PIO Treffen Berlin Mammacarcinom
|
|
|
- Raymond Pitts
- 6 years ago
- Views:
Transcription
1 PIO Treffen Berlin 2009 Mammacarcinom
2

3
4 Qualitätssicherungsprojekt Adjuvante Chemotherapie T-Status 8% 92% T 1/2 T 3/4
5 Qualitätssicherungsprojekt Adjuvante Chemotherapie T-Status T-Stadien Therapie T 1/2 (%) T 3/4 (%) FEC 97 3 FEC-Docetaxel EC-Paclitaxel DAC EC-Docetaxel Gesamt 92 8
6 Qualitätssicherungsprojekt Adjuvante Chemotherapie N-Status 14% 7% 44% 35% N 0 N1 (1-3) N2 (4-9) N3 (=10)
7 Qualitätssicherungsprojekt Adjuvante Chemotherapie N-Status FEC FEC 2% 2% 9% 87% N 0 N1 (1-3) N2 (4-9) N3 (=10)
8 Qualitätssicherungsprojekt Adjuvante Chemotherapie N-Status Taxane Taxane 13% 9% 27% 51% N 0 N1 (1-3) N2 (4-9) N3 (=10)
9 Qualitätssicherungsprojekt Adjuvante Chemotherapie N-Status Therapie N 0 (%) 1-3 (%) 4-9 (%) =10 (%) FEC FEC-Docetaxel EC-Paclitaxel DAC EC-Docetaxel Gesamt
10 Qualitätssicherungsprojekt Adjuvante Chemotherapie Zykluszahl 100,0% 90,0% 80,0% 70,0% 60,0% 50,0% 40,0% 30,0% 20,0% 10,0% 0,0% DAC FEC-Docetaxel EC-Docetaxel EC-Paclitaxel FEC tatsächlich verabreichte Zyklenzahl 93,2% 92,7% 91,5% 87,2% 93,8% G-CSF Gabe 81,1% 27,4% 16,9% 26,6% 19,2%
11 Qualitätssicherungsprojekt Adjuvante Chemotherapie Dosisreduktion 18,0% 16,9% 16,0% 14,0% 12,0% 10,0% 8,6% 8,0% 6,0% 4,0% 4,1% 6,4% 3,2% 2,0% 0,0% DAC FEC-Docetaxel EC-Paclitaxel FEC EC-Docetaxel
12 Breast Cancer Mortality Breast cancer mortality, % Peto R. Lancet. 2003;356: yr gain 4.3% (SE 1.1) Logrank 2P < Years Years 0-4 Years 5-9 Year 10+ Anthracycline 4.23 ( ) 3.33 ( ) 2.25 ( ) CMF 4.82 ( ) 3.50 ( ) 3.46 ( ) Rate ratio, from 0.83 SE SE SE 0.18 (O-E) / V / / / 20.1 CMF 35.1% Anthracycline 30.8%
13 NSABP-B11 Copyright (1998) J Natl Cancer Inst. Paik S, et al. J Natl Cancer Inst. 1998;90:
14 NSABP-B11 Copyright (1998) J Natl Cancer Inst. Paik S, et al. J Natl Cancer Inst. 1998;90:
15 NSABP-B11 Outcome erbb-2 Status RR: PAF vs PF P Value PAF vs PF P Value Interaction DFS OS RFS DDFS Negative Positive Negative Positive Negative Positive Negative Positive Copyright (1998) J Natl Cancer Inst. Paik S, et al. J Natl Cancer Inst. 1998;90:
16 NSABP-B15 Copyright (1998) J Natl Cancer Inst. Paik S, et al. J Natl Cancer Inst. 1998;90:
17 HER-2 Negative MA.5 Trial HER-2 Positive Pritchard KI, et al. NEJM. 2006;354: [2006] Massachusetts Medical Society. All rights reserved.
18 Disease-Free Survival Study HR 95% CI Anthracycline Better NSABP B11 NSABP B15 Brussels Milan DBCCG-89-D NCIC MA Total P = Overall 0.71 heterogeneity c25 = 5.3; 1.00 P =.38 heterogeneity c25 = 7.6; P = Test for interaction chi 2 = 13.7; P <.001 Copyright (1998) J Natl Cancer Inst. Gennari A, et al. J Natl Cancer Inst. 2008;100: Nonanthracycline Better P <.0001 P = HER2 positive HER2 negative
19 Overall Survival Study NSABP B11 NSABP B15 GUN3 Milan DBCCG-89-D NCIC MA-5 Total HR Overall 0.73 heterogeneity c25 = 5.2; 1.03 P =.39 heterogeneity c25 = 5.5; P =.36 95% CI Test for interaction chi 2 = 12.0; P <.001 Anthracycline Better HER2 positive Copyright (1998) J Natl Cancer Inst. Gennari A, et al. J Natl Cancer Inst. 2008;100: Nonanthracycline Better P =.056 P <.0001 P =.86 HER2 negative
20 DFS by Treatment MA.5 trial Probability (%) CMF Overexpression of Topo protein P =.01 CEF Probability (%) Normal expression of Topo protein P =.6 CEF CMF Levine MN, et al. J Clin Oncol. 2005;23: Yrs
21 Topo IIa Genamplifikation und nicht HER2 ist verantwortlich für die verbesserte Anthracyclin Sensitivität Die verbesserte Anthracyclin Sensitivität ist NICHT hervorgerufen durch HER2 Überexpression
22 DFS Non-coamplified Topo IIa by Arm: BCIRG 006 Second Interim Analysis 1.0 Disease Free (%) % 90% 83% Patients Events AC Ä T AC Ä TH P < TCH P < % 84% 78% 83% 81% 71% Year From Randomization Slamon D, et al. SABCS Abstract 52.
23 DFS Coamplified Topo IIa by Arm: BCIRG 006 Second Interim Analysis Disease Free (%) % 94% 92% Patients Events AC Ä T AC Ä TH P < TCH P < % 87% 87% 83% 83% 85% Year From Randomization Slamon D, et al. SABCS Abstract 52.
24 TC x 4 vs AC x 4 Reprinted with permission American Society of Clinical Oncology. All rights reserved. Jones SE, et al. J Clin Oncol. 2006;24:
25 DFS by Treatment for Patients With Topo IIa Amplified or Deleted Tumors MA.5 trial Patients (%) CMF Unadjusted P =.07 Adjusted P =.01 CEF Yrs Patients (%) DFS by Treatment for Patients With Normal Topo IIa CMF Unadjusted P =.75 Adjusted P =.56 CEF Yrs O'Malley FP, et al. ASCO Abstract 533.
26 OS by Treatment for Patients With Topo IIa Amplified or Deleted Tumors MA.5 trial OS by Treatment for Patients With Normal Topo IIa 80 CEF 80 CEF Patients (%) Unadjusted P =.06 Adjusted P =.01 CMF Patients (%) Unadjusted P =.41 Adjusted P =.60 CMF Yrs Yrs O'Malley FP, et al. ASCO Abstract 533.
27 Welches ist der beste prediktive Faktor für CEF vs CMF in MA.5? DFS P Value OS P Value HER2/neu Topo IIa protein* Topo IIa gene *Exploratory analysis. Levine MN, et al. J Clin Oncol. 2005;23:
28 Therapeutic Index: Most Recent BCIRG 006 Data AC Ä TH TCH Breast cancer recurrence Breast cancer deaths Grade 3/4 CHF 20 4 Acute leukemia 4* 0 Total *In both anthracycline-based arms.
