Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms. Kaaren Reichard Mayo Clinic Rochester
|
|
|
- Tobias Charles
- 5 years ago
- Views:
Transcription
1 Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms Kaaren Reichard Mayo Clinic Rochester
2 Nothing to disclose Conflict of Interest
3 Learning Objectives Present the criteria required to establish a diagnosis of MDS and MPN according to the 2016 updated WHO Classification Review the revised 2016 WHO categories of MDS and MPN Discuss changes in classification since the 2008 WHO Highlight new genetic information
4 Myeloid neoplasm classification Myelodysplastic syndromes Myeloproliferative neoplasms Mastocytosis Myeloid/lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB, FGFR1 and PCM1-JAK2 Myelodysplastic/myeloproliferative neoplasms Acute myeloid leukemia and related entities Myeloid neoplasms with germline predisposition
5 Myeloid Neoplasms: Major Subgroups and Discriminating Features Group PB counts BM cellularity % BM blasts Hematopoiesis Maturation Morphology Organomegaly MDS Cytopenias Usually increased Ineffective Present Normal or increased Dysplasia Uncommon MPN Cytoses Usually increased Effective Present Usually normal Normal except megakary ocytes Common AML Variable WBC Usually increased Ineffective or effective Usually minimal >20%; exceptions Variable Uncommon MDS/ MPN WBC usually increased Increased Varies by lineage Present Normal or slightly increased Usually dysplasia in one cell lineage Common MLNE Eosinophilia Increased Effective Present Usually normal Normal Common
6 Myelodysplastic syndromes (MDS) Clonal hematopoietic stem cell neoplasms with ineffective hematopoiesis and intact maturation Peripheral blood cytopenias Morphologic dysplasia of hematopoietic elements Varying propensity to develop maturation arrest in hematopoietic cells, with accumulation of blasts and progression to AML Cutoff of 20% blasts in bone marrow or peripheral blood distinguishes MDS from AML
7 Myelodysplastic syndromes (MDS) Clonal hematopoietic stem cell neoplasm Sustained cytopenias: (hemoglobin < 10g/dl, neutrophil count <1.8 x 109/L and platelet count <100 x 109/L) Intact maturation of hematopoietic lineages with 10% dysplastic cells in at least one lineage, and increased intramedullary cell death (apoptosis)(ineffective hematopoiesis) Variable blast percentage but < 20% in blood and bone marrow Increased risk of transformation to acute myeloid leukemia
8 Biologic Spectrum of MDS Indolent low-grade subtypes Low blast counts Typically low risk of progression to AML Morbidity and mortality due to cytopenias and/or complications of infection, bleeding, transfusion Aggressive subtypes Higher blast counts, genetic instability Often rapidly progress to AML



9 Dysplasia assessment WHO threshold: 10% of cells in any lineage must manifest dysplastic morphology to call that lineage dysplastic May be interobserver variability Dysplasia is not specific for MDS May observe dysplasia in bone marrow of normal volunteers and even more frequently in patients with non-neoplastic cytopenias
10 Beyond morphology for MDS diagnosis Flow cytometry Abnormal flow cytometry patterns predict MDS with good sensitivity and specificity WHO 2016 and ELN guidelines do not permit a diagnosis of MDS solely based on flow cytometry Considered supportive of a diagnosis More data needed on findings in reactive conditions Flow is important to evaluate for lymphomas that can present with cytopenia mimicking MDS
11 Beyond morphology for MDS diagnosis Genetic abnormalities Karyotype abnormalities ~50% of MDS cases have a normal karyotype Sub-karyotypic genetic alterations Microdeletions, other small imbalances Gene mutations (detected mainly in the clinical realm by next generations sequencing assays)
12 MDS-defining cytogenetic abnormalities Unbalanced Primary MDS Therapy-related MDS -7 or del(7q) 10% 50% del(5q) to t(5q) 10% 40% i(17q) or t(17p) 3-5% -13 or del(13q) 3% del(11q) 3% del(12p) or t(12p) 3% del(9q) 1-2% idic(x)(q13) 1-2% Balanced t(11;16)(q23;p13.3) 3% t(3;21)(q26.2;q22.1) 2% t(1;3)(p36.3;q21.2) 1% t(2;11)(p21;q23) 1% inv(3)(q21q26.2) 1% t(6;9)(p23;q34) 1% +8, -Y, and del(20q) are common in MDS, but can occur in non-neoplastic conditions and are not MDS-defining
13 Somatic mutations in MDS Increasing availability of sequencing has enabled significant knowledge to be gained in MDS patients Great heterogeneity in mutational landscape Recurrent genetic alterations in multiple cellular pathways: transcription factors, tumor suppressors, epigenetic modifiers, splicing machinery, etc.
14 Somatic mutations in MDS* Genetic mutation Incidence Comments RNA splicing SF3B % Strong assoc. w/rs and LR-MDS, OS, SRSF % OS prognosis U2AF1 5-10% risk for AML DNA methylation TET % DNMT3A 10% Assoc. w/ OS IDH1/IDH2 ~5% Assoc. w/ MLD and Papaemmanuil E Blood. 2013;122:3616 blasts *(not all inclusive)
15 Somatic mutations in MDS* Genetic mutation Incidence Comments Chromatin modification ASXL % OS Transcription RUNX1 10% assoc. w/ MLD and blasts NPM1 <5% DNA repair TP53 ~10% in HG-MDS; OS *(not all inclusive)
16 Can mutations = diagnosis of MDS? A subset of healthy older individuals harbor MDS-type mutations in hematopoietic cells Top genes include: DNMT3A, TET2, ASXL1, TP53, JAK2, SF3B1 Associated with increased risk of subsequent hematologic malignancy but many patients never develop MDS even after years of follow-up Designated as Clonal Hematopoiesis of Indeterminate Potential (CHIP) in the absence of cytopenias or Clonal Cytopenia of Undetermined Significance (CCUS) in the presence of cytopenias CHIP CCUS MDS Clonality Dysplasia Cytopenias Jaiswal S et al. NEJM 2014;371:2488, Genovese G et al. NEJM 2014;371:2477, Xie M et al. Nature Med 2014;20:1472; Steensma D et al. Blood 2015;126:9
17 CHIP Appears to be a precursor state to MDS Analogous to the relationship of MGUS to myeloma and monoclonal B-lymphocytosis to CLL Most patients with CHIP do not develop MDS CHIP phenomenon precludes the current use of mutations in isolation to diagnose MDS Specific mutation patterns and high mutant allele frequency may confer higher risk of MDS Mutant allele fraction 10% Spliceosome gene mutation TET2, DNMT3A or ASXL1 mutation with at least one other mutation Malcovati L et al. Blood 2017;129:3371
18 WHO 2016 MDS Classification MDS with single lineage dysplasia MDS with multilineage dysplasia MDS with ring sideroblasts MDS-RS with single lineage dysplasia MDS-RS with multilineage dysplasia MDS with isolated del(5q) MDS, unclassifiable MDS with excess blasts Refractory cytopenia of childhood (RCC)(provisional)
19 Updates in MDS Classification Molecular testing for SF3B1 mutations useful in cases with ring sideroblasts One additional cytogenetic abnormality allowed for MDS with isolated del 5q Molecular testing for TP53 mutations useful for prognosis Cases formerly fulfilling criteria for AEL, myeloid/erythroid will often become MDS-EB
