Interventions to Improve Follow-up of Positive Results on Fecal Blood Tests
|
|
|
- Camilla Stevenson
- 5 years ago
- Views:
Transcription

1 Interventions to Improve Follow-up of Positive Results on Fecal Blood Tests Results of a systematic review, Kaiser experience, and implications for the Canton of Vaud Kevin Selby, M.D. Kevin.Selby@hospvd.ch National Colorectal Cancer Roundtable 2017 Kaiser Permanente Research
2 No conflicts of interest to disclose Funding: - Swiss Cancer Research Foundation (BIL KFS [Selby]) - National Cancer Institute PROSPR (Population-based Research Optimizing Screening through Personalized Regimens) consortium (U54 CA [Corley])
3 Outline FIT-based screening programs and problems with follow-up of testpositive patients A systematic review of interventions to improve follow-up of positive fecal tests How organized programs at Kaiser and other countries follow up testpositive patients Implications for CRC screening program in the Canton of Vaud


4 Fecal immunochemical tests are ideal for mass screening RCTs with guaiac FOBT show a 15-33% reduction in CRC-specific mortality FIT are both more sensitive and more specific -> Increased detection of advanced adenomas Only one sample, no dietary or medication restrictions -> RCTs show increased adherence Sufficiently stable for mailed outreach Quantitative FIT cut-off can be varied

5 Low rates of follow-up colonoscopy after positive fecal blood tests are a problem Real-world efficacy of FIT screening depends on colonoscopy follow-up of positive tests Follow-up rates of ~50% in multiple settings in the United States Rates of 60-70% in Asia Follow-up closer to 70-90% in Canada and Europe: still a problem in many places! Challenging: follow-up involves interaction of multiple levels of care Patients are often reluctant Dis Colon Rectum. 2006;49: J Natl Cancer Inst Monogr. 2010;2010(40):58-71 Cancer Epidemiol Biomarkers Prev. 2016; 25:344-50
6 Colonoscopy delays after a positive fecal test are important Analysis of 70,000+ FIT-positive patients shows an increased risk of CRC, and specifically advancedstage CRC, when time to colonoscopy is greater than 6 months Corley et al. JAMA. 2017;317(16):
 or guaiac fecal occult blood tests")
7 Systematic review objective: Evaluate interventions to improve rates of follow-up colonoscopy for adults after a positive result on fecal immunochemical tests (FIT) or guaiac fecal occult blood tests (gfobt)
8 Methods Data Sources: Cochrane Central Register of Controlled Trials (CENTRAL), PubMed, and Embase through June 2017 English-language studies Study Selection: Randomized and nonrandomized studies Interventions to improve colonoscopy (or DCBE in older studies) follow-up of positive fecal test results in the screening setting Focus on absolute change in colonoscopy completion at 6 months, if available Data Extraction: Two reviewers extracted data and ranked study quality, and then rated overall strength of evidence for each study category Protocol available: PROSPERO: CRD
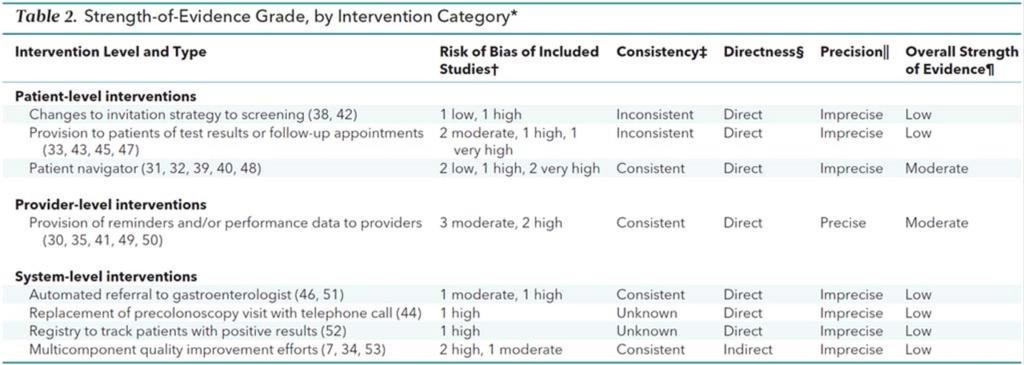
9 Results 23 studies eligible for analysis 7 randomized and 16 nonrandomized studies Only 3 at low risk of bias Number of patients ranged from 14 to of FIT follow-up, 18 of gfobt follow-up No meta analysis performed given significant heterogeneity in outcomes reported
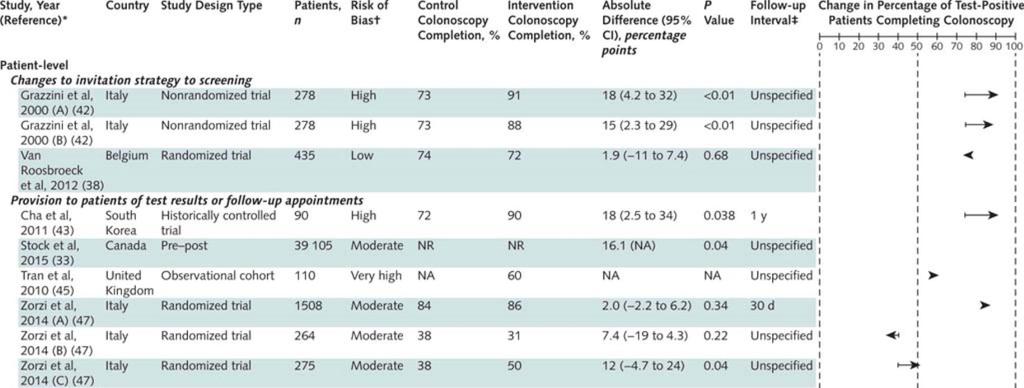
10 1. Patient-level Interventions Changes to invitation strategy to screening 2 studies, 1 randomized trial at low-risk of bias Interventions to increase screening rates don t worsen follow-up of positive tests Provision to patients of test results or follow-up appointments 4 studies, 1 randomized trial at moderate risk of bias Mailing or calling all patients to provide tests results or directly providing appointments to discuss follow-up colonoscopy RCT: among initial non-responders in Italy, a specialized nurse increased follow-up (+12% (CI 0.5 to 24))
11 1. Patient-level Interventions - continued Patient navigation 5 studies, 2 randomized trials at low-risk of bias RCT 1: Registered nurse patient navigators increased follow-up from 80.8% to 91.0% at 6 months (+ 10.1% (CI -1.5 to 22)). Trial was underpowered RCT 2: Patient navigators for multiple cancers using strengths-based approach increased from 58% to 79% at 1 year (+ 21% (CI 9.5 to 33))
12 2. Provider-level Interventions Provision to providers of reminders and/or performance data 5 studies, 2 cluster randomized All used electronic algorithms to clearly identify ordering providers / assigned primary care physician Remind those with inadequate action after 60 or 90 days 4 from integrated systems in the US, generally multi-component interventions, showed positive results (+9 to +25%) 1 used centrally generated reports in a provincial screening program, showed no difference (HR 0.95, CI 0.79 to 1.13)
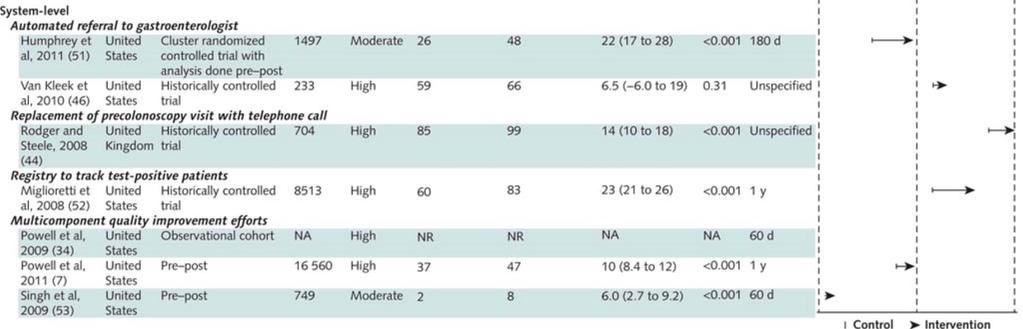
13 3. System-level Interventions Automated referral to gastroenterologist 2 studies, all positive fecal test results sent directly to gastroenterologists Both from VA medical centers, integrated EHR allowed transfer of patient information Replacement of precolonoscopy visit with telephone call 1 study, patients given choice of phone call instead of face-to-face consultation Registry to track patients with positive results 1 study, registry reviewed regularly by nurse manager, +23% improvement over several years (CI 21 to 26) Multicomponent quality improvement efforts 3 studies, all from VA, Pre-post or observational designs, only 6 to 10% improvement
14
15 Limitations Heterogeneous outcome measurements: no meta analyses Colonoscopy completion is an intermediate outcome Most U.S. studies (10 of 14) from within the VA Cannot rule out publication bias Inclusion of non-randomized studies is more complete, but higher risk of bias, may be misleading
16 Areas for further research Need greater standardization of results reporting and more RCTs Need for pragmatic trials when implementing new programs What is the effect of increased endoscopy capacity? Stratifying patient populations to target high-cost interventions Can we better engage patients electronically?
