ACTIVE SURVEILLANCE FOR RENAL MASSES: Where are we in 2016?
|
|
|
- Victor Merritt
- 6 years ago
- Views:
Transcription

1 ACTIVE SURVEILLANCE FOR RENAL MASSES: Where are we in 2016? Phillip M. Pierorazio, MD Assistant Professor of Urology and Oncology Brady Urological Institute Sidney Kimmel Cancer Center Johns Hopkins Hospital Baltimore, Maryland Fifteenth International Kidney Cancer Symposium November 4-5, 2016 Marriott Miami Biscayne Bay, Miami, Florida, USA
 Young Investigator s Award: Delayed Intervention and")
 Funded Investigator Management of Renal")

2 disclosures American Urological Association Kidney Cancer Guideline Committee National Comprehensive Cancer Network (NCCN) Young Investigator s Award: Delayed Intervention and Surveillance for Small Renal Masses (DISSRM) Registry Kidney Cancer Guidelines Committee Agency for Healthcare Research and Quality (AHRQ) Funded Investigator Management of Renal Masses and Localized Renal Cancer Myriad Genetics Kidney Cancer Advisory Board (unpaid) No relevant financial relationships to disclose. No non-fda approved use of drugs or products discussed in this presentation.
3 outline/objectives To review oncologic data from active surveillance (AS) programs. Practical considerations from an AS program. Imaging, growth rates and progression. To discuss the utility of renal mass biopsy in active surveillance. Quality of life
4 Fifteenth International Kidney Cancer Symposium November 4-5, 2016 Marriott Miami Biscayne Bay, Miami, Florida, USA oncologic data ACTIVE SURVEILLANCE FOR RENAL MASSES









 Overall")
5 ACTIVE SURVEILLANCE LITERATURE Systematic Review Medline, Embase, Cochrane Reviews: 73 peer-reviewed articles 24 original series 2 prospective cohorts Patients: 1,795 ( per study) At median follow-up (21-92 months), median: Cancer-specific survival: 100% ( %) Metastasis-free survival: 98.9% (86.2%-100%) Overall survival: 88.8% (42.8%-100%) Johnson and Pierorazio. ACAM, in submission.

6 underutilization of active surveillance Yang et al. BJU International, Volume 110, Issue 8, pages , 28 FEB 2012 DOI: /j X x Smaldone et al. Urology, 2013.
![active surveillance guideline statements AUA Guidelines [AS] is a reasonable option](/docs-images/72/67167742/images/7-2.jpg "for patients with limited life expectancy or for those who are unfit for or do not")


7 active surveillance guideline statements AUA Guidelines [AS] is a reasonable option for patients with limited life expectancy or for those who are unfit for or do not desire surgery. Patients should be willing to assume an unknown, but low, oncologic risk associated with AS. EAU Guidelines that elderly and comorbid patients with incidentally discovered [SRM] are suitable for AS based on low cancer-specific mortality and significant competing-risk mortality. NCCN AS is suitable for select patients with T1a tumors.
8 PROSPECTIVE TRIALS OF ACTIVE SURVEILLANCE Renal Cell Consortium of Canada (RCCC) Delayed Intervention and Surveillance for Small Renal Masses (DISSRM) Region Canada United States Number of centers 8 3 Start of enrollment Year of last published results Eligibility criteria ct1an0m0 mass on imaging Deemed not fit for surgery 18 years or older, ct1an0m0 mass on imaging no personal history of RCC or a known familial RCC syndrome Study arms Active Surveillance only Active Surveillance, Primary and Delayed Intervention Renal Mass Biopsy (%) Recommended (55.6%) Tumors that are benign on biopsy are followed yearly. Offered (6.4%) Biopsy results do not change surveillance protocol. Surveillance protocol CT, MRI, or ultrasound at 3 and 6 months, then every 6 months until year 3, and then yearly. Ultrasound (recommended; or CT, or MRI) every 6 months for the first 2 years and every 1 year thereafter. Definition of local progression Tumor diameter of 4 cm or greater, or Doubling of tumor volume in 12 or fewer months Maximum diameter larger than 4.0 cm, Growth rate that exceeds 0.5 cm/year, Hematuria (or symptoms) suspected to be from the SRM Number of patients in last published results 178 (AS only) PI: 274 AS: 223 (of which 21 undergo DI) Follow-up period in last 28 (mean) 25 (median) published results (months) Tumor growth rate in last 0.13 (mean) 0.11 (median) published results (cm/year) Rate of local progression of 12% 16% AS arm in last published results (%) Rate of metastatic disease Active Surveillance: 1.1% AS arm: 0% PI arm: 0.7% DI arm: 0% in last published results (%) Survival outcomes Not reported 5-year OS for PI=92%; AS=75% 5-year CSS for PI=99%; AS=100%
 Beth Israel Deaconess (Wagner) Primary Objective: Non-inferiority of AS based on historical 5 year CSS rates")
9 Opened: January 1, 2009 Prospective Registry Solid, ct1a (4cm) tumors Multi-institutional: Johns Hopkins Columbia Univ. (McKiernan) Beth Israel Deaconess (Wagner) Primary Objective: Non-inferiority of AS based on historical 5 year CSS rates (95%).
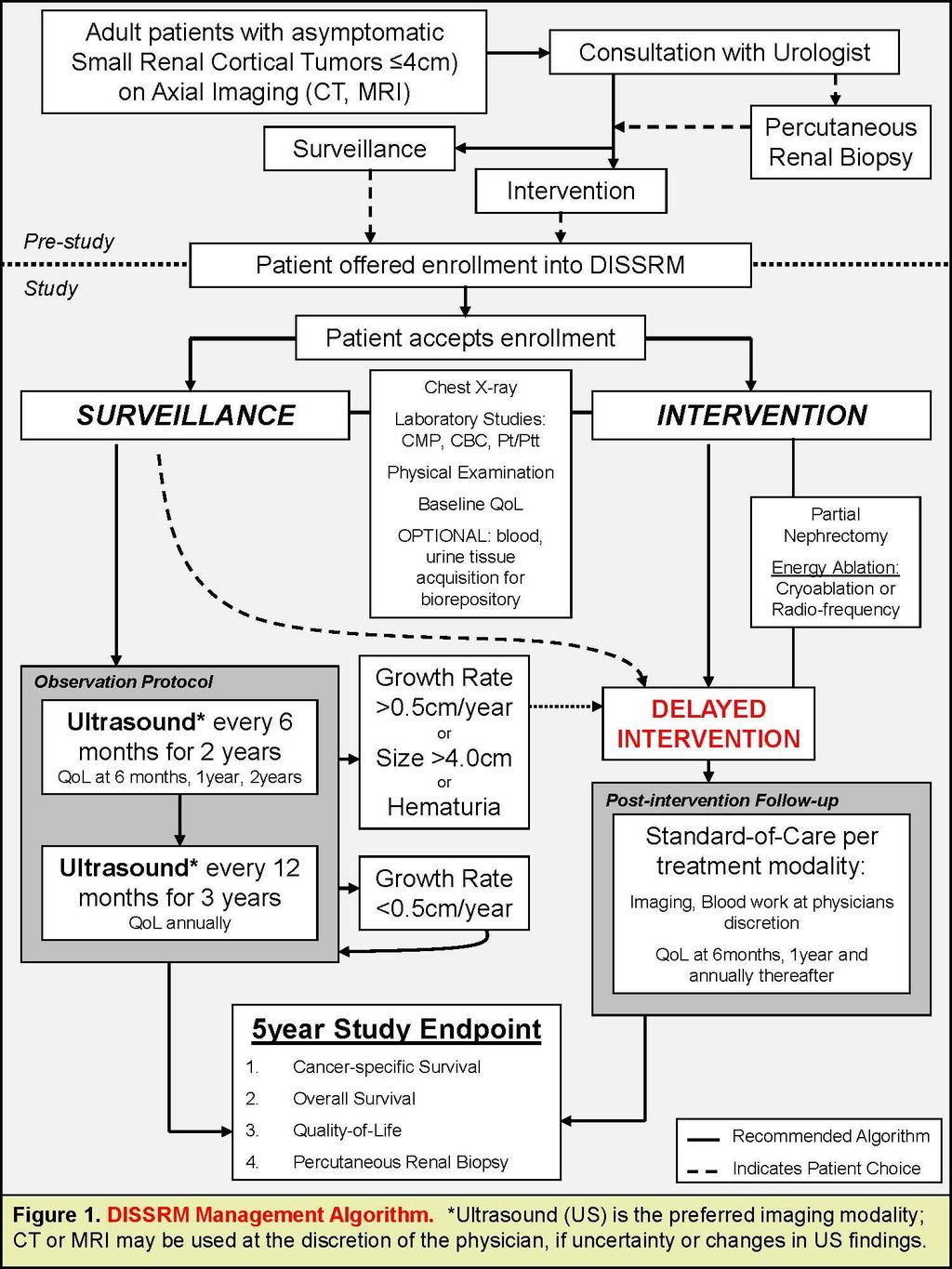
10 DISSRM: vital statistics, October 1, patients 3.01 years [IQR: ] median follow-up Primary Intervention: n=255 Active Surveillance: n=288 Crossover: n=45 Surveillance patients are: Older: 70.8 v (P<0.001) Worse Health: ECOG 2-4: 5.8% v. 2.5% (P=0.045) Charlson 0: 43.5% v. 60.1% (P<0.001) Smaller tumors: 1.8 [ ] vs. 2.5 [ ] (P<0.001) More complex tumors: 40.9% vs. 32.8% (P=0.1) intermediate- to high-renal score
11
12
13 Progression: Growth Rate >0.5cm/year (n=64) Tumor > 4cm (n=6) Metastatic Disease (n=0) Crossover (n=45)
14 active surveillance oncologic outcomes Active surveillance remains underutilized. Intermediate-term, oncologic outcomes indicate active surveillance is non-inferior to primary intervention. Cancer-specific survival is excellent. Metastases-free survival is excellent.
