Metastatic HR+ Breast Cancer - CDK 4/6 Inhibitors Charting the Path. Sandy Sehdev MD FRCPC
|
|
|
- Osborne King
- 5 years ago
- Views:
Transcription
1 Metastatic HR+ Breast Cancer - CDK 4/6 Inhibitors Charting the Path Sandy Sehdev MD FRCPC

2 Objectives To understand the approach to the treatment of hormone sensitive metastatic breast cancer and the use of CDK4/6 inhibition role in Rx sequencing benefits and toxicities appropriate patient monitoring
3 Evaluation Were the concepts presented clearly and logically? Do you feel comfortable managing these patients in the clinic?

4 Disclosure: Dr. Sehdev Grants/research support: none Honoraria: AZ and Novartis advisory boards, CAGPO presentation Consulting fees: none Patents: none Other: travel support for this meeting Probono advocacy work uottawa.ca Faculté de médecine Faculty of Medicine
5 Mitigating potential bias Neither Pfizer nor any other industry source has had direct input into the development of content Only generic names will be used, without logos The evidence basis for recommendations will be highlighted uottawa.ca Faculté de médecine Faculty of Medicine
6 Overview Approach to met ER+ disease Background evidence: CDK 4/6 inhibition Mechanism Supportive data : palbociclib / ribociclib / abemaciclib Role in Rx / sequencing Resistance Dosing / adjustments Toxicities uottawa.ca Faculté de médecine Faculty of Medicine

7 Changing Realities Increasing long term survival with metastatic ER+ breast cancer Busier clinics More complex Rx algorithms Sequencing challenges Funding lags data Survivorship challenges living with cancer living with treatments!
 1 E2 ER E2 E2 ER ER E2 ER E2 E2 ER ER")



8 SERMs Example: Tamoxifen Tablets (mixed agonistic/ antagonistic effects on ER signaling) 1 E2 ER E2 E2 ER ER E2 ER E2 E2 ER ER Direct estrogen-dependent genomic pathway NUCLEUS Indirect estrogen-independent, genomic pathway ERE Src RTKs ER Non- ERE PI3K Akt ERK ER Ras Amphiregulin TGF-alpha TF TF Akt PI3K Src FAK Non-genomic activity E2 E2 ER ER ER ERK? PELP1S rc Rb E2F ER G1 G0 ER Cyclin D1 CDK4/6 CELL CYCLE M CELL MEMBRANE S CYTOPLASM Tamoxifen activates nongenomic ER 2 Enhanced proliferation and tumor growth P P Rb P E2F Cyclin D1 G2
 2 Letrozole Tablets")



9 AROMATASE INHIBITORS Examples: Exemestane Tablets (steroidal) 1 Anastrozole Tablets (non-steroidal) 2 Letrozole Tablets (non-steroidal) 3 E2 ER E2 E2 ER ER E2 ER E2 E2 ER ER Direct estrogen-dependent genomic pathway NUCLEUS Indirect estrogen-independent, genomic pathway ERE Src RTKs ER Non- ERE PI3K Akt ERK ER Ras Amphiregulin TGF-alpha TF TF Akt PI3K Src FAK Non-genomic activity E2 E2 ER ER ER ERK PELP1S rc Rb E2F ER G1 G0 ER Cyclin D1 CDK4/6 CELL CYCLE M CELL MEMBRANE S CYTOPLASM Enhanced proliferation and tumor growth P P Rb P E2F Cyclin D1 G2


10 SERDs Example: Fulvestrant Injection (competitively antagonizes ER signaling; has no known agonist activity) 1 E2 ER E2 E2 ER ER E2 ER E2 E2 ER ER Direct estrogen-dependent genomic pathway NUCLEUS Indirect estrogen-independent, genomic pathway ERE Src RTKs ER Non- ERE PI3K Akt ERK ER Ras Amphiregulin TGF-alpha TF TF Akt PI3K Src FAK Non-genomic activity E2 E2 ER ER ER ERK PELP1S rc Rb E2F ER G1 G0 ER Cyclin D1 CDK4/6 CELL CYCLE M CELL MEMBRANE S CYTOPLASM Enhanced proliferation and tumor growth P P Rb P E2F Cyclin D1 G2
11 First-Line Endocrine Therapy in HR-positive Advanced Breast Cancer Treatments CBR (%) ORR (%) TTP (mo) PFS (mo) TAM vs Toremifene vs vs 4.9 ANA vs TAM vs vs vs 7.0 LET vs TAM 3 49 vs vs vs 6.0 EXE vs TAM 4 46 vs vs 5.8 FUL vs TAM vs vs 8.3 FACT: FUL + ANA vs ANA vs vs vs 10.2 SWOG S0226: ANA + FUL vs ANA vs 13.5
12 68F Past L breast cancer 1992: LN - Past R breast CA 2004 ER/PR + TAM x 5 yrs Back pain x 2 mo Mets to T6, sacrum, ribs 3 small lung lesions up to 11 mm Lung bx = ER+ Her2 neg
13 Plan: Denosumab 120 mg sc monthly and 1. Letrozole alone 2. Fulvestrant 500 mg monthly 3. Weekly paclitaxel chemo 4. Oral capecitabine chemo 5. LET + palbociclib
14 82F with de novo metastatic breast CA Bone mets - multiple Liver mets - multiple up to 3cm Breast mass in situ - 2 cm ER/PR ++ Her 2 negative Mild dementia Atrial fibrillation, controlled
15 Plan: Denosumab 120 mg sc monthly and 1. Letrozole alone 2. Fulvestrant 500 mg monthly 3. Weekly paclitaxel chemo 4. Oral capecitabine chemo 5. LET + palbociclib
16 Patient Age Menopausal status Comorbidities Performance status, Symptoms Expectations and preferences Toxicities to previous treatments Adherence, compliance Disease Site of metastasis Tumor burden, Pace of Disease Symptomatology and / or need for rapid response Previous endocrine treatment Disease-free interval on adjuvant setting (>12m?) Degree of response to previous ET Duration of response to previous ET *Predictive biomarkers for endocrine therapy in HR+ ABC are not available and developments in this field should be a priority of future research. Therapy Selection: Clinical Factors Agent Mechanism of action Expected toxicities Pharmacological interactions Availability, Access Cost Route of administration Tumor Histological subtype Expression of hormone receptors HER2 amplification Intrinsic subtype Predictive biomarkers* Other issues Availability of clinical research Existing guidelines Financial hardship Social support
17 Fulvestrant (Faslodex ) Estrogen Receptor Dysregulator uottawa.ca Faculté de médecine Faculty of Medicine
18 FALCON: PHASE III STUDY DESIGN Postmenopausal women Locally advanced or metastatic breast cancer ER+ and / or PgR+ HER2- Endocrine therapy-naïve Fulvestrant 500 mg (500 mg IM on Days 0, 14 and 28, then every 28 days) Primary endpoint: PFS a + placebo Secondary endpoints 1:1 OS b Anastrozole 1 mg (daily PO) + placebo Randomised, double-blind, parallel-group, international, multicentre study Follow-up for disease progression and survival ORR CBR DoR, EDoR DoCB, EDoCB HRQoL (FACT-B total and TOI) Safety Randomisation of 450 patients was planned to achieve 306 progression events; if the true PFS HR was 0.69 this would provide 90% power for statistical significance at the 5% two-sided level (log-rank test) Stratification factors: prior chemotherapy for advanced disease (yes / no); measurable vs. non-measurable disease (at baseline); locally advanced vs. metastatic disease Subgroup analysis of PFS for pre-defined baseline covariates a Assessed via RECIST 1.1, surgery / radiotherapy for disease worsening, or death; b Interim analysis at the time of PFS analysis EDoCB, expected duration of clinical benefit; EDoR, expected duration of response; FACT-B, Functional Assessment of Cancer Therapy Breast; TOI, Trial Outcome Index
19 FALCON Inclusion/Exclusion Criteria Inclusion criteria Exclusion criteria Postmenopausal Any prior endocrine therapy ER+ and/or PgR+ Locally advanced or metastatic disease Prior systemic therapy for breast cancer, other than one line of chemotherapy Radiotherapy completed < 28 days before randomisation 1 line of chemotherapy allowed for breast cancer HER2+ 1 lesion that can be assessed at baseline and suitable for repeated measurement Visceral crisis Clinicaltrials.gov, NCT ; available at: FALCON Clinical Study Protocol, 01 May 2012.
20 FALCON: BASELINE PATIENT CHARACTERISTICS Fulvestrant (N=230) Anastrozole (N=232) Median age, years (range) 64.0 (38 87) 62.0 (36 90) Race, n (%) White 175 (76.1) 174 (75.0) Any prior chemotherapy, n (%) 79 (34.3) 81 (34.9) Advanced disease 36 (15.7) 43 (18.5) Adjuvant / neoadjuvant 35 / 11 (15.2 / 4.8) 27 / 16 (11.6 / 6.9) WHO performance status, n (%) 0 / 1 / / 106 / 7 (50.9 / 46.1 / 3.0) 115 / 105 / 12 (49.6 / 45.3 / 5.2) Receptor status, n (%) ER+ / PgR+ 175 (76.1) 179 (77.2) ER+ / PgR- 44 (19.1) 43 (18.5) ER+ / PgR unknown 10 (4.3) 7 (3.0) ER- / PgR+ 1 (0.4) 3 (1.3) ER- / PgR- 0 0 Overall disease classification, n (%) Locally advanced disease 28 (12.2) 32 (13.8) Metastatic disease 202 (87.8) 200 (86.2) Visceral disease, n (%) 135 (58.7) 119 (51.3) Measurable disease, n (%) 193 (83.9) 196 (84.5)
21 FALCON: PFS IN PATIENTS WITH OR WITHOUT VISCERAL DISEASE Proportion of patients alive and progression-free HR 0.59 (95% CI 0.42, 0.84) Median PFS Fulvestrant: 22.3 months Anastrozole: 13.8 months Without visceral disease Fulvestrant (n=95) Anastrozole (n=113) Proportion of patients alive and progression-free HR 0.99 (95% CI 0.74, 1.33) Median PFS Fulvestrant: 13.8 months Anastrozole: 15.9 months With visceral disease Fulvestrant (n=135) Anastrozole (n=119) Time (months) Time (months) Post hoc interaction test p<0.01 A circle represents a censored observation
22 FALCON: SECONDARY ENDPOINTS Endpoint Fulvestrant (N=230) Anastrozole (N=232) ORR a 46.1% (89 / 193) 44.9% (88 / 196) CBR 78.3% (180 / 230) 74.1% (172 / 232) Odds ratio (95% CI) 1.07 (0.72, 1.61); p=0.729 Odds ratio (95% CI) 1.25 (0.82, 1.93); p=0.305 Median DoR 20.0 months 13.2 months - Median DoCB 22.1 months 19.1 months - EDoR 11.4 months 7.5 months EDoCB 21.9 months 17.5 months Median time to deterioration in FACT-B total score 13.8 months 11.1 months Ratio (95% CI) 1.52 (1.23, 1.89); p<0.001 Ratio (95% CI) 1.26 (1.13, 1.39); p<0.001 HR (95% CI) 0.84 (0.66, 1.07); p=0.159 a In patients with measurable disease at baseline



