Endocrine Therapy for Advanced Breast Cancer (ABC) Dr Yoon-Sim YAP Division of Medical Oncology, National Cancer Centre Singapore
|
|
|
- Gloria Hart
- 6 years ago
- Views:
Transcription



1 Endocrine Therapy for Advanced Breast Cancer (ABC) Dr Yoon-Sim YAP Division of Medical Oncology, National Cancer Centre Singapore
2 Outline Guidelines and Evolving Clinical Treatment Landscape for HR+ HER2- advanced breast cancer (ABC) Optimising endocrine therapy backbone Improving outcomes further with targeted therapy Sequencing of Treatments First Line setting vs Second-line setting & beyond Predictive Biomarkers Other Novel Therapeutic Strategies Conclusions 2
3 Treatment guidelines for HR+, HER2 advanced breast cancer ESMO 1 ABC 2 ASCO 3 NCCN 4 In HR +, HER2 disease, endocrine therapy is the treatment of first choice independent of metastatic site, unless rapid response is needed. Limited visceral metastases are not a contraindication for endocrine therapy Endocrine therapy is the preferred option for HR + disease, even in the presence of visceral disease, unless there is concern or proof of endocrine resistance or rapidly progressive disease needing a fast response Endocrine therapy should be recommended as initial treatment for patients with HR+ metastatic breast cancer except in patients with immediately life-threatening disease or in those with rapid visceral recurrence on adjuvant endocrine therapy. Endocrine therapy recommended unless there is visceral crisis, or progression with no clinical benefit after 3 sequential endocrine therapy regimens. 1. Cardoso F et al. Ann Oncol 2012;23(Suppl 7):vii11-vii19 2. Cardoso F et al. Ann Oncol 2014;25(10): ASCO Available at 4. NCCN V Available at 3
4 Chemotherapy versus Endocrine Therapy Chemotherapy has higher response rate. Wilcken et al, Cochrane System Database Review
5 Chemotherapy versus Endocrine Therapy No significant differences in overall survival. Wilcken et al, Cochrane System Database Review
6 What are the Endocrine Therapy Options? What is the evidence for doing what we do? (ie if people are practising evidence-based medicine) 6
7 Endocrine Therapy Combination Therapy Breakthroughs in hormone receptor positive (HR+) breast cancer FDA approvals of new treatments 1977 Tamoxifen 1996 Goserelin 1997 Letrozole 1999 Exemestane 2012 Everolimus + Exemestane 2002 Fulvestrant 2015 Palbociclib + Letrozole 2016 Palbociclib + Fulvestrant Megestrol Acetate 1995 Anastrozole 2017 Ribociclib (with AI) 2017 Abemaciclib (single agent or with fulvestrant)


8 ASCO Guidelines Postmenopausal Premenopausal Rugo et al, JCO

9 Courtesy of Ian Smith from ESMO 2014
10

11 Mechanism of Action of Tamoxifen and Aromatase Inhibitors Johnston, Nature Reviews Cancer 2003
12 First-line Comparative Tamoxifen Trials in Advanced Breast Cancer (2004) Tamoxifen versus N=17 Progestogens 6 Estrogens 1 Androgens 1 Anti-Estrogens 2 Aminogluthetimide 3 Formestane 1 Fadrozole 2 Fulvestrant 1 Tamoxifen always better or at least as good. Schiavon and Smith, Haematol Oncol Clin North AM
13 Rationale for OS + Tamoxifen in Premenopausal MBC Randomised study: n=161 (original target 348) Combined treatment with buserelin and tamoxifen was superior to treatment with buserelin or tamoxifen alone by objective response rate (48%, 34%, and 28% of patients who could be evaluated,respectively; P =.11 [x2 test]), median progression-free survival (9.7 months, 6.3 months, and 5.6 months; P =.03), and overall survival (3.7 years, 2.5 years, and 2.9 years; P =.01). 5-year survival were 34.2% (95% confidence interval [CI] = 20.4% 48.0%), 14.9% (95% CI =3.9% 25.9%), and 18.4% (95% CI = 7.0% 29.8%), respectively. Klijn et al, JNCI

14 Use of 2 nd line AIs v megesterol acetate AIs: RR, TTP and overall survival only slightly better than megestrol acetate Smith NEJM 2003
15 Progestins Mechanism of action unclear. May inhibit aromatase activity or increase estrogen turnover, since estrogen levels fall during therapy. May also act through the glucocorticoid receptor, androgen receptor, or progesterone receptor. Activity appears to be maintained in patients who are refractory to SAIs. Side-effects: weight gain, fluid retention, thromboembolic complications, PV bleeding. Willemse, EJC 1990; Abrams, JCO 1999
16 What is the optimal 1 st -line endocrine therapy? PFS / TTP of AIs as 1 st -line endocrine therapy trials in HR+ MBC Trial AI (response rate, %) Tamoxifen (response rate, %) AI (PFS, mths) Tamoxifen (PFS, mths) Hazard Ratio Nabholtz et al, 2000 (n=353) Anastrozole vs tamoxifen Bonneterre et al, 2001 (n=668) Anastrozole vs tamoxifen Mouridsen et al, 2001 (n=907) Letrozole vs tamoxifen Paridaens et al, 2008 (n=371) Exemestane vs tamoxifen Range Meta-analysis: compared to tamoxifen, there was a statistically significant survival benefit (11 percent relative hazard reduction, 95% CI 1 to 19 percent) for first-line third generation SAIs, but not for aminoglutethimide or second generation SAIs. Mauri et al, JNCI 2006 Johnston, SABCS


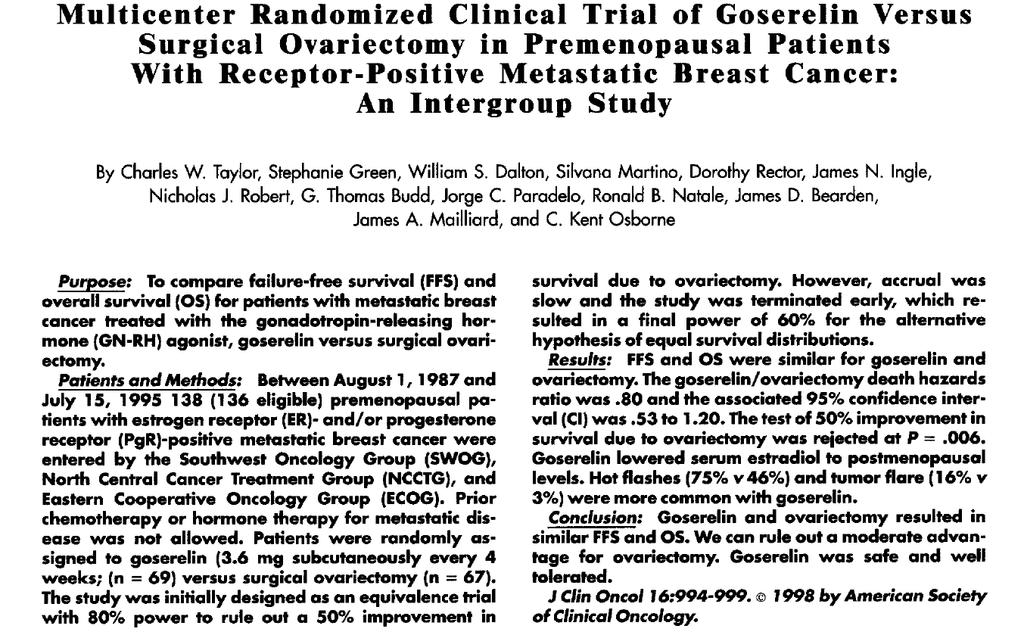
17 AI + Ovarian Suppression in Premenopausal Is it better than tamoxifen + ovarian suppression?? No randomised trials with tamoxifen and OS for comparison in metastatic setting. 17
18 What are the endocrine options after AI? How good is tamoxifen after an AI? TAMRAD (Tamoxifen vs Tamoxifen + Everolimus after AI) (Bachelot et al, JCO 2012) Tamoxifen arm (26% received 1 line of palliative chemo): 6mth clinical benefit rate 42%; TTP 4.5 mths; response rate 13% How good is exemestane (monotx) after an AI? EFECT (Chia, JCO 2008): median TTP 3.7mths; response rate 6.7% SOFEA (Johnston, Lancet Oncol 2013): median PFS 3.4mths; response rate 2.8% BOLERO-2 (Baselga, NEJM 2012): median PFS 2.8mths, response rate 0.4%. How good are progestins after an AI? No prospective data How good is fulvestrant after an AI? See following. 18
19 Mode of Action of Estradiol, Tamoxifen and Fulvestrant Estradiol E Tamoxifen T Fulvestrant + ER E AF1 + E + AF1 AF1 + ER F ER F F AF1 Receptor dimerisation No dimerisation T AF1 T AF1 AF2 AF2 ACTIVE AF1 ACTIVE AF2 INACTIVE AF1 + AF2 INACTIVE ACCELERATED RECEPTOR DEGRADATION FULLY ACTIVATED TRANSCRIPTION (tumour cell division) PARTIALLY INACTIVATED TRANSCRIPTION (reduced rate of tumour cell division) NO TRANSCRIPTION (no tumour cell division) Adapted from: Wakeling AE. Endocr-Relat Cancer 2000; 7:
20 Fulvestrant: Preclinical Activity Osborne et al, JNCI 1995 Osborne et al, Cancer Chemo and Pharm
21 Clinical Trials on Fulvestrant (250mg LD) Pretreated Pretreated Howell, JCO 2002 Osborne, JCO 2002 Treatment-naive Only just as good as tamoxifen or anastrozole Howell, JCO
22 Clinical Trials on Fulvestrant (250mg LD) Chia, JCO Only just as good as exemestane even after relapse/progresson on non-steroidal AI Caveat: 250mg dose was suboptimal Johnston, Lancet Oncol 2013
23 CONFIRM phase III Trial: Fulvestrant 250mg vs 500mg Median OS 26.4mths vs 22.3mths Di Leo et al, JNCI 2014
24 Clinical Trials on Fulvestrant (500mg HD) Primary Endpoint: CBR fulvestrant HD vs anastrozole 72.5% v 67.0% (odds ratio, 1.30; 95% CI, 0.72 to 2.38; P.386). Robertson et al, JCO 2009 Caveat: OS not preplanned analysis; not all patients participated in OS followup. 24 Ellis et al, JCO 2015
25 FALCON: Phase III 1 st line study of Fulvestrant 500 vs AI in Endocrine Therapy Naïve MBC / LABC N=450 ER +ve, HER2 negative Locally advanced (not suitable for surgery) or metastatic disease Up to 1 line of chemotherapy At least 1 lesion that can be assessed Fulvestrant 500mg i.m. Anastrozole 1mg OD Note no prior endocrine therapy allowed Primary endpoint: PFS Secondary endpoint: OS Other secondary endpoints include ORR, CBR, duration of response, duration of clinical benefit, time to deterioration of HRQoL, Safety Ellis et al, LBA14 ESMO 2016
26 Proportion of patients alive and progression free FALCON: Fulvestrant 500 vs anastrozole in 1 st -line endocrine therapy naïve ER+ MBC Proportion of patients alive and progression-free Proportion of patients alive and progression-free Number of patients at risk: Fulvestrant Anastrozole Primary endpoint: PFS HR (95% CI 0.637, 0.999) p= Median PFS Fulvestrant: 16.6 months Anastrozole: 13.8 months Time (months) Fulvestrant (n=230) Anastrozole (n=232) HR 0.59 (95% CI 0.42, 0.84) Median PFS Fulvestrant: 22.3 months Anastrozole: 13.8 months PFS without visceral disease Fulvestrant (n=95) Anastrozole (n=113) HR 0.99 (95% CI 0.74, 1.33) Median PFS Fulvestrant: 13.8 months Anastrozole: 15.9 months Time (months) PFS with visceral disease Time (months) Fulvestrant (n=135) Anastrozole (n=119) Ellis et al, LBA14 ESMO 2016; Robertson et al, Lancet 2016
27 What is the optimal 1 st -line endocrine therapy? PFS / TTP of AIs as 1 st -line endocrine therapy trials in HR+ MBC Trial Nabholtz et al Anastrozole vs tamoxifen Bonneterre et al Anastrozole vs tamoxifen Mouridsen et al Letrozole vs tamoxifen Chernozemsky et al Exemestane vs tamoxifen Paridaens et al Exemestane vs tamoxifen Mehta et al Anastrozole vs anastrozole + fulvestrant 250mg Bergh et al Anastrozole vs anastrozole + fulvestrant 250mg Ellis et al Anastrozole vs Fulvestrant 500mg Date AI (months) Tamoxifen (months) AI + fulvestrant 250mg (months) Fulvestrant 500mg (months) Hazard Ratio Is Fulvestrant the gold standard for 1 st -line treatment now? PFS benefit modest PFS benefit restricted to patients without visceral mets Only applies to endocrine naïve patients? Activity of other endocrine therapies post-fulvestrant unclear Await overall survival data.. Other more effective alternative options available now Range