29 Fig 1. Women aged 66 to 70 years: freedom from congestive heart failure (CHF) by adjuvant chemotherapy type Pinder, M. C. et al. J Clin Oncol; 25: Copyright American Society of Clinical Oncology

30 NSABP B-30: Doxorubicin and Cyclophosphamide Followed by Docetaxel Associated With Best Survival Outcomes vs Concurrent Approaches in Node-Positive EBC
31 NSABP B-30: Doxorubicin and Cyclophosphamide Followed by Docetaxel Associated With Best Survival Outcomes vs Concurrent Approaches in Node-Positive EBC Tumor size: T1-3 Lymph node: N0-1 based on clinical exam = 1 positive node determined by pathologic exam No distant metastases: M0 Established estrogen receptor and progesterone receptor status Radiation therapy plan submitted prior to randomization
32 NSABP B-30: Doxorubicin and Cyclophosphamide Followed by Docetaxel Associated With Best Survival Outcomes vs Concurrent Approaches in Node-Positive EBC I Main Findings Cycles of therapy completed AC Ä T (n = 1748) AC: 99% T: 86% AT (n = 1729): 97% TAC (n = 1740): 97% Patients evaluable for OS and DFS evaluation Intent-to-treat analyses AC Ä T: n = 1753 AT: n = 1753 TAC: n = 1758 Significant increase in OS with AC Ä T vs AT and in DFS with AC Ä T vs AT or TAC Equivalent outcomes for AT and TAC
33 NSABP B-30: Doxorubicin and Cyclophosphamide Followed by Docetaxel Associated With Best Survival Outcomes vs Concurrent Approaches in Node-Positive EBC Distant recurrence most frequent first event among all 3 study arms with significant difference in cumulative incidence between arms (P =.009) AT: n = 280 events TAC: nac Ä T: n = 218 events = 257 events Significant d ifference in cumulative incidence of regional recurrence between treatment arms (P =.02) AC Ä T: n = 16 events AT: n = 22 events TAC: n = 35 events Subgroup analyses of DFS by age, endocrine receptor status, number of lymph nodes, tumor size, hormonal therapy, or menopausal status consistently favored AC Ä T over TAC AC Ä T over AT Grade 3/4 Toxicity, % AC Ä T AT (n = 1749) (n = 1750) TAC (n = 1749) P Value Febrile neutropenia <.0001 Infection
34 NSABP B-30: Doxorubicin and Cyclophosphamide Followed by Docetaxel Associated With Best Survival Outcomes vs Concurrent Approaches in Node-Positive EBC *Among premenopausal women, OS significantly longer in patients with vs without amenorrhea Risk ratio: 0.76 (P =.038) DFS also significantly longer in patients with amenorrhea Risk ratio: 0.70 (P =.00041) Premenopausal women eligible: n = 2445 Follow-up available: n = 2366 Risk lower with amenorrhea across treatment, age, hormonal therapy subgroups
35 NSABP B-30: Doxorubicin and Cyclophosphamide Followed by Docetaxel Associated With Best Survival Outcomes vs Concurrent Approaches in Node-Positive EBC III In women with lymph nodeåpositive early breast cancer, OS with doxorubicin (A) plus cyclophosphamide (C) followed by docetaxel (T) treatment (AC Ä T) Borderline superior OS compared with concurrent combination docetaxel, doxorubicin, cyclophosphamide (TAC) Significantly superior to AT DFS with AC Ä T was significantly superior to TAC and AT Improved DFS and OS with vs without amenorrhea among premenopausal women

36 BCIRG-005: Similar DFS With AC Ä T and TAC in Patients With HER2-Normal, Node-Positive Early Breast Cancer
37 BCIRG-005: Similar DFS With AC Ä T and TAC in Patients With HER2-Normal, Node-Positive Early Breast Cancer Key eligibility criteria Histologically confirmed breast cancer Lymph node positive Tumor stage: T1-3 HER2 normal by central fluorescence in situ hybridization assay = 70 years of age Karnofsky performance score = 80% Definitive surgery with dissection of = 6 axillary lymph nodes = 60 days between surgery and randomization Exclusion criteria [2] Metastatic disease Abnormal hematologic, renal, hepatic, or cardiac function Previous therapy for breast cancer (ie, immunotherapy, hormonal treatment, gene therapy, or chemotherapy) Bilateral, invasive breast cancer Pregnancy Concurrent ovarian hormone replacement therapy AC Ä T (n = 1649) TAC (n = 1649) Median age, yrs Median Karnofsky performance score
38 BCIRG-005: Similar DFS With AC Ä T and TAC in Patients With HER2-Normal, Node-Positive Early Breast Cancer Therapy delivery Completed all planned cycles of therapy AC Ä T: 91% TAC: 94% Median relative dose intensity: 0.99 on both arms DFS and OS outcomes No significant differences between study arms DFS with doxorubicin/cyclophosphamide followed by docetaxel (AC Ä T) equivalent to combination docetaxel, doxorubicin, cyclophosphamide (TAC) in patients with HER2-normal, node-positive early breast cancer Despite higher-dose intensity with AC Ä T vs TAC Higher incidence of febrile neutropenia, increased use of granulocyte colonystimulating factor with TAC Higher incidence of sensory neuropathy, myalgia, nail changes with AC Ä T
39 BCIRG-005: Similar DFS With AC Ä T and TAC in Patients With HER2-Normal, Node-Positive Early Breast Cancer AC Ä T, % TAC, % HR (95% CI) p Value (n = 1649) (n = 1649) DFS ( ).98 OS ( ).37 No difference in DFS among subgroups by number of involved lymph nodes or hormone receptor status (including triple-negative subgroup)

40 Epirubicin, Cyclophosphamide Followed by Docetaxel Improves Survival vs Concurrent 5-Fluorouracil, Epirubicin, Cyclophosphamide in Women With Intermediate Risk Breast Cancer
41 Epirubicin, Cyclophosphamide Followed by Docetaxel Improves Survival vs Concurrent 5-Fluorouracil, Epirubicin, Cyclophosphamide in Women With Intermediate Risk Breast Cancer West German Study Group (WSG) and Arbeitsgemeinschaft Gynäkologische Onkologie (AGO) Mamma Intergroup Study EC-Doc (AM02): randomized, multicenter phase III trial [1] 5-year OS rate 5-year EFS Overall epirubicin, cyclophosphamide followed by docetaxel treatment (EC-Doc)90.2 vs fluorouracil, epirubicin, cyclophosphamide (FEC) HR ( ) EFS rates significantly higher even among patients with hormone receptor positive disease Hormone receptor status Positive 92.5 vs 88.7 HR 1.55 ( ) p.03 Negative 81.8 vs 74.9 HR 1.43 ( ) EC-Doc viable treatment option for patients with early breast cancer and 1-3 involved lymph nodes
42 First Author/Stu dy Picart (Belgian) Type No. of Patients Median FU (years) Antrazykline Hochdosis vs Normaldosis Treatment DFS (%) P OS (%) P N * 8 EC, IV Fumoleau 6 Premenop (FASG 01) ausal N FEC50, IV 8 HEC, IV Bonneterr e 3 (FASG 05) 3 FEC50, IV 3 FEC75, IV N FEC50, IV 6 FEC100, IV
43 Antrazykline Hochdosis vs Normaldosis Budman 7 (CALGB 8541) N+ 1, FAC60, IV Linden 9 (INT-0137) High-risk N or N+ Henderson 8 (CALGB 9344) 6 FAC40, IV FAC30, IV , AC A C intensified N+ 3, AC (60, 75 or 90 mg/m 2 ) paclitaxel x
44 Fig 1. Kaplan-Meier estimates of event-free survival (EFS) for higher-dose epirubicin and cyclophosphamide (HEC) versus lower-dose epirubicin and cyclophosphamide (EC) de Azambuja, E. et al. J Clin Oncol; 27: Copyright American Society of Clinical Oncology
45 Vergleich Antrazykline vs CMF First Author/Stu dy Type No. of Patients Median FU (years) Treatment DFS (%) P OS (%) P Piccart study (Belgian) Bonadonn a (BClin Oncol 22: , 2004) N * 6 CMF, oral 45.39, HEC x CMF N+ (1 3) CMF, IV q3w/1 DOX (up to 12 cycles) 8 EC, IV 39.21; EC x CMF 8 HEC, IV 50.03; HEC x EC 8 CMF, IV 4 DOX Bonadonn a (, 2004A, et al. J Clin Oncol 22: ) N+ (> 3) DOX 8 CMF, IV 49 Figures not specified 57 NS 56 NS 59 NS
46 Levine, Premenopa NCICCTG usal N+ MA5 (Levine MN, Pritchard KI, Bramwell VH, et al. J Clin Oncol 23: , 2005) Colozza, GOIRC (Colozza M, Bisagni G, Mosconi AM, et al. Eur J Cancer 38: , 2002) Martin, GEICAM N (ER ) or N+ High-risk N or N+ 2 CMF, IV q3w CMF, oral CEF120, oral CMF, IV Weekly EPI 4 for 4 months FAC, IV (Martin M, Villar A, Sole-Calvo A, et al. Ann Oncol 14: , 2003) 6 CMF, IV, q3w NS
47 Ejlertsen (Ejlertsen B, Mouridsen HT, Jensen MB, et al. Eur J Cancer 43: , 2007) Coombes, Premenopa ICCG (Coombes usal N+ RC, Bliss JM, Wils J, et al. J Clin Oncol 14:35-45, 1996) Poole, NEAT + BR9601 (Poole CJ, Earl HM, Hiller L, et al. N Engl J Med 355: , 2006) Premenopa 1, FEC, IV HR = 0.84 HR = 0.79 usal N or N+ 9 CMF, IV <.04 < FEC2, IV 5-year 86.6 figures not specified 6 CMF2, IV , EPI 4 76 v v 75 (EPI CMF, oral CMF v CMF) CMF, oral EPI CMF versus CMF <.001 Total, N 2,391 Or <.001 and N+ 4 EPI 4 CMF, IV 8 CMF q3w, IV
48 Fig 1. Meta-analysis of hazard ratios (HR) in trials comparing anthracycline- versus non-anthracyclinebased regimens by HER-2/neu status Pritchard, K. I. et al. J Clin Oncol; 26:
49 Fig 2. Meta-analysis of disease-free survival hazard ratios (HRs) in trials comparing different anthracycline-based regimens by HER-2/neu status Pritchard, K. I. et al. J Clin Oncol; 26:
50 Fig 3. Meta-analysis of disease-free survival hazard ratios (HRs) in trials comparing taxane-containing with non-taxane-containing regimens by HER-2/neu status Pritchard, K. I. et al. J Clin Oncol; 26: Copyright American Society of Clinical Oncology
51 HER2 Positivity Associated With Increased Risk of Recurrence Even in Patients With Small Breast Cancer Tumors Rahkit SABCS 2008 ~ 10% of node-negative invasive breast cancers = 1 cm tested HER2 positive In patients with tumors = 1 cm, HER2 positivity associated with significantly shorter recurrence-free survival (RFS), distant RFS (DRFS) HER2 positivity associated with 2.7-fold increased risk of recurrence in 5 years Suggests potential value of anti-her2 therapy in this patient population Background HER2-positive breast cancer aggressive; associated with poor clinical outcomes Randomized clinical trials demonstrating clinical benefit of trastuzumab with adjuvant chemotherapy in early-stage HER2-positive breast cancer largely excluded node-negative tumors = 1 cm Outcomes in patients with small HER2-positive tumors not well defined Current study determined risk of recurrence with T stage 1a, 1b node-negative, HER2-positive breast cancer Summary of Study Design Data gathered from University of Texas M. D. Anderson Cancer Center Breast Cancer Management System database of node-negative invasive breast cancers Patients diagnosed with T stage 1a, 1b N0M0 breast cancer Tumors = 1 cm Excluded patients treated with adjuvant chemotherapy or trastuzumab Second data set from 2 European institutes used for validation Hormone receptor status assessed using standard immunohistochemistry HER2 status assessed by immunohistochemistry (IHC) or fluorescence in situ hybridization (FISH) IHC: 3+ receptor overexpression FISH: gene copy/cep-17 ratio > 2.0
52 5-year RFS rate: HER2-positive vs HER2-negative patients (77.1% vs 93.7%,; P <.0001) Multiple factors significantly associated with RFS in these patients Factors not significantly associated with DRFS Hormone receptor status (negative vs positive; P =.111) Menopausal status (P =.069) Histology (ductal vs other; P =.882) T stage (1a vs 1b; P =.576) Grade (1/2 vs 3; P =.188) Data from 350 European patients analyzed for validity Patient characteristics Median age: 60 years (range: 29-88) HER2 positive: 6% T stage 1b: 86% Grade 3: 14% 5-year RFS significantly lower in HER2-positive vs HER2-negative patients (87.4% vs 97.0%; P =.043) No significant difference in 5-year DRFS with HER2-positive vs HER2-negative disease (92.3% vs 97.0%; P =.449) Overall 5-year RFS in University of Texas M. D. Anderson Cancer Center patient group: 92.0% Overall 5-year DRFS: 96.2% Reference Rakkhit R, Broglio K, Peintinger F, et al. Significant increased recurrence rates among breast cancer patients with HER2-positive tumors 1 cm or smaller. Program and abstracts of the 31st Annual San Antonio Breast Cancer Symposium; December 10-14, 2008; San Antonio, Texas. Abstract 701.
