Case #2: Hormonal Therapy for Advanced Premenopausal Breast Cancer
|
|
|
- Godfrey Butler
- 5 years ago
- Views:
Transcription


1 Case #2: Hormonal Therapy for Advanced Premenopausal Breast Cancer Fellow Presenter: Katherine Clifton, MD Faculty Discussant: Debu Tripathy, MD 7 th Annual June 1, 2018
2 Topics to Be Discussed: Staging and biomarker determination Selection and sequencing of therapy in the metastatic setting for HR+/HER- MBC CDK 4/6 inhibitors in premenopausal patients Management of refractory disease HR, hormone receptor; HER, human epidermal growth factor receptor; MBC, metastatic breast cancer; CDK, cyclin-dependent kinases
3 The Case 42-year-old female presents after self-palpating a left breast mass Past medical history: Seasonal allergies Past surgical history: Exploratory laparotomy with removal of ovarian cysts (benign) Social history: Works as a chemist, no tobacco or illicit drug use, drinks 5 glasses of wine per week Gynecologic history: G2 P2, premenopausal Family history: Denies any family history of breast or ovarian cancer
4 MD Anderson Exam Physical exam: 2.5-cm x 3-cm left breast mass with no skin or nipple changes Palpable left axillary node No right breast masses or right axillary lymphadenopathy

5 Imaging Bilateral mammogram: Left breast spiculated mass measuring 5 cm with left axillary dense nodes Ultrasound: Left breast mass at 3:30 measuring 3.0 cm x 2.4 cm x 1.6 cm, and an abnormal left axillary node measuring 1.8 cm and suspicious left second space internal mammary lymph node
6 Pathology Core biopsy of breast mass: Invasive ductal carcinoma, Nottingham combined histologic grade 2, ER positive (90%, 3+), PR positive (90%, 2+), HER2/neu nonamplified by FISH FNA of left axillary lymph node: Positive for metastatic disease FNA of left internal mammary lymph node: Positive for metastatic disease ER, estrogen receptor; PR, progesterone receptor; FNA, fine-needle aspiration; FISH, fluorescence in situ hybridization
7 Staging: Stage IIIB (ct2n3bm0) ER/PR+ HER2 CT chest, abdomen/pelvis: No evidence of distant metastatic disease Bone scan: No evidence of osseous involvement Genetic testing (indication: Breast cancer diagnosed <age 50 years): negative for BRCA1/2 mutations CT, computed tomography Amin MB, et al (ed). AJCC Cancer Staging Manual. 8 th edition. Switzerland: Springer, 2017.
8 Treatment Neoadjuvant: Paclitaxel 80 mg/m 2 IV weekly x 12 weeks, followed by FAC: 5-fluorouracil 500 mg/m 2 IV, doxorubicin 50 mg/m 2 IV, and cyclophosphamide 500 mg/m 2 IV every 3 weeks x 4 cycles Surgery: Segmental mastectomy with left axillary node dissection Pathology: Invasive ductal carcinoma, grade 2 measuring 3.2 cm, 7/15 lymph nodes positive. ypt2n2a IV, intravenous

9 1x: Lymph node with metastatic IDC
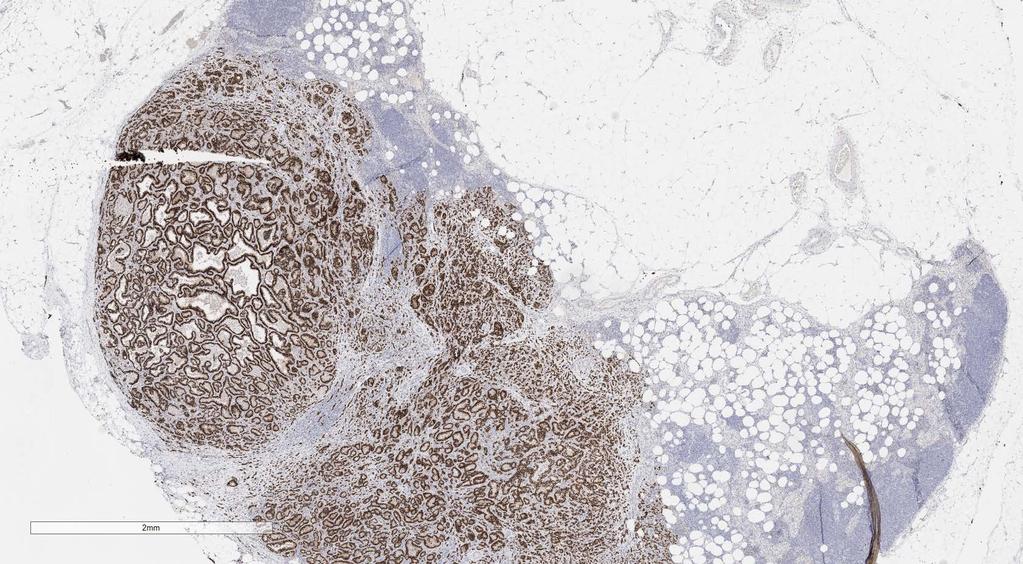
10 1x ER

11 10x H&E Stained Slide
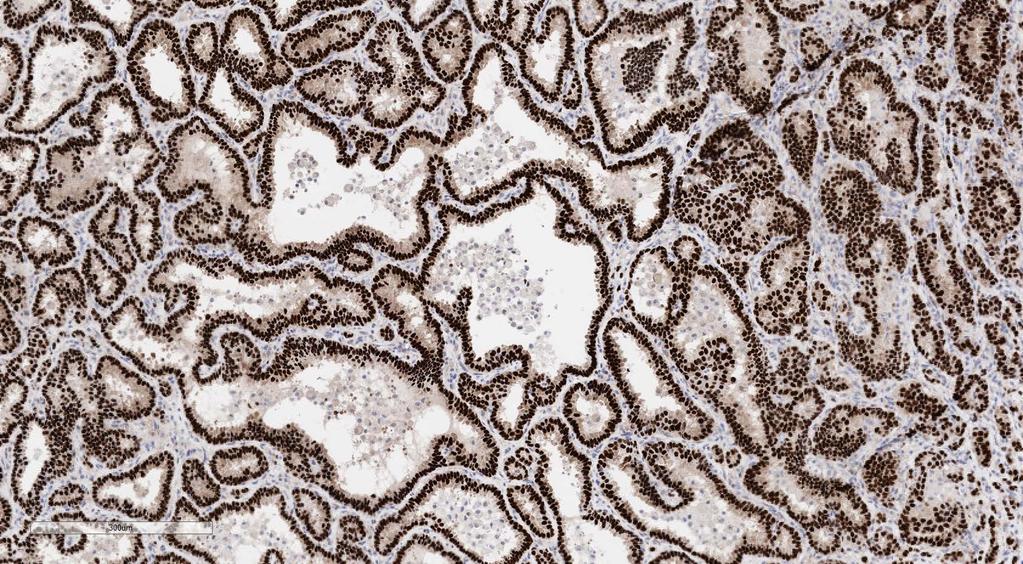
12 10X ER
13 MD Anderson Treatment Radiation to chest wall and supraclavicular fields Adjuvant hormonal therapy: Tamoxifen started as patient premenopausal prior to chemotherapy Side effects: Hot flashes, abnormal vaginal bleeding (biopsy benign) 5 months after completing chemotherapy, patient s regular menstrual cycles resumed 1.5 years later, patient presented with shortness of breath

14 PE, pulmonary embolism Vascular Medicine. Accessed May 24, Found to have new PE
15 Workup CBC WBC 11.3 Hemoglobin 12.2 Platelets 152 Other INR 1.0 CBC, complete blood count; WBC, white blood cell; INR, international normalized ratio Chemistries Na 140 K 4 Cl 102 HCO3 24 BUN 11 Cr 0.62 Glucose 135 ALT 91 AST 172 AP 205 Tbili 0.8 Albumin 3.8
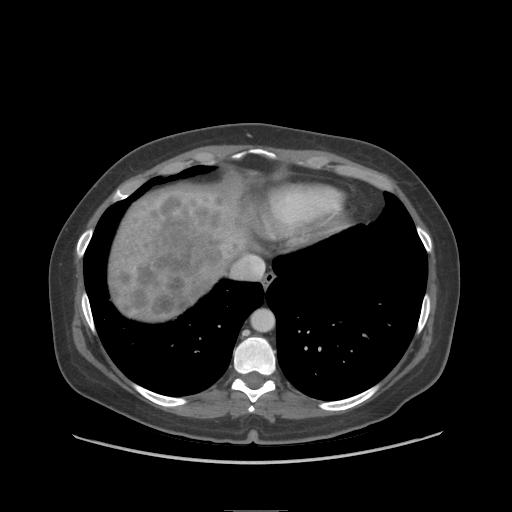
16
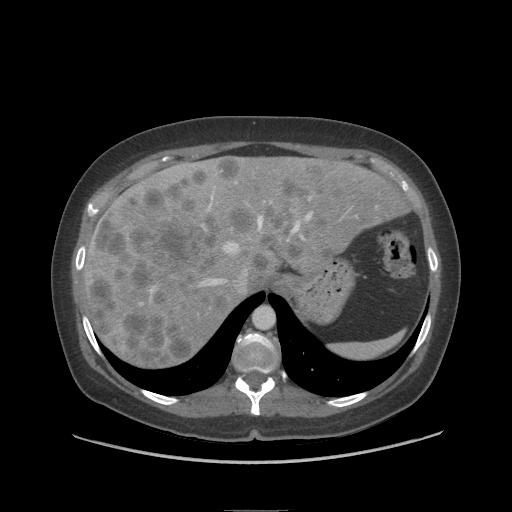
17
18

19 Bone scan: Multiple foci of abnormal increased radiotracer activity, compatible with bone metastases involving the spine, multiple ribs bilaterally, and pelvis
20 Workup Liver Biopsy: Moderately to poorly differentiated adenocarcinoma, consistent with metastasis from patient s known breast primary. ER positive (100%), PR positive (95%), and HER2 negative (0 by IHC) IHC, immunohistochemistry
21 21 Question 1 Part A Which therapy would you choose for the patient as front-line in the metastatic setting 1.5 years post initiation of adjuvant hormonal therapy? 1. Combination chemotherapy 2. Single-agent chemotherapy 3. Aromatase inhibitor with ovarian suppression +/- CDK inhibitor 4. Fulvestrant with ovarian suppression+/- CDK inhibitor
22 Question 1 Part B If you decided to use endocrine therapy in this patient, would you also use a CDK inhibitor? 1. Yes 2. No
23 MD Anderson Treatment Patient received 4 cycles of docetaxel 75 mg/m 2 IV every 3 weeks Side effects: Grade 1 neuropathy, nausea, fatigue Repeat labs show improvement in LFTs Restaging scans: LFT, liver function test
24 Initial Follow Up
25 MD Anderson Treatment Patient received an additional 5 cycles of docetaxel with continued improvement of liver metastasis on most recent restaging LFTs have normalized Although irregular, she continues to have menstrual cycles Patient has now developed worsening neuropathy and fatigue secondary to chemotherapy
