Surgical Treatment of Melanoma Across the Disease Spectrum:
|
|
|
- Kerry Cannon
- 5 years ago
- Views:
Transcription
1 AOCD Annual Fall Meeting October 28 th, 2017 New Orleans, Louisiana Surgical Treatment of Melanoma Across the Disease Spectrum: Standards of Care and Evolving Paradigms Merrick Ross, M.D. Professor of Surgical Oncology M.D. Anderson Cancer Center
2 Surgical Treatment of Melanoma Across the Stage I and II - SLN biopsy Disease Spectrum Topics Stage III - completion dissection? - neo-adjuvant strategies for advanced nodal disease Stage IV - metastasectomy in the new melanoma landscape
3 The New Melanoma Landscape Recently approved systemic therapies for Stage IV - B-Raf mutant: Vemurafenib, dabrafenib, trametinib, dabrafenid / trametinib - Ipilimumab, anti-pd-1, (combination of anti- CTLA4 / anti-pd-1) Survival rates of resected Stage IV disease Novel intralesional agents (oncolytic immunotherapy) Integration of Sentinel Lymph s Node (SLN) biopsy - the new Stage I / II disease - the new Stage III disease

4 Stage I and II Primary Melanoma Components of Treatment 1. Wide excision - margins appropriate for thickness - reconstruction 2. Sentinel Node Biopsy - indications - technique
5 Lymph Node Involvement and Melanoma Regional nodes, most common site of first recurrence after wide excision of primary melanoma - 15%-50% chance for in-basin failure after dissection - > 50% chance for distant relapse


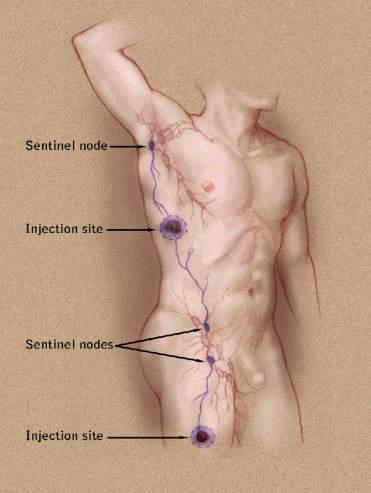


6 Sentinel Lymph Node Biopsy
7 Sentinel Node Biopsy Goals Minimally invasive approach to nodal staging Improve the disease outcome for the node positive patients - survival - regional control Prevent the development of clinical nodal involvement
8 Regional Control?
9 Risk Factors for Regional Recurrence After Surgery Alone Reference Regional Failure Rate Fuhrmann, % Kretschmer, % Lee, % Shen, % Hughes, % Monsour, % Miller, % O Brien, % Calabro, % Bowsher, % Byers, % Weighted average: 692 failures / 3350 patients = 21%
10 Risk Factors for Regional Recurrence After Surgery Alone Characteristic Extracapsular extension Regional Failure Rate 31% - 63% References Lee, Calabro, Shen, Monsour 4 involved lymph nodes 22% - 63% Lee, Calabro, Miller, Kretschmer Lymph node 3 cm 42% - 80% Lee Cervical lymph node location 33% - 50% Lee, Bowsher, Monsour 30% 50% if high-risk features present
11 In-Basin Failure Selective Lymphadenectomy vs ELND (Node Positive Only) % Nodal Failure ELND Slingluff, 1997 SLN MDACC Study, 2003

12 Does early treatment of lymph node disease improve survival? Microscopic Macroscopic

13 MSLT I: Trial Design Melanoma >1 mm or > Clark IV Randomization DSS: Primary Endpoint DFS: Secondary Endpoint Wide excision alone 40% 60% Wide excision + SLN SLN + SLN - CLND for Recurrence Occult Stage III Immediate CLND No recurrence: observation Observation
")


14 Survival (%) Morton Melanoma A 50 Year Odyssey Specific 14 Survival Node+ Final Dataset (intent to treat) 100 Group # Event / Estimate S(t) ± SE % Total N 5-year 10-year OBS, had nodal recur. 48/ ± ± 5.6 SNB+ 70 / ± ± SNB HR: % C.I. ( ) Log Rank P=0.006 OBS Time (years)
15 Unraveling Heterogeneity of Stage I/II Melanoma 5-Year Survival Rate by T-Classification System The new stage I / II 7th Edition T-category 6 th Edition SLN Subset* T1a Ia 95 ± ± 1.1 Ib T1b 91 ± ± 1.5 T2a 89 ± ± 0.6 IIa T2b 77 ± ± 2.0 T3a 79 ± ± 1.5 IIb T3b 63 ± ± 2.5 T4a 67 ± ± 3.6 IIc AJCC T4b ± 1.9 *Stage-appropriate 67 ± 3.6 use of SLN biopsy
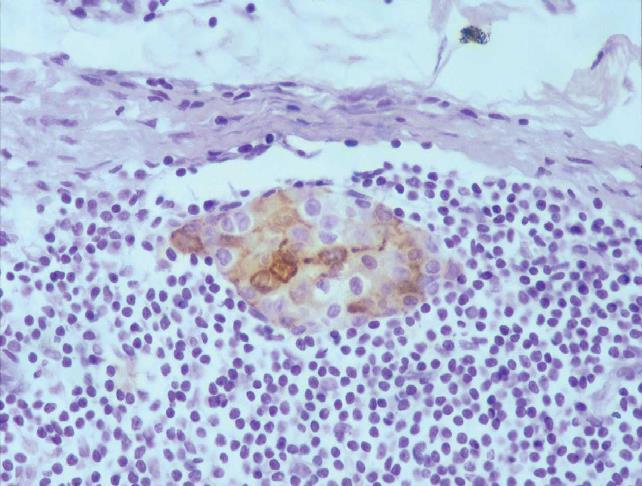
16 SLN Biopsy Multi-Disciplinary Components Pre-operative lymphoscintigraphy - accurate technique - accurate reading - surgeon to look at images Surgical approach - injection of radio-colloid and blue dye - removal of all SLN s - images in the room Pathological evaluation - serial sections and immuno-stains

17 Constellation of Node Positive Disease New Stage IIII
18 AJCC Stage III 5-Year Survival by Tumor Burden, # of Nodes, and Primary Tumor Ulceration Ulceration Patients with Nodal Metastases (Stage III) No. of Nodal Micrometastases (+/- SE) No. of Nodal Macrometastases (+/- SE) Absent 81.5± ± ± ± ± ±9. 1 (777) (246) (46) (75) (67) (50) Present 56.6± ± ± ± ± ±6.7 (531) (223) (49) (88) (93) (68) Balch, Gershenwald, Soong et al., J Clin Oncol, May 2010


