The Beginning radical Radical Mastectomy mastectomy
|
|
|
- Thomas Rogers
- 6 years ago
- Views:
Transcription

1 Controversies about Surgical Treatment of Breast Cancer Schlomo Schneebaum MD Breast Health Center Department of Surgery Tel-Aviv Sourasky Medical, Center Tel-Aviv ISRAEL 2nd International Congress of Breast Disease Centers 9-10 February 2012 Paris FRANCE

2 The Beginning radical Radical Mastectomy mastectomy

3 A surgeon is not a barber anymore Previously: Radical Mastectomy Today: Modified radical Mastectomy Quadrantectomy and Axillary lymph node dissection Lumpectomy and Axillary lymph node dissection Lumpectomy and sentinel lymph node dissection
4 A surgeon has become a taylor - Personalized treatment Wide local incision with the intention of a 1 cm free margin including reconstruction of the breast where dead space should be kept to a minimum. Any oncoplastic technique should always be applied. Skin sparing mastectomy and immediate reconstruction. Sentinel node biopsy (if preoperative assessment is negative). Axillary lymph node dissection if pre lymph node assessment or SN is positive (> isolated tumor cells). Mastectomy with or without ALND.
5 Breast Cancer Tumor Genetic Luminal A (ER+, PR+, HER2-) Luminal B (ER+, PR+, HER2+) HER2 (ER-, PR-, HER2+) Basal (ER-, PR-, HER2-) Subtypes
6 Breast Cancer Tumor Genetic Subtypes
7 Controversies about Surgical Treatment of Breast Cancer Breast Bilumpectomy Nipple Sparing Mastectomy Axilary lymph node dissection Completion Axillary Dissection DCIS
8 Controversies about Surgical Treatment of Breast Cancer Breast Bilumpectomy - No Data Nipple Sparing Mastectomy No Data (only descriptive reports of feasibility) In a risk reducing mastectomy study the only two recurrences were in patients who underwent nipple sparing mastectomy Old data of subcutaneous mastectomy had bad results
9 Controversies about Surgical Treatment of Breast Cancer Axillary Lymph node Dissection Important component in breast cancer treatment Curative element in the Halstedian Concept Important prognostic source of information Regional control

10 SENTINEL NODE CONCEPT The lymph node nearest to the primary tumor site on the direct drainage pathway is the most likely site of early metastasis SN Non-SNN
11 NSABP B-32 randomized phase 3 trial Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negativenegative patients with breast cancer: overall survival findings from the NSABP B-32 randomised phase 3 trial David N Krag, Stewart J Anderson, Thomas B Julian, Ann M Brown, Seth P Harlow, Joseph P Costantino, Takamaru Ashikaga, Donald L Weaver, Eleftherios P Mamounas, Lynne M Jalovec, Thomas G Frazier, R Dirk Noyes, Robidoux, Hugh M C Scarth, Norman AndrיWolmark
12 NSABP B-32 randomized phase 3 trial Conclusion: There is no significant difference in survival between SLN followed by ALND and SLN surgery alone in patients with negative SLNs.




13 Sentinel Node Biopsy-2012 Standard of care Better staging Less morbidity Today Dilemma Is completion ALND necessary? Is Sentinel node biopsy justified for DCIS?
14 Completion Axillary Dissection Following Positive Sentinel Node Biopsy Several Retrospective Studies: Usually associated with only one axillary L.N. are: Tumor size < 1 cm Micrometastasis No extranodal extension No subgroup could be identified in which axillary dissection may be omitted
15 Prediction of Non-SLN Metastasis With MSKCC Nomogram Tumor type and nuclear grade Lymphovascular invasion Multifocality of primary tumor Estrogen receptor status Number of negative SLNs Number of positive SLNs Pathologic size in centimeters Methods of detection of SLN metastasis Van Zee KZ et al. Ann Surg Oncol. 2003
16 Prediction of Non-SLN Metastasis With MSKCC Nomogram Van Zee KZ et al. Ann Surg Oncol. 2003
17 Prediction of Non-SLN Metastasis With MSKCC Nomogram Nomogram was examined by Receiver Operating Curve (ROC) The inherent capacity of a test to discriminate a diseased from a nondiseased subject across all possible levels of positivity Area under the ROC:» 0.5 flipping a coin 1.0 perfect test 702 patients who underwent complete ALND Area under ROC curve patients prospective group Area under ROC curve 0.77 Van Zee KZ et al. Ann Surg Oncol. 2003
18 Prediction of Non-SLN Metastasis Conclusion With MSKCC Nomogram Given the institutional variation in SLN technique and pathological processing we recommend that the Nomogram be validated at each institution before its use for patient counseling. Lampert LA et al. Ann Surg Oncol. 2006
19 A surgeon has become a taylor - Personalized treatment Axillary lymph node dissection if pre lymph node assessment or SN is positive (> isolated tumor cells). Axillary lymph node dissection if pre lymph node assessment or SN is positive (>micrometastasis). Axillary lymph node dissection if pre lymph node assessment or SN is positive (> 2 lymph nodes involved).
20 Characteristics of Positive Sentinel Lymph Node in Breast Cancer Patients as Predictor of Non Sentinel Lymph Node Metastasis Baruch E, Yaal-Hahoshen N, Stadler Y, Kahn P, Gat A, Sperber F, Even-Sapir E, Skornick Y, Inbar M, Schneebaum S Breast Health Center, Department of Surgery "A", Department of Oncology, Pathology, Nuclear Medicine, and Mammography Unit of Radiology Tel-Aviv Sourasky Medical Center, Sackler Faculty of Medicine, Tel Aviv University, Tel-Aviv, Israel 14th Congress of the European Society of Surgical Oncology September, 2008 The Netherlands - Hague
21 Testing the nomogram on our population: Patients From November 1994 through July 2007, 568 breast cancer patients underwent SLN biopsy at the Tel Aviv-Sourasky Medical Center. 103 (18 18%) had a positive SLN biopsy. 80 of them had consecutive CALND. 13 of them had Neo-adjuvant therapy prior to the SLN biopsy.
22 Testing the nomogram on our population: Methods A nomogram score was calculated for each patient. For the Neo-Adj group 2 scores:» Tumor size based on pathology.» Tumor size based on Pre-Neo Imaging. The MSKCC nomogram was assessed by the area under ROC curve. To address the calibration accuracy of the nomogram, a calibration plot was drawn. Univariate logistic regression analysis was applied to our database variables.
23 Results 103 patients had positive SLN biopsy. 80 patients underwent CALND. 32 (40%) with Non-SLN involvement. 23 patients with positive SLN did not undergo CALND. In a mean follow up of 3 years, only 1 of them had distant recurrence with no axillary recurrence.