17 Outline FIT-based screening programs and problems with follow-up of testpositive patients A systematic review of interventions to improve follow-up of positive fecal tests How organized programs at Kaiser and in other countries follow up test-positive patients Implications for CRC screening program in the Canton of Vaud
, with 83%")
18 Follow-up of positive FIT at Kaiser Permanente Northern California KPNC: integrated healthcare system with 4.5 million members Mailed FIT outreach since 2006 Approximately 20,000 positive FIT per year Median time to colonoscopy in 2015 of 36 days (IQR 24 to 73), with 83% having had a colonoscopy by 6 months How is this being done?
19 Traditional flow FIT read as positive Primary care provider (PCP) notified Patient given result and appointment scheduled Sees GI for colonoscopy
20 Increasing responsibility assumed by GI to manage FIT positive patients Primary care provider (PCP) notified FIT read as positive e-consult GI receives FIT+ patient list and/or e- consult Patient given result and appointment scheduled Navigator call to explain colonoscopy logistics, risks and preparation Colonoscopy completed
21 Overall organization of FIT-positive follow-up within Kaiser Permanente Northern California Primary care provider (PCP) notified Minimum 3 attempts to contact patient Registered letter if no phone or contact FIT read as positive e-consult GI receives FIT+ patient list and/or e- consult Patient given result and appointment scheduled Navigator call to explain colonoscopy logistics, risks and preparation Colonoscopy completed
22 Primary care provider (PCP) notified Minimum 3 attempts to contact patient Registered letter if no phone or contact FIT read as positive e-consult GI receives FIT+ patient list and/or e- consult Patient given result and appointment scheduled Navigator call to explain colonoscopy logistics, risks and preparation Colonoscopy completed Adequate colonoscopy capacity (staff and endoscopy suites) Organizational supports in place to ensure success Registry of FIT+ patients with real-time updates (PROMPT) GI Staff member designated responsible Frequent feedback of FIT+ follow-up performance Financial rewards to management for attaining colonoscopy access targets
23 Examples from other countries Ontario, Canada: 75% colonoscopy completion Originally results by letter only to GP Later results sent to patient and reminder / performance letters for GP Curr Oncol. 2017; 24(1):47-51 United Kingdom: 80-85% completion Results by letter to patient and GP Call from Specialist Screening Practitioner, usually a nurse J Med Screen. 2017; 24(1):12-19 Netherlands: 75-80% completion Results by letter to patient and GP Scheduled pre-colonoscopy appointment at a colonoscopy center. Colonoscopy appointments managed centrally Gastroenterology. 2017;152(4):
24 Examples from other countries France: 85-90% follow-up. Results by letter to GP and patient. GPs to coordinate referral. If no report of completed colonoscopy, reminders sent at 3 and 6 months, emphasizing need. After 12 months, patient excluded from programme. British Journal of Cancer. 2013; 109: Italy: Long-time program in Veneto region has 90+% follow-up Trained operators contact FIT+ subjects by phone call to communicate result and invite them to colonoscopy. Exam can be scheduled immediately Repeat calls if initial refusal / difficulty with scheduling Emphasize free colonoscopy Gut, 2016; 0:1-7
25 Outline FIT-based screening programs and problems with follow-up of testpositive patients A systematic review of interventions to improve follow-up of positive fecal tests How organized programs in other countries follow up test-positive patients Implications for CRC screening program in the Canton of Vaud
26 Canton of Vaud CRC screening program Launched in 2015 with first mailed invitations in 2016 Target population of 180,000 people aged 50-69, rolling invitations over 5-7 years All participants offered choice of FIT and colonoscopy Initial projections of participation rates of 30% for FIT and 10-15% for colonoscopy Reimbursement without deductible of 90% of cost of appointment for inclusion, test of choice, and follow-up colonoscopy
27 Population registry from canton Rolling invitations based on birth year Invitation letter: - Information brochure - Refusal form letter GP Consultation specific billing code Patient entered into central database No response, no billing receipt received Receipt of refusal FIT Prescription for pharmacy Colonoscopy Coordinated by GP Temporary or definitive exclusion from the program Repeat invitations after 3 months Next invitation in 2 years if no answer Test picked up at the pharmacy. Test performed by patient at home and sent to central lab. FIT normal Next invitation in 2 years Positive FIT Return to GP Colonoscopy done by gastroenterologist of choice Normal exam Reinvitation in 10 years Positive colonoscopy. Pathology results to tumor registry

28 Population registry from canton Rolling invitations based on birth year Invitation letter: - Information brochure - Refusal form letter GP Consultation specific billing code Patient entered into central database No response, no billing receipt received Receipt of refusal FIT Prescription for pharmacy Colonoscopy Coordinated by GP Temporary or definitive exclusion from the program Repeat invitations after 3 months Next invitation in 2 years if no answer Test picked up at the pharmacy. Test performed by patient at home and sent to central lab. FIT normal Next invitation in 2 years Positive FIT Return to GP Colonoscopy done by gastroenterologist of choice Normal exam Reinvitation in 10 years Positive colonoscopy. Pathology results to tumor registry
29 Handling of positive tests Results of positive tests mailed to both the patient and GP, with the GP receiving result 24 hours ahead Recommended follow-up is colonoscopy, with 90% of cost reimbursed by the program Early indicators show about 90% of test-positive patients have gotten a colonoscopy Target: European recommendations of diagnostic colonoscopy within 31 days of referral. Referral within 15 days of a positive FIT. Acceptable proportion getting colonoscopy: 90%. Desired: 95%
30 What implications from this research for the Canton of Vaud? For now, too early to precisely measure follow-up rates Proportion of FIT-positive patients with colonoscopy completed at 6 months should be monitored as a performance measure Vaudois program very decentralized emphasis on GP and gastroenterologist autonomy, Will likely require centralized tracking and individualized reminders Inclusion via GP may be an advantage (clear responsibility) Patient navigators have been used successfully in other organized programs and could be considered
31 Conclusions 1. More work and research are needed in this important area 2. Patient navigators appear to work and are used by many organized screening programs internationally can be expensive, often require centralized control 3. Provider reminder systems, direct referral to gastroenterologists, and central management of colonoscopy appointments are promising, less labor-intensive interventions




32 Thank you! Doug Corley & research group at Kaiser DOR Supporters at University of Lausanne Swiss Cancer Research Foundation
33 Extra slides Contact information: Kevin Selby Post-doctoral Fellow at the Kaiser Permanente Division of Research Oakland, CA Chef de Clinique, Policlinique médicale universitaire Lausanne, Switzerland
34
35

36

37
38
39 Appendix B: Criteria used for determining risk of bias of individual studies, based on guidelines of the Agency for Healthcare Research and Quality (AHRQ) (36) and the Grading of Recommendations Assessments, Development and Evaluation (GRADE) working group (37) Study type Randomized controlled trial Criteria used Considered to be at low risk of bias. Upgraded to moderate risk if there was concern for the following problems in the study design or reporting. - Lack of allocation concealment - Lack of blinding that influences outcomes - Incomplete accounting of patients and outcome events - Selective outcome reporting bias - Recruitment bias in cluster-randomized trials Observational study or non-randomized interventional study (for example a pre-post or non-randomized parallel group study design) Considered to be at high risk of bias. Downgraded to moderate risk if the study design adequately accounted for and reported all of the following elements. Upgraded to very high risk if there were severe or multiple problems with these elements. - Development and application of appropriate eligibility criteria - Adequate measurement of both exposure and outcome - Adequate control for confounding, with both accurate measurement of all known prognostic factors and adjustment for these factors - Adequate follow-up of all participants
Positive Results on Fecal Blood Tests
 Interventions to Improve Follow-up of Positive Results on Fecal Blood Tests Results of a systematic review and Kaiser experience Kevin Selby, M.D. kevin.j.selby@kp.org National Colorectal Cancer Roundtable
Interventions to Improve Follow-up of Positive Results on Fecal Blood Tests Results of a systematic review and Kaiser experience Kevin Selby, M.D. kevin.j.selby@kp.org National Colorectal Cancer Roundtable
HOW TO ASSURE FOLLOW UP COLONOSCOPY FOR POSITIVE FIT FROM THE PROCESS SIDE JANUARY 30 TH, :00 PM ET
 HOW TO ASSURE FOLLOW UP COLONOSCOPY FOR POSITIVE FIT FROM THE PROCESS SIDE JANUARY 30 TH, 2018 1:00 PM ET 1 Purpose of Todays Webinar Review evidence and processes to help ensure that patients obtain a
HOW TO ASSURE FOLLOW UP COLONOSCOPY FOR POSITIVE FIT FROM THE PROCESS SIDE JANUARY 30 TH, 2018 1:00 PM ET 1 Purpose of Todays Webinar Review evidence and processes to help ensure that patients obtain a
TPMG experience in improving colorectal cancer screening rates
 TPMG experience in improving colorectal cancer screening rates Theodore R. Levin, MD Clinical Lead for CRC screening, The Permanente Medical Group, Inc Kaiser Permanente Northern California Kaiser Permanente
TPMG experience in improving colorectal cancer screening rates Theodore R. Levin, MD Clinical Lead for CRC screening, The Permanente Medical Group, Inc Kaiser Permanente Northern California Kaiser Permanente
Implementing communication material to promote shared decision making in colorectal cancer screening in primary care - experiences in Switzerland
 Implementing communication material to promote shared decision making in colorectal cancer screening in primary care - experiences in Switzerland Lugano, September 15th, 2017 Prof. Dr. med Reto Auer Berner
Implementing communication material to promote shared decision making in colorectal cancer screening in primary care - experiences in Switzerland Lugano, September 15th, 2017 Prof. Dr. med Reto Auer Berner
The New Grade A: USPSTF Updated Colorectal Cancer Screening Guidelines, What does it all mean?
