TYPE 1 GAUCHER DISEASE PRESENTING AS PERSISTENT THROMBOCYTOPENIA, ASSOCIATED FACTOR XI DEFICIENCY & EMERGENT MYELOMA
|
|
|
- Ursula Fitzgerald
- 5 years ago
- Views:
Transcription
1 TYPE 1 GAUCHER DISEASE PRESENTING AS PERSISTENT THROMBOCYTOPENIA, ASSOCIATED FACTOR XI DEFICIENCY & EMERGENT MYELOMA Trish Hyland, Medical Scientist, Department of Haematology, Cork University Hospital
2 INTRODUCTION Gaucher disease (GB) is an autosomal recessive inherited disorder of glycolipid storage Caused by absence or low activity of glucocerebrosidase (Gcase) resulting in accumulation of its substrate glucocerebroside in macrophages, termed Gaucher cells Gaucher cells infiltrate the reticuloendothelial system Type 1 GD is pan-ethnic, incidence of 1:100,000 but most common in Ashkenazi Jews (1: 450) It is estimated to affect approximately 2-4% of the entire Irish community
3 INTRODUCTION It presents at any age - infancy to adulthood Clinical manifestations include hepatosplenomegaly, pancytopenia and bone complications Most frequent presentations are with symptomatic splenomegaly or thrombocytopenia Thrombocytopenia is caused by hyperslenism and/or bone marrow infiltration by Gaucher cells compromising megakaryopoiesis
4 CASE PRESENTATION 27 year old lady from Lithuania referred to Haematology team, Cork University Hospital with thrombocytopenia in pregnancy (12 weeks) Full blood count: Platelet count - 55 x 10 9 /L Past medical history; Hepatitis C infection Osteomyelitis Nephritis Chronic thrombocytopenia Haemoglobin g/l White cell count 4.8 x 10 9 /L No significant bleeding history
5 LABORATORY INVESTIGATION Clotting screen: PT 11.2 ( secs) APTT 36 (23-31 secs) Further clotting studies/factor assays performed; Inhibitor screen - negative Lupus screen normal Antiphospholipid antibodies - normal Von Willebrand screen normal Factor IX w/n normal range Factor XII w/n normal range Factor XI level at 43 % - mild deficiency
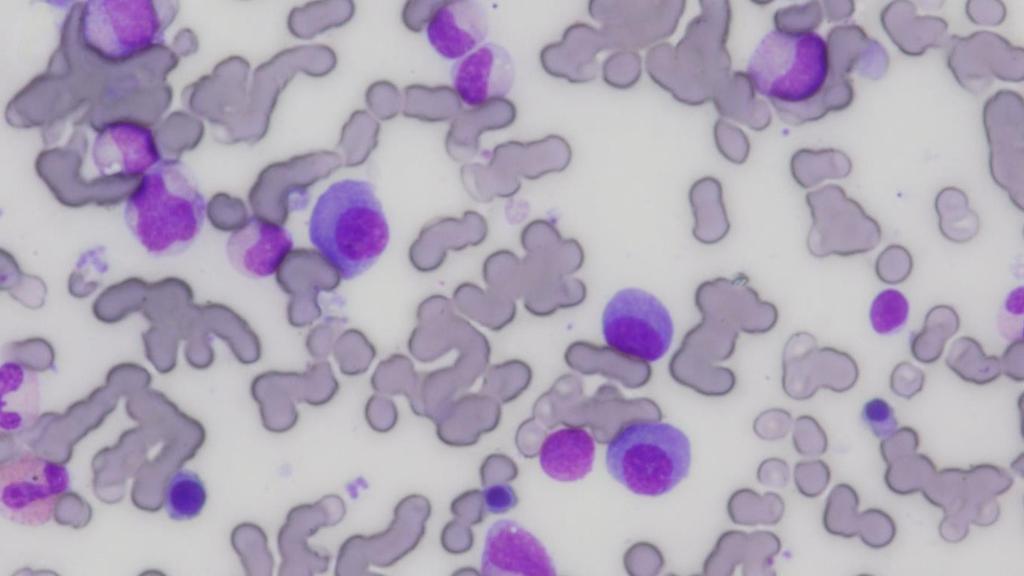
6 LABORATORY INVESTIGATION Hereditary or acquired, most commonly factor XI deficiency is an inherited coagulation abnormality Her pregnancy proceeded uneventfully & patients platelet count remained stable between x 10 9 /L She attended Haematology OPD clinic for follow-up; Persistent thrombocytopenia Clinical splenomegaly Bone pains and fatigue Bone marrow biopsy and peripheral blood morphology was performed Blood morphology; normochromic normocytic anaemia Bone marrow aspirate showed the presence of Gaucher cells
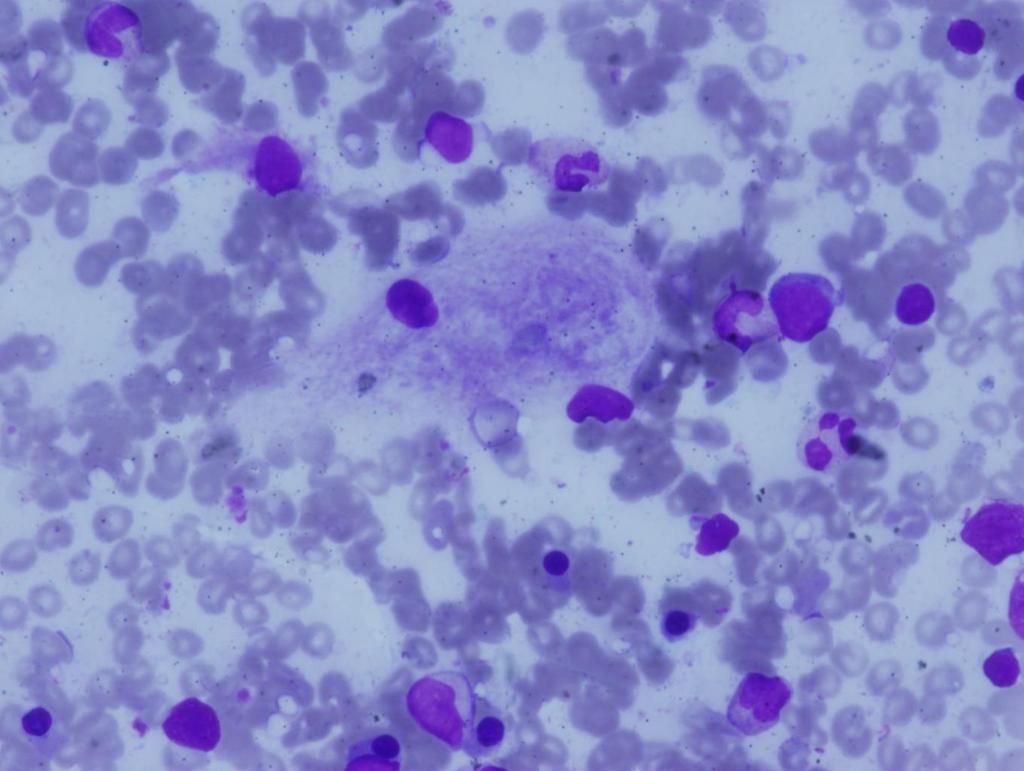
7
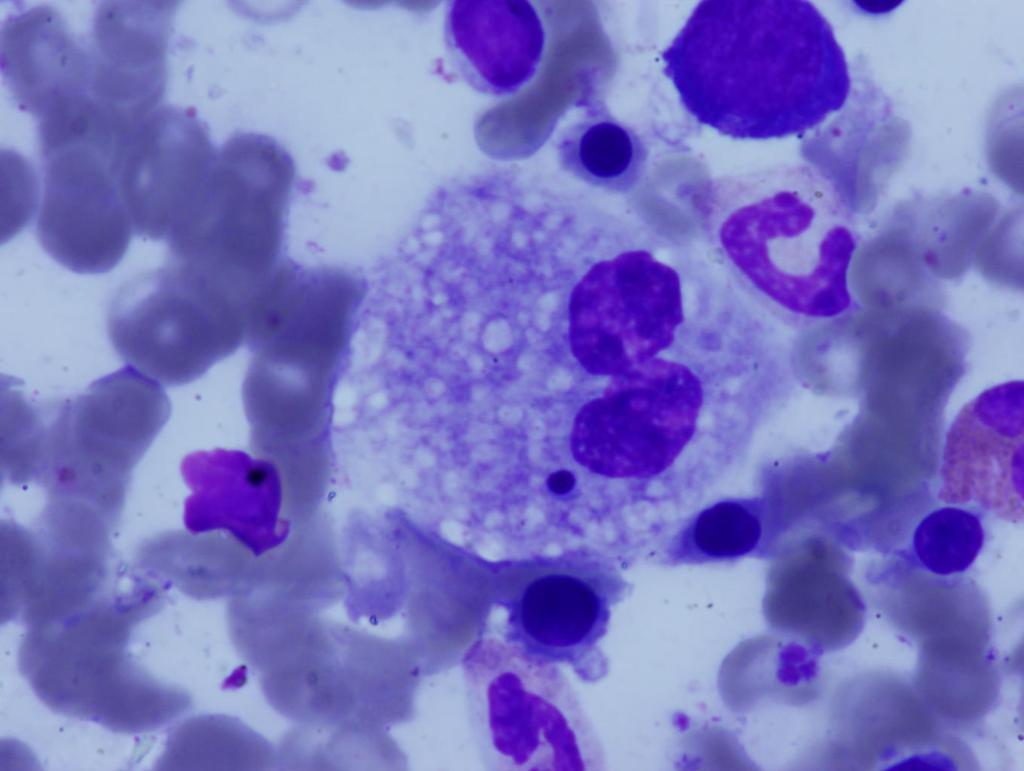
8
9 LABORATORY DIAGNOSIS Demonstration of the presence of Gaucher cells is not diagnostic of GD Pseudo-Gaucher cells/storage cells are morphologically similar thus could be confused with Gaucher cells Present in other haematological conditions e.g chronic myeloid leukaemia, haemoglobinopathies and other storage conditions like Niemann pick disease
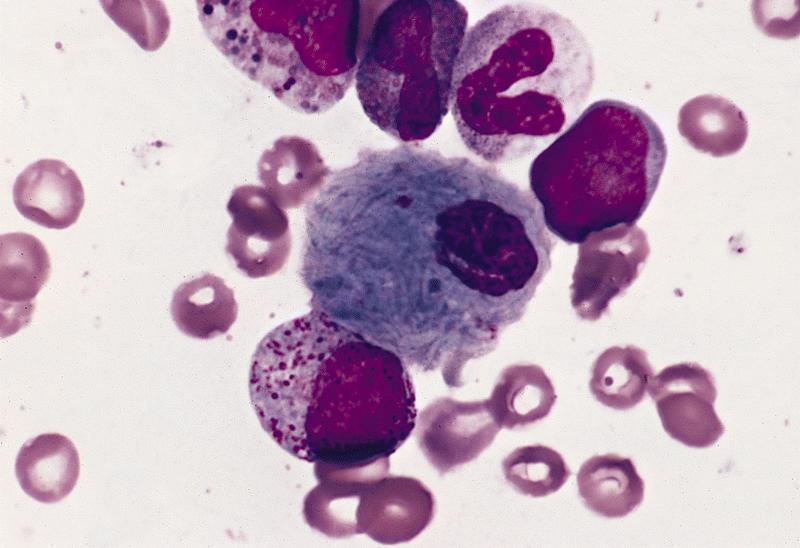
10
11 LABORATORY DIAGNOSIS Measurement of glucocerebrosidase activity in peripheral blood leukocytes Chitotriosidase is an enzyme that is overexpressed by Gaucher cells. A prognostic marker useful for indicating disease burden and monitoring treatment of GD Patient samples referred to lysosomal storage disease unit, Royal Free hospital, London Glucocerebrosidase 0.2 umol/g/h ( ) < 15% of mean normal activity is diagnostic of GD Chitotriosidase umol/l/h ( )
12 DIAGNOSIS - IMAGING DEXA scan was performed normal Whole skeletal MRI; Diffuse marrow infiltration Osteonecrosis of humerus (right and left) Established bone infarction
13 TREATMENT 18 month wait before treatment commenced owing to cost; 250,000 a year for ERT Patient commenced on Enzyme Replacement Therapy; Velaglucerase, given intravenously at home, twice weekly Reduces the accumulation of the toxic substrates Response to treatment: Improved bone pain Reduced fatigue No new bone lesion and evidence of healing in skeletal disease
14 Laboratory results pretreatment Full blood count Hb: 11.3 g/dl Laboratory results posttreatment Hb: 13.4 g/dl (~ 20 months) Full blood count PLT: 76 x10 9 /L PLT: 199 x x10 9 /L Coagulation APTT: 37 secs Factor XI: IU/ml Chitotriosidase umol/l/hr ( umol/l/hr) Coagulation APTT: 25 secs Factor XI: IU/ml Chitotriosidase 935 umol/l/hr
15 FACTOR XI DEFICIENCY & GAUCHER DISEASE Normalisation of Factor XI levels post treatment indicated that this deficiency was acquired and not inherited In type 1 GD, coagulation abnormalities, in particular deficiency of factor IX and XI are found in a number of patients Consumption of the coagulation factor due on-going low level coagulation activation possibly due to mononuclear cell activation
16 MYELOMA & GAUCHER DISEASE GD patients have increased risk of developing monoclonal gammopathies in particular multiple myeloma Hypothesised mechanism; Gaucher cell resembles an alternatively activated macrophage which is believed to cause hyper stimulation of the immune system
17 In GD, elevated levels of pro-inflammatory cytokines in particular interleukin 6 (IL-6), may correlate with clonal expansion of B cells. IL-6 is involved in growth and survival of myeloma cells Concern about the association of GD and myeloma prompted further laboratory testing; Serum protein electrophoresis Serum free light chain assay
18 Serum free light chain assay: Free kappa chains mg/l ( ) Free lambda chains mg/l ( ) Serum K: L ratio 0.13 ( ) Serum protein electrophoresis: IgG g/l (6.0 16) IgA 2.13 g/l ( ) IgM 1.02 g/l ( ) Paraprotein level 2.6 g/l
