Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico
|
|
|
- Domenic Stewart
- 5 years ago
- Views:
Transcription
1 Terapia Immunomodulante e Target Therapies nel Trattamento del Melanoma Metastatico Pier Francesco Ferrucci Direttore, Unità di Oncologia Medica del Melanoma Istituto Europeo di Oncologia - Milano Pisa, 13/11/2015
2 Agenda 1. IMMUNOTERAPIA: Anti-CTLA4 Anti-PD1 Combinazioni anti-ctla4 e anti-pd1 2. TERAPIA TARGET: Anti-BRAF Anti-MEK Combinazioni anti-braf e antimek

3 The T-Cell Antitumor Response 1 Tumor antigens released by tumor cells 2 Tumor antigens presented to T cells 3 T cells are activated; they proliferate and differentiate into effector and memory cells 4 Effector T cells recognize tumor antigens 5 T cells kill tumor cells
 Activated T- Tumor Cell 2 Secretion of immunosuppressive factors (eg, TGF-B) 3 cell T-reg 4 Recruitment of immunosuppressive cell types (eg,")
4 Tumors Use Complex, Overlapping Mechanisms to Evade and Suppress the Immune System APC 1 Inhibition of tumor antigen presentation (eg, down regulation of MHC I) Inhibition of attack by immune cells (eg, disruption of T-cell checkpoint pathways) Activated T- Tumor Cell 2 Secretion of immunosuppressive factors (eg, TGF-B) 3 cell T-reg 4 Recruitment of immunosuppressive cell types (eg, Tregs)

5 Regulation of T-Cell Activation: Balancing Activating and Inhibitory Signals Immune checkpoints limit, or check, an ongoing immune response Prevents damage to the body s healthy tissues Negative co-stimulation, also called co-inhibition, helps shut down immune responses PD-1, CTLA-4, and LAG-3 are examples of co-inhibitory checkpoint molecules Amplitude and quality of a T- cell response is regulated by a balance of activating and inhibitory signals APC/ Tumor B7-2 (CD86) PD-L1 PD-L2 MHC CD40 CD137L PD-1 B7-1 (CD80) LAG-3 CD40L CD137 T cell CD28 Activation B7-1 (CD80) CTLA-4 Inhibition TCR Inhibition Inhibition Inhibition Activation Activation CTLA-4 = cytotoxic T-lymphocyte antigen-4; LAG-3 = lymphocyte activation gene-3; PD-1 = programmed death-1; PD-L1 = programmed death-ligand 1. OX40L OX40 Activation
6 Rationale for Blockade of Immune Checkpoint Molecules CTLA-4 and PD1
7 CTLA-4 and PD-1/L1 Checkpoint Blockade Priming phase (lymph node) Effector phase (peripheral tissue) Dendritic cell T cell T-cell migration T cell Cancer cell MHC TCR TCR MHC Dendritic cell B7 CD28 CTLA-4 T cell T cell PD-1 PD-L1 Cancer cell Ribas A. N Engl J Med. 2012;366:
8 Ipilimumab: Mechanism of Action CTLA-4 T cell activation T cell inhibition T cell potentiation T cell T cell T cell APC TCR MHC CD28 B7 APC TCR MHC CD28 CTLA-4 B7 APC TCR MHC B7 CTLA-4 IPILIMUMAB blocks CTLA-4 Adapted from Weber. J Cancer Immunol Immunother 2009;58:823.
9 Study Design MDX010-20: Randomized, Double-blind, Phase III Pre-treated Metastatic Melanoma (N=676) R A N D O M I Z E Ipilimumab 3 mg/kg + gp100 Ipilimumab 3 mg/kg + placebo gp100 + placebo (N=403) (N=137) (N=136) Primary endpoint: overall survival Secondary objectives: BORR, duration of response, PFS Hodi S et al. NEJM 2010;363(8):711-23
10 Proportion of patients alive (%) Durability of Survival Benefit with Ipilimumab in Heavily Pretreated Patients: 100 lpilimumab alone 80 lpilimumab + gp100 gp100 alone Ipilimumab + gp Years mos, months 95% CI HR P value 1-year OS (%) 2-year OS (%) a 3-year OS (%) b < Ipilimumab gp a Patients randomised 2 years prior to study survival cut-off date (N = 474) b Patients randomised 3 years prior to study survival cut-off date (N = 259) Hodi FS, et al. N Engl J Med 2010;363: McDermott D, et al. Ann Oncol 2013;24:2694 8
11 Specific Patterns of Response Ipilimumab monotherapy resulted in four distinct response patterns, 2 captured with conventional RECIST/WHO criteria and 2 by new irrc: 1. shrinkage in baseline lesions, without new lesions; 2. durable stable disease (in some patients followed by a slow, steady decline in total tumor burden); 3. response after an increase in total tumor burden; 4. response in the presence of new lesions. All these patterns were associated with favorable survival.
12
13 Specific Patterns of Toxicities




14 SKIN: Immune-related dermatitis Back: confluent red rash Back: close up of papular lesions Right upper arm: vacuolar changes Anti-CD8 staining: extensive epidermal exocytosis Jaber SH, et al. Arch Dermatol 2006;142:

15 GASTROINTESTINAL: Immune-related Enterocolitis
 12/3/04 headache and fatigue after 5 doses (10.")

16 ENDOCRINE: Immune-related Endocrinopathies 6/30/04 baseline (4.5 mm) 12/3/04 headache and fatigue after 5 doses (10.8 mm) Ipilimumab-related pituitary swelling and dysfunction Resolution of symptoms with hormone replacement therapy, with slow return of some endocrine function Blansfield JA, et al. J Immunother 2005;28:

17 LIVER: Immune-related Hepatitis Monitor liver function tests (LFTs): increases in AST and ALT or total bilirubin should be evaluated to exclude other causes of hepatic injury and monitored until resolution Withold ipilimumab dosing in patients with moderate aspartate AST or ALT elevations of > 5 to 8 times ULN, or moderate total bilirubin elevation of > 3 to 5.1 Permanently discontinue ipilimumab for any of the following: Severe AST or ALT elevations of > 8 times ULN; Total bilirubin elevations of > 5 times ULN; Symptoms of hepatotoxicity. Systemic high-dose corticosteroids may be required
18 PD1 Pathway As a Key Checkpoint in Cancer
19 Effects of PD1 Signalling on T-cell Function Normal function: attenuate immune responses to avoid immune system attack of self Direct effects on activated CD4+/CD8+ T cells PD1: PD-L1/L2 = proliferation PD1: PD-L1 = IL-2 PD1: PD-L1 = CD8+ T-cell anergy Indirect effects via Treg cells PD1: PD-L1 = naïve CD4+ cell conversion Treg PD1: PD-L1 = Treg function (inhibition of CD8+ T-cell responses) Blank C, et al. Cancer Immunol Immunother. 2007;56: Carter LL, et al. Eur J Immunol 2002;32: Chikuma S, et al. J Immunol 2009;182:




