The Immunotherapy of Oncology
|
|
|
- Theodore Atkins
- 6 years ago
- Views:
Transcription
1 The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014
2 Disclosures: Geoffrey R. Weiss, M.D. None
3 The History A. Chekov: It has long been noted that the growth of malignant tumors halts for a time when this disease [erysipelas] is present. Coley s Toxins: Strep pyogenes, Serr marcescens. BCG for superficial bladder cancer. Coley WB, AmJMedSci, 1893 Lamm DL, NEJM, 1991
4 Interleukin-2/LAK Cells NCI Surgery Branch # Patients Cancer Total Responses Melanoma 7 4 Colorectal 9 3 Sarcoma 4 0 Renal Cell 3 3 Lung 1 1 Esophagus 1 0 Total (44%) Rosenberg et al., NEJM, 1985

5 IL-2/LAK Clinical Protocol week L A K High-dose IL-2 600,000 IU/kg Q8hr x 14 doses Lymphocytapheresis Tumor measurements at Week 6 and 12 then every 12 weeks Repeat Q12 weeks Max 3 cycles
6 High-Dose Interleukin-2 in Renal Cell Carcinoma 255 metastatic RCC patients. 7 clinical trials of high-dose IL-2 alone. 15% overall response in metastatic RCC. Median duration of response: 54 months ( mos). Interleukin-2 FDA-approved for metastatic RCC in 1992.
7 High-Dose Interleukin-2 in Metastatic Malignant Melanoma 270 MM patients treated with high-dose interleukin-2 in 8 clinical trials 16% overall response rate in metastatic MM: 24 without progression at 1 year 10 CRs > 3-8 years Interleukin-2 FDA-approved 1998 for MMM

8 Sipuleucel-T for Advanced Prostate Cancer
9 Sipuleucel-T for Advanced Prostate Cancer 512 pts. Leukapheresis Wks 0, 2, 4 PMCs (APCs)+ PA2024 PMCs (APCs) Placebo Infusion 341 pts Infusion 171 pts PA2024=PAP/GMCSF Fusion Product Kantoff P et al ASCO GU Kantoff P et al. NEJM 2010
10 Sipuleucel-T for Advanced Prostate Cancer
11
12
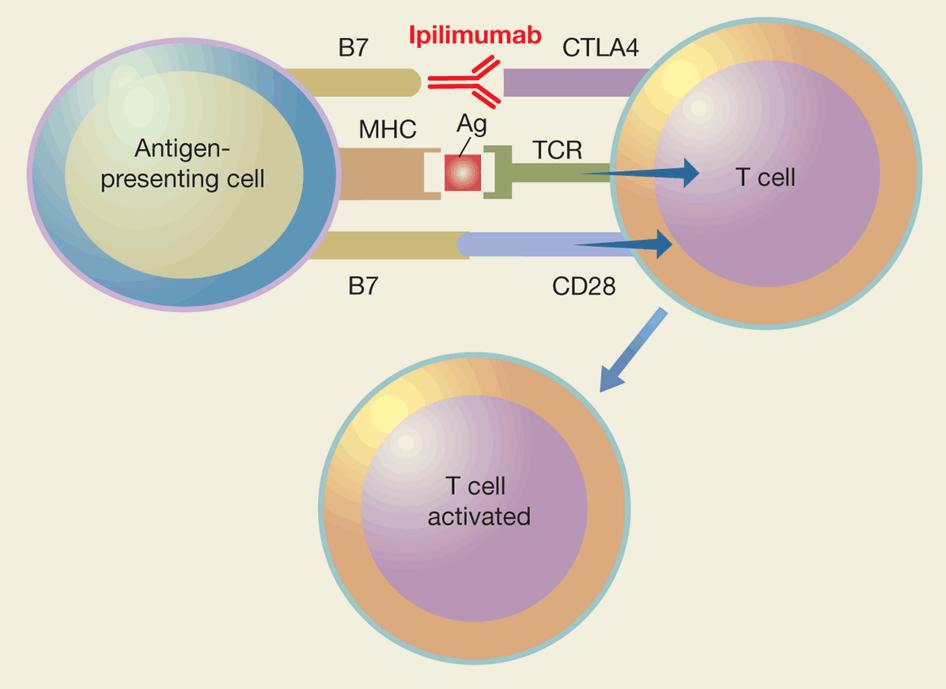
13 CTLA-4 BLOCKADE MELANOMA
14 Ipilimumab vs. Ipi/gp100 vs. gp100 In Metastatic Melanoma Phase III Trial 2 nd Line Therapy 676 patients: Stages III-IV Melanoma Category Med OS ORR 2-year Surv Ipilimumab 10.1 mos 10.9% Ipilimumab + gp100 Hodi FS et al, NEJM mos 5.7% 24% gp mos 1.5% 14% HR 0.68 P < 0.003
15 Hodi FS et al. N Engl J Med 2010; 363:
16 Ipilimumab plus Dacarbazine for Metastatic Melanoma Randomized phase III trial ipilimumab 10 mg/kg iv q3wks x 4 dacarbazine 850 mg/m 2 iv q3wks x 4 Untreated MMM Primary endpoint: OS placebo dacarbazine 850 mg/m 2 iv q3wks x 4 dacarbazine given alone weeks Robert C, NEJM 2011
17 Dacarbazine + Ipilimumab Overall Survival, Robert C et al. N Engl J Med 2011;364:
18 Dacarbazine + Ipilimumab Overall Survival study. Michele Maio et al. JCO 2015;33:
19 Tremilimumab in Metastatic Melanoma 655 Pts No prior Rx Tremilimumab, 15 mg/kg Chemo (Physician Choice) Endpoint Tremilimumab Chemo Med OS 12.6 mos 10.7 mos HR for Death 0.88 P=0.127 Ribas A et al. J Clin Oncol 2013
20
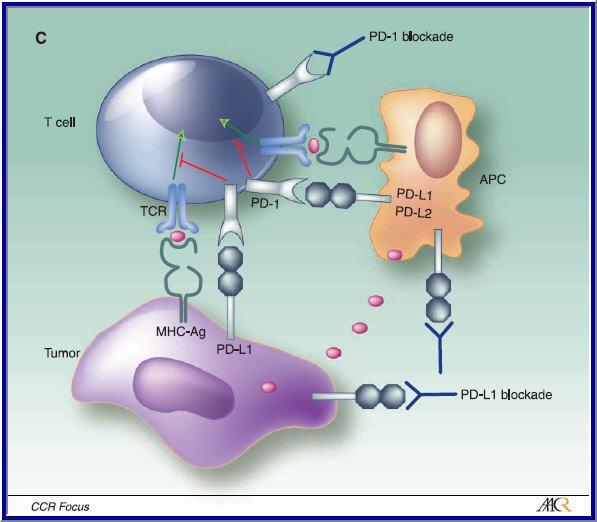
21 Immune Checkpoint Inhibitors Nivolumab and Pembrolizumab Nivolumab: Fully human IgG4 antibody, blocks ligand activation of PD-1 receptor. Pembrolizumab: Humanized IgG4 antibody, blocks ligand activation of PD-1 receptor.