20 MDS with ring sideroblasts (MDS-RS) Now includes single lineage and multilineage dysplasia categories Usually requires >15% ring sideroblasts; however the diagnosis can be made with >5% in the presence of SF3B1 mutation Secondary causes of ring sideroblasts must be excluded
21 MDS with ring sideroblasts; Strong association of MDS-RS with SF3B1 mutation Seen in ~70% of MDS- RS cases Probable early event in disease development SF3B1 is a spliceosome gene Favorable clinical outcome SF3B1 association Cumulative probability of survival Time in months Malcovati L, et al. SF3B1 mutation identifies a distinct subset of myelodysplastic syndrome withring sideroblasts. Blood Jul 9;126(2):
 The presence of a TP53 mutation is associated with an inferior response in patients treated with")
22 MDS with isolated del(5q) Updates No adverse effect on clinical outcome with one additional cytogenetic abnormality except -7 and del(7q) The presence of a TP53 mutation is associated with an inferior response in patients treated with lenalidomide
23 MDS with isolated del(5q): Key tips Diagnosis as MDS with isolated del(5q) even in the presence of a single additional cytogenetic abnormality (except -7 and del(7q) Testing for TP53 mutation is recommended in these patients
24 Change in blast counting in 2016 WHO Blasts in bone marrow are counted as % of total cells, not as % of nonerythroid cells Change from WHO 2008 Previously blast %, with >50% erythroid precursors, calculated out of the nonerythroid cells Patients previously diagnosed as acute erythroid leukemia (AEL) may not require intensive chemotherapy Overall survival AEL MDS-erythroid MDS-typical Months Wang Sa et al. Mod Pathol. 2016;29:1221
25 Effect of change in blast counting? Myeloid neoplasms with 50% erythroids but with myeloid blasts <20% of all cells are now classified as MDS. Many cases previously diagnosed as AEL are no classified as MDS-EB. Pure erythroid leukemia remains as an AML subtype (AML, NOS) Malignant proliferation of proerythroblasts
26 What testing should be performed in the bone marrow workup of MDS? Peripheral Blood CBC Cytologic review with differential count (% blasts) Bone marrow aspirate Cytologic review with differential count (% blasts) % dysplasia and lineage(s) affected Iron stain
27 What testing should be performed in the bone marrow workup of MDS? Bone marrow core biopsy Cytologic review/assess concordance with aspirate findings Flow cytometry may be helpful but not required Flow blast % should not replace morphologic % Immunohistochemistry for blasts Bone marrow aspirate % is the gold standard Exceptions: aspirate is suboptimal, morpholgoic discordance Caveat: not all blasts are CD34 positive
28 What genetic testing should be performed in the bone marrow workup of MDS? Cytogenetics required on all cases Detect del(5q), complex, other FISH testing generally not indicated if adequate karyotype (20 metaphases) SF3B1 mutation MDS-RS still defined by iron stain, but mutation analysis allows diagnosis if only a small number of ring sideroblasts are present TP53 mutation in del(5q) Molecular testing (NGS) has utility
29 Myeloproliferative neoplasms Clonal hematopoietic stem cell disorders Characterized by effective hematopoiesis and proliferation of one or more of the erythroid, granulocytic or megakaryocytic lineages Variable blast percentage but < 20% in blood and bone marrow Often organomegaly Variable propensity to develop fibrosis and AML
30 WHO 2016 Classification of MPNs* Chronic myeloid leukemia, BCR-ABL1-positive Chronic neutrophilic leukemia Polycythemia vera Primary myelofibrosis Essential thrombocythemia Chronic eosinophilic leukemia, NOS Myeloproliferative neoplasm, unclassifiable Mastocytosis is now its own category Arber DA, Orazi A, Hasserjian RP et al. The 2016 revision to the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia. Blood. 2016

31 Chronic myeloid leukemia, BCR-ABL1 positive: Updates Name change from WHO 4 th edition (2008) myeloid New definition of lymphoid blast crisis Any lymphoblast(s) in the PB raise concern for blast crisis Cases with >5% lymphoblasts in the BM should be diagnosed as blast crisis Resistance to TKI treatment is included in the definition of disease progression Lymphoid blast phase
(q34.")
, BCR-ABL1 Targeted therapy against tyrosine kinase")
32 Chronic myeloid leukemia, Most often diagnosed in chronic phase Hallmark genetic abnormality: t(9;22)(q34.1;q11.2), BCR-ABL1 Targeted therapy against tyrosine kinase (ABL) BCR-ABL1 positive Typical chronic phase appearance
33 Chronic myeloid leukemia, BCR-ABL1 positive Disease monitoring Quantitative BCR-ABL1 transcript levels Goal: complete cytogenetic remission by 12 months Goal: major molecular remission by months (3 log reduction; <0.1%)

34 Chronic myeloid leukemia, Disease progression Evidence of morphologic evolution Evidence of laboratory evolution Evidence of genetic evolution Development of resistance to TKI therapy Mutation testing BCR-ABL1 positive
35 CML, accelerated phase Any one or more of the following hematologic/cytogenetic criteria or response-to-tki criteria: Persistent or increasing WBC (>10 X 10 9 /L), unresponsive to therapy Persistent or increasing splenomegaly, unresponsive to therapy Persistent thrombocytosis (>1000 X 10 9 /L), unresponsive to therapy Persistent thrombocytopenia (<100 X 109/ L) unrelated to therapy 20% or more basophils in the PB 10-19% blasts*in the PB and/or BM Additional clonal chromosomal abnormalities in Ph+ cells at diagnosis that include "major route" abnormalities (second Ph, trisomy 8, isochromosome 17q, trisomy 19), complex karyotype, or abnormalities of 3q26.2 Any new clonal chromosomal abnormality in Ph+ cells that occurs during therapy "Provisional" Response-to-TKI Criteria Hematologic resistance to the first TKI (or failure to achieve a complete hematologic response**to the first TKI) or Any hematological, cytogenetic or molecular indications of resistance to two sequential TKIs or Occurrence of two or more mutations in BCR-ABL1 during TKI therapy Large clusters or sheets of small, abnormal megakaryocytes, associated with marked reticulin or collagen fibrosis in biopsy specimens may be considered as presumptive evidence of AP, although these findings are usually associated with one or more of the criteria listed above. *The finding of bona fide lymphoblasts in the blood or marrow, even if less than 10%, should prompt concern that lymphoblastic transformation may be imminent and warrants further clinical and genetic investigation; 20% or more blasts in blood or bone marrow, or an infiltrative proliferation of blasts in an extramedullary site is CML, blast phase. **Complete hematologic response: WBC <10x109/L, Platelet count <450 x 10 9 /L, no immature granulocytes in the differential, and spleen nonpalpable.