15 Fifteenth International Kidney Cancer Symposium November 4-5, 2016 Marriott Miami Biscayne Bay, Miami, Florida, USA practical considerations ACTIVE SURVEILLANCE FOR RENAL MASSES
16

17 imaging modality in DISSRM 197 (62.5%) 84 (26.7%) 34 (10.8%) 387 (42.3%) 197 (24.5%) 331 (36.2%) Surveillance protocol: Renal mass imaging every 6 months for 2 years, annually thereafter. Axial imaging required within 6 months. Annual chest imaging, complete metabolic panel. Ultrasound is the preferred surveillance modality. Active surveillance can/should be highly individualized. Variable time intervals are reasonable based on patient/tumor risk stratification. Alternating axial imaging for surgical candidates.
18 Tumor Size (cm) growth rates in active surveillance Overall Growth Rate (n=251) Median: 0.09 cm/year (IQR, to 0.31) Time (Years)
19 Grwoth Rate (cm/year) growth rates in active surveillance Waterfall Plot of Overall Tumor Growth Rates 30.8% <0 cm/year in % 0 cm/year in % cm/year 20.8% >0.5 cm/year in 33
20 growth rates in active surveillance Growth of SRMs in AS Patients Time Mean GR (cm/year) SD 6 months 0.22 ± months 0.12 ± months 0.13 ± months 0.09 ±0.25 Growth Time (Years) Variability in growth rate is high within the first year of imaging and decreases with longer follow-up. Avoid intervention. Consider renal mass biopsy.
21 Tumor Size (cm) growth rates in active surveillance Overall Growth Rate (n=251) Median: 0.09 cm/year (IQR, to 0.31) Most growing tumors demonstrate non-linear growth Time (Years)
22 positive growth periods by pathology Benign, chromophobe & low grade, pt1-2 High grade or pt3 (and above) Favorable 86 (69.4%) Unfavorable 38 (30.6%) # % # % % % % % % % % 3 7.9% 4 0 0% 2 5.3% Number of positive growth periods was positively correlated with unfavorable pathology. Overall growth rate (mean[sd] cm/year) 0.7[1.7] vs 1.6[2.8], p=0.07 Cochran-Armitage trend test (p=0.02) Somers D (0.15, 95%CI[0.02, 0.29])
23 rethinking progression 30% of patients progress by 7 years. Growth rate >0.5cm/year (n=64) Delayed intervention (n=45) Most (75%) are elective crossovers Tumor size >4cm (n=6) Metastatic disease (n=0) no deaths Oncologic outcomes are driven by tumor stage, size. Growth rate is a poor predictor of malignant potential. Grade and stage reclassification? Persistent growth?
24 practical considerations Surveillance can/should be highly individualized. Ultrasound is preferred imaging modality. Most SRM will grow slowly (or not at all). Traditional thoughts about progression while on active surveillance are challenged by contemporary data. Growth rate within the first year (especially 6 months) is a highly variable. Unreliable predictor of overall growth rate. Tumor size and stage drive cancer-specific survival. Growth rate is a likely adjunct to tumor size. Persistent growth versus linear growth rate
25 Fifteenth International Kidney Cancer Symposium November 4-5, 2016 Marriott Miami Biscayne Bay, Miami, Florida, USA role of renal mass biopsy ACTIVE SURVEILLANCE FOR RENAL MASSES
26 systematic review: percutaneous renal biopsy 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% Performance Characteristics 97.5% 96.2% 99.8% Sensitvity Specificity Positive Predictive Value 68.5% Negative Predictive Value 14% Non-Diagnostic Rate Lower limit of Negative Predictive Value as all patients in this series underwent extirpation. Moderate level of evidence. Histology: 90% concordance Grade (14 studies, 688 tumors) 87.8% low-grade tumors 16.0% upgraded 50% for high-grade tumors


27 Only 40% of high-grade tumors are grade 3-4. Tumor Heterogeneity
28 renal mass biopsy in DISSRM Year Active Surveillance Intervention Crossover / 543 (16.8%) 45 / 288 (15.6%) 34 / 255 (13.3%) 12 / 45 (26.7%) 5%
29 renal mass biopsy in AS Renal mass biopsy is not a requisite for safe active surveillance. A well-informed consultation regarding the risk-stratification of a given patient s renal mass can help decide if/when RMB is useful. Specific roles for RMB: Young women with masses <2cm who desire surgery Growing mass on AS SRM considering radical nephrectomy Patients who want more information Gray zone patients
30 Fifteenth International Kidney Cancer Symposium November 4-5, 2016 Marriott Miami Biscayne Bay, Miami, Florida, USA quality of life ACTIVE SURVEILLANCE FOR RENAL MASSES
31 Quality of Life favors primary intervention patients Driven by perceived differences in physical health, not mental health domains Patel, et al
32 Mental (emotional) quality of life improves for all patients Patel, et al Patel, et al. JUROL, 2016.
33 active surveillance for renal masses where are we in 2016? Prospective data supports active surveillance as a safe, non-inferior management strategy for patients with ct1a (<4cm) tumors. Imaging intervals/modalities should be individualized. Ultrasound is the preferred AS modality. Alternating axial imaging for surgical candidates. Short-term growth rates are unreliable predictors of malignant potential. Overall tumor size is our best predictor of outcome. Intervention should not be based on GR in 1 st year. Consistent growth may indicate malignant potential. Renal mass biopsy has a role, but is not essential for AS. Quality of life is preserved (perhaps improved) in a structured AS program.









34 Mohamad Allaf, MD Michael Gorin, MD Michael Johnson, MD Mark Riffon, MPH Heather Gausepohl, NP Tina Driscoll Hiten Patel, MD Alice Semerjian, MD Alex Jang Ridwan Alam JHH kidney cancer team
RENAL CANCER. Dr. Giandomenico Roviello. Oncologia Medica Ospedale San Donato Arezzo
 RENAL CANCER Dr. Giandomenico Roviello Oncologia Medica Ospedale San Donato Arezzo Abstracts Abstract Number: 433. Cryoablation of ct1 renal masses in the healthy patient: Early outcomes from Mayo Clinic.
RENAL CANCER Dr. Giandomenico Roviello Oncologia Medica Ospedale San Donato Arezzo Abstracts Abstract Number: 433. Cryoablation of ct1 renal masses in the healthy patient: Early outcomes from Mayo Clinic.
