Nodal Treatment in Melanoma: Snow to MSLT-II
|
|
|
- John McDowell
- 5 years ago
- Views:
Transcription

1 Nodal Treatment in Melanoma: Snow to MSLT-II Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Program Director, JWCI Complex General Surgical Oncology Fellowship Director, Therapeutic Immunology February 27, 2016
2 Outline History Elective Node Dissection Sentinel Lymph Node MSLT-I Indications (Thin/Thick) RT-PCR evaluation of SLN Nodal Ultrasound Completion Node Dissection

3 Herbert Lumley Snow, MD
4 Elective Lymph Node Dissection A radical cure is alone thus rendered possible in the more common instance of the more common forms of Cancer. It was, and It is essential to remove, whenever possible, those lymph glands which first receive the infective protoplasm, and bar its entrance into the blood, before they have undergone increase in bulk. This is Anticipatory Gland-Excision, a simple common-sense measure, adding nothing to the gravity of a surgical operation, while most materially enhancing its efficacy..
5 Elective Lymph Node Dissection: WHO #14 All (>1.5mm)
6 Elective Lymph Node Dissection: WHO #14 All (>1.5mm) mm >4.0mm
7 Elective Lymph Node Dissection: Intergroup Balch, Ann Surg Oncol, 2000
8 Intergroup ELND: Subgroups 1-2 mm Age < 60 Limb Melanoma Non-ulcerated
9 Problem: Identification of patients
10 Problem: Identification of patients 80% of patients undergoing ELND had negative nodes Others have concomitant systemic spread not cured by ELND
11 Problem: Identification of patients 80% of patients undergoing ELND had negative nodes Others have concomitant systemic spread not cured by ELND Only a subset can benefit from nodal surgery
12 History of the Sentinel Node Concept Rudolph Virchow
13 History of the Sentinel Node Concept Rudolph Virchow Leonard R. Braithwaite, FRCS (1923) glans sentinel Upper abdominal node trapping bacterial from the ileum/cecum
14 History of the Sentinel Node Concept Rudolph Virchow Leonard R. Braithwaite, FRCS (1923) glans sentinel Upper abdominal node trapping bacterial from the ileum/cecum Joseph Weinberg (1950/1951) Blue dye injection for stomach/lung
15 History of the Sentinel Node Concept Rudolph Virchow Leonard R. Braithwaite, FRCS (1923) glans sentinel Upper abdominal node trapping bacterial from the ileum/cecum Joseph Weinberg (1950/1951) Blue dye injection for stomach/lung Gould (1960) Parotid tumor upper neck LN
16 History of the Sentinel Node Concept Rudolph Virchow Leonard R. Braithwaite, FRCS (1923) glans sentinel Upper abdominal node trapping bacterial from the ileum/cecum Joseph Weinberg (1950/1951) Blue dye injection for stomach/lung Gould (1960) Parotid tumor upper neck LN Cabanas (1977) Penile carcinoma Superficial groin LN

17 Donald L. Morton, MD

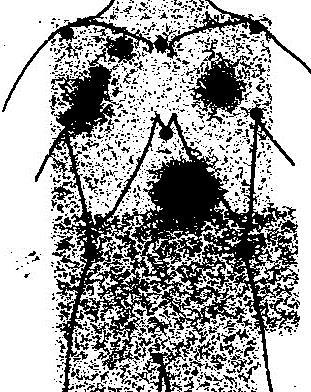
18 Lymphoscintigraphy for Nodal Irradiation
19 Lymphoscintigraphy for Melanoma
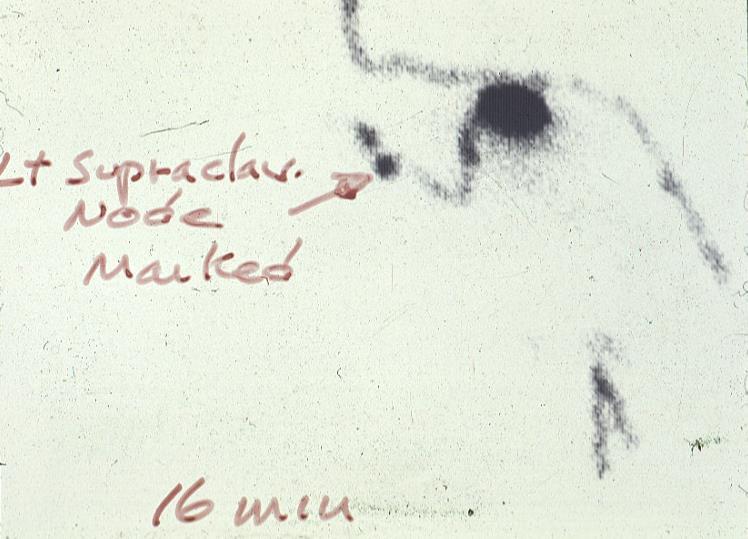
20 Lymphoscintigraphy for Melanoma Cutaneous Lymphoscintigraphy Tc 99m Human Serum Albumin
21
22
23
24
25 Dermal Lymphatics


26 Dermal Lymphatics
27 Intraoperative Identification
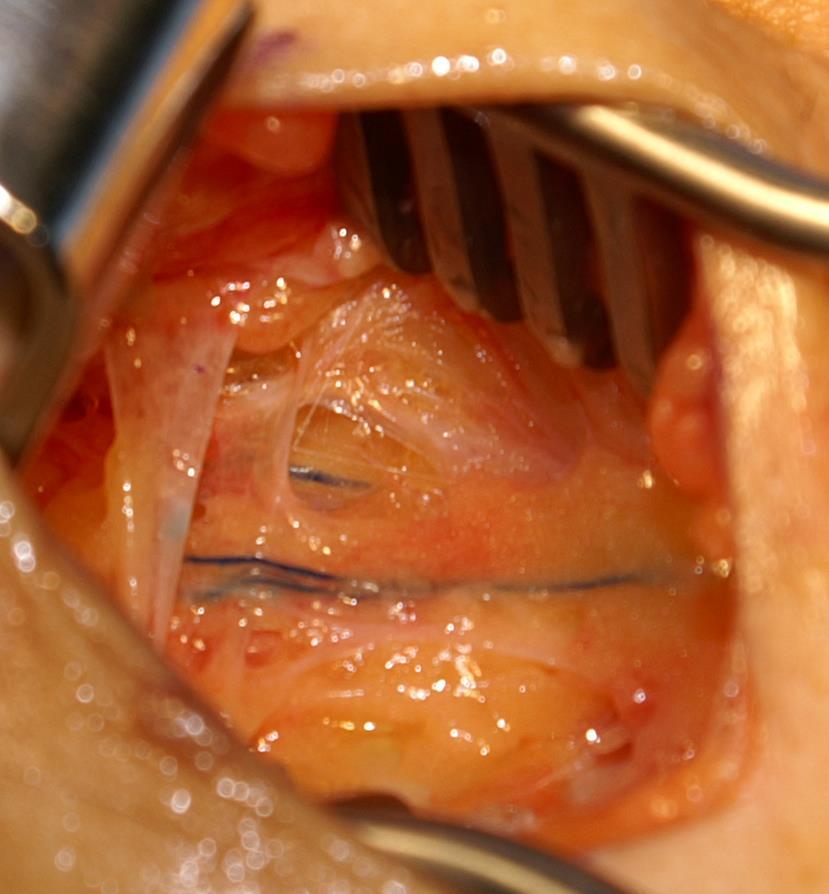
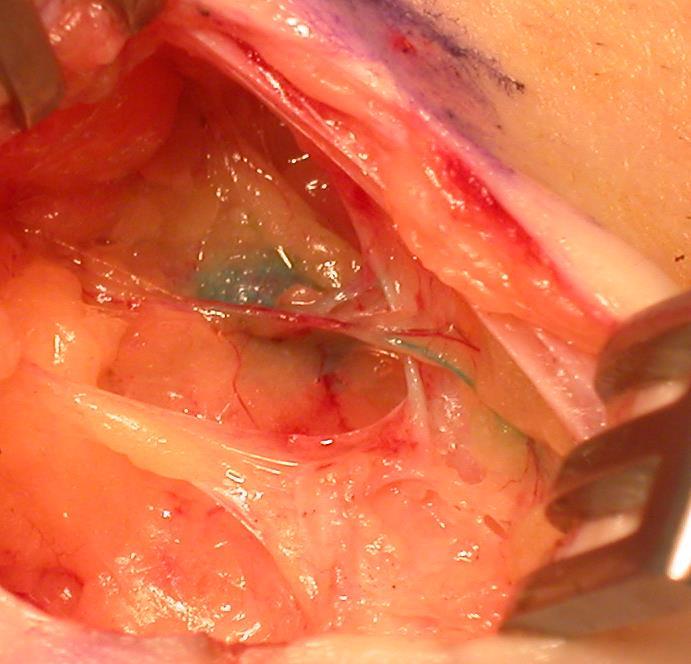
28 Intraoperative Identification

29 Multicenter Selective Lymphadenectomy Trials
30 MSLT-I: Trial Design Melanoma >1 mm or > Clark IV (primary analysis mm)
31 MSLT-I: Trial Design Melanoma >1 mm or > Clark IV (primary analysis mm) Randomization Wide excision alone 40% 60% Wide excision + SLN
32 MSLT-I: Trial Design Melanoma >1 mm or > Clark IV (primary analysis mm) Randomization Wide excision alone 40% 60% Wide excision + SLN CLND for Recurrence No recurrence: observation
33 MSLT-I: Trial Design Melanoma >1 mm or > Clark IV (primary analysis mm) Randomization Wide excision alone 40% 60% Wide excision + SLN SLN + SLN - CLND for Recurrence No recurrence: observation
34 MSLT-I: Trial Design Melanoma >1 mm or > Clark IV (primary analysis mm) Randomization Wide excision alone 40% 60% Wide excision + SLN SLN + SLN - CLND for Recurrence Immediate CLND No recurrence: observation Observation
35 MSLT-I: Trial Design Melanoma >1 mm or > Clark IV (primary analysis mm) Randomization DSS: Primary Endpoint DFS: Secondary Endpoint Wide excision alone 40% 60% Wide excision + SLN SLN + SLN - CLND for Recurrence Immediate CLND No recurrence: observation Observation
36 MSLT-I: Trial Design Melanoma >1 mm or > Clark IV (primary analysis mm) Randomization DSS: Primary Endpoint DFS: Secondary Endpoint Wide excision alone 40% 60% Wide excision + SLN SLN + SLN - Occult Stage III CLND for Recurrence Immediate CLND No recurrence: observation Observation
37 MSLT-I prognosis
38 MSLT-I prognosis
39 MSLT-I prognosis

