EU Guidelines for quality assurance in organization, implementation and monitoring of colorectal cancer screening programme. Jožica Maučec Zakotnik
|
|
|
- Blake Ralph Hamilton
- 6 years ago
- Views:
Transcription
1
2 EU Guidelines for quality assurance in organization, implementation and monitoring of colorectal cancer screening programme Jožica Maučec Zakotnik
3 EU guidelines
4 Luxembourg 2010
5 EU guidelines - chapters Evidence for effectiveness of guaiac and immunochemical FOBT, endoscopy screening Organisation and participation Evaluation and interpretation of screening outcomes indicators QA in endoscopy in colorectal cancer screening and diagnosis
6 EU guidelines - chapters Professional requirements and training QA in pathology in colorectal cancer screening and diagnosis Management of lesions detected in colorectal cancer screening Colonoscopic surveillance following adenoma removal Communication
7 Topics recommended to be improved in Croatia AREAS OF RECOMMENDATIONS Legal framework Governance Organisation Implementation of the Programme Information system data provision Quality assurance Financing
8 LEGAL FRAMEWORK There is a need for a stronger legal framework to support the Programme organisation, management and implementation. It should clearly define: legal establishment of the Programme, appointment of the responsible authority of the Programme, other stakeholders and providers of the programme and the relationships among them financial framework screening registry and the responsible holder of the screening registry Protocols and guidelines, supporting the organisation, implementation, evaluation, surveillance and monitoring, shall be defined in a form of regulation, adopted by Ministry of Health.
9 EU recommendation Appropriate political and financial support are crucial to the successful implementation of any screening programme. Council Recommendation on Cancer Screening of 2 December 2003 spells out fundamental principles of best practice in early detection of cancer and invites EU Member States to take common action to implement cancer screening programmes with an organised, populationbased approach and with appropriate quality assurance at all levels
10 GOVERNANCE Legally authorized institution/body (existing or to create new) should be responsible for organization, management and implementation of the Programme. It should employ enough competent staff, to assure all the necessary activities of excellent governance of the Programme: Provision of appropriate organization of the Programme Planning and Coordination of detailed budgeting scheme Implementation of the Programme professional guidelines development and implementation professional training quality control monitoring and evaluation
11 EU recommendation A colorectal cancer screening programme is a multidisciplinary undertaking. The objective is to: reduce mortality from and possibly incidence of colorectal cancer WITHOUT adversely affecting the health status of those who participate in screening. The effectiveness is a function of the quality of the individual components of the process. The public health perspective in the planning and provision of screening services requires commitment to ensuring equity of access and sustainability of the programme over time.
12 ORGANISATION FOR BETTER QUALITY ASSURANCE Centrally organized and centrally managed CRC screening program is recommended to assure high Quality of the Programme Centralization of some procedures of the Programme should be considered: The use of immunochemical fecal occult blood (ifobt) test Central laboratory for ifobt test readings Greater centralization of pathohistological laboratory diagnostics
13 EU recommendation Which strategy for screening to choose? What we have to take into account, when designig and implementing the screening programme and choosing the screening strategy? The costs of screening organisation (including infrastructure, information technology, screening promotion, training and quality assurance), The occurrence of adverse effects and The likelihood that patients will actually complete the tests
14
15

16 Screened population (screenig uptake) regarding sex and screening round in Programme Svit 70,00% 60,00% 50,00% 40,00% 50,0 47,7 44,8 61,0 57,9 54,9 55,5 52,8 49,9 1. presejalni krog 30,00% 20,00% 2. presejalni krog 3. presejalni krog 10,00% 0,00% moški ženski skupaj SVITOV DAN 2015
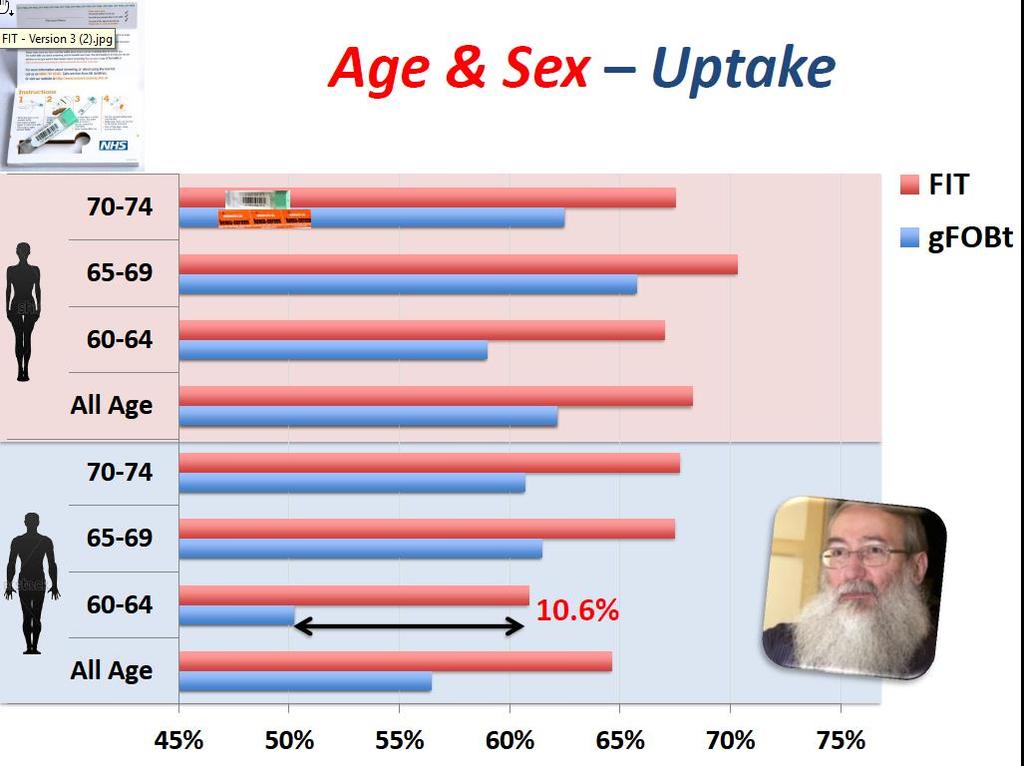
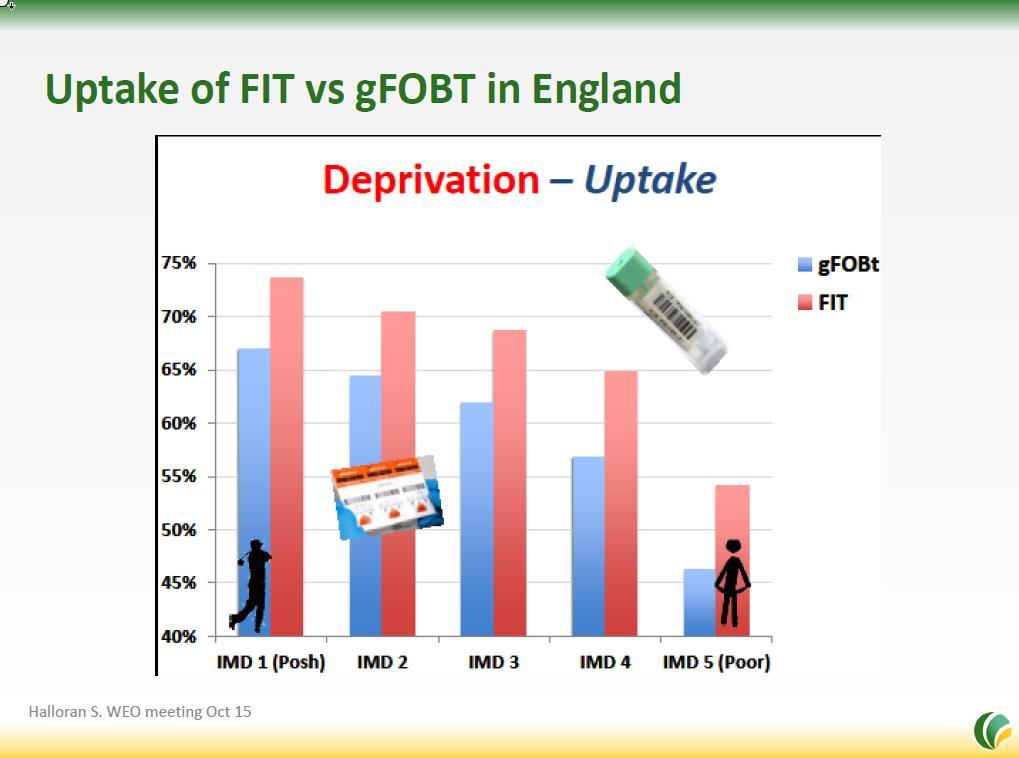
17 Examples of programme performance Screening test Country % Adherence Reference gfobt Finland 72.0 Artama M, Acta Oncol 2016 England 56.0 Halloran S, Gut 2016 Scotland 55.3 Steel RJ, Gut 2012 France 52.8 Hamza M, Dig Liv Dis 2014 FIT (ifobt) Netherlands 71.3 Toes-Zoutendijk M, submitted Italy 47.1 Zorzi M, Epidemiol Prev 2015 Spain 43.8 Salas Trejo D, EU J Can Prev 2016 Spain (Basque) 68.5 Portillo I, WEO Meeting 2015 Slovenia 59.7 Zakotnik J, ISIS 2016
18 IMPLEMENTATION Increasing the response rate of the target population to at least 45 % should be achieved by: Systematic and planned promotion based on identified obstacles and written communication strategy Introducing the call/recall (reminder) system Stronger involvement of family medicine doctors and district nurses in recruitment of non-responders Payment of additional work could be connected to the level of the response rate of the individual family doctor s list of patients Stronger involvement of civil society (NGO, opinion leaders, ambassadors) in the Program promotion Stronger involvement of PH proffesionals at county level in targeted community promotion of CRC screenig peogramme to influence responce rate in the programme

19 Invitation to join the Program Svit No response Invitee responds with signed consent Written reminder Respondent receives testing kit for 2 stool samples by regular mail Respondent not returning the test kit Written reminder 2X Respondent returning the test kit to the central lab by mail Test results for tested participants Positive Negative Colonoscopy Invited for ifobt after 2 years 3rd Alpe Adria Danube Symposium
20 PATIENT CENTERED PROGRAMME Higher response rate of the target population could be achieved trough using patient friendly procedures and solutions: Simple manuals, use of social networks and support, clear messages Using user friendly test kit Colonoscopy without pain or with less pain Treating minor lesions (polyps) inside the first screening colonoscopy Needs of disabled people and language/ethnic minorities should be detected and fulfilled
21 EU recommendation Taking into account the perspective of the individual requires commitment to promoting informed participation and to providing a high quality, safe service.
