Clinical Study Prognostic Value of Mandard and Dworak Tumor Regression Grading in Rectal Cancer: Study of a Single Tertiary Center
|
|
|
- Jody Lawrence
- 6 years ago
- Views:
Transcription
1 ISRN Surgery, Article ID , 8 pages Clinical Study Prognostic Value of Mandard and Dworak Tumor Regression Grading in Rectal Cancer: Study of a Single Tertiary Center Marisa D. Santos, 1 Cristina Silva, 1 Anabela Rocha, 1 Eduarda Matos, 2 Carlos Nogueira, 1 and Carlos Lopes 3,4 1 Department of Surgery, Digestive Surgery Service, Hospital de Santo António, Largo Professor Abel Salazar, Porto, Portugal 2 Department of Community Health, Instituto de Ciências Biomédicas Abel Salazar, Rua Jorge Viterbo Ferreira No. 228, Porto, Portugal 3 Department of Pathology, Pathological Anatomy Service, Hospital de Santo António, Largo Professor Abel Salazar, Porto, Portugal 4 Department of Pathology and Molecular Immunology, Instituto de Ciências Biomédicas Abel Salazar, Rua Jorge Viterbo Ferreira No. 228, Porto, Portugal Correspondence should be addressed to Marisa D. Santos; marisadsantos@gmail.com Received 29 December 2013; Accepted 21 January 2014; Published 4 March 2014 Academic Editors: S. Huerta and A. Wibe Copyright 2014 Marisa D. Santos et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Goal. To evaluate the prognostic value of Mandard and Dworak grading systems regarding neoadjuvant chemoradiotherapy (CRT) response on rectal cancer. Materials and Methods.We queried ourcenter s database forpatients with colo rectal cancer with locally advanced rectal cancer (LARC) who received neoadjuvant CRT followed by total mesorectum excision (TME) between 2003 and After excluding 18 patients from the initial query the remaining 139 were reassessed for disease recurrence and survival; the specimens slides were reviewed and classified according to two tumor regression grading (TRG) systems: Mandard and Dworak. Based on these TRG scores, two patient groups were created: patients with good response versus patients with bad response (Mandard TRG1+2 versus Mandard TRG3+4+5 and Dworak TRG4+3 versus Dworak TRG2+1+0). Overall survival (OS), diseasefree survival (DFS), and disease recurrence were then evaluated. Results. Mean age was 64.2 years and median follow up was 56 months. No significant survival difference was found when comparing patients with Dworak TRG4+3versus Dworak TRG2+1+0 (P = 0.10). Mandard TRG1+2 presented with significantly better OS and DFS than Mandard TRG3+4+5 (OS P = 0.013; DFS P = 0.007). Conclusions. Mandard system provides higher accuracy over Dworak system in predicting rectal cancer prognosis when neoadjuvant CRT is applied for tumor regression. 1. Introduction Improved outcome in the treatment of locally advanced rectal cancer (LARC) is related to the introduction of total mesorectal excision (TME) and neoadjuvant treatment [1 3]. In locally advanced rectal cancer (LARC) the use of neoadjuvant chemoradiotherapy (CRT) reduces locoregional recurrence and can lead to better prognosis depending on the tumor regression grade. Rectal cancer prognosis appears to be relatedtoneoadjuvantcrtresponse[4 6]. After curative surgery with TME, tumor extension through the rectal wall (pt), spreading to the regional lymph nodes (pn) and the circumferential resection margin (CRM) constitutethemaincriteriatoestimateprognosisinrectal carcinomapatients [7]. In LARC, chemoradiotherapy applied before surgery may change the pathologic stage and CRM of the resected specimen. Several studies have demonstrated that clinical outcome depends not only on the initial stage of the tumor, but also on the CRT-induced tumor response which varies among individual patients [8].
2 2 ISRN Surgery Tumor response to neoadjuvant CRT can induce cytoreduction and downstaging of the lesion and can also cause histological changes which can be assessed by tumor regression systems, which in turn offer another method for evaluating tumor regression. Tumor regression can range from zero evidence of treatment efficacy to a complete response (ypcr) with no viable tumor cells identified. It is well established that patients with pcr after chemoradiation have better long-term outcomes than those without pcr [5, 9, 10]. Complete response, however, accounts for less than one third of the patients, and the majority of patients present either partial or no response at all. The prognostic value of partial or near complete response is an important topic and research is underway [6, 11]. In order to quantify neoadjuvant CRT response, several grades can be used, being particularly important in situations where the pathological response is not complete [12 18]. There is no consensual regression grading system for pathologists who are presented with resected tumor specimens following neoadjuvant chemoradiotherapy. Most have 3 to 5 levels, allowing group creation according to the responses. This lack of consensus impeaches clinical management and leaves clinicians without a uniform scoring regression system that could guide their decisions. The value of tumor regression grading systems as an independent prognostic factor for disease-free survival has been demonstrated in several studies [6, 19 21]. The present study aims to evaluate the accuracy of Mandard and Dworak systems in rectal cancer neoadjuvant chemoradiotherapy (CRT) as a prognostic factor, mainly for patients who achieved a near complete response. 2. Material and Methods A single-institution database was queried for consecutive patients with LARC, biopsy-proven rectal adenocarcinoma, who underwent neoadjuvant CRT followed by elective radical surgery with TME with curative intent between January 1, 2003,andDecember31,2011. Admission criteria were patients with rectal cancers located less than 12 cm distance anal verge and clinical stage T2N+M0 or ct3/4 N0/+M0. Exclusion criteria were patients with other diagnosed neoplasia, short course RT, yp stage IV, R1/R2 surgery, and death within 60-day postoperative time. All patients receiving neoadjuvant CRT who were operated within 8 weeks after radiotherapy conclusion were included in this analysis. Patients receiving short-course radiation were excluded since no downstaging occurs when immediate surgery is carried out. Staging included rigid proctoscopy, total colonoscopy, chest, abdominal and pelvic CT scan, endorectal ultrasound (ERUS), pelvic magnetic resonance image (MRI) (since 2008), and carcinoembryonic antigen serum levels. The neoadjuvant CRT protocol included a total irradiation of 50.4 Gy in 28 fractions and 5-fluorouracil by infusion pump. Radical surgery was consisted mainly for sphincter saving rectal resection (SSRE) or abdominoperineal resection (APR) with TME. Regarding operative procedure selection, we considered the distance of the lesion to the anus, the comorbidities of the patient, and the condition of the anal sphincter. Operated patients were subjected to adjuvant chemotherapy protocol for 6 months performed preferably with 5- fluorouracil (5-FU) or a combination 5-FU and oxaliplatinum. Standard pathologic tumor staging of the resected specimen was performed in accordance with the guidelines of the American Joint Committee on Cancer (AJCC). Circumferential resection margin (CRM) was scored as positive when cancers cells were within 1 mm of the margin. Evidence of ypcr was defined as an absence of viable adenocarcinoma inthesurgicalspecimenorthepresenceoflakesofmucus without tumor cells. The histology of all surgical specimens was reviewed and confirmed by an independent element and was classified based on two tumor regression grading systems: Mandard and Dworak (Figures 1 and 2) Patients Were Divided in 4 Groups according to TRG. Mandard system, good responders were defined as Mandard TRG3+TRG4+TRG5; bad responders were defined as Mandard TRG1+TRG2. Dworak system, good responders were defined as Dworak TRG3+TRG4; bad responders were defined as Dworak TRG2+TRG1+TRG0. The groups in both systems (good responders versus bad responders) were used to evaluate outcome results. Disease recurrence was evaluated according to location: locoregional (LR), systemic (DR), or mixed. None of the patients were lost for followup. All surviving patients were observed and their current status was confirmed Statistical Analysis. Mandard and Dworak TRG groups (good/bad) were compared in relation to age, sex, tumor distance from anal verge, clinical stage, surgical procedure performed, and pathological stage (yp stage) using the Student s t-student and the X 2. Survival time was defined as the interval between the beginning of neoadjuvant therapy and the date of the last observation. Oncologic outcomes were evaluated for overall survival (OS), disease-free survival (DFS), overall recurrence (OR), local recurrence (LR), and distant recurrence (DR). Survival curves were performed using the Kaplan-Meier method and compared using the log-rank test. The influence of the covariates, Mandard TRG, Dworak TRG, ypn stage, ypt stage, and tumor distance from anal verge on the cumulative probability rates, was examined using the proportional hazard model (forward stepwise method) described by Cox. s are two-sided and P < 0.05 was considered significant. The statistical analysis was done using IBM SPSS Statistics version 20.










