Diffuse Large B-cell Lymphoma: Is Cell of Origin Necessary for Treatment Selection?
|
|
|
- Clifton Scott
- 5 years ago
- Views:
Transcription



1 Diffuse Large B-cell Lymphoma: Is Cell of Origin Necessary for Treatment Selection? Andrew D. Zelenetz, MD, PhD Memorial Sloan Kettering Cancer Center NCCN.org For Clinicians NCCN.org/patients For Patients
2 WHO 2016: Diffuse Large B Cell Lymphoma is Multiples Diseases Diffuse large B cell lymphoma (DLBCL), NOS Germinal Center Cell of origin (COO) to Activated B Cell be determined by best Unclassified available means Tcell/histiocyte rich large B cell lymphoma Primary DLBCL of the CNS Primary cutaneous DLBCL, leg type EBV positive DLBCL, NOS EBV+ Mucocutaneous ulcer DLBCL associated with chronic inflammation Lymphomatoid granulomatosis Primary mediastinal (thymic) large B cell lymphoma Intravascular large B cell lymphoma ALK positive large B cell lymphoma Plasmablastic lymphoma Primary effusion lymphoma HHV8 positive DLBCL, NOS
3 Cell of Origin (COO) in DLBCL Contributes to Biological and Clinical Heterogeneity Coiffier, Blood 2010, 116: 2040; Alizadeh et al. Nature 2000; 403:503; Lenz et al., ASH annual meeting, 2007; Roschewski M et al. Nat Rev Clin Oncol :12


4 Cell of Origin (COO) in DLBCL Contributes to Biological and Clinical Heterogeneity Coiffier, Blood 2010, 116: 2040; Alizadeh et al. Nature 2000; 403:503; Lenz et al., ASH annual meeting, 2007; Roschewski M et al. Nat Rev Clin Oncol :12
5 Cell of Origin (COO) in DLBCL Contributes to Biological and Clinical Heterogeneity Coiffier, Blood 2010, 116: 2040; Alizadeh et al. Nature 2000; 403:503; Lenz et al., ASH annual meeting, 2007; Roschewski M et al. Nat Rev Clin Oncol :12





6 Cell of Origin (COO) in DLBCL Contributes to Biological and Clinical Heterogeneity Coiffier, Blood 2010, 116: 2040; Alizadeh et al. Nature 2000; 403:503; Lenz et al., ASH annual meeting, 2007; Roschewski M et al. Nat Rev Clin Oncol :12

7


8 COO is not the whole story: Increased complexity revealed by targeted sequencing in DLBCL Intlekofer et al, Blood :704 Copyright 2016, National Comprehensive Cancer Network. All rights reserved. No part of this publication may be reproduced or transmitted in any other form or by any means, electronic or mechanical, without first obtaining written permission from NCCN.
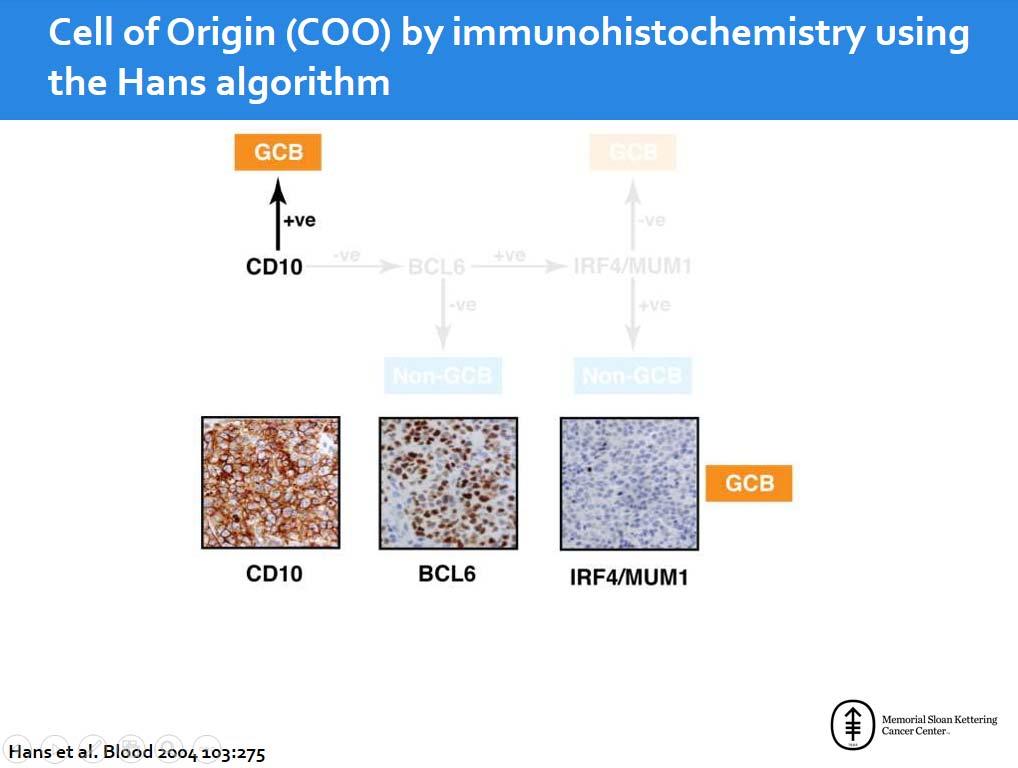
9 Determining COO in DLBCL

 Basis for subsequent classifiers Wright et al. Proc. Natl. Acad. Sci.")
10 Wright Classifier enables patient level assignment of COO Wright classifier: statistical method based on Bayes' rule that estimates the probability of membership in one of two cancer subgroups Included 27 genes which separated patients into: GCB, ABC or Type 3 (now referred to as unclassifiable) Basis for subsequent classifiers Wright et al. Proc. Natl. Acad. Sci. USA :9991
11 Methods for determination of COO Gene Expression Profiling (GEP) on fresh tissue The gold standard Needs the Wright classifier to make patient level assignment to ABC, GCB or unclassifiable Not practically applicable in clinical practice Immunohistochemistry Widely available Reproducibility may be difficult Many assays (Hans, Choi, Muris) Lack of correlation with GEP in many studies GEP of formalin fixed paraffin embedded (FFPE) tissue Multiple platforms Hybrid capture/fluorescent reporter emerging as a widely validated assay
12
13

14

15

16

17

18

19

20

21

22
23 Is Cell of Origin Prognostic?
24 Prognostic value of Lymph2Cx assay Population registry based analysis of patients with de novo DLBCL treated with R CHOP; n=344, 5 excluded for low tumor content 339 analyzed Lymph2Cx assay permitted assigning COO 335/339 (99%) cases ABC: 32% (108 of 335); GCB 56% (189 of 335); Unclassified 11% (38 of 335) Scott et al. J Clin Oncol :2848
25 GEP on FFPE tissue does not universally show a prognostic difference RICOVER60: Retrospective application of Lymph2Cx REMoDL B: Prospective COO by Illumina DASL array Progression-Free Survival 1.0 GCB ABC p= GCB ABC 0.8 Technical Fail(n=29) R CHOP x5 (n=159) Trial Registration R CHOP Cycle 1 Molecular phenotype result received from HMDS and randomised Screen Fail (n=130) ABC (n=248) Randomisation R CHOP x5 (n=364) GCB (n=477) RB CHOP x5 (n=361) Target population Unclassifiable (n=201) Randomisation R CHOP x5 (n=99) RB CHOP x5 (n=102) Overall Survival p= Pfreunschuh, personal communication; Davies, ASH 2015
26 Can chemotherapy influence outcome by COO?
27 Dose Adjusted (DA) EPOCH R Drug Rituximab Doxorubicin Vincristine Etoposide Cyclophosphamide Prednisone Filgrastim* Dose 375 mg/m 2 day 1 IVPB 10 mg/m 2 /day x4 by CI 0.4 mg/m 2 /day x 4 by CI 50 mg/m 2 /day x 4 by CI 750 mg/m 2 day 5 IVBP 60 mg/m 2 BID days 1 5 oral Weight adjusted dose starting day 5 until ANC > 5000/μL *Recent data from MSKCC showed identical rate of dose adjustment with filgrastim or pegfilgrastim Dosed every 21 days if ANC > 1/μLand PLTS > 100KμL Dose adjusted based on ANC nadir: >500/μL, increase cytotoxic drugs by 20% <500/μLfor 1 3 days, no change <500/μLfor >3 days or FN, decrease cytotoxic drugs by 20% Wilson, J Clin Oncol : ; Lunning et al. SHO, abstract
28 CALGB 59910: Multi center DA EPOCH R, Outcomes Testable hypothesis: DA EPOCH R is particularly favorable for GCB DLBCL Wilson W H et al. Haematologica 2012;97:
29 CALGB 50303: DA EPOCH R vs RCHOP21 De Novo DLBCL No discordant disease CS IIX IV R A N D O M I Z E DA EPOCH R R CHOP n= 478 patients (239 per treatment arm) OBJECTIVES: Primary EFS untreated de novo DLBCL treated with RCHOP vs DA R EPOCH Determine molecular predictors of outcome (using molecular profiling) in patients treated with these regimens. Secondary Compare ORR and OS Compare the toxicity of these regimens in these patients. Correlate the clinical parameters (i.e., toxicity, response, survival outcomes, and laboratory results) with molecular profiling in patients treated with these regimens. Determine the use of molecular profiling for pathological diagnosis Data to be presented at ASH 2016


