Assessment of Efficacy and Immune Related RECIST criteria
|
|
|
- Lydia McDonald
- 5 years ago
- Views:
Transcription




1 Assessment of Efficacy and Immune Related RECIST criteria Dr Kenneth O Byrne Princess Alexandra Hospital and Queensland University of Technology, Brisbane, Australia & Trinity College, Dublin, Ireland

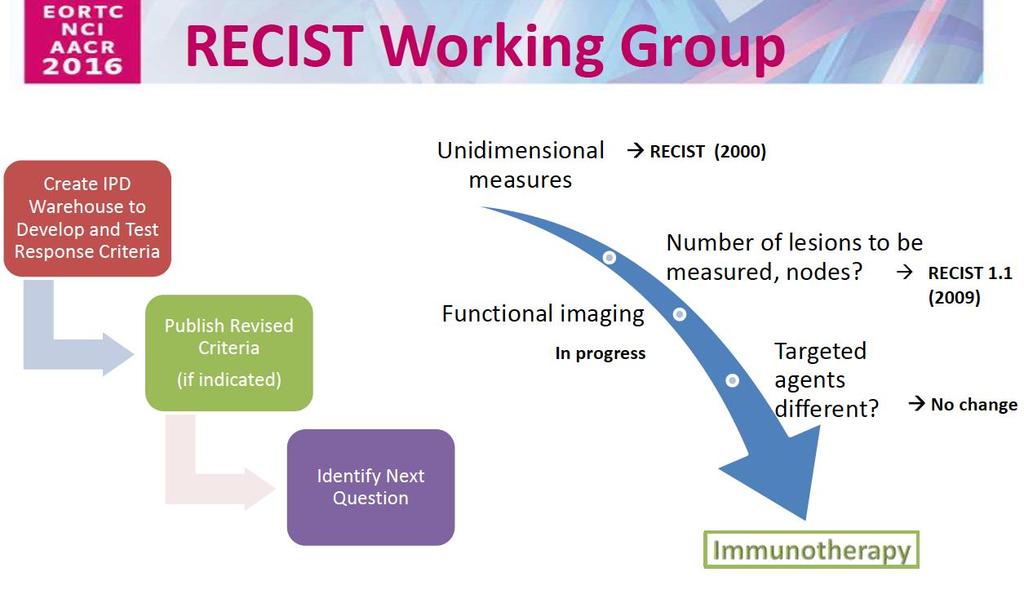
2 History of RECIST (Response Evaluation Criteria in Solid Tumors 1960s Early attempts to standardize tumor response to oncologic agents 1979 Mid-1990s World Health Organization (WHO) standardized criteria for response assessment; published in 1981 International Working Party simplified response criteria New criteria was presented at the American Society for Clinical Oncology meeting; RECIST 1.0 criteria published in 2000 RECIST updated, latest version - RECIST 1.1, was published RECIST allows clinicians to determine whether a patient responds to therapy, whether they are stable, or whether their disease has progressed
3 RECIST Response Criteria Target Lesions - includes all measurable lesions*; max 2 per organ, 5 lesions total Evaluation of Target Lesions RECIST Guideline Non-Target Lesions all other lesions not classified as a target lesion or sites of disease Evaluation of non-target lesions RECIST Guideline CR Disappearance of all target lesions; confirmed at > 4 weeks CR Disappearance of all nontarget lesions; normalization of tumor markers PR > 30% decrease of SoD from baseline, confirmed at > 4 weeks PD Appearance of > 1 new lesions and/or progression of existing non-target lesions PD > 20% increase from smallest sum of diameters recorded and 5 mm absolute increase over lowest sum SD Persistence of > 1 non-target lesion; tumor marker level above normal SD Neither PR or PD CR (Complete Response); PR (Partial Response); PD (Progressive Disease); SD (Stable Disease) *measurable lesion = > 10 mm in longest diameter by CT Scan; > 20 mm in longest diameter by x-ray sources: Eisenhauer et al., 2009; Nishino et al, 2010; and RECIST, Applying the Rules, National Cancer Institute,


4 RECIST 1.1 Time Point Response Tumor evaluation should occur every 6-8 weeks where the benefit of the therapy is not known o Repetitive tumor evaluations depend on whether the trial has a goal of response rate or the time to an event (e.g. Progression- Free Survival (PFS)) source: Eisenhauer et al., 2009
5 RECIST for Determining Tumor Response is Applicable to Cytotoxic and Targeted Therapy Agents o Cytotoxic agents directly kill a tumor cell or prevent tumor cells from dividing (e.g. chemotherapy); therefore, response of cytotoxic agents can be easily measured from the start of therapy o Early increase in tumor burden and/or an early increase in tumor size signifies progressive disease o Once progression is detected, drug cessation is recommended o Response after initial treatment of a cytotoxic agent can often predict remission and survival
6 Immuno-oncology agents differ from cytotoxic agents in that they stimulate an innate immune response against the tumor Vaccines: trigger the immune system to initiate an anti-tumor response against an existing cancer Monoclonal Antibodies: antibodies directed against tumor cells; they can block signaling pathways needed for tumor growth and trigger an immune-mediatedcytotoxic response Checkpoint inhibitors: tumors escape detection by the immune system through expression of checkpoint proteins on their cell surface. CTLA-4 and PD-1 receptors are examples of checkpoint receptors; targeted inhibition towards these receptors enhances T cell response towards the tumor Cytokines: stimulates a broad-based immune response (e.g. interleukin-2 and interferon-α) Source:
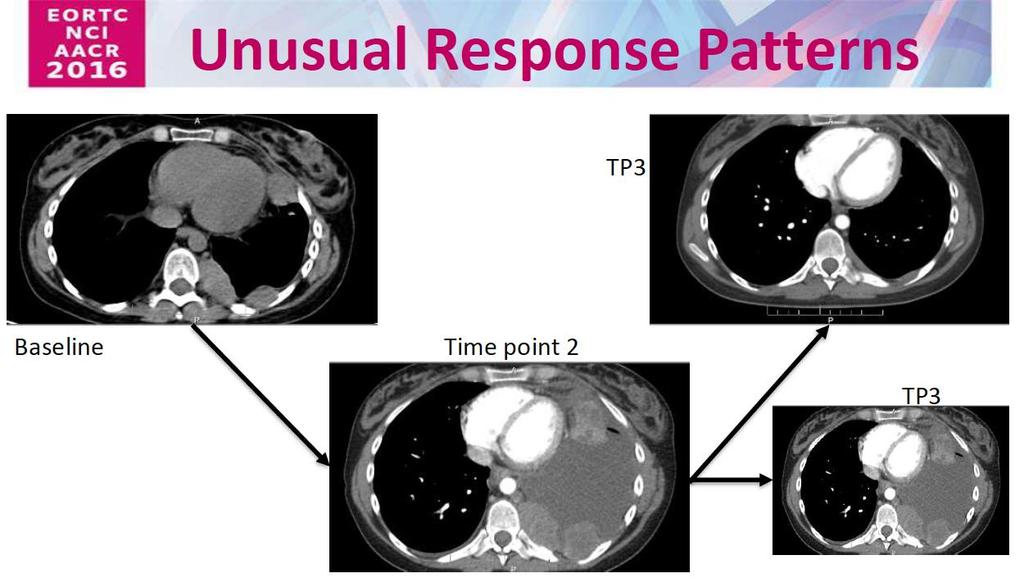
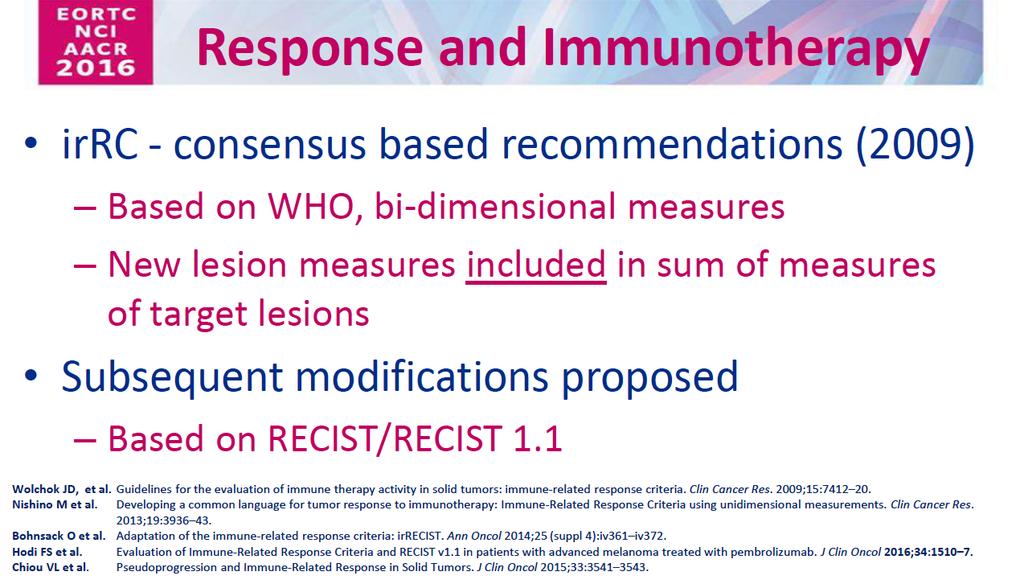
7 The unique mechanism of action of immuno- oncology agents requires modified tumor response criteria RECIST may not provide a complete assessment of immunotherapeutics Anti-tumor response to immunotherapy may take longer compared to cytotoxic agent response Clinical response to immune therapies can manifest after conventional progressive disease (PD) Pseudnoprogression Discontinuation of immune therapy may not be appropriate in some cases, unless PD is confirmed Allowance for clinically insignificant PD (e.g., small new lesions in the presence of other responsive lesions) is recommended Durable stable disease may represent antitumor activity source: Wolchock et al., 2009

8 Differing mechanism of immunotherapy
9
10 Ipilimumab clinical observations and evaluation of a novel set of response criteria Ipilimumab: human, monoclonal antibody that binds to the cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) on T cells. Blocking CTLA-4 from interacting with its ligands augments a T cell immune response to tumor cells Ipilimumab is indicated for the treatment of unresectable or metastatic melanoma Ipilimumab was studied in three multicenter phase II trials evaluating 487 patients with unresectable stage III or IV melanoma Activity was categorized using a novel set of criteria Tumor assessments carried out at week 12 following the end of the induction dosing period (ipilimumab 10 mg/kg every three weeks times x4) source: Wolchock et al., 2009
11 Four patterns of response were observed in patients treated with ipilimumab Overall, ~30% of patients had disease control (CR, PR, or SD) Of the 4 patterns of response observed two met conventional criteria for tumor response: Response in baseline lesions stable disease with slow, steady decline in total tumor volume SPD = sum of the product of perpendicular diameters Triangles = ipilimumab dosing time points source: Wolchock et al., 2009
 Triangles = ipilimumab dosing time points N=tumor burden of new")
12 The other two response patterns observed go against the standard criteria for tumor response Responses after an initial increase in total tumor burden Reduction in total tumor burden during or after the appearance of new lesions SPD = sum of the product of perpendicular diameters (used in WHO criteria) Triangles = ipilimumab dosing time points N=tumor burden of new lesions


13 A number of ipilimumab treated patients initially characterized as PD, are considered PR or SD using the irrc Guideline source: Wolchock et al., 2009
14 Association of response withsurvival
15 Clinical trials utilizing both irrc and RECIST 1.1 to measure tumor response 411 pts, 192 were on MK-3475 (pembrolizumab) > 28 weeks 215 patients had either a CR, PR, or SD by RECIST and irrc 51 patients had PD by RECIST, but had either a CR, PR, or SD by irrc Authors concluded: conventional criteria such as RECIST may underestimate the benefit of MK-3475 in approximately 10% of treated pts.

