Management of Triple Negative Breast Cancer. Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology
|
|
|
- Elmer Newman
- 5 years ago
- Views:
Transcription
1
2 Management of Triple Negative Breast Cancer Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology
3 Outline Heterogeneity of TNBC Targeting TNBC by subtypes New antibody drug coniugates

4 Clinical Heterogeneity of TNBC Subtype Gene expression profile Clinical Basal-like 1 high Ki-67; DNA damage response BRCA-associated Basal-like 2 GF pathways Higher pcr Immunomodulatory Immune genes Mesenchymal Cell motility Lower DDFS Mesenchymal stem-like Cell motility; claudin-low Luminal androgen receptor Steroid pathways Apocrine features, higher LRF; PI3Kmut Lehman BD, et al. J Clin Invest 2011;121:
5 Metastatic triple-negative breast cancer Subtype Gene expression profile Clinical Basal-like 1 high Ki-67; DNA damage response BRCA-associated Basal-like 2 GF pathways Higher pcr Immunomodulatory Immune genes Mesenchymal Cell motility Lower DDFS Mesenchymal stem-like Cell motility; claudin-low Luminal androgen receptor Steroid pathways Apocrine features, higher LRF; PI3Kmut Lehman BD, et al. J Clin Invest 2011;121:
6 Basal like 1 TNBC Triple negative breast cancer and BRCA-mutations Clinical behavior Genomic instability Stephens et al Nature 2009 vol. 462 (7276) pp 1005
7 Basal like 1 TNBC HER2- MBC + gbrcamt chemo for MBC (prior A and T. No plat resistance) 2:1 N~300 ~ 150 TNBC Olaparib 300 mg tablets bid 2:1 randomization Chemo TPC Capecitabine Eribulin Vinorelbine Treat until progression Primary endpoint PFS 70% prior chemotherapy for MBC (30% prior platinum) 57% BRCA1 50% TNBC Robson M et al, NEJM 2017
8 Olaparib in basal like 1 Non-response Response Stable disease Partial response Complete response Olaparib 300 mg bd (n=167) Chemotherapy TPC (n=66) Median response onset Olaparib: 47 days Patients, % Chemotherapy TPC: 45 days Among patients with metastatic HER2-negative BC and a germline BRCA1/2 mutation in the OlympiAD study, the objective response rate with olaparib tablet monotherapy was double that seen with standard chemotherapy TPC Stable disease was for 5 weeks, recorded 6 weeks after randomization. Chemotherapy TPC, treatment of physician s choice (including capecitabine, eribulin or vinorelbine) Robson M et al, NEJM 2017

9 Olaparib in basal like 1 QoL olaparib > chemotherapy Response rate % to % Robson M et al, NEJM 2017

10 Olaparib in basal like 1 Robson M et al, NEJM 2017
11 Olaparib in basal like 1 Tumour burden Olaparib 300 mg bid Chemotherapy TPC 1 metastatic site, n Median PFS, months HR (95% CI) 0.62 (0.35, 1.13) etastati sites, Median PFS, months HR (95% CI) 0.59 (0.43, 0.82) Tumour location Olaparib 300 mg bid Chemotherapy TPC Visceral, n Median PFS, months HR (95% CI) 0.64 (0.47,0.86) Non-visceral, n Median PFS, months HR (95% CI) 0.65 (0.30,1.65) Although the study was not powered to detect differences in treatment effect between subgroups, the PFS benefit for olaparib over chemotherapy TPC across tumour burden and location subgroups was consistent with that seen in the overall population 1 HR, hazard ratio. Non-visceral disease includes lymph nodes, soft tissue, cutaneous and bone only. 1. Robson M et al. N Engl J Med 2017;377: Robson M et al, NEJM 2017

12 Veliparib in basal like 1
13 Veliparib in basal like Median PFS, months (95% CI) Placebo + C/P N = ( ) Veliparib + C/P N = 95 HR P value * 14.1 ( ) ( ) Probability of Progression-Free Survival RR % to % However no pcr with veliparib in neoadjuvant setting 0.0 Placebo + C/P Veliparib + C/P Months Since Randomization Phase III BROCADE 3 pending Han et al, Annals of Oncol 2018; Geyer et al, ASCO 2017
14 Cisplatin in basal like 1 ER-, PgR-/unknown & HER2- or known BRCA1/2 Metastatic or recurrent locally advanced Exclusions include: Adju a t ta a e i o ths Previous platinum treatment Non-anthracyclines for MBC A Priori subgroup analyses: BRCA1/2 mutation RANDOMISE Basal-like subgroups (PAM50 (1:1) and IHC) Biomarkers of HRD Tutt A et al, 2104 Carboplatin (C) AUC 6 q3w, 6 cycles On progression, crossover if appropriate n-376 BRCA1/2 = 9%/12% Docetaxel (D) 100mg/m 2 q3w, 6 cycles On progression, crossover if appropriate Docetaxel (D) 100mg/m 2 q3w, 6 cycles Carboplatin (C) AUC 6 q3w, 6 cycles 13
15 Cisplatin in basal like 1 Randomised treatment - all patients (N=376) % with OR at cycle 3 or 6 (95% CI) Carboplatin Docetaxel 59/188 (31.4%) 67/188 (35.6%) Absolute difference (C-D) -4.2% (95% CI to 5.3) Exact p = 0.44 Crossover treatment - all patients (N=182) % with OR at cycle 3 or 6 (95% CI) Carboplatin (Crossover=Docetaxel) Docetaxel (Crossover=Carboplatin) 21/92* (22.8%) 23/90* (25.6%) Absolute difference (D-C) -2.8% (95% CI to 9.6) Exact p = 0.73 *Denominator excludes those with no first progression and those not starting crossover treatment 14 Tutt, SABCS 2014
16 Cisplatin in basal like 1 % patients progression free Median PFS: Carboplatin: 3.1 mths (95% CI = 2.5 to 4.2) Docetaxel: 4.5 mths (95% CI = 4.1 to 5.2) Restricted mean survival to 15 mths: Carboplatin: 4.8 mths Docetaxel: 5.2 mths Absolute difference: -0.4 (95% CI -1.1 to 0.3) p = 0.29 Carboplatin = 181 /188 0 Docetaxel = / Months from randomisation Number of events/at risk C: 0/188 90/98 40/56 32/22 9/13 5/8 0/7 D: 0/188 57/130 60/69 48/20 7/13 6/5 152/3
17 Cisplatin in basal like 1 % patients alive Median OS: Carboplatin: 12.4 mths (95% CI = 10.4 to 15.3) Docetaxel: 12.3 mths (95% CI = 10.5 to 13.6) 40 Restricted mean survival to 15 mths: 30 Carboplatin: 10.7 mths Docetaxel: 10.8 mths 20 Absolute difference: (95% CI -1.1 to 0.8) p = Months from randomisation Number of events/at risk C: 0/188 23/165 18/141 24/114 22/89 14/71 22/44 D: 0/188 11/176 20/151 35/110 19/85 23/58 16/39
18 Cisplatin in basal like 1 Germline BRCA 1/2 Mutation (n=43) Carboplatin Docetaxel No Germline BRCA 1/2 Mutation (n=273) Percentage with OR at cycle 3 or 6 (95% CI) /25 (68.0%) 6/18 (33.3%) Absolute difference (C-D) 34.7% (95% CI 6.3 to 63.1) Exact p = 0.03 Percentage with OR at cycle 3 or 6 (95% CI) Carboplatin Docetaxel 36/128 (28.1%) 53/145 (36.6%) Absolute difference (C-D) -8.5% (95% CI to 2.6) Exact p = 0.16 Interaction: randomised treatment & BRCA 1/2 status: p =
19 Cisplatin in basal like 1 % patients progression free Median PFS: C + BRCA 1/2 mutated 6.8mnths (95% CI = 4.4 to 8.1) C + BRCA1/2 not mutated 3.1mnths (95% CI = 2.4 to 4.2) Carboplatin + BRCA1/2 mutated Carboplatin + BRCA1/2 not mutated Months from randomisation Tutt, SABCS 2014