30 Sequential Non cross resistant chemotherapy

31 MSKCC /08 146: DLBCL Risk Adapted for Therapy CS IIX, III or IV disease, age adjusted IPI 1, 2, or 3 Risk Factors, Transplant Eligible Repeat Bx R C 1000 HO uncapped P 14 x 4 + PET Bx + Bx CS IIX, III or IV disease, age-adjusted IPI 1, 2, or 3 Risk Factors, Transplant Eligible Repeat Bx R R C 1000 HO uncapped P 14 x3 C 1000 HO uncapped P 21 x 1 + PET Bx + Bx 80% Ki 67 < 80% ICE X 2 RICE x 1 followed by HDT/ASCT ICE X 3 followed by Observation Augmented RICE x 2 followed by HDT/ASCT Augmented RICE x 2 followed by Observation ICE X 3 followed by Observation Prospective, biopsy controlled determination of positive PET Treatment is adapted by biopsy, not PET No radiation therapy permitted except for testicular disease IT methotrexate for aahr, paranasal sinus, testis, BM Two studies with highly similar outcomes, combined analysis
32 Sequential R-CHOP ICE: Overall and Progression-Free Survival by COO
33 Sequential R-CHOP ICE: Overall and Progression-Free Survival by COO COO by IHC [Hans] Testable hypothesis: Sequential R CHOP ICE is particularly favorable for ABC DLBCL
34 LNH03 2B: R ACVBP v R CHOP Patients: Untreated DLBCL, age 18 59, aaipi score =1 (high LDH, stage III/IV, ECOG PS >1) MTX R IFM VP16 Ara C R ACVBP 14 R Wks 4 IT MTX Wks R CHOP 21 *No radiotherapy in both arms Recher et al. Lancet :

35 LNH03 2B: Influence of Cell of Origin Molina et al. J Clin Oncol :3996


36 LNH03 2B: Influence of Cell of Origin Molina et al. J Clin Oncol :3996

37
38 Comparison of R CHOP/ICE and ACVBP with Consolidation R CHOP/ICE Drug (cytotoxic) DI mg/m 2 / week Total mg/m 2 Rituximab Doxorubicin Cyclophosphamide ACVBP + Consolidation Drug (cytotoxic) DI mg/m 2 / week Total mg/m 2 Rituximab Doxorubicin Cyclophosphamide Vindesine 1 8 Vincristine Bleomycin *10 *80 Prednisone *250 *2000 Prednisone Methotrexate Ifosfamide Ifosfamide Etoposide Etoposide Carboplatin **2.5 **15 *FLAT dosing **Dose as AUC Cytarabine Recher et al. Lancet : , Moskowtiz et al J. Clin. Oncol :
39 New Agents in DLBCL
 4 (23.5) SD 7 (17.5) 7 (30.4) 0 PD 21 (52.5) 14 (60.9) 7 (41.2) Unknown 1 (2.5) 0 1 (5.9) ORR (CR + PR) 11 (27.5) 2 (8.7) 9 (52.9) PFS, mo Median 2.6 1.7 6.2 95% CI 0.9 4.2 0.3 3.1 2.9 9.")
40 Lenalidomide for DLBCL: Impact of Cell of Origin All GCB Non GCB CD10 BCL6 Lenalidomide cycles Median (Range) 2 (1 35) 2 (1 21) 4 (1 35) Response CR 6 (15.0) 1 (4.3) 5 (29.4) PR 5 (12.5) 1 (4.3) 4 (23.5) SD 7 (17.5) 7 (30.4) 0 PD 21 (52.5) 14 (60.9) 7 (41.2) Unknown 1 (2.5) 0 1 (5.9) ORR (CR + PR) 11 (27.5) 2 (8.7) 9 (52.9) PFS, mo Median % CI IRF4 Hernandez Ilizaliturri et al, Cancer :5058
41 Frontline R CHOP + Lenalidomide (RL CHOP) in DLBCL or FL: Phase II Study Designs Untreated DLBCL (or FL, gr 3 Mayo only) R CHOP + Lenalidomide Response was evaluated using PET/CT by standard criteria Two trials with slightly different dose schedules of lenalidomide Compared with historical R CHOP control (with similar baseline characteristics) Chiappella et al. ASH 2012, Abstract 903; Nowakowski et al. ASH 2012, Abstract 689.
42 Italian Series: Lenalidomide + R-CHOP21 in Elderly Untreated DLBCL: Efficacy Response n (%) ORR 45 (92) CR 42 (86) PR 3 (6) SD 0 PD 3 (6) Median follow up: 22 months 2 year OS = 92% 2 year PFS = 73% overall 84% IPI LI 65% IPI IH/H 81% 71% 74% 61% 2 yrs PFS GC: 71% (95% CI: 40 88) 2 yrs PFS non GC: 81% (95% CI: 51 93) p yrs EFS GC: 61% (95% CI: 33 80) 2 yrs EFS non GC: 74% (95% CI: 45 90) p Chiappella et al. ASH 2012, Abstract 903.
43 RL CHOP vs R CHOP Control Patients Characteristics Characteristic R2CHOP RCHOP (N=64) (N=87) p value Age 0.01 Median (range) 65 (22 87) 61 (41 86) Gender 0.53 Male 40 (62.5%) 50 (57.5%) IPI 0.05 Low 7 (10.9%) 18 (20.7%) Low Intermed. 24 (37.5%) 16 (18.4%) High Intermed. 24 (37.5%) 38 (43.7%) High 9 (14.1%) 15 (17.2%) Ann Arbor Stage (10.9%) 20(23.0%) 3 19 (29.7%) 14 (16.1%) 4 38 (59.4%) 53 (60.9%) ECOG PS (46.9%) 32(36.8%) 1 28 (43.8%) 41 (47.1%) 2 6 (9.4%) 11 (12.6%) 3 0(0.0%) 3(3.4%) 87 DLBCL consecutive contemporary patients treated with RCHOP Identified in MCR lymphoma database Same eligibility: stage 2 4 disease No major differences in clinical characteristics Nowakowski et al. ASH 2012, ASCO 2014
44 Mayo Series: Outcomes for RL CHOP v R CHOP Case Match Control by Cell of Origin Non GC DLBCL GC DLBCL Nowakowski et al. ASH 2012, ASCO 2014