 TRG4")





 TRG3 Very few")
 tumor")


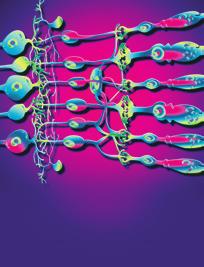
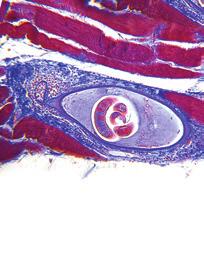
3 ISRN Surgery 3 Mandard good responders (TRG1 + TRG2) TRG1 TRG2 Mandard bad responders (TRG3 + TRG4 + TRG5) TRG3 TRG5 TRG4 Mandard TRG system TRG1 No viable cancer cells, complete response TRG2 Single cells or small groups of cancer cells TRG3 Residual cancer outgrown by fibrosis TRG4 Significant fibrosis outgrown by cancer TRG5 No fibrosis with extensive residual cancer Figure 1: Mandard system. Dworak good responders (TRG3 + TRG4) TRG4 TRG3 Dworak bad responders (TRG0 + TRG1 + TRG2) TRG2 TRG1 Dworak TRG system TRG0 No regression TRG1 Dominant tumor mass with obvious fibrosis and/or vasculopathy TRG2 Dominant fibrotic changes with few tumor cells or groups (easy to find) TRG3 Very few (difficult to find microscopically) tumor cells in fibrotic tissue with or without mucus substance TRG4 No tumor cells, only fibrotic mass (total regression) Figure 2: Dworak system. TRG0
4 4 ISRN Surgery Table 1: Clinical parameters and of TRG groups. Mandard Dworak Variables n = 139 Good versus bad response Good versus bad response Sex Male 87 (62.6%) Female 52 (37.4%) Age Mean (range) 64.2 (32 82) Tumor distance from anal verge >6 cm 68 (48.9%) 6 cm 71 (51.1%) Clinical stage II 77 (53.5%) III 67 (46.5%) Surgical procedure SSRR (sphincter saving rectal resection) 88 (63.3%) APR (abdominoperineal resection) 46 (33.1%) Other (rectal resection without anastomose) 5 (3.6%) Table 2: Comparison between TRG and pathological variables. Variables n (%) Mandard good Mandard bad Dworak good Dworak bad ypt stage T (0 2) 88 (66.1) 42 (60) 7 (10.1) < (66.7) 13 (15.3) T (3-4) 56 (38.9) 28 (40) 62 (89.9) 18 (33.3) 72 (84.7) ypn stage N0 5 (3.5) 61 (87.1) 36 (52.2) < (87) 50 (58.8) N (1-2) 139 (96.5) 9 (12.9) 33 (47.8) 7 (13) 35 (41.2) < Results The database query returned 157 patients. We excluded 18 patients: 11 patients with positive radial margin (R1 surgery), 3 patients yp stage IV, and four deaths within 60 days of postoperative period. The remaining 139 patients were evaluated. The analysis of the clinical characteristics and surgery performed on the 139 patients can be seen in Table Surgery. Sphincter saving rectal resection with anastomosis (with or without protective ileostomy) was performed on 88 patients (63.3%). Abdominal-perineal resection was performedon46patients,andfivepatientsweresubjected to proctectomy with definitive stoma. The perioperative morbidity of the series was of 25% with 11 abdominal or pelvic abscesses, 2 anastomose leaks, 5 reoperations, and 2 readmissions Pathology. Stage distribution is shown in Table 2. The average number of dissected lymph nodes in the surgical specimen was 8.2 (range 0 22). Circumferential resection margin >1mm was confirmedin all 139 patients. Response to neoadjuvant therapy is characterized in Table 1 with clinical parameters. TRG Classification.TheuseofMandardandDworaksystems allowed us to define two groups as previously mentioned: good responders (Mandard TRG1+2 or Dworak 3+4) and bad responders (Mandard TRG3+4+5 or Dworak TRG2+1+0). Using Mandard system a good response to neoadjuvant CRTwasattributedto70patients(50.4%)andabadresponse was attributed to 69 patients (49.6%). Using Dworak system a good response to neoadjuvant CRT was attributed to 54 patients (38.8%) and a bad response was attributed to 85 patients (61.2%). The number of patients with a complete response (ypcr) is the same according to both systems (Mandard TRG1/Dworak TRG4 in %). Table 2 shows T and N pathological staging according to Mandard and Dworak groups. Mandard TRG seems to better
5 ISRN Surgery 5 n (%) Table 3: Clinical long-term outcome. Mandard good Mandard bad Dworak good Dworak bad Overall recurrence disease 26 (18.7) 7 (10) 19 (27.5) 7 (12.9) 19 (22.3) Local 4 (2.9) 1 (1.4) 3 (4.3) 1 (1.8) 3 (3.5) Distant 20 (14.4) 6 (8.6) 14 (20.3) 6 (11.1) 14 (16.4) Local and distant 2 (1.4) 0 (0) 2 (2.9) 0 (0) 2 (2.3) Five-year overall survival (OS) Five-year disease free survival (DFS) Log rank test; Breslow test. Table 4: Clinical long-term outcome, survival percent. (%) Mandard good Mandard bad Dworak good Dworak bad response (%) response (%) response (%) response (%) (se = 4.2) (se = 5.4) (se = 6.3) (se = 6.4) (se = 5.5) (se = 4.1) (se = 5.1) (se = 6.3) (se = 6.2) (se = 5.4) relate with ypn stage while Dworak TRG relates with ypt stage Disease Recurrence Pelvic Recurrence. Four patients (2.7%) had isolated pelvic recurrence. Among patients on the good response groups (Mandard and Dworak), pelvic recurrence appeared, 45 months after surgery, in 1 out of 70 (1.4%) and in 1 out of 54 (1.8%), respectively, patients with ypcr (Table 3) Distant Recurrence. Distant recurrence without pelvic recurrence appeared in 20 of the 139 patients (14.4%). If we consider only the patients with a good response, distant recurrence appeared in 6 out of 70 (8.6%) patients with Mandard s good response and in 6 out of 54 (11.1%) patients with Dworak s good response. For patients who had a complete pathologic response distant recurrence emerged in one patient only (brain metastasis 25 months after surgery) Mixed Recurrence. Two patients (1.4%) had pelvic and distant disease. All were classified as bad responders according to Mandard and Dworak systems Survival. The mean follow-up was 56 months (range 6 125).Fiveyearsoverallsurvival(OS)andfiveyearsdisease free survival were 72.3% and 72.1%, respectively (Table 4). The survival of patients who showed a good response on Mandard TGR was significantly higher than the ones with bad responses, according to 5-year overall survival (OS) and 5-year disease free survival(p = and resp.) as shown in Table 4 and Figures 3 and 4. Using Dworak system the results point in the same direction but without being statistically significant (according to the log-rank test, but not the Breslow test Table 4 and Figures 5 and 6). Table 5: Survival in patients Mandard TRG(1+2) versus Mandard TRG(3+4+5), the only significant covariable retained in the multivariable analysis tested by the likelihood ratio test (stepwise forward model). Hazard ratio (95% confidence interval) OS 0.46 ( ) DFS 0.34 ( ) The two groups (good responders versus bad responders) on the two TGR (Mandard and Dworak) are statistically comparable with respect to age, sex, clinical stage, and surgical procedures performed with the exception of tumor distance from anal verge (P = 0.009/P = 0.02), ypn stage (ypn0/ypn+) (P = < 0.001/P = 0.001), and ypt stage (ypt0-2/ypt3-4) (P < 0.001/P < 0.001)(Tables1 and 2). CoxregressionmodelindicatesthatMandardTRGis the only independent factor influencing overall survival (OS) and DFS after factoring in the following variables: Mandard TRG, Dworak TRG, ypn stage (ypn0/ypn+), ypt stage, and distance from anal verge (Table 5). 4. Discussion Neoadjuvant CRT followed by TEM surgery is the widely accepted treatment for LARC [22 24]. Histologic changes after neoadjuvant CRT for rectal carcinoma vary considerably, with some entities showing complete absence of tumor cells, whereas others exhibit a mass of tumor cells with little or no regressive changes. Besides complete response, partial responsecanalsobequantified.amethodtoassesstreatment response is accomplished by grading histologic changes in theresectedspecimenthatarecausedbyneoadjuvantcrt. Tumor regression grading has been proposed in a variety of classifications but their accuracy to correlate CRT induced histological changes with disease prognosis is not always
6 6 ISRN Surgery Cumulative overall survival Cumulative disease-free survival Time (months) TRG Mandard Bad response Good response Bad response-censored Good response-censored Figure 3: Five-year overall survival, comparison of the two groups Mandard Time (months) TRG Mandard Bad response Good response Bad response-censored Good response-censored Figure 4: Five-year disease-free survival, comparison of the two groups Mandard. present. Although there are no consensual pathological standards, Mandard and Dworak systems [12, 13] are broadly being used. For this reason we applied them in our studies. The former one essentially counts the number of residual tumor cells while the later one focuses on the quantification of fibrosis (Figures 1 and 2). Both have 5 levels and are consistent in identifying a complete response (ypcr) but differences arise when the response is partial. Although early data suggest that the greatest degree of tumour regression is associated with the best clinical outcome, the clinical implication of moderate degrees of tumour regression is currently unclear. In our studies the outcome for patients with a near complete response (Mandard TRG2 or Dworak TRG3) is almost similar to the outcome for patients with complete response (Mandard TRG1 or Dworak TRG4). This result suggests thatitmaybepossibletocombinetumorsintoagroupof good responders (Mandard TRG1+2/Dworak TRG4+3) and a group of bad responders (Mandard TRG3+4+5/Dworak TRG2+1+0), since those who show significant histopathological regression and complete pathologic regression have a similarly better prognosis than the remaining poorly responding patients. This kind of division was also used by other authors [15, 19, 20, 25]. Our experience tells us that in defining a near complete response, Mandard TRG2 identifies a larger number of patients with better prognosis than Dworak TRG3. This finding may explain the better correlation between Mandard grading and disease prognosis, rather than with Dworak grading. Good responders have higher 5-year