53 doch behandeln? Wie keine Daten Matthew Ellis, MD, PhD: At our center, we have a single-arm study of 12 treatments of weekly paclitaxel plus trastuzumab as a treatment for the lower-risk spectrum of HER2-positive disease. This important question is not likely to be answered anytime soon because it would take approximately 6000 lower-risk patients to be randomized to treatment with or without trastuzumab, which is nearly impossible to achieve because of lack of funding to conduct such a trial, as well as potential difficulties with acceptance of randomization to no anti-her2 therapy (E. Perez)
54 Tau Expression Correlates With Survival Outcomes in Early Breast Cancer: Analysis of NSABP-B28 SABCS 2008 Retrospective analysis [1] of tissue microarray data from the National Surgical Adjuvant Breast and Bowel Project (NSABP)-B28 randomized phase III trial Summary of Key Conclusions High levels of Tau protein expression correlate with longer DFS and OS in patients with early-stage breast cancer treated with adjuvant anthracycline, paclitaxel, and hormonal therapy No significant interaction between Tau expression and paclitaxel outcomes Background Results on the predictive and prognostic value of Tau inconsistent [2-4] Low Tau protein expression may be associated with decreased responsiveness of estrogen receptor (ER) positive tumors to endocrine therapy Current study sought to evaluate the association of Tau protein expression with survival outcomes in patients with early-stage, node-positive breast cancer receiving adjuvant therapy Summary of Study Design 3060 previously untreated patients with node-positive breast cancer randomized to receive 4 courses of doxorubicin/cyclophosphamide (AC) or AC followed by 4 additional courses of paclitaxel (ACT) Patients with hormone receptor positive tumors also received adjuvant hormonal therapy (tamoxifen) Current study included patients from NSABP-B28 with tissue microarray data (n = 1942; 63%) Tau immunohistochemistry (IHC) results correlated with survival outcomes Main Findings Lack of consensus in results from 2 pathologists 32% of overall IHC results conflicted 8% of Tau-only results conflicted Final consensus scoring indicated that 43% of cancers Tau positive Tau expression significantly more common in ER-positive, progesterone receptor (PgR)-positive, HER2-negative, and low-grade tumors No correlation between Tau positivity and lymph node positivity, age of patient, or tumor size
55 Survival 10 years after randomization significantly higher in Tau-positive compared with Tau-negative tumors OS: P <.0001 DFS: P <.0001 No significant effect of paclitaxel on Tau outcomes In univariate analyses, Tau, ER, HER2 expression, grade, tumor size, nodal status independently and significantly associated with DFS and OS (P <.003) Several factors associated with survival on multivariate analysis DFS Treatment: ACT vs AC (P =.032) Tumor size: < 2 vs > 4 cm (P =.011) Tumor grade: low vs high (P =.0077) Lymph node involvement: = 3 vs > 3 (P <.0001) ER expression: positive vs negative (P =.00047) Tau expression: positive vs negative (P =.018) OS Age: = 49 vs > 60 years (P =.0046) Tumor size: < 2.0 vs cm (P =.014) Tumor grade: low vs intermediate or high (P =.0016) Lymph node involvement: = 3 vs > 3 (P <.0001) ER expression: positive vs negative (P =.0001) Tau expression: positive vs negative (P =.0001) Tau remained significant predictor of survival after adjusting for age, nodal status, histological grade, tumor size Increased survival in Tau-positive patients may have resulted from favorable prognosis for Tau-positive, ER-positive cancers Of Tau-positive cancers, 88% ER positive ~ 40% of ER-positive cancers Tau negative In ER-positive patients, Tau-positive patients had improved survival DFS: P =.0018 OS: P = <.0001 No significant interaction between low Tau expression and Paclitaxel efficacy overall or based on ER status
56 Luminal A Molecular Subtype Associated With Better Prognosis in Invasive, Nonmetastatic Breast Cancer Retrospective molecular analysis of samples from the Nurses Health Study In women with invasive, nonmetastatic breast cancer, luminal A tumors associated with better prognosis than luminal B, HER2 subtype, and basallike tumors Additional unclassifiable subset comparable to basal-like tumors in survival outcomes and may represent additional subtype of basal-like tumors Background Molecular analysis of tumor types and correlation with clinical outcomes could help better tailor therapy to patients Current study compared survival outcomes among various molecular phenotypes in women with invasive, nonmetastatic breast cancer Summary of Study Design Patients (N = 2021) with invasive, nonmetastatic breast cancer from the Nurses Health Study Diagnosed between 1976 and 1996 Tissue samples available for microarray and immunohistochemical analysis Samples classified into 5 subgroups based on molecular characteristics: 1) Luminal A, 2) luminal B, 3) HER, 4) basal like, and 5) not classified Disease Risk of death/recurrence higher for subtypes other than luminal A according to multivariate analysis (adjustments: age, diagnosis time, body mass index, node status, and tumor grade, stage, size) Total deaths: n = 725 Breast cancer deaths: n = 435 Recurrences: n = 463 Reference Dawood S, Collins LC, Connolly JL, et al. Defining breast cancer prognosis based on molecular phenotypes: results from a large cohort study. Program and abstracts of the 31st Annual San Antonio Breast Cancer Symposium; December 10-14, 2008; San Antonio, Texas. Abstract 1068.
57
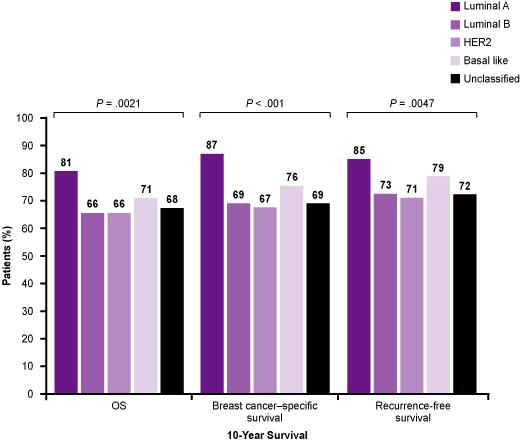
58

59 Correspondence between Molecular Class and Clinicopathological Features of Breast Cancer Sotiriou C and Pusztai L. N Engl J Med 2009;360:

60 Commercially Available Genomic Assays for the Prediction of Clinical Outcome in Patients with Breast Cancer Sotiriou C and Pusztai L. N Engl J Med 2009;360:

61 Molecular Classification, Gene-Expression Signatures, and Clinical Outcome Sotiriou C and Pusztai L. N Engl J Med 2009;360:
62 Vorhersage der Wirksamkeit von Chemotherapie This 30-gene predictor showed higher sensitivity than a clinical predictor that included age, nuclear grade, and ER status (92% vs. 61%). It also correctly identified 92% of the patients who achieved a pathologic complete response. The positive predictive value of the pharmacogenomic signature was a modest 52%, but its negative predictive value was 96%.
63
64
Nadia Harbeck Breast Center University of Cologne, Germany
 Evidence in Favor of Taxane Based Combinations and No Anthracycline in Adjuvant and Metastatic Settings Nadia Harbeck Breast Center University of Cologne, Germany Evidence in Favor of Taxane Based Combinations
Evidence in Favor of Taxane Based Combinations and No Anthracycline in Adjuvant and Metastatic Settings Nadia Harbeck Breast Center University of Cologne, Germany Evidence in Favor of Taxane Based Combinations
Non-Anthracycline Adjuvant Therapy: When to Use?