36 Chronic neutrophilic leukemia: Updates The CSF3R mutation is strongly associated with chronic neutrophilic leukemia Membrane proximal mutation: T615A, T618I Truncating mutation CSF3R is often co-mutated (SETBP1, ASXL1) Maxson, New Engl J Med, 2013 Lasho TL, Leukemia, 2014 Tefferi, Curr Opin Hematol Elliott MA, Am J Hematol. 2015
 constitute - < 10% of the white blood cells Myeloblasts rarely observed Monocyte count < 1 x 10 9 /L No dysgranulopoiesis Peripheral blood")
37 Chronic neutrophilic leukemia Peripheral blood white blood cell count >25 x 10 9 /L Segmented neutrophils plus banded neutrophils constitute >80% of the white blood cells Neutrophil precursors (promyelocytes, myelocytes, and metamyelocytes) constitute - < 10% of the white blood cells Myeloblasts rarely observed Monocyte count < 1 x 10 9 /L No dysgranulopoiesis Peripheral blood Neutrophilia; Minimal left shift; May see toxic changes; No dysplasia

38 Chronic neutrophilic leukemia Hypercellular bone marrow Neutrophil granulocytes increased in percentage and number Neutrophil maturation appears normal Myeloblasts constitute <5% of the nucleated cells
39 Chronic neutrophilic leukemia Does not satisfy WHO criteria for BCR-ABL 1-positive chronic myeloid leukemia, polycythaemia vera, essential thrombocythaemia, or primary myelofibrosis No rearrangement of PDGFRA, PDGFRB, or FGFR1, or PCM1-JAK2 fusion CSF3R T6181 or another activating CSF3R mutation OR Persistent neutrophilia (>3 months), splenomegaly, and no identifiable cause of reactive neutrophilia including absence of a plasma cell neoplasm or, if a plasma cell neoplasm is present, demonstration of clonality of myeloid cells by cytogenetic or molecular studies
40 Exemplary case


41 CNL versus acml CNL Neutrophilia lacking significant left shift or granulocytic dysplasia Atypical CML Neutrophilia with left shift and significant granulocytic dysplasia Majority CSFR3 mutation <10% CSFR3 mutation
42 New data incorporated into the WHO 2016 classification of the classic BCR- ABL1 negative MPNs: PV, ET, PMF The discovery of novel molecular findings in particular the CALR mutation Revise major and minor diagnostic criteria To improve diagnosis To enable discrimination amongst the various early disease presentations (PV) To provide standardized morphologic criteria of MPNs
43 ET, PV, PMF: Distinct diseases with different natural history ET Survival (%) PMF PV Years Tefferi A et al. Blood. 2014;124:
44 Mutations and MPN Subtypes JAK2 >95% of PV have a JAK2 V617F mutation (exon 14), remaining harbor exon 12 mutation 50-60% of PMF and ET have JAK2 V617F mutation CALR 20-30% of PMF and ET have CALR exon 9 mutations MPL 5-10% of PMF and ET have MPL exon 10 mutation Remaining cases are noted as triple-negative
45 Survival ET: Survival is the longest for triple-negative and shortest for MPL-mutated patients. Median survival: 19 years for JAK2 and 20 years for CALR-mutated cases PMF: Triple negative median survival 2.3 years; CALR mutated 15.9 years PV: Median survival 13.7 years Tefferi A et al. Blood 2014;124:



46 Comparative BM features PV ET PMF Hypercellular with panmyelosis with a spectrum of megakaryocyte size Normocellular with giant, hyper-lobulated megakaryocytes Hypercellular with ranulocytic hyperplasia with significant megakaryocyte atypia

47 Value of Megakaryocytes CML 60b09 58b10 PV PMF ET 60b29:CSP a25
48 Criteria for Polycythemia Vera* Major Elevated hemoglobin concentration(> 16.5 g/dl in men;> 16.0 g/dl in women) or Elevated hematocrit (> 49% in men; > 48% in women) or Increased red blood cell mass (> 25% above mean normal predicted value) Bone marrow biopsy showing age-adjusted hypercellularity with trilineage growth (panmyelosis), including prominent erythroid, granulocytic, and megakaryocytic proliferation with pleomorphic, mature megakaryocytes (size differences) Presence of JAK2 V617F or JAK2 exon 12 mutation Minor Subnormal serum erythropoietin level *The diagnosis requires either all 3 major or the first 2 major and the minor criterion.


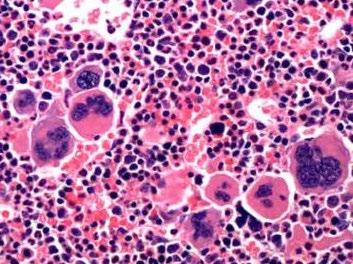
49 MPN: Polycythemia Vera BM: Spectrum megakaryocytes, panmyelosis; Bld: erythrocytosis, low serum erythropoietin level
50 Criteria for PMF, prefibrotic/early stage (All major + 1 minor criteria)* Major Atypical meg hyperplasia without fibrosis, with increased cellularity, granulocytic proliferation, and often decreased erythropoiesis Does not meet criteria for PV, CML, MDS or other myeloid neoplasm JAK2, MPL, or CALR mutation or, presence of another clonal marker, or absence of minor reactive BM reticulin fibrosis Minor Palpable splenomegaly Leukocytosis 11 x 10 9 /L Anemia not attributed to a comorbid condition Increase in serum LDH above reference range *For a diagnosis of overt phase PMF: presence of either reticulin and/or collagen fibrosis grades 2 or 3; Leukoerythroblastosis represents one more minor criterion


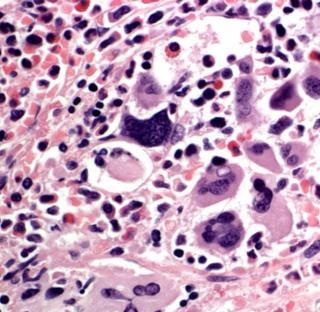
51 MPN: Primary Myelofibrosis BM: pleomorphic megakaryocytes; Bld: LER
52 Criteria for Essential Thrombocythemia Major Minor 1. Platelet count > 450 x 10 9 /L 2. Bone marrow biopsy showing proliferation mainly of the megakaryocytic lineage, with increased numbers of enlarged, mature megakaryocytes with hyperlobulated nuclei; no significant increase or left shift in neutrophil granulopoiesis or erythropoiesis; very rarely MF-1 reticulin fibrosis 3. WHO criteria for BCR-ABL1 positive chronic myeloid leukemia, polycytaemia vera, primary myelofibrosis, or other myeloid neoplasms are not met 4. JAK2, CALR, or MPL mutation Presence of a clonal marker or Absence of evidence of reactive thrombocytosis The diagnosis of essential thrombocythaemia requires that either all major criteria or the first 3 major criteria plus the minor criterion are met.


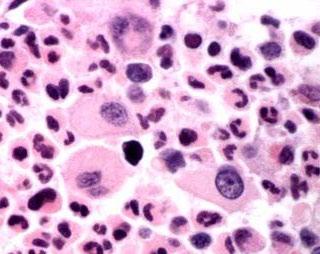
53 MPN: Essential Thrombocythemia 1.7 million plts 59a36 BM: hyperlobulated megas; Bld: plts
54 Key take-away points: MDS Molecular testing for SF3B1 mutations useful in cases with ring sideroblasts Threshold lowered to 5% rings if SF3B1 positive One additional cytogenetic abnormality allowed for MDS with isolated del 5q Cannot be -7, del(7q) or MDS-related abnormality Cases formerly fulfilling criteria for AEL, myeloid/erythroid will often become MDS-EB Alert clinician to monitor carefully for progression to overt AML Test for NPM1 and MLL mutations; if positive suggest evolving AML Molecular testing for TP53 mutations useful for prognosis
55 Key take-away points: MPN Inclusion of novel molecular findings in addition to JAK2 and MPL mutations; in particular the CALR mutation provides proof of clonality, and has diagnostic and prognostic importance CSF3R mutation and its strong association with CNL PV was likely under-diagnosed using the previous WHO 2008 hemoglobin/hematocrit cutoffs; New cut-offs and BM morphology improve diagnosing early PV Only one minor criterion to diagnose pre-pmf Various minor refinements
56 Questions?
WHO Update to Myeloproliferative Neoplasms
 WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms (MPN and MDS/MPN) Attilio Orazi, MD, FRCPath Weill Cornell Medical College/ NY Presbyterian Hospital, New York, NY USA EAHP EDUCATIONAL SESSION: Updated WHO classification
Myeloproliferative Neoplasms (MPN and MDS/MPN) Attilio Orazi, MD, FRCPath Weill Cornell Medical College/ NY Presbyterian Hospital, New York, NY USA EAHP EDUCATIONAL SESSION: Updated WHO classification
Myelodysplastic syndromes
 Myelodysplastic syndromes Robert P Hasserjian Massachusetts General Hospital, Boston, MA Disclosure of Relevant Financial Relationships Dr. Hasserjian declares he has no conflict(s) of interest to disclose.
