Sunita D Nasta MD FACP Associate Prof of Clinical Med January 26, 2018
|
|
|
- Edmund Fields
- 6 years ago
- Views:
Transcription

1 Sunita D Nasta MD FACP Associate Prof of Clinical Med January 26, 2018
2

3 Escalated dosing (100, 150, 200, and 300 mg) of oral azacitadine combined with R-CHOP21 Untreated DLBCL, grade 3B follicular lymphoma, or transformed FL :IPI score >2 ECOG PF <2 Ann Arbor stage II-IV Primed with CC-486 for 7 days prior to R-CHOP on day 1 of cycle 1. Thereafter, given for 14 days (Day 8-21) Standard G-CSF administration allowed Given for 6 cycles (Cycle=21 days) Endpoints Safety DLT Maximal administered dose of CC-486 combined with R-CHOP Secondary endpoints:pk, Preliminary efficacy(orr, CR)
4 33 patients enrolled Median age=65 years (25-80) >60 years (67%) Male (55%) DLBCL (97%, 32 patients including 5 transformed from FL) 3B FL = 1 patient Stage III-IV disease (91%) IPI >3 (58%) 91% completed 6 full cycles CC-486 dose reduction occurred in 9 patients (27%) due to adverse events 150 mg discontinued in 1 patient due to febrile neutropenia
5 Neutropenia (70%), Grade 3-4 (58%), Grade 3-4 febrile neutropenia (21%) Nausea (64%) Constipation (58%) Fatigue (55%) Vomiting (48%) Diarrhea (48%) DLT seen in 2 patients including grade 4 neutropenia (200 mg cohort) and 1 grade 4 neutropenia (300 mg cohort) Maximal administered dose was 300 mg and identified as the recommended phase II dose
6 97% ORR (85% PET-negative CR) IPI score patients >3, ORR=100% (84% CR) Correlative analysis Decreased IFN- α2a and increased IFN-β and IFN-λ in blood (n=24), and significant tumor and cf-dna hypomethylation Similar toxicities consistent with R-CHOP and azacitidine Promising efficacy in high-risk previously untreated DLBCL or grade 3B FL




7 Jakub Svoboda, Daniel J. Landsburg, Sunita Dwivedy Nasta, Stefan K. Barta, Nadia Khan, Henry C. Fung, Carlyn Rose Tan, Joanne Filicko- O'Hara, Sameh Gaballa, Lauren Strelec, Sarah J. Nagle, Steven M. Bair, Sheryl Mitnick, Terease S. Waite, Rachel L. Sargent, Agata M. Bogusz, Ziver Sahin, Anthony R. Mato, and Stephen J. Schuster Svoboda et al, ASH 2017
8 A phase I/II multicenter study Enrollment began in 1/2014 and completed in 6/2017 Key eligibility criteria Age 18 years and above Histologically confirmed CD30+ PMBL, DLBCL, or grey zone lymphoma Previously untreated No specific cut off percentage for CD30 stain required, but tumor had to be positive by immunohistochemistry Measurable disease Any stage ECOG PS 0-3 Primary Objectives Phase I: safety and maximum tolerated dose of combination Phase II: overall response rate (ORR) at the end of systemic treatment 7 Secondary Objective Phase I: ORR Phase I and II: progression free survival (PFS), overall survival (OS) Correlative studies: outcomes for each lymphoma subtype, correlation with CD30 expression and customized NanoString assay 7) Cheson et al, JCO 2007; 25:5, Svoboda et al, ASH 2017
9 33 PATIENTS CONSENTED PENN (N=26), FCCC (N=6), TJUH (N=1) 1 PATIENT RE-CLASSIFIED FROM GZL TO chl 32 PATIENTS ENROLLED 1 PATIENT WITHDREW CONSENT 31 PATIENTS EVALUABLE FOR TOXICITY 2 PATIENTS WITHOUT EOT ASSESSMENT 29 PATIENTS EVALUABLE FOR EFFICACY Svoboda et al, ASH 2017
10 ALL PATIENTS (N=31) Age Median 37 years Range years Female 15 (48%) Elevated LDH 21 (68%) Stage III-IV 13 (42%) Lymphoma subtype PMBL 23 (74%) DLBCL 6 (19%) GZL 2 (7%) ECOG PS Median 1 Range 0-2 PMBL: TUMOR SIZE (N=23) Bulky ( 7.5 cm) 21 (91%) Median size 9.5 cm Range cm Svoboda et al, ASH 2017
11 HEMATOLOGICAL ADVERSE EVENTS (AE) AE Total (N=31) G1 G2 G3 G4 Leukopenia 77% 13% 32% 16% 16% Neutropenia* (NTP) 68% 3% 23% 13% 29% Lymphopenia 94% 6% 16% 45% 26% Febrile NTP** 23% % - Anemia 25% 19% 3% 3% G3/4 AEs BV-R-CHP/R-CHOP/DA-EPOCH-R Grade 3 or 4 AE BV+R-CHP N=31 R-CHOP 8 N=233 EPOCH-R 8 N=232 All AE 87% 76% 97% Hematologic 74% 73% 97% Nonhematologic 35% 41% 71% 8) CALBG/Alliance Wilson et al, Blood 2016, Abstract 469 Thrombocytopenia 6% 3% 3% - - No treatment related deaths NON-HEMATOLOGICAL AES IN 10% OF PATIENTS AE Total (N=31) Sensory neuropathy 45% 35% 10% Fatigue 42% 42% G1 G2 G3 G4 Nausea 42% 29% 10% 3% Diarrhea 26% 16% 10% Mucositis 19% 16% 3% Motor neuropathy 10% 7% 3% Constipation 10% 10% Early discontinuation due to AE: 1 patient discontinued protocol treatment due to G3 sepsis and G3 cardiomyopathy after C4 1 patient discontinued BV due to G2 pneumonitis after C5 Dose reduction: 2 patients required BV dose reduction to 1.2 mg/kg due to sensory neuropathy 1 patient developed AML at 2 years from completion of therapy *) 16% had no G-CSF, 6% had G-CSF support 2 cycles **) Total of 9 NTP fever episodes in 7 patients Svoboda et al, ASH 2017
: overall response rate at the end of")

12 Phase I (N=6): no DLT with the starting dose of BV 1.8 mg/kg in combination with R-CHP Phase I/II (N=29): overall response rate at the end of treatment PET/CT imaging TOTAL N=29 PMBL N=22 DLBC L N=5 GZL N=2 ORR 100% 100% 100% 100% CR 86% 82% 100% 100% PR 14% 18% Pre-treatment Post-treatment ORR: overall response rate CR: complete response PR: partial response Svoboda et al, ASH 2017

13 Phase III randomized prospective trial September 2012-July 2015 Randomized Obinutuzumab 1000 mg IV on D1 and D8 cycle 1 and 2 then day 1 of cycle 3-4 Rituximab 375 mg/m2 IV D1 of each cycle PET Scan Performed at baseline, after 2 and 4 cycles of induction immunochemotherapy PET2+/PET4- patients received autologous stem cell transplant PET4+ were treated according to investigator choice Primary endpoint 2y-event free survival defined by PET positivity after 2 or 4 induction cycles, progression or relapse Secondary objectives Safety Response rates Progression free survival Overall survival
14 670 patients enrolled: Median age=48 y; Male 55.7%;IPI>2=41.8% N=336 randomized to obinutuzumab plus chemotherapy N=165 G-ACVBP N=171 G-CHOP N=334 randomized to rituximab plus chemotherapy N=162 R-ACVBP N=172 R-CHOP 455 SAEs N=250 obinutuzumab (N=10 fatal; N=7 G-ACVBP arm) N=205 rituximab (N=1 fatal) Median follow-up=25.2 months 42.4% had an event Third interim analysis; recommended stopping trial Stratified 2y-EFS not statistically different between arms (p=0.1321, above the futility bound of 0.069) For IPI 1 patients, 2-year EFS was 61.3% (95%CI; ) for G-CHOP versus 59.9% (95%CI; ) for R-CHOP
15 Consistent with previous studies, obinutuzumab plus chemotherapy is not superior to rituximab plus chemotherapy Cell of origin data is currently under investigation using nanostring technology

16
:1800-1808. 2. Van den Neste E, et al. BMT. 2016;51:51-57.")
17 Patients with relapsed or refractory DLBCL have a poor prognosis Low rate of response to salvage therapy (CR 8%; PR 18%)1 Short survival (median OS 4 months)2 SOC for these patients is high dose chemotherapy followed by auto-sct Only about a quarter of these patients can receive a transplant 1. Crump M, et al. Blood. 2017;130(16): Van den Neste E, et al. BMT. 2016;51:51-57.
18 100 r/r DLBCL ~ 50 transplant eligible ~ 50 transplant ineligible (age, comorbidit y) ~ 25 responded to chemother apy and proceeded to transplant ~ 25 transplant ineligible (nonresponsiv e to chemotherapy ) ~ 10 cured ~ 15 relapsed after transplant ~ 90 No available SOC chemo options Figure adapted from Friedberg JW. J Am Soc Hematol Educ Book. 2011;1: DLBCL, diffuse large B-cell lymphoma; R/R, relapsed/refractory; SOC, 18 standard of care.
19 ASH Abstract First Author Description LBA-6 Neelapu 3026 Schuster Pivotal Phase 2 ZUMA-1 Trial of Kte- C19 in Patients With Relapsed/Refractory DLBCL Phase 2a Study of CTL019 in Patients With Relapsed/Refractory DLBCL and tfl
20 Original Article Chimeric Antigen Receptor T Cells in Refractory B- Cell Lymphomas Stephen J. Schuster, M.D., Jakub Svoboda, M.D., Elise A. Chong, M.D., Sunita D. Nasta, M.D., Anthony R. Mato, M.D., Özlem Anak, M.D., Jennifer L. Brogdon, Ph.D., Iulian Pruteanu-Malinici, Ph.D., Vijay Bhoj, M.D., Ph.D., Daniel Landsburg, M.D., Mariusz Wasik, M.D., Bruce L. Levine, Ph.D., Simon F. Lacey, Ph.D., Jan J. Melenhorst, Ph.D., David L. Porter, M.D., and Carl H. June, M.D. N Engl J Med Volume 377(26): December 28, 2017

