Nov 2018 workshops Analysis of the responses received with final diagnoses Case 1: Chest biopsy from 52 year old woman with multiple nodular swellings on the body for 6 yrs. Mostly on the
88-year-old Female with Lymphadenopathy. Faizi Ali, MD
 88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
Bone Marrow. Procedures Blood Film Aspirate, Cell Block Trephine Biopsy, Touch Imprint
 Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
Aggressive B cell Lymphomas
 Aggressive B cell Lymphomas I have nothing to disclose. Disclosures Raju K. Pillai City of Hope National Medical Center Outline WHO 2016 Classification Large B cell Lymphomas New entities and changes in
Aggressive B cell Lymphomas I have nothing to disclose. Disclosures Raju K. Pillai City of Hope National Medical Center Outline WHO 2016 Classification Large B cell Lymphomas New entities and changes in
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders
 Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
VENTANA hematopathology solutions Comprehensive aids for detecting and subtyping
 VENTANA hematopathology solutions Comprehensive aids for detecting and subtyping 1 12/4/2015 9:47:24 AM 2 Hematopathology diagnostic solutions Contents VENTANA hematopathology assays 3 Detecting and subtyping
VENTANA hematopathology solutions Comprehensive aids for detecting and subtyping 1 12/4/2015 9:47:24 AM 2 Hematopathology diagnostic solutions Contents VENTANA hematopathology assays 3 Detecting and subtyping
Classification! Immunohistochemical classification of haematolymphoid tumours. Malignant lymphoproliferative diseases
 Immunohistochemical classification of haematolymphoid tumours Haematolymphoid Neoplasias: Leukaemia vs Lymphoma C L O N A L M A L I G N A N C I E S Stephen Hamilton-Dutoit Institute of Pathology Aarhus
Immunohistochemical classification of haematolymphoid tumours Haematolymphoid Neoplasias: Leukaemia vs Lymphoma C L O N A L M A L I G N A N C I E S Stephen Hamilton-Dutoit Institute of Pathology Aarhus
VENTANA hematopathology solutions. Deliver diagnostic confidence
 VENTANA hematopathology solutions Deliver diagnostic confidence 2 Hematopathology diagnostic solutions Contents VENTANA hematopathology assays 3 Detecting and subtyping hematological cancers 4 The importance
VENTANA hematopathology solutions Deliver diagnostic confidence 2 Hematopathology diagnostic solutions Contents VENTANA hematopathology assays 3 Detecting and subtyping hematological cancers 4 The importance
Unknown Case 6. Ann T. Moriarty, MD
 Unknown Case 6 Ann T. Moriarty, MD Unknown Case 6 61 year old male with an enlarged cervical lymph node. He has a history of lung carcinoma, renal cell carcinoma and lymphoma. Case 6 Image 1: Fine needle
Unknown Case 6 Ann T. Moriarty, MD Unknown Case 6 61 year old male with an enlarged cervical lymph node. He has a history of lung carcinoma, renal cell carcinoma and lymphoma. Case 6 Image 1: Fine needle
Case 3. Ann T. Moriarty,MD
 Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
Aggressive B-cell Lymphoma 2013
 Aggressive B-cell Lymphoma 2013 Diffuse Large B-Cell Lymphoma Burkitt Lymphoblastic lymphoma Gray zone Intermediate DLBCL/HL Intermediate BL/DLBCL Diffuse Large B-cell lymphoma Common morphology: diffuse
Aggressive B-cell Lymphoma 2013 Diffuse Large B-Cell Lymphoma Burkitt Lymphoblastic lymphoma Gray zone Intermediate DLBCL/HL Intermediate BL/DLBCL Diffuse Large B-cell lymphoma Common morphology: diffuse
Cost-Effective Strategies in the Workup of Hematologic Neoplasm. Karl S. Theil, Claudiu V. Cotta Cleveland Clinic
 Cost-Effective Strategies in the Workup of Hematologic Neoplasm Karl S. Theil, Claudiu V. Cotta Cleveland Clinic In the past 12 months, we have not had a significant financial interest or other relationship
Cost-Effective Strategies in the Workup of Hematologic Neoplasm Karl S. Theil, Claudiu V. Cotta Cleveland Clinic In the past 12 months, we have not had a significant financial interest or other relationship
Follicular Lymphoma: the WHO
 Follicular Lymphoma: the WHO and the WHERE? Yuri Fedoriw, MD Associate Professor of Pathology and Laboratory Medicine Director of Hematopathology University of North Carolina Chapel Hill, NC Disclosure
Follicular Lymphoma: the WHO and the WHERE? Yuri Fedoriw, MD Associate Professor of Pathology and Laboratory Medicine Director of Hematopathology University of North Carolina Chapel Hill, NC Disclosure
Diffuse large B-cell lymphoma (DLBCL) is one of the
 is one of the") Practical Applications in Immunohistochemistry Evaluation of Diffuse Large B-Cell Lymphoma and Related Large B-Cell Lymphomas Dennis P. O Malley, MD; Aaron Auerbach, MD; Lawrence M. Weiss, MD Context.