19 7 th ed. AJCC Database - Regional LN Paradigm Shift Macroscopic 19% N=560 N=2334 Microscopic 81%
20 Incidence of Positive SLN: AJCC Stage Grouping Percent Positive SLN Ia Ib IIa IIb IIc Consensus Threshold: 5%-8% AJCC Stage
21
22 Rationale for CLND Probability of + NSLN (Staging) Improved regional control Improved survival Less morbidity
23 Only patients with nonsentinel lymph node involvement can derive benefit from CLND
24 10%-20% have additional nodes involved by routine histology A selective approach to completion dissection is rational! Assessment of risk for non-sentinel node metastases
25 CLND for melanoma Completion LND - positive NSLN The strong independent prognostic significance of a positive NSLN has been confirmed by four separate studies. Author Year # + NSLN HR P Ghaferi <0.01 Weiner Brown <0.001 Pasquali <0.001 CLND is a great (though very expensive and morbid) staging tool.
26 CLND for melanoma Completion LND - positive NSLN All patients Two nodes positive only Ariyan C, Ann Surg Oncol 2009; 16(1):186
27 CLND for melanoma Clinical equipoise: Prevailing practice A review of the NCDB identified 2942 melanoma patients with a positive sentinel node treated Only half of these patients went on to completion lymph node dissection. Predictors of CLND included treatment at an NCI designated cancer center, non lower extremity primary tumors, and age < 75. Bilmoria K, Ann Surg Oncol 2008; 15(6):1566
28 What is the fractional benefit of the CLND above what is achieved by just removing the involved SLN(s)?
29 Patients with MM 1mm (n=4650) SLNB SLNB positive (n=930) SLNB negative (n= 3720) Exclusion criteria Patients refusal Randomization (n=558) Follow-up Arm A: Observation* (n=279) Radical Lymphadenectomy and Follow-up* (n=279) German Trial Design (DeCOG-SLT)
30 Melanoma - specific survival Arm A: 84.3% (78.8%; 89.8%) Arm B: 82.7% (76.6%; 88.8%) HR (Arm B vs. Arm A) 1.01 (0.64; 1.59) p=0.98 DeCOG study secondary endpoint Leiter, ASCO 2015
31 Tumor load SN per patient > 3 n.a. Histological criteria H&E positive Immunhisto. pos. (S100, HMB45, Melan A) not specified Size of metastases in the SLN single cells / <0,5 mm 0,5-1,00 mm 1,01-2,00 mm 2,01-5,00 mm 5, mm others Arm A (Observation) N = % % 7 3.% 1 0.4% % % % % % % % 4 1.7% % Arm B (Radical LAD) N = % % 6 2.5% 7 2.9% % % % % % % % 3 1.3% % P- value % of Pts with < 1mm of SLN tumor burden
32 CLND for melanoma Clinical equipoise: MSLT-II trial Positive SLN N=1755 Stratify by extent of nodal involvement Completion LND Observation (with nodal basin U/S) Nodal recurrence only No nodal recurrence only Observation Therapeutic LND Observation IRB
33 Nodal Basin Control According to Randomized Treatment Arm
34 Overall Melanoma-Specific Survival According to Treatment Arm
35 Surgical Morbidity of Lymphadenectomy Microscopic vs Palpable disease (MSLT-1) Compared morbidity of formal dissection in node positive patients - SLN positive vs delayed for palpable nodal disease Hospital stay - shorter for SLN positive patients Symptomatic lymphedema - less in SLN positive group, 12% vs 20%,p=.04 Farries, et al, Ann Surg Oncol, 2010
36 Reasons for CLND after Positive SLNBx complete staging - need 2 positive nodes for high priority adjuvant trial of Anti-PD-1 vs IFN - number of + nodes and presence of non-sln involvement prognostic Improved regional disease control and less post-dissection morbidity for patients with nonsentinel node involvement
37 Completion Node Dissection Conclusions No direct evidence that CLND provides a survival benefit SLN biopsy may be therapeutic for the patients with only SLN disease (80% of the SLN+ patients) Prognosis in patients with non-sln involvement is particularly unfavorable A selective approach based on predicted risk of non- SLN involvement is rational Improved regional disease control and accurate staging may be the only benefits of CLND
38 Working Model Predicting Risk for Additional Positive Nodes No. of pts in group No. additional pos LN Score* N % *Score = sum of Breslow thickness (0 or 1 for 2 mm or > 2 mm, respectively), SLN focus (0, 1, 2, or 3 for 0.5, >0.5 and 2, >2 and 10, or > 10 mm, respectively) Number of SLNs harvested (0, 1, or 2 for > 3, 2, or 1 respectively) Gershenwald et al, JCO 2008

39
40 Spectrum of Advanced Disease Nodal disease (Stage IIIb/c) - with or without known primary - resectable vs unresectable Limited local/satelite/intransit metastases - stage IIIb: intransit only - stage IIIc: with nodes Resectable (oligometastatic) stage IV disease
41 Resectable Stage III and Selected Oligometastatic Stage IV Melanoma Standard of care Upfront Surgery Selective use of adjuvant nodal basin irradiation (stages III b/c) Systemic adjuvant therapy - resected stage III: interferon, ipilimumab, or clinical trial - resected stage IV: clinical trial or observation
42 Advanced Stage III Melanoma Management Goals Durable Local/Regional Control - long term survival - palliation (expectant palliation) - minimize morbidity and functional deficits Reduce the risk for distant failure
43 Surgery Adjuvant Therapy Stage III patients have a high risk of recurrence after upfront surgery 70% Adjuvant therapy options are not optimal: controversy with high dose interferon, peg-intron and high dose ipilimumab Nodal basin irradiation has significant risk of lymphedema Delay in the treatment of the micrometastatic disease Disadvantages
44 Neoadjuvant Therapy Surgery Adjuvant Therapy Potential Advantages Tumor shrinkage Decreased surgical morbidity - better regional disease control - avoid the morbidity of adjuvant XRT Destruction of micro-metastases Prevent distant disease spread Objective measure of patient s response to therapy Personalization of adjuvant therapy Potential pathway for new drug evaluation/registration

45 Approvals:10 for metastatic disease, 2 adjuvant Adjuvant therapy Peg IFN 1996 HD Interferon Biochemotherapy ipilimumab US approval for metastatic disease, adjuvant timeline
46 Poor Outcomes for Clinical Stage III Melanoma 8 th Edition AJCC Draft Clinical Stage IIIC MDACC Historical Controls (n=144) SOC: Surgery +/- Adjuvant Melanoma-Specific Survival Probability IIIA: N = 1006, 5yr = 93%, 10yr = 88% IIIB: N = 1170, 5yr = 83%, 10yr = 77% IIIC: N = 2201, 5yr = 69%, 10yr = 60% IIID: N = 205, 5yr = 32%, 10yr = 24% Years Since Diagnosis Gershenwald et al AJCC Cancer Staging Manual Eighth Edition, 2017.
47 Activity of Dabrafenib + Trametinib in Stage IV 617 patients, median PFS 11.1 months, median OS 25.6 months Overall response rate 67%, Disease control rate 91% Very favorable outcomes in patients that achieved a CR (16%) Best predictors of CR: Sum of diameters & < 3 metastatic sites Hypothesis: More frequent CRs and durable responses in Stage III Subgroup n OS rate (95% CI) 1 year 2 year CR % (91 99) 88% (82 95) PR % (79 88) 55% (49 61) SD % (43 60) 33% (26 42) PD 35 38% (25 59) 13% (5 40) Not evaluable 16 14% (2 86) 14% (2 86) Long et al, Lancet Oncology, In Press PFS rate (95% CI) Subgroup n 1 year 2 year CR % (84 96) 68% (59 79) PR % (46 57) 29% (24 35) SD % (15 30) 6% (2 19) PD 35 0% 0% Not evaluable 16 25% (5 100) 25% (5 100)

 Treated with")

 December")
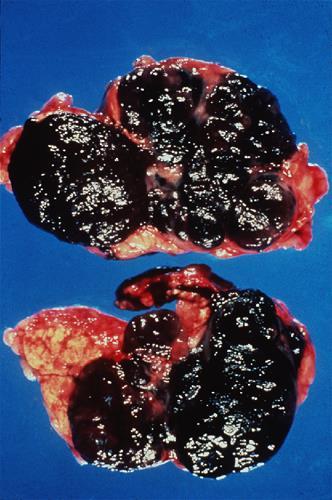
48 Case Example (1) 47 yo female with prior hx of R arm melanoma presented with bulky adenopathy in R axilla (? resectable). Biopsy - melanoma (BRAF mut) Treated with neoadjuvant BRAF/MEKi x 8 weeks with excellent radiologic response Path = fibrosis, no viable tumor cells (pcr) October 2013 (Pre-BRAF/MEKi) December 2013 (Post-BRAF/MEKi)