24 ROC Curve and Calibration plot: Excluding Neo-Adj Patients obse erved expected AUC=0.64 R=0.96
25 Trends in and outcomes from sentinel lymph node biopsy (SLNB) alone vs. SLNB with axillary lymph node dissection for node-positive breast cancer patients: experience from the SEER database NCCN guidelines: completion of axillary dissection for patients with N>0.2 mm Approximately 50% - no further metastases SEER data : 26,986 patients with a positive sentinel node biopsy and at least 24 months follow-up Yi et al, Ann Surg Oncol 2010
26 Trends in and outcomes from sentinel lymph node biopsy (SLNB) alone vs. SLNB with axillary lymph node dissection for node-positive breast cancer patients: experience from the SEER database Yi et al, Ann Surg Oncol 2010
27 Trends in and outcomes from sentinel lymph node biopsy (SLNB) alone vs. SLNB with axillary lymph node dissection for node-positive breast cancer patients: experience from the SEER database Multivariate analysis of factors associated with undergoing Characteristic SLNB alone Odds ratio P value (95% CI) Age ( ) < Segmental mastectomy 2.8 ( ) < T1 1.2 ( ) < Micrometastasis 3.8 ( ) < Grade: Low/intermediate Estrogen receptor Positive 1.4 ( ) < ( ) Yi et al, JCO 2010
28 Completion Axillary Dissection Following Positive Sentinel Node Biopsy American College of Surgery - Oncology Group (ACOSOG) Z0011 trial Multicenter study Aim: Significance of axillary LN dissection for SLN positive (H&E) patients Randomization: ALND vs. No additional axillary treatment
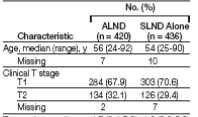
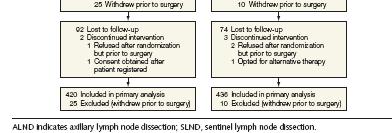
29 ACOSOG Z0011- Axillary Dissection vs. No Axillary Dissection in Women With Sentinel Node Metastasis non-inferiority: at least 75% 5 year survival in the control arm. Study terminated early due to low accrual and low overall mortality 20 years of follow-up would be needed to reach a conclusion 445 and 446 patients enrolled Study design: treatment arm 80% 5 year overall survival; Guilliano et al, JAMA 2011

30
31 ACOSOG Z0011- Axillary Dissection vs. No Axillary Dissection in Women With Sentinel Node Metastasis Results: Median follow-up 6.3 years. 5 year survival 92% rate of wound infections, axillary seromas, and paresthesias for ALND vs. SLND: 70% vs. 25%, P <.001 Lymphedema in the ALND group was significantly more common by subjective report (P <.001). Guilliano et al, JAMA 2011
32 ACOSOG Z0011- Axillary Dissection vs No Axillary Dissection in Women With Sentinel Node Metastasis Survival of the ALND Group Compared With SLND-Alone Group Median follow-up 6.3 years. 5 year survival 92% Guilliano et al, JAMA 2011
33 Partial recruitment (intended 1900 vs. 891) Mostly T1 (intended: T1 and T2) Mostly ER positive All patients radiated Tangent All patients received Chemo Most of the patients SLN metastasis after first surgery Short follow up
34 Prediction of Non-SLN Metastasis With Pathologic size Estrogen receptor status Methods of detection Number of positive SLNs Number of negative SLNs Tumor type and nuclear grade Lymphovascular invasion Calculated percentage MSKCC Nomogram Actual Study Data H&E 1 1 Ductal II no 12% Virtual patients FS 2 0 Lobular yes 72% FS 2 0 Ductal II no 64%
35 Completion Axillary Dissection St Gallen consensus meeting 2011 Axillary lymph node dissection is recommended if Sentinel Node is positive No Axillary lymph node dissection is recommended if Sentinel Node is positive: for isolated tumor cells only (less than 0.2 mm) for micrometastasis (0.2-2mm)
36 Completion Axillary Dissection MD Anderson implementation of Z0011 Data No Axillary lymph node dissection is recommended if Sentinel Node is positive: for isolated tumor cells only (less than 0.2 mm) for micrometastasis (0.2-2mm) For 1-2 lymph nodes ER +,PR+ patients but add radiation to the axilla Axillary lymph node dissection is recommended if Sentinel Node is positive for Lobular carcinoma ER-,PR- or HER-2 + Post Mastectomy Post Neoadjuvant Caution :young age, nodular ratio.
37 DCIS (Ductal Carcinoma In Situ) Most common presentation: Clustered microcalcifications Mass Pathologic nipple discharge Incidental findings Proliferation of malignant epithelial cells within the mammary ductal lobular system without light microscopy invasion into the surrounding stroma DCIS pts % Axillary metastasis
38 SENTINEL NODE BIOPSY IN BREAST CANCER DCIS 74 patients (DCIS/DCIS+microinvasion <1mm) n Pos. SLN Pos. IHC High-risk DCIS 38 5/38 (13%) 4/5 DCIS with microinvasion 36 5/36 (14%) 5/ complete axillary lymph node dissection, 1 non-sln (+) (High risk = high grade, large tumor palpable, multifocality) Klauber-DeMore et al. MSKCC, SSO 2000
39 SENTINEL NODE BIOPSY IN BREAST CANCER 38 pts. with DCIS or with microinvasion Indications: 1. patient requiring mastectomy 52.6% (n=20) 2. extensive multifocal/multicentric disease 23.6% (n=9) 3. pathology suspicious for microinvasion 10.5% (n=4) 4. presence of microinvasion 7.8% (n=3) 5. mammogram/sonogram suspicious for invasion 2.6% (n=1) 6. low grade lesion >=3cm 2.6% (n=1) 4/38 (10.5%) SLN positive in categories 1,2,3 and 5 Hoover et al. Abs. P78, SSO 2002
40 PRO SENTINEL NODE BIOPSY for Mastectomy: DCIS Not to lose opportunity if invasive carcinoma is ultimately discovered in their mastectomy specimen. Only a small volume of breast tissue is usually being evaluated Positive SLN can surrogate for invasion.
41 SENTINEL NODE BIOPSY for DCIS PRO Prevent second operation Palpable DCIS Radiographic involvement more than 4 cm. High nuclear grade Questionable areas of micro invasion.
42 CON SENTINEL NODE BIOPSY for DCIS Surgeon is not a Barber Only 1-2% DCIS die of breast cancer,die of missed Ca in tissue removed. 3% micro metastasis, clinical significance? 20-25% will have invasive component, unnecessary operation in 75-80%
43 SENTINEL NODE BIOPSY for DCIS While DCIS remains a disease without metastatic potential its association and coexistence with invasive carcinoma require a selective approach to staging


44
45 Reference Patients(n) ROC Correlation(r) Van Zee et al., USA, Kocsis et al., Hungary, Smidt et al., The Netherlands, ~1 Degnim et al., USA, 2005 Mayo Clinic Michigan N/A N/A Soni et al., Australia, N/A Lambert et al., USA Full database excluding neoadjuvant patients and incomplete data Ponzone et al., Italy, N/A Cripe et al., USA, Dauphine et al., USA, N/A Zgajnar et al., Slovenia, N/A* Alran et al., France, N/A Pal et al., UK, N/A Klar et al., Germany, N/A * The nomogram was biased. Published later by Cserni G, Am J Surg 2007
46 Completion Axillary Dissection Following Positive Sentinel Node Biopsy MULTICENTER STUDIES AMAROS: After Mapping of the Axilla: Radiotherapy or Surgery EORTC All patients SLND If positive: randomization to surgical treatment vs. radiation therapy Aim: Importance of CLND vs. Radiation treatment
47 Conclusion cont. Institutional variation in SLN biopsy technique and pathological processing might be responsible for wide range of results. Lack of pathological data for Neo-Adj patients impairing the nomogram s prediction ability. Cancer centers should test the performance of the MSKCC nomogram on their own population prior to introducing it into clinical use.


48 ROC curve and calibration plot: The entire population observe ed expected AUC=0.63 R=0.87




49 ROC curve for Neo-Adj group Based on imaging tumor size AUC=0.51 Based on pathological tumor size AUC=0.44
50 Randomized Trial Comparing Axillary Clearance Versus No Axillary Clearance in Older Patients With Breast Cancer: First Results of International Breast Cancer Study Group Trial patients age 60 years +, T1-3, clinically node negative Randomized to breast surgery with +/- axillary dissection (from 1999 also sentinel node) All received adjuvant tamoxifen for 5 years (from 2002 only those with ER+). Outcomes: quality of life, disease-free survival, overall survival 1,020 patients needed to assess no difference in survival In 2000 redesign (430 patients accrued)- difference in quality of life. International Breast Cancer Study Group, JCO 2006
51 Axillary Clearance in Older Patients With Breast Cancer: First Results of International Breast Cancer Study Group Trial Median age 74 80% ER+ disease. 28% node positive (ALND group) International Breast Cancer Study Group, JCO 2006
52 Randomized Trial Comparing Axillary Clearance Versus No Axillary Clearance in Older Patients With Breast Cancer: First Results of International Breast Cancer Study Group Trial International Breast Cancer Study Group, JCO 2006
53 . International Breast Cancer Study Group, JCO 2006
54 Randomized Trial Comparing Axillary Clearance Versus No Axillary Clearance in Older Patients With Breast Cancer: First Results of International Breast Cancer Study Group Trial Conclusions: avoiding axillary clearance for older women with clinically node-negative negative breast cancer who receive adjuvant tamoxifen seems safe and results in early improved quality of life. International Breast Cancer Study Group, JCO 2006
55
56 ACOSOG Z0011- Axillary Dissection vs. No Axillary Dissection in Women With Sentinel Node Metastasis Groups were similar in baseline characteristics More nodes removed in the axillary dissection group (median 17 vs. 2) Micrometastatic disease (N1mic< mic<2mm) mm) was identified in 45% of SLNB and 38% of ALND (p=0.5) Additional metastatic nodes: 27% of patients in the ALND group. Patients with micrometastatic disease- 10% had additional disease. Similar rates of adjuvant chemotherapy and radiation treatment (whole breast including low axilla). Guilliano et al, JAMA 2011
57 ACOSOG Z0011- Axillary Dissection vs. No Axillary Dissection in Women With Sentinel Node Metastasis. Hazard Ratios Comparing Overall Survival Between the ALND and SLND-Alone Groups Guilliano et al, JAMA 2011
58 Trends in and outcomes from sentinel lymph node biopsy (SLNB) alone vs. SLNB with axillary lymph node dissection for node-positive breast cancer patients: experience from the SEER database worse disease specific survival for Same overall survival patients undergoing ALND- Better loco-regional control in patients with macrometastatic disease who had ALND ( vs. 0.2%; HR, 0.30; P = 0.02). Yi et al, JCO 2010