22 INFORMATION SYSTEM DATA PROVISION Appropriate IT system should support all steps of the Programme implementation and management through: Governance of CRC screening registry by authorized institution Reliable data sources for identification and inclusion of the target population in the Program Enabling different providers to connect to the unified Programme IT system according to their role Connection of the screening registry to the national cancer registry and regular refreshment of the data Enabling the access to micro data of the Programme for analytical and research purposes
23 EU recommendation Complete and accurate recording of all relevant data on each individual and every screening test performed, including the test results, the decision made as a consequence, diagnostic and treatment procedures and the subsequent outcome, including cause of death, should be ensured. This monitoring process is of fundamental importance.
24 QUALITY ASSURANCE Assurance of high quality system at all levels of the Programme is a prerequisite of any screening program. Therefore the authorized institution/body, responsible for the Programme should develop and implement : CRC screening programme guidelines Clear inclusion criteria for the target population Standard procedures Quality indicators Accreditation system and entering criteria for Programme providers Auditing / Quality control of Programme providers Education and training for all professional groups of Programme providers
25 FINANCING The prerequisite of successful and efficient implementation of the Programme is stable and sufficient financing. The coordinating authority should prepare detailed budgeting scheme and state should provide stable and sufficient financing for Management cost sufficient staff and material cost for organization, coordination, IT system, promotion of the Programme, monitoring, evaluation, quality control Implementation costs (invitation, testing, colonoscopy, PH, ) Recalculation and definition of appropriate colonoscopy prices to assure high quality procedures Incentives for family doctors according to response rate
26 EU recommendations The programme needs political support with sustainable funding to succeed. Provisions should be made for the financing of the programme, including evaluation costs.
27 Please discuss the questions: DISCUSSION Worksheet 2 a) What are to your opinion the reasons why people in Croatia respond to invitation only in approximately 20%?. Please focus on peoples individual reasons. Please rang them according to impotrance from 1 to 10.
28 DISCUSSION Worksheet 2 Please discuss the questions in pairs: Is quality assurance important for you when working in screening programme? Rang it from 1 to 10 (1 is not important, 10 is very important). Do you know which data/indicators represents quality in your screening work? Do you report and folow this data in screening programme? Which ones? Write a list of quality indicators concerning your work in CRC screening programme on flipchart paper.
29 Reasons for non response in Slovenia Reasons for nonresponse among nonresponders - Field interview survey in 2014 Believe they are healthy 30,5% Forgotten 6,0% Lack of time and preoccupied 22,2% Screening is not important 6,0% Fear of cancer to be discovered 18,6% Lack of information 4,2% Already performed colonoscopy 15,0% Fear of expences 3,6% Negative attitute towards health sistem 14,4% Confused an invitation with advertising 3,6% Ill from other serious disease 13,8% Not know to be tested every 2 years 3,6% No need for subsequent testing after neg. test 8,4% Misplaced 3,0% Postponing 7,8% Not familiar with Svit programme brand 3,0% Did not get / noticed the inviation 7,8% Convinced that health cannot be influenced 2,4% Fear of colonoscopy 6,6% Problematic procedure of test sampling 2,4% Other 1,8%
30 EU Guidelines and Screening Programme Quality Indicators Jožica Maučec Zakotnik
31 Quality indicators in CRC screening Programme organisation, implementation and management Programme performance indicators organization Coverage by invitation Invitation response rate Unreturned fit rate Time interval between completion of test and issuing of results Referral to follow-up colonoscopy after fit Time interval between referral after positive test and performed colonoscopy Colonoscopy compliance rate Time interval between laboratory receipt and histological result Time interval between diagnosis of screen-detected cancer and start of definitive treatment Programme performance indicators outcome results (diagnosis) Inadecvate fit rate Positive fit rate Colonoscopy after positive fit rate Caecal intubation rate Rate of high-grade neoplasia reported Proportion of cancer cases not requiring surgery Endoscopic complications rate 30-day colonoscopy specific mortality Positive predictive value for detection of lesions/adenoma/advanced adenoma/cancer) Early performance indicators impact to population health Uptake/participation rate Stage of screen-detected cancers
32 First 3 screening round of Program Svit results 1. screeming round 2.screening round 3.screening round number % number % number % People invited ,4% ,3% ,6% Delivered invitations ,3% ,6% ,6% Responded to invitation (signed consent returned to Program Svit Patients not eligible for screening (history of colorectal condition) ,9% ,8% ,7% ,5% ,7% ,5% Persons not wanted to participate but responded ,3% ,3% 676 0,2% Persons received test kit ,5% ,3% ,2% Participated returned test kit ,9% ,8% ,5% - persons returned test kit appropriate for the analysis ,5% ,7% ,8% positive test ,2% ,0% ,0% negative test ,8% ,0% ,0% - persons returned only inappropriate test kits ,5% 705 0,3% 505 0,2% SVITOV DAN 2015 N of people with clonoskopy performed ,9% ,2% ,8%
33 Invitation responce rate regarding communities, 1.screening round (april 2009 marec 2011)

34 Invitation responce rate regarding communities, 2.screening round (april 2011 december 2012)
35 Invitation responce rate regarding communities, 3.screening round (januar 2013 december 2014)
36 Screened population regarding sex and screening round 70,00% 60,00% 50,00% 40,00% 50,0 47,7 44,8 61,0 57,9 54,9 55,5 52,8 49,9 1. presejalni krog 30,00% 20,00% 2. presejalni krog 3. presejalni krog 10,00% 0,00% moški ženski skupaj SVITOV DAN 2015
37 Shift in cancer stages detected in the SLO screening Stage 1. round round number share number share I. stage T1Nx (T1 Nx Mx) * ,9% ,4% I. stage (T1/2 N0 M0) ,7% ,9% Cancer register in 2008 (limited) 13,5% II. stage (T3/4 N0 M0) ,4% 99 19,8% III. stage (any T N1/2 M0) ,6% ,0% IV. stage (any T N1/2 M1) 57 6,4% 40 8,0% total with stage ,0% ,0% no data 15 Total cancers Endoscopic removal Early phase of detection (I. in II. stage): 70,0 % in 71 %
38 Effects of CRC screening in Slovenia
39 Programme performance indicators - organization 1. Coverage by invitation Share of people to whom the invitation was delivered by mail according to number of target population eligible for screening (permanent, temporary residents, insured?... ) 95% >=95% 99,6% in 2.round 2. Invitation response rate Share of people who responded to the invitation according to the number of target population who received the invitation. > =45% >=75% 57,8% in 2.round 3. Unreturned fit rate Share of people who did not returned the stool test kit among people to whom the test kit was sent. < 10% < 5% 5,2% in 2.round
40 Programme performance indicators - organization 4. Time interval between completion of test and issuing of results Share of people who received the test result in 15?, 10? days. Sending the results to people with negative test should be included in the program algorithm. > 90% in 15 days 100% 5. Referral to follow-up colonoscopy after fit Share of people appointed to colonoscopy among people with positive FOBT result. Different reasons for not being appointed should be monitored. 90% > 95% 93,2% in 2.round 6. Time interval between referral after positive test and performed colonoscopy Share of people with the first colonoscopy performed in 31 days (42 days?) after the day of appointing to the colonoscopy. > 90% in 31 days > 95% in 31 days 74,6 % in 2.round
41 Programme performance indicators - organization 7. Colonoscopy compliance rate Share of people with at least one colonoscopy in the programme among people who were after positive FOBT appointed for colonoscopy > 85% > 90% 98,9% in 2.round 8. Time interval between laboratory receipt and histological result Share of colonoscopies where result of histopathology diagnostics was available (send in paper form or entered to information system) in 5 or 10 working days. > 95% in 5 days > 95% in 5 days > 98% in 10 days (entered in > 98% in 10 days (entered in 67,9% in 5 days in 2.round information system) information system) 95,8% in 10 days in 2.round 9. Time interval between diagnosis of screen-detected cancer and start of definitive treatment Share of people with colorectal cancer who received definitive treatment in 31 calendar days after histopathology diagnosis of cancer among people who need additional treatment (surgery). > 90% in 31 days > 95%
