Common Haematological Problems in Primary Care
|
|
|
- Clementine Ramsey
- 5 years ago
- Views:
Transcription


1 23 rd March 2019 GP Hot Topics In Primary Care Common Haematological Problems in Primary Care Dr Samar Kulkarni Consultant Haematologist-Oncologist and The Christie Private Care Manchester, UK.
2 Haematology? Haematology is the study of formed elements in blood including The white blood cells (leukocytes) The red blood cells (erythrocytes) The platelets (thrombocytes) All are derived from pluripotent stem cell in the bone marrow Bone marrow is the predominant site of pathology
3 RBCs Disorders Anaemias &Others WBC Disorders Benign & Malignant Hematological Disorders Haemostatic Disorders Transfusion Medicine
4 Overview of Haematological indices Anaemia Leucocytosis & Lymphocytosis Neutropenia Thrombocytopenia Paraprotein
5 Definition of Anaemia Anaemia is a functional inability of the blood to supply the tissue with adequate O 2 for proper metabolic function Anaemia is not a disease, but rather the expression of an underlying disorder or disease
6 Diagnosis of anemia Complete blood count, CBC, will include: An RBC count: At birth: x 10 9 /L Males: x 10 9 /L Females: is x 10 9 /L Hematocrit (Hct) or packed cell volume in % or At birth: 42-60% (42-60) Males: 41-53% (41-53) Females: 38-46% (38-46)

7 CBC and RBC indices fl pg g/dl %
8 The Three Derived Indices Measurement Normal Range A. RBC count 5 million 4 to 6 B. Hemoglobin 15 g% 12 to 17 C. Hematocrit to 50 A x 3= B x 3 = C (if not then micro or macrocytosis or hypochromia) MCV C A x 10 = 90 fl MCH B A x 10 = 30 pg MCHC B C x 100 = 33%
9 Diagnosis of Anaemia Hemoglobin concentration in grams/l At birth the normal range is g/l The normal range for males is g/l The normal range for females is g/l RBC indices Use results of the RBC count, hematocrit, and hemoglobin to calculate 4 parameters: Mean corpuscular volume (MCV) is the average volume/rbc in femtoliters (10-15 L) Hct (in %)/RBC (x /L) x 10 At birth the normal range is In adults the normal range is
10 Diagnosis of Anaemia Mean corpuscular hemoglobin (MCH) is the average weight of hemoglobin/cell in picograms (pg= g) Hgb (in g/dl)/rbc(x /L) x 10 At birth the normal range is In adults the normal range is Red cell distribution width (RDW) is a measurement of the variation in RBC cell size Standard deviation/mean MCV x 100 The range for normal values is % A value > 14.5 means that there is increased variation in cell size above the normal amount (anisocytosis) A value < 11.5 means that the RBC population is more uniform in size than normal.
11 Diagnosis of Anaemia The MCV is used to classify RBCs as: Normocytic (80-100) Microcytic (<80) Macrocytic (>100) Mean corpuscular hemoglobin concentration (MCHC) is the average concentration of hemoglobin in g/dl (or %) Hgb (in g/dl)/hct (in %)x 100 At birth the normal range is In adults the normal range is The MCHC is used to classify RBCs as: Normochromic (31-37) Hypochromic (<31)
12 Mean Cell Volume (MCV) RBC volume is measured by The Mean Cell Volume or MCV and RDW MCV Microcytic < 80 fl Normocyti Macrocytic c fl > 100 fl < 6.5 µ µ > 9 µ
13 Approach to Anemia CBC Reticulocyte count MCV RI < 2% RI > 2% Underproduction Increased destruction or loss MCV < 80 Microcytic MCV MCV Normocytic MCV > 100 Macrocytic Further work up Based on history, Physical, other
 and")
14 The definitive test is serum ferritin Low serum ferritin (<12 ug/l)is diagnostic of iron deficiency Although ferritin is an acute phase reactant, it will still be low in iron deficiency Also, high TIBC Fe saturation = Fe/TIBC < 10% in Fe deficiency If ferritin is indeterminate Low serum Fe is not in itself diagnostic, neither is marrow staining Anisocytosis (heterogeneous in shape) and poikilocytosis (abnormal shape) Reactive thrombocytosis Iron Deficiency Anemia
15 Macrocytic Anemia (MCV>100) Drug Induced (hydroxyurea, AZT, MTX, chemotherapy, anticonvulsants) B12 / folate deficiency Myelodysplastic syndrome Liver disease Alcohol abuse Reticulocytes Hypothyroidism

16 Leucocytosis Leucocytosis does not mean haematological malignancy Careful history Fevers, diarrhoea, drugs, smoking Examine Skin, liver, spleen, lymph nodes Ask for a blood film What is the white cell differential? What do the white cells look like? Is the rest of the FBC normal? Consider repeating the blood count 2-4 weeks.

17 Lymphocytosis Lymphocyte Count Investigation >10 x 10 9 /L Refer to haematology for investigation >3.5 and <10 x 10 9 /L Rest of blood count normal No lymphadenopathy or splenomegaly >3.5 and <10 x 10 9 /L and anaemia or thrombocytopenia or lymphadenopathy or splenomegaly Repeat FBC and Blood film in 3-6 months: If lymphocytes are lower or the same level: no further investigation or monitoring; repeat blood count in 1 year If lymphocytes are > 10 x10 9 /L: refer to haematology for investigation Refer to haematology for investigation

18 Asymptomatic lymphocytosis Early CLL - Stage A Normal Hb, neutrophils, platelets, no organomegaly Does not require treatment (usually) Increased risk of bacterial infection and zoster Annual flu vaccination and consider for Pneumovax May increase risk of other malignancies Clinical assessment and monitor blood count every few months initially
 Symptoms/signs often none, found on routine FBC May")

19 Chronic Lymphocytic Leukaemia (CLL) Accumulation of mature B cells Commonest leukaemia (4/100,000/year) Symptoms/signs often none, found on routine FBC May have enlarged rubbery non tender lymphadenopathy, hepato/spleomegaly and systemic symptoms Investigations Flow-cytometry, can cause autoimmune haemolysis and pancytopenia
20 Isolated Neutropenia Severity Categories of Neutropenia Severity Neutrophil Count Mild x10 9 /L Moderate x10 9 /L Severe <0.5 x10 9 /L
21 Causes of Neutropenia Transient Viral infections neutropenia usually lasts 2 weeks and rarely cause clinical problems Occasionally, the neutropenia may persist for months. Persistent Benign ethnic neutropenia Individuals of African-Caribbean or Middle Eastern descent Viral infections EBV, HIV, hepatitis Autoimmuine disorders Drugs Splenomegaly ( +liver disease) Haematological diseases Myelodysplasia, leukaemia, lymphoma, myeloma, B12/folate deficiency etc. Rare congenital
22 Evaluation of a patient with Neutropenia History: Symptoms or history of recurrent infection Drug history Family history of infections Records of past FBCs (chronicity of the neutropenia) Risk factors for HIV, TB Examination: Signs of infection: oral mucosa, skin rashes, abscesses, lung infections, perianal/genital area Splenomegaly Other signs of underlying medical problems (SLE, malignancy)
23 Investigations: Evaluation of Neutropenia Repeat FBC with differential Blood film (do the cells look normal?) Paul Bunnell (IMST) B12, folate Autoantibody screen & rheumatoid factor HIV testing if clinical risk factors are present Blood cultures if the patient is pyrexial (in which case send to hospital)
24 First checks- When to seek further advice or refer to Haematology? How severe is the neutropenia? Are there any other abnormalities of the blood count? Does the patient have any symptoms relating to the neutropenia? How long has the neutropenia persisted for? Consider referral if- Persistent neutropenia <1.3 x 10 9 /L over 6-8 weeks with no obvious cause Neutropenia associated with severe and/or recurrent infection Neutropenia associated with other full blood count abnormalities Neutropenia associated with splenomegaly (NOT due to liver disease fulfils 2 week wait criteria) Suspected underlying haematological disease: i.e. clinical symptoms or on blood film
25 Thrombocytopenia Normal count (x10 9 /L) Mild Moderate Severe <30 Consider Is the low platelet count acute or chronic? Are there associated abnormalities of other blood counts? Has the FBC been repeated? Does the patient have a history suggestive of infection, autoimmune disease, or malignancy?
