Head&Neck, and Thyroid Cancers: Incorporating New Therapies into Current Treatment Algorithms
|
|
|
- Jordan Alexander
- 5 years ago
- Views:
Transcription
1 Head&Neck, and Thyroid Cancers: Incorporating New Therapies into Current Treatment Algorithms Robert Haddad, MD Disease Center Leader Head and Neck Oncology Program Dana Farber Cancer Institute Harvard Medical School Boston, MA
2 Disclosures Research Funding: BMS, Merck, Pfizer Celgene, Astra Zeneca Consultant: Merck,BMS, Eisai, Bayer, Pfizer, Astra Zeneca NCCN: Member: Head and Neck Committee NCCN: Chair: Thyroid Committee Pres
3 Head and Neck Cancer Introduction: Epidemiology, Clinical Features, Prevention, Treatment Modalities Concurrent Chemoradiotherapy Sequential Chemoradiotherapy Adjuvant Chemoradiotherapy Recurrent/Metastatic disease New drugs in Thyroid Cancer 3

4 Head and Neck Cancer Primary Disease Sites Oral Cavity Pharynx Larynx Nasal Cavity Paranasal Sinuses 4 Source: Maxwell V. Blum Cancer Resource Room
5 Epidemiology new cases per year in US. Median age of diagnosis: ~60 years Male>Female Strongly associated with tobacco and alcohol Epstein-Barr virus risk factor for nasopharynx cancers Human papillomavirus increasingly appreciated as a risk factor 5

6 Human Papillomavirus (HPV) 6 HPV-Associated Cancers > 99% of Cervical Carcinoma ~ 90% Anal Carcinomas ~ 40% Vulvar and Vaginal Carcinomas ~ 60% of Oropharynx Cancers HPV GENOME INTEGRATION LCR E6 E7 Circular 8 kb dsdna Genomes Only One Coding Strand Infect Epithelial Cells ~ 200 HPV types ~ 30 Mucosal HPVs Low-Risk: Genital Warts High-Risk: Lesions That Progress to Cancer Frequent Event During Malignant Progression Terminates Viral Life Cycle Expression of E6 and E7 Is Retained HPV E6/E7 Oncoproteins Small, Non-Enzymatic Proteins (~ 150aa E6; ~ 100aa E7) Associate With and Functionally Modify Host Cellular Protein Complexes Münger et al, 2004.
7 Human Papillomavirus (HPV)-Positive Head and Neck Cancer HPV 16 is the viral subtype in the vast majority of patients. Half of oropharynx cancers will have HPV 16 DNA. Often occurs in nonsmokers, nondrinkers Median age younger than HPV-negative patients; incidence increasing Associated with number of sexual partners and highrisk sexual practices Favorable prognosis 7 Fakhry C, et al. J Clin Oncol. 2006:24(17): Chaturvedi AK, et al. J Clin Oncol. 2008;26(4):
8 HPV testing in tumors In situ hybridization p16 immunohistochemistry PCR
9 Rising Incidence of HPV-Associated Cancers Smoking related HPV- related Chaturvedi et al, JCO 2008.
10 Survival Outcomes by HPV Status in Oropharyngeal Cancer in RTOG 0129 Ang et al NEJM 2010
11 RTOG 0129 Phase III Trial: Concomitant CRT With Standard Vs. Accelerated Fractionation RT CRT Stage III/IV (T2, N2 3, M0, or T3 4, any N, M0) SCCHN Oral cavity, oropharynx, hypopharynx, larynx No prior RT to head and neck except radioactive iodine therapy No prior surgery to primary tumor or nodes except for diagnostic biopsy Expected N = 720 R A N D O M I Z E Cisplatin (IV on D1, 22, 43) Standard fractionation RT (5 d/wk for 7 wks) Cisplatin (IV on D1, 22) Accelerated fractionation RT (5 d/wk for 3.5 wks; then twice daily, 5 d/wk for 2.5 wks) US NIH, 2010c.

 100 75 50 25 0 PFS HPV")
 HPV Negative (%) P")

12 RTOG 0129: OS and PFS by HPV Status Overall Survival (%) Overall Survival HPV negative HPV positive HR=0.38 (95% CI: ); P<0.001 Progression-Free Survival (%) PFS HPV negative HPV positive HR=0.40 (95% CI: ; P< Year Outcomes HPV Positive (%) HPV Negative (%) P Value OS <0.001 PFS <0.001 Locoregional failure <0.001 Distant metastases Ang. N Engl J Med. June 7, 2010
13 Two distinct HNSCC entities HPV positive HPV negative Anatomic site Tonsil /Base of Tongue All sites Histology Basaloid Keratinized Age Younger Older Gender 3:1 men 3:1 men SE status High Low Risk factors Sexual behavior ETOH/tobacco Cofactors should we treat them the same? Marijuana/?immune suppression ETOH/tobacco Incidence Rising Declining Survival Improved Worse There is a major change in the etiology of head and neck cancer, the incidence of OPC rapidly increasing mostly North America and Europe
14 E1308: Phase II Trial of Induction Chemotherapy Followed by Reduced- Dose Radiation and Weekly Cetuximab in Patients With HPV-Associated Resectable Squamous Cell Carcinoma of the Oropharynx ECOG- ACRIN Cancer Research Group Marur et al : JCO 2016
15 ECOG 1308: Phase II Schema Eligibility Oropharynx SCC HPV ISH + and / or p16+ Stage III, IVA Induction Chemotherapy Cisplatin 75mg/m 2 d1 Paclitaxel 90mg/m 2 d1,8,15 Cetuximab 250mg/m 2 d1,8,15 Q 21 days for 3 cycles R E S P O N S E E V A L U A T I O N Concurrent Chemoradiation CLINICAL CR Low dose IMRT 54Gy/27fx* + Cetuximab qweek CLINICAL PR/SD Full dose IMRT 69.3Gy/33fx* + Cetuximab qweek Marur et al : JCO 2016

16 Endpoint: 2yr PFS and OS * 3 high-dose pts did not go on to receive RT
17 E 1308: OS and PFS PFS (A) and OS (B) in cohort with clinical complete response to induction chemotherapy treated with low-dose radiation of 54 Gy (n = 51). 17
18 E 1308: OS and PFS 18 PFS (A) and OS (B) in favorable cohort (non-t4, non-n2c, 10 pack-year smokers) with clinical complete response to induction chemotherapy treated with low-dose radiation of 54 Gy (n = 27).
19 Summary E1308 Induction chemo followed by reduced-dose IMRT/Cetuximab was feasible in a Cooperative Group setting CCR to induction was noted in 70% (56/80), and was well tolerated. The 2yr PFS in 54Gy IMRT patients was 80% ( 95% CI 0.70, 0.88) and 2yr OS was 94%. Best results of 54Gy was in smokers <10pk-yrs, non T-4 and non-n2c: 2yr PFS and 2yr OS of 96% (n=27) At 12 months : fewer pts in low dose had difficulty with swallowing solids. This approach remains investigational. Further studies are planned
20 Treatment Approach Disease Extent T 1 N 0-1 or T 2 N 0 Treatment Surgery or RT T 2 N 1 or T 3-4 or N 2-3 Combined modality Recurrent or M 1 Surgery and/or RT Combined modality Chemotherapy 20
21 Concurrent Chemoradiotherapy
22 The Debate Over Therapeutic Sequence: MACH-NC Findings Design (No. of Studies/ No. of Subjects) Hazard Ratio (95% CI) Chemotherapy Effect (P -value) Absolute Benefit 2 Years 5 Years Adjuvant 1 (8/1854) 0.98 ( ) % 1% Neoadjuvant 1 (31/5269) Concurrent 1 (26/3727) Total 1 (65/10,850) 0.95 ( ) 0.81 ( ) 0.90 ( ) % 2% < % 8% < % 4% No. of Trials No. of Subjects Difference at 5 Years P -value PF induction % MACH-NC: Meta-Analysis of Chemotherapy in Head and Neck Cancer; PF=cisplatin + fluorouracil 1. Pignon JP, et al. Lancet. 2000;355(9208): Monnerat C, et al. Ann Oncol. 2002;13(7):
23 Concurrent Therapy: Standard of Care Cisplatin 100 mg/m 2 days 1, 22, and 43 of RT RT standard fractionation, 70 Gy over 7 weeks (2-Gy fractions) Alternative Chemotherapy regimens: 1- Weekly cisplatin 40mg/m2 2- Weekly Cetuximab 3- Weekly carboplatin auc Paclitaxel 30-45mg/m2
24 RTOG Induction Cisplatin/5-FU vs Concomitant Cisplatin vs RT Alone in Resectable SCC ICT RT (N = 173) Resectable stage III/IV SCC Glottic or supraglottic cancer Previously untreated N = 515 R A N D O M I Z E Cisplatin (100 mg/m 2, d1) 5-FU (1000 mg/m 2 /day, d1-5 C-I) every 3 wks, 2 cycles CRT (N = 171) Cisplatin (100 mg/m 2, every 3 wks, 3 cycles) RT (2 Gy/fr, 35 fr, total 70 Gy) RT (N = 171) RT (2 Gy/fr, 35 fr, total 70 Gy) RT (2 Gy/fr, 35 fr, total 70 Gy) Primary end point: larynx preservation Secondary end point: LFS LFS=laryngectomy-free survival Forastiere AA, et al. N Engl J Med. 2003;349(22):
25 RTOG Larynx Preservation (LP) Trial Arm Stomatitis* LP rate (5yrs) DFS (5yrs) OS (5yrs) RT 24% 65.7% 27.3% 53.5% Chemo RT 24% 70.5% 38.6% 59.2% ChemoRT 43% 83.6% 39.0% 54.6% * > or = Grade Forastiere AA, et al. N Engl J Med. 2003;349(22):
26 Phase III Trial: Cetuximab + RT for SCC Advanced SCC Stage III/IV N = 424 R A N D O M I Z E RT* + Cetuximab (400 mg/m 2, then 250 mg/m 2 /wk) RT* alone *Choice of: Once-daily RT: 70 Gy in 35 fractions Twice-daily RT: Gy in fractions Concomitant boost: 72 Gy in 42 fractions Grade 3-5 Toxicity RT Alone (N = 212) RT + Cetuximab (N = 208) P-value Mucositis 52% 56%.44 Acneiform Rash 1% 17% <.001 Infusion Reaction 0% 3%.01 Anemia 6% 1% Bonner JA, et al. N Engl J Med. 2006;354(6):
27 Phase III: Cetuximab + RT for SCC: Results Locoregional Control OS 47% vs 34% at 3 years P <.01 at 3 years 55% vs 45% at 3 years P =.05 at 3 years 27 Bonner JA, et al. N Engl J Med. 2006;354(6):
28 Sequential Chemoradiotherapy
29 TAX 324: Sequential Combined Modality Therapy TPF vs PF Followed by Chemoradiotherapy R A N D O M I Z E T P F P F Carboplatinum - AUC 1.5 Weekly Daily Radiotherapy Surgery as Needed TPF: Docetaxel 75 D1 + Cisplatin 100 D1 + 5-FU 1000 CI- D1-4 Q 3 weeks x3 PF: Cisplatin 100 D1 + 5-FU 1000 CI-D1-5 Q 3 weeks x 3 29 Posner MR, et al. N Engl J Med. 2007;357(17):

:1705-1715. Posner.")