overall survival and 5-year disease free survival than bad responders, albeit these results are statistically significant only when Mandard system is considered. In our analysis a good response, defined as Mandard 1 and 2 classifications, was present in 70 of the 139 patients receiving CRT (50.4%). However, the TRG cannot be considered as the only prognostic factor that affects rectal cancer patient s survival rate after chemoradiotherapy; sphincter saving surgery rate, CMR status, local recurrence rate, perineural invasion, and ypt and ypn stages are also thought to be crucial prognostic factors [7, 15, 26, 27]. In our series we analyzed those variables in the TRG groups created. The presence of a good response in either one of the two systems did not have an impact in terms of sphincter preservation surgery. When response was good in both TRG an estimated 78.5% reduction of positive lymph nodes was achieved when clinical values were compared (un+ = 28) against pathological ones (ypn+ = 6). These aspects contributed to lowering locoregional and distant recurrence in good responders. It is possible that the impactofagoodresponseinobtainingradialmarginsgreater than 1 mm and the reduction of the number of positive lymph nodes and the pathological T stage have contributed in an effective way to increase the survival of this subgroup. Mandardsystem,whichshowstheCRTeffect,seemstobe an additional prognostic factor that, along with TNM stage, predicts the survival and recurrence rates. A patient with a good response by Mandard is estimated to face a hazard ratio that is only 46% of the hazard faced by a patient who had a bad response (Table 5). Some biases and limitations of our study can be pointed out: the series is small; the histology of all surgical specimens was reviewed retrospectively; the study protocol did not
7 ISRN Surgery 7 Cumulative survival Time (months) Dworak Bad regression Good regression Bad regression-censored Good regression-censored Figure 5: Five-year overall survival, comparison of the two groups Dworak. Cumulative survival Time (months) Dworak Bad regression Good regression Bad regression-censored Good regression-censored Figure 6: Five-year disease-free survival, comparison of the two groups Dworak. provide extra paraffin blocks from surgical specimen to confirmpcrdiagnoses.thenumberofdissectedlymph nodes, average 8.2 (0 22), can also be seen as a limitation. In order to better take advantage of our data, we intend to proceed with continued research in this area and to increase thenumberofpatientsenrolledinthisstudy,maintainingas we have done so far: a single-institution database, a single andwell-definedoperativeprocedure,andtherevisionof all surgical specimens by an independent and experimented pathologist. Finally, standardization of the Mandard TRG system and more research on the factors that affect the Mandard TRG needtobedone.clearly,theaccuracy,reliability,andvalidity of the TRG system needs to be further investigated. The clinical validation of a universally accepted regression scoring system is a key research priority. 5. Conclusion The presence of tumor regression can be considered a prognostic factor. In terms of regression grades Mandard was the one that best correlated with the presence of therapeutic response and prognosis. The presence of a good response in terms of Mandard tumor regression grade was associated with a lower incidence of locoregional recurrence and improved survival. Conflict of Interests The authors of the paper do not have any financial relation oranyfinancialinterestwiththesubjectmatterormaterials discussed in this paper. References [1] M.denDulk,P.Krijnen,C.A.M.Marijnenetal., Improved overall survival for patients with rectal cancer since 1990: the effects of TME surgery and pre-operative radiotherapy, European Cancer,vol.44,no.12,pp ,2008. [2] J.K.MacFarlane,R.D.H.Ryall,andR.J.Heald, Mesorectal excision for rectal cancer, The Lancet, vol. 341, no. 8843, pp , [3] W. van Gijn, C. A. Marijnen, I. D. Nagtegaal et al., Preoperative radiotherapy combined with total mesorectal excision for resectable rectal cancer: 12-year follow-up of the multicentre, randomised controlled TME trial, The Lancet Oncology,vol.12, no. 6, pp , [4] J.M.D.Wheeler,E.Dodds,B.F.Warrenetal., Preoperative chemoradiotherapy and total mesorectal excision surgery for locally advanced rectal cancer: correlation with rectal cancer regression grade, Diseases of the Colon and Rectum,vol.47,no. 12, pp , [5] M. Maas, P. J. Nelemans, V. Valentini et al., Long-term outcome in patients with a pathological complete response after chemoradiation for rectal cancer: a pooled analysis of individual patient data, The Lancet Oncology, vol.11,no.9,pp , [6] Y. C. Lee, C. C. Hsieh, and J. P. Chuang, Prognostic significance of partial tumor regression after preoperative chemoradiotherapy for rectal cancer: a meta-analysis, Diseases of the Colon and Rectum,vol.56,no.9,pp ,2013. [7] E. J. Bown, G. M. Lloyd, K. M. Boyle, and A. S. Miller, Rectal cancer: prognostic indicators of long-term outcome in patients considered for surgery, International Colorectal Disease,vol.29,no.2,pp ,2014.
8 8 ISRN Surgery [8] H.-M. Quah, J. F. Chou, M. Gonen et al., Pathologic stage is most prognostic of disease-free survival in locally advanced rectal cancer patients after preoperative chemoradiation, Cancer, vol. 113, no. 1, pp , [9] C. Capirci, V. Valentini, L. Cionini et al., Prognostic value of pathologic complete response after neoadjuvant therapy in locally advanced rectal cancer: long-term analysis of 566 ypcr patients, International Radiation Oncology, Biology, Physics,vol.72,no.1,pp ,2008. [10] S. T. Martin, H. M. Heneghan, and D. C. Winter, Systematic review and meta-analysis of outcomes following pathological complete response to neoadjuvant chemoradiotherapy for rectal cancer, British Surgery,vol.99,no.7,pp , [11] V. Valentini, The right study design is needed to find out which patients benefit from preoperative chemoradiotherapy for intermediate staged rectal cancer, Onkologie,vol.34,no.1-2, pp. 6 8, [12] A. M. Mandard, F. Dalibard, J. C. Mandard et al., Pathologic assessment of tumor regression after preoperative chemoradiotherapy of esophageal carcinoma. Clinicopathologic correlations, Cancer, vol. 73, no. 11, pp , [13] O. Dworak, L. Keilholz, and A. Hoffmann, Pathological features of rectal cancer after preoperative radiochemotherapy, International Colorectal Disease,vol.12,no.1,pp.19 23, [14] R. Glynne-Jones and N. Anyamene, Just how useful an endpoint is complete pathological response after neoadjuvant chemoradiation in rectal cancer? International Radiation Oncology, Biology, Physics,vol.66,no.2,pp , [15] C. Rödel, P. Martus, T. Papadoupolos et al., Prognostic significance of tumor regression after preoperative chemoradiotherapy for rectal cancer, Clinical Oncology, vol. 23, no. 34, pp , [16] J. M. D. Wheeler, B. F. Warren, N. J. M. Mortensen et al., Quantification of histologic regression of rectal cancer after irradiation: a proposal for a modified staging system, Diseases of the Colon and Rectum,vol.45,no.8,pp ,2002. [17] K. Junker, Therapy-induced morphological changes in lung cancer, Pathologe, vol. 25, no. 6, pp , [18]G.T.Williams,P.Quirke,andN.A.Shepherd,Dataset for Colorectal Cancer, TheRoyalCollegeofPathologists,London, UK, 2nd edition, 2007, Migrated%2520Resources/Documents/G/G049-ColorectalDataset-Sep07.pdf. [19] A.S.Dhadda,P.Dickinson,A.M.Zaitoun,N.Gandhi,andE.M. Bessell, Prognostic importance of Mandard tumour regression grade following pre-operative chemo/radiotherapy for locally advanced rectal cancer, European Cancer,vol.47,no. 8, pp , [20] J. Suárez, R.Vera, E. Balén et al., Pathologic response assessed bymandardgradeisabetterprognosticfactorthandownstaging for disease-free survival after preoperative radiochemotherapy for advanced rectal cancer, Colorectal Disease, vol.10,no. 6, pp , [21] F. M. Vecchio, V. Valentini, B. D. Minsky et al., The relationship of pathologic tumor regression grade (TRG) and outcomes after preoperative therapy in rectal cancer, International Radiation Oncology, Biology, Physics,vol.62,no.3,pp , [22]J.-F.Bosset,L.Collette,G.Calaisetal., Chemotherapywith preoperative radiotherapy in rectal cancer, The New England Medicine, vol. 355, no. 11, pp , [23] J.-P. Gérard, T. Conroy, F. Bonnetain et al., Preoperative radiotherapy with or without concurrent fluorouracil and leucovorin in T3-4 rectal cancers: results of FFCD 9203, JournalofClinical Oncology, vol. 24, no. 28, pp , [24] R. Sauer, T. Liersch, S. Merkel et al., Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: results of the German CAO/ARO/AIO-94 randomized phase III trial after a median follow-up of 11 years, Clinical Oncology,vol.30,no.16,pp ,2012. [25] J. Arredondo, J. Baixauli, C. Beorlegui et al., Prognosis factors for recurrence in patients with locally advanced rectal cancer preoperatively treated with chemoradiotherapy and adjuvant chemotherapy, Diseases of the Colon and Rectum, vol. 56, no. 4, pp , [26]A.K.P.Chan,A.Wong,D.Jenken,J.Heine,D.Buie,andD. Johnson, Posttreatment TNM staging is a prognostic indicator ofsurvivalandrecurrenceintetheredorfixedrectalcarcinoma after preoperative chemotherapy and radiotherapy, International Radiation Oncology, Biology, Physics,vol.61,no. 3, pp , [27] A. Rullier, S. Gourgou-Bourgade, M. Jarlier et al., Predictive factors of positive circumferential resection margin after radiochemotherapy for rectal cancer: the French randomised trial ACCORD12/0405 PRODIGE 2, European Cancer,vol.49,no.1,pp.82 89,2013.