 The New Grade A: USPSTF Updated Colorectal Cancer Screening Guidelines, What does it all mean? Robert A. Smith, PhD Cancer Control, Department of Prevention and Early Detection American Cancer Society
The New Grade A: USPSTF Updated Colorectal Cancer Screening Guidelines, What does it all mean? Robert A. Smith, PhD Cancer Control, Department of Prevention and Early Detection American Cancer Society
Developing Systems to Increase Colorectal Cancer Screening at Health Centers
 Northwestern University Feinberg School of Medicine Developing Systems to Increase Colorectal Cancer Screening at Health Centers David R. Buchanan, MD, MS Chief Clinical Officer, Erie Family Health Center
Northwestern University Feinberg School of Medicine Developing Systems to Increase Colorectal Cancer Screening at Health Centers David R. Buchanan, MD, MS Chief Clinical Officer, Erie Family Health Center
Colorectal cancer screening
 26 Colorectal cancer screening BETHAN GRAF AND JOHN MARTIN Colorectal cancer is theoretically a preventable disease and is ideally suited to a population screening programme, as there is a long premalignant
26 Colorectal cancer screening BETHAN GRAF AND JOHN MARTIN Colorectal cancer is theoretically a preventable disease and is ideally suited to a population screening programme, as there is a long premalignant
An Update on the Bowel Cancer Screening Programme. Natasha Djedovic, London Hub Director 17 th September 2018
 An Update on the Bowel Cancer Screening Programme Natasha Djedovic, London Hub Director 17 th September 2018 NHS Bowel Cancer Screening Programme 2006: 60-69 yr old men & women offered guaiac Faecal Occult
An Update on the Bowel Cancer Screening Programme Natasha Djedovic, London Hub Director 17 th September 2018 NHS Bowel Cancer Screening Programme 2006: 60-69 yr old men & women offered guaiac Faecal Occult
COLORECTAL CANCER SCREENING COLLABORATIVE FINAL REPORT September 2012
 COLORECTAL CANCER SCREENING COLLABORATIVE FINAL REPORT September 2012 INTRODUCTION/HISTORY OF PROJECT Colon cancer is easily treated and often cured when caught in the early stages. Yet, it remains the
COLORECTAL CANCER SCREENING COLLABORATIVE FINAL REPORT September 2012 INTRODUCTION/HISTORY OF PROJECT Colon cancer is easily treated and often cured when caught in the early stages. Yet, it remains the
Colorectal Cancer Screening in Ohio CHCs. Ohio Association of Community Health Centers
 Colorectal Cancer Screening in Ohio CHCs Ohio Association of Community Health Centers 2 1/29/2015 Your Speakers Dr. Ted Wymyslo Ashley Ballard Randy Runyon 3 1/29/2015 Facts 3 rd most common cancer in
Colorectal Cancer Screening in Ohio CHCs Ohio Association of Community Health Centers 2 1/29/2015 Your Speakers Dr. Ted Wymyslo Ashley Ballard Randy Runyon 3 1/29/2015 Facts 3 rd most common cancer in
Time to Colonoscopy After a Positive Fecal Test and Risk of Colorectal Cancer Outcomes
 Time to Colonoscopy After a Positive Fecal Test and Risk of Colorectal Cancer Outcomes Douglas Corley MD, PhD Kaiser Permanente, Northern California For Corley DA, Jensen CD, Quinn VP, Doubeni CA, Zauber
Time to Colonoscopy After a Positive Fecal Test and Risk of Colorectal Cancer Outcomes Douglas Corley MD, PhD Kaiser Permanente, Northern California For Corley DA, Jensen CD, Quinn VP, Doubeni CA, Zauber
Faecal Immunochemical Testing (FIT) for Screening and Symptomatic Patients
 for Screening and Symptomatic Patients") Faecal Immunochemical Testing (FIT) for Screening and Symptomatic Patients Caroline Addison NE BCSP Hub Director and Consultant Clinical Scientist What is FIT Type of Faecal Occult Blood test Designed
Faecal Immunochemical Testing (FIT) for Screening and Symptomatic Patients Caroline Addison NE BCSP Hub Director and Consultant Clinical Scientist What is FIT Type of Faecal Occult Blood test Designed
The effectiveness of telephone reminders and SMS messages on compliance with colorectal cancer screening: an open-label, randomized controlled trial
 Page1 of 5 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 The effectiveness of telephone reminders and SMS messages on compliance with colorectal cancer screening: an
Page1 of 5 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 The effectiveness of telephone reminders and SMS messages on compliance with colorectal cancer screening: an
Dr Alasdair Patrick. Dr Nagham Al-Mozany. 9:45-10:10 Where Are We Up To With Bowel Cancer Screening?