30 Patient Characteristics: TPF vs PF Intent to Treat Population 30 Posner MR, et al. N Engl J Med. 2007;357(17): Posner. N Engl J Med. 2007;357:1705
31 TAX 324: Results 100 Survival 100 PFS Survival Probability (%) TPF 67% PF 54% TPF (N = 255) PF (N = 246) Log-rank p =.0058 HR = 0.70 TPF 62% PF 48% PFS Probability (%) TPF 53% PF 42% TPF (N = 255) PF (N = 246) Log-rank p =.004 HR = TPF 49% PF 37% Time (mos) Time (mos) TPF significantly improves survival and PFS compared with PF in an ICT regimen TPF significantly followed by CRT improves survival and PFS compared with PF in an ICT regimen followed by CRT Posner et al, Posner. N Engl J Med. 2007;357:1705
32 TAX 324 Phase III Trial: Docetaxel/Cisplatin/5-FU vs Cisplatin/5-FU Sequential Therapy in Advanced SCCHN: Toxicity During ICT N = 251 TPF, 243 PF During CRT N = 203 TPF, 184 PF Grade 3/4 Toxicity TPF PF Stomatitis 21% 27% Nausea 14% 14% Lethargy 5% 10% Vomiting 8% 10% Diarrhea 7% 3% Anorexia 12% 12% Neutropenia 83% 56% Febrile neutropenia 12% 7% Neutropenic infection 12% 8% Stomatitis 37% 38% Dysphagia 23% 24% Mouth, nose dryness 5% 4% Nausea 6% 6% Rash/itch 5% 2% 32 Posner MR. N Engl J Med. 2007;357(17):
33 Taxane + PF Phase III Trials Vermorken (2007) 1 Hitt (2005) 2 Chemo PF DPF PF PaPF Subjects Med PFS* 8.2 mo 11.0 mo 12 mo 20 mo Med OS* 14.5 mo 18.8 mo 37 mo 43 mo RR* 54% 68% 68% 80% P < 0.05 for all outcomes except P = 0.06 for OS in Hitt study Vermorken JB, et al. N Engl J Med. 2007;357(17): Hitt R, et al. J Clin Oncol. 2005;23(34):
34 Conclusions Overall survival advantage > 3 years with TPF sequential therapy 40.5 month improvement in median overall survival at 3 years 30% reduction in the risk of mortality (P = ) Consistent with prior phase III trial (TAX 323) Patients received a median of 3 cycles of induction chemotherapy in the TPF and PF arms. In the TPF arm, 81% of patients went on to receive CRT. Grade 3/4 treatment-emergent adverse events: Less stomatitis, thrombocytopenia, and lethargy in the TPF arm More neutropenia and febrile neutropenia (any grade) in the TPF arm 34
35 Impact of Induction Chemotherapy (CT): Opposing Views and Ongoing Controversy Pro: Allows time to optimize patient medical status; Possible customization of RT dosing based on response to treatment; provides early treatment of distant micrometastatic disease Con: Induction CT may affect adversely compliance to subsequent concurrent CT/RT or choice of CT/RT regimen; adds 2-4 months to treatment 35
36 Clinical Scenarios to Consider Induction Therapy 1. Potential distant metastasis 2. Delay in radiation simulation 3. Impending local issue (eg, airway) 4. Markedly advanced disease (eg, bulky, N2c, N2b, N3, low neck, dermal infiltration) 5. Organ preservation strategy in patients with markedly advanced disease 36
37 Neck Dissection (ND) After Chemoradiotherapy Indicated for gross residual disease Not indicated for pretreatment N1 disease that has achieved clinical complete response For pretreatment N2-3 disease, opinions vary: When pretreatment neck disease is N2-3, some centers recommend routine ND regardless of response to chemoradiotherapy. However, others will observe if a clinical complete response on PET scan 12 weeks post-therapy is achieved with chemoradiotherapy. 37 Pellitteri PK, et al. Head Neck. 2006;28(2): Ong SC, et al. J Nucl Med. 2008;49(4):
38 Adjuvant Chemoradiotherapy
39 EORTC and RTOG 9501 Phase III Trials: Adjuvant RT ± Concomitant Cisplatin Resectable SCC Oral cavity, oropharynx, hypopharynx, larynx Stage III/IV (EORTC), high risk (RTOG) Previously untreated N = 334 (EORTC) N = 459 (RTOG) Surgery R A N D O M I Z E RT+ Cisplatin (100 mg/m 2, d1,22,43) EORTC: 66 Gy over 6.5 wks RTOG: Gy over wks 39 Bernier J, et al. N Engl J Med. 2004;350(19): Cooper JS, et al. N Engl J Med. 2004;350(19):
40 Poor Risk Criteria RTOG EORTC nodes ECE +Margins Level IV/V (OC/OP) ECE +Margins Perineural disease Vascular emboli ECE = extracapsular nodal extension; OC = oral cavity; OP = oropharynx Cooper JS, et al. N Engl J Med. 2004;350(19): Bernier J, et al. N Engl J Med. 2004;350(19):
:1945-1952. 2. Cooper JS, et al. N Engl J Med. 2004;350(19):1937-1944.")
41 EORTC and RTOG 9501: Adjuvant RT ± Concomitant Cisplatin: Results OS (EORTC) 1 OS (RTOG) 2 P=0.02 P=0.19 Months After Randomization Bernier J, et al. N Engl J Med. 2004;350(19): Cooper JS, et al. N Engl J Med. 2004;350(19):
42 RTOG 9501/EORTC Which prognostic risk factors are most important? Extracapsular nodal extension and + margins: significant benefit from chemoradiotherapy Trend toward benefit for stage III-IV disease, perineural invasion, vascular embolisms, and/or clinically enlarged level IV/V lymph nodes secondary to tumors in oral cavity or oropharynx No benefit in patients with 2 or more nodes but no extracapsular extension 42 Bernier J, et al. Head Neck. 2005;27(10):
43 Survivorship /Follow-Up Assess for recurrence/2 nd primary/premalignant lesions 1st year: Q 1-3 mos 2nd year: Q 2-4 mos 3rd 5th year: Q 4-6 mos > 5 years: Q 6-12 mos TSH q 6-12 months if neck irradiated Chest imaging as indicated Speech/Swallowing evaluation/rehabilitation as indicated Counsel regarding tobacco and alcohol use Integrate general medical care Once felt disease free, imaging of primary and neck not routinely indicated unless suspicious signs or symptoms 43 NCCN Clinical Practice Guidelines in Oncology. Head and Neck Cancers. V
44 Treatment Approach Disease Extent T 1 N 0-1 or T 2 N 0 Treatment Surgery or RT T 2 N 1 or T 3-4 or N 2-3 Combined modality Recurrent or M 1 Surgery and/or RT Combined modality Chemotherapy 44
45 Palliative Chemotherapy
46 Palliative Chemotherapy Treatment for recurrent disease without surgical or radiotherapy option 1st line therapy: historically platinum-based doublet overall RR 30-40% median survival 6-9 months regardless of treatment randomized controlled trials fail to demonstrate clear improvement in OS compared to RX with single agents Active agents: cisplatin, carboplatin, 5-FU, taxanes, methotrexate, cetuximab, ifosfamide, gemcitabine (for nasopharynx cancer) and others 46 DeVita VT, et al. Cancer: Principles & Practice of Oncology. 8th ed. Lippincott Williams & Wilkins; 2008.