16
17
18
19
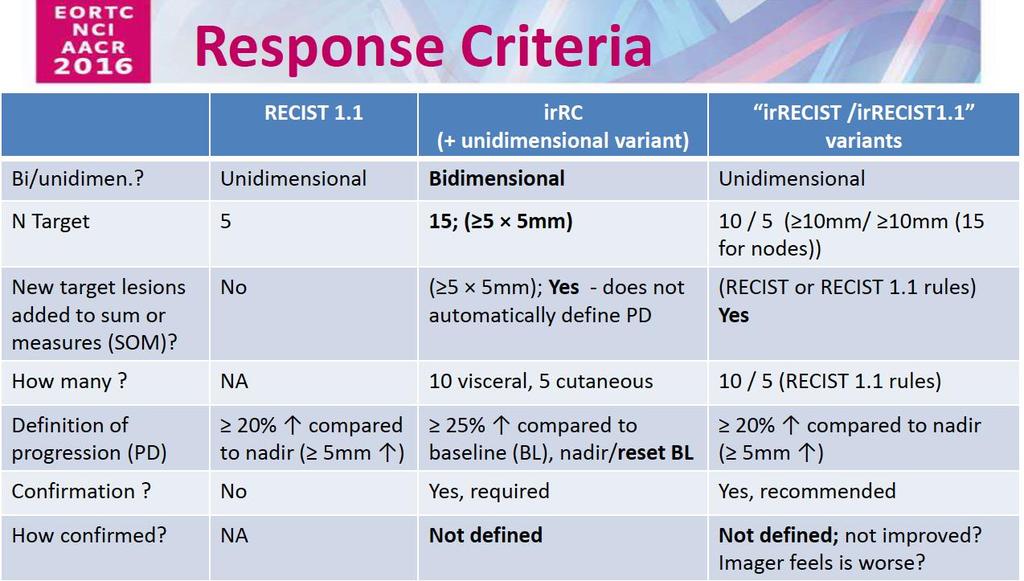
20 Differences between WHO classification and irrc WHO irrc New Measurable lesions (> 5 x 5 mm) New non-measurable lesions (<5 x 5 mm) Non-index lesions Always represent PD Always represent PD Changes contribute to defining best overall response Incorporated into total tumor burden Do not define progression (but preclude ircr) Contribute to defining ir CR
21 Using the irrc ircr: Complete disappearance of all lesions (whether measurable or not, and no new lesions, and confirmation by a repeat consecutive assessment no less than 4 weeks from date first documented irpr: decrease in tumor burden >50% relative to baseline confirmed by repeat consecutive assessment at least 4 weeks later irsd: not meeting criteria for ircr or irpr in absence of ir PD irpd: increase in tumor burden >25% relative to nadir (minimum recorded tumor burden) confirmed by repeat consecutive assessment at least 4 weeks later
22
23
24 True or Pseudoprogression? 1 2
25
26
27
28
29
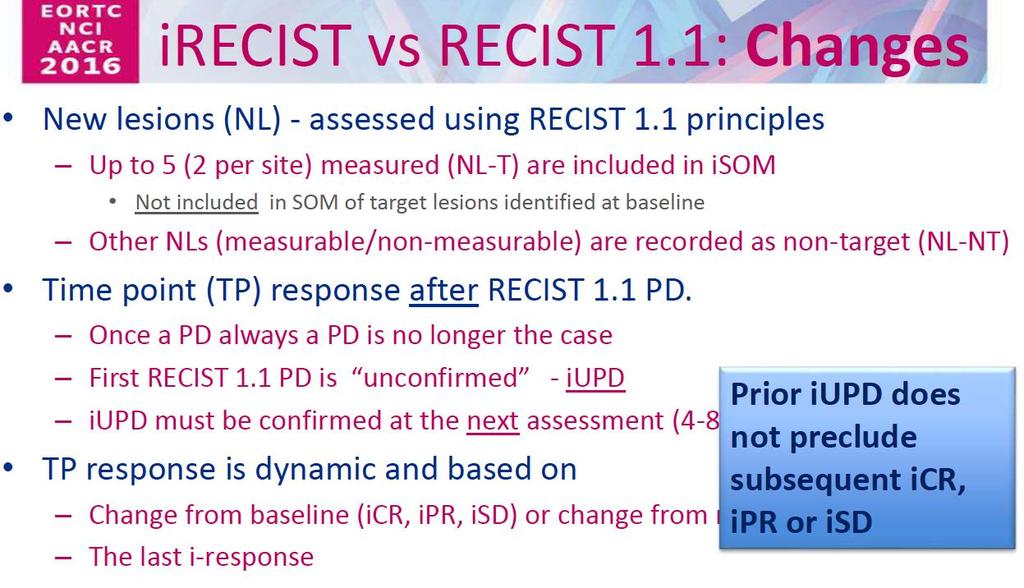
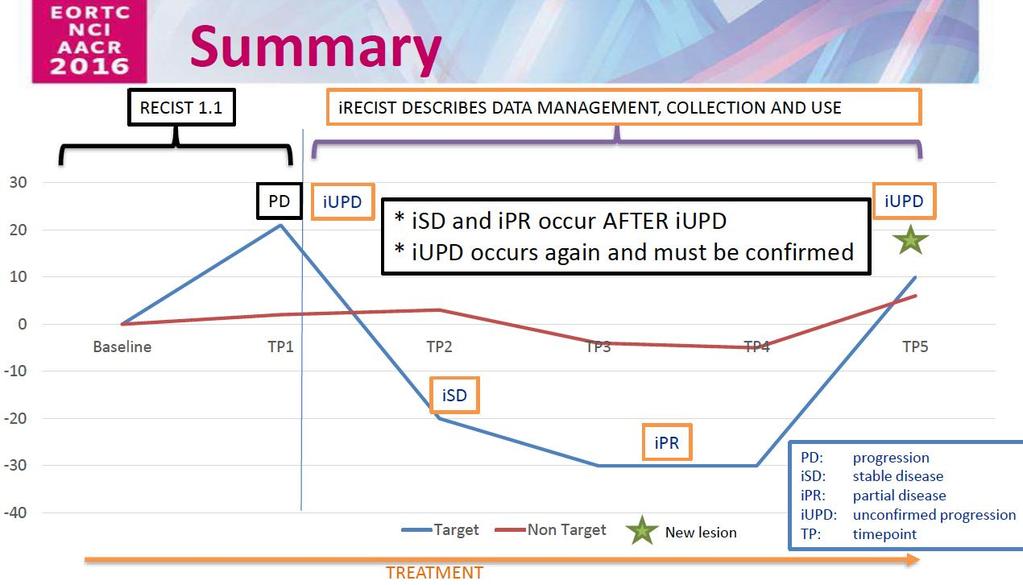
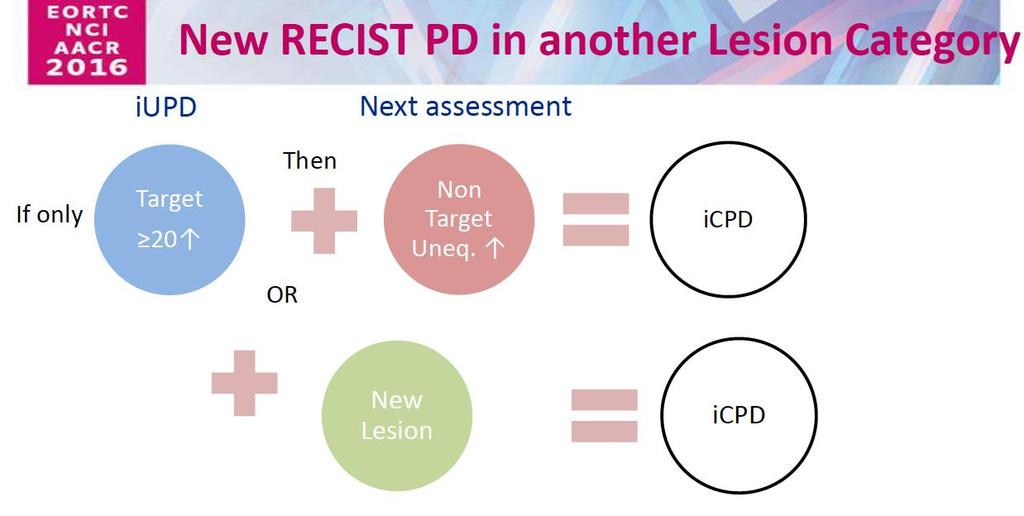
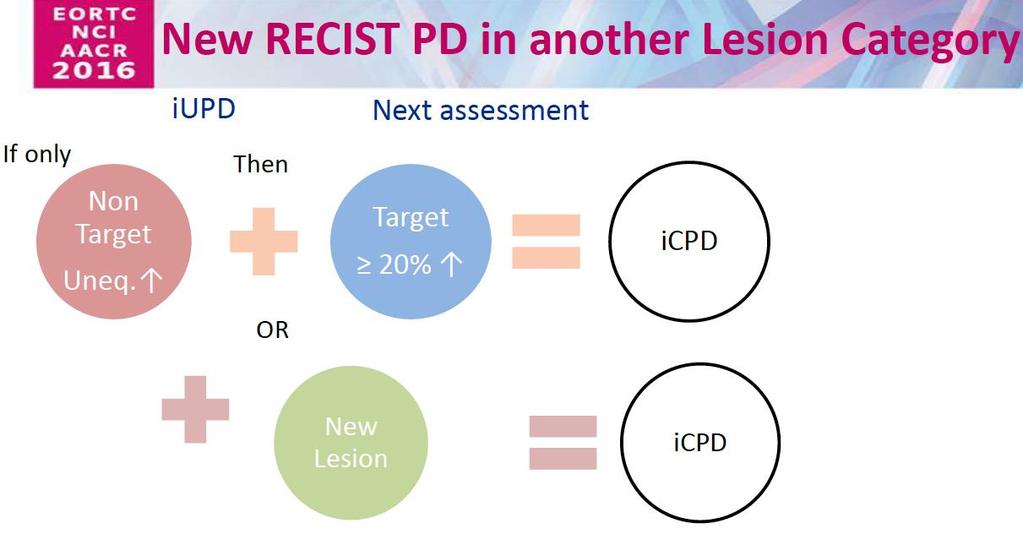
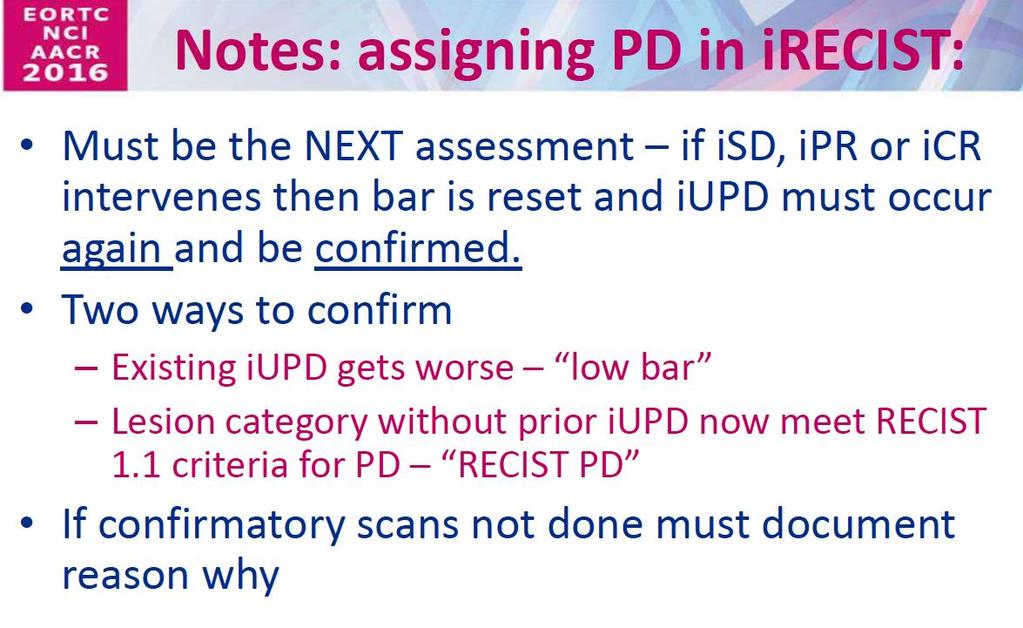
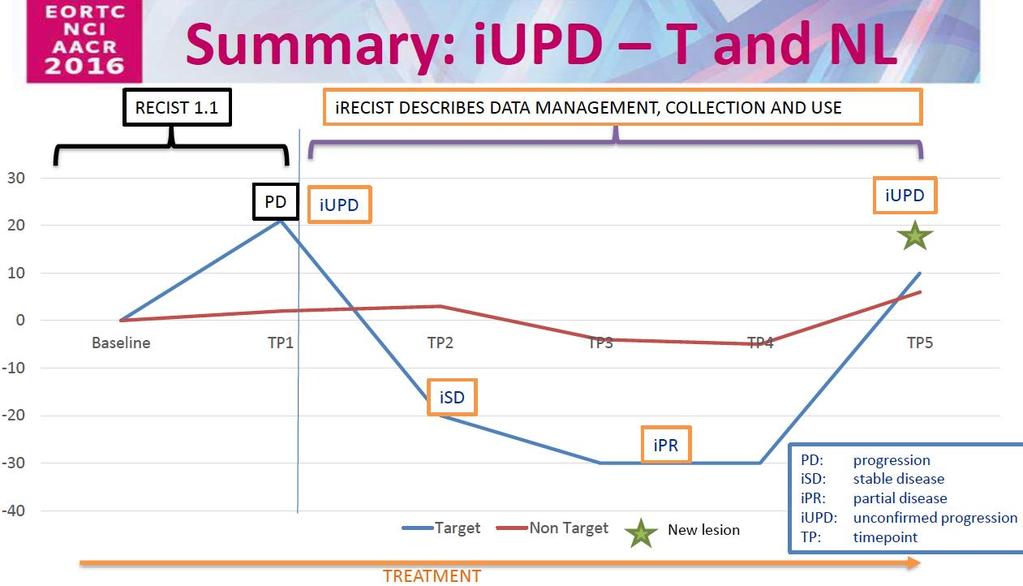
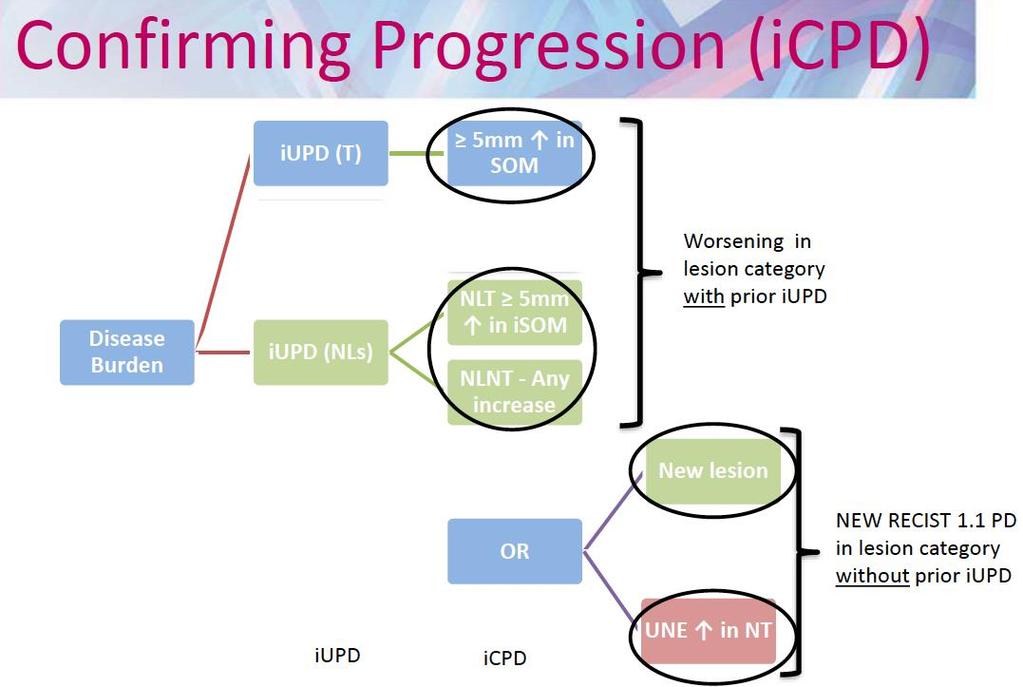
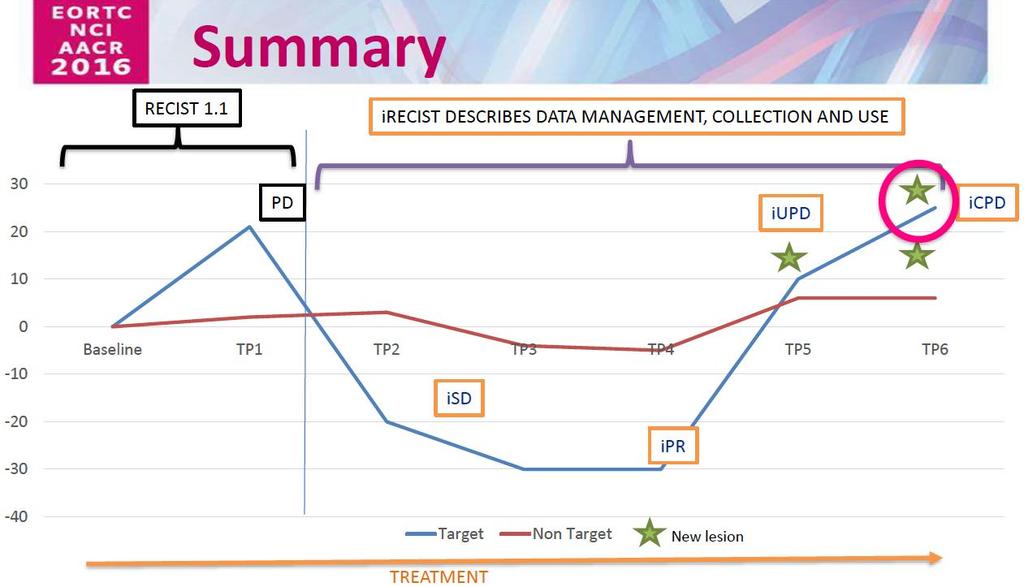
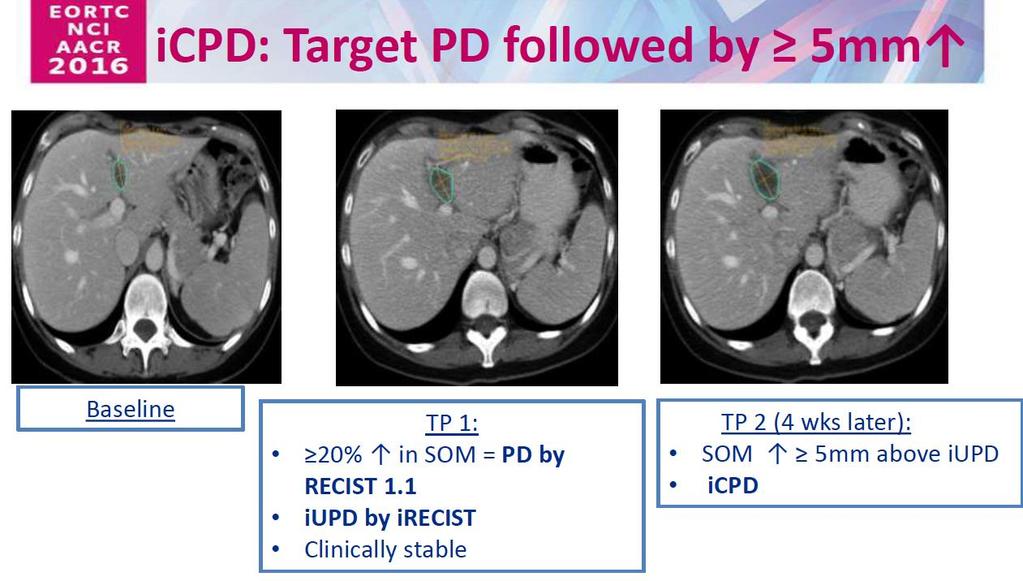
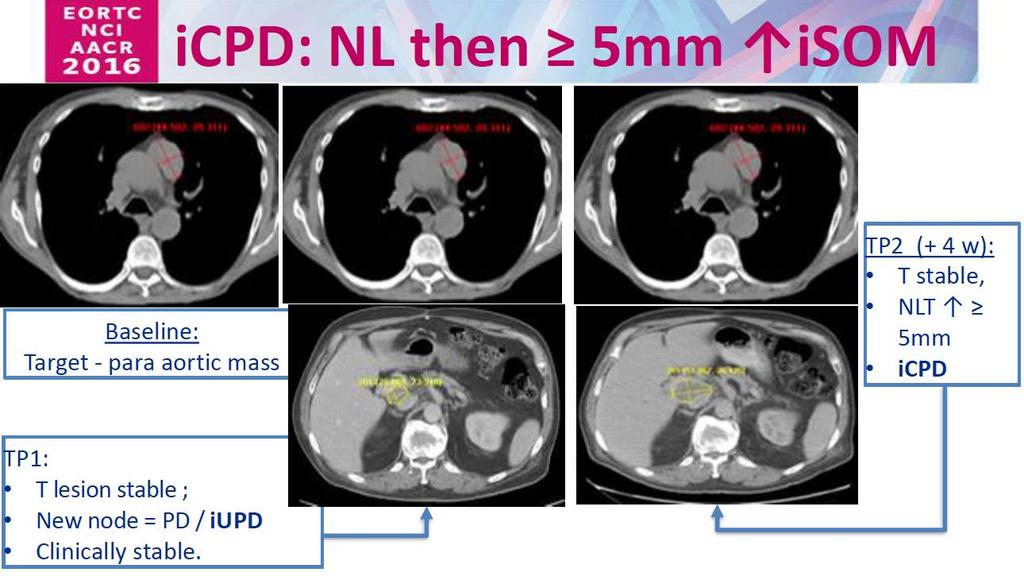
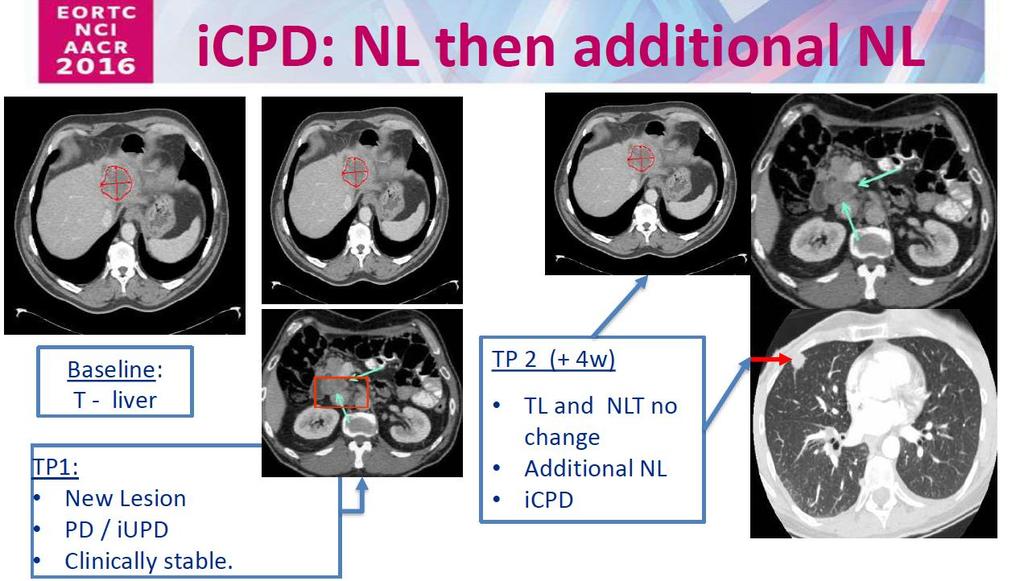
30 irecistvs RECIST1.1: Changes New lesions (NL) - assessed using RECIST1.1 principles Up to 5 (2 per site) measured (NL-T) are included in isom Not included in SOM of target lesions identified at baseline Other NLs(measurable/non-measurable) are recorded as non-target (NL-NT) Time point (TP) response after RECIST1.1 PD. Once a PD always a PD is no longer the case First RECIST1.1 PD is unconfirmed - iupd iupd must be confirmed at the next assessment (4-8 weeks). TPresponse is dynamic and based on Change from baseline (icr, ipr, isd) or change from nadir PD The last i-response
31
32
33

34
35
36
37
38
39
40
41
42
43
44
45
 Immune response distinct from RECIST response has been reported in melanoma (6.")
46 Pseudo-progression Clinical trials have reported the presence of patients with distinct immune-related patterns of response that did not meet RECIST criteria (44 of 1,126 total patients; an approximate overall incidence of 4%) Immune response distinct from RECIST response has been reported in melanoma (6.6%; 31 of 471 patients) Lung Cancer appears less than 5%
47 Immune Related Response Criteria irrc RECIST 1.0 Presence of new lesion does not define progression The measurement(s) of the new lesion(s) are included in the sum of the measurements Up to 5 new lesions per organ and 10 new lesions in total can be added to measurements irrc RECIST 1.1 Presence of new lesion does not define progression The measurement(s) of the new lesion(s) are included in the sum of the measurements (LN must be 15 mm) Up to 2 new lesions per organ and 5 new lesions in total can be added to measurements
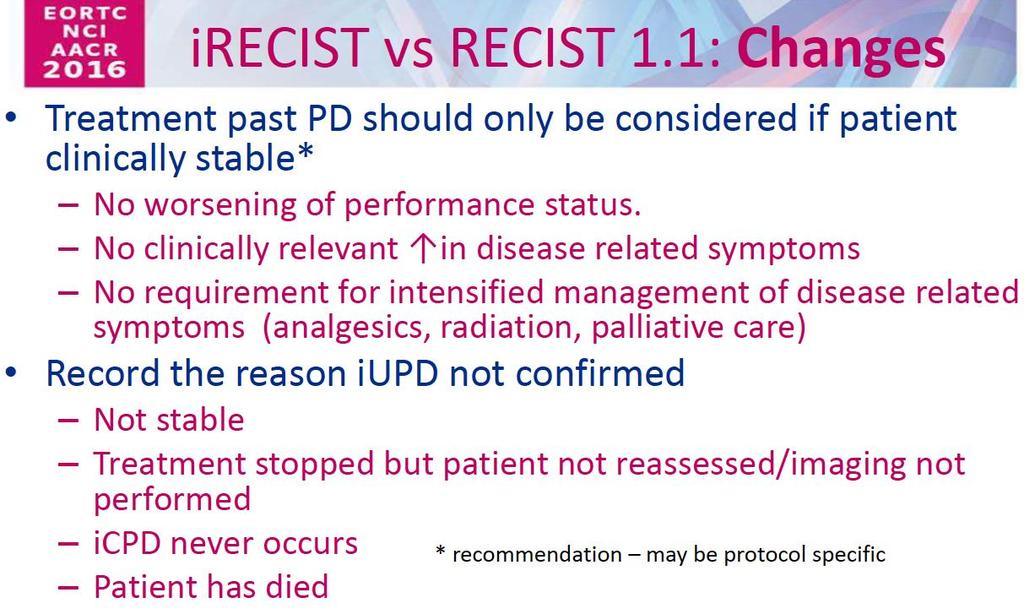
48 Implications for Patient Care Pragmatism If patient well with RECIST 1.1 PD reasonable to continue therapy but restage early If patient unwell with RECIST 1.1 stop therapy and consider alternative treatments Continuation after progression being explored OAK/Atezolizumab data suggest that, in selected well patients, maintenance may improve survival Randomised phase III data required to confirm this observation and should not be used in routine care
