Systemic therapy of triple negative advanced breast cancer. Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development
|
|
|
- Edwin Casey
- 6 years ago
- Views:
Transcription



1 Systemic therapy of triple negative advanced breast cancer Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development
2 Outline State of the Art in the management of TN advanced breast cancer Dealing with heterogeneity of TN breast cancer Targeting subtypes and clinical trials Targeting pathways and immune-system
 TN 5 56 6 34 8 (18%) 6 (13%) 24 (24%) 9 (9%) 24 (40%) 19 (33%) Patients with TN Disease Received FewerTreatments and Stayed on Each Treatment Regimen For A Shorter Interval Seahet al, ASCO")
3 TNBC in the real life Line of CT Total TNBC ER+ HER (100%) 102 (100%) 58 (100%) (80%) 79 (77%) 44 (76%) HER (58%) 56 (55%) 69 (52%) ER (29%) 38 (37%) 30 (52%) TN (18%) 6 (13%) 24 (24%) 9 (9%) 24 (40%) 19 (33%) Patients with TN Disease Received FewerTreatments and Stayed on Each Treatment Regimen For A Shorter Interval Seahet al, ASCO 2012
4 Median PFS to Chemotherapy in TNBC Initial therapy First distant relapse Time on Treatment 12 weeks 9 weeks 4 weeks Median D.F.I. First line chemo Second line chemo Third line chemo
5 Taxanesfor TNBC Retrospective subgroup analyses Placebo arm data Trial Phase N Setting Taxane Outcome in TNBC CALGB III 44 First-or second-line metastatic Paclitaxel weekly and q3w ORR = 26% TTF = 2.8 months OS = 8.6 months ECOG III 110 First-line metastatic Paclitaxel weekly ORR = 11.7% 4 PFS = 5.3 months AVADO 3 III 52 First-line metastatic Docetaxel q3w ORR = 23.1% 4 PFS = 6.1 months 1. Harris, et al. Br Cancer Res 2006; 2. O Shaughnessy, et al. SABCS Glaspy, et al. EBCC 2010; 4. Roche data on file
6 Capecitabinefor TNBC Retrospective subgroup analyses Placebo arm data Trial Phase N Setting Treatment Outcome in TNBC Pooled analysis 1 III 208 Third-line or greater metastatic Capecitabine ORR = 15% PFS = 1.7 months RIBBON-1 2 III 50 First-line metastatic Capecitabine + placebo PFS = 4.2 months 1. Rugo, et al. SABCS Glaspy, et al. EBCC 2010
7 Platinum salts for TNBC Study Agent Multiple doses N First Line ORR(%) PFS BALI-1 Cisplatin 75 mg/m 2 q3w 48 73% 6 (10.3%) 1.5 m BSI-201 Carbo -Gem AUC 2 d1, 8 q3w 62 59% 20 (32%) 3.3 m 1000 mg/m 2 d1, 8 TBCRC 001 Carbo Cetuximab AUC 2 d1, 8, 15 q4w 71 46% 13 (18%) 2.0 m
8 Targeting Triple Negative Bevacizumab beyond progression TANIA (von Minckwitz et al, Lancet Oncol 2014) PFS Manteinancewith capecitabineand bevacizumab following response to Bevacizumab IMELDA (Gligorov et al, Lancet Oncol 2014) OS
9 Ideal drug Efficacy(ORR, pfs) Safety profile Impact on QoL 3 Ideal drug Comorbidity Performance status Target oriented Schedule
10 Real life therapy Treatment Efficacy(ORR, PFS) Impact on Quality of Life Safety profile 3 Performance Status Comorbidity Target oriented Convenience of the Schedule
11 Real life therapy Treatment Efficacy(ORR, PFS) Impact on Quality of Life Safety profile 3 Performance Status Comorbidity Target oriented Convenience of the Schedule
12 Real life therapy Treatment Efficacy(ORR, PFS) Impact on Quality of Life Safety profile 3 Performance Status Comorbidity Target oriented Convenience of the Schedule
13 Clinical Heterogeneity of TNBC Subtype Gene expression profile Clinical Basal-like 1 high Ki-67; DNA damage response BRCA-associated Basal-like 2 GF pathways Higher pcr Immunomodulatory Immune genes Mesenchymal Cell motility Lower DDFS Mesenchymal stem-like Cell motility; claudin-low Luminal androgen receptor Steroid pathways Lehman BD, et al. J Clin Invest 2011;121: Apocrine features, higher LRF; PI3Kmut


14 Basal like 1 TNBC Triple negative breast cancer and BRCA-mutations Clinical behavior Genomic instability Stephens et al Nature 2009 vol. 462 (7276) pp 1005
15 Basal like 1 TNBC 54 Stage IV women Inherited BRCA1/2 Olaparib100 mg pobid Olaparib400 mg pobid Primary endpoint = Objective response rate Secondary endpoints: % tumor change Progression-free survival Demographics 400 bid (n=27) Prior chemo 3 (1-5) BRCA1 67% Triple negative 50% 30% reduced doses, 30% delayed doses for toxicity TuttA et al, Lancet 2011 Efficacy (400 bid) (n=27) n (%) Overall response rate 11 (41) CR 1 (4) PR 10 (37)
16 PARP inhibitors in metastatic TNBC gbrca1 / BRCA2 Carriers Advanced anthracycline taxane resistant breast cancer Niraparib BRAVO Trial R BMN 673 EMBRACA - NCT OLYMPIAD Olaparib-NCT Potent PARP inhibitor at MTD as continuous exposure Physician Choice within SOC options Capecitabine or Vinorelbine or Eribulin or Gemcitabine Primary endpoint PFS
17 PARP inhibition in basal like 1 Agent Company Route Current trials Rucaparib Clovis IV/oral BRCA+ Post neoadjuvant TNBC + cisplatin Olaparib AstraZeneca Oral BRCA+ Veliparib Abbott Oral BRCA+, TNBC TemodalPaclitaxel CBDCA Iniparib BiPar/ Sanofi Aventis LT673 Biomarin Oral - INO-1001 Inotek/Genentech IV MK4827 Merck Oral CEP 9722 Cephalon Oral E7016 Eisai/MGI Pharma Oral IV Dose escalation
18 Cisplatinin basal like 1 ER-, PgR-/unknown & HER2- or known BRCA1/2 Metastatic or recurrent locally advanced Exclusions include: Adjuvant taxane in 12 months Previous platinum treatment Non-anthracyclines for MBC A Priori subgroup analyses: BRCA1/2 mutationrandomise Basal-like subgroups (PAM50 (1:1) and IHC) Biomarkers of HRD TuttA et al, 2104 Carboplatin (C) AUC6 q3w, 6 cycles On progression, crossover if appropriate n-376 BRCA1/2 = 9%/12% Docetaxel (D) 100mg/m 2 q3w, 6 cycles On progression, crossover if appropriate Docetaxel (D) 100mg/m 2 q3w, 6 cycles Carboplatin (C) AUC6 q3w, 6 cycles 18
19 Cisplatinin basal like 1 Randomised treatment -all patients (N=376) % with OR at cycle 3 or 6 (95% CI) Carboplatin Docetaxel 59/188 (31.4%) 67/188 (35.6%) Absolute difference (C-D) -4.2% (95% CI to 5.3) Exact p = 0.44 Crossover treatment - all patients (N=182) % with OR at cycle 3 or 6 (95% CI) Carboplatin (Crossover=Docetaxel) Docetaxel (Crossover=Carboplatin) 21/92* (22.8%) 23/90* (25.6%) Absolute difference (D-C) -2.8% (95% CI to 9.6) Exact p = 0.73 *Denominator excludes those with no first progression and those not starting crossover treatment 19 Tutt, SABCS 2014