28 ESR1 Mutations 28 Toy et al, Nature Genetics 2013
29 New generation SERDs (Selective Estrogen Receptor Degraders - oral) Limitations of fulvestrant Poor bioavailability Requires oil-based IM formulation; limitations with increasing dose intensity Variable ER down-regulation Van Kruchten et al, 2015 SERD Company Current status GDC-0810 Genentech Phase I/II GDC-0927 Genentech Phase I RAD1901 Radius Phase I AZD9496 Astra Zeneca Phase I LSZ-102 Novartis Phase I SAR Sanofi Phase I H3b-6545 (SERCA) H3 BioMedicine Phase I FDA Breakthrough Drug Designation



 while on adjuvant ET")



30 Definitions of Endocrine Resistance in ER+ MBC PRIMARY ENDOCRINE RESISTANCE Relapse while on the first 2 years of adjuvant ET, or PD within first 6 months of 1 st line ET for MBC, while on ET SECONDARY (ACQUIRED) ENDOCRINE RESISTANCE Relapse while on adjuvant ET but after the first 2 years, or relapse within 12 months of completing adjuvant ET, or PD 6 months after initiating ET for MBC, while on ET Courtesy of Johnston, SABCS 2016; Cardoso, Annals Onc 2014
31 What can we add to endocrine therapy to overcome endocrine resistance? First-line setting CDK4/6 Inhibitor (Trials using Temsirolimus, Bevacizumab, EGFR Inhibitors negative or mixed results.) Second-line and beyond CDK4/6 Inhibitor vs mtor Inhibitor? PI3K inhibitor 31
32 Cyclin Dependent Kinase(CDK) 4/6 Inhibitors Lange and Yee, Endocrine Related Cancer 2011 Ma, ASCO

33 CDK4/6 Inhibitors O Leary et al, Nat Rev Clin Onc 2016
34 PALOMA-2 & MONALEESA-2: Design of Phase III Studies PALOMA-2 MONALEESA-2 Postmenopausal ER+ HER2 advanced breast cancer with no prior treatment for advanced disease. AI-resistant patients excluded N=666 R A N D O M I S E (2:1) Palbociclib (125 mg QD, 3/1 schedule) + letrozole (2.5 mg QD) Placebo + letrozole (2.5 mg QD) Postmenopausal women with HR+/HER2 advanced breast cancer with no prior therapy for advanced disease N=668 R A N D O M I S E (1:1) Ribociclib (600 mg QD, 3/1 schedule) + letrozole (2.5 mg QD) Placebo + letrozole (2.5 mg QD) Stratified by the presence/absence of liver and/or lung metastases Primary endpoint: PFS Secondary endpoints: Response, OS, safety, biomarkers, PROs Primary endpoint: PFS Secondary endpoints: OS (key), ORR, CBR, safety Courtesy of Johnston, SABCS 2016
 Ribociclib letrozole: ribociclib letrozole: NR NR Placebo letrozole: placebo letrozole: 14.7 14.7 Finn R, et al. NEJM.")
35 PALOMA-2 & MONALEESA-2: PFS PALOMA-2 MONALEESA-2 mpfs (months) Palbociclib letrozole: 24.8 Placebo letrozole: 14.5 mpfs mpfs (months) Ribociclib letrozole: ribociclib letrozole: NR NR Placebo letrozole: placebo letrozole: Finn R, et al. NEJM. 2016;375(20): Hortobagyi G, et al. NEJM. 2016;375(18):
 p<0.001 100 90 Ribociclib + letrozole Placebo + letrozole p=0.02 80 70 60 OR (95% CI): 1.55 (1.05 2.28) p=0.03 84.3 70.8 80 70 60 p=0.00028 80.1 71.8 50 40 30 55.3 44.")
36 Rate (%) Rate (%) PALOMA-2 & MONALEESA-2: Secondary endpoints PALOMA-2 Measurable disease MONALEESA-2 Measurable disease Palbociclib + letrozole Placebo + letrozole OR (95% CI): 2.23 ( ) p< Ribociclib + letrozole Placebo + letrozole p= OR (95% CI): 1.55 ( ) p= p= Objective response rate Clinical benefit rate 0 Objective response rate Clinical benefit rate Finn R, et al. NEJM. 2016;375(20): Finn R, et al. Abstract 507, ASCO 2016 Hortobagyi G, et al. NEJM. 2016;375(18): Hortobagyi G, et al. LBA01, ESMO 2016

:1738 1748 Other potential AEs:")
37 PALOMA-2 & MONALEESA-2: Toxicity PALOMA-2 MONALEESA-2 Finn R, et al. NEJM. 2016;375(20): Hortobagyi G, et al. NEJM. 2016;375(18): Other potential AEs: Transaminitis, prolonged QT
; 5 (2-11). 1-2 chemotherapy regimens in metastatic setting.")
38 MONARCH-1: Abemaciclib (Inhibitor of CDK4>CDK6) Phase 2 single-agent trial in metastatic HR+HER2- mbc. No. of prior systemic regimens (any setting); 5 (2-11). 1-2 chemotherapy regimens in metastatic setting. 38 Dickler et al, ASCO 2016; CCR 2017
39 MONARCH-3 Goetz et al, JCO

40 MONARCH-3 Goetz et al, JCO
41 CDK 4/6 inhibitors for ER+ MBC New Gold Standard in 1 st -line treatment Adjuvant trials have also commenced. Unanswered Questions Does every patient need CDK4/6 inhibitor upfront?