Practical Applications in Immunohistochemistry Evaluation of Diffuse Large B-Cell Lymphoma and Related Large B-Cell Lymphomas Dennis P. O Malley, MD; Aaron Auerbach, MD; Lawrence M. Weiss, MD Context.
NEW ENTITIES IN AGGRESSIVE B CELL LYMPHOMA. Joon Seong Park, M.D. Dept. of Hematology-Oncology Ajou University School of Medicine
 NEW ENTITIES IN AGGRESSIVE B CELL LYMPHOMA Joon Seong Park, M.D. Dept. of Hematology-Oncology Ajou University School of Medicine Historical background of Lymphoma classification Rappaport classification
NEW ENTITIES IN AGGRESSIVE B CELL LYMPHOMA Joon Seong Park, M.D. Dept. of Hematology-Oncology Ajou University School of Medicine Historical background of Lymphoma classification Rappaport classification
Update on the Classification of Aggressive B-cell Lymphomas and Hodgkin Lymphoma
 Update on the Classification of Aggressive B-cell Lymphomas and Hodgkin Lymphoma Nancy Lee Harris, M. D. Massachusetts General Hospital Harvard Medical School Aggressive B-cell Lymphomas WHO 4 th Edition
Update on the Classification of Aggressive B-cell Lymphomas and Hodgkin Lymphoma Nancy Lee Harris, M. D. Massachusetts General Hospital Harvard Medical School Aggressive B-cell Lymphomas WHO 4 th Edition
WHO UPDATE ON LYMPHOMAS. Dr Priya Mary Jacob Asst Professor, Pathology.
 WHO UPDATE ON LYMPHOMAS Dr Priya Mary Jacob Asst Professor, Pathology 3 rd 4 th 4 th revised 2001 2008 2017 The Change The Significance of the Change- Diagnostic, Prognostic The Rationale behind the change.
WHO UPDATE ON LYMPHOMAS Dr Priya Mary Jacob Asst Professor, Pathology 3 rd 4 th 4 th revised 2001 2008 2017 The Change The Significance of the Change- Diagnostic, Prognostic The Rationale behind the change.