20 Anti-PD1 Mechanism of Action Recognition of tumour by T cell through MHC/antigen interaction mediates IFNγ release and PD-L1/2 upregulation on tumour Priming and activation of T cells through MHC/antigen and CD28/B7 interactions with antigen-presenting cells IFNγR IFNγ MHC T cell receptor T-cell receptor MHC Tumour cell PD-L1 PD-L2 PD-1 Shp-2 PI3K NFκB Other T cell Shp-2 CD28 PD-1 B7 PD-L1 Dendritic cell PD-1 PD-1 PD-L2 PD1 Receptor Blocking Ab
21 Activity of Anti-PD-1/PD-L1 in Patients With Advanced Melanoma Agent Pts, n ORR (at Optimal Dose), % Grades 3/4 Tx-Related AEs, % 6-Mo PFS, % 12-Mo PFS, % Median PFS, Mos 1-Yr OS, % 2-Yr OS, % Nivolumab (anti-pd-1) [1-3] (41) Pembrolizumab (anti-pd-1) [4,5] (52) NA NA > BMS NA NA NA NA NA (anti-pd-l1) [6] MPDL3280A 44 29* NA NA NA NA (anti-pd-l1) [7] *Includes 4 patients with UM without a response. 1. Topalian SL, et al. J Clin Oncol. 2014;32: Sznol M, et al. ASCO Abstract Topalian SL, et al. N Engl J Med. 2012;366: Ribas A, et al. ASCO Abstract Hamid O, et al. N Engl J Med. 2013;369: Brahmer JR, et al. N Eng J Med : Hamid O, et al. ASCO Abstract 9010.





22 CTL Infiltrates in Regressing Metastatic Melanoma Lesion After MK-3475 Treatment Baseline: February 29, 2012 August 20, 2012 CD8+ IHC CD8+ IHC Ribas A, et al. ASCO Abstract 9009.
23 AEs in > 5% of Patients Adverse Event (N = 135) All Grades, n (%) Grades 3/4, n (%) Any 107 (79.3) 17 (12.6) Fatigue 41 (30.4) 2 (1.5) Rash 28 (20.7) 3 (2.2) Pruritus 28 (20.7) 1 (0.7) Diarrhea 27 (20.0) 1 (0.7) Myalgia 16 (11.9) 0 Headache 14 (10.4) 0 Increased AST 13 (9.6) 2 (1.5) Asthenia 13 (9.6) 0 Nausea 13 (9.6) 0 Vitiligo 12 (8.9) 0 Hypothyroidism 11 (8.1) 1 (0.7) Increased ALT 11 (8.1) 0 Cough 11 (8.1) 0 Pyrexia 10 (7.4) 0 Chills 9 (6.7) 0 Abdominal pain 7 (5.2) 1 (0.7)
24 Anti-PD1 in Advanced Melanoma: Expert Perspective Excellent toxicity profile (Grade 3/4 iraes: 13% Pembro, 22% Nivo) Response rates in Ipi-naive pts 41% (Nivo), 52% (Pembro) - Lower response rates in patients who progressed after Ipi, BRAF inhibitor, or LDH >ULN Response duration (even when stopped): 81% at 1y (Pembro), 64% beyond 24 wks (Nivo) Median DoR of 22.9 mos (Nivo) Survival outcomes: Extimated median OS is >24 mo (Pembro) 2-yr OS: 48%; 3-yr OS: 41% (Nivo)
25 Rationale for concurrent Blockade of Immune Checkpoint Molecules CTLA-4 and PD1
 Dendritic cell MHC B7 TCR CD28 + + + B7 CTLA-4 - - -")
 PD1 blockade (nivolumab) Ribas A.")
26 Blocking CTLA-4 and PD1 Perifery Tumour microenvironment Activation (cytokines, lysis, proliferation, migration to tumour) Dendritic cell MHC B7 TCR CD B7 CTLA anti-ctla T cell T cell TCR MHC PD1 PD-L1 anti-pd1 PD1 PD-L2 anti-pd1 Tumour cell CTLA-4 blockade (ipilimumab) PD1 blockade (nivolumab) Ribas A. N Engl J Med 2012;366(26):
27
28 CA : Study Design Study design: Randomized, double-blind, phase III study to compare NIVO alone or NIVO + IPI to IPI alone NIVO 3 mg/kg Q2W + IPI-matched placebo Unresectable or Metatastic Melanoma Previously untreated Tissue available for PD-L1 testing Randomize 1:1:1 Stratify by: PD-L1 status* BRAF status AJCC M stage NIVO 1 mg/kg + IPI 3 mg/kg Q3W for 4 doses then NIVO 3 mg/kg Q2W + NIVOmatched placebo Treat until progression** or unacceptable toxicity IPI 3 mg/kg Q3W for 4 doses + NIVO-matched placebo *Verfied PD-L1 assay using 5% cutoff, was used for the stratification of patients; validated PD-L1 assay was used for the results of the study. **Patients could have been treated beyond progression under protocol-defined circumstances. 28
29 Proportion alive and progression-free Co-primary Endpoint: PFS (Intent-to-Treat) NIVO (N=316) NIVO + IPI (N=314) IPI (N=315) Median PFS, months (95% CI) 6.9 ( ) 11.5 ( ) 2.9 ( ) 0.8 HR (95% CI) vs. IPI 0.57 ( )* 0.42 ( )* HR (95% CI) vs. NIVO ( )** *Stratified log-rank P< vs. IPI **Exploratory endpoint NIVO NIVO + IPI IPI 0.0 Number at Risk NIVO NIVO + IPI IPI Months
30 Response to Treatment NIVO (N=316) NIVO + IPI (N=314) IPI (N=315) 19.0 (14.9 ORR, % (95% CI) 43.7 ( ) 57.6 ( ) 23.8) Two-sided P value vs IPI < < Best overall response % Complete response Partial response Stable disease Progressive disease Unknown Duration of response (months) Median (95% CI) NR (11.7, NR) NR (13.1, NR) NR (6.9, NR) NR, not reached. 30
31 Proportion alive and progression-free Proportion alive and progression-free PFS by PD-L1 Status (5% Cutoff) 1.0 PD-L1-positive ( 5%)* PD-L1-negative (<5%)* mpfs HR mpfs HR 0.0 NIVO NIVO + IPI IPI NIVO NIVO + IPI IPI NIVO NIVO + IPI IPI Number at Risk NIVO 80 NIVO + IPI IPI Months Number at Risk Months NIVO NIVO + IPI IPI Similar results were obtained using a 1% cutoff. *Per validated PD-L1 assay. 31
32 ORR by PD-L1 Status (5% Cutoff) NIVO + IPI resulted in a higher ORR vs. NIVO alone regardless of PD-L1 status NIVO NIVO + IPI IPI PD-L1- positive ORR, % (95% CI) 57.5 (45.9, 68.5) 72.1 (59.9, 82.3) 21.3 (12.7, 32.3) PD-L1- negative ORR, % (95% CI) 41.3 (34.6, 48.4) 54.8 (47.8, 61.6) 17.8 (12.8, 23.8) PD-L1 positivity defined as 5% tumor cell surface staining. Pre-treatment tumor specimens were centrally assessed by PD-L1 immunohistochemistry (using a validated BMS/Dako assay). 32