20 Cisplatinin basal like 1 % patients progression free Median PFS: Carboplatin: 3.1 mths(95% CI = 2.5 to 4.2) Docetaxel: 4.5 mths(95% CI = 4.1 to 5.2) Restricted mean survival to 15 mths: Carboplatin: 4.8 mths Docetaxel: 5.2 mths Absolute difference: -0.4 (95% CI -1.1 to 0.3) p = 0.29 Carboplatin = 181 /188 0 Docetaxel= / Months from randomisation Number of events/at risk C: 0/188 90/98 40/56 32/22 9/13 5/8 0/7 D: 0/188 57/130 60/69 48/20 7/13 6/5 202/3
21 Cisplatinin basal like 1 % patients alive Median OS: Carboplatin: 12.4 mths (95% CI = 10.4 to 15.3) Docetaxel: 12.3 mths (95% CI = 10.5 to 13.6) 40 Restricted mean survival to 15 mths: 30 Carboplatin: 10.7 mths Docetaxel: 10.8 mths 20 Absolute difference: (95% CI -1.1 to 0.8) p = Months from randomisation Number of events/at risk C: 0/188 23/165 18/141 24/114 22/89 14/71 22/44 D: 0/188 11/176 20/151 35/110 19/85 23/58 16/39 21
22 Cisplatinin basal like 1 GermlineBRCA 1/2 Mutation (n=43) Carboplatin Docetaxel No GermlineBRCA 1/2 Mutation (n=273) Percentage with OR at cycle 3 or 6 (95% CI) /25 (68.0%) 6/18 (33.3%) Absolute difference (C-D) 34.7% (95% CI 6.3 to 63.1) Exact p = 0.03 Percentage with OR at cycle 3 or 6 (95% CI) Carboplatin Docetaxel 36/128 (28.1%) 53/145 (36.6%) Absolute difference (C-D) -8.5% (95% CI to 2.6) Exact p = 0.16 Interaction: randomised treatment & BRCA 1/2 status: p =
23 Cisplatinin basal like 1 % patients progression free Median PFS: C + BRCA 1/2 mutated 6.8mnths (95% CI = 4.4 to 8.1) C + BRCA1/2 not mutated 3.1mnths (95% CI = 2.4 to 4.2) Carboplatin + BRCA1/2 mutated Carboplatin + BRCA1/2 not mutated Months from randomisation Tutt, SABCS 2014


24 Basal like 2:Growth factor signalling Lisa A. Carey et al. JCO 2012;30:
25 Basal like 2:Growth factor signalling Lisa A. Carey et al. JCO 2012;30:
26 Basal like 2:Growth factor signalling The combination of cetuximab plus Carboplatin in metastatic TNBC produced responses in fewer than 20% of patients. EGFR pathway analysis showed that most TNBCs involved activation. Lisa A. Carey et al. JCO 2012;30:
27 Clinical Heterogeneity of TNBC Subtype Gene expression profile Clinical Basal-like 1 high Ki-67; DNA damage response BRCA-associated Basal-like 2 GF pathways Higher pcr Immunomodulatory Immune genes Mesenchymal Cell motility Lower DDFS Mesenchymal stem-like Cell motility; claudin-low Luminal androgen receptor Steroid pathways Lehman BD, et al. J Clin Invest 2011;121: Apocrine features, higher LRF; PI3Kmut
28 Evidencefrom clinicaltrials
29 Pembrolizumabin TNBC Recurrent or metastatic ER-/PR-/HER2- breast cancer ECOG PS 0-1 PD-L1+ tumour No systemic steroid therapy Pembro 10 mg/kg Q2W CR PR/SD Discontinuation permitted Treat for 24 moor until PD or toxicity No autoimmune disease (active or history of) No active brain metastases Confirmed PD Discontinue PD-L1 positivity: 58% of all patients screened had PD-L1-positive tumors Treatment: 10 mg/kg IV Q2W Response assessment: Performed every 8 weeks per RECIST v1.1 a PD-L1 expression was assessed in archival tumor samples using a prototype IHC assay and the 22C3 antibody. Only patients with PD-L1 staining in the stroma or in 1% of tumor cells were eligible for enrollment. b If clinically stable, patients are permitted to remain on pembrolizumab until progressive disease is confirmed on a second scan performed 4 weeks later. If progressive disease is confirmed, pembrolizumab is discontinued. An exception may be granted for patients with clinical stability or improvement after consultation with the sponsor.
30 Pembrolizumabin TNBC n =32 Confirmed complete response (nodal disease) Confirmed partial response Stable disease Progressive disease Objective response rate: 18.5% Stable disease: 25.9% Nanda, SABCS 2015
31 Pembrolizumabin TNBC Responder Nonresponder PD after CR, PR, or SD Last dose Treatment ongoing Best overall response CR PR SD PD Median follow-up duration: 9.9 months (range, ) Median time to response: 18 weeks (range, 7-32) Median duration of response a : not reached (range, 15 to 40+ weeks) PFS 1.9 ms; 6 mspfs-23% Time, weeks a Kaplan-Meier estimate. Analysis cut-off date: November 10, Nanda, SABCS 2014
32 Phase IbStudy of Atezolizumaband Nab- Paclitaxel in mtnbc Best Overall Response 1L (n = 9) Confirmed ORR (95% CI) a 66.7% (29.9, 92.5) ORR 88.9% (95% CI) b (51.7, 99.7) 2L (n = 8) 25% (3.2, 65.1) 75.0% (34.9, 96.8) 3L+ (n = 7) 28.6% (3.7, 71.0) 42.9% (9.9, 81.6) All Patients N = % (22.1, 63.4) 70.8% (48.9, 87.4) CR 11.1% % PR 77.8% 75.0% 42.9% 66.7% Response rates were higher for patients who received atezolizumab/nabpaclitaxel treatment as 1L therapy compared to 2L+ SD 11.1% 25.0% 28.6% 20.8% PD % 8.3% a Confirmed ORR defined as at least 2 consecutive assessments of complete or partial response. b Including investigator-assessed unconfirmed responses. Efficacy-evaluable patients were dosed by June 1, 2015, and were evaluable for response by RECIST v1.1. Minimum efficacy follow up was 3 months. Adams S, et al. SABCS [abstract ].



33 Phase IbStudy of Atezolizumaband Nab- Paclitaxel in mtnbc Including investigator-assessed unconfirmed responses. 11 of 17 responses (65%) continued on treatment at time of data cut off Adams S, et al. SABCS [abstract ].
34 Phase IbStudy of Atezolizumaband Nab- Paclitaxel in mtnbc PD-L1 IHC IC Status Patients N = 24 PD-L1 IHC TC Status Patients N = 24 IC3 ( 10%) a 1 IC2 ( 5% and <10%) IC1 ( 1% and < 5%) IC0 (< 1%) TC3 ( 50%) TC2 ( 5% and < 50%) TC1 ( 1% and < 5%) TC0 (< 1%) Unknown 8 Unknown 8 a Percent of IC or TC staining positive for PD-L1. Expression of PD-L1 in TNBC is mostly restricted to IC Adams S, et al. SABCS [abstract ].
35 Phase IbStudy of Atezolizumaband Nab- Paclitaxel in mtnbc IC0 (n = 7) IC1/2/3 (n = 9) Unknown (n = 8) ORR (95% CI) 57.1% (18.4, 90.1) 77.8% (40.0, 97.2) 75% (34.9, 96.8) CR % PR 57.1% 77.8% 62.5% SD 42.9% 22.2% 0 PD % Including investigator-assessed unconfirmed responses. Responses were observed in both IC0 and IC1/2/3 patients Adams S, et al. SABCS [abstract ].

36 Phase IbStudy of Atezolizumaband Nab- Paclitaxel in mtnbc Proliferating activated CD8+ T cells transiently peaked at the end of the first cycle of atezolizumab treatment Adams S, et al. SABCS [abstract ].