21 Study Overview
22 Progression-free Survival, Response Duration, and Overall Survival. Schuster SJ et al. N Engl J Med ;377:

23 Characteristics of the Patients at Baseline. Schuster SJ et al. N Engl J Med ;377:

24 Adverse Events of Special Interest That May Have Been Related to CTL019 Therapy. Schuster SJ et al. N Engl J Med ;377:
25 Original Article Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma Sattva S. Neelapu, M.D., Frederick L. Locke, M.D., Nancy L. Bartlett, M.D., Lazaros J. Lekakis, M.D., David B. Miklos, M.D., Ph.D., Caron A. Jacobson, M.D., M.M.Sc., Ira Braunschweig, M.D., Olalekan O. Oluwole, M.B., B.S., M.P.H., Tanya Siddiqi, M.D., Yi Lin, M.D., Ph.D., John M. Timmerman, M.D., Patrick J. Stiff, M.D., Jonathan W. Friedberg, M.D., M.M.Sc., Ian W. Flinn, M.D., Ph.D., Andre Goy, M.D., Brian T. Hill, M.D., Ph.D., Mitchell R. Smith, M.D., Ph.D., Abhinav Deol, M.D., Umar Farooq, M.D., Peter McSweeney, M.D., Javier Munoz, M.D., Irit Avivi, M.D., Januario E. Castro, M.D., Jason R. Westin, M.D., Julio C. Chavez, M.D., Armin Ghobadi, M.D., Krishna V. Komanduri, M.D., Ronald Levy, M.D., Eric D. Jacobsen, M.D., Thomas E. Witzig, M.D., Patrick Reagan, M.D., Adrian Bot, M.D., Ph.D., John Rossi, M.S., Lynn Navale, M.S., Yizhou Jiang, Ph.D., Jeff Aycock, B.A., Meg Elias, R.N., B.S.N., David Chang, M.D., Ph.D., Jeff Wiezorek, M.D., and William Y. Go, M.D., Ph.D. N Engl J Med Volume 377(26): December 28, 2017

26 Study Overview
27 Objective Response Rate among the 101 Treated Patients. Neelapu SS et al. N Engl J Med ;377:
28 Kaplan Meier Estimates of the Duration of Response, Progression-free Survival, and Overall Survival. Neelapu SS et al. N Engl J Med ;377:
29 CAR T-Cell Expansion and Correlations with Response and Adverse Events. Neelapu SS et al. N Engl J Med ;377:

30 Treatment Disposition and Baseline Characteristics of the Patients. Neelapu SS et al. N Engl J Med ;377:

31 Adverse Events, the Cytokine Release Syndrome, and Neurologic Events Associated with Treatment. Neelapu SS et al. N Engl J Med ;377:
32 Conclusions
33 Single-arm global pivotal trial of tisagenlecleucel in patients with r/r DLBCL (NCT ) Screening, apheresis, and cryopreservatio n Enrollm ent Bridging chemotherapy Tisagenlecl eucel manufactur ing Restagi ng, lymphodepl etion a Tisagenlecl eucel infusion b Safety and efficacy follow-up Imaging at months 1, 3, 6, 9, a To be completed 2 to 14 days prior to tisagenlecleucel infusion. b Infusion conducted on an in- or outpatient basis at investigator discretion. 33 DLBCL, diffuse large B-cell lymphoma; r/r, relapsed/refractory.

34 Global clinical trial with centralized manufacturing of tisagenlecleucel 27 sites in 10 countries across North America, Europe, Australia and Asia * * * Manufacturing sites 34
35 Key eligibility criteria 18 years of age Central confirmation of histology 2 prior lines of therapy for DLBCL PD after or ineligible for auto-sct No prior anti-cd19 therapy No active CNS involvement Endpoints Primary endpoint: best overall response rate (ORR: CR + PR) Lugano criteria used for response assessment by IRC 1 Null hypothesis of ORR 20% Secondary endpoints: DOR, OS, safety 1. Cheson BD, et al. J Clin Oncol. 2014;32(27): auto-sct, autologous stem cell transplant; CNS, central nervous system; CR, complete response; DLBCL, diffuse large B-cell lymphoma; DOR, duration of response; IRC, Independent Review Committee; ORR, overall response rate; OS, overall survival; PD, progressive disease; PR, partial response.
36 Pending infusion n = 5 Enrolled n = 147 Infused n = 99 Enrollment began July 2015 Discontinued before Total = infusion 43 Inability to manufacture Patient status related a = 9 = 34 n n Evaluable for response b n = 81 a Death (n = 16); physician decision (n = 12); patient decision (n = 3); adverse event (n = 2); protocol deviation (n = 1). b Patients who had 3 months of follow-up or earlier progression of disease 3
37 Patients (N = 99) Age, median (range), years 56 (22-76) 65 years, % 23 ECOG performance status 0/1 55/45 Central histology review Diffuse large B-cell lymphoma, % 80 Transformed follicular lymphoma, % 19 Double/triple hits in CMYC/BCL2/BCL6 genes, % 15 a Cell of origin b Germinal center B-cell type, % 52 Nongerminal center B-cell type, % 42 Number of prior lines of antineoplastic therapy, % 2/3/4-6 44/31/19 Refractory/relapsed to last therapy, % 52/48 Prior auto-sct, % 47 Bridging chemotherapy: 89/99 Lymphodepleting chemotherapy: 92/99 a CMYC + BCL2, n = 4; CMYC + BCL2 + BCL6, n = 8; CMYC + BCL6, n = b Determined by the Choi algorithm. auto-sct, autologous stem cell transplant; ECOG, Eastern Cooperative Oncology Group.
 38 Response at 6 Months (n = 46) ORR (CR + PR) 53 38 37 CR 40 32 30 PR 14 6 7 Durability of responses is shown by the stability between 3 and 6 month response rates")
38 Response Rate, % Best Overall Response Rate a (N = 81) a P <.0001; (95% CI, 42%-64%). Null hypothesis of ORR 20%. Response at 3 Months (N = 81) 38 Response at 6 Months (n = 46) ORR (CR + PR) CR PR Durability of responses is shown by the stability between 3 and 6 month response rates Response at 3 months is indicative of the long term benefit of this treatment CR, complete response; ORR, overall response rate; PR, partial response.
![ORR n/n (%) [95% CI] All patients Null hypothesis of ORR 20% 43/81 (53.1) [41.7-64.3] Age, years < 65 32/64 (50.0) [37.2-62.8] 65 11/17 (64.7) [38.3-85.8] Sex Female 18/29 (62.1) [42.3-79.](/docs-images/74/71453605/images/39-1.jpg "3] Male 25/52 (48.1) [34.0-62.4] Prior antineoplastic therapy 2 lines 22/41 (53.7) [37.4-69.3] > 2 lines 21/40 (52.5) [36.1-68.5] Cell of origin a Nongerminal center 19/34 (55.9) [37.9-72.")
39 ORR n/n (%) [95% CI] All patients Null hypothesis of ORR 20% 43/81 (53.1) [ ] Age, years < 65 32/64 (50.0) [ ] 65 11/17 (64.7) [ ] Sex Female 18/29 (62.1) [ ] Male 25/52 (48.1) [ ] Prior antineoplastic therapy 2 lines 22/41 (53.7) [ ] > 2 lines 21/40 (52.5) [ ] Cell of origin a Nongerminal center 19/34 (55.9) [ ] Germinal center 19/41 (46.3) [ ] Rearranged MYC/BCL2/BCL6 Double/triple hits 5/12 (41.7) [ ] Other 38/69 (55.1) [ ] a Data from 6 patients are missing ORR, overall response rate.