Immuno-Oncology Applications
 Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
How Can We Evaluate Response to New Agents? Recent update of imaging response assessment for cancer immunotherapy
 2018 KLCA Symposium How Can We Evaluate Response to New Agents? Recent update of imaging response assessment for cancer immunotherapy KYUNG WON KIM, MD, PhD Seoul Asan Medical Center Asan Medical Center
2018 KLCA Symposium How Can We Evaluate Response to New Agents? Recent update of imaging response assessment for cancer immunotherapy KYUNG WON KIM, MD, PhD Seoul Asan Medical Center Asan Medical Center
Applying the New irecist Guidelines Radiologic and Clinical Trial Considerations
 Applying the New irecist Guidelines Radiologic and Clinical Trial Considerations Author: K. Luby, Mint Medical www.irecist.com irecist 1 : Guidelines for response criteria for use in trials testing immunotherapeutics
Applying the New irecist Guidelines Radiologic and Clinical Trial Considerations Author: K. Luby, Mint Medical www.irecist.com irecist 1 : Guidelines for response criteria for use in trials testing immunotherapeutics
IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER
 Gynecologic Cancer InterGroup Cervix Cancer Research Network IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Cervix
Gynecologic Cancer InterGroup Cervix Cancer Research Network IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Cervix
New Data from Ongoing Melanoma Study and Clinical Development Strategy Update
 New Data from Ongoing Melanoma Study and Clinical Development Strategy Update Webcast - 29 th / 30 th May 2018 (ASX: IMM, NASDAQ: IMMP) Notice: Forward Looking Statements The purpose of the presentation
New Data from Ongoing Melanoma Study and Clinical Development Strategy Update Webcast - 29 th / 30 th May 2018 (ASX: IMM, NASDAQ: IMMP) Notice: Forward Looking Statements The purpose of the presentation
Melanoma: Immune checkpoints
 ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
Evaluation of Lung Cancer Response: Current Practice and Advances
 Evaluation of Lung Cancer Response: Current Practice and Advances Jeremy J. Erasmus I have no financial relationships, arrangements or affiliations and this presentation will not include discussion of
Evaluation of Lung Cancer Response: Current Practice and Advances Jeremy J. Erasmus I have no financial relationships, arrangements or affiliations and this presentation will not include discussion of
Guidelines for the Evaluation of Immune Therapy Activity in Solid Tumors: Immune-Related Response Criteria
 Published OnlineFirst November 24, 2009; DOI: 10.1158/1078-0432.CCR-09-1624 Cancer Therapy: Clinical Guidelines for the Evaluation of Immune Therapy Activity in Solid Tumors: Immune-Related Response Criteria
Published OnlineFirst November 24, 2009; DOI: 10.1158/1078-0432.CCR-09-1624 Cancer Therapy: Clinical Guidelines for the Evaluation of Immune Therapy Activity in Solid Tumors: Immune-Related Response Criteria
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER. Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia
 IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Distinguishing self from non-self T cells trained in the thymus as
IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Distinguishing self from non-self T cells trained in the thymus as
Immunotherapy Concept Turned Reality
 Authored by: Jennifer Dolan Fox, PhD VirtualScopics Inc. jennifer_fox@virtualscopics.com +1 585 249 6231 Immunotherapy Concept Turned Reality Introduction While using the body s own immune system as a
Authored by: Jennifer Dolan Fox, PhD VirtualScopics Inc. jennifer_fox@virtualscopics.com +1 585 249 6231 Immunotherapy Concept Turned Reality Introduction While using the body s own immune system as a
Marshall T Bell Research Resident University of Colorado Grand Rounds Nov. 21, 2011
 Marshall T Bell Research Resident University of Colorado Grand Rounds Nov. 21, 2011 Most common form of cancer in adults ages 25-29 3-5% of skin cancers but 65-75% of deaths Most common metastasis to small
Marshall T Bell Research Resident University of Colorado Grand Rounds Nov. 21, 2011 Most common form of cancer in adults ages 25-29 3-5% of skin cancers but 65-75% of deaths Most common metastasis to small
Frédéric Triebel MD, PhD World Immunotherapy Congress Basel, October 30, 2018
 Two ACTive immunotherapies in melanoma (TACTI-mel): results of a phase I trial combining a soluble LAG-3 receptor (Eftilagimod Alpha) with Pembrolizumab Frédéric Triebel MD, PhD World Immunotherapy Congress
Two ACTive immunotherapies in melanoma (TACTI-mel): results of a phase I trial combining a soluble LAG-3 receptor (Eftilagimod Alpha) with Pembrolizumab Frédéric Triebel MD, PhD World Immunotherapy Congress
Radiographic Assessment of Response An Overview of RECIST v1.1
 Radiographic Assessment of Response An Overview of RECIST v1.1 Stephen Liu, MD Georgetown University May 15 th, 2015 Presentation Objectives To understand the purpose of RECIST guidelines To describe the
Radiographic Assessment of Response An Overview of RECIST v1.1 Stephen Liu, MD Georgetown University May 15 th, 2015 Presentation Objectives To understand the purpose of RECIST guidelines To describe the
Programming LYRIC Response in Immunomodulatory Therapy Trials Yang Wang, Seattle Genetics, Inc., Bothell, WA
 PharmaSUG 2017 Paper BB12 Programming LYRIC Response in Immunomodulatory Therapy Trials Yang Wang, Seattle Genetics, Inc., Bothell, WA ABSTRACT The LYmphoma Response to Immunomodulatory therapy Criteria
PharmaSUG 2017 Paper BB12 Programming LYRIC Response in Immunomodulatory Therapy Trials Yang Wang, Seattle Genetics, Inc., Bothell, WA ABSTRACT The LYmphoma Response to Immunomodulatory therapy Criteria
FDG PET for therapy response assessment in lymphoma: Beyond Lugano Classification
 FDG PET for therapy response assessment in lymphoma: Beyond Lugano Classification Yan Xuexian, MD, DABNM Department of Nuclear Medicine and PET, SGH National Cancer Center Singapore Duke-NUS Medical School
FDG PET for therapy response assessment in lymphoma: Beyond Lugano Classification Yan Xuexian, MD, DABNM Department of Nuclear Medicine and PET, SGH National Cancer Center Singapore Duke-NUS Medical School
WHY LOOK FOR ADDITIONAL DATA TO ENRICH THE KAPLAN-MEIER CURVES? Immuno-oncology, only an example
 WHY LOOK FOR ADDITIONAL DATA TO ENRICH THE KAPLAN-MEIER CURVES? Immuno-oncology, only an example YIDOU ZHANG Health Economics and Payer Analytics Director Oncology Payer Evidence and Pricing, AstraZeneca
WHY LOOK FOR ADDITIONAL DATA TO ENRICH THE KAPLAN-MEIER CURVES? Immuno-oncology, only an example YIDOU ZHANG Health Economics and Payer Analytics Director Oncology Payer Evidence and Pricing, AstraZeneca