 Northwestern University Feinberg School of Medicine Non-Anthracycline Adjuvant Therapy: When to Use? William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley Center for
Northwestern University Feinberg School of Medicine Non-Anthracycline Adjuvant Therapy: When to Use? William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley Center for
Evolving Insights into Adjuvant Chemotherapy. Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology
 Evolving Insights into Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic
Evolving Insights into Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic
Neo-adjuvant and adjuvant treatment for HER-2+ breast cancer
 Neo-adjuvant and adjuvant treatment for HER-2+ breast cancer Angelo Di Leo «Sandro Pitigliani» Medical Oncology Unit Hospital of Prato Istituto Toscano Tumori Prato, Italy NOAH: Phase III, Open-Label Trial
Neo-adjuvant and adjuvant treatment for HER-2+ breast cancer Angelo Di Leo «Sandro Pitigliani» Medical Oncology Unit Hospital of Prato Istituto Toscano Tumori Prato, Italy NOAH: Phase III, Open-Label Trial
Considerations in Adjuvant Chemotherapy. Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology
 Considerations in Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic Treatment
Considerations in Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology 80 70 60 50 40 30 20 10 0 EBCTCG 2005/6 Overview Control Arms with No Systemic Treatment
Adjuvant Chemotherapy + Trastuzumab
 Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Adjuvant Chemotherapy + Trastuzumab (Optimal Drugs / Dosage / Trastuzumab) Adjuvant Chemotherapy (Optimal Drugs / Optimal Dosage
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Adjuvant Chemotherapy + Trastuzumab (Optimal Drugs / Dosage / Trastuzumab) Adjuvant Chemotherapy (Optimal Drugs / Optimal Dosage
OPTIMIZING NONANTHRACYLINES FOR EARLY BREAST CANCER. Stephen E. Jones, M.D. US Oncology Research, McKesson Specialty Health The Woodlands, Tx
 OPTIMIZING NONANTHRACYLINES FOR EARLY BREAST CANCER Stephen E. Jones, M.D. US Oncology Research, McKesson Specialty Health The Woodlands, Tx ANTHRACYCLINES AND TAXANES ARE COMMONLY USED USED IN MOST REGIMENS
OPTIMIZING NONANTHRACYLINES FOR EARLY BREAST CANCER Stephen E. Jones, M.D. US Oncology Research, McKesson Specialty Health The Woodlands, Tx ANTHRACYCLINES AND TAXANES ARE COMMONLY USED USED IN MOST REGIMENS
Postoperative Adjuvant Chemotherapies. Stefan Aebi Luzerner Kantonsspital
 Postoperative Adjuvant Chemotherapies Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Does Chemotherapy Work in Older Patients? ER : Chemotherapy vs nil Age
Postoperative Adjuvant Chemotherapies Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Does Chemotherapy Work in Older Patients? ER : Chemotherapy vs nil Age
Anthracyclines for Breast Cancer? Are Adjuvant Anthracyclines Dispensible? Needs to be Answered in a Large Prospective Trial
 Anthracyclines for Breast Cancer? Are Adjuvant Anthracyclines Dispensible? Needs to be Answered in a Large Prospective Trial Joanne L. Blum, MD, PhD Baylor-Sammons Cancer Dallas, TX Early Breast Cancer
Anthracyclines for Breast Cancer? Are Adjuvant Anthracyclines Dispensible? Needs to be Answered in a Large Prospective Trial Joanne L. Blum, MD, PhD Baylor-Sammons Cancer Dallas, TX Early Breast Cancer
EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY. Dr. Carlos Garbino
 EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY Dr. Carlos Garbino EARLY BREAST CANCER ADJUVANT CHEMOTHERAPY SUSTANTIVE DIFFICULTIES FOR A WORLDWIDE APPLICABILITY DUE TO IMPORTANT INEQUALITIES + IN DIFFERENT
EARLY STAGE BREAST CANCER ADJUVANT CHEMOTHERAPY Dr. Carlos Garbino EARLY BREAST CANCER ADJUVANT CHEMOTHERAPY SUSTANTIVE DIFFICULTIES FOR A WORLDWIDE APPLICABILITY DUE TO IMPORTANT INEQUALITIES + IN DIFFERENT
Treatment of HER-2 positive breast cancer
 EJC SUPPLEMENTS 6 (2008) 21 25 available at www.sciencedirect.com journal homepage: www.ejconline.com Treatment of HER-2 positive breast cancer Matteo Clavarezza, Marco Venturini * Ospedale Sacro Cuore
EJC SUPPLEMENTS 6 (2008) 21 25 available at www.sciencedirect.com journal homepage: www.ejconline.com Treatment of HER-2 positive breast cancer Matteo Clavarezza, Marco Venturini * Ospedale Sacro Cuore
Non-anthracycline Adjuvant regimens in Early Breast Cancer. Yeesoo Chae, MD, PhD Medical Oncology Kyungpook National University Medical Center
 Non-anthracycline Adjuvant regimens in Early Breast Cancer Yeesoo Chae, MD, PhD Medical Oncology Kyungpook National University Medical Center Contents Role of Anthracyclines in adjuvant treatment EBCTCG2012
Non-anthracycline Adjuvant regimens in Early Breast Cancer Yeesoo Chae, MD, PhD Medical Oncology Kyungpook National University Medical Center Contents Role of Anthracyclines in adjuvant treatment EBCTCG2012
SANDRA M. SWAIN. Washington Cancer Institute, Washington, District of Columbia, USA
 The Oncologist Early-Stage Breast Cancer: Clinical Update Chemotherapy: Updates and New Perspectives SANDRA M. SWAIN Washington Cancer Institute, Washington, District of Columbia, USA Key Words. Breast
The Oncologist Early-Stage Breast Cancer: Clinical Update Chemotherapy: Updates and New Perspectives SANDRA M. SWAIN Washington Cancer Institute, Washington, District of Columbia, USA Key Words. Breast
SANDRA M. SWAIN. Washington Cancer Institute, Washington, District of Columbia, USA
 The Oncologist Chemotherapy: Updates and New Perspectives SANDRA M. SWAIN Washington Cancer Institute, Washington, District of Columbia, USA Key Words. Breast cancer Chemotherapy Taxane Trastuzumab Ki-67
The Oncologist Chemotherapy: Updates and New Perspectives SANDRA M. SWAIN Washington Cancer Institute, Washington, District of Columbia, USA Key Words. Breast cancer Chemotherapy Taxane Trastuzumab Ki-67
Existe-t-il un sous groupe à risque qui pourrait bénéficier d une modification de la durée de traitement par trastuzumab? X. Pivot CHRU De Besançon
 Existe-t-il un sous groupe à risque qui pourrait bénéficier d une modification de la durée de traitement par trastuzumab? X. Pivot CHRU De Besançon In 25 results of 4 Adjuvant Herceptin trials have definitively
Existe-t-il un sous groupe à risque qui pourrait bénéficier d une modification de la durée de traitement par trastuzumab? X. Pivot CHRU De Besançon In 25 results of 4 Adjuvant Herceptin trials have definitively
DR. BOMAN N. DHABHAR Consulting Oncologist Jaslok Hospital, Fortis Hospital Mulund, Wockhardt Hospital Mumbai & BND Onco Centre INDIA
 Recent Advances of Docetaxel in Management of Breast Cancer DR. BOMAN N. DHABHAR Consulting Oncologist Jaslok Hospital, Fortis Hospital Mulund, Wockhardt Hospital Mumbai & BND Onco Centre INDIA 1 ADJUVANT
Recent Advances of Docetaxel in Management of Breast Cancer DR. BOMAN N. DHABHAR Consulting Oncologist Jaslok Hospital, Fortis Hospital Mulund, Wockhardt Hospital Mumbai & BND Onco Centre INDIA 1 ADJUVANT
新竹馬偕紀念醫院癌症中心 乳癌化學治療藥物處方
 新竹馬偕紀念醫院癌症中心 乳癌化學治療藥物處方 文件修訂記錄 修正次數 修正日期 修正版別 修 改 內 容 1 2011.04.07 1.0 初次訂定 2 2013.05.08 2.0 修訂 3 2013.04.30 3.0 修訂 :Triple-Negative Breast Cancer 處方 新增 :Neoadjuvant-p7~8 4 2014.04.29 4.0 修訂 :FEC + Trastuzumab
新竹馬偕紀念醫院癌症中心 乳癌化學治療藥物處方 文件修訂記錄 修正次數 修正日期 修正版別 修 改 內 容 1 2011.04.07 1.0 初次訂定 2 2013.05.08 2.0 修訂 3 2013.04.30 3.0 修訂 :Triple-Negative Breast Cancer 處方 新增 :Neoadjuvant-p7~8 4 2014.04.29 4.0 修訂 :FEC + Trastuzumab
30 TH ANNUAL SAN ANTONIO BREAST CANCER SYMPOSIUM (SABCS) NEW ADVANCES IN THE TREATMENT OF BREAST CANCER
 NEW ADVANCES IN THE TREATMENT OF BREAST CANCER") EDUCATIONAL HIGHLIGHTS FROM DATA PRESENTED AT THE 30 TH ANNUAL SAN ANTONIO BREAST CANCER SYMPOSIUM (SABCS) NEW ADVANCES IN THE TREATMENT OF BREAST CANCER DECEMBER 13 16, 2007, SAN ANTONIO, TX, USA 2 CONTENTS
EDUCATIONAL HIGHLIGHTS FROM DATA PRESENTED AT THE 30 TH ANNUAL SAN ANTONIO BREAST CANCER SYMPOSIUM (SABCS) NEW ADVANCES IN THE TREATMENT OF BREAST CANCER DECEMBER 13 16, 2007, SAN ANTONIO, TX, USA 2 CONTENTS
Best of San Antonio 2008
 Best of San Antonio 2008 Ellie Guardino, MD/PhD Assistant Professor Stanford University BIG 1 98: a randomized double blind phase III study evaluating letrozole and tamoxifen given in sequence as adjuvant
Best of San Antonio 2008 Ellie Guardino, MD/PhD Assistant Professor Stanford University BIG 1 98: a randomized double blind phase III study evaluating letrozole and tamoxifen given in sequence as adjuvant
Sustained benefits for women with HER2-positive early breast cancer JORGE MADRID BIG GOCCHI PROTOCOLO HERA
 Sustained benefits for women with HER2-positive early breast cancer JORGE MADRID BIG GOCCHI PROTOCOLO HERA The fascinating history of Herceptin 1981 1985 1987 1990 1992 1998 2000 2005 2006 2008 2011 Murine
Sustained benefits for women with HER2-positive early breast cancer JORGE MADRID BIG GOCCHI PROTOCOLO HERA The fascinating history of Herceptin 1981 1985 1987 1990 1992 1998 2000 2005 2006 2008 2011 Murine
Breast Cancer Earlier Disease. Stefan Aebi Luzerner Kantonsspital
 Breast Cancer Earlier Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Switzerland Breast Cancer Earlier Disease Diagnosis and Prognosis Local Therapy Surgery Radiation therapy Adjuvant
Breast Cancer Earlier Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Switzerland Breast Cancer Earlier Disease Diagnosis and Prognosis Local Therapy Surgery Radiation therapy Adjuvant
Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers
 日大医誌 75 (1): 10 15 (2016) 10 Original Article Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers Naotaka Uchida 1), Yasuki Matsui 1), Takeshi Notsu 1) and Manabu