Myelodysplastic syndromes Robert P Hasserjian Massachusetts General Hospital, Boston, MA Disclosure of Relevant Financial Relationships Dr. Hasserjian declares he has no conflict(s) of interest to disclose.
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms
 & Myeloproliferative neoplasms") Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms. Curtis A. Hanson, MD
 Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Case Presentation. Attilio Orazi, MD
 Case Presentation Attilio Orazi, MD Weill Cornell Medical College/ NYP Hospital Department of Pathology and Laboratory Medicine New York, NY United States History 60 year old man presented with anemia
Case Presentation Attilio Orazi, MD Weill Cornell Medical College/ NYP Hospital Department of Pathology and Laboratory Medicine New York, NY United States History 60 year old man presented with anemia
Disclosures. Myeloproliferative Neoplasms: A Case-Based Approach. Objectives. Myeloproliferative Neoplasms. Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Chronic Myelomonocytic Leukemia with molecular abnormalities SH
 Chronic Myelomonocytic Leukemia with molecular abnormalities SH2017-0351 Madhu P. Menon MD,PhD, Juan Gomez MD, Kedar V. Inamdar MD,PhD and Kristin Karner MD Madhu P Menon, MD, PhD Henry Ford Hospital Patient
Chronic Myelomonocytic Leukemia with molecular abnormalities SH2017-0351 Madhu P. Menon MD,PhD, Juan Gomez MD, Kedar V. Inamdar MD,PhD and Kristin Karner MD Madhu P Menon, MD, PhD Henry Ford Hospital Patient
Heme 9 Myeloid neoplasms
 Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
SH A CASE OF PERSISTANT NEUTROPHILIA: BCR-ABL
 SH2017-0124 A CASE OF PERSISTANT NEUTROPHILIA: BCR-ABL NEGATIVE John R Goodlad 1, Pedro Martin-Cabrera 2, Catherine Cargo 2 1. Department of Pathology, NHS Greater Glasgow & Clyde, QEUH, Glasgow 2. Haematological
SH2017-0124 A CASE OF PERSISTANT NEUTROPHILIA: BCR-ABL NEGATIVE John R Goodlad 1, Pedro Martin-Cabrera 2, Catherine Cargo 2 1. Department of Pathology, NHS Greater Glasgow & Clyde, QEUH, Glasgow 2. Haematological
Myelodysplastic/Myeloproliferative Neoplasms (MDS/MPN) Updated
 Updated") Myelodysplastic/Myeloproliferative Neoplasms (MDS/MPN) Updated Attilio Orazi, MD, FRCPath. (Engl.) Professor of Pathology and Laboratory Medicine Weill Cornell Medical College/NYP Hospital New York, NY
Myelodysplastic/Myeloproliferative Neoplasms (MDS/MPN) Updated Attilio Orazi, MD, FRCPath. (Engl.) Professor of Pathology and Laboratory Medicine Weill Cornell Medical College/NYP Hospital New York, NY
Disclosures for Ayalew Tefferi
 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosure BCR/ABL1-Negative Classical Myeloproliferative Neoplasms
 Disclosure BCR/ABL1-Negative Classical Myeloproliferative Neoplasms Sonam Prakash declares affiliation with Incyte Corporation: Advisor for Hematopathology Publications Steering Committee Sonam Prakash,
Disclosure BCR/ABL1-Negative Classical Myeloproliferative Neoplasms Sonam Prakash declares affiliation with Incyte Corporation: Advisor for Hematopathology Publications Steering Committee Sonam Prakash,
MDS/MPN MPN MDS. Discolosures. Advances in the Diagnosis of Myeloproliferative Neoplasms. Myeloproliferative neoplasms
 Discolosures Advances in the Diagnosis of Myeloproliferative Neoplasms Consulting income from Promedior, Inc. Robert P Hasserjian, MD Associate Professor Massachusetts General Hospital and Harvard Medical
Discolosures Advances in the Diagnosis of Myeloproliferative Neoplasms Consulting income from Promedior, Inc. Robert P Hasserjian, MD Associate Professor Massachusetts General Hospital and Harvard Medical
Approaching myeloid neoplasms: diagnostic algorithms
 Approaching myeloid neoplasms: diagnostic algorithms Alexandar Tzankov Histopathology Pathology Content Integration of clinical and laboratory data Bone marrow evaluation approaching Myeloproliferative
Approaching myeloid neoplasms: diagnostic algorithms Alexandar Tzankov Histopathology Pathology Content Integration of clinical and laboratory data Bone marrow evaluation approaching Myeloproliferative
Myelodysplastic syndromes: revised WHO classification and distinction from non-neoplastic conditions
 Myelodysplastic syndromes: revised WHO classification and distinction from non-neoplastic conditions Robert P Hasserjian, MD Associate Professor Massachusetts General Hospital and Harvard Medical School
Myelodysplastic syndromes: revised WHO classification and distinction from non-neoplastic conditions Robert P Hasserjian, MD Associate Professor Massachusetts General Hospital and Harvard Medical School
Chronic Idiopathic Myelofibrosis (CIMF)
") Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD. Part 4 MYELOID NEOPLASMS
 HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
Pathology. #11 Acute Leukemias. Farah Banyhany. Dr. Sohaib Al- Khatib 23/2/16
 35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms. Daniel A. Arber, MD Stanford University
 Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms Daniel A. Arber, MD Stanford University What is an integrated approach? What is an integrated approach? Incorporating all diagnostic
Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms Daniel A. Arber, MD Stanford University What is an integrated approach? What is an integrated approach? Incorporating all diagnostic
Myeloid neoplasms. Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories:
 Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Juvenile Myelomonocytic Leukemia (JMML)
") Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
Myelodysplastic Syndromes Myeloproliferative Disorders
 Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
Hematology Unit Lab 2 Review Material
 Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
MPN What's new in the morphological classification, grading of fibrosis and the impact of novel drugs
 MPN What's new in the morphological classification, grading of fibrosis and the impact of novel drugs Hans Michael Kvasnicka University of Frankfurt, Germany hans-michael.kvasnicka@kgu.de Disclosure of
MPN What's new in the morphological classification, grading of fibrosis and the impact of novel drugs Hans Michael Kvasnicka University of Frankfurt, Germany hans-michael.kvasnicka@kgu.de Disclosure of
Bone marrow histopathology in Ph - CMPDs. - the new WHO classification - Juergen Thiele Cologne, Germany
 Bone marrow histopathology in Ph - CMPDs - the new WHO classification - Juergen Thiele Cologne, Germany Current issues in MPNs concerning morphology 1.Prodromal stages of disease 2.Impact of histopathology
Bone marrow histopathology in Ph - CMPDs - the new WHO classification - Juergen Thiele Cologne, Germany Current issues in MPNs concerning morphology 1.Prodromal stages of disease 2.Impact of histopathology
WHO 2016/17 update on Myeloproliferative Neoplasms. Anna Ruskova Auckland City Hospital New Zealand