PTAC meeting held on 5 & 6 May (minutes for web publishing)
") PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
III Sessione I risultati clinici
 10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
Innovations in Immunotherapy - Melanoma. Systemic Therapies October 27, 2018 Charles L. Bane, MD
 Innovations in Immunotherapy - Melanoma Systemic Therapies October 27, 2018 Charles L. Bane, MD Melanoma Prognosis Survival at 10 years Stage I: 90% Stage II: 60% Stage III: 40% Stage IV: 10% 2 Indications
Innovations in Immunotherapy - Melanoma Systemic Therapies October 27, 2018 Charles L. Bane, MD Melanoma Prognosis Survival at 10 years Stage I: 90% Stage II: 60% Stage III: 40% Stage IV: 10% 2 Indications
THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER
 Gynecologic Cancer InterGroup Cervix Cancer Research Network THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum
Gynecologic Cancer InterGroup Cervix Cancer Research Network THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum
Breast Cancer Immunotherapy. Leisha A. Emens, MD PhD Johns Hopkins University Bloomberg Kimmel Institute for Cancer Immunotherapy
 Breast Cancer Immunotherapy Leisha A. Emens, MD PhD Johns Hopkins University Bloomberg Kimmel Institute for Cancer Immunotherapy Conflict of Interest I have the following financial relationships to disclose:
Breast Cancer Immunotherapy Leisha A. Emens, MD PhD Johns Hopkins University Bloomberg Kimmel Institute for Cancer Immunotherapy Conflict of Interest I have the following financial relationships to disclose:
Slide 1. Slide 2. Slide 3. Immunotherapy in Lung Cancer. Disclosures. Objectives. No disclosures relevant to this talk
 Slide 1 Immunotherapy in Lung Cancer Lyudmila Bazhenova, MD Associate Clinical Professor, Moores UCSD Cancer Center Slide 2 Disclosures No disclosures relevant to this talk Slide 3 Objectives Review immune
Slide 1 Immunotherapy in Lung Cancer Lyudmila Bazhenova, MD Associate Clinical Professor, Moores UCSD Cancer Center Slide 2 Disclosures No disclosures relevant to this talk Slide 3 Objectives Review immune
Immunotherapy in Lung Cancer. Lyudmila Bazhenova, MD Associate Clinical Professor, Moores UCSD Cancer Center
 Immunotherapy in Lung Cancer Lyudmila Bazhenova, MD Associate Clinical Professor, Moores UCSD Cancer Center Disclosures No disclosures relevant to this talk Objectives Review immune pathways Immunology
Immunotherapy in Lung Cancer Lyudmila Bazhenova, MD Associate Clinical Professor, Moores UCSD Cancer Center Disclosures No disclosures relevant to this talk Objectives Review immune pathways Immunology
Understanding novel response patterns of immunotherapies Dr. Souhil Zaim, Chief Medical Officer, Median Technologies
 Imaging in immuno-oncology Understanding novel response patterns of immunotherapies Dr. Souhil Zaim, Chief Medical Officer, Median Technologies Contents 02 Introduction 03 History of Immunotherapy 06 The
Imaging in immuno-oncology Understanding novel response patterns of immunotherapies Dr. Souhil Zaim, Chief Medical Officer, Median Technologies Contents 02 Introduction 03 History of Immunotherapy 06 The
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Understanding Checkpoint Inhibitors: Approved Agents, Drugs in Development and Combination Strategies. Michael A. Curran, Ph.D.