26 Question 2 Part A What treatment regimen would you consider next? 1. Continue docetaxel 2. Eribulin 3. Ovarian suppression with endocrine therapy +/- CDK inhibitor
27 Question 2 Part B If choosing ovarian suppression with CDK inhibitor + endocrine therapy in a premenopausal patient, which CDK inhibitor would you select (assuming all are available in your practice)? 1. Palbociclib 2. Ribociclib 3. Abemaciclib
28 Question 2 Part C What endocrine partner would you choose? 1. Aromatase inhibitor 2. Fulvestrant 3. Tamoxifen
29 Treatment Patient is started on leuprolide acetate followed by palbociclib 125 mg PO days 1-21 and letrozole CBC prior to C1: CBC prior to C2: CBC WBC 11.9 ANC Hemoglobin 12.2 Platelets 160 CBC WBC 2.3 ANC 1.33 Hemoglobin 11.5 Platelets 105 PO, by mouth
30 Monitoring on Palbociclib Monitor CBC prior to start of palbociclib and at beginning of each cycle, as well as day 15 of first 2 cycles ANC Grading: Grade 1: LLN 1500 Grade 2: <1500 Grade 3: 500- <1000 Grade 4: <500 Palbociclib [prescribing information]. New York, New York; Pfizer, Inc; 2017.
31 Treatment Palbociclib is continued at same dose with continued grade 2 neutropenia but no further side effects Patient undergoes restaging scans after 3 cycles:

32 Prior Scan Current Scan
33 MD Anderson Restaging CT chest, abdomen/pelvis: Continued decrease in size of hepatic metastases with an example 4.1 cm x 3.1 cm segment-8 metastasis decreased from 4.2 cm x 3.7 cm and a 3.7 cm x 3.1 cm segment-6 metastasis decreased from 4.2 cm x 3.7 cm Increasing sclerosis of multifocal osseous metastases, which may be related to posttreatment effects
34 Treatment Patient continues on palbociclib 125 mg PO days 1-21 and letrozole for an additional 2 cycles CBC prior to C6: CBC WBC 2.9 ANC 2.03 Hemoglobin 12.5 Platelets 83
35 Monitoring on Palbociclib Table applies to all hematologic adverse events except lymphopenia (unless lymphopenia is associated with clinical event such as opportunistic infection) Thrombocytopenia Grading: Grade 1: LLN 75 Grade 2: Grade 3: Grade 4: <10 Palbociclib [prescribing information]. New York, New York; Pfizer, Inc; 2017.
36 Treatment Patient continues on palbociclib 125 mg PO days 1-21 and letrozole for a total of 6 cycles
37 Question 3 If patient developed worsening aromatase-related side effects, such as joint pain, could you consider changing to tamoxifen? 1. Yes 2. No
38 Question 4 What treatment would you offer the patient upon progression? 1. CDK inhibitor + fulvestrant 2. Fulvestrant alone 3. Capecitabine 4. Everolimus + exemestane
39 Case #2: Faculty Discussant: Debu Tripathy, MD 7 th Annual June 1, 2018

40 Gene Expression Profiles Reveal Distinct Breast Cancer Subsets HER2 Enriched 1. 15% to 20% of cases 2. Prognostic/predictive 2. Proliferation 3. Two types (ER /+) Basal 1. 10% to 15% of cases 2. ER/PR/HER2 3. Proliferative 4. EGFR, c-kit, myc, p53 mutations 5. Includes BRCA1 mutations Luminal A and B 1. ER+, PR+/ 2. Prognostic/predictive 3. ER-GATA3, CCND1 amplif, PI3K, RUNX1 mutations Ki67, STK6, survivin, cyclin B1, MYBL2 Sorlie T, et al. Proc Natl Acad Sci USA. 2003;100(14):
:61-70. 41")
41 Genomic Landscape Varies Among Receptor Subtypes of Breast Cancer The Cancer Genome Atlas Network. Nature. 2012;490(7418):
42 Question 1 Which therapy would you choose for the patient as front-line in the metastatic setting 1.5 years post initiation of adjuvant hormonal therapy? 1. Combination chemotherapy 2. Single-agent chemotherapy 3. Aromatase inhibitor with ovarian suppression +/- CDK inhibitor 4. Fulvestrant with ovarian suppression+/- CDK inhibitor Would you use a CDK inhibitor with endocrine therapy? 1. Yes 2. No

:3069-3103.")
43 Diagnosis and Treatment of Hormone Receptor Positive Metastatic Breast Cancer *OS if premenopausal, and if so, can use AI after tamoxifen/toremifene Adapted from Rugo HS, et al. J Clin Oncol. 2016;34(25): OS, overall survival
44 Question 2 Part A What treatment regimen would you consider next? 1. Continue docetaxel 2. Eribulin 3. Ovarian suppression with endocrine therapy +/- CDK inhibitor
45 Question 2 Part B If choosing ovarian suppression with CDK inhibitor + endocrine therapy in a premenopausal patient, which CDK inhibitor would you select (assuming all are available in your practice)? 1. Palbociclib 2. Ribociclib 3. Abemaciclib What endocrine partner would you choose? 1. Aromatase inhibitor 2. Fulvestrant 3. Tamoxifen
")



:6173-6182. Lange CA, et al.")
46 CDK4/6 Controls Cell-Cycle Progression From G1 to S Phase by Regulating the Activity of Rb Synthesis of D-type cyclins (cyclin D1, D2, and D3) and association with CDK4/6 is initiated in response to mitogenic signaling pathways 1 Active cyclin D CDK4/6 phosphorylates Rb, decoupling Rb from E2F and allowing transcription of genes required for cell cycle progression 1 Rb inhibits E2F-mediated transcription by binding to and sequestering E2F 2 E2F activates transcription of genes necessary for S-phase entry and cell cycle progression 2 1. Lange CA, et al. Endocr Relat Cancer. 2011;18(4):C Rader J, et al. Clin Cancer Res. 2013;19(22): Lange CA, et al. Endocr Relat Cancer. 2011;18(4):C19-24.
