Implementing of Population-based FOBT Screening
|
|
|
- Mark Ford
- 5 years ago
- Views:
Transcription









1 Implementing of Population-based FOBT Screening gfobt to FIT Experience from England Prof Stephen P. Halloran




2 Guaiac FOBt Haem 2H 2 O 2 = 2H O 2 Oxidised guaiaconic acid is blue

3 Biennial Bowel Cancer Screening in the UK 1990 Trial evidence 2000 Pilot programmes 2006 Commence screening England Two yearly FOBT screen Phase year olds Phase Phase 3 55 Flexi Sig
")
 10m 13m")
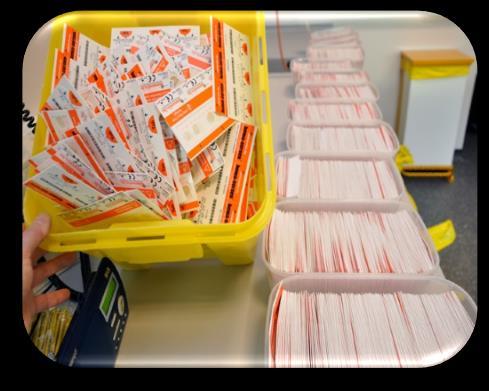
4 England 2006 Biennial Screening for Bowel Cancer England 5 Hubs Screening Hub Activities Organisation Call & recalls (25,000 /week) Laboratory analysis Helpline (>3,000 /week) Make appointments Web-based Population Screening Served Data System (millions) 10m 13m 10m 14.6m 8m
 Colonoscopy Site Clinic Sites Clinic Sites Quality Assurance 1.")


5 Bowel Cancer Screening Colonoscopy Site Clinic Sites Southern Hub (Guildford) Screening Centres (17) Colonoscopy Site Clinic Sites Clinic Sites Quality Assurance 1. Accreditation: Centres & labs. lab staff /endoscopists Screening Activities 2. Facilities: Scope cleaning, patient facilities & privacy 3. Key Performance Explain procedures indicators: Centres monitor quality 4. Continuous Assess audit: suitability Intermediate outcomes 5. Continuous evaluation: Programme evaluation group Provide colonoscopy, CTC etc 6. Peer Review: Labs, endoscopy, pathology, etc 14.6 million



")


6 Bowel Cancer Screening Colonoscopy Site Clinic Sites Southern Hub (Guildford) Screening Centres (17) Colonoscopy Site Clinic Sites Clinic Sites 14.6 million






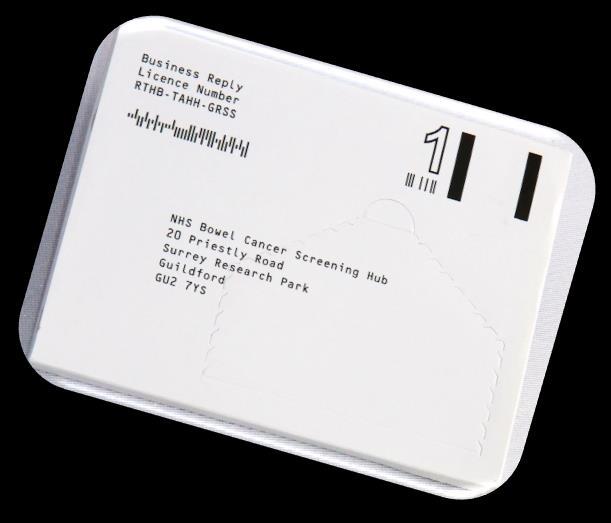
7 Screening Timeline Webbased Screening Data System Start 2 yearly Screening Cycle Day 8 Invitation Kit & Spatula Return Envelope <2 days +ve Specialist Screening Practitioner Result Clinic Screening Patient & GP Appointment Colonoscopy Letter Kit Read (1 day) <14 days <14 days Surveillance Colonoscopy Day 1 Day 29 Month 3 2 Years Pre-Invitation At Screening Due Date Kit Returned -ve Result Patient letter & GP letter /e-message Reminder Letter No Response GP Letter/ E-Comms Next Pre-Invitation Dedicated Freephone Helpline Service (



8
9 Directly age standardised incidence rate per 100,000 population 80,0 Cancer Registry Age Standardised CRC Incidence ,0 76,0 74,0 72,0 70,0 68,0 66,0 Colorectal Cancer Screening? 64,0 62,0 60, Person ASI Lower CI Upper CI

10 Have done well?





11 Why change to FIT?




12 Time for an overhaul!





13 now have the tools, to do job even better!




")
14 Training % Uptake 70% 65% 60% 55% 50% Gender Area deprivation FIT Pilot (England) Info. IT Finance







15 Training Target pop n - 50% of England 40,000 FIT invitations Complete in 6 months FIT Pilot (England) Info. IT Finance FIT Pilot FIT Pilot


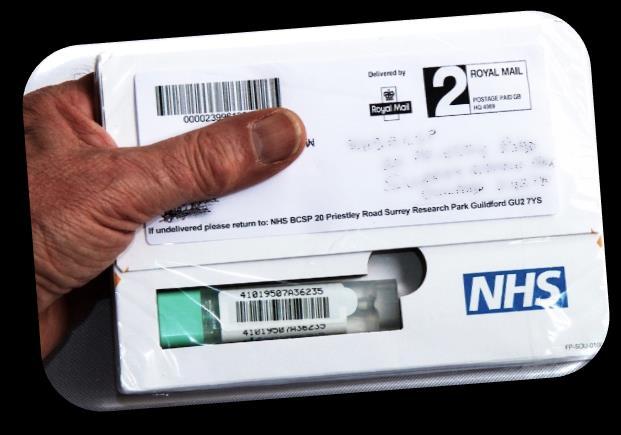

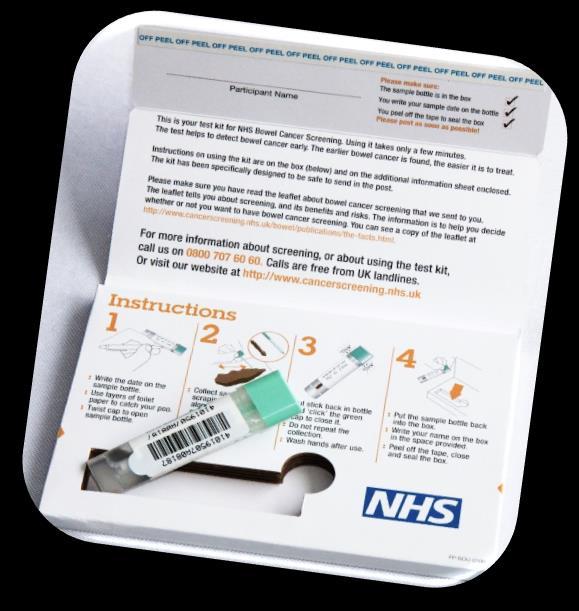

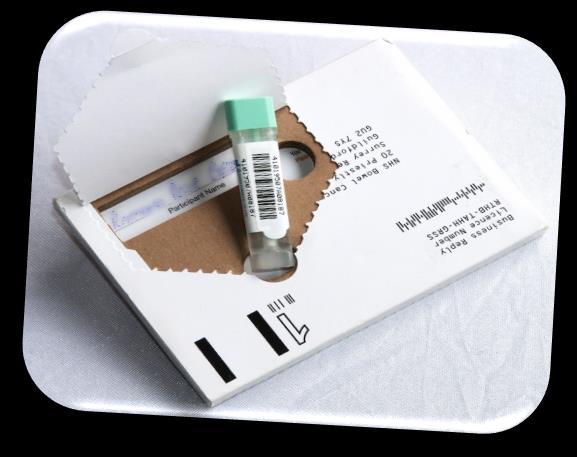


16 Make FIT Packaging Attractive Simple to use Safe for mailing Informative Reliable

 Midlands & North West Hub More Deprivation")

17 Moss S, Halloran SP et al Increased uptake and improved outcomes of bowel cancer screening with a faecal immunochemical test: results from a pilot study within the national screening programme in England Gut doi: /gutjnl FIT Pilot (England) Midlands & North West Hub More Deprivation Population 13.1 m gfobt Kits = 537,770 FIT Kits = 19,289 Both Hubs Population 27.8 m gfobt Kits = 1,126,087 FIT Kits = 40,930 Southern Hub Less Deprivation Population 14.7 m gfobt Kits = 588,317 FIT Kits = 21,641 FIT Pilot FIT Pilot





18 OC Sensor Diana analyser results ughb/g faeces FIT Pilot QA data 5 batches of 30 samples in both Hubs April October 2014 y=x Line of best fit y=0.997x R²= Diana 1 Wren SH result Diana 2 Lark SH result Diana1 Blackbird M&NWH Result Diana 2 Robin M&NWH result Mean OC Sensor Diana result ug Hb/g faeces
19 FIT in London Uptake & Deprivation 2014 South, Midlands & NW Pilot (IMD Index of Multiple Deprivation) 75% 70% gfobt FIT 65% 60% 55% 50% 45% 40% IMD 1 (Posh) IMD 2 IMD 3 IMD 4 IMD 5 (Poor)

20 Uptake & Deprivation 2014 South, Midlands & NW Pilot (IMD Index of Multiple Deprivation) 75% gfobt 70% 65% 6.7% 6.0% 6.8% FIT 60% 8.0% 55% 50% 7.9% 45% 40% IMD 1 (Posh) IMD 2 IMD 3 IMD 4 IMD 5 (Poor)