Contemporary Role of Renal Mass Biopsy
 Contemporary Role of Renal Mass Biopsy Jeffrey K. Mullins, MD Director Urologic Oncology CHI Memorial Chattanooga Urology Associates September 8, 2018 Disclosures I, Jeffrey Mullins, do not have a financial
Contemporary Role of Renal Mass Biopsy Jeffrey K. Mullins, MD Director Urologic Oncology CHI Memorial Chattanooga Urology Associates September 8, 2018 Disclosures I, Jeffrey Mullins, do not have a financial
Renal Mass Biopsy: Needed Now More than Ever
 Renal Mass Biopsy: Needed Now More than Ever Stuart G. Silverman, MD, FACR Professor of Radiology Harvard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Boston,
Renal Mass Biopsy: Needed Now More than Ever Stuart G. Silverman, MD, FACR Professor of Radiology Harvard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Boston,
Phase 3 Perioperative Nivolumab in M0 RCC (PROSPER RCC, ECOG ACRIN 8143) A UROLOGIST S PERSPECTIVE
 A UROLOGIST S PERSPECTIVE") Phase 3 Perioperative Nivolumab in M0 RCC (PROSPER RCC, ECOG ACRIN 8143) A UROLOGIST S PERSPECTIVE Mohamad E. Allaf, MD Associate Professor of Urology, Oncology, & BME MEA Endowed Director, Minimally Invasive
Phase 3 Perioperative Nivolumab in M0 RCC (PROSPER RCC, ECOG ACRIN 8143) A UROLOGIST S PERSPECTIVE Mohamad E. Allaf, MD Associate Professor of Urology, Oncology, & BME MEA Endowed Director, Minimally Invasive
Surveillance Strategies in Kidney Cancer: When is Enough? Role of Survivorship Clinic in Long-Term Follow-Up of Kidney Cancer
 Surveillance Strategies in Kidney Cancer: When is Enough? Role of Survivorship Clinic in Long-Term Follow-Up of Kidney Cancer Brandon Manley, MD Assistant Member, Genitourinary Oncology Department of Genitourinary
Surveillance Strategies in Kidney Cancer: When is Enough? Role of Survivorship Clinic in Long-Term Follow-Up of Kidney Cancer Brandon Manley, MD Assistant Member, Genitourinary Oncology Department of Genitourinary
AUA Guidelines Renal Mass and Localized Kidney Cancer
 AUA Guidelines Renal Mass and Localized Kidney Cancer Steven C. Campbell, MD, PhD Chair AUA Guidelines Panel Professor Surgery, Vice Chair, Program Director Department of Urology Glickman Urological and
AUA Guidelines Renal Mass and Localized Kidney Cancer Steven C. Campbell, MD, PhD Chair AUA Guidelines Panel Professor Surgery, Vice Chair, Program Director Department of Urology Glickman Urological and
RCC in Adolescents and Young Adults (AYAs): Diagnosis and Management
: Diagnosis and Management") RCC in Adolescents and Young Adults (AYAs): Diagnosis and Management Nicholas G. Cost, M.D. Assistant Professor, Department of Surgery, Division of Urology University of Colorado Cancer Center Fifteenth
RCC in Adolescents and Young Adults (AYAs): Diagnosis and Management Nicholas G. Cost, M.D. Assistant Professor, Department of Surgery, Division of Urology University of Colorado Cancer Center Fifteenth
WHAT IS THE ROLE OF ACTIVE SURVEILLANCE
 WHAT IS THE ROLE OF ACTIVE SURVEILLANCE IN THE CONTEXT OF RENAL ABLATION AND PARTIAL NEPHRECTOMY? Alessandro Volpe University of Eastern Piedmont Novara, Italy RCC INCIDENCE SEER DATABASE (1975-2006) RCC
WHAT IS THE ROLE OF ACTIVE SURVEILLANCE IN THE CONTEXT OF RENAL ABLATION AND PARTIAL NEPHRECTOMY? Alessandro Volpe University of Eastern Piedmont Novara, Italy RCC INCIDENCE SEER DATABASE (1975-2006) RCC
Clinical Stage Migration and Survival for Renal Cell Carcinoma in the United States
 ava ilable at www.sciencedirect.com journa l homepage: euoncology.europeanurology.com Clinical Stage Migration and Survival for Renal Cell Carcinoma in the United States Hiten D. Patel *, Mohit Gupta,
ava ilable at www.sciencedirect.com journa l homepage: euoncology.europeanurology.com Clinical Stage Migration and Survival for Renal Cell Carcinoma in the United States Hiten D. Patel *, Mohit Gupta,
Renal Mass Biopsy Should be Used for Most SRM - PRO
 Renal Mass Biopsy Should be Used for Most SRM - PRO Tony Finelli, MD, MSc, FRCSC Head, Division of Urology GU Site Lead, Princess Margaret Cancer Center GU Cancer Lead, Cancer Care Ontario Associate Professor,
Renal Mass Biopsy Should be Used for Most SRM - PRO Tony Finelli, MD, MSc, FRCSC Head, Division of Urology GU Site Lead, Princess Margaret Cancer Center GU Cancer Lead, Cancer Care Ontario Associate Professor,
Canadian Urological Association guidelines for followup of patients after treatment of nonmetastatic
 Canadian Urological Association guidelines for followup of patients after treatment of nonmetastatic renal cell carcinoma Wassim Kassouf, Leonardo L. Monteiro, Darrel E. Drachenberg, Adrian S. Fairey,
Canadian Urological Association guidelines for followup of patients after treatment of nonmetastatic renal cell carcinoma Wassim Kassouf, Leonardo L. Monteiro, Darrel E. Drachenberg, Adrian S. Fairey,
Renal biopsy is mandatory for every small renal mass
 Renal biopsy is mandatory for every small renal mass Ben Challacombe Consultant Urologist The Urology Centre Guy s and St. Thomas Hospital NHS Foundation Trust Oncocytoma High Risk Partial converted to
Renal biopsy is mandatory for every small renal mass Ben Challacombe Consultant Urologist The Urology Centre Guy s and St. Thomas Hospital NHS Foundation Trust Oncocytoma High Risk Partial converted to
Canadian Guidelines for Management of the Small Renal Mass (SRM)
") Canadian Guidelines for Management of the Small Renal Mass (SRM) Michael A.S. Jewett*, Ricardo Rendon, Louis Lacombe, Pierre I. Karakiewicz, Simon Tanguay, Wes Kassouf, Mike Leveridge, Ilias Cagiannos,
Canadian Guidelines for Management of the Small Renal Mass (SRM) Michael A.S. Jewett*, Ricardo Rendon, Louis Lacombe, Pierre I. Karakiewicz, Simon Tanguay, Wes Kassouf, Mike Leveridge, Ilias Cagiannos,
ablativi Vincenzo Ficarra Direttore Clinica di Urologia Azienda Ospedaliera Universitaria di Udine
 Sorveglianza attiva e trattamenti ablativi Vincenzo Ficarra Direttore Clinica di Urologia Azienda Ospedaliera Universitaria di Udine Risk of mortality in RCC patients Kutikov A. et al. J Clin Oncol 2010;
Sorveglianza attiva e trattamenti ablativi Vincenzo Ficarra Direttore Clinica di Urologia Azienda Ospedaliera Universitaria di Udine Risk of mortality in RCC patients Kutikov A. et al. J Clin Oncol 2010;
Is renal cryoablation becoming an effective alternative to partial nephrectomy?
 Is renal cryoablation becoming an effective alternative to partial nephrectomy? J GARNON 1, G TSOUMAKIDOU 1, H LANG 2, A GANGI 1 1 department of interventional radiology 2 department of urology University
Is renal cryoablation becoming an effective alternative to partial nephrectomy? J GARNON 1, G TSOUMAKIDOU 1, H LANG 2, A GANGI 1 1 department of interventional radiology 2 department of urology University
Lymphadenectomy in RCC: Yes, No, Clinical Trial?