59 NSABP B-32 randomized phase 3 trial Sentinel-lymph-node resection compared with conventional axillary-lymph-node dissection in clinically node-negative patients with breast cancer: overall survival findings from the NSABP B-32 randomised phase 3 trial David N Krag, Stewart J Anderson, Thomas B Julian, Ann M Brown, Seth P Harlow, Joseph P Costantino, Takamaru Ashikaga, Donald L Weaver, Eleftherios P Mamounas, Lynne M Jalovec, Thomas G Frazier, Robidoux, Hugh M C Scarth, Norman Rי Dirk Noyes, Andr Wolmark
60 NSABP B-32 randomized phase 3 trial
61 NSABP B-32 randomized phase 3 trial
62 Univariate Analysis Parameter Number of positive SLN excised Number of total SLN excised Tumor size Tumor grade Tumor type ER Status Neo-Adjuvant treatment Lympho-vascular invasion PR Status Number of negative SLN excised Her-2 Status Pathological detection method Multifocality Age P

63 NSABP B-32 randomized phase 3 trial
64 Completion Axillary Dissection Following Positive Sentinel Node Biopsy RESTROSPECTIVE STUDIES Predictors of positive non-sln Stage of primary tumor, SLN metastases size (micro vs. macro), lymphovascular invasion (1) Tumor size >1cm, SLN metastases size, extranodal extension, apex L.N. involvement (2) SLN metastases size (3) Primary tumor size, SLN metastases size, lymphovascular invasion (4) Conclusion: Pts. With T1a-T1b or G1 tumor should be spared ALND. (4) 1. Weiser et al, SSO Kuijit GP et al. EJSO Fan YG et al. Ann Oncol Surg Gipponi M. et al. EJSO 2006
65 Completion Axillary Dissection Following Positive Sentinel Node Conclusion Biopsy No subgroup could be identified in which axillary dissection may be omitted Usually associated with only one axillary L.N. are: Tumor size < 1 cm Micrometastasis No extranodal extension Kuijit GP et al. EJSO 2006
66
67 ACOSOG Z0011- Axillary Dissection vs. No Axillary Dissection in Women With Sentinel Node Metastasis Patients with limited metastatic disease in the axilla (stage 2) have very good 5 year survival. Limited disease- high rate of micrometastatic disease (only 27% had additional metastatic lymph nodes). 2/3 of the patients were randomized after final pathology documented a positive sentinel node. Limited follow-up (6.3 years). The Z0011 trial did not include patients undergoing mastectomy, lumpectomy without radiotherapy, partial- breast irradiation, neoadjuvant therapy 67 and 69% were ER+- Can conclusions be drawn for different subtypes of breast cancer (Her2n+, triple negative?) Guilliano et al, JAMA 2011
68 SENTINEL NODE BIOPSY IN BREAST CANCER NASBP B 04 STUDY MODIFIED RADICAL MASTECTOMY (MRM) vs. TOTAL MASTECTOMY (TM) MRM 38% AXILLARY METASTASIS TM ONLY 18% REQUIRED AXILLARY DISSECTION AT 10 YEARS - SAME DFS; OVERALL SURVIVAL Fisher B et al. NEJM 1988
69 Orr RK, Ann Surg Oncol, 1999
70 Impact of prophylactic axillary dissection on breast cancer survival-metanalysis axillary dissection confers a survival advantage of 5.4%;(95% CI ), Orr RK, Ann Surg Oncol, 1999
71 Impact of prophylactic axillary dissection on breast cancer survival-metanalysis
72

73
74 Prediction of Non-SLN Metastasis With MSKCC Nomogram Nomogram was examined by Receiver Operating Curve (ROC) The inherent capacity of a test to discriminate a diseased from a nondiseased subject across all possible levels of positivity Area under the ROC:» 0.5 flipping a coin 1.0 perfect test 702 patients who underwent complete ALND Area under ROC curve patients prospective group Area under ROC curve 0.77 Van Zee KZ et al. Ann Surg Oncol. 2003
75 Prediction of Non-SLN Metastasis With No of patients site MSKCC Nomogram Nijmegen, Netherlands 696 Bacs-Kiskum County Teaching Hospital, Hungary Texas M.D. Anderson Cancer Center Positive SLN with completion ALND Intraopertative method Frozen section Touch imprint cytology Touch imprint cytology Results : ROC Correlation Obs. to Pred Conclusions: Nomogram is valid for populations that differ considerably from the population from which it was developed. Nomogram could not be validated Authors warn against the unvalidated use Nomogram also accurate for TIC
76 Prediction of Non-SLN Metastasis With MSKCC Nomogram Possible explanation to Bacs-Kiskum results discrepancy Number of SLN removed: Removal of maximum 3 (B.K.) Removal of all blue and hot (MSKCC) B.K. mean SLNs and median 1 SLN MSKCC mean 2.7 SLNs and median 2 SLNs Studies show that in 98% of positive SLN the positive node is in the first three nodes. Therefore fewer nodes removed would imply higher number of non SLN positive. Lampert LA et al. Ann Surg Oncol. 2006
77 ROC Curve and Calibration plot: Excluding Neo-Adj Patients obse erved expected AUC=0.64 R=0.96
78 CON SENTINEL NODE BIOPSY for Surgeon is not a Barber DCIS Age 55 or younger O.R P= Core needle biopsy O.R P= Size DCIS greater than 4 cm O.R P= High grade O.R P= NOT to PERFORM just because we can
79 SENTINEL NODE BIOPSY for DCIS PRO Image guided core needle biopsy Identify benign Maybe upstaged Prevent second operation Palpable DCIS Radiographic involvement more than 4 cm. High nuclear grade Questionable areas of micro invasion.
Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer
 - Official Statement - Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer Sentinel lymph node (SLN) biopsy has replaced axillary lymph node dissection (ALND) for the
- Official Statement - Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer Sentinel lymph node (SLN) biopsy has replaced axillary lymph node dissection (ALND) for the
The Role of Sentinel Lymph Node Biopsy and Axillary Dissection
 The Role of Sentinel Lymph Node Biopsy and Axillary Dissection Henry Mark Kuerer, MD, PhD, FACS Department of Surgical Oncology University of Texas MD Anderson Cancer Center SLN Biopsy Revolutionized surgical
The Role of Sentinel Lymph Node Biopsy and Axillary Dissection Henry Mark Kuerer, MD, PhD, FACS Department of Surgical Oncology University of Texas MD Anderson Cancer Center SLN Biopsy Revolutionized surgical
Results of the ACOSOG Z0011 Trial
 DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
Debate Axillary dissection - con. Prof. Dr. Rodica Anghel Institute of Oncology Bucharest
 Debate Axillary dissection - con Prof. Dr. Rodica Anghel Institute of Oncology Bucharest Summer School of Oncology, third edition Updated Oncology 2015: State of the Art News & Challenging Topics Bucharest,
Debate Axillary dissection - con Prof. Dr. Rodica Anghel Institute of Oncology Bucharest Summer School of Oncology, third edition Updated Oncology 2015: State of the Art News & Challenging Topics Bucharest,
Implications of ACOSOG Z11 for Clinical Practice: Surgical Perspective
 :$;7)#*8'-87*4BCD'E7)F'31$4.$&'G$H'E7)F&'GE'>??ID >?,"'@4,$)4*,#74*8'!74/)$++'74',"$'A.,.)$'7%'()$*+,'!*42$)!7)74*67&'!3 6 August 2011 Implications of ACOSOG Z11 for Clinical
:$;7)#*8'-87*4BCD'E7)F'31$4.$&'G$H'E7)F&'GE'>??ID >?,"'@4,$)4*,#74*8'!74/)$++'74',"$'A.,.)$'7%'()$*+,'!*42$)!7)74*67&'!3 6 August 2011 Implications of ACOSOG Z11 for Clinical
Implications of ACOSOG Z11 for Clinical Practice: Surgical Perspective
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA 6 August 2011 Implications of ACOSOG Z11 for Clinical
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA 6 August 2011 Implications of ACOSOG Z11 for Clinical
Page 1. AD vs. no AD. Survival. Randomized Trials. All trials reported higher survival in the AD group. Years. Node-NegativeNegative
 Sentinel Node Biopsy: The Past, The Present, and The Future Thomas B. Julian, M.D., F.A.C.S. Associate Professor of Human Oncology Drexel University College of Medicine Director of Breast Surgical Oncology
Sentinel Node Biopsy: The Past, The Present, and The Future Thomas B. Julian, M.D., F.A.C.S. Associate Professor of Human Oncology Drexel University College of Medicine Director of Breast Surgical Oncology
Sentinel Node Biopsy. Is There Any Role for Axillary Dissection? JCCNB Nov 20, Stephen B. Edge, MD
 Sentinel Node Biopsy Is There Any Role for Axillary Dissection? JCCNB Nov 20, 2010 Tokyo, Japan Stephen B. Edge, MD Roswell Park Cancer Institute University at Buffalo Buffalo, NY USA SNB with Clinically
Sentinel Node Biopsy Is There Any Role for Axillary Dissection? JCCNB Nov 20, 2010 Tokyo, Japan Stephen B. Edge, MD Roswell Park Cancer Institute University at Buffalo Buffalo, NY USA SNB with Clinically
Why Do Axillary Dissection? Nodal Treatment and Survival NSABP B04. Revisiting Axillary Dissection for SN Positive Patients
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA Why Do Axillary Dissection? 6 August 2011 Implications
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA Why Do Axillary Dissection? 6 August 2011 Implications
Updates on management of the axilla in breast cancer the surgical point of view
 Updates on management of the axilla in breast cancer the surgical point of view Edwige Bourstyn Centre des maladies du sein Hôpital Saint Louis Paris Sentinel lymph node biopsy (SLNB) is the standard of
Updates on management of the axilla in breast cancer the surgical point of view Edwige Bourstyn Centre des maladies du sein Hôpital Saint Louis Paris Sentinel lymph node biopsy (SLNB) is the standard of
Radiotherapy Implications of ACOSOG Z-11 for Clinical Practice. Julia White, MD Professor of Radiation Oncology Medical College of Wisconsin
 1 Radiotherapy Implications of ACOSOG Z-11 for Clinical Practice Julia White, MD Professor of Radiation Oncology Medical College of Wisconsin Disclosures: none Agenda 1. ACOSOG Z-11: Another perspective
1 Radiotherapy Implications of ACOSOG Z-11 for Clinical Practice Julia White, MD Professor of Radiation Oncology Medical College of Wisconsin Disclosures: none Agenda 1. ACOSOG Z-11: Another perspective
Recent Update in Surgery for the Management of Breast Cancer
 Recent Update in Surgery for the Management of Breast Cancer Wonshik Han, MD, PhD Professor, Department of Surgery, Seoul National University College of Medicine Chief of Breast Care Center, Seoul National
Recent Update in Surgery for the Management of Breast Cancer Wonshik Han, MD, PhD Professor, Department of Surgery, Seoul National University College of Medicine Chief of Breast Care Center, Seoul National
M D..,., M. M P.. P H., H, F. F A.. A C..S..