21 gfobt in London FIT in London Uptake & Deprivation 2015 London Pilot 75% 70% gfobt FIT 65% 60% 55% 8.3% 7.7% 10.0% London 50% 45% 7.4% 9.8% 40% IMD 1 (Posh) IMD 2 IMD 3 IMD 4 IMD 5 (Poor)
 Both 20,0% 20,0% 20,0% 20,0% 19,4%")
22 % of Population Deprivation Index in the Two Pilot Hubs 35% 30% 25% 20% 15% Midlands & NW Hub 10% 5% 0% Southern Hub IMD 1 (Posh) IMD 2 IMD 3 IMD 4 IMD 5 (Poor) IMD n/k Mid & NW 14,0% 17,9% 18,1% 19,9% 29,7% 0,4% Southern 25,5% 21,9% 21,7% 20,1% 9,9% 0,8% (IMD Index of Multiple Deprivation) Both 20,0% 20,0% 20,0% 20,0% 19,4% 0,6%
23 Uptake at First Invitation 2014/5 South, Midlands, NW & London Pilots Both 1 st invitation (mostly 60 year old subjects) FIT gfobt 10.9% Increase Southern 9.7% 38.6% London 52.4% 14.4% Increase Mid & NW 12.2% 40% 45% 50% 55% 60% 65%
24 Uptake in Prevalent Episodes 2014/5 South, Midlands, NW & London Pilots Both 1 5 invitations but no previous response FIT gfobt 11.6% Increase Southern Mid & NW 11.3% 11.8% London 9.7% 19.5% Uptake doubles! 0% 5% 10% 15% 20% 25% 30%
25 Uptake in Incident Episodes 2014/5 South, Midlands, NW & London Pilots Both 1 5 previous participation episodes 4.2% Increase FIT gfobt Southern 4.1% Mid & NW 4.3% 82% 84% 86% 88% 90% 92%
26 Male Female Uptake by Age and Sex 2014 South, Midlands, NW Pilot All Age All Age All invitation by age and sex 10.6% FIT gfobt 45% 50% 55% 60% 65% 70% 75%


27 Uptake & All Episodes 2014 South, Midlands, NW Pilot Both 0 5 previous screening invitations 7.1% Increase FIT gfobt Southern Mid & NW 7.3% 7.0% 290,000 Additional screens each year! 50% 55% 60% 65% 70%
28 12,0% % Positivity & Deprivation FIT Cut-off - 20 ug Hb/g Faeces 10,0% 8,0% 6,0% 4,0% 2,0% 0,0% IMD 1 (Posh) IMD 2 IMD 3 IMD 4 IMD 5 (Poor)


29 My age? You mean now or when we first sat down?
30 Faecal Immunochemical Test (FIT) & Positivity Thresholds adopted by National Bowel Cancer Screening Programmes (1 st October 2016) England (April 2018) Scotland (Dec. 2017) Netherlands Southern Ireland New Zealand Canada (Quebec) France Portugal Norway (pilot) Denmark Hungary Iceland (planned) Italy (North <20) Korea Malta Singapore Slovenia Spain (Catalonia)<20 Taiwan Uraguay England (pilot) Australia Lithuania (pilot) Latvia (pilot) Belgium (Flanders) Switzerland (no t Netherlands (pilot) New Zealand (pilot) Israel Austria Sweden (pilot) Predicted FIT positivity - % of participants referred for colonoscopy 12% 7.8% 5.2% 2.9% 2.1% 1.7% 1.5% Colonoscopy Capacity Problems Threshold used in the FIT pilot in England? Faecal Immunochemical Test (FIT) threshold (ug haemoglobin /g faeces)
31 Faecal Immunochemical Test (FIT) & Positivity Thresholds adopted by National Bowel Cancer Screening Programmes (1 st October 2016) England (April 2018) Scotland (Dec. 2017) Netherlands Southern Ireland New Zealand Canada (Quebec) France Portugal Norway (pilot) Denmark Hungary Iceland (planned) Italy (North <20) Korea Malta Singapore Slovenia Spain (Catalonia)<20 Taiwan Uraguay England (pilot) Australia Lithuania (pilot) Latvia (pilot) Belgium (Flanders) Switzerland (no t Netherlands (pilot) New Zealand (pilot) Israel Austria Sweden (pilot) No. of cancers missed relative to those detected using a 20ug/g threshold ,900 2,900 3,500 3,600 Colonoscopy Capacity Problems Data from 2014/5 FIT Screening Pilot in England Based on Pilot uptake and extrapolated to 2.6 million completed FIT p.a.? Faecal Immunochemical Test (FIT) threshold (ug haemoglobin /g faeces)
32 FIT & Missed Advanced Adenomas Thresholds adopted by National Bowel Cancer Screening Programmes (1 st October 2016) England (April 2018) Scotland (Dec. 2017) Netherlands Southern Ireland New Zealand Canada (Quebec) France Portugal Norway (pilot) Denmark Hungary Iceland (planned) Italy (North <20) Korea Malta Singapore Slovenia Spain (Catalonia)<20 Taiwan Uraguay England (pilot) Australia Lithuania (pilot) Latvia (pilot) Belgium (Flanders) Switzerland (no t Netherlands (pilot) New Zealand (pilot) Israel Austria Sweden (pilot) No. of missed advanced adenomas relative to those detected using a 20ug/g threshold ,000 25,000 30,000 34,000 35,000 Data from 2014/5 FIT Screening Pilot in England Based on Pilot uptake and extrapolated to 2.6 million completed FIT p.a Faecal Immunochemical Test (FIT) threshold (ug haemoglobin /g faeces)



33 gfobt FIT 180 FIT 150 FIT 100 FIT 40 FIT 20 Normal 17.5% 4.0% 8.3% Colonoscopy Cancer 10.1% 14.0% High-risk Adenoma Intermediate-risk Adenoma Abnormal 30.6% 19.5% Low-risk Adenoma

34 Colonoscopy gfobt Normal Cancer FIT % 10.6% High-risk Adenoma Polypectomy rate increase to >64% 16.5% 23.9% more polyps in each category Intermediate-risk Adenoma Abnormal 18.6% 18.3% Low-risk Adenoma
35 Proportion of CR cancers diagnosed in women 70% Proportion of colorectal cancers that occur in Women (C18-C ) Source: cruk.org/cancerstats 60% 50% 40% 60:40 split Men:Women 30% 20% 10% 0% Age Range (years)
36 Male Female All Registered Colorectal Cancers - % by gender July 2006 December 2014 Screen -ve - 2y interval cancer Screen +ve cancer Screen +ve Screen +ve 0,0% 10,0% 20,0% 30,0% 40,0% 50,0% 60,0% 70,0%
37 Male Female All Registered Colorectal Cancers - % by gender July 2006 December 2014 Screen -ve - 2y interval cancer Screen +ve cancer Screen +ve 33,7% Screen +ve 66,3% 0,0% 10,0% 20,0% 30,0% 40,0% 50,0% 60,0% 70,0%



38 Male Female All Registered Colorectal Cancers - % by gender July 2006 December 2014 Screen -ve - 2y interval cancer Screen +ve cancer Screen -ve 45,2% Screen +ve 33,7% Screen -ve 54,8% Screen +ve 66,3% 0,0% 10,0% 20,0% 30,0% 40,0% 50,0% 60,0% 70,0%
39 Cancers detected /5,000 male & 5,000 female participants (completed FIT) % Cancers Detection in 10,000 FIT Screened Participants (50:50 male & female) 2014 Pilot Data Expected Male Cancers detected in men Expected Female Cancers detected in women Expect 60% of cancers to be in men 10 40% 5 0 Expect 40% of cancers to be in women 20μg 40μg 60μg 80μg 100μg 120μg 140μg 150μg 180μg 200μg gfobt FIT Concentration ug/g
40 Cancers detected /5,000 male & 5,000 female participants (completed FIT) % Cancers Detection in 10,000 FIT Screened Participants (50:50 male & female) 2014 Pilot Data Expected Male Cancers detected in men Expected Female Cancers detected in women Expect 60% of cancers to be in men 10 40% 5 0 Expect 40% of cancers to be in women 20μg 40μg 60μg 80μg 100μg 120μg 140μg 150μg 180μg 200μg gfobt FIT Concentration ug/g
41 Cancers detected /5,000 male & 5,000 female participants (completed FIT) 25 Cancers Detection in 10,000 FIT Screened Participants (50:50 male & female) 2014 Pilot Data Cancers detected in men 20 Cancers detected in women μg 40μg 60μg 80μg 100μg 120μg 140μg 150μg 180μg 200μg gfobt FIT Concentration ug/g
42 Cancers detected /5,000 male & 5,000 female participants (completed FIT) 25 Cancers Detection in 10,000 FIT Screened Participants (50:50 male & female) 2014 Pilot Data Cancers detected in men 20 Cancers detected in women % Men (60%) 10 cancers/ 5,000 participants μg 40μg 60μg 80μg 100μg 120μg 140μg 150μg 180μg 200μg gfobt FIT Concentration ug/g
43 Cancers detected /5,000 male & 5,000 female participants (completed FIT) 25 Cancers Detection in 10,000 FIT Screened Participants (50:50 male & female) 2014 Pilot Data Cancers detected in men 20 Cancers detected in women % Men (60%) 10 cancers/ 5,000 participants 5 40% 0 20μg 40μg 60μg 80μg 100μg 120μg 140μg 150μg 180μg 200μg gfobt FIT Concentration ug/g Women (40%) 6.7 cancers/ 5,000 participants
44 Cancers detected /5,000 male & 5,000 female participants (completed FIT) 25 Cancers Detection in 10,000 FIT Screened Participants (50:50 male & female) 2014 Pilot Data Cancers detected in men 20 Cancers detected in women % 40% Men FIT Threshold 180ug/g Positivity = 2.0% PPV = 12.6% 0 Women FIT Threshold 60ug/g Positivity = 2.8% PPV = 5.1% 20μg 40μg 60μg 80μg 100μg 120μg 140μg 150μg 180μg 200μg gfobt FIT Concentration ug/g
 No")
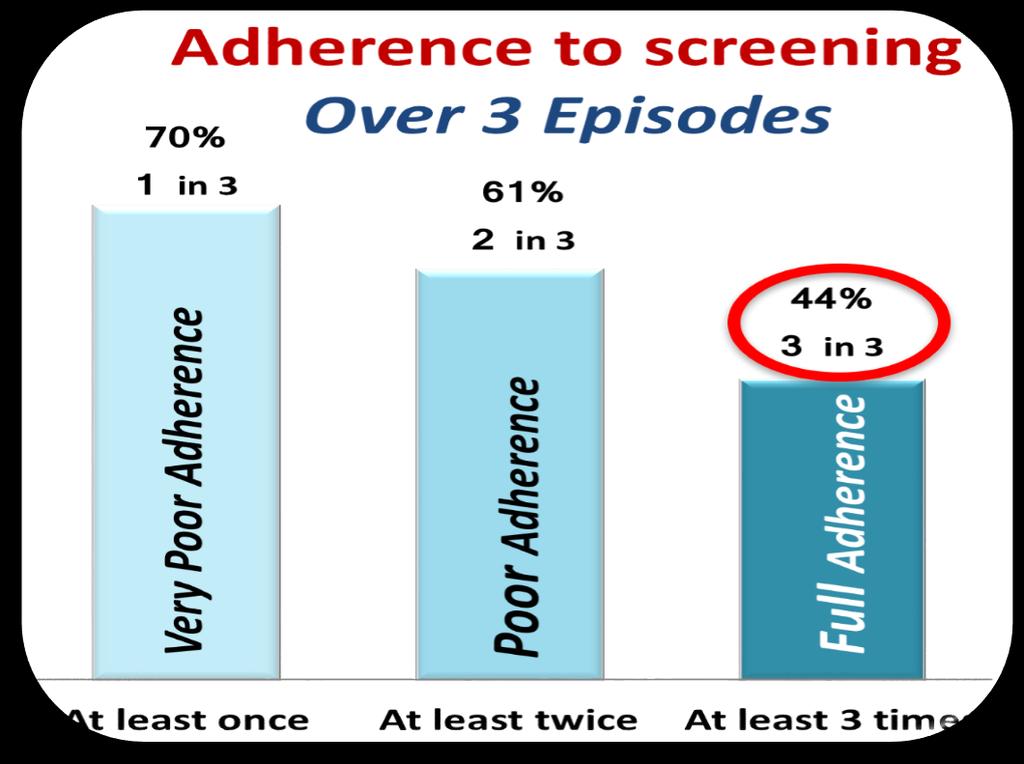
45 FIRST PREVALENT INCIDENT FIRST PREVALENT INCIDENT FIRST PREVALENT INCIDENT FIRST PREVALENT INCIDENT FIRST PREVALENT INCIDENT FIRST PREVALENT INCIDENT FIRST PREVALENT INCIDENT FIRST PREVALENT INCIDENT FIRST PREVALENT INCIDENT FIRST PREVALENT INCIDENT FIRST PREVALENT INCIDENT % Cancer Detection Rate Screen Episode & FIT threshold Cancer Detection Rate 0,6% First Invitation (60 year olds) No response to previous invitations Participated previously 0,5% 0,4% 0,3% 0,2% 0,1% 0,0% FIT gfobt gfobt
46 FIRST PREVALENT INCIDENT FIRST PREVALENT INCIDENT FIRST PREVALENT INCIDENT FIRST PREVALENT INCIDENT FIRST PREVALENT INCIDENT FIRST PREVALENT INCIDENT FIRST PREVALENT INCIDENT FIRST PREVALENT INCIDENT FIRST PREVALENT INCIDENT FIRST PREVALENT INCIDENT FIRST PREVALENT INCIDENT % Cancer Detection Rate Screen Episode & FIT threshold Cancer Detection Rate 0,6% First Invitation (60 year olds) No response to previous invitations Participated previously 0,5% 0,4% x5.1 0,3% 0,2% x2.5 0,1% x1 0,0% FIT gfobt 140 gfobt