42 Programme performance indicators outcome 10. Inadequate fit rate results (diagnosis) Share of people with at least one inadequate fit test, who did not manage to receive test result (positive or negative) among screened (sent stool samples). 11. Positive fit rate Share of people with positive test result among people with test result. 12. Colonoscopy after positive fit rate Share of people with at least one colonoscopy in the programme among people with a positive FOBT test result. < 3% <1% 0,3% in 2.round international standards not clearly defined 6,0% in 2.round no standard >85% 92,2% in 2.round
43 Programme performance indicators outcome results (diagnosis) 13. Caecal intubation rate a. Share of total colonoscopies among all performed colonoscopies. b. Share of total colonoscopies according to the number of people with at least one colonoscopy. > 90% >=95% 98,8 % in 2. round 14. Rate of high-grade neoplasia reported Share of findings which histopathologists classified as high-grade displasia among all findings with histopathology diagnose. < 10% 6,6 % in 2. round 15. Proportion of cancer cases not requiring surgery Share of people with colorectal cancer detected who did not need surgery, because cancer was removed at endoscopy among people with colorectal cancer as the worst finding detected at colonoscopy. reference standard not clearly defined no standard 24,30 % in 2. round
44 Programme performance indicators outcome results (diagnosis) 16. Proportion of adenoma cases referred for surgery Share of people with adenoma as the worst finding who were referred to surgery, among people with adenoma as the worst finding at colonoscopy. no generally accepted standard no standard 2,4% 1.round 17. Surgery compliance rate Share of people referred to surgery with the procedure performed, according to all people referred to surgery. > 90% > 95% 87 % in 2. round
45 Programme performance indicators outcome results (diagnosis) 19. Endoscopic complications rate Share of screening or therapeutic colonoscopies with complications among all colonoscopies. Type of serious complications should be identified and reported from all colonoscopy providers inside the programme. < 0,5% diagnostic colonoscopy < 2,5% therapeutic colonoscopy 0,3% during diagnostic colonoscopy 0,81% during therapeutic colonoscopy < 1/1000 perforations requiring surgery 0,02% serious complications, diagnostic no standard < 1/1000 immediate or delayed bleeding colonoscopy requiring surgery 0,24% serious complications, therapeutic colonoscopy day colonoscopy specific mortality Share of people who died in 30 days after colonoscopy because of colonoscopy complications, among all people with at least one colonoscopy. no standard 0% 0,00007% in 2.round
46 Programme performance indicators outcome results (diagnosis) 18. Positive predictive value for detection of lesions/adenoma/advanced adenoma/cancer) a. Positive predictive value of colonoscopy Share of people with at least one lesion /one adenoma/one advanced adenoma/one carcinoma counting the worst finding, among people at least one colonoscopy performed. PPV for advanced adenoma and carcinoma at colonoscopy First test>25% First test>30% 43,3% in 1. round Next test>15% Next test>20% b. Positive predictive value of FOBT test Share of people with at least one lesion /one adenoma/one advanced adenoma/one carcinoma counting the worst finding, among people with positive FOBT test result. First test>25% First test>30% 39,3% in 1. round Next test>15% Next test>20%
47 Early performance indicators impact to 21. Uptake/participation rate population health Share of people with returned test kit (suitable for testing or not) among all people delivered the invitation minus people excluded because of previous bowel cancer or bowel decease > 45% >65% 55,5% in 3. round 22. Lesions/adenoma/advanced adenoma/cancer detection rate of FOBT Share of people with at least one lesion /one adenoma/one advanced adenoma/one carcinoma counting the worst finding, among people with FOBT test result (positive and negative). CRC: >2/1000 in 1.round, >1/1000 in subsequent Advanced adenoma: >7,5/1000 in 1.round, >5/1000 in subsequent CRC: >2,5/1000 in 1.round, >1,5/1000 in subsequent Advanced adenoma: >10/1000 in 1.round, >7,5/1000 in subsequent CRC: 3,5/1000 in 1. round, 2/1000 in 2.round Advanced adenoma: 21/1000 in 1. round, 17/1000 in 2.round
48 Early performance indicators impact to population health 23. Stage of screen-detected cancers Share of people with different cancer stage among all people with cancer diagnosed inside screening programme, counting the worst finding. TNM (I, II, III, IV) classification is used. stage 3 or higher <30% stage 3 or higher <20% 29,8% in 1. round 24. Interval cancers Share of people with interval cancer (primary colorectal cancer) diagnosed before next planed FOBT or planed colonoscopy control, among people with FOBT test result or people with colonoscopy performed. For this definition strict rules of time period of repeated invitation to next screening round must be followed by screening managing institution. no generally accepted reference standard
49 Quality of colonoscopy indicators 25.Colonoscopists with sufficient number of conducted colonoscopies Share of colonoscopists who performed at least 200 colonoscopies per year inside and outside the programme among all colonoscopists in the programme. 85% >= % > Bowel cleansing, quality of colonoscopy preparation Share of colonoscopies with good cleansing among all performed colonoscopies. > 90% >=95% 96,9% in 2. round
50 Quality of colonoscopy indicators 27. Colonoscopy withdrawal time Share of colonoscopies without polypectomy or biopsy with at least 6 minutes withdrawal time among all colonoscopies without polypectomy or biopsy. >= 90% 6 min 28. Adenoma detection rate (ADR) of first colonoscopy Share of first colonoscopies with detected at least one adenoma among all first colonoscopies men>=50% women>=30% men>=60% women>=40% men>=61,3% in 2. round women>=39,6% in 2. round
51 Quality of colonoscopy indicators 29. Left and right colon adenoma detection proportion Share of adenomas detected in left/ right colon among all adenomas detected in entire colon. Right hemicolon includes flexura lienalis, colon transversum flexura hepatica, colon ascendens, and cecum. Left hemicolon includes anus, rectum, colon sigmoideum and colon descendens. Left/right colon Left colon < 63,4% in 2.round Left colon < 60 % proportion 65% / Right colon > 36,6% in Right colon > 40% 35% 2.round 30. Sessile serrated lesion in right colon detection rate (SSLR) Share of first colonoscopies with at least one detected sessile serrated lesion in right hemicolon among number of all first colonoscopies. > 4% men: 1,4% in 2. round women: 1,7% in 2. round
52 Quality of colonoscopy indicators 31. Mean adenomas per procedure map), (Mean adenomas per positive procedure map+) Share of all adenomas detected in first colonoscopies among number of all first colonoscopies (map) or among number of all first colonoscopies with at least one adenoma detected (map+) no standard no standard MAP (2.round) 1,05 aden/colon MAP+ (2.round) 2,02 aden/+colon 32. Referral to surgery or tertiary endoscopy in the same or another facility Share of people referred to surgery or additional colonoscopy for polypectomy among number of people with findings at colonoscopy. < 5 %
53 DISCUSSION Worksheet 3- group A Quality assurance in organization and management to achieve adequate response rate of target population. 45% response rate is the bottom target agreed in EU guidelines if the screening programme goals in improving population health are to be reached. Professionally mixed group discuss and answer the questions: a) Is the current organization of the screening programme optimal to achieve this target response rate in Croatia? How it can be improved? b) Which are the fields where do you see the necessary development of the coordinating institution HZJZ (NIPH) and county public health institutes if you have in mind how to achieve 45% response rate? Rapporteur of the group will have to report to coordinator and to other groups.
54 DISCUSSION Worksheet 3- group B EU guidelines for quality assurance in CRC screening programme define quality indicators in all steps of organisation, management, implementation and evaluation as a prerequisite to run an organized, population based screening programme. Professionally mixed group discuss and answer the questions: a) What are the main challenges to be improved for quality assurance of CRO colorectal cancer screening programme in organisation, management and implementation, and evaluation? b) Where changes are most needed? What should be done first, what next? Rang them in importance. c) Which changes are the easiest to implement and which most difficult?? Please rang them from the easiest to introduce to the more complicated. Rapporteur of the group will have to report to coordinator and to other groups. Use flipchart paper to colect important masages to be reorted.
