The Multi-Modality Clinical Model for SBRT/SABR (Pancreatic Cancer)
|
|
|
- Amy Bell
- 6 years ago
- Views:
Transcription



 Pancreatic Cancer: Stereotactic Body Radiation")

1 Stereotactic Body Radiation Therapy (SBRT) for Pancreatic Cancer December 9, 2016 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: Toll Only: or Submit a question to the Event Producer via the Q&A Panel The Multi-Modality Clinical Model for SBRT/SABR (Pancreatic Cancer) Pancreatic Cancer: Stereotactic Body Radiation Therapy (SBRT) & Translational Paradigms Joseph Herman, MD, MSc Professor Director, Clinical Research Department of Radiation Oncology MD Anderson Cancer Center 1
2 Disclosure Relevant Financial Relationship(s) AbbVie, Oncosil, and BTG: Consulting Viragh Family Foundation: Funding for trial Gonzalez and McKnight Family Foundations: Translational Studies Off Label Usage Aduro: GVAX Merck: Pembro Overview In 2015, approximately 48,960 people were diagnosed with PCA Nearly 40% of PCA patients present with non-metastatic localized disease 2
 Pancreatic MDC: Case Review Present Cases using outline Review")
3 What stage am I? Resectable Borderline Resectable Unresectable or Locally Advanced Metastatic (tumor spread beyond the pancreas and to another location) Pancreatic MDC: Case Review Present Cases using outline Review Pathology Review Images CT/PET/MRI/ EUS Discuss Case and reach consensus See patients and discuss options Enroll in trials/studies Dictate note and cc to referring physician Nutrition, Pain, Enzymes 3


")

4 Where is my pancreas? Where is my tumor? Resectability: Contact with Veins Less than 180º More than 180º Deformity Slide(s) courtesy of Dr. Mahmoud Al-Hawary ** Veins can be reconstructed 4



5 Resectability: Contact with Arteries Assessment based on: Degree of tumor contact with the vessel circumference Whether vessel caliber narrowing or contour deformity is present Less than 180º More than 180º Deformity Difficult to resect arteries Slide(s) courtesy of Dr. Mahmoud Al-Hawary Prospective Identification of Anatomically Resectable Pancreatic Cancer by CT Scan 1. Absence of disease outside of the pancreas 2. Tissue plane between tumor and SMA/CA 3 V A T 2 3. Open SMV-PV confluence 1 Use of these criteria yield high rates of microscopically complete (R0) resection 5
 Deemed resectable Neoadjuvant therapy recommended Tumor encases a major blood vessel(s) Deemed unresectable or LAPC New role for definitive therapy Resection")
6 Borderline Resectable and Locally Advanced Pancreatic Cancer Borderline Resectable Locally Advanced (Unresectable) SMA Patient Selection? SMA Tumor abuts a major blood vessel(s) Deemed resectable Neoadjuvant therapy recommended Tumor encases a major blood vessel(s) Deemed unresectable or LAPC New role for definitive therapy Resection Determined by Vessel Involvement Resectable Borderline Locally advanced SMV/PV AHPBA/SSO/SSAT/NCCN Resectable No contact Borderline Abut, encase or occlude Locally Advanced Not reconstructable SMA No contact Abut Encased CHA No contact Abut or shortsegment encase Long-segment encase Celiac Trunk No contact <180 >180 6

7 We need better systemic therapy AND radiation therapy! Medical Oncology Radiation Oncology Locally Advanced and Borderline Resectable PCA Treatment focus is on performance status rather than stage: ECOG 0-1, young FFX ECOG >1 or elderly GEM or GEM/NAB-P Maximize chemotherapy 4-6 months then reevaluate for local therapy (radiation +/- surgery) 7
8 Chemotherapy: Systemic Therapy Gemcitabine Gemcitabine + X Gemcitabine + Abraxane FOLFIRINOX (5-FU, Irinotecan, Oxaliplatin) Immunotherapy Targeted therapy NCCN Guidelines Rationale for More Intense Local Treatment in LAPC 30% Local only disease JHU Autopsy Series 60% Local progression - MDACC phase II trial Patients die of biliary, gastric, SMV/portal obstruction Iacobuzio-Donahue et al, JCO, 2009 Crane et al, JCO,



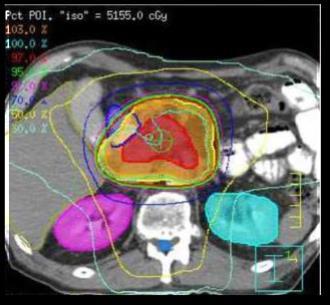
9 Potential Effects of Radiation SBRT CRT Tumor SMV SMA Positive Surgical Margin Well-vascularized rim, hypoxic core Outline of Tumor Mass on CT Slide courtesy of Chris Crane, MD Stereotactic RT: Modern Treatment Devices CYBER-KNIFE TRILOGY SYNERGY 9

10 007: Stereotactic Body Radiation Therapy (SBRT)? Goldfinger (1964) Evolution of Radiation Therapy 3-D CRT IMRT IMRT Plan ABC IGRT SBRT Plan 10




 SBRT")
")
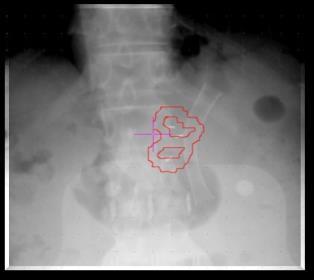
11 What Are Fiducials? Civco Knurled Gold Fiducials Gold Anchor Core Oncology Visicoil Civco Coupled Markers Placed via endoscopic ultrasound (similar to biopsy) SBRT Planning & Delivery (videos) Respiratory Control Plan Quality Assurance 11


 IMRT Dose")
12 GI Atlas Intensity Modulated RT Planning & Delivery PTV Treatment Plan (1.75 Gy x 30 fractions) IMRT Dose Volume Histogram 12

 Tumor Treatment Plan (5-6.")
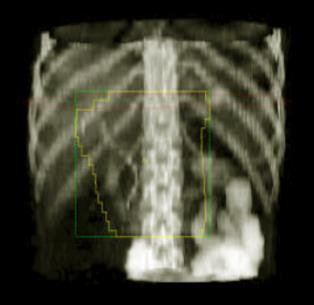
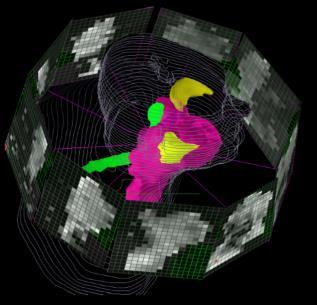
13 MDACC Dose Escalation - LAPC IMRT Gy/Image guided + breath hold N=49 63Gy-70Gy / 28 fx ms-22.6 mo N= Gy / 28fx ms- 17.9mo Krishnan and Crane IJROBP 2016 Stereotactic Body Radiation Therapy (SBRT) Planning & Delivery (fiducials and breath hold) Tumor Treatment Plan (5-6.6 Gy x 5 fractions) SBRT Dose Volume Histogram 13
14 JHU SBRT: Overall Survival Median OS from diagnosis = 20.1 mos (95% CI: ) Data with standard chemoradiation for pancreas cancer 14

15 Patient with BLR PDAC (Intergroup Definition) P R E- R E GI S T E R E N R O L L m FOLFIRINOX 2 months R E S T A G E 50.4g EBRT + CAPE R E S T A G E SURGERY R E S T A G E GEM 2 months F O L L O W Centralized radiographic review of pretreatment and restaging studies Prospective QC of all modalities Protocol-mandated operative indications and procedures Analysis and reporting of survival rates and objective response metrics What did we learn from A021101? FOLFIRINOX and Radiation is Acceptable in Borderline (non-metastatic disease) R0 operations possible in 64% patients but vascular resection 80% 33% resections <5% viable cells, 13% pcr (no tumor) 1/3 resected patients did not start postop chemo, emphasizing need for more preoperative Rx Median OS of all enrolled patients: 22 months Katz, JAMA Surg
 +")