20 PARP inhibitors in metastatic TNBC HER2- MBC + gbrcamt Prior chemo 2:1 Talazoparib (BMN 673) 1 mg po qd 2:1 randomization Chemo TPC Capecitabine Eribulin Gemcitabine Vinorelbine Treat until progression Primary endpoint PFS HER2- MBC + gbrcamt No platinum-r 2:1 Niraparib 100 mg po qd 2:1 randomization Primary endpoint PFS Chemo TPC Menu of 4 drugs
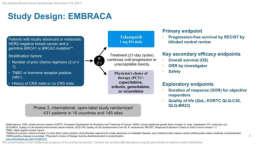
21 Talazoparib
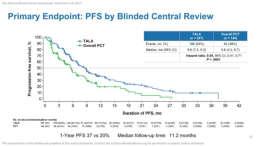
22 Talazoparib

23 Basal like 2:Growth factor signalling Lisa A. Carey et al. JCO 2012;30:
24 Basal like 2:Growth factor signalling Lisa A. Carey et al. JCO 2012;30:

25 Basal like 2:Growth factor signalling The combination of cetuximab plus Carboplatin in metastatic TNBC produced responses in fewer than 20% of patients. EGFR pathway analysis showed that most TNBCs involved activation. Lisa A. Carey et al. JCO 2012;30:
26 Subsets of triple-negative breast cancer Subtype Gene expression profile Clinical Basal-like 1 high Ki-67; DNA damage response BRCA-associated Basal-like 2 GF pathways Higher pcr Immunomodulatory Immune genes Mesenchymal Cell motility Lower DDFS Mesenchymal stem-like Cell motility; claudin-low Luminal androgen receptor Steroid pathways Apocrine features, higher LRF; PI3Kmut Lehman BD, et al. J Clin Invest 2011;121:
27 Evidence from clinical trials Pembrolizumab (Merck) Humanized IgG4 anti- PD-1 antibody MPDL3280 (Genentech) engineered human IgG1 anti-pd-l1 antibody
28 Pembrolizumab in TNBC Recurrent or metastatic ER-/PR-/HER2- breast cancer ECOG PS 0-1 PD-L1+ tumour No systemic steroid therapy Pembro 10 mg/kg Q2W CR PR/SD Discontinuation permitted Treat for 24 mo or until PD or toxicity No autoimmune disease (active or history of) No active brain metastases Confirmed PD Discontinue PD-L1 positivity: 58% of all patients screened had PD-L1-positive tumors Treatment: 10 mg/kg IV Q2W Response assessment: Performed every 8 weeks per RECIST v1.1 a PD-L1 expression was assessed in archival tumor samples using a prototype IHC assay and the 22C3 antibody. Only patients with PD-L1 staining in the stroma or i % of tu or ells ere eligi le for e roll e t. b If clinically stable, patients are permitted to remain on pembrolizumab until progressive disease is confirmed on a second scan perfor ed eeks later. If progressi e disease is confirmed, pembrolizumab is discontinued. An exception may be granted for patients with clinical stability or improvement after consultation with the sponsor.

29 Pembrolizumab in TNBC n =32 Confirmed complete response (nodal disease) Confirmed partial response Stable disease Progressive disease Objective response rate: 18.5% Stable disease: 25.9% Nanda, SABCS 2015
30 Pembrolizumab in TNBC Cohort A (N = 170): Previously Treated, Regardless of PD-L1 Expression Cohort B (N = 52): Previously Untreated, PD-L1 Positive Complete response ORR, % Partial response ORR, % % % 4.8% 4.7% Total PD-L1 Positive PD-L1 Negative 0 Total (All PD-L1 Positive) Adams S et al. ASCO 2017
31 Anti PD1 and anti PDL1 in TNBC Anti-PD-L1/PD-1 single agent in mtnbc 1L, PDL1+/- Objective Response Rate (%) 30% 20% 10% 0% 26% 1L Atezolizumab (n=115) 11% 2L+ No clear relationship with PD-L1 positivity 23% 1L Keynote-086, Cohort B Pembrolizumab (n=222) 4.7% 2L+ Keynote-086, Cohort A CR PR CR PR Schmid P, et al. AACR 2017; Adams S, et al ASCO 2017
32 Role of TILs in TNBC 4% Atezolizumab Pembrolizumab (Cohort A: >2nd line) Pembrolizumab (Cohort B: 1st line) 39.1% Objective Response Rate (%) 30% 20% 10% 0% 19% TIL high 2 9% TIL low Different levels by source of sample (archival vs new) and organ site sampled: LN>lung>liver Metastatic breast cancer is a low TIL disease 6.4% TIL high 2 1.9% TIL low TIL high 8.7% TIL low Schmid P, et al. AACR 2017; Adams S, et al ASCO 2017, Loi, ESMO 2017
33 Phase Ib Study of Atezolizumab and Nab- Paclitaxel in mtnbc Best Overall Response 1L (n = 9) Confirmed ORR (95% CI) a 66.7% (29.9, 92.5) ORR (95% CI) b 88.9% (51.7, 99.7) 2L (n = 8) 25% (3.2, 65.1) 75.0% (34.9, 96.8) 3L+ (n = 7) 28.6% (3.7, 71.0) 42.9% (9.9, 81.6) All Patients N = % (22.1, 63.4) 70.8% (48.9, 87.4) CR 11.1% % PR 77.8% 75.0% 42.9% 66.7% Response rates were higher for patients who received atezolizumab/nabpaclitaxel treatment as 1L therapy compared to 2L+ SD 11.1% 25.0% 28.6% 20.8% PD % 8.3% a Confirmed ORR defined as at least 2 consecutive assessments of complete or partial response. b Including investigator-assessed unconfirmed responses. Efficacy-evaluable patients were dosed by June 1, 2015, and were evaluable for response by RECIST v1.1. Mi i u effi a follo up as o ths. Adams S, et al. SABCS [abstract ].
 continued on treatment at time of data cut off Adams S, et al. SABCS.")
34 Phase Ib Study of Atezolizumab and Nab- Paclitaxel in mtnbc Including investigator-assessed unconfirmed responses. 11 of 17 responses (65%) continued on treatment at time of data cut off Adams S, et al. SABCS [abstract ].
35 Phase III Study of Atezolizumab and Nab- Paclitaxel in mtnbc Randomized, double-blind, placebo-controlled Phase 3 trial of nab-paclitaxel ± atezolizumab as 1 st line therapy in mtnbc (NCT ) Study design Histologically documented locally advanced or metastatic TNBC No prior therapy for advanced disease ECOG PS 0-1 Measurable disease per RECIST v1.1 Patients with significant CV or CNS disease (except asymptomatic brain metastases), autoimmune disease or prior checkpoint inhibitor therapy are excluded Target accrual: ~350 pts Stratification factors: Presence of liver metastases Prior taxane therapy Nab-paclitaxel 100 mg/m 2 QW 3/4 + Atezolizumab 840 mg Q2W PD-L1 expression status (centrally evaluated by IHC using the SP142 assay) R 1:1 Nab-paclitaxel 100 mg/m 2 QW 3/4 + Placebo Q2W Co-primary endpoints: PFS in all patients PFS according to PD-L1 expression Secondary endpoints: OS ORR Response duration Safety/tolerability PK HR QoL Emens et al. SABCS 2015 (abstract OT )
36 Neoadjuvant Neoadjuvant paclitaxel x 12 +/- pembrolizumab followed by AC x 4 Adaptive randomization on I-SPY 2 Signature All HER2- TNBC HR+/HER2- Estimated pcr rate (95% probabilty interval) Pembro 0.46 ( ) 0.60 ( ) 0.34 ( ) Control 0.16 ( ) 0.20 ( ) 0.13 ( ) Probability pembro is superior to control Predictive probability of success in phase 3 > 99% 99% >99% >99% >99% 88% Nanda et al, ASCO 2017, Abstract 506 The Bayesian model estimated pcr rates adjust to characteristics of the I-SPY 2 population. The raw pcr rates are higher than the 35 model estimate of in TNBC.