9 MEDIATORS of INFLAMMATION The Scientific World Journal Gastroenterology Research and Practice Diabetes Research International Endocrinology Immunology Research Disease Markers Submit your manuscripts at BioMed Research International PPAR Research Obesity Ophthalmology Evidence-Based Complementary and Alternative Medicine Stem Cells International Oncology Parkinson s Disease Computational and Mathematical Methods in Medicine AIDS Behavioural Neurology Research and Treatment Oxidative Medicine and Cellular Longevity
Case Report 17-Week Delay Surgery after Chemoradiation in Rectal Cancer with Complete Pathological Response
 Case Reports in Surgery Volume 2015, Article ID 816491, 5 pages http://dx.doi.org/10.1155/2015/816491 Case Report 17-Week Delay Surgery after Chemoradiation in Rectal Cancer with Complete Pathological
Case Reports in Surgery Volume 2015, Article ID 816491, 5 pages http://dx.doi.org/10.1155/2015/816491 Case Report 17-Week Delay Surgery after Chemoradiation in Rectal Cancer with Complete Pathological
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Radiotherapy for rectal cancer. Karin Haustermans Department of Radiation Oncology
 Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
Radiotherapy for rectal cancer Karin Haustermans Department of Radiation Oncology O U T L I N E RT with TME surgery? Neoadjuvant or adjuvant RT? 5 x 5 Gy or long-course CRT? RT with new drugs? Selection
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
State of the art: Standard(s) of radio/chemotherapy for rectal cancer
 of radio/chemotherapy for rectal cancer") State of the art: Standard(s) of radio/chemotherapy for rectal cancer Dr Ian Chau Consultant Medical Oncologist The Royal Marsden Hospital London & Surrey Disclosure Advisory Board: Sanofi Oncology, Eli-
State of the art: Standard(s) of radio/chemotherapy for rectal cancer Dr Ian Chau Consultant Medical Oncologist The Royal Marsden Hospital London & Surrey Disclosure Advisory Board: Sanofi Oncology, Eli-
1. Background. increased sphincter preservation rate. Nonetheless, the 5- year disease-free survival and overall survival rates were
 Gastroenterology Research and Practice Volume 2016, Article ID 7870815, 5 pages http://dx.doi.org/10.1155/2016/7870815 Research Article Does Extending the Waiting Time of Low-Rectal Cancer Surgery after
Gastroenterology Research and Practice Volume 2016, Article ID 7870815, 5 pages http://dx.doi.org/10.1155/2016/7870815 Research Article Does Extending the Waiting Time of Low-Rectal Cancer Surgery after
RECTAL CANCER CLINICAL CASE PRESENTATION
 RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
Carcinoma del retto: Highlights
 Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
Carcinoma del retto: Highlights Stefano Cordio Struttura Complessa di Oncologia Medica ARNAS Garibaldi Catania Roma 17 Febbraio 2018 Disclosures Advisory Committee, research funding and speakers bureau
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016. Background
 Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Mini J.Elnaggar M.D. Radiation Oncology Ochsner Medical Center 9/23/2016 Background Mostly adenocarcinoma (scc possible, but treated like anal cancer) 39, 220 cases annually Primary treatment: surgery
Rectal Cancer: Classic Hits
 Rectal Cancer: Classic Hits Charles M. Friel, MD Associate Professor of Surgery Section of Colon and Rectal Surgery University of Virginia September 28, 2016 None Disclosures 1 Objectives Review the Classic
Rectal Cancer: Classic Hits Charles M. Friel, MD Associate Professor of Surgery Section of Colon and Rectal Surgery University of Virginia September 28, 2016 None Disclosures 1 Objectives Review the Classic
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh
 Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
Early Rectal Cancer Surgical options Organ Preservation? Chinna Reddy Colorectal Surgeon Western General, Edinburgh What is Early rectal cancer? pt1t2n0m0 Predictors for LN involvement Size Depth Intramural
What Is the Ideal Tumor Regression Grading System in Rectal Cancer Patients after Preoperative Chemoradiotherapy?
 pissn 1598-2998, eissn 25-9256 Cancer Res Treat. 216;48(3):998-19 Original Article http://dx.doi.org/1.4143/crt.215.254 Open Access What Is the Ideal Tumor Regression Grading System in Rectal Cancer Patients
pissn 1598-2998, eissn 25-9256 Cancer Res Treat. 216;48(3):998-19 Original Article http://dx.doi.org/1.4143/crt.215.254 Open Access What Is the Ideal Tumor Regression Grading System in Rectal Cancer Patients
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
Case Report Mucinous Adenocarcinoma Arising in Chronic Perianal Fistula: Good Results with Neoadjuvant Chemoradiotherapy Followed by Surgery
 Hindawi Publishing Corporation Case Reports in Surgery Volume 2014, Article ID 386150, 5 pages http://dx.doi.org/10.1155/2014/386150 Case Report Mucinous Adenocarcinoma Arising in Chronic Perianal Fistula:
Hindawi Publishing Corporation Case Reports in Surgery Volume 2014, Article ID 386150, 5 pages http://dx.doi.org/10.1155/2014/386150 Case Report Mucinous Adenocarcinoma Arising in Chronic Perianal Fistula:
Current Issues and Controversies in the Management of Rectal Cancer
 Current Issues and Controversies in the Management of Rectal Cancer Ghazi M. Nsouli MD 11 th Annual Congress of the Lebanese Society of Gastroenterology November 16, 2012 GMN 20121116 1 Staging of rectal
Current Issues and Controversies in the Management of Rectal Cancer Ghazi M. Nsouli MD 11 th Annual Congress of the Lebanese Society of Gastroenterology November 16, 2012 GMN 20121116 1 Staging of rectal
Neoadjuvant Therapy for Rectal Cancer is Overrated. Joon H. Lee, Research Resident University of Colorado 8/31/2009
 Neoadjuvant Therapy for Rectal Cancer is Overrated Joon H. Lee, Research Resident University of Colorado 8/31/2009 Objectives Brief overview of staging rectal cancer Current guidelines for evaluation and
Neoadjuvant Therapy for Rectal Cancer is Overrated Joon H. Lee, Research Resident University of Colorado 8/31/2009 Objectives Brief overview of staging rectal cancer Current guidelines for evaluation and
Preoperative or Postoperative Therapy for the Management of Patients with Stage II or III Rectal Cancer
 Evidence-Based Series 2-4 Version 2 A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Preoperative or Postoperative Therapy for the Management of Patients with
Evidence-Based Series 2-4 Version 2 A Quality Initiative of the Program in Evidence-Based Care (PEBC), Cancer Care Ontario (CCO) Preoperative or Postoperative Therapy for the Management of Patients with
Correspondence should be addressed to Taha Numan Yıkılmaz;
 Advances in Medicine Volume 2016, Article ID 8639041, 5 pages http://dx.doi.org/10.1155/2016/8639041 Research Article External Validation of the Cancer of the Prostate Risk Assessment Postsurgical Score
Advances in Medicine Volume 2016, Article ID 8639041, 5 pages http://dx.doi.org/10.1155/2016/8639041 Research Article External Validation of the Cancer of the Prostate Risk Assessment Postsurgical Score
PROCARE FINAL FEEDBACK Definitions
 1 PROCARE FINAL FEEDBACK 2006-2014 Definitions Version 0.2 29/10/2015 2 Table of Contents Introduction... 3 Part 1: PROCARE indicators 2006-2014... 4 1.1. Methods... 4 1.1.1. Descriptive numbers... 4 1.1.2.
1 PROCARE FINAL FEEDBACK 2006-2014 Definitions Version 0.2 29/10/2015 2 Table of Contents Introduction... 3 Part 1: PROCARE indicators 2006-2014... 4 1.1. Methods... 4 1.1.1. Descriptive numbers... 4 1.1.2.