 Ribociclib LEE011 FDA Approved (September 27, 2017) Abemaciclib LY2835219 FDA, US Food and Drug")
47 CDK4/6 Inhibitors in Clinical Use/Testing FDA Approved (February 4, 2015) Palbociclib PD FDA Approved (March 13, 2017) Ribociclib LEE011 FDA Approved (September 27, 2017) Abemaciclib LY FDA, US Food and Drug Administration
48 Properties of Approved CDK4/6 Inhibitors IC 50 (nm) on target CDKs CDK4 cyclin D1 CDK6 cyclin D1/2/3 IC 50 (nm) on other CDKs CDK1 cyclin B CDK2 cyclin A/E CDK5 p25 CDK9 cyclin T Ribociclib Palbociclib Abemaciclib ,000 76,000 43,900 NR >10,000 >10,000 >10,000 NR Kinase partition index Lipophilicity (clogp) IC 50 against bone marrow mononuclear cells (nm) 1700 ± ± ± 27 Half-life 33 hr to 42 hr 26 hr to 27 hr 17 hr to 38 hr T max 1 hr to 5 hr 6 hr to 12 hr 4 hr to 6 hr Tripathy D, et al. Clin Cancer Res. 2017;23(13):
 P<.")
49 PALOMA-2: Phase 3 Study Palbociclib + Letrozole as First-Line Therapy in HR+, HER2 Advanced BC PALOMA-2 (N = 666) Postmenopausal women 18 years of age ER+, HER2 ABC No prior systemic treatment for advanced disease Palbociclib + Letrozole vs Placebo + Letrozole Median PFS 24.8 months vs 14.5 months HR = 0.58 (95% CI: ) P<.001 Palbociclib + letrozole n = 444 Placebo + letrozole n = 222 BC, breast cancer; ABC, advance breast cancer; PFS, progression-free survival; CI, confidence interval Finn RS, et al. N Engl J Med. 2016;375(20):
50 Finn RS, et al. N Engl J Med. 2016;375(20): Subgroup Analysis: PALOMA-2
:1925-1936.")
51 Finn RS, et al. N Engl J Med. 2016;375(20): Adverse Events: PALOMA-2
52 PALOMA-3: Progression-Free Survival Relapsed on or within 12 months after completion of adjuvant ET or within 1 month after therapy for advanced disease Probability of Progression-Free Survival, % ET, endocrine therapy Turner NC, et al. N Engl J Med. 2015;373(3):
53 MONALEESA-2: Phase III Double-Blind, Placebo- Controlled Study of Ribociclib + Letrozole N = 668 Postmenopausal women with HR+, HER2 advanced breast cancer No prior therapy for advanced disease Randomization (1:1) Stratified by the presence/absence of liver and/or lung metastases Ribociclib + Letrozole* n = 334 Placebo + Letrozole* n = 334 Primary endpoint PFS (locally assessed per RECIST v1.1) Secondary endpoints OS (key) ORR CBR Safety Tumor assessments were performed every 8 weeks for 18 months, then every 12 weeks thereafter Final analysis planned after 302 PFS events 93.5% power to detect a 33% risk reduction (HR = 0.67) with one-sided α = 2.5% *Ribociclib 600 mg per day, 3 weeks on/1 week off; letrozole 2.5 mg/day. With supportive independent central review; MONALEESA-2 is registered at ClinicalTrials.gov (NCT ). CBR, clinical benefit rate; ORR, overall response rate; RECIST, Response Evaluation Criteria In Solid Tumors Hortobagyi GN, et al. N Engl J Med. 2016;375(18):
54 MONALEESA-2: Primary Endpoint at First Analysis Probability of progression-free survival, % Ribociclib + Letrozole Placebo + Letrozole Ribo + Let ORR* 52.7% 37.1% Placebo + LET *In measurable disease, P<.001 Ribo + LET n = 334 PBO + LET n = 334 Number of events, n (%) 93 (27.8) 150 (44.9) Median PFS, months (95% CI) NR (19.3 NR) 14.7 ( ) Hazard ratio (95% CI) ( ) One-sided P value No. Patients at Risk Months Ribo + LET PBO + LET Hortobagyi GN, et al. N Engl J Med. 2016;375(18):
55 MONALEESA-2: Secondary Endpoints Rate, % All Patients P = Patients With Measurable Disease Rate, % P = Ribociclib + Letrozole Placebo + Letrozole 0 Objective Response Rate ORR 0 Objective Response Rate ORR Clinical benefit rate in patients with measurable disease*: 80% ribociclib arm vs 72% placebo arm (P =.02) Overall survival data were immature at the cutoff date for interim analysis Hortobagyi GN, et al. N Engl J Med. 2016;375(18):
56 MONALEESA-7 Pre/Perimenopausal With Ovarian Suppression + AI or Tamoxifen With Placebo vs Ribociclib ELIGIBILITY PFS (investigator assessment) Ribociclib + tamoxifen/nsai n = 335 Placebo + tamoxifen/nsai n = 337 Number of events, n (%) 131 (39.1) 187 (55.5) Median PFS, months (95% CI) 23.8 (19.2 NR) 13.0 ( ) Hazard ratio (95% CI) ( ) One-sided P value Pre/perimenopausal women (per NCCN guidelines) 1 measurable lesion (RECIST 1.1) or 1 predominantly lytic bone lesion ECOG performance status of 1 1 line of chemotherapy for ABC Prior (neo)adjuvant therapy was allowed: If no prior endocrine therapy OR if 12 months since the last dose, patient was eligible for tamoxifen or an NSAI, per investigator/patient choice If last dose of tamoxifen was <12 months prior to randomization, patient was eligible for an NSAI If last dose of AI/NSAI was <12 months prior to randomization, patient was eligible for tamoxifen Probability of PFS,% NSAI, non-steroidal aromatase inhibitors; NCCN, National Comprehensive Cancer Network; ECOG, Eastern Cooperative Oncology Group Tripathy D, et al. Lancet Oncol. May 24, 2018 [epub ahead of print] CI, confidence interval; NR, not reached. Goserelin included in all combinations No. at risk Time (months) Ribociclib + tamoxifen/nsai Placebo + tamoxifen/nsai
57 MONALEESA-7 Pre/Perimenopausal With Ovarian Suppression + AI or Tamoxifen With Placebo vs Ribociclib PFS (Investigator Assessment) Ribociclib Arm n = 87 Tamoxifen Placebo Arm n = 90 Ribociclib Arm n = 248 NSAI Placebo Arm n = 247 Number of events, n Median PFS, months (95% CI) 22.1 ( ) 11.0 ( ) 27.5 (19.1 NR) 13.8 ( ) Hazard ratio (95% CI) ( ) ( ) Tripathy D, et al. Lancet Oncol. May 24, 2018 [epub ahead of print].