19 LABORATORY DIAGNOSIS Serum calcium - normal Serum creatinine normal Haemoglobin 13.4 g/dl Diagnosis of monoclonal gammopathy of undetermined significance (MGUS) Four month follow-up, patient complaining of increasing bone pain. Paraprotein levels and serum free light chains were re-checked:
20 Serum free light chain assay: Sept 2015 May 2015 Free kappa chains mg/l mg/l Free lambda chains 342mg/L 101 mg/l Serum K: L ratio Serum protein electrophoresis: IgG g/l g/l IgA 1.17 g/l 2.13 g/l IgM 0.76 g/l 1.02 g/l Paraprotein level 21.8 g/l 2.6 g/l
21 LABORATORY DIAGNOSIS Bone marrow biopsy; Plasma cells present ; >60% in trephine and approximately 30% in aspirate Immunophenotyping: Immunophenotyping detected 12% clonal plasma cells Skeletal survey; Skeletal survey showed new lytic bony lesions The results were consistent with a diagnosis of multiple myeloma (IgG)
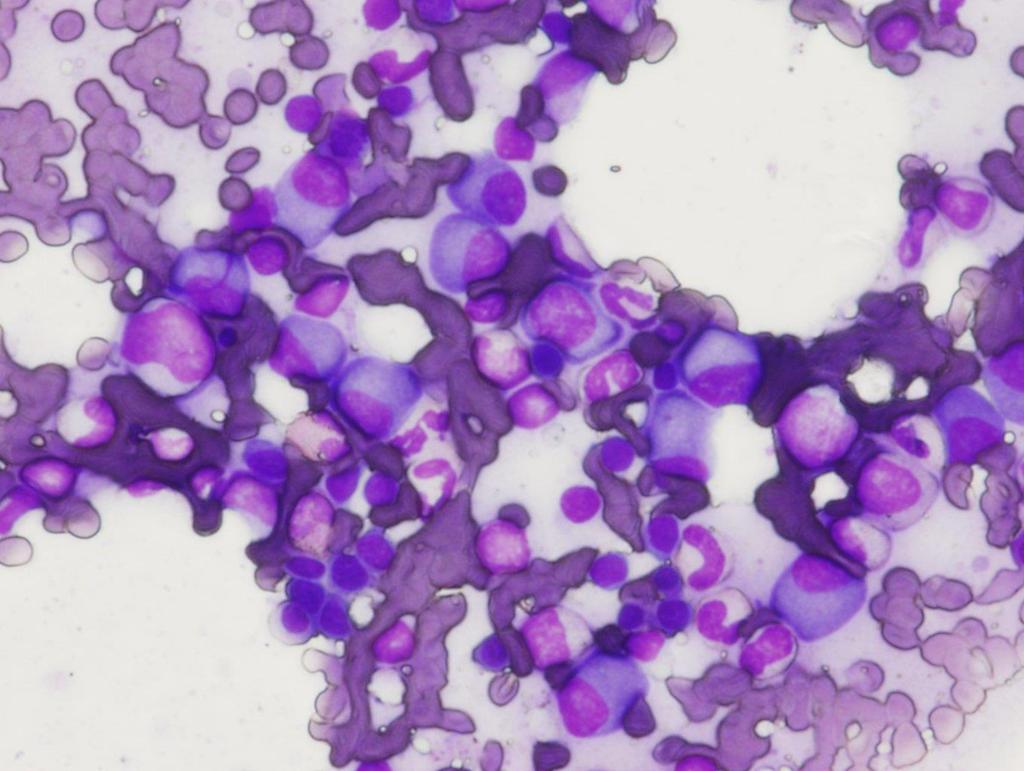
22
23
24 TREATMENT Initially the patient was treated with chemotherapy, then underwent an autologous stem cell transplant Patient had an excellent response to treatment, now on maintenance chemotherapy Continued Enzyme replacement therapy throughout Currently clinically very well
25 CONCLUSION Heightened awareness of the association of Gaucher Disease with splenomegaly and unremitting haematological abnormalities like thrombocytopenia may help minimise delayed diagnosis of this rare disease Highlight the associated myeloma risk with this disease
26 ACKNOWLEDGEMENTS Dr Cleona Duggan, Consultant Haematologist, Cork University Hospital Dr Rachael Brodie, Specialist Registrar, Haematology, Cork University Hospital Dr Norma Reidy, Chief Medical Scientist, Haematology, Cork University Hospital
Southern Derbyshire Shared Care Pathology Guidelines. MGUS (Monoclonal Gammopathy of Undetermined Significance)
") Southern Derbyshire Shared Care Pathology Guidelines MGUS (Monoclonal Gammopathy of Undetermined Significance) Purpose of guideline This guideline provides information about the risk stratification of
Southern Derbyshire Shared Care Pathology Guidelines MGUS (Monoclonal Gammopathy of Undetermined Significance) Purpose of guideline This guideline provides information about the risk stratification of
Anaemias and other Pesky Haematology Questions
 Anaemias and other Pesky Haematology Questions 3 main topics How do I work out an anaemia.. That oh too common paraprotein patient. Those mildly raised lymphocyte count GP discussed patient with me over
Anaemias and other Pesky Haematology Questions 3 main topics How do I work out an anaemia.. That oh too common paraprotein patient. Those mildly raised lymphocyte count GP discussed patient with me over
Medical Policy An independent licensee of the Blue Cross Blue Shield Association
 Substrate Reduction Therapy Page 1 of 7 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Substrate Reduction Therapy! Prime Therapeutics will review Prior Authorization
Substrate Reduction Therapy Page 1 of 7 Medical Policy An independent licensee of the Blue Cross Blue Shield Association Title: Substrate Reduction Therapy! Prime Therapeutics will review Prior Authorization
Candidates must answer ALL questions
 Time allowed: Three hours. Part 1 examination Haematology: First paper Tuesday 22 March 2016 Candidates must answer ALL questions Question 1: General Haematology A 16 year old non-european is referred
Time allowed: Three hours. Part 1 examination Haematology: First paper Tuesday 22 March 2016 Candidates must answer ALL questions Question 1: General Haematology A 16 year old non-european is referred
Rory McCulloch. Specialty Trainee Haematology Royal Devon & Exeter Hospital
 Rory McCulloch Specialty Trainee Haematology Royal Devon & Exeter Hospital Anaemia 1 Haematological disorders Anaemia 2 Non-haematological disorders Substrates: Iron, folate, vitamin B12 Red cell mass
Rory McCulloch Specialty Trainee Haematology Royal Devon & Exeter Hospital Anaemia 1 Haematological disorders Anaemia 2 Non-haematological disorders Substrates: Iron, folate, vitamin B12 Red cell mass
M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016
 + M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016 + Disclosures Advisory Boards: AMGEN, Lundbeck, NOVARTIS + Subtypes of Plasma Cell Disorders Increased Plasma
+ M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016 + Disclosures Advisory Boards: AMGEN, Lundbeck, NOVARTIS + Subtypes of Plasma Cell Disorders Increased Plasma
Multiple myeloma Biological & Clinical Aspects Isabelle Vande Broek, MD, PhD
 Multiple myeloma Biological & Clinical Aspects Isabelle Vande Broek, MD, PhD Department of Oncology & Hematology AZ Nikolaas Iridium Kanker Netwerk Introduction Multiple myeloma = Kahler s disease Dr.
Multiple myeloma Biological & Clinical Aspects Isabelle Vande Broek, MD, PhD Department of Oncology & Hematology AZ Nikolaas Iridium Kanker Netwerk Introduction Multiple myeloma = Kahler s disease Dr.
Hematology 101. Rachid Baz, M.D. 5/16/2014
 Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
2017 Repeat Audit of Red cell and Platelet Transfusion in Adult Haematology Patients
 07 Repeat Audit of Red cell and Platelet Transfusion in Adult Haematology Patients Haematology Audit July 07 The audit was conducted on adults undergoing surgery and who received a transfusion during a
07 Repeat Audit of Red cell and Platelet Transfusion in Adult Haematology Patients Haematology Audit July 07 The audit was conducted on adults undergoing surgery and who received a transfusion during a