47 Cancer Detection Rate 0,45% Age & FIT Threshold Cancer Detection Rate 0,40% 0,35% ,30% 0,25% 0,20% 0,15% 0,10% 0,05% 0,00% FIT 20 FIT 100 FIT 150 FIT180 gfobt Age Group







48 The Future of Quantitative FIT Multivariate Risk Scores Quantitative FIT concentration Age & Sex Multivariate Bowel Cancer Risk Score Better Screening! PPV Cost Effectiveness Colonoscopy Referrals Screening history Indices of Deprivation Postcode Medical History IBD, Crohns, DM, etc Family History 1 st and 2 nd deg. relatives Life style Smoking, exercise, diet, obesity


49 Developed a Multivariable Risk Prediction Model Logistic linear regression Artificial neural networks Machine learning So far neural networks in the lead. Marked increase in detection of advanced adenomas Better Screening! PPV Cost Effectiveness Colonoscopy Referrals Collaborators Jennifer Cooper, Nick Parsons, Sian Taylor-Phillips






50 FIT An opportunity to personalise population-based screening? Better Screening by - focusing on individuals...as well as on populations? Personalising population-based screening 1. Intelligent use of FIT data 2. Incorporate personal risk 3. Personalised invitation 4. Personalised interpretation of the FIT Screen
51
52



53 FIT 4 Me Screening Systems
54
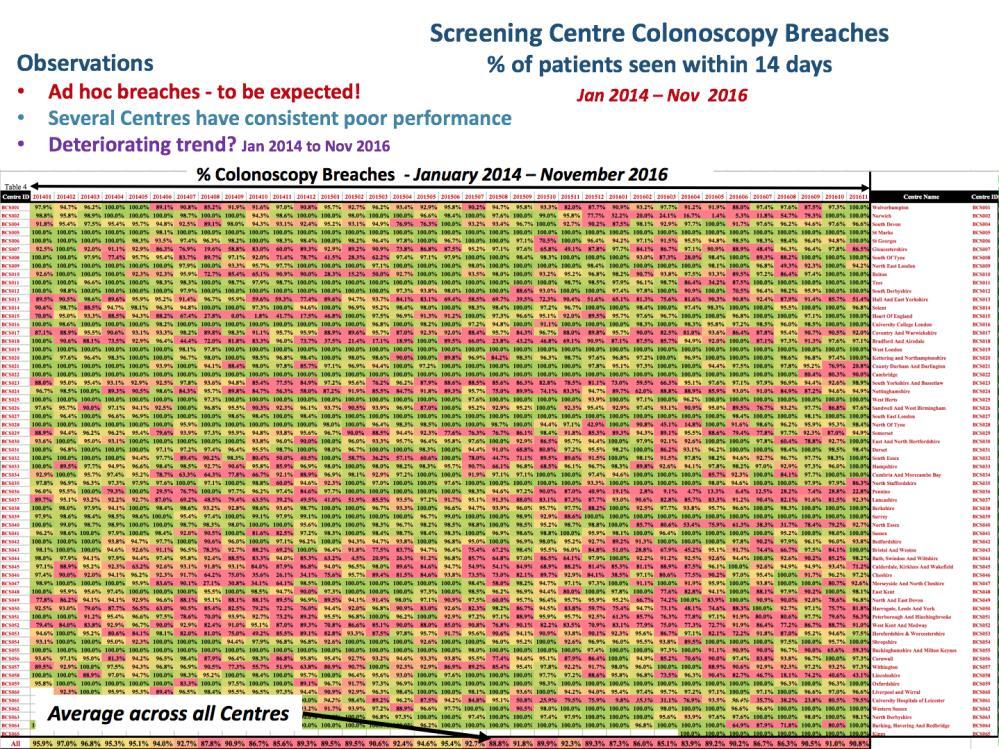
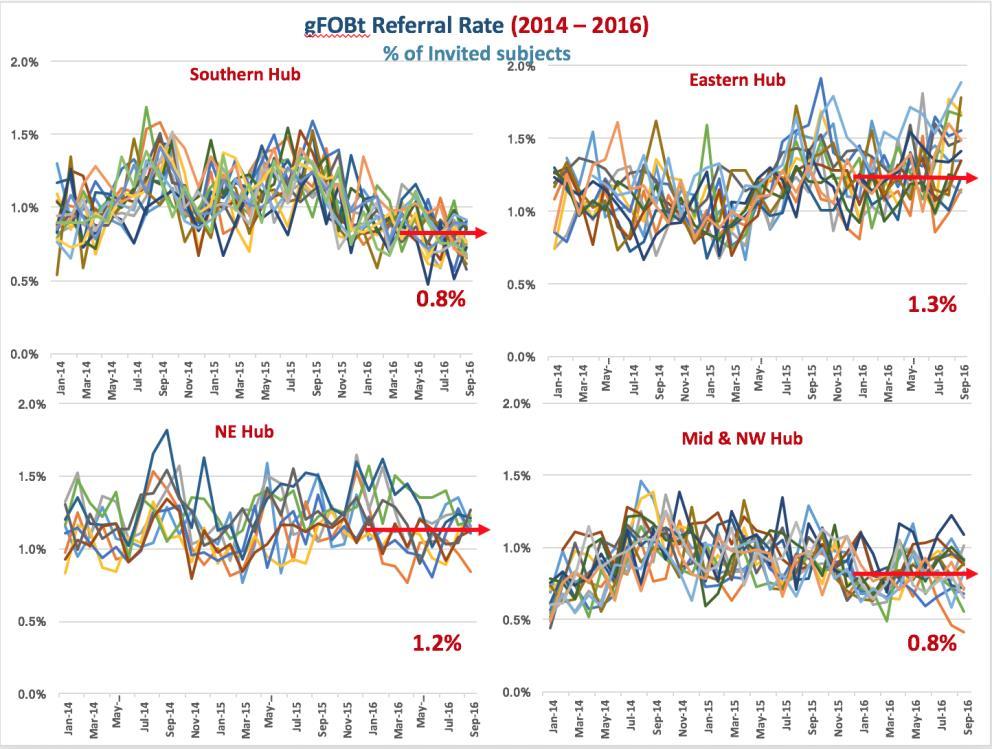
 Variation between areas - Hubs and Screening")

55 Plan for sophisticated, multi-variate, FIT-based risk score Start with a simple, single FIT threshold 1. Understand impact of FIT on Volume & Complexity of colonoscopy /pathology 2. Review current colonoscopy resource Current volume current colonoscopy volume Current performance - 2 week breaches, bowel scope rollout etc) Variation between areas - Hubs and Screening Centres 3. Estimates for 2018/9?Eligible population,?fit uptake What would have been the gfobt uptake, positivity and referral rates FIT positivity and referral rates at different thresholds 4. Agree a single FIT threshold - based on OC-Sensor 5. Advise Commissioners, Centres and CEOs of likely impact of FIT in 2018/8 6. Check performance of procured FIT test against that used in the pilot.
56 Tuesday, September 26, :30 11:30 Chairs: O. Májek, S. Halloran 9:30 9:50 Faecal testing in colorectal cancer screening: state of art S. Halloran 9:50 10:00 Czech National Coordination Centre for Prevention of Serious Diseases: platform for systematic introduction of innovations to early disease detection O. Májek 10:00 10:20 Implementation of population-based faecal occult blood testing and transition to immunochemical tests: experience from England S. Halloran 10:20 10:35 Role of general practitioners in population-based colorectal cancer screening: current situation and future prospects B. Seifert 10:35 10:50 Quantitative immunochemical tests: evidence on accuracy and implementation considerations in the Czech Republic P. Kocna 10:50 11:05 Quality-assured immunochemical testing proposal for a pilot project in the Czech Republic O. Májek, Š. Suchánek 11:05 11:30 Structured discussion & wrap-up 26th Tuesday 12:00 - press conference - Thierry Ponchon could give insight into goals of UEG. SPH programme in England and how important is to have a good governance, quality assurance and political support Session title: Why do we have different levels of participation in Europe? Influence of the population type. How to tackle inequalities. Date: Wednesday, September 27 Time: 14:20 15:50