22 Nivolumab in Cancer Treatment Phase I trial. Advanced melanoma, NSCLC, renal cell cancer, CR prostate cancer, colorectal cancer. Nivolumab: 1 mg/kg; 3 mg/kg; 10 mg/kg; i.v, Q2wks. 5 expansion cohorts for each disease. IHC for tumor PDL-1 expression. Topalian SL et al. NEJM 2012.
23 Nivolumab in Cancer Treatment 296 patients. No maximum tolerated dose defined. 3 deaths from pulmonary toxicity. Responses NSCLC Melanoma Renal cell 18% (14/76) 28% (26/94) 27% (9/33) Topalian SL et al. NEJM 2012.
24 Nivolumab in Cancer Treatment 20/31 responses exceeded 1 year s duration. None of PDL-1 negative tumors had response. 9 of 25 PDL-1 positive tumors had response. Dominant toxicities: Diarrhea (11%), Rash (12%), Pruritis (9%). Topalian SL et al. NEJM 2012.
25 PD-1/PDL-1 BLOCKADE MELANOMA
26 Nivolumab vs. DTIC in Metastatic Melanoma Phase III as 1 st Line Therapy No prior Rx, BRAF negative 418 Pts Nivo, 3 mg/kg, iv, Q2wks + Placebo DTIC, 1000 mg/m 2, iv, Q3wks + Placebo Robert C et al. NEJM, 2014
27 Nivolumab vs. DTIC in Metastatic Melanoma Category Nivo DTIC OS 1 Yr 72.9% 42.1% Med PFS 5.1 mos 2.2 mos ORR 40% 13.9% HR for Death 0.42 P<0.001 Robert C et al. NEJM, 2014
28 Pembrolizumab in Melanoma KEYNOTE-001 Phase I-II trial with expansion cohort in melanoma. Objectives: assess safety and antitumor activity. 135 patients treated: 1) prior ipilimumab, or 2) < 2 prior regimens for advanced disease. Pembrolizumab administered i.v. over 30 minutes. Cohort 10 mg/kg Q2 wks 10 mg/kg Q3 wks 2 mg/kg Q 3 wks No prior Ipi Prior Ipi
29 Pembrolizumab in Melanoma KEYNOTE-001 Safety 135 patients at least 1 dose pembrolizumab. Common symptoms: fatigue, myalgia, headache, fever. 2% serious/life-threatening toxicity. Autoimmune reactions Vitiligo 9% Hypothyroidism 8% Pneumonitis 4% Hamid O, NEJM, 2013



 38% (44) Prior")



30 Pembrolizumab in Melanoma KEYNOTE-001 % Response (# patients) Cohort 10 mg/kg Q 2 wks 10 mg/kg Q 3 wks 2 mg/kg Q 3 wks Total No prior ipi 49 % (19) 26% (5) 25% (5) 38% (44) Prior ipi 62% (8) 27% (7) -- Among 135 patients treated, median PFS = 36 weeks. Duration of response mos. One-year overall survival 81%. Hamid O, NEJM, 2013
31 KEYNOTE-006 Pembrolizumab vs. Ipilimumab Pembro, 10 mg/kg, iv Q 2 weeks 834 pts Pembro, 10 mg/kg, iv Q 3 weeks St III-IV Unresect. Ipilimumab, 3 mg/kg, iv Q 3 wks x 4 < 1 prior Rx
32 KEYNOTE-006 Pembrolizumab vs. Ipilimumab The study was closed early due to achievement of PFS and OS endpoints. Results to be presented at AACR Annual Meeting 2015 (April 18-22, 2015).
33 BMS Anti-PDL-1 in Metastatic Melanoma Phase I, > 2nd Line 55 Melanoma pts subset mg/kg, iv, Q2wks, up to 96 weeks. ORR (all doses): 17% Additional 27% SD > 24 weeks. Brahmer JR, NEJM, 2012.
34 BMS Anti-PDL-1 in Metastatic Melanoma Brahmer JR et al. NEJM, 2012
35 MPDL-3280A Anti-PDL-1 in Metastatic Melanoma Phase 1, no prior checkpoint-inhibitor 45 Melanoma pts subset mg/kg, Q3wks, iv. ORR, 26% for cohorts > 1 mg/kg. Responses observed in tumors and TIL expressing high levels PDL-1. Herbst RS et al. Nature, 2014

36 MPDL-3280A Anti-PDL-1 in Metastatic Melanoma
37 Predictive Biomarkers Ipilimumab activity Increased abs. lymphocyte count. Expression of inducible T-cell costimulator (ICOS). Tumor microenvironment inflammatory genes. Circulating immunosuppressive myeloid-derived suppressor cells. Maintenance of high clonotypes of TCRb chains.
38 Predictive Biomarkers PD-1/PDL-1 blockade activity Tumor PDL-1 expression: mixed results. Intrapatient tumor heterogeneity of IHC staining. Tumor vs. immune cell expression. High baseline CD8 cell densities at tumor margin.