47 EXTREME: Study Design R A N D O M I Z E N = FU 1000 mg/m 2 d1-4 with Cisplatin 100 mg/m 2 d1 or Carboplatin AUC 5 d1 6 cycles maximum 5-FU 1000 mg/m 2 d1-4 with Cisplatin 100 mg/m 2 d1 or Carboplatin AUC 5 d1 plus Cetuximab 250 mg/m 2 /week* q 3 weeks No treatment Cetuximab POD or toxicity POD or toxicity *Loading dose of 400 mg/m 2 on week 1 47 Vermorken JB, et al. N Engl J Med. 2008;359(11):
48 EXTREME: First-Line Platinum/5-FU ± Cetuximab in Recurrent/Metastatic SCC: Survival OS Survival Probability Patients at Risk: Platinum/5-FU Cetuximab + Platinum/5-FU 7.4 mos Platinum/5-FU Cetuximab + Platinum/5-FU 10.1 mos HR (95% CI)=0.797 ( ) Strat. log-rank test: Survival Time (months) RR 18% 35% 48 Vermorken JB, et al. N Engl J Med. 2008;359(11):
49 EXTREME: Overall Survival C225+Platinum+FU Platinum+5-FU HR P-value N = 222 N = months 7.4 months Conclusion: Addition of cetuximab to standard first-line platinum-based chemotherapy improves overall survival. 49 Vermorken JB, et al. N Engl J Med. 2008;359(11):
50 Keynote 012: Pembrolizumab in Recurrent and /or Metastatic Head and Neck Carcinoma 50 Chow et al: JCO 2016
 ECOG PS 0-1 PD-L1+ (initial cohort) PD-L1+ or PD-L1- (expansion cohort)")



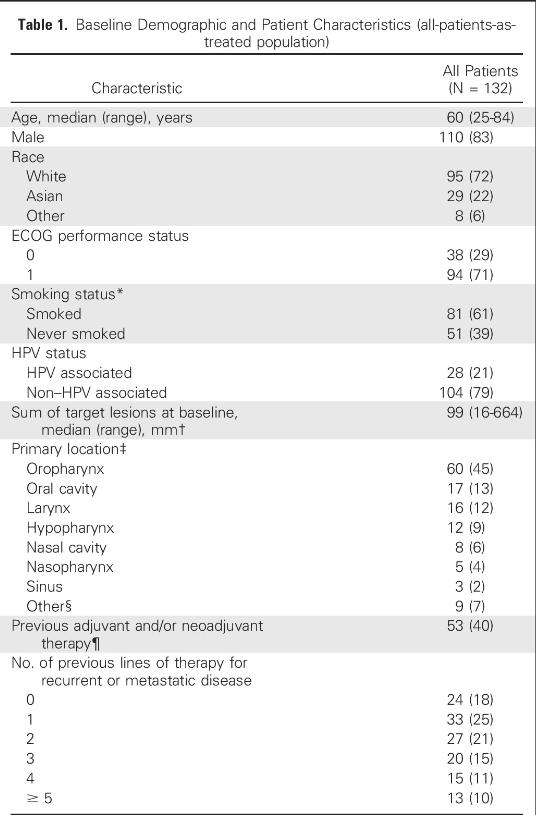
51 KEYNOTE-012 Trial Initial Cohort Patients R/M HNSCC Measurable disease (RECIST v1.1) ECOG PS 0-1 PD-L1+ (initial cohort) PD-L1+ or PD-L1- (expansion cohort) Pembrolizumab 10 mg/kg Q2W N = 60 Expansion Cohort Pembrolizumab 200 mg Q3W N = 132 Continue until: 24 months of treatment PD Intolerable toxicity Combined analyses of Initial and Expansion cohorts Response assessment: Every 8 weeks Primary end points: ORR (RECIST v1.1, central imaging vendor), safety Secondary end points: ORR (investigator), PFS, OS, response duration, ORR in HPV+ patients Additional cohorts included bladder cancer, TN breast cancer, and gastric cancer. Treatment beyond progression was allowed. Initial cohort only.
52 Baseline Demographics
53 53 Antitumor Activity of Pembrolizumab
54 Efficacy of Pembrolizumab Max change in Target lesions Median PFS 2 months Treatment exposure and Response duration in responders Median OS 8 months 54





55 CheckMate 141 Study Design Randomized, global, phase 3 trial of the efficacy and safety of nivolumab versus investigator s choice in patients with R/M SCCHN Key Eligibility Criteria R/M SCCHN of the oral cavity, pharynx, or larynx Nivolumab 3 mg/kg IV q2w Not amenable to curative therapy Progression on or within 6 months of last dose of platinum-based therapy ECOG PS 0 1 Documentation of p16 to determine HPV status No active CNS metastases Stratification factor Prior cetuximab treatment R 2:1 Investigator s Choice Methotrexate 40 mg/m² IV weekly Docetaxel 30 mg/m² IV weekly Cetuximab 400 mg/m² IV once, then 250 mg/m² weekly) Primary endpoint OS Other endpoints PFS ORR Safety DOR Biomarkers Quality of life Ferris et al : NEJM 2016 CNS, central nervous system; DOR, duration of response; ECOG PS, Eastern Cooperative Oncology Group performance status; HPV, human papillomavirus; ORR, objective response rate; OS, overall survival; PFS, progression-free survival; R, randomized; R/M, recurrent/metastatic; SCCHN, squamous cell carcinoma of the head and neck; Clinicaltrials.gov. NCT
56 Demographics (1) Nivolumab (n = 240) n (%) Investigator s Choice (n = 121) n (%) Total (N = 361) n (%) Median age (years) < (71.7) 76 (62.8) 248 (68.7) (28.3) 45 (37.2) 113 (31.3) Gender Male 197 (82.1) 103 (85.1) 300 (83.1) Race White 196 (81.7) 104 (86.0) 300 (83.1) Asian 29 (12.1) 14 (11.6) 43 (11.9) Other 15 (6.3) 3 (2.5) 18 (5.0) Smoking/tobacco use Current/former 191 (79.6) 85 (70.2) 276 (76.5) Never 39 (16.3) 31 (25.6) 70 (19.4)
57 Demographics (2) Nivolumab (n = 240) n (%) Investigator s Choice (n = 121) n (%) Total (N = 361) n (%) ECOG performance status 0 49 (20.4) 23 (19.0) 72 (19.9) (78.8) 94 (77.7) 283 (78.4) 2 1 (0.4) 3 (2.5) 4 (1.1) Not reported 1 (0.4) 1 (0.8) 2 (0.6) Number of prior lines of systemic cancer therapy (43.8) 58 (47.9) 163 (45.2) 2 81 (33.8) 45 (37.2) 126 (34.9) 3 54 (22.5) 18 (14.9) 72 (19.9) Site of primary tumor Oral cavity 108 (45.0) 67 (55.4) 175 (48.5) Pharynx 92 (38.3) 36 (29.8) 128 (35.5) Larynx 34 (14.2) 15 (12.4) 49 (13.6)
58 Treatment Administration Nivolumab (n = 240) Investigator s Choice (n = 121) Total (N = 361) Patients receiving 1 dose, n (%) 236 (98.3) 111 (91.7) 347 (96.1) Investigator s choice therapy, n (%) Methotrexate 46 (38.0) Docetaxel 52 (43.0) Cetuximab 13 (10.7) Median time on therapy, mo (95% CI) Median duration of follow-up, mo (range) 1.9 ( ) 1.9 ( ) 5.3 (0 16.8) 4.6 (0 15.2) Number of deaths, n (%) 133 (55.4) 85 (70.2) 218 (60.4) Ongoing treatment, n (%) 41 (17.4) 3 (2.7) 44 (12.7)
59 Overall Survival Median OS, mo (95% CI) HR (97.73% CI) p-value Overall Survival (% of patients) Nivolumab (n = 240) 7.5 ( ) Investigator s Choice (n = 121) 5.1 ( ) 0.70 ( ) 1-year OS rate (95% CI) 36.0% ( ) 16.6% ( ) Months No. at Risk Nivolumab Investigator s Choice
60 Conclusions : PD-1 inhibitors in SCCHN Nivolumab is the first agent to demonstrate a significant improvement in survival in patients with SCCHN who progress after platinum-based therapy in a randomized, phase 3 comparative trial Pembrolizumab has shown robust, durable antitumor activity in heavily pretreated patients with R/M HNSCC Nivolumab and Pembrolizumab demonstrated a benefit in the overall study population, regardless of PD-L1 expression or p16 status Safety profile for both agents is favorable and consistent with prior studies Nivolumab and Pembrolizumab represents a new standard of care option for patients with R/M SCCHN after platinum-based therapy
61 RAI-Refractory Thyroid Carcinoma
62 Advanced Thyroid Cancer Patients with advanced, progressive thyroid carcinoma that is refractory to radioactive iodine (RaI) have few treatment options. All types of thyroid carcinoma (papillary, follicular, medullary, and anaplastic) are poorly responsive to traditional systemic chemotherapy. A number of targeted agents are now approved or under investigation in this patient population
63 Radioactive-Iodine (RAI)-Refractory Differentiated Thyroid Cancer (DTC) It is estimated that in the USA in 2013 there will be: > new cases of thyroid cancer, and 1850 deaths due to thyroid cancer In approximately 5 15% of patients with thyroid cancer, the disease becomes refractory to RAI Median survival for patients with RAI-refractory DTC and distant metastases is estimated to be years Patients often suffer multiple complications associated with disease progression Sorafenib approved in USA in 2013 based on DECISION trial Lenvatinib approved in USA in 2015 based on SELECT trial 1. Howlader N et al. SEER Cancer Statistics Review; 2. Xing M et al. Lancet 2013; 381: ; 3. Pacini F et al. Expert Rev Endocrinol Metab 2012;7:541 54; 4. Durante C et al. J Clin Endocrinol Metab 2006;91: Robbins RJ et al. J Clin Endocrinol Metab 2006;91: Brose et al Lancet Apr 23.