37 Phase III Study of Atezolizumaband Nab- Paclitaxel in mtnbc Randomized, double-blind, placebo-controlled Phase 3 trial of nab-paclitaxel ±atezolizumabas 1 st line therapy in mtnbc(nct ) Study design Histologically documented locally advanced or metastatic TNBC No prior therapy for advanced disease ECOG PS 0-1 Measurable disease per RECIST v1.1 Patients with significant CV or CNS disease (except asymptomatic brain metastases), autoimmune disease or prior checkpoint inhibitor therapy are excluded Target accrual: ~350 pts Stratification factors: Presence of liver metastases Prior taxanetherapy Nab-paclitaxel 100 mg/m 2 QW 3/4 + Atezolizumab 840 mg Q2W PD-L1 expression status (centrally evaluated by IHC using the SP142 assay) R 1:1 Nab-paclitaxel 100 mg/m 2 QW 3/4 + Placebo Q2W Co-primary endpoints: PFS in all patients PFS according to PD-L1 expression Secondary endpoints: OS ORR Response duration Safety/tolerability PK HR QoL Emens et al. SABCS 2015 (abstract OT )
38 Immunotherapy in TNBC
39 Immunotherapy in TNBC Phase Setting Subtype PD-L1 expression as inclusion criteria Combination/comparator Primary EP Nivolumab II Metastatic TN No Monotherapy after inductionwith RT and CT Pembrolizumab II Metastatic IBC HER2- No monotherapy Disease control rate Ib/II Metastatic TN No + eribulin DLT/ORR II Metastatic TN CohortB (positive) Cohort C (strong) Ib/II Metastatic/ LABC TN Presenceof PD-L1 expression monotherapy PFS ORR/Safety + nabpaclitaxel Safety/ORR II Metastatic HR+ No + Tamoxifen + Vorinostat Safety/ORR Atezolizumab III Metastatic TN No + nabpaclitaxelvs nabpaclitaxel Durvalumab II Metastatic HER2- No + tremelimumab(az) ORR PFS
40 Adaptive Phase II Randomized Non-comparative Trial of NivolumabAfter Induction Treatment in Triple-negative Breast Cancer (TNBC) Patients: TONIC-trial (The Netherlands Cancer Institute) Treatment Arm Active Comparator: Radiation therapy Radiotherapy on metastatic lesion Active Comparator: Low dose doxorubicin 15mgflatdose,onceweeklyfor2weeks Active Comparator: Cyclophosphamide metronomic schedule, 50 mg daily orally for 2weeks Active Comparator: Cisplatin 40mg/m2,weeklyfor2weeks Active Comparator: No induction treatment Assigned intervention Nivolumab 3 mg/kg, every 2 weeks after induction treatment Radiation: Radiation therapy 20 Gy to metastatic lesion Nivolumab 3 mg/kg, every 2 weeks after induction treatment Low dose doxorubicn Nivolumab 3 mg/kg, every 2 weeks after induction treatment Metronomics CTX Nivolumab 3 mg/kg, every 2 weeks after induction treatment Weekly cisplatin Nivolumab 3 mg/kg, every 2 weeks after induction treatment


41 Targeting stromaand inflammation G. Curigliano et al. The Breast, 2015
 No active brain metastases Pembro")


42 Targeting stromaand inflammation Recurrent or metastatic LBC or IBC ECOG PS 0-1 No systemic steroid therapy No autoimmune disease (active or history of) No active brain metastases Pembro 200 mg Q3W + CTX 50 mg/die Complete Response Partial Response or Stable Disease Confirmed Progressive Disease b Discontinuation Permitted Treat for 24 months or until progression or intolerable toxicity Discontinue PD-L1 positivity: Stratification factor Treatment: metronomic CT plus pembrolizumab Response assessment: Performed every 8 weeks per RECIST v1.1 PI G. Curigliano et al.
43 Immunotherapyof TNBC? Is there a rational for immune-based therapy in TNBC? YES Evidences from clinical data? LIMITED Can you enhance immunogenicity? MAY BE Can we monitor and to predict response? NO, BUT
44 Clinical Heterogeneity of TNBC Subtype Gene expression profile Clinical Basal-like 1 high Ki-67; DNA damage response BRCA-associated Basal-like 2 GF pathways Higher pcr Immunomodulatory Immune genes Mesenchymal Cell motility Lower DDFS Mesenchymal stem-like Cell motility; claudin-low Luminal androgen receptor Steroid pathways Lehman BD, et al. J Clin Invest 2011;121: Apocrine features, higher LRF; PI3Kmut

45 Notch pathway Phase 1b Study of docetaxel + PF in Triplenegative Breast Cancer PF
46 Notch pathway Characteristic Mean (range) age, years PF 100 mg BID/ D 75 mg/m 2 (N = 8) PF 100 mg BID/ D 100 mg/m 2 (N = 3) PF 150 mg BID/ D 75 mg/m 2 (N = 11) All Dose Levels (N = 22) 57 (43-76) 43 (32-64) 46 (27-69) 50 (27-76) ECOG PS, n (%) 0/1 4/4 (50/50) 1/2 (33/67) 8/3 (73/27) 13/9 (59/41) Primary Diagnosis, n 1/7 (13/87) 0/3 (0/100) 3/8 (27/73) 4/18 (18/82) (%) locally recurrent/metastatic Prior Systemic Therapies, n (%) 1st line/ 2 nd line 4/4 (50/50) 3/0 (100/0) 7/4 (64/36) 14/8 (64/36) G Curigliano, ASCO 2015
47 Clinical Heterogeneity of TNBC Subtype Gene expression profile Clinical Basal-like 1 high Ki-67; DNA damage response BRCA-associated Basal-like 2 GF pathways Higher pcr Immunomodulatory Immune genes Mesenchymal Cell motility Lower DDFS Mesenchymal stem-like Cell motility; claudin-low Luminal androgen receptor Steroid pathways Lehman BD, et al. J Clin Invest 2011;121: Apocrine features, higher LRF; PI3Kmut

48 Luminal Androgen Receptor Enzalutamide Inhibits AR Signaling in 3 Different Ways Preclinical Activity of Enzalutamide in an AR+ TNBC Cell Line (MDA-MB-453) 1 T Enzalutamide: Inhibits binding of androgens to AR T AR Cell cytoplasm Enza Enza 2 3 Inhibits AR nuclear translocation Inhibits AR-mediated DNA binding AR Cell nucleus AR = androgen receptor T = testosterone. 48 DHT = dihydrotestosterone; TNBC = triple-negative breast cancer. Cochrane DR et al. Breast Cancer Res. 2014;16:R7; Traina TA et al. J Clin Oncol. 2015;33(suppl 7):abstr 1003.
