Case year old male with abdominal lymphadenopathy Treated with 8 cycles of R-CHOP One year later B-symptoms and progressive disease
|
|
|
- Antonia Wiggins
- 5 years ago
- Views:
Transcription
1 Codirectors Tsieh Sun, M.D., FASCP Francisco Vega, M.D., Ph.D. Department of Hematopathology UT MD Anderson Cancer Center Houston Texas
2 There is no conflict of interest involved in the content and presentation of this workshop
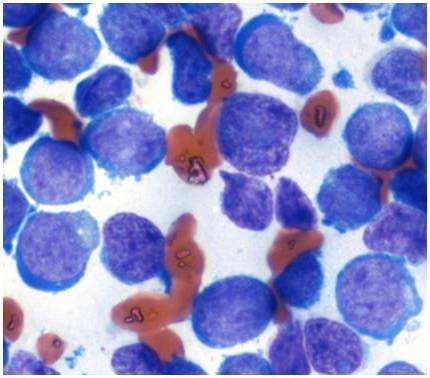
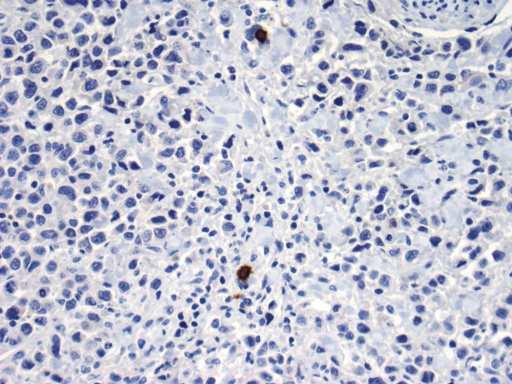
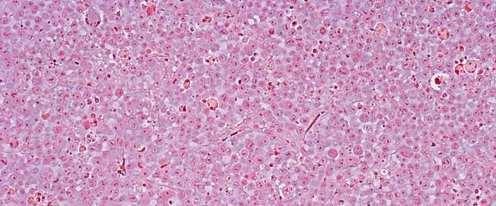
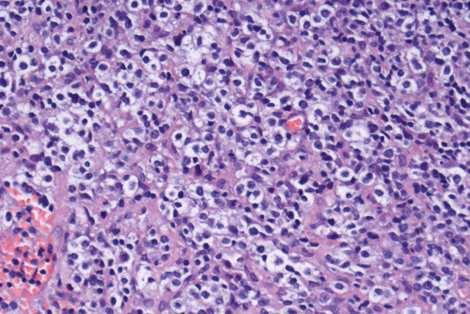
3 Case 1 67 year old male with abdominal lymphadenopathy Treated with 8 cycles of R-CHOP One year later B-symptoms and progressive disease




4 Retroperitoneum 2006 Inguinal LN 2007 BCL2 IgH/BCL2 MYC
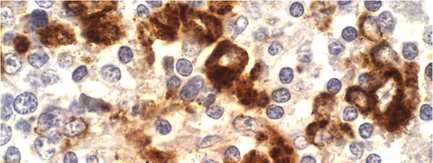
5 Double-Hit Lymphoma B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma (DLBCL) and Burkitt lymphoma (BL)






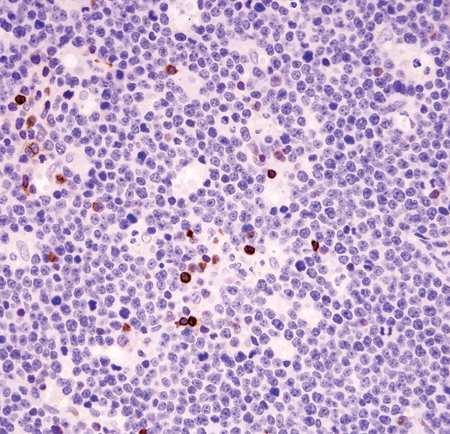
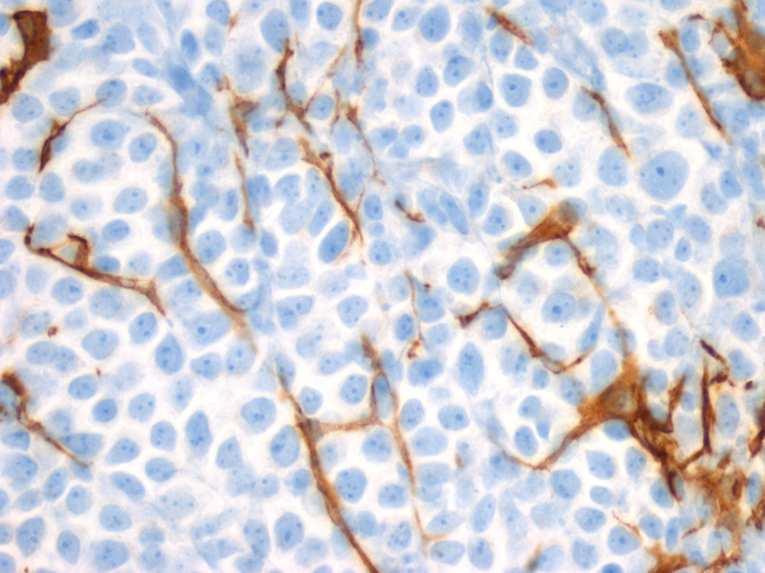
6 BCL-2 Ki-67





7 BCL-2 Ki-67




8 BCL-2 BCL-6
9 DLBCL/BL Definition Aggressive B-cell lymphoma with morphological and genetic features of both DLBCL and BL This is a heterogeneous category and not a distinct entity This category also includes "double-hit" or "triplehit" lymphomas (cases with translocations involving MYC and BCL2, and/or BCL6 genes)
10 DLBCL/BL Possible Scenarios for Diagnosis 1) Neoplasm resembles BL but too much variation in cell size and nuclear contours 2) Neoplasm resembles BL but atypical immunophenotype &/or genetic findings 3) Neoplasms with blastic chromatin with lymphoblastic lymphoma-like appearance
11 DLBCL/BL Immunophenotypic Features Frequent germinal center cell phenotype (CD10+ and BCL6+) Variable but usually high Ki-67 In double-hit lymphomas, BCL2 is usually strongly positive Lymphomas morphologically defined as BL with BCL2 positivity can also be placed in this category
12 DLBCL/BL Genetic Features Complex karyotype (> 3 abnormalities) MYC translocations in up to 50% of the cases: ~ 60% of cases involve Ig gene loci ~ 40% of cases other translocation partners ~ 15% have BCL2 translocations sometimes together with MYC rearrangements (double-hit lymphomas) BCL6 translocations are less frequent (along with BCL2 translocations define triple-hit lymphomas)