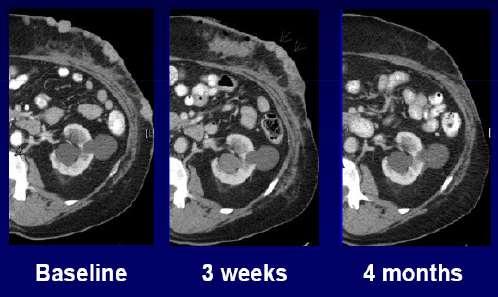
33 Rapid and durable changes in target lesions





34 Tempo mese + 2 mesi + 5 mesi + 8 mesi + 12 mesi
35 Safety Summary Patients Reporting Event, % Treatment-related adverse event (AE) Treatment-related AE leading to discontinuation NIVO (N=313) NIVO + IPI (N=313) IPI (N=311) Any Grade Grade 3 4 Any Grade Grade 3 4 Any Grade Grade Diarrhea Colitis Treatment-related death* *One reported in the NIVO group (neutropenia) and one in the IPI group (cardiac arrest) 35
36 Concurrent Therapy With Ipilimumab and Nivolumab: Expert Perspective Up to 70% ORR with 17% CRs and 82% in remission for all patients receiving concurrent treatment Up to 50% rate of grade 3/4 iraes at optimal doses: LFTs, lipase, amylase, rash, colitis BRAF status, PD-L1 tumor staining not clearly associated with response (maybe to Nivo) Response in sequential patients associated with plasma ipilimumab levels prior to starting nivolumab Concurrent 2-yr OS of 79% = impressive!!! Benefit worth the toxicity?
37 Molecularly Targeted Therapy

38 New Targets New Drugs
39
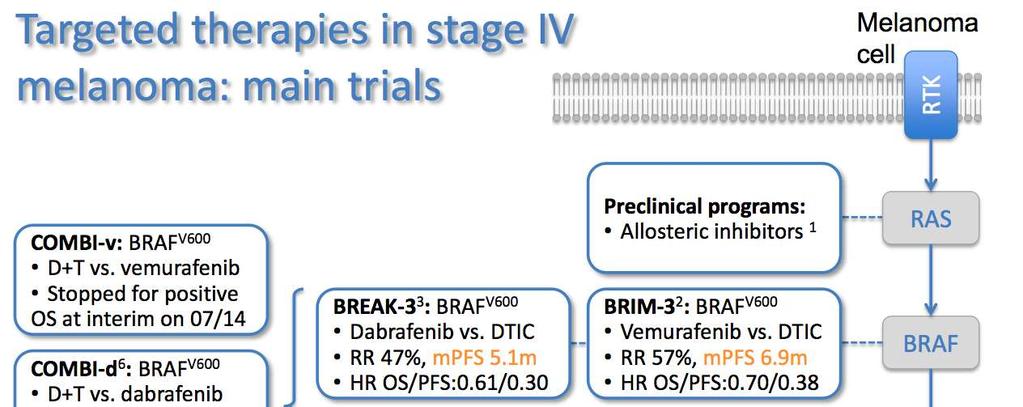
40 Rationale for Combination of BRAFi + MEKi in BRAF Mutant Tumors

41 Rationale for Combination of BRAFi + MEKi in BRAF Mutant Tumors RAS BRAF MEK perk Proliferation Survival Invasion Metastasis BRAFi : RR 77% MEKi RR 35% Goals of Combination: Improve complete response rate Decrease incidence of BRAFi-induced proliferative skin lesions Suppress MAP kinase dependent resistance mechanisms and improve duration of response
42


43 COMBI-v n=495 Co-BRIM


44 COMBI-v Co-BRIM 11.3 months HR=0.60
45 COMBI-v Co-BRIM
46
47
48 COMBI-v Co-BRIM

49
50 What may the Future Hold? Evaluation earlier in disease Optimization Biomarkers Schedule/regimen Outcomes assessment Evaluation across cancer types Immune checkpoints inhibitors Evaluation in combination Chemotherapy Radiotherapy Targeted agents Other I-O therapies Novel targets
51 What may the Future Hold? Evaluation earlier in disease Optimization Biomarkers Schedule/regimen Outcomes assessment Evaluation across cancer types Immune checkpoints inhibitors Evaluation in combination Chemotherapy Radiotherapy Targeted agents Other I-O therapies Novel targets
52