 Implications of NSABP B-32 and Loco-Regional Therapy Considerations After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H, F.A.C.S. Professor of Surgery Northeastern Ohio Medical University Medical
Implications of NSABP B-32 and Loco-Regional Therapy Considerations After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H, F.A.C.S. Professor of Surgery Northeastern Ohio Medical University Medical
Evaluating the Z011 study and how local-regional therapy for early breast cancer may change
 Evaluating the Z011 study and how local-regional therapy for early breast cancer may change Karen Hoffman, M.D., M.H.Sc., M.P.H. Dept of Radiation Oncology The University of Texas MD Anderson Cancer Center
Evaluating the Z011 study and how local-regional therapy for early breast cancer may change Karen Hoffman, M.D., M.H.Sc., M.P.H. Dept of Radiation Oncology The University of Texas MD Anderson Cancer Center
Breast Surgery When Less is More and More is Less. E MacIntosh, MD June 6, 2015
 Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Breast Surgery When Less is More and More is Less E MacIntosh, MD June 6, 2015 Presenter Disclosure Faculty: E. MacIntosh Relationships with commercial interests: None Mitigating Potential Bias Not applicable
Breast Cancer. Most common cancer among women in the US. 2nd leading cause of death in women. Mortality rates though have declined
 Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women Mortality rates though have declined 1 in 8 women will develop breast cancer Breast Cancer Breast cancer increases
Breast Cancer. Saima Saeed MD
 Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Breast Cancer Saima Saeed MD Breast Cancer Most common cancer among women in the US 2nd leading cause of death in women 1 in 8 women will develop breast cancer Incidence/mortality rates have declined Breast
Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy
 Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy Rebecca Warburton MD Department of Surgery, University of British Columbia Mount Saint Joseph Hospital, Providence Health Care
Surgical Considerations in Breast Cancer treated with Neoadjuvant Therapy Rebecca Warburton MD Department of Surgery, University of British Columbia Mount Saint Joseph Hospital, Providence Health Care
Surgical Therapy: Sentinel Node Biopsy and Breast Conservation
 Surgical Therapy: Sentinel Node Biopsy and Breast Conservation Stephen B. Edge, MD Professor of Surgery and Oncology Roswell Park Cancer Institute University at Buffalo Dr. Roswell Park: Tradition in Cancer
Surgical Therapy: Sentinel Node Biopsy and Breast Conservation Stephen B. Edge, MD Professor of Surgery and Oncology Roswell Park Cancer Institute University at Buffalo Dr. Roswell Park: Tradition in Cancer
Relevance. Axillary Node Recurrence. Purpose. Case Presentation: Is axillary staging required? Two trends have emerged:
 Axillary Node Recurrence N.L. Davis Associate Professor of Surgery, UBC Head of Surgical Oncology, BCCA Relevance In an attempt to minimize long term complications and to maximize cancer control, the management
Axillary Node Recurrence N.L. Davis Associate Professor of Surgery, UBC Head of Surgical Oncology, BCCA Relevance In an attempt to minimize long term complications and to maximize cancer control, the management
16/09/2015. ACOSOG Z011 changing practice. Presentation outline. Nodal mets #1 prognostic tool. Less surgery no change in oncologic outcomes
 ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
EDITORIAL. Ann Surg Oncol (2011) 18: DOI /s
 18: DOI /s") Ann Surg Oncol (2011) 18:2407 2412 DOI 10.1245/s10434-011-1593-7 EDITORIAL Multidisciplinary Considerations in the Implementation of the Findings from the American College of Surgeons Oncology Group (ACOSOG)
Ann Surg Oncol (2011) 18:2407 2412 DOI 10.1245/s10434-011-1593-7 EDITORIAL Multidisciplinary Considerations in the Implementation of the Findings from the American College of Surgeons Oncology Group (ACOSOG)
Evaluation of the Axilla Post Z-0011 Trial New Paradigm
 Evaluation of the Axilla Post Z-0011 Trial New Paradigm Belinda Curpen, MD, FRCPC; Tetyana Dushenkovska; Mia Skarpathiotakis MD, FRCPC; Carrie Betel, MD, FRCPC; Kalesha Hack, MD, FRCPC; Lara Richmond,
Evaluation of the Axilla Post Z-0011 Trial New Paradigm Belinda Curpen, MD, FRCPC; Tetyana Dushenkovska; Mia Skarpathiotakis MD, FRCPC; Carrie Betel, MD, FRCPC; Kalesha Hack, MD, FRCPC; Lara Richmond,
Evolution of Breast Surgery
 Evolution of Breast Surgery Natasha Rueth MD Surgical Oncologist Piper Breast Center and Alina Health Surgical Specialists Minneapolis, MN Definitions Radical Mastectomy: Removal of breast, chest muscles,
Evolution of Breast Surgery Natasha Rueth MD Surgical Oncologist Piper Breast Center and Alina Health Surgical Specialists Minneapolis, MN Definitions Radical Mastectomy: Removal of breast, chest muscles,
Sentinel Lymph Node Biopsy for Breast Cancer
 Sentinel Lymph Node Biopsy for Breast Cancer Registrar Tutorial Adam Cichowitz Surgical Registrar The Royal Melbourne Hospital Sentinel Lymph Node Biopsy Axillary LN status important prognostic factor
Sentinel Lymph Node Biopsy for Breast Cancer Registrar Tutorial Adam Cichowitz Surgical Registrar The Royal Melbourne Hospital Sentinel Lymph Node Biopsy Axillary LN status important prognostic factor
Evolution of Regional Nodal Management of Breast Cancer
 Evolution of Regional Nodal Management of Breast Cancer Bruce G. Haffty, MD Director (Interim) Rutgers Cancer Institute of New Jersey Professor and Chair Department of Radiation Oncology Rutgers, The State
Evolution of Regional Nodal Management of Breast Cancer Bruce G. Haffty, MD Director (Interim) Rutgers Cancer Institute of New Jersey Professor and Chair Department of Radiation Oncology Rutgers, The State
Savitri Krishnamurthy, MD 1
 EVOLVING TRENDS IN PATHOLOGIC EVALUATION OF AXILLARY LYMPH NODES IN BREAST CANCER Savitri Krishnamurthy, M.D. Professor Department of Pathology University of Texas M. D. Anderson Cancer Center AXILLARY
EVOLVING TRENDS IN PATHOLOGIC EVALUATION OF AXILLARY LYMPH NODES IN BREAST CANCER Savitri Krishnamurthy, M.D. Professor Department of Pathology University of Texas M. D. Anderson Cancer Center AXILLARY
Advances in Breast Surgery. Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015
 Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
Advances in Breast Surgery Catherine Campo, D.O. Breast Surgeon Meridian Health System April 17, 2015 Objectives Understand the surgical treatment of breast cancer Be able to determine when a lumpectomy
Surgical Issues in Neoadjuvant Chemotherapy
 14 th Bossche Mamma Congress Ruwenbergstraat 7 5271 AG Sint Michielsgestel June 14, 2016 Surgical Issues in Neoadjuvant Chemotherapy Tari A. King MD FACS Chief, Breast Surgery Dana Farber/Brigham and Women
14 th Bossche Mamma Congress Ruwenbergstraat 7 5271 AG Sint Michielsgestel June 14, 2016 Surgical Issues in Neoadjuvant Chemotherapy Tari A. King MD FACS Chief, Breast Surgery Dana Farber/Brigham and Women
Neoadjuvant Treatment of. of Radiotherapy
 Neoadjuvant Treatment of Breast Cancer: Role of Radiotherapy Neoadjuvant Chemotherapy Many new questions for radiation oncology? lack of path stage to guide indications should treatment response affect
Neoadjuvant Treatment of Breast Cancer: Role of Radiotherapy Neoadjuvant Chemotherapy Many new questions for radiation oncology? lack of path stage to guide indications should treatment response affect