49 Luminal Androgen Receptor Eligibility AR positive advanced TNBC* ECOG-PS 1 Any number of prior therapies permissible Evaluable bone-only disease allowed No CNS metastases Sufficient tissue to enable biomarker discovery Endpoints Primary CBR16 Other Key Endpoints CBR24 Response rate PFS OS Safety AR biomarker discovery Treatment Enzalutamide 160 mg/day orally Stage 1 3 of 26 Evaluable have CBR16 Go to Stage 2 Stage 2 9 of 62 Evaluable have CBR16 Rejection of H 0 Statistical Considerations 85% power to detect true CBR16 = 8% tested against 1-sided alternative (CBR16 20%); alpha = 5% *A separate consent allowed tissue submission for central AR IHC testing at any time. AR positive was defined as IHC staining in >0% of tumor nuclei. Physicians and patients were blinded to actual % AR staining. AR = androgen receptor; CBR = clinical benefit rate; CBR16 = 16-week CBR; CBR24 = 24- week CBR; ECOG-PS = Eastern Cooperative Oncology Group Performance Status; H 0 = null hypothesis; IHC = immunohistochemistry; ITT = intent-totreat.; TNBC = triple negative breast cancer NCT Courtesy of J. Cortes, ECCO 2015
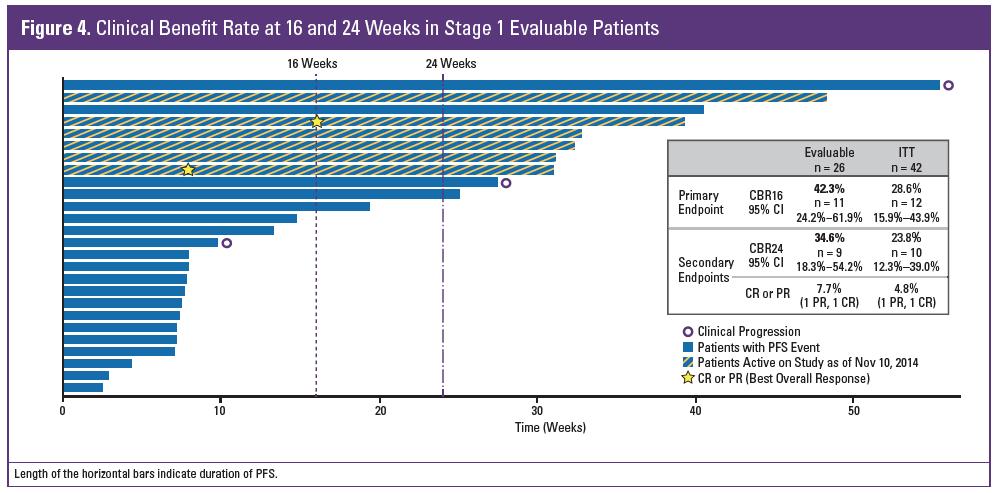
50 Response to enzalutamide
51 Luminal Androgen Receptor Hierarchical clustering according to biology AR IHC CBR16 PREDICT AR AR IHC 1% <1% CBR16 Yes No Not treated PREDICT AR Positive Negative Responders clustered within a recognized and distinct pattern that includes AR genes significantly different in responders at 1% false discovery rate A diagnostic test (PREDICT AR) was created and validated Parker, et al ASCO 2015 Data Cut-off 01 July 2015 *Includes duplicates and samples from tissue collected for optional AR testing.; CBR16 = clinical benefit rate at week 16; AR = androgen receptor; IHC immunohistochemistry 1. Doane AS et al. Oncogene. 2006;25: ; 2. Farmer P et al. Oncogene. 2005;24: ; 3. Smid M et al. Cancer Res. 2008;68: ; 4. Charafe-Jauffret E et al. Oncogene. 2006;25: Parker, et al J Clin Oncol NCT Courtesy of J. Cortes, ECCO 2015
52 Luminal Androgen Receptor ITT Population 100 n = 118 Overall Survival (%) PREDICT AR mos 32.3 weeks (95% CI: 20.7, 48.3) PREDICT AR+ mos 75.6 weeks (95% CI: 51.6, 91.4) 0 Patients at risk PREDICT AR+ PREDICT AR Data cutoff 1Jul2015 ITT = intent to treat; mos = median survival; CI = confidence interval; Weeks PREDICT AR+ mos 18.0 months PREDICT AR mos 7.5 months NCT Courtesy of J. Cortes, ECCO 2015
53 Luminal Androgen Receptor 100 n = 63 Overall Survival (%) PREDICT AR mos 43.4 weeks (95% CI: 32.9, NYR) PREDICT AR+ mos NYR (95% CI: 55.4, NYR) 0 Patients at risk PREDICT AR+ PREDICT AR Data cutoff 1Jul2015. CI= confidence interval; mos = median survival; NYR = not yet reached Weeks PREDICT AR+ mos not yet reached PREDICT AR mos 10.1 months NCT Courtesy of J. Cortes, ECCO 2015
54 Challenges Small phase II maybe NOT be enough to interpret data Run large trials in low-incidence disease to generate knowledge about drug and disease Change statistical hypothesis since expectations are higher now
55 Conclusions Select the right partner and validate studies with the same backbone Demonstrate bioactivity and not MTD Metastatic breast cancer is not always the right setting: Neoadjuvant Post-neoadjuvant can be more informative
56 Thank you Slides available contacting:
Management of Triple Negative Breast Cancer. Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology
 Management of Triple Negative Breast Cancer Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology Outline Heterogeneity of TNBC Targeting TNBC by subtypes New antibody drug
Management of Triple Negative Breast Cancer Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology Outline Heterogeneity of TNBC Targeting TNBC by subtypes New antibody drug
ESMO Preceptorship Breast Cancer. Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development Istituto Europeo di Oncologia
 ESMO Preceptorship Breast Cancer Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development Istituto Europeo di Oncologia Outline Rational for immune-based therapy in BC How to
ESMO Preceptorship Breast Cancer Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development Istituto Europeo di Oncologia Outline Rational for immune-based therapy in BC How to
Treatment of Triple Negative Breast Cancer. Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology
 Treatment of Triple Negative Breast Cancer Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology Outline Neoadjuvant treatment in triple negative EBC Picking optimal adjuvant
Treatment of Triple Negative Breast Cancer Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology Outline Neoadjuvant treatment in triple negative EBC Picking optimal adjuvant
ENFERMEDAD AVANZADA Qué hacemos con el triple negativo? Nuevas aproximaciones
 ENFERMEDAD AVANZADA Qué hacemos con el triple negativo? Nuevas aproximaciones Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative
ENFERMEDAD AVANZADA Qué hacemos con el triple negativo? Nuevas aproximaciones Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative
Triple Negative Breast Cancer: Part 2 A Medical Update
 Triple Negative Breast Cancer: Part 2 A Medical Update April 29, 2015 Tiffany A. Traina, MD Breast Medicine Service Memorial Sloan Kettering Cancer Center Weill Cornell Medical College Overview What is
Triple Negative Breast Cancer: Part 2 A Medical Update April 29, 2015 Tiffany A. Traina, MD Breast Medicine Service Memorial Sloan Kettering Cancer Center Weill Cornell Medical College Overview What is
Alternativas terapéuticas en fenotipo triple negativo Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid
 Alternativas terapéuticas en fenotipo triple negativo Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative Breast Cancer Immunohistochemistry
Alternativas terapéuticas en fenotipo triple negativo Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative Breast Cancer Immunohistochemistry
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Overview and future horizons of PARP inhibitors in BRCAassociated. Judith Balmaña
 Overview and future horizons of PARP inhibitors in BRCAassociated breast cancer Judith Balmaña PARP inhibitors: Mechanism of action Clinical development: Monotherapy In combination with chemotherapy Ongoing
Overview and future horizons of PARP inhibitors in BRCAassociated breast cancer Judith Balmaña PARP inhibitors: Mechanism of action Clinical development: Monotherapy In combination with chemotherapy Ongoing
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC)
") Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
La malattia triplo negativa metastatica: quali trattamenti nella pratica clinica?
 2018 CARCINOMA MAMMARIO: I TRAGUARDI RAGGIUNTI E LE NUOVE SFIDE La malattia triplo negativa metastatica: quali trattamenti nella pratica clinica? Roma, 27 Ottobre 2018 Relatore: Francesca Poggio Disclosure
2018 CARCINOMA MAMMARIO: I TRAGUARDI RAGGIUNTI E LE NUOVE SFIDE La malattia triplo negativa metastatica: quali trattamenti nella pratica clinica? Roma, 27 Ottobre 2018 Relatore: Francesca Poggio Disclosure
非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和
 資料 2 2 非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和 1 Preclinical studies Therapeutic Window: Efficacy/Toxicity Disease Specificity Subtype Specificity Combination: Concurrent/Sequential Therapeutic situation: Response/
資料 2 2 非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和 1 Preclinical studies Therapeutic Window: Efficacy/Toxicity Disease Specificity Subtype Specificity Combination: Concurrent/Sequential Therapeutic situation: Response/
Triple Negative Breast Cancer. Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008
 Triple Negative Breast Cancer Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008 Triple Negative Breast Cancer 15% 25% Triple Negative 20% HER2+ ER+ Low Grade
Triple Negative Breast Cancer Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008 Triple Negative Breast Cancer 15% 25% Triple Negative 20% HER2+ ER+ Low Grade
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Triple Negative Breast cancer New treatment options arenowhere?
 Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer
 Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
PARP inhibitors for breast cancer
 PARP inhibitors for breast cancer Mark Robson, MD Memorial Sloan Kettering Cancer Center Agenda Mechanism of action Clinical studies Resistance mechanisms Future directions Poly (ADP-ribose) Polymerases
PARP inhibitors for breast cancer Mark Robson, MD Memorial Sloan Kettering Cancer Center Agenda Mechanism of action Clinical studies Resistance mechanisms Future directions Poly (ADP-ribose) Polymerases
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings. Eve Rodler, MD University of California at Davis October 2016
 Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
Breast Cancer Immunotherapy. Leisha A. Emens, MD PhD Johns Hopkins University Bloomberg Kimmel Institute for Cancer Immunotherapy
 Breast Cancer Immunotherapy Leisha A. Emens, MD PhD Johns Hopkins University Bloomberg Kimmel Institute for Cancer Immunotherapy Conflict of Interest I have the following financial relationships to disclose:
Breast Cancer Immunotherapy Leisha A. Emens, MD PhD Johns Hopkins University Bloomberg Kimmel Institute for Cancer Immunotherapy Conflict of Interest I have the following financial relationships to disclose:
Triple negative breast cancer -neoadjuvant and adjuvant systemic therapy
 Triple negative breast cancer -neoadjuvant and adjuvant systemic therapy Sung-Bae Kim, MD, PhD Department of Oncology Asan Medical Center University of Ulsan College of Medicine Seoul, Korea DISCLOSURE
Triple negative breast cancer -neoadjuvant and adjuvant systemic therapy Sung-Bae Kim, MD, PhD Department of Oncology Asan Medical Center University of Ulsan College of Medicine Seoul, Korea DISCLOSURE
Breast : ASCO Abstracts for Review
 Breast : ASCO 2011 Susana Campos, MD, MPH Dana Farber Cancer Institute Abstracts for Review Prevention Neoadjuvant Metastatic Brain mets LBA 504: Exemestane for primary prevention of breast cancer in postmenopausal
Breast : ASCO 2011 Susana Campos, MD, MPH Dana Farber Cancer Institute Abstracts for Review Prevention Neoadjuvant Metastatic Brain mets LBA 504: Exemestane for primary prevention of breast cancer in postmenopausal
Triple-Negative Breast Cancer
 June 2017 Triple-Negative Breast Cancer Amir Sonnenblick, MD, PhD Sharett institute of oncology Hadassah-Hebrew university medical center, Jerusalem, Israel This presentation is the intellectual property
June 2017 Triple-Negative Breast Cancer Amir Sonnenblick, MD, PhD Sharett institute of oncology Hadassah-Hebrew university medical center, Jerusalem, Israel This presentation is the intellectual property
Expert Review: The Role of PARP Inhibition in the Treatment of Breast Cancer. Reference Slides
 Expert Review: The Role of PARP Inhibition in the Treatment of Breast Cancer Reference Slides Overview BRCA Mutations and Breast Cancer Patients with BRCA mutations have an estimated 55% to 65% cumulative
Expert Review: The Role of PARP Inhibition in the Treatment of Breast Cancer Reference Slides Overview BRCA Mutations and Breast Cancer Patients with BRCA mutations have an estimated 55% to 65% cumulative
TNBC: What s new Déjà vu All Over Again? Lucy R. Langer, MD MSHS Compass Oncology - SABCS 2016 Review February 21, 2017
 TNBC: What s new Déjà vu All Over Again? Lucy R. Langer, MD MSHS Compass Oncology - SABCS 2016 Review February 21, 2017 The problem with TNBC 1. Generally more aggressive 2. ONLY chemotherapy 3. No other
TNBC: What s new Déjà vu All Over Again? Lucy R. Langer, MD MSHS Compass Oncology - SABCS 2016 Review February 21, 2017 The problem with TNBC 1. Generally more aggressive 2. ONLY chemotherapy 3. No other
The next wave of successful drug therapy strategies in HER2-positive breast cancer. Hans Wildiers University Hospitals Leuven Belgium
 The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents
 Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute
 Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Immunotherapy for Breast Cancer Clinical Development
 Immunotherapy for Breast Cancer Clinical Development Laurence Buisseret, MD, PhD Breast Cancer Translational Research Laboratory Institut Jules Bordet Université Libre de Bruxelles (ULB) ESMO preceptorship
Immunotherapy for Breast Cancer Clinical Development Laurence Buisseret, MD, PhD Breast Cancer Translational Research Laboratory Institut Jules Bordet Université Libre de Bruxelles (ULB) ESMO preceptorship
Novel Chemotherapy Agents for Metastatic Breast Cancer. Joanne L. Blum, MD, PhD Baylor-Sammons Cancer Center Dallas, TX
 Novel Chemotherapy Agents for Metastatic Breast Cancer Joanne L. Blum, MD, PhD Baylor-Sammons Cancer Center Dallas, TX New Chemotherapy Agents in Breast Cancer New classes of drugs Epothilones Halichondrin
Novel Chemotherapy Agents for Metastatic Breast Cancer Joanne L. Blum, MD, PhD Baylor-Sammons Cancer Center Dallas, TX New Chemotherapy Agents in Breast Cancer New classes of drugs Epothilones Halichondrin
Terapia sistemica neoadiuvante: in quali tumori? Quali risultati? Dott. Giacomo Pelizzari
 Terapia sistemica neoadiuvante: in quali tumori? Quali risultati? Dott. Giacomo Pelizzari Neoadjuvant Treatment A window of opportunity Rational: Historically proposed to enable breast-conserving surgery
Terapia sistemica neoadiuvante: in quali tumori? Quali risultati? Dott. Giacomo Pelizzari Neoadjuvant Treatment A window of opportunity Rational: Historically proposed to enable breast-conserving surgery
NOVITA SUL TRATTAMENTO DEL CARCINOMA MAMMARIO: MALATTIA TRIPLO NEGATIVA
 SUPERNOVAE IN ONCOLOGIA NOVITA SUL TRATTAMENTO DEL CARCINOMA MAMMARIO: MALATTIA TRIPLO NEGATIVA Dr. Matteo Lambertini U.O. Oncologia Medica 2 IRCCS AOU San Martino IST, Genova Pisa, 14 novembre 2015 AGENDA
SUPERNOVAE IN ONCOLOGIA NOVITA SUL TRATTAMENTO DEL CARCINOMA MAMMARIO: MALATTIA TRIPLO NEGATIVA Dr. Matteo Lambertini U.O. Oncologia Medica 2 IRCCS AOU San Martino IST, Genova Pisa, 14 novembre 2015 AGENDA
Post-ASCO 2017 Cancer du sein Triple Négatif
 Post-ASCO 217 Cancer du sein Triple Négatif A.Ladjeroud, K.Bouzid Centre Pierre et Marie Curie- Alger Oran, 3 Septembre 217 Phase III Investigation of Neoadjuvant Carboplatin ± Veliparib in Combination
Post-ASCO 217 Cancer du sein Triple Négatif A.Ladjeroud, K.Bouzid Centre Pierre et Marie Curie- Alger Oran, 3 Septembre 217 Phase III Investigation of Neoadjuvant Carboplatin ± Veliparib in Combination
Recent Therapeutic Advances for Thoracic Malignancies
 Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
Systemic therapy for TN advanced breast cancer
 Systemic therapy for TN advanced breast cancer Javier Cortes, Ramon y Cajal University Hospital, Madrid Vall d Hebron Institute of Oncology (VHIO) & Medica Scientia Innovation Research (MedSIR), Barcelona,
Systemic therapy for TN advanced breast cancer Javier Cortes, Ramon y Cajal University Hospital, Madrid Vall d Hebron Institute of Oncology (VHIO) & Medica Scientia Innovation Research (MedSIR), Barcelona,
Edith A. Perez, Ahmad Awada, Joyce O Shaughnessy, Hope Rugo, Chris Twelves, Seock-Ah Im, Carol Zhao, Ute Hoch, Alison L. Hannah, Javier Cortes
 BEACON: A Phase 3 Open-label, Randomized, Multicenter Study of Etirinotecan Pegol (EP) versus Treatment of Physician s Choice (TPC) in Patients With Locally Recurrent or Metastatic Breast Cancer Previously
BEACON: A Phase 3 Open-label, Randomized, Multicenter Study of Etirinotecan Pegol (EP) versus Treatment of Physician s Choice (TPC) in Patients With Locally Recurrent or Metastatic Breast Cancer Previously