 Lymphadenectomy in RCC: Yes, No, Clinical Trial? Viraj Master MD PhD FACS Professor Associate Chair for Clinical Affairs and Quality Director of Clinical Research Unit Department of Urology Emory University
Lymphadenectomy in RCC: Yes, No, Clinical Trial? Viraj Master MD PhD FACS Professor Associate Chair for Clinical Affairs and Quality Director of Clinical Research Unit Department of Urology Emory University
Small Renal Mass Guidelines. Clif Vestal, MD USMD Arlington, Texas
 Small Renal Mass Guidelines Clif Vestal, MD USMD Arlington, Texas Evaluation/Diagnosis 1. Obtain high quality, multiphase, cross-sectional abdominal imaging to optimally characterize/stage the renal mass.
Small Renal Mass Guidelines Clif Vestal, MD USMD Arlington, Texas Evaluation/Diagnosis 1. Obtain high quality, multiphase, cross-sectional abdominal imaging to optimally characterize/stage the renal mass.
NCCN AND AUA GUIDELINES FOR RCC:
 NCCN AND AUA GUIDELINES FOR RCC: DO THEY EFFECTIVELY CAPTURE RECURRENCES FOLLOWING NEPHRECTOMY? Suzanne B. Stewart, MD 1, R. Houston Thompson, MD 1, Sarah P. Psutka, MD 1, John C. Cheville, MD 2, Christine
NCCN AND AUA GUIDELINES FOR RCC: DO THEY EFFECTIVELY CAPTURE RECURRENCES FOLLOWING NEPHRECTOMY? Suzanne B. Stewart, MD 1, R. Houston Thompson, MD 1, Sarah P. Psutka, MD 1, John C. Cheville, MD 2, Christine
BJUI. Active surveillance of small renal masses offers short-term oncological efficacy equivalent to radical and partial nephrectomy
 BJUI Active surveillance of small renal masses offers short-term oncological efficacy equivalent to radical and partial nephrectomy Nilay Patel, David Cranston, M. Zeeshan Akhtar, Caroline George, Andrew
BJUI Active surveillance of small renal masses offers short-term oncological efficacy equivalent to radical and partial nephrectomy Nilay Patel, David Cranston, M. Zeeshan Akhtar, Caroline George, Andrew
Fifteenth International Kidney Cancer Symposium
 The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
A randomized phase 2 trial of CRLX101 in combination with bevacizumab in patients with metastatic renal cell carcinoma (mrcc) vs standard of care
 vs standard of care") A randomized phase 2 trial of CRLX101 in combination with bevacizumab in patients with metastatic renal cell carcinoma (mrcc) vs standard of care Martin H. Voss 1, Thomas Hutson 2, Arif Hussain 3, Ulka
A randomized phase 2 trial of CRLX101 in combination with bevacizumab in patients with metastatic renal cell carcinoma (mrcc) vs standard of care Martin H. Voss 1, Thomas Hutson 2, Arif Hussain 3, Ulka
PROSTATE CANCER SURVEILLANCE
 PROSTATE CANCER SURVEILLANCE ESMO Preceptorship on Prostate Cancer Singapore, 15-16 November 2017 Rosa Nadal National Cancer Institute, NIH Bethesda, USA DISCLOSURE No conflicts of interest to declare
PROSTATE CANCER SURVEILLANCE ESMO Preceptorship on Prostate Cancer Singapore, 15-16 November 2017 Rosa Nadal National Cancer Institute, NIH Bethesda, USA DISCLOSURE No conflicts of interest to declare
Guidelines for the Management of Renal Cancer West Midlands Expert Advisory Group for Urological Cancer
 Guidelines for the Management of Renal Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Guidelines for the Management of Renal Cancer West Midlands Expert Advisory Group for Urological Cancer West Midlands Clinical Networks and Clinical Senate Coversheet for Network Expert Advisory Group
Vincenzo Ficarra. Direttore Clinica di Urologia Azienda Ospedaliera Universitaria di Udine
 Best Papers on Kidney Cancer Vincenzo Ficarra Direttore Clinica di Urologia Azienda Ospedaliera Universitaria di Udine Uro-oncological oncological topics Renal Tumor biopsy Positive Surgical Margins after
Best Papers on Kidney Cancer Vincenzo Ficarra Direttore Clinica di Urologia Azienda Ospedaliera Universitaria di Udine Uro-oncological oncological topics Renal Tumor biopsy Positive Surgical Margins after
RAPN. in T1b Renal Masses? A. Mottrie. G. Denaeyer, P. Schatteman, G. Novara
 RAPN in T1b Renal Masses? A. Mottrie G. Denaeyer, P. Schatteman, G. Novara Department of Urology O.L.V. Clinic Aalst OLV Vattikuti Robotic Surgery Institute Aalst Belgium Guidelines on Renal Cell Carcinoma
RAPN in T1b Renal Masses? A. Mottrie G. Denaeyer, P. Schatteman, G. Novara Department of Urology O.L.V. Clinic Aalst OLV Vattikuti Robotic Surgery Institute Aalst Belgium Guidelines on Renal Cell Carcinoma
Sommerakademie Munich, June
 Active surveillance: Shrinking the grey zone Sommerakademie Munich, June 30 2016 Active surveillance Overview of 20 year history Laurence Klotz, MD, CM Professor of Surgery Sunnybrook Heatlh Sciences Centre
Active surveillance: Shrinking the grey zone Sommerakademie Munich, June 30 2016 Active surveillance Overview of 20 year history Laurence Klotz, MD, CM Professor of Surgery Sunnybrook Heatlh Sciences Centre
Patient Selection for Surgery in RCC with Thrombus. E. Jason Abel, M.D.
 Patient Selection for Surgery in RCC with Thrombus E. Jason Abel, M.D. RCC with venous invasion Venous invasion occurs in ~10% of RCC Surgery more complex Increased risk for morbidity Thrombus may be confined
Patient Selection for Surgery in RCC with Thrombus E. Jason Abel, M.D. RCC with venous invasion Venous invasion occurs in ~10% of RCC Surgery more complex Increased risk for morbidity Thrombus may be confined
MRI in the Enhanced Detection of Prostate Cancer: What Urologists Need to Know
 MRI in the Enhanced Detection of Prostate Cancer: What Urologists Need to Know Michael S. Cookson, MD, FACS Professor and Chair Department of Urology Director of Prostate and Urologic Oncology University
MRI in the Enhanced Detection of Prostate Cancer: What Urologists Need to Know Michael S. Cookson, MD, FACS Professor and Chair Department of Urology Director of Prostate and Urologic Oncology University
Management of High Risk Renal Cell Carcinoma
 Management of High Risk Renal Cell Carcinoma Peter E. Clark, MD Professor and Chair, Department of Urology Carolinas HealthCare System Chair, Urologic Oncology Levine Cancer Institute October 14, 2017
Management of High Risk Renal Cell Carcinoma Peter E. Clark, MD Professor and Chair, Department of Urology Carolinas HealthCare System Chair, Urologic Oncology Levine Cancer Institute October 14, 2017
St. Dominic s Annual Cancer Report Outcomes
 St. Dominic s 2017 Annual Cancer Report Outcomes Cancer Program Practice Profile Reports (CP3R) St. Dominic s Cancer Committee monitors and ensures that patients treated at St. Dominic Hospital receive
St. Dominic s 2017 Annual Cancer Report Outcomes Cancer Program Practice Profile Reports (CP3R) St. Dominic s Cancer Committee monitors and ensures that patients treated at St. Dominic Hospital receive
VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE
 Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Session 3 Advanced prostate cancer VALUE AND ROLE OF PSA AS A TUMOUR MARKER OF RESPONSE/RELAPSE 1 PSA is a serine protease and the physiological role is believed to be liquefying the seminal fluid PSA
Indications For Partial
 Indications For Partial Nephrectomy Christopher G. Wood, M. D., FACS Professor and Deputy Chairman Douglas E. Johnson, M. D. Endowed Professorship in Urology Department of Urology The University of Texas
Indications For Partial Nephrectomy Christopher G. Wood, M. D., FACS Professor and Deputy Chairman Douglas E. Johnson, M. D. Endowed Professorship in Urology Department of Urology The University of Texas
SAMPLING OF POST NEPHRECTOMY CANCER CARE (5)
") SAMPLING OF POST NEPHRECTOMY CANCER CARE (5) Universally recognized post-nephrectomy cancer treatment. Sampling: National Comprehensive Cancer Network (NCCN) NCCN Clinical Practice Guidelines in Oncology
SAMPLING OF POST NEPHRECTOMY CANCER CARE (5) Universally recognized post-nephrectomy cancer treatment. Sampling: National Comprehensive Cancer Network (NCCN) NCCN Clinical Practice Guidelines in Oncology
Focal Therapy is a Fool s Paradise : The whole prostate must be treated!