58 Differences in PFS based on age in population receiving palbociclib as standard of care Clifton et al., ASCO 2018
59 MONARCH 1: Monotherapy in Patients Progressing on Prior Endocrine and 2 Prior Chemotherapies Investigator-Assessed Response Confirmed objective response rate (ORR = CR + PR) (95% CI) CR PR Abemaciclib 200 mg (N = 132) 19.7% ( ) 0% 19.7% Stable disease 6 months 22.7% Clinical benefit rate (CBR = ORR +SD 6 mo) 42.4 % Dickler MN, et al. Clin Cancer Res. 2017;23(17): CR, complete response; SD, stable disease
60 Study Summary of CDK 4/6 Inhibitor Results in HR+ MBC First-Line Metastatic Breast Cancer PALOMA-1 Letrozole Letrozole + palbociclib PALOMA-2 Letrozole + placebo Letrozole + palbociclib MONALEESA-2 Letrozole + placebo Letrozole + ribociclib MONALEESA-7 (pre-menopausal) Letrozole + goserelin + placebo Letrozole + goserelin + ribociclib MONARCH 3 Letrozole + placebo Letrozole + abemaciclib Second-Line Metastatic Breast Cancer BOLERO-2 Exemestane + placebo Exemestane + everolimus PALOMA-3 Fulvestrant + palbociclib Fulvestrant + placebo MONARCH 2 Fulvestrant + abemaciclib Fulvestrant + placebo Refractory Metastatic Breast Cancer N ORR,* % (Mz) 33 (39) 43 (56) 35 (44) 42 (55) 28 (37) 41 (53) 30 (36) 41 (51) 35 (44) 48 (59) (48) 16 (21) CBR,* % mpfs, mo (95% CI) 10.2 ( ) 20.2 ( ) 14.5 ( ) 24.8 (22.1-NR) 14.7 ( ) NR (19.3-NR) 13.0 ( ) 23.8 (19.2-NR) 14.7 NR (7.5-NR) 3.8 ( ) mpfs HR ( ) 0.58 ( ) ( ) ( ) ( ) 0.43 ( ) ( ) ( ) MONARCH 1 (Phase II) Abemaciclib 132 (20) N/A N/A.0004 <.0001 P-value <.001 < < mpfs, median progression-free survival in months; NA, not applicable; *% (Mz), in patients with measurable disease; for CBR, Mz values provided
61 Question 3 If patient developed worsening aromatase-related side effects, such as joint pain, could you consider changing to tamoxifen? 1. Yes 2. No
62 Question 4 What treatment would you offer the patient upon progression? 1. CDK inhibitor + fulvestrant 2. Fulvestrant alone 3. Capecitabine 4. Everolimus + exemestane
63 Revote
64 Workup Liver Biopsy: Moderately to poorly differentiated adenocarcinoma, consistent with metastasis from patient s known breast primary. ER positive (100%), PR positive (95%), and HER2 negative (0 by IHC) IHC, immunohistochemistry
65 65 Question 1 Part A Which therapy would you choose for the patient as front-line in the metastatic setting 1.5 years post initiation of adjuvant hormonal therapy? 1. Combination chemotherapy 2. Single-agent chemotherapy 3. Aromatase inhibitor with ovarian suppression +/- CDK inhibitor 4. Fulvestrant with ovarian suppression+/- CDK inhibitor
66 Question 1 Part B If you decided to use endocrine therapy in this patient, would you also use a CDK inhibitor? 1. Yes 2. No
67
68
RIBOCICLIB EN PRIMERA LINEA DE TRATAMIENTO. Dra. Elena Aguirre H.U. Miguel Servet
 RIBOCICLIB EN PRIMERA LINEA DE TRATAMIENTO Dra. Elena Aguirre H.U. Miguel Servet INTRODUCTION ADVANCED BREAST CANCER HR+/HER2- YES Consider Chemo VISCERAL CRISIS? NO Endocrine Therapy X3 Toxicity Progresive
RIBOCICLIB EN PRIMERA LINEA DE TRATAMIENTO Dra. Elena Aguirre H.U. Miguel Servet INTRODUCTION ADVANCED BREAST CANCER HR+/HER2- YES Consider Chemo VISCERAL CRISIS? NO Endocrine Therapy X3 Toxicity Progresive
First-Line Ribociclib + Letrozole for Postmenopausal Women With HR+, HER2-, Advanced Breast Cancer: First Results From the Phase III MONALEESA-2 Study
 First-Line Ribociclib + Letrozole for Postmenopausal Women With HR+, HER2-, Advanced Breast Cancer: First Results From the Phase III MONALEESA-2 Study Abstract LBA1 Hortobagyi GN, Stemmer SM, Burris HA,
First-Line Ribociclib + Letrozole for Postmenopausal Women With HR+, HER2-, Advanced Breast Cancer: First Results From the Phase III MONALEESA-2 Study Abstract LBA1 Hortobagyi GN, Stemmer SM, Burris HA,
Metastatic breast cancer: sequence of therapies
 Metastatic breast cancer: sequence of therapies Clinical Case Discussion Nadia Harbeck, MD PhD Breast Center, Department of Gynecology and Obstetrics University of Munich, Ludwig-Maximilians University
Metastatic breast cancer: sequence of therapies Clinical Case Discussion Nadia Harbeck, MD PhD Breast Center, Department of Gynecology and Obstetrics University of Munich, Ludwig-Maximilians University
Targeting CDK 4/6. Jee Hyun Kim, M.D., Ph.D. Seoul National University College of Medicine
 2016.04.30 GBCC Education Symposium Targeting CDK 4/6 Jee Hyun Kim, M.D., Ph.D. Seoul National University College of Medicine Contents Cyclins -CDKs in cell cycle control CDK 4/6 in breast cancer Preclinical
2016.04.30 GBCC Education Symposium Targeting CDK 4/6 Jee Hyun Kim, M.D., Ph.D. Seoul National University College of Medicine Contents Cyclins -CDKs in cell cycle control CDK 4/6 in breast cancer Preclinical
Outline of the presentation
 Outline of the presentation Breast cancer subtypes and classification Clinical need in estrogen-positive (ER+) metastatic breast cancer (mbc) Sulforaphane and SFX-01: the preclinical evidence STEM Phase
Outline of the presentation Breast cancer subtypes and classification Clinical need in estrogen-positive (ER+) metastatic breast cancer (mbc) Sulforaphane and SFX-01: the preclinical evidence STEM Phase
Inibitori delle chinasi ciclino dipendenti nel trattamento della malattia metastatica HR-positiva Gli studi clinici
 Inibitori delle chinasi ciclino dipendenti nel trattamento della malattia metastatica HR-positiva Gli studi clinici Laura Orlando UOC Oncologia & Breast Unit Brindisi Verona 22/04/2016 Summary Studi con
Inibitori delle chinasi ciclino dipendenti nel trattamento della malattia metastatica HR-positiva Gli studi clinici Laura Orlando UOC Oncologia & Breast Unit Brindisi Verona 22/04/2016 Summary Studi con
TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive metastatic breast cancer
 TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive metastatic breast cancer Marta Bonotto Department of Oncology University Hospital of Udine TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive
TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive metastatic breast cancer Marta Bonotto Department of Oncology University Hospital of Udine TRIALs of CDK4/6 inhibitor in women with hormone-receptor-positive
Collaborative Management of Patients With Advanced Estrogen Receptor Positive Breast Cancer
 Collaborative Management of Patients With Advanced Estrogen Receptor Positive Breast Cancer Lee Schwartzberg, MD, FACP Heather Greene, FNP, AOCNP West Cancer Center Memphis, Tennessee Learning Objectives
Collaborative Management of Patients With Advanced Estrogen Receptor Positive Breast Cancer Lee Schwartzberg, MD, FACP Heather Greene, FNP, AOCNP West Cancer Center Memphis, Tennessee Learning Objectives
Multimedia Appendix 6 Educational Materials Table of Contents. Intervention Educational Materials Audio Script (version 1)
") Multimedia Appendix 6 Educational Materials Table of Contents Intervention Educational Materials... 1 Audio Script (version 1)... 1 Text (version 1)... 5 Slides (version 1)... 17 Audio Script (version
Multimedia Appendix 6 Educational Materials Table of Contents Intervention Educational Materials... 1 Audio Script (version 1)... 1 Text (version 1)... 5 Slides (version 1)... 17 Audio Script (version
Metastatic Breast Cancer What is new? Subtypes and variation?
 Metastatic Breast Cancer What is new? Subtypes and variation? Anne Blaes, MD, MS University of Minnesota, Division of Hematology/Oncology Director, Adult Cancer Survivor Program Current estimates for metastatic
Metastatic Breast Cancer What is new? Subtypes and variation? Anne Blaes, MD, MS University of Minnesota, Division of Hematology/Oncology Director, Adult Cancer Survivor Program Current estimates for metastatic
What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland
 What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland Outline Early breast cancer Advanced breast cancer Open questions Outline Early breast cancer
What is new in HR+ Breast Cancer? Olivia Pagani Breast Unit and Institute of oncology of Southern Switzerland Outline Early breast cancer Advanced breast cancer Open questions Outline Early breast cancer
Update on New Perspectives in Endocrine-Sensitive Breast Cancer. James R. Waisman, MD
 Update on New Perspectives in Endocrine-Sensitive Breast Cancer James R. Waisman, MD Nothing to disclose DISCLOSURE TAILORx Oncotype Recurrence Score TAILORx Study Design Sparano, J Clin Oncol 2008;26:721-728
Update on New Perspectives in Endocrine-Sensitive Breast Cancer James R. Waisman, MD Nothing to disclose DISCLOSURE TAILORx Oncotype Recurrence Score TAILORx Study Design Sparano, J Clin Oncol 2008;26:721-728
ESMO SUMMIT MIDDLE EAST 2018
 ESMO SUMMIT MIDDLE EAST 2018 Breast Clinical Cases Presentation Hampig Raphael Kourie, MD, MSc, MBioethics Faculty of Medicine, Saint Joseph University of Beirut, Lebanon 6-7 April 2018, Dubai, UAE CONFLICT
ESMO SUMMIT MIDDLE EAST 2018 Breast Clinical Cases Presentation Hampig Raphael Kourie, MD, MSc, MBioethics Faculty of Medicine, Saint Joseph University of Beirut, Lebanon 6-7 April 2018, Dubai, UAE CONFLICT
It is a malignancy originating from breast tissue
 59 Breast cancer 1 It is a malignancy originating from breast tissue including both early stages which are potentially curable, and metastatic breast cancer (MBC) which is usually incurable. Most breast
59 Breast cancer 1 It is a malignancy originating from breast tissue including both early stages which are potentially curable, and metastatic breast cancer (MBC) which is usually incurable. Most breast
Updates From San Antonio Breast Cancer Symposium 2017
 Updates From San Antonio Breast Cancer Symposium 2017 Rob Coleman University of Sheffield Presentation Outline New Insights into adjuvant endocrine treatment Duration of treatment Perioperative therapy
Updates From San Antonio Breast Cancer Symposium 2017 Rob Coleman University of Sheffield Presentation Outline New Insights into adjuvant endocrine treatment Duration of treatment Perioperative therapy
Highlights of. Metastatic & Advanced Breast Cancer
 Highlights of Metastatic & Advanced Breast Cancer 1 Financial Disclosure(s) I currently have or have had the following relevant financial relations to disclose: Speaker s Bureau: Novartis 2 Off Label Use
Highlights of Metastatic & Advanced Breast Cancer 1 Financial Disclosure(s) I currently have or have had the following relevant financial relations to disclose: Speaker s Bureau: Novartis 2 Off Label Use
Cancers du Sein Métastatiques
 Cancers du Sein Métastatiques Véronique Diéras Journée Laurence Leroyer Rennes 18 mai 2018 Plan ESME Inhibiteurs CDK 4/6 RH+ Inhibiteurs PARP Anticorps drogue-conjugués Perspectives 2018-2019 ESME Time
Cancers du Sein Métastatiques Véronique Diéras Journée Laurence Leroyer Rennes 18 mai 2018 Plan ESME Inhibiteurs CDK 4/6 RH+ Inhibiteurs PARP Anticorps drogue-conjugués Perspectives 2018-2019 ESME Time
Endocrine Therapy 2017: Is There a Better Single Agent and when Should we Use it?