13





14 Burkitt Lymphoma CD10 BCL2 Ki-67 TCL-1
15 32/M, skin lesion on his trunk with B symptoms for 6 months Hematology: no cytopenia or leukocytosis
16 IHC-skin: Positive for CD4, CD56, CD68, negative for CD3, CD5, CD8, CD20, MPO, lysozyme Flow-skin: Positive for CD2, CD4, CD7, CD45, CD56, HLA-DR, negative for CD3, CD8, CD10, CD13, CD19, CD33, CD34, CD117, TdT, MPO Flow-BM: Positive for CD2, CD4, CD7, CD13, CD33, CD56, negative for CD3, CD8, CD11c, CD14, CD19, CD20, CD57, κ, λ, TdT TCR rearrangement: germline


17


18


19


20
21 Brody J et al. Acute agranular CD4-positive natural killer cell leukemia, Cancer 1995;75: WHO classification: Blastic NK-cell lymphoma WHO/EORTC classification for cutaneous lymphomas: CD4+/CD56+ hematodermic neoplasms WHO classification: Blastic plasmacytoid dendritic cell neoplasm
22 History: skin lesion, followed by bone marrow or lymph node involvement. Leukemic phase may or may not be present. Morphology: Immature blast-like cell with no cytoplasmic granules. Pearl necklace appearance, rare. Immunophenotype: diagnostic Molecular genetics: No specific karyotype or gene rearrangement
23 Basic immunophenotype: CD4+, CD56+, cell lineage marker negative Specific markers: CD123, blood dendritic cell antigen 2 (BDCA2), CD2-associated adaptor protein (CD2AP) Additional markers: T-cell leukemia/lymphoma 1 (TCL1), cutaneous lymphocyte-associated antigen (CLA), BDCA4
24 Cutaneous T-cell lymphoma: CD4+, CLA+, but CD56, CD123, BDCA2/CD2AP negative NK lymphoma: CD56+, but CD4 and PDC marker negative. EBV+ and cytotoxic proteins+ M4/M5/CMML: CD4, CD56, CD68, CD123 positive, but BDCA2 and CD2AP negative. Myelomonocytic panel positive.
25 Case 3 75 year old female with red/violaceous plaques and nodules in the distal aspect of her right leg




26


27 CD10 MUM1 CD20 CD3 BCL-2
28 Primary Cutaneous Diffuse Large B-Cell Lymphoma, Leg Type
29 Primary Cutaneous DLBCL, Leg Type Definition Primary defined on the basis of morphologic features Confluent sheets of large cells with round nuclei, ie, centroblasts and immunoblasts (large cleaved cells are not allowed)
30 Primary Cutaneous DLBCL, Leg Type Clinical Findings Elderly (79 yrs) and females patients Rapidly growing tumors most commonly on the distal aspect of the leg 20% multiple skin lesions at presentation Ulceration is common Similar tumors can arise in other skin areas Aggressive behavior 5 yrs survival rate, ~50%
31 Primary Cutaneous DLBCL, Leg Type Important Features for the Diagnosis Monomorphism of the infiltrate Lack of background inflammatory cells Lack of stromal reaction Lack of networks of follicular dendritic cells
32 Primary Cutaneous DLBCL, Leg Type Immunohistochemistry CD20+ BCL-2+ (strong;100%) BCL6+ (30%) MUM-1+ (80%) HGAL+ (~30%) IgM+ (100%) CD10+ (weak; 25%) FOXP1+ (80%) CD10-
33 Primary Cutaneous Follicle Center Lymphoma






34 BCL-2
, LMO2+ (100%) CD10+")
 FOXP1-")
35 Primary Cutaneous Follicle Center Lymphoma BCL6+ (100%), LMO2+ (100%) CD10+ (37%) Negativity for CD10 correlates with a diffuse pattern BCL2- (60%) FOXP1- BCL-6 BCL-2
36 Primary Cutaneous Follicle Center Lymphoma Molecular Genetics t(14;18) by PCR: 60% of PCFCL* t(14;18) by FISH: 41% of cases & t(14;18)(q32;q21) frequently occurs in PCFCL The cases positive for t(14;18) are more frequently positive for BCL2 (54.5% vs 25%) *Weinberg et al. Am J Surg Pathol 2009; & Streubel et al. Am J Surg Pathol 2006;
37 71/Μ, admitted for splenectomy H/O polycythemia vera 5 yrs ago Lab findings: WBC 16,500/µl, Hb 11.8 g/dl, Hct 35%, platelets 325,000/µl, LDH 690 U/L
38 Spleen: Extramedullary hematopoiesis Bone marrow: myelofibrosis and megakaryocytic hyperplasia Normal karyotype and FISH for BCR-ABL 1 negative CT: Portal vein thrombosis (1 month later)


39


40


41


42
43 Polycythemia vera: Hb 18.5 g/dl (16.5 g/dl); JAK2 V617F/JAK2 exon 12 (95%) Essential thrombocythemia: Platelets > 450K/µl; BM: proliferation of large, mature megakaryocytes; JAK2 or MPL mutations (50%) Primary myelofibrosis: Myelofibrosis with atypical megakaryocytic hyperplasia; JAK2 or MPL mutation (50%). Myelosis (prefibrotic)
44 Leukoerythroblastosis Increased serum LDH Anemia Splenomegaly One or more B-symptoms


45

46
47 Case 5 31 year old female with L2 dorsal vertebral mass and left supraclavicular lymph node




48










49 CD20 CD4 IgA EMA CD79a EBER CD30 CD45 ALK
50 ALK-Positive Diffuse Large B- Cell Lymphoma
 Clathrin (CTCL)-ALK t(2;5)(p23;q35) (10%) NPM-ALK t(2;3)(p23;q27) (?) SEC31A-ALK t(2;5)(p23.1;q35) (?")
51 ALK+ DLBCL Definition Diffuse large B-cell lymphoma expressing ALK protein and associated with ALK gene abnormalities t(2;17)(p23;q23) (70%) Clathrin (CTCL)-ALK t(2;5)(p23;q35) (10%) NPM-ALK t(2;3)(p23;q27) (?) SEC31A-ALK t(2;5)(p23.1;q35) (?) Sequestosome 1 (SQSTM1)-ALK
52 ALK+ DLBCL Epidemiology Rare tumor, less than 1% of all cases of DLBCL - ~ 80 cases reported to date Median age is 40 years (range 9-85) with 30% of cases occur in the pediatric population More frequent in male than female (ratio of 5 to 1) No apparent ethnic predisposition No association with immunosuppression
53 ALK+ DLBCL Immunophenotypic Features By definition ALK+ The pattern of ALK expression predicts ALK partner in fusion gene: -Clathrin (CLTC) and SEC31A: Granular/cytoplasmic -NPM: Nuclear, nucleolar, and cytoplasmic -Sequestosome 1 (SQSTM1): Diffuse/cytoplasmic Takeuchi K et al. Haematologica 2011;96:464-7.
54 ALK+ DLBCL Immunophenotypic Features Positive for: -CD138, VS38, EMA, -CD45/LCA (weak) -CD4 (50%) and CD43 (rare) -cyto Ig (90%) [IgA>95%; rare cases IgG] -CD57 & cytokeratin (~10%; dot like) Negative for: CD30, CD20, EBER
55 Pathologic Pearls Consider performing ALK on all tumors with plasmablastic features in particular in cases not associated to HIV Remember that these tumors are negative for CD20, CD30 and EBER Morphologic overlap with plasmablastic lymphoma
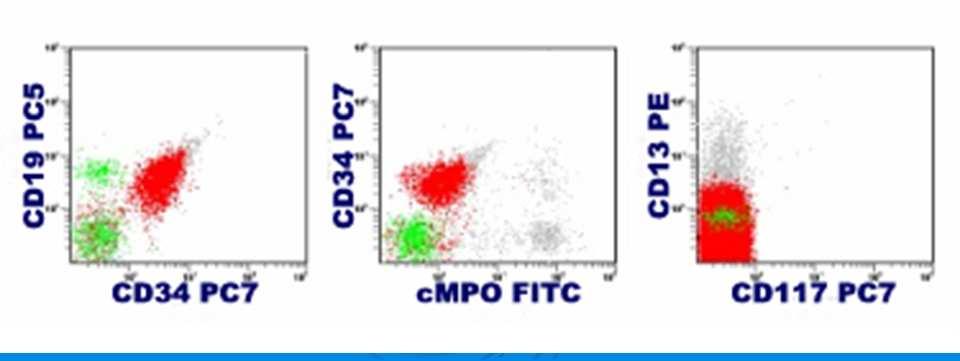
56 48/M, high fever and severe back pain for several days. Platelets dropped from 208,000 to 30,000/µl; WBC 10,500/µl with 13% blasts; Hct 33%, Hb 11.7 g/dl Epistaxis and oral mucosal bleeding. P.E. No organomegaly and lymphadenopathy