 Focal Therapy is a Fool s Paradise : The whole prostate must be treated! Ofer Yossepowitch, MD Head, Department of Urology Tel Aviv Sourasky Medical Center Preaching against focal therapy in a focal therapy
Focal Therapy is a Fool s Paradise : The whole prostate must be treated! Ofer Yossepowitch, MD Head, Department of Urology Tel Aviv Sourasky Medical Center Preaching against focal therapy in a focal therapy
Management of Locally Reccurent Renal Cell Carcinoma. Jose A. Karam, MD, FACS Assistant Professor Department of Urology
 Management of Locally Reccurent Renal Cell Carcinoma Jose A. Karam, MD, FACS Assistant Professor Department of Urology DefiniAons Defini&ve treatment Aiming for cure Abla&on therapy Radiofrequency abla&on
Management of Locally Reccurent Renal Cell Carcinoma Jose A. Karam, MD, FACS Assistant Professor Department of Urology DefiniAons Defini&ve treatment Aiming for cure Abla&on therapy Radiofrequency abla&on
Clinical/Surgical trials that will change my practice
 Clinical/Surgical trials that will change my practice Mr Jim M Adshead Herts and Beds Urological Cancer Centre, Lister Hospital What s changed and where do I feel we are clutching at straws? Regional Specialist
Clinical/Surgical trials that will change my practice Mr Jim M Adshead Herts and Beds Urological Cancer Centre, Lister Hospital What s changed and where do I feel we are clutching at straws? Regional Specialist
Focal Ablative Therapies for Kidney Cancer
 Focal Ablative Therapies for Kidney Cancer Robert J. Hamilton, MD, MPH, FRCSC Staff Urologist, Princess Margaret Cancer Centre Assistant Prof., Dept. of Surgery (Urology), University of Toronto ICUC January
Focal Ablative Therapies for Kidney Cancer Robert J. Hamilton, MD, MPH, FRCSC Staff Urologist, Princess Margaret Cancer Centre Assistant Prof., Dept. of Surgery (Urology), University of Toronto ICUC January
MR-US Fusion Guided Biopsy: Is it fulfilling expectations?
 MR-US Fusion Guided Biopsy: Is it fulfilling expectations? Kenneth L. Gage MD, PhD Assistant Member Department of Diagnostic Imaging and Interventional Radiology 4 th Annual New Frontiers in Urologic Oncology
MR-US Fusion Guided Biopsy: Is it fulfilling expectations? Kenneth L. Gage MD, PhD Assistant Member Department of Diagnostic Imaging and Interventional Radiology 4 th Annual New Frontiers in Urologic Oncology
EUROPEAN UROLOGY 61 (2012)
") EUROPEAN UROLOGY 61 (2012) 1156 1161 available at www.sciencedirect.com journal homepage: www.europeanurology.com Platinum Priority Kidney Cancer Editorial by Alvin C. Goh and Inderbir S. Gill on pp. 1162
EUROPEAN UROLOGY 61 (2012) 1156 1161 available at www.sciencedirect.com journal homepage: www.europeanurology.com Platinum Priority Kidney Cancer Editorial by Alvin C. Goh and Inderbir S. Gill on pp. 1162
Characterization of Patients with Poor-
 Characterization of Patients with Poor- Risk Metastatic Renal Cell Carcinoma Hamieh L 1 *, McKay RR 1 *, Lin X 2, Simantov R 2, Choueiri TK 1 *Equal contributions 1 Dana-Farber Cancer Institute, Boston,
Characterization of Patients with Poor- Risk Metastatic Renal Cell Carcinoma Hamieh L 1 *, McKay RR 1 *, Lin X 2, Simantov R 2, Choueiri TK 1 *Equal contributions 1 Dana-Farber Cancer Institute, Boston,
Screening and Risk Stratification of Men for Prostate Cancer Metastasis and Mortality
 Screening and Risk Stratification of Men for Prostate Cancer Metastasis and Mortality Sanoj Punnen, MD, MAS Assistant Professor of Urologic Oncology University of Miami, Miller School of Medicine and Sylvester
Screening and Risk Stratification of Men for Prostate Cancer Metastasis and Mortality Sanoj Punnen, MD, MAS Assistant Professor of Urologic Oncology University of Miami, Miller School of Medicine and Sylvester
Diagnostic accuracy of percutaneous renal tumor biopsy May 10 th 2018
 Diagnostic accuracy of percutaneous renal tumor biopsy May 10 th 2018 Dr. Tzahi Neuman Dep.Of Pathology Hadassah Medical Center Jerusalem, Israel, (tneuman@hadassah.org.il) Disclosure: 1 no conflicts of
Diagnostic accuracy of percutaneous renal tumor biopsy May 10 th 2018 Dr. Tzahi Neuman Dep.Of Pathology Hadassah Medical Center Jerusalem, Israel, (tneuman@hadassah.org.il) Disclosure: 1 no conflicts of
RCC in ADPKD / CKD / ESRD
 RCC in ADPKD / CKD / ESRD FOIU 2018 David A. Goldfarb, MD,FACS Professor of Surgery, Cleveland Clinic Lerner College of Medicine Glickman Urological and Kidney Institute Cleveland Clinic, Cleveland, Ohio
RCC in ADPKD / CKD / ESRD FOIU 2018 David A. Goldfarb, MD,FACS Professor of Surgery, Cleveland Clinic Lerner College of Medicine Glickman Urological and Kidney Institute Cleveland Clinic, Cleveland, Ohio
Consensus and Controversies in Cancer of Prostate BASIS FOR FURHTER STUDIES. Luis A. Linares MD FACRO Medical Director
 BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
BASIS FOR FURHTER STUDIES Main controversies In prostate Cancer: 1-Screening 2-Management Observation Surgery Standard Laparoscopic Robotic Radiation: (no discussion on Cryosurgery-RF etc.) Standard SBRT
Damian Dupuy, MD. Image Guided Intervention (IGI) Studies 10:25 11:05 AM
 Studies 10:25 11:05 AM") Damian Dupuy, MD Image Guided Intervention (IGI) Studies 10:25 11:05 AM Image Guided Intervention (IGI) Studies Damian E. Dupuy, M.D., FACR Professor of Diagnostic Imaging The Warren Alpert Medical School
Damian Dupuy, MD Image Guided Intervention (IGI) Studies 10:25 11:05 AM Image Guided Intervention (IGI) Studies Damian E. Dupuy, M.D., FACR Professor of Diagnostic Imaging The Warren Alpert Medical School
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective
 Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC
 The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College
The Rationale for Immunotherapy as an Adjuvant Treatment for Locally Advanced BC Seth P. Lerner, MD, FACS Professor, Scott Department of Urology Beth and Dave Swalm Chair in Urologic Oncology Baylor College
Cytoreductive Nephrectomy
 Cytoreductive Nephrectomy Stephen H. Culp, M.D., Ph.D. Assistant Professor, Department of Urology Outline The Historics of CN The current status of CN The importance of patient selection Cytoreductive
Cytoreductive Nephrectomy Stephen H. Culp, M.D., Ph.D. Assistant Professor, Department of Urology Outline The Historics of CN The current status of CN The importance of patient selection Cytoreductive
Surgeons Perspective: LN as a Draining Pattern. Jose A. Karam, MD, FACS Associate Professor Department of Urology
 Surgeons Perspective: LN as a Draining Pattern Jose A. Karam, MD, FACS Associate Professor Department of Urology Disclosures EMD Serono, Pfizer, Novartis: Advisory board/consultant Disclosures I perform
Surgeons Perspective: LN as a Draining Pattern Jose A. Karam, MD, FACS Associate Professor Department of Urology Disclosures EMD Serono, Pfizer, Novartis: Advisory board/consultant Disclosures I perform
Who are Candidates for Laparoscopic or Open Radical Nephrectomy. Arieh Shalhav
 Who are Candidates for Laparoscopic or Open Radical Nephrectomy Arieh Shalhav Fritz Duda Chair of Urologic Surgery Professor of Surgery and the Comprehensive Cancer Research Center Who are Candidates for
Who are Candidates for Laparoscopic or Open Radical Nephrectomy Arieh Shalhav Fritz Duda Chair of Urologic Surgery Professor of Surgery and the Comprehensive Cancer Research Center Who are Candidates for
The High-Dose Aldesleukin (IL-2) Select Trial in Patients with Metastatic RCC
 Select Trial in Patients with Metastatic RCC") The High-Dose Aldesleukin (IL-2) Select Trial in Patients with Metastatic RCC D McDermott, M Ghebremichael, S Signoretti, K Margolin, J Clark, J Sosman, J Dutcher, T Logan, R Figlin and M Atkins on behalf
The High-Dose Aldesleukin (IL-2) Select Trial in Patients with Metastatic RCC D McDermott, M Ghebremichael, S Signoretti, K Margolin, J Clark, J Sosman, J Dutcher, T Logan, R Figlin and M Atkins on behalf
What is the role of partial nephrectomy in the context of active surveillance and renal ablation?