57 20% Polyp/Adenoma 18% % 2% 2% 6% 7% 9% 8% 8% England Screening Outcomes Episode /12 0% 0% 1% 17% 1 st Episode (Prevalent) 10% 17% 13% 11% Cancer detected High-risk adenoma Intermediate-risk adenoma Low-risk adenoma Abnormal finding Abnormal, no histology Normal result 28% No result 27% 31% 16% 21% 26% British Society of Gastroenterologists - Guidelines High Risk: - >=5 adenomas / > 2 cm adenoma Intermediate Risk: 3/4 small adenomas / >= 1 cm adenoma Low Risk: 1-2 <1 cm adenomas

58 20% 18% 2% 2% 2% 6% 7% 9% 8% 8% England Screening Outcomes Episode 1, /12 0% 0% 1% 17% 1 st Episode (Prevalent) 2 nd Episode (Incident) 10% 17% 13% 11% Cancer detected High-risk adenoma Intermediate-risk adenoma Low-risk adenoma Abnormal finding Abnormal, no histology Normal result 28% No result 27% 31% 16% 21% 26%

 2 nd Episode")


59 20% 18% 2% 2% 2% 6% 7% 9% 8% 8% England Screening Outcomes Episode 1, 2 & /12 17% 10% 11% Cancer detected High-risk adenoma 0% 0% 1% 1 st Episode (Prevalent) 2 nd Episode (Incident) 17% 13% Intermediate-risk adenoma Low-risk adenoma Abnormal finding Abnormal, no histology 3 rd Episode (Incident) 28% Normal result No result 27% 31% 16% 21% 26% Polypectomy Rate 48%

60 Web-based Screening System Uptake and Demographics - Sept 2013 Response No Response Sept 2013
61 Positivity FIT Threshold and Positivity 2014 South, Midlands & NW Pilot 9,0% 8,0% 7.9% 7,0% 6,0% 5,0% 4,0% 3,0% 2,0% 1,0% 0,0% gfobt FIT 20 FIT 40 FIT 100 FIT 150 FIT 180 ug Haemoglobin / g Faeces