26 Thrombocytopenia Medication history (the list is endless!)? Examine for spleen, lymph nodes, skin rashes, musculoskeletal abnormalities Request blood film: Platelet clumping May-Hegglin (large platelets that machine doesn t count) Hypersegmented neutrophils & macrocytosis (B12 / folate deficiency) Lymphocytosis etc. -? CLL Macrocytosis and Pelgeroid neutrophils - MDS
27 Thrombocytopenia Isolated thrombocytopenia, normal blood film and physical examination: bone marrow test may not be necessary If patient is asymptomatic: monitoring with serial blood counts is required Most patients with isolated mild thrombocytopenia do not develop clinical disease Those that do, the commonest group is autoimmune in origin Consider HIV and Hepatitis C as an underlying cause without other explanation
28 Leukaemia Acute leukemia is characterized by an abnormal proliferation of immature white blood cells, called blasts or progenitor cells Two main forms of acute leukemia Acute lymphoblastic leukemia A cancer at the earliest stages of lymphocyte maturation Occurs more often in the young Acute nonlymphoblastic leukemia Usually a malignancy of the myeloblast More common in adults
 B : Acute lymphoid")



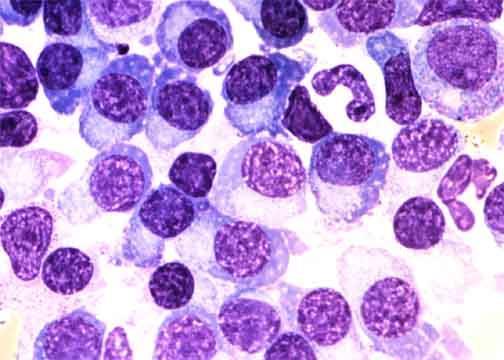
29 A B C D A : Picture of bone marrow smear (control) B : Acute lymphoid leukemia (ALL); Proliferation of small lymphoblasts. C : Acute myeloid leukemia (AML); Proliferation of large myeloblasts. D : Chronic myeloid leukemia (CML); Proliferation of granulocytes at various stages of maturation.
30 Functional Presentation of Leukaemia Leukaemia present with signs and symptoms of Anaemia Neutropenia with infection and fever Thrombocytopenia with bleeding Patients may present critically unwell


31 Physical Findings Fever Pallor Icterus Bruising/Bleeding Lymphadenopathy Liver or spleen enlargement Generally unwell
32 Disorder Associated with Monoclonal Protein Neoplastic cell proliferation Multiple myeloma Solitary plasmacytoma Waldenstrom macroglobulinemia Heavy chain disease Primary amyloidosis Undetermined significance Monoclonal gammopathy of undetermined significance (MGUS) Transient M protein Viral infection Post-valve replacement Malignacy Bowel cancer, Breast cancer Immune dysregulation HIV, Old age Chronic inflamation
33 Paraproteins Does the patient have symptoms? Does the patient have clinical signs (e.g. nodes)? How high is the paraprotein concentration? What sort of paraprotein is it? IgA / IgG ~ Myeloma IgM / IgG ~ Lymphoma Are the other Igs suppressed? Is the blood count normal? Are the renal function and calcium normal? Most paraproteins are incidental and usually represent MGUS
34 Monoclonal Gammopathy of Undetermined Significance (MGUS) Common, age-related Prevalence: 3.2% in persons over 50 yrs old (Minnesota) Approximately 5% in age above 70yr Higher prevalence in African populations.? Association with inflammatory states: obesity, Gaucher s disease Increased risk for thrombosis and fractures Risk of progression in entire population: 1% per year Risk factors for progression: %PC, level M spike, raised free light chain, IgA protein,?decline in uninvolved Ig s
35 Probability of Progression among 1384 Residents of Southeastern Minnesota in Whom Monoclonal Gammopathy of Undetermined Significance (MGUS) Was Diagnosed from 1960 through 1994 Kyle, R. A. et al. N Engl J Med 2002;346: Risk of progression to serious disease 1% per year
36 1% of people > 50 yrs age 10% of people > 80 yrs age 10% will develop myeloma How to monitor? MGUS: How to Monitor 6 monthly FBC, U&E, calcium, and paraprotein quantitation Refer to haematology if- Falling Hb, Rising urea or calcium, Rising paraprotein, bone pain, lymphadenopathy
37 Criteria for Diagnosis MGUS <3 g M spike <10% PC Smoldering MM 3 g M spike OR 10% PC Active MM 10% PC M spike + AND AND CRAB Negative CRAB: Positive CRAB: Calcium, Renal, Anaemia, Bones Kyle RA. N Engl J Med 2002; 346: 564
38 Myeloma Malignant clonal proliferation of plasma cells Incidence 5/100,000, peak age 70 years Symptoms and signs: - Osteolytic bone lesions backache, pathological fractures. - Hypercalcaemia - Anaemia, thrombocytopenia, neutropenia - Recurrent bacterial infections - Renal impairment (light chain deposition) - Can present acutely with cord compression, hyperviscocity or renal failure.
39 Number of cases 0-4 How common is it in UK? 1% of All Cancers 2 nd common Haematological Malignancy Rate per 100,000 population per 100,000 Numbers of new 3-4 cases cases and in age 35 yr./gp specific Surgery incidence rates, Male cases Female cases Male rates Female rates Age at diagnosis
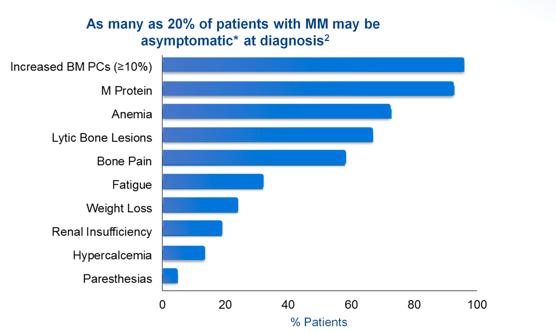
40 Clinical presentation
41 Diagnostic Evaluation History and physical examination Blood work-up Full blood count Urea, Creatinine, Calcium, Albumin Serum protein electrophoresis (SPEP) and immunofixation Serum free light chains 2 -microglobulin Urine Bence Jone Protein Skeletal survey Bone marrow examination with cytogenetics

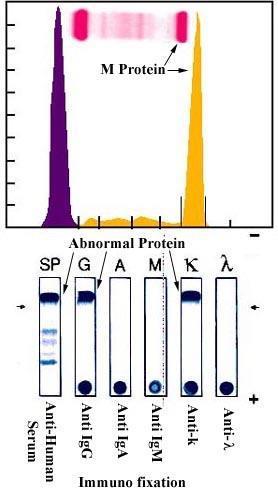
42 Myeloma
43 International Staging System (ISS) For Symptomatic Myeloma Stage I Criteria β2m < 3.5 mg/l albumin 3.5 g/dl Median Survival (mo) 62 II* Not stage I or III 44 III β2m 5.5 mg/l 29 *β2m < 3.5 mg/l and albumin < 3.5 g/dl or β2m < 5.5 mg/l, any albumin Greipp et al. J Clin Oncol 2005; 23:
 1.0 0.8 0.")