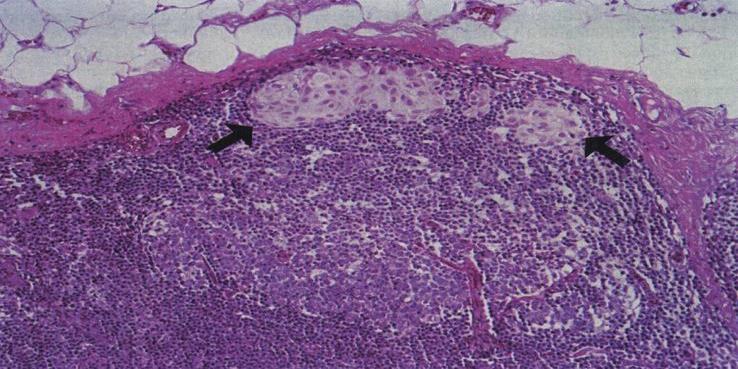
49 Pathological Response Before After Lymph node with extensive fibrosis and melanin deposition in the extracapsular tissue
 Phase 2 Randomized Trial vs Standard of Care of Surgery +")
50 Neoadjuvant BRAF and MEK Inhibition Neoadjuvant and Adjuvant Dabrafenib and Trametinib Compared to Upfront Surgery in Patients With Clinical Stage III or Oligometastatic Stage IV Melanoma (Combi-Neo) Phase 2 Randomized Trial vs Standard of Care of Surgery + Adjuvant
51 Combi-Neo n=28 Arm A Upfront surgery Scheduled within 0-4 weeks Surgical resection Standard of care adjuvant therapy (interferon vs. observation) Clinical and radiographic follow up n=56 Pathologic assessment of tumor + research biopsy Assess relapse-free survival, overall survival, toxicity Patients with stage IIIB/IIIC or oligometastatic stage IV (<3 lesions), + BRAF mutation Arm B Neoadjuvant BRAFi/MEKI Neoadjuvant BRAF/MEK x 8 weeks Restaging via CTs followed by surgical resection Adjuvant BRAF/MEK x 44 weeks Clinical and radiographic follow up Blood draw and tumor biopsy Pre-treatment On treatment biopsy / blood draw (arm B only) Blood draw and tumor biopsy at surgery Restaging CT scans every 3 months with blood draws Blood draw and tumor biopsy at relapse






52 A B E F Excellent Responder: 79% decrease by RECIST and Pathologic CR C Poor Responder: 23% decrease by RECIST and viable tumor at surgery D G H
53 Neoadjuvant and Adjuvant D+T Significantly Improved RFS over SOC HR % CI ( ) P<0.0001
54 Patients with pcr had Improved RFS compared to those without pcr
55 Neoadjuvant Strategy Checkpoint Blockade Neoadjuvant and Adjuvant Checkpoint Blockade in Patients With Clinical Stage III or Oligometastatic Stage IV Melanoma (NCT ) Nivolumab vs Ipi / Nivo Phase 2 randomized trial

56 Baseline reduction from baseline in target lesions (%) Baseline reduction from baseline in target lesions (%) Baseline reduction from baseline in target lesions (%) Tumor Burden Change From Baseline from CheckMate- 067 NIVO + IPI Median change: -51.9% IPI Median change: +5.9% NIVO Median change: -34.5% Confirmed responder 30% reduction in tumor burden by RECIST v1.1 Presented by J. Wolchok ASCO 2015
 Restaging via CTs followed by surgical resection Adjuvant Nivolumab x 6 months Follow up")
57 n= : Neoadjuvant Checkpoint Arm A Neoadjuvant Nivolumab (4 doses) Restaging via CTs followed by surgical resection Pathologic assessment with correlative studies Adjuvant Nivolumab x 6 months Follow up with restaging q 12 weeks x 2 years n=20 Arm B Neoadjuvant Ipilimumab & Nivolumab (3 doses) Restaging via CTs followed by surgical resection Adjuvant Nivolumab x 6 months Follow up with restaging q 12 weeks x 2 years Patients with stage IIIB/IIIC or oligometastatic stage IV ( 3 lesions) Blood draw and tumor biopsy Pre-treatment On treatment biopsy / blood draw (prior to dose 2 and dose 3) Blood draw and tumor harvested at surgery Restaging CT scans q 12 weeks Research blood draws Blood draw and tumor biopsy at relapse
58 Intralesional Therapy (Oncolytic Immunotherapy): Goals Locally ablative therapy for local disease control High, local concentration Palliation/symptom control Induction of systemic host immune antitumor activity Augment the local injected response Response in distant and uninjected regional metastases Systemic adjuvant response (treat micrometatases) Limited systemic toxicity Durable response 58
59 Drug Agencies in US and Europe Approve T-VEC October 27, 2015 T-VEC: US approval for the local treatment of unresectable cutaneous, subcutaneous, and nodal lesions in patients with melanoma recurrent after initial surgery December 16, 2015 T-VEC: EU approval for Stages IIIB, IIIC, IVM1a metastatic melanoma 59
60 Percentage Change From Baseline Lesion-level and patient-level responses to T-VEC Tumor area change: Lesion type: injected Lesion type: uninjected non-visceral Lesion type: uninjected visceral % > 50% to < 25% 100% to 50% I Lesion n = 2116 Patient n = % decrease 64% OR 33% 100% decrease 47% CR 15% Lesion n = 981 Lesion n = 177 Patient n = % decrease 34% OR 18% 100% decrease 22% CR 6% Patient n = 79 50% decrease 15% OR 14% 100% decrease 9% CR 3% To be included in the lesion-level response analysis, lesions were required to have at least 2 measurements. For the patient-level response analysis, only patients with at least 1 lesion represented in the corresponding waterfall plot were included. Responses were per investigator Andtbacka RHI, et al. SSO 2014 abstract PCC-121. Kaufman H, et al. ASCO 2014 abstract 9008a.