23
24 Targeted Rx: CDK 4/6 Inhibition Palbociclib (Ibrance ), Ribociclib (Kisqali ) approved; abemaciclib (Verzenio ) uottawa.ca Faculté de médecine Faculty of Medicine
25 Combination Therapy: Rationale Growth factor RTK (eg, EGFR, HER2) Cell membrane Idelalisib Buparlisib Everolimus PI3K mtor RAS RAF MEK Dabrafenib Vemurafenib Cobimetinib Trametinib P Cyclin D D CDK4/ CDK6 X Rb E2F Rb P Nucleus AI Fulvestrant Tamoxifen ER Palbociclib Ribociclib Abemaciclib E2F G1-S transition gene expression O Leary B, et al. Nat Rev Clin Oncol. 2016;13:
26 Pl3K/Akt (ER/PR/AR) Wnt/β-catenin NF-κB STATs MAPKs p53 p21 Active tumor suppressor Cyclin D CDK4/6 M G0 E2F Rb p16 G2 S G1 Gene transcription E2F R P P P P Rb Inactive

27
28 PALBOCICLIB (IBRANCE ) uottawa.ca Faculté de médecine Faculty of Medicine
29 PALOMA-1 / TRIO 18: First Line Palbociclib and Letrozole in Advanced Breast Cancer Phase 2 Palbociclib Plus Letrozole for First-Line Treatment of ER+ HER2- Advanced Breast Cancer Finn RS, et al. Lancet Oncol 2015;16:25-35
30 Cohort 1 Cohort 2 ER+/HER2 ABC R A N D O M I Z A T I O N a Palbociclib 125 mg/day b + letrozole 2.5 mg/day 1:1 Letrozole 2.5 mg/day ER+/HER2 ABC with CCND1 amplification and/or loss of P16 R A N D O M I Z A T I O N a Palbociclib 125 mg/day b + letrozole 2.5 mg/day 1:1 Letrozole 2.5 mg/day n=66 n=99 Randomized, phase II, open-label trial at 50 centres in 12 countries (NCT ) Key eligibility criteria: inoperable locally recurrent disease, postmenopausal status, no prior therapy for ABC, no prior CDK inhibitors, no letrozole within 12 months, no prior/current brain metastases, measurable disease (RECIST 1.0) or bone-only disease, ECOG PS 1, adequate bone marrow and renal function
31 PFS PFS probability (%) PAL + LET (N=84) LET (N=81) No. of events (%) 41 (49) 59 (73) Median PFS, months (95% CI) HR (95% CI) 20.2 ( ) ( ) P value ( ) Palbociclib + letrozole Letrozole Time (months) No. of patients at risk PAL + LET LET
32
33 PALOMA-3: Study Design 1 4 Phase III, double-blind study involving 144 centers in 17 countries (NCT ) HR+, HER2 MBC Pre/perimenopausal a,b or postmenopausal b Progressed on prior endocrine therapy: 2:1 Randomization N=521 c n=347 Palbociclib (125 mg QD; 3 weeks on/1 week off) + fulvestrant d (500 mg IM Q4W) on or within 12 months of completion of adjuvant treatment on or within 1 month after treatment for MBC 1 prior chemotherapy regimen for advanced cancer Stratification: Visceral metastases Sensitivity to prior hormonal therapy Pre-/peri- vs. postmenopausal n=174 Placebo (3 weeks on/1 week off) + fulvestrant d (500 mg IM Q4W)
34 Characteristic Pt Characteristics - 1 Palbociclib + fulvestrant (n=347) ITT population Placebo + fulvestrant (n=174) Median age, years (range) 57 (30 88) 56 (29 80) Self-reported race, n (%) White 252 (73) 133 (76) Asian 74 (21) 31 (18) Black or other 21 (6) 10 (6) ECOG PS, n (%) (59) 116 (67) (41) 58 (33) Menopausal status, n (%) Pre- or perimenopausal 72 (21) 36 (21) Postmenopausal 275 (79) 138 (79) Non-measurable disease, n (%) Bone 75 (22) 36 (21) Others 4 (1) 0 Measurable disease, n (%) Any measurable disease 268 (77) 138 (79) Visceral disease a 206 (59) 105 (60) Lung involvement 100 (29) 45 (26) Liver involvement 127 (37) 81 (47) Peritoneal involvement 2 (1) 1 (1) Brain or pleural involvement, or both 4 (1) 2 (1)
35 Pt Characteristics - 2 ITT population Characteristic Palbociclib + fulvestrant (n=347) Placebo + fulvestrant (n=174) No. of previous lines of endocrine treatment, n (%) (46) 91 (52) (40) 61 (35) 3 47 (14) 22 (13) Purpose of most recent treatment a, n (%) Adjuvant therapy 74 (21) 40 (23) Treatment of advanced or MBC 273 (79) 133 (76) Disease-free interval b, n (%) Data available 233 (67) 123 (71) >24 months 192 (82) 101 (82) months 30 (13) 19 (15) <12 months 11 (5) 3 (2) Previous chemotherapy, n (%) Neoadjuvant or adjuvant therapy only c 139 (40) 74 (43) Treatment of metastatic disease (with or without adjuvant or neoadjuvant) 113 (33) 64 (37)
36 Pt Characteristics - 3 ITT population Palbociclib + fulvestrant (n=347) Placebo + fulvestrant (n=174) Characteristic Previous endocrine therapy, n (%) AI 137 (39) 70 (40) Tamoxifen 51 (15) 23 (13) AI and tamoxifen 159 (46) 81 (47) Previous sensitivity to endocrine therapy a, n (%) Yes 274 (79) 136 (78) No 73 (21) 38 (22) ER or PR status confirmed by central laboratory testing, n (%) ER+ and PR+ Median of distribution 81 (23) 40 (23) <Median of distribution 71 (20) 29 (17) ER+ or PR+ Median of distribution 179 (52) 100 (57) <Median of distribution 165 (48) 90 (52) Central laboratory tested, median H-score (IQR); mean (SD) b, n (%) ER 110 (40 160); 107 (74) 114 (23 150); 99 (72) PR 10 (0 100); 53 (68) 20 (0 100); 51 (62)
37 Time to first dose delay : 64 days (range, ) Average duration of dose delay : 3 days (range, 2 16) Time to first dose interruption : 18 days (range, 1 482) Average duration of interruption for any reason: 6 days (range, 1 20) Time to dose reduction ( ): 57 days (range, ) Time to dose reduction (125 75): 36 days (range, 29 85) Time to dose reduction ( ): 34 days (range, ) Time to dose reduction from (125 75): 120 days (range, ) Delays and Interruptions 1st dose reduction 1st dose reduction; 2 dose reductions (n=22); 0,06 Percent 1st dose reduction; Dose Delay (n=123 ); 0,36 1st dose reduction; Dose Interruption (n=187 ) ; 0,54 1st dose reduction; 1 dose reduction (n=95); 0,28
38 PFS: Central Review PFS probability (%) Palbociclib + fulvestrant Placebo + fulvestrant PAL + FUL (n=147) PBO + FUL (n=64) Median PFS, months (95% CI) NE 3.8 ( ) HR (95% CI) 0.37 ( ) P value < Time (months)

39 PFS - subgroups

40 PFS - subgroups

41 Magnitude of ER Tumour hormone receptor expression was quantified by the central laboratory in 250 patients in the palbociclib + fulvestrant group and 130 patients in the placebo + fulvestrant group around 60% of patients in each group provided metastatic tissue samples The level of hormone receptor expression did not influence the magnitude of PFS benefit from palbociclib (sub premium interaction P=0.32 for ER and P=0.54 for PR)