 Understanding Checkpoint Inhibitors: Approved Agents, Drugs in Development and Combination Strategies Michael A. Curran, Ph.D. MD Anderson Cancer Center Department of Immunology Disclosures I have research
Understanding Checkpoint Inhibitors: Approved Agents, Drugs in Development and Combination Strategies Michael A. Curran, Ph.D. MD Anderson Cancer Center Department of Immunology Disclosures I have research
Immunotherapy for the Treatment of Melanoma. Marlana Orloff, MD Thomas Jefferson University Hospital
 Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
The oncology specific domains TU, TR and RS: What to know as a statistical analyst
 Your statistical health consultancy CHM staying healthy CRO getting healthy TEMP WORK team health The oncology specific domains TU, TR and RS: What to know as a statistical analyst PhUSE EU Connect 2018,
Your statistical health consultancy CHM staying healthy CRO getting healthy TEMP WORK team health The oncology specific domains TU, TR and RS: What to know as a statistical analyst PhUSE EU Connect 2018,
Engineered Immune Cells for Cancer Therapy : Current Status and Prospects
 When Engineering Meets Immunology Engineered Immune Cells for Cancer Therapy : Current Status and Prospects Yong Taik Lim, Ph.D. Nanomedical Systems Laboratory (http://www.nanomedicalsystems.org) SKKU
When Engineering Meets Immunology Engineered Immune Cells for Cancer Therapy : Current Status and Prospects Yong Taik Lim, Ph.D. Nanomedical Systems Laboratory (http://www.nanomedicalsystems.org) SKKU
Overview: Immunotherapy in CNS Metastases
 Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
Immunotherapy in non-small cell lung cancer
 Immunotherapy in non-small cell lung cancer Geoffrey Peters and Thomas John Olivia Newton-John Cancer Research Institute, Heidelberg, Victoria, Australia. Email: Geoffrey.peters@austin.org.au Abstract
Immunotherapy in non-small cell lung cancer Geoffrey Peters and Thomas John Olivia Newton-John Cancer Research Institute, Heidelberg, Victoria, Australia. Email: Geoffrey.peters@austin.org.au Abstract
KEYNOTE 695: TAVO Phase 2b Melanoma Trial Preliminary Data for SITC November 6, 2018
 KEYNOTE 695: TAVO Phase 2b Melanoma Trial Preliminary Data for SITC 2018 November 6, 2018 1 FORWARD-LOOKING STATEMENTS To the extent statements contained in the following presentations are not descriptions
KEYNOTE 695: TAVO Phase 2b Melanoma Trial Preliminary Data for SITC 2018 November 6, 2018 1 FORWARD-LOOKING STATEMENTS To the extent statements contained in the following presentations are not descriptions
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
The Galectin-3 Inhibitor GR-MD-02 for Combination Cancer Immunotherapy
 The Galectin-3 Inhibitor GR-MD-02 for Combination Cancer Immunotherapy Supplemental Information to Corporate Presentation February 6, 2018 NASDAQ: GALT www.galectintherapeutics.com 2018 2017 Galectin Therapeutics
The Galectin-3 Inhibitor GR-MD-02 for Combination Cancer Immunotherapy Supplemental Information to Corporate Presentation February 6, 2018 NASDAQ: GALT www.galectintherapeutics.com 2018 2017 Galectin Therapeutics
CRITICAL SUCCESS FACTORS FOR CLINICAL TRIALS OF IMMUNE CHECKPOINT INHIBITORS
 CRITICAL SUCCESS FACTORS FOR CLINICAL TRIALS OF IMMUNE CHECKPOINT INHIBITORS August 2015 Thomas Moehler, MD, PhD, Vice President, Medical & Scientific Affairs Cheryl Askew, PhD, Senior Director Sven Tang,
CRITICAL SUCCESS FACTORS FOR CLINICAL TRIALS OF IMMUNE CHECKPOINT INHIBITORS August 2015 Thomas Moehler, MD, PhD, Vice President, Medical & Scientific Affairs Cheryl Askew, PhD, Senior Director Sven Tang,
CA 125 definitions agreed by GCIG November 2005
 CA 125 definitions agreed by GCIG November 2005 The GCIG has agreed criteria for defining response and progression of ovarian carcinoma which use the serum marker CA 125, and the situations where these
CA 125 definitions agreed by GCIG November 2005 The GCIG has agreed criteria for defining response and progression of ovarian carcinoma which use the serum marker CA 125, and the situations where these
Disclosures Information Brendan D. Curti, MD
 The MITCI (Phase 1b) study: A novel immunotherapy combination of intralesional Coxsackievirus A21 and systemic ipilimumab in advanced melanoma patients with or without previous immune checkpoint therapy
The MITCI (Phase 1b) study: A novel immunotherapy combination of intralesional Coxsackievirus A21 and systemic ipilimumab in advanced melanoma patients with or without previous immune checkpoint therapy
irecist On behalf of the RECIST Working Group (RWG) and Immunotherapy Subcommittee
 and Immunotherapy Subcommittee") irecist A guideline for data management and data collection for trials testing immunotherapeutics Lesley Seymour MD, PhD Canadian Cancer Trials Group, Kingston, Ontario On behalf of the RECIST Working
irecist A guideline for data management and data collection for trials testing immunotherapeutics Lesley Seymour MD, PhD Canadian Cancer Trials Group, Kingston, Ontario On behalf of the RECIST Working
New Systemic Therapies in Advanced Melanoma
 New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
Immunotherapy for the Treatment of Cancer
 Immunotherapy for the Treatment of Cancer Jason Muhitch, PhD Assistant Professor Department of Urology Department of Immunology Roswell Park Comprehensive Cancer Center Oncology for Scientists March 15,
Immunotherapy for the Treatment of Cancer Jason Muhitch, PhD Assistant Professor Department of Urology Department of Immunology Roswell Park Comprehensive Cancer Center Oncology for Scientists March 15,
Cancer Immunotherapy Survey
 CHAPTER 8: Cancer Immunotherapy Survey All (N=100) Please classify your organization. Academic lab or center Small biopharmaceutical company Top 20 Pharma Mid-size pharma Diagnostics company Other (please
CHAPTER 8: Cancer Immunotherapy Survey All (N=100) Please classify your organization. Academic lab or center Small biopharmaceutical company Top 20 Pharma Mid-size pharma Diagnostics company Other (please
How to evaluate tumor response? Yonsei University College of Medicine Kim, Beom Kyung
 How to evaluate tumor response? Yonsei University College of Medicine Kim, Beom Kyung End points in research for solid cancers Overall survival (OS) The most ideal one, but requires long follow-up duration
How to evaluate tumor response? Yonsei University College of Medicine Kim, Beom Kyung End points in research for solid cancers Overall survival (OS) The most ideal one, but requires long follow-up duration
Ipilimumab ASCO Data Review and Discussion Webcast. Monday, June 2, 2008
 Ipilimumab ASCO Data Review and Discussion Webcast Monday, June 2, 2008 Slide 2 Forward Looking Statements Except for historical information, the matters contained in this slide presentation may constitute
Ipilimumab ASCO Data Review and Discussion Webcast Monday, June 2, 2008 Slide 2 Forward Looking Statements Except for historical information, the matters contained in this slide presentation may constitute
Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment
 Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment 1 Introductions Peter Langecker, MD, PhD Executive Medical Director, Global Oncology Clinipace Worldwide Mark Shapiro Vice President
Immune Checkpoint Inhibitors: The New Breakout Stars in Cancer Treatment 1 Introductions Peter Langecker, MD, PhD Executive Medical Director, Global Oncology Clinipace Worldwide Mark Shapiro Vice President
Welcome to the RECIST 1.1 Quick Reference
 Welcome to the RECIST 1.1 Quick Reference *Eisenhauer, E. A., et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur J Cancer 2009;45:228-47. Subject Eligibility
Welcome to the RECIST 1.1 Quick Reference *Eisenhauer, E. A., et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur J Cancer 2009;45:228-47. Subject Eligibility
Immunotherapy for the Treatment of Head and Neck Cancers. Barbara Burtness, MD Yale University
 Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
For personal use only
 The global leader in developing LAG-3 therapeutics BioCentury 25th Annual NewsMakers in the Biotech Industry Conference New York 7 th September 2018 (ASX: IMM, NASDAQ: IMMP) Notice: Forward Looking Statements
The global leader in developing LAG-3 therapeutics BioCentury 25th Annual NewsMakers in the Biotech Industry Conference New York 7 th September 2018 (ASX: IMM, NASDAQ: IMMP) Notice: Forward Looking Statements
Tumor Growth rates to better capture therapeutic activity in cancer patients
 Tumor Growth rates to better capture therapeutic activity in cancer patients Charles Ferté MD PhD Statistical and biomedical models for imaging in cancer Apr 2016, 8th - ISPED Serge Koscielny 2 Background
Tumor Growth rates to better capture therapeutic activity in cancer patients Charles Ferté MD PhD Statistical and biomedical models for imaging in cancer Apr 2016, 8th - ISPED Serge Koscielny 2 Background
Immuno-Oncology: Essentials for Nurses in Cancer Care
 Immuno-Oncology: Essentials for Nurses in Cancer Care BERNADINE O LEARY RN, MN, CON (C) CLINICAL EDUCATOR, EASTERN HEALTH CANCER CARE PROGRAM COURSE FACILITATOR- EASTERN HEALTH ADULT CHEMOTHERAPY COURSE
Immuno-Oncology: Essentials for Nurses in Cancer Care BERNADINE O LEARY RN, MN, CON (C) CLINICAL EDUCATOR, EASTERN HEALTH CANCER CARE PROGRAM COURSE FACILITATOR- EASTERN HEALTH ADULT CHEMOTHERAPY COURSE
RECIST 1.1 Criteria Handout. Medical Imaging. ICONplc.com/imaging
 RECIST 1.1 Criteria Handout Medical Imaging ICONplc.com/imaging 2 Contents Basic Paradigm 3 3 Image Acquisition 44 Measurable Lesions 55 Non-Measurable Lesions. 66 Special Lesion Types 77 Baseline Lesion
RECIST 1.1 Criteria Handout Medical Imaging ICONplc.com/imaging 2 Contents Basic Paradigm 3 3 Image Acquisition 44 Measurable Lesions 55 Non-Measurable Lesions. 66 Special Lesion Types 77 Baseline Lesion
ICLIO Webinar: Immuno-Oncology: From a Community Radiologist Perspective Michael J. DeLeo III, MD
 ICLIO Webinar: Immuno-Oncology: From a Community Radiologist Perspective Michael J. DeLeo III, MD Foundation Medical Partners Southern New Hampshire Health System December 1, 2016 accc-iclio.org Overview
ICLIO Webinar: Immuno-Oncology: From a Community Radiologist Perspective Michael J. DeLeo III, MD Foundation Medical Partners Southern New Hampshire Health System December 1, 2016 accc-iclio.org Overview
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy. What every patient needs to know. James Larkin
 Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Division of Hematology-Oncology, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, South Korea
 Antitumor Activity and Safety of FPA144, an ADCCenhanced, FGFR2b Isoform-Selective Monoclonal Antibody, in Patients with FGFR2b + Gastric Cancer and Advanced Solid Tumors Jeeyun Lee 1, Johanna Bendell
Antitumor Activity and Safety of FPA144, an ADCCenhanced, FGFR2b Isoform-Selective Monoclonal Antibody, in Patients with FGFR2b + Gastric Cancer and Advanced Solid Tumors Jeeyun Lee 1, Johanna Bendell
Immunotherapies. Supporting health professionals to safely care for patients receiving immunotherapy in the cancer setting.