57

58


59


60

61
62
63 T cell: CD3, except for CD3 zeta B cell: CD19, with coexpression of CD79a, CD10 or cytoplasmic CD22 Myeloid cell: Myeloperoxidase Monocyte: Nonspecific esterase, CD11c, CD14, CD64, lysozyme (2 markers)
64 FISH for MYC gene rearrangement: negative Rule out Burkitt lymphoma RT-PCR for Fms-like tyrosine kinase 3/internal tandem duplication (FLT3/ITD): negative High incidence in AML and poor prognostic indicator but potential target for therapy
65 t(9;22)(q34;q11.2); BCR-ABL 1 t(v;11q23); MLL rearranged B/myeloid NOS T/myeloid NOS Mixed phenotype acute leukemia, NOS - rare type (T/B; T/B/myeloid)
66 t(8;21)(q22;q22) t(15;17)(q22;q12) inv (16)(p13.1q22) or t(16;16)(p13.1;q22) Acute leukemia with FGFR1 mutation CML with lymphoid blast crisis MDS-related AML Therapy-related AML
67 Case 7 35 year old male with large mediastinal mass



68





69 CD20 CD79a CD30 CD15 CD45 EBV-LMP1
70 B-cell lymphoma, unclassifiable, with features intermediate between DLBCL and Classical Hodgkin Lymphoma
71 DLBCL/CHL Definition Lymphoma with clinical, morphologic, &/or immunophenotypic features between DLBCL and classical HL It does not include composite or sequential cases of both neoplasms
72 DLBCL/CHL Epidemiology and Prognosis Young patients, yrs (range:13-70 yrs) More frequent in males than females More common in western countries Less common in african americans Aggressive course and poorer outcome than CHL or primary mediastinal B-cell lymphoma
73 DLBCL/CHL Clinical Presentation Anterior mediastinal mass Direct extension into lungs Advanced clinical stage (III or IV) Supraclavicular LNs can be involved Other peripheral LNs are rarely involved





74 CD20
75 DLBCL/CHL Immunophenotypic Features Mixed phenotype Common markers of CHL Expression of markers usually absent in CHL: CD45 (LCA)+, CD20+ & uniformly strong, CD79a+ OCT2+ and BOB1+ Other markers: EBV+; EBER &/or LMP1
76 DLBCL/CHL Lack of uniform diagnostic criteria Minimal criteria required? Deviation of a single marker is enough? CD20 expression in otherwise typical CHL is not sufficient (?) CD15 expression in otherwise typical PMBL seems to be sufficient BOB.1 and OCT2




77 PMLBCL CD20 CD30 MUM1
78 70/M, chest pain, fever, night sweat for 2 wks. P.B.: WBC 14,500/µl, 77.5% poly, 12.2% lymph, 9.1% mono; Hb 15.7 g/dl, platelets 279,000/µl LDH 282 U/L CT: mass in post. mediastinal space with compression of subclavian vein