40 100 Probabilty of Relapse Free, % Time From Onset of 0 Patients at risk Response, months Efficacy analysis set = all patients who received a tisagenlecleucel infusion 3 months prior to data-cut date Median DOR and OS not reached Almost all patients in CR at month 3 remained in CR No patients proceeded to transplant while in response CR, complete response; DOR, duration of response; OS, overall response.
 were infused as outpatients 20/26 patients (77%) remained outpatient for 3 days after infusion 41 (N = 99) Grade 3,")
41 AESI a All Grades, % a Occurring within 8 weeks of tisagenlecleucel infusion. b Cytokine release syndrome was graded using the Febrile Penn scale. neutropenia c At day No deaths due to tisagenlecleucel, CRS or cerebral edema 26 patients (26%) were infused as outpatients 20/26 patients (77%) remained outpatient for 3 days after infusion 41 (N = 99) Grade 3, % Grade 4, % Cytokine release syndrome b Neurological events Prolonged cytopenia c Infections AESI, adverse events of special interest; CRS, cytokine release syndrome.
42 1. Porter DL, et al. Sci Transl Med. 2015;7(303):303ra139. Patients (N = 99) Time to onset, median (range), days a,b 3 (1-9) Duration, median (range), days a 7 (2-30) Hypotension that required intervention, % High-dose vasopressors 6 Intubated, % 8 a Calculated based only on patients who had cytokine release syndrome (n = 57), excluding 1 patient Corticosteroids who had onset on day b Cytokine release syndrome was graded using the Penn scale and managed by a protocolspecific algorithm Anticytokine therapy, % 16 Tocilizumab 15
43 Durable responses were associated with persistent transgene levels in blood Tisagenlecleucel Transgene, copies/µg DNA 100, , CR (n = 26) / PR (n = 5) LLOQ = 50 copies/µg Time From Infusion, days 1. Awasthi R, et al. Blood. 2017;130(suppl 1) [abstract 5211]. CR, complete response; PR, partial response. 4
44 Response (tumor response at month 3) No apparent relationship Responses observed across full range of doses Dose ( CAR- positive viable T cells) a Safety (CRS and neurological events) No relationship observed between dose and neurological events Higher probability of CRS with higher doses CRS is manageable per algorithm Exposure (maximal expansion from qpcr data) a 1 patient received a dose < CAR-positive viable T cells. Dose and exposure were independent No expansion (AUC 0-28d and C max )- response relationship observed 1. Awasthi R, et al. Blood. 2017;130(suppl 1) [abstract 5211]. CRS, cytokine release syndrome. 44
45 Best ORR 53% (CR 40%); P <.0001 ORR 38% (CR 32%) at 3 months; ORR 37% (CR 30%) at 6 months Almost all patients in CR at month 3 remained in CR Median DOR and OS were not reached AEs were effectively managed by appropriately trained studysite personnel No deaths were attributed to tisagenlecleucel, CRS or cerebral edema Tisagenlecleucel was safely administered in both the inpatient and outpatient settings 45 AE, adverse event; CR, complete remission; CRS, cytokine release syndrome; DOR, duration of response; ORR, overall response rate; OS, overall survival.
46
:normal LDH, ECOG PF 0-1, <Stage II, and no tumor lesion >7")
47 Goal: Validate a lower intensity therapy, DA- EPOCH-R, in adult patients with BL, including HIV+ patients Use risk-adapted approach based on baseline risk category and interim PET scans after 2 cycles Population Newly diagnosed BL 18 and older Any HIV status Low risk(lr):normal LDH, ECOG PF 0-1, <Stage II, and no tumor lesion >7 cm
48 Low risk patients received 2 cycles of DA-EPOCH-R without IT followed by PET If interim PET was negative Receive 1 more cycle High risk patients with negative brain MRI and CSF cytology/flow cytometry received 2 cycles of DA- EPOCH-R without IT therapy followed by PET If interim PET was negative Received 4 additional cycles of DA-EPOCH-R including IT MTX 12 mg on day 1 and 5 (Total of 8 doses) High-risk patients with active CNS disease at baseline received concurrent MTX 12 mg IT twice weekly for 2 weeks past negative (minimum of 4 weeks), followed by MTX 12 mg once weekly x 6 and MTX 12 mg monthly x 6 No cranial radiation administered
49 113 patients enrolled 110 patients completed therapy, 3 patients on treatment Median age =49y (18-86y) >50y (49%) >60y (26%) Male (79%) Stage III-IV (69%) Elevated LDH (66%) CNS involvement (10%) HIV+ (26%) Low risk (12%); high risk (88%) Median follow-up=35.7 months PFS for all patients beyond 10.2 months= 85.7% (95% CI: %) Freedom-from-progression= 91.8 (95% CI: %) Overall survival= 85.9% (95% CI: %) HIV status did not impact survival and therapy was equally effective across all age groups Patients with BM and/or CNS involvement were at highest risk of treatment failure No progression or death in the LR group 14 deaths in HR arm (7 due to disease progression, 3 occurred during treatment)
50 DA-EPOCH-R cures most adult patients with BL irrespective of HIV status Low risk treated with 3 cycles of systemic therapy and no IT therapy High risk patients are more favorably treated with more intensive regimens Patients with BM and/or CNS involvement are at the highest risk of treatment failure

51 Hua-Jay J. Cherng, Rachel Lynn Sargent, Sunita Dwivedy Nasta, Jakub Svoboda, Stephen J. Schuster, Anthony R. Mato, April Schrank-Hacker, Jennifer J.D. Morrissette and Daniel J. Landsburg Blood :4136;
52 Hua-Jay J. Cherng et al. Blood 2017;130: by American Society of Hematology
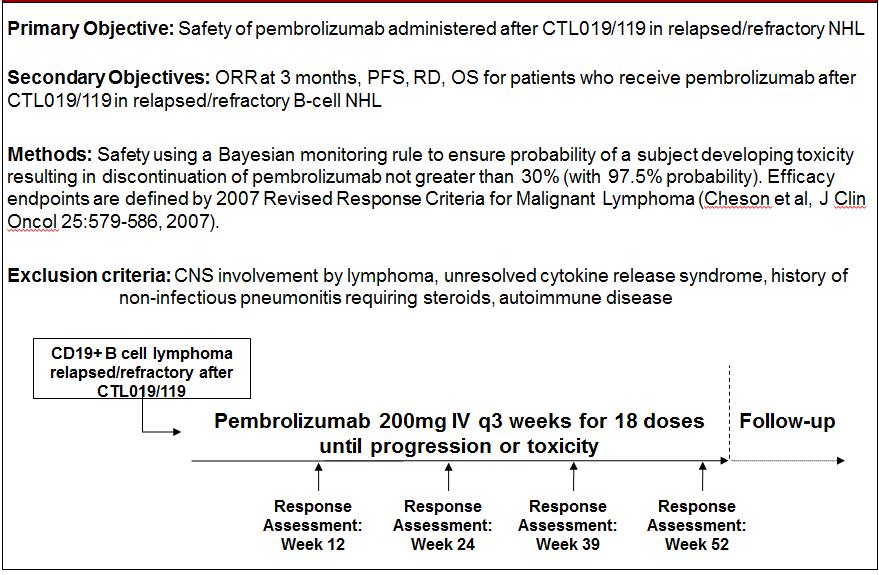
53 Elise A. Chong, J. Joseph Melenhorst, Jakub Svoboda, Sunita Dwivedy Nasta, Daniel J. Landsburg, Anthony R. Mato, Lifeng Tian, Harit Parakandi, Simon F. Lacey, Carl H. June, Stephen J. Schuster
54