42
43 PALMOMA-2: First Line Palbociclib and Letrozole in Advanced Breast Cancer Phase III Richard S. Finn, Miguel Martin, Hope S. Rugo, Stephen Jones, Seock-Ah Im, Karen Gelmon, Nadia Harbeck, Oleg N. Lipatov, Janice M. Walshe, Stacy Moulder, Eric Gauthier, Dongrui R. Lu, Sophia Randolph, Véronique Diéras, Dennis J. Slamon N Engl J Med 2016 Nov 17;375(20):
44 PALOMA-2: Phase III Study Design in Postmenopausal Patients with ER+, HER2 Advanced Breast Cancer Phase III, randomized, double-blind trial at 186 centres in 17 countries Treatment continued until objective disease progression, unacceptable toxicity, or withdrawal of consent. Crossover was not allowed Palbociclib/placebo dose reductions were allowed per protocol. Letrozole dose reductions were not permitted Postmenopausal ER+, HER2 advanced breast cancer No prior systemic treatment for advanced disease Prior (neo)adjuvant treatment with anastrozole or letrozole was allowed if the disease-free interval was 12 months from completion of therapy Measurable disease according to RECIST v1.1 or bone-only disease ECOG PS 0 2 Adequate organ function No advanced, symptomatic visceral spread at risk of short-term life-threatening complications N=666 a 2:1 RANDOMIZATION Palbociclib (125 mg QD, 3/1 schedule b ) + letrozole (2.5 mg QD) Placebo (3/1 schedule) + letrozole (2.5 mg QD)
 141 (63.5) 65 years 181 (40.8) 81 (36.5) Race, n (%) White 344 (77.5) 172 (77.5) Asian 65 (14.6) 30 (13.5) Black 8 (1.8) 3 (1.4) Other 27 (6.1) 17 (7.7) ECOG PS, n (%) 0 257 (57.9) 102 (45.")
45 PALOMA-2: Demographics and Baseline Characteristics (ITT Population) Age, n (%) Palbociclib + letrozole (N=444) Placebo + letrozole (N=222) Median (range) 62 (30 89) 61 (28 88) <65 years 263 (59.2) 141 (63.5) 65 years 181 (40.8) 81 (36.5) Race, n (%) White 344 (77.5) 172 (77.5) Asian 65 (14.6) 30 (13.5) Black 8 (1.8) 3 (1.4) Other 27 (6.1) 17 (7.7) ECOG PS, n (%) (57.9) 102 (45.9) (40.1) 117 (52.7) 2 9 (2.0) 3 (1.4) Disease site, n (%) Visceral a 214 (48.2) 110 (49.5) Non-visceral 230 (51.8) 112 (50.5) Bone-only 103 (23.2) 48 (21.6) No. of disease sites (31.1) 66 (29.7) (26.4) 52 (23.4) (25.2) 61 (27.5) 4 77 (17.3) 43 (19.4) Disease-free interval, b n (%) Newly metastatic disease 167 (37.6) 81 (36.5) 12 months 99 (22.3) 48 (21.6) >12 months 178 (40.1) 93 (41.9)
 II 137 (30.9) 68 (30.6) III 72 (16.2) 39 (17.6) IV 138 (31.1) 72 (32.4) Unknown 36 (8.1) 12 (5.4) Other or data missing a 10 (2.3) 1 (0.5) Recurrence type, n (%) Locoregional 2 (0.5) 2 (0.")
46 PALOMA-2: Demographics and Baseline Characteristics (ITT Population) Disease stage at initial diagnosis, n (%) Palbociclib + letrozole (N=444) Placebo + letrozole (N=222) I 51 (11.5) 30 (13.5) II 137 (30.9) 68 (30.6) III 72 (16.2) 39 (17.6) IV 138 (31.1) 72 (32.4) Unknown 36 (8.1) 12 (5.4) Other or data missing a 10 (2.3) 1 (0.5) Recurrence type, n (%) Locoregional 2 (0.5) 2 (0.9) Local 6 (1.4) 3 (1.4) Regional 3 (0.7) 1 (0.5) Distant 294 (66.2) 145 (65.3) Newly diagnosed 139 (31.3) 71 (32.0) Prior adjuvant or neoadjuvant therapy, n (%) Chemotherapy 213 (48.0) 109 (49.1) Neoadjuvant 54 (12.2) 32 (14.4) Adjuvant 180 (40.5) 89 (40.1) Adjuvant hormonal therapy b 249 (56.1) 126 (56.8) Tamoxifen 209 (47.1) 98 (44.1) Anastrozole 56 (12.6) 29 (13.1) Letrozole 36 (8.1) 16 (7.2) Exemestant 30 (6.8) 13 (5.9) Goserelin 5 (1.1) 6 (2.7) Toremifene 7 (1.6) 1 (0.5) Other 3 (0.7) 4 (1.8)
 HR 0.65 (95% CI 0.51, 0.84) 2-sided P=0.001 Palbociclib + letrozole (n=444) Median (95% CI) PFS 30.")
 Placebo + letrozole (n=222) 0 0 3 6 9 12 15 18 21 24 27 30 33 Time from randomization (months) Number of")
47 PFS: Central Review PFS probability (%) Median (95% CI) PFS 19.3 months ( ) HR 0.65 (95% CI 0.51, 0.84) 2-sided P=0.001 Palbociclib + letrozole (n=444) Median (95% CI) PFS 30.5 months (27.4 NE) Placebo + letrozole (n=222) Time from randomization (months) Number of patients at risk PAL + LET PCB + LET
48 PFS: Subgroups Subgroup Palbociclib Letrozole, n (%) Placebo Letrozole, n (%) HR (95% CI) All randomized patients 444 (100) 222 (100) 0.58 ( ) Age Race Site of metastatic disease at baseline Prior hormonal therapy Disease-free interval Region <65 years 65 years White Asian Visceral a Non-visceral Yes No ECOG performance status 0 1/2 Bone-only disease at baseline Measurable disease Prior chemotherapy Most recent therapy Number of disease sites Histopathological classification Newly metastatic disease 12 months >12 months North America Europe Asia/Pacific Yes No Yes No Yes No Aromatase inhibitor Antiestrogen 1 2 Ductal carcinoma Lobular carcinoma 263 (59.2) 181 (40.8) 344 (77.5) 65 (14.6) 214 (48.2) 230 (51.8) 249 (56.1) 195 (43.9) 167 (37.6) 99 (22.3) 178 (40.1) 168 (37.8) 212 (47.7) 64 (14.4) 257 (57.9) 187 (42.1) 103 (23.2) 341 (76.8) 338 (76.1) 106 (23.9) 213 (48.0) 231 (52.0) 91 (20.5) 154 (34.7) 138 (31.1) 306 (68.9) 356 (80.2) 68 (15.3) 141 (63.5) 81 (36.5) 172 (77.5) 30 (13.5) 110 (49.5) 112 (50.5) 126 (56.8) 96 (43.2) 81 (36.5) 48 (21.6) 93 (41.9) 99 (44.6) 95 (42.8) 28 (12.6) 102 (45.9) 120 (54.1) 48 (21.6) 174 (78.4) 171 (77.0) 51 (23.0) 109 (49.1) 113 (50.9) 44 (19.8) 75 (33.8) 66 (29.7) 156 (70.3) 184 (82.9) 30 (13.5) 0.57 ( ) 0.57 ( ) 0.58 ( ) 0.48 ( ) 0.63 ( ) 0.50 ( ) 0.53 ( ) 0.63 ( ) 0.67 ( ) 0.50 ( ) 0.52 ( ) 0.61 ( ) 0.57 ( ) 0.49 ( ) 0.65 ( ) 0.53 ( ) 0.36 ( ) 0.65 ( ) 0.66 ( ) 0.35 ( ) 0.53 ( ) 0.61 ( ) 0.55 ( ) 0.56 ( ) 0.51 ( ) 0.61 ( ) 0.59 ( ) 0.46 ( ) In favor of PAL + LET In favor of PCB + LET
 Placebo + letrozole (N=222) 444 222 42.1 (37.5 46.9) 84.9 (81.2 88.1) 22.5 (19.8 28.0) 34.7 (28.4 41.3) 70.3 (63.8 76.2) 16.8 c (14.2 28.")
49 PALOMA-2: Overall Response (ITT population) All randomized patients, n ORR, a % (95% CI) CBR, b % (95% CI) Median DoR, months Patients with measurable disease ORR, a % (95% CI) CBR, b % (95% CI) Median DoR, months Palbociclib + letrozole (N=444) Placebo + letrozole (N=222) ( ) 84.9 ( ) 22.5 ( ) 34.7 ( ) 70.3 ( ) 16.8 c ( ) ( ) 84.3 ( ) 22.5 ( ) 44.4 ( ) 70.8 ( ) 16.8 ( ) Odds ratio (95% CI) 1.40 ( ) 2.39 ( ) NR 1.55 ( ) 2.23 ( ) NR 2-sided P value (exact) 0.06 < NR 0.03 <0.001 NR

50

51 PALOMA-2: All-causality Hematological AEs Occurring in 15% of Patients in Either Arm (As-treated Population) Palbociclib + letrozole (N=444) Placebo + letrozole (N=222) Any grade Grade 3 Grade 4 Any grade Grade 3 Grade 4 Any AE, % Neutropenia a Leukopenia Anemia a Thrombocytopenia a
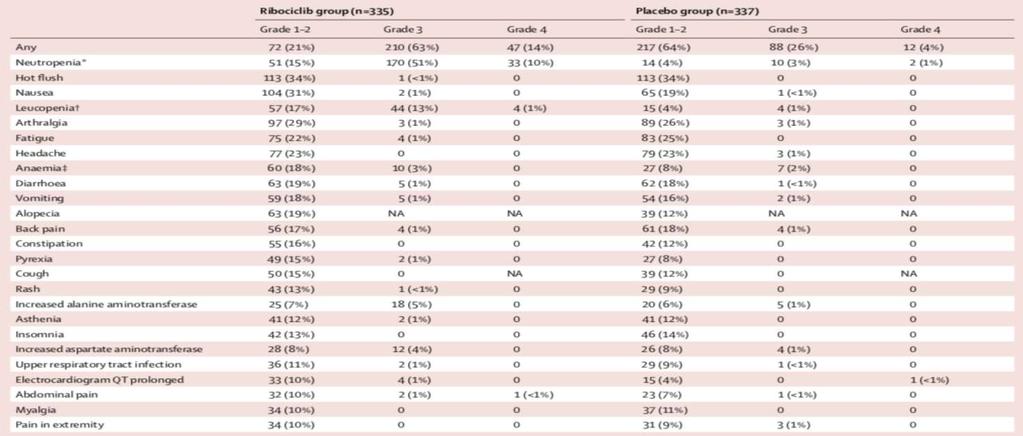
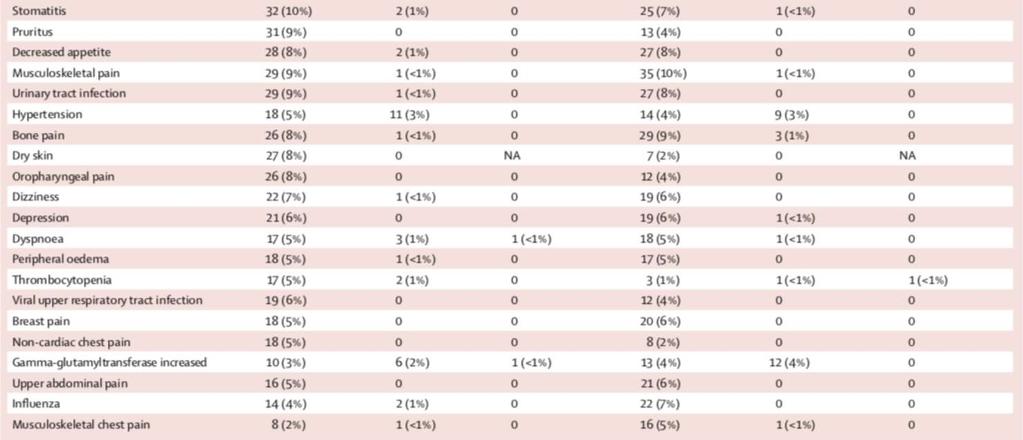
52 Non Hematological AEs (>15%) Palbociclib + letrozole (N=444) Placebo + letrozole (N=222) Any Grade Grade 3 Grade 4 Any Grade Grade 3 Grade 4 Any AE (%) Fatigue Nausea Arthralgia Alopecia a Diarrhea Cough Back pain Headache Hot flush Constipation Rash b Asthenia Vomiting Pain in extremity Stomatitis
53 Quality of Life on Rx





54 A different balance of CDK4 vs. CDK6 may contribute to differential toxicities The unique role of CDK6, rather than CDK4, in hematologic cells indicates that such cells could be more sensitive to CDK6 inhibition vs. CDK4 inhibition Abemaciclib has a different balance of selectivity for CDK4 vs. CDK6 CDK4/Cyclin D1 Ki [ATP] CDK6/Cyclin D3 Ki [ATP] Abemaciclib Palbociclib 0.6 nm 2.9 nm 14X 1.4X 8.2 nm 4.0 nm CDK4>CDK6 CDK4 CDK6 Differential inhibition of CDK4 vs. CDK6 may contribute to: Different toxicological profile vs. other CDK4&6 inhibitors Lower neutropenia Continuous dosing Facilitating sustained target inhibition 1. Scheicher et al. Blood, 2015; 125(1), Laurentix E et al Stem Cell 2015; 16: Torres et al.. Poster presented at AACR Abstract 310
55 POST EVEROLIMUS

56 Post EVEROLIMUS PFS 2.9 mo PALOMA-3 PFS 9.5 mo
57 RIBOCICLIB (Kisqali ) uottawa.ca Faculté de médecine Faculty of Medicine


58 MONALEESA-2: Ribociclib + Letrozole as First-Line Therapy Prolonged PFS in Patients With HR+, HER2 ABC N = 668 Postmenopausal HR+, HER2 ABC No prior therapy for advanced disease Stratification: Presence/absence of liver and/or lung metastases R 1:1 Ribociclib + Letrozole Placebo + Letrozole Endpoints Primary: PFS Secondary: OS ORR CBR ECOG PS deterioration Safety QoL

59 Published on October 8, Hortobagyi G, et al. NEJM, 2016 DOI: /NEJMoa MONALEESA-2: Patient Characteristics
60 MONALEESA-2 ASCO 2017 Update

61 MONALEESA-2 - Subgroups
62 MONALEESA-2:OS Data Immature 100 Probability of OS (%) Ribociclib + Letrozole n=334 Placebo + Letrozole n=334 Number of events, n (%) 50 (15.0) 66 (19.8) Median OS, months (95% CI) NR (NR NR) 33.0 (33.0 NR) Hazard ratio (95% CI) ( ) p value No. at Risk Ribociclib + Letrozole Placebo + Letrozole Time (Months)
63 MONALEESA-2: Duration of Response

64
65 MONALEESA-7 First-Line Therapy With Ribociclib + ET in Premenopausal Women N = 672 Pre/perimenopausal women with HR+, HER2 ABC No prior endocrine therapy for advanced disease 1 line of CT for advanced disease RIBO a + TAM/NSAI + GOS PBO + TAM/NSAI + GOS Primary endpoint: PFS Secondary endpoints: OS, CBR, ORR, safety, TTR, DOR, HRQoL Tripathy D, et al. SABCS Abstract GS2-05 [oral presentation].
66 PFS: Central Review