45 E1412: RL-CHOP vs. R-CHOP R-CHOP N=100 evaluable pts DLBCL R 1:1 Stratification Age IPI 10% path ineligibility rate total ~220 pts# RL-CHOP N=100 evaluable pts # up to 300 patients can be enrolled to meet a goal of 50 ABC DLBCL patients per arm as defined by GEP
46 ROBUST (NCT ): Lenalidomide Plus R CHOP Chemotherapy (R2 CHOP) Versus Placebo Plus R CHOP Chemotherapy in Subjects With Untreated ABC DLBCL, Phase 3, double blind, placebo controlled Inclusion DLBCL, ABC type, untreated COO by Lymph2Cx Measurable disease by CT/MRI ECOG 0 2 Age IPI 2 Exclusion Lymphoma other than DLBCL HIV, HBV, HCV active infections LVEF <45% Peripheral neuropathy, grade 2 Other malignancies < 5 years disease free Sample Size/Statistical Plan Sample size: % to detect increase in PFS of 60% Double blind, placebo controlled Randomization 1:1 Placebo + R CHOP 4 Lenalidomide + R CHOP 4 Study Start Date: January 2015 Estimated Study Completion Date: September 2022 Estimated Primary Completion Date: June 2018 Evaluation Interim evaluation after cycle 4 EOT (6 cycles) FDG PET Interim Evaluation NR off study Placebo + R CHOP 2 Lenalidomide + R CHOP 2 Clinical Endpoints EOT Evaluation IWG 2007 with Deauville PET Primary: Progression free survival Secondary: OS, CRR, Duration of CR, TTNT, ORR, QOL
 GCB (N = 12) Unclassifiable (N = 8) Unknown (N = 3) Only includes pts with post")
47 Ibrutinib in Rel/Ref DLBCL: Phase II Eligibility (N = 70) Relapsed/refractory de novo DLBCL Progressive disease (PD) after ASCT or ineligible for ASCT Archival tissue for central review No primary mediastinal DLBCL, transformed DLBCL or CNS involvement Ibrutinib: 560 mg/d, PO % Change from Baseline SPD ABC (N = 23) GCB (N = 12) Unclassifiable (N = 8) Unknown (N = 3) Only includes pts with post baseline LN measurements *Best response was PD due to clinical progression Wilson WH et al. Proc ASH 2012;Abstract 686.
48 Ibrutinib in Rel/Ref ABC subtype DLBCL: Conclusions Ibrutinib showed a clinically meaningful response rate in relapsed/refractory ABC DLBCL, but not in other molecular subtypes ORR: 23% all patients, 41% ABC (17% CR), 5% GCB (all PR) Responses by mutational status Did not require CD79b mutation But were better if mutated MYD88 mutations seemed to cause resistance Unless associated with CD79b mutation CARD11 mutation did not respond Expected result since BTK is upstream of CARD11 Results were consistent with an essential role of BCR signaling in ABC DLBCL Future clinical trials of ibrutinib in DLBCL should screen for DLBCL subtype Wilson et al. ASH 2012, Abstract 686.
49 R CHOP + Ibrutinib: Phase 1b Schema PART 1: Newly diagnosed: FL, MCL, DLBCL PART 2: DLBCL only R CHOP+Ibrutinib 3 dosing cohorts: 280 mg 420 mg 560 mg R CHOP+Ibrutinib 560 mg R CHOP x 6 cycles maximum; Ibrutinib dosed from daily starting day 3 Dose reductions; 4 patients required dose reduction of ibrutinib Febrile neutropenia (FN) G3 (N=2) Diarrhea G3 (N=1) Prolonged bleed time (N=1) 2 patients required dose reduction of doxorubicin due to FN 7 patients required dose reduction of vincristine with the majority in cycle 4/5 Efficacy (N=22) ORR 100%: CR 91%, PR 9% Non GC DLBCL: CR 4/4 GC DLBCL: CR 12/14, PCR 2/14 Not assigned: CR 4/4 Younes et al. ASH 2013, Abstract 852
50 PHEONIX (NCT ): Ibrutinib in Combination With R CHOP in Subjects With Newly Diagnosed Non Germinal Center Diffuse Large B Cell Lymphoma, Phase 3, double blind, placebo controlled Inclusion DLBCL, non GC, untreated Stage II (not candidates for RT), III, IV 1 measurable site R IPI 1 ECOG 0 2 LVEF WNL Exclusion Major surgery within 4 weeks CNS disease Prior indolent lymphoma Warfarin Concomitant CYP3A inhibitors Sample Size/Statistical Plan Sample size: 800 Study completion: 50% deaths or 7 years ACCURAL COMPLETE Interim analysis after 270 EFS events Cure 40 to 50%; HR for uncured 0.75 Double blind, placebo controlled Randomization 1:1 Arm A: placebo + R CHOP 4 Arm B: ibrutinib + R CHOP 4 Study Start Date: September 2013 Estimated Study Completion Date: June 2020 Estimated Primary Completion Date: June 2018 Evaluation Interim evaluation after cycle 4 EOT (6 8 cycles) FDG PET Stratifications RIPI 1 2 v 3 5 US v Rest of World 6 v 8 cycles Interim Evaluation NR off study Arm A: placebo + R CHOP 2 4 Arm B: ibrutinib + R CHOP 2 4 EOT Evaluation Lugano Revised Criteria Clinical Endpoints Primary: Event free survival Secondary: PFS, OS, CRR, QOL, ibrutinib: clearance, volume of distribution, AUC, minimal concentration, AEs
51 Cell of origin in DLBCL Cell of origin identifies tumors with distinct biology Determination of cell of origin by IHC is inexact, GEP of FFPE is superior and emerging as a clinical assay Prognostic significance of COO still controversial Retrospective studies consistently demonstrate GCB with better outcomes than ABC Prospective studies have not always confirmed this? Accrual biases? Treatments appear to be influenced by cell of origin Lenalidomide and ibrutinib have activity in ABC DLBCL explained by underlying biology Somatic mutations, chromosomal amplification and loss, epigenetic changes, and expression of particular genes (MYC, BCL2 and BCL6) also influence outcome COO is an important consideration but is not the only factor that influences treatment and outcome
52 Lymphoma Disease Management Team Lymphoma Service John Gerecitano Paul Hamlin Steve Horwitz Matt Matasar Alison Moskowitz Craig Moskowitz Ariela Noy Lia Palomba Carol Portlock Jonathan Schatz David Straus AnasYounes, Chief Andrew Zelenetz Nuclear Medicine Heiko Schoder Neetha Pandit Tasker Jorge Carasquillo Radiology James Caravelli Jurgen Rademaker Gary Ulaner Radiation Oncology Joachim Yahalom Lymphoma Transplant Program Matt Matasar Craig Sauter Craig Moskowitz Juliet Barker Jenna Goldberg Miguel Perales Sergio Giralt Hematopathology Ahmet Dogan Maria Arcila April Chiu Oscar Lin Chris Park David Park Filiz Sen

