1 st LINE ANTI-VEGF TREATMENT OF METASTATIC COLORECTAL CANCER (CRC)
|
|
|
- Allyson Amice Heath
- 6 years ago
- Views:
Transcription

1 1 st LINE ANTI-VEGF TREATMENT OF METASTATIC COLORECTAL CANCER (CRC)
2 Role of the VEGF Pathway in Oncogenesis

3 The Role of Angiogenesis in Cancer Somatic mutation Small avascular tumor Tumor secretion of proangiogenic factors stimulates angiogenesis Folkman J. N Engl J Med. 1971;285: Rapid tumor growth and metastasis Angiogenic inhibitors may reverse this process
 Genes implicated in tumorigenesis (p53, p73, src, ras, vhl, bcr-abl) Growth factors,")

4 VEGF: A Key Mediator of Angiogenesis Increased VEGF levels Environmental factors (hypoxia, ph) Genes implicated in tumorigenesis (p53, p73, src, ras, vhl, bcr-abl) Growth factors, hormones (EGF, bfgf, PDGF, IGF-1, IL-1, IL-6, estrogen) Dvorak HF. J Clin Oncol. 2002;20: Ebos JM, et al. Mol Cancer Res. 2002;1: Ferrara N, et al. Nat Med. 2003;9:
 VEGF-B PIGF VEGF-A 121 VEGF-A 165 VEGF-C VEGF-D Plasma membrane s s s s VEGFR-1 (flt-1) Endothelial cell NRP-1 Raf MEK MAPK NRP-2 PKC PLCg Host VEGF VEGFR-2")
5 The Family of VEGF and VEGFRs Epigenetic Induction Hypoxia, cytokines, sex hormones, growth factors, chemokines Genetic Induction Mutant p53, VHL, PTEN-suppressor genes, and activated oncogenes (eg, ras, src, EGFR, and erb B-2/HER2) VEGF-B PIGF VEGF-A 121 VEGF-A 165 VEGF-C VEGF-D Plasma membrane s s s s VEGFR-1 (flt-1) Endothelial cell NRP-1 Raf MEK MAPK NRP-2 PKC PLCg Host VEGF VEGFR-2 (flk-1/kdr) PI3K AKT VEGFR-3 (flt-4) Vascular permeability Proliferation Survival Migration Kerbel RS. N Engl J Med. 2008;358: Mobilization (eg, of VEGFR-2+ endothelial progenitor cells)
6 The VEGF and VEGF-Receptor Family Ligand isoforms PlGF VEGF-B VEGF-A VEGF-E VEGF-C VEGF-D VEGFR-1s VEGF-A 165 Extracellular Intracellular Receptor isoforms VEGFR-1 VEGFR-2 (Flt-1) (KDR) Angiogenesis NRP-1 VEGFR-3 (Flt-4) Lymph angiogenesis tumor metastases VEGF regulates angiogenesis via interaction with receptor tyrosine kinases VEGFR-2/KDR and VEGFR-1/Flt-1 Shinkaruk S, et al. Curr Med Chem Anti-Canc Agents. 2003;3: Luttun A, et al. Ann N Y Acad Sci. 2002;979:80-93.
7 Mechanism of Action of Agents Targeting VEGF Ligand
8 Methods for Inhibiting VEGF-Mediated Angiogenesis VEGF ligand blockade Antibodies targeting circulating VEGF Soluble decoy receptors targeting circulating VEGF VEGFR inhibition Antibodies against VEGFR extracellular domain Small molecule TKIs that prevent VEGFR activation Ferrera N, et al. Nature. 2005;438:
 Sorafenib (Bay 43-9006) Pazopanib Vandetanib Axitinib Anti-VEGF antibodies (bevacizumab) Tivozanib")
 Podar K, et al. Blood. 2005:105:1383-1395. Gori B, et al. Ther Clin Risk Manag.")
9 Agents Targeting the VEGF Pathway Small-molecule VEGFR TKIs Regorafenib Cediranib BIBF1120 Sunitinib (SU11248) Sorafenib (Bay ) Pazopanib Vandetanib Axitinib Anti-VEGF antibodies (bevacizumab) Tivozanib Motesanib VEGF P P P P P P P P VEGFR-1 VEGFR-2 Endothelial cell Soluble VEGFRs (aflibercept) Anti-VEGFR antibodies (ramucirumab) Podar K, et al. Blood. 2005:105: Gori B, et al. Ther Clin Risk Manag. 2011;7:
10 Bevacizumab Bevacizumab: a recombinant anti-vegf antibody Created by transferring the VEGF-binding regions of the murine antibody to a humanized IgG 1 framework (93% human, 7% murine) Produces a humanized IgG antibody Mediates blockade of VEGF ligand Binds and neutralizes all biologically active isoforms of VEGF FDA/EMA approved for lung cancer (NSCLC), glioblastoma, renal cancer, colorectal cancer, breast cancer, ovarian cancer, cervical cancer
11 First-line Chemotherapy + Bevacizumab in mcrc: Efficacy Comparative Regimens, Mos PFS OS IFL/Bev vs IFL [1] 10.6 vs vs 15.6 FOLFOX4/XELOX/Bev vs FOLFOX4/XELOX [2] 9.4 vs vs 19.9 FOLFOX/Bev vs FOLFIRI/Bev [3] 10.3 vs vs Hurwitz H, et al. N Engl J Med. 2004;350: Saltz LB, et al. J Clin Oncol. 2008;26: Bendell JC, et al. Oncologist. 2012;17:
12 AVF2107g: phase III trial of Bevacizumab + IFL for the 1L treatment of mcrc Previously untreated mcrc (n=923) R Bevaciz 5 mg/kg q2w + IFL (n=402) Placebo + IFL (n=411) Bevacizumab + 5-FU/LV (n=110)* Primary endpoint: OS Secondary endpoints: PFS, ORR, duration of response, safety and QoL *Pre-specified discontinuation of enrolment in arm 3 when Bevacizumab in combination with the bolus-ifl regimen was deemed no more toxic than with 5-FU/LV Hurwitz, et al. NEJM 2004
13 OS estimate PFS estimate AVF2107g: efficacy OS PFS 1.0 Bevaciz + IFL (n=402) Placebo + IFL (n=411) 1.0 Bevaciz + IFL (n=402) Placebo + IFL (n=411) 0.8 HR=0.66 p< HR=0.54 p< Time (months) Time (months) Hurwitz, et al. NEJM 2004
14 NO16966: phase III trial of Bevacizumab + FOLFOX4/ XELOX for the 1L treatment of mcrc 1,2 Recruitment June 2003 May 2004 Recruitment Feb 2004 Feb 2005 XELOX (n=317) Placebo + XELOX (n=350) Bevaciz 7.5mg/kg q3w + XELOX (n=350) FOLFOX4 (n=317) Placebo + FOLFOX4 (n=351) Bevaciz 5mg/kg q2w + FOLFOX4 (n=349) Initial 2-arm, open-label study (n=634) Protocol amended to 2x2 placebo-controlled design (n=1,400) after Bevacizumab phase III data became available 3 Primary endpoint: PFS Secondary endpoints: PFS on treatment, OS, ORR, duration of response, time to treatment failure 1. Cassidy, et al. JCO 2008; 2. Saltz, et al. JCO 2008; 3. Hurwitz, et al. NEJM 2004
15 PFS estimate OS estimate NO16966: efficacy PFS OS 1.0 Bevacizumab + XELOX/FOLFOX4 (n=699) Placebo + XELOX/FOLFOX4 (n=701) 1.0 Bevacizumab + XELOX/FOLFOX4 (n=699) Placebo + XELOX/FOLFOX4 (n=701) 0.8 HR=0.83 (97.5% CI: ) p= HR=0.89 (97.5% CI: ) p= Time (months) Time (months) Saltz, et al. JCO 2008
16 AVEX: phase III of Bevacizumab + Capecitabine for 1L treatment of mcrc patients 70 Previously untreated mcrc, age 70 years (n=280) R Bevacizumab 7.5 mg/kg q3w + Capecitabine (1000 mg/m 2 b.i.d, days 1-14) (n=140) Capecitabine (n=140) Primary endpoints: PFS Secondary endpoints: ORR, time to response, duration of response, OS, safety Cunningham, et al. ASCO GI 2013
17 PFS estimate OS estimate AVEX: Efficacy PFS OS* 1.0 Cape + Bevacizumab (n=140) Capecitabine (n=140) 1.0 Cape + Bevaciz (n=140) Capecitabine (n=140) HR 0.53 p< HR 0.79 p= Time (months) Time (months) *Study was not powered to detect differences in OS between treatment arms Cunningham, et al. ASCO GI 2013