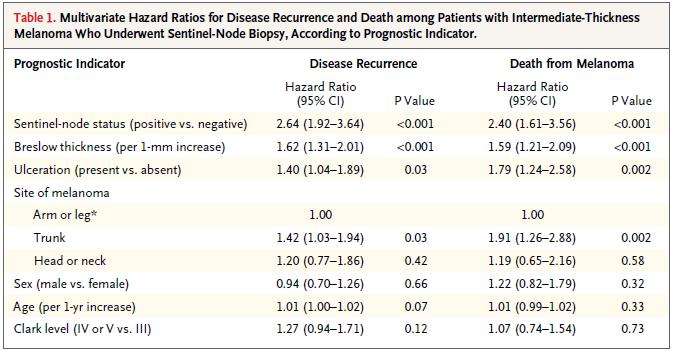

40 MSLT-I prognosis

41 Staging vs. ELND or Clin Exam
42 SLN: Learning Curve
43 SLN Biopsy and Disease-Free Survival: MSLT-I
44 SLN Biopsy and Disease-Free Survival: MSLT-I Intermediate Thickness ( mm)
 Thick ( 3.")
45 SLN Biopsy and Disease-Free Survival: MSLT-I Intermediate Thickness ( mm) Thick ( 3.5mm)
46 Delayed treatment metastatic spread within the regional nodal basin
47 Mean # Pos. Nodes Delayed treatment metastatic spread within the regional nodal basin ± ± 0.1 SNB Watch & Wait Immediate CLND Delayed CLND

48 Impact of Clinical Recurrence: Morbidity MSLT-I
49 Number of Nodes Removed Lymphedema by Extent of Dissection Lymphedema No Lymphedema p=0.61 p=0.35

50 Number of Nodes Removed Lymphedema by Extent of Dissection % 34.2% Lymphedema % 22.6% Immediate No Lymphedema 15 Delayed 10 p=0.61 p= Superficial Superficial and Deep


 ± SE 5-year 10-year 85.7 ± 1.")
51 Survival (%) Overall Melanoma Related Survival (Breslow mm) Final Dataset 100 SNB HR: 0.84 P=0.18, 95% CI ( ) Group OBS SNB # Event / Total N 97 / / 770 Estimate S(t) ± SE 5-year 10-year 85.7 ± 1.6 % 78.3 ± 2.0% 86.6 ± 1.3 % 81.4 ± 1.5 % Time (years) OBS
52 MSLT-I: Trial Design Melanoma >1 mm or > Clark IV (primary analysis mm) Randomization DSS: Primary Endpoint DFS: Secondary Endpoint Wide excision alone 40% 60% Wide excision + SLN SLN + SLN - Occult Stage III CLND for Recurrence Immediate CLND No recurrence: observation Observation
53 Survival (%) Morton A 50 Year Odyssey Melanoma Specific Survival Node+ ( mm) Final Dataset 100 Group # Event / Estimate S(t) ± SE % Total N 5-year 10-year OBS, had nodal recur. 48/ ± ± 5.6 SNB+ 70 / ± ± SNB HR: % C.I. (0.37, 0.84) Log Rank P=0.006 OBS Time (years)
 Randomization DSS: Primary Endpoint DFS: Secondary Endpoint")

54 MSLT-I: Trial Design Melanoma >1 mm or > Clark IV (primary analysis mm) Randomization DSS: Primary Endpoint DFS: Secondary Endpoint Wide excision alone 40% 60% Wide excision + SLN SLN + SLN - Occult Stage III CLND for Recurrence Immediate CLND No recurrence: observation Observation

55 Factor (%) Patient Characteristics by Intent to Treat Randomization All Strata mm Years Female SNB Watch and Wait Male Gender Ext H/N Trunk Site III IV V Clark N=1973 NS Yes No? Ulceration Mean Median Breslow Mean Age Median
56 Cumulative Incidence of Nodal Metastases Detected by Sentinel Node Biopsy or by Nodal Observation Breslow mm Breslow > 3.5 mm



57 Latent Subgroup Analysis
58 Survival (%) Morton A 50 Year Odyssey Melanoma Specific Survival Node+ ( mm) Final Dataset 100 Group # Event / Estimate S(t) ± SE % Total N 5-year 10-year OBS, had nodal recur. 48/ ± ± 5.6 SNB+ 70 / ± ± SNB HR: % C.I. (0.37, 0.84) Log Rank P=0.006 OBS Time (years)

59 Patient Selection for SLNB
60 Thin melanoma and SLND Does a positive SLN matter in thin melanoma?
61 Thin melanoma and SLND Does a positive SLN matter in thin melanoma? Wong, et al. [Ann Surg Oncol, 2006]
62 Thin melanoma and SLND Does a positive SLN matter in thin melanoma? Wong, et al. [Ann Surg Oncol, 2006] No deaths in SLN+ patients with thin lesions
63 Thin melanoma and SLND Does a positive SLN matter in thin melanoma? Wong, et al. [Ann Surg Oncol, 2006] No deaths in SLN+ patients with thin lesions BUT:
64 Thin melanoma and SLND Does a positive SLN matter in thin melanoma? Wong, et al. [Ann Surg Oncol, 2006] No deaths in SLN+ patients with thin lesions BUT: N=8 Median f/u = 25 months (median time to recurrence = 45 months)
65 Thin melanoma and SLND 31 of 631 (5%) positive
")
66 Melanoma-specific Survival Thin melanoma and SLND 31 of 631 (5%) positive
67 Thin melanoma: SLN / Prognosis
68 Thin melanoma: SLN / Prognosis

69 Thin melanoma: SLN / Prognosis


70 Survival Probability Node-Positive Thin Melanoma Outcomes Penn JWCI SLN + Penn JWCI Nodal recurrence Months
71 NCCN: SLN and Thin Melanoma Stage IA (<0.75 mm, thick, no ulceration, mitotic rate <1/mm 2 ) Stage IB (<0.75 mm thick with ulceration and/or mitotic rate >1/mm 2 )
72 NCCN: SLN and Thin Melanoma Stage IA (<0.75 mm, thick, no ulceration, mitotic rate <1/mm 2 ) Stage IB (<0.75 mm thick with ulceration and/or mitotic rate >1/mm 2 ) Usually No
73 NCCN: SLN and Thin Melanoma Stage IA (<0.75 mm, thick, no ulceration, mitotic rate <1/mm 2 ) Stage IB (<0.75 mm thick with ulceration and/or mitotic rate >1/mm 2 ) Usually No In general, SLNB is not recommended for primary melanoma <0.75 mm thick unless there is significant uncertainty about the adequacy of microstaging.
74 NCCN: SLN and Thin Melanoma Stage IA (<0.75 mm, thick, no ulceration, mitotic rate <1/mm 2 ) Stage IB (<0.75 mm thick with ulceration and/or mitotic rate >1/mm 2 ) Usually No In general, SLNB is not recommended for primary melanoma <0.75 mm thick unless there is significant uncertainty about the adequacy of microstaging. Stage IA ( mm thick, no ulceration, mitotic rate <1/mm 2 )
75 NCCN: SLN and Thin Melanoma Stage IA (<0.75 mm, thick, no ulceration, mitotic rate <1/mm 2 ) Stage IB (<0.75 mm thick with ulceration and/or mitotic rate >1/mm 2 ) Usually No In general, SLNB is not recommended for primary melanoma <0.75 mm thick unless there is significant uncertainty about the adequacy of microstaging. Stage IA ( mm thick, no ulceration, mitotic rate <1/mm 2 ) Discuss and Consider
76 NCCN: SLN and Thin Melanoma Stage IA (<0.75 mm, thick, no ulceration, mitotic rate <1/mm 2 ) Stage IB (<0.75 mm thick with ulceration and/or mitotic rate >1/mm 2 ) Usually No In general, SLNB is not recommended for primary melanoma <0.75 mm thick unless there is significant uncertainty about the adequacy of microstaging. Stage IA ( mm thick, no ulceration, mitotic rate <1/mm 2 ) Stage IB ( mm thick, with ulceration or mitotic rate >1/mm 2 ) Discuss and Consider
77 NCCN: SLN and Thin Melanoma Stage IA (<0.75 mm, thick, no ulceration, mitotic rate <1/mm 2 ) Stage IB (<0.75 mm thick with ulceration and/or mitotic rate >1/mm 2 ) Usually No In general, SLNB is not recommended for primary melanoma <0.75 mm thick unless there is significant uncertainty about the adequacy of microstaging. Stage IA ( mm thick, no ulceration, mitotic rate <1/mm 2 ) Discuss and Consider Stage IB ( mm thick, with ulceration or mitotic rate >1/mm 2 ) Discuss and Offer
 Usually No In general, SLNB is not recommended for primary melanoma <0.")
78 NCCN: SLN and Thin Melanoma Stage IA (<0.75 mm, thick, no ulceration, mitotic rate <1/mm 2 ) Stage IB (<0.75 mm thick with ulceration and/or mitotic rate >1/mm 2 ) Usually No In general, SLNB is not recommended for primary melanoma <0.75 mm thick unless there is significant uncertainty about the adequacy of microstaging. Stage IA ( mm thick, no ulceration, mitotic rate <1/mm 2 ) Discuss and Consider Stage IB ( mm thick, with ulceration or mitotic rate >1/mm 2 ) Discuss and Offer In patients with thin melanomas (<1.0 mm), apart from primary tumor thickness, there is little consensus as to what should be considered high-risk features for a positive SLN. Conventional risk factors for a positive SLN, such as ulceration, high mitotic rate, and lymphovascular invasion (LVI) are very uncommon in melanoma <0.75 mm thick.
79 SLN Selection: Thin Sentinel node studies Clinical recurrence studies Author < <1.00 Factors Bedrosian* 1/40 (2.5%) 3/31 (9.7%) 4/71 (5.6%) VGP, no other Bleicher 2/118 (1.7%) 6/154 (3.9%) 8/272 (2.9%) Age, incomplete bx Jacobs 1/NR 1/NR 2/63 (3.2%) Kesmodel 1/91 (1.1%) 8/90 (8.9%) 9/181 (5.0%) MR, Br, gender Lowe 2/NR 1/NR 3/46 (6.5%) Clark >III Nahabedian 0/NR 2/NR 2/24 (8.3%) Oliveira Filho NR NR 6/77 (7.8%) ulceration, MR, VGP Puleo NR 20/409 (4.9%) NR None predictive Wong 0/109 8/114 (7.0%) 8/223 (3.6%) None predictive Stitzenberg 3/NR 3/NR 6/146 (4.1%) None predictive Herschko 2/NR 3/NR 5/64 (7.8%) Age Morton NR NR 238/1979 (12.0%) Kalady NR NR 38/1082 (3.5%) Massi** 8/174 (4.6%) 17/113 (15%) 25/287 (8.7%) TIL Karakousis 21/684 (3.1%) 17/198 (8.6%) 38/882 (4.3%) male,<60,axial Corsetti 0/NR 5/NR 5/68 (7.4%) med TTR 52mo Schmidt-Wendtner 37/2301 (1.6%) NR NR male, ALM or LMM McKinnon NR NR NR TTR 49.8mo Woods 5/400 (1.3%) NR NR 2.8% total recur Naruns 28/649 (4.3%) NR NR male, regression TOTAL 102/4526(2.3%) 59/965 (6.1%) 372/5178 (7.2%) * These patients also in Kesmodel, not duplicated in total figures. ** up to 1.5 mm included, not included in total figures.
80 Predictors Breslow
81 Predictors Breslow Clark I II III IV V UNK
82 Predictors Breslow Clark Ulceration I II III IV V UNK 0.0 Yes No Unknown
83 Predictors Breslow Clark Ulceration I II III IV V UNK 0.0 Yes No Unknown Gender Female Male
84 Predictors Breslow Clark Ulceration I II III IV V UNK 0.0 Yes No Unknown Gender Primary Site 0.0 Female Male 0.0 Extremity Head/neck Trunk