62 Positivity FIT Threshold and Positivity 2014 South, Midlands & NW Pilot 9,0% 8,0% 7.9% 7,0% 6,0% 5,0% 4,0% 3,0% 2,0% 1,0% 1.7% 1.56% 0,0% gfobt FIT 20 FIT 40 FIT 100 FIT 150 FIT 180 ug Haemoglobin / g Faeces
Prof Stephen P. Halloran. Update on the NHS Bowel Cancer Screening Programme Focus on BS & FIT
 Prof Stephen P. Halloran Update on the NHS Bowel Cancer Screening Programme Focus on BS & FIT World Top 20 Cancers Men Incidence & Mortality (2012) Women World Colorectal Cancer 3 rd commonest cancer 4
Prof Stephen P. Halloran Update on the NHS Bowel Cancer Screening Programme Focus on BS & FIT World Top 20 Cancers Men Incidence & Mortality (2012) Women World Colorectal Cancer 3 rd commonest cancer 4
Colorectal cancer screening in England
 Colorectal cancer screening in England critical analysis Prof Stephen P. Halloran Participation Rate 57% All Screens (1.9% +ve) 52% Prevalent 1 st Screen (age 60 years) 36% Prevalent Screen (2.2% +ve)
Colorectal cancer screening in England critical analysis Prof Stephen P. Halloran Participation Rate 57% All Screens (1.9% +ve) 52% Prevalent 1 st Screen (age 60 years) 36% Prevalent Screen (2.2% +ve)
An Update on the Bowel Cancer Screening Programme. Natasha Djedovic, London Hub Director 17 th September 2018
 An Update on the Bowel Cancer Screening Programme Natasha Djedovic, London Hub Director 17 th September 2018 NHS Bowel Cancer Screening Programme 2006: 60-69 yr old men & women offered guaiac Faecal Occult
An Update on the Bowel Cancer Screening Programme Natasha Djedovic, London Hub Director 17 th September 2018 NHS Bowel Cancer Screening Programme 2006: 60-69 yr old men & women offered guaiac Faecal Occult
Bowel Cancer Screening Exploiting science brings better medicine
 Camberley & District Bowel Cancer Screening Exploiting science brings better medicine Prof Stephen P. Halloran World - All Cancers Men Incidence & Mortality (2012) Women Incidence Mortality GLOBOCAN 2012
Camberley & District Bowel Cancer Screening Exploiting science brings better medicine Prof Stephen P. Halloran World - All Cancers Men Incidence & Mortality (2012) Women Incidence Mortality GLOBOCAN 2012
Challenges for Colorectal Cancer Screening
 Challenges for Colorectal Cancer Screening a Biomarker with No Standards! Prof. Emeritus Stephen P. Halloran University of Surrey W. Europe Top 20 Cancers Men Incidence & Mortality (2012) Women World -
Challenges for Colorectal Cancer Screening a Biomarker with No Standards! Prof. Emeritus Stephen P. Halloran University of Surrey W. Europe Top 20 Cancers Men Incidence & Mortality (2012) Women World -
Faecal testing in colorectal cancer screening: State of the Art. Prof Stephen P. Halloran
 Faecal testing in colorectal cancer screening: State of the Art Prof Stephen P. Halloran Faecal Immunochemical Test (FIT) gfobt Globin (Human) Haem Guaiac test gfobt Study Cohort 10,011 L Hol et al Gut
Faecal testing in colorectal cancer screening: State of the Art Prof Stephen P. Halloran Faecal Immunochemical Test (FIT) gfobt Globin (Human) Haem Guaiac test gfobt Study Cohort 10,011 L Hol et al Gut
NHS Bowel Cancer Screening Programmes: Evaluation of pilot of Faecal Immunochemical Test : Final report.
 NHS Bowel Cancer Screening Programmes: Evaluation of pilot of Faecal Immunochemical Test : Final report. Sue Moss, Christopher Mathews Centre for Cancer Prevention, Wolfson Institute, Queen Mary University
NHS Bowel Cancer Screening Programmes: Evaluation of pilot of Faecal Immunochemical Test : Final report. Sue Moss, Christopher Mathews Centre for Cancer Prevention, Wolfson Institute, Queen Mary University
Programme September 2017 Prague, Czech Republic
 Programme 25 27 September 2017 Prague, Czech Republic Programme committee chairs Ladislav Dušek (Czech Republic) Director of the Institute of Health Information And Statistics of the Czech Republic Monday,
Programme 25 27 September 2017 Prague, Czech Republic Programme committee chairs Ladislav Dušek (Czech Republic) Director of the Institute of Health Information And Statistics of the Czech Republic Monday,
Why FIT (Faecal Immunochemical Test) is the best biomarker for CRC screening
 is the best biomarker for CRC screening") Why FIT (Faecal Immunochemical Test) is the best biomarker for CRC screening Prof. Stephen Halloran Royal Surrey County Hospital NHS Cancer Screening Programme University of Surrey gfobt Guaiacum Officinale
Why FIT (Faecal Immunochemical Test) is the best biomarker for CRC screening Prof. Stephen Halloran Royal Surrey County Hospital NHS Cancer Screening Programme University of Surrey gfobt Guaiacum Officinale
Colorectal cancer. New Zealand s place in the world. Inequities in outcomes? Assoc Prof Diana Sarfati
 Colorectal cancer New Zealand s place in the world. Inequities in outcomes? Assoc Prof Diana Sarfati Today s talk Mortality Internationally In New Zealand Incidence Trends in New Zealand Primary prevention
Colorectal cancer New Zealand s place in the world. Inequities in outcomes? Assoc Prof Diana Sarfati Today s talk Mortality Internationally In New Zealand Incidence Trends in New Zealand Primary prevention
Friday, 17 October 2014: 08:30 11:30 * * * * *
 Vienna 2014 6 th Meeting of the Expert Working Group (EWG) FIT for Screening Expert Working Group (EWG) founding members: Friday, 17 October 2014: 08:30 11:30 MEETING REPORT * * * * * Jim Allison, University
Vienna 2014 6 th Meeting of the Expert Working Group (EWG) FIT for Screening Expert Working Group (EWG) founding members: Friday, 17 October 2014: 08:30 11:30 MEETING REPORT * * * * * Jim Allison, University
SCREENING FOR BOWEL CANCER USING FLEXIBLE SIGMOIDOSCOPY REVIEW APPRAISAL CRITERIA FOR THE UK NATIONAL SCREENING COMMITTEE
 SCREENING FOR BOWEL CANCER USING FLEXIBLE SIGMOIDOSCOPY REVIEW APPRAISAL CRITERIA FOR THE UK NATIONAL SCREENING COMMITTEE The Condition 1. The condition should be an important health problem Colorectal
SCREENING FOR BOWEL CANCER USING FLEXIBLE SIGMOIDOSCOPY REVIEW APPRAISAL CRITERIA FOR THE UK NATIONAL SCREENING COMMITTEE The Condition 1. The condition should be an important health problem Colorectal
Faecal Immunochemical Testing (FIT) for Screening and Symptomatic Patients
 for Screening and Symptomatic Patients") Faecal Immunochemical Testing (FIT) for Screening and Symptomatic Patients Caroline Addison NE BCSP Hub Director and Consultant Clinical Scientist What is FIT Type of Faecal Occult Blood test Designed
Faecal Immunochemical Testing (FIT) for Screening and Symptomatic Patients Caroline Addison NE BCSP Hub Director and Consultant Clinical Scientist What is FIT Type of Faecal Occult Blood test Designed
31 countries (117 registries, 20 national) Increased coverage in countries with regional registries 50% European population Overall >20 million
 Increased coverage in countries with regional registries 50% European population Overall >20 million") 31 countries (117 registries, 20 national) Increased coverage in countries with regional registries 50% European population Overall >20 million cancer cases Adult patients (age 15+) 45 major cancer sites
31 countries (117 registries, 20 national) Increased coverage in countries with regional registries 50% European population Overall >20 million cancer cases Adult patients (age 15+) 45 major cancer sites
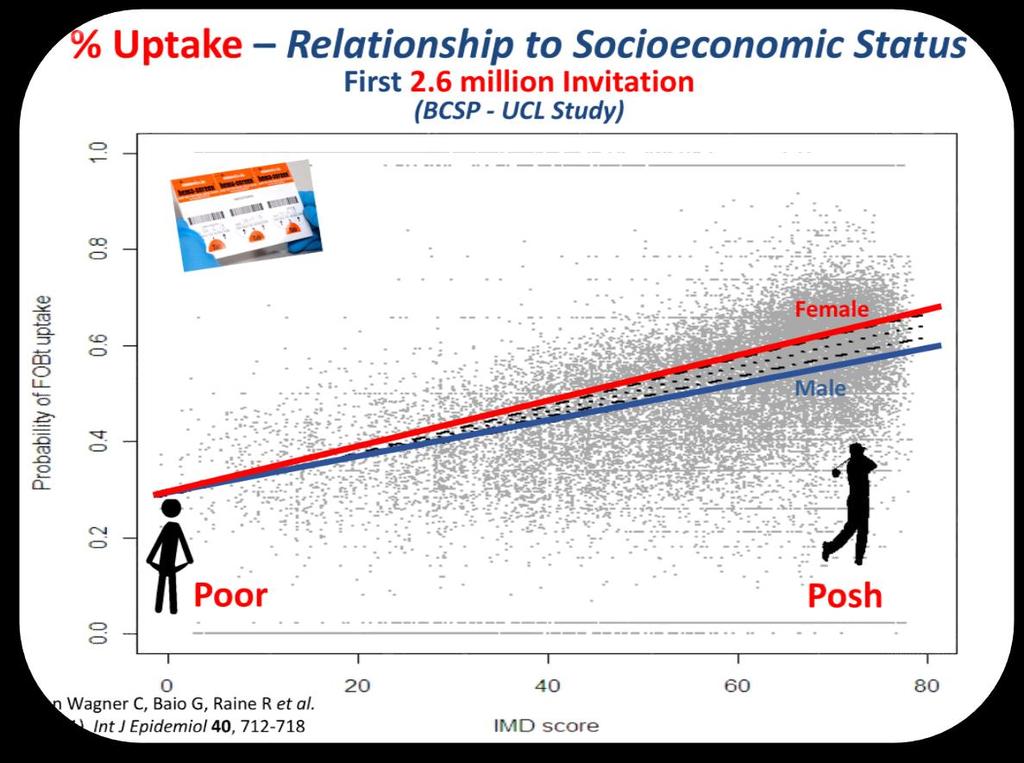
Results from 2.6 million invitations between : 54% overall uptake (von Wagner et al., 2011)
") TRICCS: Text-message Reminders in Colorectal Cancer Screening Research Department of Behavioural Science and Health University College London Christian von Wagner (c.wagner@ucl.ac.uk ) Background Colorectal
TRICCS: Text-message Reminders in Colorectal Cancer Screening Research Department of Behavioural Science and Health University College London Christian von Wagner (c.wagner@ucl.ac.uk ) Background Colorectal
Quantitative immunochemical tests: evidence on accuracy and implementation considerations in the Czech MUDr.. Petr Kocna, CSc.
 Quantitative immunochemical tests: evidence on accuracy and implementation considerations in the Czech MUDr.. Petr Kocna, CSc. European Digestive Cancer Days, Prague - 26. September 2017 QUANTITATIVE FIT
Quantitative immunochemical tests: evidence on accuracy and implementation considerations in the Czech MUDr.. Petr Kocna, CSc. European Digestive Cancer Days, Prague - 26. September 2017 QUANTITATIVE FIT
The Dutch bowel cancer screening program Relevant lessions for Ontario
 The Dutch bowel cancer screening program Relevant lessions for Ontario Ernst J Kuipers Erasmus MC University Medical Center Rotterdam - The Netherlands 1 Ismar Boas (1858 1938) Colorectal cancer screening
The Dutch bowel cancer screening program Relevant lessions for Ontario Ernst J Kuipers Erasmus MC University Medical Center Rotterdam - The Netherlands 1 Ismar Boas (1858 1938) Colorectal cancer screening
COMMISSION OF THE EUROPEAN COMMUNITIES
 COMMISSION OF THE EUROPEAN COMMUNITIES Brussels, 22.12.2008 COM(2008) 882 final REPORT FROM THE COMMISSION TO THE COUNCIL, THE EUROPEAN PARLIAMENT, THE EUROPEAN ECONOMIC AND SOCIAL COMMITTEE AND THE COMMITTEE
COMMISSION OF THE EUROPEAN COMMUNITIES Brussels, 22.12.2008 COM(2008) 882 final REPORT FROM THE COMMISSION TO THE COUNCIL, THE EUROPEAN PARLIAMENT, THE EUROPEAN ECONOMIC AND SOCIAL COMMITTEE AND THE COMMITTEE
Performance of Colorectal cancer screening in the European Union Member States Data from the second European screening report
 Performance of Colorectal cancer screening in the European Union Member States Data from the second European screening report 1 Basu P 2, Anttila A 3, Ponti A 1, Tomatis M 1, Vale DB 4, Ronco G 1, Soerjomataram
Performance of Colorectal cancer screening in the European Union Member States Data from the second European screening report 1 Basu P 2, Anttila A 3, Ponti A 1, Tomatis M 1, Vale DB 4, Ronco G 1, Soerjomataram
Reflections on the EUnetHTA CRC screening full Core Model pilot 1
 Reflections on the EUnetHTA CRC screening full Core Model pilot 1 EUnetHTA Medical Technology HTA expert meeting Brussels October 16th 2015 Karsten Berndt, Economist & Epidemiologist, EDMA HTA Task Force
Reflections on the EUnetHTA CRC screening full Core Model pilot 1 EUnetHTA Medical Technology HTA expert meeting Brussels October 16th 2015 Karsten Berndt, Economist & Epidemiologist, EDMA HTA Task Force
Annual Report. Public Health Screening Programmes TO 31 MARCH Extract: Chapter 3 : Planning for Bowel Screening Programme
 Public Health Screening Programmes Annual Report TO 31 MARCH 2007 Extract: Chapter 3 : Planning for Bowel Screening Programme Version 1.0 Published: 18 December 2007 1 Contents INTRODUCTION...3 SUMMARY...5
Public Health Screening Programmes Annual Report TO 31 MARCH 2007 Extract: Chapter 3 : Planning for Bowel Screening Programme Version 1.0 Published: 18 December 2007 1 Contents INTRODUCTION...3 SUMMARY...5
Engaging Primary Care in bowel screening
 Engaging Primary Care in bowel screening GP good practice guide for Wales December 2018 Together we will beat cancer Contents Background 3 The FIT screening pathway in Wales 4 The role of GP practices
Engaging Primary Care in bowel screening GP good practice guide for Wales December 2018 Together we will beat cancer Contents Background 3 The FIT screening pathway in Wales 4 The role of GP practices
European Partnership for Screening