79


80


81

82


83


84


85


86


87
88 Phenotype THRBCL NLPHL chl CD45 Positive Positive Negative CD20 Positive Positive Negative CD79a Positive Positive Negative BCL-6 Positive Positive Negative PAX5/BSAP Positive Positive Positive BOB1 Positive Positive Negative OCT2 Positive Positive Negative PU.1 Negative Positive Negative CD10 Variable Negative Negative BCL-2 Variable Negative Negative CD15 Negative Negative Positive CD30 Rare Negative Positive EBV Negative Negative Variable EMA Variable Positive Rare J-chain Positive Positive Negative sig Positive Positive Negative
89 BACKGROUND CELL Immunophenotype THRBCL NLPHL chl CD3 Positive Positive Positive CD57 Negative Positive Negative CD20 Negative Positive Negative CD21/CD23 Negative Positive Positive CD68 Positive Rare Variable PD1 Negative Positive Negative
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells. Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital
 Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Differential diagnosis of hematolymphoid tumors composed of medium-sized cells Brian Skinnider B.C. Cancer Agency, Vancouver General Hospital Lymphoma classification Lymphoma diagnosis starts with morphologic
Aggressive B-cell Lymphoma 2013
 Aggressive B-cell Lymphoma 2013 Diffuse Large B-Cell Lymphoma Burkitt Lymphoblastic lymphoma Gray zone Intermediate DLBCL/HL Intermediate BL/DLBCL Diffuse Large B-cell lymphoma Common morphology: diffuse
Aggressive B-cell Lymphoma 2013 Diffuse Large B-Cell Lymphoma Burkitt Lymphoblastic lymphoma Gray zone Intermediate DLBCL/HL Intermediate BL/DLBCL Diffuse Large B-cell lymphoma Common morphology: diffuse
Aggressive B-Cell Lymphomas
 Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
Aggressive B-cell Lymphomas Aggressive B-Cell Lymphomas Stephen Hamilton Dutoit Institute of Pathology Aarhus Kommunehospital B-lymphoblastic lymphoma Diffuse large cell lymphoma, NOS T-cell / histiocyte-rich;
Mixed Phenotype Acute Leukemias
 Mixed Phenotype Acute Leukemias CHEN GAO; AMY M. SANDS; JIANLAN SUN NORTH AMERICAN JOURNAL OF MEDICINE AND SCIENCE APR 2012 VOL 5 NO.2 INTRODUCTION Most cases of acute leukemia can be classified based
Mixed Phenotype Acute Leukemias CHEN GAO; AMY M. SANDS; JIANLAN SUN NORTH AMERICAN JOURNAL OF MEDICINE AND SCIENCE APR 2012 VOL 5 NO.2 INTRODUCTION Most cases of acute leukemia can be classified based
EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH
 EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH CASE E1 M: 68 yrs Left destructive sinonasal lesion.?lymphoma?adenocarcinoma CD20 CD10 BCL6 MIB1 Answers Diffuse large B cell
EQA SCHEME CIRCULATION 33 EDUCATIONAL SLIDES DR GRAEME SMITH MONKLANDS DGH CASE E1 M: 68 yrs Left destructive sinonasal lesion.?lymphoma?adenocarcinoma CD20 CD10 BCL6 MIB1 Answers Diffuse large B cell
Aggressive B-cell Lymphomas
 Neoplastic Hematopathology Update 2018 Aggressive B-cell Lymphomas Raju K. Pillai City of Hope National Medical Center I do not have any disclosures Disclosures Outline New entities and changes in WHO
Neoplastic Hematopathology Update 2018 Aggressive B-cell Lymphomas Raju K. Pillai City of Hope National Medical Center I do not have any disclosures Disclosures Outline New entities and changes in WHO
Immunopathology of Lymphoma
 Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Immunopathology of Lymphoma Noraidah Masir MBBCh, M.Med (Pathology), D.Phil. Department of Pathology Faculty of Medicine Universiti Kebangsaan Malaysia Lymphoma classification has been challenging to pathologists.
Hepatic Lymphoma Diagnosis An Algorithmic Approach
 Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
Hepatic Lymphoma Diagnosis An Algorithmic Approach Ryan M. Gill, M.D., Ph.D. University of California, San Francisco PLEASE TURN OFF YOUR CELL PHONES Disclosure of Relevant Financial Relationships USCAP
NEW ENTITIES IN AGGRESSIVE B CELL LYMPHOMA. Joon Seong Park, M.D. Dept. of Hematology-Oncology Ajou University School of Medicine
 NEW ENTITIES IN AGGRESSIVE B CELL LYMPHOMA Joon Seong Park, M.D. Dept. of Hematology-Oncology Ajou University School of Medicine Historical background of Lymphoma classification Rappaport classification
NEW ENTITIES IN AGGRESSIVE B CELL LYMPHOMA Joon Seong Park, M.D. Dept. of Hematology-Oncology Ajou University School of Medicine Historical background of Lymphoma classification Rappaport classification
76 Molecular Genetics/Immunophenotype in New Entities of the 2008 WHO Classification of Hematopoietic Neoplasms
 76 Molecular Genetics/Immunophenotype in New Entities of the 2008 WHO Classification of Hematopoietic Neoplasms Tsieh Sun MD Francisco Vega-Vazquez MD, PhD 2011 Annual Meeting Las Vegas, NV AMERICAN SOCIETY
76 Molecular Genetics/Immunophenotype in New Entities of the 2008 WHO Classification of Hematopoietic Neoplasms Tsieh Sun MD Francisco Vega-Vazquez MD, PhD 2011 Annual Meeting Las Vegas, NV AMERICAN SOCIETY
Gray Zones and Double Hits Distinguishing True Burkitt Lymphoma from Other High-Grade B-NHLs Burkitt Lymphoma Burkitt-Like Lymphoma DLBCL Patrick Tres
 Gray Zones and Double Hits Distinguishing True Burkitt Lymphoma from Other High-Grade B-NHLs Burkitt Lymphoma Burkitt-Like Lymphoma DLBCL Patrick Treseler, MD, PhD University of California San Francisco
Gray Zones and Double Hits Distinguishing True Burkitt Lymphoma from Other High-Grade B-NHLs Burkitt Lymphoma Burkitt-Like Lymphoma DLBCL Patrick Treseler, MD, PhD University of California San Francisco
Classification of Hematologic Malignancies. Patricia Aoun MD MPH
 Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Aggressive B cell Lymphomas
 Aggressive B cell Lymphomas I have nothing to disclose. Disclosures Raju K. Pillai City of Hope National Medical Center Outline WHO 2016 Classification Large B cell Lymphomas New entities and changes in
Aggressive B cell Lymphomas I have nothing to disclose. Disclosures Raju K. Pillai City of Hope National Medical Center Outline WHO 2016 Classification Large B cell Lymphomas New entities and changes in
Chronic Idiopathic Myelofibrosis (CIMF)
") Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
Lymphoma Update: Lymphoma Update: What s Likely to be New in the New WHO. Patrick Treseler, MD, PhD University of California San Francisco
 Lymphoma Update: What s Likely to be New in the New WHO Blood 127:2375; 2016 Patrick Treseler, MD, PhD University of California San Francisco Lymphoma Update: What IS New in the New WHO! Patrick Treseler,
Lymphoma Update: What s Likely to be New in the New WHO Blood 127:2375; 2016 Patrick Treseler, MD, PhD University of California San Francisco Lymphoma Update: What IS New in the New WHO! Patrick Treseler,
2010 Hematopoietic and Lymphoid ICD-O Codes - Alphabetical List THIS TABLE REPLACES ALL ICD-O-3 Codes
 Acute basophilic leukemia 9870/3 Acute biphenotypic leukemia [OBS] 9805/3 Acute erythroid leukemia 9840/3 Acute megakaryoblastic leukemia 9910/3 Acute monoblastic and monocytic leukemia 9891/3 Acute myeloid
Acute basophilic leukemia 9870/3 Acute biphenotypic leukemia [OBS] 9805/3 Acute erythroid leukemia 9840/3 Acute megakaryoblastic leukemia 9910/3 Acute monoblastic and monocytic leukemia 9891/3 Acute myeloid
2012 Hematopoietic and Lymphoid ICD-O Codes - Numerical List THIS TABLE REPLACES ALL ICD-O-3 Codes