39 LUNG CANCER
40 Nivolumab Phase II Trial in Metastatic Squamous Lung Cancer CHECKMATE patients with metastatic squamous NSCLC. Failed prior Pt-based regimen and > 1 additional regimen. Nivolumab, 3 mg/kg, i.v., Q2wks. Primary endpoint: Objective response rate. Rizvi NA, Lancet Oncol, March 2015
41 Nivolumab Phase II Trial in Metastatic Squamous Lung Cancer CHECKMATE- 063 ORR: 14.5% (17/117; 95% CI: %). CR/PR/SD: 40.5% 13/17 responses ongoing. Med Time to Resp: 3.3 mos Med Duration of Resp: not reached. 2 deaths: Pneumonia, Ischemic stroke. Rizvi NA, Lancet Oncol, March 2015
42 Nivolumab vs. Docetaxel in Advanced Squamous Lung Cancer: CHECKMATE patients 1 Pt doublet Nivolumab, 3 mg/kg, i.v Q2wks Docetaxel, 75 mg/m 2, i.v. Q3wks
43 Nivolumab vs. Docetaxel in Advanced Squamous Lung Cancer: CHECKMATE-017 Category Nivolumab (n=135) Docetaxel (n=137) Med OS (95% CI) 9.2 mos ( ) 6.0 mos ( ) P= HR 0.59 ( )
44 RENAL CELL CARCINOMA
45 Randomized Phase II Trial of Nivolumab in Renal Cell Carcinoma Blinded, randomized, multicenter trial. mrcc with clear cell component. Measurable disease At least 1 prior treatment with anti-angiogenic Rx No CNS metastases, autoimmune disease, prior immune checkpoint Rx, or >3 prior Rxs. 1 o endpoint: dose-related PFS Motzer RJ et al., JCO, Dec 2014.
46 Randomized Phase II Trial of Nivolumab in Renal Cell Carcinoma Nivolumab, 0.3 mg/kg, i.v., Q3weeks 168 pts Nivolumab, 2 mg/kg, i.v., Q3weeks Nivolumab, 10 mg/kg, i.v., Q3weeks
47 Randomized Phase II Trial of Nivolumab in Renal Cell Carcinoma Category 0.3 mg/kg 2 mg/kg 10 mg/kg mpfs (80% CI) 2.7 mos ( ) 4.0 mos ( ) 4.2 mos ( ) ORR 12 (20%) 12 (22%) 11 (20%) mos (80% CI) 18.2 mos (16-24) 25.5 mos (20-29) 24.7 mos (15-26)
48 (A) Progression-free and (B) overall survival by treatment arm (randomly assigned patients). Robert J. Motzer et al. JCO doi: /jco by American Society of Clinical Oncology
49 (A) Progression-free and (B) overall survival by treatment arm (randomly assigned patients). Robert J. Motzer et al. JCO doi: /jco by American Society of Clinical Oncology
50 Phase I nivolumab/ipilimumab in metastatic renal cell carcinoma Nivolumab, 3 mg/kg Ipilimumab, 1 mg/kg i.v. Q3wks x 4 44 mrcc patients untreated or prior Rx Nivolumab, 3 mg/kg Ipilimumab, 1 mg/kg i.v. Q3wks x 4 Both arms continue nivolumab Q2wks Hammers HJ, 2014 ASCO Annual Meeting Abstracts.
51 Phase I nivolumab/ipilimumab in metastatic renal cell carcinoma Category Arm N3 + I1 n=21 Arm N1 + I3 n=23 ORR, n (%) 6 (29) 9 (39) SD, n (%) [duration, wks] 7 (33) [6+ to 25+] 9 (39) [6+to 26.1] DOR, range (wks) PFS, range (wks)
52 LYMPHOMA
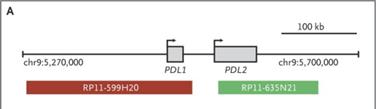
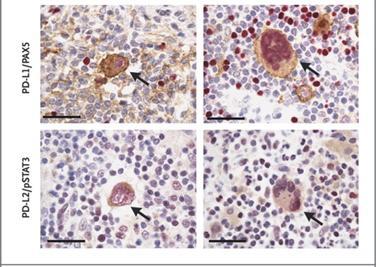
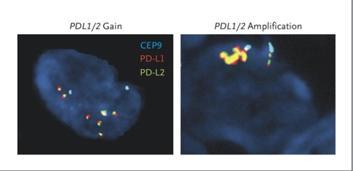
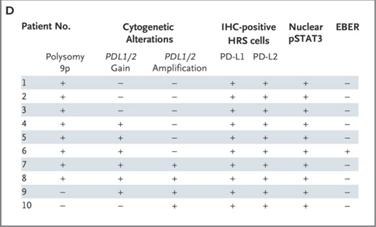
53 Immune Checkpoint Inhibition in Hodgkins Lymphoma chl has a small number of Reed Sternberg (RS) cells on background of extensive but ineffective inflammatory/immune response cells RS cells often have 9p24.1 structural mutations increased gene dosage of PD-1 ligands In EBV+ chl, viral infection also increases expression of PD-1 ligands
54
55
56
57 PD-1 Blockade with Nivolumab in R/R HL Armand et al, abstract #289, ASH 2014; Ansell et al, NEJM Dec Phase I multicenter study R/R HL, prior Rx with brentuximab 78% s/p prior ASCT Dose: 3 mg/kg q2wk until CR, PD or toxicity Response: 20/23 (87%), CR in 17%, 3 SD 6 pts SCT PFS at 24 weeks = 86% 2 pts d/c Rx: MDS, pancreatitis Toxicity: rash 20%, thrombocytopenia 17%