16 Role of Radiation Therapy in Locally Advanced Disease (LAPC)? GERCOR LAP-07 Trial Unresectable PCA 1st Gemcitabine x 4 months Gemcitabine plus erlotinib x 4 months 2nd Gemcitabine x 2 months RT (5400 cgy) + capecitabine Gemcitabine plus erlotinib x 2 months RT (5400 cgy) + capecitabine None None Erlotinib Erlotinib Hummel et al, JAMA 2016 Role of Radiation Therapy in Locally Advanced Disease (LAPC)? No survival benefit with RT Only 60% included in 2 nd randomization Local control benefit with RT With better chemotherapy, perhaps RT would have a larger impact Hummel et al, JAMA
17 What Is The Role of Neoadjuvant Therapy in LAPC? - LAP 07 Study 449 patients (4%) underwent a curative-intent resection Eleven patients (2.5%) had an R0 resection Median OS was 30.9 months Can we increase the proportion of patients getting surgery with improved systemic therapy and IMRT or SBRT? Hammel et al 2016, JAMA Benefits of SBRT vs. Standard Chemoradiation Shorter duration of radiation (3-5 days vs. 30 days) Improved quality of life Limit delay of chemotherapy and time to surgery Easily combined with other modalities Higher resection rates?? Less acute GI toxicity 17
 Toxicity Schellenberg (2008) 16 25Gy x1 100% 11.")
 39 8-12Gy x3 85% 20 41% G1-2, 9% G3 Rwigema (2011) 71 24Gy x1* 49% 10.3 39.5% G1-2, 4.2% G3 Schellenberg (2011) 20 25Gy x1 94% 11.")
18 Treatment Volumes and Dosimetry: SBRT vs. IMRT A B C D E F Pancreas SBRT Studies Study N Dose Local Control at 1 Year OS (mos) Toxicity Schellenberg (2008) 16 25Gy x1 100% % G2-4 Didolkar (2010) Gy x3 92% % G3+ Mahadevan (2010) Gy x3 78% % G1-2, 8% G3 Polistina (2010) 23 10Gy x3 50% % G1 Mahadevan (2011) Gy x3 85% 20 41% G1-2, 9% G3 Rwigema (2011) 71 24Gy x1* 49% % G1-2, 4.2% G3 Schellenberg (2011) 20 25Gy x1 94% % G1-2, 5% G3 Goyal (2012) Gy x1* 81% % G1-2, 16% G3 Lominska (2012) Gy x3-5 86% 5.9 7% G3 Gurka (2013) 10 5Gy x5 40% % Chuong (2013) Gy x5 81% % G3 18
 until toxicity or progression Primary endpoint: Late GI Toxicity > 4 months (40% to 20%) Secondary endpoints: Tumor Progression Free Survival,")
19 Phase II Multi-institutional Trial: Gemcitabine + SBRT (n=49) Johns Hopkins, Stanford, Memorial Sloan Kettering (Gem, up to 1 Cycle allowed) 1 week break F-SBRT 6.6 Gy x 5 Mon-Fri 1 week break Gem (3 wks on, 1 wk off) until toxicity or progression Primary endpoint: Late GI Toxicity > 4 months (40% to 20%) Secondary endpoints: Tumor Progression Free Survival, pre-tx biopsy, PET/CT, QOL, biomarkers Key features: Central review, dose constraints, RT quality assurance Herman JM et al. Cancer 2015 Median OS: 13.9 mos Median PFS: 7.9 mos Herman JM et al. Cancer
 Ulcer (3) Quality of Life (EORTC) Mean global QOL: Scores unchanged pre/post SBRT Surgery 5 (10%) were deemed resectable after therapy 1")

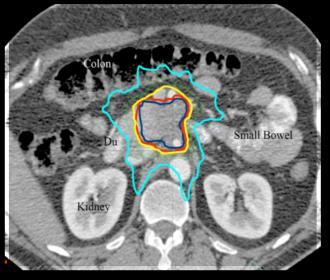
20 Phase II Multi-institutional Trial: SBRT Toxicity and QOL Toxicity Acute GI Grade 2: 0% Grade 3: 12.2% Late GI Grade 2: 2.1% Enteritis Grade 3: 8.5% Fistula (1) Ulcer (3) Quality of Life (EORTC) Mean global QOL: Scores unchanged pre/post SBRT Surgery 5 (10%) were deemed resectable after therapy 1 (2%) denied surgery The remaining 4 (8%) patients underwent margin- and node-negative resection LAPC patients may successfully be resected?! Herman JM et al. Cancer 2015 Simultaneous Integrated Boost (SIB)- Based SBRT Dose Escalation SIB delivers high doses to the tumor/ vessel interface Tuli et al. Rad Res
 Radiation therapy ULTIMATE GOAL Surgery +/- IRE Radiation")



 # MGH N=188 BR: 14 LAPC: 26 FFX CRT: 14 CRT/IORT: 10 Proton: 6 92%")
21 Current Approach Appropriate Staging Maximize chemo (4-6 months) Maximize chemo ( 6 months) Radiation therapy ULTIMATE GOAL Surgery +/- IRE Radiation therapy Maintenance chemotherapy?? LAPC: Neoadjuvant Multi-agent Chemotherapy +/- Radiation Therapy Study Surgery N Neodjuvant Chemo Radiation Type R0 Resection Med OS or Path Reponse Moffitt N=159 BR: 51 LAPC: 5 GTX 81% BR FFX 43% LA SBRT: All Gy/5 Fx BR: 96% LAPC: 100% 34.2 mos Hopkins N=88 BR: 4 LAPC: 15 Mixed SBRT: All 33 Gy/5 Fx 84% 22 mos MSKCC N=101 LAPC: 31 FFX 6 mos CRT: 50%* Chemo: 79% **CRT: 33% PR: >50% (75 vs. 22) # MGH N=188 BR: 14 LAPC: 26 FFX CRT: 14 CRT/IORT: 10 Proton: 6 92% ~32 mos *75% Gem based, **Vasc resection rate 47 vs. 7, # favor of CRT Mellon; Moningi; Sadot; Ferrone et al. 21




22 Which Patients Should Be Taken to Surgery Following Neoadjuvant Therapy? Most tumors do not shrink after neoadjuvant therapy There is a treatment effect Chemo SBRT Surgery 22
 45 (41%) Male gender 39 (58%) 56 (51%) Caucasian race 60 (90%) 98 (89%) Head of pancreas lesion 50 (75%) 77 (70%) Locally")
 100 90 80 70 60 50 40 30 20 10 0 % Margin Negativity 83% 57% Chemo SBRT 100 90 80 70 60 50 40 30 20 10 0 % Node Negativity 60% 40%")
23 Hopkins: Neoadjuvant Chemo vs. Chemo + SBRT (N=177) : Median Follow-up 17.0 mos Characteristic Chemo group, n (%) Chemo/SBRT group, n (%) No. patients Age (43%) 45 (41%) Male gender 39 (58%) 56 (51%) Caucasian race 60 (90%) 98 (89%) Head of pancreas lesion 50 (75%) 77 (70%) Locally advanced disease 16 (24%) 56 (51%) FOLFIRINOX-based chemotherapy Chemotherapy duration 4 months 34 (51%) 79 (72%) 20 (30%) 63 (57%) Hopkins: Neoadjuvant Chemo vs. Chemo + SBRT (N=177) % Margin Negativity 83% 57% Chemo SBRT % Node Negativity 60% 40% Chemo SBRT 23
24 Pathologic Complete Response or Near Pathologic Complete Response Pathologic complete response (pcr) No residual tumor can be identified or measured Near pcr Scattered microscopic foci of single cells or groups of single cells Typically within a dense area of fibrosis Demonstrating marked treatment effect Hopkins: Neoadjuvant Chemo vs. Chemo + SBRT (N=177) % pcr % Near pcr % % 30% 5 0 0% Chemo SBRT 5 0 Chemo SBRT SBRT does improve pathologic response but higher doses are needed for ablation 24