COMMISSION OF THE EUROPEAN COMMUNITIES
 COMMISSION OF THE EUROPEAN COMMUNITIES Brussels, 22.12.2008 COM(2008) 882 final REPORT FROM THE COMMISSION TO THE COUNCIL, THE EUROPEAN PARLIAMENT, THE EUROPEAN ECONOMIC AND SOCIAL COMMITTEE AND THE COMMITTEE
COMMISSION OF THE EUROPEAN COMMUNITIES Brussels, 22.12.2008 COM(2008) 882 final REPORT FROM THE COMMISSION TO THE COUNCIL, THE EUROPEAN PARLIAMENT, THE EUROPEAN ECONOMIC AND SOCIAL COMMITTEE AND THE COMMITTEE
Implementing of Population-based FOBT Screening
 Implementing of Population-based FOBT Screening gfobt to FIT Experience from England Prof Stephen P. Halloran Guaiac FOBt Haem 2H 2 O 2 = 2H 2 0 + O 2 Oxidised guaiaconic acid is blue Biennial Bowel Cancer
Implementing of Population-based FOBT Screening gfobt to FIT Experience from England Prof Stephen P. Halloran Guaiac FOBt Haem 2H 2 O 2 = 2H 2 0 + O 2 Oxidised guaiaconic acid is blue Biennial Bowel Cancer
The Dutch bowel cancer screening program Relevant lessions for Ontario
 The Dutch bowel cancer screening program Relevant lessions for Ontario Ernst J Kuipers Erasmus MC University Medical Center Rotterdam - The Netherlands 1 Ismar Boas (1858 1938) Colorectal cancer screening
The Dutch bowel cancer screening program Relevant lessions for Ontario Ernst J Kuipers Erasmus MC University Medical Center Rotterdam - The Netherlands 1 Ismar Boas (1858 1938) Colorectal cancer screening
Measuring performance and quality indicators of CRC screening
 Measuring performance and quality indicators of CRC screening Ondřej MÁJEK Institute of Biostatistics and Analyses, Masaryk University Institute of Biostatistics and Analyses, Masaryk University, Brno
Measuring performance and quality indicators of CRC screening Ondřej MÁJEK Institute of Biostatistics and Analyses, Masaryk University Institute of Biostatistics and Analyses, Masaryk University, Brno
SCREENING FOR BOWEL CANCER USING FLEXIBLE SIGMOIDOSCOPY REVIEW APPRAISAL CRITERIA FOR THE UK NATIONAL SCREENING COMMITTEE
 SCREENING FOR BOWEL CANCER USING FLEXIBLE SIGMOIDOSCOPY REVIEW APPRAISAL CRITERIA FOR THE UK NATIONAL SCREENING COMMITTEE The Condition 1. The condition should be an important health problem Colorectal
SCREENING FOR BOWEL CANCER USING FLEXIBLE SIGMOIDOSCOPY REVIEW APPRAISAL CRITERIA FOR THE UK NATIONAL SCREENING COMMITTEE The Condition 1. The condition should be an important health problem Colorectal
Colorectal cancer screening in England
 Colorectal cancer screening in England critical analysis Prof Stephen P. Halloran Participation Rate 57% All Screens (1.9% +ve) 52% Prevalent 1 st Screen (age 60 years) 36% Prevalent Screen (2.2% +ve)
Colorectal cancer screening in England critical analysis Prof Stephen P. Halloran Participation Rate 57% All Screens (1.9% +ve) 52% Prevalent 1 st Screen (age 60 years) 36% Prevalent Screen (2.2% +ve)
An Update on the Bowel Cancer Screening Programme. Natasha Djedovic, London Hub Director 17 th September 2018
 An Update on the Bowel Cancer Screening Programme Natasha Djedovic, London Hub Director 17 th September 2018 NHS Bowel Cancer Screening Programme 2006: 60-69 yr old men & women offered guaiac Faecal Occult
An Update on the Bowel Cancer Screening Programme Natasha Djedovic, London Hub Director 17 th September 2018 NHS Bowel Cancer Screening Programme 2006: 60-69 yr old men & women offered guaiac Faecal Occult
Bowel cancer screening and prevention
 Bowel cancer screening and prevention Cancer Incidence and Mortality Victoria 2012 Number 6000 5000 4000 3000 2000 Incidences = 29,387 Mortality = 10,780 Incidence Mortality 1000 0 Prostate Breast Bowel
Bowel cancer screening and prevention Cancer Incidence and Mortality Victoria 2012 Number 6000 5000 4000 3000 2000 Incidences = 29,387 Mortality = 10,780 Incidence Mortality 1000 0 Prostate Breast Bowel
WEO CRC SC Meeting. Barcelona, Spain October 23, 2015
 WEO CRC SC Meeting Barcelona, Spain October 23, 2015 Identification of serrated polyposis syndrome in the context of population-based CRC screening programs Evelien Dekker Academic Medical Center Amsterdam,
WEO CRC SC Meeting Barcelona, Spain October 23, 2015 Identification of serrated polyposis syndrome in the context of population-based CRC screening programs Evelien Dekker Academic Medical Center Amsterdam,
05/07/2018. Organisation. The English screening programme what is happening? Organisation. Bowel cancer screening in the UK is:
 Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
Screening & Surveillance Guidelines
 Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Annual Report. Public Health Screening Programmes TO 31 MARCH Extract: Chapter 3 : Planning for Bowel Screening Programme
 Public Health Screening Programmes Annual Report TO 31 MARCH 2007 Extract: Chapter 3 : Planning for Bowel Screening Programme Version 1.0 Published: 18 December 2007 1 Contents INTRODUCTION...3 SUMMARY...5
Public Health Screening Programmes Annual Report TO 31 MARCH 2007 Extract: Chapter 3 : Planning for Bowel Screening Programme Version 1.0 Published: 18 December 2007 1 Contents INTRODUCTION...3 SUMMARY...5
Interventions to Improve Follow-up of Positive Results on Fecal Blood Tests
 Interventions to Improve Follow-up of Positive Results on Fecal Blood Tests Results of a systematic review, Kaiser experience, and implications for the Canton of Vaud Kevin Selby, M.D. Kevin.Selby@hospvd.ch
Interventions to Improve Follow-up of Positive Results on Fecal Blood Tests Results of a systematic review, Kaiser experience, and implications for the Canton of Vaud Kevin Selby, M.D. Kevin.Selby@hospvd.ch
Increasing Colorectal Cancer Screening in Wyoming. Allie Bain, MPH Outreach & Education Supervisor Wyoming Integrated Cancer Services Program
 Increasing Colorectal Cancer Screening in Wyoming Allie Bain, MPH Outreach & Education Supervisor Wyoming Integrated Cancer Services Program Overview What is colorectal cancer? What are risk factors for
Increasing Colorectal Cancer Screening in Wyoming Allie Bain, MPH Outreach & Education Supervisor Wyoming Integrated Cancer Services Program Overview What is colorectal cancer? What are risk factors for
Early detection and screening for colorectal neoplasia
 Early detection and screening for colorectal neoplasia Robert S. Bresalier Department of Gastroenterology, Hepatology and Nutrition. The University of Texas. MD Anderson Cancer Center. Houston, Texas U.S.A.
Early detection and screening for colorectal neoplasia Robert S. Bresalier Department of Gastroenterology, Hepatology and Nutrition. The University of Texas. MD Anderson Cancer Center. Houston, Texas U.S.A.
Northern Ireland Bowel Cancer Screening Programme. Pathways. Version 4 1 st October 2013
 Northern Ireland Bowel Cancer Screening Programme Pathways These changes will be version controlled, led by the Quality Assurance Director for the Programme. Any updated versions will be circulated and
Northern Ireland Bowel Cancer Screening Programme Pathways These changes will be version controlled, led by the Quality Assurance Director for the Programme. Any updated versions will be circulated and
Programme Report Round One
 Programme Report 2012-2015 Round One Contents Introduction from the Head of Screening, National Screening Service 2 Message from the Clinical Director, BowelScreen 4 Message from the Programme Manager,
Programme Report 2012-2015 Round One Contents Introduction from the Head of Screening, National Screening Service 2 Message from the Clinical Director, BowelScreen 4 Message from the Programme Manager,
ENGAGING PRIMARY CARE IN BOWEL SCREENING
 ENGAGING PRIMARY CARE IN BOWEL SCREENING GP GOOD PRACTICE GUIDE SCOTLAND VERSION ENGAGING PRIMARY CARE IN BOWEL SCREENING GP GOOD PRACTICE GUIDE SCOTLAND VERSION CONTENT 2 Background & information on the
ENGAGING PRIMARY CARE IN BOWEL SCREENING GP GOOD PRACTICE GUIDE SCOTLAND VERSION ENGAGING PRIMARY CARE IN BOWEL SCREENING GP GOOD PRACTICE GUIDE SCOTLAND VERSION CONTENT 2 Background & information on the
The New Grade A: USPSTF Updated Colorectal Cancer Screening Guidelines, What does it all mean?