64 Sorafenib in Locally Advanced or Metastatic Patients with Radioactive Iodine-refractory Differentiated Thyroid Cancer The Phase 3 DECISION Trial Brose et al : Lancet Apr 23
65 DECISION Trial: Study Design N=417 randomized from Nov 2009 to Aug 2011 Locally advanced or metastatic, RAI-refractory DTC Progression (RECIST) within the previous 14 months No prior chemotherapy, targeted therapy, or thalidomide R A N D O M I Z A T I O N 1:1 Sorafenib 400 mg orally twice daily Placebo orally twice daily Primary endpoint PFS Secondary endpoints OS Response rate Safety Time to progression Disease control rate Duration of response Stratified by Geographical region (North America, Europe, Asia) Age (<60, 60 years) Progression assessed by independent central review every 8 weeks At progression: Patients on placebo allowed to cross over at the investigator s discretion Patients on sorafenib allowed to continue on open-label sorafenib at the investigator s discretion Brose M, et al. Lancet. 2014;384:
66 DECISION Trial: Progression-Free Survival PFS Probability, % Days From Randomization n Median PFS, Days (Months) Sorafenib (10.8) Placebo (5.8) HR=0.587; 95% CI: ; P< Brose M, et al. Lancet. 2014;384:
67 DECISION Trial: Overall Survival Survival Probability, % Sorafenib Placebo Median OS Not reached Not reached HR=0.802 (95% CI: ) P=0.138, one-sided Days From Randomization At progression: 150 patients on placebo (71%) received open-label sorafenib 55 patients on sorafenib (27%) received open-label sorafenib 67 Brose M, et al. Lancet. 2014;384:
68 DECISION Trial: Response Rates Endpoints Sorafenib Placebo P Value Total evaluable patients, n (%) Response rate, n (%) 24 (12.2) 1 (0.5) < Complete response 0 0 Partial response 24 (12.2) 1 (0.5) Stable disease for 6 months, n (%) Disease control rate (CR + PR + SD 6 months), n (%) Median duration of response (PRs) (range), months 82 (41.8) 67 (33.2) 106 (54.1) 68 (33.8) < ( ) NA 68 Brose M, et al. Lancet. 2014;384:
69 DECISION Trial: Most Common Treatment-Emergent AEs Adverse Event* Sorafenib, % (n=207) Placebo, % (n=209) Any Grade Grade 3/4 Any Grade Grade 3/4 Hand-foot skin reaction Diarrhea Alopecia Rash/desquamation Fatigue Weight loss Hypertension Metabolic lab (other) Anorexia Oral mucositis Pruritus Nausea Hypocalcemia *National Cancer Institute Common Terminology Criteria for Adverse Events (NCI CTCAE) version Brose M, et al. Lancet. 2014;384:
70 Summary: DECISION Trial Approved by FDA 2013 Sorafenib significantly improved PFS and extended median PFS by 5 months vs. placebo 10.8 vs 5.8 months Safety results are consistent with the known safety profile of sorafenib
71 SELECT Trial Study of (E7080) LEnvatinib in Differentiated Cancer of the Thyroid (SELECT) Schlumberger M et al : NEJM 2015
72 SELECT Trial (Study 303): Study Design Global, randomized, double-blind, phase III trial Patients with DTC (N=392) IRR evidence of progression within previous 13 months 131 I-refractory disease Measurable disease Up to 1 prior VEGF- or VEGFR-targeted therapy R A N D O M I Z A T I O N Lenvatinib (n=261) 24 mg daily po Treatment until disease progression confirmed by IRR (RECIST v1.1) Placebo (n=131) 24 mg daily po Primary endpoint PFS Secondary endpoints ORR OS Safety Lenvatinib (optional, open-label) Stratified by Geographic region (Europe, North America, other) Prior VEGF-/VEGFR-targeted therapy (0, 1) Age ( 65, >65 years) 72 IRR=independent radiologic review; ORR=objective response rate; RECIST=Response Evaluation Criteria in Solid Tumors.
 Log-rank test: P<0.")
73 SELECT Trial: Primary Endpoint, Kaplan-Meier Estimate of PFS Median PFS (95% CI), Months Lenvatinib 18.3 (15.1-NR) Progression-Free Survival, Proportion Placebo 3.6 ( ) HR (99% CI): 0.21 ( ) Log-rank test: P< Progression events, 86% Progression events, 41% Time, Months Number of patients at risk: Lenvatinib Placebo NR=not reached. Schlumberger M, et al. NEJM 2015
74 SELECT Trial: PFS by Previous VEGF-Targeted Therapy Progression-Free Survival, Proportion No Previous VEGF-Targeted Therapy (n=299) Time, Months Number of patients at risk: Lenvatinib Placebo Lenvatinib Median PFS (95% CI), Months 18.7 (16.4-NR) Placebo 3.6 ( ) HR (95% CI): 0.20 ( ) Log-rank test: P< Progression-Free Survival, Proportion Previous VEGF-Targeted Therapy: 1 Line (n=93) Time, Months Number of patients at risk: Lenvatinib Placebo Lenvatinib Median PFS (95% CI), Months 15.1 (8.8-NR) Placebo 3.6 ( ) HR (95% CI): 0.22 ( ) Log-rank test: P<0.0001
75 SELECT Trial: OS, ITT Population Overall Survival, Proportion No significant difference was observed in the RPSFT adjusted OS (secondary endpoint; P=0.051), which was used to correct for a potential crossover effect in the placebo arm Lenvatinib Placebo Median OS (95% CI), Months NR (22.0-NR) NR (20.3-NR) Number of subjects at risk: Time, Months Lenvatinib Placebo (95.6%) of 114 eligible placebo patients received open-label lenvatinib post progression ITT=intent-to-treat; IRR=independent radiologic review; RPSFT=rank-preserving structural failure time. Schlumberger M, et al. NEJM 2015
76 SELECT Trial: PFS Subgroup Analyses Baseline Tumor Events/N Median, Months HR (95% CI) Lenvatinib Placebo Lenvatinib Placebo Burden, mm 35 14/65 21/ ( ) NR /72 31/ ( ) /63 31/ ( ) >92 31/61 30/ ( ) Histology Papillary 61/141 60/ ( ) Poorly differentiated 14/28 18/ ( ) Follicular 32/92 35/ ( ) NR 3.7 Bone metastasis No 60/157 74/ ( ) Yes 47/104 39/ ( ) Lung metastasis No 17/35 7/ ( ) Yes 90/ / ( ) NR=not reached. Schlumberger M, et al. NEJM Favors Lenvatinib Favors Placebo HR and 95% CI
77 SELECT Trial: Response Rates Lenvatinib (n=261) Placebo (n=131) ORR, n (%) 169 (65) 2 (2) [95% CI] [ ] [ ] P value < Complete response, n (%) 4 (2) 0 Partial response, n (%) 165 (63) 2 (2) Stable disease 23 weeks, n (%) 40 (15) 39 (30) Progressive disease, n (%) 18 (7) 52 (40) Median time to objective response (95% CI), months* Duration of response (95% CI), months* 2.0 ( ) NR (16.8-NR) *Nonresponders were not included in the median time to response assessment. Schlumberger M, et al. NEJM 2015
78 SELECT Trial: Treatment-Emergent Adverse Events (TEAEs) Lenvatinib, n (%) (n=261) Placebo, n (%) (n=131) TEAE 260 (>99) 118 (90) TEAE reported as treatment related 254 (97) 78 (60) Serious TEAEs 133 (51) 31 (24) TEAE resulting in Dose reduction 177 (68) 6 (5) Dose interruption 215 (82) 24 (18) Discontinuation of treatment 37 (14) 3 (2.3) Fatal TEAE 20 (8) 6 (5) Fatal TEAE reported by investigator as treatment related 6 (2) 0 6/20 lenvatinib treatment-emergent deaths were considered by investigator as treatment related: Pulmonary embolism (n=1); hemorrhagic stroke (n=1); general health deterioration (n=4)
79 Most Frequent Treatment-Related AEs (>20%) Adverse Event Lenvatinib, % (n=261) Placebo, % (n=131) Any Grade Grade 3 Any Grade Grade 3 Hypertension Diarrhea Fatigue/asthenia Decreased appetite Nausea/vomiting Decreased weight Stomatitis Palmar-plantar erythrodysesthesia syndrome Proteinuria Headache Dysphonia Schlumberger M, et al. NEJM 2015
80 SELECT Trial: Conclusions In patients with RR-DTC, lenvatinib significantly prolonged median PFS by 14.7 months compared with placebo: Lenvatinib, median PFS: 18.3 months (95% CI, 15.1-NR months) Placebo, median PFS: 3.6 months (95% CI, months) HR=0.21 (99% CI, ) Response rates for lenvatinib vs placebo, respectively, were: ORR: 65% vs 2% (with CR: 2% vs 0%) The median time to objective response for lenvatinib was 2.0 months (95% CI, months) The median duration of response for lenvatinib has not been reached 75% of responders had an objective response >9.4 months Main toxicities: hypertension, proteinuria, diarrhea, fatigue, and weight loss 80
81 Summary of Advanced Thyroid Cancer Trials Targeted Therapy Compound Targets Clinical Trials Vandetanib Cabozantinib RET, VEGFR, EGFR RET, MET, VEGFR2, c-kit Approved MTC Approved MTC Sunitinib VEGFR-2, PDGFR, c-kit, RET Phase II Gefitinib EGFR Phase II Sorafenib VEGFR-2/3, BRAF, PDGFR, RET Approved DTC Lenvatinib VEGFR-1/2, PDGFR, FGFR-1 Approved DTC Motesanib VEGFR, PDGFR, c-kit, RET Phase II Pazopanib VEGFR, PDGFR, c-kit Phase II Depsipeptide HDAC inhibitor Phase II Everolimus mtor Phase II Vemurafenib BRAF Phase II Dabrafenib BRAF Phase II
82 Conclusions - 1 RAIR-DTC is a therapeutic challenge New agents are available VEGF, mtor inhibitors are active agents Lenvatinib and Sorafenib are now FDA approved. Many other agents currently in phase III

83 DTC can be an indolent disease Conclusions - 2 Many patients do not require therapy immediately Great deal of judgment should be exercised on when to initiate therapy 1- Rapidly growing disease 2- Symptomatic disease Drug-related toxicity can be significant and close monitoring is required
Recent Advances & Ongoing Challenges in Head & Neck Cancers
 Recent Advances & Ongoing Challenges in Head & Neck Cancers Robert Haddad, MD Disease Center Leader Head and Neck Oncology Program Dana Farber Cancer Institute Harvard Medical School Boston, MA Disclosures
Recent Advances & Ongoing Challenges in Head & Neck Cancers Robert Haddad, MD Disease Center Leader Head and Neck Oncology Program Dana Farber Cancer Institute Harvard Medical School Boston, MA Disclosures
Head, Neck, and Thyroid Cancers: Evidence-Based Approaches to Multimodal Management
 Head, Neck, and Thyroid Cancers: Evidence-Based Approaches to Multimodal Management Robert Haddad, MD Disease Center Leader Head and Neck Oncology Program Dana Farber Cancer Institute Harvard Medical School
Head, Neck, and Thyroid Cancers: Evidence-Based Approaches to Multimodal Management Robert Haddad, MD Disease Center Leader Head and Neck Oncology Program Dana Farber Cancer Institute Harvard Medical School
Carcinoma de Tiroide: Teràpies Diana
 Carcinoma de Tiroide: Teràpies Diana Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology THYROID CANCER:
Carcinoma de Tiroide: Teràpies Diana Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology THYROID CANCER:
Emerging Role of Immunotherapy in Head and Neck Cancer
 Emerging Role of Immunotherapy in Head and Neck Cancer Jared Weiss, MD Associate Professor of Medicine and Section Chief of Thoracic and Head/Neck Oncology UNC Lineberger Comprehensive Cancer Center Copyright
Emerging Role of Immunotherapy in Head and Neck Cancer Jared Weiss, MD Associate Professor of Medicine and Section Chief of Thoracic and Head/Neck Oncology UNC Lineberger Comprehensive Cancer Center Copyright
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers. Barbara Burtness, MD Yale University
 Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
Immunotherapy for the Treatment of Head and Neck Cancers Barbara Burtness, MD Yale University Disclosures AstraZeneca Pharmaceuticals LP, Boehringer Ingelheim, Bristol-Myers Squibb, Merck & Co., Inc.,
New Paradigms for Treatment of. Erminia Massarelli, MD, PHD, MS Clinical Associate Professor
 New Paradigms for Treatment of Head and Neck cancers Erminia Massarelli, MD, PHD, MS Clinical Associate Professor City of Hope Disclosure Statement Grant/Research Support frommerck Bristol Grant/Research
New Paradigms for Treatment of Head and Neck cancers Erminia Massarelli, MD, PHD, MS Clinical Associate Professor City of Hope Disclosure Statement Grant/Research Support frommerck Bristol Grant/Research
Adjuvant Therapy in Locally Advanced Head and Neck Cancer. Ezra EW Cohen University of Chicago. Financial Support
 Adjuvant Therapy in Locally Advanced Head and Neck Cancer Ezra EW Cohen University of Chicago Financial Support This program is made possible by an educational grant from Eli Lilly Oncology, who had no
Adjuvant Therapy in Locally Advanced Head and Neck Cancer Ezra EW Cohen University of Chicago Financial Support This program is made possible by an educational grant from Eli Lilly Oncology, who had no
Locally advanced head and neck cancer
 Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
Locally advanced head and neck cancer Radiation Oncology Perspective Petek Erpolat, MD Gazi University, Turkey Definition and Management of LAHNC Stage III or IV cancers generally include larger primary
The PARADIGM Study: A Phase III Study Comparing Sequential Therapy (ST) to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer
 to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer") The PARADIGM Study: A Phase III Study Comparing Sequential Therapy (ST) to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer Robert I. Haddad, Guilherme Rabinowits, Roy B. Tishler,
The PARADIGM Study: A Phase III Study Comparing Sequential Therapy (ST) to Concurrent Chemoradiotherapy (CRT) in Locally Advanced Head and Neck Cancer Robert I. Haddad, Guilherme Rabinowits, Roy B. Tishler,
Head and Neck Cancer:
 Head and Neck Cancer: Robert Haddad M.D. Clinical Director Head and Neck Oncology Program Dana Farber Cancer Institute Boston, MA Predictive Biomarkers: HPV Abstract 6003: Survival Outcomes By HPV Status
Head and Neck Cancer: Robert Haddad M.D. Clinical Director Head and Neck Oncology Program Dana Farber Cancer Institute Boston, MA Predictive Biomarkers: HPV Abstract 6003: Survival Outcomes By HPV Status
HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view. Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium
 HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium DISCLOSURE OF INTEREST Nothing to declare HEAD AND NECK CANCER -HPV
HPV INDUCED OROPHARYNGEAL CARCINOMA radiation-oncologist point of view Prof. dr. Sandra Nuyts Dep. Radiation-Oncology UH Leuven Belgium DISCLOSURE OF INTEREST Nothing to declare HEAD AND NECK CANCER -HPV
Medicinae Doctoris. One university. Many futures.
 Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
Medicinae Doctoris The Before and The After: Can chemotherapy revise the trajectory of gastric and esophageal cancers? Dr. David Dawe MD, FRCPC Medical Oncologist Assistant Professor Disclosures None All
State of the Art: Management of Squamous Cell Carcinoma of the Head and Neck. Raul Giglio
 State of the Art: Management of Squamous Cell Carcinoma of the Head and Neck Raul Giglio Disclosures Nothing to disclose SCCHN Outline 1. General considerations: MTD 2. Epidemiology 3. Locoregional disease
State of the Art: Management of Squamous Cell Carcinoma of the Head and Neck Raul Giglio Disclosures Nothing to disclose SCCHN Outline 1. General considerations: MTD 2. Epidemiology 3. Locoregional disease
De-Escalate Trial for the Head and neck NSSG. Dr Eleanor Aynsley Consultant Clinical Oncologist
 De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
De-Escalate Trial for the Head and neck NSSG Dr Eleanor Aynsley Consultant Clinical Oncologist 3 HPV+ H&N A distinct disease entity Leemans et al., Nature Reviews, 2011 4 Good news Improved response to
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Metastatic NSCLC: Expanding Role of Immunotherapy. Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian
 Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
Metastatic NSCLC: Expanding Role of Immunotherapy Evan W. Alley, MD, PhD Abramson Cancer Center at Penn Presbyterian Disclosures: No relevant disclosures Please note that some of the studies reported in
1 st Appraisal Committee meeting Background & Clinical Effectiveness Gillian Ells & Malcolm Oswald 24/11/2016
 Lead team presentation Nivolumab for treating recurrent or metastatic squamous-cell carcinoma of the head and neck after platinum-based chemotherapy [ID971] 1 st Appraisal Committee meeting Background
Lead team presentation Nivolumab for treating recurrent or metastatic squamous-cell carcinoma of the head and neck after platinum-based chemotherapy [ID971] 1 st Appraisal Committee meeting Background
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC)
") Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Chemotherapy and Immunotherapy in Combination Non-Small Cell Lung Cancer (NSCLC) Jeffrey Crawford, MD George Barth Geller Professor for Research in Cancer Co-Program Leader, Solid Tumor Therapeutics Program
Head and Neck cancer
 Head and Neck cancer Medical Oncologist s Role in Multidisciplinary Teams - Focus on Adjuvant & Neo-adjuvant Therapy - Hye Ryun Kim, M.D. Yonsei Cancer Center, Medical Oncology Contents I. Introduction
Head and Neck cancer Medical Oncologist s Role in Multidisciplinary Teams - Focus on Adjuvant & Neo-adjuvant Therapy - Hye Ryun Kim, M.D. Yonsei Cancer Center, Medical Oncology Contents I. Introduction
News Briefing: Highlights from the 2018 Multidisciplinary Head and Neck Cancers Symposium. Tuesday, February 13, 2018
 News Briefing: Highlights from the 2018 Multidisciplinary Head and Neck Cancers Symposium Tuesday, February 13, 2018 News Briefing: Highlights from the 2018 Multidisciplinary Head and Neck Cancers Symposium
News Briefing: Highlights from the 2018 Multidisciplinary Head and Neck Cancers Symposium Tuesday, February 13, 2018 News Briefing: Highlights from the 2018 Multidisciplinary Head and Neck Cancers Symposium
ASCO Highlights Head and Neck Cancer
 ASCO Highlights Head and Neck Cancer Anne S. Tsao, M.D. Director, Mesothelioma Program Assistant Professor July 11, 2009 The University of Texas MD ANDERSON CANCER CENTER Department of Thoracic/Head &
ASCO Highlights Head and Neck Cancer Anne S. Tsao, M.D. Director, Mesothelioma Program Assistant Professor July 11, 2009 The University of Texas MD ANDERSON CANCER CENTER Department of Thoracic/Head &
Sequencing Chemo with Radiation therapy Locally Advanced Head and Neck Cancer. Dr P Vijay Anand Reddy Director Apollo Cancer Hospital
 Sequencing Chemo with Radiation therapy Locally Advanced Head and Neck Cancer Dr P Vijay Anand Reddy Director Apollo Cancer Hospital H&N Ca - Disease Burden 15-20% of all cancers in India, 8% worldwide
Sequencing Chemo with Radiation therapy Locally Advanced Head and Neck Cancer Dr P Vijay Anand Reddy Director Apollo Cancer Hospital H&N Ca - Disease Burden 15-20% of all cancers in India, 8% worldwide
Update on the development of immune checkpoint inhibitors
 Update on the development of immune checkpoint inhibitors Jean-Pascal Machiels Department of Medical Oncology Laboratory of Medical Oncology Cliniques universitaires Saint-Luc Université catholique de
Update on the development of immune checkpoint inhibitors Jean-Pascal Machiels Department of Medical Oncology Laboratory of Medical Oncology Cliniques universitaires Saint-Luc Université catholique de
Pre- Versus Post-operative Radiotherapy
 Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Postoperative Radiation and Chemoradiation: Indications and Optimization of Practice Dislosures Clinical trial support from Genentech Inc. Sue S. Yom, MD, PhD Associate Professor UCSF Radiation Oncology
Head and NeckCancer: multi-modal therapeuticintegration
 Head and NeckCancer: multi-modal therapeuticintegration P. Ponticelli, L. Lastrucci, R. De Majo, A. Rampini U.O.C. Radioterapia Ospedale S. Donato ASL 8 -AREZZO Summary Biological considerations Clinical
Head and NeckCancer: multi-modal therapeuticintegration P. Ponticelli, L. Lastrucci, R. De Majo, A. Rampini U.O.C. Radioterapia Ospedale S. Donato ASL 8 -AREZZO Summary Biological considerations Clinical
Laryngeal and hypopharyngeal cancers
 Laryngeal and hypopharyngeal cancers Induction Chemotherapy in combined modality approaches Atenas 16.09.2017 Ana Ferreira Castro, MD Medical Oncology Centro Hospitalar do Porto Instituto de Ciências Biomédicas
Laryngeal and hypopharyngeal cancers Induction Chemotherapy in combined modality approaches Atenas 16.09.2017 Ana Ferreira Castro, MD Medical Oncology Centro Hospitalar do Porto Instituto de Ciências Biomédicas
Immunotherapy in head and neck cancer and MSI in solid tumors