55
56
57 PD1 blockade with pembrolizumab appears safe and results in clinical responses in some patients with progression of DLBCL after anti-cd19 directed chimeric antigen receptor modified T cell therapy. Analysis of the pharmacokinetics of CAR T- cells in patients treated with pembrolizumab appears to identify responding patients, and supports the hypothesis that CAR T cells may be rejuvenated by infusion of PD1 antagonists.
R/R DLBCL Treatment Landscape
 An Updated Analysis of JULIET, a Global Pivotal Phase 2 Trial of Tisagenlecleucel in Adult Patients With Relapsed or Refractory Diffuse Large B-Cell Lymphoma Abstract S799 Borchmann P, Tam CS, Jäger U,
An Updated Analysis of JULIET, a Global Pivotal Phase 2 Trial of Tisagenlecleucel in Adult Patients With Relapsed or Refractory Diffuse Large B-Cell Lymphoma Abstract S799 Borchmann P, Tam CS, Jäger U,
Background. Outcomes in refractory large B-cell lymphoma with traditional standard of care are extremely poor 1
 2-Year Follow-Up and High-Risk Subset Analysis of ZUMA-1, the Pivotal Study of Axicabtagene Ciloleucel (Axi-Cel) in Patients with Refractory Large B Cell Lymphoma Abstract 2967 Neelapu SS, Ghobadi A, Jacobson
2-Year Follow-Up and High-Risk Subset Analysis of ZUMA-1, the Pivotal Study of Axicabtagene Ciloleucel (Axi-Cel) in Patients with Refractory Large B Cell Lymphoma Abstract 2967 Neelapu SS, Ghobadi A, Jacobson
CAR-T cell therapy pros and cons
 CAR-T cell therapy pros and cons Stephen J. Schuster, MD Professor of Medicine Perelman School of Medicine of the University of Pennsylvania Director, Lymphoma Program & Lymphoma Translational Research
CAR-T cell therapy pros and cons Stephen J. Schuster, MD Professor of Medicine Perelman School of Medicine of the University of Pennsylvania Director, Lymphoma Program & Lymphoma Translational Research
CAR T-Cell Therapy for Lymphoma: Assessing Long-Term Durability. Julie M. Vose, MD, MBA
 CAR T-Cell Therapy for Lymphoma: Assessing Long-Term Durability Julie M. Vose, MD, MBA Relevant Disclosures Research Funding: Kite Pharma/Gilead, JUNO/Celgene, Novartis Honorarium/Ad Boards: Novartis,
CAR T-Cell Therapy for Lymphoma: Assessing Long-Term Durability Julie M. Vose, MD, MBA Relevant Disclosures Research Funding: Kite Pharma/Gilead, JUNO/Celgene, Novartis Honorarium/Ad Boards: Novartis,
MMAE disrupts cell division and triggers apoptosis. Pola binds to cell surface antigen CD79b. Pola is internalized; linker cleaves, releasing MMAE
 Adding Polatuzumab Vedotin (Pola) to Bendamustine and Rituximab () Treatment Improves Survival in Patients With Relapsed/Refractory DLBCL: Results of a Phase II Clinical Trial Abstract S802 Sehn LH, Kamdar
Adding Polatuzumab Vedotin (Pola) to Bendamustine and Rituximab () Treatment Improves Survival in Patients With Relapsed/Refractory DLBCL: Results of a Phase II Clinical Trial Abstract S802 Sehn LH, Kamdar
Chimeric An+gen Receptor (CAR) Modified T Cell Therapy: Mee#ng the Unmet Need in Follicular Lymphoma
 Modified T Cell Therapy: Mee#ng the Unmet Need in Follicular Lymphoma") Chimeric An+gen Receptor (CAR) Modified T Cell Therapy: Mee#ng the Unmet Need in Follicular Lymphoma Stephen J. Schuster, M.D. Director, Lymphoma Program & Lymphoma Translational Research, Abramson Cancer
Chimeric An+gen Receptor (CAR) Modified T Cell Therapy: Mee#ng the Unmet Need in Follicular Lymphoma Stephen J. Schuster, M.D. Director, Lymphoma Program & Lymphoma Translational Research, Abramson Cancer
Chimeric Antigen Receptor - CAR T cell therapy. Frederick L. Locke, MD 2/17/2017
 Chimeric Antigen Receptor - CAR T cell therapy Frederick L. Locke, MD 2/17/2017 T cells are immune system cells that normally fight infection Each T cell recognizes a specific target T cells multiply and
Chimeric Antigen Receptor - CAR T cell therapy Frederick L. Locke, MD 2/17/2017 T cells are immune system cells that normally fight infection Each T cell recognizes a specific target T cells multiply and
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma
 Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA
 DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA Ian Flinn, CB Miller, KM Ardeshna, S Tetreault, SE Assouline, PL Zinzani, J Mayer, M Merli, SD Lunin, AR Pettitt,
DYNAMO: A PHASE 2 STUDY OF DUVELISIB IN PATIENTS WITH REFRACTORY INDOLENT NON HODGKIN LYMPHOMA Ian Flinn, CB Miller, KM Ardeshna, S Tetreault, SE Assouline, PL Zinzani, J Mayer, M Merli, SD Lunin, AR Pettitt,
State of the art: CAR-T cell therapy in lymphoma
 State of the art: CAR-T cell therapy in lymphoma 14 th annual California Cancer Consortium conference Tanya Siddiqi, MD City of Hope Medical Center 8/11/18 Financial disclosures Consultant for Juno therapeutics
State of the art: CAR-T cell therapy in lymphoma 14 th annual California Cancer Consortium conference Tanya Siddiqi, MD City of Hope Medical Center 8/11/18 Financial disclosures Consultant for Juno therapeutics
CAR-T Therapy: The Past, The Present, and The Future. Nilay Shah, MD Michael Chargualaf, PharmD, BCOP WVU Medicine Mary Babb Randolph Cancer Center
 CAR-T Therapy: The Past, The Present, and The Future Nilay Shah, MD Michael Chargualaf, PharmD, BCOP WVU Medicine Mary Babb Randolph Cancer Center Objectives Review indications for FDA approved CAR-T therapy
CAR-T Therapy: The Past, The Present, and The Future Nilay Shah, MD Michael Chargualaf, PharmD, BCOP WVU Medicine Mary Babb Randolph Cancer Center Objectives Review indications for FDA approved CAR-T therapy
Supplemental Information. Phase 1 Results of ZUMA-1: A Multicenter Study. of KTE-C19 Anti-CD19 CAR T Cell Therapy. in Refractory Aggressive Lymphoma
 YMTHE, Volume 25 Supplemental Information Phase 1 Results of ZUMA-1: A Multicenter Study of KTE-C19 Anti-CD19 CAR T Cell Therapy in Refractory Aggressive Lymphoma Frederick L. Locke, Sattva S. Neelapu,
YMTHE, Volume 25 Supplemental Information Phase 1 Results of ZUMA-1: A Multicenter Study of KTE-C19 Anti-CD19 CAR T Cell Therapy in Refractory Aggressive Lymphoma Frederick L. Locke, Sattva S. Neelapu,
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma
 Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Objectives. Emily Whitehead 10/11/2018. Chimeric Antigen Recepetor T-Cells (CAR-T) CAR-T Therapy: The Past, The Present, and The Future
 CAR-T Therapy: The Past, The Present, and The Future") Objectives CAR-T Therapy: The Past, The Present, and The Future Nilay Shah, MD Michael Chargualaf, PharmD, BCOP WVU Medicine Mary Babb Randolph Cancer Center Review indications for FDA approved CAR-T therapy
Objectives CAR-T Therapy: The Past, The Present, and The Future Nilay Shah, MD Michael Chargualaf, PharmD, BCOP WVU Medicine Mary Babb Randolph Cancer Center Review indications for FDA approved CAR-T therapy
Immuntherapie maligner Lymphome. Mathias Witzens-Harig Medizinische Klinik V Universität Heidelberg
 Immuntherapie maligner Lymphome Mathias Witzens-Harig Medizinische Klinik V Universität Heidelberg 20.02.2016 Immuntherapie maligner Lymphome Allogene Stammzelltransplantation Antikörper, z.b. Rituximab
Immuntherapie maligner Lymphome Mathias Witzens-Harig Medizinische Klinik V Universität Heidelberg 20.02.2016 Immuntherapie maligner Lymphome Allogene Stammzelltransplantation Antikörper, z.b. Rituximab
The case against maintenance rituximab in Follicular lymphoma. Jonathan W. Friedberg M.D., M.M.Sc.
 The case against maintenance rituximab in Follicular lymphoma Jonathan W. Friedberg M.D., M.M.Sc. Follicular lymphoma: What are goals of treatment? Change natural history of disease: Decrease transformation
The case against maintenance rituximab in Follicular lymphoma Jonathan W. Friedberg M.D., M.M.Sc. Follicular lymphoma: What are goals of treatment? Change natural history of disease: Decrease transformation
Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL
 New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
New Targets and Treatments for Follicular Lymphoma
 Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
Have we moved beyond EPOCH for B-cell non-hodgkin lymphoma? YES!
 Have we moved beyond EPOCH for B-cell non-hodgkin lymphoma? YES! Christopher Flowers, MD, MSc Associate Professor Director, Lymphoma Program Department of Hematology and Oncology Emory School of Medicine
Have we moved beyond EPOCH for B-cell non-hodgkin lymphoma? YES! Christopher Flowers, MD, MSc Associate Professor Director, Lymphoma Program Department of Hematology and Oncology Emory School of Medicine
Update: Non-Hodgkin s Lymphoma
 2008 Update: Non-Hodgkin s Lymphoma ICML 2008: Update on non-hodgkin s lymphoma Diffuse Large B-cell Lymphoma Improved outcome of elderly patients with poor-prognosis diffuse large B-cell lymphoma (DLBCL)
2008 Update: Non-Hodgkin s Lymphoma ICML 2008: Update on non-hodgkin s lymphoma Diffuse Large B-cell Lymphoma Improved outcome of elderly patients with poor-prognosis diffuse large B-cell lymphoma (DLBCL)
Immune checkpoint inhibitors in lymphoma. Catherine Hildyard Haematology Senior Registrar Oxford University Hospitals NHS Foundation Trust