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/38705 holds various files of this Leiden University dissertation. Author: Gijn, Willem van Title: Rectal cancer : developments in multidisciplinary treatment,
Cover Page The handle http://hdl.handle.net/1887/38705 holds various files of this Leiden University dissertation. Author: Gijn, Willem van Title: Rectal cancer : developments in multidisciplinary treatment,
Rectal Cancer Update 2008 The Last 5 cm. Consensus Building
 Rectal Cancer Update 2008 The Last 5 cm Consensus Building Case Distal Rectal Cancer 65 male physician Rectal mass: 5cm from anal verge, 1cm above sphincter? Imaging choice: CT vs MR vs ERUS? Adjuvant
Rectal Cancer Update 2008 The Last 5 cm Consensus Building Case Distal Rectal Cancer 65 male physician Rectal mass: 5cm from anal verge, 1cm above sphincter? Imaging choice: CT vs MR vs ERUS? Adjuvant
Treatment of Locally Advanced Rectal Cancer: Current Concepts
 Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Treatment of Locally Advanced Rectal Cancer: Current Concepts James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Clinical Study Effect of Neoadjuvant Chemoradiotherapy on Locally Advanced Rectal Mucinous Adenocarcinoma: A Propensity Score-Matched Study
 Hindawi Gastroenterology Research and Practice Volume 2017, Article ID 5715219, 10 pages https://doi.org/10.1155/2017/5715219 Clinical Study Effect of Neoadjuvant Chemoradiotherapy on Locally Advanced
Hindawi Gastroenterology Research and Practice Volume 2017, Article ID 5715219, 10 pages https://doi.org/10.1155/2017/5715219 Clinical Study Effect of Neoadjuvant Chemoradiotherapy on Locally Advanced
Differential effect of concurrent chemotherapy regimen on clinical outcomes of preoperative chemoradiotherapy for locally advanced rectal cancer
 JBUON 2019; 24(2): 470-478 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Differential effect of concurrent chemotherapy regimen on clinical outcomes
JBUON 2019; 24(2): 470-478 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Differential effect of concurrent chemotherapy regimen on clinical outcomes
Preoperative adjuvant radiotherapy
 Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Preoperative adjuvant radiotherapy Dr John Hay Radiation Oncology Program BC Cancer Agency Vancouver Cancer Centre The key question for the surgeon Do you think that this tumour can be resected with clear
Kaoru Takeshima, Kazuo Yamafuji, Atsunori Asami, Hideo Baba, Nobuhiko Okamoto, Hidena Takahashi, Chisato Takagi, and Kiyoshi Kubochi
 Case Reports in Surgery Volume 2016, Article ID 4548798, 5 pages http://dx.doi.org/10.1155/2016/4548798 Case Report Successful Resection of Isolated Para-Aortic Lymph Node Recurrence from Advanced Sigmoid
Case Reports in Surgery Volume 2016, Article ID 4548798, 5 pages http://dx.doi.org/10.1155/2016/4548798 Case Report Successful Resection of Isolated Para-Aortic Lymph Node Recurrence from Advanced Sigmoid
Background: Patients and methods: Results: Conclusions:
 Chapter 7 7 Results of European pooled analysis of IORT containing multimodality treatment for locally advanced rectal cancer: adjuvant chemotherapy prevents local recurrence rather than distant metastase
Chapter 7 7 Results of European pooled analysis of IORT containing multimodality treatment for locally advanced rectal cancer: adjuvant chemotherapy prevents local recurrence rather than distant metastase
Preoperative capecitabine and pelvic radiation in locally advanced rectal cancer: preliminary results (Mansoura experience)
") Original Article Preoperative capecitabine and pelvic radiation in locally advanced rectal cancer: preliminary results (Mansoura experience) Abeer Hussien Anter 1, Ghada Ezzat Eladawei 2, Mahmoud Mosbah
Original Article Preoperative capecitabine and pelvic radiation in locally advanced rectal cancer: preliminary results (Mansoura experience) Abeer Hussien Anter 1, Ghada Ezzat Eladawei 2, Mahmoud Mosbah
Clinical Study Mucosal Melanoma in the Head and Neck Region: Different Clinical Features and Same Outcome to Cutaneous Melanoma
 ISRN Dermatology Volume 2013, Article ID 586915, 5 pages http://dx.doi.org/10.1155/2013/586915 Clinical Study Mucosal Melanoma in the Head and Neck Region: Different Clinical Features and Same Outcome
ISRN Dermatology Volume 2013, Article ID 586915, 5 pages http://dx.doi.org/10.1155/2013/586915 Clinical Study Mucosal Melanoma in the Head and Neck Region: Different Clinical Features and Same Outcome
M. Kripp, 1 K. Horisberger, 2 S. Mai, 3 P. Kienle, 2 T. Gaiser, 4 S. Post, 2 F. Wenz, 3 K. Merx, 1 and R.-D. Hofheinz 5. 1.
 Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2015, Article ID 273489, 8 pages http://dx.doi.org/10.1155/2015/273489 Research Article Does the Addition of Cetuximab to Radiochemotherapy
Hindawi Publishing Corporation Gastroenterology Research and Practice Volume 2015, Article ID 273489, 8 pages http://dx.doi.org/10.1155/2015/273489 Research Article Does the Addition of Cetuximab to Radiochemotherapy
The Role Of The Post-CRT MRI In Assessing Response
 Low Rectal Cancer: Is It Safe To Change The Plane Of Surgery? The Role Of The Post-CRT MRI In Assessing Response Nick Battersby, Mit Dattani, Nick West, Graham Branagan, Mark Gudgeon, Phil Quirke, Paris
Low Rectal Cancer: Is It Safe To Change The Plane Of Surgery? The Role Of The Post-CRT MRI In Assessing Response Nick Battersby, Mit Dattani, Nick West, Graham Branagan, Mark Gudgeon, Phil Quirke, Paris
Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach
 Case Reports in Surgery Volume 2013, Article ID 560712, 4 pages http://dx.doi.org/10.1155/2013/560712 Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach Shigeo
Case Reports in Surgery Volume 2013, Article ID 560712, 4 pages http://dx.doi.org/10.1155/2013/560712 Case Report Five-Year Survival after Surgery for Invasive Micropapillary Carcinoma of the Stomach Shigeo
Lower lymph node yield following neoadjuvant therapy for rectal cancer has no clinical significance
 Original Article Lower lymph node yield following neoadjuvant therapy for rectal cancer has no clinical significance Dedrick Kok Hong Chan 1,2, Ker-Kan Tan 1,2 1 Division of Colorectal Surgery, University
Original Article Lower lymph node yield following neoadjuvant therapy for rectal cancer has no clinical significance Dedrick Kok Hong Chan 1,2, Ker-Kan Tan 1,2 1 Division of Colorectal Surgery, University
Rectal Cancer : Curative treatment without surgery
 Rectal Cancer : Curative treatment without surgery Dieter Hahnloser dieter.hahnloser@chuv.ch CHUV University Hospital Lausanne Switzerland Reasons for intervention (surgery) Cure Live longer Feel better
Rectal Cancer : Curative treatment without surgery Dieter Hahnloser dieter.hahnloser@chuv.ch CHUV University Hospital Lausanne Switzerland Reasons for intervention (surgery) Cure Live longer Feel better
ADJUVANT CHEMOTHERAPY FOR RECTAL CANCER
 ESMO Preceptorship Programme Colorectal Cancer Barcelona November, 25-26, 2016 ADJUVANT CHEMOTHERAPY FOR RECTAL CANCER Andrés Cervantes Professor of Medicine OLD APPROACH TO RECTAL CANCER Surgical resection
ESMO Preceptorship Programme Colorectal Cancer Barcelona November, 25-26, 2016 ADJUVANT CHEMOTHERAPY FOR RECTAL CANCER Andrés Cervantes Professor of Medicine OLD APPROACH TO RECTAL CANCER Surgical resection
NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES. Devon Paula Richardson
 NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES by Devon Paula Richardson Submitted in partial fulfilment of the requirements for the degree of Master
NOVA SCOTIA RECTAL CANCER PROJECT: A POPULATION-BASED ASSESSMENT OF RECTAL CANCER CARE AND OUTCOMES by Devon Paula Richardson Submitted in partial fulfilment of the requirements for the degree of Master
Rob Glynne-Jones Mount Vernon Cancer Centre
 ESMO Preceptorship Programme Colorectal Cancer Valencia May 2018 State of the art: Standards of care in preoperative treatment for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures:
ESMO Preceptorship Programme Colorectal Cancer Valencia May 2018 State of the art: Standards of care in preoperative treatment for rectal cancer Rob Glynne-Jones Mount Vernon Cancer Centre My Disclosures:
IJC International Journal of Cancer
 IJC International Journal of Cancer Adjuvant chemotherapy in rectal cancer: Defining subgroups who may benefit after neoadjuvant chemoradiation and resection A pooled analysis of 3,313 patients Monique
IJC International Journal of Cancer Adjuvant chemotherapy in rectal cancer: Defining subgroups who may benefit after neoadjuvant chemoradiation and resection A pooled analysis of 3,313 patients Monique
PROCARE FINAL FEEDBACK
 1 PROCARE FINAL FEEDBACK General report 2006-2014 Version 2.1 08/12/2015 PROCARE indicators 2006-2014... 3 Demographic Data... 3 Diagnosis and staging... 4 Time to first treatment... 6 Neoadjuvant treatment...