58 Response in Tumor Burden of HL Patients Receiving Nivolumab Ansell SM et al. N Engl J Med 2014.
59
60 Pembrolizumab in chl failing brentuximab C Moskowitz et al, abstract #290, ASH 2014 Phase Ib multicenter trial R/R chl, no prior autoimmune or interstitial lung disease Pembro 10 mg/kg IV q2wk Preliminary report of 15 pts evaluated at week 12
61 Pembrolizumab in chl Failing Brentuximab C Moskowitz et al, abstract #290, ASH 2014 Median 4 prior Rx s, 67% prior ASCT 1 pt d/c Rx due to toxicity (pneumonitis) Grade 1-2 resp events in 20%, thyroid disorders in 20% week 12 = 53%: 3 CR, 5 PR PD in 4 pts, toxicity or 2 years of therapy Conclusion: clinical benefit in pretreated chl
62 Nivolumab in lymphoid malignancies AM Lesokhin et al, abstract #291, ASH 2014 Phase I multicenter study, pre-planned interim analysis Heavily pretreated pts, including ASCT 3 mg/kg q2wks x 2 yrs, or PD/ toxicity Correlatives: anti-tumor activity and expression of immunomodulatory proteins
63 Nivolumab in lymphoid malignancies AM Lesokhin et al, abstract #291, ASH 2014 Tumor n CR PR SD % PFS 24 wks DLBCL FL MF MM PTCL/ other T Toxicity: pneumonitis 11%, 1 death Very few pts with 9p alteration or PD-L1 expression PD-L1 is expressed in FL microenvironment by stroma
64 The Immunotherapy Timeline Interferona2b 1995 BCG 1970 IL Ipilimumab 2011 Nivolumab 2015 Pembrolizumab 2014
65
66 Ipilimumab plus Nivolumab Phase I trial in advanced melanoma. 2-Part study: Concurrent study-no prior ipilimumab. Sequential study- > 3 prior doses of ipilimumab. Endpoints: Safety and efficacy. Wolchok JD, NEJM, 2013
67 Concurrent Ipilimumab and Nivolumab Cohort Nivolumab (mg/kg) Ipilimumab (mg/kg) a Nivolumab/Ipilimumab i.v every 3 weeks x 4, then nivolumab alone, i.v., every 3 weeks up to 4 doses. Wolchok JD, NEJM, 2013
68 Concurrent Ipilimumab and Nivolumab Safety 53 patients treated. Cohort 3 (Niv 3/Ipi 3) exceeded acceptable toxicity. Cohort 2 (Niv 1/Ipi 3) = MTD. Serious/life-threatening toxicity in 49% of all patients. Hepatotoxicity 15% Diarrhea/colitis 9% Acute renal insufficiency 6% Wolchok JD, NEJM, 2013

 % > 80")
 Responses ongoing")

69 Concurrent Ipilimumab and Nivolumab Niv/Ipi Dose (mg/kg) % Response Rate (#) % > 80 Reduction at 12 weeks (#) Responses ongoing in 19 of 21 patients at weeks. Wolchok JD, NEJM, 2013
70 Wolchok JD et al, NEJM, 2013
71 Sequential Nivolumab and Ipilimumab 33 patients, metastatic melanoma, > 3 prior doses ipilimumab. Cohorts 6 & 7 treated with nivolumab i.v. every 2 weeks up to 48 doses. Cohort Dose (mg/kg) Hodi FS et al. ASCO Annual Meeting Abstract 2013
72 Sequential Ipilimumab and Nivolumab Safety 33 patients treated. Serious/life-threatening toxicity in 18% of all patients. Lipase elevation 6% Endocrine events 6% Three patients discontinued treatment due to toxicity. Hodi FS et al. ASCO Annual Meeting Abstract 2013

73 Sequential Nivolumab and Ipilimumab Nivolumab dose (mg/kg) % Response Rate (#) % > 80 Reduction at 8 weeks (#) Some patients who did not respond to prior ipilimumab did respond to nivolumab. Hodi FS et al. ASCO Annual Meeting Abstract 2013
Out of 129 patients with NSCLC treated with Nivolumab in a phase I trial, the OS rate at 5-y was about 16 %, clearly higher than historical rates.
 6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
Role of the Pathologist in Guiding Immuno-oncological Therapies. Scott Rodig MD, PhD
 Role of the Pathologist in Guiding Immuno-oncological Therapies Scott Rodig MD, PhD Department of Pathology, Brigham & Women s Hospital Center for Immuno-Oncology, Dana-Farber Cancer Institute Associate
Role of the Pathologist in Guiding Immuno-oncological Therapies Scott Rodig MD, PhD Department of Pathology, Brigham & Women s Hospital Center for Immuno-Oncology, Dana-Farber Cancer Institute Associate
Checkpoint Regulators Cancer Immunotherapy takes centre stage. Dr Oliver Klein Department of Medical Oncology 02 May 2015
 Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
PTAC meeting held on 5 & 6 May (minutes for web publishing)
") PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
Immunotherapy, an exciting era!!
 Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania
 Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Immuno-Oncology Applications
 Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
Immuno-Oncology Applications Lee S. Schwartzberg, MD, FACP West Clinic, P.C.; The University of Tennessee Memphis, Tn. ICLIO 1 st Annual National Conference 10.2.15 Philadelphia, Pa. Financial Disclosures
Checkpoint regulators a new class of cancer immunotherapeutics. Dr Oliver Klein Medical Oncologist ONJCC Austin Health
 Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Immunotherapy on the Horizon
 Immunotherapy on the Horizon Andrew L. Coveler Assistant Professor of Medicine, Division of Oncology University of Washington Assistant Member Fred Hutchinson Cancer Research Center Image: NASA.gov 1 2
Immunotherapy on the Horizon Andrew L. Coveler Assistant Professor of Medicine, Division of Oncology University of Washington Assistant Member Fred Hutchinson Cancer Research Center Image: NASA.gov 1 2
Immunotherapy for Metastatic Malignant Melanoma. Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg
 Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
III Sessione I risultati clinici
 10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy
: Biomarkers for Immunotherapy") Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy Lee S. Schwartzberg, MD, FACP Chief, Division of Hematology Oncology; Professor of Medicine, The University of Tennessee; The West
Post-ASCO Immunotherapy Highlights (Part 2): Biomarkers for Immunotherapy Lee S. Schwartzberg, MD, FACP Chief, Division of Hematology Oncology; Professor of Medicine, The University of Tennessee; The West
Immunotherapy for NSCLC: Current State of the Art and Future Directions. H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States
 Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
A CME-certified Oncology Exchange Program
 A CME-certified Oncology Exchange Program Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Seattle Genetics, Inc. Re-treatment with BV Bartlett
A CME-certified Oncology Exchange Program Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Seattle Genetics, Inc. Re-treatment with BV Bartlett
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD
 La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
The Really Important Questions Current Immunotherapy Trials are Not Answering
 The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
Cancer Immunotherapy Patient Forum. for the Treatment of Melanoma, Leukemia, Lymphoma, Lung and Genitourinary Cancers - November 7, 2015
 Cancer Immunotherapy Patient Forum for the Treatment of Melanoma, Leukemia, Lymphoma, Lung and Genitourinary Cancers - November 7, 2015 Biomarkers and Patient Selection Julie R. Brahmer, M.D. Director
Cancer Immunotherapy Patient Forum for the Treatment of Melanoma, Leukemia, Lymphoma, Lung and Genitourinary Cancers - November 7, 2015 Biomarkers and Patient Selection Julie R. Brahmer, M.D. Director
II sessione. Immunoterapia oltre la prima linea. Alessandro Tuzi ASST Sette Laghi, Varese
 II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
Largos Supervivientes, Tenemos datos?
 Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Immune checkpoint inhibitors in lymphoma. Catherine Hildyard Haematology Senior Registrar Oxford University Hospitals NHS Foundation Trust
 Immune checkpoint inhibitors in lymphoma Catherine Hildyard Haematology Senior Registrar Oxford University Hospitals NHS Foundation Trust Aims How immune checkpoint inhibitors work Success of immune checkpoint
Immune checkpoint inhibitors in lymphoma Catherine Hildyard Haematology Senior Registrar Oxford University Hospitals NHS Foundation Trust Aims How immune checkpoint inhibitors work Success of immune checkpoint
The Current Status of Immune Checkpoint Inhibitors: Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb
 The Current Status of Immune Checkpoint Inhibitors: A Global Overview of the Field Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb Immune Checkpoint Inhibitors Conference, March
The Current Status of Immune Checkpoint Inhibitors: A Global Overview of the Field Arvin Yang, MD PhD Oncology Global Clinical Research Bristol-Myers Squibb Immune Checkpoint Inhibitors Conference, March
Immunotherapy Treatment Developments in Medical Oncology
 Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
6/7/16. Melanoma. Updates on immune checkpoint therapies. Molecularly targeted therapies. FDA approval for talimogene laherparepvec (T- VEC)
") Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro. Immune checkpoint inhibition in DLBCL
 Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro Immune checkpoint inhibition in DLBCL Immunotherapy: The Cure is Inside Us Our immune system prevents or limit infections
Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro Immune checkpoint inhibition in DLBCL Immunotherapy: The Cure is Inside Us Our immune system prevents or limit infections
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
ASCO 2014 Highlights*
 ASCO 214 Highlights* Investor Meeting June 2, 214 *American Society of Clinical Oncology, May 3 June 3, 214 Forward-Looking Information During this meeting, we will make statements about the Company s
ASCO 214 Highlights* Investor Meeting June 2, 214 *American Society of Clinical Oncology, May 3 June 3, 214 Forward-Looking Information During this meeting, we will make statements about the Company s
A Case Study: Ipilimumab in Pre-treated Metastatic Melanoma
 A Case Study: Ipilimumab in Pre-treated Metastatic Melanoma Tai-Tsang Chen, PhD Global Biometric Sciences, Bristol-Myers Squibb EFSPI Statistical Meeting on Evidence Synthesis Brussels, Belgium November
A Case Study: Ipilimumab in Pre-treated Metastatic Melanoma Tai-Tsang Chen, PhD Global Biometric Sciences, Bristol-Myers Squibb EFSPI Statistical Meeting on Evidence Synthesis Brussels, Belgium November
Kamakshi V Rao, PharmD, BCOP, FASHP University of North Carolina Medical Center UPDATE IN REFRACTORY HODGKIN LYMPHOMA
 Kamakshi V Rao, PharmD, BCOP, FASHP University of North Carolina Medical Center UPDATE IN REFRACTORY HODGKIN LYMPHOMA Objectives Describe the current standard approach for patients with relapsed/refractory
Kamakshi V Rao, PharmD, BCOP, FASHP University of North Carolina Medical Center UPDATE IN REFRACTORY HODGKIN LYMPHOMA Objectives Describe the current standard approach for patients with relapsed/refractory
Evan J. Lipson, M.D.
 Update on treatment for Merkel cell, cutaneous squamous cell and basal cell cancers Evan J. Lipson, M.D. The Johns Hopkins University School of Medicine Bloomberg~Kimmel Institute for Cancer Immunotherapy
Update on treatment for Merkel cell, cutaneous squamous cell and basal cell cancers Evan J. Lipson, M.D. The Johns Hopkins University School of Medicine Bloomberg~Kimmel Institute for Cancer Immunotherapy
Update on Immunotherapy in Advanced Melanoma. Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017
 Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico
 Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico Pier Francesco Ferrucci Direttore, Unità di Oncologia Medica del Melanoma Istituto Europeo di Oncologia - Milano Pisa,
Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico Pier Francesco Ferrucci Direttore, Unità di Oncologia Medica del Melanoma Istituto Europeo di Oncologia - Milano Pisa,
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Heme Onc Today New York Melanoma Meeting March 22-23, 2013 PD-1 antibodies
 Heme Onc Today New York Melanoma Meeting March 22-23, 2013 PD-1 antibodies Jeffrey Weber Moffitt Cancer Center Tampa, FL Disclosures I have consulted for BMS, Merck, Genentech and GSK for Ad Boards and
Heme Onc Today New York Melanoma Meeting March 22-23, 2013 PD-1 antibodies Jeffrey Weber Moffitt Cancer Center Tampa, FL Disclosures I have consulted for BMS, Merck, Genentech and GSK for Ad Boards and
New paradigms for treating metastatic melanoma
 New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic
 Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Priming the Immune System to Kill Cancer and Reverse Tolerance. Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics
 Priming the Immune System to Kill Cancer and Reverse Tolerance Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics Learning Objectives Describe the role of the immune system in cancer
Priming the Immune System to Kill Cancer and Reverse Tolerance Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics Learning Objectives Describe the role of the immune system in cancer
Predictive Biomarkers for Pembrolizumab. Eric H. Rubin, M.D.