 Immune checkpoint inhibitors in lymphoma Catherine Hildyard Haematology Senior Registrar Oxford University Hospitals NHS Foundation Trust Aims How immune checkpoint inhibitors work Success of immune checkpoint
Immune checkpoint inhibitors in lymphoma Catherine Hildyard Haematology Senior Registrar Oxford University Hospitals NHS Foundation Trust Aims How immune checkpoint inhibitors work Success of immune checkpoint
New Agents Beyond Brentuximab vedotin for Hodgkin Lymphoma. Stephen M. Ansell, MD, PhD Professor of Medicine Mayo Clinic
 New Agents Beyond Brentuximab vedotin for Hodgkin Lymphoma Stephen M. Ansell, MD, PhD Professor of Medicine Mayo Clinic Disclosures for Stephen Ansell, MD, PhD In compliance with ACCME policy, Mayo Clinic
New Agents Beyond Brentuximab vedotin for Hodgkin Lymphoma Stephen M. Ansell, MD, PhD Professor of Medicine Mayo Clinic Disclosures for Stephen Ansell, MD, PhD In compliance with ACCME policy, Mayo Clinic
CAR T CELL IMMUNOTHERAPY FOR ALL. Stephan Grupp, MD, PhD
 CAR T CELL IMMUNOTHERAPY FOR ALL Stephan Grupp, MD, PhD Disclosures Research and/or clinical trial support from Novartis, Servier, Vertex and Kite Study steering committees, consulting, or scientific advisory
CAR T CELL IMMUNOTHERAPY FOR ALL Stephan Grupp, MD, PhD Disclosures Research and/or clinical trial support from Novartis, Servier, Vertex and Kite Study steering committees, consulting, or scientific advisory
Kamakshi V Rao, PharmD, BCOP, FASHP University of North Carolina Medical Center UPDATE IN REFRACTORY HODGKIN LYMPHOMA
 Kamakshi V Rao, PharmD, BCOP, FASHP University of North Carolina Medical Center UPDATE IN REFRACTORY HODGKIN LYMPHOMA Objectives Describe the current standard approach for patients with relapsed/refractory
Kamakshi V Rao, PharmD, BCOP, FASHP University of North Carolina Medical Center UPDATE IN REFRACTORY HODGKIN LYMPHOMA Objectives Describe the current standard approach for patients with relapsed/refractory
Bcl-2 inhibition in NHL. Jonathan W. Friedberg M.D., M.M.Sc.
 Bcl-2 inhibition in NHL Jonathan W. Friedberg M.D., M.M.Sc. BCL-2, BH3 and apoptosis: Rational therapeutic targets in NHL Antiapoptotic proteins, prevent activation of Bax and Bak, thus inhibiting apoptosis.
Bcl-2 inhibition in NHL Jonathan W. Friedberg M.D., M.M.Sc. BCL-2, BH3 and apoptosis: Rational therapeutic targets in NHL Antiapoptotic proteins, prevent activation of Bax and Bak, thus inhibiting apoptosis.
Relapsed/Refractory Hodgkin Lymphoma
 Relapsed/Refractory Hodgkin Lymphoma Anas Younes, MD Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center New York, New York, United States Case Study 32-year-old woman was diagnosed with stage
Relapsed/Refractory Hodgkin Lymphoma Anas Younes, MD Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center New York, New York, United States Case Study 32-year-old woman was diagnosed with stage
Bendamustine for Hodgkin lymphoma. Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service
 Bendamustine for Hodgkin lymphoma Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service Bendamustine in Hodgkin lymphoma Bifunctional molecule Nitrogen mustard component (meclorethamine)
Bendamustine for Hodgkin lymphoma Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service Bendamustine in Hodgkin lymphoma Bifunctional molecule Nitrogen mustard component (meclorethamine)
Update: New Treatment Modalities
 ASH 2008 Update: New Treatment Modalities ASH 2008: Update on new treatment modalities GA101 Improves tumour growth inhibition in mice and exhibits a promising safety profile in patients with CD20+ malignant
ASH 2008 Update: New Treatment Modalities ASH 2008: Update on new treatment modalities GA101 Improves tumour growth inhibition in mice and exhibits a promising safety profile in patients with CD20+ malignant
Aggressive lymphomas ASH Dr. A. Van Hoof A.Z. St.Jan, Brugge-Oostende AV
 Aggressive lymphomas ASH 2015 Dr. A. Van Hoof A.Z. St.Jan, Brugge-Oostende AV CHOP 1992 2002 R-CHOP For DLBCL High dose chemo With PBSCT Aggressive lymphomas 1.DLBCL 2.Primary Mediastinal Lymphoma 3.CNS
Aggressive lymphomas ASH 2015 Dr. A. Van Hoof A.Z. St.Jan, Brugge-Oostende AV CHOP 1992 2002 R-CHOP For DLBCL High dose chemo With PBSCT Aggressive lymphomas 1.DLBCL 2.Primary Mediastinal Lymphoma 3.CNS
OSCO/OU ASH-SABC Review. Lymphoma Update. Mohamad Cherry, MD
 OSCO/OU ASH-SABC Review Lymphoma Update Mohamad Cherry, MD Outline Diffuse Large B Cell Lymphoma Double Hit Lymphoma Follicular and Indolent B Cell Lymphomas Mantle Cell Lymphoma T Cell Lymphoma Hodgkin
OSCO/OU ASH-SABC Review Lymphoma Update Mohamad Cherry, MD Outline Diffuse Large B Cell Lymphoma Double Hit Lymphoma Follicular and Indolent B Cell Lymphomas Mantle Cell Lymphoma T Cell Lymphoma Hodgkin
New Evidence reports on presentations given at EHA/ICML Bendamustine in the Treatment of Lymphoproliferative Disorders
 New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic
 Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Immune checkpoint inhibitors in Hodgkin and non-hodgkin Lymphoma: How do they work? Where will we use them? Stephen M. Ansell, MD, PhD Mayo Clinic Conflicts of Interest Research Funding from Bristol Myers
Targeted Radioimmunotherapy for Lymphoma
 Targeted Radioimmunotherapy for Lymphoma John Pagel, MD, PhD Fred Hutchinson Cancer Center Erik Mittra, MD, PhD Stanford Medical Center Brought to you by: Financial Disclosures Disclosures Erik Mittra,
Targeted Radioimmunotherapy for Lymphoma John Pagel, MD, PhD Fred Hutchinson Cancer Center Erik Mittra, MD, PhD Stanford Medical Center Brought to you by: Financial Disclosures Disclosures Erik Mittra,
What are the hurdles to using cell of origin in classification to treat DLBCL?
 What are the hurdles to using cell of origin in classification to treat DLBCL? John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical
What are the hurdles to using cell of origin in classification to treat DLBCL? John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical
VENETOCLAX (ABT 199) Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth
 Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth") VENETOCLAX (ABT 199) Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth ABT-199 Venetoclax ABT-199 is a selective, potent, orally
VENETOCLAX (ABT 199) Simon Rule Professor of Clinical Haematology Consultant Haematologist Derriford Hospital and Peninsula Medical School Plymouth ABT-199 Venetoclax ABT-199 is a selective, potent, orally
Firenze, settembre 2017 Novità dall EHA LINFOMI Umberto Vitolo
 Firenze, 22-23 settembre 2017 Novità dall EHA LINFOMI Umberto Vitolo Hematology University Hospital Città della Salute e della Scienza Torino, Italy Disclosures Umberto Vitolo Research Support/P.I. Employee
Firenze, 22-23 settembre 2017 Novità dall EHA LINFOMI Umberto Vitolo Hematology University Hospital Città della Salute e della Scienza Torino, Italy Disclosures Umberto Vitolo Research Support/P.I. Employee
What is the best approach to the initial therapy of PTCL? standards of treatment? Should all
 What is the best approach to the initial therapy of PTCL? standards of treatment? hould all Jia Ruan, M.D., Ph.D. Center for Lymphoma and Myeloma Weill Cornell Medical College New York Presbyterian Hospital
What is the best approach to the initial therapy of PTCL? standards of treatment? hould all Jia Ruan, M.D., Ph.D. Center for Lymphoma and Myeloma Weill Cornell Medical College New York Presbyterian Hospital
Checkpoint Blockade in Hematology and Stem Cell Transplantation
 Checkpoint Blockade in Hematology and Stem Cell Transplantation Saad S. Kenderian, MD Assistant Professor of Medicine and Oncology Mayo Clinic College of Medicine October 14, 2016 2015 MFMER slide-1 Disclosures
Checkpoint Blockade in Hematology and Stem Cell Transplantation Saad S. Kenderian, MD Assistant Professor of Medicine and Oncology Mayo Clinic College of Medicine October 14, 2016 2015 MFMER slide-1 Disclosures
PCI-32765DBL1002. Janssen Research & Development, Raritan, NJ, USA; 9 Janssen Research & Development, Belgrade, Serbia; 10
 Phase 1b Study Combining Ibrutinib With Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone (R-CHOP) in Patients With CD20-Positive B-Cell Non-Hodgkin Lymphoma (NHL) Anas Younes, 1 Ian
Phase 1b Study Combining Ibrutinib With Rituximab, Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone (R-CHOP) in Patients With CD20-Positive B-Cell Non-Hodgkin Lymphoma (NHL) Anas Younes, 1 Ian
Highlights in chronic lymphocytic leukemia
 Congress Highlights CLL Highlights in chronic lymphocytic leukemia A. Janssens, MD, PhD 1 As new data on indolent non-hodgkin lymphoma (inhl) were not that compelling, only highlights on chronic lymphocytic
Congress Highlights CLL Highlights in chronic lymphocytic leukemia A. Janssens, MD, PhD 1 As new data on indolent non-hodgkin lymphoma (inhl) were not that compelling, only highlights on chronic lymphocytic
CAR T-Cell Therapy for Acute Lymphoblastic Leukemia: Identifying Appropriate Patients and Maximizing Outcomes. Shannon L.
 CAR T-Cell Therapy for Acute Lymphoblastic Leukemia: Identifying Appropriate Patients and Maximizing Outcomes Shannon L. Maude, MD, PhD CTL019 cell Lentiviral vector Anti-CD19 CAR construct CD19 Native