1 PROCARE FINAL FEEDBACK General report 2006-2014 Version 2.1 08/12/2015 PROCARE indicators 2006-2014... 3 Demographic Data... 3 Diagnosis and staging... 4 Time to first treatment... 6 Neoadjuvant treatment...
Long Term Outcomes of Preoperative versus
 RESEARCH ARTICLE Long Term Outcomes of Preoperative versus Postoperative Concurrent Chemoradiation for Locally Advanced Rectal Cancer: Experience from Ramathibodi Medical School in Thailand Pichayada Darunikorn
RESEARCH ARTICLE Long Term Outcomes of Preoperative versus Postoperative Concurrent Chemoradiation for Locally Advanced Rectal Cancer: Experience from Ramathibodi Medical School in Thailand Pichayada Darunikorn
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Clinical Study Metastasectomy of Pulmonary Metastases from Osteosarcoma: Prognostic Factors and Indication for Repeat Metastasectomy
 Respiratory Medicine Volume 2015, Article ID 570314, 5 pages http://dx.doi.org/10.1155/2015/570314 Clinical Study Metastasectomy of Pulmonary Metastases from Osteosarcoma: Prognostic Factors and Indication
Respiratory Medicine Volume 2015, Article ID 570314, 5 pages http://dx.doi.org/10.1155/2015/570314 Clinical Study Metastasectomy of Pulmonary Metastases from Osteosarcoma: Prognostic Factors and Indication
3/8/2014. Case Presentation. Primary Treatment of Anal Cancer. Anatomy. Overview. March 6, 2014
 Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Latkauskas et al. BMC Cancer (2016) 16:927 DOI /s
 16:927 DOI /s") Latkauskas et al. BMC Cancer (2016) 16:927 DOI 10.1186/s12885-016-2959-9 RESEARCH ARTICLE reoperative conventional chemoradiotherapy versus short-course radiotherapy with delayed surgery for rectal cancer:
Latkauskas et al. BMC Cancer (2016) 16:927 DOI 10.1186/s12885-016-2959-9 RESEARCH ARTICLE reoperative conventional chemoradiotherapy versus short-course radiotherapy with delayed surgery for rectal cancer:
COLON AND RECTAL CANCER
 COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
COLON AND RECTAL CANCER Mark Sun, MD Clinical Associate Professor of Surgery University of Minnesota No disclosures Objectives 1) Understand the epidemiology, management, and prognosis of colon and rectal
Research Article Survival Benefit of Adjuvant Radiation Therapy for Gastric Cancer following Gastrectomy and Extended Lymphadenectomy
 International Surgical Oncology Volume 2012, Article ID 307670, 7 pages doi:10.1155/2012/307670 Research Article Survival Benefit of Adjuvant Radiation Therapy for Gastric Cancer following Gastrectomy
International Surgical Oncology Volume 2012, Article ID 307670, 7 pages doi:10.1155/2012/307670 Research Article Survival Benefit of Adjuvant Radiation Therapy for Gastric Cancer following Gastrectomy
L impatto dell imaging sulla definizione della strategia terapeutica
 GISCoR L impatto dell imaging sulla definizione della strategia terapeutica M. Galeandro U.C. Radioterapia Oncologica ASMN-IRCCS Reggio Emilia 14 Novembre 2014 Rectal Cancer TNM AJCC-7 th edition 2010
GISCoR L impatto dell imaging sulla definizione della strategia terapeutica M. Galeandro U.C. Radioterapia Oncologica ASMN-IRCCS Reggio Emilia 14 Novembre 2014 Rectal Cancer TNM AJCC-7 th edition 2010
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Radiotherapy for Rectal Cancer. Kevin Palumbo Adelaide Radiotherapy Centre
 Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
Radiotherapy for Rectal Cancer Kevin Palumbo Adelaide Radiotherapy Centre Overview CRC are common (3 rd commonest cancer) rectal Ca approx 25-30% of all CRC. Presentation PR bleeding: beware attributing
POSSIBILITIES TO ASSESS THE EFFICACY OF THE NEOADJUVANT TREATMENT FOR LOW RECTAL CANCER, IN ORDER TO APPLY A SPHINCTER SAVING PROCEDURE
 UNIVERSITY OF MEDICINE AND PHARMACY GR. T. POPA IAȘI POSSIBILITIES TO ASSESS THE EFFICACY OF THE NEOADJUVANT TREATMENT FOR LOW RECTAL CANCER, IN ORDER TO APPLY A SPHINCTER SAVING PROCEDURE PhD THESIS (ABSTRACT)
UNIVERSITY OF MEDICINE AND PHARMACY GR. T. POPA IAȘI POSSIBILITIES TO ASSESS THE EFFICACY OF THE NEOADJUVANT TREATMENT FOR LOW RECTAL CANCER, IN ORDER TO APPLY A SPHINCTER SAVING PROCEDURE PhD THESIS (ABSTRACT)
CHAPTER 7 Concluding remarks and implications for further research
 CONCLUDING REMARKS AND IMPLICATIONS FOR FURTHER RESEARCH CHAPTER 7 Concluding remarks and implications for further research 111 CHAPTER 7 Molecular staging of large sessile rectal tumors In this thesis,
CONCLUDING REMARKS AND IMPLICATIONS FOR FURTHER RESEARCH CHAPTER 7 Concluding remarks and implications for further research 111 CHAPTER 7 Molecular staging of large sessile rectal tumors In this thesis,
Hagit Tulchinsky, MD, 1,2 Einat Shmueli, MD, 3 Arie Figer, MD, 3 Joseph M. Klausner, MD, 2 and Micha Rabau, MD 1,2
 Annals of Surgical Oncology DOI: 10.1245/s10434-008-9892-3 An Interval [7 Weeks between Neoadjuvant Therapy and Surgery Improves Pathologic Complete Response and Disease Free Survival in Patients with
Annals of Surgical Oncology DOI: 10.1245/s10434-008-9892-3 An Interval [7 Weeks between Neoadjuvant Therapy and Surgery Improves Pathologic Complete Response and Disease Free Survival in Patients with
Research Article Prognostic Factors in Advanced Non-Small-Cell Lung Cancer Patients: Patient Characteristics and Type of Chemotherapy
 SAGE-Hindawi Access to Research Lung Cancer International Volume 2011, Article ID 152125, 4 pages doi:10.4061/2011/152125 Research Article Prognostic Factors in Advanced Non-Small-Cell Lung Cancer Patients:
SAGE-Hindawi Access to Research Lung Cancer International Volume 2011, Article ID 152125, 4 pages doi:10.4061/2011/152125 Research Article Prognostic Factors in Advanced Non-Small-Cell Lung Cancer Patients:
Rectal Cancer. Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco
 Rectal Cancer Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment for Rectal Cancer Improve Local Control Improved
Rectal Cancer Madhulika G. Varma MD Associate Professor and Chief Section of Colorectal Surgery University of California, San Francisco Modern Treatment for Rectal Cancer Improve Local Control Improved
Rectal Cancer. GI Practice Guideline
 Rectal Cancer GI Practice Guideline Dr. Brian Dingle MSc, MD, FRCPC Dr. Francisco Perera MD, FRCPC (Radiation Oncologist) Dr. Jay Engel MD, FRCPC (Surgical Oncologist) Approval Date: 2006 This guideline
Rectal Cancer GI Practice Guideline Dr. Brian Dingle MSc, MD, FRCPC Dr. Francisco Perera MD, FRCPC (Radiation Oncologist) Dr. Jay Engel MD, FRCPC (Surgical Oncologist) Approval Date: 2006 This guideline
UCL. Rectum Adenocarcinoma. Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans
 Rectum Adenocarcinoma Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans Fifth Belgian Surgical Week May 6th, 2004, Oostende SOR rectum adenocarcinoma Indication of radiotherapy
Rectum Adenocarcinoma Quality of conformal radiotherapy Impact for the surgeon P. Scalliet & K. Haustermans Fifth Belgian Surgical Week May 6th, 2004, Oostende SOR rectum adenocarcinoma Indication of radiotherapy
Staging of cancer patients is an important tool for the selection
 CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2007;5:997 1003 Improvement of Staging by Combining Tumor and Treatment Parameters: The Value for Prognostication in Rectal Cancer MARLEEN J. E. M. GOSENS,* J.
CLINICAL GASTROENTEROLOGY AND HEPATOLOGY 2007;5:997 1003 Improvement of Staging by Combining Tumor and Treatment Parameters: The Value for Prognostication in Rectal Cancer MARLEEN J. E. M. GOSENS,* J.