 engineered human IgG1 anti-pd-l1 antibody MEDI4736 (AZ) Human IgG1 anti-pd-l1 antibody Tremelimumab (AZ) Human IgG2 Anti-CTLA-4")
37 Immunotherapy in TNBC Nivolumab (BMS) Human IgG4 anti-pd-1 antibody Pembrolizumab (Merck) Humanized IgG4 anti- PD-1 antibody MPDL3280 (Genentech) engineered human IgG1 anti-pd-l1 antibody MEDI4736 (AZ) Human IgG1 anti-pd-l1 antibody Tremelimumab (AZ) Human IgG2 Anti-CTLA-4 antibody
38 Adaptive Phase II Randomized Non-comparative Trial of Nivolumab After Induction Treatment in Triple-negative Breast Cancer (TNBC) Patients: TONIC-trial (The Netherlands Cancer Institute) Radiation 3 x 8 Gy Biopsy Doxorubicin 15 mg x2 Biopsy Biopsy R Cyclophosphamide 50 mg daily Biopsy Nivolumab Cisplatin 40 mg/m 2 x2 Biopsy Kok M, et al. Ann Oncol. 2017;35(suppl): Abstract LBA14. No treatment 2 weeks Biopsy
39 Adaptive Phase II Randomized Non-comparative Trial of Nivolumab After Induction Treatment in Triple-negative Breast Cancer (TNBC) Patients: TONIC-trial (The Netherlands Cancer Institute) Total (n = 50) Best ORR (CR + PR) irecist 24% CBR (CR + PR + SD) 26% CR 1 (2%) PR 11 (22%) SD weeks 1 (2%) ORR RECIST % Median PFS [95% CI] 3.4 months [ ] Median time to response [range] 2.1 months [ ] Median duration of response [95% CI] 9.0 months [5.5-NA] Kok M, et al. Ann Oncol. 2017;35(suppl): Abstract LBA14.
40 Challenges High risk breast cancer High TILs/immune activation signature/ PDL1+/ High TMB Good microbioma Low/Intermediate TILs/immune activation signature-/pdl1-/ Bad microbioma I-O as monotherapy or combination of I-O High TMB Low TMB Add CT to enhance immunogenicity or STING, TIGIT, RT No I-O
41 PARP inhibitors and IO Phase I Patients with OC or TNBC Dose level 1 Niraparib 200 mg + pembrolizumab 200 mg Phase II Patients with OC (target n = 48) or TNBC (target n = 48) RP2D Endpoint assessment Dose level 2 Niraparib 300 mg + pembrolizumab 200 mg Endpoint assessment Konstantinopoulos PA, et al. Ann Oncol. 2017;28(Suppl 5): Abstract 1143PD.
: Abstract 1143PD.")
42 PARP inhibitors and IO Konstantinopoulos PA, et al. Ann Oncol. 2017;28(Suppl 5): Abstract 1143PD.
43 Clinical Heterogeneity of TNBC Subtype Gene expression profile Clinical Basal-like 1 high Ki-67; DNA damage response BRCA-associated Basal-like 2 GF pathways Higher pcr Immunomodulatory Immune genes Mesenchymal Cell motility Lower DDFS Mesenchymal stem-like Cell motility; claudin-low Luminal androgen receptor Steroid pathways Apocrine features, higher LRF; PI3Kmut Lehman BD, et al. J Clin Invest 2011;121:

44 Notch pathway Phase 1b Study of docetaxel + PF in Triplenegative Breast Cancer PF
45 Notch pathway Characteristic Mean (range) age, years PF 100 mg BID/ PF 100 mg BID/ PF 150 mg BID/ All Dose D 75 mg/m 2 (N = 8) D 100 mg/m 2 (N = 3) D 75 mg/m 2 (N = 11) Levels (N = 22) 57 (43-76) 43 (32-64) 46 (27-69) 50 (27-76) ECOG PS, n (%) 0/1 4/4 (50/50) 1/2 (33/67) 8/3 (73/27) 13/9 (59/41) Primary Diagnosis, n 1/7 (13/87) 0/3 (0/100) 3/8 (27/73) 4/18 (18/82) (%) locally recurrent/metastatic Prior Systemic Therapies, n (%) 1st line/ 2 nd line 4/4 (50/50) 3/0 (100/0) 7/4 (64/36) 14/8 (64/36) M Locatelli et al, Oncotarget 2016
46 Clinical Heterogeneity of TNBC Subtype Gene expression profile Clinical Basal-like 1 high Ki-67; DNA damage response BRCA-associated Basal-like 2 GF pathways Higher pcr Immunomodulatory Immune genes Mesenchymal Cell motility Lower DDFS Mesenchymal stem-like Cell motility; claudin-low Luminal androgen receptor Steroid pathways Apocrine features, higher LRF; PI3Kmut Lehman BD, et al. J Clin Invest 2011;121:
47 Luminal Androgen Receptor: Bicalutamide ER/PR(-) IHC % LABC/MBC AR+ DAKO Ab > 10% Bicalutamide 150mg daily Primary endpoint = CBR24 (CR + PR + SD > 24 weeks) Screened patients 12% AR+ (mostly TNBC) Clinical Benefit Rate = 19% (95% CI 7-39%) All SD Gucalp et al CCR 2013
48 Luminal Androgen Receptor: Abiraterone MBC ER/PR % 138 screened 38% AR+ % Primary Endpoint = CBR24 Median PFS 2.8m N = 30 evaluable patients ~ 2.5 prior lines Rx ~ 50% visceral mets Most common, related AEs: fatigue (18%) HTN (12%) hypokalemia (9%) nausea (6%) CBR24 = 20% (95%CI: 8-39%) 1 confirmed CR Bonnefoi et al, Ann Onc 2016
49 Luminal Androgen Receptor: Enzalutamide ER/PR/HER2 (-) LABC/MBC AR+ Ventana > 0% Enzalutamide 160 mg daily Primary endpoint = CBR16 (CR + PR + SD > 16) Screened weeks) patients 79% AR+ (55% by 10% cutoff) Median 1 prior Rx Evaluable (n=75 AR > 10%) CBR16 35% (24-46%) CBR24 29% (20-41%) RR 8% SAE 29% PFS (%) PFS 14.7 weeks 95% CI: 8.1,
50 Luminal Androgen Receptor Gene expression classifier created = PredictAR (Basal-, apocrine+, etc to identify LAR) PREDICT AR PREDICT AR+ PREDICT AR PREDICT AR+ Total, n (%) 62 (53%) 56 (47%) CBR16, % (95% CI) n 11% (5, 21) n = 7 39% (27, 53) n = 22 CBR24, % (95% CI) n CR or PR, % n 6% (2, 16) n = 4 3% n = 2 36% (24, 49) n = 20 9% n = Prior Lines 2+ Prior Lines Active Confirmed CR or PR Time (weeks) Time (weeks) Traina et al, ASCO 2015
51 Luminal Androgen Receptor ITT Population 100 n = 118 Overall Survival (%) PREDICT AR mos 32.3 weeks (95% CI: 20.7, 48.3) PREDICT AR+ mos 75.6 weeks (95% CI: 51.6, 91.4) 0 Patients at risk PREDICT AR+ PREDICT AR Data cutoff 1Jul2015 ITT = intent to treat; mos = median survival; CI = confidence interval; Weeks PREDICT AR+ mos 18.0 months PREDICT AR mos 7.5 months NCT Courtesy of J. Cortes, ECCO 2015
52 Metastatic triple negative BC Glembatumumab Vedotin in GPNMB+ TNBC GPNMB, glycoprotein NMB Yardley DA, et al. J Clin Oncol. 2015;33(14):

53 Metastatic triple negative BC Phase II Trial Sacituzumab Govitecan Met TNBC 3/4/5 th -Line Phase II Median DoR 7.6 months Med PFS 5.5 months >90% TNBCs express Trop-2 CT, computed tomography; MRI, magnetic resonance imaging Bardia A, et al. Presented at: San Antonio Breast Cancer Symposium; December 5-9, 2017: San Antonio, Texas.