Breast Cancer: Management of the Axilla in Greg McKinnon MD FRCSC SON Vancouver Oct 2016
 Breast Cancer: Management of the Axilla in 2016 Greg McKinnon MD FRCSC SON Vancouver Oct 2016 No Disclosures Principle #1 There is no point talking about surgical therapy in isolation. From a patient
Breast Cancer: Management of the Axilla in 2016 Greg McKinnon MD FRCSC SON Vancouver Oct 2016 No Disclosures Principle #1 There is no point talking about surgical therapy in isolation. From a patient
Targeting Surgery for Known Axillary Disease. Abigail Caudle, MD Henry Kuerer, MD PhD Dept. Surgical Oncology MD Anderson Cancer Center
 Targeting Surgery for Known Axillary Disease Abigail Caudle, MD Henry Kuerer, MD PhD Dept. Surgical Oncology MD Anderson Cancer Center Nodal Ultrasound at Diagnosis Whole breast and draining lymphatic
Targeting Surgery for Known Axillary Disease Abigail Caudle, MD Henry Kuerer, MD PhD Dept. Surgical Oncology MD Anderson Cancer Center Nodal Ultrasound at Diagnosis Whole breast and draining lymphatic
Breast Cancer. Dr. Andres Wiernik 2017
 Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Breast Cancer Dr. Andres Wiernik 2017 Agenda: The Facts! (Epidemiology/Risk Factors) Biological Classification/Phenotypes of Breast Cancer Treatment approach Local Systemic Agenda: The Facts! (Epidemiology/Risk
Ultrasound or FNA for Predicting Node Positive in Breast Cancer
 Ultrasound or FNA for Predicting Node Positive in Breast Cancer Chiun Sheng Huang, MD, PhD, MPH Professor and Chairman Department of Surgery Director of Breast Care Center National Taiwan University Hospital
Ultrasound or FNA for Predicting Node Positive in Breast Cancer Chiun Sheng Huang, MD, PhD, MPH Professor and Chairman Department of Surgery Director of Breast Care Center National Taiwan University Hospital
BREAST CANCER SURGERY. Dr. John H. Donohue
 Dr. John H. Donohue HISTORY References to breast surgery in ancient Egypt (ca 3000 BCE) Mastectomy described in numerous medieval texts Petit formulated organized approach in 18 th Century Improvements
Dr. John H. Donohue HISTORY References to breast surgery in ancient Egypt (ca 3000 BCE) Mastectomy described in numerous medieval texts Petit formulated organized approach in 18 th Century Improvements
EVALUATION OF AXILLARY LYMPH NODES AFTER NEOADJUVANT SYSTEMIC THERAPY KIM, MIN JUNG SEVERANCE HOSPITAL, YONSEI UNIVERSITY
 EVALUATION OF AXILLARY LYMPH NODES AFTER NEOADJUVANT SYSTEMIC THERAPY KIM, MIN JUNG SEVERANCE HOSPITAL, YONSEI UNIVERSITY AXILLARY LYMPH NODE METASTASIS Axillary lymph node metastasis is one of the most
EVALUATION OF AXILLARY LYMPH NODES AFTER NEOADJUVANT SYSTEMIC THERAPY KIM, MIN JUNG SEVERANCE HOSPITAL, YONSEI UNIVERSITY AXILLARY LYMPH NODE METASTASIS Axillary lymph node metastasis is one of the most
Resection Margins in Breast Conserving Surgery. Alberto Costa, MD Canton Ticino Breast Unit Lugano, Switzerland
 Resection Margins in Breast Conserving Surgery Alberto Costa, MD Canton Ticino Breast Unit Lugano, Switzerland Breast Conserving Surgery 1 Probably one of the most important innovation in cancer surgery
Resection Margins in Breast Conserving Surgery Alberto Costa, MD Canton Ticino Breast Unit Lugano, Switzerland Breast Conserving Surgery 1 Probably one of the most important innovation in cancer surgery
Management of the Axilla at Initial Surgery Manejo da Axila em Cirurgia Inicial
 DISCIPLINA DE MASTOLOGIA ESCOLA PAULISTA DE MEDICINA UNIVERSIDADE FEDERAL DE SÃO PAULO Management of the Axilla at Initial Surgery Manejo da Axila em Cirurgia Inicial Disciplina de Mastologia Prof. Dr.
DISCIPLINA DE MASTOLOGIA ESCOLA PAULISTA DE MEDICINA UNIVERSIDADE FEDERAL DE SÃO PAULO Management of the Axilla at Initial Surgery Manejo da Axila em Cirurgia Inicial Disciplina de Mastologia Prof. Dr.
Radiation Therapy for the Oncologist in Breast Cancer
 REVIEW ARTICLE Chonnam National University Medical School Sung-Ja Ahn, M.D. Adjuvant Tamoxifen with or without in Patients 70 Years of Age with Stage I ER-Positive Breast Cancer: Efficacy Outcomes (10
REVIEW ARTICLE Chonnam National University Medical School Sung-Ja Ahn, M.D. Adjuvant Tamoxifen with or without in Patients 70 Years of Age with Stage I ER-Positive Breast Cancer: Efficacy Outcomes (10
Surgical Advances in the Treatment of Breast Cancer. Laura Kruper, MD, MSCE Chief, Breast Surgery
 Surgical Advances in the Treatment of Breast Cancer Laura Kruper, MD, MSCE Chief, Breast Surgery Nothing to disclose DISCLOSURE LESS IS MORE Radiation Lymph nodes Reconstruction Less is More! Radiation
Surgical Advances in the Treatment of Breast Cancer Laura Kruper, MD, MSCE Chief, Breast Surgery Nothing to disclose DISCLOSURE LESS IS MORE Radiation Lymph nodes Reconstruction Less is More! Radiation
Page 1. AHN-JHU Breast Cancer Symposium. Novel Local Regional Clinical Trials. Background. Neoadjuvant Chemotherapy Benefit.
 AHN-JHU Breast Cancer Symposium Novel Local Regional Clinical Trials March 22, 2019 Thomas B. Julian, MD, FACS Associate Medical Director, Cancer Program Development, ANH Cancer Institute Background In
AHN-JHU Breast Cancer Symposium Novel Local Regional Clinical Trials March 22, 2019 Thomas B. Julian, MD, FACS Associate Medical Director, Cancer Program Development, ANH Cancer Institute Background In
A Predictive Tool to Estimate the Risk of Axillary Metastases in Breast Cancer Patients with Negative Axillary Ultrasound
 Ann Surg Oncol (2014) 21:2229 2236 DOI 10.1245/s10434-014-3617-6 ORIGINAL ARTICLE BREAST ONCOLOGY A Predictive Tool to Estimate the Risk of Axillary Metastases in Breast Cancer Patients with Negative Axillary
Ann Surg Oncol (2014) 21:2229 2236 DOI 10.1245/s10434-014-3617-6 ORIGINAL ARTICLE BREAST ONCOLOGY A Predictive Tool to Estimate the Risk of Axillary Metastases in Breast Cancer Patients with Negative Axillary
Principles of breast radiation therapy
 ANZ 1601/BIG 16-02 EXPERT ESMO Preceptorship Program 2017 Principles of breast radiation therapy Boon H Chua Professor Director of Cancer and Haematology Services UNSW Sydney and Prince of Wales Hospital
ANZ 1601/BIG 16-02 EXPERT ESMO Preceptorship Program 2017 Principles of breast radiation therapy Boon H Chua Professor Director of Cancer and Haematology Services UNSW Sydney and Prince of Wales Hospital
ACRIN 6666 Therapeutic Surgery Form
 S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
Recurrence following Treatment of Ductal Carcinoma in Situ with Skin-Sparing Mastectomy and Immediate Breast Reconstruction
 Recurrence following Treatment of Ductal Carcinoma in Situ with Skin-Sparing Mastectomy and Immediate Breast Reconstruction Aldona J. Spiegel, M.D., and Charles E. Butler, M.D. Houston, Texas Skin-sparing
Recurrence following Treatment of Ductal Carcinoma in Situ with Skin-Sparing Mastectomy and Immediate Breast Reconstruction Aldona J. Spiegel, M.D., and Charles E. Butler, M.D. Houston, Texas Skin-sparing
ANNEX 1 OBJECTIVES. At the completion of the training period, the fellow should be able to:
 1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
1 ANNEX 1 OBJECTIVES At the completion of the training period, the fellow should be able to: 1. Breast Surgery Evaluate and manage common benign and malignant breast conditions. Assess the indications
Is Complete Axillary Dissection Needed Following Mastectomy and Sentinel Node Biopsy for N1 disease?