Blood Cancers in the Community
 Over to you, mate Blood Cancers in the Community National Rural Health Conference NZ Rural General Practice Network April 7, 2018 Brian Grainger Haematology Registrar Auckland Acknowledgements Dr James
Over to you, mate Blood Cancers in the Community National Rural Health Conference NZ Rural General Practice Network April 7, 2018 Brian Grainger Haematology Registrar Auckland Acknowledgements Dr James
Contents SECTION 1: PHYSIOLOGY OF BLOOD
 Contents SECTION 1: PHYSIOLOGY OF BLOOD Chapter 1: Overview of Physiology of Blood 1 Normal Haematopoiesis 1 Red Blood Cells 6 White Blood Cells 15 Immune System 27 Megakaryopoiesis 32 Normal Haemostasis
Contents SECTION 1: PHYSIOLOGY OF BLOOD Chapter 1: Overview of Physiology of Blood 1 Normal Haematopoiesis 1 Red Blood Cells 6 White Blood Cells 15 Immune System 27 Megakaryopoiesis 32 Normal Haemostasis
r). SUPPLEMENTARY/SECOND OPPORTUNITY EXAMINATION PAPER nnmlbih UNIVERSITY Sophia Blaauw INSTRUCTIONS FACULTY OF HEALTH AND APPLIED SCIENCES
. SUPPLEMENTARY/SECOND OPPORTUNITY EXAMINATION PAPER nnmlbih UNIVERSITY Sophia Blaauw INSTRUCTIONS FACULTY OF HEALTH AND APPLIED SCIENCES") r). nnmlbih UNIVERSITY OF SCIEFICE nnd TECHNOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES QUALIFICATION: BACHELOR OF MEDICAL LABORATORY SCIENCES QUALIFICATION CODE: 08BMLS
r). nnmlbih UNIVERSITY OF SCIEFICE nnd TECHNOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES QUALIFICATION: BACHELOR OF MEDICAL LABORATORY SCIENCES QUALIFICATION CODE: 08BMLS
Haematological Cancer Suspected (Adults & Children)
") Haematological Cancer Suspected (Adults & Children) Link to NICE guidelines: https://www.nice.org.uk/guidance/ng47 Patient of any age presents with symptoms of possible haematological cancer If 60 years
Haematological Cancer Suspected (Adults & Children) Link to NICE guidelines: https://www.nice.org.uk/guidance/ng47 Patient of any age presents with symptoms of possible haematological cancer If 60 years
Morphology Case Study. Presented by Niamh O Donnell, BSc, MSc. Medical Scientist Haematology Laboratory Cork University Hospital
 Morphology Case Study Presented by Niamh O Donnell, BSc, MSc. Medical Scientist Haematology Laboratory Cork University Hospital 41 year old male presented to GP for routine check-up in May 2011. FBC Results:
Morphology Case Study Presented by Niamh O Donnell, BSc, MSc. Medical Scientist Haematology Laboratory Cork University Hospital 41 year old male presented to GP for routine check-up in May 2011. FBC Results:
Multiple myeloma: from diagnosis to treatment
 Diagnostic challenges Renee Eslick Dipti Talaulikar Multiple : from diagnosis to treatment Background Multiple is characterised by the proliferation of malignant plasma cells within the bone marrow, which
Diagnostic challenges Renee Eslick Dipti Talaulikar Multiple : from diagnosis to treatment Background Multiple is characterised by the proliferation of malignant plasma cells within the bone marrow, which
Gaucher Disease: a multiorgan rare disease in Internal Medicine. M.Domenica Cappellini Fondazione Policlinico IRCCS University of Milan
 Gaucher Disease: a multiorgan rare disease in Internal Medicine M.Domenica Cappellini Fondazione Policlinico IRCCS University of Milan XXXI Congreso Nacional de la Sociedad Espanola de Medicina Interna
Gaucher Disease: a multiorgan rare disease in Internal Medicine M.Domenica Cappellini Fondazione Policlinico IRCCS University of Milan XXXI Congreso Nacional de la Sociedad Espanola de Medicina Interna
Multiple Myeloma 101: Understanding Your Labs
 Multiple Myeloma 101: Understanding Your Labs Tim Wassenaar MD MS Hematologist, Director of Clinical Trials UW Cancer Center at ProHealth Care None Disclosures Outline Define hematopoiesis WBCs, RBCs,
Multiple Myeloma 101: Understanding Your Labs Tim Wassenaar MD MS Hematologist, Director of Clinical Trials UW Cancer Center at ProHealth Care None Disclosures Outline Define hematopoiesis WBCs, RBCs,
TESTS AND INVESTIGATIONS FOR MULTIPLE MYELOMA A guide for patients and caregivers
 TESTS AND INVESTIGATIONS FOR MULTIPLE MYELOMA A guide for patients and caregivers Developed by the Myeloma Special Practice Network (M-SPN) of the Haematology Society of Australia and New Zealand (HSANZ)
TESTS AND INVESTIGATIONS FOR MULTIPLE MYELOMA A guide for patients and caregivers Developed by the Myeloma Special Practice Network (M-SPN) of the Haematology Society of Australia and New Zealand (HSANZ)
Serum free light chain (SFLC) assays. Dr Sarah Sasson SydPath Registrar
 assays. Dr Sarah Sasson SydPath Registrar") Serum free light chain (SFLC) assays Dr Sarah Sasson SydPath Registrar Introduction to SFLC Plasma cell dyscrasias such as monoclonal gammopathy of uncertain significance (MGUS) smouldering/asymptomatic
Serum free light chain (SFLC) assays Dr Sarah Sasson SydPath Registrar Introduction to SFLC Plasma cell dyscrasias such as monoclonal gammopathy of uncertain significance (MGUS) smouldering/asymptomatic
Mr Matthew Eby. Dr Humphrey Pullon
 Dr Humphrey Pullon Haematologist Hamilton Mr Matthew Eby Senior Support Services Coordinator Leukaemia & Blood Cancer Foundation New Zealand Hamilton 16:30-17:25 WS #64: Managing Haemopoetic Disease in
Dr Humphrey Pullon Haematologist Hamilton Mr Matthew Eby Senior Support Services Coordinator Leukaemia & Blood Cancer Foundation New Zealand Hamilton 16:30-17:25 WS #64: Managing Haemopoetic Disease in