53 Della serie. Grazie per l attenzione
6/7/16. Melanoma. Updates on immune checkpoint therapies. Molecularly targeted therapies. FDA approval for talimogene laherparepvec (T- VEC)
") Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
Melanoma John A Thompson MD July 17, 2016 Featuring: Updates on immune checkpoint therapies Molecularly targeted therapies FDA approval for talimogene laherparepvec (T- VEC) 1 Mechanism of ac-on of Ipilimumab
New Systemic Therapies in Advanced Melanoma
 New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
New Systemic Therapies in Advanced Melanoma Sanjay Rao, MD FRCPC Medical Oncologist (BCCA-CSI) Clinical Assistant Professor, UBC Faculty of Medicine SON Fall Update October 22, 2016 Disclosures Equity
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania
 Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy. What every patient needs to know. James Larkin
 Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
III Sessione I risultati clinici
 10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
Immunotherapy Treatment Developments in Medical Oncology
 Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Immunotherapy Treatment Developments in Medical Oncology A/Prof Phillip Parente Director Cancer Services Eastern Health Executive MOGA ATC Medical Oncology RACP www.racpcongress.com.au Summary of The Desired
Update on Immunotherapy in Advanced Melanoma. Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017
 Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
New Therapeutic Approaches to Malignant Melanoma
 2018 Master Class for Oncologists New Therapeutic Approaches to Malignant Melanoma F. Stephen Hodi, M.D. Dana-Farber Cancer Institute, Boston, MA Disclosure I have nothing to disclose. Off Label/Investigational
2018 Master Class for Oncologists New Therapeutic Approaches to Malignant Melanoma F. Stephen Hodi, M.D. Dana-Farber Cancer Institute, Boston, MA Disclosure I have nothing to disclose. Off Label/Investigational
Immunotherapy for Metastatic Malignant Melanoma. Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg
 Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Immunotherapy for Metastatic Malignant Melanoma Dr Daniel A Vorobiof Sandton Oncology Centre Johannesburg Survival in Melanoma by Stage Proportion Surviving 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 Stage
Principles and Application of Immunotherapy for Cancer: Advanced Melanoma
 In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced Melanoma This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced Melanoma This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
ASCO 2014: The Future is Here. What I Will Talk About. George W. Sledge MD Stanford University School of Medicine
 ASCO 214: The Future is Here George W. Sledge MD Stanford University School of Medicine What I Will Talk About Two paths to a Cure Slicing the pie MelMng the snowflake The Past Isn t Dead Improving PaMent
ASCO 214: The Future is Here George W. Sledge MD Stanford University School of Medicine What I Will Talk About Two paths to a Cure Slicing the pie MelMng the snowflake The Past Isn t Dead Improving PaMent
Melanoma: Immune checkpoints
 ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
Melanoma. Il parere dell esperto. V. Ferraresi. Divisione di Oncologia Medica 1
 Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Immunoterapia e melanoma maligno metastatico: siamo partiti da li. Vanna Chiarion Sileni Istituto Oncologico Veneto
 Immunoterapia e melanoma maligno metastatico: siamo partiti da li Vanna Chiarion Sileni Istituto Oncologico Veneto Vanna.chiarion@iov.veneto.it Metastatic Melanoma Available Treatment: 197 217 Zelboraf
Immunoterapia e melanoma maligno metastatico: siamo partiti da li Vanna Chiarion Sileni Istituto Oncologico Veneto Vanna.chiarion@iov.veneto.it Metastatic Melanoma Available Treatment: 197 217 Zelboraf
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD
 Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Melanoma Clinical Trials and Real World Experience
 Melanoma Clinical Trials and Real World Experience Paul Lorigan University of Manchester Manchester, UK www.christie.nhs.uk/melanoma Melanoma Bridge, Naples 214 New Benchmarks for Phase II Trials OS at
Melanoma Clinical Trials and Real World Experience Paul Lorigan University of Manchester Manchester, UK www.christie.nhs.uk/melanoma Melanoma Bridge, Naples 214 New Benchmarks for Phase II Trials OS at
MELANOMA METASTASICO: NUEVAS COMBINACIONES. Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona
 MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
MELANOMA METASTASICO: NUEVAS COMBINACIONES Dr Ana Arance MD PhD Oncología Médica Hospital Clínic Barcelona Summary of OS accross clinical trials in patients with metastatic melanoma Ugurel et al. Eur J
The Immunotherapy of Oncology
 The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
The Immunotherapy of Oncology The 30-year Overnight Success Story M Avery, BIOtech Now 2014 Disclosures: Geoffrey R. Weiss, M.D. None The History A. Chekov: It has long been noted that the growth of malignant
Approaches To Treating Advanced Melanoma
 Approaches To Treating Advanced Melanoma Suraj Venna, MD Medical Director, Melanoma and Cutaneous Oncology Inova Schar Cancer Institute Associate Professor, VCU Fairfax VA Disclosures No relevant disclosures
Approaches To Treating Advanced Melanoma Suraj Venna, MD Medical Director, Melanoma and Cutaneous Oncology Inova Schar Cancer Institute Associate Professor, VCU Fairfax VA Disclosures No relevant disclosures
Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016
 Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016
Advances in Cancer Immunotherapy for Solid Tumors Expert Perspectives on The New Data Sunday, June 5, 2016 Supported by an independent educational grant from AstraZeneca Not an official event of the 2016
Immunotherapy for NSCLC: Current State of the Art and Future Directions. H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States
 Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for NSCLC: Current State of the Art and Future Directions H. Jack West, MD Swedish Cancer Institute Seattle, Washington, United States Which of the following statements regarding immunotherapy
Immunotherapy for Melanoma. Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center
 Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Immunotherapy for Melanoma Michael Postow, MD Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center Conflicts of Interest Bristol-Myers Squibb: -Research support -Participated
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
PTAC meeting held on 5 & 6 May (minutes for web publishing)
") PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
PTAC meeting held on 5 & 6 May 2016 (minutes for web publishing) PTAC minutes are published in accordance with the Terms of Reference for the Pharmacology and Therapeutics Advisory Committee (PTAC) and
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic
 Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Melanoma- Fighting the Dark Side
 Melanoma- Fighting the Dark Side Anna C. Pavlick, BSN, MSc, DO, MBA Professor of Medicine and Dermatology Director, NYU Melanoma Program Director, NYU Clinical Trials Office NYU Perlmutter Cancer Center
Melanoma- Fighting the Dark Side Anna C. Pavlick, BSN, MSc, DO, MBA Professor of Medicine and Dermatology Director, NYU Melanoma Program Director, NYU Clinical Trials Office NYU Perlmutter Cancer Center
Immune Checkpoints. PD Dr med. Alessandra Curioni-Fontecedro Department of Hematology and Oncology Cancer Center Zurich University Hospital Zurich
 Immune Checkpoints PD Dr med. Alessandra Curioni-Fontecedro Department of Hematology and Oncology Cancer Center Zurich University Hospital Zurich Activation of T cells requires co-stimulation Science 3
Immune Checkpoints PD Dr med. Alessandra Curioni-Fontecedro Department of Hematology and Oncology Cancer Center Zurich University Hospital Zurich Activation of T cells requires co-stimulation Science 3
Immunotherapy, an exciting era!!
 Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology
 Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
New paradigms for treating metastatic melanoma
 New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
Nivolumab in Hodgkin Lymphoma
 Nivolumab in Hodgkin Lymphoma Stephen M. Ansell, MD, PhD Professor of Medicine Chair, Lymphoma Group Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers Squibb Celldex Therapeutics Seattle
Nivolumab in Hodgkin Lymphoma Stephen M. Ansell, MD, PhD Professor of Medicine Chair, Lymphoma Group Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers Squibb Celldex Therapeutics Seattle
Immunotherapies in melanoma: regulatory perspective. Jorge Camarero (AEMPS)
") Immunotherapies in melanoma: regulatory perspective Jorge Camarero (AEMPS) Challenges for the approval of anti-cancer immunotherapeutic drugs EMA-CDDF joint meeting, London 4-5 February 2016 disclaimers
Immunotherapies in melanoma: regulatory perspective Jorge Camarero (AEMPS) Challenges for the approval of anti-cancer immunotherapeutic drugs EMA-CDDF joint meeting, London 4-5 February 2016 disclaimers
Priming the Immune System to Kill Cancer and Reverse Tolerance. Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics
 Priming the Immune System to Kill Cancer and Reverse Tolerance Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics Learning Objectives Describe the role of the immune system in cancer
Priming the Immune System to Kill Cancer and Reverse Tolerance Dr. Diwakar Davar Assistant Professor, Melanoma and Phase I Therapeutics Learning Objectives Describe the role of the immune system in cancer
ONCOS-102 in melanoma Dr. Alexander Shoushtari. 4. ONCOS-102 in mesothelioma 5. Summary & closing
 ONCOS-102 in melanoma Dr. Alexander Shoushtari 4. ONCOS-102 in mesothelioma 5. Summary & closing 1 Preliminary data from C824 Activating the Alexander Shoushtari, MD Assistant Attending Physician Melanoma
ONCOS-102 in melanoma Dr. Alexander Shoushtari 4. ONCOS-102 in mesothelioma 5. Summary & closing 1 Preliminary data from C824 Activating the Alexander Shoushtari, MD Assistant Attending Physician Melanoma
Review of immunotherapy in melanoma
 Review of immunotherapy in melanoma Surein Arulananda, 1,2,3 Elizabeth Blackley, 1 Jonathan Cebon 1,2,3 1. Department of Medical Oncology, Austin Health, Heidelberg, Victoria, Australia. 2. Cancer Immunobiology
Review of immunotherapy in melanoma Surein Arulananda, 1,2,3 Elizabeth Blackley, 1 Jonathan Cebon 1,2,3 1. Department of Medical Oncology, Austin Health, Heidelberg, Victoria, Australia. 2. Cancer Immunobiology
Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro. Immune checkpoint inhibition in DLBCL
 Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro Immune checkpoint inhibition in DLBCL Immunotherapy: The Cure is Inside Us Our immune system prevents or limit infections
Mariano Provencio Servicio de Oncología Médica Hospital Universitario Puerta de Hierro Immune checkpoint inhibition in DLBCL Immunotherapy: The Cure is Inside Us Our immune system prevents or limit infections
Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy. Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016
 Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016 Overcoming toxicity A new context for evaluating toxicity
Overcoming Toxicities Associated with Novel Checkpoint Inhibitor Immunotherapy Tara C. Gangadhar, MD Assistant Professor of Medicine ICI Boston 2016 Overcoming toxicity A new context for evaluating toxicity
What we learned from immunotherapy in the past years
 What we learned from immunotherapy in the past years Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure
What we learned from immunotherapy in the past years Paolo A. Ascierto, MD Unit Melanoma, Cancer Immunotherapy and Innovative Therapies Istituto Nazionale Tumori Fondazione G. Pascale, Napoli, Italy Disclosure
Medical Treatment for Melanoma Sanjiv S. Agarwala, MD
 Medical Treatment for Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Disclosures None Overview
Medical Treatment for Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Disclosures None Overview
Immunotherapy in lung cancer. Saurabh maji
 Immunotherapy in lung cancer Saurabh maji Worldwide, lung cancer is the most common cause of cancerrelated deaths Small cell lung cancer (SCLC) presents with widespread disease at the time of diagnosis,
Immunotherapy in lung cancer Saurabh maji Worldwide, lung cancer is the most common cause of cancerrelated deaths Small cell lung cancer (SCLC) presents with widespread disease at the time of diagnosis,
Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma
 Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma Dr. J.L.Manzano S. Oncología Médica H. Germans Trias i Pujol, ICO-Badalona PRBB Auditorium,
Optimizing Immunotherapy New Approaches, Biomarkers, Sequences and Combinations Immunotherapy in the clinic Melanoma Dr. J.L.Manzano S. Oncología Médica H. Germans Trias i Pujol, ICO-Badalona PRBB Auditorium,
Immunotherapy for Renal Cell Carcinoma. James Larkin
 Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Immunotherapy for Renal Cell Carcinoma James Larkin Disclosures Institutional research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): Eisai, BMS, MSD, GSK, Pfizer, Novartis, Roche/Genentech
Principles and Application of Immunotherapy for Cancer: Advanced NSCLC
 In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced NSCLC This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
In Partnership With Principles and Application of Immunotherapy for Cancer: Advanced NSCLC This program is supported by educational grants from Genentech and Merck. About These Slides Users are encouraged
Checkpoint-Inhibitoren beim Lungenkarzinom. Dr. Helge Bischoff Thoraxklinik Heidelberg
 Checkpoint-Inhibitoren beim Lungenkarzinom Dr. Helge Bischoff Thoraxklinik Heidelberg Survival (%) First-Line: Polychemotherapy vs 9387 patients 778 patients in studies with platinum chemotherapy 1-year