 Is Complete Axillary Dissection Needed Following Mastectomy and Sentinel Node Biopsy for N1 disease? Mylin A. Torres, MD Director, Glenn Family Breast Center Louis and Rand Glenn Family Chair in Breast
Is Complete Axillary Dissection Needed Following Mastectomy and Sentinel Node Biopsy for N1 disease? Mylin A. Torres, MD Director, Glenn Family Breast Center Louis and Rand Glenn Family Chair in Breast
Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006
 Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006 Deborah Hamolsky MS, RN : DCIS Carol Franc Buck Breast Care Center UCSF Comprehensive Cancer Center Jane
Balancing Evidence and Clinical Practice in the Treatment of Localized Breast Cancer May 5, 2006 Deborah Hamolsky MS, RN : DCIS Carol Franc Buck Breast Care Center UCSF Comprehensive Cancer Center Jane
THE SURGEON S ROLE: THE AXILLA. Owen A Ung University of Queensland Royal Brisbane and Women s Hospital Wesley and St Andrews Hospital
 THE SURGEON S ROLE: THE AXILLA Owen A Ung University of Queensland Royal Brisbane and Women s Hospital Wesley and St Andrews Hospital What are the concerns with treatment to the axilla Not necessary for
THE SURGEON S ROLE: THE AXILLA Owen A Ung University of Queensland Royal Brisbane and Women s Hospital Wesley and St Andrews Hospital What are the concerns with treatment to the axilla Not necessary for
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy. Julia White MD Professor, Radiation Oncology
 Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Applicability of the ACOSOG Z0011 Criteria in Women with High-Risk Node-Positive Breast Cancer Undergoing Breast Conserving Surgery
 Ann Surg Oncol (2015) 22:1128 1132 DOI 10.1245/s10434-014-4090-y ORIGINAL ARTICLE BREAST ONCOLOGY Applicability of the ACOSOG Z0011 Criteria in Women with High-Risk Node-Positive Breast Cancer Undergoing
Ann Surg Oncol (2015) 22:1128 1132 DOI 10.1245/s10434-014-4090-y ORIGINAL ARTICLE BREAST ONCOLOGY Applicability of the ACOSOG Z0011 Criteria in Women with High-Risk Node-Positive Breast Cancer Undergoing
Practice of Axilla Surgery
 Summer School of Breast Disease 2016 Practice of Axilla Surgery Axillary Lymph Node Dissection & Sentinel Lymph Node Biopsy 연세의대외과 박세호 Contents Anatomy of the axilla Axillary lymph node dissection (ALND)
Summer School of Breast Disease 2016 Practice of Axilla Surgery Axillary Lymph Node Dissection & Sentinel Lymph Node Biopsy 연세의대외과 박세호 Contents Anatomy of the axilla Axillary lymph node dissection (ALND)
When do you need PET/CT or MRI in early breast cancer?
 When do you need PET/CT or MRI in early breast cancer? Elizabeth A. Morris MD FACR Chief, Breast Imaging Service Memorial Sloan-Kettering Cancer Center NY, NY Objectives What is the role of MRI in initial
When do you need PET/CT or MRI in early breast cancer? Elizabeth A. Morris MD FACR Chief, Breast Imaging Service Memorial Sloan-Kettering Cancer Center NY, NY Objectives What is the role of MRI in initial
Ductal Carcinoma in Situ (DCIS)
") Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Ductal Carcinoma in Situ (DCIS) Ductal Carcinoma in Situ DCIS Versions 2002 2017: Audretsch / Blohmer / Brunnert / Budach /
Diagnosis and Treatment of Patients with Primary and Metastatic Breast Cancer Ductal Carcinoma in Situ (DCIS) Ductal Carcinoma in Situ DCIS Versions 2002 2017: Audretsch / Blohmer / Brunnert / Budach /
Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer. Cheol Min Kang 2018/04/05
 Abstract No.: ABS-0075 Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer 2018/04/05 Cheol Min Kang Department of surgery, University of Ulsan
Abstract No.: ABS-0075 Clinicopathological Factors Affecting Distant Metastasis Following Loco-Regional Recurrence of breast cancer 2018/04/05 Cheol Min Kang Department of surgery, University of Ulsan
San Antonio Breast Cancer Symposium 2010: Highlights from a Surgical Perspective. Disclosures
 San Antonio Breast Cancer Symposium 2010: Highlights from a Surgical Perspective January 18, 2011 Association of Northern California Oncologists Steven Chen, MD, MBA Chief, Breast Surgery University of
San Antonio Breast Cancer Symposium 2010: Highlights from a Surgical Perspective January 18, 2011 Association of Northern California Oncologists Steven Chen, MD, MBA Chief, Breast Surgery University of
Post-Mastectomy RT after Neoadjuvant Chemotherapy (NAC)
") Post-Mastectomy RT after Neoadjuvant Chemotherapy (NAC) Jay R. Harris, M.D. Dana-Farber Cancer Institute Brigham and Women s Hospital Harvard Medical School Conclusions When considering PMRT, use both
Post-Mastectomy RT after Neoadjuvant Chemotherapy (NAC) Jay R. Harris, M.D. Dana-Farber Cancer Institute Brigham and Women s Hospital Harvard Medical School Conclusions When considering PMRT, use both
NSABP Pivotal Breast Cancer Clinical Trials: Historical Perspective, Recent Results and Future Directions
 1 1 NSABP Pivotal Breast Cancer Clinical Trials: Historical Perspective, Recent Results and Future Directions Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health
1 1 NSABP Pivotal Breast Cancer Clinical Trials: Historical Perspective, Recent Results and Future Directions Terry Mamounas, M.D., M.P.H., F.A.C.S. Medical Director, Comprehensive Breast Program UF Health
Use of the dye guided sentinel lymph node biopsy method alone for breast cancer metastasis to avoid unnecessary axillary lymph node dissection
 456 Use of the dye guided sentinel lymph node biopsy method alone for breast cancer metastasis to avoid unnecessary axillary lymph node dissection TOMOKO TAKAMARU 1, GORO KUTOMI 1, FUKINO SATOMI 1, HIROAKI
456 Use of the dye guided sentinel lymph node biopsy method alone for breast cancer metastasis to avoid unnecessary axillary lymph node dissection TOMOKO TAKAMARU 1, GORO KUTOMI 1, FUKINO SATOMI 1, HIROAKI
Sentinel Lymph Nodes for Breast Carcinoma: A Paradigm Shift. Edi Brogi MD PhD Attending Pathologist Director of Breast Pathology
 Sentinel Lymph Nodes for Breast Carcinoma: A Paradigm Shift Edi Brogi MD PhD Attending Pathologist Director of Breast Pathology Sentinel Lymph Nodes 2014 AJCC 2010 staging Micrometastases Occult metastases
Sentinel Lymph Nodes for Breast Carcinoma: A Paradigm Shift Edi Brogi MD PhD Attending Pathologist Director of Breast Pathology Sentinel Lymph Nodes 2014 AJCC 2010 staging Micrometastases Occult metastases
CURRENT CONTROVERSIES IN BREAST CANCER SURGERY Less or more!?