 Endocrine Therapy 2017: Is There a Better Single Agent and when Should we Use it? ET1 ET2 ET3 Targeted agent 1 Targeted agent 2 Hope S. Rugo, MD Director, Breast Oncology and Clinical Trials Education
Endocrine Therapy 2017: Is There a Better Single Agent and when Should we Use it? ET1 ET2 ET3 Targeted agent 1 Targeted agent 2 Hope S. Rugo, MD Director, Breast Oncology and Clinical Trials Education
Disease Update: Metastatic Breast Cancer
 Disease Update: Metastatic Breast Cancer Aimee Faso, PharmD, BCOP, CPP Oncology Clinical Specialist, GI/Breast UNC Hospitals and Clinics August 2015 Objectives Identify treatment choices of metastatic
Disease Update: Metastatic Breast Cancer Aimee Faso, PharmD, BCOP, CPP Oncology Clinical Specialist, GI/Breast UNC Hospitals and Clinics August 2015 Objectives Identify treatment choices of metastatic
NSABP: FB-11. Shannon Puhalla, MD
 NSABP: FB-11 Phase II Randomized Study Evaluating the Biological and Clinical Effects of the Combination of Palbociclib with Letrozole as Neoadjuvant Therapy in Post- Menopausal Women with Estrogen Receptor
NSABP: FB-11 Phase II Randomized Study Evaluating the Biological and Clinical Effects of the Combination of Palbociclib with Letrozole as Neoadjuvant Therapy in Post- Menopausal Women with Estrogen Receptor
Recent advances in the management of metastatic breast cancer in older adults
 Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
When is Chemotherapy indicated in Advanced Luminal Breast Cancer?
 When is Chemotherapy indicated in Advanced Luminal Breast Cancer? Soo-Chin Lee Head & Senior Consultant Department of Haematology-Oncology Clinical Care National University Cancer Institute, Singapore
When is Chemotherapy indicated in Advanced Luminal Breast Cancer? Soo-Chin Lee Head & Senior Consultant Department of Haematology-Oncology Clinical Care National University Cancer Institute, Singapore
CDK 4/6 Inhibitors: Efficacy and Side Effect Profile
 CDK 4/6 Inhibitors: Efficacy and Side Effect Profile Univ.-Prof. Dr. Christian F Singer, MPH Center for Breast Health, Medical University of Vienna Center for Familial Breast- and Ovarian Cancer, MUW Christian
CDK 4/6 Inhibitors: Efficacy and Side Effect Profile Univ.-Prof. Dr. Christian F Singer, MPH Center for Breast Health, Medical University of Vienna Center for Familial Breast- and Ovarian Cancer, MUW Christian
Management of hormone-receptor positive human epidermal receptor 2 negative advanced or metastatic breast cancers
 Review Article Page 1 of 10 Management of hormone-receptor positive human epidermal receptor 2 negative advanced or metastatic breast cancers Roger K. C. Ngan Department of Clinical Oncology, Queen Elizabeth
Review Article Page 1 of 10 Management of hormone-receptor positive human epidermal receptor 2 negative advanced or metastatic breast cancers Roger K. C. Ngan Department of Clinical Oncology, Queen Elizabeth
Aggiornamenti tra ricerca e clinica: il carcinoma della mammella
 Aggiornamenti tra ricerca e clinica: il carcinoma della mammella Filippo Montemurro Unit of (INCO) Fondazione del Piemonte per l Oncologia Candiolo Cancer Institute (IRCCs) Research Needs in Breast Cancer
Aggiornamenti tra ricerca e clinica: il carcinoma della mammella Filippo Montemurro Unit of (INCO) Fondazione del Piemonte per l Oncologia Candiolo Cancer Institute (IRCCs) Research Needs in Breast Cancer
Open Clinical Trials: What s Out There Now Paula D. Ryan, MD, PhD
 Open Clinical Trials: What s Out There Now Paula D. Ryan, MD, PhD Hanahan and Weinberg, 2000 Acquired Capabilities of Cancer Clinical Trials When should I consider a clinical trial? How do I find the right
Open Clinical Trials: What s Out There Now Paula D. Ryan, MD, PhD Hanahan and Weinberg, 2000 Acquired Capabilities of Cancer Clinical Trials When should I consider a clinical trial? How do I find the right
A case of a BRCA2-mutated ER+/HER2 breast cancer during pregnancy
 ESMO Preceptorship Programme Breast Cancer Lisbon 16,17 September 2016 Emanuela Risi Sandro Pitigliani Medical Oncology Department Hospital of Prato, Istituto Toscano Tumori, Prato, Italy A case of a BRCA2-mutated
ESMO Preceptorship Programme Breast Cancer Lisbon 16,17 September 2016 Emanuela Risi Sandro Pitigliani Medical Oncology Department Hospital of Prato, Istituto Toscano Tumori, Prato, Italy A case of a BRCA2-mutated
Mechanisms of hormone drug resistance
 Mechanisms of hormone drug resistance Ljiljana Stamatović Institute for Oncology and Radiology of Serbia Tenth UMOS Conference, Belgrade, 16-17 th May 2015. Hormone receptor-positive breast cancer (HR+
Mechanisms of hormone drug resistance Ljiljana Stamatović Institute for Oncology and Radiology of Serbia Tenth UMOS Conference, Belgrade, 16-17 th May 2015. Hormone receptor-positive breast cancer (HR+
Karcinom dojke. PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski
 Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Overcoming resistance to endocrine or HER2-directed therapy
 Overcoming resistance to endocrine or HER2-directed therapy Jane Lowe Meisel, MD Assistant Professor of Hematology and Medical Oncology Winship Cancer Institute at Emory University 1 Background While most
Overcoming resistance to endocrine or HER2-directed therapy Jane Lowe Meisel, MD Assistant Professor of Hematology and Medical Oncology Winship Cancer Institute at Emory University 1 Background While most
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings. Eve Rodler, MD University of California at Davis October 2016
 Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
MEET MARY KISQALI PATIENT PROFILES
 KISQALI PATIENT PROFILES MEET MARY Mary was recently diagnosed with HR+/HER2- metastatic breast cancer Review the data from the MONALEESA-2 trial to see how patients like Mary responded The patient profile
KISQALI PATIENT PROFILES MEET MARY Mary was recently diagnosed with HR+/HER2- metastatic breast cancer Review the data from the MONALEESA-2 trial to see how patients like Mary responded The patient profile
Online-Only Supplementary Materials
 Online-Only Supplementary Materials Online-Only Supplementary Methods: Eligibility Criteria and Study Endpoints and Assessments Supplementary Table 1. Demographic and Baseline Characteristics in Patients
Online-Only Supplementary Materials Online-Only Supplementary Methods: Eligibility Criteria and Study Endpoints and Assessments Supplementary Table 1. Demographic and Baseline Characteristics in Patients
Pharmacology Updates in Breast Cancer Chris Vaklavas, M.D.
 Pharmacology Updates in Breast Cancer Chris Vaklavas, M.D. Assistant Professor Department of Medicine, Division of Hematology/Oncology University of Alabama at Birmingham NP2540M 1802 6th Avenue South
Pharmacology Updates in Breast Cancer Chris Vaklavas, M.D. Assistant Professor Department of Medicine, Division of Hematology/Oncology University of Alabama at Birmingham NP2540M 1802 6th Avenue South
METRIC Study Key Eligibility Criteria
 The METRIC Study METRIC Study Key Eligibility Criteria The pivotal METRIC Study is evaluating glembatumumab vedotin in patients with gpnmb overexpressing metastatic triple-negative breast cancer (TNBC).