25 Proposed Alliance A021501: Preoperative Extended Chemotherapy Vs. Chemotherapy Plus Hypofractionated Radiation Therapy for BRPC of the Head of The Pancreas Arm A P R E - R E G I S T R A T I O N E N R O L L R A N D O MI Z E mffx x 4 cycles Arm B mffx x 4 cycles mffx x 4 cycles mffx x 3 cycles SBRT Surgery Surgery FOLFOX x 4 cycles F O L L O W FOLFOX x 4 cycles F O L L O W Central review of baseline imaging Central review of radiation QI Central review of preoperative imaging Central review of pathology Know Your Tumor KYT at enrollment = Re-staging Surgical Exploration in LAPC Radiographic evidence of tumor downstaging is not required for surgical evaluation Under multidisciplinary review, consider the following: 1. 4 months of chemotherapy and no distant metastases 2. Good performance status/no limiting comorbidities 3. Stable or improved CA 19-9, technically resectable 4. Ideally, <12 weeks after SBRT Katz MH, et al. Cancer. 2012;118(23): Dholakia AS, et al.. J Radiat Oncol Dec;2(4):
26 Does multi-agent chemotherapy combined with SBRT lead to improved survival and improve the likelihood that patients with LAPC undergo surgery? Results: Patient & Tumor Characteristics July 2010 to April 2015, 117 patients with LAPC received definitive Chemo + SBRT Patient or tumor characteristic N=117 Median age at diagnosis, years (range) 65 (36-88) Caucasian race 84% Male gender 52% Median baseline KPS (range) 90 (80-100) Head of pancreas tumor 58% Rosati and Herman et al. 26
27 Results: Treatment Characteristics Induction chemotherapy agent(s) None Gemcitabine-based (alone*, gem+nab-p, GTX, gem/cis) FOLFIRINOX-based Combination of both Induction chemotherapy duration (months) Median (range) 4 months SBRT dose (Gy) Median (range) 33 Gy Time in months, median (range) From diagnosis to SBRT From SBRT to the end of follow-up From diagnosis to the end of follow-up N=117 8% 49% 33% 10% 2.8 (0-22.3) 38% 33.0 ( ) 73% 4.0 ( ) 13.6 ( ) 19.4 ( ) *31% of patients received gemcitabine alone on a clinical trial or due to poor performance status Results: Overall Survival Median OS from diagnosis = 20.1 mos (95% CI: ) Median OS from SBRT = 14.5 mos (95% CI: ) 27
28 Overall Survival By Induction Chemotherapy Type / Duration No chemo Single-agent GEM Multi-agent chemo Gem-based chemo FFX-based chemo <4 months chemo 4 months chemo Results: Surgical Implications LAPC (n=117) Surgery (n=42) No Surgery (n=75) Successful resection* (n=33) Aborted (n=3) IRE (n=6) Distant Mets (n=46) R0 Resection (91%) Vessel Involvement (n=17) N0 Resection (82%) Performance Status (n=10) Path CR (15%) Other (n=2) 28
29 Results: Surgical Implications LAPC (n=117) Surgery (n=42) No Surgery (n=75) Successful resection* (n=33) Aborted (n=3) IRE (n=6) Distant Mets (n=46) R0 Resection (91%) Vessel Involvement (n=17) N0 Resection (82%) Performance Status (n=10) Path CR (15%) Other (n=2) *Three patients went to surgery + IRE Results: Surgical Implications LAPC (n=117) Surgery (n=42) No Surgery (n=75) Successful resection* (n=33) Aborted (n=3) IRE (n=6) Distant Mets (n=46) 39% R0 Resection (91%) Vessel Involvement (n=17) 15% N0 Resection (82%) Performance Status (n=10) 9% Other (n=2) 2% *Three patients went to surgery + IRE 29
30 Results: Surgical Implications LAPC (n=117) Surgery (n=42) No Surgery (n=75) Successful resection* (n=33) Aborted (n=3) IRE (n=6) Distant Mets (n=46) 39% R0 Resection (91%) Vessel Involvement (n=17) 15% N0 Resection (82%) Performance Status (n=10) 9% Other (n=2) 2% *Three patients went to surgery + IRE Results: Surgical Resection and Overall Survival Median OS (mos) P-value Surgery vs. no surgery 29.7 vs R0 resection vs. R1/R2 resection 34.7 vs
31 Current Study: Pancreatic Cancer Research Study (PanCRS) Induction Chemotherapy: mfolfirinox x 4 cycles Restage Stable or Better Disease Progression Arm 1 mfolfirinox Randomize Arm 2 SBRT+mFOLFIRINOX 8 Gy x 5 Off Study Participating Institutions: Stanford, UCSF, UCLA, Loyola, BC Cancer Agency, Duke, UTSW Pancreas SBRT: Patient selection for surgery Clinical stage is determined by imaging Can biomarkers determine a local vs. systemic profile at diagnosis and guide management Imaging (PET, CT) Tumor Sequencing Immunohistochemistry (core/cell block) ctdna (tumor/plasma) 31
 (B) Test set (12 cases) (C) Validation set (37 cases) Courtesy of Eugene Koay Clinical associations for low and high delta tumors Patient cohort: 101")
.")
32 Association of stroma and delta measurement High delta tumors have lower stroma content. (A) (B) Test set (12 cases) (C) Validation set (37 cases) Courtesy of Eugene Koay Clinical associations for low and high delta tumors Patient cohort: 101 patients who underwent upfront surgery for resectable PDAC Proportions of patients having metastasis within 6 months Overall survival Patients with high delta tumor showed poor prognosis (early distant metastasis, shorter overall survival ). The delta classification is an independent predictor of distant metastasis-free survival and overall survival. Courtesy of Eugene Koay 32

 On MVA, PET avidity at baseline")

33 After Before 12/12/2016 SBRT Tumor Response by PET Mean SUVmax (p<0.001) Mean SUVpeak (p<0.001) On MVA, PET avidity at baseline predicted for poor survival Herman et al. Cancer 2015 Total Lesion Glycolysis Predicts Path Response to Neoadj Therapy 33
 Gross tumor pathology comparison.")
 Liver specimen from pt with extensive metastatic disease.")
34 Patient Selection Smad4 (Dpc4) Status Dpc4/Smad4 Wild-Type (Local) Dpc4/Smad4 Mutant (Systemic) Gross tumor pathology comparison. A) Pancreas specimen from pt with locally advanced disease. B) Liver specimen from pt with extensive metastatic disease. Iacobuzio-Donahue et al, JCO,

35 How can we enhance the effects of RT or use RT to enhance immunotherapy? 35
 and Targeted")


36 Small Animal Radiation Research Platform: Bioluminescent Imaging (BLI) and Targeted Radiation in Small Animals Mouse SBRT SARRP Research Platform. PARP Inh In Vivo C Tuli et al, Trans Onc 2015 Tuli, et al, Rad Res 2013 Tuli, et al, Trans Onc



37 Phase I study: ABT-888 in combination with gemcitabine and IMRT for LAPC (VelGemRad) Gemcitabine: IV infusion of 1000 mg/m 2 on days 1, 8, 15 of the cycle IMRT: 36 Gy in 15 fractions (2.4 Gy/day, M-F) Veliparib: administered per dose escalation schema, 60 mg BID 1 Objective: to determine the MTD, safety and toxicity profile 2 Objectives: Measure the clinical activity of the treatment (RECIST 1.1) Evaluate tumor/blood pre/during/post treatment for DNA damage/repair proteins Assess pre-tx germline/somatic/epigenetic mutations in BRCA1/2, PALB2, PTEN Tuli et al, in preparation 73 SBRT: Immune Modulation Kamrava M., Hodge JW., et al. Mol. BioSyst., Adapted with Permission (Andrew Sharabi) 37
 Future Directions: Pancreas Vaccine GVAX: GM-CSF Secreting,")

38 SBRT Treatment Response Gross: 3.8 cm (Extensive Treatment Effects) Future Directions: Pancreas Vaccine GVAX: GM-CSF Secreting, Allogeneic, Whole Tumor Cell Vaccine GVAX GM-CSF Dendritic Cell Tumor Cell Destruction Mesothelin Tumor antigen Antigen uptake & Activation May Inhibit recurrence Limited toxicity Combined with other therapies T Cell Activation & Proliferation T Cell 38




39 Blocking CTLA-4 and PD-1 Tumor Microenvironment Activation (cytokines, lysis, proliferation, migration to tumor) Dendritic cell MHC B7 TCR CD B7 CTLA anti-ctla-4 CTLA-4 Blockade +++ T cell T cell TCR MHC PD-1 PD-L1 anti-pd-1 PD-1 PD-L2 anti-pd-1 PD-1 Blockade Tumor cell FFX +SBRT + GVAX + Anti-PD-1 in Patients with LAPC Anti-PD-1 39
:150-158 Conclusions: Multi-agent chemotherapy improves survival (>4 months) FFX > Gem/Abx SBRT improves R0 resections and path response with limited toxicity or delay")
40 Proton Beam Therapy Ling TC et al. Transl Cancer Res 2012;1(3): Conclusions: Multi-agent chemotherapy improves survival (>4 months) FFX > Gem/Abx SBRT improves R0 resections and path response with limited toxicity or delay Select LAPC patients can have surgery with favorable OS Local and distant progression still common Need better maintenance therapies Support clinical trials P s: Pain, Panc Enzymes, PANCAN, PMDC 40