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID
 DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
Cancer du sein métastatique et amélioration de la survie Pr. X. Pivot
 Cancer du sein métastatique et amélioration de la survie Pr. X. Pivot Date of preparation: November 2015. EU0250i TTP/PFS Comparaisons First line metastatic breast cancer Monotherapy Docetaxel Chan 1999
Cancer du sein métastatique et amélioration de la survie Pr. X. Pivot Date of preparation: November 2015. EU0250i TTP/PFS Comparaisons First line metastatic breast cancer Monotherapy Docetaxel Chan 1999
ESMO Preceptoship in Immuno-Oncology. Clinical Development: Breast Cancer
 ESMO Preceptoship in Immuno-Oncology Clinical Development: Breast Cancer Prof Giuseppe Curigliano, MD PhD University of Milano and Istituto Europeo di Oncologia Milano, Lombardia, Italy Outline Rational
ESMO Preceptoship in Immuno-Oncology Clinical Development: Breast Cancer Prof Giuseppe Curigliano, MD PhD University of Milano and Istituto Europeo di Oncologia Milano, Lombardia, Italy Outline Rational
Immunotherapy for the Treatment of Head and Neck Cancers. Barbara Burtness, MD Yale University
 Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Overview of nab-paclitaxel in Breast Cancer
 Overview of nab-paclitaxel in Breast Cancer William J. Gradishar MD FASCO FACP Betsy Bramsen Professor of Breast Oncology Robert H. Lurie Comprehensive Cancer Center Northwestern University Feinberg School
Overview of nab-paclitaxel in Breast Cancer William J. Gradishar MD FASCO FACP Betsy Bramsen Professor of Breast Oncology Robert H. Lurie Comprehensive Cancer Center Northwestern University Feinberg School
6/13/17. Disclosures. Treating Breast Cancer in People with Mutations. Off Label Use. I will be discussing off label use of medications today.
 Treating Breast Cancer in People with Mutations Steven J. Isakoff, MD, PhD Massachusetts General Hospital Cancer Center June 9, 2017 sisakoff@partners.org Disclosures Company ² Myriad Genetics ² AbbVie
Treating Breast Cancer in People with Mutations Steven J. Isakoff, MD, PhD Massachusetts General Hospital Cancer Center June 9, 2017 sisakoff@partners.org Disclosures Company ² Myriad Genetics ² AbbVie
Role of chemotherapy in BRCA and Triple negative breast cancer. Fernando Moreno Servicio de Oncología Médica Hospital Clinico San Carlos
 Role of chemotherapy in BRCA and Triple negative breast cancer Fernando Moreno Servicio de Oncología Médica Hospital Clinico San Carlos Association between TNBC & germline mutations in BRCA 1/2 TNBC is
Role of chemotherapy in BRCA and Triple negative breast cancer Fernando Moreno Servicio de Oncología Médica Hospital Clinico San Carlos Association between TNBC & germline mutations in BRCA 1/2 TNBC is
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Emerging Strategies in Triple-Negative Breast Cancer
 Expert Review in Immunotherapy in Breast Cancer Emerging Strategies in Triple-Negative Breast Cancer Reference Slide Deck Is Breast Cancer Immunogenic? Recent proof that breast cancer may elicit an immune
Expert Review in Immunotherapy in Breast Cancer Emerging Strategies in Triple-Negative Breast Cancer Reference Slide Deck Is Breast Cancer Immunogenic? Recent proof that breast cancer may elicit an immune
Triple negative breast cancer 2014 GASCO Annual meeting September 5 th 2014, Atlanta, GA
 Triple negative breast cancer 2014 GASCO Annual meeting September 5 th 2014, Atlanta, GA Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology,
Triple negative breast cancer 2014 GASCO Annual meeting September 5 th 2014, Atlanta, GA Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology,
10/15/2012. Inflammatory Breast Cancer vs. LABC: Different Biology yet Subtypes Exist
 Triple-Negative Breast Cancer: Optimizing Treatment for Locally Advanced Breast Cancer Beth Overmoyer MD Director, Inflammatory Breast Cancer Program Dana Farber Cancer Institute Overview Inflammatory
Triple-Negative Breast Cancer: Optimizing Treatment for Locally Advanced Breast Cancer Beth Overmoyer MD Director, Inflammatory Breast Cancer Program Dana Farber Cancer Institute Overview Inflammatory
EGFR inhibitors in NSCLC
 Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Immunotherapy in the clinic. Lung Cancer. Marga Majem 20 octubre 2017
 Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
A case of a BRCA2-mutated ER+/HER2 breast cancer during pregnancy
 ESMO Preceptorship Programme Breast Cancer Lisbon 16,17 September 2016 Emanuela Risi Sandro Pitigliani Medical Oncology Department Hospital of Prato, Istituto Toscano Tumori, Prato, Italy A case of a BRCA2-mutated
ESMO Preceptorship Programme Breast Cancer Lisbon 16,17 September 2016 Emanuela Risi Sandro Pitigliani Medical Oncology Department Hospital of Prato, Istituto Toscano Tumori, Prato, Italy A case of a BRCA2-mutated
Dieta Brandsma, Department of Neuro-oncology, Netherlands Cancer Institute, Amsterdam, The Netherlands
 What is hot in breast cancer brain metastases? Dieta Brandsma, Department of Neuro-oncology, Netherlands Cancer Institute, Amsterdam, The Netherlands 8th Annual Brain Metastases Research and Emerging Therapy
What is hot in breast cancer brain metastases? Dieta Brandsma, Department of Neuro-oncology, Netherlands Cancer Institute, Amsterdam, The Netherlands 8th Annual Brain Metastases Research and Emerging Therapy
Carrier Frequency. Breast Cancer and Treatment Options in Patients with BRCA1/2 mutations. Olivia Pagani On behalf of Bella Kaufman
 Breast Cancer and Treatment Options in Patients with BRCA1/2 mutations Olivia Pagani On behalf of Bella Kaufman Carrier Frequency Prevalence of an altered disease gene in a given population 1 Background
Breast Cancer and Treatment Options in Patients with BRCA1/2 mutations Olivia Pagani On behalf of Bella Kaufman Carrier Frequency Prevalence of an altered disease gene in a given population 1 Background
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist
 Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
NeoadjuvantTreatment In BC When, How, Who?
 NeoadjuvantTreatment In BC When, How, Who? Clifford Hudis, M.D. Chief, Breast Cancer Medicine Service, MSKCC Professor of Medicine, Weill Cornell Medical College President, ASCO 15 Potential Benefits Of
NeoadjuvantTreatment In BC When, How, Who? Clifford Hudis, M.D. Chief, Breast Cancer Medicine Service, MSKCC Professor of Medicine, Weill Cornell Medical College President, ASCO 15 Potential Benefits Of
New chemotherapy drugs in metastatic breast cancer. Guy Jerusalem, MD, PhD
 New chemotherapy drugs in metastatic breast cancer Guy Jerusalem, MD, PhD MBC Patients survival over time Median survival increases over time, but is still measured in months This is not yet a chronic
New chemotherapy drugs in metastatic breast cancer Guy Jerusalem, MD, PhD MBC Patients survival over time Median survival increases over time, but is still measured in months This is not yet a chronic
Breast Cancer and Treatment Options in Patients with BRCA1/2 mutations. Olivia Pagani On behalf of Bella Kaufman
 Breast Cancer and Treatment Options in Patients with BRCA1/2 mutations Olivia Pagani On behalf of Bella Kaufman Carrier Frequency Prevalence of an altered disease gene in a given population Background
Breast Cancer and Treatment Options in Patients with BRCA1/2 mutations Olivia Pagani On behalf of Bella Kaufman Carrier Frequency Prevalence of an altered disease gene in a given population Background
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Squamous Cell Carcinoma Standard and Novel Targets.
 Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
A view from the Oncology Clinic. Andrew Tu7 Consultant Clinical Oncologist
 A view from the Oncology Clinic Andrew Tu7 Consultant Clinical Oncologist Our pa'ents have become much more aware and are driving a changing demand Before surgery: MRI for contralateral BC; neoadjuvant
A view from the Oncology Clinic Andrew Tu7 Consultant Clinical Oncologist Our pa'ents have become much more aware and are driving a changing demand Before surgery: MRI for contralateral BC; neoadjuvant
Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma
 Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Systemic Therapy Considerations in Inflammatory Breast Cancer
 Systemic Therapy Considerations in Inflammatory Breast Cancer Shani Paluch-Shimon, MBBS, MSc Director, Breast Oncology Unit Shaare Zedek Medical Centre, Jerusalem Israel Disclosures Roche: Speakers bureau,
Systemic Therapy Considerations in Inflammatory Breast Cancer Shani Paluch-Shimon, MBBS, MSc Director, Breast Oncology Unit Shaare Zedek Medical Centre, Jerusalem Israel Disclosures Roche: Speakers bureau,
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
HER2-Targeted Rx. An Historical Perspective
 HER2-Targeted Rx An Historical Perspective Trastuzumab: Front Line Rx for MBC Median 20.3 v. 25.1 mo P = 0.046 HR 0.8 65% of control patients crossed over Slamon D, et al. N Engl J Med, 2001; 344:783 Trastuzumab:Front-line
HER2-Targeted Rx An Historical Perspective Trastuzumab: Front Line Rx for MBC Median 20.3 v. 25.1 mo P = 0.046 HR 0.8 65% of control patients crossed over Slamon D, et al. N Engl J Med, 2001; 344:783 Trastuzumab:Front-line
Immunoconjugates in Both the Adjuvant and Metastatic Setting
 Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Patient Selection: The Search for Immunotherapy Biomarkers
 Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Therapeutic Targets for Triple- Negative Breast Cancer: Focus on Platinums and EGFR Inhibition
 Therapeutic Targets for Triple- Negative Breast Cancer: Focus on Platinums and EGFR Inhibition Lisa A Carey, MD Disclosures for Lisa A Carey, MD No real or apparent conflicts of interest to disclose Basal-Like
Therapeutic Targets for Triple- Negative Breast Cancer: Focus on Platinums and EGFR Inhibition Lisa A Carey, MD Disclosures for Lisa A Carey, MD No real or apparent conflicts of interest to disclose Basal-Like
Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse?
 Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse? Mark A. Socinski, MD Professor of Medicine Multidisciplinary Thoracic Oncology Program Lineberger Comprehensive
Maintenance Therapy for Advanced NSCLC: When, What, Why & What s Left After Post-Maintenance Relapse? Mark A. Socinski, MD Professor of Medicine Multidisciplinary Thoracic Oncology Program Lineberger Comprehensive
PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER. Virginie Westeel Chest Disease Department University Hospital Besançon, France
 PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER Virginie Westeel Chest Disease Department University Hospital Besançon, France LEARNING OBJECTIVES 1. To understand the potential of perioperative
PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER Virginie Westeel Chest Disease Department University Hospital Besançon, France LEARNING OBJECTIVES 1. To understand the potential of perioperative
The Role of Angiogenesis Inhibition in Breast Cancer Today: Lessons Learned
 The Role of Angiogenesis Inhibition in Breast Cancer Today: Lessons Learned Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education UCSF Helen Diller Family Comprehensive
The Role of Angiogenesis Inhibition in Breast Cancer Today: Lessons Learned Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education UCSF Helen Diller Family Comprehensive
Locally Advanced Breast Cancer: Systemic and Local Therapy
 Locally Advanced Breast Cancer: Systemic and Local Therapy Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
Locally Advanced Breast Cancer: Systemic and Local Therapy Joseph A. Sparano, MD Professor of Medicine & Women s Health Albert Einstein College of Medicine Associate Chairman, Department of Oncology Montefiore
METRIC Study Key Eligibility Criteria
 The METRIC Study METRIC Study Key Eligibility Criteria The pivotal METRIC Study is evaluating glembatumumab vedotin in patients with gpnmb overexpressing metastatic triple-negative breast cancer (TNBC).
The METRIC Study METRIC Study Key Eligibility Criteria The pivotal METRIC Study is evaluating glembatumumab vedotin in patients with gpnmb overexpressing metastatic triple-negative breast cancer (TNBC).
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy
 Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Systemic Treatment of Triple Negative Breast Cancer
 Systemic Treatment of Triple Negative Breast Cancer Christoph Zielinski Comprehensive Cancer Center Medical University Vienna General Hospital, Vienna, Austria and Central European Cooperative Oncology
Systemic Treatment of Triple Negative Breast Cancer Christoph Zielinski Comprehensive Cancer Center Medical University Vienna General Hospital, Vienna, Austria and Central European Cooperative Oncology
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Amreen Husain, 10 Eric P. Winer, 11 Sylvia Adams, 12 Peter Schmid 13
 IMpassion130: Efficacy in immune biomarker subgroups from the global, randomized, double-blind, placebo-controlled, Phase III study of atezolizumab + nab-paclitaxel in patients with treatment-naive, locally
IMpassion130: Efficacy in immune biomarker subgroups from the global, randomized, double-blind, placebo-controlled, Phase III study of atezolizumab + nab-paclitaxel in patients with treatment-naive, locally
Management of Incurable Prostate Cancer in 2014
 Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
Management of Incurable Prostate Cancer in 2014 Julie N. Graff, MD, MCR Portland VA Medical Center Assistant Professor of Medicine Knight Cancer Institute, OHSU 2014: Cancer Estimates Stage at Diagnosis
Pathways Underlying Aggressive Breast Cancers
 Origin of Breast Cancer Subtypes Pathways Underlying Aggressive Breast Cancers HER2 and ER can be expressed in any subtype. Triple Negative -- a mixture of subtypes Joyce O Shaughnessy, MD Baylor Sammons
Origin of Breast Cancer Subtypes Pathways Underlying Aggressive Breast Cancers HER2 and ER can be expressed in any subtype. Triple Negative -- a mixture of subtypes Joyce O Shaughnessy, MD Baylor Sammons
Recent Update in Management of Breast Cancer: Medical Oncology. Jin Hee Ahn, M.D., PhD. 23-April-2015
 2015 GBCC & 4 th IBCS 1/37 Recent Update in Management of Breast Cancer: Medical Oncology Jin Hee Ahn, M.D., PhD. 23-April-2015 Department of Oncology, Asan Medical Center, UUCM, Seoul, Korea 2/37 3/37
2015 GBCC & 4 th IBCS 1/37 Recent Update in Management of Breast Cancer: Medical Oncology Jin Hee Ahn, M.D., PhD. 23-April-2015 Department of Oncology, Asan Medical Center, UUCM, Seoul, Korea 2/37 3/37
Combined Modality Therapy State of the Art. Everett E. Vokes The University of Chicago
 Combined Modality Therapy State of the Art Everett E. Vokes The University of Chicago What we Know Some patients are cured (20%) Induction and concurrent chemoradiotherapy are each superior to radiotherapy
Combined Modality Therapy State of the Art Everett E. Vokes The University of Chicago What we Know Some patients are cured (20%) Induction and concurrent chemoradiotherapy are each superior to radiotherapy
Update on Breast Cancer