 Predictive Biomarkers for Pembrolizumab Eric H. Rubin, M.D. PD-1 and PD-L1/L2 Pathway PD-1 is an immune checkpoint receptor Binding of PD-1 by its ligands PD-L1 or PD-L2 leads to downregulation of T-cell
Predictive Biomarkers for Pembrolizumab Eric H. Rubin, M.D. PD-1 and PD-L1/L2 Pathway PD-1 is an immune checkpoint receptor Binding of PD-1 by its ligands PD-L1 or PD-L2 leads to downregulation of T-cell
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy
 Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Linfoma de Hodgkin. Novos medicamentos. Otavio Baiocchi CRM-SP
 Linfoma de Hodgkin Novos medicamentos Otavio Baiocchi CRM-SP 96.074 Hodgkin Lymphoma Unique B-cell lymphoma HRS malignant cells Scattered malignant Hodgkin-Reed-Sternberg (RS) cells in a background of
Linfoma de Hodgkin Novos medicamentos Otavio Baiocchi CRM-SP 96.074 Hodgkin Lymphoma Unique B-cell lymphoma HRS malignant cells Scattered malignant Hodgkin-Reed-Sternberg (RS) cells in a background of
Developing Novel Immunotherapeutic Cancer Treatments for Clinical Use
 Developing Novel Immunotherapeutic Cancer Treatments for Clinical Use Oncology for Scientists March 8 th, 2016 Jason Muhitch, PhD Assistant Professor Department of Urology Email: jason.muhitch@roswellpark.org
Developing Novel Immunotherapeutic Cancer Treatments for Clinical Use Oncology for Scientists March 8 th, 2016 Jason Muhitch, PhD Assistant Professor Department of Urology Email: jason.muhitch@roswellpark.org
Releasing the Brakes on Tumor Immunity: Immune Checkpoint Blockade Strategies
 Releasing the Brakes on Tumor Immunity: Immune Checkpoint Blockade Strategies Jason Muhitch, PhD MIR 509 October 1 st, 2014 Email: jason.muhitch@roswellpark.org 0 Holy Grail of Tumor Immunity Exquisite
Releasing the Brakes on Tumor Immunity: Immune Checkpoint Blockade Strategies Jason Muhitch, PhD MIR 509 October 1 st, 2014 Email: jason.muhitch@roswellpark.org 0 Holy Grail of Tumor Immunity Exquisite
Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game?
 Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game? Sylvie NEGRIER MD, PhD Centre Léon Bérard, Lyon Université Lyon I IMMUNOTHERAPY: A LONG AND WIDING ROAD! WHERE
Immunotherapy versus targeted treatments in metastatic renal cell carcinoma: The return game? Sylvie NEGRIER MD, PhD Centre Léon Bérard, Lyon Université Lyon I IMMUNOTHERAPY: A LONG AND WIDING ROAD! WHERE
Approaches To Treating Advanced Melanoma
 Approaches To Treating Advanced Melanoma Suraj Venna, MD Medical Director, Melanoma and Cutaneous Oncology Inova Schar Cancer Institute Associate Professor, VCU Fairfax VA Disclosures No relevant disclosures
Approaches To Treating Advanced Melanoma Suraj Venna, MD Medical Director, Melanoma and Cutaneous Oncology Inova Schar Cancer Institute Associate Professor, VCU Fairfax VA Disclosures No relevant disclosures
ICLIO National Conference
 ICLIO National Conference Immuno-oncology In The Clinic Today Lee Schwartzberg, MD, FACP Executive Director, West Cancer Center Chief, Division of Hematology/Oncology University of Tennessee Health Science
ICLIO National Conference Immuno-oncology In The Clinic Today Lee Schwartzberg, MD, FACP Executive Director, West Cancer Center Chief, Division of Hematology/Oncology University of Tennessee Health Science
Incorporating Immunotherapy into the treatment of NSCLC
 Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Treatment and management of advanced melanoma: Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC
 Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management
 Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management Stacey Jassey Megan Brafford David Kwasny This CE activity was originally presented live at the 2015 NASP Annual Meeting
Newest Oncology Agents: PD 1 Inhibitors Clinical Information and Patient Management Stacey Jassey Megan Brafford David Kwasny This CE activity was originally presented live at the 2015 NASP Annual Meeting
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for the Treatment of Head and Neck Cancers. Barbara Burtness, MD Yale University
 Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment
 Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment Patrick Medina, Pharm.D., BCOP Professor The University of Oklahoma College of Medicine Stephenson Cancer Center Faculty Disclosure
Cancer Immunotherapy: Exploring the Role of Novel Agents in Cancer Treatment Patrick Medina, Pharm.D., BCOP Professor The University of Oklahoma College of Medicine Stephenson Cancer Center Faculty Disclosure
Immunotherapy in Lung Cancer
 Immunotherapy in Lung Cancer Jamie Poust Pharm. D., BCOP Oncology Pharmacist University of Colorado Hospital Objectives Describe the recent advances in immunotherapy for patients with lung cancer Outline
Immunotherapy in Lung Cancer Jamie Poust Pharm. D., BCOP Oncology Pharmacist University of Colorado Hospital Objectives Describe the recent advances in immunotherapy for patients with lung cancer Outline
Immunotherapy for the Treatment of Melanoma. Marlana Orloff, MD Thomas Jefferson University Hospital
 Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Brain mets under I.O.