 Dr Alasdair Patrick Gastroenterologist and General Physician Middlemore Hospital Auckland Dr Nagham Al-Mozany Colorectal Surgeon Auckland City Hospital Clinical Senior Lecturer University of Auckland 9:45-10:10
Dr Alasdair Patrick Gastroenterologist and General Physician Middlemore Hospital Auckland Dr Nagham Al-Mozany Colorectal Surgeon Auckland City Hospital Clinical Senior Lecturer University of Auckland 9:45-10:10
Colorectal cancer screening in England
 Colorectal cancer screening in England critical analysis Prof Stephen P. Halloran Participation Rate 57% All Screens (1.9% +ve) 52% Prevalent 1 st Screen (age 60 years) 36% Prevalent Screen (2.2% +ve)
Colorectal cancer screening in England critical analysis Prof Stephen P. Halloran Participation Rate 57% All Screens (1.9% +ve) 52% Prevalent 1 st Screen (age 60 years) 36% Prevalent Screen (2.2% +ve)
Implementing of Population-based FOBT Screening
 Implementing of Population-based FOBT Screening gfobt to FIT Experience from England Prof Stephen P. Halloran Guaiac FOBt Haem 2H 2 O 2 = 2H 2 0 + O 2 Oxidised guaiaconic acid is blue Biennial Bowel Cancer
Implementing of Population-based FOBT Screening gfobt to FIT Experience from England Prof Stephen P. Halloran Guaiac FOBt Haem 2H 2 O 2 = 2H 2 0 + O 2 Oxidised guaiaconic acid is blue Biennial Bowel Cancer
Global colorectal cancer screening appropriate or practical? Graeme P Young, Flinders University WCC, Melbourne
 Global colorectal cancer screening appropriate or practical? Graeme P Young, Flinders University. 2014 WCC, Melbourne Outline WHO criteria to justify screening Appropriateness: Global variation in incidence
Global colorectal cancer screening appropriate or practical? Graeme P Young, Flinders University. 2014 WCC, Melbourne Outline WHO criteria to justify screening Appropriateness: Global variation in incidence
Optimizing implementation of fecal immunochemical testing in Ontario: A randomized controlled trial
 Optimizing implementation of fecal immunochemical testing in Ontario: A randomized controlled trial J. Tinmouth, N.N. Baxter, L.F. Paszat, E. Randell, M. Serenity, R. Sutradhar, L. Rabeneck Conflicts of
Optimizing implementation of fecal immunochemical testing in Ontario: A randomized controlled trial J. Tinmouth, N.N. Baxter, L.F. Paszat, E. Randell, M. Serenity, R. Sutradhar, L. Rabeneck Conflicts of
Colorectal Cancer Screening and Risk Assessment Workflow. Documentation Guide for Health Center NextGen Users
 Colorectal Cancer Screening and Risk Assessment Workflow Documentation Guide for Health Center NextGen Users Colorectal Cancer Screening and Risk Assessment Workflow and Documentation Guide for Health
Colorectal Cancer Screening and Risk Assessment Workflow Documentation Guide for Health Center NextGen Users Colorectal Cancer Screening and Risk Assessment Workflow and Documentation Guide for Health
Debate: General surveillance/screening for colon cancer in a resource constrained environment is imperative
 Debate: General surveillance/screening for colon cancer in a resource constrained environment is imperative Dr. Meryl Oyomno Department of surgery, University of Pretoria INTRODUCTION Screening is the
Debate: General surveillance/screening for colon cancer in a resource constrained environment is imperative Dr. Meryl Oyomno Department of surgery, University of Pretoria INTRODUCTION Screening is the
Improving Outcomes in Colorectal Cancer: The Science of Screening. Colorectal Cancer (CRC)
") Improving Outcomes in Colorectal Cancer: The Science of Screening Tennessee Primary Care Association October 23, 2014 Durado Brooks, MD, MPH Director, Prostate and Colorectal Cancers Colorectal Cancer
Improving Outcomes in Colorectal Cancer: The Science of Screening Tennessee Primary Care Association October 23, 2014 Durado Brooks, MD, MPH Director, Prostate and Colorectal Cancers Colorectal Cancer
SCREENING FOR BOWEL CANCER USING FLEXIBLE SIGMOIDOSCOPY REVIEW APPRAISAL CRITERIA FOR THE UK NATIONAL SCREENING COMMITTEE
 SCREENING FOR BOWEL CANCER USING FLEXIBLE SIGMOIDOSCOPY REVIEW APPRAISAL CRITERIA FOR THE UK NATIONAL SCREENING COMMITTEE The Condition 1. The condition should be an important health problem Colorectal
SCREENING FOR BOWEL CANCER USING FLEXIBLE SIGMOIDOSCOPY REVIEW APPRAISAL CRITERIA FOR THE UK NATIONAL SCREENING COMMITTEE The Condition 1. The condition should be an important health problem Colorectal
Screening for Colorectal Cancer
 Screening for Colorectal Cancer April 1, 2014 Revised August 2014 McMaster Evidence Review and Synthesis Centre Team: Donna Fitzpatrick-Lewis, Ali Usman, Rachel Warren, Meghan Kenny, Maureen Rice, Andy
Screening for Colorectal Cancer April 1, 2014 Revised August 2014 McMaster Evidence Review and Synthesis Centre Team: Donna Fitzpatrick-Lewis, Ali Usman, Rachel Warren, Meghan Kenny, Maureen Rice, Andy
Knowledge, Attitude, Self-Efficacy, Literacy and CRC Screening in Rural Community Clinics
 Knowledge, Attitude, Self-Efficacy, Literacy and CRC Screening in Rural Community Clinics Connie Arnold, PhD LSU Health Sciences Center Shreveport Alfred Rademaker, PhD Northwestern University Terry Davis,
Knowledge, Attitude, Self-Efficacy, Literacy and CRC Screening in Rural Community Clinics Connie Arnold, PhD LSU Health Sciences Center Shreveport Alfred Rademaker, PhD Northwestern University Terry Davis,
Colorectal Cancer Screening: State of the Science
 Colorectal Cancer Screening: State of the Science LA Academy of Family Practice Convention July 9, 2016 Sandestin, FL Durado Brooks, MD, MPH Director, Prostate and Colorectal Cancers Colorectal Cancer
Colorectal Cancer Screening: State of the Science LA Academy of Family Practice Convention July 9, 2016 Sandestin, FL Durado Brooks, MD, MPH Director, Prostate and Colorectal Cancers Colorectal Cancer
FREQUENTLY ASKED QUESTIONS
 FREQUENTLY ASKED QUESTIONS What is CRC? CRC (CRC) is cancer of the large intestine (colon), the lower part of the digestive system. Rectal cancer is cancer of the last several inches of the colon. Together,
FREQUENTLY ASKED QUESTIONS What is CRC? CRC (CRC) is cancer of the large intestine (colon), the lower part of the digestive system. Rectal cancer is cancer of the last several inches of the colon. Together,
The Dutch bowel cancer screening program Relevant lessions for Ontario
 The Dutch bowel cancer screening program Relevant lessions for Ontario Ernst J Kuipers Erasmus MC University Medical Center Rotterdam - The Netherlands 1 Ismar Boas (1858 1938) Colorectal cancer screening
The Dutch bowel cancer screening program Relevant lessions for Ontario Ernst J Kuipers Erasmus MC University Medical Center Rotterdam - The Netherlands 1 Ismar Boas (1858 1938) Colorectal cancer screening
Bowel cancer screening and prevention
 Bowel cancer screening and prevention Cancer Incidence and Mortality Victoria 2012 Number 6000 5000 4000 3000 2000 Incidences = 29,387 Mortality = 10,780 Incidence Mortality 1000 0 Prostate Breast Bowel
Bowel cancer screening and prevention Cancer Incidence and Mortality Victoria 2012 Number 6000 5000 4000 3000 2000 Incidences = 29,387 Mortality = 10,780 Incidence Mortality 1000 0 Prostate Breast Bowel
Objectives. Definitions. Colorectal Cancer Screening 5/8/2018. Payam Afshar, MS, MD Kaiser Permanente, San Diego. Colorectal cancer background
 Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
National Bowel Screening Programme. Quick Guide
 National Bowel Screening Programme Quick Guide What is the National Bowel Screening Programme? This is a free programme to help detect bowel cancer. The National Bowel Screening Programme is being rolled
National Bowel Screening Programme Quick Guide What is the National Bowel Screening Programme? This is a free programme to help detect bowel cancer. The National Bowel Screening Programme is being rolled
ColonCancerCheck & Regional Updates. Cheryl Shoemaker RN, BScN, CON(C) March 19, 2014
 March 19, 2014") ColonCancerCheck & Regional Updates Cheryl Shoemaker RN, BScN, CON(C) March 19, 2014 Colorectal Cancer Facts 3 rd most commonly diagnosed cancer 2nd leading cause of cancer death in men & 3 rd cancer death
ColonCancerCheck & Regional Updates Cheryl Shoemaker RN, BScN, CON(C) March 19, 2014 Colorectal Cancer Facts 3 rd most commonly diagnosed cancer 2nd leading cause of cancer death in men & 3 rd cancer death
ADENOMA SURVEILLANCE BCSP Guidance Note No 1 Version 1 September 2009
 ADENOMA SURVEILLANCE BCSP Guidance Note No 1 Version 1 September 2009 Published by: NHS Cancer Screening Programmes Fulwood House Old Fulwood Road Sheffield S10 3TH Tel: 0114 271 1060 Fax: 0114 271 1089
ADENOMA SURVEILLANCE BCSP Guidance Note No 1 Version 1 September 2009 Published by: NHS Cancer Screening Programmes Fulwood House Old Fulwood Road Sheffield S10 3TH Tel: 0114 271 1060 Fax: 0114 271 1089
Thank You to Our Sponsors: Evaluations & CE Credits. Featured Speakers. Conflict of Interest & Disclosure Statements
 Thank You to Our Sponsors: University at Albany School of Public Health NYS Department of Health Evaluations & CE Credits Nursing Contact Hours, CME and CHES credits are available. Please visit www.phlive.org
Thank You to Our Sponsors: University at Albany School of Public Health NYS Department of Health Evaluations & CE Credits Nursing Contact Hours, CME and CHES credits are available. Please visit www.phlive.org
California Colon Cancer Control Program (CCCCP)
") California Colon Cancer Control Program (CCCCP) Diane Keys, CCCCP Program Director Chronic Disease Control Branch MISSION OF THE CALIFORNIA DEPARTMENT OF PUBLIC HEALTH Dedicated to optimizing the health
California Colon Cancer Control Program (CCCCP) Diane Keys, CCCCP Program Director Chronic Disease Control Branch MISSION OF THE CALIFORNIA DEPARTMENT OF PUBLIC HEALTH Dedicated to optimizing the health
Transition to Fecal Immunochemical Testing (FIT)
") Transition to Fecal Immunochemical Testing (FIT) Frequently Asked Questions for Primary Care Providers October 2017 Version 1.1 Overview Ontario will be transitioning from the guaiac fecal occult blood
Transition to Fecal Immunochemical Testing (FIT) Frequently Asked Questions for Primary Care Providers October 2017 Version 1.1 Overview Ontario will be transitioning from the guaiac fecal occult blood
Colorectal Cancer Screening: The Science Behind the Guidelines. CRC Incidence North Dakota. Colorectal Cancer (CRC) CRC Incidence North Dakota
 CRC Incidence North Dakota") Reaching 80% Screened For Colorectal Cancer by 2018: Using Systems Change to Increase Cancer Screening Colorectal Cancer Screening: The Science Behind the Guidelines September 2017 Jeff Hostetter, MD Based
Reaching 80% Screened For Colorectal Cancer by 2018: Using Systems Change to Increase Cancer Screening Colorectal Cancer Screening: The Science Behind the Guidelines September 2017 Jeff Hostetter, MD Based
Diabetes and Quality Measures.