 WHO 2016/17 update on Myeloproliferative Neoplasms Anna Ruskova Auckland City Hospital New Zealand BLOOD, 19 MAY 2016 x VOLUME 127, NUMBER 20 2 2016/17 Classification of Myeloproliferative Neoplasms Chronic
WHO 2016/17 update on Myeloproliferative Neoplasms Anna Ruskova Auckland City Hospital New Zealand BLOOD, 19 MAY 2016 x VOLUME 127, NUMBER 20 2 2016/17 Classification of Myeloproliferative Neoplasms Chronic
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure
 Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Polycthemia Vera (Rubra)
") Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
Update on the WHO Classification of Acute Myeloid Leukemia. Kaaren K. Reichard, MD Mayo Clinic Rochester
 Update on the WHO Classification of Acute Myeloid Leukemia Kaaren K. Reichard, MD Mayo Clinic Rochester reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Objectives Present a practical
Update on the WHO Classification of Acute Myeloid Leukemia Kaaren K. Reichard, MD Mayo Clinic Rochester reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Objectives Present a practical
Disclosures. I do not have anything to disclose. Shared Features of MPNs. Overview. Diagnosis and Molecular Monitoring in the
 Myeloproliferative Neoplasms: Diagnosis and Molecular Monitoring in the Target Therapy Era C. Cameron Yin, M.D., Ph.D. Department of Hematopathology UT MD Anderson Cancer Center Disclosures I do not have
Myeloproliferative Neoplasms: Diagnosis and Molecular Monitoring in the Target Therapy Era C. Cameron Yin, M.D., Ph.D. Department of Hematopathology UT MD Anderson Cancer Center Disclosures I do not have
MYELOPROLIFERATIVE NEOPLASMS
 9 : 2 MYELOPROLIFERATIVE NEOPLASMS Introduction William Dameshek in 1951 introduced the term Myeloproliferative disorders (MPD). This included polycythemia vera (PV), essential thrombocythemia (ET), primary
9 : 2 MYELOPROLIFERATIVE NEOPLASMS Introduction William Dameshek in 1951 introduced the term Myeloproliferative disorders (MPD). This included polycythemia vera (PV), essential thrombocythemia (ET), primary
Welcome to Master Class for Oncologists. Session 3: 9:15 AM - 10:00 AM
 Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
Myeloproliferative Neoplasms: Diagnosis and Molecular Monitoring in the Era of Target Therapy
 Myeloproliferative Neoplasms: Diagnosis and Molecular Monitoring in the Era of Target Therapy C. Cameron Yin, M.D., Ph.D. Department of Hematopathology UT MD Anderson Cancer Center Disclosures I do not
Myeloproliferative Neoplasms: Diagnosis and Molecular Monitoring in the Era of Target Therapy C. Cameron Yin, M.D., Ph.D. Department of Hematopathology UT MD Anderson Cancer Center Disclosures I do not
WHO Classification 7/2/2009
 Least Malignant Myeloproliferative Disorders Myelodysplastic Syndromes Most Malignant Acute Leukemia Classifying Hematopoietic Disorders French-American-British (FAB) World Health Organization (WHO) Thanks
Least Malignant Myeloproliferative Disorders Myelodysplastic Syndromes Most Malignant Acute Leukemia Classifying Hematopoietic Disorders French-American-British (FAB) World Health Organization (WHO) Thanks
APPROACH TO MYELODYSPLASTIC SYNDROMES IN THE ERA OF PRECISION MEDICINE
 APPROACH TO MYELODYSPLASTIC SYNDROMES IN THE ERA OF PRECISION MEDICINE Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics Department of Hematopathology The University
APPROACH TO MYELODYSPLASTIC SYNDROMES IN THE ERA OF PRECISION MEDICINE Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics Department of Hematopathology The University
Disclosures for Ayalew Tefferi
 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
74y old Female with chronic elevation of Platelet count. August 18, 2005 Faizi Ali, MD Hematopathology Fellow
 74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities
 WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities Robert W. McKenna, M.D. 1/2009 WHO Classification of Myeloid Neoplasms (4th Edition)--2008 Incorporates new information that
WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities Robert W. McKenna, M.D. 1/2009 WHO Classification of Myeloid Neoplasms (4th Edition)--2008 Incorporates new information that
Conditions that mimic neoplasia in the bone marrow. Kaaren K. Reichard Mayo Clinic Rochester
 Conditions that mimic neoplasia in the bone marrow Kaaren K. Reichard Mayo Clinic Rochester reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Multiple conditions in
Conditions that mimic neoplasia in the bone marrow Kaaren K. Reichard Mayo Clinic Rochester reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Multiple conditions in
2013 AAIM Pathology Workshop
 2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls
 Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
Disclosures for Ayalew Tefferi
 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
New WHO Classification of Myeloproliferative Neoplasms
 New WHO Classification of Myeloproliferative Neoplasms Hans Michael Kvasnicka Senckenberg Institute of Pathology, University of Frankfurt, Germany hans-michael.kvasnicka@kgu.de Principles and rationale
New WHO Classification of Myeloproliferative Neoplasms Hans Michael Kvasnicka Senckenberg Institute of Pathology, University of Frankfurt, Germany hans-michael.kvasnicka@kgu.de Principles and rationale
Myelodysplastic syndromes and the new WHO 2016 classification
 Myelodysplastic syndromes and the new WHO 2016 classification 32nd General Annual Meeting of the Belgian Hematology Society 10-11 February 2017 Gregor Verhoef, Departement of Hematology, University Hospital
Myelodysplastic syndromes and the new WHO 2016 classification 32nd General Annual Meeting of the Belgian Hematology Society 10-11 February 2017 Gregor Verhoef, Departement of Hematology, University Hospital
Template for Reporting Results of Biomarker Testing for Myeloproliferative Neoplasms
 Template for Reporting Results of Biomarker Testing for Myeloproliferative Neoplasms Version: MPNBiomarkers 1.0.0.2 Protocol Posting Date: June 2017 This biomarker template is NOT required for accreditation
Template for Reporting Results of Biomarker Testing for Myeloproliferative Neoplasms Version: MPNBiomarkers 1.0.0.2 Protocol Posting Date: June 2017 This biomarker template is NOT required for accreditation
Case #16: Diagnosis. T-Lymphoblastic lymphoma. But wait, there s more... A few weeks later the cytogenetics came back...
 Case #16: Diagnosis T-Lymphoblastic lymphoma But wait, there s more... A few weeks later the cytogenetics came back... 46,XY t(8;13)(p12;q12)[12] Image courtesy of Dr. Xinyan Lu Further Studies RT-PCR
Case #16: Diagnosis T-Lymphoblastic lymphoma But wait, there s more... A few weeks later the cytogenetics came back... 46,XY t(8;13)(p12;q12)[12] Image courtesy of Dr. Xinyan Lu Further Studies RT-PCR
MDS 101. What is bone marrow? Myelodysplastic Syndrome: Let s build a definition. Dysplastic? Syndrome? 5/22/2014. What does bone marrow do?