日大医誌 75 (1): 10 15 (2016) 10 Original Article Implications of Progesterone Receptor Status for the Biology and Prognosis of Breast Cancers Naotaka Uchida 1), Yasuki Matsui 1), Takeshi Notsu 1) and Manabu
Review Recent advances in systemic therapy Advances in adjuvant systemic chemotherapy of early breast cancer Sara López-Tarruella and Miguel Martín
 Review Recent advances in systemic therapy Advances in adjuvant systemic chemotherapy of early breast cancer Sara López-Tarruella and Miguel Martín Medical Oncology Department, Clínico San Carlos Hospital,
Review Recent advances in systemic therapy Advances in adjuvant systemic chemotherapy of early breast cancer Sara López-Tarruella and Miguel Martín Medical Oncology Department, Clínico San Carlos Hospital,
Evolving Insights into Adjuvant Chemotherapy. Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology
 Evolving Insights into Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology Dilemmas in Adjuvant Chemotherapy Is adjuvant chemotherapy effective in ER+
Evolving Insights into Adjuvant Chemotherapy Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology US Oncology Dilemmas in Adjuvant Chemotherapy Is adjuvant chemotherapy effective in ER+
Toxicities of Chemotherapy Regimens used in Early Breast Cancer
 Toxicities of Chemotherapy Regimens used in Early Breast Cancer CERCIT Workshop February 17, 2012 Carlos H Barcenas, M.D., M.S. Fellow Hematology-Oncology MD Anderson Cancer Center CERCIT Scholar Outline
Toxicities of Chemotherapy Regimens used in Early Breast Cancer CERCIT Workshop February 17, 2012 Carlos H Barcenas, M.D., M.S. Fellow Hematology-Oncology MD Anderson Cancer Center CERCIT Scholar Outline
Adjuvant chemotherapy of breast cancer
 Journal of BUON 10: 175-180, 2005 2005 Zerbinis Medical Publications. Printed in Greece REVIEW ARTICLE Adjuvant chemotherapy of breast cancer S. Bešlija Department of Medical Oncology, Institute of Oncology,
Journal of BUON 10: 175-180, 2005 2005 Zerbinis Medical Publications. Printed in Greece REVIEW ARTICLE Adjuvant chemotherapy of breast cancer S. Bešlija Department of Medical Oncology, Institute of Oncology,
Key Words. Adjuvant therapy Breast cancer Taxanes Anthracyclines
 The Oncologist Mayo Clinic Hematology/Oncology Reviews Adjuvant Therapy for Breast Cancer: Recommendations for Management Based on Consensus Review and Recent Clinical Trials BETTY A. MINCEY, a,b FRANCES
The Oncologist Mayo Clinic Hematology/Oncology Reviews Adjuvant Therapy for Breast Cancer: Recommendations for Management Based on Consensus Review and Recent Clinical Trials BETTY A. MINCEY, a,b FRANCES
Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012
 Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology, Emory
Review of adjuvant and neo-adjuvant abstracts from SABCS 2011 January 7 th 2012 Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology, Emory
Adjuvant Chemotherapy TNBC & HER2 Subtype
 Adjuvant Chemotherapy TNBC & HER2 Subtype 2015.08.15 Gun Min Kim Yonsei Cancer Center Division of Medical Oncology Department of Internal Medicine Yonsei University College of Medicine gmkim77@yuhs.ac
Adjuvant Chemotherapy TNBC & HER2 Subtype 2015.08.15 Gun Min Kim Yonsei Cancer Center Division of Medical Oncology Department of Internal Medicine Yonsei University College of Medicine gmkim77@yuhs.ac
Adjuvan Chemotherapy in Breast Cancer
 Adjuvan Chemotherapy in Breast Cancer Prof Dr Adnan Aydıner Istanbul University, Oncology Institute aa1 Slide 1 aa1 adnan aydiner; 17.02.2008 15-Year Reductions in Recurrence and Disease-Specific Mortality
Adjuvan Chemotherapy in Breast Cancer Prof Dr Adnan Aydıner Istanbul University, Oncology Institute aa1 Slide 1 aa1 adnan aydiner; 17.02.2008 15-Year Reductions in Recurrence and Disease-Specific Mortality
The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now?
 as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now?") 1 The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now? Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program
1 The Role of Pathologic Complete Response (pcr) as a Surrogate Marker for Outcomes in Breast Cancer: Where Are We Now? Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program
Non-anthracycline Adjuvant regimens in N(-) Early Breast Cancer. Yeesoo Chae, MD, PhD Medical Oncology Kyungpook National University Medical Center
 Early Breast Cancer. Yeesoo Chae, MD, PhD Medical Oncology Kyungpook National University Medical Center") Non-anthracycline Adjuvant regimens in N(-) Early Breast Cancer Yeesoo Chae, MD, PhD Medical Oncology Kyungpook National University Medical Center Case: Clinical history F/45, Premenopause C/C: Rt. Palpable
Non-anthracycline Adjuvant regimens in N(-) Early Breast Cancer Yeesoo Chae, MD, PhD Medical Oncology Kyungpook National University Medical Center Case: Clinical history F/45, Premenopause C/C: Rt. Palpable
III Congreso Internacional de Oncologia del Interior XII Jornadas de Oncologia del Interior Cordoba Argentina. Farmacogenomica y Cancer de Mama
 III Congreso Internacional de Oncologia del Interior XII Jornadas de Oncologia del Interior Cordoba Argentina Farmacogenomica y Cancer de Mama Vicente Valero, M.D., F.A.C.P. Professor of Medicine Deputy
III Congreso Internacional de Oncologia del Interior XII Jornadas de Oncologia del Interior Cordoba Argentina Farmacogenomica y Cancer de Mama Vicente Valero, M.D., F.A.C.P. Professor of Medicine Deputy
Novel Preoperative Therapies for HER2-Positive Breast Cancer. Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center
 Novel Preoperative Therapies for HER2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center Key Findings to Date in the Neoadjuvant Therapy of HER2+
Novel Preoperative Therapies for HER2-Positive Breast Cancer Debu Tripathy, MD University of Southern California Norris Comprehensive Cancer Center Key Findings to Date in the Neoadjuvant Therapy of HER2+
Herceptin Pivotal Studies
 Herceptin Pivotal Studies Nuhad K Ibrahim, MD, FACP Associate Professor of Medicine Breast Medical Oncology Department MD Anderson Cancer Center Houston, TX, USAE-mail: nibrahim@mdanderson.org Herceptin
Herceptin Pivotal Studies Nuhad K Ibrahim, MD, FACP Associate Professor of Medicine Breast Medical Oncology Department MD Anderson Cancer Center Houston, TX, USAE-mail: nibrahim@mdanderson.org Herceptin
BIOLOGICAL THERAPIES FOR BREAST CANCER Updates from the 2005 San Antonio Breast Cancer Symposium
 Emerging trends and recommendations BIOLOGICAL THERAPIES FOR BREAST CANCER Updates from the 2005 San Antonio Breast Cancer Symposium Joseph Ragaz, MD, FRCPC Top-line summary Here, Oncology Exchange presents
Emerging trends and recommendations BIOLOGICAL THERAPIES FOR BREAST CANCER Updates from the 2005 San Antonio Breast Cancer Symposium Joseph Ragaz, MD, FRCPC Top-line summary Here, Oncology Exchange presents
Oncotype DX testing in node-positive disease
 Should gene array assays be routinely used in node positive disease? Yes Christy A. Russell, MD University of Southern California Oncotype DX testing in node-positive disease 1 Validity of the Oncotype
Should gene array assays be routinely used in node positive disease? Yes Christy A. Russell, MD University of Southern California Oncotype DX testing in node-positive disease 1 Validity of the Oncotype
CASE STUDIES CLINICAL CASE SCENARIOS. Matthew J. Ellis, MD, PhD
 CLINICAL CASE SCENARIOS Matthew J. Ellis, MD, PhD Clinicians face daily challenges in the management of individual patients with breast cancer who demonstrate different characteristics in terms of estrogen
CLINICAL CASE SCENARIOS Matthew J. Ellis, MD, PhD Clinicians face daily challenges in the management of individual patients with breast cancer who demonstrate different characteristics in terms of estrogen
8/8/2011. PONDERing the Need to TAILOR Adjuvant Chemotherapy in ER+ Node Positive Breast Cancer. Overview
 Overview PONDERing the Need to TAILOR Adjuvant in ER+ Node Positive Breast Cancer Jennifer K. Litton, M.D. Assistant Professor The University of Texas M. D. Anderson Cancer Center Using multigene assay
Overview PONDERing the Need to TAILOR Adjuvant in ER+ Node Positive Breast Cancer Jennifer K. Litton, M.D. Assistant Professor The University of Texas M. D. Anderson Cancer Center Using multigene assay
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint
 Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
Assessment of Risk Recurrence: Adjuvant Online, OncotypeDx & Mammaprint William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center of Northwestern University Classical
Point of View on Early Triple Negative
 Point of View on Early Triple Negative Valentina Rossi, MD UOSD Oncologia dei Tumori della Mammella Azienda Ospedaliera S.Camillo-Forlanini VRossi@scamilloforlanini.rm.it Outline Neoadjuvant Setting IPSY-2
Point of View on Early Triple Negative Valentina Rossi, MD UOSD Oncologia dei Tumori della Mammella Azienda Ospedaliera S.Camillo-Forlanini VRossi@scamilloforlanini.rm.it Outline Neoadjuvant Setting IPSY-2
Adjuvant Chemotherapy for Elderly Women with Breast Cancer: Matti S. Aapro, M.D. IMO Clinique de Genolier Switzerland
 SIOG Berlin October 2009 Adjuvant Chemotherapy for Elderly Women with Breast Cancer: Immediate Benefit and Long-Term Risk Matti S. Aapro, M.D. IMO Clinique de Genolier Switzerland 1 2 BACKGROUND MESSAGE
SIOG Berlin October 2009 Adjuvant Chemotherapy for Elderly Women with Breast Cancer: Immediate Benefit and Long-Term Risk Matti S. Aapro, M.D. IMO Clinique de Genolier Switzerland 1 2 BACKGROUND MESSAGE
Is adjuvant chemotherapy necessary for Luminal A-like breast cancer?