The METRIC Study METRIC Study Key Eligibility Criteria The pivotal METRIC Study is evaluating glembatumumab vedotin in patients with gpnmb overexpressing metastatic triple-negative breast cancer (TNBC).
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents
 Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Novel Strategies in Systemic Therapies: Overcoming Endocrine Therapy Resistance
 Novel Strategies in Systemic Therapies: Overcoming Endocrine Therapy Resistance Richard S. Finn, MD Division of Hematology/ Oncology Director, Translational Oncology Laboratory Geffen School of Medicine
Novel Strategies in Systemic Therapies: Overcoming Endocrine Therapy Resistance Richard S. Finn, MD Division of Hematology/ Oncology Director, Translational Oncology Laboratory Geffen School of Medicine
Metastatic HR+ Breast Cancer - CDK 4/6 Inhibitors Charting the Path. Sandy Sehdev MD FRCPC
 Metastatic HR+ Breast Cancer - CDK 4/6 Inhibitors Charting the Path Sandy Sehdev MD FRCPC Objectives To understand the approach to the treatment of hormone sensitive metastatic breast cancer and the use
Metastatic HR+ Breast Cancer - CDK 4/6 Inhibitors Charting the Path Sandy Sehdev MD FRCPC Objectives To understand the approach to the treatment of hormone sensitive metastatic breast cancer and the use
Dieta Brandsma, Department of Neuro-oncology, Netherlands Cancer Institute, Amsterdam, The Netherlands
 What is hot in breast cancer brain metastases? Dieta Brandsma, Department of Neuro-oncology, Netherlands Cancer Institute, Amsterdam, The Netherlands 8th Annual Brain Metastases Research and Emerging Therapy
What is hot in breast cancer brain metastases? Dieta Brandsma, Department of Neuro-oncology, Netherlands Cancer Institute, Amsterdam, The Netherlands 8th Annual Brain Metastases Research and Emerging Therapy
Sesiones interhospitalarias de cáncer de mama. Revisión bibliográfica 4º trimestre 2015
 Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
Treatment of Metastatic Breast Cancer. Prof RCCoombes Imperial College London
 Treatment of Metastatic Breast Cancer Prof RCCoombes Imperial College London Metastatic Breast Cancer: General Guidelines Specialized oncology nurses (if possible specialized breast nurses) should be part
Treatment of Metastatic Breast Cancer Prof RCCoombes Imperial College London Metastatic Breast Cancer: General Guidelines Specialized oncology nurses (if possible specialized breast nurses) should be part
Breast Cancer Breast Managed Clinical Network
 Initial Evaluation Clinical Stage Pre-Treatment Evaluation Treatment and pathological stage Less than 4 positive lymph nodes Adjuvant Treatment ER Positive HER2 Negative (see page 2 & 3 ) HER2 Positive
Initial Evaluation Clinical Stage Pre-Treatment Evaluation Treatment and pathological stage Less than 4 positive lymph nodes Adjuvant Treatment ER Positive HER2 Negative (see page 2 & 3 ) HER2 Positive
COME HOME Innovative Oncology Business Solutions, Inc.
 Innovative Oncology Business Solutions, Inc. Breast Cancer Diagnostic/Therapeutic Pathway V11, April 2015 Required Structured Data Fields: ICD9 Code Stage Staging Components Performance Status Treatment
Innovative Oncology Business Solutions, Inc. Breast Cancer Diagnostic/Therapeutic Pathway V11, April 2015 Required Structured Data Fields: ICD9 Code Stage Staging Components Performance Status Treatment
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID
 DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
38 years old, premenopausal, had L+snbx. Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI %
 38 years old, premenopausal, had L+snbx Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI67 5-10% Question: What will you do now? 1. Give adjuvant chemotherapy 2. Send for Oncotype
38 years old, premenopausal, had L+snbx Pathology: IDC Gr.II T-1.9cm N+2/4sn ER+100%st, PR+60%st, Her2-neg, KI67 5-10% Question: What will you do now? 1. Give adjuvant chemotherapy 2. Send for Oncotype
Breast Cancer: ASCO Poster Review
 Breast Cancer: ASCO Poster Review Carmen Criscitiello, MD, PhD Istituto Europeo di Oncologia Milano HER2+ SUBTYPE Research questions in early HER2+ BC De-escalation of toxicity without compromising efficacy
Breast Cancer: ASCO Poster Review Carmen Criscitiello, MD, PhD Istituto Europeo di Oncologia Milano HER2+ SUBTYPE Research questions in early HER2+ BC De-escalation of toxicity without compromising efficacy
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC)
") Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
Current Optimal Sequence and Duration of Endocrine Treatment
 [Symposium 7] Present and Future of Endocrine Therapy 07 Apr, 2018@GBCC Current Optimal Sequence and Duration of Endocrine Treatment Breast Oncology Center The Cancer Institute Hospital of JFCR Shinji
[Symposium 7] Present and Future of Endocrine Therapy 07 Apr, 2018@GBCC Current Optimal Sequence and Duration of Endocrine Treatment Breast Oncology Center The Cancer Institute Hospital of JFCR Shinji
Introduction. Ahmad Radzi 1*, Fabian Wei Luen Lee 2 REVIEW ARTICLE
 doi: 10.18282/amor.v4.i1.255 REVIEW ARTICLE Optimizing treatment-sequencing strategies for the management of postmenopausal women with hormone receptor-positive, HER2-negative advanced breast cancer: A
doi: 10.18282/amor.v4.i1.255 REVIEW ARTICLE Optimizing treatment-sequencing strategies for the management of postmenopausal women with hormone receptor-positive, HER2-negative advanced breast cancer: A
New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer
 New Evidence reports on presentations given at ASCO 2012 New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer Presentations at ASCO 2012 Breast
New Evidence reports on presentations given at ASCO 2012 New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer Presentations at ASCO 2012 Breast
Breast Cancer. Dr. Andres Wiernik 2017
 Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Manejo do câncer de mama RH+ na adjuvância: o que há de novo?
 II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico Manejo do câncer de mama RH+ na adjuvância: o que há de novo? INGRID A. MAYER, MD, MSCI Assistant Professor of Medicine Director,
II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico Manejo do câncer de mama RH+ na adjuvância: o que há de novo? INGRID A. MAYER, MD, MSCI Assistant Professor of Medicine Director,
Clinical Management Guideline for Breast Cancer
 Initial Evaluation Clinical Stage Pre-Treatment Evaluation Treatment and pathological stage Adjuvant Treatment Less than 4 positive lymph nodes ER Positive HER2 Negative (see page 2 & 3 ) Primary Diagnosis:
Initial Evaluation Clinical Stage Pre-Treatment Evaluation Treatment and pathological stage Adjuvant Treatment Less than 4 positive lymph nodes ER Positive HER2 Negative (see page 2 & 3 ) Primary Diagnosis:
Breast Cancer. Most common cancer among women in the US. 2nd leading cause of death in women. Mortality rates though have declined
 Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Transcript and References
 Richard S. Finn, MD Associate Professor of Medicine Division of Hematology/Oncology Co-director, Signal Transduction and Therapeutics Program Jonsson Comprehensive Cancer Center Geffen School of Medicine
Richard S. Finn, MD Associate Professor of Medicine Division of Hematology/Oncology Co-director, Signal Transduction and Therapeutics Program Jonsson Comprehensive Cancer Center Geffen School of Medicine
William J. Gradishar MD
 Northwestern University Feinberg School of Medicine Adjuvant Endocrine Therapy For Postmenopausal Women SOBO 2013 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley
Northwestern University Feinberg School of Medicine Adjuvant Endocrine Therapy For Postmenopausal Women SOBO 2013 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley
Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers
 日大医誌 75 (1): 10 15 (2016) 10 Original Article Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers Naotaka Uchida 1), Yasuki Matsui 1), Takeshi Notsu 1) and Manabu
日大医誌 75 (1): 10 15 (2016) 10 Original Article Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers Naotaka Uchida 1), Yasuki Matsui 1), Takeshi Notsu 1) and Manabu
Breast cancer update. Iryna Kuchuk, MD Oncology department Meir Medical Center
 Breast cancer update Iryna Kuchuk, MD Oncology department Meir Medical Center Overview Cancer Death Rates* Among Women, US,1930-2009 Factors Associated with Reduction In Breast Cancer Mortality Early
Breast cancer update Iryna Kuchuk, MD Oncology department Meir Medical Center Overview Cancer Death Rates* Among Women, US,1930-2009 Factors Associated with Reduction In Breast Cancer Mortality Early
Clinical Trial Results Database Page 1
 Page 1 Sponsor Novartis UK Limited Generic Drug Name Letrozole/FEM345 Therapeutic Area of Trial Localized ER and/or PgR receptor positive breast cancer Study Number CFEM345EGB07 Protocol Title This study