53 NCCN Member Institutions
What are the hurdles to using cell of origin in classification to treat DLBCL?
 What are the hurdles to using cell of origin in classification to treat DLBCL? John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical
What are the hurdles to using cell of origin in classification to treat DLBCL? John P. Leonard, M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical
Have we moved beyond EPOCH for B-cell non-hodgkin lymphoma? YES!
 Have we moved beyond EPOCH for B-cell non-hodgkin lymphoma? YES! Christopher Flowers, MD, MSc Associate Professor Director, Lymphoma Program Department of Hematology and Oncology Emory School of Medicine
Have we moved beyond EPOCH for B-cell non-hodgkin lymphoma? YES! Christopher Flowers, MD, MSc Associate Professor Director, Lymphoma Program Department of Hematology and Oncology Emory School of Medicine
Aggressive lymphomas ASH Dr. A. Van Hoof A.Z. St.Jan, Brugge-Oostende AV
 Aggressive lymphomas ASH 2015 Dr. A. Van Hoof A.Z. St.Jan, Brugge-Oostende AV CHOP 1992 2002 R-CHOP For DLBCL High dose chemo With PBSCT Aggressive lymphomas 1.DLBCL 2.Primary Mediastinal Lymphoma 3.CNS
Aggressive lymphomas ASH 2015 Dr. A. Van Hoof A.Z. St.Jan, Brugge-Oostende AV CHOP 1992 2002 R-CHOP For DLBCL High dose chemo With PBSCT Aggressive lymphomas 1.DLBCL 2.Primary Mediastinal Lymphoma 3.CNS
Mantle Cell Lymphoma New scenario and concepts in front-line treatment for young pa:ents
 Mantle Cell Lymphoma New scenario and concepts in front-line treatment for young pa:ents Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Ke=ering Cancer Center Friday March 16, 2018: 11:15-11:30
Mantle Cell Lymphoma New scenario and concepts in front-line treatment for young pa:ents Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Ke=ering Cancer Center Friday March 16, 2018: 11:15-11:30
Diffuse Large B-Cell Lymphoma Front line Therapy John P. Leonard, MD Weill Cornell Medicine New York, New York USA
 Diffuse Large B-Cell Lymphoma Front line Therapy John P. Leonard, MD Weill Cornell Medicine New York, New York USA Disclosures Consulting advice: Hospira, Bayer, Juno Therapeutics, Teva, Oncotracker, Gilead
Diffuse Large B-Cell Lymphoma Front line Therapy John P. Leonard, MD Weill Cornell Medicine New York, New York USA Disclosures Consulting advice: Hospira, Bayer, Juno Therapeutics, Teva, Oncotracker, Gilead
ACCME/Disclosures. DLBCL, NOS from the clinician perspective. Diffuse large B cell lymphoma
 , NOS from the clinician perspective John P. Leonard, M.D. Weill Cornell Medicine New York Presbyterian Hospital ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the
, NOS from the clinician perspective John P. Leonard, M.D. Weill Cornell Medicine New York Presbyterian Hospital ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the
Treatment Landscape in R/R DLBCL Novel Targets and Strategies. Wyndham H. Wilson, M.D., Ph.D. Senior Investigator
 Treatment Landscape in R/R DLBCL Novel Targets and Strategies Wyndham H. Wilson, M.D., Ph.D. Senior Investigator Gene-expression profiling of DLBCL subtypes Roschewski, M. et al. (2013) Nat. Rev. Clin.
Treatment Landscape in R/R DLBCL Novel Targets and Strategies Wyndham H. Wilson, M.D., Ph.D. Senior Investigator Gene-expression profiling of DLBCL subtypes Roschewski, M. et al. (2013) Nat. Rev. Clin.
Aggressive B-cell lymphomas and gene expression profiling towards individualized therapy?
 Aggressive B-cell lymphomas and gene expression profiling towards individualized therapy? Andreas Rosenwald Institute of Pathology, University of Würzburg, Germany Barcelona, June 18, 2010 NEW WHO CLASSIFICATION
Aggressive B-cell lymphomas and gene expression profiling towards individualized therapy? Andreas Rosenwald Institute of Pathology, University of Würzburg, Germany Barcelona, June 18, 2010 NEW WHO CLASSIFICATION
Aggressive B and T cell lymphomas: Treatment paradigms in 2018
 Aggressive B and T cell lymphomas: Treatment paradigms in 2018 John P. Leonard M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical Research Associate
Aggressive B and T cell lymphomas: Treatment paradigms in 2018 John P. Leonard M.D. Richard T. Silver Distinguished Professor of Hematology and Medical Oncology Associate Dean for Clinical Research Associate
Lymphoma update: turning biology into cures. Peter Johnson
 Lymphoma update: turning biology into cures Peter Johnson Selected highlights of recent research 1. Using FDG-PET to modify treatment and avoid long term toxicity in Hodgkin lymphoma 2. Understanding how
Lymphoma update: turning biology into cures Peter Johnson Selected highlights of recent research 1. Using FDG-PET to modify treatment and avoid long term toxicity in Hodgkin lymphoma 2. Understanding how
The treatment of DLBCL. Michele Ghielmini Medical Oncology Dept Oncology Institute of Southern Switzerland Bellinzona
 The treatment of DLBCL Michele Ghielmini Medical Oncology Dept Oncology Institute of Southern Switzerland Bellinzona NHL frequency at the IOSI Mantle Cell Lymphoma 6.5 % Diffuse Large B-cell Lymphoma 37%
The treatment of DLBCL Michele Ghielmini Medical Oncology Dept Oncology Institute of Southern Switzerland Bellinzona NHL frequency at the IOSI Mantle Cell Lymphoma 6.5 % Diffuse Large B-cell Lymphoma 37%
NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary)
") NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and
NON HODGKINS LYMPHOMA: AGGRESSIVE Updated June 2015 by Dr. Manna (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Michelle Geddes (Staff Hematologist, University of Calgary) and
Radiotherapy in DLCL is often worthwhile. Dr. Joachim Yahalom Memorial Sloan-Kettering, New York
 Radiotherapy in DLCL is often worthwhile Dr. Joachim Yahalom Memorial Sloan-Kettering, New York The case for radiotherapy Past: Pre-Rituximab randomized trials Present: R-CHOP as backbone, retrospective
Radiotherapy in DLCL is often worthwhile Dr. Joachim Yahalom Memorial Sloan-Kettering, New York The case for radiotherapy Past: Pre-Rituximab randomized trials Present: R-CHOP as backbone, retrospective
What is the best second-line approach to induce remission prior to stem cell transplant? Single agent brentuximab vedotin
 What is the best second-line approach to induce remission prior to stem cell transplant? Single agent brentuximab vedotin Alison Moskowitz, MD Assistant Attending, Lymphoma Service Memorial Sloan Kettering
What is the best second-line approach to induce remission prior to stem cell transplant? Single agent brentuximab vedotin Alison Moskowitz, MD Assistant Attending, Lymphoma Service Memorial Sloan Kettering
Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009
 Treatment of DLBCL Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009 Non-hodgkin lymphomas DLBCL Most common NHL subtype throughout the world many other types of lymphoma with striking geographic variations
Treatment of DLBCL Dr. Nicolas Ketterer CHUV, Lausanne SAMO, May 2009 Non-hodgkin lymphomas DLBCL Most common NHL subtype throughout the world many other types of lymphoma with striking geographic variations
Conflict of Interest Disclosure Form NAME :James O. Armitage, M.D AFFILIATION: University of Nebraska Medical Center
 What Is Personalized Medicine For Patients With Lymphoma? Conflict of Interest Disclosure Form NAME :James O. Armitage, M.D AFFILIATION: University of Nebraska Medical Center DISCLOSURE I have no potential
What Is Personalized Medicine For Patients With Lymphoma? Conflict of Interest Disclosure Form NAME :James O. Armitage, M.D AFFILIATION: University of Nebraska Medical Center DISCLOSURE I have no potential
ESMO DOUBLE-HIT LYMPHOMAS
 ESMO DOUBLE-HIT LYMPHOMAS Professor Dr. med. Georg Lenz Director Department of Hematology and Oncology Universitätsklinikum Münster, Germany OVERVIEW Definition of double-hit lymphomas Introduction in
ESMO DOUBLE-HIT LYMPHOMAS Professor Dr. med. Georg Lenz Director Department of Hematology and Oncology Universitätsklinikum Münster, Germany OVERVIEW Definition of double-hit lymphomas Introduction in
Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge. ASH 2012 Atlanta
 Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge ASH 2012 Atlanta DLBCL How to improve on R-CHOP What at relapse Mantle cell lymphoma Do we cure patients Treatment at relapse Follicular lymphoma Watch and
Dr. A. Van Hoof Hematology A.Z. St.Jan, Brugge ASH 2012 Atlanta DLBCL How to improve on R-CHOP What at relapse Mantle cell lymphoma Do we cure patients Treatment at relapse Follicular lymphoma Watch and
Genomics in diffuse large B cell lymphoma (DLBCL) not as useful as we thought. OR IS IT?
 not as useful as we thought. OR IS IT?") Genomics in diffuse large B cell lymphoma (DLBCL) not as useful as we thought. OR IS IT? Matt McKinney MD Instructor in Medicine, Division of Hematologic Malignancies, Department of Medicine Duke University
Genomics in diffuse large B cell lymphoma (DLBCL) not as useful as we thought. OR IS IT? Matt McKinney MD Instructor in Medicine, Division of Hematologic Malignancies, Department of Medicine Duke University
Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL
 New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