 JBUON 2018; 23(4): 877-882 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Is adjuvant chemotherapy necessary for Luminal A-like breast cancer?
JBUON 2018; 23(4): 877-882 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Is adjuvant chemotherapy necessary for Luminal A-like breast cancer?
Clinical Expert Submission Template
 Clinical Expert Submission Template Thank you for agreeing to give us a personal statement on your view of the technology and the way it should be used in the NHS. Health care professionals can provide
Clinical Expert Submission Template Thank you for agreeing to give us a personal statement on your view of the technology and the way it should be used in the NHS. Health care professionals can provide
Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives
 Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives Ian Krop Dana-Farber Cancer Institute Harvard Medical School Inchon 2018 Adjuvant Trastuzumab Improves Outcomes in HER2+ Breast
Biomarkers for HER2-directed Therapies : Past Failures and Future Perspectives Ian Krop Dana-Farber Cancer Institute Harvard Medical School Inchon 2018 Adjuvant Trastuzumab Improves Outcomes in HER2+ Breast
Early Stage Disease. Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center
 SABCS 2014: Early Stage Disease Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center Topics for Discussion Chemotherapy plus 10
SABCS 2014: Early Stage Disease Hope S. Rugo, MD Professor of Medicine Director Breast Oncology and Clinical Trials Education UCSF Comprehensive Cancer Center Topics for Discussion Chemotherapy plus 10
Adjuvant chemotherapy in older breast cancer patients: how to decide?
 Adjuvant chemotherapy in older breast cancer patients: how to decide? H. Wildiers University Hospitals Leuven Belgium Wildiers H, Kunkler I, Lancet Oncol 2007 Biganzoli L, Wildiers H, Lancet Oncol. 2012
Adjuvant chemotherapy in older breast cancer patients: how to decide? H. Wildiers University Hospitals Leuven Belgium Wildiers H, Kunkler I, Lancet Oncol 2007 Biganzoli L, Wildiers H, Lancet Oncol. 2012
Common disease 175,000 new cases/year 44,000 deaths/year Less than 10% with newly diagnosed at presentation have stage IV disease Chronic disease,
 Chemotherapy for Metastatic Breast Cancer: Recent Results HARMESH R. NAIK, MD. Karmanos Cancer Institute and St. Mary Hospital Metastatic breast cancer (MBC) Common disease 175,000 new cases/year 44,000
Chemotherapy for Metastatic Breast Cancer: Recent Results HARMESH R. NAIK, MD. Karmanos Cancer Institute and St. Mary Hospital Metastatic breast cancer (MBC) Common disease 175,000 new cases/year 44,000
HER2-positive Breast Cancer
 HER2-positive Breast Cancer Multiple choices what to use when? Thomas Ruhstaller Brustzentrum St. Gallen Adjuvant setting NCIC MA5 N Engl J Med 06, 2103 6 x CEF can 6 x CMF oral HER2 + pg schlecht in allen
HER2-positive Breast Cancer Multiple choices what to use when? Thomas Ruhstaller Brustzentrum St. Gallen Adjuvant setting NCIC MA5 N Engl J Med 06, 2103 6 x CEF can 6 x CMF oral HER2 + pg schlecht in allen
Positive HER-2 tumor. How to incorporate the new drugs into neoadjuvance
 Oncology Department Vall d Hebron University Hospital Barcelona. Spain Positive HER-2 tumor. How to incorporate the new drugs into neoadjuvance Javier Cortés June/2013 MD Anderson experience Buzdar et
Oncology Department Vall d Hebron University Hospital Barcelona. Spain Positive HER-2 tumor. How to incorporate the new drugs into neoadjuvance Javier Cortés June/2013 MD Anderson experience Buzdar et
Adjuvant Systemic Therapy in Early Stage Breast Cancer
 Adjuvant Systemic Therapy in Early Stage Breast Cancer Julie R. Gralow, M.D. Director, Breast Medical Oncology Jill Bennett Endowed Professor of Breast Cancer Professor, Global Health University of Washington
Adjuvant Systemic Therapy in Early Stage Breast Cancer Julie R. Gralow, M.D. Director, Breast Medical Oncology Jill Bennett Endowed Professor of Breast Cancer Professor, Global Health University of Washington
SYSTEMIC TREATMENT OF TRIPLE NEGATIVE BREAST CANCER
 SYSTEMIC TREATMENT OF TRIPLE NEGATIVE BREAST CANCER Sunil Shrestha 1*, Ji Yuan Yang, Li Shuang and Deepika Dhakal Clinical School of Medicine, Yangtze University, Jingzhou, Hubei Province, PR. China Department
SYSTEMIC TREATMENT OF TRIPLE NEGATIVE BREAST CANCER Sunil Shrestha 1*, Ji Yuan Yang, Li Shuang and Deepika Dhakal Clinical School of Medicine, Yangtze University, Jingzhou, Hubei Province, PR. China Department
Supplementary appendix
 Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Cortazar P, Zhang L, Untch M, et al. Pathological
Supplementary appendix This appendix formed part of the original submission and has been peer reviewed. We post it as supplied by the authors. Supplement to: Cortazar P, Zhang L, Untch M, et al. Pathological
Locally Advanced Breast Cancer: Systemic and Local Therapy
 Locally Advanced Breast Cancer: Systemic and Local Therapy Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
Locally Advanced Breast Cancer: Systemic and Local Therapy Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
Treatment of Early Stage HER2-positive Breast Cancer (One size does not fit all)
") Treatment of Early Stage HER2-positive Breast Cancer (One size does not fit all) 8 November 2014 Edward H. Romond, M.D. Professor of Medicine Lucille Parker Markey Cancer Center University of Kentucky
Treatment of Early Stage HER2-positive Breast Cancer (One size does not fit all) 8 November 2014 Edward H. Romond, M.D. Professor of Medicine Lucille Parker Markey Cancer Center University of Kentucky
Oncologist. The. A New Look at Node-Negative Breast Cancer. The Oncologist 2011;16(suppl 1):51 60
:51 60") The Oncologist A New Look at Node-Negative Breast Cancer NADIA HARBECK, a CHRISTOPH THOMSSEN b a Breast Center, University of Cologne, Cologne, Germany; b Frauenklinik der Universitaet Halle, Saale, Germany
The Oncologist A New Look at Node-Negative Breast Cancer NADIA HARBECK, a CHRISTOPH THOMSSEN b a Breast Center, University of Cologne, Cologne, Germany; b Frauenklinik der Universitaet Halle, Saale, Germany
Does HER2/neu overexpression in breast cancer influence adjuvant chemotherapy and hormonal therapy choices by Ontario physicians? A physician survey
 MYERS et al. ORIGINAL ARTICLE Does HER2/neu overexpression in breast cancer influence adjuvant chemotherapy and hormonal therapy choices by Ontario physicians? A physician survey J.A. Myers MD FRCPC, G.
MYERS et al. ORIGINAL ARTICLE Does HER2/neu overexpression in breast cancer influence adjuvant chemotherapy and hormonal therapy choices by Ontario physicians? A physician survey J.A. Myers MD FRCPC, G.