42 Potential Predictors of CDK4/6 Inhibitor Activity In sensitive cell lines: Cyclin D1 (CCND1) Retinoblastoma (Rb) p16 PALOMA-1 ER+HER2- Unselected ER+HER2- Plus Amplification of CCND1 and/or Loss of p16 Finn RS, et al. Br Ca Research 2009 Finn RS, et al. Lancet Oncol 2015

43 Predictive Biomarkers? PALOMA-2: No subgroup of ER+ patients was found that did not benefit from the addition of palbociclib to letrozole. 43 Finn RS, et al. ESMO Abstract LBA15 [oral].

 advanced breast cancer (ABC): efficacy by baseline")
44 Predictive Biomarkers? Ribociclib + letrozole for first-line treatment of hormone receptor-positive (HR+), HER2- negative (HER2 ) advanced breast cancer (ABC): efficacy by baseline tumor markers 44 Andre et al, AACR 2017
45 Subgroup Analyses MONALEESA-2 PALOMA-2 Hortobagyi et al, NEJM 2016 Finn et al, NEJM

46 MONARCH-3 Patients with bone-only disease Patients without bone-only disease Goetz et al, JCO
47 Not all patients reach the next line of ABC therapy After failure of first-line therapy, a proportion of patients cannot undergo second line therapy due to rapid disease progression In general, response to further lines of therapy is worse About one third of patients stop their treatment with each new line of therapy These results are concordant with large retrospective cohort studies Study 2 nd line 3 rd line 4 th line 5 th line Dufresne et al % 56% 25% 11% Tacca et al % 68% 43% 23% Bernardo et al % 82% 36% 11% Planchat et al % 76% 56% 37% Current study; Jackisch et al ,6 100% 70% 46% 27% 1. Dufresne A et al. Breast Cancer Res Treat 2008;107: Tacca O et al. Cancer Invest 2009;27: Bernardo G et al. Cancer Res 2010;70(Suppl 24):446s,P Planchat E et al. Breast 2011;20: Jackisch C et al. BMC Cancer 2014;14: Jackisch et al. P , SABCS 2016 Courtesy of Harbeck, ESMO Asia
48 Considerations in choosing 1 st -line therapy in ER+ MBC Tumour Biology ER & PR levels Luminal Subtype / Proliferation Clinical Features Prior Endocrine Rx / DFI / Pace of Disease Visceral vs non-visceral mets / Symptoms / Tumor Burden Patient Factors Age / Co-morbidities / Geographical Logistics Patient Preference / Availability of Rx / Quality of Life Partly adapted from Johnston, SABCS 2016
49 CDK 4/6 inhibitors for ER+ MBC New Gold Standard in 1 st -line treatment Adjuvant trials have also commenced. Unanswered Questions Does every patient need CDK4/6 inhibitor upfront? Will there be improvement in Overall Survival?
 Finn et al, ASCO")
50 PALOMA-1 OS data (not powered) Finn et al, ASCO
51 MONALEESA-2 Update (OS data still immature) Hortobagyi et al, ASCO
52 CDK 4/6 inhibitors for ER+ MBC New Gold Standard in 1 st -line treatment. Adjuvant trials have also commenced. Unanswered Questions Does every patient need CDK4/6 inhibitor upfront? Will there be improvement in Overall Survival? What is the optimal treatment after CDK4/6 Inhibition? What is the optimal sequence of treatment?
53 Second-Line and Beyond BOLERO-2 & PALOMA-3: Design of Phase III studies BOLERO-2 PALOMA-3 Postmenopausal women with estrogen receptor positive locally advanced or metastatic breast cancer who are refractory to letrozole or anastrozole R A N D O M I S E (2:1) Everolimus 10 mg daily + exemestane 25 mg daily (n=485) Placebo + exemestane 25 mg daily (n=239) HR+, HER2- ABC Pre/peri or postmenopausal Progressed on prior ET on or within 12 months of adjuvant therapy and/or on therapy for advanced breast cancer 1 or more prior chemotherapy regimen for advanced cancer R A N D O M I S E (2:1) Palbociclib (125 mg QD; 3 weeks on, 1 week off) + fulvestrant (500 mg IM Q4W) (n=347) Placebo (3 weeks on, 1 week off) + fulvestrant (500 mg IM Q4W) (n=174) Primary endpoint: PFS Secondary endpoints: OS, ORR, Safety, QoL, CBR Primary endpoint: PFS Secondary endpoints: OS, OR, CBR, Safety, QoL
54 BOLERO-2 & PALOMA-3: PFS BOLERO-2 PALOMA-3 Baselga J, et al. N Engl J Med 2012;366:520-9 Turner N, et al. N Engl J Med 2015;373:209-19
55 MONARCH-2 55 Patients were required to have disease that progressed while receiving neoadjuvant or adjuvant ET, # 12 months after adjuvant ET, or while receiving ET for ABC. Patients must not have received more than one ET or any prior chemotherapy for ABC. Sledge et al, ASCO 2017; JCO 2017
56 BOLERO-2: Overall Survival Results Why? Not statistically powered to detect 4.4mth OS benefit. Imbalance in poststudy salvage chemo use? Higher rate of discontinuation of EVE due to AE: 26% vs 5% Paradoxical activation of AKT via negative feedback loop? Need predictive biomarkers? 56 Piccart et al, Ann Onc 2014

57 BOLERO-2 Correlative Genomic Analysis Progression-free survival benefit with everolimus was maintained regardless of alteration status of PIK3CA, FGFR1, and CCND1 or the pathways of which they are components. However, mtor somatic mutations may be associated with greater benefit from mtor inhibition. Somatic FGFR mutations associated with poor prognosis. High chromosomal instability associated with less everolimus benefit and worst outcome. Hortobagyi et al, JCO

58 PI3K/AKT/mTOR Pathway 58 Rodon et al, Nature Reviews Clin Onc 2013
59 PI3K Inhibitors still promising? Efficacy limited in unselected patients. Significant toxicities with Pan-PI3K Inhibitors. FERGI (n=168): fulvestrant + pictilisib vs fulvestrant + placebo: negative BELLE2 (n=1147): fulvestrant + buparlisib vs fulvestrant + placebo: positive but not clinically significant; benefit mainly with PIK3CA mutated (cdna) BELLE3 (n=432)(post-mtor inhibitor): fulvestrant + buparlisib vs fulvestrant + placebo: positive but not clinically significant; ; benefit mainly with PIK3CA mutated (tumour or cdna) Alpha-specific PI3K Inhibitors Better tolerated? Ongoing phase 3 trials Taselisib + fulvestrant vs placebo + fulvestrant (SANDPIPER) Alpelisib + fulvestrant vs placebo + fulvestrant (SOLAR) Potential activity after progression on CDK4/6 Inhibitors? 59

60 Other Novel Therapeutics HDAC Inhibitors? Immunotherapy? Etc etc Novel SERD Epigenetic Modulators? Immunotherapy, Bone-modifying agents RTK Inhibitor Still a role for chemotherapy Endocrine Resistance Inhibitors of MDM2?BCL2? Inhibitors of PI3K/MEK pathway CDK Inhibitor Inhibitors of NOTCH?WNT? Ma et al, Nature Rev Ca 2015