67 Response Rates
68 Toxicity
69 Toxicity
 97 (49.5) Median PFS, months (95% CI) NR (19.3 NR) 13.0 (12.6 16.5) Hazard ratio (95% CI) 0.535 (0.385 0.742) Ribociclib + Letrozole Placebo + Letrozole No.")
70 Kaplan-Meier Plot of Progression-free Survival in Patients With Visceral Metastases Probability of PFS (%) Ribociclib + Letrozole n=197 Placebo + Letrozole n=196 Number of events, n(%) 58 (29.4) 97 (49.5) Median PFS, months (95% CI) NR (19.3 NR) 13.0 ( ) Hazard ratio (95% CI) ( ) Ribociclib + Letrozole Placebo + Letrozole No. of patients still at risk Time (months) Ribociclib + Letrozole Placebo + Letrozole Mod. Burris H et al. SABCS 2016, Poster Session 4 Treatment: Advanced Therapy Targeted, Abstract No. P
71 ABEMACICLIB uottawa.ca Faculté de médecine Faculty of Medicine

72
73 Monarch-2: Abemaciclib (CDK4/6 inhibitor) + fulvestrant vs. placebo+fulvestrant ER+, HER2- mbc - Postmenopausal women with HR+ HER2-, metastatic BC - Resistant to or discontinued AIs, anti-estrogens, chemo/radio/immunotherapy - Patients who received previous CDK4/6 inhibitors are excluded. - Phase 3 - N=630 Randomization 2:1 Abemaciclib (150 mg once/12hrs in 28d cycle)+ Fulvestrant (500mg on day 1 + day 15 in cycle 1 then Day 1 of cycle 2 and beyond) Placebo (once/12hrs in 28d cycle)+ Fulvestrant (500mg on day 1 + day 15 in cycle 1 then Day 1 of cycle 2 and beyond) Primary endpoint: PFS Secondary endpoint: OS, ORR, DoR, DCR, CBR, PK
74 PFS: Central Review

75

76

77
78

79

80

81


82

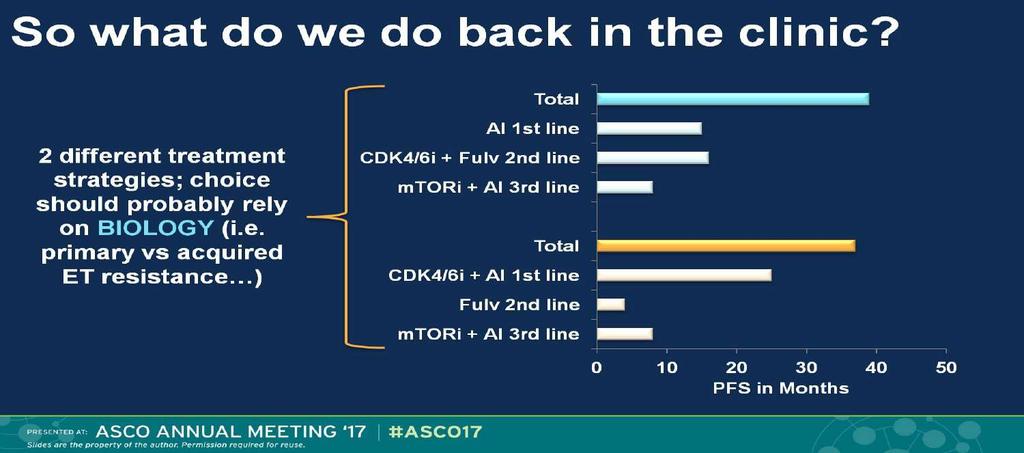
83 Are we changing practice or outcomes?
84 Targeted Rx: PI3K Inhibitors Buparlisib, Apelisib (SOLAR-1), Taselisib (SANDPIPER) uottawa.ca Faculté de médecine Faculty of Medicine
85 ESR1 Mutations and Resistance Mechanisms Frequency, relevance, effective strategies uottawa.ca Faculté de médecine Faculty of Medicine



86 Endocrine therapy resistance may be de novo or acquired 1 Only 30% of patients with metastatic disease have objective regression of tumor with initial endocrine treatment 1 The majority of patients with advanced or metastatic ER-positive disease will acquire resistance within 2-3 years of endocrine therapy 2 Almost all patients with MBC and as many as 40% of patients receiving adjuvant tamoxifen eventually relapse and die from their disease 3 Patients with HR+ MBC are often treated with multiple rounds of hormonal therapy 4 The median PFS for MBC patients treated with 1 st line hormonal therapy is The response rate for MBC patients to 2 nd line hormonal therapy is ~20% ~6-12 MONTHS 4 and declines as more therapy lines are added 4
 can be")

87 ESR1 mutation is emerging as an important mechanism for acquired resistance 1,2 ESR1 mutations are uncommon in treatment-naïve primary tumours, but highly enriched in endocrine resistant HR+ MBC 2,3 Circulating tumor DNA (ctdna) can be analyzed to detect the presence of mutations in the plasma of MBC patients 4 Genetic alteration in primary versus metastatic breast cancer % Rate of ESR1 mutations in patients with metastatic ER+ endocrine-resistant breast cancer 5 Adapted from Jeselsohn 2014

88 Functional and structural analysis has revealed aberrant characteristics of ER mutants: Exhibits enhanced estrogen independent transcriptional activity 1,2 Mutant ERα Confers cell proliferation advantage over WT ER under estrogen deprivation 3 Varying degrees of resistance to endocrine therapies 3,4 E2 ER ER E2 E2 ER E2 ER E2 E2 ER ER Direct estrogen-dependent genomic pathway NUCLEUS Indirect estrogen-independent, genomic pathway ERE Src RTKs ER Non- ERE PI3K Akt ERK ER Ras Amphiregulin TGF-alpha TF TF Akt PI3K Src FAK Non-genomic activity E2 E2 ER ER ER ERK PELP1 Src Rb E2F ER G1 G0 ER Cyclin D1 CDK4/6 CELL CYCLE M CELL MEMBRANE CYTOPLASM Enhanced proliferation and tumor growth P P Rb P E2F S Cyclin D1 G2

89
90 ESR1 Mutation Frequency Across 3 Trials Trial Experimental Comparator Patient population Patients with tumors with at least 1 ESR1 mutation at baseline* PALOMA-3 2,3 Fulvestrant + Palbociclib (n=347) Fulvestrant + Placebo (n=174) HR+, HER2 advanced breast cancer; pre-/peri- or postmenopausal; progressed on prior endocrine therapy; 1 prior chemotherapy regimen for advanced cancer (n=521) 25% (91/360) FERGI 1 Fulvestrant + Pictilisib Fulvestrant + Placebo Postmenopausal women aged 18 years with estrogen receptor +, HER2-negative breast cancer relapsed during or 6 months of AI in the adjuvant setting, or with progression during treatment in the metastatic setting (n=168) 37% (57/153) SoFEA 2 Fulvestrant-containing regimen (n = 474) Exemestane (n = 249) HR+ advanced breast cancer; post-menopausal; Prior sensitivity to AIs (n=723) 39% (63/161) Baseline ESR1 mutations across these 3 trials ranged from 25% to 39%
91 Royal Marsden Study Patients with ESR1 mutations had a significantly shorter PFS on subsequent AI-based therapy ESR1 Mutations Predict Lack of Sensitivity to Subsequent AI Therapy PFS on AI Therapy Progression-Free Survival PFS on Subsequent AI-based Therapy HR, 3.1; 95% CI, p= Years
92 At baseline, 25% of the patient population had an ESR1 mutation ESR1 mutated (n=91) PALOMA-3: 2 nd -line Efficacy Associated with Baseline Incidence of ESR1 Mutation ESR1 wild type (n=269) Fulvestrant + palbociclib improved PFS compared with fulvestrant alone in both ESR1 mutant and wild type patients

93
94 Presented By Ingrid Mayer at 2017 ASCO Annual Meeting Presented By Ingrid Mayer at 2017 ASCO Annual Meeting
95 Endocrine Therapy Modulation: 1 ST LINE PFS Study N Median PFS, months HR (95% CI) P Value MONALEESA PALOMA MONARCH Ribociclib + letrozole: 25.3 Letrozole: 16.3 Palbociclib + letrozole: 24.8 Letrozole: 14.5 Abemaciclib + letrozole: NR Letrozole or anastrozole: ( ) < ( ) < ( ) < PALOMA-3 3 (1st-line subset) 114 Palbociclib + fulvestrant: 9.5 Fulvestrant: ( ) 0.02 BOLERO-2 5 (1st-line subset) 137 Everolimus + exemestane: 11.5 Exemestane: ( ) Not Reported

96



97

98
99 NCCN GUIDELINE

100 Dosing and Adjustments uottawa.ca Faculté de médecine Faculty of Medicine

101 PALBOCICLIB

102 PALBOCICLIB
103 RIBOCICLIB
104 ECG BASELINE DAY 14 PRE CYCLE 2 RIBOCICLIB CONSIDER BASELINE ECG PRE ALL CDK 4/6 INHIBITORS

105 RIBOCICLIB
106 Future Advances Around the corner uottawa.ca Faculté de médecine Faculty of Medicine

107

108
109



110
111

112 LETROZOLE + PALBOCICLIB 68F Past L breast cancer 1992 Past R breast CA 2004 ER/PR + Back pain x 2 mo Mets to T6, sacrum, ribs 3 small lung lesions up to 11 mm Lung bx = ER+ Her2 neg

113 LETROZOLE + PALBOCICLIB 82F with de novo metastatic breast CA Bone mets - multiple Liver mets - multiple up to 3cm Breast mass in situ - 2 cm ER/PR ++ Her 2 negative Mild dementia Atrial fibrillation, controlled