 European Partnership for Screening Lawrence von Karsa Quality Assurance Group European Cancer Network for Screening and Prevention International Agency for Research on Cancer Lyon, France Work Package
European Partnership for Screening Lawrence von Karsa Quality Assurance Group European Cancer Network for Screening and Prevention International Agency for Research on Cancer Lyon, France Work Package
Risk scoring incorporating FIT in triage of symptomatic patients
 Risk scoring incorporating FIT in triage of symptomatic patients Centre for Research into Cancer Prevention and Screening University of Dundee Scotland Possible conflicts of interest None Background Symptoms
Risk scoring incorporating FIT in triage of symptomatic patients Centre for Research into Cancer Prevention and Screening University of Dundee Scotland Possible conflicts of interest None Background Symptoms
UK bowel cancer care outcomes: A comparison with Europe
 UK bowel cancer care outcomes: A comparison with Europe What is bowel cancer? Bowel cancer, which is also known as colorectal or colon cancer, is a cancer that affects either the colon or the rectum. The
UK bowel cancer care outcomes: A comparison with Europe What is bowel cancer? Bowel cancer, which is also known as colorectal or colon cancer, is a cancer that affects either the colon or the rectum. The
North West London Pathology. Faecal Occult Blood testing. Mrs Sophie Barnes FRCPath Consultant Clinical Scientist
 Faecal Occult Blood testing Mrs Sophie Barnes FRCPath Consultant Clinical Scientist Learning objectives Background Guidelines for colorectal cancer detection Tests available to detect occult blood in faeces
Faecal Occult Blood testing Mrs Sophie Barnes FRCPath Consultant Clinical Scientist Learning objectives Background Guidelines for colorectal cancer detection Tests available to detect occult blood in faeces
Screening for GI Cancer Past Present and Future. Prof. Bob Steele University of Dundee
 Screening for GI Cancer Past Present and Future Prof. Bob Steele University of Dundee Worldwide Cancer Incidence Rates UK Cancer Incidence Rates Screening The detection of disease in asymptomatic subjects
Screening for GI Cancer Past Present and Future Prof. Bob Steele University of Dundee Worldwide Cancer Incidence Rates UK Cancer Incidence Rates Screening The detection of disease in asymptomatic subjects
ENGAGING PRIMARY CARE IN BOWEL SCREENING
 ENGAGING PRIMARY CARE IN BOWEL SCREENING GP GOOD PRACTICE GUIDE SCOTLAND VERSION ENGAGING PRIMARY CARE IN BOWEL SCREENING GP GOOD PRACTICE GUIDE SCOTLAND VERSION CONTENT 2 Background & information on the
ENGAGING PRIMARY CARE IN BOWEL SCREENING GP GOOD PRACTICE GUIDE SCOTLAND VERSION ENGAGING PRIMARY CARE IN BOWEL SCREENING GP GOOD PRACTICE GUIDE SCOTLAND VERSION CONTENT 2 Background & information on the
WCPT COUNTRY PROFILE December 2017 HUNGARY
 WCPT COUNTRY PROFILE December 2017 HUNGARY HUNGARY NUMBERS WCPT Members Practising physical therapists 727 Total number of physical therapist members in your member organisation 4,000 Total number of practising
WCPT COUNTRY PROFILE December 2017 HUNGARY HUNGARY NUMBERS WCPT Members Practising physical therapists 727 Total number of physical therapist members in your member organisation 4,000 Total number of practising
WCPT COUNTRY PROFILE December 2017 SWEDEN
 WCPT COUNTRY PROFILE December 2017 SWEDEN SWEDEN NUMBERS WCPT Members Practising physical therapists 11,043 Total number of physical therapist members in your member organisation 17,906 Total number of
WCPT COUNTRY PROFILE December 2017 SWEDEN SWEDEN NUMBERS WCPT Members Practising physical therapists 11,043 Total number of physical therapist members in your member organisation 17,906 Total number of
Author's response to reviews
 Author's response to reviews Title: Study protocol: Evaluating the effectiveness of GP endorsement on increasing participation in the NHS Bowel Cancer Screening Programme: a feasibility trial Authors:
Author's response to reviews Title: Study protocol: Evaluating the effectiveness of GP endorsement on increasing participation in the NHS Bowel Cancer Screening Programme: a feasibility trial Authors:
Northern Ireland Bowel Cancer Screening Programme. Pathways. Version 4 1 st October 2013
 Northern Ireland Bowel Cancer Screening Programme Pathways These changes will be version controlled, led by the Quality Assurance Director for the Programme. Any updated versions will be circulated and
Northern Ireland Bowel Cancer Screening Programme Pathways These changes will be version controlled, led by the Quality Assurance Director for the Programme. Any updated versions will be circulated and
Screening for Colorectal Cancer: Se0ng it up and making it work. Julie8a Patnick 4 December 2014
 Screening for Colorectal Cancer: Se0ng it up and making it work Julie8a Patnick 4 December 2014 Evaluation of the UK Colorectal Cancer Screening Pilot Two sites, population ~ 1m Coventry & Warwickshire
Screening for Colorectal Cancer: Se0ng it up and making it work Julie8a Patnick 4 December 2014 Evaluation of the UK Colorectal Cancer Screening Pilot Two sites, population ~ 1m Coventry & Warwickshire
LEBANON. WCPT COUNTRY PROFILE December 2018
 LEBANON WCPT COUNTRY PROFILE December 2018 LEBANON NUMBERS 1600 1400 1200 1000 800 600 400 200 0 Physical therapists in the country Members in MO 1,480 1,480 Total PTs in country 800000 700000 600000 500000
LEBANON WCPT COUNTRY PROFILE December 2018 LEBANON NUMBERS 1600 1400 1200 1000 800 600 400 200 0 Physical therapists in the country Members in MO 1,480 1,480 Total PTs in country 800000 700000 600000 500000
NATIONAL SCREENING COMMITTEE
 Optimising Bowel Cancer Screening Phase 1: Optimising the cost effectiveness of repeated FIT screening and screening strategies combining bowel scope and FIT screening Sophie Whyte, Chloe Thomas, Ben Kearns,
Optimising Bowel Cancer Screening Phase 1: Optimising the cost effectiveness of repeated FIT screening and screening strategies combining bowel scope and FIT screening Sophie Whyte, Chloe Thomas, Ben Kearns,
WCPT COUNTRY PROFILE December 2017 SERBIA
 WCPT COUNTRY PROFILE December 2017 SERBIA SERBIA NUMBERS WCPT Members Practising physical therapists 622 Total number of physical therapist members in your member organisation 3,323 Total number of practising
WCPT COUNTRY PROFILE December 2017 SERBIA SERBIA NUMBERS WCPT Members Practising physical therapists 622 Total number of physical therapist members in your member organisation 3,323 Total number of practising
Friday, 23 October 2015: 10:15 12:00 * * * * *
 Barcelona 2015 8 th Meeting of the Expert Working Group (EWG) FIT for Screening Expert Working Group (EWG) founding members: Friday, 23 October 2015: 10:15 12:00 MEETING REPORT * * * * * Jim Allison, University
Barcelona 2015 8 th Meeting of the Expert Working Group (EWG) FIT for Screening Expert Working Group (EWG) founding members: Friday, 23 October 2015: 10:15 12:00 MEETING REPORT * * * * * Jim Allison, University
The health economic landscape of cancer in Europe
 1 Approval number The health economic landscape of cancer in Europe Bengt Jönsson, Professor Emeritus of Health Economics Stockholm School of Economics 2 Disclaimer This presentation was developed by Professor
1 Approval number The health economic landscape of cancer in Europe Bengt Jönsson, Professor Emeritus of Health Economics Stockholm School of Economics 2 Disclaimer This presentation was developed by Professor
Prevention of Bowel Cancer: which patients do I send for colonoscopy?
 Prevention of Bowel Cancer: which patients do I send for colonoscopy? Dr Chris Groves Consultant Gastroenterologist and Honorary Senior Lecturer St George s Hospital and Medical School Director, SW London
Prevention of Bowel Cancer: which patients do I send for colonoscopy? Dr Chris Groves Consultant Gastroenterologist and Honorary Senior Lecturer St George s Hospital and Medical School Director, SW London
Men & Health Work. Difference can make a difference Steve Boorman & Ian Banks RSPH Academy 2013
 Men & Health Promotion @ Work Difference can make a difference Steve Boorman & Ian Banks RSPH Academy 2013 Difference can make a Difference Mens health: State of mens health Use of services Role of the
Men & Health Promotion @ Work Difference can make a difference Steve Boorman & Ian Banks RSPH Academy 2013 Difference can make a Difference Mens health: State of mens health Use of services Role of the
DENMARK. WCPT COUNTRY PROFILE December 2018
 DENMARK WCPT COUNTRY PROFILE December 2018 DENMARK NUMBERS 14000 12000 10000 8000 6000 4000 2000 0 Physical therapists in the country Members in MO 11,720 12,975 Total PTs in country 800000 700000 600000
DENMARK WCPT COUNTRY PROFILE December 2018 DENMARK NUMBERS 14000 12000 10000 8000 6000 4000 2000 0 Physical therapists in the country Members in MO 11,720 12,975 Total PTs in country 800000 700000 600000
Czech CRC screening program at the point of switch to the population based design
 Military University Hospital First Medical Faculty of Charles University Department of Gastroenterology Czech CRC screening program at the point of switch to the population based design M. Zavoral, S.
Military University Hospital First Medical Faculty of Charles University Department of Gastroenterology Czech CRC screening program at the point of switch to the population based design M. Zavoral, S.
Interventions to Improve Follow-up of Positive Results on Fecal Blood Tests
 Interventions to Improve Follow-up of Positive Results on Fecal Blood Tests Results of a systematic review, Kaiser experience, and implications for the Canton of Vaud Kevin Selby, M.D. Kevin.Selby@hospvd.ch
Interventions to Improve Follow-up of Positive Results on Fecal Blood Tests Results of a systematic review, Kaiser experience, and implications for the Canton of Vaud Kevin Selby, M.D. Kevin.Selby@hospvd.ch
GERMANY. WCPT COUNTRY PROFILE December 2018
 GERMANY WCPT COUNTRY PROFILE December 2018 GERMANY NUMBERS 160000 140000 120000 100000 80000 60000 40000 20000 0 Physical therapists in the country Members in MO 21,502 136,000 Total PTs in country 800000
GERMANY WCPT COUNTRY PROFILE December 2018 GERMANY NUMBERS 160000 140000 120000 100000 80000 60000 40000 20000 0 Physical therapists in the country Members in MO 21,502 136,000 Total PTs in country 800000
Manuel Cardoso RARHA Executive Coordinator Public Health MD Senior Advisor Deputy General-Director of SICAD - Portugal
 Manuel Cardoso RARHA Executive Coordinator Public Health MD Senior Advisor Deputy General-Director of SICAD - Portugal Public Health Public health is the science and art of preventing disease, prolonging
Manuel Cardoso RARHA Executive Coordinator Public Health MD Senior Advisor Deputy General-Director of SICAD - Portugal Public Health Public health is the science and art of preventing disease, prolonging
Smokefree Policies in Europe: Are we there yet?
 Smokefree Policies in Europe: Are we there yet? 14 April 2015, 9:00 10:30am Rue de l Industrie 24, 1040 Brussels Permanent Partners: Temporary Partners: The research for the SFP Smokefree Map was partially
Smokefree Policies in Europe: Are we there yet? 14 April 2015, 9:00 10:30am Rue de l Industrie 24, 1040 Brussels Permanent Partners: Temporary Partners: The research for the SFP Smokefree Map was partially
508 the number of suicide deaths in deaths per 100,000 people was the suicide rate in Suicide deaths in 2013 by gender