Aggressive B cell Lymphomas
 Aggressive B cell Lymphomas Raju K. Pillai City of Hope National Medical Center I have no disclosures Outline What is new in the WHO 2016 classification Insights from genomic studies Double Hit Lymphoma
Aggressive B cell Lymphomas Raju K. Pillai City of Hope National Medical Center I have no disclosures Outline What is new in the WHO 2016 classification Insights from genomic studies Double Hit Lymphoma
Understanding your diagnosis. Dr Graham Collins Consultant Haemtologist Oxford University Hospitals
 Understanding your diagnosis Dr Graham Collins Consultant Haemtologist Oxford University Hospitals Common questions I get asked What is lymphoma? What subtype do I have and what does that mean? What are
Understanding your diagnosis Dr Graham Collins Consultant Haemtologist Oxford University Hospitals Common questions I get asked What is lymphoma? What subtype do I have and what does that mean? What are
ISIMM Tata Conference on Immunohistochemistry. Kolkata, India, January Immunohistochemistry. A cost effective approach to lymphoma diagnosis
 ISIMM Tata Conference on Immunohistochemistry. Kolkata, India, January 2018 Immunohistochemistry A cost effective approach to lymphoma diagnosis Clive R. Taylor, M.D., Ph.D., Department of Pathology, Keck
ISIMM Tata Conference on Immunohistochemistry. Kolkata, India, January 2018 Immunohistochemistry A cost effective approach to lymphoma diagnosis Clive R. Taylor, M.D., Ph.D., Department of Pathology, Keck
Non-Hodgkin Lymphoma. Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract.
 Non-Hodgkin Lymphoma Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract. Protocol revision date: January 2005 No AJCC/UICC staging system Procedures Cytology
Non-Hodgkin Lymphoma Protocol applies to non-hodgkin lymphoma involving any organ system except the gastrointestinal tract. Protocol revision date: January 2005 No AJCC/UICC staging system Procedures Cytology
Diagnostic Molecular Pathology of Lymphoid Neoplasms
 Diagnostic Molecular Pathology of Lymphoid Neoplasms (Part II) Rational use of molecular testing in lymphomas Beirut, Lebanon Friday December 2, 2011: Hematopathology Session Adam Bagg University of Pennsylvania
Diagnostic Molecular Pathology of Lymphoid Neoplasms (Part II) Rational use of molecular testing in lymphomas Beirut, Lebanon Friday December 2, 2011: Hematopathology Session Adam Bagg University of Pennsylvania
Pulmonary biopsy specimens demonstrate
 A PRACTICAL APPROACH TO THE EVALUATION OF LYMPHOID AND PLASMA CELL INFILTRATES IN THE LUNG Fiona E. Craig, MD KEYWORDS Lymphoma Pulmonary Immunophenotyping Genotyping ABSTRACT Pulmonary biopsy specimens
A PRACTICAL APPROACH TO THE EVALUATION OF LYMPHOID AND PLASMA CELL INFILTRATES IN THE LUNG Fiona E. Craig, MD KEYWORDS Lymphoma Pulmonary Immunophenotyping Genotyping ABSTRACT Pulmonary biopsy specimens
Anaplastic Large Cell Lymphoma (of T cell lineage)
") Anaplastic Large Cell Lymphoma (of T cell lineage) Definition T-cell lymphoma comprised of large cells with abundant cytoplasm and pleomorphic, often horseshoe-shaped nuclei CD30+ Most express cytotoxic
Anaplastic Large Cell Lymphoma (of T cell lineage) Definition T-cell lymphoma comprised of large cells with abundant cytoplasm and pleomorphic, often horseshoe-shaped nuclei CD30+ Most express cytotoxic
2012 by American Society of Hematology
 2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
Clinical Policy: Bendamustine (Bendeka, Treanda) Reference Number: PA.CP.PHAR.307
 Reference Number: PA.CP.PHAR.307") Clinical Policy: (Bendeka, Treanda) Reference Number: PA.CP.PHAR.307 Effective Date: 01/18 Last Review Date: 11/17 Coding Implications Revision Log Description The intent of the criteria is to ensure that
Clinical Policy: (Bendeka, Treanda) Reference Number: PA.CP.PHAR.307 Effective Date: 01/18 Last Review Date: 11/17 Coding Implications Revision Log Description The intent of the criteria is to ensure that
3/24/2017 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS. Disclosure of Relevant Financial Relationships
 DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
DENDRITIC CELL NEOPLASMS: HISTOLOGY, IMMUNOHISTOCHEMISTRY, AND MOLECULAR GENETICS Jason L. Hornick, M.D., Ph.D. Director of Surgical Pathology and Immunohistochemistry Brigham and Women s Hospital Professor
Test Utilization: Chronic Lymphocytic Leukemia
 Test Utilization: Chronic Lymphocytic Leukemia Initial Evaluation Diagnostic Criteria Selection of Tests for Prognosis Response to Therapy Challenges Assessment for persistent disease Paul J. Kurtin, M.D.