New Evidence reports on presentations given at ASH 2009 Strategies for the Treatment of Elderly DLBCL Patients, New Combination Therapy in NHL, and Maintenance Rituximab Therapy in FL From ASH 2009: Non-Hodgkin
Standard of care for patients with newly diagnosed multiple myeloma who are not eligible for a transplant
 Standard of care for patients with newly diagnosed multiple myeloma who are not eligible for a transplant Pr Philippe Moreau University Hospital, Nantes, France MP: Standard of care until 2007 J Clin Oncol
Standard of care for patients with newly diagnosed multiple myeloma who are not eligible for a transplant Pr Philippe Moreau University Hospital, Nantes, France MP: Standard of care until 2007 J Clin Oncol
Treating for Cure or Palliation: Difficult Decisions for Older Adults with Lymphoma
 Treating Frail Adults With Common Malignancies: Best Evidence to Personalize Therapy Treating for Cure or Palliation: Difficult Decisions for Older Adults with Lymphoma Raul Cordoba, MD, PhD Lymphoma Unit
Treating Frail Adults With Common Malignancies: Best Evidence to Personalize Therapy Treating for Cure or Palliation: Difficult Decisions for Older Adults with Lymphoma Raul Cordoba, MD, PhD Lymphoma Unit
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma
 Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
Bendamustine, Bortezomib and Rituximab in Patients with Relapsed/Refractory Indolent and Mantle-Cell Non-Hodgkin Lymphoma Friedberg JW et al. Proc ASH 2009;Abstract 924. Introduction > Bendamustine (B)
Diffuse Large B-Cell Lymphoma (DLBCL)
") Diffuse Large B-Cell Lymphoma (DLBCL) DLBCL/MCL Dr. Anthea Peters, MD, FRCPC University of Alberta/Cross Cancer Institute Disclosures Honoraria from Janssen, Abbvie, Roche, Lundbeck, Seattle Genetics Objectives
Diffuse Large B-Cell Lymphoma (DLBCL) DLBCL/MCL Dr. Anthea Peters, MD, FRCPC University of Alberta/Cross Cancer Institute Disclosures Honoraria from Janssen, Abbvie, Roche, Lundbeck, Seattle Genetics Objectives
Does BV as part of salvage impact outcome?
 Does BV as part of salvage impact outcome? Craig Moskowitz, MD Steven A. Greenberg Chair in Lymphoma Research Member, Memorial Sloan Kettering Cancer Center Professor of Medicine, Weill Medical College
Does BV as part of salvage impact outcome? Craig Moskowitz, MD Steven A. Greenberg Chair in Lymphoma Research Member, Memorial Sloan Kettering Cancer Center Professor of Medicine, Weill Medical College
LYSA PET adapted programs. O. Casasnovas Hematology department Hopital Le Bocage, CHU Dijon, France
 LYSA PET adapted programs O. Casasnovas Hematology department Hopital Le Bocage, CHU Dijon, France 3 phase III trials DLBCL LNH 09-1B: aaipi = 0, 18 80y : ongoing GAINED: aaipi = 1-3, 18 60y : ongoing
LYSA PET adapted programs O. Casasnovas Hematology department Hopital Le Bocage, CHU Dijon, France 3 phase III trials DLBCL LNH 09-1B: aaipi = 0, 18 80y : ongoing GAINED: aaipi = 1-3, 18 60y : ongoing
The case against maintenance rituximab in Follicular lymphoma. Jonathan W. Friedberg M.D., M.M.Sc.
 The case against maintenance rituximab in Follicular lymphoma Jonathan W. Friedberg M.D., M.M.Sc. Follicular lymphoma: What are goals of treatment? Change natural history of disease: Decrease transformation
The case against maintenance rituximab in Follicular lymphoma Jonathan W. Friedberg M.D., M.M.Sc. Follicular lymphoma: What are goals of treatment? Change natural history of disease: Decrease transformation
Who should get what for upfront therapy for MCL? Kami Maddocks, MD The James Cancer Hospital The Ohio State University
 Who should get what for upfront therapy for MCL? Kami Maddocks, MD The James Cancer Hospital The Ohio State University Treatment Challenges Several effective options, improve response durations, none curable
Who should get what for upfront therapy for MCL? Kami Maddocks, MD The James Cancer Hospital The Ohio State University Treatment Challenges Several effective options, improve response durations, none curable
OSCO/OU ASH-SABC Review. Lymphoma Update. Mohamad Cherry, MD
 OSCO/OU ASH-SABC Review Lymphoma Update Mohamad Cherry, MD Outline Diffuse Large B Cell Lymphoma Double Hit Lymphoma Follicular and Indolent B Cell Lymphomas Mantle Cell Lymphoma T Cell Lymphoma Hodgkin
OSCO/OU ASH-SABC Review Lymphoma Update Mohamad Cherry, MD Outline Diffuse Large B Cell Lymphoma Double Hit Lymphoma Follicular and Indolent B Cell Lymphomas Mantle Cell Lymphoma T Cell Lymphoma Hodgkin
Highlights of ICML 2015
 Highlights of ICML 2015 Jonathan W. Friedberg M.D. Director, James P. Wilmot Cancer Center Statistics, ICML 2015: a global meeting Almost 3700 participants. 90 countries represented. Attendees: USA 465
Highlights of ICML 2015 Jonathan W. Friedberg M.D. Director, James P. Wilmot Cancer Center Statistics, ICML 2015: a global meeting Almost 3700 participants. 90 countries represented. Attendees: USA 465
B Cell Lymphoma: Aggressive
 B Cell Lymphoma: Aggressive UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Ibrutinib approved for mantle cell lymphoma as 2nd line therapy. - Aggressive lymphomas are a group of malignant
B Cell Lymphoma: Aggressive UpToDate: Introduction: Risk Factors: Biology: Symptoms: Diagnosis: Ibrutinib approved for mantle cell lymphoma as 2nd line therapy. - Aggressive lymphomas are a group of malignant
International Conference on Malignant Lymphoma (ICML) June 14-17, 2017
 June 14-17, 2017") International Conference on Malignant Lymphoma (ICML) June 14-17, 2017 INTERIM REPORT FROM A PHASE 2 MULTICENTER STUDY OF TAZEMETOSTAT, AN EZH2 INHIBITOR: CLINICAL ACTIVITY AND FAVORABLE SAFETY IN PATIENTS
International Conference on Malignant Lymphoma (ICML) June 14-17, 2017 INTERIM REPORT FROM A PHASE 2 MULTICENTER STUDY OF TAZEMETOSTAT, AN EZH2 INHIBITOR: CLINICAL ACTIVITY AND FAVORABLE SAFETY IN PATIENTS
Head and Neck: DLBCL
 Head and Neck: DLBCL Nikhil G. Thaker Chelsea C. Pinnix Valerie K. Reed Bouthaina S. Dabaja Department of Radiation Oncology MD Anderson Cancer Center Case 60 yo male Presented with right cervical LAD
Head and Neck: DLBCL Nikhil G. Thaker Chelsea C. Pinnix Valerie K. Reed Bouthaina S. Dabaja Department of Radiation Oncology MD Anderson Cancer Center Case 60 yo male Presented with right cervical LAD
Traitement des lymphomes diffus à grandes cellules B
 Traitement des lymphomes diffus à grandes cellules B Corinne HAIOUN Unité Hémopathies Lymphoïdes- CHU Henri Mondor Université Paris Est Créteil DES Hématologie Février 2012 On February 10th, the merging
Traitement des lymphomes diffus à grandes cellules B Corinne HAIOUN Unité Hémopathies Lymphoïdes- CHU Henri Mondor Université Paris Est Créteil DES Hématologie Février 2012 On February 10th, the merging
Mantle cell lymphoma An update on management
 Mantle cell lymphoma An update on management Dr Kim Linton Consultant Medical Oncologist The Christie NHS Foundation Trust 6 th October 2016 This educational meeting is organised and sponsored by Janssen-Cilag
Mantle cell lymphoma An update on management Dr Kim Linton Consultant Medical Oncologist The Christie NHS Foundation Trust 6 th October 2016 This educational meeting is organised and sponsored by Janssen-Cilag
MMAE disrupts cell division and triggers apoptosis. Pola binds to cell surface antigen CD79b. Pola is internalized; linker cleaves, releasing MMAE
 Adding Polatuzumab Vedotin (Pola) to Bendamustine and Rituximab () Treatment Improves Survival in Patients With Relapsed/Refractory DLBCL: Results of a Phase II Clinical Trial Abstract S802 Sehn LH, Kamdar
Adding Polatuzumab Vedotin (Pola) to Bendamustine and Rituximab () Treatment Improves Survival in Patients With Relapsed/Refractory DLBCL: Results of a Phase II Clinical Trial Abstract S802 Sehn LH, Kamdar
BCL-2 Inhibitors in Follicular Lymphoma
 BCL-2 Inhibitors in Follicular Lymphoma John Gerecitano, MD, PhD Clinical Director, Lymphoma Outpatient Services Lymphoma Service/Developmental Therapeutics Clinic Department of Medicine Memorial Sloan-Kettering
BCL-2 Inhibitors in Follicular Lymphoma John Gerecitano, MD, PhD Clinical Director, Lymphoma Outpatient Services Lymphoma Service/Developmental Therapeutics Clinic Department of Medicine Memorial Sloan-Kettering
Update: Non-Hodgkin s Lymphoma
 2008 Update: Non-Hodgkin s Lymphoma ICML 2008: Update on non-hodgkin s lymphoma Diffuse Large B-cell Lymphoma Improved outcome of elderly patients with poor-prognosis diffuse large B-cell lymphoma (DLBCL)
2008 Update: Non-Hodgkin s Lymphoma ICML 2008: Update on non-hodgkin s lymphoma Diffuse Large B-cell Lymphoma Improved outcome of elderly patients with poor-prognosis diffuse large B-cell lymphoma (DLBCL)
12 th Annual Hematology & Breast Cancer Update Update in Lymphoma
 12 th Annual Hematology & Breast Cancer Update Update in Lymphoma Craig Okada, MD, PhD Assistant Professor, Hematology January 14, 2010 Governors Hotel, Portland Oregon Initial Treatment of Indolent Lymphoma
12 th Annual Hematology & Breast Cancer Update Update in Lymphoma Craig Okada, MD, PhD Assistant Professor, Hematology January 14, 2010 Governors Hotel, Portland Oregon Initial Treatment of Indolent Lymphoma
High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li,
: Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li,") High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li, M.D., Ph.D. Fudan University Shanghai Cancer Center
High grade B-cell lymphomas (HGBL): Altered terminology in the 2016 WHO Classification (Update of the 4 th Edition) and practical issues Xiao-Qiu Li, M.D., Ph.D. Fudan University Shanghai Cancer Center
La terapia dei Linfomi DLBCL può cambiare nei diversi sottotipi della nuova WHO? Annalisa Chiappella
 La terapia dei Linfomi DLBCL può cambiare nei diversi sottotipi della nuova WHO? Annalisa Chiappella Ematologia, AOU Città della Salute e della Scienza, Torino Disclosures, Annalisa Chiappella Research
La terapia dei Linfomi DLBCL può cambiare nei diversi sottotipi della nuova WHO? Annalisa Chiappella Ematologia, AOU Città della Salute e della Scienza, Torino Disclosures, Annalisa Chiappella Research
Choice of upfront treatment in the management of diffuse large B-cell lymphoma and follicular lymphoma
 Choice of upfront treatment in the management of diffuse large B-cell lymphoma and follicular lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
Choice of upfront treatment in the management of diffuse large B-cell lymphoma and follicular lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
Radiotherapy in aggressive lymphomas. Umberto Ricardi
 Radiotherapy in aggressive lymphomas Umberto Ricardi Is there (still) a role for Radiation Therapy in DLCL? NHL: A Heterogeneous Disease ALCL PMLBCL (2%) Burkitt s MCL (6%) Other DLBCL (31%) - 75% of aggressive
Radiotherapy in aggressive lymphomas Umberto Ricardi Is there (still) a role for Radiation Therapy in DLCL? NHL: A Heterogeneous Disease ALCL PMLBCL (2%) Burkitt s MCL (6%) Other DLBCL (31%) - 75% of aggressive
Defined lymphoma entities in the current WHO classification
 Defined lymphoma entities in the current WHO classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno Bellinzona, January 29-31, 2016 Evolution of lymphoma classification Rappaport Lukes
Defined lymphoma entities in the current WHO classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno Bellinzona, January 29-31, 2016 Evolution of lymphoma classification Rappaport Lukes
R/R DLBCL Treatment Landscape
 An Updated Analysis of JULIET, a Global Pivotal Phase 2 Trial of Tisagenlecleucel in Adult Patients With Relapsed or Refractory Diffuse Large B-Cell Lymphoma Abstract S799 Borchmann P, Tam CS, Jäger U,
An Updated Analysis of JULIET, a Global Pivotal Phase 2 Trial of Tisagenlecleucel in Adult Patients With Relapsed or Refractory Diffuse Large B-Cell Lymphoma Abstract S799 Borchmann P, Tam CS, Jäger U,
Today, how many PTCL patients are cured? Steven M. Horwitz M.D. Associate Attending Lymphoma Service Memorial Sloan Kettering Cancer Center
 Today, how many PTCL patients are cured? Steven M. Horwitz M.D. Associate Attending Lymphoma Service Memorial Sloan Kettering Cancer Center Today, how many PTCL patients are cured? Some but not as many
Today, how many PTCL patients are cured? Steven M. Horwitz M.D. Associate Attending Lymphoma Service Memorial Sloan Kettering Cancer Center Today, how many PTCL patients are cured? Some but not as many
Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège. 14 th post-ash meeting, January 6 th 2011, Brussels
 Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège 14 th post-ash meeting, January 6 th 2011, Brussels Hodgkin s lymphoma Follicular lymphoma Diffuse large B-cell lymphoma Mantle cell
Lymphoma Christophe BONNET Centre Hospitalier Universitaire, Ulg, Liège 14 th post-ash meeting, January 6 th 2011, Brussels Hodgkin s lymphoma Follicular lymphoma Diffuse large B-cell lymphoma Mantle cell
Unmet need for new strategies in T cell lymphoma
 In Vitro, In Vivo, and Parallel Phase I Evidence Support the Safety and Activity of Duvelisib, a PI3K δ,γ Inhibitor, in Combination with Romidepsin or Bortezomib in Relapsed/Refractory T Cell Lymphoma
In Vitro, In Vivo, and Parallel Phase I Evidence Support the Safety and Activity of Duvelisib, a PI3K δ,γ Inhibitor, in Combination with Romidepsin or Bortezomib in Relapsed/Refractory T Cell Lymphoma
CAR-T cell therapy pros and cons
 CAR-T cell therapy pros and cons Stephen J. Schuster, MD Professor of Medicine Perelman School of Medicine of the University of Pennsylvania Director, Lymphoma Program & Lymphoma Translational Research
CAR-T cell therapy pros and cons Stephen J. Schuster, MD Professor of Medicine Perelman School of Medicine of the University of Pennsylvania Director, Lymphoma Program & Lymphoma Translational Research
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma
 Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
Bendamustine is Effective Therapy in Patients with Rituximab-Refractory, Indolent B-Cell Non-Hodgkin Lymphoma Kahl BS et al. Cancer 2010;116(1):106-14. Introduction > Bendamustine is a novel alkylating
RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA
 RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA Pier Luigi Zinzani Institute of Hematology and Medical Oncology L. e A. Seràgnoli University of Bologna, Italy Slovenia, October 5 2007 Zevalin
RADIOIMMUNOTHERAPY FOR TREATMENT OF NON- HODGKIN S LYMPHOMA Pier Luigi Zinzani Institute of Hematology and Medical Oncology L. e A. Seràgnoli University of Bologna, Italy Slovenia, October 5 2007 Zevalin
A CME-certified Oncology Exchange Program
 A CME-certified Oncology Exchange Program Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Seattle Genetics, Inc. Re-treatment with BV Bartlett
A CME-certified Oncology Exchange Program Jointly provided by Potomac Center for Medical Education and Rockpointe Supported by an educational grant from Seattle Genetics, Inc. Re-treatment with BV Bartlett
Relapsed/Refractory Hodgkin Lymphoma
 Relapsed/Refractory Hodgkin Lymphoma Anas Younes, MD Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center New York, New York, United States Case Study 32-year-old woman was diagnosed with stage
Relapsed/Refractory Hodgkin Lymphoma Anas Younes, MD Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center New York, New York, United States Case Study 32-year-old woman was diagnosed with stage
Hodgkin Lymphoma New Combo-Steps
 New Drugs In Hematology Hodgkin Lymphoma New Combo-Steps Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center Monday, May 9, 2016 2:55-3:10 p.m Combinations with Immune Checkpoint
New Drugs In Hematology Hodgkin Lymphoma New Combo-Steps Anas Younes, M.D. Chief, Lymphoma Service Memorial Sloan-Kettering Cancer Center Monday, May 9, 2016 2:55-3:10 p.m Combinations with Immune Checkpoint
Addition of rituximab is not associated with survival benefit compared with CHOP alone for patients with stage I diffuse large B-cell lymphoma
 Original Article Addition of rituximab is not associated with survival benefit compared with CHOP alone for patients with stage I diffuse large B-cell lymphoma Bo Jia 1, Yuankai Shi 1, Suyi Kang 1, Sheng
Original Article Addition of rituximab is not associated with survival benefit compared with CHOP alone for patients with stage I diffuse large B-cell lymphoma Bo Jia 1, Yuankai Shi 1, Suyi Kang 1, Sheng
Diffuse large B-cell lymphomas. G. Verhoef, MD, PhD University Hospital Leuven BHS, March 9, 2013
 Diffuse large B-cell lymphomas G. Verhoef, MD, PhD University Hospital Leuven BHS, March 9, 2013 Case A 72-year-old previously healthy man presented with acute abdominal pain and a 15 kg weight loss. Positron
Diffuse large B-cell lymphomas G. Verhoef, MD, PhD University Hospital Leuven BHS, March 9, 2013 Case A 72-year-old previously healthy man presented with acute abdominal pain and a 15 kg weight loss. Positron
Aggressive B-cell Lymphomas
 Neoplastic Hematopathology Update 2018 Aggressive B-cell Lymphomas Raju K. Pillai City of Hope National Medical Center I do not have any disclosures Disclosures Outline New entities and changes in WHO
Neoplastic Hematopathology Update 2018 Aggressive B-cell Lymphomas Raju K. Pillai City of Hope National Medical Center I do not have any disclosures Disclosures Outline New entities and changes in WHO
How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES
 How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES How I Choose First Line Treatment in Follicular Lymphoma in 2017? 1. How do I take into account
How I approach newly diagnosed Follicular Lymphoma patients with advanced stage? Professeur Gilles SALLES How I Choose First Line Treatment in Follicular Lymphoma in 2017? 1. How do I take into account
Disclosures of XXXXX
 Disclosures of XXXXX Company name Research support Employee Consultant Stockholder Speakers bureau Advisory board Other Abbvie X X Genentech X X Gilead X Bayer X X Incyte X Samus Therapeutics X BCL-2 Inhibitors
Disclosures of XXXXX Company name Research support Employee Consultant Stockholder Speakers bureau Advisory board Other Abbvie X X Genentech X X Gilead X Bayer X X Incyte X Samus Therapeutics X BCL-2 Inhibitors
New Targets and Treatments for Follicular Lymphoma
 Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