 Diabetes and Quality Measures. Reducing Costs, Closing Gaps, and Improving Member Health Executive Summary According to the Centers for Disease Control, 29 million people in the U.S. have diabetes. Another
Diabetes and Quality Measures. Reducing Costs, Closing Gaps, and Improving Member Health Executive Summary According to the Centers for Disease Control, 29 million people in the U.S. have diabetes. Another
Northern Ireland Bowel Cancer Screening Programme. Pathways. Version 4 1 st October 2013
 Northern Ireland Bowel Cancer Screening Programme Pathways These changes will be version controlled, led by the Quality Assurance Director for the Programme. Any updated versions will be circulated and
Northern Ireland Bowel Cancer Screening Programme Pathways These changes will be version controlled, led by the Quality Assurance Director for the Programme. Any updated versions will be circulated and
Collaborative Approach in Managing the High Risk Diabetic Patient in a Patient Centered Medical Home
 Collaborative Approach in Managing the High Risk Diabetic Patient in a Patient Centered Medical Home Background Safety net facility serving the community for more than 140 years Employ over 3500 health
Collaborative Approach in Managing the High Risk Diabetic Patient in a Patient Centered Medical Home Background Safety net facility serving the community for more than 140 years Employ over 3500 health
ColonCancerCheck Program Report
 ColonCancerCheck 2010 Program Report Table of Contents 3 Acknowledgements 4 Message from Dr. Linda Rabeneck and Dr. Jill Tinmouth 5 Executive Summary 5 Burden of Disease 5 Ontario s Colorectal Cancer Screening
ColonCancerCheck 2010 Program Report Table of Contents 3 Acknowledgements 4 Message from Dr. Linda Rabeneck and Dr. Jill Tinmouth 5 Executive Summary 5 Burden of Disease 5 Ontario s Colorectal Cancer Screening
Increasing Colorectal Cancer Screening in Wyoming. Allie Bain, MPH Outreach & Education Supervisor Wyoming Integrated Cancer Services Program
 Increasing Colorectal Cancer Screening in Wyoming Allie Bain, MPH Outreach & Education Supervisor Wyoming Integrated Cancer Services Program Overview What is colorectal cancer? What are risk factors for
Increasing Colorectal Cancer Screening in Wyoming Allie Bain, MPH Outreach & Education Supervisor Wyoming Integrated Cancer Services Program Overview What is colorectal cancer? What are risk factors for
Prof Stephen P. Halloran. Update on the NHS Bowel Cancer Screening Programme Focus on BS & FIT
 Prof Stephen P. Halloran Update on the NHS Bowel Cancer Screening Programme Focus on BS & FIT World Top 20 Cancers Men Incidence & Mortality (2012) Women World Colorectal Cancer 3 rd commonest cancer 4
Prof Stephen P. Halloran Update on the NHS Bowel Cancer Screening Programme Focus on BS & FIT World Top 20 Cancers Men Incidence & Mortality (2012) Women World Colorectal Cancer 3 rd commonest cancer 4
Annual Report. Public Health Screening Programmes TO 31 MARCH Extract: Chapter 3 : Planning for Bowel Screening Programme
 Public Health Screening Programmes Annual Report TO 31 MARCH 2007 Extract: Chapter 3 : Planning for Bowel Screening Programme Version 1.0 Published: 18 December 2007 1 Contents INTRODUCTION...3 SUMMARY...5
Public Health Screening Programmes Annual Report TO 31 MARCH 2007 Extract: Chapter 3 : Planning for Bowel Screening Programme Version 1.0 Published: 18 December 2007 1 Contents INTRODUCTION...3 SUMMARY...5
Increasing Colorectal Cancer Screening Rates Why it s not as easy as you ve been told
 INCREASING COLORECTAL CANCER SCREENING IN NYS Increasing Colorectal Cancer Screening Rates Why it s not as easy as you ve been told 5/15/17 Syracuse, NY Martin C. Mahoney, MD, PhD Roswell Park Cancer Institute
INCREASING COLORECTAL CANCER SCREENING IN NYS Increasing Colorectal Cancer Screening Rates Why it s not as easy as you ve been told 5/15/17 Syracuse, NY Martin C. Mahoney, MD, PhD Roswell Park Cancer Institute
Dr Alasdair Patrick Gastroenterologist
 Dr Alasdair Patrick Gastroenterologist Bowel Cancer screening Dr Alasdair Patrick Gastroenterologist MacMurray Gastroenterology Case- Patient for Screening? 62 year old lady Father diagnosed with advanced
Dr Alasdair Patrick Gastroenterologist Bowel Cancer screening Dr Alasdair Patrick Gastroenterologist MacMurray Gastroenterology Case- Patient for Screening? 62 year old lady Father diagnosed with advanced
Alberta Colorectal Cancer Screening Program
 January 14 Alberta Colorectal Cancer Screening Program Standards and Guidelines Version 4.0 of 4.0 Part 1 Standards and Guidelines Draft Document Leaders Dr. Clarence Wong, Medical Lead ACRCSP, Gastroenterologist
January 14 Alberta Colorectal Cancer Screening Program Standards and Guidelines Version 4.0 of 4.0 Part 1 Standards and Guidelines Draft Document Leaders Dr. Clarence Wong, Medical Lead ACRCSP, Gastroenterologist
ENGAGING PRIMARY CARE IN BOWEL SCREENING
 ENGAGING PRIMARY CARE IN BOWEL SCREENING GP GOOD PRACTICE GUIDE SCOTLAND VERSION ENGAGING PRIMARY CARE IN BOWEL SCREENING GP GOOD PRACTICE GUIDE SCOTLAND VERSION CONTENT 2 Background & information on the
ENGAGING PRIMARY CARE IN BOWEL SCREENING GP GOOD PRACTICE GUIDE SCOTLAND VERSION ENGAGING PRIMARY CARE IN BOWEL SCREENING GP GOOD PRACTICE GUIDE SCOTLAND VERSION CONTENT 2 Background & information on the
Colon cancer screening : age 50 or over I'll talk to my doctor about it
 Vaud Colon Cancer Screening Programme Colon cancer screening : age 50 or over I'll talk to my doctor about it Dépistage du cancer du colon Canton de Vaud Contents Help deciding and family doctor 3 Colon
Vaud Colon Cancer Screening Programme Colon cancer screening : age 50 or over I'll talk to my doctor about it Dépistage du cancer du colon Canton de Vaud Contents Help deciding and family doctor 3 Colon
Achieving 80% by 2018: Working Together Can Get Us There. Zachary Gregg, MD Sentara Martha Jefferson April 18, 2016
 Achieving 80% by 2018: Working Together Can Get Us There Zachary Gregg, MD Sentara Martha Jefferson April 18, 2016 1 Prostate 21% Lung & bronchus 14% Colon & rectum 8% Urinary bladder 7% Melanoma of skin
Achieving 80% by 2018: Working Together Can Get Us There Zachary Gregg, MD Sentara Martha Jefferson April 18, 2016 1 Prostate 21% Lung & bronchus 14% Colon & rectum 8% Urinary bladder 7% Melanoma of skin
Be it Resolved that FIT is the Best Way to Screen for Colorectal Cancer DEBATE
 Be it Resolved that FIT is the Best Way to Screen for Colorectal Cancer DEBATE DEBATE Presenters PRESENTATION MODERATOR Dr. Praveen Bansal -MD, CCFP FCFP Regional Primary Care Lead, Integrated Cancer Screening,
Be it Resolved that FIT is the Best Way to Screen for Colorectal Cancer DEBATE DEBATE Presenters PRESENTATION MODERATOR Dr. Praveen Bansal -MD, CCFP FCFP Regional Primary Care Lead, Integrated Cancer Screening,
Bowel Cancer Screening Exploiting science brings better medicine