41 Johns Hopkins MD Anderson 41


42 May the force be with you and Happy Holidays! Thank you for your participation. If you have questions, please contact Patient Central at PANCAN or 42
Pancreatic Cancer and Radiation Therapy
 Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
Pancreatic Cancer and Radiation Therapy Why? Is there a role for local therapy with radiation in a disease with such a high rate of distant metastases? When? Resectable Disease Is there a role for post-op
Alliance A Alliance SWOG ECOG/ACRIN - NRG
 Preoperative chemotherapy and chemotherapy plus hypofractionated radiation therapy for borderline resectable adenocarcinoma of the head of the pancreas Alliance A021501 Alliance SWOG ECOG/ACRIN - NRG Clinical
Preoperative chemotherapy and chemotherapy plus hypofractionated radiation therapy for borderline resectable adenocarcinoma of the head of the pancreas Alliance A021501 Alliance SWOG ECOG/ACRIN - NRG Clinical
THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA. TIMUR MITIN, MD, PhD
 THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA TIMUR MITIN, MD, PhD RESECTABLE DISEASE MANAGEMENT: RESECTABLE DISEASE Resection offers the only possibility of long term survival
THE ROLE OF RADIATION THERAPY IN MANAGEMENT OF PANCREATIC ADENOCARCINOMA TIMUR MITIN, MD, PhD RESECTABLE DISEASE MANAGEMENT: RESECTABLE DISEASE Resection offers the only possibility of long term survival
SBRT in Pancreas Cancer Role of The Radiosurgery Society
 SBRT in Pancreas Cancer Role of The Radiosurgery Society Anand Mahadevan MD FRCS FRCR Chairman Division of Radiation Oncology Geisinger Health System, Danville, PA, USA. Past President and Chairman: The
SBRT in Pancreas Cancer Role of The Radiosurgery Society Anand Mahadevan MD FRCS FRCR Chairman Division of Radiation Oncology Geisinger Health System, Danville, PA, USA. Past President and Chairman: The
Questions may be submitted anytime during the presentation.
 Understanding Radiation Therapy and its Role in Treating Patients with Pancreatic Cancer Presented by Pancreatic Cancer Action Network www.pancan.org August 18, 2014 If you experience technical difficulty
Understanding Radiation Therapy and its Role in Treating Patients with Pancreatic Cancer Presented by Pancreatic Cancer Action Network www.pancan.org August 18, 2014 If you experience technical difficulty
ARROCase: Borderline Resectable Pancreatic Cancer
 ARROCase: Borderline Resectable Pancreatic Cancer Resident: Jordan Kharofa, MD Staff: Beth Erickson, MD 8/2012 Medical College of Wisconsin Department of Radiation Oncology Case Presentation: 60 year old
ARROCase: Borderline Resectable Pancreatic Cancer Resident: Jordan Kharofa, MD Staff: Beth Erickson, MD 8/2012 Medical College of Wisconsin Department of Radiation Oncology Case Presentation: 60 year old
The 2010 Gastrointestinal Cancers Symposium Oral Abstract Session: Cancers of the Pancreas, Small Bowel and Hepatobilliary Tract
 The 2010 Gastrointestinal Cancers Symposium : Cancers of the Pancreas, Small Bowel and Hepatobilliary Tract Abstract #131: Phase I study of MK 0646 (dalotuzumab), a humanized monoclonal antibody against
The 2010 Gastrointestinal Cancers Symposium : Cancers of the Pancreas, Small Bowel and Hepatobilliary Tract Abstract #131: Phase I study of MK 0646 (dalotuzumab), a humanized monoclonal antibody against
Overview. What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013
 What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013 Overview Staging and Workup Resectable Disease Surgery Adjuvant therapy Locally
What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013 Overview Staging and Workup Resectable Disease Surgery Adjuvant therapy Locally
Upper Gastrointestinal. Friday, March 2, :00 p.m. 2:45 p.m.
 Upper Gastrointestinal Friday, March 2, 2018 2:00 p.m. 2:45 p.m. Social Q&A Use your phone, tablet, or laptop to Submit questions to speakers and moderators Answer interactive questions / audience response
Upper Gastrointestinal Friday, March 2, 2018 2:00 p.m. 2:45 p.m. Social Q&A Use your phone, tablet, or laptop to Submit questions to speakers and moderators Answer interactive questions / audience response
Where are we with radiotherapy for biliary tract cancers?
 Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Where are we with radiotherapy for biliary tract cancers? Professor Maria A. Hawkins Associate Professor in Clinical Oncology MRC Group Leader/Honorary Consultant Clinical Oncologist CRUK MRC Oxford Institute
Surgical Management of Pancreatic Cancer
 I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
I Congresso de Oncologia D Or July 5-6, 2013 Surgical Management of Pancreatic Cancer Michael A. Choti, MD, MBA, FACS Department of Surgery Johns Hopkins University School of Medicine, Baltimore, MD Estimated
Pancreas SBRT. Rakendu Shukla, MD KyNam Nguyen, MD Brandon Dyer, MD Faculty Advisor: Arta Monjazeb, MD PhD University of California - Davis
 Pancreas SBRT Rakendu Shukla, MD KyNam Nguyen, MD Brandon Dyer, MD Faculty Advisor: Arta Monjazeb, MD PhD University of California - Davis December 19, 2018 Clinical Presentation 48 year old woman initially
Pancreas SBRT Rakendu Shukla, MD KyNam Nguyen, MD Brandon Dyer, MD Faculty Advisor: Arta Monjazeb, MD PhD University of California - Davis December 19, 2018 Clinical Presentation 48 year old woman initially
Dr Roopinder Gillmore July 2017
 Dr Roopinder Gillmore July 2017 Resectable Borderline / locally advanced Metastatic 15-20% 15-20% 60-70% 22-28 months 9-15 months 6-12 months Does the patient have resectable disease?? Definitely not
Dr Roopinder Gillmore July 2017 Resectable Borderline / locally advanced Metastatic 15-20% 15-20% 60-70% 22-28 months 9-15 months 6-12 months Does the patient have resectable disease?? Definitely not
Ablative Radiation Therapy For Inoperable Cholangiocarcinoma. Christopher H. Crane, M.D. Program Director, GI Section Department of Radiation Oncology
 Ablative Radiation Therapy For Inoperable Cholangiocarcinoma Christopher H. Crane, M.D. Program Director, GI Section Department of Radiation Oncology Facts about radiation treatment High doses (2x the
Ablative Radiation Therapy For Inoperable Cholangiocarcinoma Christopher H. Crane, M.D. Program Director, GI Section Department of Radiation Oncology Facts about radiation treatment High doses (2x the
Stereotactic MR-guided adaptive radiation therapy (SMART) for locally advanced pancreatic tumors
 for locally advanced pancreatic tumors") Stereotactic MR-guided adaptive radiation therapy (SMART) for locally advanced pancreatic tumors Anna Bruynzeel, Radiation Oncologist VU University Medical Center, Amsterdam, The Netherlands Current standard
Stereotactic MR-guided adaptive radiation therapy (SMART) for locally advanced pancreatic tumors Anna Bruynzeel, Radiation Oncologist VU University Medical Center, Amsterdam, The Netherlands Current standard
Pancreatic Adenocarcinoma
 Pancreatic Adenocarcinoma AProf Lara Lipton 28 April 2018 Percentage alive 5 years after diagnosis for men and women Epidemiology 6% of cancer related deaths worldwide 4 th highest cause of cancer death
Pancreatic Adenocarcinoma AProf Lara Lipton 28 April 2018 Percentage alive 5 years after diagnosis for men and women Epidemiology 6% of cancer related deaths worldwide 4 th highest cause of cancer death
Pancreatic Cancer. BIOLOGY: Not well defined (genetic and enviromental factors) CLINICAL PRESENTATION: Abd pain, jaundice, weight loss.
 CLINICAL PRESENTATION: Abd pain, jaundice, weight loss.") EloreMed Editor: Le Wang, MD, PhD Date of Update: 2/6/2018 UpToDate: Liposomal irinotecan (Onivyde) plus FU/LV is now approved for gemcitabine-refractory metastatic pancreatic cancer and recommended by
EloreMed Editor: Le Wang, MD, PhD Date of Update: 2/6/2018 UpToDate: Liposomal irinotecan (Onivyde) plus FU/LV is now approved for gemcitabine-refractory metastatic pancreatic cancer and recommended by
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic
 Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with pancreatic cancer Section AA Cancer Centre Referrals In the absence of metastatic