54 Challenges AR-targeting maybe PARPi Yes! My bet will work in somatically inactivated? I-O?
55 Conclusions Select the right partner and validate studies with the same backbone Demonstrate bioactivity and not MTD Metastatic breast cancer is not always the right setting Neoadjuvant Post-neoadjuvant can be more informative
Treatment of Triple Negative Breast Cancer. Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology
 Treatment of Triple Negative Breast Cancer Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology Outline Neoadjuvant treatment in triple negative EBC Picking optimal adjuvant
Treatment of Triple Negative Breast Cancer Giuseppe Curigliano MD, PhD University of Milano and European Institute of Oncology Outline Neoadjuvant treatment in triple negative EBC Picking optimal adjuvant
Systemic therapy of triple negative advanced breast cancer. Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development
 Systemic therapy of triple negative advanced breast cancer Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development Outline State of the Art in the management of TN advanced
Systemic therapy of triple negative advanced breast cancer Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development Outline State of the Art in the management of TN advanced
La malattia triplo negativa metastatica: quali trattamenti nella pratica clinica?
 2018 CARCINOMA MAMMARIO: I TRAGUARDI RAGGIUNTI E LE NUOVE SFIDE La malattia triplo negativa metastatica: quali trattamenti nella pratica clinica? Roma, 27 Ottobre 2018 Relatore: Francesca Poggio Disclosure
2018 CARCINOMA MAMMARIO: I TRAGUARDI RAGGIUNTI E LE NUOVE SFIDE La malattia triplo negativa metastatica: quali trattamenti nella pratica clinica? Roma, 27 Ottobre 2018 Relatore: Francesca Poggio Disclosure
ESMO Preceptorship Breast Cancer. Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development Istituto Europeo di Oncologia
 ESMO Preceptorship Breast Cancer Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development Istituto Europeo di Oncologia Outline Rational for immune-based therapy in BC How to
ESMO Preceptorship Breast Cancer Giuseppe Curigliano MD, PhD Breast Cancer Program Division of Early Drug Development Istituto Europeo di Oncologia Outline Rational for immune-based therapy in BC How to
ENFERMEDAD AVANZADA Qué hacemos con el triple negativo? Nuevas aproximaciones
 ENFERMEDAD AVANZADA Qué hacemos con el triple negativo? Nuevas aproximaciones Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative
ENFERMEDAD AVANZADA Qué hacemos con el triple negativo? Nuevas aproximaciones Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Alternativas terapéuticas en fenotipo triple negativo Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid
 Alternativas terapéuticas en fenotipo triple negativo Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative Breast Cancer Immunohistochemistry
Alternativas terapéuticas en fenotipo triple negativo Javier Cortes, Hospital Universitario Ramon y Cajal, Madrid Vall d Hebron Institute of Oncology (VHIO), Barcelona Triple Negative Breast Cancer Immunohistochemistry
Triple Negative Breast cancer New treatment options arenowhere?
 Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
Triple Negative Breast cancer New treatment options arenowhere? Ofer Rotem, M.D., B.Sc. Breast Unit, Davidoff center Rabin Medical center October 2017 Case 6/2013 - M.D., 38 years old woman, healthy, no
Expert Review: The Role of PARP Inhibition in the Treatment of Breast Cancer. Reference Slides
 Expert Review: The Role of PARP Inhibition in the Treatment of Breast Cancer Reference Slides Overview BRCA Mutations and Breast Cancer Patients with BRCA mutations have an estimated 55% to 65% cumulative
Expert Review: The Role of PARP Inhibition in the Treatment of Breast Cancer Reference Slides Overview BRCA Mutations and Breast Cancer Patients with BRCA mutations have an estimated 55% to 65% cumulative
ESMO Preceptoship in Immuno-Oncology. Clinical Development: Breast Cancer
 ESMO Preceptoship in Immuno-Oncology Clinical Development: Breast Cancer Prof Giuseppe Curigliano, MD PhD University of Milano and Istituto Europeo di Oncologia Milano, Lombardia, Italy Outline Rational
ESMO Preceptoship in Immuno-Oncology Clinical Development: Breast Cancer Prof Giuseppe Curigliano, MD PhD University of Milano and Istituto Europeo di Oncologia Milano, Lombardia, Italy Outline Rational
Triple Negative Breast Cancer: Part 2 A Medical Update
 Triple Negative Breast Cancer: Part 2 A Medical Update April 29, 2015 Tiffany A. Traina, MD Breast Medicine Service Memorial Sloan Kettering Cancer Center Weill Cornell Medical College Overview What is
Triple Negative Breast Cancer: Part 2 A Medical Update April 29, 2015 Tiffany A. Traina, MD Breast Medicine Service Memorial Sloan Kettering Cancer Center Weill Cornell Medical College Overview What is
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Immunotherapy for Breast Cancer Clinical Development
 Immunotherapy for Breast Cancer Clinical Development Laurence Buisseret, MD, PhD Breast Cancer Translational Research Laboratory Institut Jules Bordet Université Libre de Bruxelles (ULB) ESMO preceptorship
Immunotherapy for Breast Cancer Clinical Development Laurence Buisseret, MD, PhD Breast Cancer Translational Research Laboratory Institut Jules Bordet Université Libre de Bruxelles (ULB) ESMO preceptorship
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC)
") Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
Post-ASCO 2017 Cancer du sein Triple Négatif
 Post-ASCO 217 Cancer du sein Triple Négatif A.Ladjeroud, K.Bouzid Centre Pierre et Marie Curie- Alger Oran, 3 Septembre 217 Phase III Investigation of Neoadjuvant Carboplatin ± Veliparib in Combination
Post-ASCO 217 Cancer du sein Triple Négatif A.Ladjeroud, K.Bouzid Centre Pierre et Marie Curie- Alger Oran, 3 Septembre 217 Phase III Investigation of Neoadjuvant Carboplatin ± Veliparib in Combination
Systemic therapy for TN advanced breast cancer
 Systemic therapy for TN advanced breast cancer Javier Cortes, Ramon y Cajal University Hospital, Madrid Vall d Hebron Institute of Oncology (VHIO) & Medica Scientia Innovation Research (MedSIR), Barcelona,
Systemic therapy for TN advanced breast cancer Javier Cortes, Ramon y Cajal University Hospital, Madrid Vall d Hebron Institute of Oncology (VHIO) & Medica Scientia Innovation Research (MedSIR), Barcelona,
Overview and future horizons of PARP inhibitors in BRCAassociated. Judith Balmaña
 Overview and future horizons of PARP inhibitors in BRCAassociated breast cancer Judith Balmaña PARP inhibitors: Mechanism of action Clinical development: Monotherapy In combination with chemotherapy Ongoing
Overview and future horizons of PARP inhibitors in BRCAassociated breast cancer Judith Balmaña PARP inhibitors: Mechanism of action Clinical development: Monotherapy In combination with chemotherapy Ongoing
PARP inhibitors for breast cancer
 PARP inhibitors for breast cancer Mark Robson, MD Memorial Sloan Kettering Cancer Center Agenda Mechanism of action Clinical studies Resistance mechanisms Future directions Poly (ADP-ribose) Polymerases
PARP inhibitors for breast cancer Mark Robson, MD Memorial Sloan Kettering Cancer Center Agenda Mechanism of action Clinical studies Resistance mechanisms Future directions Poly (ADP-ribose) Polymerases
Emerging Strategies in Triple-Negative Breast Cancer
 Expert Review in Immunotherapy in Breast Cancer Emerging Strategies in Triple-Negative Breast Cancer Reference Slide Deck Is Breast Cancer Immunogenic? Recent proof that breast cancer may elicit an immune
Expert Review in Immunotherapy in Breast Cancer Emerging Strategies in Triple-Negative Breast Cancer Reference Slide Deck Is Breast Cancer Immunogenic? Recent proof that breast cancer may elicit an immune
Triple Negative Breast Cancer. Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008
 Triple Negative Breast Cancer Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008 Triple Negative Breast Cancer 15% 25% Triple Negative 20% HER2+ ER+ Low Grade
Triple Negative Breast Cancer Eric P. Winer, MD Dana-Farber Cancer Institute Harvard Medical School Boston, MA October, 2008 Triple Negative Breast Cancer 15% 25% Triple Negative 20% HER2+ ER+ Low Grade
Breast Cancer Immunotherapy. Leisha A. Emens, MD PhD Johns Hopkins University Bloomberg Kimmel Institute for Cancer Immunotherapy
 Breast Cancer Immunotherapy Leisha A. Emens, MD PhD Johns Hopkins University Bloomberg Kimmel Institute for Cancer Immunotherapy Conflict of Interest I have the following financial relationships to disclose:
Breast Cancer Immunotherapy Leisha A. Emens, MD PhD Johns Hopkins University Bloomberg Kimmel Institute for Cancer Immunotherapy Conflict of Interest I have the following financial relationships to disclose:
Triple-Negative Breast Cancer
 June 2017 Triple-Negative Breast Cancer Amir Sonnenblick, MD, PhD Sharett institute of oncology Hadassah-Hebrew university medical center, Jerusalem, Israel This presentation is the intellectual property
June 2017 Triple-Negative Breast Cancer Amir Sonnenblick, MD, PhD Sharett institute of oncology Hadassah-Hebrew university medical center, Jerusalem, Israel This presentation is the intellectual property
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings. Eve Rodler, MD University of California at Davis October 2016
 Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
Advances in Breast Cancer Therapeutics in the Adjuvant and Metastatic Settings Eve Rodler, MD University of California at Davis October 2016 17th Annual Advances in Oncology September 30-October 1, 2016
6/13/17. Disclosures. Treating Breast Cancer in People with Mutations. Off Label Use. I will be discussing off label use of medications today.