114 ISSUES: rebiopsy on progression value of genomic sequencing? sequencing, funding? Rx beyond progression? OS benefit?
115 THANK YOU Questions, Discussion
RIBOCICLIB EN PRIMERA LINEA DE TRATAMIENTO. Dra. Elena Aguirre H.U. Miguel Servet
 RIBOCICLIB EN PRIMERA LINEA DE TRATAMIENTO Dra. Elena Aguirre H.U. Miguel Servet INTRODUCTION ADVANCED BREAST CANCER HR+/HER2- YES Consider Chemo VISCERAL CRISIS? NO Endocrine Therapy X3 Toxicity Progresive
RIBOCICLIB EN PRIMERA LINEA DE TRATAMIENTO Dra. Elena Aguirre H.U. Miguel Servet INTRODUCTION ADVANCED BREAST CANCER HR+/HER2- YES Consider Chemo VISCERAL CRISIS? NO Endocrine Therapy X3 Toxicity Progresive
Metastatic breast cancer: sequence of therapies
 Metastatic breast cancer: sequence of therapies Clinical Case Discussion Nadia Harbeck, MD PhD Breast Center, Department of Gynecology and Obstetrics University of Munich, Ludwig-Maximilians University
Metastatic breast cancer: sequence of therapies Clinical Case Discussion Nadia Harbeck, MD PhD Breast Center, Department of Gynecology and Obstetrics University of Munich, Ludwig-Maximilians University
TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive metastatic breast cancer
 TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive metastatic breast cancer Marta Bonotto Department of Oncology University Hospital of Udine TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive
TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive metastatic breast cancer Marta Bonotto Department of Oncology University Hospital of Udine TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive
Inibitori delle chinasi ciclino dipendenti nel trattamento della malattia metastatica HR-positiva Gli studi clinici
 Inibitori delle chinasi ciclino dipendenti nel trattamento della malattia metastatica HR-positiva Gli studi clinici Laura Orlando UOC Oncologia & Breast Unit Brindisi Verona 22/04/2016 Summary Studi con
Inibitori delle chinasi ciclino dipendenti nel trattamento della malattia metastatica HR-positiva Gli studi clinici Laura Orlando UOC Oncologia & Breast Unit Brindisi Verona 22/04/2016 Summary Studi con
Endocrine Therapy 2017: Is There a Better Single Agent and when Should we Use it?
 Endocrine Therapy 2017: Is There a Better Single Agent and when Should we Use it? ET1 ET2 ET3 Targeted agent 1 Targeted agent 2 Hope S. Rugo, MD Director, Breast Oncology and Clinical Trials Education
Endocrine Therapy 2017: Is There a Better Single Agent and when Should we Use it? ET1 ET2 ET3 Targeted agent 1 Targeted agent 2 Hope S. Rugo, MD Director, Breast Oncology and Clinical Trials Education
First-Line Ribociclib + Letrozole for Postmenopausal Women With HR+, HER2-, Advanced Breast Cancer: First Results From the Phase III MONALEESA-2 Study
 First-Line Ribociclib + Letrozole for Postmenopausal Women With HR+, HER2-, Advanced Breast Cancer: First Results From the Phase III MONALEESA-2 Study Abstract LBA1 Hortobagyi GN, Stemmer SM, Burris HA,
First-Line Ribociclib + Letrozole for Postmenopausal Women With HR+, HER2-, Advanced Breast Cancer: First Results From the Phase III MONALEESA-2 Study Abstract LBA1 Hortobagyi GN, Stemmer SM, Burris HA,
Mechanisms of hormone drug resistance
 Mechanisms of hormone drug resistance Ljiljana Stamatović Institute for Oncology and Radiology of Serbia Tenth UMOS Conference, Belgrade, 16-17 th May 2015. Hormone receptor-positive breast cancer (HR+
Mechanisms of hormone drug resistance Ljiljana Stamatović Institute for Oncology and Radiology of Serbia Tenth UMOS Conference, Belgrade, 16-17 th May 2015. Hormone receptor-positive breast cancer (HR+
Targeting CDK 4/6. Jee Hyun Kim, M.D., Ph.D. Seoul National University College of Medicine
 2016.04.30 GBCC Education Symposium Targeting CDK 4/6 Jee Hyun Kim, M.D., Ph.D. Seoul National University College of Medicine Contents Cyclins -CDKs in cell cycle control CDK 4/6 in breast cancer Preclinical
2016.04.30 GBCC Education Symposium Targeting CDK 4/6 Jee Hyun Kim, M.D., Ph.D. Seoul National University College of Medicine Contents Cyclins -CDKs in cell cycle control CDK 4/6 in breast cancer Preclinical
Recent advances in the management of metastatic breast cancer in older adults
 Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Multimedia Appendix 6 Educational Materials Table of Contents. Intervention Educational Materials Audio Script (version 1)
") Multimedia Appendix 6 Educational Materials Table of Contents Intervention Educational Materials... 1 Audio Script (version 1)... 1 Text (version 1)... 5 Slides (version 1)... 17 Audio Script (version
Multimedia Appendix 6 Educational Materials Table of Contents Intervention Educational Materials... 1 Audio Script (version 1)... 1 Text (version 1)... 5 Slides (version 1)... 17 Audio Script (version
What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland
 What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland Outline Early breast cancer Advanced breast cancer Open questions Outline Early breast cancer
What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland Outline Early breast cancer Advanced breast cancer Open questions Outline Early breast cancer
Agents in the Treatment of ER+ Aromatase Inbitor-Resistant Metastatic Breast Cancer: M-THOR Inhibitors
 Agents in the Treatment of ER+ Aromatase Inbitor-Resistant Metastatic Breast Cancer: M-THOR Inhibitors Valero, M.D., Professor of Medicine and Deputy Chairman Department of Breast Medical Oncology The
Agents in the Treatment of ER+ Aromatase Inbitor-Resistant Metastatic Breast Cancer: M-THOR Inhibitors Valero, M.D., Professor of Medicine and Deputy Chairman Department of Breast Medical Oncology The
Update mbc. endokrine Therapie
 Update mbc endokrine Therapie HR neg ER pos Endokrine Resistenz Endokrine Therapie 1 st line Postmenopause AI/Tam/Fulvestrant 84% AI+ Fulvestrant 33% AI (Tam) + Everolimus 84% AI + CDK4/6 92% Prämenopause
Update mbc endokrine Therapie HR neg ER pos Endokrine Resistenz Endokrine Therapie 1 st line Postmenopause AI/Tam/Fulvestrant 84% AI+ Fulvestrant 33% AI (Tam) + Everolimus 84% AI + CDK4/6 92% Prämenopause
Novel Strategies in Systemic Therapies: Overcoming Endocrine Therapy Resistance
 Novel Strategies in Systemic Therapies: Overcoming Endocrine Therapy Resistance Richard S. Finn, MD Division of Hematology/ Oncology Director, Translational Oncology Laboratory Geffen School of Medicine
Novel Strategies in Systemic Therapies: Overcoming Endocrine Therapy Resistance Richard S. Finn, MD Division of Hematology/ Oncology Director, Translational Oncology Laboratory Geffen School of Medicine
Outline of the presentation
 Outline of the presentation Breast cancer subtypes and classification Clinical need in estrogen-positive (ER+) metastatic breast cancer (mbc) Sulforaphane and SFX-01: the preclinical evidence STEM Phase
Outline of the presentation Breast cancer subtypes and classification Clinical need in estrogen-positive (ER+) metastatic breast cancer (mbc) Sulforaphane and SFX-01: the preclinical evidence STEM Phase
Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology, Emory University, Chief of
 Endocrine Therapy of Advanced Breast Cancer School of Breast Oncology November 9 th 2013 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology,
Endocrine Therapy of Advanced Breast Cancer School of Breast Oncology November 9 th 2013 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology,
Breast cancer update. Iryna Kuchuk, MD Oncology department Meir Medical Center
 Breast cancer update Iryna Kuchuk, MD Oncology department Meir Medical Center Overview Cancer Death Rates* Among Women, US,1930-2009 Factors Associated with Reduction In Breast Cancer Mortality Early
Breast cancer update Iryna Kuchuk, MD Oncology department Meir Medical Center Overview Cancer Death Rates* Among Women, US,1930-2009 Factors Associated with Reduction In Breast Cancer Mortality Early
Endocrine Therapy for Advanced Breast Cancer (ABC) Dr Yoon-Sim YAP Division of Medical Oncology, National Cancer Centre Singapore
 Dr Yoon-Sim YAP Division of Medical Oncology, National Cancer Centre Singapore") Endocrine Therapy for Advanced Breast Cancer (ABC) Dr Yoon-Sim YAP Division of Medical Oncology, National Cancer Centre Singapore Outline Guidelines and Evolving Clinical Treatment Landscape for HR+ HER2-
Endocrine Therapy for Advanced Breast Cancer (ABC) Dr Yoon-Sim YAP Division of Medical Oncology, National Cancer Centre Singapore Outline Guidelines and Evolving Clinical Treatment Landscape for HR+ HER2-
Cancers du Sein Métastatiques
 Cancers du Sein Métastatiques Véronique Diéras Journée Laurence Leroyer Rennes 18 mai 2018 Plan ESME Inhibiteurs CDK 4/6 RH+ Inhibiteurs PARP Anticorps drogue-conjugués Perspectives 2018-2019 ESME Time
Cancers du Sein Métastatiques Véronique Diéras Journée Laurence Leroyer Rennes 18 mai 2018 Plan ESME Inhibiteurs CDK 4/6 RH+ Inhibiteurs PARP Anticorps drogue-conjugués Perspectives 2018-2019 ESME Time
When is Chemotherapy indicated in Advanced Luminal Breast Cancer?
 When is Chemotherapy indicated in Advanced Luminal Breast Cancer? Soo-Chin Lee Head & Senior Consultant Department of Haematology-Oncology Clinical Care National University Cancer Institute, Singapore
When is Chemotherapy indicated in Advanced Luminal Breast Cancer? Soo-Chin Lee Head & Senior Consultant Department of Haematology-Oncology Clinical Care National University Cancer Institute, Singapore
Case #2: Hormonal Therapy for Advanced Premenopausal Breast Cancer
 Case #2: Hormonal Therapy for Advanced Premenopausal Breast Cancer Fellow Presenter: Katherine Clifton, MD Faculty Discussant: Debu Tripathy, MD 7 th Annual June 1, 2018 Topics to Be Discussed: Staging
Case #2: Hormonal Therapy for Advanced Premenopausal Breast Cancer Fellow Presenter: Katherine Clifton, MD Faculty Discussant: Debu Tripathy, MD 7 th Annual June 1, 2018 Topics to Be Discussed: Staging
Manejo do câncer de mama RH+ na adjuvância: o que há de novo?
 II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico Manejo do câncer de mama RH+ na adjuvância: o que há de novo? INGRID A. MAYER, MD, MSCI Assistant Professor of Medicine Director,
II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico Manejo do câncer de mama RH+ na adjuvância: o que há de novo? INGRID A. MAYER, MD, MSCI Assistant Professor of Medicine Director,
Karcinom dojke. PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski
 Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Update on New Perspectives in Endocrine-Sensitive Breast Cancer. James R. Waisman, MD
 Update on New Perspectives in Endocrine-Sensitive Breast Cancer James R. Waisman, MD Nothing to disclose DISCLOSURE TAILORx Oncotype Recurrence Score TAILORx Study Design Sparano, J Clin Oncol 2008;26:721-728