Checkpoint-Inhibitoren beim Lungenkarzinom Dr. Helge Bischoff Thoraxklinik Heidelberg Survival (%) First-Line: Polychemotherapy vs 9387 patients 778 patients in studies with platinum chemotherapy 1-year
Immunotherapy for Melanoma. Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France
 Immunotherapy for Melanoma Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France Overall Survival for Metastatic Melanoma Proportion Alive 1.0 0.8 0.6 0.4 0.2 Survival data
Immunotherapy for Melanoma Caroline Robert, MD, PhD Gustave Roussy and Université Paris Sud Villejuif, France Overall Survival for Metastatic Melanoma Proportion Alive 1.0 0.8 0.6 0.4 0.2 Survival data
Melanoma: Therapeutic Progress and the Improvements Continue
 Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3
 ESMO 2016 Congress 7-11 October, 2016 Copenhagen, Denmark Table of Contents Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3 Long-term results show adjuvant therapy with ipilimumab improves OS in high
ESMO 2016 Congress 7-11 October, 2016 Copenhagen, Denmark Table of Contents Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3 Long-term results show adjuvant therapy with ipilimumab improves OS in high
Releasing the Brakes on Tumor Immunity: Immune Checkpoint Blockade Strategies
 Releasing the Brakes on Tumor Immunity: Immune Checkpoint Blockade Strategies Jason Muhitch, PhD MIR 509 October 1 st, 2014 Email: jason.muhitch@roswellpark.org 0 Holy Grail of Tumor Immunity Exquisite
Releasing the Brakes on Tumor Immunity: Immune Checkpoint Blockade Strategies Jason Muhitch, PhD MIR 509 October 1 st, 2014 Email: jason.muhitch@roswellpark.org 0 Holy Grail of Tumor Immunity Exquisite
Toxicity from Checkpoint Inhibitors. James Larkin FRCP PhD
 Toxicity from Checkpoint Inhibitors James Larkin FRCP PhD Disclosures Research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): BMS, Eisai, GSK, MSD, Novartis, Pfizer, Roche/Genentech
Toxicity from Checkpoint Inhibitors James Larkin FRCP PhD Disclosures Research support: BMS, MSD, Novartis, Pfizer Consultancy (all non-remunerated): BMS, Eisai, GSK, MSD, Novartis, Pfizer, Roche/Genentech
Immunotherapy in Lung Cancer
 Immunotherapy in Lung Cancer Jamie Poust Pharm. D., BCOP Oncology Pharmacist University of Colorado Hospital Objectives Describe the recent advances in immunotherapy for patients with lung cancer Outline
Immunotherapy in Lung Cancer Jamie Poust Pharm. D., BCOP Oncology Pharmacist University of Colorado Hospital Objectives Describe the recent advances in immunotherapy for patients with lung cancer Outline
Checkpointinhibitoren in der Uro-Onkologie. Carsten Grüllich
 Checkpointinhibitoren in der Uro-Onkologie Carsten Grüllich 07.02.15 T-cell Aktivierung und Regulation T cell Costimulation Recognition MHC I Peptide b2m mrna Tumorantigen Tumor Pardoll Nature Rev Cancer
Checkpointinhibitoren in der Uro-Onkologie Carsten Grüllich 07.02.15 T-cell Aktivierung und Regulation T cell Costimulation Recognition MHC I Peptide b2m mrna Tumorantigen Tumor Pardoll Nature Rev Cancer
Heme Onc Today New York Melanoma Meeting March 22-23, 2013 PD-1 antibodies
 Heme Onc Today New York Melanoma Meeting March 22-23, 2013 PD-1 antibodies Jeffrey Weber Moffitt Cancer Center Tampa, FL Disclosures I have consulted for BMS, Merck, Genentech and GSK for Ad Boards and
Heme Onc Today New York Melanoma Meeting March 22-23, 2013 PD-1 antibodies Jeffrey Weber Moffitt Cancer Center Tampa, FL Disclosures I have consulted for BMS, Merck, Genentech and GSK for Ad Boards and
Immunotherapy for the Treatment of Cancer
 Immunotherapy for the Treatment of Cancer Jason Muhitch, PhD Assistant Professor Department of Urology Department of Immunology Roswell Park Comprehensive Cancer Center Oncology for Scientists March 15,
Immunotherapy for the Treatment of Cancer Jason Muhitch, PhD Assistant Professor Department of Urology Department of Immunology Roswell Park Comprehensive Cancer Center Oncology for Scientists March 15,
Renal Cell Carcinoma: Systemic Therapy Progress and Promise
 Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Renal Cell Carcinoma: Systemic Therapy Progress and Promise Michael B. Atkins, M.D. Deputy Director, Lombardi Comprehensive Cancer Ctr Georgetown University Medical Center Everolimus Rini, Campbell, Escudier.
Inmunoterapia en cáncer renal metastásico: redefiniendo el tratamiento de segunda línea
 Inmunoterapia en cáncer renal metastásico: redefiniendo el tratamiento de segunda línea Daniel Castellano Oncología Médica. Unidad de Tumores Genito-Urinarios Hospital Universitario 12 de Octubre I + 12
Inmunoterapia en cáncer renal metastásico: redefiniendo el tratamiento de segunda línea Daniel Castellano Oncología Médica. Unidad de Tumores Genito-Urinarios Hospital Universitario 12 de Octubre I + 12
ASCO 2014 Highlights*
 ASCO 214 Highlights* Investor Meeting June 2, 214 *American Society of Clinical Oncology, May 3 June 3, 214 Forward-Looking Information During this meeting, we will make statements about the Company s
ASCO 214 Highlights* Investor Meeting June 2, 214 *American Society of Clinical Oncology, May 3 June 3, 214 Forward-Looking Information During this meeting, we will make statements about the Company s
Checkpoint regulators a new class of cancer immunotherapeutics. Dr Oliver Klein Medical Oncologist ONJCC Austin Health
 Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Checkpoint regulators a new class of cancer immunotherapeutics Dr Oliver Klein Medical Oncologist ONJCC Austin Health Cancer...Immunology matters Anti-tumour immune response The participants Dendritc cells
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER
 Gynecologic Cancer InterGroup Cervix Cancer Research Network IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Cervix
Gynecologic Cancer InterGroup Cervix Cancer Research Network IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Cervix
Combination Approaches in Melanoma: A Balancing Act
 Combination Approaches in Melanoma: A Balancing Act Antoni Ribas, MD, PhD Jonsson Comprehensive Cancer Center University of California Los Angeles Los Angeles, California Advances in the Treatment of Metastatic
Combination Approaches in Melanoma: A Balancing Act Antoni Ribas, MD, PhD Jonsson Comprehensive Cancer Center University of California Los Angeles Los Angeles, California Advances in the Treatment of Metastatic
Immunotherapy: Toxicity Management. Dr. Megan Lyle Medical Oncologist Liz Plummer Cancer Care Centre Cairns Hospital
 Immunotherapy: Toxicity Management Dr. Megan Lyle Medical Oncologist Liz Plummer Cancer Care Centre Cairns Hospital Disclosures Honoraria and travel support from BMS, MSD, Novartis Advisory board for MSD
Immunotherapy: Toxicity Management Dr. Megan Lyle Medical Oncologist Liz Plummer Cancer Care Centre Cairns Hospital Disclosures Honoraria and travel support from BMS, MSD, Novartis Advisory board for MSD
Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma
 With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma") Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma Abstract #3003 Ribas A, Butler M, Lutzky J, Lawrence D, Robert C, Miller W,