Pancreatic Cancer: Medical Therapeutic Approaches
 Pancreatic Cancer: Medical Therapeutic Approaches Vincent J Picozzi MD MMM Virginia Mason Medical Center Seattle WA 1 Pancreatic cancer is the hardest cancer of all to treat Pancreatic cancer: Why so difficult
Pancreatic Cancer: Medical Therapeutic Approaches Vincent J Picozzi MD MMM Virginia Mason Medical Center Seattle WA 1 Pancreatic cancer is the hardest cancer of all to treat Pancreatic cancer: Why so difficult
The Role of Radiation Therapy in the Treatment of Brain Metastases. Matthew Cavey, M.D.
 The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
The Role of Radiation Therapy in the Treatment of Brain Metastases Matthew Cavey, M.D. Objectives Provide information about the prospective trials that are driving the treatment of patients with brain
NCCN Guidelines for Hepatobiliary Cancers V Web teleconference on 10/24/17
 Guideline Page and Request HCC-4 the American Society of Radiation Oncology (ASTRO): We recommend further clarification of the eligibility criteria for surgical resection and liver transplantation, respectively.
Guideline Page and Request HCC-4 the American Society of Radiation Oncology (ASTRO): We recommend further clarification of the eligibility criteria for surgical resection and liver transplantation, respectively.
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress?
 Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
Adjuvant Chemotherapy for Rectal Cancer: Are we making progress? Hagen Kennecke, MD, MHA, FRCPC Division Of Medical Oncology British Columbia Cancer Agency October 25, 2008 Objectives Review milestones
GI Tumor Board 3/8/2018. Case #1 IDEA. Case #1 Question #1 What is the next step in management?
 GI Tumor Board Edward Kim George Poultsides Naseem Esteghamat Kenzo Hirose May Cho Alan Venook Arta Monjazeb Margaret Tempero George Fisher Andrew Ko Daniel Chang Thomas Semrad Sisi Haraldsdottir Case
GI Tumor Board Edward Kim George Poultsides Naseem Esteghamat Kenzo Hirose May Cho Alan Venook Arta Monjazeb Margaret Tempero George Fisher Andrew Ko Daniel Chang Thomas Semrad Sisi Haraldsdottir Case
Updated Imaging for Novel Pancreatic Cancer Therapy. Desiree E. Morgan, MD FSCBTMR Professor and Vice Chair Education
 Updated Imaging for Novel Pancreatic Cancer Therapy Desiree E. Morgan, MD FSCBTMR Professor and Vice Chair Education Disclosures I have no financial disclosures relevant to the educational content of this
Updated Imaging for Novel Pancreatic Cancer Therapy Desiree E. Morgan, MD FSCBTMR Professor and Vice Chair Education Disclosures I have no financial disclosures relevant to the educational content of this
The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology
 The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology (specifically, lung cancer) 2/10/18 Jeffrey Kittel, MD Radiation Oncology, Aurora St. Luke s Medical Center Outline The history
The Evolution of SBRT and Hypofractionation in Thoracic Radiation Oncology (specifically, lung cancer) 2/10/18 Jeffrey Kittel, MD Radiation Oncology, Aurora St. Luke s Medical Center Outline The history
RTOG Lung Cancer Committee 2012 Clinical Trial Update. Wally Curran RTOG Group Chairman
 RTOG Lung Cancer Committee 2012 Clinical Trial Update Wally Curran RTOG Group Chairman 1 RTOG Lung Committee: Active Trials Small Cell Lung Cancer Limited Stage (Intergroup Trial) Extensive Stage (RTOG
RTOG Lung Cancer Committee 2012 Clinical Trial Update Wally Curran RTOG Group Chairman 1 RTOG Lung Committee: Active Trials Small Cell Lung Cancer Limited Stage (Intergroup Trial) Extensive Stage (RTOG
Neoadjuvant radiotherapy for pancreatic cancer: rationale and outcomes
 Review Article Neoadjuvant radiotherapy for pancreatic cancer: rationale and outcomes Rohan Deraniyagala, Emily D. Tanzler The University of Florida College of Medicine Department of Radiation Oncology,
Review Article Neoadjuvant radiotherapy for pancreatic cancer: rationale and outcomes Rohan Deraniyagala, Emily D. Tanzler The University of Florida College of Medicine Department of Radiation Oncology,
MANAGEMENT OF COLORECTAL METASTASES. Robert Warren, MD. The Postgraduate Course in General Surgery March 22, /22/2011
 MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
MANAGEMENT OF COLORECTAL METASTASES Robert Warren, MD The Postgraduate Course in General Surgery March 22, 2011 Local Systemic LIVER TUMORS:THERAPEUTIC OPTIONS Hepatoma Cholangio. Neuroendo. Colorectal
Radiotherapy What are our options and what is on the horizon. Dr Kevin So Specialist Radiation Oncologist Epworth Radiation Oncology
 Radiotherapy What are our options and what is on the horizon Dr Kevin So Specialist Radiation Oncologist Epworth Radiation Oncology Outline Advances in radiotherapy technique Oligo - disease Advancements
Radiotherapy What are our options and what is on the horizon Dr Kevin So Specialist Radiation Oncologist Epworth Radiation Oncology Outline Advances in radiotherapy technique Oligo - disease Advancements
NIH Public Access Author Manuscript J Surg Oncol. Author manuscript; available in PMC 2012 August 01.
 NIH Public Access Author Manuscript Published in final edited form as: J Surg Oncol. 2011 August 1; 104(2): 155 161. doi:10.1002/jso.21954. Neoadjuvant GTX Chemotherapy and IMRT-Based Chemoradiation for
NIH Public Access Author Manuscript Published in final edited form as: J Surg Oncol. 2011 August 1; 104(2): 155 161. doi:10.1002/jso.21954. Neoadjuvant GTX Chemotherapy and IMRT-Based Chemoradiation for
Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D.
 Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D. Department of Surgery Grand Rounds University of Kentucky January 15, 2014 Metastatic Colorectal Cancer (CRC)
Techniques to Improve Resectability of Colorectal Liver Metastases Ching-Wei D. Tzeng, M.D. Department of Surgery Grand Rounds University of Kentucky January 15, 2014 Metastatic Colorectal Cancer (CRC)
Douglas B. Evans, MD 1, Ben George, MD 2, and Susan Tsai, MD, MHS 1
 Ann Surg Oncol (2015) 22:3409 3413 DOI 10.1245/s10434-015-4649-2 EDITORIAL PANCREATIC TUMORS Non-metastatic Pancreatic Cancer: Resectable, Borderline Resectable, and Locally Advanced-Definitions of Increasing
Ann Surg Oncol (2015) 22:3409 3413 DOI 10.1245/s10434-015-4649-2 EDITORIAL PANCREATIC TUMORS Non-metastatic Pancreatic Cancer: Resectable, Borderline Resectable, and Locally Advanced-Definitions of Increasing
Radiation Therapy and Immunotherapy: New Frontiers
 Radiation Therapy and Immunotherapy: New Frontiers Nevada Oncology Society Fall Meeting November 16 th, 2017 Anshu K. Jain, MD Radiation Oncologist, Ashland Bellefonte Cancer Center Assistant Clinical
Radiation Therapy and Immunotherapy: New Frontiers Nevada Oncology Society Fall Meeting November 16 th, 2017 Anshu K. Jain, MD Radiation Oncologist, Ashland Bellefonte Cancer Center Assistant Clinical
Pancreatic Cancer Where are we?
 Pancreatic Cancer Treatment Approaches & Options Pancreatic Cancer Action Network OUMC 9/22/2016 Russell G. Postier, MD Pancreatic Cancer Where are we? Estimated 2016 data 3% of cancer cases 7% of cancer
Pancreatic Cancer Treatment Approaches & Options Pancreatic Cancer Action Network OUMC 9/22/2016 Russell G. Postier, MD Pancreatic Cancer Where are we? Estimated 2016 data 3% of cancer cases 7% of cancer
Treatment of Colorectal Liver Metastases State of the Art
 Treatment of Colorectal Liver Metastases State of the Art Eddie K. Abdalla, MD, FACS Professor and Chairman of Surgery Chief of Hepatobiliary Surgery Hilton Metropolitan Palace Hotel Beirut 16 November,
Treatment of Colorectal Liver Metastases State of the Art Eddie K. Abdalla, MD, FACS Professor and Chairman of Surgery Chief of Hepatobiliary Surgery Hilton Metropolitan Palace Hotel Beirut 16 November,
Radiation Therapy for Liver Malignancies
 Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
Outline Radiation Therapy for Liver Malignancies Albert J. Chang, M.D., Ph.D. Department of Radiation Oncology, UCSF March 23, 2014 Rationale for developing liver directed therapies Liver directed therapies
ES-SCLC Joint Case Conference. Anthony Paravati Adam Yock
 ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
Current and emerging radiotherapy strategies for pancreatic adenocarcinoma: stereotactic, intensity modulated and particle radiotherapy
 Review Article Page 1 of 10 Current and emerging radiotherapy strategies for pancreatic adenocarcinoma: stereotactic, intensity modulated and particle radiotherapy Sweet Ping Ng, Eugene J. Koay Department
Review Article Page 1 of 10 Current and emerging radiotherapy strategies for pancreatic adenocarcinoma: stereotactic, intensity modulated and particle radiotherapy Sweet Ping Ng, Eugene J. Koay Department
De-Escalate Trial for the Head and neck NSSG. Dr Eleanor Aynsley Consultant Clinical Oncologist
 De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
Disclosures. Preoperative Treatment: Chemotherapy or ChemoRT? Adjuvant chemotherapy helps. so what about chemo first?
 Disclosures Preoperative Treatment: Chemotherapy or ChemoRT? Advisory boards Genentech (travel only), Pfizer Salary support for clinical trials Celgene, Merck, Merrimack Matthew Gubens, MD, MS Assistant
Disclosures Preoperative Treatment: Chemotherapy or ChemoRT? Advisory boards Genentech (travel only), Pfizer Salary support for clinical trials Celgene, Merck, Merrimack Matthew Gubens, MD, MS Assistant
What Is The Optimal Adjuvant Therapy in Pancreatic Adenoca: Intensified Chemotherapy March 28 th, 2015
 What Is The Optimal Adjuvant Therapy in Pancreatic Adenoca: Intensified Chemotherapy March 28 th, 2015 Eileen M. O Reilly, M.D. Associate Director David M. Rubenstein Center Pancreatic Cancer Research
What Is The Optimal Adjuvant Therapy in Pancreatic Adenoca: Intensified Chemotherapy March 28 th, 2015 Eileen M. O Reilly, M.D. Associate Director David M. Rubenstein Center Pancreatic Cancer Research
Adjuvant Therapy for Adenocarcinoma of the Pancreas: Analysis of Reported Trials and Recommendations for Future Progress
 Annals of Surgical Oncology DOI: 10.1245/s10434-008-0002-3 Adjuvant Therapy for Adenocarcinoma of the Pancreas: Analysis of Reported Trials and Recommendations for Future Progress Robert A. Wolff, MD,
Annals of Surgical Oncology DOI: 10.1245/s10434-008-0002-3 Adjuvant Therapy for Adenocarcinoma of the Pancreas: Analysis of Reported Trials and Recommendations for Future Progress Robert A. Wolff, MD,
ASCO Poster Review PANCREATIC CANCER
 ASCO Poster Review PANCREATIC CANCER Dr.ssa Michela Squadroni U.O. Oncologia Humanitas Gavazzeni Bergamo TOPICAL ISSUES Gemcitabine/Nab-paclitaxel and FOLFIRINOX comparison Neoadjuvant and perioperative
ASCO Poster Review PANCREATIC CANCER Dr.ssa Michela Squadroni U.O. Oncologia Humanitas Gavazzeni Bergamo TOPICAL ISSUES Gemcitabine/Nab-paclitaxel and FOLFIRINOX comparison Neoadjuvant and perioperative
Are we making progress? Marked reduction in operative morbidity and mortality
 Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Are we making progress? Surgical Progress Marked reduction in operative morbidity and mortality Introduction of Minimal-Access approaches for complex esophageal cancer resections Significantly better functional
Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT
 Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT Daniel J Bourgeois, III MD, MPH Board Certified Radiation Oncologist Southeast Louisiana Radiation Oncology Group (SLROG) Disclosures
Modern Dose Fractionation and Treatment Techniques for Definitive Prostate RT Daniel J Bourgeois, III MD, MPH Board Certified Radiation Oncologist Southeast Louisiana Radiation Oncology Group (SLROG) Disclosures
Pancreatic Ca Update
 Pancreatic Ca Update Caio Max S. Rocha Lima, M.D. M. Robert Cooper Professor in Medical Oncology Co-leader GI Oncology and Co-leader Phase I Program Wake Forest School of Medicine E-mail:crochali@wakehealth.edu
Pancreatic Ca Update Caio Max S. Rocha Lima, M.D. M. Robert Cooper Professor in Medical Oncology Co-leader GI Oncology and Co-leader Phase I Program Wake Forest School of Medicine E-mail:crochali@wakehealth.edu
L oncologo Alberto Zaniboni
 COME TRATTARE LA NEOPLASIA LOCALMENTE AVANZATA BORDERLINE PER RESECABILITA L oncologo Alberto Zaniboni Oncologia Medica Fondazione Poliambulanza - Brescia Pancreatic cancer deaths in 2030 Pancreatic cancer
COME TRATTARE LA NEOPLASIA LOCALMENTE AVANZATA BORDERLINE PER RESECABILITA L oncologo Alberto Zaniboni Oncologia Medica Fondazione Poliambulanza - Brescia Pancreatic cancer deaths in 2030 Pancreatic cancer
Treatment Approaches for Pancreatic Cancer: Hope on the Horizon Disclosures
 Treatment Approaches for Pancreatic Cancer: Hope on the Horizon Michael Pishvaian, MD, PhD Director, Phase I Program Assistant Professor Lombardi Comprehensive Cancer Center Georgetown University Disclosures
Treatment Approaches for Pancreatic Cancer: Hope on the Horizon Michael Pishvaian, MD, PhD Director, Phase I Program Assistant Professor Lombardi Comprehensive Cancer Center Georgetown University Disclosures
HER2-Targeted Rx. An Historical Perspective
 HER2-Targeted Rx An Historical Perspective Trastuzumab: Front Line Rx for MBC Median 20.3 v. 25.1 mo P = 0.046 HR 0.8 65% of control patients crossed over Slamon D, et al. N Engl J Med, 2001; 344:783 Trastuzumab:Front-line
HER2-Targeted Rx An Historical Perspective Trastuzumab: Front Line Rx for MBC Median 20.3 v. 25.1 mo P = 0.046 HR 0.8 65% of control patients crossed over Slamon D, et al. N Engl J Med, 2001; 344:783 Trastuzumab:Front-line
Evaluation of Suspected Pancreatic Cancer
 Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Evaluation of Suspected Pancreatic Cancer October 15, 2015 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-779-3239 Toll
Clinical Aspects of SBRT in Abdominal Regions Brian D. Kavanagh, MD, MPH University of Colorado Department of Radiation Oncology
 Clinical Aspects of SBRT in Abdominal Regions Brian D. Kavanagh, MD, MPH University of Colorado Department of Radiation Oncology Abdominal SBRT: Clinical Aspects Rationales for liver and pancreas SBRT
Clinical Aspects of SBRT in Abdominal Regions Brian D. Kavanagh, MD, MPH University of Colorado Department of Radiation Oncology Abdominal SBRT: Clinical Aspects Rationales for liver and pancreas SBRT
Hong Kong Hospital Authority Convention 2018
 Hong Kong Hospital Authority Convention 2018 Stereotactic Radiosurgery in Brain Metastases - Development of the New Treatment Paradigm in HA, Patients Profiles and Their Clinical Outcomes 8 May 2018 Dr
Hong Kong Hospital Authority Convention 2018 Stereotactic Radiosurgery in Brain Metastases - Development of the New Treatment Paradigm in HA, Patients Profiles and Their Clinical Outcomes 8 May 2018 Dr
Tumores Bilio-Pancreaticos Carlos Gomez-Martin Hospital Universitario 12 de Octubre. Madrid
 Tumores Bilio-Pancreaticos Carlos Gomez-Martin Hospital Universitario 12 de Octubre. Madrid Pancreatic Cancer Pancreatic Cancer Pancreatic Cancer Entity Resectable Borderline Resectable Locally advanced
Tumores Bilio-Pancreaticos Carlos Gomez-Martin Hospital Universitario 12 de Octubre. Madrid Pancreatic Cancer Pancreatic Cancer Pancreatic Cancer Entity Resectable Borderline Resectable Locally advanced
Locally advanced disease & challenges in management
 Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Gynecologic Cancer InterGroup Cervix Cancer Research Network Cervix Cancer Education Symposium, February 2018 Locally advanced disease & challenges in management Carien Creutzberg Radiation Oncology, Leiden
Stereotactic radiotherapy
 Stereotactic radiotherapy Influence of patient positioning and fixation on treatment planning - clinical results Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH
Stereotactic radiotherapy Influence of patient positioning and fixation on treatment planning - clinical results Frank Zimmermann Institut für Radioonkologie Universitätsspital Basel Petersgraben 4 CH
The role of chemoradiotherapy in GE junction and gastric cancer. Karin Haustermans
 The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
The role of chemoradiotherapy in GE junction and gastric cancer Karin Haustermans Overview Postoperative chemoradiotherapy Preoperative chemoradiotherapy Palliative radiation Technical aspects Overview