61 T-VEC Responses in Injected And Uninjected Lesions Cycle 1 Cycle 13 61
62 Kaplan Meier percent Primary overall survival 100 Events/N (%) Median (95% CI), months T-VEC 189/295 (64) 23.3 (19.5, 29.6) GM-CSF 101/141 (72) 18.9 (16.0, 23.7) HR = 0.79 (95% CI: 0.62, 1.00) Unadjusted log-rank P = Survival T-VEC GM-CSF Difference % (95% CI) 12-mo 73.7% 69.1% 4.6 (-4.7, 13.8) 0 24-mo 49.8% 40.3% 9.5 (-0.5, 19.6) 36-mo 38.6% 30.1% 8.5 (-1.2, 18.1) 48-mo 32.6% 21.3% 11.3 (1.0, 21.5) Patients at risk: T-VEC GM-CSF HR, hazard ratio. Kaufman H, et al. ASCO 2014 abstract 9008a.
63 Kaplan Meier percent Exploratory OS subgroup analysis by disease stage Stage IIIB/C, IV M1a 100 Log rank: P < (descriptive) 80 HR: 0.57 (95% CI: 0.40, 0.80) 100 Log rank: P = 0.71 (descriptive) 80 Stage IV M1b/c HR: 1.07 (95% CI: 0.75, 1.52) Risk set, n T-VEC GM-CSF Study month Events/n (%) median (95% CI), mo T-VEC 80/163 (49) 41.1 (30.6, NE) GM-CSF 57/86 (66) 21.5 (17.4, 29.6) Study month Risk set, n T-VEC GM-CSF Events/n (%) median (95% CI), mo T-VEC 109/131 (83) 13.4 (11.4, 16.2) GM-CSF 44 /55 (80) 15.9 (10.2,19.7) Mo, months. Kaufman H, et al. ASCO 2014 abstract 9008a.
64 Neo-Adjuvant T-VEC Resectable stage IIIb/c and M1a, N=150 Randomized phase 2 trial of standard of care upfront surgery + adjuvant vs preop T-VEC 12 weeks followed by surgery Combination Trials of Oncolytic Immunotherapy and Primary Anti-CTLA-4 endpoint: or Anti-PD-1 RFS are ongoing
65 Neoadjuvant Therapy for Advanced Resectable Melanoma Where are we Now and Where are we Going? A growing international interest has emerged in designing and completing neoadjuvant trials Ideal model for discovering and validating biomarkers of response and resistance - easy access for serial tissue acquisition Improved regional disease control and survival outcomes will lead to new treatment paradigms Novel combinations to raise the tail of the curve in the stage IV setting will be tested in the neoadjuvant setting The first International Neoadjuvant Consortium was held in November at the SMR
66 Surgery for Stage IV Disease Why? Ten new approvals in last 5 years Robust response with BRAF inhibition, but not durable Low response rate with ipilimumab High response rate with combination checkpoint blockade but significant toxicity Surgery well tolerated, 100% response rate
67 Palliation - improve quality of life - candidates for effective systemic therapy Surgery for Stage IV melanoma: Patient selection Curative intent - can a complete resection be performed? - symptoms? - morbidity of planned surgery? - associated co-morbidity? Favorable biology? - target the right patient population
68 SWOG S9430: Phase II Trial Complete Resection for Stage IV Melanoma Prospective registry - surgical resection, stage IV , 18 centers 77 patients enrolled - 8 pts: not completely resected to NED - 3 pts: no tumor in specimen - 2 pts: locoregional disease only 64 patients included in primary analysis - median age 54y, M:F 2:1 - sites: any visceral, 31%; non-visceral only, 69% - >1 site resected, 22% - 11 received some type of systemic adjuvant (8 IFN) Median RFS, 5mos; median OS, 21mos Sosman et al., Cancer 2011
69 SWOG S9430 Overall Survival Patients Completely Resected Sosman et al., Cancer 2011
70 Canvaxin Stage IV Placebo-Controlled Randomized Trial Two sites, 5 nodules, complete resection, no brain mets within 6 months of surgery NED based on repeat staging within 45 days of randomization Trial stopped by DSMB short of planned accrual April 2005 after 2 nd interim analysis 38 months median and 40% 5-year survival!
Surgical Issues in Melanoma
 Surgical Issues in Melanoma Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Director, Surgical Oncology Training Program Professor of Surgery John Wayne Cancer Institute Surgical
Surgical Issues in Melanoma Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Director, Surgical Oncology Training Program Professor of Surgery John Wayne Cancer Institute Surgical
Melanoma: Therapeutic Progress and the Improvements Continue
 Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Melanoma: Therapeutic Progress and the Improvements Continue David W. Ollila, MD Professor of Surgery Jesse and James Millis Professor of Melanoma Research May 20, 2016 Disclosures: NONE Outline 2016 Therapeutic
Sentinel Node Alphabet Soup: MSLT-1, DeCOG-SLT, MSLT-2, UNC
 Sentinel Node Alphabet Soup: MSLT-1, DeCOG-SLT, MSLT-2, UNC David W. Ollila MD James and Jesse Millis Professor of Surgery University of North Carolina, Chapel Hill Disclosures: None July 15, 2018 AJCC
Sentinel Node Alphabet Soup: MSLT-1, DeCOG-SLT, MSLT-2, UNC David W. Ollila MD James and Jesse Millis Professor of Surgery University of North Carolina, Chapel Hill Disclosures: None July 15, 2018 AJCC
Update on SLN and Melanoma: DECOG and MSLT-II. Gordon H. Hafner, MD, FACS
 Update on SLN and Melanoma: DECOG and MSLT-II Gordon H. Hafner, MD, FACS No disclosures The surgery of malignant disease is not the surgery of organs, it is of the lymphatic system. Lord Moynihan Lymph
Update on SLN and Melanoma: DECOG and MSLT-II Gordon H. Hafner, MD, FACS No disclosures The surgery of malignant disease is not the surgery of organs, it is of the lymphatic system. Lord Moynihan Lymph
Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know
 Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know Jeffrey Weber, MD, PhD Laura and Isaac Perlmutter Cancer Center NYU Langone Medical Center New York, New York What Is the Current
Immunotherapy in the Adjuvant Setting for Melanoma: What You Need to Know Jeffrey Weber, MD, PhD Laura and Isaac Perlmutter Cancer Center NYU Langone Medical Center New York, New York What Is the Current
Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy
 American Academy of Dermatology 2018 Annual Meeting San Diego, CA, February 17, 2018 Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy Christopher Bichakjian,
American Academy of Dermatology 2018 Annual Meeting San Diego, CA, February 17, 2018 Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy Christopher Bichakjian,
Topics for Discussion. Malignant Melanoma. Surgical Treatment. Current Treatment of Cutaneous Melanoma 5/17/2013. Lymph Regional nodes:
 Topics for Discussion What is a sentinel lymph node (SLN)? Utility of sentinel lymph biopsies: therapeutic or staging? Current Treatment of Cutaneous Melanoma Carlos Corvera, M.D. Associate Professor of
Topics for Discussion What is a sentinel lymph node (SLN)? Utility of sentinel lymph biopsies: therapeutic or staging? Current Treatment of Cutaneous Melanoma Carlos Corvera, M.D. Associate Professor of
Controversies and Questions in the Surgical Treatment of Melanoma
 Controversies and Questions in the Surgical Treatment of Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Division of Endocrine and Oncologic Surgery University of Pennsylvania School
Controversies and Questions in the Surgical Treatment of Melanoma Giorgos C. Karakousis, M.D. Assistant Professor of Surgery Division of Endocrine and Oncologic Surgery University of Pennsylvania School
Rebecca Vogel, PGY-4 March 5, 2012
 Rebecca Vogel, PGY-4 March 5, 2012 Historical Perspective Changes In The Staging System Studies That Started The Talk Where We Go From Here Cutaneous melanoma has become an increasingly growing problem,
Rebecca Vogel, PGY-4 March 5, 2012 Historical Perspective Changes In The Staging System Studies That Started The Talk Where We Go From Here Cutaneous melanoma has become an increasingly growing problem,
Surgical Oncology Perspective of Melanoma
 Surgical Oncology Perspective of Melanoma Hans F. Schoellhammer, MD, FACS Assistant Clinical Professor Division of Surgical Oncology September 20, 2018 Nothing to disclose DISCLOSURE Discussion Objectives
Surgical Oncology Perspective of Melanoma Hans F. Schoellhammer, MD, FACS Assistant Clinical Professor Division of Surgical Oncology September 20, 2018 Nothing to disclose DISCLOSURE Discussion Objectives
Who is the Ideal Candidate for PEG Intron?
 Who is the Ideal Candidate for PEG Intron? Sanjiv S. Agarwala, MD Chief, Oncology & Hematology St. Luke s Cancer Center Professor, Temple University School of Medicine Philadelphia, PA, USA Overview Introduction
Who is the Ideal Candidate for PEG Intron? Sanjiv S. Agarwala, MD Chief, Oncology & Hematology St. Luke s Cancer Center Professor, Temple University School of Medicine Philadelphia, PA, USA Overview Introduction
Nodal Treatment in Melanoma: Snow to MSLT-II
 Nodal Treatment in Melanoma: Snow to MSLT-II Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Program Director, JWCI Complex General Surgical Oncology Fellowship Director,
Nodal Treatment in Melanoma: Snow to MSLT-II Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Program Director, JWCI Complex General Surgical Oncology Fellowship Director,
Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective
 Procedure: An Oncologic Surgeon s Perspective") Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective Giorgos C. Karakousis, M.D. Associate Professor of Surgery Hospital of the University of Pennsylvania Disclosures
Melanoma Patients and the Sentinel Lymph Node (SLN) Procedure: An Oncologic Surgeon s Perspective Giorgos C. Karakousis, M.D. Associate Professor of Surgery Hospital of the University of Pennsylvania Disclosures
Adjuvant Therapy of High Risk Melanoma
 Adjuvant Therapy of High Risk Melanoma William Sharfman, MD, FACP Associate Professor of Oncology and Dermatology Johns Hopkins University School of Medicine July 5, 2012 Adjuvant options for Stage IIB/C
Adjuvant Therapy of High Risk Melanoma William Sharfman, MD, FACP Associate Professor of Oncology and Dermatology Johns Hopkins University School of Medicine July 5, 2012 Adjuvant options for Stage IIB/C
Melanoma Quality Reporting
 Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Medical Treatment for Melanoma Sanjiv S. Agarwala, MD
 Medical Treatment for Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Disclosures None Overview
Medical Treatment for Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Disclosures None Overview
Sentinel Lymph Node Biopsy: Current Evidence for its Role in Managing Melanoma
 Sentinel Lymph Node Biopsy: Current Evidence for its Role in Managing Melanoma John A Zitelli MD Adjunct Clinical Associate Professor Dermatology, Otolaryngology, Plastic Surgery University of Pittsburgh
Sentinel Lymph Node Biopsy: Current Evidence for its Role in Managing Melanoma John A Zitelli MD Adjunct Clinical Associate Professor Dermatology, Otolaryngology, Plastic Surgery University of Pittsburgh
Cutaneous Melanoma: Epidemiology (USA) The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)
 The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)") The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
Immunotherapy for the Treatment of Melanoma. Marlana Orloff, MD Thomas Jefferson University Hospital
 Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
Immunotherapy for the Treatment of Melanoma Marlana Orloff, MD Thomas Jefferson University Hospital Disclosures Immunocore and Castle Biosciences, Consulting Fees I will be discussing non-fda approved
NEW SURGICAL APPROACHES TO MELANOMA THERAPY
 NEW SURGICAL APPROACHES TO MELANOMA THERAPY Melanoma 2003: New Insights Into Therapy & Treatment Douglas L. Fraker, M.D. University of Pennsylvania Surgical Treatment of Melanoma Primary resection margins
NEW SURGICAL APPROACHES TO MELANOMA THERAPY Melanoma 2003: New Insights Into Therapy & Treatment Douglas L. Fraker, M.D. University of Pennsylvania Surgical Treatment of Melanoma Primary resection margins
Melanoma Surgery Update James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division
 Melanoma Surgery Update 2018 James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division Surgery for Melanoma Mainstay of treatment for potentially
Melanoma Surgery Update 2018 James R. Ouellette, DO FACS Premier Health Cancer Institute Wright State University Chief, Surgical Oncology Division Surgery for Melanoma Mainstay of treatment for potentially
Disclosures. SLNB for Melanoma 25/02/2014 SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION
 8 th Canadian Melanoma Conference February 22, 2014 Rimrock Resort Hotel, Banff, Alberta SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION Christopher Bichakjian,
8 th Canadian Melanoma Conference February 22, 2014 Rimrock Resort Hotel, Banff, Alberta SENTINEL LYMPH NODE BIOPSY FOR MELANOMA: CURRENT GUIDELINES AND THEIR CLINICAL APPLICATION Christopher Bichakjian,
Update on Immunotherapy in Advanced Melanoma. Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017
 Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
Update on Immunotherapy in Advanced Melanoma Ragini Kudchadkar, MD Assistant Professor Winship Cancer Institute Emory University Sea Island 2017 1 Outline Adjuvant Therapy Combination Immunotherapy Single
Metastasectomy for Melanoma What s the Evidence and When Do We Stop?
 Metastasectomy for Melanoma What s the Evidence and When Do We Stop? Vernon K. Sondak, M D Chair, Moffitt Cancer Center Tampa, Florida Focus on Melanoma London, UK October 15, 2013 Disclosures Dr. Sondak
Metastasectomy for Melanoma What s the Evidence and When Do We Stop? Vernon K. Sondak, M D Chair, Moffitt Cancer Center Tampa, Florida Focus on Melanoma London, UK October 15, 2013 Disclosures Dr. Sondak
No Benefit to Routine Completion Lymphadenectomy for Sentinel Lymph Node Positive Melanoma
 No Benefit to Routine Completion Lymphadenectomy for Sentinel Lymph Node Positive Melanoma Michael Lowe, MD Assistant Professor of Surgery Winship Cancer Institute Emory University School of Medicine July
No Benefit to Routine Completion Lymphadenectomy for Sentinel Lymph Node Positive Melanoma Michael Lowe, MD Assistant Professor of Surgery Winship Cancer Institute Emory University School of Medicine July
III Sessione I risultati clinici
 10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
10,30-13,15 III Sessione I risultati clinici Moderatori: Michele Maio - Valter Torri 10,30-10,45 Melanoma: anti CTLA-4 Vanna Chiarion Sileni Vanna Chiarion Sileni IOV-IRCCS,Padova Vanna.chiarion@ioveneto.it
Treatment and management of advanced melanoma: Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC
 Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
Treatment and management of advanced melanoma: 2018 Paul B. Chapman, MD Melanoma Clinical Director, Melanoma and Immunotherapeutics Service MSKCC Disclosure Paul B. Chapman, MD Nothing to disclose. Off
Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy
 Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy Dale Han, MD Assistant Professor Department of Surgery Section of Surgical Oncology No disclosures Background Desmoplastic melanoma (DM)
Desmoplastic Melanoma: Surgical Management and Adjuvant Therapy Dale Han, MD Assistant Professor Department of Surgery Section of Surgical Oncology No disclosures Background Desmoplastic melanoma (DM)
Black is the New Black or How I learned to stop worrying and love melanoma (with apologies to Dr. Strangelove)
") Black is the New Black or How I learned to stop worrying and love melanoma (with apologies to Dr. Strangelove) Provincial Cancer Care Conference 2018 Ralph P.W. Wong MD FRCPC St Boniface Site Director
Black is the New Black or How I learned to stop worrying and love melanoma (with apologies to Dr. Strangelove) Provincial Cancer Care Conference 2018 Ralph P.W. Wong MD FRCPC St Boniface Site Director
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania
 Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Immunotherapy in Unresectable or Metastatic Melanoma: Where Do We Stand? Sanjiv S. Agarwala, MD St. Luke s Cancer Center Bethlehem, Pennsylvania Overview Background Immunotherapy clinical decision questions
Michael T. Tetzlaff MD, PhD
 American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
Talimogene Laherparepvec (T-VEC) at the SCCA: an update
 at the SCCA: an update") Talimogene Laherparepvec (T-VEC) at the SCCA: an update Jennifer M. Gardner, MD Assistant Professor, Division of Dermatology University of Washington jen1110@uw.edu Northwest Melanoma Symposium: Science
Talimogene Laherparepvec (T-VEC) at the SCCA: an update Jennifer M. Gardner, MD Assistant Professor, Division of Dermatology University of Washington jen1110@uw.edu Northwest Melanoma Symposium: Science
Melanoma: Immune checkpoints
 ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
ESMO Preceptorship Programme Immuno-Oncology Siena, July 04-05, 2016 Melanoma: Immune checkpoints Michele Maio Medical Oncology and Immunotherapy-Department of Oncology University Hospital of Siena, Istituto
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology
 Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
Current Trends in Melanoma Theresa Medina, MD UCD Cutaneous Oncology Overview Melanoma incidence and prevention Approach to surgical management of early melanoma Landscape of Advanced Melanoma Therapy
An update on the Society for Immunotherapy of Cancer consensus statement on tumor immunotherapy for the treatment of cutaneous melanoma: version 2.
 Sullivan et al. Journal for ImmunoTherapy of Cancer (2018) 6:44 https://doi.org/10.1186/s40425-018-0362-6 POSITION ARTICLE AND GUIDELINES Open Access An update on the Society for Immunotherapy of Cancer
Sullivan et al. Journal for ImmunoTherapy of Cancer (2018) 6:44 https://doi.org/10.1186/s40425-018-0362-6 POSITION ARTICLE AND GUIDELINES Open Access An update on the Society for Immunotherapy of Cancer