85 Predictors Breslow Clark Ulceration I II III IV V UNK 0.0 Yes No Unknown Gender Primary Site Age 0.0 Female Male 0.0 Extremity Head/neck Trunk 0.0 < >=70
86 Predicted probabilities of Nodal Recurrence Breslow Age Sex % node recurrence <0.5 >70 female 0.1 <0.5 >70 male 0.4 < female 0.3 < male 0.9 <0.5 <50 female 0.6 <0.5 <50 male >70 female >70 male female male <50 female <50 male >70 female >70 male female male <50 female <50 male 17.4
87 Thick Melanoma? Likelihood of systemic metastasis high at presentation Too late to prevent spread
88 Prognosis: Thick?
89 Survival (%) Prognosis: Thick? 100 >3.5mm (n=173) MSLT-I 1 75 Sentinel Node (-) 50 Sentinel Node (+) 25 Group # Event / N Estimated S(t) SE 5-Year 10-Year Log Rank: P= Node(-) Node(+) 36 / / Cox Multivar: RR % C.I. ( ) Time (Months)

90 False Negative SLN
91 False Negative SLN Ann Surg Oncol. 2016;23:
92 False Negative SLN Ann Surg Oncol. 2016;23:
93 False Negative SLN Ann Surg Oncol. 2016;23:
94 False Negative SLN Ann Surg Oncol. 2016;23:
95 False Negative SLN: Surgeon LITR Excluded Ann Surg Oncol. 2016;23:
96 False Negative SLN <4 mm >4 mm Ann Surg Oncol. 2016;23:

97 Smallest Metastases



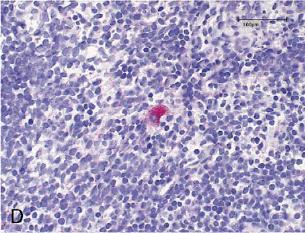
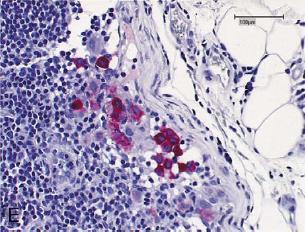
98 Isolated Tumor Cells Satzger, Am J Pathol 2007
99 Isolated Tumor Cells: Submicromets Too small to matter Ann Surg, 2008
100 Isolated Tumor Cells: Submicromets Too small to matter Ann Surg, 2008 Eur J Cancer, 2010


101 Isolated Tumor Cells: Submicromets Too small to matter Ann Surg, 2008 Eur J Cancer, 2010
102 Isolated Tumor Cells: Submicromets Unless it does matter
103 Isolated Tumor Cells: Submicromets Truly determining size may be a problem
104 Isolated Tumor Cells: Submicromets Truly determining size may be a problem
105 Isolated Tumor Cells: Submicromets Truly determining size may be a problem 20 patients with <0.1 mm SLN metastases
106 Isolated Tumor Cells: Submicromets Truly determining size may be a problem 20 patients with <0.1 mm SLN metastases Additional sections cut: upstaged in Max size: 8/20 Tumor penetrative depth: 8/20 Intranodal location: 6/20
107 Isolated Tumor Cells: Submicromets Truly determining size may be a problem 20 patients with <0.1 mm SLN metastases Additional sections cut: upstaged in Max size: 8/20 Tumor penetrative depth: 8/20 Intranodal location: 6/20
108 2009 AJCC TNM Staging System AJCC 6 th edition cut off N1 at 0.2mm
109 2009 AJCC TNM Staging System AJCC 6 th edition cut off N1 at 0.2mm AJCC 7 th edition: There is no lower threshold of tumor burden used to define the presence of regional nodal metastasis. Specifically, as a result of the consensus that volumes of regional metastatic tumor <0.2mm in diameter are clinically important, nodal tumor deposits of any size are to be included in staging nodal disease. An evidenced-based lower threshold of clinically insignificant nodal metastases has not been defined. Gershenwald et al, Ann Surg Oncol, 2010

110 Nodal Ultrasound

111 Pre-operative Morton Nodal ACS Ultrasound 111
 of patients avoided SLN biopsy due to US findings")

112 Pre-SLN Ultrasound 325 patients 6 (1.8%) of patients avoided SLN biopsy due to US findings Sensitivity 33.8% Specificity 85.7% 400 patients peripheral perfusion, loss of central echoes, balloon shape 82% sensitivity, PPV 52%
113 Morton ACS Pre-operative Nodal Ultrasound MSLT-II: Nodal Ultrasound Criteria Either 1 or 2 of the following: Length: Depth ration <2 Hypoechoic center Failure to identify nodal hilar vessel Focal rounded area of low level echoes with increased vascularity in that area
114 MSLT-II Screening Morton ACS Phase: 114 Baseline Nodal Ultrasound Screening Phase Ultrasound (US) n=2964 Baseline US+ n=109 (3.7%) Baseline US n=2855 (96.3%) Updated from: Thompson JF, et al Society of Surgical Oncology, 2011
115 MSLT-II Screening Morton ACS Phase: 115 Baseline Nodal Ultrasound Screening Phase Ultrasound (US) n=2964 Baseline US+ n=109 (3.7%) Baseline US n=2855 (96.3%) SLND Path+ n=49 SLND Path n=60 Updated from: Thompson JF, et al Society of Surgical Oncology, 2011
116 MSLT-II Screening Morton ACS Phase: 116 Baseline Nodal Ultrasound Screening Phase Ultrasound (US) n=2964 Baseline US+ n=109 (3.7%) Baseline US n=2855 (96.3%) SLND Path+ n=49 SLND Path n=60 SLND Path+ n=558 SLND Path n=2297 Updated from: Thompson JF, et al Society of Surgical Oncology, 2011
117 Pre-SLN Ultrasound Preoperative ultrasound assessment of sentinel nodes in melanoma patients does not provide reliable staging. Updated from: Thompson JF, et al Society of Surgical Oncology, 2011
118 Pre-SLN Ultrasound Preoperative ultrasound assessment of sentinel nodes in melanoma patients does not provide reliable staging. 49 (1.7%) True Positives (558 False Negative) Sensitivity was 8.1% Specificity 97.5% Updated from: Thompson JF, et al Society of Surgical Oncology, 2011
119 Pre-SLN Ultrasound Preoperative ultrasound assessment of sentinel nodes in melanoma patients does not provide reliable staging. 49 (1.7%) True Positives (558 False Negative) Sensitivity was 8.1% Specificity 97.5% Negative Predictive Value: 80.5% Median area for US detected metastases = 4.80mm 2 Median overall SLN metastasis area = <0.5mm 2 Updated from: Thompson JF, et al Society of Surgical Oncology, 2011
120 Pre-SLN Ultrasound Preoperative ultrasound assessment of sentinel nodes in melanoma patients does not provide reliable staging. 49 (1.7%) True Positives (558 False Negative) Sensitivity was 8.1% Specificity 97.5% Negative Predictive Value: 80.5% Median area for US detected metastases = 4.80mm 2 Median overall SLN metastasis area = <0.5mm 2 Sensitivity doubles (13% 23%) after first 100 cases Sensitivity and PPV increase with increasing tumor thickness SLN excision may be therapeutic (i.e. no need to proceed to CLND) Updated from: Thompson JF, et al Society of Surgical Oncology, 2011
121 Follow-up Ultrasound

122 Completion Node Dissection
123 MSLT-II: Is CLND necessary in SN(+) LN basins? 79-88% of patients have Negative NSN nodes in CLND specimen MSLT-I JWCI Cochran # SN(+) Stain CLND(+) n (%) H&E H&E IHC 22 (11.8%) 39 (12.1%) 19 (21.1%) NSN(-) % 88% 88% 79%
124 Survival Probability Disease Specific Survival Group 5-Year DSS SLN+ NSLN- 77.8% SLN+ NSLN+ 46.4% 0.6 SLN+ NSLN SLN+ NSLN+ 0 P< Disease Specific Survival (Months) Leung et al, PSCA, 2013