 What is the role of partial nephrectomy in the context of active surveillance and renal ablation? Dogu Teber Department of Urology University Hospital Heidelberg Coming from Heidelberg obligates to speak
What is the role of partial nephrectomy in the context of active surveillance and renal ablation? Dogu Teber Department of Urology University Hospital Heidelberg Coming from Heidelberg obligates to speak
Tumor necrosis is a strong predictor for recurrence in patients with pathological T1a renal cell carcinoma
 ONCOLOGY LETTERS 9: 125-130, 2015 Tumor necrosis is a strong predictor for recurrence in patients with pathological T1a renal cell carcinoma KEIICHI ITO 1, KENJI SEGUCHI 1, HIDEYUKI SHIMAZAKI 2, EIJI TAKAHASHI
ONCOLOGY LETTERS 9: 125-130, 2015 Tumor necrosis is a strong predictor for recurrence in patients with pathological T1a renal cell carcinoma KEIICHI ITO 1, KENJI SEGUCHI 1, HIDEYUKI SHIMAZAKI 2, EIJI TAKAHASHI
pan-canadian Oncology Drug Review Stakeholder Feedback on a pcodr Request for Advice Axitinib (Inlyta) for Metastatic Renal Cell Carcinoma
 for Metastatic Renal Cell Carcinoma") pan-canadian Oncology Drug Review Stakeholder Feedback on a pcodr Request for Advice Axitinib (Inlyta) for Metastatic Renal Cell Carcinoma Pfizer Canada Inc. June 29, 2017 3 Stakeholder Feedback on a pcodr
pan-canadian Oncology Drug Review Stakeholder Feedback on a pcodr Request for Advice Axitinib (Inlyta) for Metastatic Renal Cell Carcinoma Pfizer Canada Inc. June 29, 2017 3 Stakeholder Feedback on a pcodr
The role of cytoreductive. nephrectomy in elderly patients. with metastatic renal cell. carcinoma in an era of targeted. therapy
 The role of cytoreductive nephrectomy in elderly patients with metastatic renal cell carcinoma in an era of targeted therapy Dipesh Uprety, MD Amir Bista, MD Yazhini Vallatharasu, MD Angela Smith, MA David
The role of cytoreductive nephrectomy in elderly patients with metastatic renal cell carcinoma in an era of targeted therapy Dipesh Uprety, MD Amir Bista, MD Yazhini Vallatharasu, MD Angela Smith, MA David
Cancer. Description. Section: Surgery Effective Date: October 15, 2016 Subsection: Original Policy Date: September 9, 2011 Subject:
 Subject: Saturation Biopsy for Diagnosis, Last Review Status/Date: September 2016 Page: 1 of 9 Saturation Biopsy for Diagnosis, Description Saturation biopsy of the prostate, in which more cores are obtained
Subject: Saturation Biopsy for Diagnosis, Last Review Status/Date: September 2016 Page: 1 of 9 Saturation Biopsy for Diagnosis, Description Saturation biopsy of the prostate, in which more cores are obtained
Research Article Neutrophil-Lymphocyte Ratio in Small Renal Masses
 ISRN Urology, Article ID 759253, 5 pages http://dx.doi.org/10.1155/2014/759253 Research Article Neutrophil-Lymphocyte Ratio in Small Renal Masses Wassim M. Bazzi, 1 Sheila Z. Dejbakhsh, 2,3 Melanie Bernstein,
ISRN Urology, Article ID 759253, 5 pages http://dx.doi.org/10.1155/2014/759253 Research Article Neutrophil-Lymphocyte Ratio in Small Renal Masses Wassim M. Bazzi, 1 Sheila Z. Dejbakhsh, 2,3 Melanie Bernstein,
Contrast Enhanced Ultrasound of Parenchymal Masses in Children
 Contrast Enhanced Ultrasound of Parenchymal Masses in Children Sue C Kaste, DO On behalf of Beth McCarville, MD St. Jude Children s Research Hospital Memphis, TN Overview Share St. Jude experience with
Contrast Enhanced Ultrasound of Parenchymal Masses in Children Sue C Kaste, DO On behalf of Beth McCarville, MD St. Jude Children s Research Hospital Memphis, TN Overview Share St. Jude experience with
Timing of targeted therapy in patients with low volume mrcc. Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital
 1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
Management options for high-risk, BCG-refractory NMIBC. Alan M. Nieder, M.D. Columbia University Division of Urology Mount Sinai Medical Center
 Management options for high-risk, BCG-refractory NMIBC Alan M. Nieder, M.D. Columbia University Division of Urology Mount Sinai Medical Center Bladder Cancer in U.S. 4 th most common cancer in men 9 th
Management options for high-risk, BCG-refractory NMIBC Alan M. Nieder, M.D. Columbia University Division of Urology Mount Sinai Medical Center Bladder Cancer in U.S. 4 th most common cancer in men 9 th
RITE Thermochemotherapy in the treatment of BCG refractory NMIBC
 RITE Thermochemotherapy in the treatment of BCG refractory NMIBC Ben Ayres Consultant Urological Surgeon St George s Hospital London 1 Financial and Other Disclosures Off-label use of drugs, devices, or
RITE Thermochemotherapy in the treatment of BCG refractory NMIBC Ben Ayres Consultant Urological Surgeon St George s Hospital London 1 Financial and Other Disclosures Off-label use of drugs, devices, or
Key Words: kidney; carcinoma, renal cell; renal insufficiency; nephrectomy; mortality
 Comparative Effectiveness for Survival and Renal Function of Partial and Radical Nephrectomy for Localized Renal Tumors: A Systematic Review and Meta-Analysis Simon P. Kim, R. Houston Thompson, Stephen
Comparative Effectiveness for Survival and Renal Function of Partial and Radical Nephrectomy for Localized Renal Tumors: A Systematic Review and Meta-Analysis Simon P. Kim, R. Houston Thompson, Stephen
Debate: Lymphadenectomy is Important in mrcc, CON P. Mulder, M.D., Ph.D. JJ. Patard, MD, Ph.D.
 Debate: Lymphadenectomy is Important in mrcc, CON P. Mulder, M.D., Ph.D. JJ. Patard, MD, Ph.D.. Eighth European International Kidney Cancer Symposium Budapest 03-04 May 2013 The role of LND In organ confined
Debate: Lymphadenectomy is Important in mrcc, CON P. Mulder, M.D., Ph.D. JJ. Patard, MD, Ph.D.. Eighth European International Kidney Cancer Symposium Budapest 03-04 May 2013 The role of LND In organ confined
PCa Commentary. Executive Summary: The "PCa risk increased directly with increasing phi values."