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Trends in Neoadjuvant Approaches in Pancreatic Cancer
 1070 Trends in Neoadjuvant Approaches in Pancreatic Cancer Lingling Du, MD, and Andrea Wang-Gillam, MD, PhD Abstract Pancreatic cancer (PDAC) is an aggressive tumor type associated with development of
1070 Trends in Neoadjuvant Approaches in Pancreatic Cancer Lingling Du, MD, and Andrea Wang-Gillam, MD, PhD Abstract Pancreatic cancer (PDAC) is an aggressive tumor type associated with development of
Practical implementation of MR-guided RT: pancreatic SBRT as an example site
 Practical implementation of MR-guided RT: pancreatic SBRT as an example site Anna Bruynzeel, MD PhD Dept. of Radiation Oncology VU University medical center Amsterdam, The Netherlands VU University Medical
Practical implementation of MR-guided RT: pancreatic SBRT as an example site Anna Bruynzeel, MD PhD Dept. of Radiation Oncology VU University medical center Amsterdam, The Netherlands VU University Medical
Update on Limited Small Cell Lung Cancer. Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver
 Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
Overview: Immunotherapy in CNS Metastases
 Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
Overview: Immunotherapy in CNS Metastases Manmeet Ahluwalia, MD, FACP Miller Family Endowed Chair in Neuro-Oncology Director Brain Metastasis Research Program Cleveland Clinic Disclosures Consultant- Monteris
Optimal Management of Isolated HER2+ve Brain Metastases
 Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
Optimal Management of Isolated HER2+ve Brain Metastases Eliot Sims November 2013 Background Her2+ve patients 15% of all breast cancer Even with adjuvant trastuzumab 10-15% relapse Trastuzumab does not
KEYWORDS: stereotactic body radiotherapy, pancreatic cancer, chemoradiation, locally advanced, unresectable, positron emission tomography.
 Original Article Phase 2 Multi-institutional Trial Evaluating Gemcitabine and Stereotactic Body Radiotherapy for Patients With Locally Advanced Unresectable Pancreatic Adenocarcinoma Joseph M. Herman,
Original Article Phase 2 Multi-institutional Trial Evaluating Gemcitabine and Stereotactic Body Radiotherapy for Patients With Locally Advanced Unresectable Pancreatic Adenocarcinoma Joseph M. Herman,
External Beam Radiation Therapy for Thyroid Cancer
 External Beam Radiation Therapy for Thyroid Cancer C. Jillian Tsai, M.D, PH.D. Assistant Attending Director of Head and Neck Cancer Research Department of Radiation Oncology Memorial Sloan Kettering Cancer
External Beam Radiation Therapy for Thyroid Cancer C. Jillian Tsai, M.D, PH.D. Assistant Attending Director of Head and Neck Cancer Research Department of Radiation Oncology Memorial Sloan Kettering Cancer
Reirradiazione. La radioterapia stereotassica ablativa: torace. Pierluigi Bonomo Firenze
 Reirradiazione La radioterapia stereotassica ablativa: torace Pierluigi Bonomo Firenze Background Stage III NSCLC isolated locoregional recurrence in 25% of pts mostly unresectable; low RR with 2 nd line
Reirradiazione La radioterapia stereotassica ablativa: torace Pierluigi Bonomo Firenze Background Stage III NSCLC isolated locoregional recurrence in 25% of pts mostly unresectable; low RR with 2 nd line
Neoadjuvant chemoradiotherapy for locally advanced pancreas cancer rarely leads to radiological evidence of tumour regression
 DOI:10.1111/hpb.12015 HPB ORIGINAL ARTICLE Neoadjuvant chemoradiotherapy for locally advanced pancreas cancer rarely leads to radiological evidence of tumour regression Vikas Dudeja 1, Edward W. Greeno
DOI:10.1111/hpb.12015 HPB ORIGINAL ARTICLE Neoadjuvant chemoradiotherapy for locally advanced pancreas cancer rarely leads to radiological evidence of tumour regression Vikas Dudeja 1, Edward W. Greeno
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES
 DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
DOES RADIOTHERAPY TECHNIQUE / DOSE / FRACTIONATION REALLY MATTER? YES Marco Krengli Radiotherapy, Department of Translational Medicine, University of Piemonte Orientale A. Avogadro THE STANDARD OF CARE
3/8/2014. Case Presentation. Primary Treatment of Anal Cancer. Anatomy. Overview. March 6, 2014
 Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Surgical Management of Advanced Stage Colon Cancer. Nathan Huber, MD 6/11/14
 Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Surgical Management of Advanced Stage Colon Cancer Nathan Huber, MD 6/11/14 Colon Cancer Overview Approximately 50,000 attributable deaths per year Colorectal cancer is the 3 rd most common cause of cancer-related
Pre- Versus Post-operative Radiotherapy
 Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Oral Cavity Cancer Combined modality therapy
 Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
INTRAOPERATIVE RADIATION THERAPY FOR RETROPERITONEAL SARCOMA
 INTRAOPERATIVE RADIATION THERAPY FOR RETROPERITONEAL SARCOMA ISIORT 2014 Ivy A Petersen, MD Mayo Clinic Rochester, MN NOTHING TO DISCLOSE SOFT TISSUE SARCOMAS 2014 Estimated cases in the USA 12,020 diagnosed
INTRAOPERATIVE RADIATION THERAPY FOR RETROPERITONEAL SARCOMA ISIORT 2014 Ivy A Petersen, MD Mayo Clinic Rochester, MN NOTHING TO DISCLOSE SOFT TISSUE SARCOMAS 2014 Estimated cases in the USA 12,020 diagnosed
Case Conference. Craig Morgenthal Department of Surgery Long Island College Hospital
 Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Case Conference Craig Morgenthal Department of Surgery Long Island College Hospital Neoadjuvant versus Adjuvant Radiation Therapy in Rectal Carcinoma Epidemiology American Cancer Society statistics for
Treatment of 200 Locally Advanced (Stage III) Pancreatic Adenocarcinoma Patients with Irreversible Electroporation: Safety and Efficacy
 Pancreatic Adenocarcinoma Patients with Irreversible Electroporation: Safety and Efficacy") The following three articles refer to the same April 2015 ASA presentation, and the same research. But, more data is offered in the third article. Treatment of 200 Locally Advanced (Stage III) Pancreatic
The following three articles refer to the same April 2015 ASA presentation, and the same research. But, more data is offered in the third article. Treatment of 200 Locally Advanced (Stage III) Pancreatic
Triple Negative Breast cancer New treatment options arenowhere?
 Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT
 Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT David H. Ilson, MD, PhD Gastrointestinal Oncology Service Memorial Sloan Kettering Cancer Center Disclosure Consulting
Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT David H. Ilson, MD, PhD Gastrointestinal Oncology Service Memorial Sloan Kettering Cancer Center Disclosure Consulting
Updates in Immunotherapy for Urothelial Carcinoma
 Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
High Risk Localized Prostate Cancer Treatment Should Start with RT
 High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
High Risk Localized Prostate Cancer Treatment Should Start with RT Jason A. Efstathiou, M.D., D.Phil. Assistant Professor of Radiation Oncology Massachusetts General Hospital Harvard Medical School 10
肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部
 肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部 Outline Current status of radiation oncology in lung cancer Focused on stage III non-small cell lung cancer Radiation
肺癌放射治療新進展 Recent Advance in Radiation Oncology in Lung Cancer 許峰銘成佳憲國立台灣大學醫學院附設醫院腫瘤醫學部 Outline Current status of radiation oncology in lung cancer Focused on stage III non-small cell lung cancer Radiation
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org The Role of Radiosurgery in the Treatment of Gliomas Luis Souhami, MD Professor Department of Radiation
The role of Radiation Oncologist: Hi-tech treatments for liver metastases
 The role of Radiation Oncologist: Hi-tech treatments for liver metastases Icro Meattini, MD Radiotherapy-Oncology Unit AOU Careggi Hospital Florence University, Italy Liver Metastases - Background The