 The New Grade A: USPSTF Updated Colorectal Cancer Screening Guidelines, What does it all mean? Robert A. Smith, PhD Cancer Control, Department of Prevention and Early Detection American Cancer Society
The New Grade A: USPSTF Updated Colorectal Cancer Screening Guidelines, What does it all mean? Robert A. Smith, PhD Cancer Control, Department of Prevention and Early Detection American Cancer Society
Practical challenges in establishing and running the Czech national colorectal cancer screening programme
 Ústřední vojenská nemocnice - Vojenská fakultní nemocnice Praha 1. lékařská fakulta Univerzity Karlovy Interní klinika Practical challenges in establishing and running the Czech national colorectal cancer
Ústřední vojenská nemocnice - Vojenská fakultní nemocnice Praha 1. lékařská fakulta Univerzity Karlovy Interní klinika Practical challenges in establishing and running the Czech national colorectal cancer
Colorectal cancer screening
 26 Colorectal cancer screening BETHAN GRAF AND JOHN MARTIN Colorectal cancer is theoretically a preventable disease and is ideally suited to a population screening programme, as there is a long premalignant
26 Colorectal cancer screening BETHAN GRAF AND JOHN MARTIN Colorectal cancer is theoretically a preventable disease and is ideally suited to a population screening programme, as there is a long premalignant
Pathology in Slovenian CRC screening programme:
 Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
Pathology in Slovenian CRC screening programme: Findings, organisation and quality assurance Snježana Frković Grazio University Medical Center Ljubljana, Slovenia Slovenia s population: 2 million Incidence
GENERAL PRACTITIONERS IN THE 1ST LINE OF CANCER PREVENTION
 GENERAL PRACTITIONERS IN THE 1ST LINE OF CANCER PREVENTION Bohumil Seifert Dpt. Of General Practice 1st Faculty of Medicine Charles University in Prague May, 29, 2015 European Colorectal Cancer Days, Brno
GENERAL PRACTITIONERS IN THE 1ST LINE OF CANCER PREVENTION Bohumil Seifert Dpt. Of General Practice 1st Faculty of Medicine Charles University in Prague May, 29, 2015 European Colorectal Cancer Days, Brno
Bowel Cancer Screening Exploiting science brings better medicine
 Camberley & District Bowel Cancer Screening Exploiting science brings better medicine Prof Stephen P. Halloran World - All Cancers Men Incidence & Mortality (2012) Women Incidence Mortality GLOBOCAN 2012
Camberley & District Bowel Cancer Screening Exploiting science brings better medicine Prof Stephen P. Halloran World - All Cancers Men Incidence & Mortality (2012) Women Incidence Mortality GLOBOCAN 2012
Global colorectal cancer screening appropriate or practical? Graeme P Young, Flinders University WCC, Melbourne
 Global colorectal cancer screening appropriate or practical? Graeme P Young, Flinders University. 2014 WCC, Melbourne Outline WHO criteria to justify screening Appropriateness: Global variation in incidence
Global colorectal cancer screening appropriate or practical? Graeme P Young, Flinders University. 2014 WCC, Melbourne Outline WHO criteria to justify screening Appropriateness: Global variation in incidence
Improving Outcomes in Colorectal Cancer: The Science of Screening. Colorectal Cancer (CRC)
") Improving Outcomes in Colorectal Cancer: The Science of Screening Tennessee Primary Care Association October 23, 2014 Durado Brooks, MD, MPH Director, Prostate and Colorectal Cancers Colorectal Cancer
Improving Outcomes in Colorectal Cancer: The Science of Screening Tennessee Primary Care Association October 23, 2014 Durado Brooks, MD, MPH Director, Prostate and Colorectal Cancers Colorectal Cancer
Prof Stephen P. Halloran. Update on the NHS Bowel Cancer Screening Programme Focus on BS & FIT
 Prof Stephen P. Halloran Update on the NHS Bowel Cancer Screening Programme Focus on BS & FIT World Top 20 Cancers Men Incidence & Mortality (2012) Women World Colorectal Cancer 3 rd commonest cancer 4
Prof Stephen P. Halloran Update on the NHS Bowel Cancer Screening Programme Focus on BS & FIT World Top 20 Cancers Men Incidence & Mortality (2012) Women World Colorectal Cancer 3 rd commonest cancer 4
ADENOMA SURVEILLANCE BCSP Guidance Note No 1 Version 1 September 2009
 ADENOMA SURVEILLANCE BCSP Guidance Note No 1 Version 1 September 2009 Published by: NHS Cancer Screening Programmes Fulwood House Old Fulwood Road Sheffield S10 3TH Tel: 0114 271 1060 Fax: 0114 271 1089
ADENOMA SURVEILLANCE BCSP Guidance Note No 1 Version 1 September 2009 Published by: NHS Cancer Screening Programmes Fulwood House Old Fulwood Road Sheffield S10 3TH Tel: 0114 271 1060 Fax: 0114 271 1089
Exemplary Primary Care Practices 80% by 2018 Mini Webinar Series. November 10th, :00pm EST
 Exemplary Primary Care Practices 80% by 2018 Mini Webinar Series November 10th, 2015 1:00pm EST Purpose of Today s Webinar Examine best practices that primary care providers and practices can undertake
Exemplary Primary Care Practices 80% by 2018 Mini Webinar Series November 10th, 2015 1:00pm EST Purpose of Today s Webinar Examine best practices that primary care providers and practices can undertake
The choice of methods for Colorectal Cancer Screening; The Dutch experience
 The choice of methods for Colorectal Cancer Screening; The Dutch experience Monique van Leerdam, Gastroenterologist, NKI-AVL, Amsterdam The Netherlands Colorectal cancer CRC 2 nd cause of cancer related
The choice of methods for Colorectal Cancer Screening; The Dutch experience Monique van Leerdam, Gastroenterologist, NKI-AVL, Amsterdam The Netherlands Colorectal cancer CRC 2 nd cause of cancer related
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Colorectal Cancer Screening in Ohio CHCs. Ohio Association of Community Health Centers
 Colorectal Cancer Screening in Ohio CHCs Ohio Association of Community Health Centers 2 1/29/2015 Your Speakers Dr. Ted Wymyslo Ashley Ballard Randy Runyon 3 1/29/2015 Facts 3 rd most common cancer in
Colorectal Cancer Screening in Ohio CHCs Ohio Association of Community Health Centers 2 1/29/2015 Your Speakers Dr. Ted Wymyslo Ashley Ballard Randy Runyon 3 1/29/2015 Facts 3 rd most common cancer in
Thank You to Our Sponsors: Evaluations & CE Credits. Featured Speakers. Conflict of Interest & Disclosure Statements
 Thank You to Our Sponsors: University at Albany School of Public Health NYS Department of Health Evaluations & CE Credits Nursing Contact Hours, CME and CHES credits are available. Please visit www.phlive.org
Thank You to Our Sponsors: University at Albany School of Public Health NYS Department of Health Evaluations & CE Credits Nursing Contact Hours, CME and CHES credits are available. Please visit www.phlive.org
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care
 Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Digestive Health Southwest Endoscopy 2016 Quality Report
 Digestive Health 2016 Quality Report Our 2016 our quality and value management program focused on one primary area of interest: Performing high quality colonoscopy High quality Colonoscopy We selected
Digestive Health 2016 Quality Report Our 2016 our quality and value management program focused on one primary area of interest: Performing high quality colonoscopy High quality Colonoscopy We selected
Objectives. Definitions. Colorectal Cancer Screening 5/8/2018. Payam Afshar, MS, MD Kaiser Permanente, San Diego. Colorectal cancer background
 Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
National Colonoscopy Study (NCS) Screening Colonoscopy versus Annual Fecal Occult Blood Test NCT
 Screening Colonoscopy versus Annual Fecal Occult Blood Test NCT") National Colonoscopy Study (NCS) Screening Colonoscopy versus Annual Fecal Occult Blood Test NCT 00102011 Ann Zauber Sidney Winawer, Michael O Brien, John Allen, Andrew Feld, Glenn Mills, Robin Mendelsohn,
National Colonoscopy Study (NCS) Screening Colonoscopy versus Annual Fecal Occult Blood Test NCT 00102011 Ann Zauber Sidney Winawer, Michael O Brien, John Allen, Andrew Feld, Glenn Mills, Robin Mendelsohn,
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer
 Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
Transition to Fecal Immunochemical Testing (FIT)
") Transition to Fecal Immunochemical Testing (FIT) Frequently Asked Questions for Primary Care Providers October 2017 Version 1.1 Overview Ontario will be transitioning from the guaiac fecal occult blood
Transition to Fecal Immunochemical Testing (FIT) Frequently Asked Questions for Primary Care Providers October 2017 Version 1.1 Overview Ontario will be transitioning from the guaiac fecal occult blood
1 APRIL 2007 TO 31 MARCH
 Public Health Screening Programmes Annual Report 1 APRIL 2007 TO 31 MARCH 2008 Extract: Chapter 3: Planning for the Bowel Screening Programme Public Health Screening Unit Version 1.0 Published: 16 December
Public Health Screening Programmes Annual Report 1 APRIL 2007 TO 31 MARCH 2008 Extract: Chapter 3: Planning for the Bowel Screening Programme Public Health Screening Unit Version 1.0 Published: 16 December
COLORECTAL SCREENING PROGRAMME: IMPACT ON THE HOSPITAL S PATHOLOGY SERVICES SINCE ITS INTRODUCTION.