44 Survival Impact of Novel Agents on the Outcome in Post ASCT Relapsed/refractory Disease (n=387) Relapsed before 1998 Relapsed Relapsed Relapsed Relapsed P< Time (months) Kumar et al Blood 2008
45 Impact of New Drugs on Survival in BC Date of Diagnosis % alive at 5 years Before % 2003 and beyond 70%
46 Myeloma Drugs Drug Year of Approval (USA) Monthly Medicare Price at time of Approval Melphalan Bortezomib Lenalidomide Thalidomide Daratumomab Ixazonib
47 Suspected Haematological Cancers Combinations of the following symptoms and signs may suggest haematological cancer Fatigue Drenching night sweats Fever Weight loss Generalised pruritus Breathlessness Bruising Bleeding Recurrent infections Bone pain Alcohol-induced pain Abdominal pain Lymphadenopathy Splenomegaly Hepatomegaly
48 If unsure what to do or a Haematology patient is unwell, never hesitate to contact haematologist day or night
49 CBC Components Red Blood Cells (RBCs) Haematocrit (Hct) Haemoglobin (Hgb) Mean Corpuscular Volume (MCV) Mean Corpuscular Haemoglobin(MCH) Mean Corpuscular Haemoglobin Concentration (MCHC) Red cell distribution width (RDW) White Blood Cells (WBCs) Platelets Mean Platelet Volume (MPV)
50 Neutropenia The severity of neutropenia is categorised as Severity Neutrophil count (x10 9 /L) Mild Moderate Severe <0.5
51 Causes of Neutropenia Transient Viral infections: usually lasts 2 week seldom any clinical problems Occasionally may persist for months Persistent Benign ethnic neutropenia- African-Caribbean or Middle Eastern descent Viral infections : EBV, HIV, hepatitis Autoimmune disorders: SLE, RA Drugs: A long list! Splenomegaly Haematological diseases: MDS, leukaemia, lymphoma, myeloma, B12/folate deficiency
52 Evaluation of a patient with neutropenia History: History of recurrent infection? Drug history Family history of infections Records of past FBCs to establish the chronicity of the neutropenia Risk factors for HIV, TB Examination: Signs of infection: oral mucosa, skin rashes, abscesses, lung infections, perianal/genital area Splenomegaly Other signs of causative medical problems (SLE, malignancy)
53 First check: How severe? Neutropenia When to seek advice or refer to Haematology? Any other abnormalities of the blood count? Any symptoms relating to the neutropenia? How long has it persisted? Consider referral if: Persistent neutropenia <1.3 x 10 9 /L over 6-8 weeks Associated severe and/or recurrent infection Associated other full blood count abnormalities Associated splenomegaly (NOT due to liver disease fulfils 2 week wait criteria) Suspected underlying haematological disease clinical symptoms
54 If unsure what to do or a Haematology patient is unwell, never hesitate to contact haematologist day or night
Hematology 101. Rachid Baz, M.D. 5/16/2014
 Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
Hematology 101 Rachid Baz, M.D. 5/16/2014 Florida 101 Epidemiology Estimated prevalence 8,000 individuals in U.S (compare with 80,000 MM patients) Annual age adjusted incidence 3-8/million-year 1 More
Rory McCulloch. Specialty Trainee Haematology Royal Devon & Exeter Hospital
 Rory McCulloch Specialty Trainee Haematology Royal Devon & Exeter Hospital Anaemia 1 Haematological disorders Anaemia 2 Non-haematological disorders Substrates: Iron, folate, vitamin B12 Red cell mass
Rory McCulloch Specialty Trainee Haematology Royal Devon & Exeter Hospital Anaemia 1 Haematological disorders Anaemia 2 Non-haematological disorders Substrates: Iron, folate, vitamin B12 Red cell mass
GP Referral Guidelines. for. South Wales Cancer Network. Document Control Sheet. Specialty/Project Haematological Site Specific Group
 GP Referral Guidelines for South Wales Cancer Network Document Control Sheet Organisation South Wales Cancer Network Specialty/Project Haematological Site Specific Group Document Title GP Referral Guidelines
GP Referral Guidelines for South Wales Cancer Network Document Control Sheet Organisation South Wales Cancer Network Specialty/Project Haematological Site Specific Group Document Title GP Referral Guidelines
Haematological Cancer Suspected (Adults & Children)
") Haematological Cancer Suspected (Adults & Children) Link to NICE guidelines: https://www.nice.org.uk/guidance/ng47 Patient of any age presents with symptoms of possible haematological cancer If 60 years
Haematological Cancer Suspected (Adults & Children) Link to NICE guidelines: https://www.nice.org.uk/guidance/ng47 Patient of any age presents with symptoms of possible haematological cancer If 60 years
HEFT Pathology Guideline. GP Investigation and Referral Pathways for leucocyte, platelet disturbances and polycythaemia
 HEFT Pathology Guideline GP Investigation and Referral Pathways for leucocyte, platelet disturbances and polycythaemia Produced by: Dr Charalampos Kartsios (Consultant Haematologist) and Muhammad Javed
HEFT Pathology Guideline GP Investigation and Referral Pathways for leucocyte, platelet disturbances and polycythaemia Produced by: Dr Charalampos Kartsios (Consultant Haematologist) and Muhammad Javed
Anaemias and other Pesky Haematology Questions
 Anaemias and other Pesky Haematology Questions 3 main topics How do I work out an anaemia.. That oh too common paraprotein patient. Those mildly raised lymphocyte count GP discussed patient with me over
Anaemias and other Pesky Haematology Questions 3 main topics How do I work out an anaemia.. That oh too common paraprotein patient. Those mildly raised lymphocyte count GP discussed patient with me over
Michael Joffe ST6 Haematology SpR
 Michael Joffe ST6 Haematology SpR Mrs SB 71 year old female on AMU Telephone referral to haematology by medicine with Hb 102 MCV 89, normal B12, Folate, Ferritin. PMH DM General decline over several weeks
Michael Joffe ST6 Haematology SpR Mrs SB 71 year old female on AMU Telephone referral to haematology by medicine with Hb 102 MCV 89, normal B12, Folate, Ferritin. PMH DM General decline over several weeks
Collect and label sample according to standard protocols. Gently invert tube 8-10 times immediately after draw. DO NOT SHAKE. Do not centrifuge.
 Complete Blood Count CPT Code: CBC with Differential: 85025 CBC without Differential: 85027 Order Code: CBC with Differential: C915 Includes: White blood cell, Red blood cell, Hematocrit, Hemoglobin, MCV,
Complete Blood Count CPT Code: CBC with Differential: 85025 CBC without Differential: 85027 Order Code: CBC with Differential: C915 Includes: White blood cell, Red blood cell, Hematocrit, Hemoglobin, MCV,
FBC interpretation. Dr. Gergely Varga
 FBC interpretation Dr. Gergely Varga #1 71 Y/O female, c/o weakness Test Undertaken : FBC (FBC) Sample Type: Whole Blood [ - 26.09.11 14:59] Hb 7.3 g/dl* 12.0-15.5 RBC 3.5 10^12/l * 3.80-5.60 Hct 0.24
FBC interpretation Dr. Gergely Varga #1 71 Y/O female, c/o weakness Test Undertaken : FBC (FBC) Sample Type: Whole Blood [ - 26.09.11 14:59] Hb 7.3 g/dl* 12.0-15.5 RBC 3.5 10^12/l * 3.80-5.60 Hct 0.24
FBC CASES Vernon Louw Clinical Haematology 2010
 FBC CASES Vernon Louw Clinical Haematology 2010 FOR EACH OF THE FOLLOWING PATIENTS, SELECT THE MOST LIKELY FINDING FROM THE ANALYSIS OF THE PERIPHERAL BLOOD. A patient with infectious mononucleosis. A
FBC CASES Vernon Louw Clinical Haematology 2010 FOR EACH OF THE FOLLOWING PATIENTS, SELECT THE MOST LIKELY FINDING FROM THE ANALYSIS OF THE PERIPHERAL BLOOD. A patient with infectious mononucleosis. A