 Malignant lymphoma, NOS 9590/3 Non-Hodgkin lymphoma, NOS 9591/3 B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma 9596/3 Primary
Malignant lymphoma, NOS 9590/3 Non-Hodgkin lymphoma, NOS 9591/3 B-cell lymphoma, unclassifiable, with features intermediate between diffuse large B-cell lymphoma and classical Hodgkin lymphoma 9596/3 Primary
WBCs Disorders 1. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
HIGH GRADE B-CELL LYMPHOMA DAVID NOLTE, MD (PGY-2) HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD
 HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD") HIGH GRADE B-CELL LYMPHOMA DAVID NOLTE, MD (PGY-2) HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD OUTLINE High grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements Patient presentation 2008/2016
HIGH GRADE B-CELL LYMPHOMA DAVID NOLTE, MD (PGY-2) HUSSAM AL-KATEB, PHD, FACMG DEBORAH FUCHS, MD OUTLINE High grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements Patient presentation 2008/2016
Aggressive B cell Lymphomas
 Aggressive B cell Lymphomas Raju K. Pillai City of Hope National Medical Center I have no disclosures Outline What is new in the WHO 2016 classification Insights from genomic studies Double Hit Lymphoma
Aggressive B cell Lymphomas Raju K. Pillai City of Hope National Medical Center I have no disclosures Outline What is new in the WHO 2016 classification Insights from genomic studies Double Hit Lymphoma
Pathology. #11 Acute Leukemias. Farah Banyhany. Dr. Sohaib Al- Khatib 23/2/16
 35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
7 Omar Abu Reesh. Dr. Ahmad Mansour Dr. Ahmad Mansour
 7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
7 Omar Abu Reesh Dr. Ahmad Mansour Dr. Ahmad Mansour -Leukemia: neoplastic leukocytes circulating in the peripheral bloodstream. -Lymphoma: a neoplastic process in the lymph nodes, spleen or other lymphatic
3/23/2017. Disclosure of Relevant Financial Relationships. Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?!
 Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?! Judith A. Ferry Massachusetts General Hospital Disclosure of Relevant Financial Relationships USCAP requires that all
Pitfalls in Immunohistochemistry in Hematopathology: CD20 and CD3 Can Let Me Down?! Judith A. Ferry Massachusetts General Hospital Disclosure of Relevant Financial Relationships USCAP requires that all
Hematology Unit Lab 2 Review Material
 Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Defined lymphoma entities in the current WHO classification
 Defined lymphoma entities in the current WHO classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno Bellinzona, January 29-31, 2016 Evolution of lymphoma classification Rappaport Lukes
Defined lymphoma entities in the current WHO classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno Bellinzona, January 29-31, 2016 Evolution of lymphoma classification Rappaport Lukes
Non-Hodgkin s Lymphomas Version
 NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines ) Non-Hodgkin s Lymphomas Version 2.2015 NCCN.org Continue Use of Immunophenotyping/ Genetic Testing in Differential Diagnosis of Mature B-Cell
Heme 9 Myeloid neoplasms
 Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Aggressive B-cell Lymphomas Updated WHO classification Elias Campo
 Aggressive B-cell Lymphomas Updated WHO classification Elias Campo Hospital Clinic, University of Barcelona Diffuse Large B-cell Lymphoma A Heterogeneous Category Subtypes with differing: Histology and
Aggressive B-cell Lymphomas Updated WHO classification Elias Campo Hospital Clinic, University of Barcelona Diffuse Large B-cell Lymphoma A Heterogeneous Category Subtypes with differing: Histology and
Myeloid neoplasms. Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories:
 Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
WBCs Disorders. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features and
WBCs Disorders Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features and
Combinations of morphology codes of haematological malignancies (HM) referring to the same tumour or to a potential transformation
 referring to the same tumour or to a potential transformation") Major subgroups according to the World Health Organisation (WHO) Classification Myeloproliferative neoplasms (MPN) Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB or
Major subgroups according to the World Health Organisation (WHO) Classification Myeloproliferative neoplasms (MPN) Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB or
Disclosures. Myeloproliferative Neoplasms: A Case-Based Approach. Objectives. Myeloproliferative Neoplasms. Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities
 WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities Robert W. McKenna, M.D. 1/2009 WHO Classification of Myeloid Neoplasms (4th Edition)--2008 Incorporates new information that
WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities Robert W. McKenna, M.D. 1/2009 WHO Classification of Myeloid Neoplasms (4th Edition)--2008 Incorporates new information that
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure
 Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Lymphoma/CLL 101: Know your Subtype. Dr. David Macdonald Hematologist, The Ottawa Hospital
 Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Lymphoma/CLL 101: Know your Subtype Dr. David Macdonald Hematologist, The Ottawa Hospital Function of the Lymph System Lymph Node Lymphocytes B-cells develop in the bone marrow and influence the immune
Myeloproliferative Disorders - D Savage - 9 Jan 2002
 Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
The spectrum of flow cytometry of the bone marrow
 The spectrum of flow cytometry of the bone marrow Anna Porwit Lund University Faculty of Medicine Dept. of Clinical Sciences Div. Oncology and Pathology anna.porwit@med.lu.se Disclosure of speaker s interests
The spectrum of flow cytometry of the bone marrow Anna Porwit Lund University Faculty of Medicine Dept. of Clinical Sciences Div. Oncology and Pathology anna.porwit@med.lu.se Disclosure of speaker s interests
Diffuse large B-cell lymphoma (DLBCL) is one of the
 is one of the") Practical Applications in Immunohistochemistry Evaluation of Diffuse Large B-Cell Lymphoma and Related Large B-Cell Lymphomas Dennis P. O Malley, MD; Aaron Auerbach, MD; Lawrence M. Weiss, MD Context.
Practical Applications in Immunohistochemistry Evaluation of Diffuse Large B-Cell Lymphoma and Related Large B-Cell Lymphomas Dennis P. O Malley, MD; Aaron Auerbach, MD; Lawrence M. Weiss, MD Context.
Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms. Daniel A. Arber, MD Stanford University
 Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms Daniel A. Arber, MD Stanford University What is an integrated approach? What is an integrated approach? Incorporating all diagnostic
Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms Daniel A. Arber, MD Stanford University What is an integrated approach? What is an integrated approach? Incorporating all diagnostic
Extramedullary precursor T-lymphoblastic transformation of CML at presentation
 Extramedullary precursor T-lymphoblastic transformation of CML at presentation Neerja Vajpayee, Constance Stein, Bernard Poeisz & Robert E. Hutchison Clinical History 30 year old man presented to the emergency