CAR T-Cell Therapy for Acute Lymphoblastic Leukemia: Identifying Appropriate Patients and Maximizing Outcomes Shannon L. Maude, MD, PhD CTL019 cell Lentiviral vector Anti-CD19 CAR construct CD19 Native
Rituximab in the Treatment of NHL:
 New Evidence reports on presentations given at ASH 2010 Rituximab in the Treatment of NHL: Rituximab versus Watch and Wait in Asymptomatic FL, R-Maintenance Therapy in FL with Standard or Rapid Infusion,
New Evidence reports on presentations given at ASH 2010 Rituximab in the Treatment of NHL: Rituximab versus Watch and Wait in Asymptomatic FL, R-Maintenance Therapy in FL with Standard or Rapid Infusion,
Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies. Eric H. Rubin, MD Merck Research Laboratories
 Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies Eric H. Rubin, MD Merck Research Laboratories Outline Pembrolizumab P001 study - example of multiple expansion
Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies Eric H. Rubin, MD Merck Research Laboratories Outline Pembrolizumab P001 study - example of multiple expansion
RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA
 RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA Pier Luigi Zinzani Institute of Hematology and Medical Oncology L. e A. Seràgnoli University of Bologna, Italy Slovenia, October 5 2007 Zevalin
RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA Pier Luigi Zinzani Institute of Hematology and Medical Oncology L. e A. Seràgnoli University of Bologna, Italy Slovenia, October 5 2007 Zevalin
Pembrolizumab in Relapsed/Refractory Classical Hodgkin Lymphoma: Phase 2 KEYNOTE-087 Study
 Pembrolizumab in Relapsed/Refractory Classical Hodgkin Lymphoma: Phase 2 KEYNOTE-087 Study Craig H. Moskowitz, 1 Pier Luigi Zinzani, 2 Michelle A. Fanale, 3 Philippe Armand, 4 Nathalie Johnson, 5 John
Pembrolizumab in Relapsed/Refractory Classical Hodgkin Lymphoma: Phase 2 KEYNOTE-087 Study Craig H. Moskowitz, 1 Pier Luigi Zinzani, 2 Michelle A. Fanale, 3 Philippe Armand, 4 Nathalie Johnson, 5 John
Duvelisib (IPI-145), a PI3K-δ,γ Inhibitor, is Clinically Active in Patients with Relapsed/ Refractory Chronic Lymphocytic Leukemia
, a PI3K-δ,γ Inhibitor, is Clinically Active in Patients with Relapsed/ Refractory Chronic Lymphocytic Leukemia") Duvelisib (IPI-145), a PI3K-δ,γ Inhibitor, is Clinically Active in Patients with Relapsed/ Refractory Chronic Lymphocytic Leukemia Susan M. O Brien 1, Manish R. Patel 2,3, Brad Kahl 4, Steven Horwitz 5,
Duvelisib (IPI-145), a PI3K-δ,γ Inhibitor, is Clinically Active in Patients with Relapsed/ Refractory Chronic Lymphocytic Leukemia Susan M. O Brien 1, Manish R. Patel 2,3, Brad Kahl 4, Steven Horwitz 5,
Summary of Key AML Abstracts Presented at the European Hematology Association (EHA) June 22-25, 2017 Madrid, Spain
 June 22-25, 2017 Madrid, Spain") Summary of Key AML Abstracts Presented at the European Hematology Association (EHA) June 22-25, 2017 Madrid, Spain EHA 2017 ANNUAL MEETING: ABSTRACT SEARCH PAGE: https://learningcenter.ehaweb.org/eha/#!*listing=3*browseby=2*sortby=1*media=3*ce_id=1181*label=15531
Summary of Key AML Abstracts Presented at the European Hematology Association (EHA) June 22-25, 2017 Madrid, Spain EHA 2017 ANNUAL MEETING: ABSTRACT SEARCH PAGE: https://learningcenter.ehaweb.org/eha/#!*listing=3*browseby=2*sortby=1*media=3*ce_id=1181*label=15531
Treating for Cure or Palliation: Difficult Decisions for Older Adults with Lymphoma
 Treating Frail Adults With Common Malignancies: Best Evidence to Personalize Therapy Treating for Cure or Palliation: Difficult Decisions for Older Adults with Lymphoma Raul Cordoba, MD, PhD Lymphoma Unit
Treating Frail Adults With Common Malignancies: Best Evidence to Personalize Therapy Treating for Cure or Palliation: Difficult Decisions for Older Adults with Lymphoma Raul Cordoba, MD, PhD Lymphoma Unit
CARE at ASH 2014 Lymphoma. Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre
 CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
BR is an established treatment regimen for CLL in the front-line and R/R settings
 Idelalisib plus bendamustine and rituximab (BR) is superior to BR alone in patients with relapsed/refractory CLL: Results of a phase III randomized double-blind placebo-controlled study Andrew D. Zelenetz,
Idelalisib plus bendamustine and rituximab (BR) is superior to BR alone in patients with relapsed/refractory CLL: Results of a phase III randomized double-blind placebo-controlled study Andrew D. Zelenetz,
Jonathan W Friedberg, MD, MMSc
 I N T E R V I E W Jonathan W Friedberg, MD, MMSc Dr Friedberg is Professor of Medicine and Oncology and Chief of the Hematology/Oncology Division at the University of Rochester s James P Wilmot Cancer
I N T E R V I E W Jonathan W Friedberg, MD, MMSc Dr Friedberg is Professor of Medicine and Oncology and Chief of the Hematology/Oncology Division at the University of Rochester s James P Wilmot Cancer
Exploiting the Immune System: Chimeric Antigen Receptor-T Cell Therapy for Hematologic Malignancies
 Exploiting the Immune System: Chimeric Antigen Receptor-T Cell Therapy for Hematologic Malignancies Maurice Alexander, PharmD, BCOP, CPP Clinical Specialist, Blood and Marrow Transplant UNC Bone Marrow
Exploiting the Immune System: Chimeric Antigen Receptor-T Cell Therapy for Hematologic Malignancies Maurice Alexander, PharmD, BCOP, CPP Clinical Specialist, Blood and Marrow Transplant UNC Bone Marrow
eastern cooperative oncology group Michael Williams, Fangxin Hong, Brad Kahl, Randy Gascoyne, Lynne Wagner, John Krauss, Sandra Horning
 Results of E4402 (RESORT): A Randomized Phase III Study Comparing Two Different Rituximab Dosing Strategies for Low Tumor Burden Indolent B-Cell Lymphoma Michael Williams, Fangxin Hong, Brad Kahl, Randy
Results of E4402 (RESORT): A Randomized Phase III Study Comparing Two Different Rituximab Dosing Strategies for Low Tumor Burden Indolent B-Cell Lymphoma Michael Williams, Fangxin Hong, Brad Kahl, Randy
What is the best second-line approach to induce remission prior to stem cell transplant? Single agent brentuximab vedotin
 What is the best second-line approach to induce remission prior to stem cell transplant? Single agent brentuximab vedotin Alison Moskowitz, MD Assistant Attending, Lymphoma Service Memorial Sloan Kettering
What is the best second-line approach to induce remission prior to stem cell transplant? Single agent brentuximab vedotin Alison Moskowitz, MD Assistant Attending, Lymphoma Service Memorial Sloan Kettering
Phase I Study of Carfilzomib and Panobinostat for Patients with Relapsed and Refractory Myeloma: A Multicenter MMRC Clinical Trial
 Phase I Study of Carfilzomib and Panobinostat for Patients with Relapsed and Refractory Myeloma: A Multicenter MMRC Clinical Trial Jonathan L. Kaufman, Todd Zimmerman, Cara A. Rosenbaum, Anuj Mahindra,
Phase I Study of Carfilzomib and Panobinostat for Patients with Relapsed and Refractory Myeloma: A Multicenter MMRC Clinical Trial Jonathan L. Kaufman, Todd Zimmerman, Cara A. Rosenbaum, Anuj Mahindra,
International Conference on Malignant Lymphoma (ICML) June 14-17, 2017
 June 14-17, 2017") International Conference on Malignant Lymphoma (ICML) June 14-17, 2017 INTERIM REPORT FROM A PHASE 2 MULTICENTER STUDY OF TAZEMETOSTAT, AN EZH2 INHIBITOR: CLINICAL ACTIVITY AND FAVORABLE SAFETY IN PATIENTS
International Conference on Malignant Lymphoma (ICML) June 14-17, 2017 INTERIM REPORT FROM A PHASE 2 MULTICENTER STUDY OF TAZEMETOSTAT, AN EZH2 INHIBITOR: CLINICAL ACTIVITY AND FAVORABLE SAFETY IN PATIENTS
Update: Chronic Lymphocytic Leukemia
 ASH 2008 Update: Chronic Lymphocytic Leukemia Improving Patient Response to Treatment with the Addition of Rituximab to Fludarabine-Cyclophosphamide ASH 2008: Update on chronic lymphocytic leukemia CLL-8
ASH 2008 Update: Chronic Lymphocytic Leukemia Improving Patient Response to Treatment with the Addition of Rituximab to Fludarabine-Cyclophosphamide ASH 2008: Update on chronic lymphocytic leukemia CLL-8
Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge. ASH 2012 Atlanta
 Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge ASH 2012 Atlanta DLBCL How to improve on R-CHOP What at relapse Mantle cell lymphoma Do we cure patients Treatment at relapse Follicular lymphoma Watch and
Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge ASH 2012 Atlanta DLBCL How to improve on R-CHOP What at relapse Mantle cell lymphoma Do we cure patients Treatment at relapse Follicular lymphoma Watch and
Management of high-risk diffuse large B cell lymphoma: case presentation
 Management of high-risk diffuse large B cell lymphoma: case presentation Daniel J. Landsburg, MD Assistant Professor of Clinical Medicine Perelman School of Medicine University of Pennsylvania January
Management of high-risk diffuse large B cell lymphoma: case presentation Daniel J. Landsburg, MD Assistant Professor of Clinical Medicine Perelman School of Medicine University of Pennsylvania January
Chimeric Antigen Receptor T Cells in Refractory B-Cell Lymphomas
 The new england journal of medicine Original Article Chimeric Antigen Receptor T Cells in Refractory B-Cell Lymphomas Stephen J. Schuster, M.D., Jakub Svoboda, M.D., Elise A. Chong, M.D., Sunita D. Nasta,
The new england journal of medicine Original Article Chimeric Antigen Receptor T Cells in Refractory B-Cell Lymphomas Stephen J. Schuster, M.D., Jakub Svoboda, M.D., Elise A. Chong, M.D., Sunita D. Nasta,
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma
 with classical Hodgkin lymphoma") PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
[ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014
![[ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014](/thumbs/73/68853651.jpg "[ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014") [ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014 Forward-Looking Statements These slides and the accompanying oral presentation contain forward-looking statements. Actual events or results may
[ NASDAQ: MEIP ] Analyst & Investor Event December 8, 2014 Forward-Looking Statements These slides and the accompanying oral presentation contain forward-looking statements. Actual events or results may
NASDAQ: TGTX. 33 rd Annual JP Morgan Healthcare Conference
 NASDAQ: TGTX 33 rd Annual JP Morgan Healthcare Conference January 2015 Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private Securities
NASDAQ: TGTX 33 rd Annual JP Morgan Healthcare Conference January 2015 Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private Securities
Safety and Efficacy of Venetoclax Plus Low-Dose Cytarabine in Treatment-Naïve Patients Aged 65 Years With Acute Myeloid Leukemia
 Safety and Efficacy of Venetoclax Plus Low-Dose Cytarabine in Treatment-Naïve Patients Aged 65 Years With Acute Myeloid Leukemia Abstract 102 Wei AH, Strickland SA, Roboz GJ, Hou J-Z, Fiedler W, Lin TL,
Safety and Efficacy of Venetoclax Plus Low-Dose Cytarabine in Treatment-Naïve Patients Aged 65 Years With Acute Myeloid Leukemia Abstract 102 Wei AH, Strickland SA, Roboz GJ, Hou J-Z, Fiedler W, Lin TL,
NASDAQ: TGTX Jefferies Healthcare Conference June 2015
 NASDAQ: TGTX Jefferies Healthcare Conference June 2015 Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private Securities Litigation
NASDAQ: TGTX Jefferies Healthcare Conference June 2015 Forward Looking Safe Harbor Statement This presentation contains forward-looking statements within the meaning of the Private Securities Litigation
Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma
 The new england journal of medicine Original Article Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma S.S. Neelapu, F.L. Locke, N.L. Bartlett, L.J. Lekakis, D.B. Miklos, C.A.
The new england journal of medicine Original Article Axicabtagene Ciloleucel CAR T-Cell Therapy in Refractory Large B-Cell Lymphoma S.S. Neelapu, F.L. Locke, N.L. Bartlett, L.J. Lekakis, D.B. Miklos, C.A.
Supplementary Appendix to manuscript submitted by Trappe, R.U. et al:
 Supplementary Appendix to manuscript submitted by Trappe, R.U. et al: Response to rituximab induction is a predictive marker in B-cell post-transplant lymphoproliferative disorder and allows successful
Supplementary Appendix to manuscript submitted by Trappe, R.U. et al: Response to rituximab induction is a predictive marker in B-cell post-transplant lymphoproliferative disorder and allows successful
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Schuster SJ, Svoboda J, Chong EA, et al. Chimeric antigen receptor
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Schuster SJ, Svoboda J, Chong EA, et al. Chimeric antigen receptor
2012 by American Society of Hematology
 2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
2012 by American Society of Hematology Common Types of HIV-Associated Lymphomas DLBCL includes primary CNS lymphoma (PCNSL) Burkitt Lymphoma HIV-positive patients have a 60-200 fold increased incidence
ASH POSTER: LYMRIT UPDATE
 ASH POSTER: LYMRIT 37-01 UPDATE DECEMBER 2018 EDUARDO BRAVO, CEO LISA ROJKJAER, MD, CMO Nordic Nanovector ASA Kjelsåsveien 168 B, 0884 Oslo, Norway www.nordicnanovector.com IR contact: ir@nordicnanovector.com
ASH POSTER: LYMRIT 37-01 UPDATE DECEMBER 2018 EDUARDO BRAVO, CEO LISA ROJKJAER, MD, CMO Nordic Nanovector ASA Kjelsåsveien 168 B, 0884 Oslo, Norway www.nordicnanovector.com IR contact: ir@nordicnanovector.com
Standard of care for patients with newly diagnosed multiple myeloma who are not eligible for a transplant
 Standard of care for patients with newly diagnosed multiple myeloma who are not eligible for a transplant Pr Philippe Moreau University Hospital, Nantes, France MP: Standard of care until 2007 J Clin Oncol
Standard of care for patients with newly diagnosed multiple myeloma who are not eligible for a transplant Pr Philippe Moreau University Hospital, Nantes, France MP: Standard of care until 2007 J Clin Oncol
FOLLICULAR LYMPHOMA: US vs. Europe: different approach on first relapse setting?
 Indolent Lymphoma Workshop Bologna, Royal Hotel Carlton May 2017 FOLLICULAR LYMPHOMA: US vs. Europe: different approach on first relapse setting? Armando López-Guillermo Department of Hematology, Hospital
Indolent Lymphoma Workshop Bologna, Royal Hotel Carlton May 2017 FOLLICULAR LYMPHOMA: US vs. Europe: different approach on first relapse setting? Armando López-Guillermo Department of Hematology, Hospital
Multiple Myeloma Updates 2007
 Multiple Myeloma Updates 2007 Brian Berryman, M.D. Multiple Myeloma Updates 2007 Goals for today: Understand the staging systems for myeloma Understand prognostic factors in myeloma Review updates from
Multiple Myeloma Updates 2007 Brian Berryman, M.D. Multiple Myeloma Updates 2007 Goals for today: Understand the staging systems for myeloma Understand prognostic factors in myeloma Review updates from
The case for maintenance rituximab in FL
 New-York, October 23 rd 2015 The case for maintenance rituximab in FL Pr. Gilles SALLES For FL patients, progression-free survival still needs to be improved Median R-CHVP-I 66 months P
New-York, October 23 rd 2015 The case for maintenance rituximab in FL Pr. Gilles SALLES For FL patients, progression-free survival still needs to be improved Median R-CHVP-I 66 months P
Clinical Study Synopsis
 Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
Clinical Study Synopsis This Clinical Study Synopsis is provided for patients and healthcare professionals to increase the transparency of Bayer's clinical research. This document is not intended to replace
Diffuse Large B-Cell Lymphoma (DLBCL)
") Diffuse Large B-Cell Lymphoma (DLBCL) DLBCL/MCL Dr. Anthea Peters, MD, FRCPC University of Alberta/Cross Cancer Institute Disclosures Honoraria from Janssen, Abbvie, Roche, Lundbeck, Seattle Genetics Objectives
Diffuse Large B-Cell Lymphoma (DLBCL) DLBCL/MCL Dr. Anthea Peters, MD, FRCPC University of Alberta/Cross Cancer Institute Disclosures Honoraria from Janssen, Abbvie, Roche, Lundbeck, Seattle Genetics Objectives
Updates in the Treatment of Non-Hodgkin Lymphoma: ASH Topics
 Updates in the Treatment of Non-Hodgkin Lymphoma: ASH 2008 Joseph Tuscano, M.D. UC Davis Cancer Center 1 Topics Mantle Cell Lymphoma What is the standard of care for younger patients? (abstracts 581, 769,
Updates in the Treatment of Non-Hodgkin Lymphoma: ASH 2008 Joseph Tuscano, M.D. UC Davis Cancer Center 1 Topics Mantle Cell Lymphoma What is the standard of care for younger patients? (abstracts 581, 769,
Immunocellular Therapies for Relapsed/ Refractory Heme Malignancies: A Focus on CAR T-Cell Therapy
 Immunocellular Therapies for Relapsed/ Refractory Heme Malignancies: A Focus on CAR T-Cell Therapy This transcript has been edited for style and clarity and includes all slides from the presentation. This
Immunocellular Therapies for Relapsed/ Refractory Heme Malignancies: A Focus on CAR T-Cell Therapy This transcript has been edited for style and clarity and includes all slides from the presentation. This
Chemotherapy-based approaches are the optimal second-line therapy prior to stem cell transplant in relapsed HL
 Lymphoma & Myeloma 2015 Chemotherapy-based approaches are the optimal second-line therapy prior to stem cell transplant in relapsed HL Jeremy S. Abramson, MD Relevant Disclosure Consulting for Seattle
Lymphoma & Myeloma 2015 Chemotherapy-based approaches are the optimal second-line therapy prior to stem cell transplant in relapsed HL Jeremy S. Abramson, MD Relevant Disclosure Consulting for Seattle
Presented at the 60th Annual ASH Meeting and Exposition December 1 4, 2018 San Diego, CA
 Phase I/II Study of Umbralisib (TGR-1202) in Combination with Ublituximab (TG-1101) and Pembrolizumab in Patients with Relapsed/ CLL and Richter s Transformation Anthony R. Mato, MD MSCE 1, Jakub Svoboda,
Phase I/II Study of Umbralisib (TGR-1202) in Combination with Ublituximab (TG-1101) and Pembrolizumab in Patients with Relapsed/ CLL and Richter s Transformation Anthony R. Mato, MD MSCE 1, Jakub Svoboda,
Myeloma update ASH 2014
 Myeloma update ASH 2014 Updates in Newly Diagnosed Multiple Myeloma FIRST: effect of age on lenalidomide/dexamethasone vs MPT in transplantation-ineligible pts Phase III: MPT-T vs MPR-R in transplantation-ineligible