 Treating Breast Cancer in People with Mutations Steven J. Isakoff, MD, PhD Massachusetts General Hospital Cancer Center June 9, 2017 sisakoff@partners.org Disclosures Company ² Myriad Genetics ² AbbVie
Treating Breast Cancer in People with Mutations Steven J. Isakoff, MD, PhD Massachusetts General Hospital Cancer Center June 9, 2017 sisakoff@partners.org Disclosures Company ² Myriad Genetics ² AbbVie
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
TNBC: What s new Déjà vu All Over Again? Lucy R. Langer, MD MSHS Compass Oncology - SABCS 2016 Review February 21, 2017
 TNBC: What s new Déjà vu All Over Again? Lucy R. Langer, MD MSHS Compass Oncology - SABCS 2016 Review February 21, 2017 The problem with TNBC 1. Generally more aggressive 2. ONLY chemotherapy 3. No other
TNBC: What s new Déjà vu All Over Again? Lucy R. Langer, MD MSHS Compass Oncology - SABCS 2016 Review February 21, 2017 The problem with TNBC 1. Generally more aggressive 2. ONLY chemotherapy 3. No other
Immunotherapy for the Treatment of Head and Neck Cancers. Barbara Burtness, MD Yale University
 Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute
 Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Maintenance therapy in advanced non-small cell lung cancer. Egbert F. Smit MD PhD Dept Thoracic Oncology Netherlands Cancer Institute e.smit@nki.nl Evolution of front line therapy in NSCLC unselected pts
Treatment of Metastatic TRIPLE NEGATIVE BREAST CANCERS. Rebecca Dent, MD FRCP (Canada) Senior Consultant, Medical Oncology
 Senior Consultant, Medical Oncology") Treatment of Metastatic TRIPLE NEGATIVE BREAST CANCERS Rebecca Dent, MD FRCP (Canada) Senior Consultant, Medical Oncology Overview of TNBC Still best way to define in clinical practice!? Survival (%) Treatment
Treatment of Metastatic TRIPLE NEGATIVE BREAST CANCERS Rebecca Dent, MD FRCP (Canada) Senior Consultant, Medical Oncology Overview of TNBC Still best way to define in clinical practice!? Survival (%) Treatment
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Carrier Frequency. Breast Cancer and Treatment Options in Patients with BRCA1/2 mutations. Olivia Pagani On behalf of Bella Kaufman
 Breast Cancer and Treatment Options in Patients with BRCA1/2 mutations Olivia Pagani On behalf of Bella Kaufman Carrier Frequency Prevalence of an altered disease gene in a given population 1 Background
Breast Cancer and Treatment Options in Patients with BRCA1/2 mutations Olivia Pagani On behalf of Bella Kaufman Carrier Frequency Prevalence of an altered disease gene in a given population 1 Background
Triple negative breast cancer -neoadjuvant and adjuvant systemic therapy
 Triple negative breast cancer -neoadjuvant and adjuvant systemic therapy Sung-Bae Kim, MD, PhD Department of Oncology Asan Medical Center University of Ulsan College of Medicine Seoul, Korea DISCLOSURE
Triple negative breast cancer -neoadjuvant and adjuvant systemic therapy Sung-Bae Kim, MD, PhD Department of Oncology Asan Medical Center University of Ulsan College of Medicine Seoul, Korea DISCLOSURE
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer
 Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Contemporary Chemotherapy-Based Strategies for First-Line Metastatic Breast Cancer Hope S. Rugo, MD Professor of Medicine Director, Breast Oncology and Clinical Trials Education University of California
Breast Cancer and Treatment Options in Patients with BRCA1/2 mutations. Olivia Pagani On behalf of Bella Kaufman
 Breast Cancer and Treatment Options in Patients with BRCA1/2 mutations Olivia Pagani On behalf of Bella Kaufman Carrier Frequency Prevalence of an altered disease gene in a given population Background
Breast Cancer and Treatment Options in Patients with BRCA1/2 mutations Olivia Pagani On behalf of Bella Kaufman Carrier Frequency Prevalence of an altered disease gene in a given population Background
Dieta Brandsma, Department of Neuro-oncology, Netherlands Cancer Institute, Amsterdam, The Netherlands
 What is hot in breast cancer brain metastases? Dieta Brandsma, Department of Neuro-oncology, Netherlands Cancer Institute, Amsterdam, The Netherlands 8th Annual Brain Metastases Research and Emerging Therapy
What is hot in breast cancer brain metastases? Dieta Brandsma, Department of Neuro-oncology, Netherlands Cancer Institute, Amsterdam, The Netherlands 8th Annual Brain Metastases Research and Emerging Therapy
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents
 Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和
 資料 2 2 非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和 1 Preclinical studies Therapeutic Window: Efficacy/Toxicity Disease Specificity Subtype Specificity Combination: Concurrent/Sequential Therapeutic situation: Response/
資料 2 2 非臨床試験 臨床の立場から 京都大学医学部附属病院戸井雅和 1 Preclinical studies Therapeutic Window: Efficacy/Toxicity Disease Specificity Subtype Specificity Combination: Concurrent/Sequential Therapeutic situation: Response/
Squamous Cell Carcinoma Standard and Novel Targets.
 Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
The next wave of successful drug therapy strategies in HER2-positive breast cancer. Hans Wildiers University Hospitals Leuven Belgium
 The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Conversations in Oncology. November Kerry Hotel Pudong, Shanghai China
 Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Conversations in Oncology November 12-13 Kerry Hotel Pudong, Shanghai China Immunotherapy of Lung Cancer Professor Caicun Zhou All materials are for scientific exchanges. Afatinib and nintedanib are not
Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy. Raanan Berger MD PhD Sheba Medical Center, Israel
 Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy Raanan Berger MD PhD Sheba Medical Center, Israel Disclosures Honoraria, Ad board BMS, MSD, Pfizer, Astra Zeneca, Bayer,
Genomics and Genetics in BC: Precise selection for chemotherapy and Immunotherapy Raanan Berger MD PhD Sheba Medical Center, Israel Disclosures Honoraria, Ad board BMS, MSD, Pfizer, Astra Zeneca, Bayer,
METRIC Study Key Eligibility Criteria
 The METRIC Study METRIC Study Key Eligibility Criteria The pivotal METRIC Study is evaluating glembatumumab vedotin in patients with gpnmb overexpressing metastatic triple-negative breast cancer (TNBC).