 1101 Madison Street Suite 1101 Seattle, WA 98104 P 206-215-2490 www.seattleprostate.com PCa Commentary Volume 77 September October 2012 CONTENT Page The Prostate 1 Health Index Active Surveillance 2 A
1101 Madison Street Suite 1101 Seattle, WA 98104 P 206-215-2490 www.seattleprostate.com PCa Commentary Volume 77 September October 2012 CONTENT Page The Prostate 1 Health Index Active Surveillance 2 A
DAYS IN PANCREATIC CANCER
 HOSPITAL AND MEDICAL CARE DAYS IN PANCREATIC CANCER Annals of Surgical Oncology, March 27, 2012 Casey B. Duncan, Kristin M. Sheffield, Daniel W. Branch, Yimei Han, Yong-Fang g Kuo, James S. Goodwin, Taylor
HOSPITAL AND MEDICAL CARE DAYS IN PANCREATIC CANCER Annals of Surgical Oncology, March 27, 2012 Casey B. Duncan, Kristin M. Sheffield, Daniel W. Branch, Yimei Han, Yong-Fang g Kuo, James S. Goodwin, Taylor
Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015
 Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015 Outline Epidemiology of prostate cancer Purpose of screening Method of screening Contemporary screening trials
Health Screening Update: Prostate Cancer Zamip Patel, MD FSACOFP Convention August 1 st, 2015 Outline Epidemiology of prostate cancer Purpose of screening Method of screening Contemporary screening trials
Carcinoma renale (I): Posters Review. Elena Verzoni Oncologia Medica 1 SS.Oncologia Genitourinaria Fondazione IRCCS Istituto Nazionale Tumori Milano
: Posters Review. Elena Verzoni Oncologia Medica 1 SS.Oncologia Genitourinaria Fondazione IRCCS Istituto Nazionale Tumori Milano") Carcinoma renale (I): Posters Review Elena Verzoni Oncologia Medica 1 SS.Oncologia Genitourinaria Fondazione IRCCS Istituto Nazionale Tumori Milano Agenda: Best Posters in Localized RCC Surgery: CN (#
Carcinoma renale (I): Posters Review Elena Verzoni Oncologia Medica 1 SS.Oncologia Genitourinaria Fondazione IRCCS Istituto Nazionale Tumori Milano Agenda: Best Posters in Localized RCC Surgery: CN (#
Sergio Bracarda MD. Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy
 San Donato Hospital Arezzo, Italy") Sergio Bracarda MD Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy Ninth European International Kidney Cancer Symposium Dublin 25-26
Sergio Bracarda MD Head, Medical Oncology Department of Oncology AUSL-8 Istituto Toscano Tumori (ITT) San Donato Hospital Arezzo, Italy Ninth European International Kidney Cancer Symposium Dublin 25-26
Open clinical uro-oncology trials in Canada
 Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Open clinical uro-oncology trials in Canada Eric Winquist, MD, George Rodrigues, MD London Health Sciences Centre, London, Ontario, Canada bladder cancer A PHASE II PROTOCOL FOR PATIENTS WITH STAGE T1
Renal cancer in adults
 Renal cancer in adults Diagnosis, treatment and follow-up NADIA BENAHMED, JO ROBAYS, SABINE STORDEUR, THIERRY GIL, STEVEN JONIAU, NICOLAAS LUMEN, LAURETTE RENARD, SANDRINE RORIVE, DIRK SCHRIJVERS, BERTRAND
Renal cancer in adults Diagnosis, treatment and follow-up NADIA BENAHMED, JO ROBAYS, SABINE STORDEUR, THIERRY GIL, STEVEN JONIAU, NICOLAAS LUMEN, LAURETTE RENARD, SANDRINE RORIVE, DIRK SCHRIJVERS, BERTRAND
Role and extension of lymph node dissection in kidney, bladder and prostate cancer. Omar Ghanem (PGY3 ) Moderator: Dr A. Noujem 30 th March 2017
 Moderator: Dr A. Noujem 30 th March 2017") Role and extension of lymph node dissection in kidney, bladder and prostate cancer Omar Ghanem (PGY3 ) Moderator: Dr A. Noujem 30 th March 2017 Bladder Cancer LN dissection in Bladder cancer 25% of patients
Role and extension of lymph node dissection in kidney, bladder and prostate cancer Omar Ghanem (PGY3 ) Moderator: Dr A. Noujem 30 th March 2017 Bladder Cancer LN dissection in Bladder cancer 25% of patients
Renal Masses in Patients with Known Extrarenal Primary Primary Cancer Primary Primary n Met Mets s RCC Beni L mphoma Lung Breast Others
 The Importance of Stuart G. Silverman, MD, FACR Professor of Radiology Harvard ard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Boston, MA The Importance of
The Importance of Stuart G. Silverman, MD, FACR Professor of Radiology Harvard ard Medical School Director, Abdominal Imaging and Intervention Brigham and Women s Hospital Boston, MA The Importance of
KIDNEY HEALTH. Kidney Masses and Localized Kidney Tumors: A Patient Guide
 KIDNEY HEALTH Kidney Masses and Localized Kidney Tumors: A Patient Guide Table of Contents Kidney & Adrenal Health Committee Renal Mass Committee.... 2 Patient Story.... 3 Introduction: I have a kidney
KIDNEY HEALTH Kidney Masses and Localized Kidney Tumors: A Patient Guide Table of Contents Kidney & Adrenal Health Committee Renal Mass Committee.... 2 Patient Story.... 3 Introduction: I have a kidney
UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA. Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA
 UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA DISCLAIMER Please note: The views expressed within this presentation
UPDATE FROM ASCO GU FEBRUARY 2018, SAN FRANCISCO, USA Prof. David Pfister University Hospital of Cologne Germany RENAL CELL CARCINOMA DISCLAIMER Please note: The views expressed within this presentation
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
Vincenzo Ficarra 1,2,3. Associate Editor BJU International
 Partial Nephrectomy for RCC Vincenzo Ficarra 1,2,3 1 Director Department of Urology University of Udine, Italy 2 Associate Editor BJU International 3 Scientific Director OLV Robotic Surgery Institute,
Partial Nephrectomy for RCC Vincenzo Ficarra 1,2,3 1 Director Department of Urology University of Udine, Italy 2 Associate Editor BJU International 3 Scientific Director OLV Robotic Surgery Institute,
Patient and Hospital Characteristics Associated with Nephron-Sparing Surgery for Small, Localized Kidney Cancers in California,
 Patient and Hospital Characteristics Associated with Nephron-Sparing Surgery for Small, Localized Kidney Cancers in California, 2012-2015 Brenda M. Giddings, M.A. California Cancer Reporting and Epidemiologic
Patient and Hospital Characteristics Associated with Nephron-Sparing Surgery for Small, Localized Kidney Cancers in California, 2012-2015 Brenda M. Giddings, M.A. California Cancer Reporting and Epidemiologic
Radical Prostatectomy:
 Overtreatment and undertreatment Radical Prostatectomy: An Emerging Standard of Care for High Risk Prostate Cancer Matthew R. Cooperberg, MD,MPH UCSF Radiation Oncology Update San Francisco, CA April 2,
Overtreatment and undertreatment Radical Prostatectomy: An Emerging Standard of Care for High Risk Prostate Cancer Matthew R. Cooperberg, MD,MPH UCSF Radiation Oncology Update San Francisco, CA April 2,
Title: What is the role of pre-operative PET/PET-CT in the management of patients with
 Title: What is the role of pre-operative PET/PET-CT in the management of patients with potentially resectable colorectal cancer liver metastasis? Pablo E. Serrano, Julian F. Daza, Natalie M. Solis June
Title: What is the role of pre-operative PET/PET-CT in the management of patients with potentially resectable colorectal cancer liver metastasis? Pablo E. Serrano, Julian F. Daza, Natalie M. Solis June
Clinically Localized Prostate Cancer: AUA/ASTRO/SUO Guideline Very Low-/Low-Risk Disease
 Clinically Localized Prostate Cancer: AUA/ASTRO/SUO Guideline Very Low-/Low-Risk Disease Jeffrey A. Cadeddu, MD Professor, Department of Urology UT Southwestern Medical Center Vice-Chair, AUA/ASTRO/SUO
Clinically Localized Prostate Cancer: AUA/ASTRO/SUO Guideline Very Low-/Low-Risk Disease Jeffrey A. Cadeddu, MD Professor, Department of Urology UT Southwestern Medical Center Vice-Chair, AUA/ASTRO/SUO
Fifteenth International Kidney Cancer Symposium November 4-5, 2016 Marriott Miami Biscayne Bay, Miami, Florida, USA