Innovations in Rectal Cancer Surgery
 Innovations in Rectal Cancer Surgery A. D Hoore MD PhD, EBSQ-CR, (hon)fascrs A. Wolthuis MD PhD, EBSQ-CR, FACS G. Bislenghi MD Departement of Abdominal Surgery University Hospitals Leuven, Belgium invasiveness
Innovations in Rectal Cancer Surgery A. D Hoore MD PhD, EBSQ-CR, (hon)fascrs A. Wolthuis MD PhD, EBSQ-CR, FACS G. Bislenghi MD Departement of Abdominal Surgery University Hospitals Leuven, Belgium invasiveness
Pathohistological Assessment of the Circular Margin of Resection During Total Mesorectal Excision, Conducted on The Malignant Formations of the Rectum
 International Journal of Research Studies in Science, Engineering and Technology Volume 4, Issue 5, 2017, PP 17-22 ISSN : 2349-476X http://dx.doi.org/10.22259/ijrsset.0405004 Pathohistological Assessment
International Journal of Research Studies in Science, Engineering and Technology Volume 4, Issue 5, 2017, PP 17-22 ISSN : 2349-476X http://dx.doi.org/10.22259/ijrsset.0405004 Pathohistological Assessment
Meta analysis in Rectal Cancer
 Meta analysis in Rectal Cancer Dr. Monica Irukulla Professor and Head Department of Radiation Oncology Nizam s Institute of Medical Sciences hyderabad Areas of meta analysis in rectal cancers Epidemiology
Meta analysis in Rectal Cancer Dr. Monica Irukulla Professor and Head Department of Radiation Oncology Nizam s Institute of Medical Sciences hyderabad Areas of meta analysis in rectal cancers Epidemiology
COLON AND RECTAL CANCER
 No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
No disclosures COLON AND RECTAL CANCER Mark Sun, MD Clinical Assistant Professor of Surgery University of Minnesota Colon and Rectal Cancer Statistics Overall Incidence 2016 134,490 new cases 8.0% of all
Opportunity for palliative care Research
 Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
Differential lymph node retrieval in rectal cancer: associated factors and effect on survival
 Original Article Differential lymph node retrieval in rectal cancer: associated factors and effect on survival Cedrek McFadden 1, Brian McKinley 1, Brian Greenwell 2, Kaylee Knuckolls 1, Patrick Culumovic
Original Article Differential lymph node retrieval in rectal cancer: associated factors and effect on survival Cedrek McFadden 1, Brian McKinley 1, Brian Greenwell 2, Kaylee Knuckolls 1, Patrick Culumovic
Index. Surg Oncol Clin N Am 14 (2005) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Surg Oncol Clin N Am 14 (2005) 433 439 Index Note: Page numbers of article titles are in boldface type. A Abdominosacral resection, of recurrent rectal cancer, 202 215 Ablative techniques, image-guided,
Disclosure. Acknowledgement. What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Rectal cancer imaging. None
 What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
What is the Best Workup for Rectal Cancer Staging: US/MRI/PET? Zhen Jane Wang, MD Assistant Professor in Residence UC SF Department of Radiology Disclosure None Acknowledgement Hueylan Chern, MD, Department
Locoregional treatment Session Oral Abstract Presentation Saulo Brito Silva
 Locoregional treatment Session Oral Abstract Presentation Saulo Brito Silva Background Post-operative radiotherapy (PORT) improves disease free and overall suvivallin selected patients with breast cancer
Locoregional treatment Session Oral Abstract Presentation Saulo Brito Silva Background Post-operative radiotherapy (PORT) improves disease free and overall suvivallin selected patients with breast cancer
Surgical Management of Advanced Stage Colon Cancer. Nathan Huber, MD 6/11/14
 Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Research Article Prognostic Implication of Predominant Histologic Subtypes of Lymph Node Metastases in Surgically Resected Lung Adenocarcinoma
 BioMed Research International, Article ID 64568, 6 pages http://dx.doi.org/.55/24/64568 Research Article Prognostic Implication of Predominant Histologic Subtypes of Lymph Node Metastases in Surgically
BioMed Research International, Article ID 64568, 6 pages http://dx.doi.org/.55/24/64568 Research Article Prognostic Implication of Predominant Histologic Subtypes of Lymph Node Metastases in Surgically
SMJ Singapore Medical Journal
 SMJ Singapore Medical Journal ONLINE FIRST PUBLICATION Online first papers have undergone full scientific review and copyediting, but have not been typeset or proofread. To cite this article, use the DOIs
SMJ Singapore Medical Journal ONLINE FIRST PUBLICATION Online first papers have undergone full scientific review and copyediting, but have not been typeset or proofread. To cite this article, use the DOIs
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE
 NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of preoperative high dose rate brachytherapy for rectal cancer Rectal cancer is a
NATIONAL INSTITUTE FOR HEALTH AND CARE EXCELLENCE INTERVENTIONAL PROCEDURES PROGRAMME Interventional procedure overview of preoperative high dose rate brachytherapy for rectal cancer Rectal cancer is a
Short course radiation therapy for rectal cancer in the elderly: can radical surgery be avoided?
 Short communication Short course radiation therapy for rectal cancer in the elderly: can radical surgery be avoided? Michael A. Cummings 1, Kenneth Y. Usuki 1, Fergal J. Fleming 2, Mohamedtaki A. Tejani
Short communication Short course radiation therapy for rectal cancer in the elderly: can radical surgery be avoided? Michael A. Cummings 1, Kenneth Y. Usuki 1, Fergal J. Fleming 2, Mohamedtaki A. Tejani
R. J. L. F. Loffeld, 1 P. E. P. Dekkers, 2 and M. Flens Introduction
 ISRN Gastroenterology Volume 213, Article ID 87138, 5 pages http://dx.doi.org/1.1155/213/87138 Research Article The Incidence of Colorectal Cancer Is Decreasing in the Older Age Cohorts in the Zaanstreek
ISRN Gastroenterology Volume 213, Article ID 87138, 5 pages http://dx.doi.org/1.1155/213/87138 Research Article The Incidence of Colorectal Cancer Is Decreasing in the Older Age Cohorts in the Zaanstreek
A Review of Rectal Cancer. Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center
 A Review of Rectal Cancer Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center No disclosures Disclosures About me.. Grew up in Southern Illinois
A Review of Rectal Cancer Tim Geiger, MD Assistant Professor of Surgery, Colon and Rectal Surgery Vanderbilt University Medical Center No disclosures Disclosures About me.. Grew up in Southern Illinois
Peritoneal Involvement in Stage II Colon Cancer
 Anatomic Pathology / PERITONEAL INVOLVEMENT IN STAGE II COLON CANCER Peritoneal Involvement in Stage II Colon Cancer A.M. Lennon, MB, MRCPI, H.E. Mulcahy, MD, MRCPI, J.M.P. Hyland, MCh, FRCS, FRCSI, C.
Anatomic Pathology / PERITONEAL INVOLVEMENT IN STAGE II COLON CANCER Peritoneal Involvement in Stage II Colon Cancer A.M. Lennon, MB, MRCPI, H.E. Mulcahy, MD, MRCPI, J.M.P. Hyland, MCh, FRCS, FRCSI, C.
Cover Page. The handle holds various files of this Leiden University dissertation.
 Cover Page The handle http://hdl.handle.net/1887/38705 holds various files of this Leiden University dissertation. Author: Gijn, Willem van Title: Rectal cancer : developments in multidisciplinary treatment,
Cover Page The handle http://hdl.handle.net/1887/38705 holds various files of this Leiden University dissertation. Author: Gijn, Willem van Title: Rectal cancer : developments in multidisciplinary treatment,
The role of neoadjuvant radiotherapy for locally-advanced rectal cancer with resectable synchronous metastasis
 Original Article The role of neoadjuvant radiotherapy for locally-advanced rectal cancer with resectable synchronous metastasis Croix C. Fossum 1, Jasim Y. Alabbad 2, Lindsay B. Romak 3, Christopher L.
Original Article The role of neoadjuvant radiotherapy for locally-advanced rectal cancer with resectable synchronous metastasis Croix C. Fossum 1, Jasim Y. Alabbad 2, Lindsay B. Romak 3, Christopher L.
WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER?