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD
 Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
Immunotherapy of Melanoma Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA Overview Metastatic Melanoma
When Do I Consider Myself Cured?
 The Melanoma Patient Symposium - Science to Survivorship When Do I Consider Myself Cured? 26 September 2009 Jeffrey E. Gershenwald, MD, FACS Professor of Surgery, Dept. of Surgical Oncology Professor,
The Melanoma Patient Symposium - Science to Survivorship When Do I Consider Myself Cured? 26 September 2009 Jeffrey E. Gershenwald, MD, FACS Professor of Surgery, Dept. of Surgical Oncology Professor,
MELANOMA: THE BEST OF THE YEAR Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone
 MELANOMA: THE BEST OF THE YEAR 2018 Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone The Best of the Year 2018: MELANOMA CHIRURGIA TERAPIA ADIUVANTE TERAPIA PER MALATTIA AVANZATA The Best of the Year
MELANOMA: THE BEST OF THE YEAR 2018 Dott.ssa Silvia Quadrini UOC Oncologia ASL Frosinone The Best of the Year 2018: MELANOMA CHIRURGIA TERAPIA ADIUVANTE TERAPIA PER MALATTIA AVANZATA The Best of the Year
Work-up/Follow-up: Baseline and Surveillance Studies for Cutaneous Melanoma Patients
 2018 AAD Annual Meeting, San Diego, CA Work-up/Follow-up: Baseline and Surveillance Studies for Cutaneous Melanoma Patients Susan M. Swetter, MD, FAAD Professor of Dermatology Director, Pigmented Lesion
2018 AAD Annual Meeting, San Diego, CA Work-up/Follow-up: Baseline and Surveillance Studies for Cutaneous Melanoma Patients Susan M. Swetter, MD, FAAD Professor of Dermatology Director, Pigmented Lesion
Melanoma. Il parere dell esperto. V. Ferraresi. Divisione di Oncologia Medica 1
 Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
Melanoma Il parere dell esperto V. Ferraresi Divisione di Oncologia Medica 1 MELANOMA and ESMO 2017.what happens? New data and updates ADJUVANT THERAPY with CHECKPOINT INHIBITORS (CA209-238 trial) AND
NCCN Guidelines for Cutaneous Melanoma V Meeting on 06/20/18
 ME-1, ME-3, ME-B Submission from Castle Biosciences, Inc (05/30/18) to consider inclusion of the DecisionDx-Melanoma test in the guidelines as a prognostic test that provides stratification according to
ME-1, ME-3, ME-B Submission from Castle Biosciences, Inc (05/30/18) to consider inclusion of the DecisionDx-Melanoma test in the guidelines as a prognostic test that provides stratification according to
When to Integrate Surgery for Metatstatic Urothelial Cancers
 When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
When to Integrate Surgery for Metatstatic Urothelial Cancers Wade J. Sexton, M.D. Senior Member and Professor Department of Genitourinary Oncology Moffitt Cancer Center Case Presentation #1 67 yo male
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy. What every patient needs to know. James Larkin
 Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Melanoma: From Chemotherapy to Targeted Therapy and Immunotherapy What every patient needs to know James Larkin Melanoma Therapy 1846-2017 Surgery 1846 Cytotoxic Chemotherapy 1946 Checkpoint Inhibitors
Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3
 ESMO 2016 Congress 7-11 October, 2016 Copenhagen, Denmark Table of Contents Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3 Long-term results show adjuvant therapy with ipilimumab improves OS in high
ESMO 2016 Congress 7-11 October, 2016 Copenhagen, Denmark Table of Contents Summary... 2 MELANOMA AND OTHER SKIN TUMOURS... 3 Long-term results show adjuvant therapy with ipilimumab improves OS in high
Marshall T Bell Research Resident University of Colorado Grand Rounds Nov. 21, 2011
 Marshall T Bell Research Resident University of Colorado Grand Rounds Nov. 21, 2011 Most common form of cancer in adults ages 25-29 3-5% of skin cancers but 65-75% of deaths Most common metastasis to small
Marshall T Bell Research Resident University of Colorado Grand Rounds Nov. 21, 2011 Most common form of cancer in adults ages 25-29 3-5% of skin cancers but 65-75% of deaths Most common metastasis to small
Results of the ACOSOG Z0011 Trial
 DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
DCIS and Early Breast Cancer Symposium JUNE 15-17 2012 CAPPADOCIA Results of the ACOSOG Z0011 Trial Kelly K. Hunt, M.D. Professor of Surgery Axillary Node Dissection Staging, Regional control, Survival
47. Melanoma of the Skin
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Single Technology Appraisal (STA) Nivolumab for adjuvant treatment of resected stage III and IV melanoma
 Nivolumab for adjuvant treatment of resected stage III and IV melanoma") Single Technology Appraisal (STA) Nivolumab for adjuvant treatment of resected stage III and IV Response to consultee and commentator comments on the draft remit and draft scope (pre-referral) Comment:
Single Technology Appraisal (STA) Nivolumab for adjuvant treatment of resected stage III and IV Response to consultee and commentator comments on the draft remit and draft scope (pre-referral) Comment:
The Role of Sentinel Lymph Node Biopsy and Axillary Dissection
 The Role of Sentinel Lymph Node Biopsy and Axillary Dissection Henry Mark Kuerer, MD, PhD, FACS Department of Surgical Oncology University of Texas MD Anderson Cancer Center SLN Biopsy Revolutionized surgical
The Role of Sentinel Lymph Node Biopsy and Axillary Dissection Henry Mark Kuerer, MD, PhD, FACS Department of Surgical Oncology University of Texas MD Anderson Cancer Center SLN Biopsy Revolutionized surgical
M D..,., M. M P.. P H., H, F. F A.. A C..S..
 Implications of NSABP B-32 and Loco-Regional Therapy Considerations After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H, F.A.C.S. Professor of Surgery Northeastern Ohio Medical University Medical
Implications of NSABP B-32 and Loco-Regional Therapy Considerations After Neoadjuvant Chemotherapy Terry Mamounas, M.D., M.P.H, F.A.C.S. Professor of Surgery Northeastern Ohio Medical University Medical
Sentinel Lymph Node Biopsy: Past and Present Implications for the Management of Cutaneous Melanoma with Nodal Metastasis
 American Journal of Clinical Dermatology (2018) 19 (Suppl 1):S24 S30 https://doi.org/10.1007/s40257-018-0379-0 REVIEW ARTICLE Sentinel Lymph Node Biopsy: Past and Present Implications for the Management
American Journal of Clinical Dermatology (2018) 19 (Suppl 1):S24 S30 https://doi.org/10.1007/s40257-018-0379-0 REVIEW ARTICLE Sentinel Lymph Node Biopsy: Past and Present Implications for the Management
Cutaneous melanoma: new developments for 2018
 Cutaneous melanoma: new developments for 2018 and beyond KIM MARGOLIN, M.D., FASCO CITY OF HOPE MEDICAL ONCOLOGY CORONADO, CALIFORNIA SEPTEMBER 20, 2018 DISCLOSURE Consultant for ImaginAb, Nektar Therapeutics,
Cutaneous melanoma: new developments for 2018 and beyond KIM MARGOLIN, M.D., FASCO CITY OF HOPE MEDICAL ONCOLOGY CORONADO, CALIFORNIA SEPTEMBER 20, 2018 DISCLOSURE Consultant for ImaginAb, Nektar Therapeutics,
Management of the patient with Lymph Node Involvement. Michael A Henderson Peter MacCallum Cancer Center Univ of Melbourne
 Management of the patient with Lymph Node Involvement Michael A Henderson Peter MacCallum Cancer Center Univ of Melbourne Lymph Node Field Recurrence Most important prognostic factor for early stage melanoma
Management of the patient with Lymph Node Involvement Michael A Henderson Peter MacCallum Cancer Center Univ of Melbourne Lymph Node Field Recurrence Most important prognostic factor for early stage melanoma
How can we reduce the mortality from melanoma in Australia?
 How can we reduce the mortality from melanoma in Australia? Professor Grant McArthur MB BS PhD Peter MacCallum Cancer Centre Melbourne, Australia University of Melbourne, Parkville, Australia What is melanoma?
How can we reduce the mortality from melanoma in Australia? Professor Grant McArthur MB BS PhD Peter MacCallum Cancer Centre Melbourne, Australia University of Melbourne, Parkville, Australia What is melanoma?
ORIGINAL ARTICLE. Clinical Node-Negative Thick Melanoma
 ORIGINAL ARTICLE Clinical Node-Negative Thick Melanoma George I. Salti, MD; Ashwin Kansagra, MD; Michael A. Warso, MD; Salve G. Ronan, MD ; Tapas K. Das Gupta, MD, PhD, DSc Background: Patients with T4
ORIGINAL ARTICLE Clinical Node-Negative Thick Melanoma George I. Salti, MD; Ashwin Kansagra, MD; Michael A. Warso, MD; Salve G. Ronan, MD ; Tapas K. Das Gupta, MD, PhD, DSc Background: Patients with T4
Molecular Enhancement of Sentinel Node Evaluation
 Cochran Illustrations 060104 Molecular Enhancement of Sentinel Node Evaluation Alistair Cochran, MD and Rong Huang MD Departments of Pathology and Laboratory Medicine and Surgery, David Geffen School of