18 p=0.137 p=0.582 p p=0.160 p= p=0.314 p=0.014 p=0.182 Median OS (months) Summary: OS in RCTs of Bevacizumab 1L 25 AVF0780g (n=104) 1 AVF2107g (n=813) 2 AVF2192g (n=209) 3 NO16966 (n=1,400) 4 AGITG MAX (n=313) 5 ARTIST (n=214) 6 AVEX (n=280) Kabbinavar, et al. JCO 2003; 2. Hurwitz, et al. NEJM 2004; 3. Kabbinavar, et al. JCO 2005; 4. Saltz, et al. JCO 2008; 5. Tebbutt, et al. JCO 2010; 6. Guan, et al. Chin J Cancer 2011; 7. Cunningham, et al. ASCO GI 2013
19 p=0.005 p=0.217 p p= p= p p p Median PFS (months) Summary: PFS in RCTs of Bevacizumab 1L 15 AVF0780g* (n=104) 1 AVF2107g (n=813) 2 AVF2192g (n=209) 3 NO16966 (n=1,400) 4 AGITG MAX (n=313) 5 ARTIST (n=214) 6 AVEX (n=280) *TTP 1. Kabbinavar, et al. JCO 2003; 2. Hurwitz, et al. NEJM 2004; 3. Kabbinavar, et al. JCO 2005; 4. Saltz, et al. JCO 2008; 5. Tebbutt, et al. JCO 2010; 6. Guan, et al. Chin J Cancer 2011; 7. Cunningham, et al. ASCO GI 2013
20 Bevacizumab-Associated Toxicity Adverse Event Grade 3 ATE Grade 3/4 HTN Incidence With Bev Across Indications, [1] % 2.6 GI perforations Grade 3 hemorrhagic event Wound complications Comments Risk of ATE increased in pts 65 yrs of age or older or with ATE history 5-18* Patients should receive otherwise standard CV prophylaxis and have BP monitored and managed 15 *Predominantly grade 3. May apply more to NSCLC. When surgery conducted during bev therapy. Bev not recommended for pts with active hemorrhage Risk of major bleeding does not appear to be increased in pts receiving full-dose anticoagulation tx without other risk factors Discontinue 4-8 wks before surgery; resume 6-8 wks postsurgery Potential for increased VTE risk controversial; increased risk noted in 1 study but not in others. [2,3] 1. Bevacizumab [package insert]. South San Francisco, CA: Genentech; Nalluri SR, et al. JAMA. 2008;300; Hurwitz H, et al. J Clin Oncol. 2011;29:
21 Strategies for patients with good disease control after 1 st line chemo Continuous therapy until progression or toxicities Maintenance therapy Treatment holidays
22 Progression Progression Phase III CAIRO3 trial of continued bevacizumab + capecitabine versus observation PFS1 PFS2/ TT2P Arm A Previously untreated mcrc (n=558) Bev + CAPOX (x6) CR PR SD R Observation Bev + capecitabine PFS2: re-introduction Bev + CAPOX TT2P: any treatment combination, including Bev + CAPOX Arm B Primary endpoint: PFS after re-introduction = PFS2 Secondary endpoints: PFS1, OS, TT2P, ORR, safety Koopman, et al. ASCO 2013
23 Progression Progression CAIRO3: definition of PFS1 PFS1 Arm A Previously untreated mcrc (n=558) Bev + CAPOX (x6) CR PR SD R Observation Bev + capecitabine PFS2: re-introduction Bev + CAPOX TT2P: any treatment combination, including Bev + CAPOX Arm B PFS1: time from randomisation until first progression after observation or maintenance treatment Koopman, et al. ASCO 2013
24 PFS1 estimate CAIRO3: secondary endpoint of PFS Maintenance bevacizumab Observation Median PFS1, months Stratified HR (95% CI) 0.44 ( ) p< Adjusted* HR 0.41 p< Time (months) Pts at risk Observation Continued Bev *Adjusted for covariates with imbalances at baseline Koopman, et al. ASCO 2013
25 Progression Progression CAIRO3: definition of TT2P TT2P Arm A Observation Previously untreated mcrc (n=558) Bev + CAPOX (x6) CR PR SD R Any treatment combination, including Bev + CAPOX Bev + capecitabine Arm B TT2P: time to second progression of disease, time from randomisation to progression upon any treatment including bevacizumab + CAPOX, given after PFS1 Koopman, et al. ASCO 2013
26 TT2P estimate CAIRO3: TT2P Maintenance bevacizumab Observation Median TT2P, months Stratified HR (95% CI) 0.67 ( ) p= Adjusted* HR 0.63 p= Pts at risk Observation Continued Bev Time (months) *Adjusted for covariates with imbalances at baseline Koopman, et al. ASCO 2013
27 Maintenance Bevacizumab: MACRO Trial Patients with newly diagnosed mcrc and ECOG PS 2 Capecitabine + Oxaliplatin + Bevacizumab x 6 cycles q3w (n = 239) Capecitabine + Oxaliplatin + Bevacizumab x 6 cycles q3w (n = 241) Capecitabine + Oxaliplatin + Bevacizumab until progression Bevacizumab until progression Diaz-Rubio E, et al. Oncologist. 2012;17:15-25.
28 Survival Probability MACRO: Overall Survival (ITT) XELOX-Bev Bev Patients, n Events, n (%) 175 (73) 174 (7%) Censored, n (%) 64 (27) 67 (28) Median (95% CI) 23.2 (19.79, ) ( ) HR: 1.05 (95% CI: ) 0.25 XELOX-Bev Bev Patients at Risk, n XELOX-Bev Bev Mos Diaz-Rubio E, et al. Oncologist. 2012;17:15-25.
29 TRIBE: phase III trial of 1L bevacizumab + FOLFOXIRI vs bevacizumab + FOLFIRI followed by bevacizumab/5-fu/lv until progression Induction Maintenance Previously untreated, unresectable mcrc R Bevacizumab + FOLFIRI (up to 12 cycles) (n=508) Bevacizumab + FOLFOXIRI (up to 12 cycles) Bevacizumab + 5-FU/LV Bevacizumab + 5-FU/LV PD PD Primary endpoint: PFS Secondary endpoints: response rate, secondary R0 resection rate, OS, safety, biomarker evaluation Falcone, et al. ASCO 2013
30 TRIBE: FINAL OS RESULTS Cremolini et al. ASCO GI 2015
31 TRIBE: toxicity profile Grade 3/4 AE, % Bevacizumab + FOLFIRI (n=254) Bevacizumab + FOLFOXIRI (n=250) p-value Nausea Vomiting Diarrhoea Stomatitis Neutropenia <0.001 Febrile neutropenia Neurotoxicity 0 5 <0.001 Hypertension Venous thrombosis Arterial thrombosis Bleeding Safety population; yellow box indicates a difference in incidence of grade 3 AE between treatment arms of 5% Falcone, et al. ASCO 2013
32 Bevacizumab + chemotherapy & potentially curative resection of liver mets Study Experimental arm n R0 resection rate (%) ORR (%) NO Bevacizumab + XELOX/FOLFOX NR First-BEAT 1 Bevacizumab + chemotherapy NR ETNA 2 Bevacizumab + chemotherapy NR Gruenberger* 3 Bevacizumab + XELOX BOXER 4 Bevacizumab + XELOX GONO 5 Bevacizumab + FOLFOXIRI Trials in patients with borderline resectable disease NR = not reported *Patients borderline resectable based on multiple risk factors for early recurrence ; NR in patients with liver-only metastases 1. Okines, et al. Br J Cancer 2009; 2. Smith, et al. ESMO Gruenberger, et al. JCO 2008; 4. Wong, et al. Ann Oncol Masi, et al. Lancet Oncol 2010
33
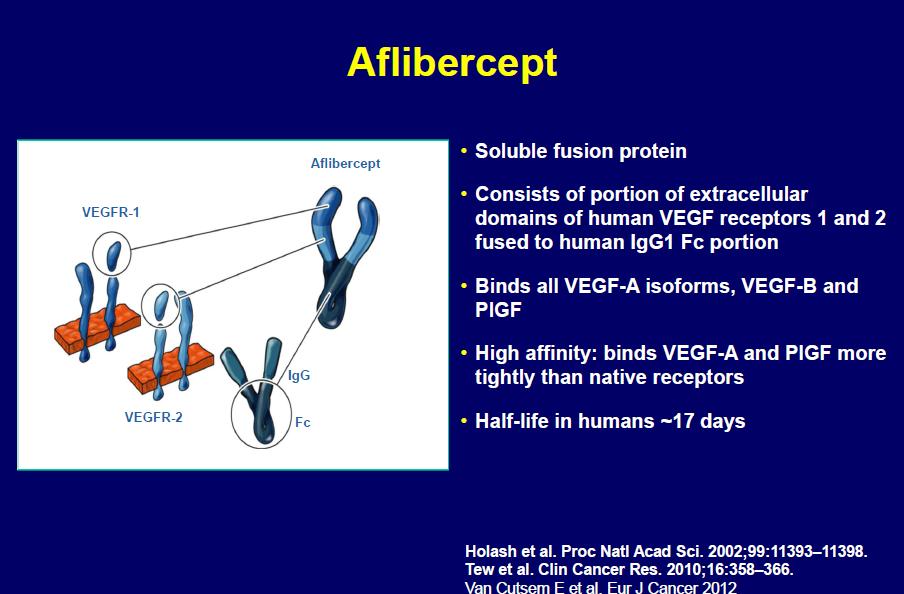
34 Aflibercept (VEGF-Trap) Fully human fusion protein consisting of VEGFR-1 Ig domain 2 VEGFR-2 Ig domain 3 Human IgG1 Fc ~ 110,000 MW Kd = 0.5 pm for VEGF 164 Blocks VEGF and PlGF Stronger binding than Bev t 1/2 ~ 17 days In phase III development VEGFR-1 K d pm The Structure of VEGF Trap VEGFR-2 K d pm Fc VEGF Trap K d < 1 pm t 1/2 ~ 25 days VEGF-Trap is a fusion protein consisting of VEGFR-1 Ig domain 2 and VEGFR-2 lg domain 3 bound to human IgG1 Fc. VEGF-Trap contains all human amino acids and has a K d of 0.5 pm for VEGF 165.
