Theragnostics Neuroendocrine and Prostate Cancer
|
|
|
- Gervais Scott Lester
- 5 years ago
- Views:
Transcription
1 Theragnostics Neuroendocrine and Prostate Cancer
2 Target Audience: Pharmacists ACPE#: L01-P Activity Type: Knowledge-based Target Audience: ACPE#: Activity Type:
3 Disclosures Financial: Employed by Advanced Accelerator Applications (AAA) / Novartis The American Pharmacists Association is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education.
4 Learning Objectives 1. To understand clinical indications and utilization of 68Ga - DOTATATE imaging in NETs 2. To understand clinical indications and utilization of 177 Lu- DOTATATE Target Audience: therapy in NETs 3. To understand potential clinical benefits and research ACPE#: applications of 177 Lu-PSMA 4. To understand benefits of Theragnostics in NM space Activity Type:






5 Impact of Theragnostics Patients Physicians Payors More effective care through personalized interventions Reduce or eliminate unnecessary treatment Better diagnose and stage disease Select optimal therapies Monitor treatment response and disease progression Reduce costs from unnecessary treatments Improve patient management & outcomes 5







6 Improving Patient Management through Unique Theragnostic Platform Same Targeting Molecule Ga-68 labeled Ga-68 PET Lu-177 labeled Lu-177 PRRT / RLT Diagnosis Selection for PRRT / RLT or other treatment Follow-up ELECTRONS TREAT TUMORS FROM WITHIN GAMMA RAYS DETECTED BY PET/CT CAMERA PRRT = Peptide Receptor Radionuclide Therapy RLT = RadioLigand Therapy 6
7 Oncology Theragnostics Pipeline Product Indications Preclinical Phase I Phase II Phase III Filing Marketed Status Lutetium Lu 177 dotatate* Neuroendocrine tumors Therapeutic Phase III Netter-1 study in NETs Orphan Drug Designation Approved in EU for GEP-NETs NDA in US under review Ga-68 dotatate/ edotreotide Neuroendocrine tumors NETSPOT : PET Diagnostic SOMAKIT-TOC : PET Diagnostic PET diagnostics for localization of NETs Orphan Drug Designation Approved in US and EU 177Lu PSMA-R2 Prostate cancer Therap. Exclusive license from John s Hopkins for series of candidates in prostate cancer Clinical studies planned for Ga PSMA-R2 Prostate cancer PET Diag. Exclusive license from John s Hopkins for series of candidates in prostate cancer Clinical studies planned for Lu NeoBOMB1 GIST Prostate cancer Breast cancer Therapeutic GRPR antagonist Exclusive license from Erasmus MC and Demokritos University Clinical studies planned in GIST, BC and PC 68Ga NeoBOMB1 GIST Prostate cancer Breast cancer PET Diagnostic * USAN lutetium Lu 177 dotatate / INN: lutetium ( 177 Lu) oxodotreotide GRPR antagonist Exclusive license from Erasmus MC and Demokritos University Clinical studies planned in GIST, BC and PC 7
")
8 Neuroendocrine Tumors (NETs) 8

9 9 Neuroendocrine tumors (NETs) are a heterogeneous group of relatively rare tumors1 NETs consist of a spectrum of malignancies that can arise from neuroendocrine cells throughout the body NETs may be grouped according to the embryologic origin of the primary site: Foregut: respiratory tract, stomach, duodenum, biliary system, and pancreas Midgut: small bowel, appendix, cecum, and proximal colon Hindgut: distal colon and rectum 1 Alexandraki, K.I., et al.; Endocrine 2012, 41,

10 10 GI tract and pancreas are the most frequent localizations of NETs1 Neuroendocrine cells are widely distributed throughout the body NETS can appear in almost every organ or tissue The most frequent localization is the digestive system followed by bronchopulmonary NETs, including thymus and then unknown origin 1Dasari A, et al. JAMA Oncol. 2017
11 11 NETs have historically been considered as rare tumors Incidence has been increasing (>600% over the last 4 decades) and NETs are now the second most prevalent gastrointestinal cancer after colon cancer; more prevalent than pancreatic, gastric, esophageal or hepatic cancer or any two of these combined 1Dasari A, et al. JAMA Oncol. 2017
12 NETs are Heterogeneous EXTENT OF DISEASE Low tumor burden/resectable Widely metastatic High tumor burden/unresectable Liver dominant PACE OF GROWTH Stable Progressive PRIMARY SITE Foregut Midgut Hindgut Pancreas GRADE / DIFFERENTIATION Low-grade Int.-grade High-grade Well diff. Poorly diff. HORMONE STATUS Functional Non-Functional SSTRs High expression Low/absent expression 12

13 13 Delayed Diagnosis Results in Most Patients Being Metastatic Upon Diagnosis1 60% of NETs are non-functioning or asymptomatic Metastatic disease is increasingly prevalent in GI-NETs and PNETs At initial diagnosis, 40-50% of patients present with metastases 1Alexandraki, K.I., et al.; Endocrine 2012, 41,
14 14 NETs pose high morbidity burden on patients and survival rates have not increased with current treatments GEP-NETs constitute a lifethreatening disease and are associated with debilitating clinical symptoms 1,2 5-Year Survival Among Various NET Tumors, SEER (Lawrence et al. 2011) A recent survey of oncologists reported that nearly one third of patients were managed by watch and wait, also indicative of the unmet need in this disease state 3 Percent Kanakis and Kaltsas Pape et al Casciano 2013

15 15 Treatment Options for NETs are Dependent on diagnosis and Extent of Disease Somatostatin Analogues (SSA): SSAs are synthetic forms of somatostatin They bind to the somatostatin receptors (SSTRs) overexpressed by NETs Like somatostatin, they inhibit hormone release by the target cells, resulting in symptoms relief 80% of NETs overexpress SSTRs Some guidelines may recommend SSAs for NETs symptom control or as antiproliferative therapy Inhibitors of mammalian target of Rapamycin (mtor): Everolimus: adults with progressive neuroendocrine tumors of pancreatic origin (PNET) and adults with progressive, well-differentiated, non-functional neuroendocrine tumors (NET) of gastrointestinal (GI) or lung origin that are unresectable, locally advanced or metastatic. Not indicated for the treatment of patients with functional carcinoid tumors. Tyrosine kinase inhibitors (TKIs): Sunitinib: progressive, well-differentiated pancreatic neuroendocrine tumors (pnet) in patients with unresectable locally advanced or metastatic disease. Surgery: Only curative treatment, mainly used in grade 1 or grade 2 Radiofrequency ablation: Can relieve symptoms in 70% of cases for approximately 1 year and provide local liver control in most patients Radioembolization and chemo-embolization: Recommended as 1st line treatment in patients with progressive or symptomatic tumors of midgut origin if metastases are confined to the liver and 2nd line treatment for liver metastases of PNETs
16 Diagnostic Challenges NETs Heterogeneous No unique and specific clinical presentation (vague symptoms) Diagnosis is often delayed by 5-7 years 1 60 to 70% of patients have metastatic diseases at diagnosis 1 Diagnosis is complex and multimodal based on 2 Clinical symptoms (non-functioning vs functioning tumors) Biological Markers Specific: 5-HIAA, PNETS hormones Non specific: Chromogranins, Neuron Specific Enolase Pathology (differentiation, proliferation, primary) Imaging (primary location, staging) 1. Alexandraki & Kaltsas Endocrine 2012, 41: 40-52; 2. Oberg Exp Rev Endocrinol Metab 2011, 6 (1):
17 Non-Functioning NETs The majority of NETs are non-functioning GEP-NETs No specific clinical symptoms related to a specific secretion Either truly non-functional or the secretion is not clinically relevant Tumors can be asymptomatic until their volume provokes mass effects Pain, discomfort, anorexia, weight loss, jaundice Late diagnosis Intestinal NETs are often revealed by non-specific abdominal pain or emergency clinical presentations Obstruction / Perforation / Bleeding Late diagnosis due to aspecific, misleading symptoms (different for lung NETs) 17
18 Functioning NETs (Carcinoid Syndrome) The carcinoid syndrome is the most typical clinical manifestation of GEP NETs: 1,2 Diarrhea (60-80%) 1, Flushing (60-85%) 1, Abdominal pain, Sweating, Bronchial wheezing (due to bronchospasm: pseudo-asthma) 10% 1 Due to the release and interaction of hormones (that have effects on intestinal motility (diarrhea) and on vasoconstriction), mainly 2 Serotonin, Prostaglandins, Histamine, Tachykinins Serotonin (5-HT), derived from the amino acid tryptophan, is stored and secreted by some NE cells; it is inactivated in the liver into 5- hydroxyindoleacetic acid (5-HIAA) 2 1. Pape et al. Neuroendocrinology 2012, 95: ; 2.Strosberg Best Practice & Research Clinical Gastroenterology 2012, 26:
: Overexpressed in Most NETs, but most commonly in")