The METRIC Study METRIC Study Key Eligibility Criteria The pivotal METRIC Study is evaluating glembatumumab vedotin in patients with gpnmb overexpressing metastatic triple-negative breast cancer (TNBC).
Immunotherapy in the clinic. Lung Cancer. Marga Majem 20 octubre 2017
 Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Immunotherapy in the clinic. Lung Cancer Marga Majem 20 octubre 2017 mmajem@santpau.cat Immunotherapy in the clinic. Lung Cancer Agenda Where we come from? Immunotherapy in Second line Immunotherapy in
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy
 Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
Indication for- and timing of cytoreductive nephrectomy Kidney- and bladder cancer: Immunotherapy Axel Bex, MD, PhD The Netherlands Cancer Institute Oslo, September 4, 2018 Financial and Other Disclosures
San Antonio Breast Cancer Symposium December 5-9, 2017
 Sacituzumab Govitecan (IMMU-132), an Anti-Trop-2-SN-38 Antibody-Drug Conjugate, as 3rd-line Therapeutic Option for Patients With Relapsed/Refractory Metastatic Triple-Negative Breast Cancer (mtnbc): Efficacy
Sacituzumab Govitecan (IMMU-132), an Anti-Trop-2-SN-38 Antibody-Drug Conjugate, as 3rd-line Therapeutic Option for Patients With Relapsed/Refractory Metastatic Triple-Negative Breast Cancer (mtnbc): Efficacy
NOVITA SUL TRATTAMENTO DEL CARCINOMA MAMMARIO: MALATTIA TRIPLO NEGATIVA
 SUPERNOVAE IN ONCOLOGIA NOVITA SUL TRATTAMENTO DEL CARCINOMA MAMMARIO: MALATTIA TRIPLO NEGATIVA Dr. Matteo Lambertini U.O. Oncologia Medica 2 IRCCS AOU San Martino IST, Genova Pisa, 14 novembre 2015 AGENDA
SUPERNOVAE IN ONCOLOGIA NOVITA SUL TRATTAMENTO DEL CARCINOMA MAMMARIO: MALATTIA TRIPLO NEGATIVA Dr. Matteo Lambertini U.O. Oncologia Medica 2 IRCCS AOU San Martino IST, Genova Pisa, 14 novembre 2015 AGENDA
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer
 Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Triple negative breast cancer 2014 GASCO Annual meeting September 5 th 2014, Atlanta, GA
 Triple negative breast cancer 2014 GASCO Annual meeting September 5 th 2014, Atlanta, GA Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology,
Triple negative breast cancer 2014 GASCO Annual meeting September 5 th 2014, Atlanta, GA Ruth M. O Regan, MD Professor and Vice-Chair for Educational Affairs, Department of Hematology and Medical Oncology,
Recent Update in Management of Breast Cancer: Medical Oncology. Jin Hee Ahn, M.D., PhD. 23-April-2015
 2015 GBCC & 4 th IBCS 1/37 Recent Update in Management of Breast Cancer: Medical Oncology Jin Hee Ahn, M.D., PhD. 23-April-2015 Department of Oncology, Asan Medical Center, UUCM, Seoul, Korea 2/37 3/37
2015 GBCC & 4 th IBCS 1/37 Recent Update in Management of Breast Cancer: Medical Oncology Jin Hee Ahn, M.D., PhD. 23-April-2015 Department of Oncology, Asan Medical Center, UUCM, Seoul, Korea 2/37 3/37
Amreen Husain, 10 Eric P. Winer, 11 Sylvia Adams, 12 Peter Schmid 13
 IMpassion130: Efficacy in immune biomarker subgroups from the global, randomized, double-blind, placebo-controlled, Phase III study of atezolizumab + nab-paclitaxel in patients with treatment-naive, locally
IMpassion130: Efficacy in immune biomarker subgroups from the global, randomized, double-blind, placebo-controlled, Phase III study of atezolizumab + nab-paclitaxel in patients with treatment-naive, locally
Triple Negative Breast Cancer
 GASCO 2016 San Antonio Breast Cancer Symposium Review Triple Negative Breast Cancer Amelia Zelnak, MD, MSc Atlanta Cancer Care Northside Hospital Cancer Institute Disclosures: consultant for Novartis,
GASCO 2016 San Antonio Breast Cancer Symposium Review Triple Negative Breast Cancer Amelia Zelnak, MD, MSc Atlanta Cancer Care Northside Hospital Cancer Institute Disclosures: consultant for Novartis,
Karcinom dojke. PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski
 Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Karcinom dojke PANEL: Semir Bešlija, Zdenka Gojković, Robert Šeparović, Tajana Silovski MBC: HER2 PHEREXA: Study Design Multicenter, randomized, open-label phase III trial Stratified by prior CNS disease,
Highlights of. Metastatic & Advanced Breast Cancer
 Highlights of Metastatic & Advanced Breast Cancer 1 Financial Disclosure(s) I currently have or have had the following relevant financial relations to disclose: Speaker s Bureau: Novartis 2 Off Label Use
Highlights of Metastatic & Advanced Breast Cancer 1 Financial Disclosure(s) I currently have or have had the following relevant financial relations to disclose: Speaker s Bureau: Novartis 2 Off Label Use
HER2-Targeted Rx. An Historical Perspective
 HER2-Targeted Rx An Historical Perspective Trastuzumab: Front Line Rx for MBC Median 20.3 v. 25.1 mo P = 0.046 HR 0.8 65% of control patients crossed over Slamon D, et al. N Engl J Med, 2001; 344:783 Trastuzumab:Front-line
HER2-Targeted Rx An Historical Perspective Trastuzumab: Front Line Rx for MBC Median 20.3 v. 25.1 mo P = 0.046 HR 0.8 65% of control patients crossed over Slamon D, et al. N Engl J Med, 2001; 344:783 Trastuzumab:Front-line
Highlights in breast cancer
 CONGRESS HIGHLIGHTS SPECIAL EDITION 309 Highlights in breast cancer W. Lybaert, MD In this article, the most important new studies presented at ESMO 2017 in Madrid in early (EBC) and metastatic breast
CONGRESS HIGHLIGHTS SPECIAL EDITION 309 Highlights in breast cancer W. Lybaert, MD In this article, the most important new studies presented at ESMO 2017 in Madrid in early (EBC) and metastatic breast
Edith A. Perez, Ahmad Awada, Joyce O Shaughnessy, Hope Rugo, Chris Twelves, Seock-Ah Im, Carol Zhao, Ute Hoch, Alison L. Hannah, Javier Cortes
 BEACON: A Phase 3 Open-label, Randomized, Multicenter Study of Etirinotecan Pegol (EP) versus Treatment of Physician s Choice (TPC) in Patients With Locally Recurrent or Metastatic Breast Cancer Previously
BEACON: A Phase 3 Open-label, Randomized, Multicenter Study of Etirinotecan Pegol (EP) versus Treatment of Physician s Choice (TPC) in Patients With Locally Recurrent or Metastatic Breast Cancer Previously
Incorporating Immunotherapy into the treatment of NSCLC
 Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Incorporating Immunotherapy into the treatment of NSCLC Suresh S. Ramalingam, MD Roberto C. Goizueta Chair for Cancer Research Assistant Dean for Cancer Research Deputy Director, Winship Cancer Institute
Immunoconjugates in Both the Adjuvant and Metastatic Setting
 Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
Immunoconjugates in Both the Adjuvant and Metastatic Setting Mark Pegram, M.D. Director, Stanford Breast Oncology Program Co-Director, Molecular Therapeutics Program Trastuzumab Treatment of Breast Tumor
San Francisco, CA United States January 27, 2018
 San Francisco, CA United States January 27, 2018 San Francisco, CA USA January 27, 2018 Immunotherapy for Breast Cancer HOPE S. RUGO, MD Professor of Medicine Division of Hematology and Oncology Director,
San Francisco, CA United States January 27, 2018 San Francisco, CA USA January 27, 2018 Immunotherapy for Breast Cancer HOPE S. RUGO, MD Professor of Medicine Division of Hematology and Oncology Director,
How I Approach Triple Negative Breast Cancer (TNBC) Dr Tan Yew Oo Specialist Medical Oncologist Farrer Park Medical Centre Singapore
 Dr Tan Yew Oo Specialist Medical Oncologist Farrer Park Medical Centre Singapore") How I Approach Triple Negative Breast Cancer (TNBC) Dr Tan Yew Oo Specialist Medical Oncologist Farrer Park Medical Centre Singapore Connexion: Integrated Healthcare & Hospitality Complex Levels 11 to
How I Approach Triple Negative Breast Cancer (TNBC) Dr Tan Yew Oo Specialist Medical Oncologist Farrer Park Medical Centre Singapore Connexion: Integrated Healthcare & Hospitality Complex Levels 11 to
Combination Immunotherapy Approaches Chemotherapy, Radiation Therapy, and Dual Checkpoint Therapy
 Combination Immunotherapy Approaches Chemotherapy, Radiation Therapy, and Dual Checkpoint Therapy Dr. David B. Page Providence Portland Medical Center Earle A. Chiles Research Institute Funding & Disclosures
Combination Immunotherapy Approaches Chemotherapy, Radiation Therapy, and Dual Checkpoint Therapy Dr. David B. Page Providence Portland Medical Center Earle A. Chiles Research Institute Funding & Disclosures
Immune checkpoint inhibitors in NSCLC
 1 Immune checkpoint inhibitors in NSCLC Rolf Stahel University Hospital of Zürich Zürich, November 3, 2017 2 What can we learn from the clinical experience of second line immunotherapy of advanced NSCLC?