 Brain mets under I.O. Bernard Escudier Gustave Roussy, Villejuif, France Disclosure Honorarium received from BMS, Novartis, Pfizer, Bayer, Roche, Exelixis, Ipsen, Eisai, Calithera Travel Grant from BMS,
Brain mets under I.O. Bernard Escudier Gustave Roussy, Villejuif, France Disclosure Honorarium received from BMS, Novartis, Pfizer, Bayer, Roche, Exelixis, Ipsen, Eisai, Calithera Travel Grant from BMS,
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
News from ASCO. Niven Mehra, Medical Oncologist. Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital
 News from ASCO Niven Mehra, Medical Oncologist Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital Disclosures Speaker fees: Merck, Bayer Advisory boards: Janssen-Cilag Research and
News from ASCO Niven Mehra, Medical Oncologist Radboud UMC Institute of Cancer Research and The Royal Marsden Hospital Disclosures Speaker fees: Merck, Bayer Advisory boards: Janssen-Cilag Research and
Patient Selection: The Search for Immunotherapy Biomarkers
 Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER
 Gynecologic Cancer InterGroup Cervix Cancer Research Network IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Cervix
Gynecologic Cancer InterGroup Cervix Cancer Research Network IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Cervix
Toxicity from Checkpoint Inhibitors. James Larkin FRCP PhD
 Toxicity from Checkpoint Inhibitors James Larkin FRCP PhD Disclosures Research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): BMS, Eisai, GSK, MSD, Novartis, Pfizer, Roche/Genentech
Toxicity from Checkpoint Inhibitors James Larkin FRCP PhD Disclosures Research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): BMS, Eisai, GSK, MSD, Novartis, Pfizer, Roche/Genentech
New Frontiers in Metastatic Melanoma: A Closer Look at the Role of Immunotherapy
 New Frontiers in Metastatic Melanoma: A Closer Look at the Role of Immunotherapy Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology
New Frontiers in Metastatic Melanoma: A Closer Look at the Role of Immunotherapy Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology
 Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
Immunotherapy for Melanoma. Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France
 Immunotherapy for Melanoma Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France Overall Survival for Metastatic Melanoma Proportion Alive 1.0 0.8 0.6 0.4 0.2 Survival data
Immunotherapy for Melanoma Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France Overall Survival for Metastatic Melanoma Proportion Alive 1.0 0.8 0.6 0.4 0.2 Survival data
Highlights from AACR 2015: The Emerging Potential of Immunotherapeutic Approaches in Non-Small Cell Lung Cancer
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Immunoterapia e farmaci innovativi
 Immunoterapia e farmaci innovativi Emilio Bria Oncologia Medica, Dipart. di Medicina, Università di Verona, Az. Osp. Univ. Int., Verona emilio.bria@univr.it Padova, 29 Ottobre 2015 Disclosures Advisory
Immunoterapia e farmaci innovativi Emilio Bria Oncologia Medica, Dipart. di Medicina, Università di Verona, Az. Osp. Univ. Int., Verona emilio.bria@univr.it Padova, 29 Ottobre 2015 Disclosures Advisory
Society for Immunotherapy of Cancer (SITC) Immunotherapy for the Treatment of Brain Metastases
 Immunotherapy for the Treatment of Brain Metastases") Society for Immunotherapy of Cancer (SITC) Immunotherapy for the Treatment of Brain Metastases Geoffrey T. Gibney, MD Georgetown-Lombardi Comprehensive Cancer Center Medstar-Georgetown University Hospital
Society for Immunotherapy of Cancer (SITC) Immunotherapy for the Treatment of Brain Metastases Geoffrey T. Gibney, MD Georgetown-Lombardi Comprehensive Cancer Center Medstar-Georgetown University Hospital
Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration trials and future considerations
 Gong et al. Journal for ImmunoTherapy of Cancer (2018) 6:8 DOI 10.1186/s40425-018-0316-z REVIEW Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration
Gong et al. Journal for ImmunoTherapy of Cancer (2018) 6:8 DOI 10.1186/s40425-018-0316-z REVIEW Development of PD-1 and PD-L1 inhibitors as a form of cancer immunotherapy: a comprehensive review of registration
Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma
 Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma Dr. J.L.Manzano S. Oncología Médica H. Germans Trias i Pujol, ICO-Badalona PRBB Auditorium,
Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma Dr. J.L.Manzano S. Oncología Médica H. Germans Trias i Pujol, ICO-Badalona PRBB Auditorium,
Melanoma: Therapeutic Progress and the Improvements Continue
 Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
What we learned from immunotherapy in the past years
 What we learned from immunotherapy in the past years Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure
What we learned from immunotherapy in the past years Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure
CheckMate 012: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer
 CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
Immunotherapies for Advanced NSCLC: Current State of the Field. H. Jack West Swedish Cancer Institute Seattle, Washington
 Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
New Systemic Therapies in Advanced Melanoma
 New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
Immunotherapy for Genitourinary Cancers
 Immunotherapy for Genitourinary Cancers Susan F. Slovin, MD, PhD Genitourinary Oncology Service Sidney Kimmel Center for Prostate and Urologic Cancers Memorial Sloan Kettering Cancer Center New York, New
Immunotherapy for Genitourinary Cancers Susan F. Slovin, MD, PhD Genitourinary Oncology Service Sidney Kimmel Center for Prostate and Urologic Cancers Memorial Sloan Kettering Cancer Center New York, New
Updates in Immunotherapy for Urothelial Carcinoma
 Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Improving Immunotherapy for Melanoma
 Improving Immunotherapy for Melanoma David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/ Harvard Cancer Center Harvard Medical School Immunotherapy Improvement Model All patients All
Improving Immunotherapy for Melanoma David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/ Harvard Cancer Center Harvard Medical School Immunotherapy Improvement Model All patients All
Current experience in immunotherapy for metastatic renal cell carcinoma
 Current experience in immunotherapy for metastatic renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute FOIU, Tel Aviv, 3 July 2018 Financial and Other Disclosures Off-label use of drugs,
Current experience in immunotherapy for metastatic renal cell carcinoma Axel Bex, MD, PhD The Netherlands Cancer Institute FOIU, Tel Aviv, 3 July 2018 Financial and Other Disclosures Off-label use of drugs,
Immunotherapy in Non-Small Cell Lung Cancer
 Immunotherapy in Non-Small Cell Lung Cancer Renato G. Martins Stephen H. Petersdorf Endowed Chair in Cancer Care Associate Medical Director, Solid Tumor Adult Oncology, Seattle Cancer Care Alliance Professor,