35
36 Role of VEGF Pathway in Tumor Growth VEGF-C VEGF-D VEGF binds to VEGFR2 receptor; VEGF-C, -D compete for binding to VEGFR2 VEGF-A Ramucirumab VEGFR2 VEGFR2 Endothelial cell membrane VEGF-A VEGF-C VEGF-D Ramucirumab binds to VEGFR2, blocks VEGF ligand binding Ligand binding activates VEGFR2 and p44/p42 MAP kinases No signaling Angiogenesis Tumor growth Inhibit new blood vessel formation and tumor growth

37 Multiple signaling pathways activated in CRC
38 3 rd LINE 2 nd LINE E3200 ML18147 Chemo +Bevacizumab vs Chemo +Placebo months months VELOUR FOLFIRI +Aflibercept vs FOLFIRI +Placebo 13.5 months 12.0 months RAISE FOLFIRI +Ramucirumab vs FOLFIRI +Placebo 13.3 months 11.7 months CORRECT Regorafenib vs Placebo 6.4 months 5.0 months

39
40
41 RAISE: SAFETY ANALYSIS Addition of Ramucirumab to FOLFIRI associated with: Higher incidence of hypertension Severe neutropenia: 38.4% vs 23.3%), Severe fatigue: 11.5% vs 7.8% Severe thrombocytopenia: 3.0% vs 0.8% Severe proteinuria: 3.0% vs 0.2% Ramucirumab did not appear to increase febrile neutropenia: 3.6% vs 2.7%
42 CORRECT: Common Adverse Events Treatment-related adverse events occurring in >10% of patients in either group from start of treatment to 30 days after end of treatment Regorafanib (n=500) Placebo (n=253) Any Gr Gr 3 Gr 4 Any Gr Gr 3 Gr 4 Fatigue, n (%) 237 (47) 46 (9) 2 (<1) 71 (28) 12 (5) 1 (<1) Hand-foot skin reaction, n (%) 233 (47) 83 (17) 0 19 (8) 1 (<1) 0 Diarrhea, n (%) 169 (34) 35 (7) 1 (<1) 21 (8) 2 (1) 0 Anorexia, n (%) 152 (30) 16 (3) 0 39 (15) 7 (3) 0 Voice changes, n (%) 147 (29) 1 (<1) 0 14 (6) 0 0 Hypertension, n (%) 139 (28) 36 (7) 0 15 (6) 2 (1) 0 Oral mucositis, n (%) 136 (27) 15 (3) 0 9 (4) 0 0 Rash or desquamation, n (%) 130 (26) 29 (6) 0 10 (4) 0 0 Nausea, n (%) 72 (14) 2 (<1) 0 28 (11) 0 0 Weight loss, n (%) 69 (14) (2) 0 0 Thrombocytopenia, n (%) 63 (13) 13 (3) 1 (<1) 5 (2) 1 (<1) 0 1. Grothey A, et al. Lancet [epub].
43 Approx. Prices per month Bevacizumab -> 1, /month Aflibercept -> 2, /month Regorafenib -> 3, /month Ramucirumab -> ~10,000 /month (?)
44 Overall survival in phase III trials 1997 ~12 months 1* 2007 >20 months >30 months 6,7 *Based on a meta-analysis of >19 trials of 5-FU/LV 1. Thirion, et al. JCO 2004; 2. Hurwitz, et al. NEJM Van Cutsem, et al. NEJM 2009; 4. Van Cutsem, et al. JCO Goldberg, et al. Oncologist 2007; 6. Falcone, et al. ASCO 2013; 7. Takahari, et al. ASCO 2013
Does it matter which chemotherapy regimen you partner with the biologic agents?
 Does it matter which chemotherapy regimen you partner with the biologic agents? Yes, it does matter! Axel Grothey Disclosures Research Funding to MAYO Clinic Genentech Bayer Eisai Pfizer Imclone Potential
Does it matter which chemotherapy regimen you partner with the biologic agents? Yes, it does matter! Axel Grothey Disclosures Research Funding to MAYO Clinic Genentech Bayer Eisai Pfizer Imclone Potential
Conflicts of Interest GI Malignancies: An Update on Current Treatment Options
 Conflicts of Interest GI Malignancies: An Update on Current Treatment Options Nothing to disclose Trevor McKibbin, PharmD, MS, BCOP Clinical Specialist, Hematology/Oncology Winship Cancer Institute of
Conflicts of Interest GI Malignancies: An Update on Current Treatment Options Nothing to disclose Trevor McKibbin, PharmD, MS, BCOP Clinical Specialist, Hematology/Oncology Winship Cancer Institute of
Targeted Therapies in Metastatic Colorectal Cancer: An Update
 Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Targeted Therapies in Metastatic Colorectal Cancer: An Update ASCO 2007: Targeted Therapies in Metastatic Colorectal Cancer: An Update Bevacizumab is effective in combination with XELOX or FOLFOX-4 Bevacizumab
Incorporating biologics in the management of older patients with metastatic colorectal cancer
 Incorporating biologics in the management of older patients with metastatic colorectal cancer D Papamichael MB BS MD FRCP Cyprus Oncology Centre GSK Satellite Symposium SIOG APAC Singapore 12-13 July 2014
Incorporating biologics in the management of older patients with metastatic colorectal cancer D Papamichael MB BS MD FRCP Cyprus Oncology Centre GSK Satellite Symposium SIOG APAC Singapore 12-13 July 2014
Angiogenesis and tumor growth
 Anti-angiogenic agents: where we are? Martin Reck Department of Thoracic Oncology Hospital Grosshansdorf Germany Angiogenesis and tumor growth Journal of experimental Medicine 1972; 133: 275-88 1 Angiogenesis
Anti-angiogenic agents: where we are? Martin Reck Department of Thoracic Oncology Hospital Grosshansdorf Germany Angiogenesis and tumor growth Journal of experimental Medicine 1972; 133: 275-88 1 Angiogenesis
What s New in Colon Cancer? Therapy over the last decade
 What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
What s New in Colon Cancer? 9/19/2014 Michael McNamara, MD Therapy over the last decade Cytotoxic chemotherapy - 5FU ( Mayo, Roswell, Infusional) - Xeloda (01 ) - Oxaliplatin (02 ) - Irinotecan (96 ) Anti-
ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS. Andrés Cervantes. Professor of Medicine
 CHEMOTHERAPY +/- TARGETED AGENTS. Andrés Cervantes. Professor of Medicine") ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS Andrés Cervantes Professor of Medicine 1995 One option Advances in the treatment of mcrc 2000
ADVANCED COLORECTAL CANCER: UNRESECTABLE OR BORDERLINE RESECTABLE (GROUP 1) CHEMOTHERAPY +/- TARGETED AGENTS Andrés Cervantes Professor of Medicine 1995 One option Advances in the treatment of mcrc 2000
Nuevos Agentes en el Manejo de Cáncer Colorectal: Dónde Incorporalos?