 CURRENT CONTROVERSIES IN BREAST CANCER SURGERY Less or more!? I have no Disclosures Wolfgang Gatzemeier Breast Unit Milan, Italy 17th ESO-ESMO- EONS Masterclass in Clinical Oncology 24-29 MARCH 2018 Optimal
CURRENT CONTROVERSIES IN BREAST CANCER SURGERY Less or more!? I have no Disclosures Wolfgang Gatzemeier Breast Unit Milan, Italy 17th ESO-ESMO- EONS Masterclass in Clinical Oncology 24-29 MARCH 2018 Optimal
Breast Cancer Earlier Disease. Stefan Aebi Luzerner Kantonsspital
 Breast Cancer Earlier Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Switzerland Breast Cancer Earlier Disease Diagnosis and Prognosis Local Therapy Surgery Radiation therapy Adjuvant
Breast Cancer Earlier Disease Stefan Aebi Luzerner Kantonsspital stefan.aebi@onkologie.ch Switzerland Breast Cancer Earlier Disease Diagnosis and Prognosis Local Therapy Surgery Radiation therapy Adjuvant
Feasibility of Preoperative Axillary Lymph Node Marking with a Clip in Breast Cancer Patients before Neoadjuvant Chemotherapy: A Preliminary Study
 [ABS-0078] GBCC 2018 Feasibility of Preoperative Axillary Lymph Node Marking with a Clip in Breast Cancer Patients before Neoadjuvant Chemotherapy: A Preliminary Study Eun Young Kim 1, Kwan Ho Lee 1, Yong
[ABS-0078] GBCC 2018 Feasibility of Preoperative Axillary Lymph Node Marking with a Clip in Breast Cancer Patients before Neoadjuvant Chemotherapy: A Preliminary Study Eun Young Kim 1, Kwan Ho Lee 1, Yong
Case Scenario 1 History and Physical 3/15/13 Imaging Pathology
 Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Case Scenario 1 History and Physical 3/15/13 The patient is an 84 year old white female who presented with an abnormal mammogram. The patient has a five year history of refractory anemia with ringed sideroblasts
Breast Surgery: Yesterday, Today and Tomorrow
 Breast Surgery: Yesterday, Today and Tomorrow Baptist Hospital Gladys L. Giron, MD, FACS October 11,2014 Homestead Hospital Baptist Children s Hospital Doctors Hospital Baptist Cardiac & Vascular Institute
Breast Surgery: Yesterday, Today and Tomorrow Baptist Hospital Gladys L. Giron, MD, FACS October 11,2014 Homestead Hospital Baptist Children s Hospital Doctors Hospital Baptist Cardiac & Vascular Institute
PMRT for N1 breast cancer :CONS. Won Park, M.D., Ph.D Department of Radiation Oncology Samsung Medical Center
 PMRT for N1 breast cancer :CONS Won Park, M.D., Ph.D Department of Radiation Oncology Samsung Medical Center DBCG 82 b & c Overgaard et al Radiot Oncol 2007 1152 pln(+), 8 or more nodes removed Systemic
PMRT for N1 breast cancer :CONS Won Park, M.D., Ph.D Department of Radiation Oncology Samsung Medical Center DBCG 82 b & c Overgaard et al Radiot Oncol 2007 1152 pln(+), 8 or more nodes removed Systemic
Post Neoadjuvant therapy: issues in interpretation
 Post Neoadjuvant therapy: issues in interpretation Disclosure: Overview D Prognostic features in assessment of post treatment specimens: Tumor size Cellularity Grade Receptors LN Neoadjuvant chemotherapy:
Post Neoadjuvant therapy: issues in interpretation Disclosure: Overview D Prognostic features in assessment of post treatment specimens: Tumor size Cellularity Grade Receptors LN Neoadjuvant chemotherapy:
Cryoablation in the Management of Early Stage Breast Cancer
 13 th Annual Pacific Northwest Breast and Gynecologic Care Conference Cryoablation in the Management of Early Stage Breast Cancer Dennis R. Holmes, M.D., Inc. Int. Director, Margie Peterson Breast Center
13 th Annual Pacific Northwest Breast and Gynecologic Care Conference Cryoablation in the Management of Early Stage Breast Cancer Dennis R. Holmes, M.D., Inc. Int. Director, Margie Peterson Breast Center
What the surgeon wants from the radiologist before breast cancer surgery. Erica Patocskai Isabelle Trop
 What the surgeon wants from the radiologist before breast cancer surgery Erica Patocskai Isabelle Trop Centre Hospitalier de l université de Montréal CAR, April 2013 Plan What is the role of MRI for breast
What the surgeon wants from the radiologist before breast cancer surgery Erica Patocskai Isabelle Trop Centre Hospitalier de l université de Montréal CAR, April 2013 Plan What is the role of MRI for breast
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO
 BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Medical Center Philadelphia, PA Professor (Adjunct)
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Medical Center Philadelphia, PA Professor (Adjunct)
Prediction of Lymph Node Involvement in Patients with Breast Tumors Measuring 3 5 cm in a Middle-Income Setting: the Role of CancerMath
 DOI 10.1007/s00268-014-2752-3 BRIEF ORIGINAL SCIENTIFIC REPORT Prediction of Lymph Node Involvement in Patients with Breast Tumors Measuring 3 5 cm in a Middle-Income Setting: the Role of CancerMath E.
DOI 10.1007/s00268-014-2752-3 BRIEF ORIGINAL SCIENTIFIC REPORT Prediction of Lymph Node Involvement in Patients with Breast Tumors Measuring 3 5 cm in a Middle-Income Setting: the Role of CancerMath E.
Ductal Carcinoma-in-Situ: New Concepts and Controversies
 Ductal Carcinoma-in-Situ: New Concepts and Controversies James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Ductal Carcinoma-in-Situ: New Concepts and Controversies James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS Case Presentation
Radiation and DCIS. The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging
 Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
Radiation and DCIS The 16 th Annual Conference on A Multidisciplinary Approach to Comprehensive Breast Care and Imaging Einsley-Marie Janowski, MD, PhD Assistant Professor Department of Radiation Oncology
The Challenge of Individualizing Loco-Regional Treatments for Patients with Localized Breast Cancer
 The Challenge of Individualizing Loco-Regional Treatments for Patients with Localized Breast Cancer Le défi des traitements locorégionaux individualisés pour les patientes présentant un cancer du sein
The Challenge of Individualizing Loco-Regional Treatments for Patients with Localized Breast Cancer Le défi des traitements locorégionaux individualisés pour les patientes présentant un cancer du sein
Controversies and Questions in the Surgical Treatment of Melanoma
 Controversies and Questions in the Surgical Treatment of Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Division of Endocrine and Oncologic Surgery University of Pennsylvania School
Controversies and Questions in the Surgical Treatment of Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Division of Endocrine and Oncologic Surgery University of Pennsylvania School
Breast Imaging: Multidisciplinary Approach. Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina
 Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
Breast Imaging: Multidisciplinary Approach Madelene Lewis, MD Assistant Professor Associate Program Director Medical University of South Carolina No Disclosures Objectives Discuss a multidisciplinary breast
Case Scenario 1. 2/15/2011 The patient received IMRT 45 Gy at 1.8 Gy per fraction for 25 fractions.
 Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Case Scenario 1 1/3/11 A 57 year old white female presents for her annual mammogram and is found to have a suspicious area of calcification, spread out over at least 4 centimeters. She is scheduled to
Advances in Localized Breast Cancer
 Advances in Localized Breast Cancer Melissa Camp, MD, MPH and Fariba Asrari, MD June 18, 2018 Moderated by Elissa Bantug 1 Advances in Surgery for Breast Cancer Melissa Camp, MD June 18, 2018 2 Historical
Advances in Localized Breast Cancer Melissa Camp, MD, MPH and Fariba Asrari, MD June 18, 2018 Moderated by Elissa Bantug 1 Advances in Surgery for Breast Cancer Melissa Camp, MD June 18, 2018 2 Historical
Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer
 Young Investigator Award, Global Breast Cancer Conference 2018 Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer ㅑ Running head: Revisiting estrogen positive tumors
Young Investigator Award, Global Breast Cancer Conference 2018 Only Estrogen receptor positive is not enough to predict the prognosis of breast cancer ㅑ Running head: Revisiting estrogen positive tumors
Surgical Management of the Axilla
 Surgical Management of the Axilla Jean-Francois Boileau, MD, MSc, FRCSC Surgical Oncologist, Montreal Jewish General Hospital Segal Cancer Centre Associate Member, Department of Oncology, McGill University
Surgical Management of the Axilla Jean-Francois Boileau, MD, MSc, FRCSC Surgical Oncologist, Montreal Jewish General Hospital Segal Cancer Centre Associate Member, Department of Oncology, McGill University
At many centers in the United States and worldwide,
 ORIGINAL ARTICLES A Declining Rate of Completion Axillary Dissection in Sentinel Lymph Node-positive Breast Cancer Patients Is Associated With the Use of a Multivariate Nomogram Julia Park, MS, Jane V.
ORIGINAL ARTICLES A Declining Rate of Completion Axillary Dissection in Sentinel Lymph Node-positive Breast Cancer Patients Is Associated With the Use of a Multivariate Nomogram Julia Park, MS, Jane V.