Immunotherapy in Non-Small Cell Lung Cancer Renato G. Martins Stephen H. Petersdorf Endowed Chair in Cancer Care Associate Medical Director, Solid Tumor Adult Oncology, Seattle Cancer Care Alliance Professor,
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD
 Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy. Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016
 Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016 Overcoming toxicity A new context for evaluating toxicity
Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016 Overcoming toxicity A new context for evaluating toxicity
Immunotherapy for the Treatment of Cancer
 Immunotherapy for the Treatment of Cancer Jason Muhitch, PhD Assistant Professor Department of Urology Department of Immunology Roswell Park Comprehensive Cancer Center Oncology for Scientists March 15,
Immunotherapy for the Treatment of Cancer Jason Muhitch, PhD Assistant Professor Department of Urology Department of Immunology Roswell Park Comprehensive Cancer Center Oncology for Scientists March 15,
Clinical: Ipilimumab (MDX-010) Update and Next Steps
 Update and Next Steps") Clinical: Ipilimumab (MDX-010) Update and Next Steps Geoffrey M. Nichol, M.D., M.B.A. Senior Vice President, Product Development Medarex, Inc. R&D Day December 9, 2005 Ipilimumab: New Class of Cancer Therapy
Clinical: Ipilimumab (MDX-010) Update and Next Steps Geoffrey M. Nichol, M.D., M.B.A. Senior Vice President, Product Development Medarex, Inc. R&D Day December 9, 2005 Ipilimumab: New Class of Cancer Therapy
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer
 Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Immunotherapy for Melanoma. Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center
 Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
New Era of Cancer Therapy Immuno-Oncology: PD1/PD-L1 inhibitors
 New Era of Cancer Therapy Immuno-Oncology: PD1/PD-L1 inhibitors Farah Brasfield, MD Chair, Regional Chiefs of Oncology Kaiser Permanente Jennifer Chang, PharmD, MPH Supervisor, Drug Information Services
New Era of Cancer Therapy Immuno-Oncology: PD1/PD-L1 inhibitors Farah Brasfield, MD Chair, Regional Chiefs of Oncology Kaiser Permanente Jennifer Chang, PharmD, MPH Supervisor, Drug Information Services
Immunotherapies in melanoma: regulatory perspective. Jorge Camarero (AEMPS)
") Immunotherapies in melanoma: regulatory perspective Jorge Camarero (AEMPS) Challenges for the approval of anti-cancer immunotherapeutic drugs EMA-CDDF joint meeting, London 4-5 February 2016 disclaimers
Immunotherapies in melanoma: regulatory perspective Jorge Camarero (AEMPS) Challenges for the approval of anti-cancer immunotherapeutic drugs EMA-CDDF joint meeting, London 4-5 February 2016 disclaimers
Medical Treatment of Advanced Lung Cancer
 Medical Treatment of Advanced Lung Cancer Oncology for Scientists April 26, 2018 Edwin Yau, MD., Ph.D. Assistant Professor of Oncology Department of Medicine Department of Cancer Genetics and Genomics
Medical Treatment of Advanced Lung Cancer Oncology for Scientists April 26, 2018 Edwin Yau, MD., Ph.D. Assistant Professor of Oncology Department of Medicine Department of Cancer Genetics and Genomics
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS
 IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
Índice. Melanoma Cáncer de Pulmón Otros tumores
 Índice Melanoma Cáncer de Pulmón Otros tumores Carcinoma de Vejiga Carcinoma de Células Renales Carcinoma de Cabeza y Cuello Carcinomas del tubo digestivo Cáncer de Mama MELANOMA CIRUGÍA CIRUGÍA + INFa
Índice Melanoma Cáncer de Pulmón Otros tumores Carcinoma de Vejiga Carcinoma de Células Renales Carcinoma de Cabeza y Cuello Carcinomas del tubo digestivo Cáncer de Mama MELANOMA CIRUGÍA CIRUGÍA + INFa
Review of immunotherapy in melanoma
 Review of immunotherapy in melanoma Surein Arulananda, 1,2,3 Elizabeth Blackley, 1 Jonathan Cebon 1,2,3 1. Department of Medical Oncology, Austin Health, Heidelberg, Victoria, Australia. 2. Cancer Immunobiology
Review of immunotherapy in melanoma Surein Arulananda, 1,2,3 Elizabeth Blackley, 1 Jonathan Cebon 1,2,3 1. Department of Medical Oncology, Austin Health, Heidelberg, Victoria, Australia. 2. Cancer Immunobiology
Checkpoint Blockade in Hematology and Stem Cell Transplantation
 Checkpoint Blockade in Hematology and Stem Cell Transplantation Saad S. Kenderian, MD Assistant Professor of Medicine and Oncology Mayo Clinic College of Medicine October 14, 2016 2015 MFMER slide-1 Disclosures
Checkpoint Blockade in Hematology and Stem Cell Transplantation Saad S. Kenderian, MD Assistant Professor of Medicine and Oncology Mayo Clinic College of Medicine October 14, 2016 2015 MFMER slide-1 Disclosures
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento
 tra la prima e la seconda linea di trattamento") Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
We re Reaching Ludicrous Speed: New Immunotherapy Oncology Medications
 We re Reaching Ludicrous Speed: New Immunotherapy Oncology Medications Adam Peele, PharmD, BCPS, BCOP Oncology Pharmacy Manager Cone Health Disclosures Merck Pharmaceuticals Speaker s Bureau 1 Objectives
We re Reaching Ludicrous Speed: New Immunotherapy Oncology Medications Adam Peele, PharmD, BCPS, BCOP Oncology Pharmacy Manager Cone Health Disclosures Merck Pharmaceuticals Speaker s Bureau 1 Objectives
Practice changing studies in lung cancer 2017
 1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
The PD-1 pathway of T cell exhaustion
 The PD-1 pathway of T cell exhaustion SAMO 18.3.2016 Overview T cell exhaustion Biology of PD-1 Mechanism Ligands expressed on tumor cell and on non-tumor cells other receptor pairs Biomarkers for apd-1/pd-l1
The PD-1 pathway of T cell exhaustion SAMO 18.3.2016 Overview T cell exhaustion Biology of PD-1 Mechanism Ligands expressed on tumor cell and on non-tumor cells other receptor pairs Biomarkers for apd-1/pd-l1
Best Practices in the Treatment and Management of Metastatic Melanoma. Melanoma
 Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant
Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant
Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016
 Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016
Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016
Immunotherapy in Patients with Non-Small Cell Lung Cancer
 LIVE WEBINARS Immunotherapy in Patients with Non-Small Cell Lung Cancer Presented by: Leora Horn, MD, MSc Vanderbilt-Ingram Cancer Center July 14, 216 Moderated by Rose K. Joyce NCCN, Conferences and Meetings
LIVE WEBINARS Immunotherapy in Patients with Non-Small Cell Lung Cancer Presented by: Leora Horn, MD, MSc Vanderbilt-Ingram Cancer Center July 14, 216 Moderated by Rose K. Joyce NCCN, Conferences and Meetings
WHY LOOK FOR ADDITIONAL DATA TO ENRICH THE KAPLAN-MEIER CURVES? Immuno-oncology, only an example
 WHY LOOK FOR ADDITIONAL DATA TO ENRICH THE KAPLAN-MEIER CURVES? Immuno-oncology, only an example YIDOU ZHANG Health Economics and Payer Analytics Director Oncology Payer Evidence and Pricing, AstraZeneca
WHY LOOK FOR ADDITIONAL DATA TO ENRICH THE KAPLAN-MEIER CURVES? Immuno-oncology, only an example YIDOU ZHANG Health Economics and Payer Analytics Director Oncology Payer Evidence and Pricing, AstraZeneca