125 Survival Probability Disease Specific Survival Group 5-Year DSS SLN+ NSLN- 77.8% SLN+ NSLN+ 46.4% 0.6 SLN+ NSLN SLN+ NSLN+ 0 P< Disease Specific Survival (Months) Leung et al, PSCA, 2013
126 Equipoise: Advantages Potential removal of more cancer (10-20%) Complete Staging Information Clinical trial eligibility? Disadvantages Additional surgery Larger incision JP drain Potential complications: Lymphedema Disease may already be systemic Ultrasound may pick up any recurrence at an early time point
127 Is CLND necessary in SN(+) LN basins? p=0.07


128 Is CLND necessary in SN(+) LN basins? p=0.07
129 Is CLND necessary in SN(+) LN basins? RFS MSS Multivariable: HR 1.51, p=0.09
130 Regional recurrence CLND-HR 0.46, 95% CI , p=0.016 Age 65 y- HR 2.17, 95% CI , p=0.013
131 Melanoma-specific survival
132 Subgroup Analysis
133 Subgroup Analysis
134
135 DeCOG CLND Trial 1,258 patients melanoma and positive SLNB. ( ) 483 (39%) agreed to randomization (Missed accrual goals.) 241 patients underwent observation only 242 received CLND.
136 DeCOG CLND Trial 1,258 patients melanoma and positive SLNB. ( ) 483 (39%) agreed to randomization (Missed accrual goals.) 241 patients underwent observation only 242 received CLND. Mean follow-up: 34 months. Improved regional nodal recurrence
, DMFS (P= 0.76) MSS (P = 0.")
137 DeCOG CLND Trial 1,258 patients melanoma and positive SLNB. ( ) 483 (39%) agreed to randomization (Missed accrual goals.) 241 patients underwent observation only 242 received CLND. Mean follow-up: 34 months. Improved regional nodal recurrence No significant treatment-related difference in the 5-year RFS (P = 0.72), DMFS (P= 0.76) MSS (P = 0.86) In this early analysis of trial results, no survival benefit was achieved by CLND in melanoma patients with positive SLNB. A subsequent analysis three years after inclusion of the last patient is planned.
138
139 MSLT-II: Trial Design Melanoma >1.2 mm or > Clark IV, n=3500 Melanoma: + SLN (Outside Center) n=700
140 MSLT-II: Trial Design Melanoma >1.2 mm or > Clark IV, n=3500 LM/SL: standard and molecular assessment Melanoma: + SLN (Outside Center) n=700 -
141 MSLT-II: Trial Design Melanoma >1.2 mm or > Clark IV, n=3500 LM/SL: standard and molecular assessment Melanoma: + SLN (Outside Center) n=
142 MSLT-II: Trial Design Melanoma >1.2 mm or > Clark IV, n=3500 LM/SL: standard and molecular assessment Melanoma: + SLN (Outside Center) n= Observation
143 MSLT-II: Trial Design Melanoma >1.2 mm or > Clark IV, n=3500 LM/SL: standard and molecular assessment Melanoma: + SLN (Outside Center) n= Observation Randomization n=1926
144 MSLT-II: Trial Design Melanoma >1.2 mm or > Clark IV, n=3500 LM/SL: standard and molecular assessment Melanoma: + SLN (Outside Center) n= Observation Randomization n=1926 Stratification: MSLT-I Center Breslow Ulceration SLN H&E vs. PCR
145 MSLT-II: Trial Design Melanoma >1.2 mm or > Clark IV, n=3500 LM/SL: standard and molecular assessment Melanoma: + SLN (Outside Center) n= Observation Randomization n=1926 Stratification: MSLT-I Center Breslow Ulceration SLN H&E vs. PCR Immediate CLND Nodal Ultrasound
146 MSLT-II: Trial Design Melanoma >1.2 mm or > Clark IV, n=3500 LM/SL: standard and molecular assessment Melanoma: + SLN (Outside Center) n= Observation Randomization n=1926 Stratification: MSLT-I Center Breslow Ulceration SLN H&E vs. PCR Immediate CLND Nodal Ultrasound Observation
147 MSLT-II: Trial Design Melanoma >1.2 mm or > Clark IV, n=3500 LM/SL: standard and molecular assessment Melanoma: + SLN (Outside Center) n= Observation Randomization n=1926 Stratification: MSLT-I Center Breslow Ulceration SLN H&E vs. PCR Immediate CLND Nodal Ultrasound Recur No Recur Observation Delayed CLND Observation
148 MSLT-II Accrual: Complete

149 Thank You
Surgical Issues in Melanoma
 Surgical Issues in Melanoma Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Director, Surgical Oncology Training Program Professor of Surgery John Wayne Cancer Institute Surgical
Surgical Issues in Melanoma Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Director, Surgical Oncology Training Program Professor of Surgery John Wayne Cancer Institute Surgical
Update on SLN and Melanoma: DECOG and MSLT-II. Gordon H. Hafner, MD, FACS
 Update on SLN and Melanoma: DECOG and MSLT-II Gordon H. Hafner, MD, FACS No disclosures The surgery of malignant disease is not the surgery of organs, it is of the lymphatic system. Lord Moynihan Lymph
Update on SLN and Melanoma: DECOG and MSLT-II Gordon H. Hafner, MD, FACS No disclosures The surgery of malignant disease is not the surgery of organs, it is of the lymphatic system. Lord Moynihan Lymph
Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy
 American Academy of Dermatology 2018 Annual Meeting San Diego, CA, February 17, 2018 Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy Christopher Bichakjian,
American Academy of Dermatology 2018 Annual Meeting San Diego, CA, February 17, 2018 Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy Christopher Bichakjian,
Controversies and Questions in the Surgical Treatment of Melanoma
 Controversies and Questions in the Surgical Treatment of Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Division of Endocrine and Oncologic Surgery University of Pennsylvania School
Controversies and Questions in the Surgical Treatment of Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Division of Endocrine and Oncologic Surgery University of Pennsylvania School
Rebecca Vogel, PGY-4 March 5, 2012
 Rebecca Vogel, PGY-4 March 5, 2012 Historical Perspective Changes In The Staging System Studies That Started The Talk Where We Go From Here Cutaneous melanoma has become an increasingly growing problem,
Rebecca Vogel, PGY-4 March 5, 2012 Historical Perspective Changes In The Staging System Studies That Started The Talk Where We Go From Here Cutaneous melanoma has become an increasingly growing problem,
Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective
 Procedure: An Oncologic Surgeon s Perspective") Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective Giorgos C. Karakousis, M.D. Associate Professor of Surgery Hospital of the University of Pennsylvania Disclosures
Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective Giorgos C. Karakousis, M.D. Associate Professor of Surgery Hospital of the University of Pennsylvania Disclosures
Melanoma Surgery Update James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division
 Melanoma Surgery Update 2018 James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division Surgery for Melanoma Mainstay of treatment for potentially
Melanoma Surgery Update 2018 James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division Surgery for Melanoma Mainstay of treatment for potentially
Sentinel Node Alphabet Soup: MSLT-1, DeCOG-SLT, MSLT-2, UNC
 Sentinel Node Alphabet Soup: MSLT-1, DeCOG-SLT, MSLT-2, UNC David W. Ollila MD James and Jesse Millis Professor of Surgery University of North Carolina, Chapel Hill Disclosures: None July 15, 2018 AJCC
Sentinel Node Alphabet Soup: MSLT-1, DeCOG-SLT, MSLT-2, UNC David W. Ollila MD James and Jesse Millis Professor of Surgery University of North Carolina, Chapel Hill Disclosures: None July 15, 2018 AJCC
Topics for Discussion. Malignant Melanoma. Surgical Treatment. Current Treatment of Cutaneous Melanoma 5/17/2013. Lymph Regional nodes:
 Topics for Discussion What is a sentinel lymph node (SLN)? Utility of sentinel lymph biopsies: therapeutic or staging? Current Treatment of Cutaneous Melanoma Carlos Corvera, M.D. Associate Professor of
Topics for Discussion What is a sentinel lymph node (SLN)? Utility of sentinel lymph biopsies: therapeutic or staging? Current Treatment of Cutaneous Melanoma Carlos Corvera, M.D. Associate Professor of
No Benefit to Routine Completion Lymphadenectomy for Sentinel Lymph Node Positive Melanoma
 No Benefit to Routine Completion Lymphadenectomy for Sentinel Lymph Node Positive Melanoma Michael Lowe, MD Assistant Professor of Surgery Winship Cancer Institute Emory University School of Medicine July
No Benefit to Routine Completion Lymphadenectomy for Sentinel Lymph Node Positive Melanoma Michael Lowe, MD Assistant Professor of Surgery Winship Cancer Institute Emory University School of Medicine July
Sentinel Lymph Node Biopsies in Cutaneous Melanoma: A systematic review of the literature. Sasha Jenkins
 Sentinel Lymph Node Biopsies in Cutaneous Melanoma: A systematic review of the literature By Sasha Jenkins A Master s Paper submitted to the faculty of the University of North Carolina at Chapel Hill in
Sentinel Lymph Node Biopsies in Cutaneous Melanoma: A systematic review of the literature By Sasha Jenkins A Master s Paper submitted to the faculty of the University of North Carolina at Chapel Hill in
Molecular Enhancement of Sentinel Node Evaluation
 Cochran Illustrations 060104 Molecular Enhancement of Sentinel Node Evaluation Alistair Cochran, MD and Rong Huang MD Departments of Pathology and Laboratory Medicine and Surgery, David Geffen School of
Cochran Illustrations 060104 Molecular Enhancement of Sentinel Node Evaluation Alistair Cochran, MD and Rong Huang MD Departments of Pathology and Laboratory Medicine and Surgery, David Geffen School of
NEW SURGICAL APPROACHES TO MELANOMA THERAPY
 NEW SURGICAL APPROACHES TO MELANOMA THERAPY Melanoma 2003: New Insights Into Therapy & Treatment Douglas L. Fraker, M.D. University of Pennsylvania Surgical Treatment of Melanoma Primary resection margins
NEW SURGICAL APPROACHES TO MELANOMA THERAPY Melanoma 2003: New Insights Into Therapy & Treatment Douglas L. Fraker, M.D. University of Pennsylvania Surgical Treatment of Melanoma Primary resection margins
Cutaneous Melanoma: Epidemiology (USA) The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)
 The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)") The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
Disclosures. SLNB for Melanoma 25/02/2014 SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION
 8 th Canadian Melanoma Conference February 22, 2014 Rimrock Resort Hotel, Banff, Alberta SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION Christopher Bichakjian,
8 th Canadian Melanoma Conference February 22, 2014 Rimrock Resort Hotel, Banff, Alberta SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION Christopher Bichakjian,
Melanoma Quality Reporting
 Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
ORIGINAL ARTICLE PROGNOSTIC IMPLICATION OF SENTINEL LYMPH NODE BIOPSY IN CUTANEOUS HEAD AND NECK MELANOMA
 ORIGINAL ARTICLE PROGNOSTIC IMPLICATION OF SENTINEL LYMPH NODE BIOPSY IN CUTANEOUS HEAD AND NECK MELANOMA Benjamin E. Saltman, MD, 1 Ian Ganly, MD, 2 Snehal G. Patel, MD, 2 Daniel G. Coit, MD, 3 Mary Sue
ORIGINAL ARTICLE PROGNOSTIC IMPLICATION OF SENTINEL LYMPH NODE BIOPSY IN CUTANEOUS HEAD AND NECK MELANOMA Benjamin E. Saltman, MD, 1 Ian Ganly, MD, 2 Snehal G. Patel, MD, 2 Daniel G. Coit, MD, 3 Mary Sue
Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy
 Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy Dale Han, MD Assistant Professor Department of Surgery Section of Surgical Oncology No disclosures Background Desmoplastic melanoma (DM)
Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy Dale Han, MD Assistant Professor Department of Surgery Section of Surgical Oncology No disclosures Background Desmoplastic melanoma (DM)
Surgery for Melanoma and What s on the Horizon
 and What s on the Horizon Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Perelman School of Medicine at the University of Pennsylvania Background/Overview 76,870 cases of melanoma estimated
and What s on the Horizon Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Perelman School of Medicine at the University of Pennsylvania Background/Overview 76,870 cases of melanoma estimated
Sentinel Lymph Node Biopsy Is Valuable For All Cancer. Surgery Grand Rounds Debate October 6, 2008 Joel Baumgartner
 Sentinel Lymph Node Biopsy Is Valuable For All Cancer Surgery Grand Rounds Debate October 6, 2008 Joel Baumgartner History Lymphatics first described by Rasmus Bartholin in 1653 Rudolf Virchow postulated
Sentinel Lymph Node Biopsy Is Valuable For All Cancer Surgery Grand Rounds Debate October 6, 2008 Joel Baumgartner History Lymphatics first described by Rasmus Bartholin in 1653 Rudolf Virchow postulated
Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival
 MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
Radionuclide detection of sentinel lymph node
 Radionuclide detection of sentinel lymph node Sophia I. Koukouraki Assoc. Professor Department of Nuclear Medicine Medicine School, University of Crete 1 BACKGROUND The prognosis of malignant disease is
Radionuclide detection of sentinel lymph node Sophia I. Koukouraki Assoc. Professor Department of Nuclear Medicine Medicine School, University of Crete 1 BACKGROUND The prognosis of malignant disease is
AJCC 8 Implementation January 1, 2018 Melanoma of the Skin. Suraj Venna
 AJCC 8 Implementation January 1, 2018 Melanoma of the Skin Suraj Venna Personalized Medicine AJCC 8 th Edition This Time It s Personal Traditional AJCC (TNM) population-based analyses of large databases
AJCC 8 Implementation January 1, 2018 Melanoma of the Skin Suraj Venna Personalized Medicine AJCC 8 th Edition This Time It s Personal Traditional AJCC (TNM) population-based analyses of large databases
Precision Surgery for Melanoma
 Precision Surgery for Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Perelman School of Medicine at the University of Pennsylvania Background 87,110 cases of melanoma estimated in
Precision Surgery for Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Perelman School of Medicine at the University of Pennsylvania Background 87,110 cases of melanoma estimated in
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment. Justin Rivard MD, MSc, FRCSC September 21, 2018
 You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
Is There a Benefit to Sentinel Lymph Node Biopsy in Patients With T4 Melanoma?
 Is There a Benefit to Sentinel Lymph Node Biopsy in atients With T4 Melanoma? Csaba Gajdos, MD 1 ; Kent A. Griffith, MH, MS 2 ; Sandra L. Wong, MD 1 ; Timothy M. Johnson, MD 1,3 ; Alfred E. Chang, MD 1
Is There a Benefit to Sentinel Lymph Node Biopsy in atients With T4 Melanoma? Csaba Gajdos, MD 1 ; Kent A. Griffith, MH, MS 2 ; Sandra L. Wong, MD 1 ; Timothy M. Johnson, MD 1,3 ; Alfred E. Chang, MD 1
Michael T. Tetzlaff MD, PhD
 American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
Update on Lymph Node Management in Melanoma
 Update on Lymph Node Management in Melanoma John T. Vetto MD, FACS Professor of Surgery Division of Surgical Oncology Oregon Health & Science University Portland, Oregon Lymph Nodes in Melanoma Outline
Update on Lymph Node Management in Melanoma John T. Vetto MD, FACS Professor of Surgery Division of Surgical Oncology Oregon Health & Science University Portland, Oregon Lymph Nodes in Melanoma Outline
Talk to Your Doctor. Fact Sheet
 Talk to Your Doctor Hearing the words you have skin cancer is overwhelming and would leave anyone with a lot of questions. If you have been diagnosed with Stage I or II cutaneous melanoma with no apparent
Talk to Your Doctor Hearing the words you have skin cancer is overwhelming and would leave anyone with a lot of questions. If you have been diagnosed with Stage I or II cutaneous melanoma with no apparent
Clinical utilities and biological characteristics of melanoma sentinel lymph nodes
 W J C O World Journal of Clinical Oncology Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.5306/wjco.v7.i2.174 World J Clin Oncol 2016 April
W J C O World Journal of Clinical Oncology Submit a Manuscript: http://www.wjgnet.com/esps/ Help Desk: http://www.wjgnet.com/esps/helpdesk.aspx DOI: 10.5306/wjco.v7.i2.174 World J Clin Oncol 2016 April
The Role of Sentinel Lymph Node Biopsy and Axillary Dissection
 The Role of Sentinel Lymph Node Biopsy and Axillary Dissection Henry Mark Kuerer, MD, PhD, FACS Department of Surgical Oncology University of Texas MD Anderson Cancer Center SLN Biopsy Revolutionized surgical
The Role of Sentinel Lymph Node Biopsy and Axillary Dissection Henry Mark Kuerer, MD, PhD, FACS Department of Surgical Oncology University of Texas MD Anderson Cancer Center SLN Biopsy Revolutionized surgical
Thin Melanoma with Nodal Involvement: Analysis of Demographic, Pathologic, and Treatment Factors with Regard to Prognosis
 Ann Surg Oncol DOI 10.1245/s10434-016-5646-9 ORIGINAL ARTICLE MELANOMAS Thin Melanoma with Nodal Involvement: Analysis of Demographic, Pathologic, and Treatment Factors with Regard to Prognosis Giorgos
Ann Surg Oncol DOI 10.1245/s10434-016-5646-9 ORIGINAL ARTICLE MELANOMAS Thin Melanoma with Nodal Involvement: Analysis of Demographic, Pathologic, and Treatment Factors with Regard to Prognosis Giorgos
Morphological characteristics of the primary tumor and micrometastases in sentinel lymph nodes as a predictor of melanoma progression
 Morphological characteristics of the primary tumor and micrometastases in sentinel lymph nodes as a predictor of melanoma progression M.N. Kukushkina, S.I. Korovin, O.I. Solodyannikova, G.G. Sukach, A.Yu.
Morphological characteristics of the primary tumor and micrometastases in sentinel lymph nodes as a predictor of melanoma progression M.N. Kukushkina, S.I. Korovin, O.I. Solodyannikova, G.G. Sukach, A.Yu.
Epithelial Cancer- NMSC & Melanoma
 Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Melanoma. Kaushik Mukherjee MD A. Scott Pearson MD
 Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
PAPER. Prognostic Information From Sentinel Lymph Node Biopsy in Patients With Thick Melanoma
 PAPER Prognostic Information From Sentinel Lymph Node Biopsy in Patients With Thick Melanoma Charles R. Scoggins, MD, MBA; Adrianne L. Bowen, MD; Robert C. Martin II, MD, PhD; Michael J. Edwards, MD; Douglas
PAPER Prognostic Information From Sentinel Lymph Node Biopsy in Patients With Thick Melanoma Charles R. Scoggins, MD, MBA; Adrianne L. Bowen, MD; Robert C. Martin II, MD, PhD; Michael J. Edwards, MD; Douglas
Surgical Treatment of Melanoma Across the Disease Spectrum:
 AOCD Annual Fall Meeting October 28 th, 2017 New Orleans, Louisiana Surgical Treatment of Melanoma Across the Disease Spectrum: Standards of Care and Evolving Paradigms Merrick Ross, M.D. Professor of
AOCD Annual Fall Meeting October 28 th, 2017 New Orleans, Louisiana Surgical Treatment of Melanoma Across the Disease Spectrum: Standards of Care and Evolving Paradigms Merrick Ross, M.D. Professor of
Implications of ACOSOG Z11 for Clinical Practice: Surgical Perspective
 :$;7)#*8'-87*4BCD'E7)F'31$4.$&'G$H'E7)F&'GE'>??ID >?,"'@4,$)4*,#74*8'!74/)$++'74',"$'A.,.)$'7%'()$*+,'!*42$)!7)74*67&'!3 6 August 2011 Implications of ACOSOG Z11 for Clinical
:$;7)#*8'-87*4BCD'E7)F'31$4.$&'G$H'E7)F&'GE'>??ID >?,"'@4,$)4*,#74*8'!74/)$++'74',"$'A.,.)$'7%'()$*+,'!*42$)!7)74*67&'!3 6 August 2011 Implications of ACOSOG Z11 for Clinical
Why Do Axillary Dissection? Nodal Treatment and Survival NSABP B04. Revisiting Axillary Dissection for SN Positive Patients
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA Why Do Axillary Dissection? 6 August 2011 Implications
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA Why Do Axillary Dissection? 6 August 2011 Implications
Implications of ACOSOG Z11 for Clinical Practice: Surgical Perspective
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA 6 August 2011 Implications of ACOSOG Z11 for Clinical
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA 6 August 2011 Implications of ACOSOG Z11 for Clinical
Surgical Oncology Perspective of Melanoma
 Surgical Oncology Perspective of Melanoma Hans F. Schoellhammer, MD, FACS Assistant Clinical Professor Division of Surgical Oncology September 20, 2018 Nothing to disclose DISCLOSURE Discussion Objectives
Surgical Oncology Perspective of Melanoma Hans F. Schoellhammer, MD, FACS Assistant Clinical Professor Division of Surgical Oncology September 20, 2018 Nothing to disclose DISCLOSURE Discussion Objectives
1
 www.clinicaloncology.com.ua 1 Prognostic factors of appearing micrometastases in sentinel lymph nodes in skin melanoma M.N.Kukushkina, S.I.Korovin, O.I.Solodyannikova, G.G.Sukach, A.Yu.Palivets, A.N.Potorocha,
www.clinicaloncology.com.ua 1 Prognostic factors of appearing micrometastases in sentinel lymph nodes in skin melanoma M.N.Kukushkina, S.I.Korovin, O.I.Solodyannikova, G.G.Sukach, A.Yu.Palivets, A.N.Potorocha,
PAPER. Importance of Sentinel Lymph Node Biopsy in Patients With Thin Melanoma
 PAPER Importance of Sentinel Lymph Node Biopsy in Patients With Thin Melanoma Byron E. Wright, MD; Randall P. Scheri, MD; Xing Ye, MS; Mark B. Faries, MD; Roderick R. Turner, MD; Richard Essner, MD; Donald
PAPER Importance of Sentinel Lymph Node Biopsy in Patients With Thin Melanoma Byron E. Wright, MD; Randall P. Scheri, MD; Xing Ye, MS; Mark B. Faries, MD; Roderick R. Turner, MD; Richard Essner, MD; Donald
Protocol. This trial protocol has been provided by the authors to give readers additional information about their work.
 Protocol This trial protocol has been provided by the authors to give readers additional information about their work. Protocol for: Faries MB, Thompson JF, Cochran AJ, et al. Completion dissection or
Protocol This trial protocol has been provided by the authors to give readers additional information about their work. Protocol for: Faries MB, Thompson JF, Cochran AJ, et al. Completion dissection or
Tumor Mitotic Rate Added to the Equation: Melanoma Prognostic Factors Changed?
 Ann Surg Oncol (2015) 22:2978 2987 DOI 10.1245/s10434-014-4349-3 ORIGINAL ARTICLE MELANOMAS Tumor Mitotic Rate Added to the Equation: Melanoma Prognostic Factors Changed? A Single-Institution Database
Ann Surg Oncol (2015) 22:2978 2987 DOI 10.1245/s10434-014-4349-3 ORIGINAL ARTICLE MELANOMAS Tumor Mitotic Rate Added to the Equation: Melanoma Prognostic Factors Changed? A Single-Institution Database
Clinical Pathological Conference. Malignant Melanoma of the Vulva
 Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
University of Groningen
 University of Groningen Nodular Histologic Subtype and Ulceration are Tumor Factors Associated with High Risk of Recurrence in Sentinel Node-Negative Melanoma Patients Faut, Marloes; Wevers, Kevin; van
University of Groningen Nodular Histologic Subtype and Ulceration are Tumor Factors Associated with High Risk of Recurrence in Sentinel Node-Negative Melanoma Patients Faut, Marloes; Wevers, Kevin; van
Therapeutic Lymph Node Dissection in Melanoma: Different Prognosis for Different Macrometastasis Sites?
 Ann Surg Oncol (01) 19:91 91 DOI.14/s44-01-401- ORIGINAL ARTICLE MELANOMAS Therapeutic Lymph Node Dissection in Melanoma: Different Prognosis for Different Macrometastasis Sites? K. P. Wevers, MD, E. Bastiaannet,
Ann Surg Oncol (01) 19:91 91 DOI.14/s44-01-401- ORIGINAL ARTICLE MELANOMAS Therapeutic Lymph Node Dissection in Melanoma: Different Prognosis for Different Macrometastasis Sites? K. P. Wevers, MD, E. Bastiaannet,
Melanoma: Therapeutic Progress and the Improvements Continue
 Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Research Article Prediction of Sentinel Node Status and Clinical Outcome in a Melanoma Centre
 Skin Cancer Volume 2013, Article ID 904701, 7 pages http://dx.doi.org/10.1155/2013/904701 Research Article Prediction of Sentinel Node Status and Clinical Outcome in a Melanoma Centre Vera Teixeira, 1
Skin Cancer Volume 2013, Article ID 904701, 7 pages http://dx.doi.org/10.1155/2013/904701 Research Article Prediction of Sentinel Node Status and Clinical Outcome in a Melanoma Centre Vera Teixeira, 1
Impact of Prognostic Factors
 Melanoma Prognostic Factors: where we started, where are we going? Impact of Prognostic Factors Staging Management Surgical intervention Adjuvant treatment Suraj Venna, MD Assistant Clinical Professor,
Melanoma Prognostic Factors: where we started, where are we going? Impact of Prognostic Factors Staging Management Surgical intervention Adjuvant treatment Suraj Venna, MD Assistant Clinical Professor,
Results of the ACOSOG Z0011 Trial
 DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
Printed by Martina Huckova on 10/3/2011 3:04:54 PM. For personal use only. Not approved for distribution. Copyright 2011 National Comprehensive
 Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level
Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level
ORIGINAL ARTICLE. Clinical Node-Negative Thick Melanoma
 ORIGINAL ARTICLE Clinical Node-Negative Thick Melanoma George I. Salti, MD; Ashwin Kansagra, MD; Michael A. Warso, MD; Salve G. Ronan, MD ; Tapas K. Das Gupta, MD, PhD, DSc Background: Patients with T4