Myeloma update ASH 2014 Updates in Newly Diagnosed Multiple Myeloma FIRST: effect of age on lenalidomide/dexamethasone vs MPT in transplantation-ineligible pts Phase III: MPT-T vs MPR-R in transplantation-ineligible
POST ICML Indolent lymphomas relapse treatment
 POST ICML Indolent lymphomas relapse treatment Georg Hess University Medical School Johannes Gutenberg-University Mainz, Germany Treatment of relapsed indolent lymphoma 2 General categories of second line
POST ICML Indolent lymphomas relapse treatment Georg Hess University Medical School Johannes Gutenberg-University Mainz, Germany Treatment of relapsed indolent lymphoma 2 General categories of second line
Background CPX-351. Lancet J, et al. J Clin Oncol. 2017;35(suppl): Abstract 7035.
: Abstract 7035.") Overall Survival (OS) With Versus in Older Adults With Newly Diagnosed, Therapy-Related Acute Myeloid Leukemia (taml): Subgroup Analysis of a Phase 3 Study Abstract 7035 Lancet JE, Rizzieri D, Schiller
Overall Survival (OS) With Versus in Older Adults With Newly Diagnosed, Therapy-Related Acute Myeloid Leukemia (taml): Subgroup Analysis of a Phase 3 Study Abstract 7035 Lancet JE, Rizzieri D, Schiller
Enasidenib Monotherapy is Effective and Well-Tolerated in Patients with Previously Untreated Mutant-IDH2 Acute Myeloid Leukemia
 Enasidenib Monotherapy is Effective and Well-Tolerated in Patients with Previously Untreated Mutant-IDH2 Acute Myeloid Leukemia Pollyea DA 1, Tallman MS 2,3, de Botton S 4,5, DiNardo CD 6, Kantarjian HM
Enasidenib Monotherapy is Effective and Well-Tolerated in Patients with Previously Untreated Mutant-IDH2 Acute Myeloid Leukemia Pollyea DA 1, Tallman MS 2,3, de Botton S 4,5, DiNardo CD 6, Kantarjian HM
Il trattamento del Linfoma Follicolare in prima linea
 Il trattamento del Linfoma Follicolare in prima linea Dr.ssa Carola Boccomini SC Ematologia Dr. U. Vitolo AO Città della Salute e della Scienza Torino, Italy Median follow-up 3 years Median follow-up 6
Il trattamento del Linfoma Follicolare in prima linea Dr.ssa Carola Boccomini SC Ematologia Dr. U. Vitolo AO Città della Salute e della Scienza Torino, Italy Median follow-up 3 years Median follow-up 6
Highlights in Aggressive Non-Hodgkin Lymphoma From the 2017 American Society of Clinical Oncology Annual Meeting
 August 2017 Volume 15, Issue 8, Supplement 8 A SPECIAL MEETING REVIEW EDITION Highlights in Aggressive Non-Hodgkin Lymphoma From the 2017 American Society of Clinical Oncology Annual Meeting A Review of
August 2017 Volume 15, Issue 8, Supplement 8 A SPECIAL MEETING REVIEW EDITION Highlights in Aggressive Non-Hodgkin Lymphoma From the 2017 American Society of Clinical Oncology Annual Meeting A Review of
ANCO: ASCO Highlights 2018 Hematologic Malignancies
 ANCO: ASCO Highlights 2018 Hematologic Malignancies Brian A. Jonas, M.D., Ph.D. UC Davis Comprehensive Cancer Center August 25, 2018 Brian Jonas, MD, PhD ANCO: ASCO Highlights 2018 Relevant financial relationships
ANCO: ASCO Highlights 2018 Hematologic Malignancies Brian A. Jonas, M.D., Ph.D. UC Davis Comprehensive Cancer Center August 25, 2018 Brian Jonas, MD, PhD ANCO: ASCO Highlights 2018 Relevant financial relationships
Tolerability and activity of chemo-free triplet combination of umbralisib (TGR-1202), ublituximab, and ibrutinib in patients with advanced CLL and NHL
, ublituximab, and ibrutinib in patients with advanced CLL and NHL") Tolerability and activity of chemo-free triplet combination of umbralisib (TGR-1202), ublituximab, and ibrutinib in patients with advanced and NHL Loretta Nastoupil, MD 1, Matthew A. Lunning, DO 2, Julie
Tolerability and activity of chemo-free triplet combination of umbralisib (TGR-1202), ublituximab, and ibrutinib in patients with advanced and NHL Loretta Nastoupil, MD 1, Matthew A. Lunning, DO 2, Julie
Highlights of ICML 2015
 Highlights of ICML 2015 Jonathan W. Friedberg M.D. Director, James P. Wilmot Cancer Center Statistics, ICML 2015: a global meeting Almost 3700 participants. 90 countries represented. Attendees: USA 465
Highlights of ICML 2015 Jonathan W. Friedberg M.D. Director, James P. Wilmot Cancer Center Statistics, ICML 2015: a global meeting Almost 3700 participants. 90 countries represented. Attendees: USA 465
Aggressive B and T cell lymphomas: Treatment paradigms in 2018
 Aggressive B and T cell lymphomas: Treatment paradigms in 2018 John P. Leonard M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical Research Associate
Aggressive B and T cell lymphomas: Treatment paradigms in 2018 John P. Leonard M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical Research Associate
CAR-T CELLS: NEW HOPE FOR CANCER PATIENTS
 CAR-T CELLS: NEW HOPE FOR CANCER PATIENTS Natasha Kekre, MD, MPH, FRCPC Hematologist, Blood and Marrow Transplant Program, TOH Associate Scientist, Ottawa Hospital Research Institute Assistant Professor
CAR-T CELLS: NEW HOPE FOR CANCER PATIENTS Natasha Kekre, MD, MPH, FRCPC Hematologist, Blood and Marrow Transplant Program, TOH Associate Scientist, Ottawa Hospital Research Institute Assistant Professor
The treatment of DLBCL. Michele Ghielmini Medical Oncology Dept Oncology Institute of Southern Switzerland Bellinzona
 The treatment of DLBCL Michele Ghielmini Medical Oncology Dept Oncology Institute of Southern Switzerland Bellinzona NHL frequency at the IOSI Mantle Cell Lymphoma 6.5 % Diffuse Large B-cell Lymphoma 37%
The treatment of DLBCL Michele Ghielmini Medical Oncology Dept Oncology Institute of Southern Switzerland Bellinzona NHL frequency at the IOSI Mantle Cell Lymphoma 6.5 % Diffuse Large B-cell Lymphoma 37%
Managing patients with relapsed follicular lymphoma. Case
 Managing patients with relapsed follicular lymphoma John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Professor of Medicine Associate Director, Weill Cornell
Managing patients with relapsed follicular lymphoma John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Professor of Medicine Associate Director, Weill Cornell
LYSA PET adapted programs. O. Casasnovas Hematology department Hopital Le Bocage, CHU Dijon, France
 LYSA PET adapted programs O. Casasnovas Hematology department Hopital Le Bocage, CHU Dijon, France 3 phase III trials DLBCL LNH 09-1B: aaipi = 0, 18 80y : ongoing GAINED: aaipi = 1-3, 18 60y : ongoing
LYSA PET adapted programs O. Casasnovas Hematology department Hopital Le Bocage, CHU Dijon, France 3 phase III trials DLBCL LNH 09-1B: aaipi = 0, 18 80y : ongoing GAINED: aaipi = 1-3, 18 60y : ongoing
Sponsor / Company: Sanofi Drug substance(s): SAR (iniparib)
: SAR (iniparib)") These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
Disclosures WOJCIECH JURCZAK
 Disclosures WOJCIECH JURCZAK ABBVIE (RESEARCH FUNDING), CELGENE (RESEARCH FUNDING); EISAI (RESEARCH FUNDING); GILEAD (RESEARCH FUNDING); JANSEN (RESEARCH FUNDING); MORPHOSYS (RESEARCH FUNDING), MUNDIPHARMA
Disclosures WOJCIECH JURCZAK ABBVIE (RESEARCH FUNDING), CELGENE (RESEARCH FUNDING); EISAI (RESEARCH FUNDING); GILEAD (RESEARCH FUNDING); JANSEN (RESEARCH FUNDING); MORPHOSYS (RESEARCH FUNDING), MUNDIPHARMA
H. Lee Moffitt Cancer Center and Research Institute, University of California, San Francisco & Tisch Cancer Institute, Mount Sinai School of Medicine
 Pomalidomide, Cyclophosphamide, and Dexamethasone Is Superior to Pomalidomide and Dexamethasone in Relapsed and Refractory Myeloma: Results of a Multicenter Randomized Phase II Study Rachid Baz, Thomas
Pomalidomide, Cyclophosphamide, and Dexamethasone Is Superior to Pomalidomide and Dexamethasone in Relapsed and Refractory Myeloma: Results of a Multicenter Randomized Phase II Study Rachid Baz, Thomas
DYNAMO: A PHASE 2 STUDY DEMONSTRATING THE CLINICAL ACTIVITY OF DUVELISIB IN PATIENTS WITH DOUBLE-REFRACTORY INDOLENT NON-HODGKIN LYMPHOMA
 DYNAMO: A PHASE 2 STUDY DEMONSTRATING THE CLINICAL ACTIVITY OF DUVELISIB IN PATIENTS WITH DOUBLE-REFRACTORY INDOLENT NON-HODGKIN LYMPHOMA Presented at 14-ICML, 14 June 2017, Lugano Switzerland Authors
DYNAMO: A PHASE 2 STUDY DEMONSTRATING THE CLINICAL ACTIVITY OF DUVELISIB IN PATIENTS WITH DOUBLE-REFRACTORY INDOLENT NON-HODGKIN LYMPHOMA Presented at 14-ICML, 14 June 2017, Lugano Switzerland Authors
ENASIDENIB IN MUTANT-IDH2 RELAPSED OR REFRACTORY ACUTE MYELOID LEUKEMIA (R/R AML): RESULTS OF A PHASE 1 DOSE- ESCALATION AND EXPANSION STUDY
: RESULTS OF A PHASE 1 DOSE- ESCALATION AND EXPANSION STUDY") ENASIDENIB IN MUTANT-IDH2 RELAPSED OR REFRACTORY ACUTE MYELOID LEUKEMIA (R/R AML): RESULTS OF A PHASE 1 DOSE- ESCALATION AND EXPANSION STUDY Eytan M. Stein, Courtney D. DiNardo, Daniel A. Pollyea, Amir
ENASIDENIB IN MUTANT-IDH2 RELAPSED OR REFRACTORY ACUTE MYELOID LEUKEMIA (R/R AML): RESULTS OF A PHASE 1 DOSE- ESCALATION AND EXPANSION STUDY Eytan M. Stein, Courtney D. DiNardo, Daniel A. Pollyea, Amir
Development of Mogamulizumab, a defucosylated anti-ccr4 humanized monoclonal antibody
 New Drugs in Hematology Development of Mogamulizumab, a defucosylated anti-ccr4 humanized monoclonal antibody Michinori Ogura, MD, PhD Department of Hematology Tokai Central Hospital Bologna, Royal Hotel
New Drugs in Hematology Development of Mogamulizumab, a defucosylated anti-ccr4 humanized monoclonal antibody Michinori Ogura, MD, PhD Department of Hematology Tokai Central Hospital Bologna, Royal Hotel