61 Pink Ribbon Walk, October 2016 Thank you for your attention! 61
Endocrine Therapy 2017: Is There a Better Single Agent and when Should we Use it?
 Endocrine Therapy 2017: Is There a Better Single Agent and when Should we Use it? ET1 ET2 ET3 Targeted agent 1 Targeted agent 2 Hope S. Rugo, MD Director, Breast Oncology and Clinical Trials Education
Endocrine Therapy 2017: Is There a Better Single Agent and when Should we Use it? ET1 ET2 ET3 Targeted agent 1 Targeted agent 2 Hope S. Rugo, MD Director, Breast Oncology and Clinical Trials Education
When is Chemotherapy indicated in Advanced Luminal Breast Cancer?
 When is Chemotherapy indicated in Advanced Luminal Breast Cancer? Soo-Chin Lee Head & Senior Consultant Department of Haematology-Oncology Clinical Care National University Cancer Institute, Singapore
When is Chemotherapy indicated in Advanced Luminal Breast Cancer? Soo-Chin Lee Head & Senior Consultant Department of Haematology-Oncology Clinical Care National University Cancer Institute, Singapore
What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland
 What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland Outline Early breast cancer Advanced breast cancer Open questions Outline Early breast cancer
What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland Outline Early breast cancer Advanced breast cancer Open questions Outline Early breast cancer
Metastatic breast cancer: sequence of therapies
 Metastatic breast cancer: sequence of therapies Clinical Case Discussion Nadia Harbeck, MD PhD Breast Center, Department of Gynecology and Obstetrics University of Munich, Ludwig-Maximilians University
Metastatic breast cancer: sequence of therapies Clinical Case Discussion Nadia Harbeck, MD PhD Breast Center, Department of Gynecology and Obstetrics University of Munich, Ludwig-Maximilians University
Multimedia Appendix 6 Educational Materials Table of Contents. Intervention Educational Materials Audio Script (version 1)
") Multimedia Appendix 6 Educational Materials Table of Contents Intervention Educational Materials... 1 Audio Script (version 1)... 1 Text (version 1)... 5 Slides (version 1)... 17 Audio Script (version
Multimedia Appendix 6 Educational Materials Table of Contents Intervention Educational Materials... 1 Audio Script (version 1)... 1 Text (version 1)... 5 Slides (version 1)... 17 Audio Script (version
Management of hormone-receptor positive human epidermal receptor 2 negative advanced or metastatic breast cancers
 Review Article Page 1 of 10 Management of hormone-receptor positive human epidermal receptor 2 negative advanced or metastatic breast cancers Roger K. C. Ngan Department of Clinical Oncology, Queen Elizabeth
Review Article Page 1 of 10 Management of hormone-receptor positive human epidermal receptor 2 negative advanced or metastatic breast cancers Roger K. C. Ngan Department of Clinical Oncology, Queen Elizabeth
Mechanisms of hormone drug resistance
 Mechanisms of hormone drug resistance Ljiljana Stamatović Institute for Oncology and Radiology of Serbia Tenth UMOS Conference, Belgrade, 16-17 th May 2015. Hormone receptor-positive breast cancer (HR+
Mechanisms of hormone drug resistance Ljiljana Stamatović Institute for Oncology and Radiology of Serbia Tenth UMOS Conference, Belgrade, 16-17 th May 2015. Hormone receptor-positive breast cancer (HR+
Inibitori delle chinasi ciclino dipendenti nel trattamento della malattia metastatica HR-positiva Gli studi clinici
 Inibitori delle chinasi ciclino dipendenti nel trattamento della malattia metastatica HR-positiva Gli studi clinici Laura Orlando UOC Oncologia & Breast Unit Brindisi Verona 22/04/2016 Summary Studi con
Inibitori delle chinasi ciclino dipendenti nel trattamento della malattia metastatica HR-positiva Gli studi clinici Laura Orlando UOC Oncologia & Breast Unit Brindisi Verona 22/04/2016 Summary Studi con
Overcoming resistance to endocrine or HER2-directed therapy
 Overcoming resistance to endocrine or HER2-directed therapy Jane Lowe Meisel, MD Assistant Professor of Hematology and Medical Oncology Winship Cancer Institute at Emory University 1 Background While most
Overcoming resistance to endocrine or HER2-directed therapy Jane Lowe Meisel, MD Assistant Professor of Hematology and Medical Oncology Winship Cancer Institute at Emory University 1 Background While most
Targeting CDK 4/6. Jee Hyun Kim, M.D., Ph.D. Seoul National University College of Medicine
 2016.04.30 GBCC Education Symposium Targeting CDK 4/6 Jee Hyun Kim, M.D., Ph.D. Seoul National University College of Medicine Contents Cyclins -CDKs in cell cycle control CDK 4/6 in breast cancer Preclinical
2016.04.30 GBCC Education Symposium Targeting CDK 4/6 Jee Hyun Kim, M.D., Ph.D. Seoul National University College of Medicine Contents Cyclins -CDKs in cell cycle control CDK 4/6 in breast cancer Preclinical
Enhancing Endocrine Therapy for Hormone Receptor Positive Advanced Breast Cancer
 Enhancing Endocrine Therapy for Hormone Receptor Positive Advanced Breast Cancer Sung-Bae Kim, MD, PhD Professor, Dept of Oncology, Asan Medical Center University of Ulsan College of Medicine Seoul, Korea
Enhancing Endocrine Therapy for Hormone Receptor Positive Advanced Breast Cancer Sung-Bae Kim, MD, PhD Professor, Dept of Oncology, Asan Medical Center University of Ulsan College of Medicine Seoul, Korea
RIBOCICLIB EN PRIMERA LINEA DE TRATAMIENTO. Dra. Elena Aguirre H.U. Miguel Servet
 RIBOCICLIB EN PRIMERA LINEA DE TRATAMIENTO Dra. Elena Aguirre H.U. Miguel Servet INTRODUCTION ADVANCED BREAST CANCER HR+/HER2- YES Consider Chemo VISCERAL CRISIS? NO Endocrine Therapy X3 Toxicity Progresive
RIBOCICLIB EN PRIMERA LINEA DE TRATAMIENTO Dra. Elena Aguirre H.U. Miguel Servet INTRODUCTION ADVANCED BREAST CANCER HR+/HER2- YES Consider Chemo VISCERAL CRISIS? NO Endocrine Therapy X3 Toxicity Progresive
Pro: Hormone Therapy in HR positive MBC is the preferred option!
 Pro: Hormone Therapy in HR positive MBC is the preferred option! Alexandru Eniu, MD, PhD Medical Oncologist Head, Day Hospital Unit Department of Breast Tumors Cancer Institute Ion Chiricuţă Cluj-Napoca,
Pro: Hormone Therapy in HR positive MBC is the preferred option! Alexandru Eniu, MD, PhD Medical Oncologist Head, Day Hospital Unit Department of Breast Tumors Cancer Institute Ion Chiricuţă Cluj-Napoca,
Introduction. Ahmad Radzi 1*, Fabian Wei Luen Lee 2 REVIEW ARTICLE
 doi: 10.18282/amor.v4.i1.255 REVIEW ARTICLE Optimizing treatment-sequencing strategies for the management of postmenopausal women with hormone receptor-positive, HER2-negative advanced breast cancer: A
doi: 10.18282/amor.v4.i1.255 REVIEW ARTICLE Optimizing treatment-sequencing strategies for the management of postmenopausal women with hormone receptor-positive, HER2-negative advanced breast cancer: A
Aggiornamenti tra ricerca e clinica: il carcinoma della mammella
 Aggiornamenti tra ricerca e clinica: il carcinoma della mammella Filippo Montemurro Unit of (INCO) Fondazione del Piemonte per l Oncologia Candiolo Cancer Institute (IRCCs) Research Needs in Breast Cancer
Aggiornamenti tra ricerca e clinica: il carcinoma della mammella Filippo Montemurro Unit of (INCO) Fondazione del Piemonte per l Oncologia Candiolo Cancer Institute (IRCCs) Research Needs in Breast Cancer
Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology, Emory University, Chief of
 Endocrine Therapy of Advanced Breast Cancer School of Breast Oncology November 9 th 2013 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology,
Endocrine Therapy of Advanced Breast Cancer School of Breast Oncology November 9 th 2013 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology,
Outline of the presentation
 Outline of the presentation Breast cancer subtypes and classification Clinical need in estrogen-positive (ER+) metastatic breast cancer (mbc) Sulforaphane and SFX-01: the preclinical evidence STEM Phase
Outline of the presentation Breast cancer subtypes and classification Clinical need in estrogen-positive (ER+) metastatic breast cancer (mbc) Sulforaphane and SFX-01: the preclinical evidence STEM Phase
PI3K/AKT/mTOR Inhibitors in Breast Cancer
 PI3K/AKT/mTOR Inhibitors in Breast Cancer Dr Yoon-Sim YAP Division of Medical Oncology, National Cancer Centre Singapore Global Breast Cancer Conference 2015 Outline Overview of PI3K/Akt/mTOR Pathway Rationale
PI3K/AKT/mTOR Inhibitors in Breast Cancer Dr Yoon-Sim YAP Division of Medical Oncology, National Cancer Centre Singapore Global Breast Cancer Conference 2015 Outline Overview of PI3K/Akt/mTOR Pathway Rationale
Metastatic Breast Cancer What is new? Subtypes and variation?
 Metastatic Breast Cancer What is new? Subtypes and variation? Anne Blaes, MD, MS University of Minnesota, Division of Hematology/Oncology Director, Adult Cancer Survivor Program Current estimates for metastatic
Metastatic Breast Cancer What is new? Subtypes and variation? Anne Blaes, MD, MS University of Minnesota, Division of Hematology/Oncology Director, Adult Cancer Survivor Program Current estimates for metastatic
Mechanisms of Resistance to. Lisa A. Carey, M.D. University of North Carolina at Chapel Hill Lineberger Comprehensive Cancer Center