Page 1 Sponsor Novartis UK Limited Generic Drug Name Letrozole/FEM345 Therapeutic Area of Trial Localized ER and/or PgR receptor positive breast cancer Study Number CFEM345EGB07 Protocol Title This study
Breast cancer treatment
 Report from the San Antonio Breast Cancer Symposium Breast cancer treatment Determining the best options for select patient groups Sara Soldera, MD, Resident; Nathaniel Bouganim, MD, FRCPC, Medical Oncologist;
Report from the San Antonio Breast Cancer Symposium Breast cancer treatment Determining the best options for select patient groups Sara Soldera, MD, Resident; Nathaniel Bouganim, MD, FRCPC, Medical Oncologist;
Endocrine Therapy for Advanced Breast Cancer (ABC) Dr Yoon-Sim YAP Division of Medical Oncology, National Cancer Centre Singapore
 Dr Yoon-Sim YAP Division of Medical Oncology, National Cancer Centre Singapore") Endocrine Therapy for Advanced Breast Cancer (ABC) Dr Yoon-Sim YAP Division of Medical Oncology, National Cancer Centre Singapore Outline Guidelines and Evolving Clinical Treatment Landscape for HR+ HER2-
Endocrine Therapy for Advanced Breast Cancer (ABC) Dr Yoon-Sim YAP Division of Medical Oncology, National Cancer Centre Singapore Outline Guidelines and Evolving Clinical Treatment Landscape for HR+ HER2-
Breast Cancer. Saima Saeed MD
 Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
10/15/2012. Overcoming Endocrine Therapy Resistance. The Problem in ER+ Tumors is Endocrine Therapy Resistance
 Overcoming Endocrine Therapy Resistance Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology Slide Credits: Hope Rugo, MD The Problem in ER+ Tumors is Endocrine Therapy Resistance
Overcoming Endocrine Therapy Resistance Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology Slide Credits: Hope Rugo, MD The Problem in ER+ Tumors is Endocrine Therapy Resistance
Oncotype DX testing in node-positive disease
 Should gene array assays be routinely used in node positive disease? Yes Christy A. Russell, MD University of Southern California Oncotype DX testing in node-positive disease 1 Validity of the Oncotype
Should gene array assays be routinely used in node positive disease? Yes Christy A. Russell, MD University of Southern California Oncotype DX testing in node-positive disease 1 Validity of the Oncotype
Breast Cancer Diagnosis, Treatment and Follow-up
 Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
Breast Cancer Diagnosis, Treatment and Follow-up What is breast cancer? Each of the body s organs, including the breast, is made up of many types of cells. Normally, healthy cells grow and divide to produce
The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer
 The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer Cancer The Biology Century Understanding and treating the underlying tumor biology Cancer genetic studies demonstrate
The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer Cancer The Biology Century Understanding and treating the underlying tumor biology Cancer genetic studies demonstrate
Highlitghs in MBC First and second line endocrine treatments. Antonio Frassoldati Oncologia Clinica Ferrara
 Highlitghs in MBC First and second line endocrine treatments Antonio Frassoldati Oncologia Clinica Ferrara Which clinical scenario have to face First line therapy with today? Untreated metastatic breast
Highlitghs in MBC First and second line endocrine treatments Antonio Frassoldati Oncologia Clinica Ferrara Which clinical scenario have to face First line therapy with today? Untreated metastatic breast
Terapia adiuvante con inibitori delle Kinasi Cliclina Dipendenti 4/6: quale futuro? Filippo Montemurro
 Terapia adiuvante con inibitori delle Kinasi Cliclina Dipendenti 4/6: quale futuro? Filippo Montemurro Unit of Investigative Clinical Oncology Istituto di Candiolo (IRCCS) Disclosures Speaker s Honoraria
Terapia adiuvante con inibitori delle Kinasi Cliclina Dipendenti 4/6: quale futuro? Filippo Montemurro Unit of Investigative Clinical Oncology Istituto di Candiolo (IRCCS) Disclosures Speaker s Honoraria
Adjuvant Systemic Therapy in Early Stage Breast Cancer
 Adjuvant Systemic Therapy in Early Stage Breast Cancer Julie R. Gralow, M.D. Director, Breast Medical Oncology Jill Bennett Endowed Professor of Breast Cancer Professor, Global Health University of Washington
Adjuvant Systemic Therapy in Early Stage Breast Cancer Julie R. Gralow, M.D. Director, Breast Medical Oncology Jill Bennett Endowed Professor of Breast Cancer Professor, Global Health University of Washington
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint
 Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
Update mbc. endokrine Therapie
 Update mbc endokrine Therapie HR neg ER pos Endokrine Resistenz Endokrine Therapie 1 st line Postmenopause AI/Tam/Fulvestrant 84% AI+ Fulvestrant 33% AI (Tam) + Everolimus 84% AI + CDK4/6 92% Prämenopause
Update mbc endokrine Therapie HR neg ER pos Endokrine Resistenz Endokrine Therapie 1 st line Postmenopause AI/Tam/Fulvestrant 84% AI+ Fulvestrant 33% AI (Tam) + Everolimus 84% AI + CDK4/6 92% Prämenopause
The efficacy of second-line hormone therapy for recurrence during adjuvant hormone therapy for breast cancer
 517734TAM6210.1177/1758834013517734Therapeutic Advances in Medical OncologyR Mori and Y Nagao research-article2013 Therapeutic Advances in Medical Oncology Original Research The efficacy of second-line
517734TAM6210.1177/1758834013517734Therapeutic Advances in Medical OncologyR Mori and Y Nagao research-article2013 Therapeutic Advances in Medical Oncology Original Research The efficacy of second-line
Breast Cancer Earlier Disease. Stefan Aebi Luzerner Kantonsspital
 Breast Cancer Earlier Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Switzerland Breast Cancer Earlier Disease Diagnosis and Prognosis Local Therapy Surgery Radiation therapy Adjuvant
Breast Cancer Earlier Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Switzerland Breast Cancer Earlier Disease Diagnosis and Prognosis Local Therapy Surgery Radiation therapy Adjuvant
Agents in the Treatment of ER+ Aromatase Inbitor-Resistant Metastatic Breast Cancer: M-THOR Inhibitors
 Agents in the Treatment of ER+ Aromatase Inbitor-Resistant Metastatic Breast Cancer: M-THOR Inhibitors Valero, M.D., Professor of Medicine and Deputy Chairman Department of Breast Medical Oncology The
Agents in the Treatment of ER+ Aromatase Inbitor-Resistant Metastatic Breast Cancer: M-THOR Inhibitors Valero, M.D., Professor of Medicine and Deputy Chairman Department of Breast Medical Oncology The
Endocrine treatment might NOT be the preferred option in Hrpos MBC. Dr. Mircea Dediu Sanador Hospital Bucharest Summer School Bucharest 2015
 Endocrine treatment might NOT be the preferred option in Hrpos MBC Dr. Mircea Dediu Sanador Hospital Bucharest Summer School Bucharest 2015 Overall survival not improved by the AI treatment Benefit in
Endocrine treatment might NOT be the preferred option in Hrpos MBC Dr. Mircea Dediu Sanador Hospital Bucharest Summer School Bucharest 2015 Overall survival not improved by the AI treatment Benefit in
Immunoconjugates in Both the Adjuvant and Metastatic Setting
 Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
pan-canadian Oncology Drug Review Final Clinical Guidance Report Everolimus (Afinitor) for Advanced Breast Cancer March 25, 2013
 for Advanced Breast Cancer March 25, 2013") pan-canadian Oncology Drug Review Final Clinical Guidance Report Everolimus (Afinitor) for Advanced Breast Cancer March 25, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
pan-canadian Oncology Drug Review Final Clinical Guidance Report Everolimus (Afinitor) for Advanced Breast Cancer March 25, 2013 DISCLAIMER Not a Substitute for Professional Advice This report is primarily
Her 2 Positive Advanced Breast Cancer: From Evidence to Practice
 Her 2 Positive Advanced Breast Cancer: From Evidence to Practice Sunil Verma MD, FRCP(C) Medical Director, Tom Baker Cancer Center Professor and Head, Department of Oncology Cumming School of Medicine,
Her 2 Positive Advanced Breast Cancer: From Evidence to Practice Sunil Verma MD, FRCP(C) Medical Director, Tom Baker Cancer Center Professor and Head, Department of Oncology Cumming School of Medicine,
8/8/2011. PONDERing the Need to TAILOR Adjuvant Chemotherapy in ER+ Node Positive Breast Cancer. Overview
 Overview PONDERing the Need to TAILOR Adjuvant in ER+ Node Positive Breast Cancer Jennifer K. Litton, M.D. Assistant Professor The University of Texas M. D. Anderson Cancer Center Using multigene assay
Overview PONDERing the Need to TAILOR Adjuvant in ER+ Node Positive Breast Cancer Jennifer K. Litton, M.D. Assistant Professor The University of Texas M. D. Anderson Cancer Center Using multigene assay
Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer
 Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer Sara A. Hurvitz, MD, FACP Associate Professor of Medicine University of California Los Angeles Los Angeles, California Trastuzumab
Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer Sara A. Hurvitz, MD, FACP Associate Professor of Medicine University of California Los Angeles Los Angeles, California Trastuzumab
CDK4/6 inhibitors in advanced hormone receptor-positive breast cancer
 Perspective CDK4/6 inhibitors in advanced hormone receptor-positive breast cancer Romualdo Barroso-Sousa, Sara M. Tolaney Department of Medical Oncology, Dana-Farber Cancer Institute, Boston, MA, USA Correspondence
Perspective CDK4/6 inhibitors in advanced hormone receptor-positive breast cancer Romualdo Barroso-Sousa, Sara M. Tolaney Department of Medical Oncology, Dana-Farber Cancer Institute, Boston, MA, USA Correspondence
Expert Review: The Role of PARP Inhibition in the Treatment of Breast Cancer. Reference Slides
 Expert Review: The Role of PARP Inhibition in the Treatment of Breast Cancer Reference Slides Overview BRCA Mutations and Breast Cancer Patients with BRCA mutations have an estimated 55% to 65% cumulative
Expert Review: The Role of PARP Inhibition in the Treatment of Breast Cancer Reference Slides Overview BRCA Mutations and Breast Cancer Patients with BRCA mutations have an estimated 55% to 65% cumulative
Johns Hopkins Clinical Update Webinar
 Johns Hopkins Clinical Update Webinar Ben Ho Park, M.D., Ph.D. Department of Oncology Johns Hopkins University February 2015 This presentation is the intellectual property of the author/presenter. Contact
Johns Hopkins Clinical Update Webinar Ben Ho Park, M.D., Ph.D. Department of Oncology Johns Hopkins University February 2015 This presentation is the intellectual property of the author/presenter. Contact
Clinical activity of fulvestrant in metastatic breast cancer previously treated with endocrine therapy and/or chemotherapy
 ORIGINAL ARTICLE 2018 Mar 16. [Epub ahead of print] Clinical activity of fulvestrant in metastatic breast cancer previously treated with endocrine therapy and/or chemotherapy Mi Hwa Heo, Hee Kyung Kim,
ORIGINAL ARTICLE 2018 Mar 16. [Epub ahead of print] Clinical activity of fulvestrant in metastatic breast cancer previously treated with endocrine therapy and/or chemotherapy Mi Hwa Heo, Hee Kyung Kim,
Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012
 Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology, Emory
Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology, Emory
Hormonal Management of Metastatic Breast Cancer
 Hormonal Management of Metastatic Breast Cancer Dr. Khaled Abulkhair, PhD Medical Oncology SCE, Royal College, UK Ass. Professor of Clinical Oncology Mansoura University, Egypt Case For Discussion A 63
Hormonal Management of Metastatic Breast Cancer Dr. Khaled Abulkhair, PhD Medical Oncology SCE, Royal College, UK Ass. Professor of Clinical Oncology Mansoura University, Egypt Case For Discussion A 63
Predicting outcome in metastatic breast cancer
 Predicting outcome in metastatic breast cancer Aleix Prat, MD, PhD Medical Oncology Department Translational Genomics and Targeted Therapeutics in Solid Tumors Monday, 15 th January, Manchester, UK Disclosures
Predicting outcome in metastatic breast cancer Aleix Prat, MD, PhD Medical Oncology Department Translational Genomics and Targeted Therapeutics in Solid Tumors Monday, 15 th January, Manchester, UK Disclosures
ASCO and San Antonio Updates
 ASCO and San Antonio Updates 30 th Annual Miami Breast Cancer Conference March 7-10, 2013 Debu Tripathy, MD Professor of Medicine University of Southern California Norris Comprehensive Cancer Center Breakthroughs
ASCO and San Antonio Updates 30 th Annual Miami Breast Cancer Conference March 7-10, 2013 Debu Tripathy, MD Professor of Medicine University of Southern California Norris Comprehensive Cancer Center Breakthroughs
Department of Endocrine & Breast Surgery Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, India
 Department of Endocrine & Breast Surgery Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, India Evidence-Based Pragmatic SGPGI Breast Cancer Management Protocols (Summary) Background:
Department of Endocrine & Breast Surgery Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow, India Evidence-Based Pragmatic SGPGI Breast Cancer Management Protocols (Summary) Background:
Figure 1: PALLAS Study Schema. Endocrine adjuvant therapy may have started before randomization and be ongoing at that time.
 Figure 1: PALLAS Study Schema Endocrine adjuvant therapy may have started before randomization and be ongoing at that time. Approximately 4600 patients from approximately 500 global sites will be randomized
Figure 1: PALLAS Study Schema Endocrine adjuvant therapy may have started before randomization and be ongoing at that time. Approximately 4600 patients from approximately 500 global sites will be randomized
Update on the Management of HER2+ Breast Cancer. Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany
 Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Verzenio (abemaciclib) NEW PRODUCT SLIDESHOW
 NEW PRODUCT SLIDESHOW") Verzenio (abemaciclib) NEW PRODUCT SLIDESHOW Introduction Brand name: Verzenio Generic name: Abemaciclib Pharmacological class: Kinase inhibitor Strength and Formulation: 50mg, 100mg, 150mg, 200mg; tabs
Verzenio (abemaciclib) NEW PRODUCT SLIDESHOW Introduction Brand name: Verzenio Generic name: Abemaciclib Pharmacological class: Kinase inhibitor Strength and Formulation: 50mg, 100mg, 150mg, 200mg; tabs
My Personalized Breast Cancer Worksheet
 My Personalized Breast Cancer Worksheet KNOW For Early-Stage Breast Cancer. No Questions. Only Results. No two tumors are alike. What are the characteristics of your breast cancer and how will that effect
My Personalized Breast Cancer Worksheet KNOW For Early-Stage Breast Cancer. No Questions. Only Results. No two tumors are alike. What are the characteristics of your breast cancer and how will that effect
Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology, Emory University, Chief of
 Endocrine Therapy of Advanced Breast Cancer School of Breast Oncology November 9 th 2013 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology,
Endocrine Therapy of Advanced Breast Cancer School of Breast Oncology November 9 th 2013 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology,
Oncology. A CME-certified Supplement to the. Journal of the National Comprehensive Cancer Network. Program Overview/Statement of Need
 JNCCN Volume 16 1 Journal of the National Comprehensive Cancer Network A CME-certified to the Journal of the National Comprehensive Cancer Network Program Overview/Statement of Need Recently updated guidelines
JNCCN Volume 16 1 Journal of the National Comprehensive Cancer Network A CME-certified to the Journal of the National Comprehensive Cancer Network Program Overview/Statement of Need Recently updated guidelines
Case Scenario 1 History and Physical 3/15/13 Imaging Pathology
 Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Intro to Cancer Therapeutics
 An Intro to Cancer Therapeutics Christopher R. Chitambar, MD Professor of Medicine Division of Hematology & Oncology Froedtert and Medical College of Wisconsin Clinical Cancer Center cchitamb@mcw.edu Intro
An Intro to Cancer Therapeutics Christopher R. Chitambar, MD Professor of Medicine Division of Hematology & Oncology Froedtert and Medical College of Wisconsin Clinical Cancer Center cchitamb@mcw.edu Intro
SYNOPSIS PROTOCOL TALBOT
 SYNOPSIS PROTOCOL TALBOT A) CLINICAL TRIAL IDENTIFICATION SPONSOR - PROTOCOL CODE NUMBER : VERSION: SYNOPSIS V4.0-30/06/2015 TRIAL TITLE : Open-label, randomized, multicenter, phase II study, comparing
SYNOPSIS PROTOCOL TALBOT A) CLINICAL TRIAL IDENTIFICATION SPONSOR - PROTOCOL CODE NUMBER : VERSION: SYNOPSIS V4.0-30/06/2015 TRIAL TITLE : Open-label, randomized, multicenter, phase II study, comparing
Sponsor / Company: Sanofi Drug substance(s): SAR (iniparib)
: SAR (iniparib)") These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
These results are supplied for informational purposes only. Prescribing decisions should be made based on the approved package insert in the country of prescription. Sponsor / Company: Sanofi Drug substance(s):
Nadia Harbeck Breast Center University of Cologne, Germany
 Evidence in Favor of Taxane Based Combinations and No Anthracycline in Adjuvant and Metastatic Settings Nadia Harbeck Breast Center University of Cologne, Germany Evidence in Favor of Taxane Based Combinations
Evidence in Favor of Taxane Based Combinations and No Anthracycline in Adjuvant and Metastatic Settings Nadia Harbeck Breast Center University of Cologne, Germany Evidence in Favor of Taxane Based Combinations