Extramedullary precursor T-lymphoblastic transformation of CML at presentation Neerja Vajpayee, Constance Stein, Bernard Poeisz & Robert E. Hutchison Clinical History 30 year old man presented to the emergency
Anaplastic Large Cell Lymphoma (of T cell lineage)
") Anaplastic Large Cell Lymphoma (of T cell lineage) Definition T-cell lymphoma comprised of large cells with abundant cytoplasm and pleomorphic, often horseshoe-shaped nuclei CD30+ Most express cytotoxic
Anaplastic Large Cell Lymphoma (of T cell lineage) Definition T-cell lymphoma comprised of large cells with abundant cytoplasm and pleomorphic, often horseshoe-shaped nuclei CD30+ Most express cytotoxic
High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li,
: Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li,") High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li, M.D., Ph.D. Fudan University Shanghai Cancer Center
High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li, M.D., Ph.D. Fudan University Shanghai Cancer Center
Pathology of aggressive lymphomas
 Institute of Pathology Pathology of aggressive lymphomas Leticia Quintanilla-Martinez Changes in the new 2016 WHO Aggressive B-cell lymphoid neoplasms Major changes that impact how cases should be evaludated
Institute of Pathology Pathology of aggressive lymphomas Leticia Quintanilla-Martinez Changes in the new 2016 WHO Aggressive B-cell lymphoid neoplasms Major changes that impact how cases should be evaludated
5000 International Clinical Cytometry Society: Practical Flow Cytometry in Hematopathology A Case-Based Approach
 5000 International Clinical Cytometry Society: Practical Flow Cytometry in Hematopathology A Case-Based Approach Joseph A DiGiuseppe, MD, PhD Hartford Hospital Disclosures In the past 12 months, I have
5000 International Clinical Cytometry Society: Practical Flow Cytometry in Hematopathology A Case-Based Approach Joseph A DiGiuseppe, MD, PhD Hartford Hospital Disclosures In the past 12 months, I have
Follicular Lymphoma: the WHO
 Follicular Lymphoma: the WHO and the WHERE? Yuri Fedoriw, MD Associate Professor of Pathology and Laboratory Medicine Director of Hematopathology University of North Carolina Chapel Hill, NC Disclosure
Follicular Lymphoma: the WHO and the WHERE? Yuri Fedoriw, MD Associate Professor of Pathology and Laboratory Medicine Director of Hematopathology University of North Carolina Chapel Hill, NC Disclosure
Aggressive B-cell lymphomas and gene expression profiling towards individualized therapy?
 Aggressive B-cell lymphomas and gene expression profiling towards individualized therapy? Andreas Rosenwald Institute of Pathology, University of Würzburg, Germany Barcelona, June 18, 2010 NEW WHO CLASSIFICATION
Aggressive B-cell lymphomas and gene expression profiling towards individualized therapy? Andreas Rosenwald Institute of Pathology, University of Würzburg, Germany Barcelona, June 18, 2010 NEW WHO CLASSIFICATION
Acute Myeloid Leukemia with Recurrent Cytogenetic Abnormalities
 Acute Myeloid Leukemia with Recurrent Cytogenetic Abnormalities Acute Myeloid Leukemia with recurrent cytogenetic Abnormalities -t(8;21)(q22;q22)(aml/eto) -inv(16) or t(16;16) -t(15;17) -11q23 Acute Myeloid
Acute Myeloid Leukemia with Recurrent Cytogenetic Abnormalities Acute Myeloid Leukemia with recurrent cytogenetic Abnormalities -t(8;21)(q22;q22)(aml/eto) -inv(16) or t(16;16) -t(15;17) -11q23 Acute Myeloid
Low-grade B-cell lymphoma
 Low-grade B-cell lymphoma Patho-Basic 11. September 2018 Stephan Dirnhofer Pathology Outline Definition LPL, MBL/CLL/SLL, MCL FL Subtypes & variants Diagnosis including Grading Transformation Summary Be
Low-grade B-cell lymphoma Patho-Basic 11. September 2018 Stephan Dirnhofer Pathology Outline Definition LPL, MBL/CLL/SLL, MCL FL Subtypes & variants Diagnosis including Grading Transformation Summary Be
PRECURSOR LYMHPOID NEOPLASMS. B lymphoblastic leukaemia/lymphoma T lymphoblastic leukaemia/lymphoma
 PRECURSOR LYMHPOID NEOPLASMS B lymphoblastic leukaemia/lymphoma T lymphoblastic leukaemia/lymphoma B lymphoblastic leukaemia/lymphoma Definition: B lymphoblastic leukaemia/lymphoma is a neoplasm of precursor
PRECURSOR LYMHPOID NEOPLASMS B lymphoblastic leukaemia/lymphoma T lymphoblastic leukaemia/lymphoma B lymphoblastic leukaemia/lymphoma Definition: B lymphoblastic leukaemia/lymphoma is a neoplasm of precursor
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL)
 Hodgkin lymphoma )HL)") Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Non-Hodgkin lymphomas (NHLs) Hodgkin lymphoma )HL) Lymphoid Neoplasms: 1- non-hodgkin lymphomas (NHLs) 2- Hodgkin lymphoma 3- plasma cell neoplasms Non-Hodgkin lymphomas (NHLs) Acute Lymphoblastic Leukemia/Lymphoma
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms
 & Myeloproliferative neoplasms") Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
Many of the hematolymphoid disorders are derived
 REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
REVIEW ARTICLE Practical Immunohistochemistry in Hematopathology: A Review of Useful Antibodies for Diagnosis Ji Lu, MD and Karen L. Chang, MD Abstract: This review article offers some useful panels of
9/28/2017. Follicular Lymphoma and Nodal Marginal Zone Lymphoma. Follicular Lymphoma Definition. Low-Grade B-Cell Lymphomas in WHO Classification
 and L. Jeffrey Medeiros, MD DISCLOSURES I do not have anything to disclose Low-Grade B-Cell Lymphomas in WHO Classification Lymphoma Type Frequency Follicular lymphoma 22.1 % Extranodal MALT-lymphoma 7.6
and L. Jeffrey Medeiros, MD DISCLOSURES I do not have anything to disclose Low-Grade B-Cell Lymphomas in WHO Classification Lymphoma Type Frequency Follicular lymphoma 22.1 % Extranodal MALT-lymphoma 7.6
Pathology of aggressive lymphomas
 Institute of Pathology Pathology of aggressive lymphomas Leticia Quintanilla-Martinez Changes in the new 2016 WHO Aggressive B-cell lymphoid neoplasms Major changes that impact how cases should be evaludated
Institute of Pathology Pathology of aggressive lymphomas Leticia Quintanilla-Martinez Changes in the new 2016 WHO Aggressive B-cell lymphoid neoplasms Major changes that impact how cases should be evaludated
Immunohistochemical classification of haematolymphoid tumours. Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital
 Immunohistochemical classification of haematolymphoid tumours Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital Malignant lymphoproliferative diseases What are they? Haematolymphoid
Immunohistochemical classification of haematolymphoid tumours Stephen Hamilton-Dutoit Institute of Pathology Aarhus University Hospital Malignant lymphoproliferative diseases What are they? Haematolymphoid
Lymphoma: What You Need to Know. Richard van der Jagt MD, FRCPC
 Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Lymphoma: What You Need to Know Richard van der Jagt MD, FRCPC Overview Concepts, classification, biology Epidemiology Clinical presentation Diagnosis Staging Three important types of lymphoma Conceptualizing
Update on the Classification of Aggressive B-cell Lymphomas and Hodgkin Lymphoma
 Update on the Classification of Aggressive B-cell Lymphomas and Hodgkin Lymphoma Nancy Lee Harris, M. D. Massachusetts General Hospital Harvard Medical School Aggressive B-cell Lymphomas WHO 4 th Edition