 Update on Breast Cancer William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center Feinberg School of Medicine Northwestern University Overview PARP Inhibitors Neoadjuvant
Update on Breast Cancer William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center Feinberg School of Medicine Northwestern University Overview PARP Inhibitors Neoadjuvant
Breast cancer treatment
 Report from the San Antonio Breast Cancer Symposium Breast cancer treatment Determining the best options for select patient groups Sara Soldera, MD, Resident; Nathaniel Bouganim, MD, FRCPC, Medical Oncologist;
Report from the San Antonio Breast Cancer Symposium Breast cancer treatment Determining the best options for select patient groups Sara Soldera, MD, Resident; Nathaniel Bouganim, MD, FRCPC, Medical Oncologist;
PROSTATE CANCER HORMONE THERAPY AND BEYOND. Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute
 PROSTATE CANCER HORMONE THERAPY AND BEYOND Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute Disclosures I am a Consultant for Bayer and Sanofi-Aventis
PROSTATE CANCER HORMONE THERAPY AND BEYOND Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute Disclosures I am a Consultant for Bayer and Sanofi-Aventis
Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy. Raanan Berger MD PhD Sheba Medical Center, Israel
 Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy Raanan Berger MD PhD Sheba Medical Center, Israel Disclosures Honoraria, Ad board BMS, MSD, Pfizer, Astra Zeneca, Bayer,
Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy Raanan Berger MD PhD Sheba Medical Center, Israel Disclosures Honoraria, Ad board BMS, MSD, Pfizer, Astra Zeneca, Bayer,
Sustained benefits for women with HER2-positive early breast cancer JORGE MADRID BIG GOCCHI PROTOCOLO HERA
 Sustained benefits for women with HER2-positive early breast cancer JORGE MADRID BIG GOCCHI PROTOCOLO HERA The fascinating history of Herceptin 1981 1985 1987 1990 1992 1998 2000 2005 2006 2008 2011 Murine
Sustained benefits for women with HER2-positive early breast cancer JORGE MADRID BIG GOCCHI PROTOCOLO HERA The fascinating history of Herceptin 1981 1985 1987 1990 1992 1998 2000 2005 2006 2008 2011 Murine
Practice changing studies in lung cancer 2017
 1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
Updates in Immunotherapy for Urothelial Carcinoma
 Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Triple Negative Breast Cancer
 GASCO 2016 San Antonio Breast Cancer Symposium Review Triple Negative Breast Cancer Amelia Zelnak, MD, MSc Atlanta Cancer Care Northside Hospital Cancer Institute Disclosures: consultant for Novartis,
GASCO 2016 San Antonio Breast Cancer Symposium Review Triple Negative Breast Cancer Amelia Zelnak, MD, MSc Atlanta Cancer Care Northside Hospital Cancer Institute Disclosures: consultant for Novartis,
SYSTEMIC TREATMENT OF TRIPLE NEGATIVE BREAST CANCER
 SYSTEMIC TREATMENT OF TRIPLE NEGATIVE BREAST CANCER Sunil Shrestha 1*, Ji Yuan Yang, Li Shuang and Deepika Dhakal Clinical School of Medicine, Yangtze University, Jingzhou, Hubei Province, PR. China Department
SYSTEMIC TREATMENT OF TRIPLE NEGATIVE BREAST CANCER Sunil Shrestha 1*, Ji Yuan Yang, Li Shuang and Deepika Dhakal Clinical School of Medicine, Yangtze University, Jingzhou, Hubei Province, PR. China Department
Combination Immunotherapy Approaches Chemotherapy, Radiation Therapy, and Dual Checkpoint Therapy
 Combination Immunotherapy Approaches Chemotherapy, Radiation Therapy, and Dual Checkpoint Therapy Dr. David B. Page Providence Portland Medical Center Earle A. Chiles Research Institute Funding & Disclosures
Combination Immunotherapy Approaches Chemotherapy, Radiation Therapy, and Dual Checkpoint Therapy Dr. David B. Page Providence Portland Medical Center Earle A. Chiles Research Institute Funding & Disclosures
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA
 Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA When Are Biomarkers Ready To Use? Same Rules for Gene Expression Panels Key elements
Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA When Are Biomarkers Ready To Use? Same Rules for Gene Expression Panels Key elements
HDAC Inhibitors and PARP inhibitors. Suresh Ramalingam, MD Associate Professor Chief of Thoracic Oncology Emory University School of Medicine
 HDAC Inhibitors and PARP inhibitors Suresh Ramalingam, MD Associate Professor Chief of Thoracic Oncology Emory University School of Medicine Histone Acetylation HAT Ac Ac Ac Ac HDAC Ac Ac Ac Ac mrna DACs
HDAC Inhibitors and PARP inhibitors Suresh Ramalingam, MD Associate Professor Chief of Thoracic Oncology Emory University School of Medicine Histone Acetylation HAT Ac Ac Ac Ac HDAC Ac Ac Ac Ac mrna DACs
Triple-Negative Breast Cancer Time to Slice and Dice? Carsten Denkert, MD Charité University Hospital Berlin, Germany
 Triple-Negative Breast Cancer Time to Slice and Dice? Carsten Denkert, MD Charité University Hospital Berlin, Germany Triple-Negative Breast Cancer (TNBC) 2018 Presentation Outline The molecular heterogeneity
Triple-Negative Breast Cancer Time to Slice and Dice? Carsten Denkert, MD Charité University Hospital Berlin, Germany Triple-Negative Breast Cancer (TNBC) 2018 Presentation Outline The molecular heterogeneity
PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND!
 II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND! INGRID A. MAYER, MD, MSCI Assistant
II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND! INGRID A. MAYER, MD, MSCI Assistant
Best of San Antonio 2008
 Best of San Antonio 2008 Ellie Guardino, MD/PhD Assistant Professor Stanford University BIG 1 98: a randomized double blind phase III study evaluating letrozole and tamoxifen given in sequence as adjuvant
Best of San Antonio 2008 Ellie Guardino, MD/PhD Assistant Professor Stanford University BIG 1 98: a randomized double blind phase III study evaluating letrozole and tamoxifen given in sequence as adjuvant
Triple negative breast cancer Biology and targeted therapy
 Triple negative breast cancer Biology and targeted therapy MR SCI MED DR I BOŽOVIĆ -SPASOJEVIĆ INSTITUT ZA ONKOLOGIJU I RADIOLOGIJU SRBIJE I VA N A B O Z O V I C @ O U T L O O K. C O M Current challanges
Triple negative breast cancer Biology and targeted therapy MR SCI MED DR I BOŽOVIĆ -SPASOJEVIĆ INSTITUT ZA ONKOLOGIJU I RADIOLOGIJU SRBIJE I VA N A B O Z O V I C @ O U T L O O K. C O M Current challanges
Subtype-directed therapy of TNBC Global Breast Cancer Conference 2015 & 4th International Breast Cancer Symposium Jeju Island, Korea, April 2015
 Subtype-directed therapy of TNBC Global Breast Cancer Conference 2015 & 4th International Breast Cancer Symposium Jeju Island, Korea, April 2015 Ruth M. O Regan, MD Visiting Professor and Division Chief
Subtype-directed therapy of TNBC Global Breast Cancer Conference 2015 & 4th International Breast Cancer Symposium Jeju Island, Korea, April 2015 Ruth M. O Regan, MD Visiting Professor and Division Chief
Immunotherapy in breast cancer. Carmen Criscitiello, MD, PhD European Institute of Oncology Milan, Italy
 Immunotherapy in breast cancer Carmen Criscitiello, MD, PhD European Institute of Oncology Milan, Italy Outline Rational for immune-based therapy in breast cancer Immunogenic chemotherapy Targeting immune
Immunotherapy in breast cancer Carmen Criscitiello, MD, PhD European Institute of Oncology Milan, Italy Outline Rational for immune-based therapy in breast cancer Immunogenic chemotherapy Targeting immune
Karcinom dojke. PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski
 Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,