 Camberley & District Bowel Cancer Screening Exploiting science brings better medicine Prof Stephen P. Halloran World - All Cancers Men Incidence & Mortality (2012) Women Incidence Mortality GLOBOCAN 2012
Camberley & District Bowel Cancer Screening Exploiting science brings better medicine Prof Stephen P. Halloran World - All Cancers Men Incidence & Mortality (2012) Women Incidence Mortality GLOBOCAN 2012
Colorectal Cancer- QI process and clinic success: A Case Study at Atascosa Health Center
 Colorectal Cancer- QI process and clinic success: A Case Study at Atascosa Health Center Kaela Momtselidze Health Systems Manager Primary Care Systems American Cancer Society Sheri Frank Director of Corporate
Colorectal Cancer- QI process and clinic success: A Case Study at Atascosa Health Center Kaela Momtselidze Health Systems Manager Primary Care Systems American Cancer Society Sheri Frank Director of Corporate
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer
 Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
Guidelines for Colonoscopy Surveillance After Screening and Polypectomy: A Consensus Update by the US Multi-Society Task Force on Colorectal Cancer David A. Lieberman, 1 Douglas K. Rex, 2 Sidney J. Winawer,
Socioeconomic and ethnic inequalities in organized colorectal cancer screening participation
 Socioeconomic and ethnic inequalities in organized colorectal cancer screening participation C.M. de Klerk 1, S. Gupta 2, E. Dekker 1, M.L. Essink-Bot 3 1) Department of Gastroenterology and Hepatology,
Socioeconomic and ethnic inequalities in organized colorectal cancer screening participation C.M. de Klerk 1, S. Gupta 2, E. Dekker 1, M.L. Essink-Bot 3 1) Department of Gastroenterology and Hepatology,
NHS Bowel Cancer Screening Programme
 NHS Bowel Cancer Screening Programme Wolverhampton Bowel Cancer Screening Centre Annual Report April 2015 to March 2016 Introduction Bowel cancer is the fourth most common cancer in the UK (2012) accounting
NHS Bowel Cancer Screening Programme Wolverhampton Bowel Cancer Screening Centre Annual Report April 2015 to March 2016 Introduction Bowel cancer is the fourth most common cancer in the UK (2012) accounting
Financial Disclosers
 Slide 1 Colorectal Cancer Screening Jason Hemming, MD NESGNA November 15, 2014 Slide 2 Bio Slide 3 Financial Disclosers I have no actual or potential conflict of interest relation to this presentation
Slide 1 Colorectal Cancer Screening Jason Hemming, MD NESGNA November 15, 2014 Slide 2 Bio Slide 3 Financial Disclosers I have no actual or potential conflict of interest relation to this presentation
Recommendations on Screening for Colorectal Cancer 2016
 Recommendations on Screening for Colorectal Cancer 2016 Canadian Task Force on Preventive Health Care (CTFPHC) Putting Prevention into Practice Canadian Task Force on Preventive Health Care Groupe d étude
Recommendations on Screening for Colorectal Cancer 2016 Canadian Task Force on Preventive Health Care (CTFPHC) Putting Prevention into Practice Canadian Task Force on Preventive Health Care Groupe d étude
Colorectal Cancer Screening
 Colorectal Cancer Screening Colorectal cancer is preventable. Routine screening can reduce deaths through the early diagnosis and removal of pre-cancerous polyps. Screening saves lives, but only if people
Colorectal Cancer Screening Colorectal cancer is preventable. Routine screening can reduce deaths through the early diagnosis and removal of pre-cancerous polyps. Screening saves lives, but only if people
Colorectal Cancer Screening: Cost-Effectiveness and Adverse events October, 2005
 Colorectal Cancer Screening: Cost-Effectiveness and Adverse events October, 2005 David Lieberman MD Chief, Division of Gastroenterology Oregon Health and Science University Portland VAMC Portland, Oregon
Colorectal Cancer Screening: Cost-Effectiveness and Adverse events October, 2005 David Lieberman MD Chief, Division of Gastroenterology Oregon Health and Science University Portland VAMC Portland, Oregon
NHS Bowel Cancer Screening Programmes: Evaluation of pilot of Faecal Immunochemical Test : Final report.
 NHS Bowel Cancer Screening Programmes: Evaluation of pilot of Faecal Immunochemical Test : Final report. Sue Moss, Christopher Mathews Centre for Cancer Prevention, Wolfson Institute, Queen Mary University
NHS Bowel Cancer Screening Programmes: Evaluation of pilot of Faecal Immunochemical Test : Final report. Sue Moss, Christopher Mathews Centre for Cancer Prevention, Wolfson Institute, Queen Mary University
The burden of Colorectal Cancer in Asia. Dr Saunthari Somasundaram
 q The burden of Colorectal Cancer in Asia Dr Saunthari Somasundaram Globocan 2018: Colon Cancer Tomorrow (Incidence) Global Patterns and Trends in Colorectal Cancer Incidence and Mortality Arnold M,Sierra
q The burden of Colorectal Cancer in Asia Dr Saunthari Somasundaram Globocan 2018: Colon Cancer Tomorrow (Incidence) Global Patterns and Trends in Colorectal Cancer Incidence and Mortality Arnold M,Sierra
Colorectal Cancer Screening Guideline Issue Brief Updated May 30 th, 2018
 Colorectal Cancer Screening Guideline Issue Brief Updated May 30 th, 2018 Issue Summary The American Cancer Society has updated its colorectal screening guideline, which have been published in CA: A Journal
Colorectal Cancer Screening Guideline Issue Brief Updated May 30 th, 2018 Issue Summary The American Cancer Society has updated its colorectal screening guideline, which have been published in CA: A Journal
COLORECTAL CANCER SCREENING &THE FECAL IMMUNOCHEMICAL TEST (FIT) MATHEW ESTEY, PHD, FCACB CLINICAL CHEMIST
 MATHEW ESTEY, PHD, FCACB CLINICAL CHEMIST") COLORECTAL CANCER SCREENING &THE FECAL IMMUNOCHEMICAL TEST (FIT) MATHEW ESTEY, PHD, FCACB CLINICAL CHEMIST MATHEW.ESTEY@DYNALIFEDX.COM FACULTY /PRESENTER DISCLOSURE FACULTY: MATHEW ESTEY RELATIONSHIPS
COLORECTAL CANCER SCREENING &THE FECAL IMMUNOCHEMICAL TEST (FIT) MATHEW ESTEY, PHD, FCACB CLINICAL CHEMIST MATHEW.ESTEY@DYNALIFEDX.COM FACULTY /PRESENTER DISCLOSURE FACULTY: MATHEW ESTEY RELATIONSHIPS
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series
 Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Best Practices for Colorectal Cancer Screening March 14, 2018 12:00pm 1:00pm Robert A. Smith, PhD Vice President, Cancer
Learning and Earning with Gateway Professional Education CME/CEU Webinar Series Best Practices for Colorectal Cancer Screening March 14, 2018 12:00pm 1:00pm Robert A. Smith, PhD Vice President, Cancer
MINISTRY OF HEALTH AND LONG-TERM CARE Primary Health Care Team FACT SHEET. New and Enhanced Incentives for Colorectal Cancer Screening
 MINISTRY OF HEALTH AND LONG-TERM CARE Primary Health Care Team FACT SHEET Title: New and Enhanced Incentives for Colorectal Cancer Screening Date: April 2008 The Ontario government is launching Canada's
MINISTRY OF HEALTH AND LONG-TERM CARE Primary Health Care Team FACT SHEET Title: New and Enhanced Incentives for Colorectal Cancer Screening Date: April 2008 The Ontario government is launching Canada's
CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING
 CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING This guideline is designed to assist practitioners by providing the framework for colorectal cancer (CRC) screening, and is not intended to replace
CLINICAL PRACTICE GUIDELINE FOR COLORECTAL CANCER SCREENING This guideline is designed to assist practitioners by providing the framework for colorectal cancer (CRC) screening, and is not intended to replace
Instrument for the assessment of systematic reviews and meta-analysis
 Appendix II Annex II Instruments for the assessment of evidence As detailed in the main body of the methodological appendix (Appendix II, "Description of the methodology utilised for the collection, assessment
Appendix II Annex II Instruments for the assessment of evidence As detailed in the main body of the methodological appendix (Appendix II, "Description of the methodology utilised for the collection, assessment
Outreach Invitations Improve HCC Surveillance Rates: Results Of A Randomized Controlled Trial
 Outreach Invitations Improve HCC Surveillance Rates: Results Of A Randomized Controlled Trial Amit G. Singal MD MS UT Southwestern Medical Center and Parkland Health & Hospital System Dallas, TX, USA 1
Outreach Invitations Improve HCC Surveillance Rates: Results Of A Randomized Controlled Trial Amit G. Singal MD MS UT Southwestern Medical Center and Parkland Health & Hospital System Dallas, TX, USA 1
The choice of methods for Colorectal Cancer Screening; The Dutch experience
 The choice of methods for Colorectal Cancer Screening; The Dutch experience Monique van Leerdam, Gastroenterologist, NKI-AVL, Amsterdam The Netherlands Colorectal cancer CRC 2 nd cause of cancer related
The choice of methods for Colorectal Cancer Screening; The Dutch experience Monique van Leerdam, Gastroenterologist, NKI-AVL, Amsterdam The Netherlands Colorectal cancer CRC 2 nd cause of cancer related
Practical challenges in establishing and running the Czech national colorectal cancer screening programme
 Ústřední vojenská nemocnice - Vojenská fakultní nemocnice Praha 1. lékařská fakulta Univerzity Karlovy Interní klinika Practical challenges in establishing and running the Czech national colorectal cancer
Ústřední vojenská nemocnice - Vojenská fakultní nemocnice Praha 1. lékařská fakulta Univerzity Karlovy Interní klinika Practical challenges in establishing and running the Czech national colorectal cancer
The Current Landscape of Nurse Navigators: Oncology and the Impact on Outcomes
 The Current Landscape of Nurse Navigators: Oncology and the Impact on Outcomes SHERYL RILEY RN, OCN, CMCN DIRECTOR OF CLINICAL SERVICES SAI SYSTEMS SRILEY@SAISYSTEMS.COM 2015 SAI SYSTEMS INTERNATIONAL
The Current Landscape of Nurse Navigators: Oncology and the Impact on Outcomes SHERYL RILEY RN, OCN, CMCN DIRECTOR OF CLINICAL SERVICES SAI SYSTEMS SRILEY@SAISYSTEMS.COM 2015 SAI SYSTEMS INTERNATIONAL
Czech CRC screening program at the point of switch to the population based design
 Military University Hospital First Medical Faculty of Charles University Department of Gastroenterology Czech CRC screening program at the point of switch to the population based design M. Zavoral, S.
Military University Hospital First Medical Faculty of Charles University Department of Gastroenterology Czech CRC screening program at the point of switch to the population based design M. Zavoral, S.
Colon Cancer Screening. A Provider Opinion Survey
 Colon Cancer Screening A Provider Opinion Survey 1. Background Information What is colon cancer? Who needs to be screened? Colorectal Cancer» Presence of abnormal cells in the colon or rectum that divide
Colon Cancer Screening A Provider Opinion Survey 1. Background Information What is colon cancer? Who needs to be screened? Colorectal Cancer» Presence of abnormal cells in the colon or rectum that divide
Promoting Shared Decision Making for Colorectal Cancer Screening in Primary Care. Alison Brenner, PhD MPH
 Promoting Shared Decision Making for Colorectal Cancer Screening in Primary Care Alison Brenner, PhD MPH Background Colon Cancer Colon cancer is the third leading cause of cancer death in the United States
Promoting Shared Decision Making for Colorectal Cancer Screening in Primary Care Alison Brenner, PhD MPH Background Colon Cancer Colon cancer is the third leading cause of cancer death in the United States
80% by 2018: Maximizing the Potential with Colorectal Cancer Screening. Strategic Advice from the Michigan Forum Experts
 80% by 2018: Maximizing the Potential with Colorectal Cancer Screening Strategic Advice from the Michigan Forum Experts Colorectal Cancer Facts, Figures and Issues: A Look at Michigan 2015 4,190 new cases
80% by 2018: Maximizing the Potential with Colorectal Cancer Screening Strategic Advice from the Michigan Forum Experts Colorectal Cancer Facts, Figures and Issues: A Look at Michigan 2015 4,190 new cases
National Colonoscopy Study (NCS) Screening Colonoscopy versus Annual Fecal Occult Blood Test NCT
 Screening Colonoscopy versus Annual Fecal Occult Blood Test NCT") National Colonoscopy Study (NCS) Screening Colonoscopy versus Annual Fecal Occult Blood Test NCT 00102011 Ann Zauber Sidney Winawer, Michael O Brien, John Allen, Andrew Feld, Glenn Mills, Robin Mendelsohn,
National Colonoscopy Study (NCS) Screening Colonoscopy versus Annual Fecal Occult Blood Test NCT 00102011 Ann Zauber Sidney Winawer, Michael O Brien, John Allen, Andrew Feld, Glenn Mills, Robin Mendelsohn,
Colorectal Cancer Screening
 Colorectal Cancer Screening An Integrated Care Pathway of the Collaborative Care Network Subject Matter Expert: Kevin Wolov, DO Pathway Custodian: Pat Czapp, MD First, a Friendly Reminder... This Integrated
Colorectal Cancer Screening An Integrated Care Pathway of the Collaborative Care Network Subject Matter Expert: Kevin Wolov, DO Pathway Custodian: Pat Czapp, MD First, a Friendly Reminder... This Integrated
NHS KINGSTON. Contents
 NHS KINGSTON Contents 1. Background... 2 2. Targets and quality standards... 2 3. Service provision and performance... 3 Uptake... 3 Investigations... 6 Cancer detection... 7 Age extension... 7 4. Quality
NHS KINGSTON Contents 1. Background... 2 2. Targets and quality standards... 2 3. Service provision and performance... 3 Uptake... 3 Investigations... 6 Cancer detection... 7 Age extension... 7 4. Quality
EBI 1 Description: Automated Telephone Calls to Improve Completion of Fecal Occult Blood Testing
 EBI 1 Description: Automated Telephone Calls to Improve Completion of Fecal Occult Blood Testing Description Automated Telephone Calls Improve Completion of Fecal Occult Blood Testing is an automated telephone
EBI 1 Description: Automated Telephone Calls to Improve Completion of Fecal Occult Blood Testing Description Automated Telephone Calls Improve Completion of Fecal Occult Blood Testing is an automated telephone
Prevention of Bowel Cancer: which patients do I send for colonoscopy?