 101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
ADx Bone Marrow Report. Patient Information Referring Physician Specimen Information
 ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
Myeloproliferative Disorders - D Savage - 9 Jan 2002
 Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
Disease Usual phenotype acute leukemia precursor chronic leukemia low grade lymphoma myeloma differentiated Total WBC > 60 leukemoid reaction acute leukemia Blast Pro Myel Meta Band Seg Lymph 0 0 0 2
CHALLENGING CASES PRESENTATION
 CHALLENGING CASES PRESENTATION Michael C. Wiemann, MD, FACP Program Co-Chair and Vice President Indy Hematology Education President, Clinical St. John Providence Physician Network Detroit, Michigan 36
CHALLENGING CASES PRESENTATION Michael C. Wiemann, MD, FACP Program Co-Chair and Vice President Indy Hematology Education President, Clinical St. John Providence Physician Network Detroit, Michigan 36
ACCME/Disclosures. History. Hematopathology Specialty Conference Case #4 4/13/2016
 Hematopathology Specialty Conference Case #4 Sherrie L. Perkins MD, PhD University of Utah ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose
Hematopathology Specialty Conference Case #4 Sherrie L. Perkins MD, PhD University of Utah ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose
Session 4: Summary and Conclusions
 Session 4: Summary and Conclusions Total cases in Session 4 Myeloproliferative neoplasms 16 cases Oral #300 (CEL, NOS) Mastocytosis 2 cases Oral #156 (SM-AHN) Myeloid/lymphoid neoplasms with eosinophilia
Session 4: Summary and Conclusions Total cases in Session 4 Myeloproliferative neoplasms 16 cases Oral #300 (CEL, NOS) Mastocytosis 2 cases Oral #156 (SM-AHN) Myeloid/lymphoid neoplasms with eosinophilia
20/20 PATHOLOGY REPORTS
 20/20 PATHOLOGY REPORTS Improving the Physician Experience. Enhancing the Patient Experience. We are LabTest Diagnostics. LabTest Diagnostics has a full-service laboratory with state-of-the-art equipment
20/20 PATHOLOGY REPORTS Improving the Physician Experience. Enhancing the Patient Experience. We are LabTest Diagnostics. LabTest Diagnostics has a full-service laboratory with state-of-the-art equipment
Session II: Summary. Robert P Hasserjian, MD Professor of Pathology Massachusetts General Hospital and Harvard Medical School
 Session II: Summary Robert P Hasserjian, MD Professor of Pathology Massachusetts General Hospital and Harvard Medical School Disclosure of speaker s interests (Prefix and Last Name) (Potential) conflict
Session II: Summary Robert P Hasserjian, MD Professor of Pathology Massachusetts General Hospital and Harvard Medical School Disclosure of speaker s interests (Prefix and Last Name) (Potential) conflict
John L Frater, MD Jeffery M Klco, MD, PhD Department of Pathology and Immunology Washington University School of Medicine St Louis, Missouri
 Myeloproliferative Neoplasms: New Approaches to Diagnosis and Disease Monitoring John L Frater, MD Jeffery M Klco, MD, PhD Department of Pathology and Immunology Washington University School of Medicine
Myeloproliferative Neoplasms: New Approaches to Diagnosis and Disease Monitoring John L Frater, MD Jeffery M Klco, MD, PhD Department of Pathology and Immunology Washington University School of Medicine
Polycythemia Vera and other Myeloproliferative Neoplasms. A.Mousavi
 Polycythemia Vera and other Myeloproliferative Neoplasms A.Mousavi Chronic MPNs Multipotent hematopoietic progenitor cell is origin. Overproduction of one or more formed element of blood cells without
Polycythemia Vera and other Myeloproliferative Neoplasms A.Mousavi Chronic MPNs Multipotent hematopoietic progenitor cell is origin. Overproduction of one or more formed element of blood cells without
Myeloproliferative Neoplasms and Treatment Overview
 Myeloproliferative Neoplasms and Treatment Overview George Nesr Clinical Research Fellow in Haematology Haematology Department Imperial College Healthcare NHS Trust Overview Historical Background Pathogenesis
Myeloproliferative Neoplasms and Treatment Overview George Nesr Clinical Research Fellow in Haematology Haematology Department Imperial College Healthcare NHS Trust Overview Historical Background Pathogenesis
NON-CLASSIC MYELOPROLIFERATIVE NEOPLASMS: ARE WE REALLY AWARE OF THESE RARE DISEASES IN DAILY PRACTICE?
 NON-CLASSIC MYELOPROLIFERATIVE NEOPLASMS: ARE WE REALLY AWARE OF THESE RARE DISEASES IN DAILY PRACTICE? *Serdal Korkmaz Department of Hematology, Kayseri Training and Research Hospital, Kayseri, Turkey
NON-CLASSIC MYELOPROLIFERATIVE NEOPLASMS: ARE WE REALLY AWARE OF THESE RARE DISEASES IN DAILY PRACTICE? *Serdal Korkmaz Department of Hematology, Kayseri Training and Research Hospital, Kayseri, Turkey
HEMATOLOGIC MALIGNANCIES BIOLOGY
 HEMATOLOGIC MALIGNANCIES BIOLOGY Failure of terminal differentiation Failure of differentiated cells to undergo apoptosis Failure to control growth Neoplastic stem cell FAILURE OF TERMINAL DIFFERENTIATION
HEMATOLOGIC MALIGNANCIES BIOLOGY Failure of terminal differentiation Failure of differentiated cells to undergo apoptosis Failure to control growth Neoplastic stem cell FAILURE OF TERMINAL DIFFERENTIATION
Disclosures for Angela Fleischman
 Disclosures for Angela Fleischman Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Sierra, Incyte None None None Incyte None Presentation includes
Disclosures for Angela Fleischman Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Sierra, Incyte None None None Incyte None Presentation includes
Diagnostic Approach for Eosinophilia and Mastocytosis. Curtis A. Hanson, M.D.