19 Somatostatin Receptor Imaging Somatostatin Regulatory peptide widely distributed in the human body, nervous system and GI track Somatostatin receptors (SSTRs): Overexpressed in Most NETs, but most commonly in gastro-enteropancreatic neuroendocrine tumors (GEP-NETs), including foregut, midgut, and hindgut NETs Other tumors express somatostatin receptors: pituitary adenoma, meningioma, paraganglioma, small cell lung cancer, MTC
 111 In-pentetreotide (OctreoScan )")
20 Somatostatin Receptor Imaging Synthetic Somatostatin analogs (SSAs): 1 st line treatment is Octreotide Radioactive Labeled Somatostatin Analogs: 68 Ga-dotatate (NETSPOT ) 111 In-pentetreotide (OctreoScan ) 20
21 NETSPOT Indications NETSPOT after radiolabeling with Ga 68, is a radioactive diagnostic agent indicated for use with positron emission tomography (PET) for localization of somatostatin receptor positive neuroendocrine tumors (NETs) in adult and pediatric patients 1 Initial staging for patients with neuroendocrine tumors Restaging, detecting recurrence, and monitoring of response to therapy in patients with NETs Detection of unknown primary neuroendocrine tumor in patients with known metastatic NETs 1 NETSPOT Prescribing Information 2016
22 Reconstitution Procedure 22


23 Normal Biodistribution sstr2 expressing organs Higher uptake pituitary, thyroid, spleen, adrenals, kidney, pancreas, prostate, liver, and salivary glands Lower uptake thymus and lung No uptake cerebral cortex or in the heart 111In- pentetreotide 68Ga-dotatate



24 Examples of Functional Imaging and MRI Primary tumor in the terminal ileum (green arrows). Liver metastases not visible on 111In-pentreotide scan. 111In-Pentetreotide 68Ga-DOTATATE PET/CT MRI 24
25 Clinical Studies w/ Impact on Patient Management and Change in Outcome Safety and Efficacy of 68Ga-DOTATATE PET/CT for Diagnosis, Staging and Treatment Management of Neuroendocrine Tumors. Deppen SA, et al. J Nucl Med May;57(5): Prospective Study of 68Ga-DOTATATE Positron Emission Tomography/Computed Tomography for Detecting Gastro-Entero-Pancreatic Neuroendocrine Tumors and Unknown Primary Sites. Sadowski SM, et al. J Clin Oncol. 2015; 34: Impact of 68Ga-DOTATATE PET/CT on the Management of Neuroendocrine Tumors: The Referring Physician s Perspective Herrmann K, et al. The J. of Nuclear Medicine. 2015, 56(1): The Role of 68 Ga-DOTATATE PET in Patients with Neuroendocrine Tumors and Negative or Equivocal Finding on 111 In-DTPA-Octreotide Scintigraphy. Srirajaskanthan R, et al. J Nucl Med 2010 June;51(6): Prospective Study of 68Ga-DOTATATE Positron Emission Tomography/Computed Tomography for Detecting Gastro-Entero-Pancreatic Neuroendocrine Tumors and Unknown Primary Sites. Sadowski SM, et al. J Clin Oncol. 2015; 34: High management impact of Ga-68 DOTATATE(GaTate) PET/CT for imaging neuroendocrine and other somatostatin expressing tumours. Hofman MS, et al. J of Med Imaging and Rad Onc 56(2012): Impact of 68 Ga-DOTATATE PET-CT on the surgical management of primary neuroendocrine tumors of the pancreas or ileum. Ilhan H, et al. Ann Surg Oncol. (2015) 22:
26 Peptide Receptor Radionuclide Therapy (PRRT) 26
27 Peptide Receptor Radionuclide Therapy (PRRT) PRRT involves the systemic administration of a specific radiopharmaceutical to deliver cytotoxic radiation to a tumor1 The radiopharmaceutical is composed of a β- emitting radionuclide, chelated to a peptide1 The peptide is designed to target cell surface receptors, such as somatostatin receptors1 Structure of a radiopharmaceutical2 The affinity for SSTRs and the specificity of binding ensures a high level of specificity in the delivery of radiation to the tumor 1. Zaknun et al. Eur J Nucl Med Mol Imaging 2013, 40: Bergsma et al. Best Practice & Res Clin Gastroenterol 2012, 26:
28 Efficacy of PRRT Tumor response (%) in patients with GEP NETs treated with PRRT Study Ligand n CR+PR SD PD Valkema In-DTPA-octreotide Anthony In-DTPA-octreotide Bodei Y-DOTATOC Waldherr Y-DOTATOC Waldherr Y-DOTATOC Valkema Y-DOTATOC Bushnell Y-DOTATOC Pfeifer Y-DOTATOC Cwikla Y-DOTATATE Kwekkeboom Lu-DOTATATE Sward Lu-DOTATATE Garkavij Lu-DOTATATE Bodei Lu-DOTATATE Van der Zwan et al. Eur J Endocrinology,2015, 172: R1-8 28
29 lutetium Lu 177 dotatate Binds specifically to malignant cells that overexpress sstr2 receptors The clearance through the kidney pathway is rapid: on average 70% of the administered radioactivity is found in the urine at 24h β-emitting radionuclide - Intermediate energy with beta particle Decays with a half-life of 6.7 days Pathway penetration of 2 mm Low abundance gamma ray, which permits diagnostic imaging
, including foregut, midgut, and hindgut neuroendocrine tumors in adults. 1 Contraindication: None. 1 1 LUTATHERA [prescribing information].")
30 30 lutetium Lu 177 dotatate is the First Approved Peptide Receptor Radionuclide Therapy (PRRT) for NETs 1 Indication: LUTATHERA is indicated for the treatment of somatostatin receptor-positive gastroenteropancreatic neuroendocrine tumors (GEP-NETs), including foregut, midgut, and hindgut neuroendocrine tumors in adults. 1 Contraindication: None. 1 1 LUTATHERA [prescribing information]. January 2018.

31 31 Structure of lutetium Lu 177 dotatate lutetium Lu 177 dotatate is a molecularly targeted radiation therapy that involves the systemic administration of a radiolabeled peptide designed to target specific cell surface receptors with high affinity and specificity 1 Structure of lutetium Lu 177 dotatate 1 LUTATHERA [prescribing information]. January 2018.



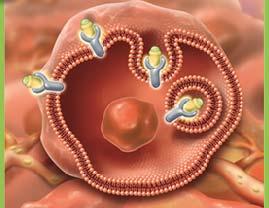
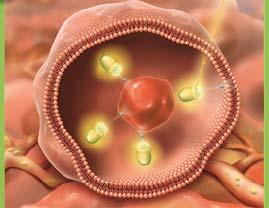
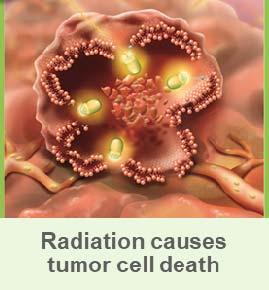
32 32 Lutetium Lu 177 Dotatate Delivers Cytotoxic Radiation1 1LUTATHERA [prescribing information]. January 2018.
33 33 Lutetium Lu 177 Dotatate Administration 1 LUTATHERA [prescribing information]. January 2018.
 is administered as an intravenous infusion over")
 1LUTATHERA [prescribing information].")
34 34 Lutetium Lu 177 Dotatate Treatment Regimen1 LUTATHERA (200 mci) is administered as an intravenous infusion over minutes every 8 weeks for a total of 4 doses (4 x 200 mci = 800 mci) 1LUTATHERA [prescribing information]. January 2018.
35 NETTER-1 (Phase III) A multicentre, stratified, open, randomized, comparator-controlled, parallel-group phase III study comparing treatment with 177 Lu-DOTA0-Tyr3-Octreotate to Octreotide LAR in patients with inoperable, progressive, somatostatin receptor positive, midgut carcinoid tumours 35


36 36 NETTER-1: International, multicenter, randomized, comparatorcontrolled, parallel-group Phase III study 1 1 Strosberg J, et al. N Engl J Med. 2017; 376:


37 37 NETTER-1: Inclusion and Exclusion Criteria1 1Strosberg J, et al. N Engl J Med. 2017; 376:
38 NETTER-1 Phase III: Study Endpoints Primary objective Compare Progression Free Survival (PFS) after treatment with lutetium Lu 177 dotatate plus 30 mg octreotide LAR (symptoms control) vs treatment with high dose (60 mg) octreotide LAR Secondary objectives Compare the Objective Response Rate between study arms Compare the Overall Survival between study arms Compare the Time to Progression between study arms Evaluate the safety and tolerability of lutetium Lu 177 dotatate Evaluate the health related quality of life (QoL) as measured by the EORTC QLQ-G.I.NET21 questionnaire 38
39 Dose Modifying Toxicity Patients who completed Tx phase, N=103* Nb of Patients (%) Number of administrations 4 79 (77%) 3 6 (6%) 2 12 (12%) 1 5 (5%) 0 1 (1%) All treated patients, N=111 Nb of Patients (%) Dose modifying toxicity No DMT 103 (93%) DMT 8 (7%) (*) without patients still under treatment (n=8) or no treatment 39

40 40 NETTER-1: included a well-balanced patient characteristics 1 1 Strosberg J, et al. N Engl J Med. 2017; 376:


41 Lu 177 dotatate demonstrated markedly longer progression-free survival 1 41 Median PFS for lutetium Lu 177 dotatate was not reached Median PFS for long acting octreotide 60 mg was 8.5 months PFS Events Lutetium Lu 177 dotatate = 27 events Octreotide LAR 60 mg = 78 events Indicates 79% risk reduction for disease progression or death (HR 0.21 [95% CI, 0.13, 0.32], P<0.0001) 1 1 LUTATHERA [prescribing information]. January 2018.
 2 Lutetium Lu 177 dotatate = 27 deaths Octreotide LAR 60 mg = 43 deaths O'Brian Fleming threshold for statistical significance at first interim analysis = 0.")
42 42 Preliminary Evidence Suggests an Overall Survival Benefit 1 Interim OS analysis showed a 48% reduction in estimated risk of death (HR 0.52; 95% CI, ) 2 Lutetium Lu 177 dotatate = 27 deaths Octreotide LAR 60 mg = 43 deaths O'Brian Fleming threshold for statistical significance at first interim analysis = Data not sufficiently mature to provide estimation of median OS in either arm 2 1 LUTATHERA [prescribing information]. January Strosberg J, et al. N Engl J Med. 2017; 376:

 Tumor grade Age Gender Tumor marker levels 1Strosberg J, et al. N Engl J Med.")
43 43 Lu 177 dotatate demonstrated consistent benefits across stratification and prognostic factors2 Consistent treatment benefits with Lu 177 dotatate were observed irrespective of stratification and prognostic factors, including: Levels of radiotracer uptake on somatostatin receptor scintigraphy (SRS) Tumor grade Age Gender Tumor marker levels 1Strosberg J, et al. N Engl J Med. 2017; 376:
 1 Notable given that response rates above 5% have not been observed in large randomized clinical trials of other systemic therapies in this patient population 2 1 LUTATHERA [prescribing")
44 44 Lu 177 dotatate demonstrated 3X greater ORR than Octreotide LAR 60 mg The response rate was 13% in the Lu 177 dotatate group compared with 4% in the Octreotide LAR 60 mg control group (P=0.0148) 1 Notable given that response rates above 5% have not been observed in large randomized clinical trials of other systemic therapies in this patient population 2 1 LUTATHERA [prescribing information]. January Strosberg J, et al. N Engl J Med. 2017; 376:
45 NETTER-1 Safety and Tolerability 2 Lu 177 dotatate and Octreotide LAR 30 mg (n=111) Octreotide LAR 60 mg (n=110) Any adverse event 106 (96%) 95 (86%) Related to treatment 95 (86%) 34 (31%) Serious adverse events 29 (26%) 26 (24%) Related to treatment 10 (9%) 1 (1%) Withdrawals due to adverse events 7 (6%) 10 (9%) Related to treatment 5 (5%) 0 (0%) 1 Strosberg J, et al. N Engl J Med. 2017; 376:
![46 Lu 177 Dotatate Demonstrated Limited Acute Side Effects1 1LUTATHERA [prescribing information]. January 2018.](/docs-images/82/86466525/images/46-5.jpg "Bone marrow toxicity (myelo-/hematotoxicity): reversible / transient reductions in blood counts affecting all lineages Most")

46 46 Lu 177 Dotatate Demonstrated Limited Acute Side Effects1 1LUTATHERA [prescribing information]. January Bone marrow toxicity (myelo-/hematotoxicity): reversible / transient reductions in blood counts affecting all lineages Most common adverse events in Lu 177 dotatate group: nausea and vomiting due to amino acid infusions. Resolved upon completion of the infusions. Adverse events leading to premature withdrawal from the trial: 7 patients (6%) in Lu 177 dotatate group 10 patients (9%) in control group

2 1Strosberg J, et al. N Engl J Med. 2017; 376:125-135 T, et al. Clin Cancer Res. 2017;23(16):4617-4624.")
47 47 NETTER-1: Hematologic Events Were Transient1 Short term hematologic events (neutropenia, leukopenia, cytopenia, thrombocytopenia) almost always come back to their normal level before the next treatment; patient recovers by the next dose For patients in which this does not occur, there is a well established dose-modification regimen Long term hematologic events (Myelodysplastic syndrome, acute leukemia) were observed in <2% of patients (Phase I/II)2 1Strosberg J, et al. N Engl J Med. 2017; 376: T, et al. Clin Cancer Res. 2017;23(16): Brabander
48 NETTER-1: Grade 3-4 Hepatotoxicity 1 Lu 177 dotatate and Octreotide LAR 30mg (N = 111) Octreotide LAR (N = 110) AST increase 4% 0% ALT increase 4% 0% Bilirubin increase 2% 0% GGT increase (at inclusion respectively 11% and 9%) 18% 13% (CTCAE V4.0; Safety Set) 1 Strosberg J, et al. N Engl J Med. 2017; 376:


49 NETTER-1: Creatinine Clearance1 1Strosberg J, et al. N Engl J Med. 2017; 376:
50 lutetium Lu 177 dotatate Biodistribution and Elimination About 75% of the injected activity cleared from the plasma with a half-life of 5 min in patients with low tumor burden About 90% of the injected activity cleared from the plasma with a half-life of 25 minutes in patients with high tumor burden The clearance is through the kidney pathway; on average, 70% of the administered radioactivity is found in the urine at 24 h The long terminal elimination half-life (2 to 7 days) corresponds to a small percentage of the administered radioactivity (below 1%) 50
51 Time to deterioration (TTD) in HRQoL We present the Quality of Life (QoL) results obtained in the NETTER-1 study comparing treatment with 177 Lu-DOTATATE to Octreotide LAR on the time to clinically relevant change (deterioration) in health related QoL (HRQoL). The method used for this assessment is a time-to-event methodology, where the event is defined as a deterioration in the patient s QoL. Time to QoL deterioration (TTD): Time from randomization to the first QoL deterioration 10 points for each patient in the corresponding domain scale. For each domain a Kaplan-Meier plot was produced showing time to event by treatment arm. Kaplan-Meier methods were used to generate a point estimate of the median time to event with corresponding 95% confidence interval (CI). The main analysis was conducted in the population that comprises all randomized patients as per intent to treat (ITT) principles
52 QoL improvement in NETTER-1 Phase III Trial1 Global Health Status TTD HR 0.406; p= Physical Functioning TTD HR 0.518; p= Strosberg Role Functioning TTD HR 0.580; p= J, et al. QoL Abstract. NANETS
53 QoL improvement in NETTER-1 Phase III Trial1 Diarrhea TTD Pain TTD HR 0.473; p= HR 0.566; p= Strosberg Fatigue TTD HR 0.621; p= J, et al. QoL Abstract. NANETS
54 Phase I/II Long-Term Efficacy, Survival, and Safety of [ 177 Lu-DOTA 0, Tyr 3 ]octreotate in Patients with Gastroenteropancreatic and Bronchial Neuroendocrine Tumors 54
55 Safety and Efficacy data: Patients treated between pts 100 mci 177 Lu- DOTATATE 810 Dutch patients 696 bronchial and GEPNETs 610pts 100mCi treated according to all inc. criteria 443 pts 600 mci 177 Lu- DOTATATE before 2013 Safety analysis Efficacy and survival analysis 55
56 Safety, n=610 Acute Toxicities: CTCAE Grade 3/4: Total hematological toxicities 10% Thrombocytopenia 5% Leukopenia 5% Lymphopenia 50%, 26% at 3 mo f/u, 6% at 30 mo f/u Hemoglobin 4% Aminotransferases (AST, ALT), 3% Creatinine 0.3% Chronic Toxicities Acute Leukemia 0.7%, observed 55 month after first therapy MDS 1.5% (no Hx of alkylating agents), observed 28 months after first therapy Renal failure 1%, most likely unrelated No liver failure 56


57 Efficacy n= month median F/U from first treatment ORR 39% SD 43% PD 12% In patients with midgut and pancreatic NETs with PD at baseline, disease control rate was 84% and 81%, respectively. 57

58 Overall Survival by Primary Tumor Pancreas best survival 58
59 Risk Factors Affecting Survival Risk Factors Elevated ALP Liver metastasis Bone metastasis Extensive Disease Poor KPS Best response: PD 59