Update on New Perspectives in Endocrine-Sensitive Breast Cancer James R. Waisman, MD Nothing to disclose DISCLOSURE TAILORx Oncotype Recurrence Score TAILORx Study Design Sparano, J Clin Oncol 2008;26:721-728
Sesiones interhospitalarias de cáncer de mama. Revisión bibliográfica 4º trimestre 2015
 Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
Management of hormone-receptor positive human epidermal receptor 2 negative advanced or metastatic breast cancers
 Review Article Page 1 of 10 Management of hormone-receptor positive human epidermal receptor 2 negative advanced or metastatic breast cancers Roger K. C. Ngan Department of Clinical Oncology, Queen Elizabeth
Review Article Page 1 of 10 Management of hormone-receptor positive human epidermal receptor 2 negative advanced or metastatic breast cancers Roger K. C. Ngan Department of Clinical Oncology, Queen Elizabeth
Highlitghs in MBC First and second line endocrine treatments. Antonio Frassoldati Oncologia Clinica Ferrara
 Highlitghs in MBC First and second line endocrine treatments Antonio Frassoldati Oncologia Clinica Ferrara Which clinical scenario have to face First line therapy with today? Untreated metastatic breast
Highlitghs in MBC First and second line endocrine treatments Antonio Frassoldati Oncologia Clinica Ferrara Which clinical scenario have to face First line therapy with today? Untreated metastatic breast
Overcoming resistance to endocrine or HER2-directed therapy
 Overcoming resistance to endocrine or HER2-directed therapy Jane Lowe Meisel, MD Assistant Professor of Hematology and Medical Oncology Winship Cancer Institute at Emory University 1 Background While most
Overcoming resistance to endocrine or HER2-directed therapy Jane Lowe Meisel, MD Assistant Professor of Hematology and Medical Oncology Winship Cancer Institute at Emory University 1 Background While most
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents
 Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Terapia adiuvante con inibitori delle Kinasi Cliclina Dipendenti 4/6: quale futuro? Filippo Montemurro
 Terapia adiuvante con inibitori delle Kinasi Cliclina Dipendenti 4/6: quale futuro? Filippo Montemurro Unit of Investigative Clinical Oncology Istituto di Candiolo (IRCCS) Disclosures Speaker s Honoraria
Terapia adiuvante con inibitori delle Kinasi Cliclina Dipendenti 4/6: quale futuro? Filippo Montemurro Unit of Investigative Clinical Oncology Istituto di Candiolo (IRCCS) Disclosures Speaker s Honoraria
Page. Objectives: Hormone Therapy Resistance: Challenges and Opportunities. Research Support From Merck
 Hormone Therapy Resistance: Challenges and Opportunities Pamela. N. Munster, MD University of California, San Francisco Financial Disclosures Research Support From Merck Objectives: Understanding the current
Hormone Therapy Resistance: Challenges and Opportunities Pamela. N. Munster, MD University of California, San Francisco Financial Disclosures Research Support From Merck Objectives: Understanding the current
10/15/2012. Overcoming Endocrine Therapy Resistance. The Problem in ER+ Tumors is Endocrine Therapy Resistance
 Overcoming Endocrine Therapy Resistance Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology Slide Credits: Hope Rugo, MD The Problem in ER+ Tumors is Endocrine Therapy Resistance
Overcoming Endocrine Therapy Resistance Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology Slide Credits: Hope Rugo, MD The Problem in ER+ Tumors is Endocrine Therapy Resistance
Mechanisms of Resistance to. Lisa A. Carey, M.D. University of North Carolina at Chapel Hill Lineberger Comprehensive Cancer Center
 Mechanisms of Resistance to Hormonal Therapy Lisa A. Carey, M.D. University of North Carolina at Chapel Hill Lineberger Comprehensive Cancer Center Antagonizing Estrogen Dependent Growth Premenopausal
Mechanisms of Resistance to Hormonal Therapy Lisa A. Carey, M.D. University of North Carolina at Chapel Hill Lineberger Comprehensive Cancer Center Antagonizing Estrogen Dependent Growth Premenopausal
Collaborative Management of Patients With Advanced Estrogen Receptor Positive Breast Cancer
 Collaborative Management of Patients With Advanced Estrogen Receptor Positive Breast Cancer Lee Schwartzberg, MD, FACP Heather Greene, FNP, AOCNP West Cancer Center Memphis, Tennessee Learning Objectives
Collaborative Management of Patients With Advanced Estrogen Receptor Positive Breast Cancer Lee Schwartzberg, MD, FACP Heather Greene, FNP, AOCNP West Cancer Center Memphis, Tennessee Learning Objectives
Enhancing Endocrine Therapy for Hormone Receptor Positive Advanced Breast Cancer
 Enhancing Endocrine Therapy for Hormone Receptor Positive Advanced Breast Cancer Sung-Bae Kim, MD, PhD Professor, Dept of Oncology, Asan Medical Center University of Ulsan College of Medicine Seoul, Korea
Enhancing Endocrine Therapy for Hormone Receptor Positive Advanced Breast Cancer Sung-Bae Kim, MD, PhD Professor, Dept of Oncology, Asan Medical Center University of Ulsan College of Medicine Seoul, Korea
Breast Cancer: ASCO Poster Review
 Breast Cancer: ASCO Poster Review Carmen Criscitiello, MD, PhD Istituto Europeo di Oncologia Milano HER2+ SUBTYPE Research questions in early HER2+ BC De-escalation of toxicity without compromising efficacy
Breast Cancer: ASCO Poster Review Carmen Criscitiello, MD, PhD Istituto Europeo di Oncologia Milano HER2+ SUBTYPE Research questions in early HER2+ BC De-escalation of toxicity without compromising efficacy
Current Optimal Sequence and Duration of Endocrine Treatment
 [Symposium 7] Present and Future of Endocrine Therapy 07 Apr, 2018@GBCC Current Optimal Sequence and Duration of Endocrine Treatment Breast Oncology Center The Cancer Institute Hospital of JFCR Shinji
[Symposium 7] Present and Future of Endocrine Therapy 07 Apr, 2018@GBCC Current Optimal Sequence and Duration of Endocrine Treatment Breast Oncology Center The Cancer Institute Hospital of JFCR Shinji
pan-canadian Oncology Drug Review Final Clinical Guidance Report Everolimus (Afinitor) for Advanced Breast Cancer March 25, 2013
 for Advanced Breast Cancer March 25, 2013") pan-canadian Oncology Drug Review Final Clinical Guidance Report Everolimus (Afinitor) for Advanced Breast Cancer March 25, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Everolimus (Afinitor) for Advanced Breast Cancer March 25, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
Online-Only Supplementary Materials
 Online-Only Supplementary Materials Online-Only Supplementary Methods: Eligibility Criteria and Study Endpoints and Assessments Supplementary Table 1. Demographic and Baseline Characteristics in Patients
Online-Only Supplementary Materials Online-Only Supplementary Methods: Eligibility Criteria and Study Endpoints and Assessments Supplementary Table 1. Demographic and Baseline Characteristics in Patients
Introduction. Ahmad Radzi 1*, Fabian Wei Luen Lee 2 REVIEW ARTICLE
 doi: 10.18282/amor.v4.i1.255 REVIEW ARTICLE Optimizing treatment-sequencing strategies for the management of postmenopausal women with hormone receptor-positive, HER2-negative advanced breast cancer: A
doi: 10.18282/amor.v4.i1.255 REVIEW ARTICLE Optimizing treatment-sequencing strategies for the management of postmenopausal women with hormone receptor-positive, HER2-negative advanced breast cancer: A
Endocrine Therapy of Advanced Breast Cancer School of Breast Oncology November 2012
 Endocrine Therapy of Advanced Breast Cancer School of Breast Oncology November 2012 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology,
Endocrine Therapy of Advanced Breast Cancer School of Breast Oncology November 2012 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology,
Predicting outcome in metastatic breast cancer
 Predicting outcome in metastatic breast cancer Aleix Prat, MD, PhD Medical Oncology Department Translational Genomics and Targeted Therapeutics in Solid Tumors Monday, 15 th January, Manchester, UK Disclosures
Predicting outcome in metastatic breast cancer Aleix Prat, MD, PhD Medical Oncology Department Translational Genomics and Targeted Therapeutics in Solid Tumors Monday, 15 th January, Manchester, UK Disclosures
Session Breast Cancer. Alessandra Fabi Il punto di vista dell esperto
 Session Breast Cancer Alessandra Fabi Il punto di vista dell esperto Roma 6-7.10.2017 The Importance of Understanding What Disease to Treat Cejalvo et al, Cancer Res 2017 Skyline Chaging at evolution of
Session Breast Cancer Alessandra Fabi Il punto di vista dell esperto Roma 6-7.10.2017 The Importance of Understanding What Disease to Treat Cejalvo et al, Cancer Res 2017 Skyline Chaging at evolution of
Updates From San Antonio Breast Cancer Symposium 2017
 Updates From San Antonio Breast Cancer Symposium 2017 Rob Coleman University of Sheffield Presentation Outline New Insights into adjuvant endocrine treatment Duration of treatment Perioperative therapy
Updates From San Antonio Breast Cancer Symposium 2017 Rob Coleman University of Sheffield Presentation Outline New Insights into adjuvant endocrine treatment Duration of treatment Perioperative therapy
Metastatic Breast Cancer What is new? Subtypes and variation?
 Metastatic Breast Cancer What is new? Subtypes and variation? Anne Blaes, MD, MS University of Minnesota, Division of Hematology/Oncology Director, Adult Cancer Survivor Program Current estimates for metastatic
Metastatic Breast Cancer What is new? Subtypes and variation? Anne Blaes, MD, MS University of Minnesota, Division of Hematology/Oncology Director, Adult Cancer Survivor Program Current estimates for metastatic
NSABP: FB-11. Shannon Puhalla, MD
 NSABP: FB-11 Phase II Randomized Study Evaluating the Biological and Clinical Effects of the Combination of Palbociclib with Letrozole as Neoadjuvant Therapy in Post- Menopausal Women with Estrogen Receptor
NSABP: FB-11 Phase II Randomized Study Evaluating the Biological and Clinical Effects of the Combination of Palbociclib with Letrozole as Neoadjuvant Therapy in Post- Menopausal Women with Estrogen Receptor
Update on the Management of HER2+ Breast Cancer. Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany
 Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Endocrine treatment might NOT be the preferred option in Hrpos MBC. Dr. Mircea Dediu Sanador Hospital Bucharest Summer School Bucharest 2015
 Endocrine treatment might NOT be the preferred option in Hrpos MBC Dr. Mircea Dediu Sanador Hospital Bucharest Summer School Bucharest 2015 Overall survival not improved by the AI treatment Benefit in
Endocrine treatment might NOT be the preferred option in Hrpos MBC Dr. Mircea Dediu Sanador Hospital Bucharest Summer School Bucharest 2015 Overall survival not improved by the AI treatment Benefit in
Disease Update: Metastatic Breast Cancer
 Disease Update: Metastatic Breast Cancer Aimee Faso, PharmD, BCOP, CPP Oncology Clinical Specialist, GI/Breast UNC Hospitals and Clinics August 2015 Objectives Identify treatment choices of metastatic