 Immunotherapy in head and neck cancer and MSI in solid tumors Brian Hunis, MD, MBA Associate Medical Director, Memorial Cancer Institute. Hollywood, FL »No disclosures Objectives»Discuss the role of immunology
Immunotherapy in head and neck cancer and MSI in solid tumors Brian Hunis, MD, MBA Associate Medical Director, Memorial Cancer Institute. Hollywood, FL »No disclosures Objectives»Discuss the role of immunology
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER
 CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
CURRENT STANDARD OF CARE IN NASOPHARYNGEAL CANCER Jean-Pascal Machiels Department of medical oncology Institut I Roi Albert II Cliniques universitaires Saint-Luc Université catholique de Louvain, Brussels,
MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS
 MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS Kyle Arneson, MD PhD Avera Medical Group Radiation Oncology Avera Cancer Institute 16 th Annual Oncology Symposium September
MANAGEMENT OF LOCALLY ADVANCED OROPHARYNGEAL CANER: HPV AND NON-HPV MEDIATED CANCERS Kyle Arneson, MD PhD Avera Medical Group Radiation Oncology Avera Cancer Institute 16 th Annual Oncology Symposium September
Concurrent Chemo- and Radiotherapy for Ororpharynx Cancer
 Concurrent Chemo- and Radiotherapy for Ororpharynx Cancer Faye Johnson MD, PhD Associate Professor Thoracic/Head and Neck Medical Oncology August 2017 Objectives Review data that support concurrent chemo-
Concurrent Chemo- and Radiotherapy for Ororpharynx Cancer Faye Johnson MD, PhD Associate Professor Thoracic/Head and Neck Medical Oncology August 2017 Objectives Review data that support concurrent chemo-
Neoadjuvant Chemotherapy in Locally Advanced Squamous Cell Cancer of Head and Neck. Mei Tang, MD
 Neoadjuvant Chemotherapy in Locally Advanced Squamous Cell Cancer of Head and Neck Mei Tang, MD Head and Neck Cancer Worldwide New cases : 644,000 Cancer deaths: 350,000 About 5% of all cancers Local Recurrence:
Neoadjuvant Chemotherapy in Locally Advanced Squamous Cell Cancer of Head and Neck Mei Tang, MD Head and Neck Cancer Worldwide New cases : 644,000 Cancer deaths: 350,000 About 5% of all cancers Local Recurrence:
Nasopharyngeal Cancer/Multimodality Treatment
 Nasopharyngeal Cancer/Multimodality Treatment PANAGIOTIS KATSAOUNIS Medical Oncologist IASO GENERAL HOSPITAL Athens, 22/10/2016 1 st Hellenic Multidisciplinary Conference on Head and Neck Cancer INTRODUCTION
Nasopharyngeal Cancer/Multimodality Treatment PANAGIOTIS KATSAOUNIS Medical Oncologist IASO GENERAL HOSPITAL Athens, 22/10/2016 1 st Hellenic Multidisciplinary Conference on Head and Neck Cancer INTRODUCTION
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist
 Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
Non-small Cell Lung Cancer: Multidisciplinary Role: Role of Medical Oncologist Vichien Srimuninnimit, MD. Medical Oncology Division Faculty of Medicine, Siriraj Hospital Outline Resectable NSCLC stage
State of the art for radiotherapy of SCCHN
 State of the art for radiotherapy of SCCHN Less side effects Cured More organ & function preservation Head & neck cancer = 42 000 new cases / year in Europe Not cured Local failure Distant failure More
State of the art for radiotherapy of SCCHN Less side effects Cured More organ & function preservation Head & neck cancer = 42 000 new cases / year in Europe Not cured Local failure Distant failure More
Disclosures. Immunotherapyin Head & NeckCancer. Actual landscape of systemic treatment in HNSCC. Head andneckcanceris an immunogeneic tumor
 Immunotherapyin Head & NeckCancer Disclosures Astra-Zeneca/medimmune: clinical trial BMS: advisory board, clinical trial Merck: advisory board, clinical trial, research funding Carla van Herpen Medical
Immunotherapyin Head & NeckCancer Disclosures Astra-Zeneca/medimmune: clinical trial BMS: advisory board, clinical trial Merck: advisory board, clinical trial, research funding Carla van Herpen Medical
Practice teaching course on head and neck cancer management
 28-29 October 2016 - Saint-Priest en Jarez, France Practice teaching course on head and neck cancer management IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org Nicolas Magné France
28-29 October 2016 - Saint-Priest en Jarez, France Practice teaching course on head and neck cancer management IMPROVING THE PATIENT S LIFE THROUGH MEDICAL EDUCATION www.excemed.org Nicolas Magné France
RT +/- Surgery. Concurrent ChemoRT +/- Surgery
 Molecular targeted approaches to head and neck cancer Lillian L. Siu Department of Medical Oncology & Hematology Princess Margaret Hospital, University of Toronto Locally Advanced HNSCC Locally Advanced
Molecular targeted approaches to head and neck cancer Lillian L. Siu Department of Medical Oncology & Hematology Princess Margaret Hospital, University of Toronto Locally Advanced HNSCC Locally Advanced
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr.
 Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
Immune Checkpoint Inhibitors for Lung Cancer William N. William Jr. Diretor de Onco-Hematologia Hospital BP, A Beneficência Portuguesa Non-Small Cell Lung Cancer PD-1/PD-L1 Inhibitors in second-line therapy
GASTRIC & PANCREATIC CANCER
 GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
GASTRIC & PANCREATIC CANCER ASCO HIGHLIGHTS 2005 Fadi Sami Farhat, MD Head of Hematology Oncology Division Hammoud Hospital University Medical Center Saida Lebanon Tel: +961 3 753 155 E-Mail: drfadi@drfadi.org
Practice changing studies in lung cancer 2017
 1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
1 Practice changing studies in lung cancer 2017 Rolf Stahel University Hospital of Zürich Cape Town, February 16, 2018 DISCLOSURE OF INTEREST Consultant or Advisory Role in the last two years I have received
Laryngeal Preservation Using Radiation Therapy. Chemotherapy and Organ Preservation
 1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
1 Laryngeal Preservation Using Radiation Therapy 1903: Schepegrell was the first to perform radiation therapy for the treatment of laryngeal cancer Conventional external beam radiation produced disappointing
SAMO MASTERCLASS HEAD & NECK CANCER. Nicolas Mach, PD Geneva University Hospital
 SAMO MASTERCLASS HEAD & NECK CANCER Nicolas Mach, PD Geneva University Hospital Epidemiology Prevention Best treatment for localized disease Best treatment for relapsed or metastatic disease Introduction
SAMO MASTERCLASS HEAD & NECK CANCER Nicolas Mach, PD Geneva University Hospital Epidemiology Prevention Best treatment for localized disease Best treatment for relapsed or metastatic disease Introduction
Head and Neck Reirradiation: Perils and Practice
 Head and Neck Reirradiation: Perils and Practice David J. Sher, MD, MPH Department of Radiation Oncology Dana-Farber Cancer Institute/ Brigham and Women s Hospital Conflicts of Interest No conflicts of
Head and Neck Reirradiation: Perils and Practice David J. Sher, MD, MPH Department of Radiation Oncology Dana-Farber Cancer Institute/ Brigham and Women s Hospital Conflicts of Interest No conflicts of
EGFR inhibitors in NSCLC
 Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Suresh S. Ramalingam, MD Associate Professor Director of Medical Oncology Emory University i Winship Cancer Institute EGFR inhibitors in NSCLC Role in 2nd/3 rd line setting Role in first-line and maintenance
Targeted Agents as Maintenance Therapy. Karen Kelly, MD Professor of Medicine UC Davis Cancer Center
 Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Targeted Agents as Maintenance Therapy Karen Kelly, MD Professor of Medicine UC Davis Cancer Center Disclosures Genentech Advisory Board Maintenance Therapy Defined Treatment Non-Progressing Patients Drug
Lenvatinib and sorafenib for treating differentiated thyroid cancer after radioactive iodine [ID1059]
![Lenvatinib and sorafenib for treating differentiated thyroid cancer after radioactive iodine [ID1059]](/thumbs/79/79823924.jpg "Lenvatinib and sorafenib for treating differentiated thyroid cancer after radioactive iodine [ID1059]") Contains AIC Lenvatinib and sorafenib for treating differentiated thyroid cancer after radioactive iodine [ID1059] Multiple Technology Appraisal Background and Clinical Effectiveness Lead team: Femi Oyebode
Contains AIC Lenvatinib and sorafenib for treating differentiated thyroid cancer after radioactive iodine [ID1059] Multiple Technology Appraisal Background and Clinical Effectiveness Lead team: Femi Oyebode
Nasopharyngeal Cancer:Role of Chemotherapy
 Nasopharyngeal Cancer:Role of Chemotherapy PANAGIOTIS KATSAOUNIS Medical Oncologist IASO GENERAL HOSPITAL Athens, 16/9/2017 2 nd Hellenic Multidisciplinary Conference on Head and Neck Cancer INTRODUCTION
Nasopharyngeal Cancer:Role of Chemotherapy PANAGIOTIS KATSAOUNIS Medical Oncologist IASO GENERAL HOSPITAL Athens, 16/9/2017 2 nd Hellenic Multidisciplinary Conference on Head and Neck Cancer INTRODUCTION
Therapy of Locally Advanced Head and Neck Cancer: State of the Art
 Therapy of Locally Advanced Head and Neck Cancer: State of the Art Barbara Burtness, MD Chief, Head and Neck ncology Medical ncology Co-Leader Senior Member Fox Chase Cancer Center Philadelphia, PA Therapy
Therapy of Locally Advanced Head and Neck Cancer: State of the Art Barbara Burtness, MD Chief, Head and Neck ncology Medical ncology Co-Leader Senior Member Fox Chase Cancer Center Philadelphia, PA Therapy
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón
 Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT
 Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT David H. Ilson, MD, PhD Gastrointestinal Oncology Service Memorial Sloan Kettering Cancer Center Disclosure Consulting
Management of Squamous Cell Cancer of the Esophagus: Surgery Should Follow Chemo + RT David H. Ilson, MD, PhD Gastrointestinal Oncology Service Memorial Sloan Kettering Cancer Center Disclosure Consulting