 Diagnostic Approach for Eosinophilia and Mastocytosis Curtis A. Hanson, M.D. 2014 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2014 MFMER slide-2 Molecular Classification
Diagnostic Approach for Eosinophilia and Mastocytosis Curtis A. Hanson, M.D. 2014 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2014 MFMER slide-2 Molecular Classification
Session 5. Pre-malignant clonal hematopoietic proliferations. Chairs: Frank Kuo and Valentina Nardi
 Session 5 Pre-malignant clonal hematopoietic proliferations Chairs: Frank Kuo and Valentina Nardi Pre-malignant clonal hematopoietic proliferations Clonal LYMPHOID proliferations: - Monoclonal gammopathy
Session 5 Pre-malignant clonal hematopoietic proliferations Chairs: Frank Kuo and Valentina Nardi Pre-malignant clonal hematopoietic proliferations Clonal LYMPHOID proliferations: - Monoclonal gammopathy
[COMPREHENSIVE GENETIC ASSAY PANEL ON
 2014 SN GENELAB AND RESEARCH CENTER DR. SALIL VANIAWALA, PH.D [COMPREHENSIVE GENETIC ASSAY PANEL ON MYELOPROLIFERATIVE NEOPLASMS] SN Genelab presents one of the most comprehensive genetic assay panel for
2014 SN GENELAB AND RESEARCH CENTER DR. SALIL VANIAWALA, PH.D [COMPREHENSIVE GENETIC ASSAY PANEL ON MYELOPROLIFERATIVE NEOPLASMS] SN Genelab presents one of the most comprehensive genetic assay panel for
Case Presentation No. 075
 Case Presentation No. 075 Session 4. Myelodysplastic Syndrome Cristina Montalvo, MD Baylor College of Medicine Houston, Texas 2007 Workshop of Society for Hematopathology and European Association for Haematopathology
Case Presentation No. 075 Session 4. Myelodysplastic Syndrome Cristina Montalvo, MD Baylor College of Medicine Houston, Texas 2007 Workshop of Society for Hematopathology and European Association for Haematopathology
Hematopathology Case Study
 www.medfusionservices.com Hematopathology Case Study CV3515-14 JUNE Clinical Presentation: Clinical Information: A 42 year old male with history of chronic myelogenous leukemia (CML) presents with an elevated
www.medfusionservices.com Hematopathology Case Study CV3515-14 JUNE Clinical Presentation: Clinical Information: A 42 year old male with history of chronic myelogenous leukemia (CML) presents with an elevated
9/25/2017. Disclosure. I have nothing to disclose. Young S. Kim MD Dept. of Pathology
 Disclosure MAST CELLNEOPLASM I have nothing to disclose. Young S. Kim MD Dept. of Pathology 1 Objectives What is mast cell lineage? Changes in updated WHO 2016 mastocytosis Issues of Mastocytosis CD30
Disclosure MAST CELLNEOPLASM I have nothing to disclose. Young S. Kim MD Dept. of Pathology 1 Objectives What is mast cell lineage? Changes in updated WHO 2016 mastocytosis Issues of Mastocytosis CD30
Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas. James J. Stark, MD, FACP
 Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS
Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS
DISCLOSURE Luca Malcovati, MD. No financial relationships to disclose
 ICUS, CCUS and CHIP Luca Malcovati, MD Department of Molecular Medicine, University of Pavia Medical School, & Department of Hematology Oncology, IRCCS Policlinico S. Matteo Foundation, Pavia, Italy DISCLOSURE
ICUS, CCUS and CHIP Luca Malcovati, MD Department of Molecular Medicine, University of Pavia Medical School, & Department of Hematology Oncology, IRCCS Policlinico S. Matteo Foundation, Pavia, Italy DISCLOSURE
Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Neoplasms. Policy Specific Section:
 Medical Policy Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Type: Medical Necessity and Investigational / Experimental Policy Specific Section:
Medical Policy Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Type: Medical Necessity and Investigational / Experimental Policy Specific Section:
Eosinophilia: A Diagnostic Approach and Test Utilization Strategies for Bone Marrow Evaluation
 Eosinophilia: A Diagnostic Approach and Test Utilization Strategies for Bone Marrow Evaluation American Society for Clinical Pathology 2014 Annual Meeting Presented by: Matthew T. Howard, MD Assistant
Eosinophilia: A Diagnostic Approach and Test Utilization Strategies for Bone Marrow Evaluation American Society for Clinical Pathology 2014 Annual Meeting Presented by: Matthew T. Howard, MD Assistant
Extramedullary precursor T-lymphoblastic transformation of CML at presentation
 Extramedullary precursor T-lymphoblastic transformation of CML at presentation Neerja Vajpayee, Constance Stein, Bernard Poeisz & Robert E. Hutchison Clinical History 30 year old man presented to the emergency
Extramedullary precursor T-lymphoblastic transformation of CML at presentation Neerja Vajpayee, Constance Stein, Bernard Poeisz & Robert E. Hutchison Clinical History 30 year old man presented to the emergency
Case Workshop of Society for Hematopathology and European Association for Haematopathology
 Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
AML: WHO classification, biology and prognosis. Dimitri Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen
 AML: WHO classification, biology and prognosis Dimitri Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen Acute myeloid leukemia Clonal expansion of undifferentiated myeloid precursors Impaired
AML: WHO classification, biology and prognosis Dimitri Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen Acute myeloid leukemia Clonal expansion of undifferentiated myeloid precursors Impaired
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed
 MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
Disclosure: Objectives/Outline. Leukemia: Genealogy of Pathology Practice: Old Diseases New Expectations. Nothing to disclose.
 RC1 Leukemia: Genealogy of Pathology Practice: Old Diseases New Expectations RC2 Disclosure: Nothing to disclose Henry Moon Lecture: UCSF Annual Conference Kathryn Foucar, MD kfoucar@salud.unm.edu May
RC1 Leukemia: Genealogy of Pathology Practice: Old Diseases New Expectations RC2 Disclosure: Nothing to disclose Henry Moon Lecture: UCSF Annual Conference Kathryn Foucar, MD kfoucar@salud.unm.edu May
Ordering Physician CLIENT,CLIENT. Collected REVISED REPORT
 HPWET Hematopathology Consultation, MML Embed Client Hematopathology Consult REVISED INAL DIAGNOSIS Interpretation Peripheral blood, bone marrow aspirate and biopsies, bilateral iliac crests: 1. Normocellular
HPWET Hematopathology Consultation, MML Embed Client Hematopathology Consult REVISED INAL DIAGNOSIS Interpretation Peripheral blood, bone marrow aspirate and biopsies, bilateral iliac crests: 1. Normocellular
Etiology. Definition MYELODYSPLASTIC SYNDROMES. De novo. Secondary MDS (10 years earlier than primary) transformation
 transformation") MYELODYSPLASTIC SYNDROMES Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics The University of Texas M.D. Anderson Cancer Center Houston, Texas No relevant COIs to
MYELODYSPLASTIC SYNDROMES Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics The University of Texas M.D. Anderson Cancer Center Houston, Texas No relevant COIs to
Bone Marrow. Procedures Blood Film Aspirate, Cell Block Trephine Biopsy, Touch Imprint
 Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
Bone Marrow Protocol applies to acute leukemias, myelodysplastic syndromes, myeloproliferative disorders, chronic lymphoproliferative disorders, malignant lymphomas, plasma cell dyscrasias, histiocytic
5/21/2018. Disclosures. Objectives. Normal blood cells production. Bone marrow failure syndromes. Story of DNA
 AML: Understanding your diagnosis and current and emerging treatments Nothing to disclose. Disclosures Mohammad Abu Zaid, MD Assistant Professor of Medicine Indiana University School of Medicine Indiana
AML: Understanding your diagnosis and current and emerging treatments Nothing to disclose. Disclosures Mohammad Abu Zaid, MD Assistant Professor of Medicine Indiana University School of Medicine Indiana
Molecular profiling in confirming the diagnosis of early myelodysplastic syndrome
 Molecular profiling of early MDS Hematopathology - March 2016 Article Molecular profiling in confirming the diagnosis of early myelodysplastic syndrome Maya Thangavelu 1,*, Ryan Olson 2, Li Li 2, Wanlong
Molecular profiling of early MDS Hematopathology - March 2016 Article Molecular profiling in confirming the diagnosis of early myelodysplastic syndrome Maya Thangavelu 1,*, Ryan Olson 2, Li Li 2, Wanlong
MPL W515L K mutation
 MPL W515L K mutation BCR-ABL genotyping The exact chromosomal defect in Philadelphia chromosome is a translocation. Parts of two chromosomes, 9 and 22, switch places. The result is a fusion gene, created
MPL W515L K mutation BCR-ABL genotyping The exact chromosomal defect in Philadelphia chromosome is a translocation. Parts of two chromosomes, 9 and 22, switch places. The result is a fusion gene, created
Characterization of MPL-mutated myeloid neoplasms: a review of 224 MPL+ cases
 Article Characterization of MPL-mutated myeloid neoplasms: a review of 224 MPL+ cases Keming Lin 1,*, Gang Xu 1, Jie-Gen Jiang 1, Mayuko Imai 1, Zhao Wu 1, Paris Petersen 1, Kim Janatpour 1, and Bashar
Article Characterization of MPL-mutated myeloid neoplasms: a review of 224 MPL+ cases Keming Lin 1,*, Gang Xu 1, Jie-Gen Jiang 1, Mayuko Imai 1, Zhao Wu 1, Paris Petersen 1, Kim Janatpour 1, and Bashar
Myelodysplastic Syndromes: WHO 2008
 Myelodysplastic Syndromes: WHO 2008 Attilio Orazi, M.D., FRCPath. (Engl.) Weill Medical College of Cornell University New York, NY Congresso Nazionale SIE - Società Italiana di Ematologia - MIC Milano
Myelodysplastic Syndromes: WHO 2008 Attilio Orazi, M.D., FRCPath. (Engl.) Weill Medical College of Cornell University New York, NY Congresso Nazionale SIE - Società Italiana di Ematologia - MIC Milano
Intro alla patologia. Giovanni Barosi. Fondazione IRCCS Policlinico San Matteo Pavia
 Settima Giornata Fiorentina dedicata ai pazienti con malattie mieloproliferative croniche Sabato 13 Maggio 2017 CRIMM Centro di Ricerca e Innovazione per le Malattie Mieloproliferative AOU Careggi Intro
Settima Giornata Fiorentina dedicata ai pazienti con malattie mieloproliferative croniche Sabato 13 Maggio 2017 CRIMM Centro di Ricerca e Innovazione per le Malattie Mieloproliferative AOU Careggi Intro
Changes to the 2016 WHO Classification for the Diagnosis of MDS
 Changes to the 2016 WHO Classification for the Diagnosis of MDS Welcome to Managing MDS. I am Dr. Ulrich Germing, and today, I will provide highlights from the 14th International Symposium on MDS in Valencia,
Changes to the 2016 WHO Classification for the Diagnosis of MDS Welcome to Managing MDS. I am Dr. Ulrich Germing, and today, I will provide highlights from the 14th International Symposium on MDS in Valencia,
MYELOPROLIFARATIVE NEOPLASMS. Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin).