Management Update: Multiple Myeloma. Presented by Prof. Dr. Khan Abul Kalam Azad Professor of Medicine Dhaka Medical College
 Management Update: Multiple Myeloma Presented by Prof. Dr. Khan Abul Kalam Azad Professor of Medicine Dhaka Medical College Introduction Multiple myeloma - clonal plasma cell neoplasm Monoclonal antibody
Management Update: Multiple Myeloma Presented by Prof. Dr. Khan Abul Kalam Azad Professor of Medicine Dhaka Medical College Introduction Multiple myeloma - clonal plasma cell neoplasm Monoclonal antibody
Criteria for Disease Assessment Joan Bladé
 Criteria for Disease Assessment Joan Bladé Unidad de Amiloidosis y Mieloma Servicio de Hematología Hospital Clínic de Barcelona COMy Meeting, París, May 4th, 2018 Response Evaluation EBMT, 1998 - CR and
Criteria for Disease Assessment Joan Bladé Unidad de Amiloidosis y Mieloma Servicio de Hematología Hospital Clínic de Barcelona COMy Meeting, París, May 4th, 2018 Response Evaluation EBMT, 1998 - CR and
Citation for published version (APA): Hovenga, S. (2007). Clinical and biological aspects of Multiple Myeloma s.n.
: Hovenga, S. (2007). Clinical and biological aspects of Multiple Myeloma s.n.") University of Groningen Clinical and biological aspects of Multiple Myeloma Hovenga, Sjoerd IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from
University of Groningen Clinical and biological aspects of Multiple Myeloma Hovenga, Sjoerd IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from
Diagnosis, monitoring and treatment of adult Gaucher patients
 Diagnosis, monitoring and treatment of adult Gaucher patients Stephan vom Dahl, M.D., Professor of Medicine St. Franziskus Hospital, Köln, Germany Podčetrtek, Slovenia, April 22, 2006 Strokovni Sestanek
Diagnosis, monitoring and treatment of adult Gaucher patients Stephan vom Dahl, M.D., Professor of Medicine St. Franziskus Hospital, Köln, Germany Podčetrtek, Slovenia, April 22, 2006 Strokovni Sestanek
Smoldering Multiple Myeloma. A Case Study
 Smoldering Multiple Myeloma A Case Study Case Presentation 53-Year-Old Male Patient presented for a routine exam No prior history of disease or family history of fhematologic disorders d or malignancies,
Smoldering Multiple Myeloma A Case Study Case Presentation 53-Year-Old Male Patient presented for a routine exam No prior history of disease or family history of fhematologic disorders d or malignancies,
Michael Joffe ST6 Haematology SpR
 Michael Joffe ST6 Haematology SpR Mrs SB 71 year old female on AMU Telephone referral to haematology by medicine with Hb 102 MCV 89, normal B12, Folate, Ferritin. PMH DM General decline over several weeks
Michael Joffe ST6 Haematology SpR Mrs SB 71 year old female on AMU Telephone referral to haematology by medicine with Hb 102 MCV 89, normal B12, Folate, Ferritin. PMH DM General decline over several weeks
GP Referral Guidelines. for. South Wales Cancer Network. Document Control Sheet. Specialty/Project Haematological Site Specific Group
 GP Referral Guidelines for South Wales Cancer Network Document Control Sheet Organisation South Wales Cancer Network Specialty/Project Haematological Site Specific Group Document Title GP Referral Guidelines
GP Referral Guidelines for South Wales Cancer Network Document Control Sheet Organisation South Wales Cancer Network Specialty/Project Haematological Site Specific Group Document Title GP Referral Guidelines
Myeloma. A guide for patients and families leukaemia.org.au
 Myeloma A guide for patients and families 1800 620 420 leukaemia.org.au Contents Acknowledgments 4 Introduction 5 The Leukaemia Foundation 6 Blood cancers 10 What is myeloma? 16 Who gets myeloma? 20 How
Myeloma A guide for patients and families 1800 620 420 leukaemia.org.au Contents Acknowledgments 4 Introduction 5 The Leukaemia Foundation 6 Blood cancers 10 What is myeloma? 16 Who gets myeloma? 20 How
Lec-14 د.خالد نافع. Medicine. Multiple Myeloma
 Fifth stage Lec-14 د.خالد نافع Medicine 24/4/2016 Multiple Myeloma Plasma cell myeloma Variants Non - secretory myeloma Indolent myeloma Smouldering myeloma Plasma cell leukaemia Plasmacytoma - Solitary
Fifth stage Lec-14 د.خالد نافع Medicine 24/4/2016 Multiple Myeloma Plasma cell myeloma Variants Non - secretory myeloma Indolent myeloma Smouldering myeloma Plasma cell leukaemia Plasmacytoma - Solitary
Hematology Case Conference 8/5/03
 Hematology Case Conference 8/5/03 Bone Marrow Case Patient: Emmxxx Lylexxx 74 year old AA female S/P craniotomy for SDH. Pt has Hx of HTN, DM, Crohn s disease, (R) nephrectomy. Bone marrow for abnormal
Hematology Case Conference 8/5/03 Bone Marrow Case Patient: Emmxxx Lylexxx 74 year old AA female S/P craniotomy for SDH. Pt has Hx of HTN, DM, Crohn s disease, (R) nephrectomy. Bone marrow for abnormal
FBC CASES Vernon Louw Clinical Haematology 2010
 FBC CASES Vernon Louw Clinical Haematology 2010 FOR EACH OF THE FOLLOWING PATIENTS, SELECT THE MOST LIKELY FINDING FROM THE ANALYSIS OF THE PERIPHERAL BLOOD. A patient with infectious mononucleosis. A
FBC CASES Vernon Louw Clinical Haematology 2010 FOR EACH OF THE FOLLOWING PATIENTS, SELECT THE MOST LIKELY FINDING FROM THE ANALYSIS OF THE PERIPHERAL BLOOD. A patient with infectious mononucleosis. A
Common Haematological Problems in Primary Care
 23 rd March 2019 GP Hot Topics In Primary Care Common Haematological Problems in Primary Care Dr Samar Kulkarni Consultant Haematologist-Oncologist and The Christie Private Care Manchester, UK. Haematology?