NSCLC: immunotherapy as a first-line treatment. Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To)
") NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
NSCLC: immunotherapy as a first-line treatment Paolo Bironzo Oncologia Polmonare AOU S. Luigi Gonzaga Orbassano (To) The 800-pound gorilla Platinum-based chemotherapy is the SOC for 1st-line therapy in
Immunotherapy for Breast Cancer. Aurelio B. Castrellon Medical Oncology Memorial Healthcare System
 Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Immunotherapy for Breast Cancer Aurelio B. Castrellon Medical Oncology Memorial Healthcare System Conflicts Research support : Cascadian therapeutics, Puma biotechnology, Odonate therapeutics, Pfizer,
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221. Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS
 Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
Clinical Trials in Transoral Endoscopic Head &Neck Surgery ECOG3311 and RTOG1221 Chris Holsinger, MD, FACS Bob Ferris, MD, PhD, FACS 1 Disclosure I have no conflicts of interest to disclose 2 Robotic H&N
Multimodular treatment in Head and Neck Squamous Cell Carcinoma (HNSCC)
") Multimodular treatment in Head and Neck Squamous Cell Carcinoma (HNSCC) Amanda Psyrri, MD,FACP Attikon University Hospital Athens, Greece Learning objectives After reading and reviewing this material,
Multimodular treatment in Head and Neck Squamous Cell Carcinoma (HNSCC) Amanda Psyrri, MD,FACP Attikon University Hospital Athens, Greece Learning objectives After reading and reviewing this material,
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective
 Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Management Guidelines and Targeted Therapies in Metastatic Non-Small Cell Lung Cancer: An Oncologist s Perspective Julie R. Brahmer, M.D. Associate Professor of Oncology The Sidney Kimmel Comprehensive
Medullary Thyroid Carcinoma: New Therapies and Trials
 Medullary Thyroid Carcinoma: New Therapies and Trials Matthew D. Ringel, MD Ralph W. Kurtz Chair and Professor of Medicine Director, Division of Endocrinology, Diabetes, and Metabolism The Ohio State University
Medullary Thyroid Carcinoma: New Therapies and Trials Matthew D. Ringel, MD Ralph W. Kurtz Chair and Professor of Medicine Director, Division of Endocrinology, Diabetes, and Metabolism The Ohio State University
Update on Head and Neck Cancer Outline. Presenter Disclosure Information. Head and Neck Cancer Primary Disease Sites. Epidemiology
 Welcome to Master Class for Oncologists Miami, FL December 19, 2009 Session 5: 4:30 PM - 5:15 PM Head and Neck Cancer: Update on Comprehensive Management Speaker: David G. Pfister, MD Chief, Head & Neck
Welcome to Master Class for Oncologists Miami, FL December 19, 2009 Session 5: 4:30 PM - 5:15 PM Head and Neck Cancer: Update on Comprehensive Management Speaker: David G. Pfister, MD Chief, Head & Neck
Neoplasie del laringe Diagnosi e trattamento
 Neoplasie del laringe Diagnosi e trattamento Venerdì 22 maggio 2015 Alessandria Trattamenti non chirurgici: Preservazione d organo, malattia localmente avanzata Marco C Merlano A.O. S.Croce e Carle, Ospedale
Neoplasie del laringe Diagnosi e trattamento Venerdì 22 maggio 2015 Alessandria Trattamenti non chirurgici: Preservazione d organo, malattia localmente avanzata Marco C Merlano A.O. S.Croce e Carle, Ospedale
The next wave of successful drug therapy strategies in HER2-positive breast cancer. Hans Wildiers University Hospitals Leuven Belgium
 The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
The next wave of successful drug therapy strategies in HER2-positive breast cancer Hans Wildiers University Hospitals Leuven Belgium Trastuzumab in 1st Line significantly improved the prognosis of HER2-positive
METRIC Study Key Eligibility Criteria
 The METRIC Study METRIC Study Key Eligibility Criteria The pivotal METRIC Study is evaluating glembatumumab vedotin in patients with gpnmb overexpressing metastatic triple-negative breast cancer (TNBC).
The METRIC Study METRIC Study Key Eligibility Criteria The pivotal METRIC Study is evaluating glembatumumab vedotin in patients with gpnmb overexpressing metastatic triple-negative breast cancer (TNBC).
Immune checkpoint blockade in lung cancer
 Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
Immune checkpoint blockade in lung cancer Raffaele Califano Department of Medical Oncology The Christie and University Hospital of South Manchester, Manchester, UK Outline Background Overview of the data
3/8/2014. Case Presentation. Primary Treatment of Anal Cancer. Anatomy. Overview. March 6, 2014
 Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Case Presentation Primary Treatment of Anal Cancer 65 year old female presents with perianal pain, lower GI bleeding, and anemia with Hb of 7. On exam 6 cm mass protruding through the anus with bulky R
Combined Modality Therapy State of the Art. Everett E. Vokes The University of Chicago
 Combined Modality Therapy State of the Art Everett E. Vokes The University of Chicago What we Know Some patients are cured (20%) Induction and concurrent chemoradiotherapy are each superior to radiotherapy
Combined Modality Therapy State of the Art Everett E. Vokes The University of Chicago What we Know Some patients are cured (20%) Induction and concurrent chemoradiotherapy are each superior to radiotherapy
Organ-Preservation Strategies in head and neck cancer. Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari
 Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Organ-Preservation Strategies in head and neck cancer Teresa Bonfill Abella Oncologia Mèdica Parc Taulí Sabadell. Hospital Universitari Larynx Hypopharynx The goal of treatment is to achieve larynx preservation
Cetuximab/cisplatin and radiotherapy in HNSCC: is there a favorite choice?
 Cent. Eur. J. Med. 9(2) 2014 279-284 DOI: 10.2478/s11536-013-0154-9 Central European Journal of Medicine Cetuximab/cisplatin and radiotherapy in HNSCC: is there a favorite choice? Jacopo Giuliani* 1, Marina
Cent. Eur. J. Med. 9(2) 2014 279-284 DOI: 10.2478/s11536-013-0154-9 Central European Journal of Medicine Cetuximab/cisplatin and radiotherapy in HNSCC: is there a favorite choice? Jacopo Giuliani* 1, Marina
A Case Review: Treatment-Naïve Patient with Head and Neck Cancer
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID
 DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
DR LUIS MANSO UNIDAD TUMORES DE MAMA Y GINECOLÓGICOS HOSPITAL 12 DE OCTUBRE MADRID RESUMEN DE ARTICULOS THERESA BOLERO 3 NOAH UP-DATE GEPAR SIXTO RADIOTHERAPY EBCTCG CTCs MISCELANEAS Lancet Oncol 2014;
Recent advances in the management of metastatic breast cancer in older adults
 Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Recent advances in the management of metastatic breast cancer in older adults Laura Biganzoli Medical Oncology Dept New Hospital of Prato Istituto Toscano Tumori Italy Important recent advances in the
Head and Neck Cancer Update Sandro V Porceddu
 Head and Neck Cancer Update Sandro V Porceddu Director, Radiation Oncology Research Princess Alexandra Hospital, Brisbane Associate Professor, University of Queensland President, Trans Tasman Radiation
Head and Neck Cancer Update Sandro V Porceddu Director, Radiation Oncology Research Princess Alexandra Hospital, Brisbane Associate Professor, University of Queensland President, Trans Tasman Radiation
MANAGEMENT OF THYROID MALIGNANCIES
 MANAGEMENT OF THYROID MALIGNANCIES Taofeek K. Owonikoko, MD, PhD Associate Professor Department of Hematology/Medical Oncology Winship Cancer Institute of Emory University Atlanta, GA 1 Disclosures Research
MANAGEMENT OF THYROID MALIGNANCIES Taofeek K. Owonikoko, MD, PhD Associate Professor Department of Hematology/Medical Oncology Winship Cancer Institute of Emory University Atlanta, GA 1 Disclosures Research
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer
 Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Reflex Testing Guidelines for Immunotherapy in Non-Small Cell Lung Cancer Jimmy Ruiz, MD Assistant Professor Thoracic Oncology Program Wake Forest Comprehensive Cancer Center Disclosures I have no actual
Oral Cavity Cancer Combined modality therapy
 Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
Oral Cavity Cancer Combined modality therapy Dr. Christos CHRISTOPOULOS Radiation Oncologist Head and Neck Cancers Centre Hospitalier Universitaire (C.H.U.) de Limoges, France Disclosure slide I have no
Lung Cancer Non-small Cell Local, Regional, Small Cell, Other Thoracic Cancers: The Question Isn t Can We, but Should We
 Lung Cancer Non-small Cell Local, Regional, Small Cell, Other Thoracic Cancers: The Question Isn t Can We, but Should We Edward Garon, MD, MS Associate Professor Director- Thoracic Oncology Program David
Lung Cancer Non-small Cell Local, Regional, Small Cell, Other Thoracic Cancers: The Question Isn t Can We, but Should We Edward Garon, MD, MS Associate Professor Director- Thoracic Oncology Program David
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer
 Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
Simultaneous Integrated Boost or Sequential Boost in the Setting of Standard Dose or Dose De-escalation for HPV- Associated Oropharyngeal Cancer Dawn Gintz, CMD, RTT Dosimetry Coordinator of Research and
3/12/2018. Head & Neck Cancer Review INTRODUCTION
 Head & Neck Cancer Review Joseph Rosales, MD March 12, 2018 INTRODUCTION Epidemiology/Risk Factors Anatomy Presentation/Workup Treatment Surgery vs Radiation Chemotherapy Side effects Special circumstances
Head & Neck Cancer Review Joseph Rosales, MD March 12, 2018 INTRODUCTION Epidemiology/Risk Factors Anatomy Presentation/Workup Treatment Surgery vs Radiation Chemotherapy Side effects Special circumstances