GP CME. James Liang Consultant Haematologist. Created by: Date:
 GP CME James Liang Consultant Haematologist Date: Created by: Scenario 52 year old European male Fit and well Brother recently diagnosed with diabetes PMHx Nil Social Hx Ex-smoker stopped 5 years ago (20
GP CME James Liang Consultant Haematologist Date: Created by: Scenario 52 year old European male Fit and well Brother recently diagnosed with diabetes PMHx Nil Social Hx Ex-smoker stopped 5 years ago (20
Evaluation of Anemia. Md. Shafiqul Bari Associate professor (Medicine) SOMC
 SOMC") Evaluation of Anemia Md. Shafiqul Bari Associate professor (Medicine) SOMC Definition Anemia is operationally defined as a reduction in one or more of the major RBC measurements Hemoglobin concentration
Evaluation of Anemia Md. Shafiqul Bari Associate professor (Medicine) SOMC Definition Anemia is operationally defined as a reduction in one or more of the major RBC measurements Hemoglobin concentration
Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss
 Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss Joanne Eddington, MN, FNP, AOCN Providence Oncology and Hematology Care Clinic - Eastside Blood Cell Abnormalities Abnormalities
Taking The Fear Out of Abnormal CBC s Problems of Production, Destruction or loss Joanne Eddington, MN, FNP, AOCN Providence Oncology and Hematology Care Clinic - Eastside Blood Cell Abnormalities Abnormalities
Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust
 Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust Regional Paediatric Specialty Trainees teaching 4 th July 2017 Scope
Abnormal blood counts in children Dr Tina Biss Consultant Paediatric Haematologist Newcastle upon Tyne Hospitals NHS Foundation Trust Regional Paediatric Specialty Trainees teaching 4 th July 2017 Scope
I. Definitions. V. Evaluation A. History B. Physical Exam C. Laboratory evaluation D. Bone marrow examination E. Specialty referrals
 I. Definitions II. III. Red blood cell life cycle Iron metabolism IV. Causes of anemia A. Kinetic approach 1. decreased production 2. increased destruction 3. blood loss B. Morphologic approach 1. normocytic
I. Definitions II. III. Red blood cell life cycle Iron metabolism IV. Causes of anemia A. Kinetic approach 1. decreased production 2. increased destruction 3. blood loss B. Morphologic approach 1. normocytic
The Complete Blood Count
 The Complete Blood Count (Cartesian Thinking at Its Best) A SEM Image of Normal Human Blood Laurie Larsson February 22, 2010 Anatomy and Philology II Dr. Danil Hammoudi Introduction A complete blood count
The Complete Blood Count (Cartesian Thinking at Its Best) A SEM Image of Normal Human Blood Laurie Larsson February 22, 2010 Anatomy and Philology II Dr. Danil Hammoudi Introduction A complete blood count
Problem Based Learning
 Problem Based Learning 2 Dania Qarqash&OmaymaHassanin Enas Ajarma Dr.Hikmat Abdel-Razeq Clinical hematology is divided into four subjects : 1- Benign hematology Anemia Benign WBC disorders Bone marrow
Problem Based Learning 2 Dania Qarqash&OmaymaHassanin Enas Ajarma Dr.Hikmat Abdel-Razeq Clinical hematology is divided into four subjects : 1- Benign hematology Anemia Benign WBC disorders Bone marrow
Western Health Specialist Clinics Access & Referral Guidelines
 Haematology Specialist Clinics at Western Health: Western Health runs MBS funded Specialist Clinics on a Wednesday and Thursday afternoon at its Sunshine Hospital site for patients who require assessment
Haematology Specialist Clinics at Western Health: Western Health runs MBS funded Specialist Clinics on a Wednesday and Thursday afternoon at its Sunshine Hospital site for patients who require assessment
Year 2003 Paper two: Questions supplied by Tricia
 QUESTION 65 A 36-year-old man presents in a post-ictal state after an observed generalised seizure. Full blood investigation shows: haemoglobin 0 g/l [128-175] mean corpuscular volume (MCV) 106 fl [80-7]
QUESTION 65 A 36-year-old man presents in a post-ictal state after an observed generalised seizure. Full blood investigation shows: haemoglobin 0 g/l [128-175] mean corpuscular volume (MCV) 106 fl [80-7]
2013 AAIM Pathology Workshop
 2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
Diseases Of The Blood
 Diseases Of The Blood DR. Associate Professor Of Pathology Faculty Of Medicine Ain Shams University Red Blood Cells and Anemia RBC=4-6 million/mm 2 Hb=12-18 g/dl Oxygen Carrying Molecule Hemoglobin Tetramer:
Diseases Of The Blood DR. Associate Professor Of Pathology Faculty Of Medicine Ain Shams University Red Blood Cells and Anemia RBC=4-6 million/mm 2 Hb=12-18 g/dl Oxygen Carrying Molecule Hemoglobin Tetramer:
King s Health Partners Haematology Institute and Network GP Referral Guide, Adult Haematology
 King s Health Partners Haematology Institute and Network GP Referral Guide, Adult Haematology 1 Version control: There are two controlled versions of this document, one for GSTT and one for KCH. While
King s Health Partners Haematology Institute and Network GP Referral Guide, Adult Haematology 1 Version control: There are two controlled versions of this document, one for GSTT and one for KCH. While
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure
 Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
HAEMATOLOGICAL EVALUATION OF ANEMIA. Sitalakshmi S Professor and Head Department of Clinical Pathology St John s medical College, Bangalore
 HAEMATOLOGICAL EVALUATION OF ANEMIA Sitalakshmi S Professor and Head Department of Clinical Pathology St John s medical College, Bangalore Learning Objectives Laboratory tests for the evaluation of anemia
HAEMATOLOGICAL EVALUATION OF ANEMIA Sitalakshmi S Professor and Head Department of Clinical Pathology St John s medical College, Bangalore Learning Objectives Laboratory tests for the evaluation of anemia
Clinical & Laboratory Assessment
 Clinical & Laboratory Assessment Dr Roger Pool NHLS & University of Pretoria Clinical Assessment (History) Anaemia ( haemoglobin) Dyspnoea (shortness of breath) Tiredness Angina Headache Clinical Assessment
Clinical & Laboratory Assessment Dr Roger Pool NHLS & University of Pretoria Clinical Assessment (History) Anaemia ( haemoglobin) Dyspnoea (shortness of breath) Tiredness Angina Headache Clinical Assessment
namib la UnIVERSITY OF SCIEnCE AnD TECHnOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES
 namib la UnIVERSITY OF SCIEnCE AnD TECHnOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES QUALIFICATION: BACHELOR OF BIOMEDICAL SCIENCES QUALIFICATION CODE: SOBBMS LEVEL: 6 COURSE
namib la UnIVERSITY OF SCIEnCE AnD TECHnOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES QUALIFICATION: BACHELOR OF BIOMEDICAL SCIENCES QUALIFICATION CODE: SOBBMS LEVEL: 6 COURSE
r). SUPPLEMENTARY/SECOND OPPORTUNITY EXAMINATION PAPER nnmlbih UNIVERSITY Sophia Blaauw INSTRUCTIONS FACULTY OF HEALTH AND APPLIED SCIENCES
. SUPPLEMENTARY/SECOND OPPORTUNITY EXAMINATION PAPER nnmlbih UNIVERSITY Sophia Blaauw INSTRUCTIONS FACULTY OF HEALTH AND APPLIED SCIENCES") r). nnmlbih UNIVERSITY OF SCIEFICE nnd TECHNOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES QUALIFICATION: BACHELOR OF MEDICAL LABORATORY SCIENCES QUALIFICATION CODE: 08BMLS
r). nnmlbih UNIVERSITY OF SCIEFICE nnd TECHNOLOGY FACULTY OF HEALTH AND APPLIED SCIENCES DEPARTMENT OF HEALTH SCIENCES QUALIFICATION: BACHELOR OF MEDICAL LABORATORY SCIENCES QUALIFICATION CODE: 08BMLS
Haematology dilemma s to refer or not to refer?
 Haematology dilemma s to refer or not to refer? NWL Pathology GP Study Day Dr Fatts Chowdhury Consultant Haematologist in Transfusion Medicine NHS Blood and Transplant Senior Honorary Clinical Lecturer
Haematology dilemma s to refer or not to refer? NWL Pathology GP Study Day Dr Fatts Chowdhury Consultant Haematologist in Transfusion Medicine NHS Blood and Transplant Senior Honorary Clinical Lecturer
Platelet and WBC disorders
 Division of Family Practice Platelet and WBC disorders Adrian Yee MD FRCPC Clinical hematologist Assistant Dean, undergraduate education, IMP asyee@uvic.ca When we understand that slide, we'll have won
Division of Family Practice Platelet and WBC disorders Adrian Yee MD FRCPC Clinical hematologist Assistant Dean, undergraduate education, IMP asyee@uvic.ca When we understand that slide, we'll have won
Pathology of Hematopoietic and Lymphoid tissue
 CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
CONTENTS Pathology of Hematopoietic and Lymphoid tissue White blood cells and lymph nodes Quantitative disorder of white blood cells Reactive lymphadenopathies Infectious lymphadenitis Tumor metastasis
Southern Derbyshire Shared Care Pathology Guidelines. MGUS (Monoclonal Gammopathy of Undetermined Significance)
") Southern Derbyshire Shared Care Pathology Guidelines MGUS (Monoclonal Gammopathy of Undetermined Significance) Purpose of guideline This guideline provides information about the risk stratification of
Southern Derbyshire Shared Care Pathology Guidelines MGUS (Monoclonal Gammopathy of Undetermined Significance) Purpose of guideline This guideline provides information about the risk stratification of
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA. April 16, 2008
 MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
MECHANISMS OF HUMAN DISEASE: LABORATORY SESSIONS LYMPHOMA April 16, 2008 FACULTY COPY GOAL: Learn the appearance of normal peripheral blood elements and lymph nodes. Recognize abnormal peripheral blood
King s Health Partners Haematology Institute and Network GP Referral Guide, Adult Haematology
 King s Health Partners Haematology Institute and Network GP Referral Guide, Adult Haematology For two week wait pathway, please continue to use existing documentation/pathways. Telephone advice and guidance
King s Health Partners Haematology Institute and Network GP Referral Guide, Adult Haematology For two week wait pathway, please continue to use existing documentation/pathways. Telephone advice and guidance
Pathology. #11 Acute Leukemias. Farah Banyhany. Dr. Sohaib Al- Khatib 23/2/16
 35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016
 + M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016 + Disclosures Advisory Boards: AMGEN, Lundbeck, NOVARTIS + Subtypes of Plasma Cell Disorders Increased Plasma
+ M-Protien, what to do next? Ismail A Sharif MD, FRCPc Internal Medicine Day 22 nd April 2016 + Disclosures Advisory Boards: AMGEN, Lundbeck, NOVARTIS + Subtypes of Plasma Cell Disorders Increased Plasma
Interpreting Blood Tests Part 1. Dr Andrew Smith
 Interpreting Blood Tests Part 1 Dr Andrew Smith Outline Part 1 (This Week) Introduction Which Tube!?! FBCs U+Es Part 2 (Next Week): More Electrolytes LFTs Clotting Extras Introduction Bloods are a core
Interpreting Blood Tests Part 1 Dr Andrew Smith Outline Part 1 (This Week) Introduction Which Tube!?! FBCs U+Es Part 2 (Next Week): More Electrolytes LFTs Clotting Extras Introduction Bloods are a core
Deconstructing the CBC
 Deconstructing the CBC Dr. Ann M. Wexler Solano Hematology Oncology September 10, 2017 What Are the Major Components of Blood? Red Blood Cells (also called erythrocytes) White Blood Cells (also called
Deconstructing the CBC Dr. Ann M. Wexler Solano Hematology Oncology September 10, 2017 What Are the Major Components of Blood? Red Blood Cells (also called erythrocytes) White Blood Cells (also called
Borderline cytopenias. Dr Taku Sugai Consultant Haematologist
 Borderline cytopenias Dr Taku Sugai Consultant Haematologist Borderline cytopenias Neutropenia Thrombocytopenia Anaemia with normal haematinics Two recent cases of cytopenias Neutropenia ANC of more than
Borderline cytopenias Dr Taku Sugai Consultant Haematologist Borderline cytopenias Neutropenia Thrombocytopenia Anaemia with normal haematinics Two recent cases of cytopenias Neutropenia ANC of more than
Symptoms and Signs in Hematology (2)/ 2013
/ 2013") Symptoms and Signs in Hematology (2)/ 2013 Abdallah Abbadi.MD.FRCP Professor of Medicine,Hematology & Oncology University of Jordan & JUH Email: abdalla.awidi@gmail.com Case one: A 24 yr old female complains
Symptoms and Signs in Hematology (2)/ 2013 Abdallah Abbadi.MD.FRCP Professor of Medicine,Hematology & Oncology University of Jordan & JUH Email: abdalla.awidi@gmail.com Case one: A 24 yr old female complains
Interpreting the CBC. Robert Miller PA Assistant Professor of Clinical Pediatrics and Family Medicine USC Keck School of Medicine Retired
 Interpreting the CBC Robert Miller PA Assistant Professor of Clinical Pediatrics and Family Medicine USC Keck School of Medicine Retired The CBC 3 Cell Lines RBCs WBCs Platelets Assess general health Make
Interpreting the CBC Robert Miller PA Assistant Professor of Clinical Pediatrics and Family Medicine USC Keck School of Medicine Retired The CBC 3 Cell Lines RBCs WBCs Platelets Assess general health Make
Disorders of Blood Cells & Blood Coagulation
 Disorders of Blood Cells & Blood Coagulation HIHIM 409 WBC count RBC count WBC differential Hemoglobin (HGB) Hematocrit (HCT) % of volume occupied by RBCs CBC Red cell indices Mean cell volume (MCV) average
Disorders of Blood Cells & Blood Coagulation HIHIM 409 WBC count RBC count WBC differential Hemoglobin (HGB) Hematocrit (HCT) % of volume occupied by RBCs CBC Red cell indices Mean cell volume (MCV) average
Aplastic anamia & Sideroblastic anemia
 Hematology Lecture 7 كلية التقنيات الصحية والطبية قسم التحليالت المرضية Aplastic anamia & Sideroblastic anemia اإلعداد: ظفر جبار دهاق فؤاد APLASTIC ANEMIA What is Aplastic anemia? Aplastic anemia is a
Hematology Lecture 7 كلية التقنيات الصحية والطبية قسم التحليالت المرضية Aplastic anamia & Sideroblastic anemia اإلعداد: ظفر جبار دهاق فؤاد APLASTIC ANEMIA What is Aplastic anemia? Aplastic anemia is a
Smoldering Multiple Myeloma. A Case Study
 Smoldering Multiple Myeloma A Case Study Case Presentation 53-Year-Old Male Patient presented for a routine exam No prior history of disease or family history of fhematologic disorders d or malignancies,
Smoldering Multiple Myeloma A Case Study Case Presentation 53-Year-Old Male Patient presented for a routine exam No prior history of disease or family history of fhematologic disorders d or malignancies,
Adult Acute leukemia. Matthew Seftel. August
 Adult Acute leukemia Matthew Seftel August 21 2007 mseftel@cancercare.mb.ca Principles 3 cases Diagnosis and classification of acute leukemia (AL) Therapy Emergencies Remission induction BMT Complications
Adult Acute leukemia Matthew Seftel August 21 2007 mseftel@cancercare.mb.ca Principles 3 cases Diagnosis and classification of acute leukemia (AL) Therapy Emergencies Remission induction BMT Complications
Pathology of Hematopoietic and Lymphoid tissue
 Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Pathology of Hematopoietic and Lymphoid tissue Peerayut Sitthichaiyakul, M.D. Department of Pathology and Forensic Medicine Faculty of Medicine, Naresuan University CONTENTS White blood cells and lymph
Full Blood Count analysis Is a 3 part-diff good enough? Dr Marion Münster, Sysmex South Africa
 Full Blood Count analysis Is a 3 part-diff good enough? Dr Marion Münster, Sysmex South Africa The Role of the FBC in clinical decision making History Examination Investigations Decision 70% FBC Laboratory
Full Blood Count analysis Is a 3 part-diff good enough? Dr Marion Münster, Sysmex South Africa The Role of the FBC in clinical decision making History Examination Investigations Decision 70% FBC Laboratory
Leukocytosis - Some Learning Points
 Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Candidates must answer ALL questions
 Time allowed: Three hours. Part 1 examination Haematology: First paper Tuesday 22 March 2016 Candidates must answer ALL questions Question 1: General Haematology A 16 year old non-european is referred
Time allowed: Three hours. Part 1 examination Haematology: First paper Tuesday 22 March 2016 Candidates must answer ALL questions Question 1: General Haematology A 16 year old non-european is referred
Approach to the child with anemia. Nittaya Wisanuyothin,MD. Pediatrics Department, Maharat Nakhonratchasima Hospital
 Approach to the child with anemia Nittaya Wisanuyothin,MD. Pediatrics Department, Maharat Nakhonratchasima Hospital Definition of anemia Hb< 2 SD or P2.5 below the mean for a healthy of the same gender
Approach to the child with anemia Nittaya Wisanuyothin,MD. Pediatrics Department, Maharat Nakhonratchasima Hospital Definition of anemia Hb< 2 SD or P2.5 below the mean for a healthy of the same gender
HEAMATOLOGICAL INDICES AND BONE MARROW BIOPSY
 HEAMATOLOGICAL INDICES AND BONE MARROW BIOPSY HEMATOCRIT Hematocrit is a measure of the percentage of the total blood volume that is made up by the red blood cells The hematocrit can be determined directly
HEAMATOLOGICAL INDICES AND BONE MARROW BIOPSY HEMATOCRIT Hematocrit is a measure of the percentage of the total blood volume that is made up by the red blood cells The hematocrit can be determined directly
Anemia 1: Fourth year Medical Students/ October/21/ 2015/ Abdallah Abbadi.MD.FRCP Professor
 Anemia 1: Fourth year Medical Students/ October/21/ 2015/ Abdallah Abbadi.MD.FRCP Professor Email: abdalla.awidi@gmail.com Main Hematological diseases A- Benign Hematology 1- Anemias 2- Bleeding disorders
Anemia 1: Fourth year Medical Students/ October/21/ 2015/ Abdallah Abbadi.MD.FRCP Professor Email: abdalla.awidi@gmail.com Main Hematological diseases A- Benign Hematology 1- Anemias 2- Bleeding disorders
Cytopaenias in HIV. Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH
 Cytopaenias in HIV Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH Introduction Cytopaenias in HIV are common Anaemias multifactorial causes Thrombocytopaenias may be the first
Cytopaenias in HIV Dr Maresce Bizaare Specialist Physician Clinical Haematology Fellow IALCH Introduction Cytopaenias in HIV are common Anaemias multifactorial causes Thrombocytopaenias may be the first
Lec-14 د.خالد نافع. Medicine. Multiple Myeloma
 Fifth stage Lec-14 د.خالد نافع Medicine 24/4/2016 Multiple Myeloma Plasma cell myeloma Variants Non - secretory myeloma Indolent myeloma Smouldering myeloma Plasma cell leukaemia Plasmacytoma - Solitary
Fifth stage Lec-14 د.خالد نافع Medicine 24/4/2016 Multiple Myeloma Plasma cell myeloma Variants Non - secretory myeloma Indolent myeloma Smouldering myeloma Plasma cell leukaemia Plasmacytoma - Solitary
The LaboratoryMatters
 Laboratory Medicine Newsletter for clinicians, pathologists & clinical laboratory technologists. A Initiative. Complete Blood Count This issue highlights: CBC, while ubiquitous, is an excellent diagnostic
Laboratory Medicine Newsletter for clinicians, pathologists & clinical laboratory technologists. A Initiative. Complete Blood Count This issue highlights: CBC, while ubiquitous, is an excellent diagnostic
If unqualified, Complete remission is considered to be Haematological complete remission
 Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Blood Cancers in the Community
 Over to you, mate Blood Cancers in the Community National Rural Health Conference NZ Rural General Practice Network April 7, 2018 Brian Grainger Haematology Registrar Auckland Acknowledgements Dr James
Over to you, mate Blood Cancers in the Community National Rural Health Conference NZ Rural General Practice Network April 7, 2018 Brian Grainger Haematology Registrar Auckland Acknowledgements Dr James
If unqualified, Complete remission is considered to be Haematological complete remission
 Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Scroll right to see the database codes for Disease status and Response Diagnosis it refers to Disease status or response to treatment AML ALL CML CLL MDS or MD/MPN or acute leukaemia secondary to previous
Hematology Case Conference 8/5/03
 Hematology Case Conference 8/5/03 Bone Marrow Case Patient: Emmxxx Lylexxx 74 year old AA female S/P craniotomy for SDH. Pt has Hx of HTN, DM, Crohn s disease, (R) nephrectomy. Bone marrow for abnormal
Hematology Case Conference 8/5/03 Bone Marrow Case Patient: Emmxxx Lylexxx 74 year old AA female S/P craniotomy for SDH. Pt has Hx of HTN, DM, Crohn s disease, (R) nephrectomy. Bone marrow for abnormal
Case #1. Robert J. Glinert, M.D. David C. Fisher, M.D. Dana Farber Cancer Institute
 Case #1 Robert J. Glinert, M.D. David C. Fisher, M.D. Dana Farber Cancer Institute Patient History Part I 76 year-old man 1997 diagnosed with MGUS (biclonal) during evaluation of (self-limited) anemia.
Case #1 Robert J. Glinert, M.D. David C. Fisher, M.D. Dana Farber Cancer Institute Patient History Part I 76 year-old man 1997 diagnosed with MGUS (biclonal) during evaluation of (self-limited) anemia.
HAEMATOLOGICAL MALIGNANCY
 HAEMATOLOGICAL MALIGNANCY Reference Compulsory reading Haematology at Glance 2 nd ed. Atul Mehta & Victor Hoffbrand Chapters: 20 to 31 Pages: 46 to 69 Pathogenesis of Haematological Malignancy Figure (a)
HAEMATOLOGICAL MALIGNANCY Reference Compulsory reading Haematology at Glance 2 nd ed. Atul Mehta & Victor Hoffbrand Chapters: 20 to 31 Pages: 46 to 69 Pathogenesis of Haematological Malignancy Figure (a)
Mr Matthew Eby. Dr Humphrey Pullon
 Dr Humphrey Pullon Haematologist Hamilton Mr Matthew Eby Senior Support Services Coordinator Leukaemia & Blood Cancer Foundation New Zealand Hamilton 16:30-17:25 WS #64: Managing Haemopoetic Disease in
Dr Humphrey Pullon Haematologist Hamilton Mr Matthew Eby Senior Support Services Coordinator Leukaemia & Blood Cancer Foundation New Zealand Hamilton 16:30-17:25 WS #64: Managing Haemopoetic Disease in
Hematology 101. Cindy Rogers, MT(ASCP) Diagnostics System Specialist
 Diagnostics System Specialist") Hematology 101 Cindy Rogers, MT(ASCP) Diagnostics System Specialist More Acronyms...» CBC» RBC» HGB» HCT» WBC» MPV» PLT» RDW» DIFF» H&H» Complete Blood Count» Red Blood Cell» Hemoglobin» Hematocrit» White
Hematology 101 Cindy Rogers, MT(ASCP) Diagnostics System Specialist More Acronyms...» CBC» RBC» HGB» HCT» WBC» MPV» PLT» RDW» DIFF» H&H» Complete Blood Count» Red Blood Cell» Hemoglobin» Hematocrit» White
Avoiding Early Cancer Claims. Presentation #4. Hank George, FALU
 Avoiding Early Cancer Claims Presentation #4 Hank George, FALU Hematology and High Risk of Early Cancer Claims Mild Anemia in elders is underpriced by insurers most likely because of its high prevalence
Avoiding Early Cancer Claims Presentation #4 Hank George, FALU Hematology and High Risk of Early Cancer Claims Mild Anemia in elders is underpriced by insurers most likely because of its high prevalence
Microcytic Hypochromic Anemia An Approach to Diagnosis
 Microcytic Hypochromic Anemia An Approach to Diagnosis Decreased hemoglobin synthesis gives rise to microcytic hypochromic anemias. Hypochromic anemias are characterized by normal cellular proliferation
Microcytic Hypochromic Anemia An Approach to Diagnosis Decreased hemoglobin synthesis gives rise to microcytic hypochromic anemias. Hypochromic anemias are characterized by normal cellular proliferation
Anemia. A case-based approach. David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017
 Anemia A case-based approach David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017 Recognizing trends Learning Objectives MCV, RDW, Ferritin, LDH, Reticulocytes Managing complex patients 1.
Anemia A case-based approach David B. Sykes, MD, PhD Hematology, MGH Cancer Center June 8, 2017 Recognizing trends Learning Objectives MCV, RDW, Ferritin, LDH, Reticulocytes Managing complex patients 1.