 Mechanisms of Resistance to Hormonal Therapy Lisa A. Carey, M.D. University of North Carolina at Chapel Hill Lineberger Comprehensive Cancer Center Antagonizing Estrogen Dependent Growth Premenopausal
Mechanisms of Resistance to Hormonal Therapy Lisa A. Carey, M.D. University of North Carolina at Chapel Hill Lineberger Comprehensive Cancer Center Antagonizing Estrogen Dependent Growth Premenopausal
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings. Eve Rodler, MD University of California at Davis October 2016
 Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
Optimizing therapy selection in ER[+] HER2[-] Advanced Breast Cancer
![Optimizing therapy selection in ER[+] HER2[-] Advanced Breast Cancer](/thumbs/77/76517551.jpg "Optimizing therapy selection in ER[+] HER2[-] Advanced Breast Cancer") Optimizing therapy selection in ER[+] HER2[-] Advanced Breast Cancer Dr Antonio Llombart-Cussac, MD, PhD Medical Oncology Division Hospital Arnau Vilanova, Valencia, Spain Disclaimer The contents herein
Optimizing therapy selection in ER[+] HER2[-] Advanced Breast Cancer Dr Antonio Llombart-Cussac, MD, PhD Medical Oncology Division Hospital Arnau Vilanova, Valencia, Spain Disclaimer The contents herein
Predicting outcome in metastatic breast cancer
 Predicting outcome in metastatic breast cancer Aleix Prat, MD, PhD Medical Oncology Department Translational Genomics and Targeted Therapeutics in Solid Tumors Monday, 15 th January, Manchester, UK Disclosures
Predicting outcome in metastatic breast cancer Aleix Prat, MD, PhD Medical Oncology Department Translational Genomics and Targeted Therapeutics in Solid Tumors Monday, 15 th January, Manchester, UK Disclosures
Current Optimal Sequence and Duration of Endocrine Treatment
 [Symposium 7] Present and Future of Endocrine Therapy 07 Apr, 2018@GBCC Current Optimal Sequence and Duration of Endocrine Treatment Breast Oncology Center The Cancer Institute Hospital of JFCR Shinji
[Symposium 7] Present and Future of Endocrine Therapy 07 Apr, 2018@GBCC Current Optimal Sequence and Duration of Endocrine Treatment Breast Oncology Center The Cancer Institute Hospital of JFCR Shinji
Update mbc. endokrine Therapie
 Update mbc endokrine Therapie HR neg ER pos Endokrine Resistenz Endokrine Therapie 1 st line Postmenopause AI/Tam/Fulvestrant 84% AI+ Fulvestrant 33% AI (Tam) + Everolimus 84% AI + CDK4/6 92% Prämenopause
Update mbc endokrine Therapie HR neg ER pos Endokrine Resistenz Endokrine Therapie 1 st line Postmenopause AI/Tam/Fulvestrant 84% AI+ Fulvestrant 33% AI (Tam) + Everolimus 84% AI + CDK4/6 92% Prämenopause
Cancers du Sein Métastatiques
 Cancers du Sein Métastatiques Véronique Diéras Journée Laurence Leroyer Rennes 18 mai 2018 Plan ESME Inhibiteurs CDK 4/6 RH+ Inhibiteurs PARP Anticorps drogue-conjugués Perspectives 2018-2019 ESME Time
Cancers du Sein Métastatiques Véronique Diéras Journée Laurence Leroyer Rennes 18 mai 2018 Plan ESME Inhibiteurs CDK 4/6 RH+ Inhibiteurs PARP Anticorps drogue-conjugués Perspectives 2018-2019 ESME Time
10/15/2012. Overcoming Endocrine Therapy Resistance. The Problem in ER+ Tumors is Endocrine Therapy Resistance
 Overcoming Endocrine Therapy Resistance Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology Slide Credits: Hope Rugo, MD The Problem in ER+ Tumors is Endocrine Therapy Resistance
Overcoming Endocrine Therapy Resistance Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology Slide Credits: Hope Rugo, MD The Problem in ER+ Tumors is Endocrine Therapy Resistance
Metastatic HR+ Breast Cancer - CDK 4/6 Inhibitors Charting the Path. Sandy Sehdev MD FRCPC
 Metastatic HR+ Breast Cancer - CDK 4/6 Inhibitors Charting the Path Sandy Sehdev MD FRCPC Objectives To understand the approach to the treatment of hormone sensitive metastatic breast cancer and the use
Metastatic HR+ Breast Cancer - CDK 4/6 Inhibitors Charting the Path Sandy Sehdev MD FRCPC Objectives To understand the approach to the treatment of hormone sensitive metastatic breast cancer and the use
Breast Cancer: ASCO Poster Review
 Breast Cancer: ASCO Poster Review Carmen Criscitiello, MD, PhD Istituto Europeo di Oncologia Milano HER2+ SUBTYPE Research questions in early HER2+ BC De-escalation of toxicity without compromising efficacy
Breast Cancer: ASCO Poster Review Carmen Criscitiello, MD, PhD Istituto Europeo di Oncologia Milano HER2+ SUBTYPE Research questions in early HER2+ BC De-escalation of toxicity without compromising efficacy
TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive metastatic breast cancer
 TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive metastatic breast cancer Marta Bonotto Department of Oncology University Hospital of Udine TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive
TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive metastatic breast cancer Marta Bonotto Department of Oncology University Hospital of Udine TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive
Page. Objectives: Hormone Therapy Resistance: Challenges and Opportunities. Research Support From Merck
 Hormone Therapy Resistance: Challenges and Opportunities Pamela. N. Munster, MD University of California, San Francisco Financial Disclosures Research Support From Merck Objectives: Understanding the current
Hormone Therapy Resistance: Challenges and Opportunities Pamela. N. Munster, MD University of California, San Francisco Financial Disclosures Research Support From Merck Objectives: Understanding the current
Endocrine treatment might NOT be the preferred option in Hrpos MBC. Dr. Mircea Dediu Sanador Hospital Bucharest Summer School Bucharest 2015
 Endocrine treatment might NOT be the preferred option in Hrpos MBC Dr. Mircea Dediu Sanador Hospital Bucharest Summer School Bucharest 2015 Overall survival not improved by the AI treatment Benefit in
Endocrine treatment might NOT be the preferred option in Hrpos MBC Dr. Mircea Dediu Sanador Hospital Bucharest Summer School Bucharest 2015 Overall survival not improved by the AI treatment Benefit in
Optimization of Hormone Treatment: New Alternative Sequences
 Optimization of Hormone Treatment: New Alternative Sequences ET1 ET2 ET3 Targeted agent 1 Targeted agent 2 Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education
Optimization of Hormone Treatment: New Alternative Sequences ET1 ET2 ET3 Targeted agent 1 Targeted agent 2 Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education
Case #2: Hormonal Therapy for Advanced Premenopausal Breast Cancer
 Case #2: Hormonal Therapy for Advanced Premenopausal Breast Cancer Fellow Presenter: Katherine Clifton, MD Faculty Discussant: Debu Tripathy, MD 7 th Annual June 1, 2018 Topics to Be Discussed: Staging
Case #2: Hormonal Therapy for Advanced Premenopausal Breast Cancer Fellow Presenter: Katherine Clifton, MD Faculty Discussant: Debu Tripathy, MD 7 th Annual June 1, 2018 Topics to Be Discussed: Staging
Endocrine Therapy of Advanced Breast Cancer School of Breast Oncology November 2012
 Endocrine Therapy of Advanced Breast Cancer School of Breast Oncology November 2012 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology,
Endocrine Therapy of Advanced Breast Cancer School of Breast Oncology November 2012 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology,
Novel Strategies in Systemic Therapies: Overcoming Endocrine Therapy Resistance
 Novel Strategies in Systemic Therapies: Overcoming Endocrine Therapy Resistance Richard S. Finn, MD Division of Hematology/ Oncology Director, Translational Oncology Laboratory Geffen School of Medicine
Novel Strategies in Systemic Therapies: Overcoming Endocrine Therapy Resistance Richard S. Finn, MD Division of Hematology/ Oncology Director, Translational Oncology Laboratory Geffen School of Medicine
First-Line Ribociclib + Letrozole for Postmenopausal Women With HR+, HER2-, Advanced Breast Cancer: First Results From the Phase III MONALEESA-2 Study
 First-Line Ribociclib + Letrozole for Postmenopausal Women With HR+, HER2-, Advanced Breast Cancer: First Results From the Phase III MONALEESA-2 Study Abstract LBA1 Hortobagyi GN, Stemmer SM, Burris HA,
First-Line Ribociclib + Letrozole for Postmenopausal Women With HR+, HER2-, Advanced Breast Cancer: First Results From the Phase III MONALEESA-2 Study Abstract LBA1 Hortobagyi GN, Stemmer SM, Burris HA,
Treatment of Metastatic Breast Cancer. Prof RCCoombes Imperial College London
 Treatment of Metastatic Breast Cancer Prof RCCoombes Imperial College London Metastatic Breast Cancer: General Guidelines Specialized oncology nurses (if possible specialized breast nurses) should be part
Treatment of Metastatic Breast Cancer Prof RCCoombes Imperial College London Metastatic Breast Cancer: General Guidelines Specialized oncology nurses (if possible specialized breast nurses) should be part
Highlitghs in MBC First and second line endocrine treatments. Antonio Frassoldati Oncologia Clinica Ferrara
 Highlitghs in MBC First and second line endocrine treatments Antonio Frassoldati Oncologia Clinica Ferrara Which clinical scenario have to face First line therapy with today? Untreated metastatic breast