23 rd March 2019 GP Hot Topics In Primary Care Common Haematological Problems in Primary Care Dr Samar Kulkarni Consultant Haematologist-Oncologist and The Christie Private Care Manchester, UK. Haematology?
If unqualified, Complete remission is considered to be Haematological complete remission
 Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Cytopaenias in HIV. Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH
 Cytopaenias in HIV Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH Introduction Cytopaenias in HIV are common Anaemias multifactorial causes Thrombocytopaenias may be the first
Cytopaenias in HIV Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH Introduction Cytopaenias in HIV are common Anaemias multifactorial causes Thrombocytopaenias may be the first
2016: Plasma Cell Disorders Pre-HCT Data
 2016: Plasma Cell Disorders Pre-HCT Data Registry Use Only Sequence Number: Date Received: Key Fields CIBMTR Center Number: Date of HCT for which this form is being completed: / / YYYY MM DD HCT type (check
2016: Plasma Cell Disorders Pre-HCT Data Registry Use Only Sequence Number: Date Received: Key Fields CIBMTR Center Number: Date of HCT for which this form is being completed: / / YYYY MM DD HCT type (check
Borderline cytopenias. Dr Taku Sugai Consultant Haematologist
 Borderline cytopenias Dr Taku Sugai Consultant Haematologist Borderline cytopenias Neutropenia Thrombocytopenia Anaemia with normal haematinics Two recent cases of cytopenias Neutropenia ANC of more than
Borderline cytopenias Dr Taku Sugai Consultant Haematologist Borderline cytopenias Neutropenia Thrombocytopenia Anaemia with normal haematinics Two recent cases of cytopenias Neutropenia ANC of more than
Western Health Specialist Clinics Access & Referral Guidelines
 Haematology Specialist Clinics at Western Health: Western Health runs MBS funded Specialist Clinics on a Wednesday and Thursday afternoon at its Sunshine Hospital site for patients who require assessment
Haematology Specialist Clinics at Western Health: Western Health runs MBS funded Specialist Clinics on a Wednesday and Thursday afternoon at its Sunshine Hospital site for patients who require assessment
Refractory M ultiple Multiple M yeloma Myeloma
 Refractory Multiple Myeloma A Case Study Case: #1 48-Year-Old Male Presented to the ER with Fatigue and Acute Severe Lower Back Pain Patient assessment: X-ray of lumbar spine: L4 compression fracture,
Refractory Multiple Myeloma A Case Study Case: #1 48-Year-Old Male Presented to the ER with Fatigue and Acute Severe Lower Back Pain Patient assessment: X-ray of lumbar spine: L4 compression fracture,
Plasma Cell Disorders (PCD) Pre-HCT Data
 Pre-HCT Data") Plasma Cell Disorders (PCD) Pre-HCT Data Registry Use Only Sequence Number: Date Received: CIBMTR Center Number: CIBMTR Recipient ID: Date of HCT for which this form is being completed: HCT type: (check
Plasma Cell Disorders (PCD) Pre-HCT Data Registry Use Only Sequence Number: Date Received: CIBMTR Center Number: CIBMTR Recipient ID: Date of HCT for which this form is being completed: HCT type: (check
Treatment of Waldenström s Macroglobulinemia Mayo Consensus
 Treatment of Waldenström s Macroglobulinemia Mayo Consensus Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Mayo Clinic College of Medicine Mayo Clinic Comprehensive Cancer Center Mayo Clinic
Treatment of Waldenström s Macroglobulinemia Mayo Consensus Scottsdale, Arizona Rochester, Minnesota Jacksonville, Florida Mayo Clinic College of Medicine Mayo Clinic Comprehensive Cancer Center Mayo Clinic
Bisphosphonates in the Management of. Myeloma Bone Disease
 Bisphosphonates in the Management of Myeloma Bone Disease James R. Berenson, MD Medical & Scientific Director Institute for Myeloma & Bone Cancer Research Los Angeles, CA Myeloma Bone Disease Myeloma cells
Bisphosphonates in the Management of Myeloma Bone Disease James R. Berenson, MD Medical & Scientific Director Institute for Myeloma & Bone Cancer Research Los Angeles, CA Myeloma Bone Disease Myeloma cells
Case #1. Robert J. Glinert, M.D. David C. Fisher, M.D. Dana Farber Cancer Institute
 Case #1 Robert J. Glinert, M.D. David C. Fisher, M.D. Dana Farber Cancer Institute Patient History Part I 76 year-old man 1997 diagnosed with MGUS (biclonal) during evaluation of (self-limited) anemia.
Case #1 Robert J. Glinert, M.D. David C. Fisher, M.D. Dana Farber Cancer Institute Patient History Part I 76 year-old man 1997 diagnosed with MGUS (biclonal) during evaluation of (self-limited) anemia.
SWOG ONCOLOGY RESEARCH PROFESSIONAL (ORP) MANUAL RESPONSE ASSESSMENT MYELOMA CHAPTER 11C REVISED: SEPTEMBER 2016
 MANUAL RESPONSE ASSESSMENT MYELOMA CHAPTER 11C REVISED: SEPTEMBER 2016") MYELOMA Quantitative Markers-Myeloma Assessment Quantitative markers are biochemicals that are recorded in tests on body fluids such as serum and urine. Applicable Disease Sites The myeloma disease site
MYELOMA Quantitative Markers-Myeloma Assessment Quantitative markers are biochemicals that are recorded in tests on body fluids such as serum and urine. Applicable Disease Sites The myeloma disease site
Smoldering Myeloma: Leave them alone!
 Smoldering Myeloma: Leave them alone! David H. Vesole, MD, PhD Co-Director, Myeloma Division Director, Myeloma Research John Theurer Cancer Center Hackensack University Medical Center Prevalence 1960 2002
Smoldering Myeloma: Leave them alone! David H. Vesole, MD, PhD Co-Director, Myeloma Division Director, Myeloma Research John Theurer Cancer Center Hackensack University Medical Center Prevalence 1960 2002
If unqualified, Complete remission is considered to be Haematological complete remission
 Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust
 Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust Regional Paediatric Specialty Trainees teaching 4 th July 2017 Scope
Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust Regional Paediatric Specialty Trainees teaching 4 th July 2017 Scope
2013 AAIM Pathology Workshop
 2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
Early View Article: Online published version of an accepted article before publication in the final form.