Update on the Classification of Aggressive B-cell Lymphomas and Hodgkin Lymphoma Nancy Lee Harris, M. D. Massachusetts General Hospital Harvard Medical School Aggressive B-cell Lymphomas WHO 4 th Edition
Mimics of Lymphoma in Routine Biopsies. Mixed follicular and paracortical hyperplasia. Types of Lymphoid Hyperplasia
 Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco Types of Lymphoid Hyperplasia Follicular hyperplasia (B-cells) Paracortical
Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco Types of Lymphoid Hyperplasia Follicular hyperplasia (B-cells) Paracortical
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders
 Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Primary Cutaneous CD30-Positive T-cell Lymphoproliferative Disorders Definition A spectrum of related conditions originating from transformed or activated CD30-positive T-lymphocytes May coexist in individual
Hematopathology Case Study
 Hematopathology Case Study AMP Outreach Course 2009 AMP Annual Meeting John Greg Howe Ph.D. Department of Laboratory Medicine Yale University School of Medicine November 19, 2009 HISTORY Case History An
Hematopathology Case Study AMP Outreach Course 2009 AMP Annual Meeting John Greg Howe Ph.D. Department of Laboratory Medicine Yale University School of Medicine November 19, 2009 HISTORY Case History An
The next lymphoma classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno
 Evolution of classification The next classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno The Lymphoma Forum of Excellence, Bellinzona, January 2011 Rappaport Lukes and Collins (immunophenotype)
Evolution of classification The next classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno The Lymphoma Forum of Excellence, Bellinzona, January 2011 Rappaport Lukes and Collins (immunophenotype)
Diagnostic Molecular Pathology of Lymphoid Neoplasms
 Diagnostic Molecular Pathology of Lymphoid Neoplasms (Part II) Rational use of molecular testing in lymphomas Beirut, Lebanon Friday December 2, 2011: Hematopathology Session Adam Bagg University of Pennsylvania
Diagnostic Molecular Pathology of Lymphoid Neoplasms (Part II) Rational use of molecular testing in lymphomas Beirut, Lebanon Friday December 2, 2011: Hematopathology Session Adam Bagg University of Pennsylvania
Case Presentation No. 075
 Case Presentation No. 075 Session 4. Myelodysplastic Syndrome Cristina Montalvo, MD Baylor College of Medicine Houston, Texas 2007 Workshop of Society for Hematopathology and European Association for Haematopathology
Case Presentation No. 075 Session 4. Myelodysplastic Syndrome Cristina Montalvo, MD Baylor College of Medicine Houston, Texas 2007 Workshop of Society for Hematopathology and European Association for Haematopathology
Burkitt lymphoma. Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8
 Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Heme 8 Burkitt lymphoma Sporadic Endemic in Africa associated with EBV Translocations involving MYC gene on chromosome 8 Most common is t(8;14) Believed to be the fastest growing tumor in humans!!!! Morphology
Changes to the Hematopoietic and Lymphoid Neoplasm Coding Manual
 Changes to the Hematopoietic and Lymphoid Neoplasm Coding Manual KCR 2018 SPRING TRAINING 2018 Hematopoietic Database Updates Updates were done to the Hematopoietic Database based on the WHO Hematopoietic
Changes to the Hematopoietic and Lymphoid Neoplasm Coding Manual KCR 2018 SPRING TRAINING 2018 Hematopoietic Database Updates Updates were done to the Hematopoietic Database based on the WHO Hematopoietic
Mimics of Lymphoma in Routine Biopsies. I have nothing to disclose regarding the information to be reported in this talk.
 Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco I have nothing to disclose regarding the information to be reported in this
Mimics of Lymphoma in Routine Biopsies Patrick Treseler, MD, PhD Professor of Pathology University of California San Francisco I have nothing to disclose regarding the information to be reported in this
Case #16: Diagnosis. T-Lymphoblastic lymphoma. But wait, there s more... A few weeks later the cytogenetics came back...
 Case #16: Diagnosis T-Lymphoblastic lymphoma But wait, there s more... A few weeks later the cytogenetics came back... 46,XY t(8;13)(p12;q12)[12] Image courtesy of Dr. Xinyan Lu Further Studies RT-PCR
Case #16: Diagnosis T-Lymphoblastic lymphoma But wait, there s more... A few weeks later the cytogenetics came back... 46,XY t(8;13)(p12;q12)[12] Image courtesy of Dr. Xinyan Lu Further Studies RT-PCR
Incidence. Bimodal age incidence 15-40, >55 years Childhood form (0-14) more common in developing countries M:F=1.5:1; in all subtypes except NS
 more common in developing countries M:F=1.5:1; in all subtypes except NS") Hodgkin Lymphoma Hodgkin Lymphoma 30% of all lymphomas Absolute incidence unchanged Arise in lymph node, cervical region Neoplastic tissues usually contain a small number of tumor cells Incidence Bimodal
Hodgkin Lymphoma Hodgkin Lymphoma 30% of all lymphomas Absolute incidence unchanged Arise in lymph node, cervical region Neoplastic tissues usually contain a small number of tumor cells Incidence Bimodal
Pathology of Hematopoietic and Lymphoid tissue
 Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA. April 16, 2008
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
Polycthemia Vera (Rubra)
") Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
5003 Immunohistochemistry in hematopathology, what's in, what's out, what's useful
 www.ascp.org/ascp2014 5003 Immunohistochemistry in hematopathology, what's in, what's out, what's useful Kathryn Rizzo, DO, PhD VIRGINIA COMMONWEALTH UNIVERSITY Department of Pathology School of Medicine
www.ascp.org/ascp2014 5003 Immunohistochemistry in hematopathology, what's in, what's out, what's useful Kathryn Rizzo, DO, PhD VIRGINIA COMMONWEALTH UNIVERSITY Department of Pathology School of Medicine
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms. Curtis A. Hanson, MD
 Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Blastic NK-Cell Leukemia / Lymphoma
 * * Blastic NK-Cell Leukemia / Lymphoma A Case Report Chun-Ming Lin Shu-Hui Wang Tseng-tong Kuo* Ching-Chi Chi Hsin-Chun Ho Hong-Shang Hong Blastic natural killer (NK) cell lymphoma / leukemia is a rare
* * Blastic NK-Cell Leukemia / Lymphoma A Case Report Chun-Ming Lin Shu-Hui Wang Tseng-tong Kuo* Ching-Chi Chi Hsin-Chun Ho Hong-Shang Hong Blastic natural killer (NK) cell lymphoma / leukemia is a rare
Pathology of Hematopoietic and Lymphoid tissue
 CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU
 Rex K.H. Au-Yeung Department of Pathology, HKU") Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Molecular Pathology of Lymphoma (Part 1) Rex K.H. Au-Yeung Department of Pathology, HKU Lecture outline Time 10:00 11:00 11:15 12:10 12:20 13:15 Content Introduction to lymphoma Review of lymphocyte biology
Recommended Timing for Transplant Consultation
 REFERRAL GUIDELINES Recommended Timing for Transplant Consultation Published jointly by the National Marrow Donor Program /Be The Match and the American Society for Blood and Marrow Transplantation BeTheMatchClinical.org
REFERRAL GUIDELINES Recommended Timing for Transplant Consultation Published jointly by the National Marrow Donor Program /Be The Match and the American Society for Blood and Marrow Transplantation BeTheMatchClinical.org