60 Erasmus compared to NETTER-1 60
 Number of Patients 850 806 List of EAP sites is available on ClinicalTrials.")
61 61 2,268 patients across 11 countries, including the US, have been treated with Lu 177 dotatate (as of 12/31/2017) 1 US Early Access Program was initiated in institutions enrolled in the Early Access Program (EAP) Number of Patients List of EAP sites is available on ClinicalTrials.gov (ID = NCT ) *Austria, Estonia, Finland, Greece, Portugal, Spain, Switzerland, Denmark United States United Kingdom France Other European Countries* 1 Data on File. Advanced Accelerator Applications 2018
62 Lutathera (Lu-177 Dotatate) Approved by FDA: January, 2018 Approved indications treatment of somatostatin receptor positive gastroenteropancreatic neuroendocrine tumors (GEP- NETs), including foregut, midgut, and hindgut neuroendocrine tumors in adults. 62
63 Oncology Theragnostics Pipeline Product Indications Preclinical Phase I Phase II Phase III Filing Marketed Status Lutetium Lu 177 dotatate* Neuroendocrine tumors Therapeutic Phase III Netter-1 study in NETs Orphan Drug Designation Approved in EU for GEP-NETs NDA in US under review Ga-68 dotatate/ edotreotide Neuroendocrine tumors NETSPOT : PET Diagnostic SOMAKIT-TOC : PET Diagnostic PET diagnostics for localization of NETs Orphan Drug Designation Approved in US and EU 177Lu PSMA-R2 Prostate cancer Therap. Exclusive license from John s Hopkins for series of candidates in prostate cancer Clinical studies planned for Ga PSMA-R2 Prostate cancer PET Diag. Exclusive license from John s Hopkins for series of candidates in prostate cancer Clinical studies planned for Lu NeoBOMB1 GIST Prostate cancer Breast cancer Therapeutic GRPR antagonist Exclusive license from Erasmus MC and Demokritos University Clinical studies planned in GIST, BC and PC 68Ga NeoBOMB1 GIST Prostate cancer Breast cancer PET Diagnostic * USAN lutetium Lu 177 dotatate / INN: lutetium ( 177 Lu) oxodotreotide GRPR antagonist Exclusive license from Erasmus MC and Demokritos University Clinical studies planned in GIST, BC and PC 63
64 Prostate Specific Membrane Antigen (PSMA)
65 Prostate Specific Membrane Antigen (PSMA) NIH Definition A type II membrane protein originally characterized by the murine monoclonal antibody (mab) 7E11-C5.3 and is expressed in all forms of prostate tissue including carcinoma. If combined with the appropriate bifunctional chelate, PSMA could be used to diagnose and/or treat prostate cancer including metastatic disease. Important to maintain specificity of PSMA once the chelate is attached
66 PSMA -Prostate Specific Membrane Antigen The American Cancer Society estimates that each year approximately 161,360 new cases of prostate cancer will be diagnosed and about 26,730 men will die of the disease. -2 nd most common cancer in men Accurate risk assessment both sensitivity and specificity in staging and re-staging is key More effective treatments needed for advanced metastatic disease Prostate Specific Membrane Antigen (PSMA), a transmembrane protein amplified on the surface of >95% of prostate cancer cells. 66
67 PSMA-R2: AAA-PSMA R2 molecule was originally developed by Johns Hopkins University - The US provisional filed on March The patent protects a formulation composed by: A Chelator A linker encompassing the one of Lu-2 (now PSMA-R2) Glu-Urea-Lys PSMA binding moiety AAA is developing PSMA-R2 for both diagnostics ( 68 Ga-PSMA-R2) and therapeutics ( 177 Lu-PSMA-R2) Theragnostics: same chelator (Dota) for both Ga 68 and Lu
68 PSMA R2: Summary of in vitro and in vivo results PSMA R2 - Preclinical development completed In vitro plasma stability: Plasma Levels in human and animal species tested at least 2 hours. In silico log P: liposolubly In vivo biodistribution (%ID/g) for -PSMA-R2: Tumor uptake: at 1h and at 4h Kidney uptake: at 0.5h Tumor-to-kidney Salivary glands uptake Biodistribution data form JHU of 177 Lu-labelled compound is in line with the corresponding 68 Ga-labelled compound In vivo efficacy: Survival of the animals at 70 days, reduction in tumor volume, Complete Tumor Remission and Tumor Recurrence assessed Extended single dose toxicity in rats: 177 Lu--PSMA-R2 : toxicity at doses at least 100 times higher than the one foreseen in human 68 68
69 68Ga-PSMA-R2 Preclinical development completed 68Ga-PSMA-R2 Phase 1 trial is expected to start in 1Q2018 Clinical Plans for 68 Ga-labelled compound: Patients with positive PSMA tumors Metastatic disease, positive lymph nodes (to receive accurate curative surgery) of being treated curatively with radiotherapy - radiotherapy planning Planning change patient management in men with Ready to enter Clinical development Feasibility and site selection completed (4 sites in USA) Phase 1/2 clinical trial to start enrolling soon 69
70 177Lu-PSMA-R2 Has potential to improve outcomes in castrate resistant prostate cancer patients at biochemical recurrence (PSA rise) on 2nd generation anti-androgens after chemotherapy PSMA R2 - Preclinical development completed IND Package submitted Ready to enter Clinical development Higher tumor uptake / higher tumor-to-target organ AUC ratio / higher radiosensitivity of the prostate tumor, which could justify avoiding individual dosimetry and supports the one-dose-fits-all approach and 3 dose regimen Feasibility and site selection completed (~15 sites in USA and EU) Phase 1/2 clinical trial to start enrolling soon Patient selection based on 68 Ga-labelled compound 70
71 NeoBOMB 1
72 NeoBOMB1: Targeting Gastrin-Releasing Peptide Receptors (GRPRs) New generation antagonist bombesin analogue, which binds selectively and with high affinity to GRPRs expressed by several types of tumors (e.g. prostate, breast or gastro-intestinal stromal tumors) GRPRs are considered relevant molecular targets for receptor mediated tumor imaging and treatment. Bombesin antagonists have superior pharmacokinetic and toxicological properties when compared to their agonist counterparts Labeled with suitable radio-metals, NeoBOMB1 can be a high-performance imaging tool for diagnosis and therapy of GRPR-positive malignancies Ongoing Phase I/IIa MITIGATE study in patients with advanced TKI-treated gastrointestinal stromal tumors (GIST) 72
73 NeoBOMB1 Clinical Plans for 68 Ga-labelled compound Basket Phase 2 clinical trial starting soon (EU) Clinical Plans for 177 Lu-labelled compound Basket Phase 1a/b clinical trial starting soon (EU) 73
74 The Ga 68 Kit Approach Cold Kit approach PSMA-R2, NeoBOMB1 is the same as NETSPOT Utilizes the eluate of commercially available Ga-68 generators directly, without the need for complex synthesis apparatus Same Distribution NETWORK 74
75 Thank You!
76 1. Assessment Question 1. What is an approved indication for Lu-177 DOTATATE in the United States? A. Metastatic Target Audience: cancer to the liver. B. Treatment of somatostatin receptor-positive GEP-NETs C. Metastatic ACPE#: neuroendocrine cancer to bone D. Endocrine blight Activity Type:
77 2. Assessment Question 2. PSMA with an appropriate chelate could be used to treat: A. Metastatic Target Audience: melanoma refractory to chemotherapy B. Primary and metastatic malignant bladder cancer C. Metastatic ACPE#: malignant substantial glioma D. Primary and metastatic prostate cancer Activity Type:
Neuroendocrine Tumors Positron Emission Tomography (PET) Imaging and Peptide Receptor Radionuclide Therapy
 Imaging and Peptide Receptor Radionuclide Therapy") Neuroendocrine Tumors Positron Emission Tomography (PET) Imaging and Peptide Receptor Radionuclide Therapy Lawrence Saperstein, M.D. Assistant Professor of Radiology and Biomedical Imaging Chief, Nuclear
Neuroendocrine Tumors Positron Emission Tomography (PET) Imaging and Peptide Receptor Radionuclide Therapy Lawrence Saperstein, M.D. Assistant Professor of Radiology and Biomedical Imaging Chief, Nuclear
PRESS RELEASE. Advanced Accelerator Applications Receives US FDA Approval for LUTATHERA for Treatment of Gastroenteropancreatic Neuroendocrine Tumors
 PRESS RELEASE Advanced Accelerator Applications Receives US FDA Approval for LUTATHERA for Treatment of Gastroenteropancreatic Neuroendocrine Tumors First-in-class Therapy Demonstrated 79% Improvement
PRESS RELEASE Advanced Accelerator Applications Receives US FDA Approval for LUTATHERA for Treatment of Gastroenteropancreatic Neuroendocrine Tumors First-in-class Therapy Demonstrated 79% Improvement
Prior Authorization Review Panel MCO Policy Submission