 Early View Article: Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Oncology Type of Article: Case Report Title:
Early View Article: Online published version of an accepted article before publication in the final form. Journal Name: Journal of Case Reports and Images in Oncology Type of Article: Case Report Title:
Understanding. Myeloma. Caring for people with cancer
 Understanding Myeloma Caring for people with cancer Understanding myeloma This booklet has been written to help you understand more about myeloma. It has been prepared and checked by doctors, haematologists,
Understanding Myeloma Caring for people with cancer Understanding myeloma This booklet has been written to help you understand more about myeloma. It has been prepared and checked by doctors, haematologists,
Selected Issues in Nonneoplastic. Orthopaedic Pathology. Diseases of Diarthrodial Joints and their Complications
 1 2 3 Selected Issues in Nonneoplastic Orthopaedic Pathology Diseases of Diarthrodial Joints and their Complications Biology of articular hyaline cartilage Arthritis Osteonecrosis Prosthetic Joints Metabolic
1 2 3 Selected Issues in Nonneoplastic Orthopaedic Pathology Diseases of Diarthrodial Joints and their Complications Biology of articular hyaline cartilage Arthritis Osteonecrosis Prosthetic Joints Metabolic
Part 1 examination. Haematology: First paper. Tuesday 20 March Candidates must answer all questions. Each question is worth a total of 25 marks.
 Part 1 examination Haematology: First paper Tuesday 20 March 2018 Candidates must answer all questions. Each question is worth a total of 25 marks. Time allowed: 3 hours Question 1: General Haematology
Part 1 examination Haematology: First paper Tuesday 20 March 2018 Candidates must answer all questions. Each question is worth a total of 25 marks. Time allowed: 3 hours Question 1: General Haematology
Interesting case seminar: Native kidneys Case Report:
 Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Interesting case seminar: Native kidneys Case Report: Proximal tubulopathy and light chain deposition disease presented as severe pulmonary hypertension with right-sided cardiac dysfunction and nephrotic
Multiple Myeloma: diagnosis and prognostic factors. N Meuleman May 2015
 Multiple Myeloma: diagnosis and prognostic factors N Meuleman May 2015 Diagnosis Diagnostic assessment of myeloma: what should we know? Is it really a myeloma? Is there a need for treatment? What is the
Multiple Myeloma: diagnosis and prognostic factors N Meuleman May 2015 Diagnosis Diagnostic assessment of myeloma: what should we know? Is it really a myeloma? Is there a need for treatment? What is the
FBC interpretation. Dr. Gergely Varga
 FBC interpretation Dr. Gergely Varga #1 71 Y/O female, c/o weakness Test Undertaken : FBC (FBC) Sample Type: Whole Blood [ - 26.09.11 14:59] Hb 7.3 g/dl* 12.0-15.5 RBC 3.5 10^12/l * 3.80-5.60 Hct 0.24
FBC interpretation Dr. Gergely Varga #1 71 Y/O female, c/o weakness Test Undertaken : FBC (FBC) Sample Type: Whole Blood [ - 26.09.11 14:59] Hb 7.3 g/dl* 12.0-15.5 RBC 3.5 10^12/l * 3.80-5.60 Hct 0.24
POTENTIAL LINK BETWEEN GAUCHER DISEASE PATHWAYS
 POTENTIAL LINK BETWEEN GAUCHER DISEASE PATHWAYS AND THOSE OF PARKINSON DISEASE Hanna Rosenbaum, MD Hematology and Bone Marrow Transplantation Rambam Medical Center and Bruce Rappaport Faculty of Medicine
POTENTIAL LINK BETWEEN GAUCHER DISEASE PATHWAYS AND THOSE OF PARKINSON DISEASE Hanna Rosenbaum, MD Hematology and Bone Marrow Transplantation Rambam Medical Center and Bruce Rappaport Faculty of Medicine
Dr Kirsten Herbert. Dr Melita Kenealy. MBBS(Hons) FRCPA FRACP. Common Blood Tests
 FRCPA FRACP. Common Blood Tests") Common Blood Tests Your Haematologist may order numerous blood and urine tests to help diagse or manage your condition. Listed below are some of the more common tests that can be ordered in a haematology
Common Blood Tests Your Haematologist may order numerous blood and urine tests to help diagse or manage your condition. Listed below are some of the more common tests that can be ordered in a haematology
The ABCs of Waldenström s Macroglobulinemia (WM)
") The ABCs of Waldenström s Macroglobulinemia (WM) Jeffrey V. Matous MD Colorado Blood Cancer Institute IWMF Ed Forum May 2017 Objectives Describe the roots underneath WM Review incidence, possible risk
The ABCs of Waldenström s Macroglobulinemia (WM) Jeffrey V. Matous MD Colorado Blood Cancer Institute IWMF Ed Forum May 2017 Objectives Describe the roots underneath WM Review incidence, possible risk
What is meant by Thrombotic Microangiopathy (TMA)?
?") What is meant by Thrombotic Microangiopathy (TMA)? Thrombotic Microangiopathy (TMA) is a group of disorders characterized by injured endothelial cells, microangiopathic hemolytic anemia (MAHA), with its
What is meant by Thrombotic Microangiopathy (TMA)? Thrombotic Microangiopathy (TMA) is a group of disorders characterized by injured endothelial cells, microangiopathic hemolytic anemia (MAHA), with its
TREATMENTS FOR GAUCHER DISEASE
 TREATMENTS FOR GAUCHER DISEASE Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices
TREATMENTS FOR GAUCHER DISEASE Non-Discrimination Statement and Multi-Language Interpreter Services information are located at the end of this document. Coverage for services, procedures, medical devices
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Anemia(s), 412 426 categories in morphologic approach to, macrocytic, 412 414 microcytic, 412 414 normocytic, 412 413 categorizing, 412
Index Note: Page numbers of article titles are in boldface type. A Anemia(s), 412 426 categories in morphologic approach to, macrocytic, 412 414 microcytic, 412 414 normocytic, 412 413 categorizing, 412
An analysis of clinical profile and laboratory parameters in multiple myeloma
 Original article: An analysis of clinical profile and laboratory parameters in multiple myeloma 1 Aadarsh Sharma, 2 Dr.Swaroop N Shashidhar, 3 Karuna Rameshkumar, 4 L.N Samaga,, 5 Kishan Prasad HL, 6 Jayaprakash
Original article: An analysis of clinical profile and laboratory parameters in multiple myeloma 1 Aadarsh Sharma, 2 Dr.Swaroop N Shashidhar, 3 Karuna Rameshkumar, 4 L.N Samaga,, 5 Kishan Prasad HL, 6 Jayaprakash
Panobinostat, Bortezomib and Dexamethasone
 Panobinostat, Bortezomib and Dexamethasone Indication Treatment of relapsed/refractory multiple myeloma in patients who have received at least 2 prior regimens, including bortezomib and an immunomodulatory
Panobinostat, Bortezomib and Dexamethasone Indication Treatment of relapsed/refractory multiple myeloma in patients who have received at least 2 prior regimens, including bortezomib and an immunomodulatory
UNUSUAL PRESENTATIONS OF SYSTEMIC LUPUS ERYTHEMATOSUS
 UNUSUAL PRESENTATIONS OF SYSTEMIC LUPUS ERYTHEMATOSUS Presenter- Dr. Meghana B S Prof Dr. NAGARAJA B S Prof Dr. NIRMALA A C Dr. SIVARANJANI H Dr. B C PRAKASH Dr. MUMTAZ ALI KHAN A 60 year old lady, k/c/o
UNUSUAL PRESENTATIONS OF SYSTEMIC LUPUS ERYTHEMATOSUS Presenter- Dr. Meghana B S Prof Dr. NAGARAJA B S Prof Dr. NIRMALA A C Dr. SIVARANJANI H Dr. B C PRAKASH Dr. MUMTAZ ALI KHAN A 60 year old lady, k/c/o
Clinical & Laboratory Assessment
 Clinical & Laboratory Assessment Dr Roger Pool NHLS & University of Pretoria Clinical Assessment (History) Anaemia ( haemoglobin) Dyspnoea (shortness of breath) Tiredness Angina Headache Clinical Assessment
Clinical & Laboratory Assessment Dr Roger Pool NHLS & University of Pretoria Clinical Assessment (History) Anaemia ( haemoglobin) Dyspnoea (shortness of breath) Tiredness Angina Headache Clinical Assessment
Monoclonal Gammopathy with Systemic Amyloidosis: An Evaluation of Diagnostic Elements
 : 51-55 Monoclonal Gammopathy with Systemic Amyloidosis: An Evaluation of Diagnostic Elements 1 C. T Subashini*, 1 E. George & 2 U Nor Aini 1 Department of Pathology, Faculty of Medicine and Health Sciences,
: 51-55 Monoclonal Gammopathy with Systemic Amyloidosis: An Evaluation of Diagnostic Elements 1 C. T Subashini*, 1 E. George & 2 U Nor Aini 1 Department of Pathology, Faculty of Medicine and Health Sciences,
Leukemias. Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College
 Leukemias Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College Introduction Leukaemias are malignant disorders of the haematopoietic stem cell compartment,
Leukemias Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College Introduction Leukaemias are malignant disorders of the haematopoietic stem cell compartment,
Tracking Disease Status for Multiple Myeloma
 Tracking Disease Status for Multiple Myeloma This appendix is intended to provide additional resources when determining: Best response to line of therapy pre-transplant; Disease Status at the Last Evaluation
Tracking Disease Status for Multiple Myeloma This appendix is intended to provide additional resources when determining: Best response to line of therapy pre-transplant; Disease Status at the Last Evaluation
Haemostasis & Coagulation disorders Objectives:
 Haematology Lec. 1 د.ميسم مؤيد علوش Haemostasis & Coagulation disorders Objectives: - Define haemostasis and what are the major components involved in haemostasis? - How to assess the coagulation status?