Cochran Illustrations 060104 Molecular Enhancement of Sentinel Node Evaluation Alistair Cochran, MD and Rong Huang MD Departments of Pathology and Laboratory Medicine and Surgery, David Geffen School of
Implications of ACOSOG Z11 for Clinical Practice: Surgical Perspective
 :$;7)#*8'-87*4BCD'E7)F'31$4.$&'G$H'E7)F&'GE'>??ID >?,"'@4,$)4*,#74*8'!74/)$++'74',"$'A.,.)$'7%'()$*+,'!*42$)!7)74*67&'!3 6 August 2011 Implications of ACOSOG Z11 for Clinical
:$;7)#*8'-87*4BCD'E7)F'31$4.$&'G$H'E7)F&'GE'>??ID >?,"'@4,$)4*,#74*8'!74/)$++'74',"$'A.,.)$'7%'()$*+,'!*42$)!7)74*67&'!3 6 August 2011 Implications of ACOSOG Z11 for Clinical
Debate Axillary dissection - con. Prof. Dr. Rodica Anghel Institute of Oncology Bucharest
 Debate Axillary dissection - con Prof. Dr. Rodica Anghel Institute of Oncology Bucharest Summer School of Oncology, third edition Updated Oncology 2015: State of the Art News & Challenging Topics Bucharest,
Debate Axillary dissection - con Prof. Dr. Rodica Anghel Institute of Oncology Bucharest Summer School of Oncology, third edition Updated Oncology 2015: State of the Art News & Challenging Topics Bucharest,
Immunotherapy, an exciting era!!
 Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Immunotherapy, an exciting era!! Yousef Zakharia MD University of Iowa and Holden Comprehensive Cancer Center Alliance Meeting, Chicago November 2016 Presentation Objectives l General approach to immunotherapy
Management of Brain Metastases Sanjiv S. Agarwala, MD
 Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
Management of Brain Metastases Sanjiv S. Agarwala, MD Professor of Medicine Temple University School of Medicine Chief, Oncology & Hematology St. Luke s Cancer Center, Bethlehem, PA, USA Incidence (US):
Timing of targeted therapy in patients with low volume mrcc. Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital
 1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
1 Timing of targeted therapy in patients with low volume mrcc Eli Rosenbaum Davidoff Cancer Center Beilinson Hospital 2 Wont be discussing: Symptomatic patients High volume disease Rapidly growing metastases
Best Practices in the Treatment and Management of Metastatic Melanoma. Melanoma
 Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant
Best Practices in the Treatment and Management of Metastatic Melanoma Philip Friedlander MD PhD Director of Melanoma Medical Oncology Program Assistant Professor Division of Hematology Oncology Assistant
Why Do Axillary Dissection? Nodal Treatment and Survival NSABP B04. Revisiting Axillary Dissection for SN Positive Patients
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA Why Do Axillary Dissection? 6 August 2011 Implications
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA Why Do Axillary Dissection? 6 August 2011 Implications
New paradigms for treating metastatic melanoma
 New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
New paradigms for treating metastatic melanoma Paul B. Chapman, MD Melanoma Clinical Director Melanoma and Immunotherapeutics Service Memorial Sloan Kettering Cancer Center, New York 20 th Century Overall
The Really Important Questions Current Immunotherapy Trials are Not Answering
 The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
The Really Important Questions Current Immunotherapy Trials are Not Answering David McDermott, MD Beth Israel Deaconess Medical Center Dana Farber/Harvard Cancer Center Harvard Medical School PD-1 Pathway
Clinical Case Conference Melanoma
 Clinical Case Conference Melanoma Epidemiology ~60,000 cases and 8,000 deaths per year in US Caucasian:African American = 10:1 15% arise from existing nevi 91% are cutaneous 15% are LN+ at presentation
Clinical Case Conference Melanoma Epidemiology ~60,000 cases and 8,000 deaths per year in US Caucasian:African American = 10:1 15% arise from existing nevi 91% are cutaneous 15% are LN+ at presentation
Innovations in Immunotherapy - Melanoma. Systemic Therapies October 27, 2018 Charles L. Bane, MD
 Innovations in Immunotherapy - Melanoma Systemic Therapies October 27, 2018 Charles L. Bane, MD Melanoma Prognosis Survival at 10 years Stage I: 90% Stage II: 60% Stage III: 40% Stage IV: 10% 2 Indications
Innovations in Immunotherapy - Melanoma Systemic Therapies October 27, 2018 Charles L. Bane, MD Melanoma Prognosis Survival at 10 years Stage I: 90% Stage II: 60% Stage III: 40% Stage IV: 10% 2 Indications
Approaches To Treating Advanced Melanoma
 Approaches To Treating Advanced Melanoma Suraj Venna, MD Medical Director, Melanoma and Cutaneous Oncology Inova Schar Cancer Institute Associate Professor, VCU Fairfax VA Disclosures No relevant disclosures
Approaches To Treating Advanced Melanoma Suraj Venna, MD Medical Director, Melanoma and Cutaneous Oncology Inova Schar Cancer Institute Associate Professor, VCU Fairfax VA Disclosures No relevant disclosures
Implications of ACOSOG Z11 for Clinical Practice: Surgical Perspective
 Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA 6 August 2011 Implications of ACOSOG Z11 for Clinical
Memorial Sloan-Kettering Cancer Center 1275 York Avenue, New York, NY 10065 10th International Congress on the Future of Breast Cancer Coronado, CA 6 August 2011 Implications of ACOSOG Z11 for Clinical
CheckMate 012: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer
 CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
CheckMate 12: Safety and Efficacy of First Line Nivolumab and Ipilimumab in Advanced Non-Small Cell Lung Cancer Abstract 31 Hellmann MD, Gettinger SN, Goldman J, Brahmer J, Borghaei H, Chow LQ, Ready NE,
Viewpoint from a health care professional
 Viewpoint from a health care professional Christoph Hoeller Skin Cancer Center at the Department of Dermatology Medical University of Vienna Austria Certified Skin Tumor Center The fifth annual regulatory
Viewpoint from a health care professional Christoph Hoeller Skin Cancer Center at the Department of Dermatology Medical University of Vienna Austria Certified Skin Tumor Center The fifth annual regulatory
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy. Julia White MD Professor, Radiation Oncology
 Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Radiotherapy Management of Breast Cancer Treated with Neoadjuvant Chemotherapy Julia White MD Professor, Radiation Oncology Agenda Efficacy of radiotherapy in the management of breast cancer in the Adjuvant
Melanoma 10/12/18 Justin J. Baker, M.D.
 Objectives Review Incidence Risk Factors for Development Detection 10/12/18 Justin J. Baker, M.D. Treatment of Surgery Medicine Radiation What is Incidence Cancer of Melanocytes Melanocytes are normal
Objectives Review Incidence Risk Factors for Development Detection 10/12/18 Justin J. Baker, M.D. Treatment of Surgery Medicine Radiation What is Incidence Cancer of Melanocytes Melanocytes are normal
Sentinel Lymph Node Biopsies in Cutaneous Melanoma: A systematic review of the literature. Sasha Jenkins
 Sentinel Lymph Node Biopsies in Cutaneous Melanoma: A systematic review of the literature By Sasha Jenkins A Master s Paper submitted to the faculty of the University of North Carolina at Chapel Hill in
Sentinel Lymph Node Biopsies in Cutaneous Melanoma: A systematic review of the literature By Sasha Jenkins A Master s Paper submitted to the faculty of the University of North Carolina at Chapel Hill in
Morphological characteristics of the primary tumor and micrometastases in sentinel lymph nodes as a predictor of melanoma progression
 Morphological characteristics of the primary tumor and micrometastases in sentinel lymph nodes as a predictor of melanoma progression M.N. Kukushkina, S.I. Korovin, O.I. Solodyannikova, G.G. Sukach, A.Yu.
Morphological characteristics of the primary tumor and micrometastases in sentinel lymph nodes as a predictor of melanoma progression M.N. Kukushkina, S.I. Korovin, O.I. Solodyannikova, G.G. Sukach, A.Yu.
ASCO 2014: The Future is Here. What I Will Talk About. George W. Sledge MD Stanford University School of Medicine
 ASCO 214: The Future is Here George W. Sledge MD Stanford University School of Medicine What I Will Talk About Two paths to a Cure Slicing the pie MelMng the snowflake The Past Isn t Dead Improving PaMent
ASCO 214: The Future is Here George W. Sledge MD Stanford University School of Medicine What I Will Talk About Two paths to a Cure Slicing the pie MelMng the snowflake The Past Isn t Dead Improving PaMent
AJCC 8 Implementation January 1, 2018 Melanoma of the Skin. Suraj Venna
 AJCC 8 Implementation January 1, 2018 Melanoma of the Skin Suraj Venna Personalized Medicine AJCC 8 th Edition This Time It s Personal Traditional AJCC (TNM) population-based analyses of large databases
AJCC 8 Implementation January 1, 2018 Melanoma of the Skin Suraj Venna Personalized Medicine AJCC 8 th Edition This Time It s Personal Traditional AJCC (TNM) population-based analyses of large databases