1 Immune checkpoint inhibitors in NSCLC Rolf Stahel University Hospital of Zürich Zürich, November 3, 2017 2 What can we learn from the clinical experience of second line immunotherapy of advanced NSCLC?
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID
 DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
Immunotherapy in breast cancer. Carmen Criscitiello, MD, PhD European Institute of Oncology Milan, Italy
 Immunotherapy in breast cancer Carmen Criscitiello, MD, PhD European Institute of Oncology Milan, Italy Outline Rational for immune-based therapy in breast cancer Immunogenic chemotherapy Targeting immune
Immunotherapy in breast cancer Carmen Criscitiello, MD, PhD European Institute of Oncology Milan, Italy Outline Rational for immune-based therapy in breast cancer Immunogenic chemotherapy Targeting immune
Breast : ASCO Abstracts for Review
 Breast : ASCO 2011 Susana Campos, MD, MPH Dana Farber Cancer Institute Abstracts for Review Prevention Neoadjuvant Metastatic Brain mets LBA 504: Exemestane for primary prevention of breast cancer in postmenopausal
Breast : ASCO 2011 Susana Campos, MD, MPH Dana Farber Cancer Institute Abstracts for Review Prevention Neoadjuvant Metastatic Brain mets LBA 504: Exemestane for primary prevention of breast cancer in postmenopausal
Checkpoint Inibitors for Bladder Cancer
 Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Checkpoint Inibitors for Bladder Cancer Daniel P. Petrylak, MD Professor of Medicine and Urology Director, GU Translational Working Group Co Director, Signal Transduction Program Smilow Cancer Center,
Immunotherapies for Advanced NSCLC: Current State of the Field. H. Jack West Swedish Cancer Institute Seattle, Washington
 Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
Immunotherapies for Advanced NSCLC: Current State of the Field H. Jack West Swedish Cancer Institute Seattle, Washington Nivolumab in Squamous NSCLC Chemo-pretreated (1 st line) Adv squamous NSCLC N =
PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND!
 II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND! INGRID A. MAYER, MD, MSCI Assistant
II Simpósio Internacional de Câncer de Mama para o Oncologista Clínico PROGNOSTICO DE PACIENTES COM CA DE MAMA METASTATICO HER2+: PODEMOS FAZER MAIS? TDM-1 AND BEYOND! INGRID A. MAYER, MD, MSCI Assistant
PROSTATE CANCER HORMONE THERAPY AND BEYOND. Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute
 PROSTATE CANCER HORMONE THERAPY AND BEYOND Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute Disclosures I am a Consultant for Bayer and Sanofi-Aventis
PROSTATE CANCER HORMONE THERAPY AND BEYOND Przemyslaw Twardowski MD Professor of Oncology Department of Urologic Oncology John Wayne Cancer Institute Disclosures I am a Consultant for Bayer and Sanofi-Aventis
New chemotherapy drugs in metastatic breast cancer. Guy Jerusalem, MD, PhD
 New chemotherapy drugs in metastatic breast cancer Guy Jerusalem, MD, PhD MBC Patients survival over time Median survival increases over time, but is still measured in months This is not yet a chronic
New chemotherapy drugs in metastatic breast cancer Guy Jerusalem, MD, PhD MBC Patients survival over time Median survival increases over time, but is still measured in months This is not yet a chronic
Recent Therapeutic Advances for Thoracic Malignancies
 Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
Recent Therapeutic Advances for Thoracic Malignancies Developed in collaboration Learning Objectives Upon completion, participants should be able to: Interpret new developments in the use of radiation
Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA
 Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA When Are Biomarkers Ready To Use? Same Rules for Gene Expression Panels Key elements
Gene Signatures in Breast Cancer: Moving Beyond ER, PR, and HER2? Lisa A. Carey, M.D. University of North Carolina USA When Are Biomarkers Ready To Use? Same Rules for Gene Expression Panels Key elements
Patient Selection: The Search for Immunotherapy Biomarkers
 Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Patient Selection: The Search for Immunotherapy Biomarkers Mark A. Socinski, MD Executive Medical Director Florida Hospital Cancer Institute Orlando, Florida Patient Selection Clinical smoking status Histologic
Subtype-directed therapy of TNBC Global Breast Cancer Conference 2015 & 4th International Breast Cancer Symposium Jeju Island, Korea, April 2015
 Subtype-directed therapy of TNBC Global Breast Cancer Conference 2015 & 4th International Breast Cancer Symposium Jeju Island, Korea, April 2015 Ruth M. O Regan, MD Visiting Professor and Division Chief
Subtype-directed therapy of TNBC Global Breast Cancer Conference 2015 & 4th International Breast Cancer Symposium Jeju Island, Korea, April 2015 Ruth M. O Regan, MD Visiting Professor and Division Chief
Updates in Immunotherapy for Urothelial Carcinoma
 Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
Updates in Immunotherapy for Urothelial Carcinoma Andrew J Armstrong MD ScM FACP DUA 2018 Copyright 2006 SciMed. Talk Outline Immunotherapy progress in 2017: 5 new approved PD-1/PD-L1 inhibitory agents
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS
 IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
IMMUNOTHERAPY FOR GASTROINTESTINAL CANCERS Dr Elizabeth Smyth Cambridge University Hospitals NHS Foundation Trust ESMO Gastric Cancer Preceptorship Valencia 2018 DISCLOSURES Honoraria for advisory role
Science-Based Innovation-Focused ADC Company. Corporate Overview June 2018
 Science-Based Innovation-Focused ADC Company Corporate Overview June 2018 Forward-Looking Statements This presentation, in addition to historical information, contains certain forwardlooking statements
Science-Based Innovation-Focused ADC Company Corporate Overview June 2018 Forward-Looking Statements This presentation, in addition to historical information, contains certain forwardlooking statements
Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma
 Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
PARP Inhibitors: Patients Selection. Dr. Cristina Martin Lorente Hospital de la Santa Creu i Sant Pau Formigal, June 23th 2016
 PARP Inhibitors: Patients Selection Dr. Cristina Martin Lorente Hospital de la Santa Creu i Sant Pau Formigal, June 23th 2016 OVARIAN CANCER (OC): MULTIPLES DISEASES Different types with different behaviour
PARP Inhibitors: Patients Selection Dr. Cristina Martin Lorente Hospital de la Santa Creu i Sant Pau Formigal, June 23th 2016 OVARIAN CANCER (OC): MULTIPLES DISEASES Different types with different behaviour
New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer
 New Evidence reports on presentations given at ASCO 2012 New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer Presentations at ASCO 2012 Breast
New Evidence reports on presentations given at ASCO 2012 New Targeted Agents Demonstrate Greater Efficacy and Tolerability in the Treatment of HER2-positive Breast Cancer Presentations at ASCO 2012 Breast
Current Issues in Checkpoint Immunotherapy for NSCLC: A Perspective from January 2018