 Nuevos Agentes en el Manejo de Cáncer Colorectal: Dónde Incorporalos? Prof. Dr. Paulo M. Hoff Instituto do Câncer do Estado de São Paulo - ICESP Faculdade de Medicina Universidade de São Paulo (USP) Conflicts
Nuevos Agentes en el Manejo de Cáncer Colorectal: Dónde Incorporalos? Prof. Dr. Paulo M. Hoff Instituto do Câncer do Estado de São Paulo - ICESP Faculdade de Medicina Universidade de São Paulo (USP) Conflicts
What s New? Dr. Barbara Melosky
 Metastatic Colorectal o Carcinoma a What s New? Dr. Barbara Melosky Objectives Review any recent changes regarding treatment t t options for mcrc Discuss the common and expected toxicities of treatment
Metastatic Colorectal o Carcinoma a What s New? Dr. Barbara Melosky Objectives Review any recent changes regarding treatment t t options for mcrc Discuss the common and expected toxicities of treatment
Κίκα Πλοιαρχοπούλου. Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών
 Κίκα Πλοιαρχοπούλου Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών Time (months) Survival outcomes in mcrc have progressively improved over the past two decades Treatment options for many patients Multidisciplinary
Κίκα Πλοιαρχοπούλου Παθολόγος Ογκολόγος Ευρωκλινική Αθηνών Time (months) Survival outcomes in mcrc have progressively improved over the past two decades Treatment options for many patients Multidisciplinary
Colon Cancer Molecular Target Agents
 Colon Cancer Molecular Target Agents Ci Caio Max SR S. Rocha Lima, M.D. MD Professor of Medicine CDi CoDiretor Cl Colorectal tlheptobiliary, Pancreatic SDG, and Phase I Unit University of Miami & Silvester
Colon Cancer Molecular Target Agents Ci Caio Max SR S. Rocha Lima, M.D. MD Professor of Medicine CDi CoDiretor Cl Colorectal tlheptobiliary, Pancreatic SDG, and Phase I Unit University of Miami & Silvester
First line treatment in metastatic colorectal cancer
 First line treatment in metastatic colorectal cancer Claus-Henning Köhne University Clinic Onkology and Haematology North West German Cancer Center (NWTZ) A non authorised version of ESMO guidelines was
First line treatment in metastatic colorectal cancer Claus-Henning Köhne University Clinic Onkology and Haematology North West German Cancer Center (NWTZ) A non authorised version of ESMO guidelines was
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan
 State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
State of the Art: Colorectal Cancer Liver Metastasis Dr. Iain Tan Consultant GI Medical Oncologist National Cancer Centre Singapore Clinician Scientist, Genome Institute of Singapore OS (%) Overall survival
MEETING SUMMARY ESMO 2018, Munich, Germany. Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER
 MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
MEETING SUMMARY ESMO 2018, Munich, Germany Dr. Jenny Seligmann University of Leeds, UK HIGHLIGHTS ON COLORECTAL CANCER DISCLAIMER Please note: The views expressed within this presentation are the personal
Chemotherapy for resectable liver mets: Options and Issues. Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA
 Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Chemotherapy for resectable liver mets: Options and Issues Herbert Hurwitz Duke University Medical Center Durham, North Carolina, USA Chemotherapy regimens in 1 st line mcrc Standard FOLFOX-Bev FOLFIRI-Bev
Metastatic Colorectal Cancer. Update 2015
 Metastatic Colorectal Cancer Update 2015 A/Prof Jeremy Shapiro GI Medical Oncologist Cabrini Hospital, Melbourne 1 Not all pts with metastatic CRC are equal 1 st consideration can patient be cured by resection
Metastatic Colorectal Cancer Update 2015 A/Prof Jeremy Shapiro GI Medical Oncologist Cabrini Hospital, Melbourne 1 Not all pts with metastatic CRC are equal 1 st consideration can patient be cured by resection
Colorectal Cancer Therapy and Associated Toxicity
 Colorectal Cancer Therapy and Associated Toxicity Mountain States Cancer Conference November 6, 2010 Colin D. Weekes, M.D., Ph.D Assistant Professor University of Colorado GI Cancers Are Common 2009 Estimated
Colorectal Cancer Therapy and Associated Toxicity Mountain States Cancer Conference November 6, 2010 Colin D. Weekes, M.D., Ph.D Assistant Professor University of Colorado GI Cancers Are Common 2009 Estimated
Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? VEGF Is the Only Angiogenic Factor Present Throughout the Tumor Life Cycle
 Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? Martin Reck Department e t of Thoracic c Oncology ogy Hospital Grosshansdorf Germany VEGF Is the Only Angiogenic Factor Present Throughout
Antiangiogenic Agents in NSCLC Where are we? Which biomarkers? Martin Reck Department e t of Thoracic c Oncology ogy Hospital Grosshansdorf Germany VEGF Is the Only Angiogenic Factor Present Throughout
Antiangiogenic therapy in GI cancer: current status and future directions
 Riccardo Giampieri, MD, PhD Università Politecnica delle Marche Ospedali Riuniti diancona Antiangiogenic therapy in GI cancer: current status and future directions Before starting Summary - Antiangiogenesis
Riccardo Giampieri, MD, PhD Università Politecnica delle Marche Ospedali Riuniti diancona Antiangiogenic therapy in GI cancer: current status and future directions Before starting Summary - Antiangiogenesis
Advances in Chemotherapy of Colorectal Cancer
 Advances in Chemotherapy of Colorectal Cancer Richard M. Goldberg Lineberger Comprehensive Cancer Center University of North Carolina at Chapel Hill Disease Settings Adjuvant Therapy MOSAIC, FOLFOX Andre
Advances in Chemotherapy of Colorectal Cancer Richard M. Goldberg Lineberger Comprehensive Cancer Center University of North Carolina at Chapel Hill Disease Settings Adjuvant Therapy MOSAIC, FOLFOX Andre
Dr. Iain Tan. Senior Consultant GI Medical Oncologist National Cancer Centre Singapore
 ESMO-ASIA 2017 Preceptorship (GI cancers) Session: Metastatic colorectal cancer, liver limited metastases Topic: Unresectable or borderline resectable : chemotherapy +/- targeted agents Dr. Iain Tan Senior
ESMO-ASIA 2017 Preceptorship (GI cancers) Session: Metastatic colorectal cancer, liver limited metastases Topic: Unresectable or borderline resectable : chemotherapy +/- targeted agents Dr. Iain Tan Senior
Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer
 Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer Cetuximab with Chemotherapy (CT) as First-Line Treatment for Metastatic Colorectal Cancer (mcrc): Analysis of
Cetuximab with Chemotherapy as Treatment for Stage III Colon or Metastatic Colorectal Cancer Cetuximab with Chemotherapy (CT) as First-Line Treatment for Metastatic Colorectal Cancer (mcrc): Analysis of
Konzepte bei der Therapie des metastasierten kolorektalen Karzinoms
 21. Ärzte Fortbildungskurs in Klinischer Onkologie 24.-26. Februar 2011 Kantonspital St. Gallen / Schweiz Konzepte bei der Therapie des metastasierten kolorektalen Karzinoms Claus-Henning Köhne Klinik
21. Ärzte Fortbildungskurs in Klinischer Onkologie 24.-26. Februar 2011 Kantonspital St. Gallen / Schweiz Konzepte bei der Therapie des metastasierten kolorektalen Karzinoms Claus-Henning Köhne Klinik
Tobias Engel Ayer Botrel 1,2*, Luciana Gontijo de Oliveira Clark 1, Luciano Paladini 1 and Otávio Augusto C. Clark 1
 Botrel et al. BMC Cancer (2016) 16:677 DOI 10.1186/s12885-016-2734-y RESEARCH ARTICLE Open Access Efficacy and safety of bevacizumab plus chemotherapy compared to chemotherapy alone in previously untreated
Botrel et al. BMC Cancer (2016) 16:677 DOI 10.1186/s12885-016-2734-y RESEARCH ARTICLE Open Access Efficacy and safety of bevacizumab plus chemotherapy compared to chemotherapy alone in previously untreated
Fighting a Smarter War On Colon Cancer:
 Fighting a Smarter War On Colon Cancer: Value as a new endpoint? John L. Marshall, MD Tel: (202) 444-0275 Fax: (202) 444-1229 http://lombardi.georgetown.edu/gi Stakeholder Motivation Stakeholders FDA CMS/Payers
Fighting a Smarter War On Colon Cancer: Value as a new endpoint? John L. Marshall, MD Tel: (202) 444-0275 Fax: (202) 444-1229 http://lombardi.georgetown.edu/gi Stakeholder Motivation Stakeholders FDA CMS/Payers
2/20/14& Medical Management of Colon and Rectal Cancer: An Overview. Outline / Learning Objectives. How common is colon cancer?