 Immunotherapies Supporting health professionals to safely care for patients receiving immunotherapy in the cancer setting. INDEX Select a topic below for more information Principles of immunotherapy Classes
Immunotherapies Supporting health professionals to safely care for patients receiving immunotherapy in the cancer setting. INDEX Select a topic below for more information Principles of immunotherapy Classes
Checkpoint regulators a new class of cancer immunotherapeutics. Dr Oliver Klein Medical Oncologist ONJCC Austin Health
 Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Melanoma. Il parere dell esperto. V. Ferraresi. Divisione di Oncologia Medica 1
 Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Immunotherapy for Melanoma. Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center
 Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Emerging Strategies in Triple-Negative Breast Cancer
 Expert Review in Immunotherapy in Breast Cancer Emerging Strategies in Triple-Negative Breast Cancer Reference Slide Deck Is Breast Cancer Immunogenic? Recent proof that breast cancer may elicit an immune
Expert Review in Immunotherapy in Breast Cancer Emerging Strategies in Triple-Negative Breast Cancer Reference Slide Deck Is Breast Cancer Immunogenic? Recent proof that breast cancer may elicit an immune
Evan J. Lipson, M.D.
 Update on treatment for Merkel cell, cutaneous squamous cell and basal cell cancers Evan J. Lipson, M.D. The Johns Hopkins University School of Medicine Bloomberg~Kimmel Institute for Cancer Immunotherapy
Update on treatment for Merkel cell, cutaneous squamous cell and basal cell cancers Evan J. Lipson, M.D. The Johns Hopkins University School of Medicine Bloomberg~Kimmel Institute for Cancer Immunotherapy
Haemato-Oncology ESMO PRECEPTORSHIP PROGRAMME IMMUNO-ONCOLOGY. Development and clinical experience Monique Minnema, hematologist
 Haemato-Oncology ESMO PRECEPTORSHIP PROGRAMME IMMUNO-ONCOLOGY Development and clinical experience Monique Minnema, hematologist Consultancy for disclosures Amgen, Celgene, Jansen Cilag, BMS, Takeda Immune
Haemato-Oncology ESMO PRECEPTORSHIP PROGRAMME IMMUNO-ONCOLOGY Development and clinical experience Monique Minnema, hematologist Consultancy for disclosures Amgen, Celgene, Jansen Cilag, BMS, Takeda Immune
Innovation in Prevention, Early Detection & Diagnosis of Colorectal Cancer Heidelberg Workshop Session VI, Oncology Pipeline June 6, 2014
 Innovation in Prevention, Early Detection & Diagnosis of Colorectal Cancer Heidelberg Workshop Session VI, Oncology Pipeline June 6, 2014 Bernd Mueller MSD Sharp & Dohme, Germany Normal Immune Surveillance:
Innovation in Prevention, Early Detection & Diagnosis of Colorectal Cancer Heidelberg Workshop Session VI, Oncology Pipeline June 6, 2014 Bernd Mueller MSD Sharp & Dohme, Germany Normal Immune Surveillance:
Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment
 Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment Patrick Medina, Pharm.D., BCOP Professor The University of Oklahoma College of Medicine Stephenson Cancer Center Faculty Disclosure
Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment Patrick Medina, Pharm.D., BCOP Professor The University of Oklahoma College of Medicine Stephenson Cancer Center Faculty Disclosure
Cytokines: Interferons, Interleukins and Beyond. Michael B. Atkins, MD Georgetown-Lombardi Comprehensive Cancer Center
 Cytokines: Interferons, Interleukins and Beyond Michael B. Atkins, MD Georgetown-Lombardi Comprehensive Cancer Center Disclosures Advisory Boards: Bristol-Myers Squibb,Amgen, Novartis, Alkermes, Infinity,
Cytokines: Interferons, Interleukins and Beyond Michael B. Atkins, MD Georgetown-Lombardi Comprehensive Cancer Center Disclosures Advisory Boards: Bristol-Myers Squibb,Amgen, Novartis, Alkermes, Infinity,
Checkpoint Regulators Cancer Immunotherapy takes centre stage. Dr Oliver Klein Department of Medical Oncology 02 May 2015
 Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
IMMUNOTARGET THERAPY: ASPETTI GENERALI
 IMMUNOTARGET THERAPY: ASPETTI GENERALI Alessandro Minisini Dipartimento di Oncologia Azienda Ospedaliero Universitaria Udine Verona, 19 settembre 2015 HALLMARKS OF CANCER Douglas Hanahan, Robert A. Weinberg,
IMMUNOTARGET THERAPY: ASPETTI GENERALI Alessandro Minisini Dipartimento di Oncologia Azienda Ospedaliero Universitaria Udine Verona, 19 settembre 2015 HALLMARKS OF CANCER Douglas Hanahan, Robert A. Weinberg,
NewLink Genetics Corporation
 Cantor Fitzgerald Global Healthcare Conference NewLink Genetics Corporation NASDAQ: NLNK September 25, 2017 Forward-Looking Disclaimer This presentation contains forward-looking statements of NewLink that
Cantor Fitzgerald Global Healthcare Conference NewLink Genetics Corporation NASDAQ: NLNK September 25, 2017 Forward-Looking Disclaimer This presentation contains forward-looking statements of NewLink that
Coxsackievirus A21: The basic facts
 Phase II CALM Extension study: Intratumoral CAVATAK TM increases immune- cell infiltrates and up- regulates immune- checkpoint molecules in the microenvironment of lesions from advanced melanoma padents
Phase II CALM Extension study: Intratumoral CAVATAK TM increases immune- cell infiltrates and up- regulates immune- checkpoint molecules in the microenvironment of lesions from advanced melanoma padents
Immuno-Oncology Therapies and Precision Medicine: Personal Tumor-Specific Neoantigen Prediction by Machine Learning
 Immuno-Oncology Therapies and Precision Medicine: Personal Tumor-Specific Neoantigen Prediction by Machine Learning Yi-Hsiang Hsu, MD, SCD Sep 16, 2017 yihsianghsu@hsl.harvard.edu HSL GeneticEpi Center,
Immuno-Oncology Therapies and Precision Medicine: Personal Tumor-Specific Neoantigen Prediction by Machine Learning Yi-Hsiang Hsu, MD, SCD Sep 16, 2017 yihsianghsu@hsl.harvard.edu HSL GeneticEpi Center,
A Phase 2 Study of Glembatumumab Vedotin, an Antibody Drug Conjugate Targeting gpnmb, in Advanced Melanoma
 A Phase 2 Study of Glembatumumab Vedotin, an Antibody Drug Conjugate Targeting gpnmb, in Advanced Melanoma Patrick A. Ott, MD, PhD 1, Anna C. Pavlick, DO 2, Douglas B. Johnson, MD 3, Lowell Hart, MD 4,
A Phase 2 Study of Glembatumumab Vedotin, an Antibody Drug Conjugate Targeting gpnmb, in Advanced Melanoma Patrick A. Ott, MD, PhD 1, Anna C. Pavlick, DO 2, Douglas B. Johnson, MD 3, Lowell Hart, MD 4,
IMMUNOTHERAPY FOR CANCER A NEW HORIZON. Ekaterini Boleti MD, PhD, FRCP Consultant in Medical Oncology Royal Free London NHS Foundation Trust
 IMMUNOTHERAPY FOR CANCER A NEW HORIZON Ekaterini Boleti MD, PhD, FRCP Consultant in Medical Oncology Royal Free London NHS Foundation Trust ASCO Names Advance of the Year: Cancer Immunotherapy No recent
IMMUNOTHERAPY FOR CANCER A NEW HORIZON Ekaterini Boleti MD, PhD, FRCP Consultant in Medical Oncology Royal Free London NHS Foundation Trust ASCO Names Advance of the Year: Cancer Immunotherapy No recent
Immunotherapy for Metastatic Malignant Melanoma. Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg
 Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Interleukin-2 Single Agent and Combinations
 Interleukin-2 Single Agent and Combinations Michael K Wong MD PhD Norris Cancer Center University of Southern California mike.wong@med.usc.edu Disclosures Advisory Board Attendance Merck Bristol Myers
Interleukin-2 Single Agent and Combinations Michael K Wong MD PhD Norris Cancer Center University of Southern California mike.wong@med.usc.edu Disclosures Advisory Board Attendance Merck Bristol Myers
MEASUREMENT OF EFFECT SOLID TUMOR EXAMPLES
 MEASUREMENT OF EFFECT SOLID TUMOR EXAMPLES Although response is not the primary endpoint of this trial, subjects with measurable disease will be assessed by standard criteria. For the purposes of this
MEASUREMENT OF EFFECT SOLID TUMOR EXAMPLES Although response is not the primary endpoint of this trial, subjects with measurable disease will be assessed by standard criteria. For the purposes of this
Immunotherapy for the Treatment of Brain Metastases
 Society for Immunotherapy of Cancer (SITC) Immunotherapy for the Treatment of Brain Metastases Lawrence G. Lum, MD, DSc Karmanos Cancer Institute and Wayne State University Advances in Cancer Immunotherapy
Society for Immunotherapy of Cancer (SITC) Immunotherapy for the Treatment of Brain Metastases Lawrence G. Lum, MD, DSc Karmanos Cancer Institute and Wayne State University Advances in Cancer Immunotherapy
Endogenous and Exogenous Vaccination in the Context of Immunologic Checkpoint Blockade
 Endogenous and Exogenous Vaccination in the Context of Immunologic Checkpoint Blockade Jedd Wolchok Ludwig Center for Cancer Immunotherapy Memorial Sloan-Kettering Cancer Center MEMORIAL SLOAN- KETTERING
Endogenous and Exogenous Vaccination in the Context of Immunologic Checkpoint Blockade Jedd Wolchok Ludwig Center for Cancer Immunotherapy Memorial Sloan-Kettering Cancer Center MEMORIAL SLOAN- KETTERING