 The West London Medical Journal 2009 Vol No 1 pp 23-31 COLORECTAL SCREENING PROGRAMME: IMPACT ON THE HOSPITAL S PATHOLOGY SERVICES SINCE ITS INTRODUCTION. Competing interests: None declared ABSTRACT Sarah
The West London Medical Journal 2009 Vol No 1 pp 23-31 COLORECTAL SCREENING PROGRAMME: IMPACT ON THE HOSPITAL S PATHOLOGY SERVICES SINCE ITS INTRODUCTION. Competing interests: None declared ABSTRACT Sarah
Colon Cancer Screening. A Provider Opinion Survey
 Colon Cancer Screening A Provider Opinion Survey 1. Background Information What is colon cancer? Who needs to be screened? Colorectal Cancer» Presence of abnormal cells in the colon or rectum that divide
Colon Cancer Screening A Provider Opinion Survey 1. Background Information What is colon cancer? Who needs to be screened? Colorectal Cancer» Presence of abnormal cells in the colon or rectum that divide
2. CANCER AND CANCER SCREENING
 2. CANCER AND CANCER SCREENING INTRODUCTION The incidence of cancer and premature mortality from cancer are higher in Islington compared to the rest of England. Although death rates are reducing, this
2. CANCER AND CANCER SCREENING INTRODUCTION The incidence of cancer and premature mortality from cancer are higher in Islington compared to the rest of England. Although death rates are reducing, this
Faecal Immunochemical Testing (FIT) for Screening and Symptomatic Patients
 for Screening and Symptomatic Patients") Faecal Immunochemical Testing (FIT) for Screening and Symptomatic Patients Caroline Addison NE BCSP Hub Director and Consultant Clinical Scientist What is FIT Type of Faecal Occult Blood test Designed
Faecal Immunochemical Testing (FIT) for Screening and Symptomatic Patients Caroline Addison NE BCSP Hub Director and Consultant Clinical Scientist What is FIT Type of Faecal Occult Blood test Designed
Screening for Colorectal Cancer: Se0ng it up and making it work. Julie8a Patnick 4 December 2014
 Screening for Colorectal Cancer: Se0ng it up and making it work Julie8a Patnick 4 December 2014 Evaluation of the UK Colorectal Cancer Screening Pilot Two sites, population ~ 1m Coventry & Warwickshire
Screening for Colorectal Cancer: Se0ng it up and making it work Julie8a Patnick 4 December 2014 Evaluation of the UK Colorectal Cancer Screening Pilot Two sites, population ~ 1m Coventry & Warwickshire
Citation for published version (APA): Wijkerslooth de Weerdesteyn, T. R. (2013). Population screening for colorectal cancer by colonoscopy
: Wijkerslooth de Weerdesteyn, T. R. (2013). Population screening for colorectal cancer by colonoscopy") UvA-DARE (Digital Academic Repository) Population screening for colorectal cancer by colonoscopy de Wijkerslooth, T.R. Link to publication Citation for published version (APA): Wijkerslooth de Weerdesteyn,
UvA-DARE (Digital Academic Repository) Population screening for colorectal cancer by colonoscopy de Wijkerslooth, T.R. Link to publication Citation for published version (APA): Wijkerslooth de Weerdesteyn,
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series
 Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Best Practices for Colorectal Cancer Screening March 14, 2018 12:00pm 1:00pm Robert A. Smith, PhD Vice President, Cancer
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Best Practices for Colorectal Cancer Screening March 14, 2018 12:00pm 1:00pm Robert A. Smith, PhD Vice President, Cancer
FECAL OCCULT BLOOD TEST (FOBT) Common Guaiac versus Immunochemical Test
 Common Guaiac versus Immunochemical Test") FECAL OCCULT BLOOD TEST (FOBT) Common Guaiac versus Immunochemical Test LIMBACH-LABORATORY H E I D E L B E R G H J Roth H Schmidt-Gayk Estimated incidence of cancer in Europe and European Union, 2006 Limbach
FECAL OCCULT BLOOD TEST (FOBT) Common Guaiac versus Immunochemical Test LIMBACH-LABORATORY H E I D E L B E R G H J Roth H Schmidt-Gayk Estimated incidence of cancer in Europe and European Union, 2006 Limbach
FREQUENTLY ASKED QUESTIONS
 FREQUENTLY ASKED QUESTIONS What is CRC? CRC (CRC) is cancer of the large intestine (colon), the lower part of the digestive system. Rectal cancer is cancer of the last several inches of the colon. Together,
FREQUENTLY ASKED QUESTIONS What is CRC? CRC (CRC) is cancer of the large intestine (colon), the lower part of the digestive system. Rectal cancer is cancer of the last several inches of the colon. Together,
Primary care at the forefront of colorectal cancer screening
 Primary care at the forefront of colorectal cancer screening Presentation by Bohumil Seifert Department of General Practice, 1st Faculy of Medicine, Charles University in Prague 04/05/2012 Introduction
Primary care at the forefront of colorectal cancer screening Presentation by Bohumil Seifert Department of General Practice, 1st Faculy of Medicine, Charles University in Prague 04/05/2012 Introduction
Challenges for Colorectal Cancer Screening
 Challenges for Colorectal Cancer Screening a Biomarker with No Standards! Prof. Emeritus Stephen P. Halloran University of Surrey W. Europe Top 20 Cancers Men Incidence & Mortality (2012) Women World -
Challenges for Colorectal Cancer Screening a Biomarker with No Standards! Prof. Emeritus Stephen P. Halloran University of Surrey W. Europe Top 20 Cancers Men Incidence & Mortality (2012) Women World -
Colorectal Cancer Screening. Paul Berg MD
 Colorectal Cancer Screening Paul Berg MD What is clinical integration? AMA Definition The means to facilitate the coordination of patient care across conditions, providers, settings, and time in order
Colorectal Cancer Screening Paul Berg MD What is clinical integration? AMA Definition The means to facilitate the coordination of patient care across conditions, providers, settings, and time in order
Engaging Primary Care in bowel screening
 Engaging Primary Care in bowel screening GP good practice guide for Wales December 2018 Together we will beat cancer Contents Background 3 The FIT screening pathway in Wales 4 The role of GP practices
Engaging Primary Care in bowel screening GP good practice guide for Wales December 2018 Together we will beat cancer Contents Background 3 The FIT screening pathway in Wales 4 The role of GP practices
Bowel Screening Wales E-Bulletin October 2010
 Bowel Screening Wales E-Bulletin October 2010 News I am delighted to have returned to work after 5 months sick leave and would like to thank everyone for all their hard work and kind wishes while I was
Bowel Screening Wales E-Bulletin October 2010 News I am delighted to have returned to work after 5 months sick leave and would like to thank everyone for all their hard work and kind wishes while I was
Kenneth D. Chi, MD Medical Director, GI Lab Advocate Lutheran General Hospital Center for Digestive Health May 7, 2016
 Kenneth D. Chi, MD Medical Director, GI Lab Advocate Lutheran General Hospital Center for Digestive Health May 7, 2016 Why have Quality Indicators? Pre-procedure Quality Indicators Intra-procedure Quality
Kenneth D. Chi, MD Medical Director, GI Lab Advocate Lutheran General Hospital Center for Digestive Health May 7, 2016 Why have Quality Indicators? Pre-procedure Quality Indicators Intra-procedure Quality
HOW TO EVALUATE ACTIVITIES INTENDED TO INCREASE AWARENESS AND USE OF COLORECTAL CANCER SCREENING. Using your toolkit to conduct an evaluation
 EVALUATION TOOLKIT HOW TO EVALUATE ACTIVITIES INTENDED TO INCREASE AWARENESS AND USE OF COLORECTAL CANCER SCREENING Using your toolkit to conduct an evaluation Welcome Mary Doroshenk, MA Director National
EVALUATION TOOLKIT HOW TO EVALUATE ACTIVITIES INTENDED TO INCREASE AWARENESS AND USE OF COLORECTAL CANCER SCREENING Using your toolkit to conduct an evaluation Welcome Mary Doroshenk, MA Director National
Colorectal Cancer Screening
 Colorectal Cancer Screening Colorectal cancer is preventable. Routine screening can reduce deaths through the early diagnosis and removal of pre-cancerous polyps. Screening saves lives, but only if people
Colorectal Cancer Screening Colorectal cancer is preventable. Routine screening can reduce deaths through the early diagnosis and removal of pre-cancerous polyps. Screening saves lives, but only if people
UK Bowel Cancer screening Dr Voi Shim Wong BsC MD FRCP. Consultant Gastroenterologist Accredited BCSP colonoscopist Whittington + UCL Hospitals
 UK Bowel Cancer screening 2017 Dr Voi Shim Wong BsC MD FRCP Consultant Gastroenterologist Accredited BCSP colonoscopist Whittington + UCL Hospitals Bowel Cancer Contents UK Bowel Cancer Screening Programme
UK Bowel Cancer screening 2017 Dr Voi Shim Wong BsC MD FRCP Consultant Gastroenterologist Accredited BCSP colonoscopist Whittington + UCL Hospitals Bowel Cancer Contents UK Bowel Cancer Screening Programme
Alberta Colorectal Cancer Screening Program
 January 14 Alberta Colorectal Cancer Screening Program Standards and Guidelines Version 4.0 of 4.0 Part 1 Standards and Guidelines Draft Document Leaders Dr. Clarence Wong, Medical Lead ACRCSP, Gastroenterologist
January 14 Alberta Colorectal Cancer Screening Program Standards and Guidelines Version 4.0 of 4.0 Part 1 Standards and Guidelines Draft Document Leaders Dr. Clarence Wong, Medical Lead ACRCSP, Gastroenterologist
2019 COLLECTION TYPE: MIPS CLINICAL QUALITY MEASURES (CQMS) MEASURE TYPE: Outcome High Priority
 MEASURE TYPE: Outcome High Priority") Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Preventive Care 2019 COLLECTION TYPE: MIPS CLINICAL QUALITY
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care Meaningful Measure Area: Preventive Care 2019 COLLECTION TYPE: MIPS CLINICAL QUALITY
Northern Ireland Bowel Cancer Screening Programme
 Northern Ireland Bowel Cancer Screening Programme Inaugural Report April 2010 March 2013 Published: 30 October 2014 (amended: 3 December 2014) 2 P a g e Contents Contents... 3 Foreword... 7 1 Introduction...
Northern Ireland Bowel Cancer Screening Programme Inaugural Report April 2010 March 2013 Published: 30 October 2014 (amended: 3 December 2014) 2 P a g e Contents Contents... 3 Foreword... 7 1 Introduction...