Test Utilization: Chronic Lymphocytic Leukemia Initial Evaluation Diagnostic Criteria Selection of Tests for Prognosis Response to Therapy Challenges Assessment for persistent disease Paul J. Kurtin, M.D.
LYMPHOMAS an overview of some subtypes of NHLs
 One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li,
: Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li,") High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li, M.D., Ph.D. Fudan University Shanghai Cancer Center
High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li, M.D., Ph.D. Fudan University Shanghai Cancer Center
ECP meeting, Lisbon, september 2012 Slide seminar New and old challenges in the diagnosis of peripheral T-cell lymphomas
 ECP meeting, Lisbon, september 2012 Slide seminar New and old challenges in the diagnosis of peripheral T-cell lymphomas Philippe Gaulard, Dept of Pathology, INSERM U955, Hôpital Henri Mondor, 94010 -
ECP meeting, Lisbon, september 2012 Slide seminar New and old challenges in the diagnosis of peripheral T-cell lymphomas Philippe Gaulard, Dept of Pathology, INSERM U955, Hôpital Henri Mondor, 94010 -
5/16/2018 HEMATOPATHOLOGY FOR CYTOPATHOLOGISTS HEMATOPATHOLOGY FOR C CYTOPATHOLOGISTS I HAVE NOTHING TO C DISCLOSE
 HEMATOPATHOLOGY FOR C CYTOPATHOLOGISTS Kathryn Lindsey, MD McKee Cytology Symposium HEMATOPATHOLOGY FOR C CYTOPATHOLOGISTS Kathryn Lindsey, MD McKee Cytology Symposium I HAVE NOTHING TO C DISCLOSE Kathryn
HEMATOPATHOLOGY FOR C CYTOPATHOLOGISTS Kathryn Lindsey, MD McKee Cytology Symposium HEMATOPATHOLOGY FOR C CYTOPATHOLOGISTS Kathryn Lindsey, MD McKee Cytology Symposium I HAVE NOTHING TO C DISCLOSE Kathryn
Lymphoma: The Basics. Dr. Douglas Stewart
 Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
Lymphoma: The Basics Dr. Douglas Stewart Objectives What is lymphoma? How common is it? Why does it occur? How do you diagnose it? How do you manage it? How do you follow patients after treatment? What
Lymphoma Read with the experts
 Lymphoma Read with the experts Marc Seltzer, MD Associate Professor of Radiology Geisel School of Medicine at Dartmouth Director, PET-CT Course American College of Radiology Learning Objectives Recognize
Lymphoma Read with the experts Marc Seltzer, MD Associate Professor of Radiology Geisel School of Medicine at Dartmouth Director, PET-CT Course American College of Radiology Learning Objectives Recognize
Lymphoma classification: a still ongoing journey
 Lymphoma classification: a still ongoing journey Stefano A. Pileri Professor of Pathology, Bologna University Medical School Director of Haematopathology, St. Orsola Policlinic (at present) Director of
Lymphoma classification: a still ongoing journey Stefano A. Pileri Professor of Pathology, Bologna University Medical School Director of Haematopathology, St. Orsola Policlinic (at present) Director of
I n the past 10 years, fine needle aspiration (FNA) cytology
 cytology") 821 ORIGINAL ARTICLE Fine needle aspiration cytology in the diagnosis of uncommon types of lymphoma F Mayall, A Darlington, B Harrison... See end of article for authors affiliations... Correspondence to:
821 ORIGINAL ARTICLE Fine needle aspiration cytology in the diagnosis of uncommon types of lymphoma F Mayall, A Darlington, B Harrison... See end of article for authors affiliations... Correspondence to:
Hematopathology Specialty Conference Case #1
 Hematopathology Specialty Conference Case #1 Robert (Bob) Ohgami, MD, PhD Assistant Professor Stanford University Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships
Hematopathology Specialty Conference Case #1 Robert (Bob) Ohgami, MD, PhD Assistant Professor Stanford University Disclosure of Relevant Financial Relationships Disclosure of Relevant Financial Relationships
10/31/2017. Immunodeficiencies. Outline. Discuss EBV. Non-destructive Polymorphic Monomorphic Therapies Challenges
 I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Outline Transplant Congenital Autoimmunity T-cell/immune
I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Outline Transplant Congenital Autoimmunity T-cell/immune
2010 Hematopoietic and Lymphoid ICD-O Codes - Alphabetical List THIS TABLE REPLACES ALL ICD-O-3 Codes
 Acute basophilic leukemia 9870/3 Acute biphenotypic leukemia [OBS] 9805/3 Acute erythroid leukemia 9840/3 Acute megakaryoblastic leukemia 9910/3 Acute monoblastic and monocytic leukemia 9891/3 Acute myeloid
Acute basophilic leukemia 9870/3 Acute biphenotypic leukemia [OBS] 9805/3 Acute erythroid leukemia 9840/3 Acute megakaryoblastic leukemia 9910/3 Acute monoblastic and monocytic leukemia 9891/3 Acute myeloid
2012 Hematopoietic and Lymphoid ICD-O Codes - Numerical List THIS TABLE REPLACES ALL ICD-O-3 Codes
 Malignant lymphoma, NOS 9590/3 Non-Hodgkin lymphoma, NOS 9591/3 B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma 9596/3 Primary
Malignant lymphoma, NOS 9590/3 Non-Hodgkin lymphoma, NOS 9591/3 B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma 9596/3 Primary
Lymphocytoma Cutis. Cynthia M. Magro MD. Director of Dermatopathology Weill Medical College of Cornell University New York, New York
 Lymphocytoma Cutis Cynthia M. Magro MD Professor of Pathology Director of Dermatopathology Weill Medical College of Cornell University New York, New York Lymphocytoma Cutis Falls under other designations
Lymphocytoma Cutis Cynthia M. Magro MD Professor of Pathology Director of Dermatopathology Weill Medical College of Cornell University New York, New York Lymphocytoma Cutis Falls under other designations
Chapter 12 The Role of Fine Needle Aspiration Biopsy in the Diagnosis and Management of Hematopoietic Neoplasms
 Chapter 12 The Role of Fine Needle Aspiration Biopsy in the Diagnosis and Management of Hematopoietic Neoplasms Rana S. Hoda FINE NEEDLE ASPIRATION Introduction Fine needle aspiration (FNA) is a well-established
Chapter 12 The Role of Fine Needle Aspiration Biopsy in the Diagnosis and Management of Hematopoietic Neoplasms Rana S. Hoda FINE NEEDLE ASPIRATION Introduction Fine needle aspiration (FNA) is a well-established
Patterns of lymph node biopsy pathology at. Chris Hani Baragwanath Academic Hospital. over a period of three years Denasha Lavanya Reddy
 Patterns of lymph node biopsy pathology at Chris Hani Baragwanath Academic Hospital over a period of three years 2010-2012 Denasha Lavanya Reddy Student number: 742452 A research report submitted to the
Patterns of lymph node biopsy pathology at Chris Hani Baragwanath Academic Hospital over a period of three years 2010-2012 Denasha Lavanya Reddy Student number: 742452 A research report submitted to the
Update in Lymphoma Imaging
 Update in Lymphoma Imaging Victorine V. Muse, MD Lymphoma Update in Lymphoma Imaging Victorine V Muse, MD Heterogeneous group of lymphoid neoplasms divided into two broad histological categories Hodgkin
Update in Lymphoma Imaging Victorine V. Muse, MD Lymphoma Update in Lymphoma Imaging Victorine V Muse, MD Heterogeneous group of lymphoid neoplasms divided into two broad histological categories Hodgkin
FINALIZED SEER SINQ S NOVEMBER 2011
 : 20110133 Multiple primaries/heme & Lymphoid Neoplasms: A patient was diagnosed 7/31/08 with DLBCL (9680/3) (biopsy left supraclav. node), stage IIIB. Treated with chemo. 10/14/10 biopsy right supraclav.