Disease Update: Metastatic Breast Cancer Aimee Faso, PharmD, BCOP, CPP Oncology Clinical Specialist, GI/Breast UNC Hospitals and Clinics August 2015 Objectives Identify treatment choices of metastatic
Her 2 Positive Advanced Breast Cancer: From Evidence to Practice
 Her 2 Positive Advanced Breast Cancer: From Evidence to Practice Sunil Verma MD, FRCP(C) Medical Director, Tom Baker Cancer Center Professor and Head, Department of Oncology Cumming School of Medicine,
Her 2 Positive Advanced Breast Cancer: From Evidence to Practice Sunil Verma MD, FRCP(C) Medical Director, Tom Baker Cancer Center Professor and Head, Department of Oncology Cumming School of Medicine,
The next wave of successful drug therapy strategies in HER2-positive breast cancer. Hans Wildiers University Hospitals Leuven Belgium
 The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
Pro: Hormone Therapy in HR positive MBC is the preferred option!
 Pro: Hormone Therapy in HR positive MBC is the preferred option! Alexandru Eniu, MD, PhD Medical Oncologist Head, Day Hospital Unit Department of Breast Tumors Cancer Institute Ion Chiricuţă Cluj-Napoca,
Pro: Hormone Therapy in HR positive MBC is the preferred option! Alexandru Eniu, MD, PhD Medical Oncologist Head, Day Hospital Unit Department of Breast Tumors Cancer Institute Ion Chiricuţă Cluj-Napoca,
Optimization of Hormone Treatment: New Alternative Sequences
 Optimization of Hormone Treatment: New Alternative Sequences ET1 ET2 ET3 Targeted agent 1 Targeted agent 2 Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education
Optimization of Hormone Treatment: New Alternative Sequences ET1 ET2 ET3 Targeted agent 1 Targeted agent 2 Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education
Aggiornamenti tra ricerca e clinica: il carcinoma della mammella
 Aggiornamenti tra ricerca e clinica: il carcinoma della mammella Filippo Montemurro Unit of (INCO) Fondazione del Piemonte per l Oncologia Candiolo Cancer Institute (IRCCs) Research Needs in Breast Cancer
Aggiornamenti tra ricerca e clinica: il carcinoma della mammella Filippo Montemurro Unit of (INCO) Fondazione del Piemonte per l Oncologia Candiolo Cancer Institute (IRCCs) Research Needs in Breast Cancer
ASCO 2018 Breast Cancer Highlights
 ASCO 2018 Breast Cancer Highlights Angie DeMichele, MD, MSCE Jill & Alan Miller Endowed Chair in Breast Cancer Excellence Professor of Medicine and Epidemiology Co-Leader, Breast Cancer Program, Abramson
ASCO 2018 Breast Cancer Highlights Angie DeMichele, MD, MSCE Jill & Alan Miller Endowed Chair in Breast Cancer Excellence Professor of Medicine and Epidemiology Co-Leader, Breast Cancer Program, Abramson
CDK 4/6 Inhibitors: Efficacy and Side Effect Profile
 CDK 4/6 Inhibitors: Efficacy and Side Effect Profile Univ.-Prof. Dr. Christian F Singer, MPH Center for Breast Health, Medical University of Vienna Center for Familial Breast- and Ovarian Cancer, MUW Christian
CDK 4/6 Inhibitors: Efficacy and Side Effect Profile Univ.-Prof. Dr. Christian F Singer, MPH Center for Breast Health, Medical University of Vienna Center for Familial Breast- and Ovarian Cancer, MUW Christian
Highlights of. Metastatic & Advanced Breast Cancer
 Highlights of Metastatic & Advanced Breast Cancer 1 Financial Disclosure(s) I currently have or have had the following relevant financial relations to disclose: Speaker s Bureau: Novartis 2 Off Label Use
Highlights of Metastatic & Advanced Breast Cancer 1 Financial Disclosure(s) I currently have or have had the following relevant financial relations to disclose: Speaker s Bureau: Novartis 2 Off Label Use
Extended Hormonal Therapy
 Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
Treatment of Metastatic Breast Cancer. Prof RCCoombes Imperial College London
 Treatment of Metastatic Breast Cancer Prof RCCoombes Imperial College London Metastatic Breast Cancer: General Guidelines Specialized oncology nurses (if possible specialized breast nurses) should be part
Treatment of Metastatic Breast Cancer Prof RCCoombes Imperial College London Metastatic Breast Cancer: General Guidelines Specialized oncology nurses (if possible specialized breast nurses) should be part
Optimizing therapy selection in ER[+] HER2[-] Advanced Breast Cancer
![Optimizing therapy selection in ER[+] HER2[-] Advanced Breast Cancer](/thumbs/77/76517551.jpg "Optimizing therapy selection in ER[+] HER2[-] Advanced Breast Cancer") Optimizing therapy selection in ER[+] HER2[-] Advanced Breast Cancer Dr Antonio Llombart-Cussac, MD, PhD Medical Oncology Division Hospital Arnau Vilanova, Valencia, Spain Disclaimer The contents herein
Optimizing therapy selection in ER[+] HER2[-] Advanced Breast Cancer Dr Antonio Llombart-Cussac, MD, PhD Medical Oncology Division Hospital Arnau Vilanova, Valencia, Spain Disclaimer The contents herein
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID
 DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
Pharmacology Updates in Breast Cancer Chris Vaklavas, M.D.
 Pharmacology Updates in Breast Cancer Chris Vaklavas, M.D. Assistant Professor Department of Medicine, Division of Hematology/Oncology University of Alabama at Birmingham NP2540M 1802 6th Avenue South
Pharmacology Updates in Breast Cancer Chris Vaklavas, M.D. Assistant Professor Department of Medicine, Division of Hematology/Oncology University of Alabama at Birmingham NP2540M 1802 6th Avenue South
Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer
 Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer Sara A. Hurvitz, MD, FACP Associate Professor of Medicine University of California Los Angeles Los Angeles, California Trastuzumab
Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer Sara A. Hurvitz, MD, FACP Associate Professor of Medicine University of California Los Angeles Los Angeles, California Trastuzumab
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings. Eve Rodler, MD University of California at Davis October 2016
 Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
Recent Update in Management of Breast Cancer: Medical Oncology. Jin Hee Ahn, M.D., PhD. 23-April-2015
 2015 GBCC & 4 th IBCS 1/37 Recent Update in Management of Breast Cancer: Medical Oncology Jin Hee Ahn, M.D., PhD. 23-April-2015 Department of Oncology, Asan Medical Center, UUCM, Seoul, Korea 2/37 3/37
2015 GBCC & 4 th IBCS 1/37 Recent Update in Management of Breast Cancer: Medical Oncology Jin Hee Ahn, M.D., PhD. 23-April-2015 Department of Oncology, Asan Medical Center, UUCM, Seoul, Korea 2/37 3/37
Oncology. A CME-certified Supplement to the. Journal of the National Comprehensive Cancer Network. Program Overview/Statement of Need
 JNCCN Volume 16 1 Journal of the National Comprehensive Cancer Network A CME-certified to the Journal of the National Comprehensive Cancer Network Program Overview/Statement of Need Recently updated guidelines
JNCCN Volume 16 1 Journal of the National Comprehensive Cancer Network A CME-certified to the Journal of the National Comprehensive Cancer Network Program Overview/Statement of Need Recently updated guidelines
Verzenio (abemaciclib) NEW PRODUCT SLIDESHOW
 NEW PRODUCT SLIDESHOW") Verzenio (abemaciclib) NEW PRODUCT SLIDESHOW Introduction Brand name: Verzenio Generic name: Abemaciclib Pharmacological class: Kinase inhibitor Strength and Formulation: 50mg, 100mg, 150mg, 200mg; tabs
Verzenio (abemaciclib) NEW PRODUCT SLIDESHOW Introduction Brand name: Verzenio Generic name: Abemaciclib Pharmacological class: Kinase inhibitor Strength and Formulation: 50mg, 100mg, 150mg, 200mg; tabs
ORMONOTERAPIA ADIUVANTE: QUALE LA DURATA OTTIMALE? MARIANTONIETTA COLOZZA
 ORMONOTERAPIA ADIUVANTE: QUALE LA DURATA OTTIMALE? MARIANTONIETTA COLOZZA THE NATURAL HISTORY OF HORMONE RECEPTOR- POSITIVE BREAST CANCER IS VERY LONG Recurrence hazard rate 0.3 0.2 0.1 0 ER+ (n=2,257)
ORMONOTERAPIA ADIUVANTE: QUALE LA DURATA OTTIMALE? MARIANTONIETTA COLOZZA THE NATURAL HISTORY OF HORMONE RECEPTOR- POSITIVE BREAST CANCER IS VERY LONG Recurrence hazard rate 0.3 0.2 0.1 0 ER+ (n=2,257)
Edith A. Perez, Ahmad Awada, Joyce O Shaughnessy, Hope Rugo, Chris Twelves, Seock-Ah Im, Carol Zhao, Ute Hoch, Alison L. Hannah, Javier Cortes
 BEACON: A Phase 3 Open-label, Randomized, Multicenter Study of Etirinotecan Pegol (EP) versus Treatment of Physician s Choice (TPC) in Patients With Locally Recurrent or Metastatic Breast Cancer Previously
BEACON: A Phase 3 Open-label, Randomized, Multicenter Study of Etirinotecan Pegol (EP) versus Treatment of Physician s Choice (TPC) in Patients With Locally Recurrent or Metastatic Breast Cancer Previously
abstract n engl j med 375;20 nejm.org November 17,
 The new england journal of medicine established in 1812 November 17, 2016 vol. 375 no. 20 Palbociclib and Letrozole in Advanced Breast Cancer Richard S. Finn, M.D., Miguel Martin, M.D., Hope S. Rugo, M.D.,
The new england journal of medicine established in 1812 November 17, 2016 vol. 375 no. 20 Palbociclib and Letrozole in Advanced Breast Cancer Richard S. Finn, M.D., Miguel Martin, M.D., Hope S. Rugo, M.D.,
Hormonal Management of Metastatic Breast Cancer
 Hormonal Management of Metastatic Breast Cancer Dr. Khaled Abulkhair, PhD Medical Oncology SCE, Royal College, UK Ass. Professor of Clinical Oncology Mansoura University, Egypt Case For Discussion A 63
Hormonal Management of Metastatic Breast Cancer Dr. Khaled Abulkhair, PhD Medical Oncology SCE, Royal College, UK Ass. Professor of Clinical Oncology Mansoura University, Egypt Case For Discussion A 63
PI3K/AKT/mTOR Inhibitors in Breast Cancer
 PI3K/AKT/mTOR Inhibitors in Breast Cancer Dr Yoon-Sim YAP Division of Medical Oncology, National Cancer Centre Singapore Global Breast Cancer Conference 2015 Outline Overview of PI3K/Akt/mTOR Pathway Rationale
PI3K/AKT/mTOR Inhibitors in Breast Cancer Dr Yoon-Sim YAP Division of Medical Oncology, National Cancer Centre Singapore Global Breast Cancer Conference 2015 Outline Overview of PI3K/Akt/mTOR Pathway Rationale
HER2-Targeted Rx. An Historical Perspective
 HER2-Targeted Rx An Historical Perspective Trastuzumab: Front Line Rx for MBC Median 20.3 v. 25.1 mo P = 0.046 HR 0.8 65% of control patients crossed over Slamon D, et al. N Engl J Med, 2001; 344:783 Trastuzumab:Front-line
HER2-Targeted Rx An Historical Perspective Trastuzumab: Front Line Rx for MBC Median 20.3 v. 25.1 mo P = 0.046 HR 0.8 65% of control patients crossed over Slamon D, et al. N Engl J Med, 2001; 344:783 Trastuzumab:Front-line
Clinical Spotlight Key Advances in Hormone Receptor Positive Breast Cancer: Updates From the 2018 Oncology Annual Meeting in Chicago
 Clinical Spotlight Key Advances in Hormone Receptor Positive Breast Cancer: Updates From the 2018 Oncology Annual Meeting in Chicago Reference Slide Deck Abstract 1000 Abstract 1001 Abstract 1002 Abstract