 Prevention of Bowel Cancer: which patients do I send for colonoscopy? Dr Chris Groves Consultant Gastroenterologist and Honorary Senior Lecturer St George s Hospital and Medical School Director, SW London
Prevention of Bowel Cancer: which patients do I send for colonoscopy? Dr Chris Groves Consultant Gastroenterologist and Honorary Senior Lecturer St George s Hospital and Medical School Director, SW London
1 APRIL 2007 TO 31 MARCH
 Public Health Screening Programmes Annual Report 1 APRIL 2007 TO 31 MARCH 2008 Extract: Chapter 3: Planning for the Bowel Screening Programme Public Health Screening Unit Version 1.0 Published: 16 December
Public Health Screening Programmes Annual Report 1 APRIL 2007 TO 31 MARCH 2008 Extract: Chapter 3: Planning for the Bowel Screening Programme Public Health Screening Unit Version 1.0 Published: 16 December
Wellness Coaching for People with Prediabetes
 Wellness Coaching for People with Prediabetes PUBLIC HEALTH RESEARCH, PRACTICE, AND POLICY Volume 12, E207 NOVEMBER 2015 ORIGINAL RESEARCH Wellness Coaching for People With Prediabetes: A Randomized Encouragement
Wellness Coaching for People with Prediabetes PUBLIC HEALTH RESEARCH, PRACTICE, AND POLICY Volume 12, E207 NOVEMBER 2015 ORIGINAL RESEARCH Wellness Coaching for People With Prediabetes: A Randomized Encouragement
PROSPERO International prospective register of systematic reviews
 PROSPERO International prospective register of systematic reviews Prophylactic cranial irradiation in patients with non-small-cell lung cancer: a systematic review and meta-analysis of randomized controlled
PROSPERO International prospective register of systematic reviews Prophylactic cranial irradiation in patients with non-small-cell lung cancer: a systematic review and meta-analysis of randomized controlled
STANDING COMMITTEE ON PUBLIC ACCOUNTS
 Legislative Assembly of Ontario Assemblée législative de l Ontario STANDING COMMITTEE ON PUBLIC ACCOUNTS CANCER SCREENING PROGRAMS (Section 4.01, 2014 Annual Report of the Auditor General of Ontario) 1
Legislative Assembly of Ontario Assemblée législative de l Ontario STANDING COMMITTEE ON PUBLIC ACCOUNTS CANCER SCREENING PROGRAMS (Section 4.01, 2014 Annual Report of the Auditor General of Ontario) 1
Author's response to reviews
 Author's response to reviews Title: Study protocol: Evaluating the effectiveness of GP endorsement on increasing participation in the NHS Bowel Cancer Screening Programme: a feasibility trial Authors:
Author's response to reviews Title: Study protocol: Evaluating the effectiveness of GP endorsement on increasing participation in the NHS Bowel Cancer Screening Programme: a feasibility trial Authors:
IARC Handbook Volume 17: Colorectal Cancer Screening. Béatrice Lauby-Secretan, PhD on behalf of the IARC Working Group for Volume 17
 IARC Handbook Volume 17: Colorectal Cancer Screening Béatrice Lauby-Secretan, PhD on behalf of the IARC Working Group for Volume 17 IARC Handbooks of Cancer Prevention An important part of cancer prevention
IARC Handbook Volume 17: Colorectal Cancer Screening Béatrice Lauby-Secretan, PhD on behalf of the IARC Working Group for Volume 17 IARC Handbooks of Cancer Prevention An important part of cancer prevention
Transforming Hepatitis B Care in Kaiser Permanente Mid-Atlantic States Through a Registry and Coordinator Supported Pathway
 Transforming Hepatitis B Care in Kaiser Permanente Mid-Atlantic States Through a Registry and Coordinator Supported Pathway V3.28.19c Michael Horberg, MD, MAS, FACP, FIDSA Executive Director Research,
Transforming Hepatitis B Care in Kaiser Permanente Mid-Atlantic States Through a Registry and Coordinator Supported Pathway V3.28.19c Michael Horberg, MD, MAS, FACP, FIDSA Executive Director Research,
Systematic reviews and meta-analyses of observational studies (MOOSE): Checklist.
: Checklist.") Systematic reviews and meta-analyses of observational studies (MOOSE): Checklist. MOOSE Checklist Infliximab reduces hospitalizations and surgery interventions in patients with inflammatory bowel disease:
Systematic reviews and meta-analyses of observational studies (MOOSE): Checklist. MOOSE Checklist Infliximab reduces hospitalizations and surgery interventions in patients with inflammatory bowel disease:
Predictive Model for Detection of Colorectal Cancer in Primary Care by Analysis of Complete Blood Counts
 Predictive Model for Detection of Colorectal Cancer in Primary Care by Analysis of Complete Blood Counts Kinar, Y., Kalkstein, N., Akiva, P., Levin, B., Half, E.E., Goldshtein, I., Chodick, G. and Shalev,
Predictive Model for Detection of Colorectal Cancer in Primary Care by Analysis of Complete Blood Counts Kinar, Y., Kalkstein, N., Akiva, P., Levin, B., Half, E.E., Goldshtein, I., Chodick, G. and Shalev,
GENERAL PRACTITIONERS IN THE 1ST LINE OF CANCER PREVENTION
 GENERAL PRACTITIONERS IN THE 1ST LINE OF CANCER PREVENTION Bohumil Seifert Dpt. Of General Practice 1st Faculty of Medicine Charles University in Prague May, 29, 2015 European Colorectal Cancer Days, Brno
GENERAL PRACTITIONERS IN THE 1ST LINE OF CANCER PREVENTION Bohumil Seifert Dpt. Of General Practice 1st Faculty of Medicine Charles University in Prague May, 29, 2015 European Colorectal Cancer Days, Brno
80% by 2018 FORUM II. Workshop: Effectively Using Electronic Health Records. Henry Oliver F
 80% by 2018 FORUM II Workshop: Effectively Using Electronic Health Records Henry Oliver F EHR Best Practices Guide: A look under the hood Michelle Tropper, MPH Clinical Quality Improvement Specialist July
80% by 2018 FORUM II Workshop: Effectively Using Electronic Health Records Henry Oliver F EHR Best Practices Guide: A look under the hood Michelle Tropper, MPH Clinical Quality Improvement Specialist July
Colorectal Cancer Screening
 Colorectal Cancer Screening Colonoscopy is the gold standard for colorectal cancer screening 2 Focus on Colorectal Cancer Screening at Piedmont Healthcare Screening for colorectal cancer saves lives. Of
Colorectal Cancer Screening Colonoscopy is the gold standard for colorectal cancer screening 2 Focus on Colorectal Cancer Screening at Piedmont Healthcare Screening for colorectal cancer saves lives. Of
THE ROLE OF THE CLINICAL CARE TEAM IN COLORECTAL CANCER SCREENING
 THE ROLE OF THE CLINICAL CARE TEAM IN COLORECTAL CANCER SCREENING Dr. Andrea Anderson, MD, FAAFP Director of Family Medicine Unity Health Care Core Faculty National Family Medicine Residency Financial
THE ROLE OF THE CLINICAL CARE TEAM IN COLORECTAL CANCER SCREENING Dr. Andrea Anderson, MD, FAAFP Director of Family Medicine Unity Health Care Core Faculty National Family Medicine Residency Financial
FIT Overview. Objectives 6/23/2014
 ADDS 2014: Plenary 2 FIT Update Clarence Wong, MD FRCPC Associate Professor of Medicine, University of Alberta Provincial Medical Lead, Alberta Colorectal Cancer Screening Program 1 Objectives After this
ADDS 2014: Plenary 2 FIT Update Clarence Wong, MD FRCPC Associate Professor of Medicine, University of Alberta Provincial Medical Lead, Alberta Colorectal Cancer Screening Program 1 Objectives After this
Cancer Control in the Workplace: A Corporate Standard
 Healthy Outcomes Conference, Whistler, BC March 31 April 2, 2009 Cancer Control in the Workplace: A Corporate Standard Dr. Alain Sotto, Hon.BSc, MD, CCFP(EM), FCBOM Chief Physician, Ontario Power Generation
Healthy Outcomes Conference, Whistler, BC March 31 April 2, 2009 Cancer Control in the Workplace: A Corporate Standard Dr. Alain Sotto, Hon.BSc, MD, CCFP(EM), FCBOM Chief Physician, Ontario Power Generation
80% by 2018 FORUM II. Workshop: Implementing Screening Across Community Health Centers. Decatur B
 80% by 2018 FORUM II Workshop: Implementing Screening Across Community Health Centers Decatur B Steps for Increasing Colorectal Cancer Screening Rates: A Manual for Community Health Centers Laura Makaroff,
80% by 2018 FORUM II Workshop: Implementing Screening Across Community Health Centers Decatur B Steps for Increasing Colorectal Cancer Screening Rates: A Manual for Community Health Centers Laura Makaroff,
2012 Chronic Respiratory. Program Evaluation. Our mission is to improve the health and quality of life of our members
 2012 Chronic Respiratory Program Evaluation Our mission is to improve the health and quality of life of our members 2012 Chronic Respiratory Program Evaluation Program Title: Chronic Respiratory Program
2012 Chronic Respiratory Program Evaluation Our mission is to improve the health and quality of life of our members 2012 Chronic Respiratory Program Evaluation Program Title: Chronic Respiratory Program
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care
 Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION: