Resident Seminar Aug 19 th, 2015 Colon: Neoplastic. Scott Rieder Dr. Colquhoun
|
|
|
- Lilian Lawrence
- 5 years ago
- Views:
Transcription

1 Resident Seminar Aug 19 th, 2015 Colon: Neoplastic Scott Rieder Dr. Colquhoun
2 Objectives Medical Expert: 1. The biologic basis of colon neoplasia 2. Colon cancer screening (guidelines and evidence) 3. Pathology and management of polyps 4. Management of the malignant polyp 5. Presentation, diagnosis and management of colon cancer 6. Staging of colon cancer and prognosis 7. Management of colon cancer 8. Management of colon cancer emergencies 9. Role of neo-adjuvant and adjuvant care in colon cancer 10. Treatment of metastatic colon cancer 11. Post operative surveillance following curative resection of colon cancer 12. Palliation of metastatic colon cancer (role of stenting, ostomy, etc ) 13. Diagnosis and management of desmoids tumors and other FAP associated tumors
3 Objectives Collaborator: 1. Role of radiation and chemotherapy in the management of colon cancer 2. Management and palliation of colon cancer Health Advocate: 1. Colon cancer screening 2. Screening in high risk populations 3. Post-operative surveillance of curatively resected colon cancer Scholar: 1. Review of seminal paper
4 Epidemiology 3 rd most commonly diagnosed malignancy in Canada It is the 2 nd leading cause of cancer death, behind lung cancer It is estimated that 25,000 people with diagnosed with CRC in Canada, and that over 9000 Canadians will die from CRC in 2015
5 Risk Factors Age Race Inflammatory Bowel Disease Family History/Genetic Syndromes Obesity High-fat diet Alcohol Smoking Diabetes Geography

6 CRC Incidence with age

7 Familial Cancer Syndromes It is estimated that around 15% of CRC occur in the background of a genetically inherited disorder, with FAP and HNPCC causing approximately 5% of all CRCs
8 Familial Cancer Syndromes FAP and variants Cowden syndrome Peutz-Jeghers HNPCC MAP
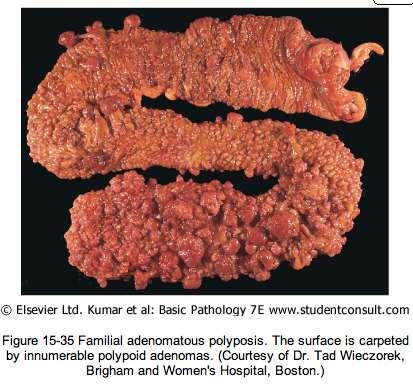

9 Familial Adenomatous Polyposis (FAP)
10 Familial Adenomatous Polyposis (FAP) Autosomal dominant disorder caused by mutations (>100 identified) in the adenomatous polyposis coli (APC) gene, located on the q-arm of chromosome 5 Classic FAP is described as greater than 100 adenomatous polyps throughout the colon in a lifetime Polyps typically start to develop when these patients are in their teens, and lifetime risk of CRC approaches 100% 1/3 of newly diagnosed FAP patients are likely caused by de novo mutations or represent genetic mosaics The clinical presentation for FAP patients may include diarrhea, abdominal cramping/bloating and lower GI bleeds, but many are asymptomatic until they develop cancer
11 Genetic Screening for FAP
12 Extracolonic disease in FAP Patients with FAP have many extracolonic manifestations of their disease that require close observation Gastric fundal polyps are common but rarely transform into gastric cancer Osteomas occurs in 20% of patients with FAP but require no special treatment or surveillance Adenomas of the small bowel, gallbladder and bile duct are also associated with FAP Greater than 30% of FAP patients will develop duodenal polyposis with 4-15% of FAP patients progressing to duodenal and periampullary adenocarcinoma over their lifetime Screening with EGD should begin at age 25 and patients should be scoped at repeat intervals according to their Spigelman stage

13 EGD Screening in FAP Stage 0-1: Every 4 years Stage 2: Every 2-3 years Stage 3: 6-12 months Stage 4: Consider resection
14 FAP Variants Gardener Syndrome Turcott Syndrome Attenuated FAP



15 Gardener Syndrome Described by Gardener in the 1950s in patients with FAP and is associated with extracolonic lesions including: Osteomas of the face and skull Unerupted and/or supernumerary teeth Epidermal cysts, lipomas and fibromas Desmoid tumours Adrenal adenomas Nasal angiofibromas
16 Gardener Syndrome Extracolonic malignancies associated with GS: Thyroid Pancreatic Gastric Hepatoblastoma CNS Recommended screening in GS patients: Annual thyroid exam and US, starting at age 10 LFTs and abdominal US q6 months in GS children until the age of 10 Generally all other screening guided by FAP principles or investigations as symptoms arise


17 Desmoid Tumours in FAP
18 Desmoid tumours in FAP Desmoids are fibromatous lesions that can arise in patients with FAP, primarily in the abdominal wall and within the abdomen Although they are benign growths, they can occasionally be locally aggressive, causing intestinal obstruction or bowel ischemia and are responsible for 9-15% of deaths in patients with FAP For extra-abdominal desmoids, complete surgical resection is indicated In FAP, patients with intra-abdominal desmoids often cannot undergo surgical resection due to the tumours being seated at the root of the mesentery, in these patients either RT or systemic therapy (tamoxifen and sulindac) is indicated
 and Lynch syndrome (gliomas) Term of historical use")
19 Turcott Syndrome First used by Turcott to describe association between FAP and brain tumours Through genetic studies, has been shown to be associated with both FAP (medullablastomas) and Lynch syndrome (gliomas) Term of historical use only
20 Attenuated FAP Less severe diagnosis than classic FAP Described as greater than but less than 100 lifetime polyps Adenomas typically present at a later age than FAP (mean age 44) Lifetime risk of CRC still extremely high (~80%)


21 Cowden Syndrome Mutation in the phosphatase and tensin homolog gene (PTEN) tumour suppressor gene on chromosome 10 Autosomal dominant inheritance Trichelemmomas, acral keratoses and oral papillomas are typical manifestations Predisposed to multiple malignancies, including: Breast Endometrial Renal Colorectal caners Risk of CRC ~18% higher than normal population
22 Peutz-Jeghers Syndrome Characterized by multiple hamartomatous polyps throughout the GI tract and pigmented mucocutaenous macules that form at a young age Mutation in the STK11 gene, another tumour suppressor Autosomal dominant inheritance Lifelong risk of cancers in GI tract: Colorectal (40%) Stomach (30%) Small bowel (13%) Pancreas (11-35%) EGD/Colonoscopy at age 8, and every 3 years after if polyps detected Capsule endoscopy at age 8 and q3 years for patients with multiple polyps seen in small bowel


23 Peutz-Jeghers Syndrome
24 Hereditary Nonpolyposis Colorectal Cancer HNPCC is the most common cause of inheritable CRC Autosomal dominant inheritance Called HNPCC when patients meet the Amsterdam criteria Lynch syndrome now reserved for those with identified microsatellite instability in DNA mismatch repair gene mutations (MLH1, MSH2, MSH6 and PMS2)

25 Amsterdam Criteria/Bethesda Guidelines

26 DNA MMR Genes in Lynch Syndrome
27 Lynch Syndrome Individuals with Lynch syndrome carry a 70% lifetime risk of CRC and occurs at an earlier age (mean 44, compared to in sporadic CRC) They are also at risk for metachronous cancers, with ~10% of patients developing more than one lifetime cancer The adenomas in Lynch patients tend to be more proximal, flat and are more likely to contain villous histology There is also an accelerated polyp to cancer sequence in these patients (~35 months) Pathology of Lynch CRCs often demonstrates mucinous, signet ring cell or medullary histologic type cancers that are more poorly differentiated compared to sporadic CRCs Should undergo colonoscopic surveillance starting at age 20 every 1-2 years

28 Lynch Syndrome


29 Muir-Torre Syndrome A variant of HNPCC Defined as at least one sebaceous skin tumour and one visceral malignancy Should undergo annual skin exams in addition to typical HNPCC screening
30 MUTYH-Associated Polyposis Affected individuals typically have multiple colonic polyps and have had APC mutations excluded MUTYH genes are responsible for repairing oxidative damage to DNA, and individuals with MAP have biallelic mutations in MUTYH Lifetime risk of CRC in these patients is 70-75% Also at risk of developing duodenal and gastric polyps In patients with diagnosed MAP and a colon cancer, total colectomy is indicated
31 Polyp to Cancer Sequence Almost all CRC cancers arise from benign neoplasms
32 Rationale for CRC Screening Screening for and removing premalignant can reduce death by CRC Adenoma to cancer sequence takes between years in an an average risk patient Screening methods include stool testing, cross-sectional imaging and direct visualization NCCN generally recommends colonoscopy over other methods as the primary screening tool for CRC
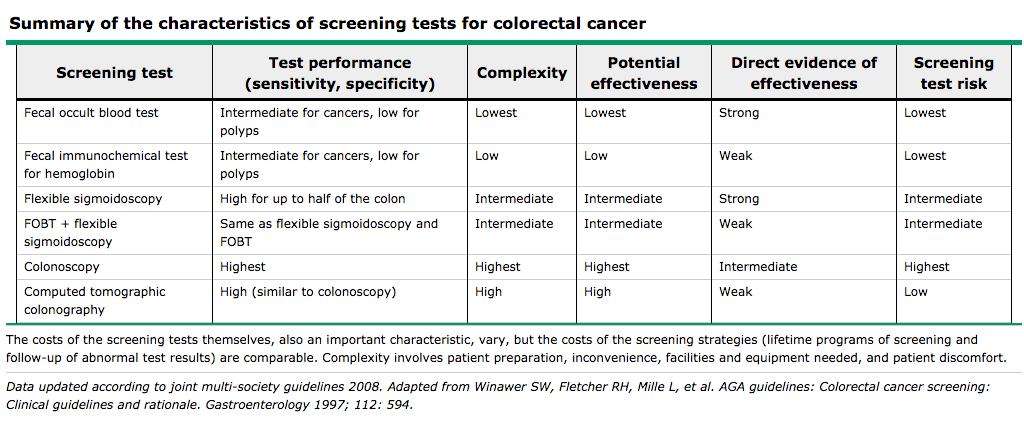
33 Screening Test Characteristics

34 Screening Guidelines Average Risk
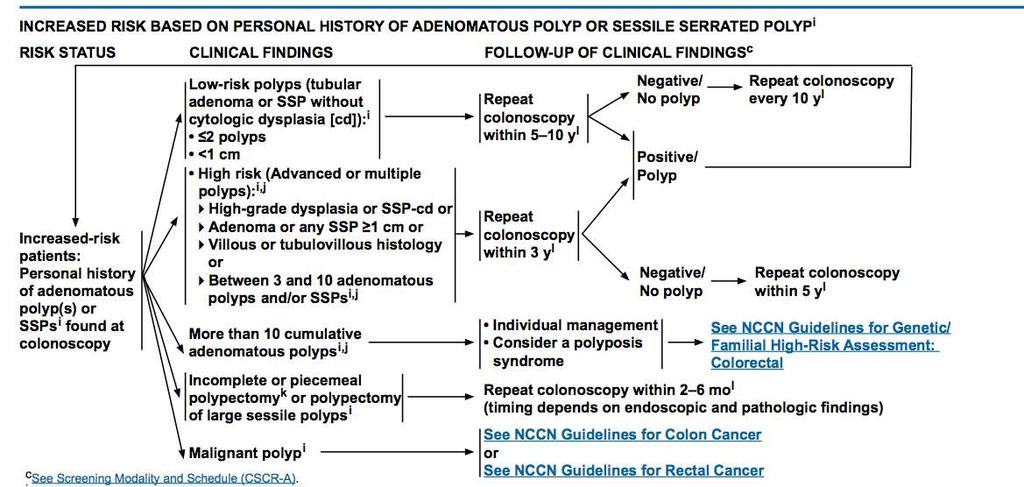
35 Increased Personal History/Adenoma/SSP

36 Inflammatory Bowel Disease Screening

37 Endoscopic Appearance of Colonic Polyps Polyps may be classified in part by their morphology: Penduculated Sessile Flat Depressed
38 Pathology of Colonic Polyps Hyperplastic - most common non-neoplastic polyp in colon, typically found in rectosigmoid and less than 5mm in size, generally carry very low risk of malignant transformation Serrated Adenoma More prevalent in proximal colon, lack typical dysplasia seen in adenomas but develop foci of dysplasia within the polyp, tend to be large and flat (more difficult to remove endoscopically) Tubular Adenoma 80% of all colonic polyps, characteristic branches of adenomatous epithelium Villous Adenoma 10% of all colonic polyps, characteristic long narrow glands extending to center of polyp Tubulovillous Adenoma A combination of tubular and villous pathology


39 Pathology of Colonic Polyps Hyperplastic polyp with saw tooth pattern
 Villous Histology Number of colonic")
40 Pathology of Colonic Polyps All adenomas are dysplastic, but are graded as having either highgrade or low-grade dysplasia Risk factors that increase the risk of high-grade dysplasia and malignancy: Size (>1cm) Villous Histology Number of colonic polyps



41 Management of Colonic Polyps When a polyp is detected, endoscopic polypectomy is generally recommended when feasible, and can be achieved through a variety of means: Cold/hot biopsy Cold/hot snare Piecemeal excision Fulguration with cautery or APC Injection assisted mucosal resection Submucosal dissection Surgical resection

42 Management of Colonic Polyps A new approach to previously unresectable polyps is to combine the endoscopic resection with laparoscopic assistance Specimen sent for frozen to ensure no malignacy May reduce morbidity of formal resection in selected patients
43 The Malignant Polyp Resected polyps with malignant foci represent a challenge to both the patient and surgeon on whether or not to proceed to surgical resection Some guiding principles to not proceed to segmental colectomy include: Low grade malignancies No lymphovascular invasion Polyp specimen resected en mass Negative (>2mm) margin If all of these criteria are not met, surgical resection should be strongly considered, based on clinical acumen, patient wishes and patient factors
44 Presentation of colon cancer Generally colon cancer presents in one of three ways: Symptoms from tumour (local or metastatic) Routine screening or surveillance Surgical emergency
45 Presentation of colon cancer Common symptoms include: Altered bowel habits (typically for left-sided cancer/rectal cancers Hematochezia (rectal and sigmoid) Anemia Abdominal pain and bloating Typically patients who present symptomatic have a worse prognosis than those picked up on routine screening or found incidentally Patients presenting with obstruction and perforation carry the worst prognosis, including those with node-negative disease



46 Diagnosis of colon cancer If a colon cancer is suspected or being screened for; barium enema, CT colonography or colonoscopy may be utilized for diagnosis Colonoscopy is preferred as it is the only method that can achieve tissue diagnosis Most common colon cancer is adenocarcinoma
47 Staging of CRC Once a diagnosis of CRC has been established, patients should be sent for a CT scan of their chest, abdomen and pelvis to assess for metastatic disease Carcinoembryonic antigen (CEA) level, a glycoprotein produced in the GI tract during neonatal development and secreted by CRC cancers, should be drawn CEA is not a tool for diagnosis or staging, it is used for follow-up after treatment

48 Staging of CRC
49 Prognosis
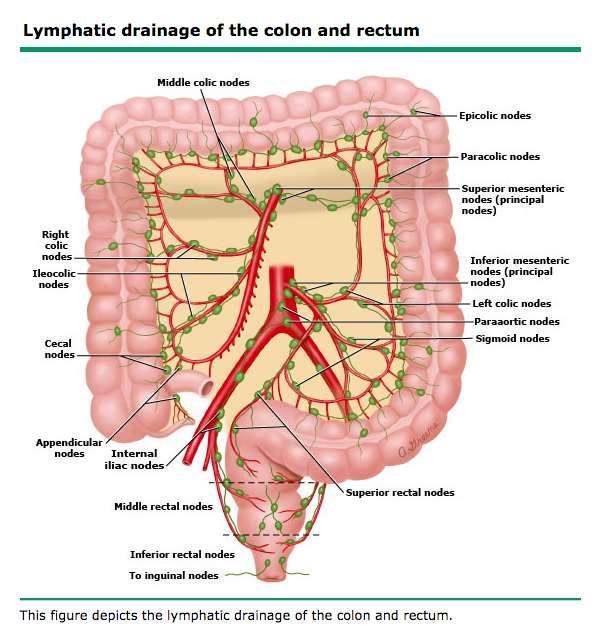
50 Management of CRC Currently surgical resection is the only way to achieve cure in CRC Principle of surgical resection is to remove the primary cancer along with the major vascular pedicles and lymphatic drainage of the diseased segment of colon and to remove en bloc any invasion of the cancer to adjacent structures Both open and laparoscopic approaches to resection have demonstrated equivalent cure rates and no difference in perioperative complications After full workup, plan for treatment can be done alone with the surgeon or in conjunction with a multi-disciplinary team depending on the complexity

51 Segmental colon resection
52 Emergency Colon Surgery Patients may present with colonic obstruction, or with colonic perforation and peritonitis Urgent operations are indicated in the setting of complete obstruction, perforation with frank contamination, peritonitis or sepsis In these setting, primary anastomosis post resection may not be feasible and an ostomy may be brought out In patients with a near-obstructing mass, a colonic stent may be considered as a bridge to planned surgery, although this is generally reserved for patients are high risk for surgery and would benefit from medical optimization
53 Neo-adjuvant therapy Preoperative radiotherapy generally does not play a role in colon cancers for curative intent (very different from rectal cancer) Patients presenting with potentially resectable metastatic disease (typically lung and liver mets) may go for neoadjuvant chemotherapy prior to resection
54 Principes of Pathologic Review After resection of the primary tumour, several pathologic features of the tumour need to be reported to aid in possible adjuvant therapy as well as timing of followup: Grade T-stage (depth of penetration) Number of nodes evaluated and positive nodes Margins (Proximal, distal, and radial) Lymphovascular invasion Perineural invasion Extranodal tumour deposits

55 Adjuvant therapy for CRC The role of adjuvant therapy depends on the stage of disease and patient factors, however in general stage one no role for adjuvant therapy stage two adjuvant therapy may offer some benefit, but studies still unclear stage three/four adjuvant therapy has proven benefit Radiation therapy can be added to T4 tumours affixed to other structures or with positive resection margin
56 Adjuvant therapy for CRC First line therapy typically involves treatment with FOLFOX or FOLFIRI +/- avastin FOL Folinic acid, Allows for purine/pyrimidine synthesis in the setting of 5-FU therapy F Fluorouracil (5-FU), Blocks synthesis of thymidine OX Oxaliplatin Platinum-based cytotoxic agent that prevents DNA transcription and replication IRI irinotecan, a topoisomerase inhibitor Avastin Bevacizumab, monoclonal antibody that inhibits VEG-F
57 Adjuvant therapy for CRC
58 Nonoperative metastatic disease Capecitabine Oral prodrug to 5-FU Panitumumab Inhibits EGFR and subsequently cell growth

59 Postoperative follow-up


60 Palliative CRC Although resection and cure is not an option with these patients, there are interventions offered by surgeons to alleviate symptoms and prolong life Generally complications of diffuse disease include obstruction, perforation and bleeding Surgical options include primary resection and anastomosis, diverting ostomy and surgical bypass Colonic stenting has a role in large bowel obstructions secondary to CRC who are not ideal operative candidates


61 Laparoscopic vs Open for CRC


62 Laparoscopic vs Open for CRC

63 Laparoscopic vs Open for CRC No difference in perioperative complications, recurrence or 5 year survival
64 Thanks for your attention
Colonic Polyp. Najmeh Aletaha. MD
 Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Colonic Polyp Najmeh Aletaha. MD 1 Polyps & classification 2 Colorectal cancer risk factors 3 Pathogenesis 4 Surveillance polyp of the colon refers to a protuberance into the lumen above the surrounding
Familial Adenomatous Polyposis
 Familial Adenomatous Polyposis 1 in 10,000 incidence 100 s to 1000 s of colonic adenomas by teens Cancer risk: colon, gastric, duodenum (periampulla), small bowel, pancreas, papillary thyroid, childhood
Familial Adenomatous Polyposis 1 in 10,000 incidence 100 s to 1000 s of colonic adenomas by teens Cancer risk: colon, gastric, duodenum (periampulla), small bowel, pancreas, papillary thyroid, childhood
colorectal cancer Colorectal cancer hereditary sporadic Familial 1/12/2018
 colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
colorectal cancer Adenocarcinoma of the colon and rectum is the third most common site of new cancer cases and deaths in men (following prostate and lung or bronchus cancer) and women (following breast
Familial and Hereditary Colon Cancer
 Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer
 Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Familial and Hereditary Colon Cancer Aasma Shaukat, MD, MPH, FACG, FASGE, FACP GI Section Chief, Minneapolis VAMC Associate Professor, Division of Gastroenterology, Department of Medicine, University of
Pathology reports, related operative reports and consult letters must be provided with a request for assessment.
 Page 1 of 6 Polyposis Syndromes Inherited risk for colorectal cancer is associated with a number of polyposis syndromes (genes), some of which are well-defined and others are less common. Identification
Page 1 of 6 Polyposis Syndromes Inherited risk for colorectal cancer is associated with a number of polyposis syndromes (genes), some of which are well-defined and others are less common. Identification
Colorectal Neoplasia. Dr. Smita Devani MBChB, MRCP. Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi
 Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
Colorectal Neoplasia Dr. Smita Devani MBChB, MRCP Consultant Physician and Gastroenterologist Aga Khan University Hospital, Nairobi Case History BT, 69yr male Caucasian History of rectal bleeding No change
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE
 COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
COLON CANCER CARE GUIDELINES NON-METASTATIC DISEASE Guideline Authors: Todd S. Crocenzi, M.D.; Mark Whiteford, M.D.; Matthew Solhjem, M.D.; Carlo Bifulco, M.D.; Melissa Li, M.D.; Christopher Cai, M.D.;
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY
 OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
OPEN ACCESS TEXTBOOK OF GENERAL SURGERY COLORECTAL POLYPS P Goldberg POLYP A polyp is a localised elevated lesion arising from a epithelial surface. If it has a stalk it is called a pedunculated polyp
Risk of Colorectal Cancer (CRC) Hereditary Syndromes in GI Cancer GENETIC MALPRACTICE
 Hereditary Syndromes in GI Cancer GENETIC MALPRACTICE") Identifying the Patient at Risk for an Inherited Syndrome Sapna Syngal, MD, MPH, FACG Director, Gastroenterology Director, Familial GI Program Dana-Farber/Brigham and Women s Cancer Center Associate Professor
Identifying the Patient at Risk for an Inherited Syndrome Sapna Syngal, MD, MPH, FACG Director, Gastroenterology Director, Familial GI Program Dana-Farber/Brigham and Women s Cancer Center Associate Professor
Index. Note: Page numbers of article titles are in boldface type.
 Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
Index Note: Page numbers of article titles are in boldface type. A Abdominal surgery prior as factor in laparoscopic colorectal surgery, 554 555 Abscess(es) CRC presenting as, 539 540 Adenocarcinoma of
By: Tania Cortas, MD Arizona Oncology 03/10/2015
 By: Tania Cortas, MD Arizona Oncology 03/10/2015 Epidemiology In the United States, CRC incidence rates have declined about 2 to 3 percent per year over the last 15 years Death rates from CRC have declined
By: Tania Cortas, MD Arizona Oncology 03/10/2015 Epidemiology In the United States, CRC incidence rates have declined about 2 to 3 percent per year over the last 15 years Death rates from CRC have declined
Colon Cancer Screening & Surveillance. Amit Patel, MD PGY-4 GI Fellow
 Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
Colon Cancer Screening & Surveillance Amit Patel, MD PGY-4 GI Fellow Epidemiology CRC incidence and mortality rates vary markedly around the world. Globally, CRC is the third most commonly diagnosed cancer
Classification of polyposis syndromes two major groups. Adenomatous polyposis syndromes. Hamartomatous polyposis syndromes
 Hereditary polyposis syndromes Classification of polyposis syndromes two major groups adenomatous and non-adenomatous polyposis syndromes Adenomatous polyposis syndromes Familial adenomatous polyposis(fap)
Hereditary polyposis syndromes Classification of polyposis syndromes two major groups adenomatous and non-adenomatous polyposis syndromes Adenomatous polyposis syndromes Familial adenomatous polyposis(fap)
For identification, support and follow up related to Familial Gastrointestinal Cancer conditions. South Island Cancer Nurses Network September 2013
 For identification, support and follow up related to Familial Gastrointestinal Cancer conditions South Island Cancer Nurses Network September 2013 Who are we? Specialist multidisciplinary team: Nurse coordinators,
For identification, support and follow up related to Familial Gastrointestinal Cancer conditions South Island Cancer Nurses Network September 2013 Who are we? Specialist multidisciplinary team: Nurse coordinators,
B Base excision repair, in MUTYH-associated polyposis and colorectal cancer, BRAF testing, for hereditary colorectal cancer, 696
 Index Note: Page numbers of article titles are in boldface type. A Adenomatous polyposis, familial. See Familial adenomatous polyposis. Anal anastomosis, ileal-pouch, proctocolectomy with, in FAP, 591
Index Note: Page numbers of article titles are in boldface type. A Adenomatous polyposis, familial. See Familial adenomatous polyposis. Anal anastomosis, ileal-pouch, proctocolectomy with, in FAP, 591
Neoplastic Colon Polyps. Joyce Au SUNY Downstate Grand Rounds, October 18, 2012
 Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
Neoplastic Colon Polyps Joyce Au SUNY Downstate Grand Rounds, October 18, 2012 CASE 55M with Hepatitis C, COPD (FEV1=45%), s/p vasectomy, knee surgery Meds: albuterol, flunisolide, mometasone, tiotropium
UPDATE IN THE MANAGEMENT AND TREATMENT OF COLORECTAL CANCER. Edwin A. Empaynado, MD Advocare Colon and Rectal Surgical Specialists
 UPDATE IN THE MANAGEMENT AND TREATMENT OF COLORECTAL CANCER Edwin A. Empaynado, MD Advocare Colon and Rectal Surgical Specialists WHAT IS COLON CANCER? WHAT CAUSES COLORECTAL CANCER? WHAT ARE THE RISK
UPDATE IN THE MANAGEMENT AND TREATMENT OF COLORECTAL CANCER Edwin A. Empaynado, MD Advocare Colon and Rectal Surgical Specialists WHAT IS COLON CANCER? WHAT CAUSES COLORECTAL CANCER? WHAT ARE THE RISK
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University
 Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University") COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University 1. I am a surgeon; of course I have nothing to disclose.
COLON CANCER GENETICS (FOR SURGEONS) Mark W. Arnold MD Chief, Division of Colon and Rectal Surgery Professor of Surgery The Ohio State University 1. I am a surgeon; of course I have nothing to disclose.
Locally Advanced Colon Cancer. Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery
 Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
Locally Advanced Colon Cancer Feiran Lou MD. MS. Richmond University Medical Center Department of Surgery Case 34 yo man presented with severe RLQ abdominal pain X 24 hrs. No nausea/vomiting/fever. + flatus.
GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS. Family Health Clinical Genetics. Clinical Genetics department
 GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS Full Title of Guideline: Author (include email and role): Division & Speciality: GUIDELINES FOR THE GENETIC MANAGEMENT OF A FAMILY
GENETIC MANAGEMENT OF A FAMILY HISTORY OF FAP or MUTYH ASSOCIATED POLYPOSIS Full Title of Guideline: Author (include email and role): Division & Speciality: GUIDELINES FOR THE GENETIC MANAGEMENT OF A FAMILY
Surveying the Colon; Polyps and Advances in Polypectomy
 Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Surveying the Colon; Polyps and Advances in Polypectomy Educational Objectives Identify classifications of polyps Describe several types of polyps Verbalize rationale for polypectomy Identify risk factors
Screening & Surveillance Guidelines
 Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Chapter 2 Screening & Surveillance Guidelines I. Eligibility Coloradans ages 50 and older (average risk) or under 50 at elevated risk for colon cancer (personal or family history) that meet the following
Colonic polyps and colon cancer. Andrew Macpherson Director of Gastroentology University of Bern
 Colonic polyps and colon cancer Andrew Macpherson Director of Gastroentology University of Bern Improtance of the problem of colon cancers - Epidemiology Lifetime risk 5% Incidence/10 5 /annum (US Detroit
Colonic polyps and colon cancer Andrew Macpherson Director of Gastroentology University of Bern Improtance of the problem of colon cancers - Epidemiology Lifetime risk 5% Incidence/10 5 /annum (US Detroit
COLON CANCER & GENETICS VERMONT COLORECTAL CANCER SUMMIT NOVEMBER 15, 2014
 COLON CANCER & GENETICS VERMONT COLORECTAL CANCER SUMMIT NOVEMBER 15, 2014 WENDY MCKINNON, MS, CGC CERTIFIED GENETIC COUNSELOR FAMILIAL CANCER PROGRAM UNIVERSIT Y OF VERMONT MEDICAL CENTER 1 CHARACTERISTICS
COLON CANCER & GENETICS VERMONT COLORECTAL CANCER SUMMIT NOVEMBER 15, 2014 WENDY MCKINNON, MS, CGC CERTIFIED GENETIC COUNSELOR FAMILIAL CANCER PROGRAM UNIVERSIT Y OF VERMONT MEDICAL CENTER 1 CHARACTERISTICS
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER
 Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
EARLY DETECTION OF COLORECTAL CANCER. Epidemiology of CRC
 Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Razvan I. Arsenescu, MD Assistant Professor of Medicine Division of Digestive Diseases EARLY DETECTION OF COLORECTAL CANCER Epidemiology of CRC Colorectal cancer (CRC) is a common and lethal disease Environmental
Hereditary Gastric Cancer
 Hereditary Gastric Cancer Dr Bastiaan de Boer Consultant Pathologist Department of Anatomical Pathology PathWest Laboratory Medicine, QE II Medical Centre Clinical Associate Professor School of Pathology
Hereditary Gastric Cancer Dr Bastiaan de Boer Consultant Pathologist Department of Anatomical Pathology PathWest Laboratory Medicine, QE II Medical Centre Clinical Associate Professor School of Pathology
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci. Colon polyps. Colorectal cancer
 Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Patologia sistematica V Gastroenterologia Prof. Stefano Fiorucci Colon polyps Colorectal cancer Harrison s Principles of Internal Medicine 18 Ed. 2012 Colorectal cancer 70% Colorectal cancer CRC and colon
Mr Chris Wakeman. General Surgeon University of Otago, Christchurch. 12:15-12:40 Management of Colorectal Cancer
 Mr Chris Wakeman General Surgeon University of Otago, Christchurch 12:15-12:40 Management of Colorectal Cancer Bowel cancer Chris Wakeman Colorectal Surgeon Christchurch Sam Simon (Simpsons) Elizabeth
Mr Chris Wakeman General Surgeon University of Otago, Christchurch 12:15-12:40 Management of Colorectal Cancer Bowel cancer Chris Wakeman Colorectal Surgeon Christchurch Sam Simon (Simpsons) Elizabeth
Cancer Genomics 101. BCCCP 2015 Annual Meeting
 Cancer Genomics 101 BCCCP 2015 Annual Meeting Objectives Identify red flags in a person s personal and family medical history that indicate a potential inherited susceptibility to cancer Develop a systematic
Cancer Genomics 101 BCCCP 2015 Annual Meeting Objectives Identify red flags in a person s personal and family medical history that indicate a potential inherited susceptibility to cancer Develop a systematic
Gastric and Colon Cancer. Dr. Andres Wiernik 2017
 Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
Gastric and Colon Cancer Dr. Andres Wiernik 2017 GASTRIC CANCER Gastric Cancer Classification Epidemiology General principles of Management 25% GE Junction Gastric Cancer 75% Gastric Cancer Epidemiology
GI EMERGENCIES Acute Abdominal Pain
 GI EMERGENCIES Acute Abdominal Pain Marcia Cruz-Correa, MD, PhD, AGAF. FASGE Associate Professor of Medicine, Biochemistry, Surgery Director Translational Research University of Puerto Rico Comprehensive
GI EMERGENCIES Acute Abdominal Pain Marcia Cruz-Correa, MD, PhD, AGAF. FASGE Associate Professor of Medicine, Biochemistry, Surgery Director Translational Research University of Puerto Rico Comprehensive
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL RECTAL CANCER GI Site Group Rectal Cancer Authors: Dr. Jennifer Knox, Dr. Mairead McNamara 1. INTRODUCTION 3 2. SCREENING AND
Objectives. Definitions. Colorectal Cancer Screening 5/8/2018. Payam Afshar, MS, MD Kaiser Permanente, San Diego. Colorectal cancer background
 Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Colorectal Cancer Screening Payam Afshar, MS, MD Kaiser Permanente, San Diego Objectives Colorectal cancer background Colorectal cancer screening populations Colorectal cancer screening modalities Colonoscopy
Serrated Polyps and a Classification of Colorectal Cancer
 Serrated Polyps and a Classification of Colorectal Cancer Ian Chandler June 2011 Structure Serrated polyps and cancer Molecular biology The Jass classification The familiar but oversimplified Vogelsteingram
Serrated Polyps and a Classification of Colorectal Cancer Ian Chandler June 2011 Structure Serrated polyps and cancer Molecular biology The Jass classification The familiar but oversimplified Vogelsteingram
David P. Ryan, M.D. Clinical Director, MGH Cancer Center Chief, Hematology-Oncology, MGH
 Colon Cancer 2015 David P. Ryan, M.D. Clinical Director, MGH Cancer Center Chief, Hematology-Oncology, MGH Colon Cancer Case presentation 72yo woman presented 1/03 abd discomfort and nausea Found to have
Colon Cancer 2015 David P. Ryan, M.D. Clinical Director, MGH Cancer Center Chief, Hematology-Oncology, MGH Colon Cancer Case presentation 72yo woman presented 1/03 abd discomfort and nausea Found to have
Colorectal adenocarcinoma leading cancer in developed countries In US, annual deaths due to colorectal adenocarcinoma 57,000.
 Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Colonic Neoplasia Remotti Colorectal adenocarcinoma leading cancer in developed countries In US, annual incidence of colorectal adenocarcinoma 150,000. In US, annual deaths due to colorectal adenocarcinoma
Colorectal Cancer Syndromes. Barbara Jung, MD AGAF Associate Professor and Chief University of Illinois at Chicago
 Colorectal Cancer Syndromes Barbara Jung, MD AGAF Associate Professor and Chief University of Illinois at Chicago Outline Colon cancer General Genetics, Risk, Screening Specific Syndromes, when to suspect,
Colorectal Cancer Syndromes Barbara Jung, MD AGAF Associate Professor and Chief University of Illinois at Chicago Outline Colon cancer General Genetics, Risk, Screening Specific Syndromes, when to suspect,
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines
 Post Polypectomy Surveillance Guidelines") Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Alberta Colorectal Cancer Screening Program (ACRCSP) Post Polypectomy Surveillance Guidelines June 2013 ACRCSP Post Polypectomy Surveillance Guidelines - 2 TABLE OF CONTENTS Background... 3 Terms, Definitions
Disclosures. Colorectal Cancer Update GAFP November Risk Assessment. Colon and Rectal Cancer The Challenge. Issues in Colon and Rectal Cancer
 Disclosures Colorectal Cancer Update GAFP November 2006 Robert C. Hermann, MD Georgia Center for Oncology Research and Education Northwest Georgia Oncology Centers, PC WellStar Health System Marietta,
Disclosures Colorectal Cancer Update GAFP November 2006 Robert C. Hermann, MD Georgia Center for Oncology Research and Education Northwest Georgia Oncology Centers, PC WellStar Health System Marietta,
Colon Cancer Screening. Layth Al-Jashaami, MD GI Fellow, PGY 4
 Colon Cancer Screening Layth Al-Jashaami, MD GI Fellow, PGY 4 -Colorectal cancer (CRC) is a common and lethal cancer. -It has the highest incidence among GI cancers in the US, estimated to be newly diagnosed
Colon Cancer Screening Layth Al-Jashaami, MD GI Fellow, PGY 4 -Colorectal cancer (CRC) is a common and lethal cancer. -It has the highest incidence among GI cancers in the US, estimated to be newly diagnosed
ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes
 ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes Sapna Syngal, MD, MPH, FACG, 1,2,3 Randall E. Brand, MD, FACG, 4 James M. Church, MD, FACG, 5,6,7
ACG Clinical Guideline: Genetic Testing and Management of Hereditary Gastrointestinal Cancer Syndromes Sapna Syngal, MD, MPH, FACG, 1,2,3 Randall E. Brand, MD, FACG, 4 James M. Church, MD, FACG, 5,6,7
General Surgery Grand Grounds
 General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
General Surgery Grand Grounds University of Colorado Health Sciences Center Case Presentation December 24, 2009 Adam Lackey, PGY-5 J.L. - 2111609 27 YO female with chief complaint of abdominal pain. PMHx:
COLORECTAL CARCINOMA
 QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
QUICK REFERENCE FOR HEALTHCARE PROVIDERS MANAGEMENT OF COLORECTAL CARCINOMA Ministry of Health Malaysia Malaysian Society of Colorectal Surgeons Malaysian Society of Gastroenterology & Hepatology Malaysian
Navigators Lead the Way
 RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
RN Navigators Their Role in patients with Cancers of the GI tract Navigators Lead the Way Nurse Navigator Defined Nurse Navigator A clinically trained individual responsible for the identification and
Development of Carcinoma Pathways
 The Construction of Genetic Pathway to Colorectal Cancer Moriah Wright, MD Clinical Fellow in Colorectal Surgery Creighton University School of Medicine Management of Colon and Diseases February 23, 2019
The Construction of Genetic Pathway to Colorectal Cancer Moriah Wright, MD Clinical Fellow in Colorectal Surgery Creighton University School of Medicine Management of Colon and Diseases February 23, 2019
Hereditary Colorectal Cancer Syndromes Miguel A. Rodriguez-Bigas, MD
 Hereditary Colorectal Cancer Syndromes Miguel A. Rodriguez-Bigas, MD Living Beyond Cancer A-Z January 12,2019 Hereditary CRC Syndromes Objectives are to discuss the : Most common Hereditary CRC syndromes
Hereditary Colorectal Cancer Syndromes Miguel A. Rodriguez-Bigas, MD Living Beyond Cancer A-Z January 12,2019 Hereditary CRC Syndromes Objectives are to discuss the : Most common Hereditary CRC syndromes
Colon, or Colorectal, Cancer Information
 Colon, or Colorectal, Cancer Information Definition Colon, or colorectal, cancer is cancer that starts in the large intestine (colon) or the rectum (end of the colon). Other types of cancer can affect
Colon, or Colorectal, Cancer Information Definition Colon, or colorectal, cancer is cancer that starts in the large intestine (colon) or the rectum (end of the colon). Other types of cancer can affect
This is the portion of the intestine which lies between the small intestine and the outlet (Anus).
.") THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
THE COLON This is the portion of the intestine which lies between the small intestine and the outlet (Anus). 3 4 5 This part is responsible for formation of stool. The large intestine (colon- coloured
Hereditary GI tumor syndromes ACG guidelines of genetic testing and management. Dr. med. Henrik Csaba Horváth PhD
 Hereditary GI tumor syndromes ACG guidelines of genetic testing and management Dr. med. Henrik Csaba Horváth PhD Genetic testing and management of hereditary GI tumor syndromes June 29, 2016 2 Clinical
Hereditary GI tumor syndromes ACG guidelines of genetic testing and management Dr. med. Henrik Csaba Horváth PhD Genetic testing and management of hereditary GI tumor syndromes June 29, 2016 2 Clinical
Hereditary Non Polyposis Colorectal Cancer(HNPCC) From clinic to genetics
 From clinic to genetics") From clinic to genetics Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Autosomal dominant Question 2) Incidence of
From clinic to genetics Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Question 1) Clinical pattern of inheritance of the HNPCC-Syndrome? Autosomal dominant Question 2) Incidence of
Bowel obstruction and tumors
 Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Bowel obstruction and tumors Intestinal Obstruction Obstruction of the GI tract may occur at any level, but the small intestine is most often involved because of its relatively narrow lumen. Causes: Hernias
Content. Diagnostic approach and clinical management of Lynch Syndrome: guidelines. Terminology. Identification of Lynch Syndrome
 of Lynch Syndrome: guidelines 17/03/2009 Content Terminology Lynch Syndrome Presumed Lynch Syndrome Familial Colorectal Cancer Identification of Lynch Syndrome Amsterdam II criteria Revised Bethesda Guidelines
of Lynch Syndrome: guidelines 17/03/2009 Content Terminology Lynch Syndrome Presumed Lynch Syndrome Familial Colorectal Cancer Identification of Lynch Syndrome Amsterdam II criteria Revised Bethesda Guidelines
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM
 OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
OFCCR CLINICAL DIAGNOSIS AND TREATMENT FORM Name: _, OFCCR # _ OCGN # _ OCR Group # _ HIN# Sex: MALE FEMALE UNKNOWN Date of Birth: DD MMM YYYY BASELINE DIAGNOSIS & TREATMENT 1. Place of Diagnosis: Name
COLON CANCER PROFILE 2012} Cancer Outcomes Analysis Report. The Institute for. Cancer Care
 COLON CANCER PROFILE 2012} Cancer Outcomes Analysis Report The Institute for Cancer Care FACT} People with a first-degree relative (parent, sibling, or children) who has colon cancer are between two and
COLON CANCER PROFILE 2012} Cancer Outcomes Analysis Report The Institute for Cancer Care FACT} People with a first-degree relative (parent, sibling, or children) who has colon cancer are between two and
Colorectal Cancer in 2006: New Developments
 James J. Stark, MD Colorectal Cancer in 2006: New Developments Melissa Bennett, MS, CGC Myriad Genetic Laboratories Thomas Duntemann,, MD Ray Ramirez, Jr., MD Hereditary Colon Cancer and Genetic Testing
James J. Stark, MD Colorectal Cancer in 2006: New Developments Melissa Bennett, MS, CGC Myriad Genetic Laboratories Thomas Duntemann,, MD Ray Ramirez, Jr., MD Hereditary Colon Cancer and Genetic Testing
What All of Us Should Know About Cancer and Genetics
 What All of Us Should Know About Cancer and Genetics Beth A. Pletcher, MD, FAAP, FACMG Associate Professor of Pediatrics UMDNJ- New Jersey Medical School Disclosures I have no relevant financial relationships
What All of Us Should Know About Cancer and Genetics Beth A. Pletcher, MD, FAAP, FACMG Associate Professor of Pediatrics UMDNJ- New Jersey Medical School Disclosures I have no relevant financial relationships
A superficial radiotherapy B single pass curettage C excision with 2 mm margins D excision with 5 mm margins E Mohs micrographic surgery.
 1- A 63-year-old woman presents with a non-healing lesion on her right temple that has been present for over two years. On examination there is a 6 mm well defined lesion with central ulceration, telangiectasia
1- A 63-year-old woman presents with a non-healing lesion on her right temple that has been present for over two years. On examination there is a 6 mm well defined lesion with central ulceration, telangiectasia
Policy Specific Section: Medical Necessity and Investigational / Experimental. October 14, 1998 March 28, 2014
 Medical Policy Genetic Testing for Colorectal Cancer Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Laboratory/Pathology Original Policy Date: Effective Date: October
Medical Policy Genetic Testing for Colorectal Cancer Type: Medical Necessity and Investigational / Experimental Policy Specific Section: Laboratory/Pathology Original Policy Date: Effective Date: October
CRC and Endoscopy. Objectives. Background
 CRC and Endoscopy Darren Ballard, MD Assistant Professor Gastroenterology/Hepatology Medical College of Wisconsin Objectives Review background demographics and pathways for colon cancer Review colorectal
CRC and Endoscopy Darren Ballard, MD Assistant Professor Gastroenterology/Hepatology Medical College of Wisconsin Objectives Review background demographics and pathways for colon cancer Review colorectal
Colon Cancer Update Christie J. Hilton, DO
 POMA Winter Conference Christie Hilton DO Medical Oncology January 2018 None Colon Cancer Numbers Screening (brief update) Practice changing updates in colon cancer MSI Testing Immunotherapy in Colon Cancer
POMA Winter Conference Christie Hilton DO Medical Oncology January 2018 None Colon Cancer Numbers Screening (brief update) Practice changing updates in colon cancer MSI Testing Immunotherapy in Colon Cancer
Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes
 Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes Policy Number: 2.04.08 Last Review: 1/2019 Origination: 1/2004 Next Review: 1/2020 Policy Blue Cross and Blue Shield of Kansas
Genetic Testing for Lynch Syndrome and Other Inherited Colon Cancer Syndromes Policy Number: 2.04.08 Last Review: 1/2019 Origination: 1/2004 Next Review: 1/2020 Policy Blue Cross and Blue Shield of Kansas
FACT SHEET 49. What is meant by a family history of bowel cancer? What is bowel cancer? What causes bowel cancer?
 Important points The most important factors that can influence an individual s chance of developing bowel cancer are getting older and having a family history of bowel cancer A family history of bowel
Important points The most important factors that can influence an individual s chance of developing bowel cancer are getting older and having a family history of bowel cancer A family history of bowel
Yes when meets criteria below. Dean Health Plan covers when Medicare also covers the benefit.
 Genetic Testing for Lynch Syndrome MP9487 Covered Service: Prior Authorization Required: Additional Information: Yes when meets criteria below Yes-as shown below Pre and post test genetic counseling is
Genetic Testing for Lynch Syndrome MP9487 Covered Service: Prior Authorization Required: Additional Information: Yes when meets criteria below Yes-as shown below Pre and post test genetic counseling is
DIGESTIVE SYSTEM SURGICAL PROCEDURES May 1, 2015 INTESTINES (EXCEPT RECTUM) Asst Surg Anae
 Asst Surg Anae") ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
ENDOSCOPY Z50 Duodenoscopy (not to be claimed if Z399 and/or Z00 performed on same patient within 3 months)... 92.10 Z9 Subsequent procedure (within three months following previous endoscopic procedure)...
Structured Follow-Up after Colorectal Cancer Resection: Overrated. R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007
 Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
Structured Follow-Up after Colorectal Cancer Resection: Overrated R. Taylor Ripley University of Colorado Grand Rounds April 23, 2007 Guidelines for Colonoscopy Production: Surveillance US Multi-Society
Colorectal Cancer - Working in Partnership. David Baty Genetics, Ninewells Hospital
 Colorectal Cancer - Working in Partnership David Baty Genetics, Ninewells Hospital Genetics and Pathology National initiatives Colorectal cancer Inherited CRC Sporadic CRC The Liquid Biopsy The future?
Colorectal Cancer - Working in Partnership David Baty Genetics, Ninewells Hospital Genetics and Pathology National initiatives Colorectal cancer Inherited CRC Sporadic CRC The Liquid Biopsy The future?
Disclosure. Polyps in Pediatrics. Learning Objectives. Case Presentation I. Case Presentation II
 Disclosure Polyps in Pediatrics I have no relationships with commercial companies to disclose. Sonal Desai, MD Division of Pediatric Gastroenterology May 31, 2013 Pediatric Grand Rounds Learning Objectives
Disclosure Polyps in Pediatrics I have no relationships with commercial companies to disclose. Sonal Desai, MD Division of Pediatric Gastroenterology May 31, 2013 Pediatric Grand Rounds Learning Objectives
Historical. Note: The parenthetical numbers in the Clinical Indications section refer to the source documents cited in the References Section below.
 Clinical UM Guideline Subject: Colonoscopy Guideline #: CG-SURG-01 Current Effective Date: 01/21/2015 Status: Revised Last Review Date: 05/15/2014 Description Colonoscopy describes the direct visual inspection
Clinical UM Guideline Subject: Colonoscopy Guideline #: CG-SURG-01 Current Effective Date: 01/21/2015 Status: Revised Last Review Date: 05/15/2014 Description Colonoscopy describes the direct visual inspection
Genetic testing all you need to know
 Genetic testing all you need to know Sue Clark Consultant Colorectal Surgeon, St Mark s Hospital, London, UK. Colorectal cancer Familial 33% Polyposis syndromes
Genetic testing all you need to know Sue Clark Consultant Colorectal Surgeon, St Mark s Hospital, London, UK. Colorectal cancer Familial 33% Polyposis syndromes
BOWEL CANCER. Causes of bowel cancer
 A cancer is an abnormality in an organ that grows without control. The growth is often quite slow, but will continue unabated until it is detected. It can cause symptoms by its presence in the organ or
A cancer is an abnormality in an organ that grows without control. The growth is often quite slow, but will continue unabated until it is detected. It can cause symptoms by its presence in the organ or
Adenoma to Carcinoma Pathway
 It is widely accepted that more than 95% of colorectal cancers arise from adenomatous polyps, which are generally defined as benign lesions with dysplastic epithelium that have variable potential for malignancy.
It is widely accepted that more than 95% of colorectal cancers arise from adenomatous polyps, which are generally defined as benign lesions with dysplastic epithelium that have variable potential for malignancy.
CHEMOTHERAPY FOR COLON CANCER OUTLINE OF TODAY S TALK. Colon Cancer Epidemiology 11/6/2012 GATRA/GCCR FALL CONFERENCE NOVEMBER 14 16, 2012
 CHEMOTHERAPY FOR COLON CANCER JONATHAN C. BENDER,MD MEDICAL DIRECTOR OF PIEDMONT FAYETTE CANCER CENTER OUTLINE OF TODAY S TALK 1. Overview of Colon Cancer in the US 2. Colon Cancer staging and risks of
CHEMOTHERAPY FOR COLON CANCER JONATHAN C. BENDER,MD MEDICAL DIRECTOR OF PIEDMONT FAYETTE CANCER CENTER OUTLINE OF TODAY S TALK 1. Overview of Colon Cancer in the US 2. Colon Cancer staging and risks of
A Brief Overview of Screening and Management of Colorectal Cancer
 A Brief Overview of Screening and Management of Colorectal Cancer Gentry King MD Assistant Professor Hematology and Medical Oncology University of Colorado Disclosures Nothing to disclose Objectives Review
A Brief Overview of Screening and Management of Colorectal Cancer Gentry King MD Assistant Professor Hematology and Medical Oncology University of Colorado Disclosures Nothing to disclose Objectives Review
Duodenal adenomas Management. Dr Stratis Alexandridis Consultant Gastroenterologist BRI
 Duodenal adenomas Management Dr Stratis Alexandridis Consultant Gastroenterologist BRI Introduction Ampullary and non ampullary polyps of the duodenum are diagnosed within and outside genetic syndromes.
Duodenal adenomas Management Dr Stratis Alexandridis Consultant Gastroenterologist BRI Introduction Ampullary and non ampullary polyps of the duodenum are diagnosed within and outside genetic syndromes.
MEDICAL POLICY SUBJECT: GENETIC TESTING FOR INHERITED SUSCEPTIBILITY TO COLORECTAL CANCER. POLICY NUMBER: CATEGORY: Laboratory Test
 MEDICAL POLICY SUBJECT: GENETIC TESTING FOR INHERITED SUSCEPTIBILITY TO COLORECTAL CANCER POLICY NUMBER: 2.02.11 CATEGORY: Laboratory Test EFFECTIVE DATE: 09/16/99 REVISED DATE: 04/19/01, 05/16/02, 06/19/03,
MEDICAL POLICY SUBJECT: GENETIC TESTING FOR INHERITED SUSCEPTIBILITY TO COLORECTAL CANCER POLICY NUMBER: 2.02.11 CATEGORY: Laboratory Test EFFECTIVE DATE: 09/16/99 REVISED DATE: 04/19/01, 05/16/02, 06/19/03,
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE
 COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
COLORECTAL CANCER FAISALGHANISIDDIQUI MBBS; FCPS; PGDIP-BIOETHICS; MCPS-HPE PROFESSOR OF SURGERY & DIRECTOR, PROFESSIONAL DEVELOPMENT CENTRE J I N N A H S I N D H M E D I C A L U N I V E R S I T Y faisal.siddiqui@jsmu.edu.pk
Primary Care Approach to Genetic Cancer Syndromes
 Primary Care Approach to Genetic Cancer Syndromes Jason M. Goldman, MD, FACP FAU School of Medicine Syndromes Hereditary Breast and Ovarian Cancer (HBOC) Hereditary Nonpolyposis Colorectal Cancer (HNPCC)
Primary Care Approach to Genetic Cancer Syndromes Jason M. Goldman, MD, FACP FAU School of Medicine Syndromes Hereditary Breast and Ovarian Cancer (HBOC) Hereditary Nonpolyposis Colorectal Cancer (HNPCC)
Management of higher risk of colorectal cancer. Huw Thomas
 Management of higher risk of colorectal cancer Huw Thomas Colorectal Cancer 41,000 new cases pa in UK 16,000 deaths pa 60% 5 year survival Adenoma-carcinoma sequence (Morson) Survival vs stage (Dukes)
Management of higher risk of colorectal cancer Huw Thomas Colorectal Cancer 41,000 new cases pa in UK 16,000 deaths pa 60% 5 year survival Adenoma-carcinoma sequence (Morson) Survival vs stage (Dukes)
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Genetic Testing for Lynch Syndrome
 Genetic Testing for Lynch Syndrome MP9487 Covered Service: Prior Authorization Required: Additional Information: Yes when meets criteria below Yes-as shown below Pre and post-test genetic counseling is
Genetic Testing for Lynch Syndrome MP9487 Covered Service: Prior Authorization Required: Additional Information: Yes when meets criteria below Yes-as shown below Pre and post-test genetic counseling is
Genetic Testing for Familial Gastrointestinal Cancer Syndromes. C. Richard Boland, MD La Jolla, CA January 21, 2017
 Genetic Testing for Familial Gastrointestinal Cancer Syndromes C. Richard Boland, MD La Jolla, CA January 21, 2017 Disclosure Information C. Richard Boland, MD I have no financial relationships to disclose.
Genetic Testing for Familial Gastrointestinal Cancer Syndromes C. Richard Boland, MD La Jolla, CA January 21, 2017 Disclosure Information C. Richard Boland, MD I have no financial relationships to disclose.
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care
 Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Quality ID #343: Screening Colonoscopy Adenoma Detection Rate National Quality Strategy Domain: Effective Clinical Care 2018 OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY MEASURE TYPE: Outcome DESCRIPTION:
Rectal Cancer. GI Practice Guideline
 Rectal Cancer GI Practice Guideline Dr. Brian Dingle MSc, MD, FRCPC Dr. Francisco Perera MD, FRCPC (Radiation Oncologist) Dr. Jay Engel MD, FRCPC (Surgical Oncologist) Approval Date: 2006 This guideline
Rectal Cancer GI Practice Guideline Dr. Brian Dingle MSc, MD, FRCPC Dr. Francisco Perera MD, FRCPC (Radiation Oncologist) Dr. Jay Engel MD, FRCPC (Surgical Oncologist) Approval Date: 2006 This guideline
GI Polyp syndromes in children. Screening and surveillance, surgery.
 Dr Warren Hyer Consultant Paediatric Gastroenterologist St Mark s Hospital, UK GI Polyp syndromes in children Screening and surveillance, surgery. No conflict of interests to declare Objectives Understand
Dr Warren Hyer Consultant Paediatric Gastroenterologist St Mark s Hospital, UK GI Polyp syndromes in children Screening and surveillance, surgery. No conflict of interests to declare Objectives Understand
Clinical Colon Cancer Abby Siegel MD COLON CANCER. 1. Epidemiology 2. Risk factors 3. Manifestations 4. Treatment
 Clinical Colon Cancer 2008 Abby Siegel MD COLON CANCER 1. Epidemiology 2. Risk factors 3. Manifestations 4. Treatment 1 1. EPIDEMIOLOGY - Colorectal cancer is the third most common cancer in the United
Clinical Colon Cancer 2008 Abby Siegel MD COLON CANCER 1. Epidemiology 2. Risk factors 3. Manifestations 4. Treatment 1 1. EPIDEMIOLOGY - Colorectal cancer is the third most common cancer in the United
Imaging Evaluation of Polyps. CT Colonography: Sessile Adenoma. Polyps, DALMs & Megacolon Objectives
 Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Polyps, DALMs & Megacolon: Pathology and Imaging of the Colon and Rectum Angela D. Levy and Leslie H. Sobin Washington, DC Drs. Levy and Sobin have indicated that they have no relationships which, in the
Hyperplastische Polyps Innocent bystanders?
 Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
Hyperplastische Polyps Innocent bystanders?? K. Geboes P th l i h O tl dk d Pathologische Ontleedkunde, KULeuven Content Historical Classification Relation Hyperplastic polyps carcinoma The concept cept
ADVANCES IN COLORECTAL CANCERS IS THERE HOPE? Dr Lim Hwee Yong Medical Oncologist
 ADVANCES IN COLORECTAL CANCERS IS THERE HOPE? Dr Lim Hwee Yong Medical Oncologist limhweeyong@live.com CRC: Epidemiology in 2012 Third most common cancer diagnosis in US [1] Estimated 143,460 new cases
ADVANCES IN COLORECTAL CANCERS IS THERE HOPE? Dr Lim Hwee Yong Medical Oncologist limhweeyong@live.com CRC: Epidemiology in 2012 Third most common cancer diagnosis in US [1] Estimated 143,460 new cases
ADJUVANT CHEMOTHERAPY...
 Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
Colorectal Pathway Board: Non-Surgical Oncology Guidelines October 2015 Organization» Table of Contents ADJUVANT CHEMOTHERAPY... 2 DUKES C/ TNM STAGE 3... 2 DUKES B/ TNM STAGE 2... 3 LOCALLY ADVANCED
GENETICS OF COLORECTAL CANCER: HEREDITARY ASPECTS By. Magnitude of the Problem. Magnitude of the Problem. Cardinal Features of Lynch Syndrome
 GENETICS OF COLORECTAL CANCER: HEREDITARY ASPECTS By HENRY T. LYNCH, M.D. 1 Could this be hereditary Colon Cancer 4 Creighton University School of Medicine Omaha, Nebraska Magnitude of the Problem Annual
GENETICS OF COLORECTAL CANCER: HEREDITARY ASPECTS By HENRY T. LYNCH, M.D. 1 Could this be hereditary Colon Cancer 4 Creighton University School of Medicine Omaha, Nebraska Magnitude of the Problem Annual
Joint Session with ACOFP and Cancer Treatment Centers of America (CTCA): Cancer Screening: Consensus & Controversies. Ashish Sangal, M.D.
: Cancer Screening: Consensus & Controversies. Ashish Sangal, M.D.") Joint Session with ACOFP and Cancer Treatment Centers of America (CTCA): Cancer Screening: Consensus & Controversies Ashish Sangal, M.D. Cancer Screening: Consensus & Controversies Ashish Sangal, MD Director,
Joint Session with ACOFP and Cancer Treatment Centers of America (CTCA): Cancer Screening: Consensus & Controversies Ashish Sangal, M.D. Cancer Screening: Consensus & Controversies Ashish Sangal, MD Director,
Quality Measures In Colonoscopy: Why Should I Care?
 Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
Quality Measures In Colonoscopy: Why Should I Care? David Greenwald, MD, FASGE Professor of Clinical Medicine Albert Einstein College of Medicine Montefiore Medical Center Bronx, New York ACG/ASGE Best
CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION
 CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION PROVIDED AS AN EDUCATIONAL SERVICE BY THE INSTITUTE FOR CONTINUING HEALTHCARE EDUCATION SUPPORTED BY AN EDUCATIONAL GRANT FROM GENENTECH LEARNING
CASE STUDIES IN COLORECTAL CANCER: A ROUNDTABLE DISCUSSION PROVIDED AS AN EDUCATIONAL SERVICE BY THE INSTITUTE FOR CONTINUING HEALTHCARE EDUCATION SUPPORTED BY AN EDUCATIONAL GRANT FROM GENENTECH LEARNING
SMALL BOWEL ADENOCARCINOMA. Dr. C. Jeske
 SMALL BOWEL ADENOCARCINOMA Dr. C. Jeske Case presentation 54 year old female. Presents with OJ and weight loss. Abdominal examination only reveals a palpable gallbladder. ERCP reveals a circumferential
SMALL BOWEL ADENOCARCINOMA Dr. C. Jeske Case presentation 54 year old female. Presents with OJ and weight loss. Abdominal examination only reveals a palpable gallbladder. ERCP reveals a circumferential
Clinical UM Guideline
 Subject: Guideline #: Current Effective Date: 06/28/2016 Status: Revised Last Review Date: 05/05/2016 Description This document addresses colonoscopy, an endoscopic procedure which allows direct visual
Subject: Guideline #: Current Effective Date: 06/28/2016 Status: Revised Last Review Date: 05/05/2016 Description This document addresses colonoscopy, an endoscopic procedure which allows direct visual
Genetics of Pancreatic Cancer. October 6, If you experience technical difficulty during the presentation:
 Genetics of Pancreatic Cancer October 6, 2016 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-229-3239 Toll Only: 1-408-435-7088
Genetics of Pancreatic Cancer October 6, 2016 If you experience technical difficulty during the presentation: Contact WebEx Technical Support directly at: US Toll Free: 1-866-229-3239 Toll Only: 1-408-435-7088