ORIGINAL ARTICLE Clinical Node-Negative Thick Melanoma George I. Salti, MD; Ashwin Kansagra, MD; Michael A. Warso, MD; Salve G. Ronan, MD ; Tapas K. Das Gupta, MD, PhD, DSc Background: Patients with T4
M D..,., M. M P.. P H., H, F. F A.. A C..S..
 Implications of NSABP B-32 and Loco-Regional Therapy Considerations After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H, F.A.C.S. Professor of Surgery Northeastern Ohio Medical University Medical
Implications of NSABP B-32 and Loco-Regional Therapy Considerations After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H, F.A.C.S. Professor of Surgery Northeastern Ohio Medical University Medical
Sentinel Lymph Node Biopsy: Past and Present Implications for the Management of Cutaneous Melanoma with Nodal Metastasis
 American Journal of Clinical Dermatology (2018) 19 (Suppl 1):S24 S30 https://doi.org/10.1007/s40257-018-0379-0 REVIEW ARTICLE Sentinel Lymph Node Biopsy: Past and Present Implications for the Management
American Journal of Clinical Dermatology (2018) 19 (Suppl 1):S24 S30 https://doi.org/10.1007/s40257-018-0379-0 REVIEW ARTICLE Sentinel Lymph Node Biopsy: Past and Present Implications for the Management
Results, morbidity, and quality of life of melanoma patients undergoing sentinel lymph node staging Vries, Mattijs de
 University of Groningen Results, morbidity, and quality of life of melanoma patients undergoing sentinel lymph node staging Vries, Mattijs de IMPORTANT NOTE: You are advised to consult the publisher's
University of Groningen Results, morbidity, and quality of life of melanoma patients undergoing sentinel lymph node staging Vries, Mattijs de IMPORTANT NOTE: You are advised to consult the publisher's
SLN Mapping in Cervical Cancer. Memorial Sloan Kettering Cancer Center New York, USA
 Lead Grou p Log SLN Mapping in Cervical Cancer Nadeem R. Abu-Rustum, M.D. Memorial Sloan Kettering Cancer Center New York, USA Conflict of Interest Disclosure Nadeem R. Abu-Rustum, M.D. I have no financial
Lead Grou p Log SLN Mapping in Cervical Cancer Nadeem R. Abu-Rustum, M.D. Memorial Sloan Kettering Cancer Center New York, USA Conflict of Interest Disclosure Nadeem R. Abu-Rustum, M.D. I have no financial
6/22/2015. Original Paradigm. Correlating Histology and Molecular Findings in Melanocytic Neoplasms
 6 Correlating Histology and Molecular Findings in Melanocytic Neoplasms Pedram Gerami MD, Associate Professor of Dermatology and Pediatrics at Northwestern University Disclosures: I have been a consultant
6 Correlating Histology and Molecular Findings in Melanocytic Neoplasms Pedram Gerami MD, Associate Professor of Dermatology and Pediatrics at Northwestern University Disclosures: I have been a consultant
Technical Considerations. Imaging Considerations
 354 CUTANEOUS MALIGNANCY OF THE HEAD AND NECK desmoplastic melanomas are characterized by a uniform desmoplasia that is prominent throughout the entire tumor (termed pure desmoplastic melanoma), whereas
354 CUTANEOUS MALIGNANCY OF THE HEAD AND NECK desmoplastic melanomas are characterized by a uniform desmoplasia that is prominent throughout the entire tumor (termed pure desmoplastic melanoma), whereas
Sentinel Lymph Node Biopsy for Head and Neck Cutaneous Melanoma
 Sentinel Lymph Node Biopsy for Head and Neck Cutaneous Melanoma S. Ross Patton, MD - PGY III Faculty Mentor: Susan McCammon, MD The University of Texas Medical Branch (UTMB Health) Department of Otolaryngology
Sentinel Lymph Node Biopsy for Head and Neck Cutaneous Melanoma S. Ross Patton, MD - PGY III Faculty Mentor: Susan McCammon, MD The University of Texas Medical Branch (UTMB Health) Department of Otolaryngology
When Do I Consider Myself Cured?
 The Melanoma Patient Symposium - Science to Survivorship When Do I Consider Myself Cured? 26 September 2009 Jeffrey E. Gershenwald, MD, FACS Professor of Surgery, Dept. of Surgical Oncology Professor,
The Melanoma Patient Symposium - Science to Survivorship When Do I Consider Myself Cured? 26 September 2009 Jeffrey E. Gershenwald, MD, FACS Professor of Surgery, Dept. of Surgical Oncology Professor,
Increasing Age Is Associated with Worse Prognostic Factors and Increased Distant Recurrences despite Fewer Sentinel Lymph Node Positives in Melanoma
 Increasing Age Is Associated with Worse Prognostic Factors and Increased Distant Recurrences despite Fewer Sentinel Lymph Node Positives in Melanoma A. J. Page, Emory University A. Li, Emory University
Increasing Age Is Associated with Worse Prognostic Factors and Increased Distant Recurrences despite Fewer Sentinel Lymph Node Positives in Melanoma A. J. Page, Emory University A. Li, Emory University
COMPARATIVE ANALYSIS OF COLON AND RECTAL CANCERS IN SENTINEL LYMPH NODE MAPPING
 Trakia Journal of Sciences, Vol. 5, No. 1, pp 10-14, 2007 Copyright 2007 Trakia University Available online at: http://www.uni-sz.bg ISSN 1312-1723 Original Contribution COMPARATIVE ANALYSIS OF COLON AND
Trakia Journal of Sciences, Vol. 5, No. 1, pp 10-14, 2007 Copyright 2007 Trakia University Available online at: http://www.uni-sz.bg ISSN 1312-1723 Original Contribution COMPARATIVE ANALYSIS OF COLON AND
Prognosis of Sentinel Node Staged Patients with Primary Cutaneous Melanoma
 Prognosis of Sentinel Node Staged Patients with Primary Cutaneous Melanoma Otmar Elsaeßer 1., Ulrike Leiter 1 *., Petra G. Buettner 2, Thomas K. Eigentler 1, Friedegund Meier 1, Benjamin Weide 1, Gisela
Prognosis of Sentinel Node Staged Patients with Primary Cutaneous Melanoma Otmar Elsaeßer 1., Ulrike Leiter 1 *., Petra G. Buettner 2, Thomas K. Eigentler 1, Friedegund Meier 1, Benjamin Weide 1, Gisela
Melanoma Underwriting Presented at 2018 AHOU Conference. Hank George FALU
 Melanoma Underwriting Presented at 2018 AHOU Conference Hank George FALU MELANOMA EPIDEMIOLOGY 70-80,000 American cases annually Majority are in situ or thin > 20% are diagnosed age 45 8-9,000 melanoma
Melanoma Underwriting Presented at 2018 AHOU Conference Hank George FALU MELANOMA EPIDEMIOLOGY 70-80,000 American cases annually Majority are in situ or thin > 20% are diagnosed age 45 8-9,000 melanoma
Melanoma Sentinel Lymph Node Biopsy- Is it the Gold Standard? Paul K. Shitabata, M.D. Dermatopathologist Pathology Inc.
 Melanoma Sentinel Lymph Node Biopsy- Is it the Gold Standard? Paul K. Shitabata, M.D. Dermatopathologist Pathology Inc. Technical details of intraoperative lymphatic mapping for early stage melanoma
Melanoma Sentinel Lymph Node Biopsy- Is it the Gold Standard? Paul K. Shitabata, M.D. Dermatopathologist Pathology Inc. Technical details of intraoperative lymphatic mapping for early stage melanoma
SENTINEL LYMPH node (SLN) biopsy has become
 biopsy has become") COMMENTARY Sentinel Lymph Node Biopsy for Melanoma: Controversy Despite Widespread Agreement By Kelly M. McMasters, Douglas S. Reintgen, Merrick I. Ross, Jeffrey E. Gershenwald, Michael J. Edwards, Arthur
COMMENTARY Sentinel Lymph Node Biopsy for Melanoma: Controversy Despite Widespread Agreement By Kelly M. McMasters, Douglas S. Reintgen, Merrick I. Ross, Jeffrey E. Gershenwald, Michael J. Edwards, Arthur
Management of the patient with Lymph Node Involvement. Michael A Henderson Peter MacCallum Cancer Center Univ of Melbourne
 Management of the patient with Lymph Node Involvement Michael A Henderson Peter MacCallum Cancer Center Univ of Melbourne Lymph Node Field Recurrence Most important prognostic factor for early stage melanoma
Management of the patient with Lymph Node Involvement Michael A Henderson Peter MacCallum Cancer Center Univ of Melbourne Lymph Node Field Recurrence Most important prognostic factor for early stage melanoma
Sentinel Lymph Node Biopsy: Current Evidence for its Role in Managing Melanoma
 Sentinel Lymph Node Biopsy: Current Evidence for its Role in Managing Melanoma John A Zitelli MD Adjunct Clinical Associate Professor Dermatology, Otolaryngology, Plastic Surgery University of Pittsburgh
Sentinel Lymph Node Biopsy: Current Evidence for its Role in Managing Melanoma John A Zitelli MD Adjunct Clinical Associate Professor Dermatology, Otolaryngology, Plastic Surgery University of Pittsburgh
Sentinel Lymph Node Biopsy in Other Tumours: Sentinel Lymph Node Biopsy in Other Tumours. Methodology. Results. Key Questions to Consider
 Sentinel Lymph Node Biopsy in Other Tumours Dr. Rona Cheifetz Surgical Oncology Update November 24, 2006 Sentinel Lymph Node Biopsy in Other Tumours: An Operation Looking for an Application Dr. Rona Cheifetz
Sentinel Lymph Node Biopsy in Other Tumours Dr. Rona Cheifetz Surgical Oncology Update November 24, 2006 Sentinel Lymph Node Biopsy in Other Tumours: An Operation Looking for an Application Dr. Rona Cheifetz
MELANOMA LETTER. Surgical Treatment of Primary Melanoma: Where Do We Stand After MSLT-II? THE. From the Editors MSLT-II. SkinCancer.
 THE MELANOMA LETTER A PUBLICATION OF THE SKIN CANCER FOUNDATION DEBORAH S. SARNOFF, MD, President WINTER 2017, Vol. 35 DAN LATORE, Executive Director Surgical Treatment of Primary Melanoma: Where Do We
THE MELANOMA LETTER A PUBLICATION OF THE SKIN CANCER FOUNDATION DEBORAH S. SARNOFF, MD, President WINTER 2017, Vol. 35 DAN LATORE, Executive Director Surgical Treatment of Primary Melanoma: Where Do We
Work-up/Follow-up: Baseline and Surveillance Studies for Cutaneous Melanoma Patients
 2018 AAD Annual Meeting, San Diego, CA Work-up/Follow-up: Baseline and Surveillance Studies for Cutaneous Melanoma Patients Susan M. Swetter, MD, FAAD Professor of Dermatology Director, Pigmented Lesion
2018 AAD Annual Meeting, San Diego, CA Work-up/Follow-up: Baseline and Surveillance Studies for Cutaneous Melanoma Patients Susan M. Swetter, MD, FAAD Professor of Dermatology Director, Pigmented Lesion
16/09/2015. ACOSOG Z011 changing practice. Presentation outline. Nodal mets #1 prognostic tool. Less surgery no change in oncologic outcomes
 ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
Who is the Ideal Candidate for PEG Intron?
 Who is the Ideal Candidate for PEG Intron? Sanjiv S. Agarwala, MD Chief, Oncology & Hematology St. Luke s Cancer Center Professor, Temple University School of Medicine Philadelphia, PA, USA Overview Introduction
Who is the Ideal Candidate for PEG Intron? Sanjiv S. Agarwala, MD Chief, Oncology & Hematology St. Luke s Cancer Center Professor, Temple University School of Medicine Philadelphia, PA, USA Overview Introduction
Predictive Factors for the Positivity of the Sentinel Lymph Node in Malignant Melanoma