 Prior Authorization Review Panel MCO Policy Submission A separate copy of this form must accompany each policy submitted for review. Policies submitted without this form will not be considered for review.
Prior Authorization Review Panel MCO Policy Submission A separate copy of this form must accompany each policy submitted for review. Policies submitted without this form will not be considered for review.
Peptide Receptor Radionuclide Therapy (PRRT) of NET
 of NET") Peptide Receptor Radionuclide Therapy (PRRT) of NET Dr. Tuba Kendi Associate Prof of Radiology, Mayo Clinic, Rochester, MN 2014 MFMER slide-1 Relevant Financial Relationship(s) None Off Label Usage None
Peptide Receptor Radionuclide Therapy (PRRT) of NET Dr. Tuba Kendi Associate Prof of Radiology, Mayo Clinic, Rochester, MN 2014 MFMER slide-1 Relevant Financial Relationship(s) None Off Label Usage None
Peptide Receptor Radionuclide Therapy using 177 Lu octreotate
 Peptide Receptor Radionuclide Therapy using 177 Lu octreotate BLR Kam, Erasmus Medical Centre, Rotterdam DJ Kwekkeboom, Erasmus Medical Centre, Rotterdam Legal aspects As 177 Lu-[DOTA 0 -Tyr 3 ]octreotate
Peptide Receptor Radionuclide Therapy using 177 Lu octreotate BLR Kam, Erasmus Medical Centre, Rotterdam DJ Kwekkeboom, Erasmus Medical Centre, Rotterdam Legal aspects As 177 Lu-[DOTA 0 -Tyr 3 ]octreotate
Review of Gastrointestinal Carcinoid Tumors: Latest Therapies
 Review of Gastrointestinal Carcinoid Tumors: Latest Therapies Arvind Dasari, MD, MS Department of Gastrointestinal Medical Oncology The University of Texas MD Anderson Cancer Center Houston, TX, USA Neuroendocrine
Review of Gastrointestinal Carcinoid Tumors: Latest Therapies Arvind Dasari, MD, MS Department of Gastrointestinal Medical Oncology The University of Texas MD Anderson Cancer Center Houston, TX, USA Neuroendocrine
MEDICAL MANAGEMENT OF METASTATIC GEP-NET
 MEDICAL MANAGEMENT OF METASTATIC GEP-NET Jeremy Kortmansky, MD Associate Professor of Clinical Medicine Yale Cancer Center DISCLOSURES: NONE Introduction Gastrointestinal and pancreatic neuroendocrine
MEDICAL MANAGEMENT OF METASTATIC GEP-NET Jeremy Kortmansky, MD Associate Professor of Clinical Medicine Yale Cancer Center DISCLOSURES: NONE Introduction Gastrointestinal and pancreatic neuroendocrine
NET und NEC. Endoscopic and oncologic therapy
 NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
NET εντέρου Τι νεότερο/ Νέες μελέτες. Μαντώ Νικολαΐδη παθολόγος-ογκολόγος ΜΗΤΕΡΑ
 NET εντέρου Τι νεότερο/ Νέες μελέτες Μαντώ Νικολαΐδη παθολόγος-ογκολόγος ΜΗΤΕΡΑ NET: A Diverse Group of Malignancies 1-3 Wide spectrum of malignancies arising in neuroendocrine cells throughout the body
NET εντέρου Τι νεότερο/ Νέες μελέτες Μαντώ Νικολαΐδη παθολόγος-ογκολόγος ΜΗΤΕΡΑ NET: A Diverse Group of Malignancies 1-3 Wide spectrum of malignancies arising in neuroendocrine cells throughout the body
GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust
 GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust Introduction Carcinoid was old term, introduced in 1906 by German pathologist Cancinoma like More recent
GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust Introduction Carcinoid was old term, introduced in 1906 by German pathologist Cancinoma like More recent
Lu 177-Dotatate (Lutathera) Therapy Information
 Therapy Information") Lu 177-Dotatate (Lutathera) Therapy Information Information for Lu 177-dotatate therapy also known as Lutathera, for the treatment of metastatic midgut neuroendocrine tumor and other metastatic neuroendocrine
Lu 177-Dotatate (Lutathera) Therapy Information Information for Lu 177-dotatate therapy also known as Lutathera, for the treatment of metastatic midgut neuroendocrine tumor and other metastatic neuroendocrine
lutetium ( 177 Lu) oxodotreotide 370MBq/mL solution for infusion (Lutathera ) SMC No 1337/18 Advanced Accelerator Applications
 oxodotreotide 370MBq/mL solution for infusion (Lutathera ) SMC No 1337/18 Advanced Accelerator Applications") lutetium ( 177 Lu) oxodotreotide 370MBq/mL solution for infusion (Lutathera ) SMC No 1337/18 Advanced Accelerator Applications 8 June 2018 The Scottish Medicines Consortium (SMC) has completed its assessment
lutetium ( 177 Lu) oxodotreotide 370MBq/mL solution for infusion (Lutathera ) SMC No 1337/18 Advanced Accelerator Applications 8 June 2018 The Scottish Medicines Consortium (SMC) has completed its assessment
QOL Improvements in NETTER-1 Phase III Trial in Patients With Progressive Midgut Neuroendocrine Tumors
 QOL Improvements in NETTER-1 Phase III Trial in Patients With Progressive Midgut Neuroendocrine Tumors Abstract C-33 Strosberg J, Wolin E, Chasen B, Kulke M, Bushnell D, Caplin M, Baum RP, Kunz P, Hobday
QOL Improvements in NETTER-1 Phase III Trial in Patients With Progressive Midgut Neuroendocrine Tumors Abstract C-33 Strosberg J, Wolin E, Chasen B, Kulke M, Bushnell D, Caplin M, Baum RP, Kunz P, Hobday
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors
 Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
EXOCRINE: 93% Acinar Cells Duct Cells. ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others
 EXOCRINE: 93% Acinar Cells Duct Cells Digestive Enzymes Trypsin: Digests Proteins Lipases: Digests Fats Amylase: Digest Carbohydrates ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others Hormones Glucagon
EXOCRINE: 93% Acinar Cells Duct Cells Digestive Enzymes Trypsin: Digests Proteins Lipases: Digests Fats Amylase: Digest Carbohydrates ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others Hormones Glucagon
Case Report. Ameya D. Puranik, MD, FEBNM; Harshad R. Kulkarni, MD; Aviral Singh, MD; Richard P. Baum, MD, PhD ABSTRACT
 Case Report 8-YEAR SURVIVAL WITH A METASTATIC THYMIC NEUROENDOCRINE TUMOR: EMPHASIS ON REDEFINING TREATMENT OBJECTIVES USING PERSONALIZED PEPTIDE RECEPTOR RADIONUCLIDE THERAPY WITH 177 Lu- AND 90 Y-LABELED
Case Report 8-YEAR SURVIVAL WITH A METASTATIC THYMIC NEUROENDOCRINE TUMOR: EMPHASIS ON REDEFINING TREATMENT OBJECTIVES USING PERSONALIZED PEPTIDE RECEPTOR RADIONUCLIDE THERAPY WITH 177 Lu- AND 90 Y-LABELED
MEDICAL POLICY SUBJECT: PEPTIDE RECEPTOR RADIONUCLIDE THERAPY (PRRT)
") MEDICAL POLICY SUBJECT: PEPTIDE RECEPTOR PAGE: 1 OF: 6 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product (including an Essential
MEDICAL POLICY SUBJECT: PEPTIDE RECEPTOR PAGE: 1 OF: 6 If a product excludes coverage for a service, it is not covered, and medical policy criteria do not apply. If a commercial product (including an Essential
THERAPEUTIC RADIOPHARMACEUTICALS
 UnitedHealthcare of California (HMO) UnitedHealthcare Benefits Plan of California (EPO/POS) UnitedHealthcare of Oklahoma, Inc. UnitedHealthcare of Oregon, Inc. UnitedHealthcare Benefits of Texas, Inc.
UnitedHealthcare of California (HMO) UnitedHealthcare Benefits Plan of California (EPO/POS) UnitedHealthcare of Oklahoma, Inc. UnitedHealthcare of Oregon, Inc. UnitedHealthcare Benefits of Texas, Inc.
TRACTAMENT ONCOLÒGIC DELS TUMORS NEUROENDOCRINS METASTÀSICS
 TRACTAMENT ONCOLÒGIC DELS TUMORS NEUROENDOCRINS METASTÀSICS Jaume Capdevila Unitat de Tumors GI i Endocrins Hospital Universitari Vall d Hebron Barcelona Experts, acollidors i solidaris OUTLINE BACKGROUND
TRACTAMENT ONCOLÒGIC DELS TUMORS NEUROENDOCRINS METASTÀSICS Jaume Capdevila Unitat de Tumors GI i Endocrins Hospital Universitari Vall d Hebron Barcelona Experts, acollidors i solidaris OUTLINE BACKGROUND
Session 6 NEW TECHNIQUES IN RADIATION TREATMENT. Chairman : Françoise MORNEX
 Session 6 NEW TECHNIQUES IN RADIATION TREATMENT Chairman : Françoise MORNEX INTERNAL IRRADIATION FOR ENDOCRINE TUMORS Emmanuel DESHAYES INTERNAL IRRADIATION FOR ENDOCRINE TUMORS Dr Emmanuel DESHAYES Nuclear
Session 6 NEW TECHNIQUES IN RADIATION TREATMENT Chairman : Françoise MORNEX INTERNAL IRRADIATION FOR ENDOCRINE TUMORS Emmanuel DESHAYES INTERNAL IRRADIATION FOR ENDOCRINE TUMORS Dr Emmanuel DESHAYES Nuclear
Theranostics in Nuclear Medicine
 Theranostics in Nuclear Medicine Patrick FLAMEN, MD, PhD Head Nuclear Medicine Institut Jules Bordet Université Libre de Bruxelles (U.L.B.) n Theranostics in Nuclear Medicine n A form of (nuclear) diagnostic
Theranostics in Nuclear Medicine Patrick FLAMEN, MD, PhD Head Nuclear Medicine Institut Jules Bordet Université Libre de Bruxelles (U.L.B.) n Theranostics in Nuclear Medicine n A form of (nuclear) diagnostic
Cutting Edge Treatment of Neuroendocrine Tumors
 Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Cutting Edge Treatment of Neuroendocrine Tumors
 Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Lutetium-177 PSMA (LuPSMA) Theranostic Phase II trial: Efficacy, safety and QoL in patients
 Theranostic Phase II trial: Efficacy, safety and QoL in patients") Lutetium-177 PSMA (LuPSMA) Theranostic Phase II trial: Efficacy, safety and QoL in patients with castrate-resistant prostate cancer treated with LuPSMA M. S. Hofman, S. Sandhu, P. Eu, P. Jackson, T. Akhurst,
Lutetium-177 PSMA (LuPSMA) Theranostic Phase II trial: Efficacy, safety and QoL in patients with castrate-resistant prostate cancer treated with LuPSMA M. S. Hofman, S. Sandhu, P. Eu, P. Jackson, T. Akhurst,
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL NEUROENDOCRINE GASTRO-ENTERO-PANCREATIC TUMOURS GI Site Group Neuroendocrine gastro-entero-pancreatic tumours Authors: Dr.
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL NEUROENDOCRINE GASTRO-ENTERO-PANCREATIC TUMOURS GI Site Group Neuroendocrine gastro-entero-pancreatic tumours Authors: Dr.
Neuroendocrine Tumors: Just the Basics. George Fisher, MD PhD
 Neuroendocrine Tumors: Just the Basics George Fisher, MD PhD Topics that we will not discuss Some types of lung cancer: Small cell neuroendocrine lung cancer Large cell neuroendocrine lung cancer Some
Neuroendocrine Tumors: Just the Basics George Fisher, MD PhD Topics that we will not discuss Some types of lung cancer: Small cell neuroendocrine lung cancer Large cell neuroendocrine lung cancer Some
A New Proposal for Metabolic Classification of NENs Stefano Severi IRST Meldola Italy
 RADIONUCLIDE THERAPY AND ALLIED SCIENCE President: Giovanni Paganelli Chairman: Maria Salvato Baltimore USA Domenico Barone Meldola Italy A New Proposal for Metabolic Classification of NENs Stefano Severi
RADIONUCLIDE THERAPY AND ALLIED SCIENCE President: Giovanni Paganelli Chairman: Maria Salvato Baltimore USA Domenico Barone Meldola Italy A New Proposal for Metabolic Classification of NENs Stefano Severi
The PET-NET Study 2016 CNETS Grant Award
 The PET-NET Study 2016 CNETS Grant Award CANM Meeting April 21, 2017 Hagen Kennecke, MD, MHA, FRCPC Medical Oncology, BC Cancer Agency Associate Professor, University of British Columbia Raja Ampat, Indonesia
The PET-NET Study 2016 CNETS Grant Award CANM Meeting April 21, 2017 Hagen Kennecke, MD, MHA, FRCPC Medical Oncology, BC Cancer Agency Associate Professor, University of British Columbia Raja Ampat, Indonesia
Antiangiogenics are effective treatments in NETs
 RENET: A randomized phase III trial comparing REgorafenib to placebo in patients with advanced, progressive, well-differentiated NEuroendocrine Tumors (NETs). Coordinators: Dr Julien Hadoux & Dr David
RENET: A randomized phase III trial comparing REgorafenib to placebo in patients with advanced, progressive, well-differentiated NEuroendocrine Tumors (NETs). Coordinators: Dr Julien Hadoux & Dr David
Hot of the press. Γρηγόριος Καλτσάς MD FRCP Καθηγητής Παθολογίας Ενδοκρινολογίας ΕΚΠΑ
 Hot of the press Γρηγόριος Καλτσάς MD FRCP Καθηγητής Παθολογίας Ενδοκρινολογίας ΕΚΠΑ Outline Diagnostic developments Histopathology Molecular Therapeutic developments Results on PRRT Telotristat in carcinoid
Hot of the press Γρηγόριος Καλτσάς MD FRCP Καθηγητής Παθολογίας Ενδοκρινολογίας ΕΚΠΑ Outline Diagnostic developments Histopathology Molecular Therapeutic developments Results on PRRT Telotristat in carcinoid
FRANKLY SPEAKING ABOUT CANCER: NEUROENDOCRINE & CARCINOID TUMORS (NETS)
") FRANKLY SPEAKING ABOUT CANCER: NEUROENDOCRINE & CARCINOID TUMORS (NETS) Gilda s Club Quad Cities November 5 th, 2018 Joseph Dillon, MD Neuroendocrine Tumor Clinic University of Iowa Hospitals & Clinics
FRANKLY SPEAKING ABOUT CANCER: NEUROENDOCRINE & CARCINOID TUMORS (NETS) Gilda s Club Quad Cities November 5 th, 2018 Joseph Dillon, MD Neuroendocrine Tumor Clinic University of Iowa Hospitals & Clinics
Teresa Alonso Gordoa Servicio Oncología Médica Hospital Universitario Ramón y Cajal
 Teresa Alonso Gordoa Servicio Oncología Médica Hospital Universitario Ramón y Cajal Incidence per 100,000 EPIDEMIOLOGY Incidence rates of neuroendocrine tumors by primary tumor site 1.4 1.2 1.0 0.8 0.6
Teresa Alonso Gordoa Servicio Oncología Médica Hospital Universitario Ramón y Cajal Incidence per 100,000 EPIDEMIOLOGY Incidence rates of neuroendocrine tumors by primary tumor site 1.4 1.2 1.0 0.8 0.6
NET ΠΝΕΥΜΟΝΑ: τι νεότερο / νέες μελέτες
 NETMASTERCLASS 2017: an interactive workshop NET ΠΝΕΥΜΟΝΑ: τι νεότερο / νέες μελέτες Νικόλαος Τσουκαλάς MD, MSc, PhD Ογκολόγος - Παθολόγος, MSc Βιοπληροφορική Επιμελητής Α, Ογκολογικό Τμήμα Νοσηλευτικό
NETMASTERCLASS 2017: an interactive workshop NET ΠΝΕΥΜΟΝΑ: τι νεότερο / νέες μελέτες Νικόλαος Τσουκαλάς MD, MSc, PhD Ογκολόγος - Παθολόγος, MSc Βιοπληροφορική Επιμελητής Α, Ογκολογικό Τμήμα Νοσηλευτικό
Chair s presentation Lutetium (177lu) oxodotreotide for treating unresectable or metastatic neuroendocrine tumours in people with progressive disease
 oxodotreotide for treating unresectable or metastatic neuroendocrine tumours in people with progressive disease") Public slides Chair s presentation Lutetium (177lu) oxodotreotide for treating unresectable or metastatic neuroendocrine tumours in people with progressive disease 2 nd Appraisal Committee meeting Committee
Public slides Chair s presentation Lutetium (177lu) oxodotreotide for treating unresectable or metastatic neuroendocrine tumours in people with progressive disease 2 nd Appraisal Committee meeting Committee
WHAT TO EXPECT IN 2015? - Renuka Iyer, MD Associate Professor of Medicine, University at Buffalo Associate Professor of Oncology, Roswell Park Cancer
 WHAT TO EXPECT IN 2015? - Renuka Iyer, MD Associate Professor of Medicine, University at Buffalo Associate Professor of Oncology, Roswell Park Cancer Institute Overview Diagnosis: Gallium scan Biomarkers
WHAT TO EXPECT IN 2015? - Renuka Iyer, MD Associate Professor of Medicine, University at Buffalo Associate Professor of Oncology, Roswell Park Cancer Institute Overview Diagnosis: Gallium scan Biomarkers
Systemic Therapy for Gastroenteropancreatic (GEP) Neuroendocrine Tumors and Lung Carcinoid
 Neuroendocrine Tumors and Lung Carcinoid") Systemic Therapy for Gastroenteropancreatic (GEP) Neuroendocrine Tumors and Lung Carcinoid The Medical Oncology Perspective Nevena Damjanov, MD Associate professor Abramson Cancer Center of the University
Systemic Therapy for Gastroenteropancreatic (GEP) Neuroendocrine Tumors and Lung Carcinoid The Medical Oncology Perspective Nevena Damjanov, MD Associate professor Abramson Cancer Center of the University
Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide)
") GEP-NET Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide) 1 Histogenesis 16 different
GEP-NET Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide) 1 Histogenesis 16 different
PRRT in Management of NETs. Ioannis Karfis, MD PhD Assistant Head of Clinic Nuclear Medicine Dept IJB, Brussels
 PRRT in Management of NETs Ioannis Karfis, MD PhD Assistant Head of Clinic Nuclear Medicine Dept IJB, Brussels THERAPEUTIC TARGETS in NENs Pavel M: Neuroendocrinology 2013;97:99-112 THERAPEUTIC ARENA in
PRRT in Management of NETs Ioannis Karfis, MD PhD Assistant Head of Clinic Nuclear Medicine Dept IJB, Brussels THERAPEUTIC TARGETS in NENs Pavel M: Neuroendocrinology 2013;97:99-112 THERAPEUTIC ARENA in
Lu-DOTATATE PRRT dosimetry:
 177 Lu-DOTATATE PRRT dosimetry: From theory to practice Silvano Gnesin Medical Physics department Institute of Radiation Physics, Lausanne University Hospital, Lausanne, Switzerland Gwennaëlle Marin Medical
177 Lu-DOTATATE PRRT dosimetry: From theory to practice Silvano Gnesin Medical Physics department Institute of Radiation Physics, Lausanne University Hospital, Lausanne, Switzerland Gwennaëlle Marin Medical
Systemic Therapy for Pheos/Paras: Somatostatin analogues, small molecules, immunotherapy and other novel approaches in the works.
 Systemic Therapy for Pheos/Paras: Somatostatin analogues, small molecules, immunotherapy and other novel approaches in the works. Arturo Loaiza-Bonilla, MD, FACP Assistant Professor of Clinical Medicine
Systemic Therapy for Pheos/Paras: Somatostatin analogues, small molecules, immunotherapy and other novel approaches in the works. Arturo Loaiza-Bonilla, MD, FACP Assistant Professor of Clinical Medicine
Neuroendocrine Tumour Theranostics
 Neuroendocrine Tumour Theranostics Lisa Bodei Director of Targeted Radionuclide Therapy Molecular Imaging and Therapy Service Memorial Sloan Kettering Cancer Center New York Friday, April 13, 2018 Disclosure