Nivolumab for adjuvant treatment of resected stage III and IV melanoma [ID1316] STA Lead team presentation: Cost Effectiveness Part 1
![Nivolumab for adjuvant treatment of resected stage III and IV melanoma [ID1316] STA Lead team presentation: Cost Effectiveness Part 1](/thumbs/89/99008516.jpg "Nivolumab for adjuvant treatment of resected stage III and IV melanoma [ID1316] STA Lead team presentation: Cost Effectiveness Part 1") For public no AIC or CIC Nivolumab for adjuvant treatment of resected stage III and IV melanoma [ID1316] STA Lead team presentation: Cost Effectiveness Part 1 1st Appraisal Committee meeting Committee
For public no AIC or CIC Nivolumab for adjuvant treatment of resected stage III and IV melanoma [ID1316] STA Lead team presentation: Cost Effectiveness Part 1 1st Appraisal Committee meeting Committee
Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer
 - Official Statement - Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer Sentinel lymph node (SLN) biopsy has replaced axillary lymph node dissection (ALND) for the
- Official Statement - Position Statement on Management of the Axilla in Patients with Invasive Breast Cancer Sentinel lymph node (SLN) biopsy has replaced axillary lymph node dissection (ALND) for the
Locally Advanced and Metastatic Melanoma. Relevant disclosures 6/23/2018. What is the median survival of metastatic melanoma? Abel D.
 Locally Advanced and Metastatic Melanoma Abel D. Jarell, MD, FAAD Adjunct Dartmouth School of Medicine, Hanover, NH Northeast Dermatology Associates, Portsmouth, NH Relevant disclosures What is the median
Locally Advanced and Metastatic Melanoma Abel D. Jarell, MD, FAAD Adjunct Dartmouth School of Medicine, Hanover, NH Northeast Dermatology Associates, Portsmouth, NH Relevant disclosures What is the median
Dr Rosalie Stephens. Mr Richard Martin. Medical Oncologist Auckland City Hospital Auckland
 Dr Rosalie Stephens Medical Oncologist Auckland City Hospital Auckland Mr Richard Martin General Surgeon Melanoma Unit Team Waitemata District Health Board Auckland 8:30-9:25 WS #99: Interactive Case Studies
Dr Rosalie Stephens Medical Oncologist Auckland City Hospital Auckland Mr Richard Martin General Surgeon Melanoma Unit Team Waitemata District Health Board Auckland 8:30-9:25 WS #99: Interactive Case Studies
Update on Lymph Node Management in Melanoma
 Update on Lymph Node Management in Melanoma John T. Vetto MD, FACS Professor of Surgery Division of Surgical Oncology Oregon Health & Science University Portland, Oregon Lymph Nodes in Melanoma Outline
Update on Lymph Node Management in Melanoma John T. Vetto MD, FACS Professor of Surgery Division of Surgical Oncology Oregon Health & Science University Portland, Oregon Lymph Nodes in Melanoma Outline
Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival
 MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
MOLECULAR AND CLINICAL ONCOLOGY 7: 1083-1088, 2017 Patient age and cutaneous malignant melanoma: Elderly patients are likely to have more aggressive histological features and poorer survival FARUK TAS
16/09/2015. ACOSOG Z011 changing practice. Presentation outline. Nodal mets #1 prognostic tool. Less surgery no change in oncologic outcomes
 ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
ACOSOG Z011 changing practice The end of axillary US/FNA? Preoperative staging of the axilla in the era of Z011 Adena S Scheer MD MSc FRCSC Surgical Oncologist, St. Michael s Hospital Assistant Professor,
Talk to Your Doctor. Fact Sheet
 Talk to Your Doctor Hearing the words you have skin cancer is overwhelming and would leave anyone with a lot of questions. If you have been diagnosed with Stage I or II cutaneous melanoma with no apparent
Talk to Your Doctor Hearing the words you have skin cancer is overwhelming and would leave anyone with a lot of questions. If you have been diagnosed with Stage I or II cutaneous melanoma with no apparent
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón
 Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Tratamiento Multidisciplinar de Estadios Localmente Avanzados en Cáncer de Pulmón Santiago Ponce Aix Servicio Oncología Médica Hospital Universitario 12 de Octubre Madrid Stage III: heterogenous disease
Prognosis of Sentinel Node Staged Patients with Primary Cutaneous Melanoma
 Prognosis of Sentinel Node Staged Patients with Primary Cutaneous Melanoma Otmar Elsaeßer 1., Ulrike Leiter 1 *., Petra G. Buettner 2, Thomas K. Eigentler 1, Friedegund Meier 1, Benjamin Weide 1, Gisela
Prognosis of Sentinel Node Staged Patients with Primary Cutaneous Melanoma Otmar Elsaeßer 1., Ulrike Leiter 1 *., Petra G. Buettner 2, Thomas K. Eigentler 1, Friedegund Meier 1, Benjamin Weide 1, Gisela
Immunotherapy for the Treatment of Head and Neck Cancers. Robert F. Taylor, MD Aurora Health Care
 Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Immunotherapy for the Treatment of Head and Neck Cancers Robert F. Taylor, MD Aurora Health Care Disclosures No relevant financial relationships to disclose I will be discussing non-fda approved indications
Lymph node ratio is an important and independent prognostic factor for patients with stage III melanoma.
 Thomas Jefferson University Jefferson Digital Commons Department of Surgery Faculty Papers Department of Surgery 1-1-2012 Lymph node ratio is an important and independent prognostic factor for patients
Thomas Jefferson University Jefferson Digital Commons Department of Surgery Faculty Papers Department of Surgery 1-1-2012 Lymph node ratio is an important and independent prognostic factor for patients
Printed by Martina Huckova on 10/3/2011 3:04:54 PM. For personal use only. Not approved for distribution. Copyright 2011 National Comprehensive
 Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level
Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment. Justin Rivard MD, MSc, FRCSC September 21, 2018
 You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
Epithelial Cancer- NMSC & Melanoma
 Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Epithelial Cancer- NMSC & Melanoma David Chin MB, BCh, BAO, LRCP, LRCS (Ireland) MCh(MD), PhD (UQ), FRCS, FRACS (Plast) Plastic & Reconstructive Surgeon Visiting Scientist Melanoma Genomic Group & Drug
Evolution of Regional Nodal Management of Breast Cancer
 Evolution of Regional Nodal Management of Breast Cancer Bruce G. Haffty, MD Director (Interim) Rutgers Cancer Institute of New Jersey Professor and Chair Department of Radiation Oncology Rutgers, The State
Evolution of Regional Nodal Management of Breast Cancer Bruce G. Haffty, MD Director (Interim) Rutgers Cancer Institute of New Jersey Professor and Chair Department of Radiation Oncology Rutgers, The State
Melanoma. Kaushik Mukherjee MD A. Scott Pearson MD
 Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes. Disclosures
 Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
Evolving Treatment Strategies in the Management of Metastatic Melanoma: Novel Therapies for Improved Patient Outcomes Fall Managed Care Forum November 11, 2016 Matthew Taylor, M.D. Disclosures Consulting/Advisory
Impact of Prognostic Factors
 Melanoma Prognostic Factors: where we started, where are we going? Impact of Prognostic Factors Staging Management Surgical intervention Adjuvant treatment Suraj Venna, MD Assistant Clinical Professor,
Melanoma Prognostic Factors: where we started, where are we going? Impact of Prognostic Factors Staging Management Surgical intervention Adjuvant treatment Suraj Venna, MD Assistant Clinical Professor,
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R
 Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Neoadjuvant Nivolumab in Early-Stage, Resectable Non-Small Cell Lung Cancers
 Neoadjuvant Nivolumab in Early-Stage, Resectable Non-Small Cell Lung Cancers Abstract 8508 Chaft JE, Forde PM, Smith KN, Anagnostou V, Cottrell TR, Taube JM, Rekhtman N, Merghoub T, Jones DR, Hellmann
Neoadjuvant Nivolumab in Early-Stage, Resectable Non-Small Cell Lung Cancers Abstract 8508 Chaft JE, Forde PM, Smith KN, Anagnostou V, Cottrell TR, Taube JM, Rekhtman N, Merghoub T, Jones DR, Hellmann
Neoadjuvant Treatment of. of Radiotherapy
 Neoadjuvant Treatment of Breast Cancer: Role of Radiotherapy Neoadjuvant Chemotherapy Many new questions for radiation oncology? lack of path stage to guide indications should treatment response affect
Neoadjuvant Treatment of Breast Cancer: Role of Radiotherapy Neoadjuvant Chemotherapy Many new questions for radiation oncology? lack of path stage to guide indications should treatment response affect
STAGE CATEGORY DEFINITIONS
 CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c
CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c