, FRCP(Edin).") MYELOPROLIFARATIVE NEOPLASMS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin). These are a group of chronic conditions characterised by clonal proliferation of marrow precursor cells. PRV, essential thrombocyathaemia,
MYELOPROLIFARATIVE NEOPLASMS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin). These are a group of chronic conditions characterised by clonal proliferation of marrow precursor cells. PRV, essential thrombocyathaemia,
When Cancer Looks Like Something Else: How Does Mutational Profiling Inform the Diagnosis of Myelodysplasia?
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Myelodysplastic Syndrome Case 158
 Myelodysplastic Syndrome Case 158 Dong Chen MD PhD Division of Hematopathology Mayo Clinic Clinical History 86 year old man Persistent borderline anemia and thrombocytopenia. His past medical history was
Myelodysplastic Syndrome Case 158 Dong Chen MD PhD Division of Hematopathology Mayo Clinic Clinical History 86 year old man Persistent borderline anemia and thrombocytopenia. His past medical history was
Classification of Hematologic Malignancies. Patricia Aoun MD MPH
 Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Classification of Hematologic Malignancies Patricia Aoun MD MPH Objectives Know the basic principles of the current classification system for hematopoietic and lymphoid malignancies Understand the differences
Acute Myeloid Leukemia with RUNX1 and Several Co-mutations
 Case SH2017-0281 Acute Myeloid Leukemia with RUNX1 and Several Co-mutations James Bauer, MD, PhD David Yang, MD Erik Ranheim, MD, PhD Catherine Leith, MB, Bchir Clinical History Chief Complaint: 72 year
Case SH2017-0281 Acute Myeloid Leukemia with RUNX1 and Several Co-mutations James Bauer, MD, PhD David Yang, MD Erik Ranheim, MD, PhD Catherine Leith, MB, Bchir Clinical History Chief Complaint: 72 year
SUPPLEMENTARY INFORMATION
 Supplementary Information S1 Frequency of DNMT3A mutations in hematologic disorders and their associated clinical phenotypes. Disease Patient population Frequency (%) Associated Clinical Characteristics
Supplementary Information S1 Frequency of DNMT3A mutations in hematologic disorders and their associated clinical phenotypes. Disease Patient population Frequency (%) Associated Clinical Characteristics
Combinations of morphology codes of haematological malignancies (HM) referring to the same tumour or to a potential transformation
 referring to the same tumour or to a potential transformation") Major subgroups according to the World Health Organisation (WHO) Classification Myeloproliferative neoplasms (MPN) Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB or
Major subgroups according to the World Health Organisation (WHO) Classification Myeloproliferative neoplasms (MPN) Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB or
Molecular techniques in a case of concurrent BCR-ABL1 positive CML and CMML
 reprinted from november 2014 pathology laboratory medicine laboratory management Molecular techniques in a case of concurrent BCR-ABL1 positive CML and CMML CAP TODAY and the Association for Molecular
reprinted from november 2014 pathology laboratory medicine laboratory management Molecular techniques in a case of concurrent BCR-ABL1 positive CML and CMML CAP TODAY and the Association for Molecular
Histological evaluation of myeloproliferative neoplasms
 Journal of clinical and experimental hematopathology Vol. 58 No.2, 45-50, 2018 JC lin EH xp ematopathol Review Article Histological evaluation of myeloproliferative neoplasms Hideyo Fujiwara In 2017, the
Journal of clinical and experimental hematopathology Vol. 58 No.2, 45-50, 2018 JC lin EH xp ematopathol Review Article Histological evaluation of myeloproliferative neoplasms Hideyo Fujiwara In 2017, the
CLINICAL POLICY DEPARTMENT: Medical Management DOCUMENT NAME: JakafiTM REFERENCE NUMBER: NH.PHAR.98
 PAGE: 1 of 6 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
PAGE: 1 of 6 IMPORTANT REMINDER This Clinical Policy has been developed by appropriately experienced and licensed health care professionals based on a thorough review and consideration of generally accepted
CASE 106. Pancytopenia in the setting of marrow hypoplasia, a PNH clone, and a DNMT3A mutation
 CASE 106 Pancytopenia in the setting of marrow hypoplasia, a PNH clone, and a DNMT3A mutation Gabriel C. Caponetti, MD University of Pennsylvania, US Clinical history 69, F peripheral neuropathy, refractory
CASE 106 Pancytopenia in the setting of marrow hypoplasia, a PNH clone, and a DNMT3A mutation Gabriel C. Caponetti, MD University of Pennsylvania, US Clinical history 69, F peripheral neuropathy, refractory
Refresher in Blood Cell Morphology. Tracy I. George, MD Professor of Pathology University of Utah
 Refresher in Blood Cell Morphology Tracy I. George, MD Professor of Pathology University of Utah No financial conflicts of interest Objectives Recognize non-neoplastic and neoplastic disorders in the peripheral
Refresher in Blood Cell Morphology Tracy I. George, MD Professor of Pathology University of Utah No financial conflicts of interest Objectives Recognize non-neoplastic and neoplastic disorders in the peripheral
JAK2 V617F analysis. Indication: monitoring of therapy
 JAK2 V617F analysis BCR-ABL genotyping The exact chromosomal defect in Philadelphia chromosome is a translocation. Parts of two chromosomes, 9 and 22, switch places. The result is a fusion gene, created
JAK2 V617F analysis BCR-ABL genotyping The exact chromosomal defect in Philadelphia chromosome is a translocation. Parts of two chromosomes, 9 and 22, switch places. The result is a fusion gene, created