immunotherapy a guide for the patient
 immunotherapy FOR LUNG CANCER a guide for the patient TABLE OF CONTENTS lung cancer basics... 2 immunotherapy... 5 Checkpoint Inhibitors... 6-9 Monoclonal Antibodies... 9 Vaccines... 10 Adoptive T-Cell
immunotherapy FOR LUNG CANCER a guide for the patient TABLE OF CONTENTS lung cancer basics... 2 immunotherapy... 5 Checkpoint Inhibitors... 6-9 Monoclonal Antibodies... 9 Vaccines... 10 Adoptive T-Cell
Mind the Gap : Challenges in First-in- Man Evaluation of Immuno-Oncology Drugs
 Mind the Gap : Challenges in First-in- Man Evaluation of Immuno-Oncology Drugs Ignacio Garcia-Ribas MD, PhD Senior Medical Director Early Clinical Research & Development, Oncology Therapeutic Area Takeda
Mind the Gap : Challenges in First-in- Man Evaluation of Immuno-Oncology Drugs Ignacio Garcia-Ribas MD, PhD Senior Medical Director Early Clinical Research & Development, Oncology Therapeutic Area Takeda
Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3
 ESMO 2016 Congress 7-11 October, 2016 Copenhagen, Denmark Table of Contents Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3 Long-term results show adjuvant therapy with ipilimumab improves OS in high
ESMO 2016 Congress 7-11 October, 2016 Copenhagen, Denmark Table of Contents Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3 Long-term results show adjuvant therapy with ipilimumab improves OS in high
Durable Response Rate in High Grade Glioma: an Emerging Endpoint for Immunotherapeutics. Timothy Cloughesy, MD University of California, Los Angeles
 Durable Response Rate in High Grade Glioma: an Emerging Endpoint for Immunotherapeutics Timothy Cloughesy, MD University of California, Los Angeles Disclosure 2 FDA Endpoints for the Approval of Cancer
Durable Response Rate in High Grade Glioma: an Emerging Endpoint for Immunotherapeutics Timothy Cloughesy, MD University of California, Los Angeles Disclosure 2 FDA Endpoints for the Approval of Cancer
Heme Onc Today New York Melanoma Meeting March 22-23, 2013 PD-1 antibodies
 Heme Onc Today New York Melanoma Meeting March 22-23, 2013 PD-1 antibodies Jeffrey Weber Moffitt Cancer Center Tampa, FL Disclosures I have consulted for BMS, Merck, Genentech and GSK for Ad Boards and
Heme Onc Today New York Melanoma Meeting March 22-23, 2013 PD-1 antibodies Jeffrey Weber Moffitt Cancer Center Tampa, FL Disclosures I have consulted for BMS, Merck, Genentech and GSK for Ad Boards and
Update on Immunotherapy in Advanced Melanoma. Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017
 Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
Developing Novel Immunotherapeutic Cancer Treatments for Clinical Use
 Developing Novel Immunotherapeutic Cancer Treatments for Clinical Use Oncology for Scientists March 8 th, 2016 Jason Muhitch, PhD Assistant Professor Department of Urology Email: jason.muhitch@roswellpark.org
Developing Novel Immunotherapeutic Cancer Treatments for Clinical Use Oncology for Scientists March 8 th, 2016 Jason Muhitch, PhD Assistant Professor Department of Urology Email: jason.muhitch@roswellpark.org
Renal Cell Carcinoma: Systemic Therapy Progress and Promise
 Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Management of Brain Metastases Sanjiv S. Agarwala, MD
 Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
New paradigms for treating metastatic melanoma
 New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
Immuno-Oncology Therapies and Precision Medicine: Personal Tumor-Specific Neoantigen Prediction by Machine Learning
 Immuno-Oncology Therapies and Precision Medicine: Personal Tumor-Specific Neoantigen Prediction by Machine Learning Yi-Hsiang Hsu, MD, SCD Sep 16, 2017 yihsianghsu@hsl.harvard.edu Director & Associate
Immuno-Oncology Therapies and Precision Medicine: Personal Tumor-Specific Neoantigen Prediction by Machine Learning Yi-Hsiang Hsu, MD, SCD Sep 16, 2017 yihsianghsu@hsl.harvard.edu Director & Associate
MELANOMA METASTASICO: NUEVAS COMBINACIONES. Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona
 MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
(generic name: ipilimumab) Injection 50 mg ( Yervoy ), a human anti-human CTLA-4 monoclonal. August 21, 2018
 Injection 50 mg ( Yervoy ), a human anti-human CTLA-4 monoclonal. August 21, 2018") August 21, 2018 Opdivo Approved for Supplemental Applications for Expanded Indications of Malignant Pleural Mesothelioma and Adjuvant Treatment of Melanoma, Change in Dosage and Administration (D&A) of
August 21, 2018 Opdivo Approved for Supplemental Applications for Expanded Indications of Malignant Pleural Mesothelioma and Adjuvant Treatment of Melanoma, Change in Dosage and Administration (D&A) of
Cancer Immunotherapy Future from the Past?
 Disclaimer This talk is intended for educational value, and includes comments on unlicensed drugs. Please liaise with a specialist if you have a clinical query. Cancer Immunotherapy Future from the Past?
Disclaimer This talk is intended for educational value, and includes comments on unlicensed drugs. Please liaise with a specialist if you have a clinical query. Cancer Immunotherapy Future from the Past?
ONO PHARMACEUTICAL CO., LTD. and Bristol-Myers Squibb Announce Strategic Immuno-Oncology Collaboration in Japan, South Korea and Taiwan
 ONO PHARMACEUTICAL CO., LTD. and Bristol-Myers Squibb Announce Strategic Immuno-Oncology Collaboration in Japan, South Korea and Taiwan Companies to develop and commercialize Opdivo (nivolumab), ipilimumab,
ONO PHARMACEUTICAL CO., LTD. and Bristol-Myers Squibb Announce Strategic Immuno-Oncology Collaboration in Japan, South Korea and Taiwan Companies to develop and commercialize Opdivo (nivolumab), ipilimumab,
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD
 Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Happy New Year in 2017!!! Year of Rooster
 Happy New Year in 2017!!! Year of Rooster 1957 1969 1981 1993 2005 2017 The Agenda Introduction of Oncology Why Standards? Oncology-specific Standards: Response Criteria guideline and CDISC Standards-driven
Happy New Year in 2017!!! Year of Rooster 1957 1969 1981 1993 2005 2017 The Agenda Introduction of Oncology Why Standards? Oncology-specific Standards: Response Criteria guideline and CDISC Standards-driven
Tumor Immunology: A Primer
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Novel RCC Targets from Immuno-Oncology and Antibody-Drug Conjugates
 Novel RCC Targets from Immuno-Oncology and Antibody-Drug Conjugates Christopher Turner, MD Vice President, Clinical Science 04 November 2016 Uveal Melanoma Celldex Pipeline CANDIDATE INDICATION Preclinical
Novel RCC Targets from Immuno-Oncology and Antibody-Drug Conjugates Christopher Turner, MD Vice President, Clinical Science 04 November 2016 Uveal Melanoma Celldex Pipeline CANDIDATE INDICATION Preclinical
Immunotherapies in melanoma: regulatory perspective. Jorge Camarero (AEMPS)
") Immunotherapies in melanoma: regulatory perspective Jorge Camarero (AEMPS) Challenges for the approval of anti-cancer immunotherapeutic drugs EMA-CDDF joint meeting, London 4-5 February 2016 disclaimers
Immunotherapies in melanoma: regulatory perspective Jorge Camarero (AEMPS) Challenges for the approval of anti-cancer immunotherapeutic drugs EMA-CDDF joint meeting, London 4-5 February 2016 disclaimers
Immunotherapy for dmmr metastatic colorectal cancer. Prof.dr. Kees Punt Dept. Medical Oncology AUMC
 Immunotherapy for dmmr metastatic colorectal cancer Prof.dr. Kees Punt Dept. Medical Oncology AUMC Active specific immunotherapy (ASI) in stage II-III colon cancer Vaccination with autologous tumor + BCG
Immunotherapy for dmmr metastatic colorectal cancer Prof.dr. Kees Punt Dept. Medical Oncology AUMC Active specific immunotherapy (ASI) in stage II-III colon cancer Vaccination with autologous tumor + BCG
Priming the Immune System to Kill Cancer and Reverse Tolerance. Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics
 Priming the Immune System to Kill Cancer and Reverse Tolerance Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics Learning Objectives Describe the role of the immune system in cancer
Priming the Immune System to Kill Cancer and Reverse Tolerance Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics Learning Objectives Describe the role of the immune system in cancer
ONCOS-102 in melanoma Dr. Alexander Shoushtari. 4. ONCOS-102 in mesothelioma 5. Summary & closing
 ONCOS-102 in melanoma Dr. Alexander Shoushtari 4. ONCOS-102 in mesothelioma 5. Summary & closing 1 Preliminary data from C824 Activating the Alexander Shoushtari, MD Assistant Attending Physician Melanoma
ONCOS-102 in melanoma Dr. Alexander Shoushtari 4. ONCOS-102 in mesothelioma 5. Summary & closing 1 Preliminary data from C824 Activating the Alexander Shoushtari, MD Assistant Attending Physician Melanoma