 Medical Management of Colon and Rectal Cancer: An Overview Jonathan Grim, MD, PhD VA Puget Sound Health Care System Fred Hutchinson Cancer Research Center UW Medicine Outline / Learning Objectives Epidemiology
Medical Management of Colon and Rectal Cancer: An Overview Jonathan Grim, MD, PhD VA Puget Sound Health Care System Fred Hutchinson Cancer Research Center UW Medicine Outline / Learning Objectives Epidemiology
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO. Dra. Ruth Vera Complejo Hospitalario de Navarra
 MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO Dra. Ruth Vera Complejo Hospitalario de Navarra GOALS Prolongation of survival Cure Improving tumour-related symptoms Stopping tumour progression
MÁS ALLA DE LA PRIMERA LÍNEA: SECUENCIA DE TRATAMIENTO Dra. Ruth Vera Complejo Hospitalario de Navarra GOALS Prolongation of survival Cure Improving tumour-related symptoms Stopping tumour progression
Colon cancer: Highlights. Filippo Pietrantonio Istituto Nazionale dei Tumori di Milano
 Colon cancer: Highlights Filippo Pietrantonio Istituto Nazionale dei Tumori di Milano Agenda 1) Metastatic colorectal cancer First-line treatment molecularly unselected: FOLFOXIRI-bev (CHARTA trial) Later-line
Colon cancer: Highlights Filippo Pietrantonio Istituto Nazionale dei Tumori di Milano Agenda 1) Metastatic colorectal cancer First-line treatment molecularly unselected: FOLFOXIRI-bev (CHARTA trial) Later-line
DALLA CAPECITABINA AL TAS 102
 DALLA CAPECITABINA AL TAS 102 Milano 29 settembre 2016 LE PROSPETTIVE NELLA RICERCA Armando Santoro Humanitas Cancer Center THE 1,2.AND 3 LINE CHEMOTHERAPY IN CRC M BEVACIZUMAB AFLIBERCET RAS wt RAS mu
DALLA CAPECITABINA AL TAS 102 Milano 29 settembre 2016 LE PROSPETTIVE NELLA RICERCA Armando Santoro Humanitas Cancer Center THE 1,2.AND 3 LINE CHEMOTHERAPY IN CRC M BEVACIZUMAB AFLIBERCET RAS wt RAS mu
Targeted and Chemotherapeutic Approaches to Management of Metastatic Colorectal Cancer. Nicole M. Ross, MSN, CRNP, AOCNP Fox Chase Cancer Center
 Targeted and Chemotherapeutic Approaches to Management of Metastatic Colorectal Cancer Nicole M. Ross, MSN, CRNP, AOCNP Fox Chase Cancer Center Learning Objectives Critically evaluate current clinical
Targeted and Chemotherapeutic Approaches to Management of Metastatic Colorectal Cancer Nicole M. Ross, MSN, CRNP, AOCNP Fox Chase Cancer Center Learning Objectives Critically evaluate current clinical
David N. Robinson, MD
 David N. Robinson, MD Background and Treatment of mrcc Background ~ 64,770 new cases of kidney/renal pelvis cancers will be diagnosed in the US in 2012 with an estimated 13,570 deaths [1] ~ 75% are clear-cell
David N. Robinson, MD Background and Treatment of mrcc Background ~ 64,770 new cases of kidney/renal pelvis cancers will be diagnosed in the US in 2012 with an estimated 13,570 deaths [1] ~ 75% are clear-cell
AIOM GIOVANI Perugia, Luglio 2017
 AIOM GIOVANI 2017 Perugia, 07-08 Luglio 2017 Scelta delle linee successive nel paziente RAS e BRAF wild-type con particolare accento su nuovi bersagli terapeutici Francesca Battaglin U.O.C. Oncologia Medica
AIOM GIOVANI 2017 Perugia, 07-08 Luglio 2017 Scelta delle linee successive nel paziente RAS e BRAF wild-type con particolare accento su nuovi bersagli terapeutici Francesca Battaglin U.O.C. Oncologia Medica
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS
 Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
Is it possible to cure patients with liver metastases? Taghizadeh Ali MD Oncologist, MUMS Survival Rates of by Stage of Adenocarcinoma of the Colon Liver Resection New Perspective Colorectal cancer liver
Where Are Anti-Angiogenic Agents Positioned Within Cancer Care Guidelines?
 Introduction Additionally, other anti-angiogenic drugs, including sorafenib, sunitinib, axitinib, pazopanib, vandetanib, The development and subsequent use of drugs for treating cancer cabozantinib, and
Introduction Additionally, other anti-angiogenic drugs, including sorafenib, sunitinib, axitinib, pazopanib, vandetanib, The development and subsequent use of drugs for treating cancer cabozantinib, and
The treatment of metastatic colorectal cancer in 2007
 The treatment of metastatic colorectal cancer in 2007 Prof Eric Van Cutsem, MD, PhD Gastrointestinal Oncology Unit University Hospital Gasthuisberg Leuven - Belgium CRC is a major health concern Life-time
The treatment of metastatic colorectal cancer in 2007 Prof Eric Van Cutsem, MD, PhD Gastrointestinal Oncology Unit University Hospital Gasthuisberg Leuven - Belgium CRC is a major health concern Life-time
JY Douillard MD, PhD Professor of Medical Oncology
 Colorectal Cancer ESMO Preceptorship Program Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer Basic strategy and groups (RASwt/mut, BRAF mut) JY Douillard
Colorectal Cancer ESMO Preceptorship Program Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer Basic strategy and groups (RASwt/mut, BRAF mut) JY Douillard
A retrospective analysis of the safety and efficacy of apatinib in treating advanced metastatic colorectal cancer
 Oncology and Translational Medicine DOI 10.1007/s10330-017-0235-5 October 2017, Vol. 3, No. 5, P210 P216 ORIGINAL ARTICLE A retrospective analysis of the safety and efficacy of apatinib in treating advanced
Oncology and Translational Medicine DOI 10.1007/s10330-017-0235-5 October 2017, Vol. 3, No. 5, P210 P216 ORIGINAL ARTICLE A retrospective analysis of the safety and efficacy of apatinib in treating advanced
JY Douillard MD, PhD Professor of Medical Oncology
 ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Vienna 26-27 Program October 2015 Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer
ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Vienna 26-27 Program October 2015 Prague May 22-23rd 2014 Review of the ESMO Consensus Conference on metastatic colo-rectal cancer
The Current Champion: Angiogenesis inhibitors
 The Current Champion: Angiogenesis inhibitors Baek-Yeol RYOO University of Ulsan College of Medicine ASAN Medical Center Dept. of Oncology Seoul, Korea Survival probability Sorafenib: Overall Survival
The Current Champion: Angiogenesis inhibitors Baek-Yeol RYOO University of Ulsan College of Medicine ASAN Medical Center Dept. of Oncology Seoul, Korea Survival probability Sorafenib: Overall Survival
THE ROLE OF PREDICTIVE AND PROGNOSTIC MARKERS IN COLORECTAL CANCER
 THE ROLE OF PREDICTIVE AND PROGNOSTIC MARKERS IN COLORECTAL CANCER Cathy Eng, M.D., F.A.C.P. Associate Professor Associate Medical Director, Colorectal Center Dept of GI Medical Oncology November 5, 2010
THE ROLE OF PREDICTIVE AND PROGNOSTIC MARKERS IN COLORECTAL CANCER Cathy Eng, M.D., F.A.C.P. Associate Professor Associate Medical Director, Colorectal Center Dept of GI Medical Oncology November 5, 2010
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors?
 Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
Have Results of Recent Randomized Trials Changed the Role of mtor Inhibitors? Bernard Escudier Institut Gustave Roussy Villejuif, France EIKCS Lyon April 2015 What is the current role of mtor inhibitors?
Chemotherapy of colon cancers
 Chemotherapy of colon cancers Stage distribution Stage I : 15% T 1,2 NO Stage IV: 20 25% M+ Stage II : 20 30% T3,4 NO Stage III N+: 30 40% clinical stages I, II, or III colon cancer are at risk for having
Chemotherapy of colon cancers Stage distribution Stage I : 15% T 1,2 NO Stage IV: 20 25% M+ Stage II : 20 30% T3,4 NO Stage III N+: 30 40% clinical stages I, II, or III colon cancer are at risk for having
Update on the Management of HER2+ Breast Cancer. Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany
 Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
New Options in Metastatic Colorectal Cancer. Jeffrey A. Bubis, DO, FACOI, FACP Fleming Island Baptist South Palatka
 New Options in Metastatic Colorectal Cancer Jeffrey A. Bubis, DO, FACOI, FACP Fleming Island Baptist South Palatka 4 th most frequently diagnosed CA in the US 2 nd leading cause of CA death in the US Incidence
New Options in Metastatic Colorectal Cancer Jeffrey A. Bubis, DO, FACOI, FACP Fleming Island Baptist South Palatka 4 th most frequently diagnosed CA in the US 2 nd leading cause of CA death in the US Incidence
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Toxicity by Age Group. Old Factor 1: Age. Disclosures. Predicting survival in metastatic colorectal cancer. Personalized Medicine - Decision Tools -
 Disclosures Predicting survival in metastatic colorectal cancer Daniel Sargent, PhD Mayo Clinic Consulting activities Amgen Pfizer Roche/Genentech Sanofi-Aventis Genomic Health Personalized Medicine -
Disclosures Predicting survival in metastatic colorectal cancer Daniel Sargent, PhD Mayo Clinic Consulting activities Amgen Pfizer Roche/Genentech Sanofi-Aventis Genomic Health Personalized Medicine -
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective
 Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
VEGF-Inhibitors in NSCLC. Martin Reck Department of Thoracic Oncology Hospital Grosshansdorf Germany
 VEGF-Inhibitors in NSCLC Martin Reck Department of Thoracic Oncology Hospital Grosshansdorf Germany Conflicts of interest Advisory Board: AstraZeneca Bristol-Myers Squibb Daiichi Sankyo Eli Lilly Merck
VEGF-Inhibitors in NSCLC Martin Reck Department of Thoracic Oncology Hospital Grosshansdorf Germany Conflicts of interest Advisory Board: AstraZeneca Bristol-Myers Squibb Daiichi Sankyo Eli Lilly Merck
Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
 Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
Efficacy Results from the ToGA Trial: A Phase III Study of Trastuzumab Added to Standard Chemotherapy in First-Line HER2- Positive Advanced Gastric Cancer Van Cutsem E et al. Proc ASCO 2009;Abstract LBA4509.
La strategia terapeutica del carcinoma del colon metastatico
 Dalla Capecitabina al TAS-102 Milano, 29 settembre 2016 La strategia terapeutica del carcinoma del colon metastatico Gianluca Masi U.O. di Oncologia Medica Universitaria Azienda Ospedaliero-Universitaria
Dalla Capecitabina al TAS-102 Milano, 29 settembre 2016 La strategia terapeutica del carcinoma del colon metastatico Gianluca Masi U.O. di Oncologia Medica Universitaria Azienda Ospedaliero-Universitaria
pan-canadian Oncology Drug Review Final Clinical Guidance Report Aflibercept (Zaltrap) for Metastatic Colorectal Cancer September 5, 2014
 for Metastatic Colorectal Cancer September 5, 2014") pan-canadian Oncology Drug Review Final Clinical Guidance Report Aflibercept (Zaltrap) for Metastatic Colorectal Cancer September 5, 2014 DISCLAIMER Not a Substitute for Professional Advice This report
pan-canadian Oncology Drug Review Final Clinical Guidance Report Aflibercept (Zaltrap) for Metastatic Colorectal Cancer September 5, 2014 DISCLAIMER Not a Substitute for Professional Advice This report
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD
 METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
METASTATIC COLORECTAL CANCER: TUMOR MUTATIONAL ANALYSIS AND ITS IMPACT ON CHEMOTHERAPY SUMA SATTI, MD INTRODUCTION Second leading cause of cancer related death in the United States. 136,830 cases in 2014
Third Line and Beyond: Management of Refractory Colorectal Cancer
 Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Third Line and Beyond: Management of Refractory Colorectal Cancer George A. Fisher MD PhD Stanford University 1 Overview Defining the chemo refractory and intolerant Agents approved in 3 rd line setting
Cancer Cell Research 14 (2017)
") Available at http:// www.cancercellresearch.org ISSN 2161-2609 Efficacy and safety of bevacizumab for patients with advanced non-small cell lung cancer Ping Xu, Hongmei Li*, Xiaoyan Zhang Department of
Available at http:// www.cancercellresearch.org ISSN 2161-2609 Efficacy and safety of bevacizumab for patients with advanced non-small cell lung cancer Ping Xu, Hongmei Li*, Xiaoyan Zhang Department of
Managing mcrc Across Disease Continuum: Front-Line Therapy and Treatment Beyond Progression
 Managing mcrc Across Disease Continuum: Front-Line Therapy and Treatment Beyond Progression Guillermo Méndez, MD Sección Oncología Hospital de Gastroenterología Bonorino Udaondo Carlos B. Udaondo y Fundación
Managing mcrc Across Disease Continuum: Front-Line Therapy and Treatment Beyond Progression Guillermo Méndez, MD Sección Oncología Hospital de Gastroenterología Bonorino Udaondo Carlos B. Udaondo y Fundación
Adjuvant treatment Colon Cancer
 ESMO Preceptorship Colorectal Cancer, October 2016 Singapore Adjuvant treatment Colon Cancer Claus-Henning Köhne University Clinic for Onkology und Haematology Oldenburg, Germany Aim of the lecture Adjuvant
ESMO Preceptorship Colorectal Cancer, October 2016 Singapore Adjuvant treatment Colon Cancer Claus-Henning Köhne University Clinic for Onkology und Haematology Oldenburg, Germany Aim of the lecture Adjuvant
The Role of Angiogenesis Inhibition in Breast Cancer Today: Lessons Learned
 The Role of Angiogenesis Inhibition in Breast Cancer Today: Lessons Learned Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education UCSF Helen Diller Family Comprehensive
The Role of Angiogenesis Inhibition in Breast Cancer Today: Lessons Learned Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education UCSF Helen Diller Family Comprehensive
Review Article Advances of Targeted Therapy in Treatment of Unresectable Metastatic Colorectal Cancer
 BioMed Research International Volume 2016, Article ID 7590245, 14 pages http://dx.doi.org/10.1155/2016/7590245 Review Article Advances of Targeted Therapy in Treatment of Unresectable Metastatic Colorectal
BioMed Research International Volume 2016, Article ID 7590245, 14 pages http://dx.doi.org/10.1155/2016/7590245 Review Article Advances of Targeted Therapy in Treatment of Unresectable Metastatic Colorectal
12 AISF Special Conference Sorafenib: magnitude of benefit, side effects and stopping rules 9 years after approval
 12 AISF Special Conference Sorafenib: magnitude of benefit, side effects and stopping rules 9 years after approval ARMANDO SANTORO Roma 10-6-2016 SORAFENIB APPROVAL 29 OCTOBER 2007 Marketing authorization
12 AISF Special Conference Sorafenib: magnitude of benefit, side effects and stopping rules 9 years after approval ARMANDO SANTORO Roma 10-6-2016 SORAFENIB APPROVAL 29 OCTOBER 2007 Marketing authorization
Table Selected Clinical Trials of Anti-Angiogenesis Therapy in Gynecologic Malignancies
 Table Selected Clinical Trials of Anti-Angiogenesis Therapy in Gynecologic Malignancies Uterus Study N Eligibility Regimen RR (No. of Responses) Median OS Grade 3/4 Toxicities Nimeiri et al[42] Total:
Table Selected Clinical Trials of Anti-Angiogenesis Therapy in Gynecologic Malignancies Uterus Study N Eligibility Regimen RR (No. of Responses) Median OS Grade 3/4 Toxicities Nimeiri et al[42] Total:
Metastatic Colorectal Cancer : The role of Personalised Medicine, Biomarkers and Early tumour shrinkage. Dr Lee-Ann Jones
 Metastatic Colorectal Cancer : The role of Personalised Medicine, Biomarkers and Early tumour shrinkage Dr Lee-Ann Jones Aim Metastatic Colorectal Cancer: Past: 5FU, oxaliplatin, irinotecan..blanket treatment
Metastatic Colorectal Cancer : The role of Personalised Medicine, Biomarkers and Early tumour shrinkage Dr Lee-Ann Jones Aim Metastatic Colorectal Cancer: Past: 5FU, oxaliplatin, irinotecan..blanket treatment
Advanced HER2+ Breast Cancer: New Options and How to Deploy Them. José Baselga MD, PhD
 Advanced HER2 Breast Cancer: New Options and How to Deploy Them José Baselga MD, PhD HER2 signaling results in a multitude of cellular effects, including increased cellular proliferation HER2 HER3 RAS
Advanced HER2 Breast Cancer: New Options and How to Deploy Them José Baselga MD, PhD HER2 signaling results in a multitude of cellular effects, including increased cellular proliferation HER2 HER3 RAS
Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First?
 Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First? Marc Peeters, MD, PhD Head of the Oncology Department Antwerp University Hospital Antwerp, Belgium marc.peeters@uza.be 71-year-old
Case 1 Metastatic Pancreatic Adenocarcinoma: What Therapy Should I Select First? Marc Peeters, MD, PhD Head of the Oncology Department Antwerp University Hospital Antwerp, Belgium marc.peeters@uza.be 71-year-old
Ashita Waterston Beatson West of Scotland Cancer Centre
 Ashita Waterston Beatson West of Scotland Cancer Centre Aim of treatment Scheduling and choice of treatments are dictated by aim: Down staging for resectability: upfront intensive Prolong survival: combination
Ashita Waterston Beatson West of Scotland Cancer Centre Aim of treatment Scheduling and choice of treatments are dictated by aim: Down staging for resectability: upfront intensive Prolong survival: combination
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD
 La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
La revolución de la inmunoterapia: dónde la posicionamos? Javier Puente, MD, PhD Hospital Universitario Clinico San Carlos Medical Oncology Department Thoracic & Urological Cancer Unit Complutense University
Treatment of Renal Cell Carcinoma (RCC) in the Era of Targeted Agents
 in the Era of Targeted Agents") Conflict of Interest Treatment of Renal Cell Carcinoma (RCC) in the Era of Targeted Agents None Patrick Medina, PharmD, BCOP Associate Professor University of Oklahoma OKC, OK Learning Objectives Epidemiology
Conflict of Interest Treatment of Renal Cell Carcinoma (RCC) in the Era of Targeted Agents None Patrick Medina, PharmD, BCOP Associate Professor University of Oklahoma OKC, OK Learning Objectives Epidemiology
Development of Conventional Chemotherapy in mcrc BSC vs. Chemo, Biochemical modulation, Oral fluoropyrimidines, Developmentof combination chemotherapy
 ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Valencia May Program 20-21st 2016 Prague May 22-23rd 2014 Development of Conventional Chemotherapy in mcrc BSC vs. Chemo, Biochemical
ESMO Preceptorship Colorectal Cancer Colorectal ESMO Cancer Preceptorship Valencia May Program 20-21st 2016 Prague May 22-23rd 2014 Development of Conventional Chemotherapy in mcrc BSC vs. Chemo, Biochemical
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Novel Chemotherapy Agents for Metastatic Breast Cancer. Joanne L. Blum, MD, PhD Baylor-Sammons Cancer Center Dallas, TX
 Novel Chemotherapy Agents for Metastatic Breast Cancer Joanne L. Blum, MD, PhD Baylor-Sammons Cancer Center Dallas, TX New Chemotherapy Agents in Breast Cancer New classes of drugs Epothilones Halichondrin
Novel Chemotherapy Agents for Metastatic Breast Cancer Joanne L. Blum, MD, PhD Baylor-Sammons Cancer Center Dallas, TX New Chemotherapy Agents in Breast Cancer New classes of drugs Epothilones Halichondrin
Rationale for VEGFR-targeted Therapy in RCC
 Rationale for VEGFR-targeted Therapy in RCC EIKCS, Budapest, May 2013 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial Management Group Honoraria Astra Zeneca + + + Astellas
Rationale for VEGFR-targeted Therapy in RCC EIKCS, Budapest, May 2013 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial Management Group Honoraria Astra Zeneca + + + Astellas
GASTRIC & PANCREATIC CANCER
 GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
New Agents for Head and Neck Cancer. Ezra Cohen, MD Associate Professor of Medicine University of Chicago Chicago, IL
 New Agents for Head and Neck Cancer Ezra Cohen, MD Associate Professor of Medicine University of Chicago Chicago, IL Disclosure Dr. Cohen has the following relevant financial relationships with commercial
New Agents for Head and Neck Cancer Ezra Cohen, MD Associate Professor of Medicine University of Chicago Chicago, IL Disclosure Dr. Cohen has the following relevant financial relationships with commercial
1 st line chemotherapy and contribution of targeted agents in non-driver addicted NSCLC
 1 st line chemotherapy and contribution of targeted agents in non-driver addicted NSCLC Dr Ross Soo, FRACP National University Cancer Institute, Singapore National University Health System Cancer Science
1 st line chemotherapy and contribution of targeted agents in non-driver addicted NSCLC Dr Ross Soo, FRACP National University Cancer Institute, Singapore National University Health System Cancer Science
Recent advances in the management of metastatic breast cancer in older adults
 Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Angiogenesis in Ovarian Cancer
 Angiogenesis in Ovarian Cancer Dr Shibani Nicum Consultant Medical Oncologist and Lead for Gynae- Oncology Oxford University Hospitals Content 1. Epithelial Ovarian Cancer : epidemiology 2. Angiogenesis-normal
Angiogenesis in Ovarian Cancer Dr Shibani Nicum Consultant Medical Oncologist and Lead for Gynae- Oncology Oxford University Hospitals Content 1. Epithelial Ovarian Cancer : epidemiology 2. Angiogenesis-normal
Perioperative chemotherapy for colorectal cancer livermetastases: what is the optimal strategy?
 Perioperative chemotherapy for colorectal cancer livermetastases: what is the optimal strategy? Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be A classical case
Perioperative chemotherapy for colorectal cancer livermetastases: what is the optimal strategy? Prof Eric Van Cutsem, MD, PhD Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be A classical case
Strategy for the treatment of metastatic CRC through the lines
 Strategy for the treatment of metastatic CRC through the lines I Congresso de Oncologia D Or 2013: Satellite Symposium, ROCHE David Cosgrove, MD Johns Hopkins University Disclosures No relevant financial
Strategy for the treatment of metastatic CRC through the lines I Congresso de Oncologia D Or 2013: Satellite Symposium, ROCHE David Cosgrove, MD Johns Hopkins University Disclosures No relevant financial
What to do after 1st-line failure in mcrc?
 What to do after 1st-line failure in mcrc? Werner Scheithauer Univ.Klinik für Innere Med. I & CCC, Med.Uni.Wien-AKH mcrc front-line treatment strategy today Updated results of head-to-head trials in mcrc,
What to do after 1st-line failure in mcrc? Werner Scheithauer Univ.Klinik für Innere Med. I & CCC, Med.Uni.Wien-AKH mcrc front-line treatment strategy today Updated results of head-to-head trials in mcrc,
Lung Cancer Case. Since the patient was symptomatic, a targeted panel was sent. ALK FISH returned in 2 days and was positive.
 Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
Lung Cancer Case Jonathan Riess, M.D. M.S. Assistant Professor of Medicine University of California Davis School of Medicine UC Davis Comprehensive Cancer Center 63 year-old woman, never smoker, presents
Checkpoint Inibitors for Bladder Cancer
 Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better?
 Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Negative Trials in RCC: Where Did We Go Wrong? Can We Do Better? 9 th European Kidney Cancer Symposium, Dublin, April 2014 Tim Eisen Tim Eisen - Disclosures Company Research Support Advisory Board Trial
Evidenze cliniche nel trattamento del RCC
 Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
Criteri di scelta nel trattamento sistemico del carcinoma renale Evidenze cliniche nel trattamento del RCC Alessandro Morabito Unità Sperimentazioni Cliniche Istituto Nazionale Tumori di Napoli Napoli,
Karcinom dojke. PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski
 Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer
 Non-Small Cell Lung Cancer") Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer Jyoti D. Patel, MD Associate Professor Feinberg School of Medicine Robert H Lurie Comprehensive Cancer Center Northwestern
Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer Jyoti D. Patel, MD Associate Professor Feinberg School of Medicine Robert H Lurie Comprehensive Cancer Center Northwestern
The role of Maintenance treatment Appropriate endpoints according to ESMO consensus
 ESMO Preceptorship Programme Colorectal Cancer Singapore-October 20-22 2016 JY Douillard, MD, PhD, CMO ESMO The role of Maintenance treatment Appropriate endpoints according to ESMO consensus MAINTENANCE
ESMO Preceptorship Programme Colorectal Cancer Singapore-October 20-22 2016 JY Douillard, MD, PhD, CMO ESMO The role of Maintenance treatment Appropriate endpoints according to ESMO consensus MAINTENANCE
Review of the ESMO consensus conference on metastatic colorectal cancer Basic strategies and groups. Chemotherapy and targeted agents in 1st line
 ESMO Preceptorship Programme Colorectal Cancer Valencia, 18th May 2018 Review of the ESMO consensus conference on metastatic colorectal cancer Basic strategies and groups Chemotherapy and targeted agents
ESMO Preceptorship Programme Colorectal Cancer Valencia, 18th May 2018 Review of the ESMO consensus conference on metastatic colorectal cancer Basic strategies and groups Chemotherapy and targeted agents
OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER
 OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER E-Learning Module Stavros Gkolfinopoulos 1, Demetris Papamichael 1, George Pentheroudakis 2 1. Cyprus Oncology Centre, Nicosia, Cyprus 2.
OPTIMISING OUTCOMES FOR PATIENTS WITH ADVANCED COLORECTAL CANCER E-Learning Module Stavros Gkolfinopoulos 1, Demetris Papamichael 1, George Pentheroudakis 2 1. Cyprus Oncology Centre, Nicosia, Cyprus 2.
Medical Therapy of Colorectal Cancer in the Biomarker Era
 Medical Therapy of Colorectal Cancer in the Biomarker Era Axel Grothey Professor of Oncology Mayo Clinic College of Medicine Rochester, Minnesota Disclosures Consulting activities (honoraria went to the
Medical Therapy of Colorectal Cancer in the Biomarker Era Axel Grothey Professor of Oncology Mayo Clinic College of Medicine Rochester, Minnesota Disclosures Consulting activities (honoraria went to the
The next wave of successful drug therapy strategies in HER2-positive breast cancer. Hans Wildiers University Hospitals Leuven Belgium
 The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
Targe:ng HER2 in Metasta:c Breast Cancer in 2014
 Targe:ng HER2 in Metasta:c Breast Cancer in 2014 Kimberly L. Blackwell MD Professor Department of Medicine and Radia:on Oncology Duke University Medical Center Director, Breast Cancer Program Duke Cancer
Targe:ng HER2 in Metasta:c Breast Cancer in 2014 Kimberly L. Blackwell MD Professor Department of Medicine and Radia:on Oncology Duke University Medical Center Director, Breast Cancer Program Duke Cancer
Metastatic Renal Cancer Medical Treatment
 Metastatic Renal Cancer Medical Treatment Bohuslav Melichar, M.D., Ph.D. Professor and Head Department of Oncology Palacký University Medical School and Teaching Hospital Olomouc, Czech Republic Peculiarities
Metastatic Renal Cancer Medical Treatment Bohuslav Melichar, M.D., Ph.D. Professor and Head Department of Oncology Palacký University Medical School and Teaching Hospital Olomouc, Czech Republic Peculiarities
Understanding predictive and prognostic markers
 Understanding predictive and prognostic markers Professor Aimery de Gramont Chairman of ARCAD Foundation and GERCOR, Paris FRANCE Understanding predictive and prognostic markers Aimery de Gramont Prognostic
Understanding predictive and prognostic markers Professor Aimery de Gramont Chairman of ARCAD Foundation and GERCOR, Paris FRANCE Understanding predictive and prognostic markers Aimery de Gramont Prognostic
Targeted therapy in lung cancer : experience of NIO-RABAT
 Targeted therapy in lung cancer : experience of NIO-RABAT I.ELGHISSASSI, H.ERRIHANI Medical oncology department, NIO- RABAT 02-05- 2012, FEZ In Morocco, lung cancer is the most common tumor among men At
Targeted therapy in lung cancer : experience of NIO-RABAT I.ELGHISSASSI, H.ERRIHANI Medical oncology department, NIO- RABAT 02-05- 2012, FEZ In Morocco, lung cancer is the most common tumor among men At
Contemporary Management of Glioblastoma
 Contemporary Management of Glioblastoma Incidence Rates of Primary Brain Tumors Central Brain Tumor Registry of the United States, 1992-1997 100 Number of Cases per 100,000 Population 10 1 0.1 x I x I
Contemporary Management of Glioblastoma Incidence Rates of Primary Brain Tumors Central Brain Tumor Registry of the United States, 1992-1997 100 Number of Cases per 100,000 Population 10 1 0.1 x I x I
Ηπατοκυτταρικός Καρκίνος Συστηματική Θεραπεία. Θωμάς Μακατσώρης Επίκ. Καθ. Παθολογίας-Ογκολογίας Ιατρική Σχολή Πανεπιστημίου Πατρών 11/5/2018
 Ηπατοκυτταρικός Καρκίνος Συστηματική Θεραπεία Θωμάς Μακατσώρης Επίκ. Καθ. Παθολογίας-Ογκολογίας Ιατρική Σχολή Πανεπιστημίου Πατρών 11/5/2018 Advisory Board Disclosures Roche, Boeringer, Sanofi, Astra Zeneca,
Ηπατοκυτταρικός Καρκίνος Συστηματική Θεραπεία Θωμάς Μακατσώρης Επίκ. Καθ. Παθολογίας-Ογκολογίας Ιατρική Σχολή Πανεπιστημίου Πατρών 11/5/2018 Advisory Board Disclosures Roche, Boeringer, Sanofi, Astra Zeneca,
ANTI-EGFR IN MCRC? Assoc. Prof. Gerald Prager, Medical University of Vienna, Austria
 IS IT TIME TO RE-CHALLENGE ANTI-EGFR IN MCRC? Assoc. Prof. Gerald Prager, Medical University of Vienna, Austria Dr. Andrea Sartore-Bianchi, Oncologia Clinica Molecolare, Niguarda Cancer Center, Milano,
IS IT TIME TO RE-CHALLENGE ANTI-EGFR IN MCRC? Assoc. Prof. Gerald Prager, Medical University of Vienna, Austria Dr. Andrea Sartore-Bianchi, Oncologia Clinica Molecolare, Niguarda Cancer Center, Milano,
Chemotherapy for Advanced Gastric Cancer
 Chemotherapy for Advanced Gastric Cancer Andrés Cervantes Professor of Medicine DISCLOSURE OF INTEREST Employment: None Consultant or Advisory Role: Merck Serono, Roche, Beigene, Bayer, Servier, Lilly,
Chemotherapy for Advanced Gastric Cancer Andrés Cervantes Professor of Medicine DISCLOSURE OF INTEREST Employment: None Consultant or Advisory Role: Merck Serono, Roche, Beigene, Bayer, Servier, Lilly,
Cetuximab plus 5-FU/FA/oxaliplatin (FOLFOX-4) in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS)
 in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS)") Cetuximab plus 5-FU/FA/oxaliplatin (FOLFOX-4) in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS) C Bokemeyer, E Staroslawska, A Makhson, I Bondarenko, JT Hartmann,
Cetuximab plus 5-FU/FA/oxaliplatin (FOLFOX-4) in the first-line treatment of metastatic colorectal cancer: a large-scale Phase II study (OPUS) C Bokemeyer, E Staroslawska, A Makhson, I Bondarenko, JT Hartmann,
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents
 Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center