Highlitghs in MBC First and second line endocrine treatments Antonio Frassoldati Oncologia Clinica Ferrara Which clinical scenario have to face First line therapy with today? Untreated metastatic breast
Update on New Perspectives in Endocrine-Sensitive Breast Cancer. James R. Waisman, MD
 Update on New Perspectives in Endocrine-Sensitive Breast Cancer James R. Waisman, MD Nothing to disclose DISCLOSURE TAILORx Oncotype Recurrence Score TAILORx Study Design Sparano, J Clin Oncol 2008;26:721-728
Update on New Perspectives in Endocrine-Sensitive Breast Cancer James R. Waisman, MD Nothing to disclose DISCLOSURE TAILORx Oncotype Recurrence Score TAILORx Study Design Sparano, J Clin Oncol 2008;26:721-728
Endocrine Therapy in Breast Cancer: State of the Art
 Endocrine Therapy in Breast Cancer: State of the Art 12 AUG 2018 Mark Pegram, M.D. Susy Yuan-Huey Hung Professor of Oncology Associate Director for Clinical Research Director, Stanford Breast Oncology
Endocrine Therapy in Breast Cancer: State of the Art 12 AUG 2018 Mark Pegram, M.D. Susy Yuan-Huey Hung Professor of Oncology Associate Director for Clinical Research Director, Stanford Breast Oncology
La via del segnale PI3K/AKT/mTOR Inibitori di mtor nel carcinoma mammario
 La via del segnale PI3K/AKT/mTOR Inibitori di mtor nel carcinoma mammario Alessandra Modena U.O.C. Oncologia Medica Direttore: Dott.ssa Stefania Gori Ospedale Sacro Cuore - Don Calabria 29 novembre 2016
La via del segnale PI3K/AKT/mTOR Inibitori di mtor nel carcinoma mammario Alessandra Modena U.O.C. Oncologia Medica Direttore: Dott.ssa Stefania Gori Ospedale Sacro Cuore - Don Calabria 29 novembre 2016
Recent Update in Management of Breast Cancer: Medical Oncology. Jin Hee Ahn, M.D., PhD. 23-April-2015
 2015 GBCC & 4 th IBCS 1/37 Recent Update in Management of Breast Cancer: Medical Oncology Jin Hee Ahn, M.D., PhD. 23-April-2015 Department of Oncology, Asan Medical Center, UUCM, Seoul, Korea 2/37 3/37
2015 GBCC & 4 th IBCS 1/37 Recent Update in Management of Breast Cancer: Medical Oncology Jin Hee Ahn, M.D., PhD. 23-April-2015 Department of Oncology, Asan Medical Center, UUCM, Seoul, Korea 2/37 3/37
Oncology. A CME-certified Supplement to the. Journal of the National Comprehensive Cancer Network. Program Overview/Statement of Need
 JNCCN Volume 16 1 Journal of the National Comprehensive Cancer Network A CME-certified to the Journal of the National Comprehensive Cancer Network Program Overview/Statement of Need Recently updated guidelines
JNCCN Volume 16 1 Journal of the National Comprehensive Cancer Network A CME-certified to the Journal of the National Comprehensive Cancer Network Program Overview/Statement of Need Recently updated guidelines
Agents in the Treatment of ER+ Aromatase Inbitor-Resistant Metastatic Breast Cancer: M-THOR Inhibitors
 Agents in the Treatment of ER+ Aromatase Inbitor-Resistant Metastatic Breast Cancer: M-THOR Inhibitors Valero, M.D., Professor of Medicine and Deputy Chairman Department of Breast Medical Oncology The
Agents in the Treatment of ER+ Aromatase Inbitor-Resistant Metastatic Breast Cancer: M-THOR Inhibitors Valero, M.D., Professor of Medicine and Deputy Chairman Department of Breast Medical Oncology The
DEJEUNER-DEBAT Alternatives d administration des chimiothérapies (Session Plénière ) Salle : Salle Camille Blanc
 Salle : Salle Camille Blanc") DEJEUNER-DEBAT Alternatives d administration des chimiothérapies (Session Plénière ) Salle : Salle Camille Blanc Revue des essais cliniques en cours et perspectives Dr Cristian Villanueva CHRU Besançon
DEJEUNER-DEBAT Alternatives d administration des chimiothérapies (Session Plénière ) Salle : Salle Camille Blanc Revue des essais cliniques en cours et perspectives Dr Cristian Villanueva CHRU Besançon
Terapia adiuvante con inibitori delle Kinasi Cliclina Dipendenti 4/6: quale futuro? Filippo Montemurro
 Terapia adiuvante con inibitori delle Kinasi Cliclina Dipendenti 4/6: quale futuro? Filippo Montemurro Unit of Investigative Clinical Oncology Istituto di Candiolo (IRCCS) Disclosures Speaker s Honoraria
Terapia adiuvante con inibitori delle Kinasi Cliclina Dipendenti 4/6: quale futuro? Filippo Montemurro Unit of Investigative Clinical Oncology Istituto di Candiolo (IRCCS) Disclosures Speaker s Honoraria
Manejo do câncer de mama RH+ na adjuvância: o que há de novo?
 II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico Manejo do câncer de mama RH+ na adjuvância: o que há de novo? INGRID A. MAYER, MD, MSCI Assistant Professor of Medicine Director,
II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico Manejo do câncer de mama RH+ na adjuvância: o que há de novo? INGRID A. MAYER, MD, MSCI Assistant Professor of Medicine Director,
Hormonal Management of Metastatic Breast Cancer
 Hormonal Management of Metastatic Breast Cancer Dr. Khaled Abulkhair, PhD Medical Oncology SCE, Royal College, UK Ass. Professor of Clinical Oncology Mansoura University, Egypt Case For Discussion A 63
Hormonal Management of Metastatic Breast Cancer Dr. Khaled Abulkhair, PhD Medical Oncology SCE, Royal College, UK Ass. Professor of Clinical Oncology Mansoura University, Egypt Case For Discussion A 63
Il trattamento medico
 III Sessione: La malattia in fase avanzata Il trattamento medico Emilio Bria Oncologia, Dipartimento di Medicina, Università di Verona, Azienda Ospedaliera Universitaria Integrata Verona emilio.bria@univr.it
III Sessione: La malattia in fase avanzata Il trattamento medico Emilio Bria Oncologia, Dipartimento di Medicina, Università di Verona, Azienda Ospedaliera Universitaria Integrata Verona emilio.bria@univr.it
The efficacy of second-line hormone therapy for recurrence during adjuvant hormone therapy for breast cancer
 517734TAM6210.1177/1758834013517734Therapeutic Advances in Medical OncologyR Mori and Y Nagao research-article2013 Therapeutic Advances in Medical Oncology Original Research The efficacy of second-line
517734TAM6210.1177/1758834013517734Therapeutic Advances in Medical OncologyR Mori and Y Nagao research-article2013 Therapeutic Advances in Medical Oncology Original Research The efficacy of second-line
Updates From San Antonio Breast Cancer Symposium 2017
 Updates From San Antonio Breast Cancer Symposium 2017 Rob Coleman University of Sheffield Presentation Outline New Insights into adjuvant endocrine treatment Duration of treatment Perioperative therapy
Updates From San Antonio Breast Cancer Symposium 2017 Rob Coleman University of Sheffield Presentation Outline New Insights into adjuvant endocrine treatment Duration of treatment Perioperative therapy
Fulvestrant: cuándo y dónde usarlo? Dra. S. López-Tarruella
 Fulvestrant: cuándo y dónde usarlo? Dra. S. López-Tarruella FULVESTRANT mechanism of action Carlson et al Clin Breast Cancer 2005; Howell Crit Rev Oncol Hematol 2016; Robertson et al Cancer Res 2001; De
Fulvestrant: cuándo y dónde usarlo? Dra. S. López-Tarruella FULVESTRANT mechanism of action Carlson et al Clin Breast Cancer 2005; Howell Crit Rev Oncol Hematol 2016; Robertson et al Cancer Res 2001; De
LA MALATTIA METASTATICA. La malattia HR positiva/her2 negativa: quale terapia di I linea? Come scegliere? Jennifer Foglietta P.O.
 LA MALATTIA METASTATICA La malattia HR positiva/her2 negativa: quale terapia di I linea? Come scegliere? Jennifer Foglietta P.O. Narni-Amelia (TR) Outline Re-testing metastatic disease Chemo- vs endocrine-therapy
LA MALATTIA METASTATICA La malattia HR positiva/her2 negativa: quale terapia di I linea? Come scegliere? Jennifer Foglietta P.O. Narni-Amelia (TR) Outline Re-testing metastatic disease Chemo- vs endocrine-therapy
Recent advances in the management of metastatic breast cancer in older adults
 Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
ASCO 2017 WEBCAST. Elacestrant (RAD1901) June, 4, 2017
 June, 4, 2017") ASCO 2017 WEBCAST Elacestrant (RAD1901) June, 4, 2017 NASDAQ: RDUS Disclaimer: RAD1901 is an investigational agent Please refer to the ASCO 2017 poster for complete details Safe Harbor Any statements made
ASCO 2017 WEBCAST Elacestrant (RAD1901) June, 4, 2017 NASDAQ: RDUS Disclaimer: RAD1901 is an investigational agent Please refer to the ASCO 2017 poster for complete details Safe Harbor Any statements made
Current standards and practice changing studies in Luminal ABC in 2017
 Current standards and practice changing studies in Luminal ABC in 2017 F. Cardoso, MD Director, Breast Unit, Champalimaud Clinical Center, Lisbon, Portugal ESO Breast Cancer Program Coordinator ESMO Board
Current standards and practice changing studies in Luminal ABC in 2017 F. Cardoso, MD Director, Breast Unit, Champalimaud Clinical Center, Lisbon, Portugal ESO Breast Cancer Program Coordinator ESMO Board
Disease Update: Metastatic Breast Cancer
 Disease Update: Metastatic Breast Cancer Aimee Faso, PharmD, BCOP, CPP Oncology Clinical Specialist, GI/Breast UNC Hospitals and Clinics August 2015 Objectives Identify treatment choices of metastatic
Disease Update: Metastatic Breast Cancer Aimee Faso, PharmD, BCOP, CPP Oncology Clinical Specialist, GI/Breast UNC Hospitals and Clinics August 2015 Objectives Identify treatment choices of metastatic
A vision for HER2 future