Changing Perceptions of Early-Stage Breast Cancer: Contributions from Histopathology and Biology A New Look at Node-Negative Breast Cancer
 The Oncologist Changing Perceptions of Early-Stage Breast Cancer: Contributions from Histopathology and Biology A New Look at Node-Negative Breast Cancer NADIA HARBECK, a CHRISTOPH THOMSSEN b a Breast
The Oncologist Changing Perceptions of Early-Stage Breast Cancer: Contributions from Histopathology and Biology A New Look at Node-Negative Breast Cancer NADIA HARBECK, a CHRISTOPH THOMSSEN b a Breast
Early and locally advanced breast cancer: diagnosis and management
 National Institute for Health and Care Excellence Final Early and locally advanced breast cancer: diagnosis and management [E] Evidence reviews for adjuvant chemotherapy NICE guideline NG101 Evidence reviews
National Institute for Health and Care Excellence Final Early and locally advanced breast cancer: diagnosis and management [E] Evidence reviews for adjuvant chemotherapy NICE guideline NG101 Evidence reviews
Adjuvant systemic therapies in women with operable breast cancer: A daily medical practice in a single institution
 Turkish Journal of Cancer Volume 35, No.3, 2005 123 Adjuvant systemic therapies in women with operable breast cancer: A daily medical practice in a single institution B NNAZ DEM RKAN 1, LKNUR B LKAY GÖRKEM
Turkish Journal of Cancer Volume 35, No.3, 2005 123 Adjuvant systemic therapies in women with operable breast cancer: A daily medical practice in a single institution B NNAZ DEM RKAN 1, LKNUR B LKAY GÖRKEM
Cáncer de mama HER2+/RE+ vs HER2+/RE : Una misma enfermedad? Dra E. Ciruelos Departamento de Oncología Médica Hospital Universitario 12 de Octubre
 Cáncer de mama HER2+/RE+ vs HER2+/RE : Una misma enfermedad? Dra E. Ciruelos Departamento de Oncología Médica Hospital Universitario 12 de Octubre Recurrence of HER2-positive breast cancer (A) Time to
Cáncer de mama HER2+/RE+ vs HER2+/RE : Una misma enfermedad? Dra E. Ciruelos Departamento de Oncología Médica Hospital Universitario 12 de Octubre Recurrence of HER2-positive breast cancer (A) Time to
Invasive Breast Cancer
 Invasive Breast Cancer Eileen Rakovitch MD MSc FRCPC Sunnybrook Health Sciences Centre Medical Director, Louise Temerty Breast Cancer Centre LC Campbell Chair in Breast Cancer Research Associate Professor,
Invasive Breast Cancer Eileen Rakovitch MD MSc FRCPC Sunnybrook Health Sciences Centre Medical Director, Louise Temerty Breast Cancer Centre LC Campbell Chair in Breast Cancer Research Associate Professor,
TRANSPARENCY COMMITTEE OPINION. 15 February 2006
 The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 15 February 2006 Taxotere 20 mg, concentrate and solvent for solution for infusion B/1 vial of Taxotere and 1 vial
The legally binding text is the original French version TRANSPARENCY COMMITTEE OPINION 15 February 2006 Taxotere 20 mg, concentrate and solvent for solution for infusion B/1 vial of Taxotere and 1 vial
Breast Cancer Breast Managed Clinical Network
 Initial Evaluation Clinical Stage Pre-Treatment Evaluation Treatment and pathological stage Less than 4 positive lymph nodes Adjuvant Treatment ER Positive HER2 Negative (see page 2 & 3 ) HER2 Positive
Initial Evaluation Clinical Stage Pre-Treatment Evaluation Treatment and pathological stage Less than 4 positive lymph nodes Adjuvant Treatment ER Positive HER2 Negative (see page 2 & 3 ) HER2 Positive
original articles introduction
 Annals of Oncology 19. List HJ, Reiter R, Singh B et al. Expression of the nuclear coactivator AIB1 in normal and malignant breast tissue. Breast Cancer Res Treat 2001; 68: 21 28. 20. Jansson A, Delander
Annals of Oncology 19. List HJ, Reiter R, Singh B et al. Expression of the nuclear coactivator AIB1 in normal and malignant breast tissue. Breast Cancer Res Treat 2001; 68: 21 28. 20. Jansson A, Delander
Sesiones interhospitalarias de cáncer de mama. Revisión bibliográfica 4º trimestre 2015
 Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
Sesiones interhospitalarias de cáncer de mama Revisión bibliográfica 4º trimestre 2015 Selected papers Prospective Validation of a 21-Gene Expression Assay in Breast Cancer TAILORx. NEJM 2015 OS for fulvestrant
Use of Taxanes in Older Breast Cancer Patients
 SIOG Guidelines Update 2014: Use of Taxanes in Older Breast Cancer Patients Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Fundamental steps Task Force (TF) on
SIOG Guidelines Update 2014: Use of Taxanes in Older Breast Cancer Patients Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Fundamental steps Task Force (TF) on
Chemotherapy for Isolated Locoregional Recurrence
 Chemotherapy for Isolated Locoregional Recurrence Michelle Melisko MD Assistant Clinical Professor UCSF Helen Diller Family Comprehensive Cancer Center MBC and Improved Median Survival with New Therapies
Chemotherapy for Isolated Locoregional Recurrence Michelle Melisko MD Assistant Clinical Professor UCSF Helen Diller Family Comprehensive Cancer Center MBC and Improved Median Survival with New Therapies
BREAST CANCER RISK REDUCTION (PREVENTION)
") BREAST CANCER RISK REDUCTION (PREVENTION) Articles Anastrozole for prevention of breast cancer in high-risk postmenopausal women (IBIS-II): an international, double-blind, randomised placebo-controlled
BREAST CANCER RISK REDUCTION (PREVENTION) Articles Anastrozole for prevention of breast cancer in high-risk postmenopausal women (IBIS-II): an international, double-blind, randomised placebo-controlled
Harmesh Naik, MD. Hope Cancer Clinic
 Harmesh Naik, MD. Hope Cancer Clinic A brief review of adjuvant therapy of breast cancer Summarize selected new developments in adjuvant therapy of breast cancer Discussion is limited to early stage breast
Harmesh Naik, MD. Hope Cancer Clinic A brief review of adjuvant therapy of breast cancer Summarize selected new developments in adjuvant therapy of breast cancer Discussion is limited to early stage breast
Role of Genomic Profiling in (Minimally) Node Positive Breast Cancer
 Node Positive Breast Cancer") Role of Genomic Profiling in (Minimally) Node Positive Breast Cancer Kathy S. Albain, MD, FACP Professor of Medicine Dean s Scholar Loyola University Chicago Stritch School of Medicine Cardinal Bernardin
Role of Genomic Profiling in (Minimally) Node Positive Breast Cancer Kathy S. Albain, MD, FACP Professor of Medicine Dean s Scholar Loyola University Chicago Stritch School of Medicine Cardinal Bernardin
Treatment of Early-Stage HER2+ Breast Cancer
 Treatment of Early-Stage HER2+ Breast Cancer Chau T. Dang, MD Chief, MSK Westchester Medical Oncology Service Breast Medicine Service Memorial Sloan Kettering Cancer Center Disclosures I have research
Treatment of Early-Stage HER2+ Breast Cancer Chau T. Dang, MD Chief, MSK Westchester Medical Oncology Service Breast Medicine Service Memorial Sloan Kettering Cancer Center Disclosures I have research
Hormone receptor and Her2 neu (Her2) analysis
 analysis") ORIGINAL ARTICLE Impact of Triple Negative Phenotype on Breast Cancer Prognosis Henry G. Kaplan, MD* and Judith A. Malmgren, PhD à *Swedish Cancer Institute at Swedish Medical Center; HealthStat Consulting
ORIGINAL ARTICLE Impact of Triple Negative Phenotype on Breast Cancer Prognosis Henry G. Kaplan, MD* and Judith A. Malmgren, PhD à *Swedish Cancer Institute at Swedish Medical Center; HealthStat Consulting
Anthracyclines in the elderly breast cancer patients
 Anthracyclines in the elderly breast cancer patients Etienne GC Brain, MD PhD Medical Oncology Centre René Huguenin, Saint-Cloud & Group GERICO, FNCLCC, Paris Centre René Huguenin - Saint-Cloud Facts about
Anthracyclines in the elderly breast cancer patients Etienne GC Brain, MD PhD Medical Oncology Centre René Huguenin, Saint-Cloud & Group GERICO, FNCLCC, Paris Centre René Huguenin - Saint-Cloud Facts about
William J. Gradishar MD
 Northwestern University Feinberg School of Medicine Adjuvant Endocrine Therapy For Postmenopausal Women SOBO 2013 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley
Northwestern University Feinberg School of Medicine Adjuvant Endocrine Therapy For Postmenopausal Women SOBO 2013 William J. Gradishar MD Betsy Bramsen Professor of Breast Oncology Director, Maggie Daley
The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer
 The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer Cancer The Biology Century Understanding and treating the underlying tumor biology Cancer genetic studies demonstrate
The Oncotype DX Assay in the Contemporary Management of Invasive Early-stage Breast Cancer Cancer The Biology Century Understanding and treating the underlying tumor biology Cancer genetic studies demonstrate
Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer. Cheol Min Kang 2018/04/05
 Abstract No.: ABS-0075 Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer 2018/04/05 Cheol Min Kang Department of surgery, University of Ulsan
Abstract No.: ABS-0075 Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer 2018/04/05 Cheol Min Kang Department of surgery, University of Ulsan
Adjuvant Systemic Therapies in Breast Cancer
 Adjuvant Systemic Therapies in Breast Cancer Leonel F. Hernandez-Aya, MD a, Ana M. Gonzalez-Angulo, MD, MSc b,c,d, * KEYWORDS Adjuvant Breast cancer Adjuvant endocrine Adjuvant chemotherapy Adjuvant HER-2-targeted
Adjuvant Systemic Therapies in Breast Cancer Leonel F. Hernandez-Aya, MD a, Ana M. Gonzalez-Angulo, MD, MSc b,c,d, * KEYWORDS Adjuvant Breast cancer Adjuvant endocrine Adjuvant chemotherapy Adjuvant HER-2-targeted
Coming of Age: Breast Cancer in Seniors HYMAN B. MUSS
 The Oncologist Understanding and Treating Triple-Negative Breast Cancer Across the Age Spectrum Coming of Age: Breast Cancer in Seniors HYMAN B. MUSS The University of North Carolina Lineberger Cancer
The Oncologist Understanding and Treating Triple-Negative Breast Cancer Across the Age Spectrum Coming of Age: Breast Cancer in Seniors HYMAN B. MUSS The University of North Carolina Lineberger Cancer
Impact of chemotherapy-induced amenorrhea on the prognosis of early breast cancer patients
 Impact of chemotherapy-induced amenorrhea on the prognosis of early breast cancer patients Hanaa M.Kohel, MD 1 ; Yousri A.Rostom, MD 2 ; Osama H.El-Zaafarany, MD 3 ; Hazem F.Elaakad, MD 4 (1)Medical Research
Impact of chemotherapy-induced amenorrhea on the prognosis of early breast cancer patients Hanaa M.Kohel, MD 1 ; Yousri A.Rostom, MD 2 ; Osama H.El-Zaafarany, MD 3 ; Hazem F.Elaakad, MD 4 (1)Medical Research
NSABP Pivotal Breast Cancer Clinical Trials: Historical Perspective, Recent Results and Future Directions
 1 1 NSABP Pivotal Breast Cancer Clinical Trials: Historical Perspective, Recent Results and Future Directions Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health
1 1 NSABP Pivotal Breast Cancer Clinical Trials: Historical Perspective, Recent Results and Future Directions Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health
Prognostic significance of stroma tumorinfiltrating lymphocytes according to molecular subtypes of breast cancer
 Prognostic significance of stroma tumorinfiltrating lymphocytes according to molecular subtypes of breast cancer Hee Jung Kwon, Nuri Jang, Min Hui Park, Young Kyung Bae Department of Pathology, Yeungnam
Prognostic significance of stroma tumorinfiltrating lymphocytes according to molecular subtypes of breast cancer Hee Jung Kwon, Nuri Jang, Min Hui Park, Young Kyung Bae Department of Pathology, Yeungnam
Taxotere * and carboplatin plus Herceptin (trastuzumab) (TCH): the first approved non-anthracycline Herceptin-containing regimen 1
 (TCH): the first approved non-anthracycline Herceptin-containing regimen 1") Important data from BCIRG 006 Taxotere * and carboplatin plus Herceptin (trastuzumab) (TCH): the first approved non-anthracycline Herceptin-containing regimen 1 in the adjuvant treatment of HER2+ breast
Important data from BCIRG 006 Taxotere * and carboplatin plus Herceptin (trastuzumab) (TCH): the first approved non-anthracycline Herceptin-containing regimen 1 in the adjuvant treatment of HER2+ breast
Breast cancer remains the most common malignancy and the second leading. cause of cancer mortality in women in the United States.