 Current Issues in Checkpoint Immunotherapy for NSCLC: A Perspective from January 2018 David R. Gandara, MD University of California Davis Comprehensive Cancer Center Disclosures Research Grants: AstraZeneca/Medi,
Current Issues in Checkpoint Immunotherapy for NSCLC: A Perspective from January 2018 David R. Gandara, MD University of California Davis Comprehensive Cancer Center Disclosures Research Grants: AstraZeneca/Medi,
Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer
 Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer Sara A. Hurvitz, MD, FACP Associate Professor of Medicine University of California Los Angeles Los Angeles, California Trastuzumab
Expanding Therapeutic Strategies for HER2-Positive Metastatic Breast Cancer Sara A. Hurvitz, MD, FACP Associate Professor of Medicine University of California Los Angeles Los Angeles, California Trastuzumab
Cancer du sein métastatique et amélioration de la survie Pr. X. Pivot
 Cancer du sein métastatique et amélioration de la survie Pr. X. Pivot Date of preparation: November 2015. EU0250i TTP/PFS Comparaisons First line metastatic breast cancer Monotherapy Docetaxel Chan 1999
Cancer du sein métastatique et amélioration de la survie Pr. X. Pivot Date of preparation: November 2015. EU0250i TTP/PFS Comparaisons First line metastatic breast cancer Monotherapy Docetaxel Chan 1999
Update on Breast Cancer
 Update on Breast Cancer William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center Feinberg School of Medicine Northwestern University Overview PARP Inhibitors Neoadjuvant
Update on Breast Cancer William J. Gradishar, MD Professor of Medicine Robert H. Lurie Comprehensive Cancer Center Feinberg School of Medicine Northwestern University Overview PARP Inhibitors Neoadjuvant
A Giant Leap in the Treatment Options for Advanced Bladder Cancer
 A Giant Leap in the Treatment Options for Advanced Bladder Cancer Yohann Loriot, MD, PhD Department of Cancer Medicine & INSERM U981 Gustave Roussy Villejuif, France Clinical Features of Bladder Cancer
A Giant Leap in the Treatment Options for Advanced Bladder Cancer Yohann Loriot, MD, PhD Department of Cancer Medicine & INSERM U981 Gustave Roussy Villejuif, France Clinical Features of Bladder Cancer
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
II sessione. Immunoterapia oltre la prima linea. Alessandro Tuzi ASST Sette Laghi, Varese
 II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
II sessione Immunoterapia oltre la prima linea Alessandro Tuzi ASST Sette Laghi, Varese AGENDA Immunotherapy post-chemo ( true 2/3L ) Immunotherapy in oncogene addicted NSCLC (yes/no? when?) Immunotherapy
Largos Supervivientes, Tenemos datos?
 Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Largos Supervivientes, Tenemos datos? Javier Puente, MD, PhD Medical Oncology Department. Hospital Clinico San Carlos Associate Professor of Medicine. Complutense University of Madrid. Summary Snapshot
Terapia sistemica neoadiuvante: in quali tumori? Quali risultati? Dott. Giacomo Pelizzari
 Terapia sistemica neoadiuvante: in quali tumori? Quali risultati? Dott. Giacomo Pelizzari Neoadjuvant Treatment A window of opportunity Rational: Historically proposed to enable breast-conserving surgery
Terapia sistemica neoadiuvante: in quali tumori? Quali risultati? Dott. Giacomo Pelizzari Neoadjuvant Treatment A window of opportunity Rational: Historically proposed to enable breast-conserving surgery
Role of chemotherapy in BRCA and Triple negative breast cancer. Fernando Moreno Servicio de Oncología Médica Hospital Clinico San Carlos
 Role of chemotherapy in BRCA and Triple negative breast cancer Fernando Moreno Servicio de Oncología Médica Hospital Clinico San Carlos Association between TNBC & germline mutations in BRCA 1/2 TNBC is
Role of chemotherapy in BRCA and Triple negative breast cancer Fernando Moreno Servicio de Oncología Médica Hospital Clinico San Carlos Association between TNBC & germline mutations in BRCA 1/2 TNBC is
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento
 tra la prima e la seconda linea di trattamento") Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
Il ruolo di PD-L1 (42%) tra la prima e la seconda linea di trattamento Alessia Pochesci Divisione di Oncologia Toracica Istituto Europeo di Oncologia, Milano Tutor: Prof.ssa Silvia Novello Dott.ssa Chiara
10/15/2012. Inflammatory Breast Cancer vs. LABC: Different Biology yet Subtypes Exist
 Triple-Negative Breast Cancer: Optimizing Treatment for Locally Advanced Breast Cancer Beth Overmoyer MD Director, Inflammatory Breast Cancer Program Dana Farber Cancer Institute Overview Inflammatory
Triple-Negative Breast Cancer: Optimizing Treatment for Locally Advanced Breast Cancer Beth Overmoyer MD Director, Inflammatory Breast Cancer Program Dana Farber Cancer Institute Overview Inflammatory
Breast cancer treatment
 Report from the San Antonio Breast Cancer Symposium Breast cancer treatment Determining the best options for select patient groups Sara Soldera, MD, Resident; Nathaniel Bouganim, MD, FRCPC, Medical Oncologist;
Report from the San Antonio Breast Cancer Symposium Breast cancer treatment Determining the best options for select patient groups Sara Soldera, MD, Resident; Nathaniel Bouganim, MD, FRCPC, Medical Oncologist;
Update on the Management of HER2+ Breast Cancer. Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany
 Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Update on the Management of HER2+ Breast Cancer Christian Jackisch, MD, PhD Sana Klinikum Offenbach Offenbach, Germany Outline Treatment strategies for HER2-positive metastatic breast cancer since First
Endocrine Therapy 2017: Is There a Better Single Agent and when Should we Use it?
 Endocrine Therapy 2017: Is There a Better Single Agent and when Should we Use it? ET1 ET2 ET3 Targeted agent 1 Targeted agent 2 Hope S. Rugo, MD Director, Breast Oncology and Clinical Trials Education
Endocrine Therapy 2017: Is There a Better Single Agent and when Should we Use it? ET1 ET2 ET3 Targeted agent 1 Targeted agent 2 Hope S. Rugo, MD Director, Breast Oncology and Clinical Trials Education
Triple-Negative Breast Cancer Time to Slice and Dice? Carsten Denkert, MD Charité University Hospital Berlin, Germany
 Triple-Negative Breast Cancer Time to Slice and Dice? Carsten Denkert, MD Charité University Hospital Berlin, Germany Triple-Negative Breast Cancer (TNBC) 2018 Presentation Outline The molecular heterogeneity
Triple-Negative Breast Cancer Time to Slice and Dice? Carsten Denkert, MD Charité University Hospital Berlin, Germany Triple-Negative Breast Cancer (TNBC) 2018 Presentation Outline The molecular heterogeneity
Medical Treatment of Advanced Lung Cancer
 Medical Treatment of Advanced Lung Cancer Oncology for Scientists April 26, 2018 Edwin Yau, MD., Ph.D. Assistant Professor of Oncology Department of Medicine Department of Cancer Genetics and Genomics
Medical Treatment of Advanced Lung Cancer Oncology for Scientists April 26, 2018 Edwin Yau, MD., Ph.D. Assistant Professor of Oncology Department of Medicine Department of Cancer Genetics and Genomics