Case B14. Pathological WBC counts. Pseudopelger cells
 Pathological counts Case B14 Pseudopelger cells Diagnosis: B-PLL An 86-year-old woman treated for breast cancer in 2008 with surgery and postoperative irradiation. Six years later she now consulted her
Pathological counts Case B14 Pseudopelger cells Diagnosis: B-PLL An 86-year-old woman treated for breast cancer in 2008 with surgery and postoperative irradiation. Six years later she now consulted her
The ABCs of Waldenström s Macroglobulinemia (WM)
") The ABCs of Waldenström s Macroglobulinemia (WM) Jeffrey V. Matous MD Colorado Blood Cancer Institute IWMF Ed Forum May 2017 Objectives Describe the roots underneath WM Review incidence, possible risk
The ABCs of Waldenström s Macroglobulinemia (WM) Jeffrey V. Matous MD Colorado Blood Cancer Institute IWMF Ed Forum May 2017 Objectives Describe the roots underneath WM Review incidence, possible risk
DR SUDHIR MEHTA MD,MNAMS,FICP. Senior Professor & Head Medical Unit SMS Medical College & Hospital Jaipur
 DR SUDHIR MEHTA MD,MNAMS,FICP Senior Professor & Head Medical Unit SMS Medical College & Hospital Jaipur s.smehta@hotmail.com CBC..What is the Utility of performing this basic Hematology Test? 10/31/2010
DR SUDHIR MEHTA MD,MNAMS,FICP Senior Professor & Head Medical Unit SMS Medical College & Hospital Jaipur s.smehta@hotmail.com CBC..What is the Utility of performing this basic Hematology Test? 10/31/2010
WBCs Disorders 1. Dr. Nabila Hamdi MD, PhD
 WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
WBCs Disorders 1 Dr. Nabila Hamdi MD, PhD ILOs Compare and contrast ALL, AML, CLL, CML in terms of age distribution, cytogenetics, morphology, immunophenotyping, laboratory diagnosis clinical features
Leukemias. Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College
 Leukemias Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College Introduction Leukaemias are malignant disorders of the haematopoietic stem cell compartment,
Leukemias Prof. Mutti Ullah Khan Head of Department Medical Unit-II Holy Family Hospital Rawalpindi Medical College Introduction Leukaemias are malignant disorders of the haematopoietic stem cell compartment,
Approach to a pale child
 Approach to a pale child Dr. Dafalla Ahmed Babiker Jazan university objectives Definition of anemia Classification and causes Important points in history and physical examination Investigations. Definition
Approach to a pale child Dr. Dafalla Ahmed Babiker Jazan university objectives Definition of anemia Classification and causes Important points in history and physical examination Investigations. Definition
TYPE 1 GAUCHER DISEASE PRESENTING AS PERSISTENT THROMBOCYTOPENIA, ASSOCIATED FACTOR XI DEFICIENCY & EMERGENT MYELOMA
 TYPE 1 GAUCHER DISEASE PRESENTING AS PERSISTENT THROMBOCYTOPENIA, ASSOCIATED FACTOR XI DEFICIENCY & EMERGENT MYELOMA Trish Hyland, Medical Scientist, Department of Haematology, Cork University Hospital
TYPE 1 GAUCHER DISEASE PRESENTING AS PERSISTENT THROMBOCYTOPENIA, ASSOCIATED FACTOR XI DEFICIENCY & EMERGENT MYELOMA Trish Hyland, Medical Scientist, Department of Haematology, Cork University Hospital
Haematology for GP's
 Haematology for GP's Dr Christina Zouvelou Consultant Haematologist SOUTHEND UNIVERSITY HOSPITALS NHS FT SPIRE WELLESLEY HOSPITAL Time to Learn, 03/07/2018 Anaemia Careful history (duration, symptoms,
Haematology for GP's Dr Christina Zouvelou Consultant Haematologist SOUTHEND UNIVERSITY HOSPITALS NHS FT SPIRE WELLESLEY HOSPITAL Time to Learn, 03/07/2018 Anaemia Careful history (duration, symptoms,
Faculty of Medicine Dr. Tariq Aladily
 Iron deficiency anemia The most common anemia worldwide Only 10% of ingested iron is absorbed Most dietary iron occurs in meat products Absorbed in duodenum Hepcidin By inhibiting ferroportin, hepcidin
Iron deficiency anemia The most common anemia worldwide Only 10% of ingested iron is absorbed Most dietary iron occurs in meat products Absorbed in duodenum Hepcidin By inhibiting ferroportin, hepcidin
CHAPTER:4 LEUKEMIA. BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY 8/12/2009
 LEUKEMIA CHAPTER:4 1 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Leukemia A group of malignant disorders affecting the blood and blood-forming tissues of
LEUKEMIA CHAPTER:4 1 BY Mrs. K.SHAILAJA., M. PHARM., LECTURER DEPT OF PHARMACY PRACTICE, SRM COLLEGE OF PHARMACY Leukemia A group of malignant disorders affecting the blood and blood-forming tissues of
MYELOPROLIFARATIVE NEOPLASMS. Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin).
, FRCP(Edin).") MYELOPROLIFARATIVE NEOPLASMS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin). These are a group of chronic conditions characterised by clonal proliferation of marrow precursor cells. PRV, essential thrombocyathaemia,
MYELOPROLIFARATIVE NEOPLASMS Dr. Hasan Fahmawi, MRCP(UK), FRCP(Edin). These are a group of chronic conditions characterised by clonal proliferation of marrow precursor cells. PRV, essential thrombocyathaemia,
What is a hematological malignancy? Hematology and Hematologic Malignancies. Etiology of hematological malignancies. Leukemias
 Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
Hematology and Hematologic Malignancies Cancer of the formed elements of the blood What is a hematological malignancy? A hematologic malignancy is a malignancy (or cancer) of any of the formed elements
Classification of Anaemia
 Classification of Anaemia Dr Roger Pool Department of Haematology NHLS & University of Pretoria MEASUREMENT OF HAEMATOCRIT The haematocrit ratio (Hct) is the proportion of blood made up of cells - mainly
Classification of Anaemia Dr Roger Pool Department of Haematology NHLS & University of Pretoria MEASUREMENT OF HAEMATOCRIT The haematocrit ratio (Hct) is the proportion of blood made up of cells - mainly
(anemia) ก hemoglobin concentration, hematocrit deviation 1 1 ก hemoglobin, hematocrit mean corpuscular volume (MCV) 2
 ก hemoglobin concentration, hematocrit deviation 1 1 ก hemoglobin, hematocrit mean corpuscular volume (MCV) 2") ก ก. ก ก.. ก (anemia) ก hemoglobin concentration, hematocrit ก ก ก 2 Standard deviation 1 1 ก hemoglobin, hematocrit mean corpuscular volume (MCV) 2 Hemoglobin hematocrit MCV (g/dl) (%) (fl) ( ) 0.5-1.9
ก ก. ก ก.. ก (anemia) ก hemoglobin concentration, hematocrit ก ก ก 2 Standard deviation 1 1 ก hemoglobin, hematocrit mean corpuscular volume (MCV) 2 Hemoglobin hematocrit MCV (g/dl) (%) (fl) ( ) 0.5-1.9
Forms Revision: Myeloma Changes
 Sharing knowledge. Sharing hope. Forms Revision: Myeloma Changes J. Brunner, PA-C and A. Dispenzieri, MD February 2013 Disclosures Janet Brunner, PA-C I have no relevant conflicts of interest to disclose.
Sharing knowledge. Sharing hope. Forms Revision: Myeloma Changes J. Brunner, PA-C and A. Dispenzieri, MD February 2013 Disclosures Janet Brunner, PA-C I have no relevant conflicts of interest to disclose.
UNUSUAL PRESENTATIONS OF SYSTEMIC LUPUS ERYTHEMATOSUS
 UNUSUAL PRESENTATIONS OF SYSTEMIC LUPUS ERYTHEMATOSUS Presenter- Dr. Meghana B S Prof Dr. NAGARAJA B S Prof Dr. NIRMALA A C Dr. SIVARANJANI H Dr. B C PRAKASH Dr. MUMTAZ ALI KHAN A 60 year old lady, k/c/o
UNUSUAL PRESENTATIONS OF SYSTEMIC LUPUS ERYTHEMATOSUS Presenter- Dr. Meghana B S Prof Dr. NAGARAJA B S Prof Dr. NIRMALA A C Dr. SIVARANJANI H Dr. B C PRAKASH Dr. MUMTAZ ALI KHAN A 60 year old lady, k/c/o
Types of Anaemias and their Management. S. Moncrieffe, Pharm.D., MPH, Dip.Ed., RPh. PSJ CE Mandeville Hotel April 27, 2014
 Types of Anaemias and their Management S. Moncrieffe, Pharm.D., MPH, Dip.Ed., RPh. PSJ CE Mandeville Hotel April 27, 2014 Objectives At the end of the presentations participants should be able to: 1. Define
Types of Anaemias and their Management S. Moncrieffe, Pharm.D., MPH, Dip.Ed., RPh. PSJ CE Mandeville Hotel April 27, 2014 Objectives At the end of the presentations participants should be able to: 1. Define
Hematology: Challenging Cases with Your Participation COPYRIGHT
 Hematology: Challenging Cases with Your Participation Reed E. Drews, MD Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Question 1 Question 1 64-year-old man is evaluated during
Hematology: Challenging Cases with Your Participation Reed E. Drews, MD Beth Israel Deaconess Medical Center Harvard Medical School Boston, MA Question 1 Question 1 64-year-old man is evaluated during
Criteria for Disease Assessment Joan Bladé
 Criteria for Disease Assessment Joan Bladé Unidad de Amiloidosis y Mieloma Servicio de Hematología Hospital Clínic de Barcelona COMy Meeting, París, May 4th, 2018 Response Evaluation EBMT, 1998 - CR and
Criteria for Disease Assessment Joan Bladé Unidad de Amiloidosis y Mieloma Servicio de Hematología Hospital Clínic de Barcelona COMy Meeting, París, May 4th, 2018 Response Evaluation EBMT, 1998 - CR and
Anemia In the Insurance Applicant What do the numbers mean?