Winship Cancer Institute of Emory University New Targets and Treatments for Follicular Lymphoma Jonathon B. Cohen, MD, MS Assistant Professor Div of BMT, Emory University Intro/Outline Follicular lymphoma,
Policy for Central Nervous System [CNS] Prophylaxis in Lymphoid Malignancies
![Policy for Central Nervous System [CNS] Prophylaxis in Lymphoid Malignancies](/thumbs/90/104309591.jpg "Policy for Central Nervous System [CNS] Prophylaxis in Lymphoid Malignancies") Policy for Central Nervous System [CNS] Prophylaxis in Lymphoid Malignancies UNCONTROLLED WHEN PRINTED Note: NOSCAN Haematology MCN has approved the information contained within this document to guide
Policy for Central Nervous System [CNS] Prophylaxis in Lymphoid Malignancies UNCONTROLLED WHEN PRINTED Note: NOSCAN Haematology MCN has approved the information contained within this document to guide
CARE at ASH 2014 Lymphoma. Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre
 CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
CARE at ASH 2014 Lymphoma Dr. Diego Villa Medical Oncologist British Columbia Cancer Agency Vancouver Cancer Centre High-yield lymphoma sessions Sat, Dec 6 th Sun, Dec 7 th Mon, Dec 8 th EDUCATIONAL SESSIONS
Bendamustine for Hodgkin lymphoma. Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service
 Bendamustine for Hodgkin lymphoma Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service Bendamustine in Hodgkin lymphoma Bifunctional molecule Nitrogen mustard component (meclorethamine)
Bendamustine for Hodgkin lymphoma Alison Moskowitz, MD Assistant Attending Memorial Sloan Kettering, Lymphoma Service Bendamustine in Hodgkin lymphoma Bifunctional molecule Nitrogen mustard component (meclorethamine)
Aggressive B-cell Lymphomas Updated WHO classification Elias Campo
 Aggressive B-cell Lymphomas Updated WHO classification Elias Campo Hospital Clinic, University of Barcelona Diffuse Large B-cell Lymphoma A Heterogeneous Category Subtypes with differing: Histology and
Aggressive B-cell Lymphomas Updated WHO classification Elias Campo Hospital Clinic, University of Barcelona Diffuse Large B-cell Lymphoma A Heterogeneous Category Subtypes with differing: Histology and
eastern cooperative oncology group Michael Williams, Fangxin Hong, Brad Kahl, Randy Gascoyne, Lynne Wagner, John Krauss, Sandra Horning
 Results of E4402 (RESORT): A Randomized Phase III Study Comparing Two Different Rituximab Dosing Strategies for Low Tumor Burden Indolent B-Cell Lymphoma Michael Williams, Fangxin Hong, Brad Kahl, Randy
Results of E4402 (RESORT): A Randomized Phase III Study Comparing Two Different Rituximab Dosing Strategies for Low Tumor Burden Indolent B-Cell Lymphoma Michael Williams, Fangxin Hong, Brad Kahl, Randy
Post-ESMO Berne
 Post-ESMO Berne 23.10.2015 Lymphoma Update Panagiotis Samaras Department of Oncology Hemato-Oncology Center University Hospital Zurich Diffuse Large B-Cell Lymphoma (DLBCL) PCNSL Hodgkin s Lymphoma Mantle
Post-ESMO Berne 23.10.2015 Lymphoma Update Panagiotis Samaras Department of Oncology Hemato-Oncology Center University Hospital Zurich Diffuse Large B-Cell Lymphoma (DLBCL) PCNSL Hodgkin s Lymphoma Mantle
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective
 Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
GLSG/OSHO Study Group. Supported by Deutsche Krebshilfe
 GLSG/OSHO Study Group Supported by Deutsche Krebshilfe founded in 1985 Comparison of Two Consecutive Study Generations of the GLSG Overall Survival Follicular Lymphomas Questions for the Next Steps of
GLSG/OSHO Study Group Supported by Deutsche Krebshilfe founded in 1985 Comparison of Two Consecutive Study Generations of the GLSG Overall Survival Follicular Lymphomas Questions for the Next Steps of
Aggressive NHL and Hodgkin Lymphoma. Dr. Carolyn Faught November 10, 2017
 Aggressive NHL and Hodgkin Lymphoma Dr. Carolyn Faught November 10, 2017 What does aggressive mean? Shorter duration of symptoms Generally need treatment at time of diagnosis Immediate, few days, few weeks
Aggressive NHL and Hodgkin Lymphoma Dr. Carolyn Faught November 10, 2017 What does aggressive mean? Shorter duration of symptoms Generally need treatment at time of diagnosis Immediate, few days, few weeks
Mantle Cell Lymphoma. A schizophrenic disease
 23 maggio, 2018 Mantle Cell Lymphoma A schizophrenic disease Patients relapsed after Auto transplant EBMT registry 2000-2009 (n=360) 19 months OS 24 months OS Dietrich S, Ann Oncol 2014 Patients receiving
23 maggio, 2018 Mantle Cell Lymphoma A schizophrenic disease Patients relapsed after Auto transplant EBMT registry 2000-2009 (n=360) 19 months OS 24 months OS Dietrich S, Ann Oncol 2014 Patients receiving
Open questions in the treatment of Follicular Lymphoma. Prof. Michele Ghielmini Head Medical Oncology Dept Oncology Institute of Southern Switzerland
 Open questions in the treatment of Follicular Lymphoma Prof. Michele Ghielmini Head Medical Oncology Dept Oncology Institute of Southern Switzerland Survival of major lymphoma subtypes at IOSI 1.00 cause-specific
Open questions in the treatment of Follicular Lymphoma Prof. Michele Ghielmini Head Medical Oncology Dept Oncology Institute of Southern Switzerland Survival of major lymphoma subtypes at IOSI 1.00 cause-specific
Multiple Myeloma Updates 2007
 Multiple Myeloma Updates 2007 Brian Berryman, M.D. Multiple Myeloma Updates 2007 Goals for today: Understand the staging systems for myeloma Understand prognostic factors in myeloma Review updates from
Multiple Myeloma Updates 2007 Brian Berryman, M.D. Multiple Myeloma Updates 2007 Goals for today: Understand the staging systems for myeloma Understand prognostic factors in myeloma Review updates from
CNS Lymphoma. Las Vegas-- March 10-12, 2016
 CNS Lymphoma Las Vegas-- March 10-12, 2016 Frequency 3% of primary cerebral tumors 1% of NHLs Recent developments and controversies in PCNSL Hottinger et al Current Opinion in Oncology Vol 27 No. 6 November
CNS Lymphoma Las Vegas-- March 10-12, 2016 Frequency 3% of primary cerebral tumors 1% of NHLs Recent developments and controversies in PCNSL Hottinger et al Current Opinion in Oncology Vol 27 No. 6 November
Novita da EHA 2016 Copenhagen Linfomi
 Firenze, 16th September 2016 Marco Ladetto MD, Az Osp Santi Antonio e Biagio e Cesare Arrigo, Alessandria, Italy EU Novita da EHA 2016 Copenhagen Linfomi THREE QUESTIONS TO ADDRESS: 1. Is ASCT still the
Firenze, 16th September 2016 Marco Ladetto MD, Az Osp Santi Antonio e Biagio e Cesare Arrigo, Alessandria, Italy EU Novita da EHA 2016 Copenhagen Linfomi THREE QUESTIONS TO ADDRESS: 1. Is ASCT still the
Treatment Nodal Marginal Zone Lymphoma
 Workshop : Indolent lymphomas Treatment Nodal Marginal Zone Lymphoma Catherine Thieblemont Hôpital Saint-Louis, Paris - France Bologna 16th, 2017 Ø No standardized treatment Ø Similarly treated as FL Treatment
Workshop : Indolent lymphomas Treatment Nodal Marginal Zone Lymphoma Catherine Thieblemont Hôpital Saint-Louis, Paris - France Bologna 16th, 2017 Ø No standardized treatment Ø Similarly treated as FL Treatment
Aggressive B cell Lymphomas
 Aggressive B cell Lymphomas I have nothing to disclose. Disclosures Raju K. Pillai City of Hope National Medical Center Outline WHO 2016 Classification Large B cell Lymphomas New entities and changes in
Aggressive B cell Lymphomas I have nothing to disclose. Disclosures Raju K. Pillai City of Hope National Medical Center Outline WHO 2016 Classification Large B cell Lymphomas New entities and changes in
Practical Application of PET adapted Therapy in Hodgkin Lymphoma
 Practical Application of PET adapted Therapy in Hodgkin Lymphoma Matthew Matasar, MD Lymphoma and Adult BMT Services Director, Lymphoma Survivorship Clinic Memorial Sloan Kettering Cancer Center New York,
Practical Application of PET adapted Therapy in Hodgkin Lymphoma Matthew Matasar, MD Lymphoma and Adult BMT Services Director, Lymphoma Survivorship Clinic Memorial Sloan Kettering Cancer Center New York,
Angioimmunoblastic T-cell lymphoma: nobody knows what to do...
 Angioimmunoblastic T-cell lymphoma: nobody knows what to do... Felicitas Hitz, Onkologie/Hämatologie St.Gallen SAMO Lucerne 17.9.2011 : Problems PTCL are rare diseases with even rarer subgroups Difficulte
Angioimmunoblastic T-cell lymphoma: nobody knows what to do... Felicitas Hitz, Onkologie/Hämatologie St.Gallen SAMO Lucerne 17.9.2011 : Problems PTCL are rare diseases with even rarer subgroups Difficulte
Clinical Advances in Lymphoma
 Conflicts of Interest Clinical Advances in Lymphoma Alex F. Herrera, MD Assistant t Professor Department of Hematology and HCT City of Hope BMS research funding (institutional), consultancy Genentech research
Conflicts of Interest Clinical Advances in Lymphoma Alex F. Herrera, MD Assistant t Professor Department of Hematology and HCT City of Hope BMS research funding (institutional), consultancy Genentech research
New Evidence reports on presentations given at EHA/ICML Bendamustine in the Treatment of Lymphoproliferative Disorders
 New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
New Evidence reports on presentations given at EHA/ICML 2011 Bendamustine in the Treatment of Lymphoproliferative Disorders Report on EHA/ICML 2011 presentations Efficacy and safety of bendamustine plus