WHO Update to Myeloproliferative Neoplasms
 WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
Monoclonal B-cell Lymphocytosis
 Entity Centred Approach Lymphoma Classification: WHO and Beyond Clinically meaningful categories Dr Stefan Dojcinov University Hospital of Wales, Cardiff WHO UPDATE - NEW ENTITIES Early lesions lymphoma
Entity Centred Approach Lymphoma Classification: WHO and Beyond Clinically meaningful categories Dr Stefan Dojcinov University Hospital of Wales, Cardiff WHO UPDATE - NEW ENTITIES Early lesions lymphoma
Methods used to diagnose lymphomas
 Institut für Pathologie Institut für Pathologie Methods used to diagnose lymphomas Prof. Dr.Med. Leticia Quintanilla-Fend Molecular techniques NGS histology Cytology AS-PCR Sanger seq. MYC Immunohistochemistry
Institut für Pathologie Institut für Pathologie Methods used to diagnose lymphomas Prof. Dr.Med. Leticia Quintanilla-Fend Molecular techniques NGS histology Cytology AS-PCR Sanger seq. MYC Immunohistochemistry
HEMATOPATHOLOGY DIAGNOSIS & SUBTYPING. Use of IHC. Use of Polymerase Chain Reaction (PCR) Use of Flow Cytometry
 Use of Flow Cytometry") HEMATOPATHOLOGY DIAGNOSIS & SUBTYPING HEMATOPATHOLOGY DIAGNOSIS & SUBTYPING The 2008 WHO classification system for tumors of hematopoietic and lymphoid tissues specifies that various combinations of immunophenotypic
HEMATOPATHOLOGY DIAGNOSIS & SUBTYPING HEMATOPATHOLOGY DIAGNOSIS & SUBTYPING The 2008 WHO classification system for tumors of hematopoietic and lymphoid tissues specifies that various combinations of immunophenotypic
88-year-old Female with Lymphadenopathy. Faizi Ali, MD
 88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
88-year-old Female with Lymphadenopathy Faizi Ali, MD Clinical History A 88-year-old caucasian female presented to our hospital with the complaints of nausea, vomiting,diarrhea, shortness of breath and
Easy Trick to Spot Leukemia for Pediatricians
 Easy Trick to Spot Leukemia for Pediatricians Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital Most Common Pediatric Cancers Age 0-14 Leukemia 32%
Easy Trick to Spot Leukemia for Pediatricians Piya Rujkijyanont, MD Division of Hematology-Oncology Department of Pediatrics Phramongkutklao Hospital Most Common Pediatric Cancers Age 0-14 Leukemia 32%
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology. Songlin Zhang, MD, PhD LSUHSC-Shreveport
 From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
From Morphology to Molecular Pathology: A Practical Approach for Cytopathologists Part 1-Cytomorphology Songlin Zhang, MD, PhD LSUHSC-Shreveport I have no Conflict of Interest. FNA on Lymphoproliferative
Case 3. Ann T. Moriarty,MD
 Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
Case 3 Ann T. Moriarty,MD Case 3 59 year old male with asymptomatic cervical lymphadenopathy. These images are from a fine needle biopsy of a left cervical lymph node. Image 1 Papanicolaou Stained smear,100x.
Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent
 Int J Clin Exp Med 2014;7(1):307-311 www.ijcem.com /ISSN:1940-5901/IJCEM1311029 Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent Qilin Ao 2, Ying Wang 1, Sanpeng Xu 2,
Int J Clin Exp Med 2014;7(1):307-311 www.ijcem.com /ISSN:1940-5901/IJCEM1311029 Case Report A case of EBV positive diffuse large B-cell lymphoma of the adolescent Qilin Ao 2, Ying Wang 1, Sanpeng Xu 2,
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies
 Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Pearls and pitfalls in interpretation of lymphoid lesions in needle biopsies Megan S. Lim MD PhD University of Pennsylvania October 8, 2018 Objectives To understand how the trend toward less invasive lymph
Use of MYC, BCL2 and BCL6 FISH for investigations of high grade B cell lymphoma
 Use of MYC, BCL2 and BCL6 FISH for investigations of high grade B cell lymphoma Dr Anthony Bench Haematopathology and Oncology Diagnostic Service Cambrıdge Unıversıty Hospitals NHS Foundatıon Trust Cambridge
Use of MYC, BCL2 and BCL6 FISH for investigations of high grade B cell lymphoma Dr Anthony Bench Haematopathology and Oncology Diagnostic Service Cambrıdge Unıversıty Hospitals NHS Foundatıon Trust Cambridge
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD. Part 4 MYELOID NEOPLASMS
 HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
2012 by American Society of Hematology
 2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
ACCME/Disclosures 4/13/2016. Clinical History
 ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS which they or their spouse/partner
AML: WHO classification, biology and prognosis. Dimitri Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen
 AML: WHO classification, biology and prognosis Dimitri Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen Acute myeloid leukemia Clonal expansion of undifferentiated myeloid precursors Impaired
AML: WHO classification, biology and prognosis Dimitri Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen Acute myeloid leukemia Clonal expansion of undifferentiated myeloid precursors Impaired
DETERMINATION OF A LYMPHOID PROCESS
 Chapter 2 Applications of Touch Preparation Cytology to Intraoperative Consultations: Lymph Nodes and Extranodal Tissues for Evaluation of Hematolymphoid Disorders INTRODUCTION As discussed in Chap. 1,
Chapter 2 Applications of Touch Preparation Cytology to Intraoperative Consultations: Lymph Nodes and Extranodal Tissues for Evaluation of Hematolymphoid Disorders INTRODUCTION As discussed in Chap. 1,
FOLLICULARITY in LYMPHOMA
 FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
FOLLICULARITY in LYMPHOMA Reactive Follicular Hyperplasia Follicular Hyperplasia irregular follicles Follicular Hyperplasia dark and light zones Light Zone Dark Zone Follicular hyperplasia MIB1 Follicular
LYMPHOMAS an overview of some subtypes of NHLs
 One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
One of the confusing aspects of the lymphoid neoplasms concerns the use of the descriptive terms "leukemia" and "lymphoma." LYMPHOMAS an overview of some subtypes of NHLs Leukemia is used for lymphoid
Contents. vii. Preface... Acknowledgments... v xiii
 Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
Contents Preface... Acknowledgments... v xiii SECTION I 1. Introduction... 3 Knowledge-Based Diagnosis... 4 Systematic Examination of the Lymph Node... 7 Cell Type Identification... 9 Cell Size and Cellularity...
Pathology #07. Hussein Al-Sa di. Dr. Sohaib Al-Khatib. Mature B-Cell Neoplasm. 0 P a g e
 Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
Pathology #07 Mature B-Cell Neoplasm Hussein Al-Sa di Dr. Sohaib Al-Khatib 0 P a g e Thursday 18/2/2016 Our lecture today (with the next 2 lectures) will be about lymphoid tumors This is a little bit long
HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO
 HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO HODGKIN LYMPHOMA CLASSIFICATION Lukes & Butler Rye WHO-2016 Linphocytic and/or histiocytic Nodular & diffuse Nodular Sclerosis Lymphocyte
HODGKIN LYMPHOMA DR. ALEJANDRA ZARATE OSORNO HOSPITAL ESPAÑOL DE MEXICO HODGKIN LYMPHOMA CLASSIFICATION Lukes & Butler Rye WHO-2016 Linphocytic and/or histiocytic Nodular & diffuse Nodular Sclerosis Lymphocyte