 Dr. Andrew Seidman s Commentary I. Breast Cancer Overview Breast cancer remains the most common malignancy and the second leading cause of cancer mortality in women in the United States. The following
Dr. Andrew Seidman s Commentary I. Breast Cancer Overview Breast cancer remains the most common malignancy and the second leading cause of cancer mortality in women in the United States. The following
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy. Julia White MD Professor, Radiation Oncology
 Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Introduction. Approximately 20% of invasive breast cancers
 Introduction Approximately 2% of invasive breast cancers overexpress HER2 The current standard of care for neoadjuvant therapy is dual-targeted therapy with trastuzumab and pertuzumab plus chemotherapy
Introduction Approximately 2% of invasive breast cancers overexpress HER2 The current standard of care for neoadjuvant therapy is dual-targeted therapy with trastuzumab and pertuzumab plus chemotherapy
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC)
") Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011
 Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011 Robert W. Carlson, M.D. Professor of Medicine Stanford University Chair, NCCN Breast Cancer Treatment Guidelines Panel Selection of
Multigene Testing in NCCN Breast Cancer Treatment Guidelines, v1.2011 Robert W. Carlson, M.D. Professor of Medicine Stanford University Chair, NCCN Breast Cancer Treatment Guidelines Panel Selection of
Endocrine Therapy in Premenopausal Breast Cancer. Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology, PA US Oncology
 Endocrine Therapy in Premenopausal Breast Cancer Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology, PA US Oncology Ovarian Ablation or Suppression vs. Not in ER + or ER UK Breast Cancer
Endocrine Therapy in Premenopausal Breast Cancer Joyce O Shaughnessy, MD Baylor Sammons Cancer Center Texas Oncology, PA US Oncology Ovarian Ablation or Suppression vs. Not in ER + or ER UK Breast Cancer
Impact of BMI on pathologic complete response (pcr) following neo adjuvant chemotherapy (NAC) for locally advanced breast cancer
 following neo adjuvant chemotherapy (NAC) for locally advanced breast cancer") Impact of BMI on pathologic complete response (pcr) following neo adjuvant chemotherapy (NAC) for locally advanced breast cancer Rachna Raman, MD, MS Fellow physician University of Iowa hospitals and clinics
Impact of BMI on pathologic complete response (pcr) following neo adjuvant chemotherapy (NAC) for locally advanced breast cancer Rachna Raman, MD, MS Fellow physician University of Iowa hospitals and clinics
PMRT for N1 breast cancer :CONS. Won Park, M.D., Ph.D Department of Radiation Oncology Samsung Medical Center
 PMRT for N1 breast cancer :CONS Won Park, M.D., Ph.D Department of Radiation Oncology Samsung Medical Center DBCG 82 b & c Overgaard et al Radiot Oncol 2007 1152 pln(+), 8 or more nodes removed Systemic
PMRT for N1 breast cancer :CONS Won Park, M.D., Ph.D Department of Radiation Oncology Samsung Medical Center DBCG 82 b & c Overgaard et al Radiot Oncol 2007 1152 pln(+), 8 or more nodes removed Systemic
XII Michelangelo Foundation Seminar
 XII Michelangelo Foundation Seminar The opportunity of the neoadjuvant approach L. Gianni, Milan, I XII Michelangelo Foundation Seminar Milano, October 12, 2012 The opportunity of the neoadjuvant approach
XII Michelangelo Foundation Seminar The opportunity of the neoadjuvant approach L. Gianni, Milan, I XII Michelangelo Foundation Seminar Milano, October 12, 2012 The opportunity of the neoadjuvant approach
Recent advances in adjuvant systemic treatment for breast cancer: all systems go!
 REVIEW ARTICLE Recent advances in adjuvant systemic treatment for breast cancer: all systems go! P.N. Fishman MD* and S. Verma MD MSEd* KEY WORDS Breast cancer, adjuvant, treatment 1. INTRODUCTION Breast
REVIEW ARTICLE Recent advances in adjuvant systemic treatment for breast cancer: all systems go! P.N. Fishman MD* and S. Verma MD MSEd* KEY WORDS Breast cancer, adjuvant, treatment 1. INTRODUCTION Breast
Extended Hormonal Therapy
 Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
Extended Hormonal Therapy Dr. Caroline Lohrisch, Medical Oncologist, BC Cancer Agency Vancouver Centre November 1, 2014 www.fpon.ca Optimal Endocrine Therapy for Women with Hormone Receptor Positive Early
Her 2 Positive Advanced Breast Cancer: From Evidence to Practice
 Her 2 Positive Advanced Breast Cancer: From Evidence to Practice Sunil Verma MD, FRCP(C) Medical Director, Tom Baker Cancer Center Professor and Head, Department of Oncology Cumming School of Medicine,
Her 2 Positive Advanced Breast Cancer: From Evidence to Practice Sunil Verma MD, FRCP(C) Medical Director, Tom Baker Cancer Center Professor and Head, Department of Oncology Cumming School of Medicine,
OPTIMAL ENDOCRINE THERAPY IN EARLY BREAST CANCER
 OPTIMAL ENDOCRINE THERAPY IN EARLY BREAST CANCER STEPHEN E. JONES, M.D. US ONCOLOGY RESEARCH THE WOODLANDS, TX TOPICS PREMENOPAUSAL BREAST CANCER POSTMENOPAUSAL BREAST CANCER THE FUTURE TOPICS PREMENOPAUSAL
OPTIMAL ENDOCRINE THERAPY IN EARLY BREAST CANCER STEPHEN E. JONES, M.D. US ONCOLOGY RESEARCH THE WOODLANDS, TX TOPICS PREMENOPAUSAL BREAST CANCER POSTMENOPAUSAL BREAST CANCER THE FUTURE TOPICS PREMENOPAUSAL
Systemic Therapy of HER2-positive Breast Cancer
 Systemic Therapy of HER2-positive Breast Cancer Tanja Cufer, MD, PhD University Clinic Golnik, Medical Faculty Ljubljana, Slovenia ESO ESMO Masterclass, Belgrade 2018 HER2-positive Breast Cancer Adjuvant
Systemic Therapy of HER2-positive Breast Cancer Tanja Cufer, MD, PhD University Clinic Golnik, Medical Faculty Ljubljana, Slovenia ESO ESMO Masterclass, Belgrade 2018 HER2-positive Breast Cancer Adjuvant
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings. Eve Rodler, MD University of California at Davis October 2016
 Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
FDA Briefing Document Oncologic Drugs Advisory Committee Meeting. September 12, sbla /51 Pertuzumab (PERJETA ) Applicant: Genentech, Inc.
 Applicant: Genentech, Inc.") /51 FDA Briefing Document Oncologic Drugs Advisory Committee Meeting September 12, 2013 /51 Pertuzumab (PERJETA ) Applicant: Genentech, Inc. Disclaimer: The attached package contains background information
/51 FDA Briefing Document Oncologic Drugs Advisory Committee Meeting September 12, 2013 /51 Pertuzumab (PERJETA ) Applicant: Genentech, Inc. Disclaimer: The attached package contains background information
The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer
 The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer Laura Spring, MD Breast Medical Oncology Massachusetts General Hospital Primary Mentor: Dr. Aditya Bardia
The Neoadjuvant Model as a Translational Tool for Drug and Biomarker Development in Breast Cancer Laura Spring, MD Breast Medical Oncology Massachusetts General Hospital Primary Mentor: Dr. Aditya Bardia