 School of Medical Oncology Department of Medical and Biological Sciences - University of Udine Department of Oncology - University Hospital of Udine A vision for HER2 future Current therapeutic algorithm
School of Medical Oncology Department of Medical and Biological Sciences - University of Udine Department of Oncology - University Hospital of Udine A vision for HER2 future Current therapeutic algorithm
Transcript and References
 Richard S. Finn, MD Associate Professor of Medicine Division of Hematology/Oncology Co-director, Signal Transduction and Therapeutics Program Jonsson Comprehensive Cancer Center Geffen School of Medicine
Richard S. Finn, MD Associate Professor of Medicine Division of Hematology/Oncology Co-director, Signal Transduction and Therapeutics Program Jonsson Comprehensive Cancer Center Geffen School of Medicine
Highlights of. Metastatic & Advanced Breast Cancer
 Highlights of Metastatic & Advanced Breast Cancer 1 Financial Disclosure(s) I currently have or have had the following relevant financial relations to disclose: Speaker s Bureau: Novartis 2 Off Label Use
Highlights of Metastatic & Advanced Breast Cancer 1 Financial Disclosure(s) I currently have or have had the following relevant financial relations to disclose: Speaker s Bureau: Novartis 2 Off Label Use
Collaborative Management of Patients With Advanced Estrogen Receptor Positive Breast Cancer
 Collaborative Management of Patients With Advanced Estrogen Receptor Positive Breast Cancer Lee Schwartzberg, MD, FACP Heather Greene, FNP, AOCNP West Cancer Center Memphis, Tennessee Learning Objectives
Collaborative Management of Patients With Advanced Estrogen Receptor Positive Breast Cancer Lee Schwartzberg, MD, FACP Heather Greene, FNP, AOCNP West Cancer Center Memphis, Tennessee Learning Objectives
Targeting mtor pathway in ER+/Her2- breast cancers. Fabrice ANDRE Gustave Roussy
 Targeting mtor pathway in ER+/Her2- breast cancers Fabrice ANDRE Gustave Roussy Outline mtor pathway Clinical development of rapalogs in breast cancer Moving beyond rapalogs mtor pathway LKB1 Ras-raf-
Targeting mtor pathway in ER+/Her2- breast cancers Fabrice ANDRE Gustave Roussy Outline mtor pathway Clinical development of rapalogs in breast cancer Moving beyond rapalogs mtor pathway LKB1 Ras-raf-
Sesiones interhospitalarias de cáncer de mama. Revisión bibliográfica 4º trimestre 2015
 Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
SABCS 2017 WEBCAST. Elacestrant (RAD1901) Update. December 7, 2017
 Update. December 7, 2017") SABCS 2017 WEBCAST Elacestrant (RAD1901) Update December 7, 2017 NASDAQ: RDUS Disclaimer: Elacestrant is an investigational agent Please refer to the SABCS 2017 poster for complete details Safe Harbor
SABCS 2017 WEBCAST Elacestrant (RAD1901) Update December 7, 2017 NASDAQ: RDUS Disclaimer: Elacestrant is an investigational agent Please refer to the SABCS 2017 poster for complete details Safe Harbor
Overcoming Endocrine Resistance in ER+ Breast Cancer
 Overcoming Endocrine Resistance in ER+ Breast Cancer Richard S. Finn, MD Associate Professor of Medicine Division of Hematology/Oncology Director Signal Transduction and Therapeutics Program Jonsson Comprehensive
Overcoming Endocrine Resistance in ER+ Breast Cancer Richard S. Finn, MD Associate Professor of Medicine Division of Hematology/Oncology Director Signal Transduction and Therapeutics Program Jonsson Comprehensive
Her 2 Positive Advanced Breast Cancer: From Evidence to Practice
 Her 2 Positive Advanced Breast Cancer: From Evidence to Practice Sunil Verma MD, FRCP(C) Medical Director, Tom Baker Cancer Center Professor and Head, Department of Oncology Cumming School of Medicine,
Her 2 Positive Advanced Breast Cancer: From Evidence to Practice Sunil Verma MD, FRCP(C) Medical Director, Tom Baker Cancer Center Professor and Head, Department of Oncology Cumming School of Medicine,
CDK4/6 inhibitors in advanced hormone receptor-positive breast cancer
 Perspective CDK4/6 inhibitors in advanced hormone receptor-positive breast cancer Romualdo Barroso-Sousa, Sara M. Tolaney Department of Medical Oncology, Dana-Farber Cancer Institute, Boston, MA, USA Correspondence
Perspective CDK4/6 inhibitors in advanced hormone receptor-positive breast cancer Romualdo Barroso-Sousa, Sara M. Tolaney Department of Medical Oncology, Dana-Farber Cancer Institute, Boston, MA, USA Correspondence
pan-canadian Oncology Drug Review Final Clinical Guidance Report Everolimus (Afinitor) for Advanced Breast Cancer March 25, 2013
 for Advanced Breast Cancer March 25, 2013") pan-canadian Oncology Drug Review Final Clinical Guidance Report Everolimus (Afinitor) for Advanced Breast Cancer March 25, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Everolimus (Afinitor) for Advanced Breast Cancer March 25, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
Endocrine therapy for ER-positive/HER2-negative metastatic breast cancer
 Review Article Page 1 of 16 Endocrine therapy for ER-positive/HER2-negative metastatic breast cancer Tomás Reinert 1,2, Bruno de Paula 3, Maryam Nemati Shafaee 4, Pedro Henrique Souza 5, Matthew J. Ellis
Review Article Page 1 of 16 Endocrine therapy for ER-positive/HER2-negative metastatic breast cancer Tomás Reinert 1,2, Bruno de Paula 3, Maryam Nemati Shafaee 4, Pedro Henrique Souza 5, Matthew J. Ellis
Endocrine Therapy of Metastatic Breast Cancer
 Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Endocrine Therapy of Metastatic Breast Cancer Endocrine Therapy of Metastatic Breast Cancer Version 2002: Gerber / Friedrichs
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Endocrine Therapy of Metastatic Breast Cancer Endocrine Therapy of Metastatic Breast Cancer Version 2002: Gerber / Friedrichs
The benefit of abemaciclib in prognostic subgroups: An exploratory analysis of combined data from the MONARCH 2 and 3 studies
 The benefit of in prognostic subgroups: An exploratory analysis of combined data from the MONARCH 2 and 3 studies Matthew P. Goetz¹, Joyce O Shaughnessy², George W. Sledge Jr.³, Miguel Martin⁴, Yong Lin⁵,
The benefit of in prognostic subgroups: An exploratory analysis of combined data from the MONARCH 2 and 3 studies Matthew P. Goetz¹, Joyce O Shaughnessy², George W. Sledge Jr.³, Miguel Martin⁴, Yong Lin⁵,
Clinical activity of fulvestrant in metastatic breast cancer previously treated with endocrine therapy and/or chemotherapy
 ORIGINAL ARTICLE 2018 Mar 16. [Epub ahead of print] Clinical activity of fulvestrant in metastatic breast cancer previously treated with endocrine therapy and/or chemotherapy Mi Hwa Heo, Hee Kyung Kim,
ORIGINAL ARTICLE 2018 Mar 16. [Epub ahead of print] Clinical activity of fulvestrant in metastatic breast cancer previously treated with endocrine therapy and/or chemotherapy Mi Hwa Heo, Hee Kyung Kim,
Extended Hormonal Therapy
 Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
Enhancing Endocrine Therapy for Hormone Receptor Positive Advanced Breast Cancer: Cotargeting Signaling Pathways
 JNCI J Natl Cancer Inst (2015) 107(10): djv212 doi:10.1093/jnci/djv212 First published online August 6, 2015 Review Enhancing Endocrine Therapy for Hormone Receptor Positive Advanced Breast Cancer: Cotargeting
JNCI J Natl Cancer Inst (2015) 107(10): djv212 doi:10.1093/jnci/djv212 First published online August 6, 2015 Review Enhancing Endocrine Therapy for Hormone Receptor Positive Advanced Breast Cancer: Cotargeting
Best of San Antonio 2008
 Best of San Antonio 2008 Ellie Guardino, MD/PhD Assistant Professor Stanford University BIG 1 98: a randomized double blind phase III study evaluating letrozole and tamoxifen given in sequence as adjuvant
Best of San Antonio 2008 Ellie Guardino, MD/PhD Assistant Professor Stanford University BIG 1 98: a randomized double blind phase III study evaluating letrozole and tamoxifen given in sequence as adjuvant
Update in the treatment of Her2- overexpressing breast cancers. Fabrice ANDRE Institut Gustave Roussy Villejuif, France
 Update in the treatment of Her2- overexpressing breast cancers Fabrice ANDRE Institut Gustave Roussy Villejuif, France Questions Should tumors
Update in the treatment of Her2- overexpressing breast cancers Fabrice ANDRE Institut Gustave Roussy Villejuif, France Questions Should tumors
Session Breast Cancer. Alessandra Fabi Il punto di vista dell esperto
 Session Breast Cancer Alessandra Fabi Il punto di vista dell esperto Roma 6-7.10.2017 The Importance of Understanding What Disease to Treat Cejalvo et al, Cancer Res 2017 Skyline Chaging at evolution of
Session Breast Cancer Alessandra Fabi Il punto di vista dell esperto Roma 6-7.10.2017 The Importance of Understanding What Disease to Treat Cejalvo et al, Cancer Res 2017 Skyline Chaging at evolution of
Breast cancer update. Iryna Kuchuk, MD Oncology department Meir Medical Center
 Breast cancer update Iryna Kuchuk, MD Oncology department Meir Medical Center Overview Cancer Death Rates* Among Women, US,1930-2009 Factors Associated with Reduction In Breast Cancer Mortality Early
Breast cancer update Iryna Kuchuk, MD Oncology department Meir Medical Center Overview Cancer Death Rates* Among Women, US,1930-2009 Factors Associated with Reduction In Breast Cancer Mortality Early