Indications and Technical Considerations for Adjuvant Radiation after Neoadjuvant Chemotherapy in Breast Cancer
 Indications and Technical Considerations for Adjuvant Radiation after Neoadjuvant Chemotherapy in Breast Cancer Wendy A. Woodward, M.D. Ph.D. A sociate Profesor Section Chief, Breast Radiation Oncology
Indications and Technical Considerations for Adjuvant Radiation after Neoadjuvant Chemotherapy in Breast Cancer Wendy A. Woodward, M.D. Ph.D. A sociate Profesor Section Chief, Breast Radiation Oncology
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO
 BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Healthcare Network Philadelphia, PA Professor
BREAST CONSERVATION TREATMENT IN EARLY STAGE DISEASE AND DCIS LAWRENCE J. SOLIN, MD, FACR, FASTRO Chairman Department of Radiation Oncology Albert Einstein Healthcare Network Philadelphia, PA Professor
Breast Cancer: Current Approaches to Diagnosis and Treatment
 Breast Cancer: Current Approaches to Diagnosis and Treatment Barbara L. Smith, MD, Ph.D. Massachusetts General Hospital Division of Surgical Oncology No Disclosures Incidence of Breast Cancer USA 2018
Breast Cancer: Current Approaches to Diagnosis and Treatment Barbara L. Smith, MD, Ph.D. Massachusetts General Hospital Division of Surgical Oncology No Disclosures Incidence of Breast Cancer USA 2018
Invasive Breast Cancer
 Invasive Breast Cancer Eileen Rakovitch MD MSc FRCPC Sunnybrook Health Sciences Centre Medical Director, Louise Temerty Breast Cancer Centre LC Campbell Chair in Breast Cancer Research Associate Professor,
Invasive Breast Cancer Eileen Rakovitch MD MSc FRCPC Sunnybrook Health Sciences Centre Medical Director, Louise Temerty Breast Cancer Centre LC Campbell Chair in Breast Cancer Research Associate Professor,
Abstract 80 DCIS Treated With Excision Alone Using the National Comprehensive Cancer Network (NCCN) Guidelines
 Guidelines") Media Tip Sheet Contact: Jeanne-Marie Phillips HealthFlash Marketing 203-363-0347 jphillips@healthflashmarketing.com Additional Notable Research and Presented at the 14 th Annual Meeting of the American
Media Tip Sheet Contact: Jeanne-Marie Phillips HealthFlash Marketing 203-363-0347 jphillips@healthflashmarketing.com Additional Notable Research and Presented at the 14 th Annual Meeting of the American
Surgical Issues in Melanoma
 Surgical Issues in Melanoma Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Director, Surgical Oncology Training Program Professor of Surgery John Wayne Cancer Institute Surgical
Surgical Issues in Melanoma Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Director, Surgical Oncology Training Program Professor of Surgery John Wayne Cancer Institute Surgical
Jose A Torres, MD 1/12/2017
 Jose A Torres, MD 1/12/2017 Background Globally leading cause of cancer related death in women ~249,000 Americans diagnosed with invasive breast cancer ~40,890 will die of their disease Breast cancer risk
Jose A Torres, MD 1/12/2017 Background Globally leading cause of cancer related death in women ~249,000 Americans diagnosed with invasive breast cancer ~40,890 will die of their disease Breast cancer risk
Should we still be performing IHC on all sentinel nodes?
 Miami Breast Cancer Conference 31 st Annual Conference March 8, 2014 Should we still be performing IHC on all sentinel nodes? Donald L. Weaver, MD Professor of Pathology University of Vermont USA Miami
Miami Breast Cancer Conference 31 st Annual Conference March 8, 2014 Should we still be performing IHC on all sentinel nodes? Donald L. Weaver, MD Professor of Pathology University of Vermont USA Miami
Clinical Outcome of Reconstruction With Tissue Expanders for Patients With Breast Cancer and Mastectomy
 Clinical Outcome of Reconstruction With Tissue Expanders for Patients With Breast Cancer and Mastectomy Mitsui Memorial Hospital Department of Breast and Endocine surgery Daisuke Ota No financial support
Clinical Outcome of Reconstruction With Tissue Expanders for Patients With Breast Cancer and Mastectomy Mitsui Memorial Hospital Department of Breast and Endocine surgery Daisuke Ota No financial support
Update on Sentinel Node Biopsy in Endometrial Cancer: Feasibility, Technique, Impact
 Update on Sentinel Node Biopsy in Endometrial Cancer: Feasibility, Technique, Impact Bjørn Hagen, MD, PhD St Olavs Hospital Trondheim University Hospital Trondheim, Norway Endometrial Cancer (EC) The most
Update on Sentinel Node Biopsy in Endometrial Cancer: Feasibility, Technique, Impact Bjørn Hagen, MD, PhD St Olavs Hospital Trondheim University Hospital Trondheim, Norway Endometrial Cancer (EC) The most
Financial Disclosure. Learning Objectives. None. To understand the clinical applicability of the NCDB Breast Cancer PUF
 Preoperative Prediction of Node Negative Disease After Neoadjuvant Chemotherapy in Patients Presenting with Node Negative or Node Positive Breast Cancer Brittany L Murphy MD, Tanya Hoskin MS, Courtney
Preoperative Prediction of Node Negative Disease After Neoadjuvant Chemotherapy in Patients Presenting with Node Negative or Node Positive Breast Cancer Brittany L Murphy MD, Tanya Hoskin MS, Courtney
Controversies in Breast Pathology ELENA PROVENZANO ADDENBROOKES HOSPITAL, CAMBRIDGE
 Controversies in Breast Pathology ELENA PROVENZANO ADDENBROOKES HOSPITAL, CAMBRIDGE Neoadjuvant Chemotherapy Indications: Management of locally advanced invasive breast cancers including inflammatory breast
Controversies in Breast Pathology ELENA PROVENZANO ADDENBROOKES HOSPITAL, CAMBRIDGE Neoadjuvant Chemotherapy Indications: Management of locally advanced invasive breast cancers including inflammatory breast
ALND. Dr. MJ Vrancken
 ALND Dr. MJ Vrancken ALND in primary surgery se1ng Axillary lymph node dissec8on (ALND) Very nice opera8on; dorsal approach 2 ALND in primary surgery se1ng Axillary lymph node dissec8on (ALND) Very nice
ALND Dr. MJ Vrancken ALND in primary surgery se1ng Axillary lymph node dissec8on (ALND) Very nice opera8on; dorsal approach 2 ALND in primary surgery se1ng Axillary lymph node dissec8on (ALND) Very nice
Case study 1. Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research
 NCCN/JCCNB Seminar in Japan April 15, 2012 Case study 1 Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research Present illness: A 50y.o.premenopausal
NCCN/JCCNB Seminar in Japan April 15, 2012 Case study 1 Rie Horii, M.D., Ph.D. Division of Pathology Cancer Institute Hospital, Japanese Foundation for Cancer Research Present illness: A 50y.o.premenopausal
Breast Imaging. Jamie L. Wagner, DO, FACOS. Digital vs Analog Mammography (2-D) Surgical Oncologist. Patient with Cancer. Radiology/ Interventional
 Surgical Oncologist. Patient with Cancer. Radiology/ Interventional") Breast Cancer Prevention, Treatment, and Survivorship Jamie L. Wagner, DO, FACOS Assistant Professor Chief, Division of Breast Surgery Department of Surgery Anesthesiology Surgical Oncologist Patient with
Breast Cancer Prevention, Treatment, and Survivorship Jamie L. Wagner, DO, FACOS Assistant Professor Chief, Division of Breast Surgery Department of Surgery Anesthesiology Surgical Oncologist Patient with
Update on SLN and Melanoma: DECOG and MSLT-II. Gordon H. Hafner, MD, FACS
 Update on SLN and Melanoma: DECOG and MSLT-II Gordon H. Hafner, MD, FACS No disclosures The surgery of malignant disease is not the surgery of organs, it is of the lymphatic system. Lord Moynihan Lymph
Update on SLN and Melanoma: DECOG and MSLT-II Gordon H. Hafner, MD, FACS No disclosures The surgery of malignant disease is not the surgery of organs, it is of the lymphatic system. Lord Moynihan Lymph
Sparing sentinel node biopsy through axillary lymph node fine needle aspiration in primary breast cancers
 Cheng et al. World Journal of Surgical Oncology 2013, 11:296 WORLD JOURNAL OF SURGICAL ONCOLOGY RESEARCH Sparing sentinel node biopsy through axillary lymph node fine needle aspiration in primary breast
Cheng et al. World Journal of Surgical Oncology 2013, 11:296 WORLD JOURNAL OF SURGICAL ONCOLOGY RESEARCH Sparing sentinel node biopsy through axillary lymph node fine needle aspiration in primary breast
Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective
 Procedure: An Oncologic Surgeon s Perspective") Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective Giorgos C. Karakousis, M.D. Associate Professor of Surgery Hospital of the University of Pennsylvania Disclosures
Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective Giorgos C. Karakousis, M.D. Associate Professor of Surgery Hospital of the University of Pennsylvania Disclosures
UK Interdisciplinary Breast Cancer Symposium. Should lobular phenotype be considered when deciding treatment? Michael J Kerin
 UK Interdisciplinary Breast Cancer Symposium Should lobular phenotype be considered when deciding treatment? Michael J Kerin Professor of Surgery National University of Ireland, Galway and Galway University
UK Interdisciplinary Breast Cancer Symposium Should lobular phenotype be considered when deciding treatment? Michael J Kerin Professor of Surgery National University of Ireland, Galway and Galway University