Learn more about diffuse large B-cell lymphoma (DLBCL), the most common aggressive form of B-cell non-hodgkin s lymphoma 1
, the most common aggressive form of B-cell non-hodgkin s lymphoma 1") Learn more about diffuse large B-cell lymphoma (DLBCL), the most common aggressive form of B-cell non-hodgkin s lymphoma 1 Expression of B-cell surface antigens drives several non-hodgkin s lymphomas (NHLs)
Learn more about diffuse large B-cell lymphoma (DLBCL), the most common aggressive form of B-cell non-hodgkin s lymphoma 1 Expression of B-cell surface antigens drives several non-hodgkin s lymphomas (NHLs)
Rituximab in the Treatment of NHL:
 New Evidence reports on presentations given at ASH 2010 Rituximab in the Treatment of NHL: Rituximab versus Watch and Wait in Asymptomatic FL, R-Maintenance Therapy in FL with Standard or Rapid Infusion,
New Evidence reports on presentations given at ASH 2010 Rituximab in the Treatment of NHL: Rituximab versus Watch and Wait in Asymptomatic FL, R-Maintenance Therapy in FL with Standard or Rapid Infusion,
NK/T cell lymphoma Recent advances. Y.L Kwong University Department of Medicine Queen Mary Hospital
 NK/T cell lymphoma Recent advances Y.L Kwong University Department of Medicine Queen Mary Hospital Natural killer cell lymphomas NK cell lymphomas are mainly extranodal lymphomas Clinical classification
NK/T cell lymphoma Recent advances Y.L Kwong University Department of Medicine Queen Mary Hospital Natural killer cell lymphomas NK cell lymphomas are mainly extranodal lymphomas Clinical classification
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC)
") Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
Clinical Research on PARP Inhibitors and Triple-Negative Breast Cancer (TNBC) Eric P Winer, MD Disclosures for Eric P Winer, MD No real or apparent conflicts of interest to disclose Key Topics: PARP and
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma
 with classical Hodgkin lymphoma") PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
PET-adapted therapies in the management of younger patients (age 60) with classical Hodgkin lymphoma Ryan Lynch MD Assistant Professor, University of Washington Assistant Member, Fred Hutchinson Cancer
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial
 Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
Addition of Rituximab to Fludarabine and Cyclophosphamide in Patients with CLL: A Randomized, Open-Label, Phase III Trial Hallek M et al. Lancet 2010;376:1164-74. Introduction > In patients with CLL, the
Lymphoma. André Bosly M.D.,Ph.D. Post ASH meeting 10/01/2014 Sheraton Brussels National Airport
 Lymphoma André Bosly M.D.,Ph.D. Post ASH meeting 10/01/2014 Sheraton Brussels National Airport Lymphoma Hodgkin Lymphoma (HL) Indolent Lymphoma (inhl) Diffuse Large B Cell Lymphoma (DLBCL) Hodgkin Lymphoma
Lymphoma André Bosly M.D.,Ph.D. Post ASH meeting 10/01/2014 Sheraton Brussels National Airport Lymphoma Hodgkin Lymphoma (HL) Indolent Lymphoma (inhl) Diffuse Large B Cell Lymphoma (DLBCL) Hodgkin Lymphoma
Pathology of aggressive lymphomas
 Institute of Pathology Pathology of aggressive lymphomas Leticia Quintanilla-Martinez Changes in the new 2016 WHO Aggressive B-cell lymphoid neoplasms Major changes that impact how cases should be evaludated
Institute of Pathology Pathology of aggressive lymphomas Leticia Quintanilla-Martinez Changes in the new 2016 WHO Aggressive B-cell lymphoid neoplasms Major changes that impact how cases should be evaludated
Non-Hodgkin s and Hodgkin lymphoma: using disease characteristics as a guide to treatment selection. Arnold Freedman, M.D.
 2017 Master Class for Oncologists Non-Hodgkin s and Hodgkin lymphoma: using disease characteristics as a guide to treatment selection Arnold Freedman, M.D. 2018 Master Class Course Disclosure Disclosure
2017 Master Class for Oncologists Non-Hodgkin s and Hodgkin lymphoma: using disease characteristics as a guide to treatment selection Arnold Freedman, M.D. 2018 Master Class Course Disclosure Disclosure
CME Information LEARNING OBJECTIVES
 CME Information LEARNING OBJECTIVES Identify patients with MM who have undergone autologous stem cell transplant and would benefit from maintenance lenalidomide. Counsel older patients (age 65 or older)
CME Information LEARNING OBJECTIVES Identify patients with MM who have undergone autologous stem cell transplant and would benefit from maintenance lenalidomide. Counsel older patients (age 65 or older)
Two Cycles of Chemoradiation: 2 Cycles is Enough. Concurrent Chemotherapy / RT Regimens
 1 Two Cycles of Chemoradiation: 2 Cycles is Enough Heather Wakelee, M.D. Assistant Professor of Medicine, Oncology Stanford University Concurrent Chemotherapy / RT Regimens Cisplatin 50 mg/m 2 on days
1 Two Cycles of Chemoradiation: 2 Cycles is Enough Heather Wakelee, M.D. Assistant Professor of Medicine, Oncology Stanford University Concurrent Chemotherapy / RT Regimens Cisplatin 50 mg/m 2 on days
Targeted Radioimmunotherapy for Lymphoma
 Targeted Radioimmunotherapy for Lymphoma John Pagel, MD, PhD Fred Hutchinson Cancer Center Erik Mittra, MD, PhD Stanford Medical Center Brought to you by: Financial Disclosures Disclosures Erik Mittra,
Targeted Radioimmunotherapy for Lymphoma John Pagel, MD, PhD Fred Hutchinson Cancer Center Erik Mittra, MD, PhD Stanford Medical Center Brought to you by: Financial Disclosures Disclosures Erik Mittra,
Follicular Lymphoma 2016:
 Follicular Lymphoma 2016: Evolving Management Strategies Randeep Sangha, MD Medical Oncology, Cross Cancer Institute Associate Professor, University of Alberta Edmonton, AB Disclosures I have no actual
Follicular Lymphoma 2016: Evolving Management Strategies Randeep Sangha, MD Medical Oncology, Cross Cancer Institute Associate Professor, University of Alberta Edmonton, AB Disclosures I have no actual
Supplementary Appendix to manuscript submitted by Trappe, R.U. et al:
 Supplementary Appendix to manuscript submitted by Trappe, R.U. et al: Response to rituximab induction is a predictive marker in B-cell post-transplant lymphoproliferative disorder and allows successful
Supplementary Appendix to manuscript submitted by Trappe, R.U. et al: Response to rituximab induction is a predictive marker in B-cell post-transplant lymphoproliferative disorder and allows successful
What is the best approach to the initial therapy of PTCL? standards of treatment? Should all
 What is the best approach to the initial therapy of PTCL? standards of treatment? hould all Jia Ruan, M.D., Ph.D. Center for Lymphoma and Myeloma Weill Cornell Medical College New York Presbyterian Hospital
What is the best approach to the initial therapy of PTCL? standards of treatment? hould all Jia Ruan, M.D., Ph.D. Center for Lymphoma and Myeloma Weill Cornell Medical College New York Presbyterian Hospital
ORIGINAL ARTICLE. Annals of Oncology 28: , 2017 doi: /annonc/mdx128 Published online 7 April 2017
 Annals of Oncology 28: 54 546, 27 doi:.93/annonc/mdx28 Published online 7 April 27 ORIGINAL ARTICLE Outcome of elderly patients with diffuse large B-cell lymphoma treated with R-CHOP: results from the
Annals of Oncology 28: 54 546, 27 doi:.93/annonc/mdx28 Published online 7 April 27 ORIGINAL ARTICLE Outcome of elderly patients with diffuse large B-cell lymphoma treated with R-CHOP: results from the
Characteristics and treatment of DLBCL in elderly patients
 Characteristics and treatment of DLBCL in elderly patients Lysa Experience or From Stephan to Ruth Eli 5/02/16 F.Peyrade Nice France Age at Diagnosis http://seer.cancer.gov/ E(x) 10,00 9,00 8,00 7,00 6,00
Characteristics and treatment of DLBCL in elderly patients Lysa Experience or From Stephan to Ruth Eli 5/02/16 F.Peyrade Nice France Age at Diagnosis http://seer.cancer.gov/ E(x) 10,00 9,00 8,00 7,00 6,00
The next lymphoma classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno
 Evolution of classification The next classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno The Lymphoma Forum of Excellence, Bellinzona, January 2011 Rappaport Lukes and Collins (immunophenotype)
Evolution of classification The next classification Luca Mazzucchelli Istituto cantonale di patologia, Locarno The Lymphoma Forum of Excellence, Bellinzona, January 2011 Rappaport Lukes and Collins (immunophenotype)
Lymphoma Update 2018
 Lymphoma Update 2018 Sonali M. Smith, MD Elwood V. Jensen Professor of Medicine Section of Hematology/Oncology Director, Lymphoma Program The University of Chicago April 18, 2018 Disclosure Information
Lymphoma Update 2018 Sonali M. Smith, MD Elwood V. Jensen Professor of Medicine Section of Hematology/Oncology Director, Lymphoma Program The University of Chicago April 18, 2018 Disclosure Information
How to Integrate the New Drugs into the Management of Multiple Myeloma
 How to Integrate the New Drugs into the Management of Multiple Myeloma Carol Ann Huff, MD The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins NCCN.org For Clinicians NCCN.org/patients For Patients
How to Integrate the New Drugs into the Management of Multiple Myeloma Carol Ann Huff, MD The Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins NCCN.org For Clinicians NCCN.org/patients For Patients