 ORIGINAL RESEARCH SURGERY // ANATOMO-PATHOLOGY Predictive Factors for the Positivity of the Sentinel Lymph Node in Malignant Melanoma Călin Crăciun, Orsolya Hankó- Bauer, Zalán Benedek, Sorin Sorlea, Marius
ORIGINAL RESEARCH SURGERY // ANATOMO-PATHOLOGY Predictive Factors for the Positivity of the Sentinel Lymph Node in Malignant Melanoma Călin Crăciun, Orsolya Hankó- Bauer, Zalán Benedek, Sorin Sorlea, Marius
An estimated 76,690 patients will be diagnosed with invasive
 SONDAK ET AL Evidence-Based Clinical Practice Guidelines on the Use of Sentinel Lymph Node Biopsy in Melanoma Vernon K. Sondak, MD, Sandra L. Wong, MD, Jeffrey E. Gershenwald, MD, and John F. Thompson,
SONDAK ET AL Evidence-Based Clinical Practice Guidelines on the Use of Sentinel Lymph Node Biopsy in Melanoma Vernon K. Sondak, MD, Sandra L. Wong, MD, Jeffrey E. Gershenwald, MD, and John F. Thompson,
Clinical Case Conference Melanoma
 Clinical Case Conference Melanoma Epidemiology ~60,000 cases and 8,000 deaths per year in US Caucasian:African American = 10:1 15% arise from existing nevi 91% are cutaneous 15% are LN+ at presentation
Clinical Case Conference Melanoma Epidemiology ~60,000 cases and 8,000 deaths per year in US Caucasian:African American = 10:1 15% arise from existing nevi 91% are cutaneous 15% are LN+ at presentation
ORIGINAL ARTICLE. Predictors of Occult Nodal Metastasis in Patients With Thin Melanoma
 ORIGINAL ARTICLE Predictors of Occult Nodal Metastasis in Patients With Thin Melanoma Mark B. Faries, MD; Leslie A. Wanek, PhD; David Elashoff, PhD; Byron E. Wright, MD; Donald L. Morton, MD Hypothesis:
ORIGINAL ARTICLE Predictors of Occult Nodal Metastasis in Patients With Thin Melanoma Mark B. Faries, MD; Leslie A. Wanek, PhD; David Elashoff, PhD; Byron E. Wright, MD; Donald L. Morton, MD Hypothesis:
47. Melanoma of the Skin
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Sentinel Node Localisation of Melanoma
 Sentinel Node Localisation of Melanoma V Bongers, Diakonessenhuis, Utrecht 1. Introduction A melanoma is mostly a malignancy of the skin. The sentinel lymph node (SLN) concept of sequential progression
Sentinel Node Localisation of Melanoma V Bongers, Diakonessenhuis, Utrecht 1. Introduction A melanoma is mostly a malignancy of the skin. The sentinel lymph node (SLN) concept of sequential progression
Canadian Scientific Journal. Intraoperative color detection of lymph nodes metastases in thyroid cancer
 Canadian Scientific Journal 2 (2014) Contents lists available at Canadian Scientific Journal Canadian Scientific Journal journal homepage: Intraoperative color detection of lymph nodes metastases in thyroid
Canadian Scientific Journal 2 (2014) Contents lists available at Canadian Scientific Journal Canadian Scientific Journal journal homepage: Intraoperative color detection of lymph nodes metastases in thyroid
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Measure #264: Sentinel Lymph Node Biopsy for Invasive Breast Cancer National Quality Strategy Domain: Effective Clinical Care
 Measure #264: Sentinel Lymph Node Biopsy for Invasive Breast Cancer National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY DESCRIPTION: The percentage
Measure #264: Sentinel Lymph Node Biopsy for Invasive Breast Cancer National Quality Strategy Domain: Effective Clinical Care 2016 PQRS OPTIONS FOR INDIVIDUAL MEASURES: REGISTRY ONLY DESCRIPTION: The percentage
Evaluation of the Axilla Post Z-0011 Trial New Paradigm
 Evaluation of the Axilla Post Z-0011 Trial New Paradigm Belinda Curpen, MD, FRCPC; Tetyana Dushenkovska; Mia Skarpathiotakis MD, FRCPC; Carrie Betel, MD, FRCPC; Kalesha Hack, MD, FRCPC; Lara Richmond,
Evaluation of the Axilla Post Z-0011 Trial New Paradigm Belinda Curpen, MD, FRCPC; Tetyana Dushenkovska; Mia Skarpathiotakis MD, FRCPC; Carrie Betel, MD, FRCPC; Kalesha Hack, MD, FRCPC; Lara Richmond,
Advances in Surgical Management of Primary Melanoma: Identifying Patients Who Need More than Conventional Wide Local Excision
 Advances in Surgical Management of Primary Melanoma: Identifying Patients Who Need More than Conventional Wide Local Excision Christopher J. Miller, MD Director of Penn Dermatology Oncology Center Associate
Advances in Surgical Management of Primary Melanoma: Identifying Patients Who Need More than Conventional Wide Local Excision Christopher J. Miller, MD Director of Penn Dermatology Oncology Center Associate
Update on Sentinel Node Biopsy in Endometrial Cancer: Feasibility, Technique, Impact
 Update on Sentinel Node Biopsy in Endometrial Cancer: Feasibility, Technique, Impact Bjørn Hagen, MD, PhD St Olavs Hospital Trondheim University Hospital Trondheim, Norway Endometrial Cancer (EC) The most
Update on Sentinel Node Biopsy in Endometrial Cancer: Feasibility, Technique, Impact Bjørn Hagen, MD, PhD St Olavs Hospital Trondheim University Hospital Trondheim, Norway Endometrial Cancer (EC) The most
What are the new AJCC Staging System changes, and how will they affect my patients?
 What are the new AJCC Staging System changes, and how will they affect my patients? Emily Y. Chu, M.D., Ph.D. Assistant Professor of Dermatology & Pathology and Laboratory Medicine University of Pennsylvania
What are the new AJCC Staging System changes, and how will they affect my patients? Emily Y. Chu, M.D., Ph.D. Assistant Professor of Dermatology & Pathology and Laboratory Medicine University of Pennsylvania
Recurrence of cutaneous melanoma of the head and neck after negative sentinel lymph node biopsy
 ORIGINAL ARTICLE Recurrence of cutaneous melanoma of the head and neck after negative sentinel lymph node biopsy Melinda V. Davis Malesevich, MD, 1 Ryan Goepfert, MD, 2 Mark Kubik, MD, 1 Dianna B. Roberts,
ORIGINAL ARTICLE Recurrence of cutaneous melanoma of the head and neck after negative sentinel lymph node biopsy Melinda V. Davis Malesevich, MD, 1 Ryan Goepfert, MD, 2 Mark Kubik, MD, 1 Dianna B. Roberts,
Sentinel Lymph Node Biopsy for Melanoma: Indications and Rationale
 Sentinel lymph node biopsy is recommended for most patients with melanomas 0.76 mm and for all good surgical candidates with melanomas 1.0 mm. Catherine Hickson. Figs in Alizarin Crimson. Oil on Belgian
Sentinel lymph node biopsy is recommended for most patients with melanomas 0.76 mm and for all good surgical candidates with melanomas 1.0 mm. Catherine Hickson. Figs in Alizarin Crimson. Oil on Belgian
Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma. Michael T. Tetzlaff MD, PhD
 Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational and Molecular Pathology
Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational and Molecular Pathology
Nodal staging in localized melanoma. The experience of the Brescia Melanoma Unit
 The British Association of Plastic Surgeons (2003) 56, 534 539 Nodal staging in localized melanoma. The experience of the Brescia Melanoma Unit Giorgio Manca a, *, Fabio Facchetti b, Claudio Pizzocaro
The British Association of Plastic Surgeons (2003) 56, 534 539 Nodal staging in localized melanoma. The experience of the Brescia Melanoma Unit Giorgio Manca a, *, Fabio Facchetti b, Claudio Pizzocaro
ORIGINAL ARTICLE MELANOMAS. Ann Surg Oncol (2015) 22: DOI /s z
 22: DOI /s z") Ann Surg Oncol (2015) 22:2972 2977 DOI 10.1245/s10434-015-4615-z ORIGINAL ARTICLE MELANOMAS Detailed Pathological Examination of Completion Node Dissection Specimens and Outcome in Melanoma Patients with
Ann Surg Oncol (2015) 22:2972 2977 DOI 10.1245/s10434-015-4615-z ORIGINAL ARTICLE MELANOMAS Detailed Pathological Examination of Completion Node Dissection Specimens and Outcome in Melanoma Patients with
PAPER. Is Completion Lymphadenectomy After a Positive Sentinel Lymph Node Biopsy for Cutaneous Melanoma Always Necessary?
 PAPER Is Completion Lymphadenectomy After a Positive Sentinel Lymph Node Biopsy for Cutaneous Melanoma Always Necessary? Nahel Elias, MD; Kenneth K. Tanabe, MD; Arthur J. Sober, MD; Michele A. Gadd, MD;
PAPER Is Completion Lymphadenectomy After a Positive Sentinel Lymph Node Biopsy for Cutaneous Melanoma Always Necessary? Nahel Elias, MD; Kenneth K. Tanabe, MD; Arthur J. Sober, MD; Michele A. Gadd, MD;
Management of the Axilla at Initial Surgery Manejo da Axila em Cirurgia Inicial
 DISCIPLINA DE MASTOLOGIA ESCOLA PAULISTA DE MEDICINA UNIVERSIDADE FEDERAL DE SÃO PAULO Management of the Axilla at Initial Surgery Manejo da Axila em Cirurgia Inicial Disciplina de Mastologia Prof. Dr.
DISCIPLINA DE MASTOLOGIA ESCOLA PAULISTA DE MEDICINA UNIVERSIDADE FEDERAL DE SÃO PAULO Management of the Axilla at Initial Surgery Manejo da Axila em Cirurgia Inicial Disciplina de Mastologia Prof. Dr.
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD
 Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
Occurrence of Lymphedema Following Sentinel Node Biopsy (SNB) for Lower Extremity Melanoma
 for Lower Extremity Melanoma") Original Article Elmer Press Occurrence of Lymphedema Following Sentinel Node Biopsy (SNB) for Lower Extremity Melanoma Patrick D. Magoon a, Roger A. Graham b, d, Janice G. Rothschild b, Yoojin Lee c Abstract
Original Article Elmer Press Occurrence of Lymphedema Following Sentinel Node Biopsy (SNB) for Lower Extremity Melanoma Patrick D. Magoon a, Roger A. Graham b, d, Janice G. Rothschild b, Yoojin Lee c Abstract
LYMPHATIC DRAINAGE PATTERNS OF HEAD AND NECK CUTANEOUS MELANOMA OBSERVED ON LYMPHOSCINTIGRAPHY AND SENTINEL LYMPH NODE BIOPSY
 LYMPHATIC DRAINAGE PATTERNS OF HEAD AND NECK CUTANEOUS MELANOMA OBSERVED ON LYMPHOSCINTIGRAPHY AND SENTINEL LYMPH NODE BIOPSY Doris Lin, MD, 1 Benjamin L. Franc, MD, 2 Mohammed Kashani-Sabet, MD, 3 Mark
LYMPHATIC DRAINAGE PATTERNS OF HEAD AND NECK CUTANEOUS MELANOMA OBSERVED ON LYMPHOSCINTIGRAPHY AND SENTINEL LYMPH NODE BIOPSY Doris Lin, MD, 1 Benjamin L. Franc, MD, 2 Mohammed Kashani-Sabet, MD, 3 Mark
Proposed All Wales Vulval Cancer Guidelines. Dr Amanda Tristram
 Proposed All Wales Vulval Cancer Guidelines Dr Amanda Tristram Previous FIGO staging FIGO Stage Features TNM Ia Lesion confined to vulva with
Proposed All Wales Vulval Cancer Guidelines Dr Amanda Tristram Previous FIGO staging FIGO Stage Features TNM Ia Lesion confined to vulva with
Sentinel Lymph Node Biopsy for Breast Cancer
 Sentinel Lymph Node Biopsy for Breast Cancer Registrar Tutorial Adam Cichowitz Surgical Registrar The Royal Melbourne Hospital Sentinel Lymph Node Biopsy Axillary LN status important prognostic factor
Sentinel Lymph Node Biopsy for Breast Cancer Registrar Tutorial Adam Cichowitz Surgical Registrar The Royal Melbourne Hospital Sentinel Lymph Node Biopsy Axillary LN status important prognostic factor