 An overview of suicide statistics This document summarises information about suicide deaths in New Zealand covering up to 13. It does not attempt to explain causes of suicidal behaviour or causes of changes
An overview of suicide statistics This document summarises information about suicide deaths in New Zealand covering up to 13. It does not attempt to explain causes of suicidal behaviour or causes of changes
Dr Alasdair Patrick. Dr Nagham Al-Mozany. 9:45-10:10 Where Are We Up To With Bowel Cancer Screening?
 Dr Alasdair Patrick Gastroenterologist and General Physician Middlemore Hospital Auckland Dr Nagham Al-Mozany Colorectal Surgeon Auckland City Hospital Clinical Senior Lecturer University of Auckland 9:45-10:10
Dr Alasdair Patrick Gastroenterologist and General Physician Middlemore Hospital Auckland Dr Nagham Al-Mozany Colorectal Surgeon Auckland City Hospital Clinical Senior Lecturer University of Auckland 9:45-10:10
PROGRESS ON HCQI RESEARCH AND DEVELOPMENT WORK
 PROGRESS ON HCQI RESEARCH AND DEVELOPMENT WORK Ian Brownwood, HCQI Project, OECD HCQI Expert Group Meeting 21 and 22 may 2015 R&D Agenda for 2014 Primary Care Indicators Avoidable Hospital Admission Indicators
PROGRESS ON HCQI RESEARCH AND DEVELOPMENT WORK Ian Brownwood, HCQI Project, OECD HCQI Expert Group Meeting 21 and 22 may 2015 R&D Agenda for 2014 Primary Care Indicators Avoidable Hospital Admission Indicators
FIT for symptomatic patients. Facilitator name
 FIT for symptomatic patients Facilitator name Context colorectal cancer Colorectal cancer in the UK 41,804 new cases in 2015 15,903 deaths in 2014 Fourth most common cancer Second most common cause of
FIT for symptomatic patients Facilitator name Context colorectal cancer Colorectal cancer in the UK 41,804 new cases in 2015 15,903 deaths in 2014 Fourth most common cancer Second most common cause of
Colorectal cancer screening
 26 Colorectal cancer screening BETHAN GRAF AND JOHN MARTIN Colorectal cancer is theoretically a preventable disease and is ideally suited to a population screening programme, as there is a long premalignant
26 Colorectal cancer screening BETHAN GRAF AND JOHN MARTIN Colorectal cancer is theoretically a preventable disease and is ideally suited to a population screening programme, as there is a long premalignant
Extract from Cancer survival in Europe by country and age: results of EUROCARE-5 a population-based study
 EUROCARE-5 on-line database Data and methods Extract from Cancer survival in Europe 1999 2007 by country and age: results of EUROCARE-5 a population-based study De Angelis R, Sant M, Coleman MP, Francisci
EUROCARE-5 on-line database Data and methods Extract from Cancer survival in Europe 1999 2007 by country and age: results of EUROCARE-5 a population-based study De Angelis R, Sant M, Coleman MP, Francisci
Differences make a Difference
 Differences make a Difference The European Mens Health Forum: Overview European Mens Health: An oxymoron? Mens use of services: Self-care & navigation Good practice: Wot does work? A Storm is coming: Man
Differences make a Difference The European Mens Health Forum: Overview European Mens Health: An oxymoron? Mens use of services: Self-care & navigation Good practice: Wot does work? A Storm is coming: Man
IOSH No Time to Lose campaign: working together to tackle asbestos-related cancer #NTTLasbestos. Jonathan Hughes IOSH Vice President
 IOSH No Time to Lose campaign: working together to tackle asbestos-related cancer #NTTLasbestos Jonathan Hughes IOSH Vice President About the Institution of Occupational Safety and Health (IOSH) www.iosh.co.uk
IOSH No Time to Lose campaign: working together to tackle asbestos-related cancer #NTTLasbestos Jonathan Hughes IOSH Vice President About the Institution of Occupational Safety and Health (IOSH) www.iosh.co.uk
Global colorectal cancer screening appropriate or practical? Graeme P Young, Flinders University WCC, Melbourne
 Global colorectal cancer screening appropriate or practical? Graeme P Young, Flinders University. 2014 WCC, Melbourne Outline WHO criteria to justify screening Appropriateness: Global variation in incidence
Global colorectal cancer screening appropriate or practical? Graeme P Young, Flinders University. 2014 WCC, Melbourne Outline WHO criteria to justify screening Appropriateness: Global variation in incidence
EuropaColon Uniting citizens in the fight against colorectal cancer. Zorana Maravic Director of Group Development May, 2013
 EuropaColon Uniting citizens in the fight against colorectal cancer Zorana Maravic Director of Group Development May, 2013 Colorectal cancer in Europe today >450,000 new diagnoses every year 2nd most common
EuropaColon Uniting citizens in the fight against colorectal cancer Zorana Maravic Director of Group Development May, 2013 Colorectal cancer in Europe today >450,000 new diagnoses every year 2nd most common
The cancer burden in the European Union and the European Region: the current situation and a way forward
 The cancer burden in the European Union and the European Region: the current situation and a way forward Presented by Zsuzsanna Jakab WHO Regional Director for Europe Informal Meeting of Health Ministers
The cancer burden in the European Union and the European Region: the current situation and a way forward Presented by Zsuzsanna Jakab WHO Regional Director for Europe Informal Meeting of Health Ministers
WEO CRC SC Meeting. Barcelona, Spain October 23, 2015
 WEO CRC SC Meeting Barcelona, Spain October 23, 2015 THE HEMOGLOBIN CONCENTRATION IN A NEGATIVE RESULT AS A PREDICTOR FOR ADVANCED NEOPLASIA Isabel Portillo, Eunare Arana-Arri, Isabel Idigoras, Lorea Martínez-Indart.
WEO CRC SC Meeting Barcelona, Spain October 23, 2015 THE HEMOGLOBIN CONCENTRATION IN A NEGATIVE RESULT AS A PREDICTOR FOR ADVANCED NEOPLASIA Isabel Portillo, Eunare Arana-Arri, Isabel Idigoras, Lorea Martínez-Indart.
Bowel cancer screening and prevention
 Bowel cancer screening and prevention Cancer Incidence and Mortality Victoria 2012 Number 6000 5000 4000 3000 2000 Incidences = 29,387 Mortality = 10,780 Incidence Mortality 1000 0 Prostate Breast Bowel
Bowel cancer screening and prevention Cancer Incidence and Mortality Victoria 2012 Number 6000 5000 4000 3000 2000 Incidences = 29,387 Mortality = 10,780 Incidence Mortality 1000 0 Prostate Breast Bowel
Practical challenges in establishing and running the Czech national colorectal cancer screening programme
 Ústřední vojenská nemocnice - Vojenská fakultní nemocnice Praha 1. lékařská fakulta Univerzity Karlovy Interní klinika Practical challenges in establishing and running the Czech national colorectal cancer
Ústřední vojenská nemocnice - Vojenská fakultní nemocnice Praha 1. lékařská fakulta Univerzity Karlovy Interní klinika Practical challenges in establishing and running the Czech national colorectal cancer
D7.1 Report summarising results of survey of EU countries to identify volumes and trends in relation to the import and export of stem cells
 Disclaimer: The content of this Deliverable represents the views of the author only and is his/her sole responsibility; it cannot be considered to reflect the views of the European Commission and/or the
Disclaimer: The content of this Deliverable represents the views of the author only and is his/her sole responsibility; it cannot be considered to reflect the views of the European Commission and/or the
D7.1 Report summarising results of survey of EU countries to identify volumes and trends in relation to the import and export of stem cells
 Disclaimer: The content of this Deliverable represents the views of the author only and is his/her sole responsibility; it cannot be considered to reflect the views of the European Commission and/or the
Disclaimer: The content of this Deliverable represents the views of the author only and is his/her sole responsibility; it cannot be considered to reflect the views of the European Commission and/or the
MENTAL HEALTH CARE. OECD HCQI Expert meeting 17 th of May, Rie Fujisawa
 MENTAL HEALTH CARE OECD HCQI Expert meeting 17 th of May, 2013 Rie Fujisawa Mental health indicators Any hospital readmissions for patients with schizophrenia Same hospital readmissions for patients with
MENTAL HEALTH CARE OECD HCQI Expert meeting 17 th of May, 2013 Rie Fujisawa Mental health indicators Any hospital readmissions for patients with schizophrenia Same hospital readmissions for patients with
Primary care at the forefront of colorectal cancer screening
 Primary care at the forefront of colorectal cancer screening Presentation by Bohumil Seifert Department of General Practice, 1st Faculy of Medicine, Charles University in Prague 04/05/2012 Introduction
Primary care at the forefront of colorectal cancer screening Presentation by Bohumil Seifert Department of General Practice, 1st Faculy of Medicine, Charles University in Prague 04/05/2012 Introduction
NHS Bowel Cancer Screening Programme
 NHS Bowel Cancer Screening Programme Wolverhampton Bowel Cancer Screening Centre Annual Report April 2016 to March 2017 @RWT_NHS Introduction Bowel cancer is the fourth most common cancer in the UK after
NHS Bowel Cancer Screening Programme Wolverhampton Bowel Cancer Screening Centre Annual Report April 2016 to March 2017 @RWT_NHS Introduction Bowel cancer is the fourth most common cancer in the UK after
To: all bowel screening centre directors and programme managers. Dear colleague
 Professor Julietta Patnick CBE Director JP/LC 11 January 2013 To: all bowel screening centre directors and programme managers Fulwood House Old Fulwood Road Sheffield S10 3TH Tel: 0114 271 1060 Fax: 0114
Professor Julietta Patnick CBE Director JP/LC 11 January 2013 To: all bowel screening centre directors and programme managers Fulwood House Old Fulwood Road Sheffield S10 3TH Tel: 0114 271 1060 Fax: 0114
(Bowel) Cancer Screening an update. Mike Hulme-Moir Colorectal Surgeon CD NZ Bowel Screening Pilot
 Cancer Screening an update. Mike Hulme-Moir Colorectal Surgeon CD NZ Bowel Screening Pilot") (Bowel) Cancer Screening an update Mike Hulme-Moir Colorectal Surgeon CD NZ Bowel Screening Pilot Screening The application of tests, examinations or other procedures. to sort out apparently well persons
(Bowel) Cancer Screening an update Mike Hulme-Moir Colorectal Surgeon CD NZ Bowel Screening Pilot Screening The application of tests, examinations or other procedures. to sort out apparently well persons
THE CVD CHALLENGE IN NORTHERN IRELAND. Together we can save lives and reduce NHS pressures
 THE CVD CHALLENGE IN NORTHERN IRELAND Together we can save lives and reduce NHS pressures The challenge of CVD continues today. Around 225,000 people in Northern Ireland live with the burden of cardiovascular
THE CVD CHALLENGE IN NORTHERN IRELAND Together we can save lives and reduce NHS pressures The challenge of CVD continues today. Around 225,000 people in Northern Ireland live with the burden of cardiovascular
1 APRIL 2007 TO 31 MARCH
 Public Health Screening Programmes Annual Report 1 APRIL 2007 TO 31 MARCH 2008 Extract: Chapter 3: Planning for the Bowel Screening Programme Public Health Screening Unit Version 1.0 Published: 16 December
Public Health Screening Programmes Annual Report 1 APRIL 2007 TO 31 MARCH 2008 Extract: Chapter 3: Planning for the Bowel Screening Programme Public Health Screening Unit Version 1.0 Published: 16 December
Allied Health: Sustainable Integrated Health Care for all Australians