Clinical Spotlight Key Advances in Hormone Receptor Positive Breast Cancer: Updates From the 2018 Oncology Annual Meeting in Chicago Reference Slide Deck Abstract 1000 Abstract 1001 Abstract 1002 Abstract
Management of Hormone Receptor Positive Metastatic Breast Cancer
 Management of Hormone Receptor Positive Metastatic Breast Cancer Adam Brufsky, MD, PhD Professor of Medicine University of Pittsburgh Improving Outcomes for Metastatic Breast Cancer Giordano SH 24 Chia
Management of Hormone Receptor Positive Metastatic Breast Cancer Adam Brufsky, MD, PhD Professor of Medicine University of Pittsburgh Improving Outcomes for Metastatic Breast Cancer Giordano SH 24 Chia
LA MALATTIA METASTATICA. La malattia HR positiva/her2 negativa: quale terapia di I linea? Come scegliere? Jennifer Foglietta P.O.
 LA MALATTIA METASTATICA La malattia HR positiva/her2 negativa: quale terapia di I linea? Come scegliere? Jennifer Foglietta P.O. Narni-Amelia (TR) Outline Re-testing metastatic disease Chemo- vs endocrine-therapy
LA MALATTIA METASTATICA La malattia HR positiva/her2 negativa: quale terapia di I linea? Come scegliere? Jennifer Foglietta P.O. Narni-Amelia (TR) Outline Re-testing metastatic disease Chemo- vs endocrine-therapy
MEDICAL ONCOLOGY NEWS IN BREAST CANCER 2014
 MEDICAL ONCOLOGY NEWS IN BREAST CANCER 2014 Dr Thomas Yau Clinical Assistant Professor MBBS(HK), MRCP (UK), FHKCP (Med Onc), FHKAM( Medicine), FRCP(London) Queen Mary Hospital The University of Hong Kong
MEDICAL ONCOLOGY NEWS IN BREAST CANCER 2014 Dr Thomas Yau Clinical Assistant Professor MBBS(HK), MRCP (UK), FHKCP (Med Onc), FHKAM( Medicine), FRCP(London) Queen Mary Hospital The University of Hong Kong
Metronomic chemotherapy for breast cancer
 Metronomic chemotherapy for breast cancer M. Colleoni International Breast Cancer Study Group (IBCSG), Division of Medical Senology, European Institute of Oncology Metronomic Scheduling and Inhibition
Metronomic chemotherapy for breast cancer M. Colleoni International Breast Cancer Study Group (IBCSG), Division of Medical Senology, European Institute of Oncology Metronomic Scheduling and Inhibition
ASCO 2017 WEBCAST. Elacestrant (RAD1901) June, 4, 2017
 June, 4, 2017") ASCO 2017 WEBCAST Elacestrant (RAD1901) June, 4, 2017 NASDAQ: RDUS Disclaimer: RAD1901 is an investigational agent Please refer to the ASCO 2017 poster for complete details Safe Harbor Any statements made
ASCO 2017 WEBCAST Elacestrant (RAD1901) June, 4, 2017 NASDAQ: RDUS Disclaimer: RAD1901 is an investigational agent Please refer to the ASCO 2017 poster for complete details Safe Harbor Any statements made
Post-ASCO 2017 Cancer du sein Triple Négatif
 Post-ASCO 217 Cancer du sein Triple Négatif A.Ladjeroud, K.Bouzid Centre Pierre et Marie Curie- Alger Oran, 3 Septembre 217 Phase III Investigation of Neoadjuvant Carboplatin ± Veliparib in Combination
Post-ASCO 217 Cancer du sein Triple Négatif A.Ladjeroud, K.Bouzid Centre Pierre et Marie Curie- Alger Oran, 3 Septembre 217 Phase III Investigation of Neoadjuvant Carboplatin ± Veliparib in Combination
Targe:ng HER2 in Metasta:c Breast Cancer in 2014
 Targe:ng HER2 in Metasta:c Breast Cancer in 2014 Kimberly L. Blackwell MD Professor Department of Medicine and Radia:on Oncology Duke University Medical Center Director, Breast Cancer Program Duke Cancer
Targe:ng HER2 in Metasta:c Breast Cancer in 2014 Kimberly L. Blackwell MD Professor Department of Medicine and Radia:on Oncology Duke University Medical Center Director, Breast Cancer Program Duke Cancer
Clinical activity of fulvestrant in metastatic breast cancer previously treated with endocrine therapy and/or chemotherapy
 ORIGINAL ARTICLE 2018 Mar 16. [Epub ahead of print] Clinical activity of fulvestrant in metastatic breast cancer previously treated with endocrine therapy and/or chemotherapy Mi Hwa Heo, Hee Kyung Kim,
ORIGINAL ARTICLE 2018 Mar 16. [Epub ahead of print] Clinical activity of fulvestrant in metastatic breast cancer previously treated with endocrine therapy and/or chemotherapy Mi Hwa Heo, Hee Kyung Kim,
Current standards and practice changing studies in Luminal ABC in 2017
 Current standards and practice changing studies in Luminal ABC in 2017 F. Cardoso, MD Director, Breast Unit, Champalimaud Clinical Center, Lisbon, Portugal ESO Breast Cancer Program Coordinator ESMO Board
Current standards and practice changing studies in Luminal ABC in 2017 F. Cardoso, MD Director, Breast Unit, Champalimaud Clinical Center, Lisbon, Portugal ESO Breast Cancer Program Coordinator ESMO Board
LAPATINIB-Resistance to small Molecule ErbB2 Tyrosine Kinase Inhibitor (TKI)
") LAPATINIB-Resistance to small Molecule ErbB2 Tyrosine Kinase Inhibitor (TKI) Prim Mr Sc Dr Suzana Vasović Institute for oncology and radiology of Serbia UMOS, X Conference, 16.05.2015 Belgrade How do we
LAPATINIB-Resistance to small Molecule ErbB2 Tyrosine Kinase Inhibitor (TKI) Prim Mr Sc Dr Suzana Vasović Institute for oncology and radiology of Serbia UMOS, X Conference, 16.05.2015 Belgrade How do we
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer
 Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Lung Cancer Case. Since the patient was symptomatic, a targeted panel was sent. ALK FISH returned in 2 days and was positive.
 Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
Targeting mtor pathway in ER+/Her2- breast cancers. Fabrice ANDRE Gustave Roussy
 Targeting mtor pathway in ER+/Her2- breast cancers Fabrice ANDRE Gustave Roussy Outline mtor pathway Clinical development of rapalogs in breast cancer Moving beyond rapalogs mtor pathway LKB1 Ras-raf-
Targeting mtor pathway in ER+/Her2- breast cancers Fabrice ANDRE Gustave Roussy Outline mtor pathway Clinical development of rapalogs in breast cancer Moving beyond rapalogs mtor pathway LKB1 Ras-raf-
Targeted Therapies in Melanoma
 Mutations and Targets Targeted Therapies in Melanoma ckit NRAS
Mutations and Targets Targeted Therapies in Melanoma ckit NRAS
William J. Gradishar MD
 Northwestern University Feinberg School of Medicine Adjuvant Endocrine Therapy For Postmenopausal Women SOBO 2013 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley
Northwestern University Feinberg School of Medicine Adjuvant Endocrine Therapy For Postmenopausal Women SOBO 2013 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley
Translational Platform for the Development of Targeted Therapeutics
 Translational Platform for the Development of Targeted Therapeutics Ondřej Kalous, MD Associate Project Scientist UCLA Translational Oncology Research Laboratories (TORL) Jonsson Comprehensive Cancer Center
Translational Platform for the Development of Targeted Therapeutics Ondřej Kalous, MD Associate Project Scientist UCLA Translational Oncology Research Laboratories (TORL) Jonsson Comprehensive Cancer Center
Endocrine Therapy of Metastatic Breast Cancer
 Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Endocrine Therapy of Metastatic Breast Cancer Endocrine Therapy of Metastatic Breast Cancer Version 2002: Gerber / Friedrichs
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Endocrine Therapy of Metastatic Breast Cancer Endocrine Therapy of Metastatic Breast Cancer Version 2002: Gerber / Friedrichs
SYNOPSIS PROTOCOL TALBOT
 SYNOPSIS PROTOCOL TALBOT A) CLINICAL TRIAL IDENTIFICATION SPONSOR - PROTOCOL CODE NUMBER : VERSION: SYNOPSIS V4.0-30/06/2015 TRIAL TITLE : Open-label, randomized, multicenter, phase II study, comparing
SYNOPSIS PROTOCOL TALBOT A) CLINICAL TRIAL IDENTIFICATION SPONSOR - PROTOCOL CODE NUMBER : VERSION: SYNOPSIS V4.0-30/06/2015 TRIAL TITLE : Open-label, randomized, multicenter, phase II study, comparing
Chemotherapy and Hormonal Therapy in the Metastatic Setting, ER+/HER-2- and TNBC
 15TH ANNUAL MIAMI CANCER MEETING (MCM)April 27-29, 2018 Miami, Florida Chemotherapy and Hormonal Therapy in the Metastatic Setting, ER+/HER-2- and TNBC Vicente Valero, M.D., F.A.C.P. Professor of Medicine
15TH ANNUAL MIAMI CANCER MEETING (MCM)April 27-29, 2018 Miami, Florida Chemotherapy and Hormonal Therapy in the Metastatic Setting, ER+/HER-2- and TNBC Vicente Valero, M.D., F.A.C.P. Professor of Medicine
Overcoming Endocrine Resistance in ER+ Breast Cancer
 Overcoming Endocrine Resistance in ER+ Breast Cancer Richard S. Finn, MD Associate Professor of Medicine Division of Hematology/Oncology Director Signal Transduction and Therapeutics Program Jonsson Comprehensive
Overcoming Endocrine Resistance in ER+ Breast Cancer Richard S. Finn, MD Associate Professor of Medicine Division of Hematology/Oncology Director Signal Transduction and Therapeutics Program Jonsson Comprehensive
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy. What every patient needs to know. James Larkin
 Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Open Clinical Trials: What s Out There Now Paula D. Ryan, MD, PhD
 Open Clinical Trials: What s Out There Now Paula D. Ryan, MD, PhD Hanahan and Weinberg, 2000 Acquired Capabilities of Cancer Clinical Trials When should I consider a clinical trial? How do I find the right
Open Clinical Trials: What s Out There Now Paula D. Ryan, MD, PhD Hanahan and Weinberg, 2000 Acquired Capabilities of Cancer Clinical Trials When should I consider a clinical trial? How do I find the right
Breast cancer treatment
 Report from the San Antonio Breast Cancer Symposium Breast cancer treatment Determining the best options for select patient groups Sara Soldera, MD, Resident; Nathaniel Bouganim, MD, FRCPC, Medical Oncologist;
Report from the San Antonio Breast Cancer Symposium Breast cancer treatment Determining the best options for select patient groups Sara Soldera, MD, Resident; Nathaniel Bouganim, MD, FRCPC, Medical Oncologist;
C. Bourgier, I. Ray-Coquard, J. Provencal, C. Cropet, A.V. Bourcier, V. Delecroix, A. Reynaud-Bougnoux, J. Cretin, T. Bachelot
 1 Exploratory Subgroup Analysis of the TAMRAD Phase 2 GINECO Trial Evaluating Tamoxifen (TAM) Plus Everolimus (RAD) vs TAM Alone in Patients With Hormone-Receptor Positive, HER2-Negative Metastatic Breast
1 Exploratory Subgroup Analysis of the TAMRAD Phase 2 GINECO Trial Evaluating Tamoxifen (TAM) Plus Everolimus (RAD) vs TAM Alone in Patients With Hormone-Receptor Positive, HER2-Negative Metastatic Breast
Immunoconjugates in Both the Adjuvant and Metastatic Setting
 Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Study Period: 27 March 2008 (first subject enrolled) to 05 May 2010 (data cutoff date for primary analysis)
 to 05 May 2010 (data cutoff date for primary analysis)") Date: 20 July 2011 Page 2 of 3375 2. SYNOPSIS Name of Sponsor: mgen Inc., Thousand Oaks, C US Name of Finished Product: Not applicable Name of ctive Ingredient: Ganitumab (MG 479) Title of Study: n International,
Date: 20 July 2011 Page 2 of 3375 2. SYNOPSIS Name of Sponsor: mgen Inc., Thousand Oaks, C US Name of Finished Product: Not applicable Name of ctive Ingredient: Ganitumab (MG 479) Title of Study: n International,