The role of Radiation Oncologist: Hi-tech treatments for liver metastases Icro Meattini, MD Radiotherapy-Oncology Unit AOU Careggi Hospital Florence University, Italy Liver Metastases - Background The
Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey
 Updated Oncology 2015: State of the Art News & Challenging Topics CURRENT STATUS OF STEREOTACTIC RADIOSURGERY IN BRAIN METASTASES Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey Bucharest,
Updated Oncology 2015: State of the Art News & Challenging Topics CURRENT STATUS OF STEREOTACTIC RADIOSURGERY IN BRAIN METASTASES Mehmet Ufuk ABACIOĞLU Neolife Medical Center, İstanbul, Turkey Bucharest,
Trimodality Therapy for Muscle Invasive Bladder Cancer
 Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Trimodality Therapy for Muscle Invasive Bladder Cancer Brita Danielson, MD, FRCPC Radiation Oncologist, Cross Cancer Institute Assistant Professor, Department of Oncology University of Alberta Edmonton,
Gastroesophag Gastroesopha eal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. G. H addock Haddock M.D.
 Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
Gastroesophageal Junction Adenocarcinoma: What is the best adjuvant regimen? Michael G. Haddock M.D. Mayo Clinic Rochester, MN Locally Advanced GE Junction ACA CT S CT or CT S CT/RT Proposition Chemoradiation
Pancreatic Cancer: Light at the End of the (Very Long) Tunnel
 Tunnel") Pancreatic Cancer: Light at the End of the (Very Long) Tunnel Daniel Renouf, MD, MPH, FRCPC Medical Oncologist, BC Cancer Agency University of British Columbia Objectives 1. Discuss recent updates in systemic
Pancreatic Cancer: Light at the End of the (Very Long) Tunnel Daniel Renouf, MD, MPH, FRCPC Medical Oncologist, BC Cancer Agency University of British Columbia Objectives 1. Discuss recent updates in systemic
Intra-arterial Targeted Delivery of Gemcitabine in Treatment of Patients with Loco-regional Pancreatic Tumors
 Intra-arterial Targeted Delivery of Gemcitabine in Treatment of Patients with Loco-regional Pancreatic Tumors Alexander Rosemurgy, M.D., Sharona Ross, M.D., Paul Vitulli, M.D., Florida Hospital Tampa,
Intra-arterial Targeted Delivery of Gemcitabine in Treatment of Patients with Loco-regional Pancreatic Tumors Alexander Rosemurgy, M.D., Sharona Ross, M.D., Paul Vitulli, M.D., Florida Hospital Tampa,
Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First?
 Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First? Marc Peeters, MD, PhD Head of the Oncology Department Antwerp University Hospital Antwerp, Belgium marc.peeters@uza.be 71-year-old
Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First? Marc Peeters, MD, PhD Head of the Oncology Department Antwerp University Hospital Antwerp, Belgium marc.peeters@uza.be 71-year-old
Review Article Neoadjuvant Therapy in Pancreatic Cancer: An Emerging Strategy
 Gastroenterology Research and Practice, Article ID 183852, 9 pages http://dx.doi.org/10.1155/2014/183852 Review Article Neoadjuvant Therapy in Pancreatic Cancer: An Emerging Strategy Alessandro Bittoni,
Gastroenterology Research and Practice, Article ID 183852, 9 pages http://dx.doi.org/10.1155/2014/183852 Review Article Neoadjuvant Therapy in Pancreatic Cancer: An Emerging Strategy Alessandro Bittoni,
Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen?
 Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
Department of Radiation Oncology Chairman: Prof. Dr. Matthias Guckenberger Alleinige Radiochirurgie und alleinige Systemtherapie zwei «extreme» Entwicklungen in der Behandlung von Hirnmetastasen? Matthias
Histopathologic tumor response after induction chemotherapy and stereotactic body radiation therapy for borderline resectable pancreatic cancer
 Original Article Histopathologic tumor response after induction chemotherapy and stereotactic body radiation therapy for borderline resectable pancreatic cancer Michael D. Chuong 1, Jessica M. Frakes 2,
Original Article Histopathologic tumor response after induction chemotherapy and stereotactic body radiation therapy for borderline resectable pancreatic cancer Michael D. Chuong 1, Jessica M. Frakes 2,
Pancreatic Ductal Adenocarcinoma. Razvan Popescu Tumor Center Aarau Switzerland
 Pancreatic Ductal Adenocarcinoma Razvan Popescu Tumor Center Aarau Switzerland Median Survival of Patients With Pancreatic Cancer Localized/ Resectable 15-24 months 10% Locally Advanced 6-15 months 30%
Pancreatic Ductal Adenocarcinoma Razvan Popescu Tumor Center Aarau Switzerland Median Survival of Patients With Pancreatic Cancer Localized/ Resectable 15-24 months 10% Locally Advanced 6-15 months 30%
Opportunity for palliative care Research
 Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
Opportunity for palliative care Research Role of Radiotherapy in Multidisciplinary Management of Rectal Cancers Dr Sushmita Pathy Associate Professor Department of Radiation Oncology Dr BRA Institute Rotary
Reference No: Author(s) 12/05/16. Approval date: committee. June Operational Date: Review:
 12/05/16. Approval date: committee. June Operational Date: Review:") Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Adenocarcinoma Dr Colin Purcell, Consultant Medical Oncologist & on behalf of the GI Oncologists Group, Cancer
Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Adenocarcinoma Dr Colin Purcell, Consultant Medical Oncologist & on behalf of the GI Oncologists Group, Cancer
Pancreas Case Scenario #1
 Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Pancreas Case Scenario #1 An 85 year old white female presented to her primary care physician with increasing abdominal pain. On 8/19 she had a CT scan of the abdomen and pelvis. This showed a 4.6 cm mass
Old and New Radiation for Bladder and Upper Tract Cancers. Bridget Koontz Radiation Oncology Duke Cancer Institute
 Old and New Radiation for Bladder and Upper Tract Cancers Bridget Koontz Radiation Oncology Duke Cancer Institute Disclosures Janssen funded clinical research BlueEarth Diagnostics advisory board member
Old and New Radiation for Bladder and Upper Tract Cancers Bridget Koontz Radiation Oncology Duke Cancer Institute Disclosures Janssen funded clinical research BlueEarth Diagnostics advisory board member
Utility of 18 F-FDG PET/CT in metabolic response assessment after CyberKnife radiosurgery for early stage non-small cell lung cancer
 Utility of F-FDG PET/CT in metabolic response assessment after CyberKnife radiosurgery for early stage non-small cell lung cancer Ngoc Ha Le 1*, Hong Son Mai 1, Van Nguyen Le 2, Quang Bieu Bui 2 1 Department
Utility of F-FDG PET/CT in metabolic response assessment after CyberKnife radiosurgery for early stage non-small cell lung cancer Ngoc Ha Le 1*, Hong Son Mai 1, Van Nguyen Le 2, Quang Bieu Bui 2 1 Department
Esophageal Cancer. What is the value of performing PET scan routinely for staging of esophageal cancers
 Esophageal Cancer What is the value of performing PET scan routinely for staging of esophageal cancers What is the sensitivity and specificity of PET scan for metastatic lesions When should PET scan be
Esophageal Cancer What is the value of performing PET scan routinely for staging of esophageal cancers What is the sensitivity and specificity of PET scan for metastatic lesions When should PET scan be
RADIATION THERAPY WITH ONCE-WEEKLY GEMCITABINE IN PANCREATIC CANCER: CURRENT STATUS OF CLINICAL TRIALS
 doi:10.1016/s0360-3016(03)00449-8 Int. J. Radiation Oncology Biol. Phys., Vol. 56, No. 4, Supplement, pp. 10 15, 2003 Copyright 2003 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/03/$
doi:10.1016/s0360-3016(03)00449-8 Int. J. Radiation Oncology Biol. Phys., Vol. 56, No. 4, Supplement, pp. 10 15, 2003 Copyright 2003 Elsevier Inc. Printed in the USA. All rights reserved 0360-3016/03/$
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Colon Cancer Liver Metastases: Liver-Directed Therapy
 Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014
Colon Cancer Liver Metastases: Liver-Directed Therapy Shishir K. Maithel, MD FACS Assistant Professor of Surgery Division of Surgical Oncology Winship Cancer Institute Emory University August 10, 2014