 Allied Health: Sustainable Integrated Health Care for all Australians Catherine Turnbull Chief Allied and Scientific Health Advisor SA Health Presentation to Indigenous Allied Health Australia Conference,
Allied Health: Sustainable Integrated Health Care for all Australians Catherine Turnbull Chief Allied and Scientific Health Advisor SA Health Presentation to Indigenous Allied Health Australia Conference,
Overview of drug-induced deaths in Europe - What does the data tell us?
 Overview of drug-induced deaths in Europe - What does the data tell us? João Matias, Isabelle Giraudon, Julián Vicente EMCDDA expert group on the key-indicator Drug-related deaths and mortality among drug
Overview of drug-induced deaths in Europe - What does the data tell us? João Matias, Isabelle Giraudon, Julián Vicente EMCDDA expert group on the key-indicator Drug-related deaths and mortality among drug
Best practices in collecting and processing data in CRC screening and after it
 Best practices in collecting and processing data in CRC screening and after it The potential of harmonized information policy in effective national implementation of CRC screening Ladislav Dušek, Czech
Best practices in collecting and processing data in CRC screening and after it The potential of harmonized information policy in effective national implementation of CRC screening Ladislav Dušek, Czech
COLORECTAL CANCER: A CHALLENGE FOR HEALTHY LIFESTYLE, SCREENING AND PROPER CARE
 COLORECTAL CANCER: A CHALLENGE FOR HEALTHY LIFESTYLE, SCREENING AND PROPER CARE Brno, 29 May 2015: For the fourth time in a row, the second largest city of the Czech Republic will host the European Colorectal
COLORECTAL CANCER: A CHALLENGE FOR HEALTHY LIFESTYLE, SCREENING AND PROPER CARE Brno, 29 May 2015: For the fourth time in a row, the second largest city of the Czech Republic will host the European Colorectal
Weekly Influenza Surveillance Report. Week 11
 Weekly Influenza Surveillance Report Week 11 Report produced: 22/03/2001 Influenza activity in Ireland For the week ending the 18/03/01, week 11, influenza activity has increased. Sentinel general practices
Weekly Influenza Surveillance Report Week 11 Report produced: 22/03/2001 Influenza activity in Ireland For the week ending the 18/03/01, week 11, influenza activity has increased. Sentinel general practices
Alcohol-related harm in Europe and the WHO policy response
 Alcohol-related harm in Europe and the WHO policy response Lars Moller Programme Manager World Health Organization Regional Office for Europe Date of presentation NCD global monitoring framework: alcohol-related
Alcohol-related harm in Europe and the WHO policy response Lars Moller Programme Manager World Health Organization Regional Office for Europe Date of presentation NCD global monitoring framework: alcohol-related
European Collaboration on Dementia. Luxembourg, 13 December 2006
 European Collaboration on Dementia Luxembourg, 13 December 2006 2005 Call for projects Special attention has also to be given to information and definition of indicators on neurodegenerative, neurodevelopment,
European Collaboration on Dementia Luxembourg, 13 December 2006 2005 Call for projects Special attention has also to be given to information and definition of indicators on neurodegenerative, neurodevelopment,
CNAPA Meeting Luxembourg September 2016
 CNAPA Meeting Luxembourg September 2016 Manuel Cardoso RARHA Executive Coordinator Public Health MD Senior Advisor Deputy General-Director of SICAD - Portugal RARHA Events Policy Dialogue and Final Conference
CNAPA Meeting Luxembourg September 2016 Manuel Cardoso RARHA Executive Coordinator Public Health MD Senior Advisor Deputy General-Director of SICAD - Portugal RARHA Events Policy Dialogue and Final Conference
real-time AQ data 2007 and plans for 2008
 real-time AQ data 2007 and plans for 2008 Tim Haigh - project manager Information Resources http://www.eea.europa.eu/maps/ozone/map/ Where is all the data coming from? EEA NRT Database 4000 2000 700 EEA
real-time AQ data 2007 and plans for 2008 Tim Haigh - project manager Information Resources http://www.eea.europa.eu/maps/ozone/map/ Where is all the data coming from? EEA NRT Database 4000 2000 700 EEA
Screening for Cervical Cancer in Europe
 Asturias, 23 October, 2011 Asturias, 23 October Screening for Cervical Cancer in Europe M. Arbyn Unit Cancer Epidemiology, IPH, Brussels, Belgium Rue Juliette Wytsmanstraat 14 1050 Brussels Belgium T +32
Asturias, 23 October, 2011 Asturias, 23 October Screening for Cervical Cancer in Europe M. Arbyn Unit Cancer Epidemiology, IPH, Brussels, Belgium Rue Juliette Wytsmanstraat 14 1050 Brussels Belgium T +32
Cross Border Genetic Testing for Rare Diseases
 Cross Border Genetic Testing for Rare Diseases EUCERD Joint Action WP8 Helena Kääriäinen National Institute for Health an Welfare, Helsinki, Finland Starting point Possibilities and demand for genetic
Cross Border Genetic Testing for Rare Diseases EUCERD Joint Action WP8 Helena Kääriäinen National Institute for Health an Welfare, Helsinki, Finland Starting point Possibilities and demand for genetic
Bowel Cancer Prevention and Screening. Harriet Wynne, Cancer Council Victoria
 Bowel Cancer Prevention and Screening Harriet Wynne, Cancer Council Victoria New cases and deaths for the Victoria population in 2013 Thursfield V, et al. Cancer in Victoria: Statistics & trends 2013.
Bowel Cancer Prevention and Screening Harriet Wynne, Cancer Council Victoria New cases and deaths for the Victoria population in 2013 Thursfield V, et al. Cancer in Victoria: Statistics & trends 2013.
05/07/2018. Organisation. The English screening programme what is happening? Organisation. Bowel cancer screening in the UK is:
 Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
Organisation The English screening programme what is happening? Phil Quirke Lead Pathologist Bowel Cancer Screening PHE England Bowel Cancer Screening Pathology Committee Started 2006 with roll out 4 devolved
Joint Programming in Neurodegenerative Disease Research (JPND)
") Joint Programming in Neurodegenerative Disease Research (JPND) Building Alliances and Collaborations Prof. Philippe Amouyel, MD, PhD JPND Chair France Disclosure CEO of Fondation Plan Alzheimer Conference
Joint Programming in Neurodegenerative Disease Research (JPND) Building Alliances and Collaborations Prof. Philippe Amouyel, MD, PhD JPND Chair France Disclosure CEO of Fondation Plan Alzheimer Conference
Predictors of Repeat Participation in the NHS Bowel Cancer Screening Programme
 Lo, SH; Halloran, S; Snowball, J; Seaman, H; Wardle, J; von Wagner, C; (2015) Predictors of repeat participation in the NHS bowel cancer screening programme. Br J Cancer, 112 (1) 199-206. 10.1038/bjc.2014.569.
Lo, SH; Halloran, S; Snowball, J; Seaman, H; Wardle, J; von Wagner, C; (2015) Predictors of repeat participation in the NHS bowel cancer screening programme. Br J Cancer, 112 (1) 199-206. 10.1038/bjc.2014.569.
Cancer Research UK response to All Party Parliamentary Group on Cancer consultation Cancer across the Domains
 Cancer Research UK response to All Party Parliamentary Group on Cancer consultation Cancer across the Domains 29 August 2013 About Cancer Research UK 1 Cancer Research UK is the world s leading cancer
Cancer Research UK response to All Party Parliamentary Group on Cancer consultation Cancer across the Domains 29 August 2013 About Cancer Research UK 1 Cancer Research UK is the world s leading cancer
Inequalities in health: challenges and opportunities in Europe Dr Zsuzsanna Jakab WHO Regional Director for Europe
 Inequalities in health: challenges and opportunities in Europe Dr Zsuzsanna Jakab WHO Regional Director for Europe 21st Congress of the European Association of Dental Public Health 1 October 2016 Budapest
Inequalities in health: challenges and opportunities in Europe Dr Zsuzsanna Jakab WHO Regional Director for Europe 21st Congress of the European Association of Dental Public Health 1 October 2016 Budapest
Pharmaceutical, Medical and Health-related Government and Regulatory bodies around the world.
 1 International International Conference on Harmonization (ICH) World Health Organization (WHO) 2 Argentina National Administration of Drugs, Food and medical Technology. Australia s Department of health
1 International International Conference on Harmonization (ICH) World Health Organization (WHO) 2 Argentina National Administration of Drugs, Food and medical Technology. Australia s Department of health
Engagement in language assessment / Regions of Europe
 Summary table: Engagement in language / Regions of This table lists the statistically significant differences in the engagement in activities by the respondents from different s of : If the word or appears
Summary table: Engagement in language / Regions of This table lists the statistically significant differences in the engagement in activities by the respondents from different s of : If the word or appears
GENERAL PRACTITIONERS IN THE 1ST LINE OF CANCER PREVENTION
 GENERAL PRACTITIONERS IN THE 1ST LINE OF CANCER PREVENTION Bohumil Seifert Dpt. Of General Practice 1st Faculty of Medicine Charles University in Prague May, 29, 2015 European Colorectal Cancer Days, Brno
GENERAL PRACTITIONERS IN THE 1ST LINE OF CANCER PREVENTION Bohumil Seifert Dpt. Of General Practice 1st Faculty of Medicine Charles University in Prague May, 29, 2015 European Colorectal Cancer Days, Brno
2. CANCER AND CANCER SCREENING
 2. CANCER AND CANCER SCREENING INTRODUCTION The incidence of cancer and premature mortality from cancer are higher in Islington compared to the rest of England. Although death rates are reducing, this
2. CANCER AND CANCER SCREENING INTRODUCTION The incidence of cancer and premature mortality from cancer are higher in Islington compared to the rest of England. Although death rates are reducing, this
FOURIER STUDY GREYLOCK PRESS: CTS PRODUCT SAMPLE - FOURIER YES. Did the study achieve its main objective?
 FOURIER STUDY Did the study achieve its main objective? 2 15% 1 5% 9.8% YES FOURIER compared Repatha with placebo in patients who were taking a statin and had hardening or narrowing of the arteries and
FOURIER STUDY Did the study achieve its main objective? 2 15% 1 5% 9.8% YES FOURIER compared Repatha with placebo in patients who were taking a statin and had hardening or narrowing of the arteries and
Bowel Cancer Screening
 Bowel Cancer Screening Dr John Hancock FRCP Consultant Gastroenterologist University Hospital of North Tees Outline Background Current bowel cancer screening programme Tees Screening Centre Future Flexi
Bowel Cancer Screening Dr John Hancock FRCP Consultant Gastroenterologist University Hospital of North Tees Outline Background Current bowel cancer screening programme Tees Screening Centre Future Flexi
PROMOTION AND PROTECTION OF ALL HUMAN RIGHTS, CIVIL, POLITICAL, ECONOMIC, SOCIAL AND CULTURAL RIGHTS, INCLUDING THE RIGHT TO DEVELOPMENT
 UNITED NATIONS A General Assembly Distr. LIMITED A/HRC/11/L.16 16 June 2009 Original: ENGLISH HUMAN RIGHTS COUNCIL Eleventh session Agenda item 3 PROMOTION AND PROTECTION OF ALL HUMAN RIGHTS, CIVIL, POLITICAL,
UNITED NATIONS A General Assembly Distr. LIMITED A/HRC/11/L.16 16 June 2009 Original: ENGLISH HUMAN RIGHTS COUNCIL Eleventh session Agenda item 3 PROMOTION AND PROTECTION OF ALL HUMAN RIGHTS, CIVIL, POLITICAL,