 CANCER STAGING TNM and prognosis in CRC WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER? Alessandro Lugli, MD Institute of Pathology University of Bern Switzerland Maastricht, June 19
CANCER STAGING TNM and prognosis in CRC WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER? Alessandro Lugli, MD Institute of Pathology University of Bern Switzerland Maastricht, June 19
PATHOLOGIC FACTORS PROGNOSTIC OF SURVIVAL IN PATIENTS WITH GI TRACT AND PANCREATIC CARCINOMA TREATED WITH NEOADJUVANT THERAPY
 PATHOLOGIC FACTORS PROGNOSTIC OF SURVIVAL IN PATIENTS WITH GI TRACT AND PANCREATIC CARCINOMA TREATED WITH NEOADJUVANT THERAPY Jeannelyn S. Estrella, MD Department of Pathology The UT MD Anderson Cancer
PATHOLOGIC FACTORS PROGNOSTIC OF SURVIVAL IN PATIENTS WITH GI TRACT AND PANCREATIC CARCINOMA TREATED WITH NEOADJUVANT THERAPY Jeannelyn S. Estrella, MD Department of Pathology The UT MD Anderson Cancer
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Best Papers. F. Fusco
 Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Best Papers UROLOGY F. Fusco Best papers - 2015 RP/RT Oncological outcomes RP/RT IN ct3 Utilization trends RP/RT Complications Evolving role of elnd /Salvage LND This cohort reflects the current clinical
Wait-and-see or radical surgery for rectal cancer patients with a clinical complete response after neoadjuvant chemoradiotherapy: a cohort study
 /, Vol. 6, No. 39 Wait-and-see or radical surgery for rectal cancer patients with a clinical complete response after neoadjuvant chemoradiotherapy: a cohort study Jun Li 1, Hao Liu 2, Jie Yin 3, Sai Liu
/, Vol. 6, No. 39 Wait-and-see or radical surgery for rectal cancer patients with a clinical complete response after neoadjuvant chemoradiotherapy: a cohort study Jun Li 1, Hao Liu 2, Jie Yin 3, Sai Liu
Treatment strategy of metastatic rectal cancer
 35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
35.Schweizerische Koloproktologie-Tagung Treatment strategy of metastatic rectal cancer Gilles Mentha University hospital of Geneva Bern, January 18th, 2014 Colorectal cancer is the third most frequent
Fourth versus eighth week surgery after neoadjuvant radiochemotherapy in T3-4/N0+ rectal cancer: Istanbul R-01 study
 Original Article Fourth versus eighth week surgery after neoadjuvant radiochemotherapy in T3-4/N0+ rectal cancer: Istanbul R-01 study Sezer Saglam 1, Dursun Bugra 2, Esra K. Saglam 3, Oktar Asoglu 4, Emre
Original Article Fourth versus eighth week surgery after neoadjuvant radiochemotherapy in T3-4/N0+ rectal cancer: Istanbul R-01 study Sezer Saglam 1, Dursun Bugra 2, Esra K. Saglam 3, Oktar Asoglu 4, Emre
Original Article The value of lymph node ratio in the prediction of rectal cancer patient survival after preoperative chemoradiotherapy
 Int J Clin Exp Pathol 2018;11(12):5992-6001 www.ijcep.com /ISSN:1936-2625/IJCEP0086231 Original Article The value of lymph node ratio in the prediction of rectal cancer patient survival after preoperative
Int J Clin Exp Pathol 2018;11(12):5992-6001 www.ijcep.com /ISSN:1936-2625/IJCEP0086231 Original Article The value of lymph node ratio in the prediction of rectal cancer patient survival after preoperative
Rectal cancer: Poster Session Review
 AIOM PostASCO GI Roma, 5-6 febbraio 2016 Rectal cancer: Poster Session Review Sara Lonardi SS Trattamento Multidisciplinare Tumori Colorettali - UOC Oncologia Medica 1 Dipartimento di Oncologia Clinica
AIOM PostASCO GI Roma, 5-6 febbraio 2016 Rectal cancer: Poster Session Review Sara Lonardi SS Trattamento Multidisciplinare Tumori Colorettali - UOC Oncologia Medica 1 Dipartimento di Oncologia Clinica
Pre- Versus Post-operative Radiotherapy
 Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Case Report Two Cases of Small Cell Cancer of the Maxillary Sinus Treated with Cisplatin plus Irinotecan and Radiotherapy
 Case Reports in Otolaryngology Volume 2013, Article ID 893638, 4 pages http://dx.doi.org/10.1155/2013/893638 Case Report Two Cases of Small Cell Cancer of the Maxillary Sinus Treated with Cisplatin plus
Case Reports in Otolaryngology Volume 2013, Article ID 893638, 4 pages http://dx.doi.org/10.1155/2013/893638 Case Report Two Cases of Small Cell Cancer of the Maxillary Sinus Treated with Cisplatin plus
Transanal endoscopic microsurgery for early rectal cancer: single center experience
 Original paper Videosurgery Transanal endoscopic microsurgery for early rectal cancer: single center experience Narimantas Samalavicius 1,2, Marijus Ambrazevicius 1, Alfredas Kilius 1, Kestutis Petrulis
Original paper Videosurgery Transanal endoscopic microsurgery for early rectal cancer: single center experience Narimantas Samalavicius 1,2, Marijus Ambrazevicius 1, Alfredas Kilius 1, Kestutis Petrulis
ASCO GI 2018 Rectal Cancer Poster Review Filippo Pietrantonio INT Milan
 ASCO GI 2018 Rectal Cancer Poster Review Filippo Pietrantonio INT Milan Rome, 16 February 18 AGENDA rectal cancer data - Staging - Prognostic Factors - Management strategies Staging AJCC 7 edition staging:
ASCO GI 2018 Rectal Cancer Poster Review Filippo Pietrantonio INT Milan Rome, 16 February 18 AGENDA rectal cancer data - Staging - Prognostic Factors - Management strategies Staging AJCC 7 edition staging:
Index. Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
Note: Page numbers of article titles are in boldface type. A Abdominoperineal excision, of rectal cancer, 93 111 current controversies in, 106 109 extent of perineal dissection and removal of pelvic floor,
NUMERATOR: Reports that include the pt category, the pn category and the histologic grade
 Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
State-of-the-art of surgery for resectable primary tumors
 Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
Early colorectal cancer State-of-the-art of surgery for resectable primary tumors (Special focus on rectal cancer surgery) Stefan Heinrich & Hauke Lang Department of General, Visceral and University Hospital
Evaluation of the Efficacy of Modified De Gramont and Modified FOLFOX4 Regimens for Adjuvant Therapy of Locally Advanced Rectal Cancer
 Efficacy of Modified De Gramont and FOLFOX4 Regimens for Locally Advanced Rectal Cancer RESEARCH COMMUNICATION Evaluation of the Efficacy of Modified De Gramont and Modified FOLFOX4 Regimens for Adjuvant
Efficacy of Modified De Gramont and FOLFOX4 Regimens for Locally Advanced Rectal Cancer RESEARCH COMMUNICATION Evaluation of the Efficacy of Modified De Gramont and Modified FOLFOX4 Regimens for Adjuvant
NUMERATOR: Reports that include the pt category, the pn category and the histologic grade
 Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Clinical Study Postchemotherapy Histopathological Evaluation of Ovarian Carcinoma: A 40-Case Study
 Chemotherapy Research and Practice Volume 2015, Article ID 197871, 4 pages http://dx.doi.org/10.1155/2015/197871 Clinical Study Postchemotherapy Histopathological Evaluation of Ovarian Carcinoma: A 40-Case
Chemotherapy Research and Practice Volume 2015, Article ID 197871, 4 pages http://dx.doi.org/10.1155/2015/197871 Clinical Study Postchemotherapy Histopathological Evaluation of Ovarian Carcinoma: A 40-Case
Is adjuvant radiotherapy warranted in resected pt1-2 node-positive rectal cancer?
 Peng et al. Radiation Oncology 2013, 8:290 RESEARCH Open Access Is adjuvant radiotherapy warranted in resected pt1-2 node-positive rectal cancer? Junjie Peng 1,2, Xinxiang Li 1,2, Ying Ding 3, Debing Shi
Peng et al. Radiation Oncology 2013, 8:290 RESEARCH Open Access Is adjuvant radiotherapy warranted in resected pt1-2 node-positive rectal cancer? Junjie Peng 1,2, Xinxiang Li 1,2, Ying Ding 3, Debing Shi
Neoadjuvant treatment Evolution and Current Status
 Neoadjuvant treatment Evolution and Current Status Dr Andrew See Radiation Oncologist 2017 Rectal Cancer Symposium Friday 10 th November 2017 2 1 Major Randomised Trials Supporting Neoadjuvant CRT Trial
Neoadjuvant treatment Evolution and Current Status Dr Andrew See Radiation Oncologist 2017 Rectal Cancer Symposium Friday 10 th November 2017 2 1 Major Randomised Trials Supporting Neoadjuvant CRT Trial
Radiotherapy and Conservative Surgery For Merkel Cell Carcinoma - The British Columbia Cancer Agency Experience
 Radiotherapy and Conservative Surgery For Merkel Cell Carcinoma - The British Columbia Cancer Agency Experience Poster No.: RO-0003 Congress: RANZCR FRO 2012 Type: Scientific Exhibit Authors: C. Harrington,
Radiotherapy and Conservative Surgery For Merkel Cell Carcinoma - The British Columbia Cancer Agency Experience Poster No.: RO-0003 Congress: RANZCR FRO 2012 Type: Scientific Exhibit Authors: C. Harrington,
Available at journal homepage:
 European Journal of Cancer (2012) 48, 1781 1790 Available at www.sciencedirect.com journal homepage: www.ejconline.com What is the clinical benefit of preoperative chemoradiotherapy with 5FU/leucovorin
European Journal of Cancer (2012) 48, 1781 1790 Available at www.sciencedirect.com journal homepage: www.ejconline.com What is the clinical benefit of preoperative chemoradiotherapy with 5FU/leucovorin