Neuroendocrine Tumour Theranostics Lisa Bodei Director of Targeted Radionuclide Therapy Molecular Imaging and Therapy Service Memorial Sloan Kettering Cancer Center New York Friday, April 13, 2018 Disclosure
Physical Bases : Which Isotopes?
 Physical Bases : Which Isotopes? S. Gnesin Institute of Radiation Physics, Lausanne University Hospital, Lausanne, Switzerland 1/53 Theranostic Bruxelles, 2 Octobrer 2017 Theranostic : use of diagnostic
Physical Bases : Which Isotopes? S. Gnesin Institute of Radiation Physics, Lausanne University Hospital, Lausanne, Switzerland 1/53 Theranostic Bruxelles, 2 Octobrer 2017 Theranostic : use of diagnostic
Nuevas alternativas en el manejo de TNE avanzados
 Nuevas alternativas en el manejo de TNE avanzados Jaume Capdevila Hospital Universitari Vall d Hebron Barcelona Coordinación científica: Dr. Fernando Rivera Hospital Universitario Marqués de Valdecilla,
Nuevas alternativas en el manejo de TNE avanzados Jaume Capdevila Hospital Universitari Vall d Hebron Barcelona Coordinación científica: Dr. Fernando Rivera Hospital Universitario Marqués de Valdecilla,
OPTIMISING OUTCOMES IN GASTROINTESTINAL NEUROENDOCRINE TUMOURS
 OPTIMISING OUTCOMES IN GASTROINTESTINAL NEUROENDOCRINE TUMOURS Dr Mairéad McNamara Senior lecturer, University of Manchester & Honorary Consultant in Medical Oncology, The Christie NHS Foundation Trust
OPTIMISING OUTCOMES IN GASTROINTESTINAL NEUROENDOCRINE TUMOURS Dr Mairéad McNamara Senior lecturer, University of Manchester & Honorary Consultant in Medical Oncology, The Christie NHS Foundation Trust
MEDICAL POLICY EFFECTIVE DATE: 06/21/07 REVISED DATE: 05/14/08, 04/16/09, 03/18/10, 03/17/11, 03/15/12, 02/21/13, 02/20/14, 02/19/15
 MEDICAL POLICY PAGE: 1 OF: 6 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
MEDICAL POLICY PAGE: 1 OF: 6 If the member's subscriber contract excludes coverage for a specific service it is not covered under that contract. In such cases, medical policy criteria are not applied.
Ga68 Imaging. Roland HUSTINX Division of Nuclear Medicine and Oncologic Imaging Centre Hospitalier Universitaire de Liège Belgium
 Ga68 Imaging Roland HUSTINX Division of Nuclear Medicine and Oncologic Imaging Centre Hospitalier Universitaire de Liège Belgium 68 Ga Produced by a 68 Ge/ 68 Ga generator Decays by positron emission
Ga68 Imaging Roland HUSTINX Division of Nuclear Medicine and Oncologic Imaging Centre Hospitalier Universitaire de Liège Belgium 68 Ga Produced by a 68 Ge/ 68 Ga generator Decays by positron emission
Patient information file
 Internal irradiation of neuroendocrine tumors with Yttrium-90-DOTATOC, a radiolabeled somatostatin analogue Patient information file Ladies and Gentlemen You are diagnosed with a neuroendocrine tumor and
Internal irradiation of neuroendocrine tumors with Yttrium-90-DOTATOC, a radiolabeled somatostatin analogue Patient information file Ladies and Gentlemen You are diagnosed with a neuroendocrine tumor and
Background. Capdevila J, et al. Ann Oncol. 2018;29(Suppl 8): Abstract 1307O. 1. Dasari A, et al. JAMA Oncol. 2017;3(10):
: Abstract 1307O. 1. Dasari A, et al. JAMA Oncol. 2017;3(10):") Efficacy of Lenvatinib in Patients With Advanced Pancreatic (pannets) and Gastrointestinal (ginets) WHO Grade 1/2 (G1/G2) Neuroendocrine Tumors: Results of the International Phase II TALENT Trial (GETNE
Efficacy of Lenvatinib in Patients With Advanced Pancreatic (pannets) and Gastrointestinal (ginets) WHO Grade 1/2 (G1/G2) Neuroendocrine Tumors: Results of the International Phase II TALENT Trial (GETNE
Specialised Services Policy CP66: 68-gallium DOTA- peptide scanning for the Management of Neuroendocrine Tumours (NETs)
") Specialised Services Policy CP66: Management of Neuroendocrine Tumours (NETs) Document Author: Assistant Planner for Cancer and Blood Executive Lead: Director of Quality and Nursing Approved by: Management
Specialised Services Policy CP66: Management of Neuroendocrine Tumours (NETs) Document Author: Assistant Planner for Cancer and Blood Executive Lead: Director of Quality and Nursing Approved by: Management
FMU-ICRP Workshop on Radiological Protection in Medicine Current Status in Radionuclide Therapy Tuesday, October 3, 2017 Makoto Hosono, MD PhD Kindai
 FMU-ICRP Workshop on Radiological Protection in Medicine Current Status in Radionuclide Therapy Tuesday, October 3, 2017 Makoto Hosono, MD PhD Kindai University Faculty of Medicine, Osaka, Japan Current
FMU-ICRP Workshop on Radiological Protection in Medicine Current Status in Radionuclide Therapy Tuesday, October 3, 2017 Makoto Hosono, MD PhD Kindai University Faculty of Medicine, Osaka, Japan Current
EXOCRINE: 93% Acinar Cells Duct Cells. ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others
 EXOCRINE: 93% Acinar Cells Duct Cells Digestive Enzymes Trypsin: Digests Proteins Lipases: Digests Fats Amylase: Digest Carbohydrates ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others Hormones Glucagon
EXOCRINE: 93% Acinar Cells Duct Cells Digestive Enzymes Trypsin: Digests Proteins Lipases: Digests Fats Amylase: Digest Carbohydrates ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others Hormones Glucagon
Diagnosing and monitoring NET
 Diagnosing and monitoring NET Inaccurate or delayed diagnosis of neuroendocrine tumors (NET) is common, because many NET are small and asymptomatic. 1 When symptoms are present, they are usually nonspecific
Diagnosing and monitoring NET Inaccurate or delayed diagnosis of neuroendocrine tumors (NET) is common, because many NET are small and asymptomatic. 1 When symptoms are present, they are usually nonspecific
SARCOPHAGINE CHELATORS AND COPPER ISOTOPES FOR IMAGING AND THERAPY
 SEEING IS BELIEVING SARCOPHAGINE CHELATORS AND COPPER ISOTOPES FOR IMAGING AND THERAPY Sydney Vital and STEaM Neuroendocrine Tumour Preceptorship May 2018 Amos Hedt Head of Clinical Development 1 CLARITY
SEEING IS BELIEVING SARCOPHAGINE CHELATORS AND COPPER ISOTOPES FOR IMAGING AND THERAPY Sydney Vital and STEaM Neuroendocrine Tumour Preceptorship May 2018 Amos Hedt Head of Clinical Development 1 CLARITY
Austin Radiological Association Ga-68 NETSPOT (Ga-68 dotatate)
") Austin Radiological Association Ga-68 NETSPOT (Ga-68 dotatate) Overview Ga-68 dotatate binds to somatostatin receptors, with highest affinity for subtype 2 receptors (sstr2). It binds to cells that express
Austin Radiological Association Ga-68 NETSPOT (Ga-68 dotatate) Overview Ga-68 dotatate binds to somatostatin receptors, with highest affinity for subtype 2 receptors (sstr2). It binds to cells that express
Case Presentation. Marianne Ellen Pavel. Charité University Medicine Berlin. ESMO Preceptorship on GI Neuroendocrine Tumors
 Case Presentation Marianne Ellen Pavel Charité University Medicine Berlin ESMO Preceptorship on GI Neuroendocrine Tumors Session 3; Singapore November 2, 2012 06.11.2012 Medical History 46-year-old man
Case Presentation Marianne Ellen Pavel Charité University Medicine Berlin ESMO Preceptorship on GI Neuroendocrine Tumors Session 3; Singapore November 2, 2012 06.11.2012 Medical History 46-year-old man
Strategies in the Management of Neuroendocrine Tumors. Dr. Jean Maroun Dr. Elena Tsvetkova
 Strategies in the Management of Neuroendocrine Tumors Dr. Jean Maroun Dr. Elena Tsvetkova 1 A ZORSE 2 Neuroendocrine Tumour Classification Neuroendocrine Tumours Carcinoid Tumours Pancreatic Neuroendocrine
Strategies in the Management of Neuroendocrine Tumors Dr. Jean Maroun Dr. Elena Tsvetkova 1 A ZORSE 2 Neuroendocrine Tumour Classification Neuroendocrine Tumours Carcinoid Tumours Pancreatic Neuroendocrine
Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology
 Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology OUTLINE Molecular Rationale for the use of SSAs in
Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology OUTLINE Molecular Rationale for the use of SSAs in
Neuroendocrine Tumors
 Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
Imaging of Neuroendocrine Metastases
 Imaging of Neuroendocrine Metastases Aoife Kilcoyne, Shaunagh McDermott, Colin McCarthy,Manuel Patino, Dushyant Sahani, Michael Blake Abdominal Imaging Division Massachusetts General Hospital Disclosure
Imaging of Neuroendocrine Metastases Aoife Kilcoyne, Shaunagh McDermott, Colin McCarthy,Manuel Patino, Dushyant Sahani, Michael Blake Abdominal Imaging Division Massachusetts General Hospital Disclosure