: 20110133 Multiple primaries/heme & Lymphoid Neoplasms: A patient was diagnosed 7/31/08 with DLBCL (9680/3) (biopsy left supraclav. node), stage IIIB. Treated with chemo. 10/14/10 biopsy right supraclav.
A 64yo female with tuberculous empyema not improving on treatment: A tribute and farewell to Dr. Alphonse Kayembe
 A 64yo female with tuberculous empyema not improving on treatment: A tribute and farewell to Dr. Alphonse Kayembe Continuing Medical Education Announcement Harvard Medical School RSS 3081: Monthly BOTSOGO
A 64yo female with tuberculous empyema not improving on treatment: A tribute and farewell to Dr. Alphonse Kayembe Continuing Medical Education Announcement Harvard Medical School RSS 3081: Monthly BOTSOGO
11/2/2017. Immunodeficiencies. Joo Y. Song, MD Assistant Professor of Clinical Pathology. I have no financial disclosures.
 I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Transplant Autoimmunity Drugs T-cell dysfunction (Age,
I have no financial disclosures Joo Y. Song, MD Assistant Professor of Clinical Pathology City of Hope National Medical Center Immunodeficiencies Transplant Autoimmunity Drugs T-cell dysfunction (Age,
WHO 4th ED Classification of Mature B-cell Neoplasms
 WHO 4th ED Classification of Mature B-cell Neoplasms Chronic lymphocytic leukemia /Small lymphocytic lymphoma B-cell prolymphocytic leukaemia Splenic marginal zone lymphoma Hairy cell leukemia Splenic
WHO 4th ED Classification of Mature B-cell Neoplasms Chronic lymphocytic leukemia /Small lymphocytic lymphoma B-cell prolymphocytic leukaemia Splenic marginal zone lymphoma Hairy cell leukemia Splenic
INTRODUCTION TO PATHOLOGICAL TECHNIQUES. 1. Types of routine biopsy procedures 2. Special exams (IHC, FISH)
") INTRODUCTION TO PATHOLOGICAL TECHNIQUES 1. Types of routine biopsy procedures 2. Special exams (IHC, FISH) Biopsy-Indications Diffuse/multifocal lesions (neoplastic, inflammatory, etc) Etiology of the
INTRODUCTION TO PATHOLOGICAL TECHNIQUES 1. Types of routine biopsy procedures 2. Special exams (IHC, FISH) Biopsy-Indications Diffuse/multifocal lesions (neoplastic, inflammatory, etc) Etiology of the
Lymphoid Neoplasms. Sylvie Freeman Department of Clinical Immunology, University of Birmingham
 Lymphoid Neoplasms Sylvie Freeman Department of Clinical Immunology, University of Birmingham Incidence of Haematological Malignancies UK2001 (CRUK) Malignancy New Cases All Cancers 271,000 Leukaemia 6,760
Lymphoid Neoplasms Sylvie Freeman Department of Clinical Immunology, University of Birmingham Incidence of Haematological Malignancies UK2001 (CRUK) Malignancy New Cases All Cancers 271,000 Leukaemia 6,760
Pathology of the Lymphoid System
 Pathology of the Lymphoid System Learning Objectives: Define lymphadenitis and enumerate its types. Briefly describe the morphological appearance of reactive lymph node. Describe the microscopic picture
Pathology of the Lymphoid System Learning Objectives: Define lymphadenitis and enumerate its types. Briefly describe the morphological appearance of reactive lymph node. Describe the microscopic picture