Phase 1 Study Combining Anti-PD-L1 (MEDI4736) With BRAF (Dabrafenib) and/or MEK (Trametinib) Inhibitors in Advanced Melanoma Abstract #3003 Ribas A, Butler M, Lutzky J, Lawrence D, Robert C, Miller W,
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD
 La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
Out of 129 patients with NSCLC treated with Nivolumab in a phase I trial, the OS rate at 5-y was about 16 %, clearly higher than historical rates.
 6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
6th Meeting on external quality assessment in molecular pathology, Naples, May 12-13, 2017 Overview of clinical development of checkpoint inhibitors in solid tumors Pr Jaafar BENNOUNA University of Nantes
IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER. Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia
 IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Distinguishing self from non-self T cells trained in the thymus as
IMMUNOTHERAPY IN THE TREATMENT OF CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum Cancer Centre, Melbourne Australia Distinguishing self from non-self T cells trained in the thymus as
THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER
 Gynecologic Cancer InterGroup Cervix Cancer Research Network THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum
Gynecologic Cancer InterGroup Cervix Cancer Research Network THE ROLE OF TARGETED THERAPY AND IMMUNOTHERAPY IN THE TREATMENT OF ADVANCED CERVIX CANCER Linda Mileshkin, Medical Oncologist Peter MacCallum
Immunotherapy for the Treatment of Melanoma. Marlana Orloff, MD Thomas Jefferson University Hospital
 Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
CheckMate 012: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer
 CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
The Really Important Questions Current Immunotherapy Trials are Not Answering
 The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
IMMUNOTARGET THERAPY: ASPETTI GENERALI
 IMMUNOTARGET THERAPY: ASPETTI GENERALI Alessandro Minisini Dipartimento di Oncologia Azienda Ospedaliero Universitaria Udine Verona, 19 settembre 2015 HALLMARKS OF CANCER Douglas Hanahan, Robert A. Weinberg,
IMMUNOTARGET THERAPY: ASPETTI GENERALI Alessandro Minisini Dipartimento di Oncologia Azienda Ospedaliero Universitaria Udine Verona, 19 settembre 2015 HALLMARKS OF CANCER Douglas Hanahan, Robert A. Weinberg,
AACR 2018 Investor Meeting
 AACR 218 Investor Meeting April 16, 218 1 Forward-Looking Information This presentation contains statements about the Company s future plans and prospects that constitute forward-looking statements for
AACR 218 Investor Meeting April 16, 218 1 Forward-Looking Information This presentation contains statements about the Company s future plans and prospects that constitute forward-looking statements for
Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-028 Study
 Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-28 Study Abstract 427O Mehnert JM, Bergsland E, O Neil BH, Santoro A, Schellens
Pembrolizumab for Patients With PD-L1 Positive Advanced Carcinoid or Pancreatic Neuroendocrine Tumors: Results From the KEYNOTE-28 Study Abstract 427O Mehnert JM, Bergsland E, O Neil BH, Santoro A, Schellens
New treatments in melanoma
 New treatments in melanoma Paolo A. Ascierto, MD Istituto Nazionale Tumori Fondazione G. Pascale, Naples, Italy Meta-analysis of Phase II cooperative group trials in metastatic stage IV melanoma to determine
New treatments in melanoma Paolo A. Ascierto, MD Istituto Nazionale Tumori Fondazione G. Pascale, Naples, Italy Meta-analysis of Phase II cooperative group trials in metastatic stage IV melanoma to determine
Developing Novel Immunotherapeutic Cancer Treatments for Clinical Use
 Developing Novel Immunotherapeutic Cancer Treatments for Clinical Use Oncology for Scientists March 8 th, 2016 Jason Muhitch, PhD Assistant Professor Department of Urology Email: jason.muhitch@roswellpark.org
Developing Novel Immunotherapeutic Cancer Treatments for Clinical Use Oncology for Scientists March 8 th, 2016 Jason Muhitch, PhD Assistant Professor Department of Urology Email: jason.muhitch@roswellpark.org
Bristol-Myers Squibb, Braine-l Alleud, Belgium; 12 MD Anderson Cancer Center, Houston, TX, USA
 3531 Combination of nivolumab (NIVO) + ipilimumab (IPI) in the treatment of patients (pts) with deficient DNA mismatch repair (dmmr)/high microsatellite instability (MSI-H) metastatic colorectal cancer
3531 Combination of nivolumab (NIVO) + ipilimumab (IPI) in the treatment of patients (pts) with deficient DNA mismatch repair (dmmr)/high microsatellite instability (MSI-H) metastatic colorectal cancer
Understanding Checkpoint Inhibitors: Approved Agents, Drugs in Development and Combination Strategies. Michael A. Curran, Ph.D.
 Understanding Checkpoint Inhibitors: Approved Agents, Drugs in Development and Combination Strategies Michael A. Curran, Ph.D. MD Anderson Cancer Center Department of Immunology Disclosures I have research
Understanding Checkpoint Inhibitors: Approved Agents, Drugs in Development and Combination Strategies Michael A. Curran, Ph.D. MD Anderson Cancer Center Department of Immunology Disclosures I have research
II sessione. Immunoterapia oltre la prima linea. Alessandro Tuzi ASST Sette Laghi, Varese
 II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
Fifteenth International Kidney Cancer Symposium November 4-5, 2016 Marriott Miami Biscayne Bay, Miami, Florida, USA
 The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
The following presentation should not be regarded as an endorsement of a particular product/drug/technique by the speaker. The presentation topics were assigned to the speakers by the scientific committee
Checkpoint Regulators Cancer Immunotherapy takes centre stage. Dr Oliver Klein Department of Medical Oncology 02 May 2015
 Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Checkpoint Regulators Cancer Immunotherapy takes centre stage Dr Oliver Klein Department of Medical Oncology 02 May 2015 Adjuvant chemotherapy improves outcome in early breast cancer FDA approval of Imatinib
Ipilimumab ASCO Data Review and Discussion Webcast. Monday, June 2, 2008
 Ipilimumab ASCO Data Review and Discussion Webcast Monday, June 2, 2008 Slide 2 Forward Looking Statements Except for historical information, the matters contained in this slide presentation may constitute
Ipilimumab ASCO Data Review and Discussion Webcast Monday, June 2, 2008 Slide 2 Forward Looking Statements Except for historical information, the matters contained in this slide presentation may constitute
Update on the development of immune checkpoint inhibitors
 Update on the development of immune checkpoint inhibitors Jean-Pascal Machiels Department of Medical Oncology Laboratory of Medical Oncology Cliniques universitaires Saint-Luc Université catholique de
Update on the development of immune checkpoint inhibitors Jean-Pascal Machiels Department of Medical Oncology Laboratory of Medical Oncology Cliniques universitaires Saint-Luc Université catholique de