WEO CRC SC Meeting. Barcelona, Spain October 23, 2015
 WEO CRC SC Meeting Barcelona, Spain October 23, 2015 THE HEMOGLOBIN CONCENTRATION IN A NEGATIVE RESULT AS A PREDICTOR FOR ADVANCED NEOPLASIA Isabel Portillo, Eunare Arana-Arri, Isabel Idigoras, Lorea Martínez-Indart.
WEO CRC SC Meeting Barcelona, Spain October 23, 2015 THE HEMOGLOBIN CONCENTRATION IN A NEGATIVE RESULT AS A PREDICTOR FOR ADVANCED NEOPLASIA Isabel Portillo, Eunare Arana-Arri, Isabel Idigoras, Lorea Martínez-Indart.
The National Guidelines For Colorectal Cancer Screening and Diagnosis.
 The National Guidelines For Colorectal Cancer Screening and Diagnosis www.mohap.gov.ae December, 2014 Adapted from HAAD Standard for Colorectal Cancer Screening & Diagnosis 2014 The National Cancer Screening
The National Guidelines For Colorectal Cancer Screening and Diagnosis www.mohap.gov.ae December, 2014 Adapted from HAAD Standard for Colorectal Cancer Screening & Diagnosis 2014 The National Cancer Screening
GIQIC18 Appropriate follow-up interval of not less than 5 years for colonoscopies with findings of 1-2 tubular adenomas < 10 mm
 GI Quality Improvement Consortium, Ltd. (GIQuIC) 1 Following is an overview of the clinical quality measures in GIQuIC that can be reported to CMS for the Quality performance category of the Merit-Based
GI Quality Improvement Consortium, Ltd. (GIQuIC) 1 Following is an overview of the clinical quality measures in GIQuIC that can be reported to CMS for the Quality performance category of the Merit-Based
Fact sheet on bowel cancer screening programme
 Fact sheet on bowel cancer screening programme What does the bowel cancer screening programme involve? The bowel cancer screening programme focuses on men and women from 55 to 75 years of age. Every two
Fact sheet on bowel cancer screening programme What does the bowel cancer screening programme involve? The bowel cancer screening programme focuses on men and women from 55 to 75 years of age. Every two
Positive Results on Fecal Blood Tests
 Interventions to Improve Follow-up of Positive Results on Fecal Blood Tests Results of a systematic review and Kaiser experience Kevin Selby, M.D. kevin.j.selby@kp.org National Colorectal Cancer Roundtable
Interventions to Improve Follow-up of Positive Results on Fecal Blood Tests Results of a systematic review and Kaiser experience Kevin Selby, M.D. kevin.j.selby@kp.org National Colorectal Cancer Roundtable
Are you ready for the Colorectal Cancer Screening Pilot Programme?
 Are you ready for the Colorectal Cancer Screening Pilot Programme? Dr Regina CHING Head, Surveillance and Epidemiology Branch Centre for Health Protection Department of Health 7 December 2014 Hong Kong
Are you ready for the Colorectal Cancer Screening Pilot Programme? Dr Regina CHING Head, Surveillance and Epidemiology Branch Centre for Health Protection Department of Health 7 December 2014 Hong Kong
Cervical cancer screening in Norway
 Cervical cancer screening in Norway «The future of cancer screening in Estonia: health benefits and best practices» 17 November 2016, Tartu Stefan Lönnberg Cancer Registry of Norway Screening governance
Cervical cancer screening in Norway «The future of cancer screening in Estonia: health benefits and best practices» 17 November 2016, Tartu Stefan Lönnberg Cancer Registry of Norway Screening governance
Colonoscopy Quality Data
 Colonoscopy Quality Data www.dhsgi.com Introduction Colorectal cancer is the second leading cause of cancer related deaths in the United States, in men and women combined. In 2016, there are expected to
Colonoscopy Quality Data www.dhsgi.com Introduction Colorectal cancer is the second leading cause of cancer related deaths in the United States, in men and women combined. In 2016, there are expected to
Research Article Development of Polyps and Cancer in Patients with a Negative Colonoscopy: A Follow-Up Study of More Than 20 Years
 ISRN Gastroenterology, Article ID 261302, 4 pages http://dx.doi.org/10.1155/2014/261302 Research Article Development of Polyps and Cancer in Patients with a Negative Colonoscopy: A Follow-Up Study of More
ISRN Gastroenterology, Article ID 261302, 4 pages http://dx.doi.org/10.1155/2014/261302 Research Article Development of Polyps and Cancer in Patients with a Negative Colonoscopy: A Follow-Up Study of More
11/9/2015 OUTLINE. Quality Indicators for the Doctor Performing Screening Colonoscopy: What you should expect from your Endoscopist
 Quality Indicators for the Doctor Performing Screening Colonoscopy: What you should expect from your Endoscopist Anil K Sharma MD FACP Professor of Clinical Medicine, University of Rochester Chief of Gastroenterology,
Quality Indicators for the Doctor Performing Screening Colonoscopy: What you should expect from your Endoscopist Anil K Sharma MD FACP Professor of Clinical Medicine, University of Rochester Chief of Gastroenterology,
Ontario s New Colorectal Cancer Screening Program. OHA May 15, 2007
 Ontario s New Colorectal Cancer Screening Program OHA May 15, 2007 Outline The Context Facts About Colorectal Cancer Research and Background Information The CRC Screening Program Average Risk Screening
Ontario s New Colorectal Cancer Screening Program OHA May 15, 2007 Outline The Context Facts About Colorectal Cancer Research and Background Information The CRC Screening Program Average Risk Screening
Czech CRC screening program at the point of switch to the population based design
 Military University Hospital First Medical Faculty of Charles University Department of Gastroenterology Czech CRC screening program at the point of switch to the population based design M. Zavoral, S.
Military University Hospital First Medical Faculty of Charles University Department of Gastroenterology Czech CRC screening program at the point of switch to the population based design M. Zavoral, S.
Colorectal Cancer Screening in Canada MONITORING & EVALUATION OF QUALITY INDICATORS RESULTS REPORT
 Colorectal Cancer Screening in Canada MONITORING & EVALUATION OF QUALITY INDICATORS RESULTS REPORT JANUARY 2011 DECEMBER 2012 Acknowledgments The Canadian Partnership Against Cancer would like to gratefully
Colorectal Cancer Screening in Canada MONITORING & EVALUATION OF QUALITY INDICATORS RESULTS REPORT JANUARY 2011 DECEMBER 2012 Acknowledgments The Canadian Partnership Against Cancer would like to gratefully
CRC Risk Factors. U.S. Adherence Rates Cancer Screening. Genetic Model of Colorectal Cancer. Epidemiology and Clinical Consequences of CRC
 10:45 11:45 am Guide to Colorectal Cancer Screening SPEAKER Howard Manten M.D. Presenter Disclosure Information The following relationships exist related to this presentation: Howard Manten MD: No financial
10:45 11:45 am Guide to Colorectal Cancer Screening SPEAKER Howard Manten M.D. Presenter Disclosure Information The following relationships exist related to this presentation: Howard Manten MD: No financial
Colorectal Cancer Screening
 Colorectal Cancer Screening An Integrated Care Pathway of the Collaborative Care Network Subject Matter Expert: Kevin Wolov, DO Pathway Custodian: Pat Czapp, MD First, a Friendly Reminder... This Integrated
Colorectal Cancer Screening An Integrated Care Pathway of the Collaborative Care Network Subject Matter Expert: Kevin Wolov, DO Pathway Custodian: Pat Czapp, MD First, a Friendly Reminder... This Integrated
Colorectal Cancer Screening: A Clinical Update
 11:05 11:45am Colorectal Cancer Screening: A Clinical Update SPEAKER Kevin A. Ghassemi, MD Presenter Disclosure Information The following relationships exist related to this presentation: Kevin A. Ghassemi,
11:05 11:45am Colorectal Cancer Screening: A Clinical Update SPEAKER Kevin A. Ghassemi, MD Presenter Disclosure Information The following relationships exist related to this presentation: Kevin A. Ghassemi,
NHS Bowel Cancer Screening Programmes: Evaluation of pilot of Faecal Immunochemical Test : Final report.
 NHS Bowel Cancer Screening Programmes: Evaluation of pilot of Faecal Immunochemical Test : Final report. Sue Moss, Christopher Mathews Centre for Cancer Prevention, Wolfson Institute, Queen Mary University
NHS Bowel Cancer Screening Programmes: Evaluation of pilot of Faecal Immunochemical Test : Final report. Sue Moss, Christopher Mathews Centre for Cancer Prevention, Wolfson Institute, Queen Mary University
Efficacy, effectiveness, quality: sources of data
 Efficacy, effectiveness, quality: sources of data Ondřej MÁJEK Institute of Biostatistics and Analyses, Masaryk University Institute of Biostatistics and Analyses, Masaryk University, Brno Key Questions
Efficacy, effectiveness, quality: sources of data Ondřej MÁJEK Institute of Biostatistics and Analyses, Masaryk University Institute of Biostatistics and Analyses, Masaryk University, Brno Key Questions
Bowel Cancer Prevention and Screening. Harriet Wynne, Cancer Council Victoria
 Bowel Cancer Prevention and Screening Harriet Wynne, Cancer Council Victoria New cases and deaths for the Victoria population in 2013 Thursfield V, et al. Cancer in Victoria: Statistics & trends 2013.