Two Cycles of Chemoradiation: 2 Cycles is Enough. Concurrent Chemotherapy / RT Regimens
 1 Two Cycles of Chemoradiation: 2 Cycles is Enough Heather Wakelee, M.D. Assistant Professor of Medicine, Oncology Stanford University Concurrent Chemotherapy / RT Regimens Cisplatin 50 mg/m 2 on days
1 Two Cycles of Chemoradiation: 2 Cycles is Enough Heather Wakelee, M.D. Assistant Professor of Medicine, Oncology Stanford University Concurrent Chemotherapy / RT Regimens Cisplatin 50 mg/m 2 on days
ES-SCLC Joint Case Conference. Anthony Paravati Adam Yock
 ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
ES-SCLC Joint Case Conference Anthony Paravati Adam Yock Case 57 yo woman with 35 pack year smoking history presented with persistent cough and rash Chest x-ray showed a large left upper lobe/left hilar
Larynx Hypopharynx. Therapy algorithms. Why larynx preservation at all? State of the art Jean Louis Lefebvre,Lille Jan Klozar,Prague
 Larynx Hypopharynx Moderation Rainald Knecht,Hamburg State of the art Jean Louis Lefebvre,Lille Debate pro CRT Jan Klozar,Prague contra CRT Marshall Posner,Boston Clinical cases all Therapy algorithms
Larynx Hypopharynx Moderation Rainald Knecht,Hamburg State of the art Jean Louis Lefebvre,Lille Debate pro CRT Jan Klozar,Prague contra CRT Marshall Posner,Boston Clinical cases all Therapy algorithms
Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer
 in Cervical Cancer") Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer Nicoletta Colombo, MD University of Milan-Bicocca European Institute of Oncology Milan, Italy NACT in Cervical Cancer NACT Stage -IB2 -IIA>4cm
Update on Neoadjuvant Chemotherapy (NACT) in Cervical Cancer Nicoletta Colombo, MD University of Milan-Bicocca European Institute of Oncology Milan, Italy NACT in Cervical Cancer NACT Stage -IB2 -IIA>4cm
CALGB Thoracic Radiotherapy for Limited Stage Small Cell Lung Cancer
 CALGB 30610 Thoracic Radiotherapy for Limited Stage Small Cell Lung Cancer Jeffrey A. Bogart Department of Radiation Oncology Upstate Medical University Syracuse, NY Small Cell Lung Cancer Estimated 33,000
CALGB 30610 Thoracic Radiotherapy for Limited Stage Small Cell Lung Cancer Jeffrey A. Bogart Department of Radiation Oncology Upstate Medical University Syracuse, NY Small Cell Lung Cancer Estimated 33,000
Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer
 Non-Small Cell Lung Cancer") Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer Jyoti D. Patel, MD Associate Professor Feinberg School of Medicine Robert H Lurie Comprehensive Cancer Center Northwestern
Choosing Optimal Therapy for Advanced Non-Squamous (NS) Non-Small Cell Lung Cancer Jyoti D. Patel, MD Associate Professor Feinberg School of Medicine Robert H Lurie Comprehensive Cancer Center Northwestern
Chemotherapy for Advanced Gastric Cancer
 Chemotherapy for Advanced Gastric Cancer Andrés Cervantes Professor of Medicine DISCLOSURE OF INTEREST Employment: None Consultant or Advisory Role: Merck Serono, Roche, Beigene, Bayer, Servier, Lilly,
Chemotherapy for Advanced Gastric Cancer Andrés Cervantes Professor of Medicine DISCLOSURE OF INTEREST Employment: None Consultant or Advisory Role: Merck Serono, Roche, Beigene, Bayer, Servier, Lilly,
Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer.
 Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer Reference Slides ALK Rearrangement in NSCLC ALK (anaplastic lymphoma kinase) is a receptor
Virtual Journal Club: Front-Line Therapy and Beyond Recent Perspectives on ALK-Positive Non-Small Cell Lung Cancer Reference Slides ALK Rearrangement in NSCLC ALK (anaplastic lymphoma kinase) is a receptor
Squamous Cell Carcinoma Standard and Novel Targets.
 Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Squamous Cell Carcinoma Standard and Novel Targets. Mohamed K. Mohamed, MD, PhD Director of Thoracic Oncology Cone Health Cancer Center Greensboro, NC 1 Mohamed Mohamed, MD, PhD Squamous Cell Carcinoma:
Lung Cancer Epidemiology. AJCC Staging 6 th edition
 Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Surgery for stage IIIA NSCLC? Sometimes! Anne S. Tsao, M.D. Associate Professor Director, Mesothelioma Program Director, Thoracic Chemo-Radiation Program May 7, 2011 The University of Texas MD ANDERSON
Self-Assessment Module 2016 Annual Refresher Course
 LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
LS16031305 The Management of s With r. Lin Learning Objectives: 1. To understand the changing demographics of oropharynx cancer, and the impact of human papillomavirus on overall survival and the patterns
Thoracic and head/neck oncology new developments
 Thoracic and head/neck oncology new developments Goh Boon Cher Department of Hematology-Oncology National University Cancer Institute of Singapore Research Clinical Care Education Scope Lung cancer Screening
Thoracic and head/neck oncology new developments Goh Boon Cher Department of Hematology-Oncology National University Cancer Institute of Singapore Research Clinical Care Education Scope Lung cancer Screening
Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies. Eric H. Rubin, MD Merck Research Laboratories
 Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies Eric H. Rubin, MD Merck Research Laboratories Outline Pembrolizumab P001 study - example of multiple expansion
Use of Single-Arm Cohorts/Trials to Demonstrate Clinical Benefit for Breakthrough Therapies Eric H. Rubin, MD Merck Research Laboratories Outline Pembrolizumab P001 study - example of multiple expansion
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents
 Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
Evolving Paradigms in HER2+ MBC: Strategies for Individualizing Therapy with Available Agents Kimberly L. Blackwell MD Professor Department of Medicine and Radiation Oncology Duke University Medical Center
PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER. Virginie Westeel Chest Disease Department University Hospital Besançon, France
 PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER Virginie Westeel Chest Disease Department University Hospital Besançon, France LEARNING OBJECTIVES 1. To understand the potential of perioperative
PERIOPERATIVE TREATMENT OF NON SMALL CELL LUNG CANCER Virginie Westeel Chest Disease Department University Hospital Besançon, France LEARNING OBJECTIVES 1. To understand the potential of perioperative
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only.
 The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
The following slides are provided as presented by the author during the live educa7onal ac7vity and are intended for reference purposes only. If you have any ques7ons, please contact Imedex via email at:
INMUNOTERAPIA: NUEVO PARADIGMA EN LOS TUMORES DE CABEZA Y CUELLO. Dra. Lara Iglesias H.U.12 Octubre
 INMUNOTERAPIA: NUEVO PARADIGMA EN LOS TUMORES DE CABEZA Y CUELLO Dra. Lara Iglesias H.U.12 Octubre INTRODUCCIÓN INFORME SEOM DE EVALUACIÓN DE FÁRMACOS: NIVOLUMAB EN CÁNCER EPIDERMOIDE DE CABEZA Y CUELLO
INMUNOTERAPIA: NUEVO PARADIGMA EN LOS TUMORES DE CABEZA Y CUELLO Dra. Lara Iglesias H.U.12 Octubre INTRODUCCIÓN INFORME SEOM DE EVALUACIÓN DE FÁRMACOS: NIVOLUMAB EN CÁNCER EPIDERMOIDE DE CABEZA Y CUELLO
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease
 Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
Tristate Lung Meeting 2014 Pro-Con Debate: Surgery has no role in the management of certain subsets of N2 disease Jennifer E. Tseng, MD UFHealth Cancer Center-Orlando Health Sep 12, 2014 Background Approximately
MANAGEMENT OF CA HYPOPHARYNX
 MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
MANAGEMENT OF CA HYPOPHARYNX GENERAL TREATMENT RECOMMENDATIONS BASED ON HYPOPHARYNX TUMOR STAGE For patients presenting with early-stage definitive radiotherapy alone or voice-preserving surgery are viable
HPV and Head and Neck Cancer: What it means for you and your patients
 HPV and Head and Neck Cancer: What it means for you and your patients Financial Disclosure: None November 8, 2013 Steven J. Wang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery
HPV and Head and Neck Cancer: What it means for you and your patients Financial Disclosure: None November 8, 2013 Steven J. Wang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery
Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma
 Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Pieter E. Postmus University of Liverpool Liverpool, UK Plotting the course: optimizing treatment strategies in patients with advanced adenocarcinoma Disclosures Advisor Bristol-Myers Squibb AstraZeneca
Update on Limited Small Cell Lung Cancer. Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver
 Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
Update on Limited Small Cell Lung Cancer Laurie E Gaspar MD, MBA Prof/Chair Radiation Oncology University of Colorado Denver Objectives - Limited Radiation Dose Radiation Timing Radiation Volume PCI Neurotoxicity
The Role of Docetaxel in the Treatment of Head and Neck Cancer
 GBMC Head and Neck Conference The Role of Docetaxel in the Treatment of Head and Neck Cancer Simon Best December 7, 2007 Needs assessment: Providers who participate in the care of head and neck cancer
GBMC Head and Neck Conference The Role of Docetaxel in the Treatment of Head and Neck Cancer Simon Best December 7, 2007 Needs assessment: Providers who participate in the care of head and neck cancer
Overview. What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013
 What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013 Overview Staging and Workup Resectable Disease Surgery Adjuvant therapy Locally
What s New in the Treatment of Pancreatic Cancer? Lots! Steven J. Cohen, M.D. Fox Chase Cancer Center September 17, 2013 Overview Staging and Workup Resectable Disease Surgery Adjuvant therapy Locally