 Anemia In the Insurance Applicant What do the numbers mean? Lisa Duckett, M.D. Vice President and Medical Director September 12, 2017 Goals of the presentation Develop a consistent way to analyze Complete
Anemia In the Insurance Applicant What do the numbers mean? Lisa Duckett, M.D. Vice President and Medical Director September 12, 2017 Goals of the presentation Develop a consistent way to analyze Complete
Morphology Case Study. Presented by Niamh O Donnell, BSc, MSc. Medical Scientist Haematology Laboratory Cork University Hospital
 Morphology Case Study Presented by Niamh O Donnell, BSc, MSc. Medical Scientist Haematology Laboratory Cork University Hospital 41 year old male presented to GP for routine check-up in May 2011. FBC Results:
Morphology Case Study Presented by Niamh O Donnell, BSc, MSc. Medical Scientist Haematology Laboratory Cork University Hospital 41 year old male presented to GP for routine check-up in May 2011. FBC Results:
BONE MARROW PERIPHERAL BLOOD Erythrocyte
 None Disclaimer Objectives Define anemia Classify anemia according to pathogenesis & clinical significance Understand Red cell indices Relate the red cell indices with type of anemia Interpret CBC to approach
None Disclaimer Objectives Define anemia Classify anemia according to pathogenesis & clinical significance Understand Red cell indices Relate the red cell indices with type of anemia Interpret CBC to approach
Disclosures/COI. Cases in Hematopathology. Outline. Heme Path Findings Not to Miss. Normal Peripheral Smear 6/30/2016
 Disclosures/COI Cases in Hematopathology Vamsi Kota Assistant Professor Department of Hematology & Medical Oncology Leukemia/BMT I have no disclosures or conflicts of interest regarding this presentation.
Disclosures/COI Cases in Hematopathology Vamsi Kota Assistant Professor Department of Hematology & Medical Oncology Leukemia/BMT I have no disclosures or conflicts of interest regarding this presentation.
Red cell disorder. Dr. Ahmed Hasan
 Red cell disorder Dr. Ahmed Hasan Things to be learned in this lecture Definition and clinical feature of anemia. Classification of anemia. Know some details of microcytic anemia Question of the lecture:
Red cell disorder Dr. Ahmed Hasan Things to be learned in this lecture Definition and clinical feature of anemia. Classification of anemia. Know some details of microcytic anemia Question of the lecture:
CSP. Common Sense Pathology CONTENTS. Role of the FBC How to interpret results Value of the blood film
 CSP Common Sense Pathology APRIL 2004 A REGULAR CASE-BASED SERIES ON PRACTICAL PATHOLOGY FOR GPs CONTENTS Role of the FBC How to interpret results Value of the blood film A JOINT INITIATIVE OF The Royal
CSP Common Sense Pathology APRIL 2004 A REGULAR CASE-BASED SERIES ON PRACTICAL PATHOLOGY FOR GPs CONTENTS Role of the FBC How to interpret results Value of the blood film A JOINT INITIATIVE OF The Royal
Preferred Clinical Services for Leading Age Florida August 26-27, 2015
 DIAGNOSIS CODING ESSENTIALS FOR LONG-TERM CARE: CHAPTER 3, D CODES DISEASES OF THE BLOOD AND BLOOD-FORMING ORGANS AND CERTAIN DISORDERS INVOLVING THE IMMUNE MECHANISM Preferred Clinical Services for Leading
DIAGNOSIS CODING ESSENTIALS FOR LONG-TERM CARE: CHAPTER 3, D CODES DISEASES OF THE BLOOD AND BLOOD-FORMING ORGANS AND CERTAIN DISORDERS INVOLVING THE IMMUNE MECHANISM Preferred Clinical Services for Leading
Laboratory Examination
 Todd Zimmerman, M.D. 64 year old African American male presents to establish care with PCG. Meds: Norvasc 5 mg daily PMHx: HTN x 20 years, poorly controlled SHx: No tobacco, illicit; rare EtOH ROS: Negative
Todd Zimmerman, M.D. 64 year old African American male presents to establish care with PCG. Meds: Norvasc 5 mg daily PMHx: HTN x 20 years, poorly controlled SHx: No tobacco, illicit; rare EtOH ROS: Negative
Clinical implications for decreased lymphocytes (lymphopenia) o Corticosteroid therapy, adrenocortical hyperfunction, stress, shock
 o Corticosteroid therapy, adrenocortical hyperfunction, stress, shock") Learning Objectives At the completion of this program, the participants will be able to: 1. Identify the components of the CBC and Differential and their clinical implications. 2. Identify normal pediatric
Learning Objectives At the completion of this program, the participants will be able to: 1. Identify the components of the CBC and Differential and their clinical implications. 2. Identify normal pediatric
Kathleen Finnegan MS MT(ASCP)SHCM
SHCM") Kathleen Finnegan MS MT(ASCP)SHCM Discuss the history of hematology automation and digital differentials. Discuss the HemoFAXS Hematology Analysis System by Tissue Gnostics. Review automated microscopy
Kathleen Finnegan MS MT(ASCP)SHCM Discuss the history of hematology automation and digital differentials. Discuss the HemoFAXS Hematology Analysis System by Tissue Gnostics. Review automated microscopy
GP Education Haematology laboratory abnormalities- when to refer? Priyanka Mehta Consultant Haematologist UH Bristol NHS Trust
 GP Education Haematology laboratory abnormalities- when to refer? Priyanka Mehta Consultant Haematologist UH Bristol NHS Trust Topics for discussion Abnormal FBCs Lymphocytosis high and low platelets cytopenias
GP Education Haematology laboratory abnormalities- when to refer? Priyanka Mehta Consultant Haematologist UH Bristol NHS Trust Topics for discussion Abnormal FBCs Lymphocytosis high and low platelets cytopenias
Low grade High grade , immune suppression chronic persistent inflammation viruses B-symptoms
 We've one category for lymphoid neoplasm which is the lymphoma in contrast to that of myeloid which has three categories; acute myeloid leukemias, myeloproliferative & myelodysplastic disorders. Lymphoma
We've one category for lymphoid neoplasm which is the lymphoma in contrast to that of myeloid which has three categories; acute myeloid leukemias, myeloproliferative & myelodysplastic disorders. Lymphoma
Table 8.1. Epidemiology of Leukemia in the United States (2010) Annual Deaths. Mean Age. Percentage of All Leukemias (%) (Number of New Cases)
 Annual Deaths. Mean Age. Percentage of All Leukemias (%) (Number of New Cases)") Table 8.1. Epidemiology of Leukemia in the United States (2010) Type of Leukemia Annual Incidence (Number of New Cases) Percentage of All Leukemias (%) Annual Deaths Mean Age Acute lymphocytic 5,330 12
Table 8.1. Epidemiology of Leukemia in the United States (2010) Type of Leukemia Annual Incidence (Number of New Cases) Percentage of All Leukemias (%) Annual Deaths Mean Age Acute lymphocytic 5,330 12
Should we treat Smoldering MM patients? María-Victoria Mateos University Hospital of Salamanca Salamanca. Spain
 Should we treat Smoldering MM patients? María-Victoria Mateos University Hospital of Salamanca Salamanca. Spain Should we treat some patients with Stage I MM? Len-dex is a promising and atractive option
Should we treat Smoldering MM patients? María-Victoria Mateos University Hospital of Salamanca Salamanca. Spain Should we treat some patients with Stage I MM? Len-dex is a promising and atractive option
Hematology 101. Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD
 Hematology 101 Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD Hematocrits Plasma White cells Red cells Normal, Hemorrhage, IDA, Leukemia,
Hematology 101 Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD Hematocrits Plasma White cells Red cells Normal, Hemorrhage, IDA, Leukemia,
Management Update: Multiple Myeloma. Presented by Prof. Dr. Khan Abul Kalam Azad Professor of Medicine Dhaka Medical College
 Management Update: Multiple Myeloma Presented by Prof. Dr. Khan Abul Kalam Azad Professor of Medicine Dhaka Medical College Introduction Multiple myeloma - clonal plasma cell neoplasm Monoclonal antibody
Management Update: Multiple Myeloma Presented by Prof. Dr. Khan Abul Kalam Azad Professor of Medicine Dhaka Medical College Introduction Multiple myeloma - clonal plasma cell neoplasm Monoclonal antibody