Bowel Cancer Prevention and Screening Harriet Wynne, Cancer Council Victoria New cases and deaths for the Victoria population in 2013 Thursfield V, et al. Cancer in Victoria: Statistics & trends 2013.
Pathology in Slovenian CRC screening programme: Organisation and quality assurance. Snježana Frković Grazio and Matej Bračko
 Pathology in Slovenian CRC screening programme: Organisation and quality assurance Snježana Frković Grazio and Matej Bračko June 2009 to December 2013 (first three rounds) 33 969 colonoscopies were performed
Pathology in Slovenian CRC screening programme: Organisation and quality assurance Snježana Frković Grazio and Matej Bračko June 2009 to December 2013 (first three rounds) 33 969 colonoscopies were performed
Colorectal Cancer Screening and Risk Assessment Workflow. Documentation Guide for Health Center NextGen Users
 Colorectal Cancer Screening and Risk Assessment Workflow Documentation Guide for Health Center NextGen Users Colorectal Cancer Screening and Risk Assessment Workflow and Documentation Guide for Health
Colorectal Cancer Screening and Risk Assessment Workflow Documentation Guide for Health Center NextGen Users Colorectal Cancer Screening and Risk Assessment Workflow and Documentation Guide for Health
Prevention of Bowel Cancer: which patients do I send for colonoscopy?
 Prevention of Bowel Cancer: which patients do I send for colonoscopy? Dr Chris Groves Consultant Gastroenterologist and Honorary Senior Lecturer St George s Hospital and Medical School Director, SW London
Prevention of Bowel Cancer: which patients do I send for colonoscopy? Dr Chris Groves Consultant Gastroenterologist and Honorary Senior Lecturer St George s Hospital and Medical School Director, SW London
Bowel Cancer Screening
 Bowel Cancer Screening Dr John Hancock FRCP Consultant Gastroenterologist University Hospital of North Tees Outline Background Current bowel cancer screening programme Tees Screening Centre Future Flexi
Bowel Cancer Screening Dr John Hancock FRCP Consultant Gastroenterologist University Hospital of North Tees Outline Background Current bowel cancer screening programme Tees Screening Centre Future Flexi
Be it Resolved that FIT is the Best Way to Screen for Colorectal Cancer DEBATE
 Be it Resolved that FIT is the Best Way to Screen for Colorectal Cancer DEBATE DEBATE Presenters PRESENTATION MODERATOR Dr. Praveen Bansal -MD, CCFP FCFP Regional Primary Care Lead, Integrated Cancer Screening,
Be it Resolved that FIT is the Best Way to Screen for Colorectal Cancer DEBATE DEBATE Presenters PRESENTATION MODERATOR Dr. Praveen Bansal -MD, CCFP FCFP Regional Primary Care Lead, Integrated Cancer Screening,
Reflections on the EUnetHTA CRC screening full Core Model pilot 1
 Reflections on the EUnetHTA CRC screening full Core Model pilot 1 EUnetHTA Medical Technology HTA expert meeting Brussels October 16th 2015 Karsten Berndt, Economist & Epidemiologist, EDMA HTA Task Force
Reflections on the EUnetHTA CRC screening full Core Model pilot 1 EUnetHTA Medical Technology HTA expert meeting Brussels October 16th 2015 Karsten Berndt, Economist & Epidemiologist, EDMA HTA Task Force
Is there justification for levels of polyp competency? Dr Roland Valori Gloucestershire Hospitals United Kingdom
 Is there justification for levels of polyp competency? Dr Roland Valori Gloucestershire Hospitals United Kingdom What exactly will be required? Defining levels of polypectomy competency in terms of complexity/time/risk
Is there justification for levels of polyp competency? Dr Roland Valori Gloucestershire Hospitals United Kingdom What exactly will be required? Defining levels of polypectomy competency in terms of complexity/time/risk
An Introduction to MUTYH Associated Polyposis (MAP)
") An Introduction to MUTYH Associated Polyposis (MAP) 1 An Introduction to MUTYH Associated Polyposis(MAP) Contents What is MUTYH Associated Polyposis (MAP)? 2 What causes MUTYH Associated Polyposis (MAP)?
An Introduction to MUTYH Associated Polyposis (MAP) 1 An Introduction to MUTYH Associated Polyposis(MAP) Contents What is MUTYH Associated Polyposis (MAP)? 2 What causes MUTYH Associated Polyposis (MAP)?
Colon cancer screening : age 50 or over I'll talk to my doctor about it
 Vaud Colon Cancer Screening Programme Colon cancer screening : age 50 or over I'll talk to my doctor about it Dépistage du cancer du colon Canton de Vaud Contents Help deciding and family doctor 3 Colon
Vaud Colon Cancer Screening Programme Colon cancer screening : age 50 or over I'll talk to my doctor about it Dépistage du cancer du colon Canton de Vaud Contents Help deciding and family doctor 3 Colon
QA Processes. Philip DaCosta BSCP QA Lead, Yorkshire & the Humber September 2013
 QA Processes Philip DaCosta BSCP QA Lead, Yorkshire & the Humber September 2013 Standards QA visits Dashboards BCSP standards Standards for Organisation Service delivery Reporting Data quality Audit and
QA Processes Philip DaCosta BSCP QA Lead, Yorkshire & the Humber September 2013 Standards QA visits Dashboards BCSP standards Standards for Organisation Service delivery Reporting Data quality Audit and
Performance of Colorectal cancer screening in the European Union Member States Data from the second European screening report
 Performance of Colorectal cancer screening in the European Union Member States Data from the second European screening report 1 Basu P 2, Anttila A 3, Ponti A 1, Tomatis M 1, Vale DB 4, Ronco G 1, Soerjomataram
Performance of Colorectal cancer screening in the European Union Member States Data from the second European screening report 1 Basu P 2, Anttila A 3, Ponti A 1, Tomatis M 1, Vale DB 4, Ronco G 1, Soerjomataram
Service specification No. 26A NHS bowel scope screening programme
 Service specification No. 26A NHS bowel scope screening programme NHS England INFORMATION READER BOX Directorate Medical Commissioning Operations Patients and Information Nursing Trans. & Corp. Ops. Commissioning
Service specification No. 26A NHS bowel scope screening programme NHS England INFORMATION READER BOX Directorate Medical Commissioning Operations Patients and Information Nursing Trans. & Corp. Ops. Commissioning
NHS KINGSTON. Contents
 NHS KINGSTON Contents 1. Background... 2 2. Targets and quality standards... 2 3. Service provision and performance... 3 Uptake... 3 Investigations... 6 Cancer detection... 7 Age extension... 7 4. Quality
NHS KINGSTON Contents 1. Background... 2 2. Targets and quality standards... 2 3. Service provision and performance... 3 Uptake... 3 Investigations... 6 Cancer detection... 7 Age extension... 7 4. Quality
Colorectal Cancer Screening
 Colorectal Cancer Screening Colonoscopy is the gold standard for colorectal cancer screening 2 Focus on Colorectal Cancer Screening at Piedmont Healthcare Screening for colorectal cancer saves lives. Of
Colorectal Cancer Screening Colonoscopy is the gold standard for colorectal cancer screening 2 Focus on Colorectal Cancer Screening at Piedmont Healthcare Screening for colorectal cancer saves lives. Of
Colon Screening in 2014 Offering Patients a Choice. Clark A Harrison MD The Nevada Colon Cancer Partnership
 Colon Screening in 2014 Offering Patients a Choice Clark A Harrison MD The Nevada Colon Cancer Partnership Objectives 1. Understand the incidence and mortality rates for CRC in the US. 2. Understand risk
Colon Screening in 2014 Offering Patients a Choice Clark A Harrison MD The Nevada Colon Cancer Partnership Objectives 1. Understand the incidence and mortality rates for CRC in the US. 2. Understand risk
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists. International authors and editors
 We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
We are IntechOpen, the world s leading publisher of Open Access books Built by scientists, for scientists 4,100 116,000 120M Open access books available International authors and editors Downloads Our
GI Screening/Surveillance in Lynch Syndrome
 GI Screening/Surveillance in Lynch Syndrome M Appleyard Royal Brisbane and Women s Hospital Brisbane, Australia GI Disease and Lynch Syndrome What are risks of GI disease in Lynch? Who do we screen for
GI Screening/Surveillance in Lynch Syndrome M Appleyard Royal Brisbane and Women s Hospital Brisbane, Australia GI Disease and Lynch Syndrome What are risks of GI disease in Lynch? Who do we screen for
Bowel Screening Colonoscopy in Glasgow How well are we doing? How well should we be doing? How can we evidence and improve performance?
 Bowel Screening Colonoscopy in Glasgow 2017 How well are we doing? How well should we be doing? How can we evidence and improve performance? Bowel Screening Standards - Scotland Definitions Completion
Bowel Screening Colonoscopy in Glasgow 2017 How well are we doing? How well should we be doing? How can we evidence and improve performance? Bowel Screening Standards - Scotland Definitions Completion
When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool
 When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool Adenomas/Carcinoma Sequence Providing Time for Screening Normal 5-20 yrs 5-15 yrs
When is a programmed follow-up meaningful and how should it be done? Professor Alastair Watson University of Liverpool Adenomas/Carcinoma Sequence Providing Time for Screening Normal 5-20 yrs 5-15 yrs