Haematology Lec. 1 د.ميسم مؤيد علوش Haemostasis & Coagulation disorders Objectives: - Define haemostasis and what are the major components involved in haemostasis? - How to assess the coagulation status?
Myeloma Support Group: Now and the Horizon. Brian McClune, DO
 Myeloma Support Group: Now and the Horizon Brian McClune, DO Disclosures Consultant to Celgene Objectives Transplant for myeloma- is there any thing new? High risk disease University protocols New therapies?
Myeloma Support Group: Now and the Horizon Brian McClune, DO Disclosures Consultant to Celgene Objectives Transplant for myeloma- is there any thing new? High risk disease University protocols New therapies?
Case Workshop of Society for Hematopathology and European Association for Haematopathology
 Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
APPROACHING TO PANCYTOPENIA
 APPROACHING TO PANCYTOPENIA P A T C H A R E E K O M V I L A I S A K, M. D. A S S I S T A N T P R O F E S S O R D I V I S I O N O F P E D I A T R I C H E M A T O L O G Y O N C O L O G Y, D E P A R T M E
APPROACHING TO PANCYTOPENIA P A T C H A R E E K O M V I L A I S A K, M. D. A S S I S T A N T P R O F E S S O R D I V I S I O N O F P E D I A T R I C H E M A T O L O G Y O N C O L O G Y, D E P A R T M E
Jo Abraham MD Division of Nephrology University of Utah
 Jo Abraham MD Division of Nephrology University of Utah 68 year old male presented 3 weeks ago with a 3 month history of increasing fatigue He reported a 1 week history of increasing dyspnea with a productive
Jo Abraham MD Division of Nephrology University of Utah 68 year old male presented 3 weeks ago with a 3 month history of increasing fatigue He reported a 1 week history of increasing dyspnea with a productive
The importance of thrombocytopenia and its causes
 SYSMEX EDUCATIONAL ENHANCEMENT AND DEVELOPMENT NO 4 2017 SEED HAEMATOLOGY The importance of thrombocytopenia and its causes Key words: Thrombocytopenia, thrombocytopenic, low levels of platelets What is
SYSMEX EDUCATIONAL ENHANCEMENT AND DEVELOPMENT NO 4 2017 SEED HAEMATOLOGY The importance of thrombocytopenia and its causes Key words: Thrombocytopenia, thrombocytopenic, low levels of platelets What is
Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma:
 1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
1 Lancashire and South Cumbria Haematology NSSG Guidelines for Follicular Lymphoma: 2018-19 1.1 Pretreatment evaluation The following tests should be performed: FBC, U&Es, creat, LFTs, calcium, LDH, Igs/serum
Year 2002 Paper two: Questions supplied by Jo 1
 Year 2002 Paper two: Questions supplied by Jo 1 Question 70 A 25 year old previously well male student presents with recent exertional dyspnoea, epistaxis and bruising. There is no history of medication,
Year 2002 Paper two: Questions supplied by Jo 1 Question 70 A 25 year old previously well male student presents with recent exertional dyspnoea, epistaxis and bruising. There is no history of medication,
Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT
 The Kidney in Multiple Myeloma Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT Normal Cell Plasma cells produce antibodies that bind to antigens,
The Kidney in Multiple Myeloma Tarek ElBaz, MD. Prof. Internal Medicine Chief, Division of Renal Medicine Al Azhar University President, ESNT Normal Cell Plasma cells produce antibodies that bind to antigens,
Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN
 Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN The student should be able:» To identify the mechanism of homeostasis and the role of vessels, platelets
Dr. MUBARAK ABDELRAHMAN MD PEDIATRICS AND CHILD HEALTH Assistant Professor FACULTY OF MEDICINE -JAZAN The student should be able:» To identify the mechanism of homeostasis and the role of vessels, platelets
Case: The patient is a 73 year old woman with vague complaints of dyspepsia and abdominal pain. Upper endoscopy showed features of gastritis and a
 Case: The patient is a 73 year old woman with vague complaints of dyspepsia and abdominal pain. Upper endoscopy showed features of gastritis and a nodular lesion in the body of the stomach. The patient
Case: The patient is a 73 year old woman with vague complaints of dyspepsia and abdominal pain. Upper endoscopy showed features of gastritis and a nodular lesion in the body of the stomach. The patient
Congenital dyserythropoietic anaemia type II-like dysplastic anaemia preceding the development of non-hodgkin lymphoma a case report.
 Malaysian J Pathol 2005; 27(1) : 39 43 CONGENITAL DYSERYTHROPOIETIC ANAEMIA CASE REPORT Congenital dyserythropoietic anaemia type II-like dysplastic anaemia preceding the development of non-hodgkin lymphoma
Malaysian J Pathol 2005; 27(1) : 39 43 CONGENITAL DYSERYTHROPOIETIC ANAEMIA CASE REPORT Congenital dyserythropoietic anaemia type II-like dysplastic anaemia preceding the development of non-hodgkin lymphoma
There are two main causes of a low platelet count
 Thrombocytopenia Thrombocytopenia is a condition in which a person's blood has an unusually low level of platelets Platelets, also called thrombocytes, are found in a person's blood along with red blood
Thrombocytopenia Thrombocytopenia is a condition in which a person's blood has an unusually low level of platelets Platelets, also called thrombocytes, are found in a person's blood along with red blood
John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne
 John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne Overview of coagulation Testing coagulation Coagulopathy in ICU Incidence Causes Evaluation Management Coagulation
John Davidson Consultant in Intensive Care Medicine Freeman Hospital, Newcastle upon Tyne Overview of coagulation Testing coagulation Coagulopathy in ICU Incidence Causes Evaluation Management Coagulation
MYE FORMS REVEALED RESPONSE CODES OBJECTIVES. Stringent Complete Response (scr) Complete Response (CR) I have no conflicts of interest to disclose
 Complete Response (CR) I have no conflicts of interest to disclose") I have no conflicts of interest to disclose MYE FORMS REVEALED Janet Brunner, PA-C CIBMTR MKE New10_1.ppt OBJECTIVES 1) Be able to describe the criteria required for each myeloma response code 2) Be able
I have no conflicts of interest to disclose MYE FORMS REVEALED Janet Brunner, PA-C CIBMTR MKE New10_1.ppt OBJECTIVES 1) Be able to describe the criteria required for each myeloma response code 2) Be able
UKITP INITAL INFORMATION SHEET (2.4)
") UKITP INITAL INFORMATION SHEET (2.4) Barts Health NHS Trust The Royal London Hospital Pathology and Pharmacy Building 80 Newark Street, London E1 2ES Centre for Haematology Institute of and Molecular Science
UKITP INITAL INFORMATION SHEET (2.4) Barts Health NHS Trust The Royal London Hospital Pathology and Pharmacy Building 80 Newark Street, London E1 2ES Centre for Haematology Institute of and Molecular Science
Haematology and Haematological Oncology
 Haematology and Haematological Oncology Updated on 23 Feb 2017 I) OBJECTIVES 1. To provide a broad training and in-depth experience at a level sufficient for trainees to acquire competence and professionalism
Haematology and Haematological Oncology Updated on 23 Feb 2017 I) OBJECTIVES 1. To provide a broad training and in-depth experience at a level sufficient for trainees to acquire competence and professionalism
IMAGING FINDINGS OF GAUCHER DISEASE IN ALL OVER THE BODY