IMUNOTERAPIA NO CÂNCER DE PULMÃO: PRINCÍPIOS
 IMUNOTERAPIA NO CÂNCER DE PULMÃO: PRINCÍPIOS Dr. Gilberto de Castro Junior Professor Colaborador Livre-Docente Faculdade de Medicina da USP. Serviço de Oncologia Clínica - Instituto do Câncer do Estado
IMUNOTERAPIA NO CÂNCER DE PULMÃO: PRINCÍPIOS Dr. Gilberto de Castro Junior Professor Colaborador Livre-Docente Faculdade de Medicina da USP. Serviço de Oncologia Clínica - Instituto do Câncer do Estado
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Interleukin-2 Single Agent and Combinations
 Interleukin-2 Single Agent and Combinations Michael K Wong MD PhD Norris Cancer Center University of Southern California mike.wong@med.usc.edu Disclosures Advisory Board Attendance Merck Bristol Myers
Interleukin-2 Single Agent and Combinations Michael K Wong MD PhD Norris Cancer Center University of Southern California mike.wong@med.usc.edu Disclosures Advisory Board Attendance Merck Bristol Myers
Immunotherapy in Colorectal cancer
 Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
Immunotherapy in Colorectal cancer Ahmed Zakari, MD Associate Professor University of Central Florida, College of Medicine Medical Director, Gastro Intestinal Cancer Program Florida Hospital Cancer Institute
Clinical Activity and Safety of Anti-PD-1 (BMS , MDX-1106) in Patients with Advanced Non-Small-Cell Lung Cancer
 in Patients with Advanced Non-Small-Cell Lung Cancer") Clinical Activity and Safety of Anti-PD-1 (BMS-936558, MDX-1106) in Patients with Advanced Non-Small-Cell Lung Cancer J.R. Brahmer, 1 L. Horn, 2 S.J. Antonia, 3 D. Spigel, 4 L. Gandhi, 5 L.V. Sequist,
Clinical Activity and Safety of Anti-PD-1 (BMS-936558, MDX-1106) in Patients with Advanced Non-Small-Cell Lung Cancer J.R. Brahmer, 1 L. Horn, 2 S.J. Antonia, 3 D. Spigel, 4 L. Gandhi, 5 L.V. Sequist,
Melanoma in Focus: Update on Novel Therapy, Emerging Agents, and Optimizing Patient Care Presentation 1
 Presentation 1 The following is a transcript from a web-based CME -certified multimedia activity. Interactivity applies only when viewing the activity online. This activity is supported by educational
Presentation 1 The following is a transcript from a web-based CME -certified multimedia activity. Interactivity applies only when viewing the activity online. This activity is supported by educational
Biomarkers for immunotherapy. John Haanen MD PhD
 Biomarkers for immunotherapy John Haanen MD PhD Clear value of mobilizing endogenous tumor-specific T cell responses 1. TIL therapy J. Haanen, NKI-AVL 1. Checkpoint blockade C. Robert, NEJM 2015 Where
Biomarkers for immunotherapy John Haanen MD PhD Clear value of mobilizing endogenous tumor-specific T cell responses 1. TIL therapy J. Haanen, NKI-AVL 1. Checkpoint blockade C. Robert, NEJM 2015 Where
Nivolumab in Patients With DNA Mismatch Repair Deficient/Microsatellite Instability High Metastatic Colorectal Cancer: Update From CheckMate 142
 Nivolumab in Patients With DNA Mismatch Repair Deficient/Microsatellite Instability High Metastatic Colorectal Cancer: Update From CheckMate 142 Abstract #519 Overman MJ, Lonardi S, Leone F, McDermott
Nivolumab in Patients With DNA Mismatch Repair Deficient/Microsatellite Instability High Metastatic Colorectal Cancer: Update From CheckMate 142 Abstract #519 Overman MJ, Lonardi S, Leone F, McDermott
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Adverse effects of Immunotherapy. Asha Nayak M.D
 Adverse effects of Immunotherapy Asha Nayak M.D None Financial Disclosures Objectives Understand intensity of the AEs. Understanding unique side-effects. Develop effective monitoring and management guidelines.
Adverse effects of Immunotherapy Asha Nayak M.D None Financial Disclosures Objectives Understand intensity of the AEs. Understanding unique side-effects. Develop effective monitoring and management guidelines.
New Frontiers in Metastatic Melanoma: A Closer Look at the Role of Immunotherapy
 New Frontiers in Metastatic Melanoma: A Closer Look at the Role of Immunotherapy Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology
New Frontiers in Metastatic Melanoma: A Closer Look at the Role of Immunotherapy Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology
Kombination von Checkpointinhibitoren beim malignen Melanom
 Kombination von Checkpointinhibitoren beim malignen Melanom Dirk Jäger Medizinische Onkologie Nationales Centrum für Tumorerkrankungen Universitätsklinikum Heidelberg Ipilimumab beim metastasierten Melanom
Kombination von Checkpointinhibitoren beim malignen Melanom Dirk Jäger Medizinische Onkologie Nationales Centrum für Tumorerkrankungen Universitätsklinikum Heidelberg Ipilimumab beim metastasierten Melanom
Immunotherapy in Patients with Non-Small Cell Lung Cancer
 LIVE WEBINARS Immunotherapy in Patients with Non-Small Cell Lung Cancer Presented by: Leora Horn, MD, MSc Vanderbilt-Ingram Cancer Center July 14, 216 Moderated by Rose K. Joyce NCCN, Conferences and Meetings
LIVE WEBINARS Immunotherapy in Patients with Non-Small Cell Lung Cancer Presented by: Leora Horn, MD, MSc Vanderbilt-Ingram Cancer Center July 14, 216 Moderated by Rose K. Joyce NCCN, Conferences and Meetings
Immune Checkpoint Therapy Toxicities: Lessons learned and new strategies to improve outcomes
 Immune Checkpoint Therapy Toxicities: Lessons learned and new strategies to improve outcomes Geoffrey T. Gibney, MD Associate Professor Co-leader, Melanoma Disease Group Lombardi Comprehensive Cancer Center
Immune Checkpoint Therapy Toxicities: Lessons learned and new strategies to improve outcomes Geoffrey T. Gibney, MD Associate Professor Co-leader, Melanoma Disease Group Lombardi Comprehensive Cancer Center
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento
 tra la prima e la seconda linea di trattamento") Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
Checkpoint Inibitors for Bladder Cancer
 Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
OPTIMAL MANAGEMENT OF IMMUNE- RELATED ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT INHIBITORS
 OPTIMAL MANAGEMENT OF IMMUNE- RELATED ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT INHIBITORS Alberto Fusi Charité Comprehensive Cancer Centre Berlin, Germany 1 Immune check point blockade with CTLA-4, anti-pd-1
OPTIMAL MANAGEMENT OF IMMUNE- RELATED ADVERSE EVENTS ASSOCIATED WITH CHECKPOINT INHIBITORS Alberto Fusi Charité Comprehensive Cancer Centre Berlin, Germany 1 Immune check point blockade with CTLA-4, anti-pd-1
Nivolumab in combination with ipilimumab in metastatic renal cell carcinoma (mrcc): Results of a phase I trial
: Results of a phase I trial") Nivolumab in combination with ipilimumab in metastatic renal cell carcinoma (mrcc): Results of a phase I trial H. Hammers, E.R. Plimack, J.R. Infante, M.S. Ernstoff, B. Rini, D.F. McDermott, A. Razak,
Nivolumab in combination with ipilimumab in metastatic renal cell carcinoma (mrcc): Results of a phase I trial H. Hammers, E.R. Plimack, J.R. Infante, M.S. Ernstoff, B. Rini, D.F. McDermott, A. Razak,