Targeting the PI3 kinase mtor pathway in breast cancer. Dr Nicholas Turner. Madrid 2014
 Targeting the PI3 kinase mtor pathway in breast cancer Dr Nicholas Turner Madrid 2014 Relevant disclosures Honoraria and/or Research funding Novartis AstraZeneca Roche Targeting PI3 kinase mtor pathway
Targeting the PI3 kinase mtor pathway in breast cancer Dr Nicholas Turner Madrid 2014 Relevant disclosures Honoraria and/or Research funding Novartis AstraZeneca Roche Targeting PI3 kinase mtor pathway
Update on the Management of HER2+ Breast Cancer. Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany
 Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Clinical Spotlight Key Advances in Hormone Receptor Positive Breast Cancer: Updates From the 2018 Oncology Annual Meeting in Chicago
 Clinical Spotlight Key Advances in Hormone Receptor Positive Breast Cancer: Updates From the 2018 Oncology Annual Meeting in Chicago Reference Slide Deck Abstract 1000 Abstract 1001 Abstract 1002 Abstract
Clinical Spotlight Key Advances in Hormone Receptor Positive Breast Cancer: Updates From the 2018 Oncology Annual Meeting in Chicago Reference Slide Deck Abstract 1000 Abstract 1001 Abstract 1002 Abstract
Chemotherapy and Hormonal Therapy in the Metastatic Setting, ER+/HER-2- and TNBC
 15TH ANNUAL MIAMI CANCER MEETING (MCM)April 27-29, 2018 Miami, Florida Chemotherapy and Hormonal Therapy in the Metastatic Setting, ER+/HER-2- and TNBC Vicente Valero, M.D., F.A.C.P. Professor of Medicine
15TH ANNUAL MIAMI CANCER MEETING (MCM)April 27-29, 2018 Miami, Florida Chemotherapy and Hormonal Therapy in the Metastatic Setting, ER+/HER-2- and TNBC Vicente Valero, M.D., F.A.C.P. Professor of Medicine
Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer
 Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer Sara A. Hurvitz, MD, FACP Associate Professor of Medicine University of California Los Angeles Los Angeles, California Trastuzumab
Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer Sara A. Hurvitz, MD, FACP Associate Professor of Medicine University of California Los Angeles Los Angeles, California Trastuzumab
G1 Corporate Overview March 11, 2019
 G1 Corporate Overview March 11, 2019 www.g1therapeutics.com NASDAQ: GTHX 1 Forward-looking statements This presentation and the accompanying oral commentary contain forward-looking statements within the
G1 Corporate Overview March 11, 2019 www.g1therapeutics.com NASDAQ: GTHX 1 Forward-looking statements This presentation and the accompanying oral commentary contain forward-looking statements within the
Claudio Zamagni Milano 16 giugno 2018 AIOM Post-ASCO BREAST CANCER HIGHLIGHTS ASCO 2018
 Claudio Zamagni Milano 16 giugno 2018 AIOM Post-ASCO BREAST CANCER HIGHLIGHTS ASCO 2018 (Neo)Adjuvant Advanced De-escalation ER+ve HER2 ve Node ve TAILORx HER2 +ve Persephone PerElisa PARPi in gbrcam HER2
Claudio Zamagni Milano 16 giugno 2018 AIOM Post-ASCO BREAST CANCER HIGHLIGHTS ASCO 2018 (Neo)Adjuvant Advanced De-escalation ER+ve HER2 ve Node ve TAILORx HER2 +ve Persephone PerElisa PARPi in gbrcam HER2
Emerging Approaches for (Neo)Adjuvant Therapy for ER+ Breast Cancer
Adjuvant Therapy for ER+ Breast Cancer") Emerging Approaches for (Neo)Adjuvant Therapy for E+ Breast Cancer Cynthia X. Ma, M.D., Ph.D. Associate Professor of Medicine Washington University in St. Louis Outline Current status of adjuvant endocrine
Emerging Approaches for (Neo)Adjuvant Therapy for E+ Breast Cancer Cynthia X. Ma, M.D., Ph.D. Associate Professor of Medicine Washington University in St. Louis Outline Current status of adjuvant endocrine
SYNOPSIS PROTOCOL TALBOT
 SYNOPSIS PROTOCOL TALBOT A) CLINICAL TRIAL IDENTIFICATION SPONSOR - PROTOCOL CODE NUMBER : VERSION: SYNOPSIS V4.0-30/06/2015 TRIAL TITLE : Open-label, randomized, multicenter, phase II study, comparing
SYNOPSIS PROTOCOL TALBOT A) CLINICAL TRIAL IDENTIFICATION SPONSOR - PROTOCOL CODE NUMBER : VERSION: SYNOPSIS V4.0-30/06/2015 TRIAL TITLE : Open-label, randomized, multicenter, phase II study, comparing
Update on Systemic Treatment of Breast Cancer
 Update on Systemic Treatment of Breast Cancer Christoph C. Zielinski Clinical Division of Oncology Department of Medicine I and Comprehensive Cancer Center (www.ccc.ac.at) Medical University Vienna - General
Update on Systemic Treatment of Breast Cancer Christoph C. Zielinski Clinical Division of Oncology Department of Medicine I and Comprehensive Cancer Center (www.ccc.ac.at) Medical University Vienna - General
Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA
 Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA When Are Biomarkers Ready To Use? Same Rules for Gene Expression Panels Key elements
Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA When Are Biomarkers Ready To Use? Same Rules for Gene Expression Panels Key elements
PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND!
 II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND! INGRID A. MAYER, MD, MSCI Assistant
II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND! INGRID A. MAYER, MD, MSCI Assistant
ASCO 2018 Breast Cancer Highlights
 ASCO 2018 Breast Cancer Highlights Angie DeMichele, MD, MSCE Jill & Alan Miller Endowed Chair in Breast Cancer Excellence Professor of Medicine and Epidemiology Co-Leader, Breast Cancer Program, Abramson
ASCO 2018 Breast Cancer Highlights Angie DeMichele, MD, MSCE Jill & Alan Miller Endowed Chair in Breast Cancer Excellence Professor of Medicine and Epidemiology Co-Leader, Breast Cancer Program, Abramson
MEDICAL ONCOLOGY NEWS IN BREAST CANCER 2014
 MEDICAL ONCOLOGY NEWS IN BREAST CANCER 2014 Dr Thomas Yau Clinical Assistant Professor MBBS(HK), MRCP (UK), FHKCP (Med Onc), FHKAM( Medicine), FRCP(London) Queen Mary Hospital The University of Hong Kong
MEDICAL ONCOLOGY NEWS IN BREAST CANCER 2014 Dr Thomas Yau Clinical Assistant Professor MBBS(HK), MRCP (UK), FHKCP (Med Onc), FHKAM( Medicine), FRCP(London) Queen Mary Hospital The University of Hong Kong
William J. Gradishar MD
 Northwestern University Feinberg School of Medicine Adjuvant Endocrine Therapy For Postmenopausal Women SOBO 2013 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley
Northwestern University Feinberg School of Medicine Adjuvant Endocrine Therapy For Postmenopausal Women SOBO 2013 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley
Post-ESMO 2012: Tamara Rordorf Klinik für Onkologie UniversitätsSpital Zürich T.Rordorf, SAMO Luzern 1
 Post-ESMO 2012: Breast Cancer Tamara Rordorf Klinik für Onkologie UniversitätsSpital Zürich 1 Neoadjuvant treatment (in Her-2 positive disease) neoadjuvant trials abstracts: breast sparing surgery, biomarkers,
Post-ESMO 2012: Breast Cancer Tamara Rordorf Klinik für Onkologie UniversitätsSpital Zürich 1 Neoadjuvant treatment (in Her-2 positive disease) neoadjuvant trials abstracts: breast sparing surgery, biomarkers,
Triple Negative Breast Cancer. Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008
 Triple Negative Breast Cancer Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008 Triple Negative Breast Cancer 15% 25% Triple Negative 20% HER2+ ER+ Low Grade
Triple Negative Breast Cancer Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008 Triple Negative Breast Cancer 15% 25% Triple Negative 20% HER2+ ER+ Low Grade
Breast Cancer Advanced Disease. Stefan Aebi Luzerner Kantonsspital
 Breast Cancer Advanced Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch How to Guidelines and Consensus Breast Cancer Advanced Disease Prognosis Clonal (and diagnostic) evolution: Biopsy
Breast Cancer Advanced Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch How to Guidelines and Consensus Breast Cancer Advanced Disease Prognosis Clonal (and diagnostic) evolution: Biopsy
Choosing between different hormonal therapies. Rudy Van den Broecke UZ Ghent
 Choosing between different hormonal therapies Rudy Van den Broecke UZ Ghent What is the golden standard in premenopausal hormonal sensitive early breast cancer? Ovarian Suppression alone 5 years Tamoxifen
Choosing between different hormonal therapies Rudy Van den Broecke UZ Ghent What is the golden standard in premenopausal hormonal sensitive early breast cancer? Ovarian Suppression alone 5 years Tamoxifen
Enhancing Endocrine Therapy Combination Strategies for the Treatment of Postmenopausal HR1/HER2 Advanced Breast Cancer
 Breast Cancer Enhancing Endocrine Therapy Combination Strategies for the Treatment of Postmenopausal HR1/ Advanced Breast Cancer KATHLEEN I. PRITCHARD, a STEPHEN K. CHIA, b CHRISTINE SIMMONS, b DEANNA
Breast Cancer Enhancing Endocrine Therapy Combination Strategies for the Treatment of Postmenopausal HR1/ Advanced Breast Cancer KATHLEEN I. PRITCHARD, a STEPHEN K. CHIA, b CHRISTINE SIMMONS, b DEANNA
LAPATINIB-Resistance to small Molecule ErbB2 Tyrosine Kinase Inhibitor (TKI)
") LAPATINIB-Resistance to small Molecule ErbB2 Tyrosine Kinase Inhibitor (TKI) Prim Mr Sc Dr Suzana Vasović Institute for oncology and radiology of Serbia UMOS, X Conference, 16.05.2015 Belgrade How do we
LAPATINIB-Resistance to small Molecule ErbB2 Tyrosine Kinase Inhibitor (TKI) Prim Mr Sc Dr Suzana Vasović Institute for oncology and radiology of Serbia UMOS, X Conference, 16.05.2015 Belgrade How do we