 IMAGING FINDINGS OF GAUCHER DISEASE IN ALL OVER THE BODY V. Katsaros 1, P. Lampropoulou 2, M. Mitropoulou 1, A. Nikolaou 1, C. Drossos 2 Departments of CT and MRI 1 IKA Oncology Hospital and 2 Athens General
IMAGING FINDINGS OF GAUCHER DISEASE IN ALL OVER THE BODY V. Katsaros 1, P. Lampropoulou 2, M. Mitropoulou 1, A. Nikolaou 1, C. Drossos 2 Departments of CT and MRI 1 IKA Oncology Hospital and 2 Athens General
HAEMATOLOGICAL MALIGNANCY
 HAEMATOLOGICAL MALIGNANCY Reference Compulsory reading Haematology at Glance 2 nd ed. Atul Mehta & Victor Hoffbrand Chapters: 20 to 31 Pages: 46 to 69 Pathogenesis of Haematological Malignancy Figure (a)
HAEMATOLOGICAL MALIGNANCY Reference Compulsory reading Haematology at Glance 2 nd ed. Atul Mehta & Victor Hoffbrand Chapters: 20 to 31 Pages: 46 to 69 Pathogenesis of Haematological Malignancy Figure (a)
Part 1 examination. Haematology: First paper. Tuesday 25 September 2018
 Part 1 examination Haematology: First paper Tuesday 25 September 2018 Candidates must answer all questions. Each question is worth a total of 25 marks. Time allowed: 3 hours 1. Haemato-oncology. A 22 year
Part 1 examination Haematology: First paper Tuesday 25 September 2018 Candidates must answer all questions. Each question is worth a total of 25 marks. Time allowed: 3 hours 1. Haemato-oncology. A 22 year
, Malcolm Tait, Barry Frank Jacobson, Evashin Pillay and Susan J. Louw. Elizabeth Sarah Mayne *
 Mayne et al. Thrombosis Journal (2018) 16:30 https://doi.org/10.1186/s12959-018-0184-2 CASE REPORT Open Access Combination of acquired von Willebrand syndrome (AVWS) and Glanzmann thrombasthenia in monoclonal
Mayne et al. Thrombosis Journal (2018) 16:30 https://doi.org/10.1186/s12959-018-0184-2 CASE REPORT Open Access Combination of acquired von Willebrand syndrome (AVWS) and Glanzmann thrombasthenia in monoclonal
Management of Multiple Myeloma: The Changing Paradigm
 Management of Multiple Myeloma: The Changing Paradigm High-Dose Chemotherapy and Stem Cell Transplantation Todd Zimmerman, MD University of Chicago Medical Center Case Presentation R.M. is a 64 year old
Management of Multiple Myeloma: The Changing Paradigm High-Dose Chemotherapy and Stem Cell Transplantation Todd Zimmerman, MD University of Chicago Medical Center Case Presentation R.M. is a 64 year old
Clinical Guidelines for Leukaemia and other Myeloid Disorders MDS
 Clinical Guidelines for Leukaemia and other Myeloid Disorders MDS Reference Number Version Status Executive Lead(s) Name and Job Title Author(s) Name and Job Title 13-2H-106 2 Dr Helen Barker MDT Lead
Clinical Guidelines for Leukaemia and other Myeloid Disorders MDS Reference Number Version Status Executive Lead(s) Name and Job Title Author(s) Name and Job Title 13-2H-106 2 Dr Helen Barker MDT Lead
monoclonal gammopathy of undetermin Citation Rheumatology international, 33(1),
,") NAOSITE: Nagasaki University's Ac Title Author(s) Renal thrombotic microangiopathies/ in a patient with primary Sjögren's monoclonal gammopathy of undetermin Koga, Tomohiro; Yamasaki, Satoshi; Atsushi;
NAOSITE: Nagasaki University's Ac Title Author(s) Renal thrombotic microangiopathies/ in a patient with primary Sjögren's monoclonal gammopathy of undetermin Koga, Tomohiro; Yamasaki, Satoshi; Atsushi;
GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS
 GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS This guideline covers the management of patients being treated with Vitamin K antagonists (VKA): Warfarin Acenocoumarol
GUIDELINES FOR MANAGEMENT OF BLEEDING AND EXCESSIVE ANTICOAGULATION WITH ORAL ANTICOAGULANTS This guideline covers the management of patients being treated with Vitamin K antagonists (VKA): Warfarin Acenocoumarol
Careers in Haematology
 Careers in Haematology A guide for medical students and junior doctors About haematology: Haematology is the medical speciality concerned with blood disorders. Your non-medical friends however will always
Careers in Haematology A guide for medical students and junior doctors About haematology: Haematology is the medical speciality concerned with blood disorders. Your non-medical friends however will always
Should we treat Smoldering MM patients? María-Victoria Mateos University Hospital of Salamanca Salamanca. Spain
 Should we treat Smoldering MM patients? María-Victoria Mateos University Hospital of Salamanca Salamanca. Spain Should we treat some patients with Stage I MM? Len-dex is a promising and atractive option
Should we treat Smoldering MM patients? María-Victoria Mateos University Hospital of Salamanca Salamanca. Spain Should we treat some patients with Stage I MM? Len-dex is a promising and atractive option
QUESTIONS OF HEMATOLOGY AND THEIR ANSWERS
 QUESTIONS OF HEMATOLOGY AND THEIR ANSWERS WHAT IS TRUE AND WHAT IS FALSE? Questions 1 Iron deficiency anemia a) Is usually associated with a raised MCV. b) The MCH is usually low. c) Is most commonly due
QUESTIONS OF HEMATOLOGY AND THEIR ANSWERS WHAT IS TRUE AND WHAT IS FALSE? Questions 1 Iron deficiency anemia a) Is usually associated with a raised MCV. b) The MCH is usually low. c) Is most commonly due
TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006
 TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006 CTU blood product transfusion guidelines 2006 1 Summary of guidelines RED CELLS (10-15ml/kg) This applies to ward patients / icu patients who are stable.
TRANSFUSION GUIDELINES FOR CARDIOTHORACIC UNIT 2006 CTU blood product transfusion guidelines 2006 1 Summary of guidelines RED CELLS (10-15ml/kg) This applies to ward patients / icu patients who are stable.
Amyloidosis: What to do and how to diagnose: An Update 2017
 Amyloidosis: What to do and how to diagnose: An Update 2017 Jonathan L. Kaufman, MD Associate Professor Hematology & Oncology Winship Cancer Institute of Emory University Amyloidosis Protein Conformation/Deposition
Amyloidosis: What to do and how to diagnose: An Update 2017 Jonathan L. Kaufman, MD Associate Professor Hematology & Oncology Winship Cancer Institute of Emory University Amyloidosis Protein Conformation/Deposition
WHO Classification. B-cell chronic lymphocytic leukemia/small T-cell granular lymphocytic leukemia
 Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
Blood Malignancies-II Prof. Dr. Herman Hariman, a Ph.D, SpPK (KH). Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. of Clinical Pathology, School of Medicine, University of North Sumatra WHO classification
Clinical Guidelines for Leukaemia and other Myeloid Disorders MDS
 Clinical Guidelines for Leukaemia and other Myeloid Disorders MDS Reference Number Version Status Executive Lead(s) Name and Job Title Author(s) Name and Job Title 13-2H-106 1 Dr Helen Barker MDT Lead
Clinical Guidelines for Leukaemia and other Myeloid Disorders MDS Reference Number Version Status Executive Lead(s) Name and Job Title Author(s) Name and Job Title 13-2H-106 1 Dr Helen Barker MDT Lead
Laboratory Examination
 Todd Zimmerman, M.D. 64 year old African American male presents to establish care with PCG. Meds: Norvasc 5 mg daily PMHx: HTN x 20 years, poorly controlled SHx: No tobacco, illicit; rare EtOH ROS: Negative
Todd Zimmerman, M.D. 64 year old African American male presents to establish care with PCG. Meds: Norvasc 5 mg daily PMHx: HTN x 20 years, poorly controlled SHx: No tobacco, illicit; rare EtOH ROS: Negative