 The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer. American Society of Clinical Oncology Clinical Practice Guideline
 Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer American Society of Clinical Oncology Clinical Practice Guideline Introduction ASCO convened an Expert Panel to develop recommendations
Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer American Society of Clinical Oncology Clinical Practice Guideline Introduction ASCO convened an Expert Panel to develop recommendations
DOSE. Dose Optimization in Stone Evaluation:
 Dose Optimization in Stone Evaluation: DOSE October 21st 2017 Chris Moore MD Associate Professor, Department of Emergency Medicine Yale University School of Medicine Disclosures I am currently funded by
Dose Optimization in Stone Evaluation: DOSE October 21st 2017 Chris Moore MD Associate Professor, Department of Emergency Medicine Yale University School of Medicine Disclosures I am currently funded by
Solitary Contralateral Adrenal Metastases after Nephrectomy for Renal Cell Carcinoma
 Original Report ISSN 1537-744X; DOI 10.1100/tsw.2004.39 Solitary Contralateral Adrenal after Nephrectomy for Renal Cell Carcinoma Nikolaos Antoniou, M.D. and Demetrios Karanastasis, M.D. General Hospital
Original Report ISSN 1537-744X; DOI 10.1100/tsw.2004.39 Solitary Contralateral Adrenal after Nephrectomy for Renal Cell Carcinoma Nikolaos Antoniou, M.D. and Demetrios Karanastasis, M.D. General Hospital
Best Papers. F. Fusco
 Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Complex case Presentations
 Complex case Presentations Case Presentations April 2016 Lisa M Pickering Case presentations: chromophobe renal carcinoma 60 year old man. ECOG PS 0 No significant comorbodities August 2009: L radical
Complex case Presentations Case Presentations April 2016 Lisa M Pickering Case presentations: chromophobe renal carcinoma 60 year old man. ECOG PS 0 No significant comorbodities August 2009: L radical
Spinal cord compression as a first presentation of cancer: A case report
 J Pain Manage 2013;6(4):319-322 ISSN: 1939-5914 Nova Science Publishers, Inc. Spinal cord compression as a first presentation of cancer: A case report Nicholas Lao, BMSc(C), Michael Poon, MD(C), Marko
J Pain Manage 2013;6(4):319-322 ISSN: 1939-5914 Nova Science Publishers, Inc. Spinal cord compression as a first presentation of cancer: A case report Nicholas Lao, BMSc(C), Michael Poon, MD(C), Marko
Date Modified: March 31, Clinical Quality Measures for PQRS
 Date Modified: March 31, 2015 2015 Clinical Quality s for PQRS # Domain Title Description Type Denominator Numerator Denominator Exclusions/Exceptions 1 Patient Safety Prostate Biopsy Antibiotic Process
Date Modified: March 31, 2015 2015 Clinical Quality s for PQRS # Domain Title Description Type Denominator Numerator Denominator Exclusions/Exceptions 1 Patient Safety Prostate Biopsy Antibiotic Process
Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute
 Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 23 March 2012, Sao Paulo, Brazil Surgery of RCC Locally confined (small) renal tumours Locally advanced disease Metastatic
Surgery of Renal Cell Carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute 23 March 2012, Sao Paulo, Brazil Surgery of RCC Locally confined (small) renal tumours Locally advanced disease Metastatic
AVEO and Astellas Announce TAURUS Patient Preference Clinical Study Comparing Tivozanib with Sunitinib in First-Line Kidney Cancer
 FOR IMMEDIATE RELEASE AVEO and Astellas Announce TAURUS Patient Preference Clinical Study Comparing Tivozanib with Sunitinib in First-Line Kidney Cancer Study designed to build upon safety profile demonstrated
FOR IMMEDIATE RELEASE AVEO and Astellas Announce TAURUS Patient Preference Clinical Study Comparing Tivozanib with Sunitinib in First-Line Kidney Cancer Study designed to build upon safety profile demonstrated
Prostate Cancer: 2010 Guidelines Update
 Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Prostate Cancer: 2010 Guidelines Update James L. Mohler, MD Chair, NCCN Prostate Cancer Panel Associate Director for Translational Research, Professor and Chair, Department of Urology, Roswell Park Cancer
Hepatobiliary and Pancreatic Malignancies
 Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Hepatobiliary and Pancreatic Malignancies Gareth Eeson MD MSc FRCSC Surgical Oncologist and General Surgeon Kelowna General Hospital Interior Health Consultant, Surgical Oncology BC Cancer Agency Centre
Metastatic renal cancer (mrcc): Evidence-based treatment
: Evidence-based treatment") Metastatic renal cancer (mrcc): Evidence-based treatment José M. Ruiz Morales, M.D. Hospital Médica Sur April 18th, 2018 4th ESO-ESMO Latin American Masterclass in Clinical Oncology Disclosures Consulting:
Metastatic renal cancer (mrcc): Evidence-based treatment José M. Ruiz Morales, M.D. Hospital Médica Sur April 18th, 2018 4th ESO-ESMO Latin American Masterclass in Clinical Oncology Disclosures Consulting:
RENAL MASS AND LOCALIZED RENAL CANCER: AUA GUIDELINE
 1 Approved by the AUA Board of Directors April2017 Authors disclosure of potential conflicts of interest and author/staff contributions appear at the end of the article. 2017 by the American Urological
1 Approved by the AUA Board of Directors April2017 Authors disclosure of potential conflicts of interest and author/staff contributions appear at the end of the article. 2017 by the American Urological
Lessons learned for the conduct of a successful screening trial
 Lessons learned for the conduct of a successful screening trial Christine D. Berg, M.D. Adjunct Professor Department of Radiation Oncology Johns Hopkins Medicine IOM State of the Science in Ovarian Cancer
Lessons learned for the conduct of a successful screening trial Christine D. Berg, M.D. Adjunct Professor Department of Radiation Oncology Johns Hopkins Medicine IOM State of the Science in Ovarian Cancer
Surgical Management of Metastatic and Locally Recurrent Kidney Cancer: Does it Make Sense?
 Surgical Management of Metastatic and Locally Recurrent Kidney Cancer: Does it Make Sense? Philippe E. Spiess, MD, FACS Associate Member Department of GU Oncology Department of Tumor Biology Moffitt Cancer
Surgical Management of Metastatic and Locally Recurrent Kidney Cancer: Does it Make Sense? Philippe E. Spiess, MD, FACS Associate Member Department of GU Oncology Department of Tumor Biology Moffitt Cancer
Active surveillance: Shrinking the grey zone. Sommerakademi e Munich, June rd FOIUS Tel Aviv, July 2016
 Active surveillance: Shrinking the grey zone Active surveillance: 3 rd FOIUS Tel Aviv, July 2016 Shrinking the grey zone Sommerakademi e Munich, June 30 2016 Active Surveillance for low risk PCa What has
Active surveillance: Shrinking the grey zone Active surveillance: 3 rd FOIUS Tel Aviv, July 2016 Shrinking the grey zone Sommerakademi e Munich, June 30 2016 Active Surveillance for low risk PCa What has
The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters.
 An Exploration of Risk Stratification for Active Surveillance and Androgen Deprivation Therapy Side Effects for Prostate Cancer Utilizing Data From the Surveillance, Epidemiology, and End Results Database
An Exploration of Risk Stratification for Active Surveillance and Androgen Deprivation Therapy Side Effects for Prostate Cancer Utilizing Data From the Surveillance, Epidemiology, and End Results Database
ACTIVE SURVEILLANCE OR WATCHFUL WAITING
 Prostate Cancer ACTIVE SURVEILLANCE OR WATCHFUL WAITING María Teresa Bourlon, MD MS Head, Urologic Oncology Clinic Hemato-Oncology Department Instituto Nacional de Ciencias Médicas y Nutrición Salvador
Prostate Cancer ACTIVE SURVEILLANCE OR WATCHFUL WAITING María Teresa Bourlon, MD MS Head, Urologic Oncology Clinic Hemato-Oncology Department Instituto Nacional de Ciencias Médicas y Nutrición Salvador