Somatuline Depot. Somatuline Depot (lanreotide) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.27 Subject: Somatuline Depot Page: 1 of 5 Last Review Date: December 8, 2017 Somatuline Depot Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.27 Subject: Somatuline Depot Page: 1 of 5 Last Review Date: December 8, 2017 Somatuline Depot Description
A QUICK LOOK AT LUTATHERA (lutetium Lu 177 dotatate)
") A QUICK LOOK AT LUTATHERA (lutetium Lu 177 dotatate) What is LUTATHERA? LUTATHERA is a medicine that uses radiation to kill cancer cells, which means it works differently than most other cancer medicines.
A QUICK LOOK AT LUTATHERA (lutetium Lu 177 dotatate) What is LUTATHERA? LUTATHERA is a medicine that uses radiation to kill cancer cells, which means it works differently than most other cancer medicines.
PNET 3/7/2015. GI and Pancreatic NETs. The Postgraduate Course in Breast and Endocrine Surgery. Decision Tree. GI and Pancreatic NETs.
 GI and Pancreatic NETs The Postgraduate Course in Breast and Endocrine Surgery Disclosures Ipsen NET Advisory Board Marines Memorial Club and Hotel San Francisco, CA Eric K Nakakura San Francisco, CA March
GI and Pancreatic NETs The Postgraduate Course in Breast and Endocrine Surgery Disclosures Ipsen NET Advisory Board Marines Memorial Club and Hotel San Francisco, CA Eric K Nakakura San Francisco, CA March
Cowen Annual Healthcare Conference. March 2018
 Cowen Annual Healthcare Conference March 2018 Forward Looking Statements Certain of the statements made in this presentation are forward looking, such as those, among others, relating to future spending,
Cowen Annual Healthcare Conference March 2018 Forward Looking Statements Certain of the statements made in this presentation are forward looking, such as those, among others, relating to future spending,
An Overview of NETS. Richard R.P. Warner M.D
 An Overview of NETS Richard R.P. Warner M.D Diagnosis and Treatment Approaches Carcinoid (and other NETs) not as benign as originally described 13-50% of all carcinoids have distant metastases when first
An Overview of NETS Richard R.P. Warner M.D Diagnosis and Treatment Approaches Carcinoid (and other NETs) not as benign as originally described 13-50% of all carcinoids have distant metastases when first
Toward More Aggressive Management of Neuroendocrine Tumors: Current and Future Perspectives
 Toward More Aggressive Management of Neuroendocrine Tumors: Current and Future Perspectives Moderator: Ashley Grossman, MD, FRCP Professor of Neuroendocrinology William Harvey Research Institute Barts
Toward More Aggressive Management of Neuroendocrine Tumors: Current and Future Perspectives Moderator: Ashley Grossman, MD, FRCP Professor of Neuroendocrinology William Harvey Research Institute Barts
2015: Year in Review Results of Recent Trials
 2015: Year in Review Results of Recent Trials Pamela L. Kunz, MD Assistant Professor of Medicine / GI Oncology Director, Stanford NET Program Stanford University School of Medicine Disclosures Research
2015: Year in Review Results of Recent Trials Pamela L. Kunz, MD Assistant Professor of Medicine / GI Oncology Director, Stanford NET Program Stanford University School of Medicine Disclosures Research
Color Codes Pathology and Genetics Medicine and Clinical Pathology Surgery Imaging
 Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
Therapeutic Radiopharmaceuticals in Oncology
 Therapeutic Radiopharmaceuticals in Oncology Policy Number: 6.01.60 Last Review: 9/2018 Origination: 9/2018 Next Review: 9/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
Therapeutic Radiopharmaceuticals in Oncology Policy Number: 6.01.60 Last Review: 9/2018 Origination: 9/2018 Next Review: 9/2019 Policy Blue Cross and Blue Shield of Kansas City (Blue KC) will provide coverage
TUMORES NEUROENDOCRINOS. Miguel Navarro. Salamanca
 TUMORES NEUROENDOCRINOS Miguel Navarro. Salamanca Introduction to Neuroendocrine Tumours (NETs) NETs are relatively RARE At least 40 different entities are described arising in different organs. Different
TUMORES NEUROENDOCRINOS Miguel Navarro. Salamanca Introduction to Neuroendocrine Tumours (NETs) NETs are relatively RARE At least 40 different entities are described arising in different organs. Different
Sandostatin LAR. Sandostatin LAR (octreotide acetate) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.09 Subject: Sandostatin LAR Page: 1 of 5 Last Review Date: March 16, 2018 Sandostatin LAR Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.09 Subject: Sandostatin LAR Page: 1 of 5 Last Review Date: March 16, 2018 Sandostatin LAR Description
NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction
 NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Diagnostic & therapeutic
NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Diagnostic & therapeutic
Recent Advances in Gastrointestinal Cancers
 Recent Advances in Gastrointestinal Cancers Ursina R. Teitelbaum, MD Section of Hematology/Oncology Abramson Cancer Center PENN 2016 Updates in Oncology June 23, 2016 none Disclosures ASCO 2016 Highlights:
Recent Advances in Gastrointestinal Cancers Ursina R. Teitelbaum, MD Section of Hematology/Oncology Abramson Cancer Center PENN 2016 Updates in Oncology June 23, 2016 none Disclosures ASCO 2016 Highlights:
Pharmacy Prior Authorization Somatostatin Analogs Clinical Guideline
 Sandostatin LAR (octreotide) Signifor (pasireotide) Signifor LAR (pasireotide) Somatuline Depot (lanreotide) octreotide FDA Approved Indications: Acromegaly: Octreotide Injection is indicated to reduce
Sandostatin LAR (octreotide) Signifor (pasireotide) Signifor LAR (pasireotide) Somatuline Depot (lanreotide) octreotide FDA Approved Indications: Acromegaly: Octreotide Injection is indicated to reduce
THERANOSTICS MOLEKULARE BILDGEBUNG MITTELS PET/CT
 THERANOSTICS MOLEKULARE BILDGEBUNG MITTELS PET/CT UND RADIOREZEPTORTHERAPIE VON NET Richard P. Baum Klinik für Molekulare Radiotherapie / Zentrum für Molekulare Bildgebung (PET/CT) ENETS Center of Excellence,
THERANOSTICS MOLEKULARE BILDGEBUNG MITTELS PET/CT UND RADIOREZEPTORTHERAPIE VON NET Richard P. Baum Klinik für Molekulare Radiotherapie / Zentrum für Molekulare Bildgebung (PET/CT) ENETS Center of Excellence,
Ronald C. Walker, MD, Prof of Radiology Vanderbilt University Medical Center Nashville, TN. Ga-DOTATATE PET/CT imaging Initial Vanderbilt experience
 Ronald C. Walker, MD, Prof of Radiology Vanderbilt University Medical Center Nashville, TN 68 Ga-DOTATATE PET/CT imaging Initial Vanderbilt experience Disclosures: No financial disclosures or conflicts
Ronald C. Walker, MD, Prof of Radiology Vanderbilt University Medical Center Nashville, TN 68 Ga-DOTATATE PET/CT imaging Initial Vanderbilt experience Disclosures: No financial disclosures or conflicts
NICaN Pancreatic Neuroendocrine Tumour SACT protocols. 1.0 Dr M Eatock Final version issued
 Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Neuro-endocrine Tumours Dr Martin Eatock, Consultant Medical Oncologist & on behalf of the GI Oncologists Group,
Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Neuro-endocrine Tumours Dr Martin Eatock, Consultant Medical Oncologist & on behalf of the GI Oncologists Group,
Dr. Sandip Basu Radiation Medicine Center (BARC) Tata Memorial Centre Annexe, Parel, Mumbai
 Tata Memorial Centre Annexe, Parel, Mumbai") Newer Radionuclide Therapies Dr. Sandip Basu Radiation Medicine Center (BARC) Tata Memorial Centre Annexe, Parel, Mumbai NICSTAR-2018 5 th -7 th March, 2018 A. Receptor over-expression in Tumors as Target:
Newer Radionuclide Therapies Dr. Sandip Basu Radiation Medicine Center (BARC) Tata Memorial Centre Annexe, Parel, Mumbai NICSTAR-2018 5 th -7 th March, 2018 A. Receptor over-expression in Tumors as Target:
SCOPE TODAYS SESSION. Case 1: Case 2. Basic Theory Stuff: Heavy Stuff. Basic Questions. Basic Questions
 MONDAY TEACHING SCOPE TODAYS SESSION Case 1: Basic Questions Case 2 Basic Questions Basic Theory Stuff: AJCC TNM + Stage Group for Carcinoid of the Appendix Management of Carcinoid of the Appendix (NCCN)
MONDAY TEACHING SCOPE TODAYS SESSION Case 1: Basic Questions Case 2 Basic Questions Basic Theory Stuff: AJCC TNM + Stage Group for Carcinoid of the Appendix Management of Carcinoid of the Appendix (NCCN)
Tumor markers. Chromogranin A. Analyte Information
 Tumor markers Chromogranin A Analyte Information -1-2018-04-22 Chromogranin A Introduction Chromogranin A (CgA) is a 439-amino acid protein with a molecular weight of 48 to 60 kda, depending on glycosylation
Tumor markers Chromogranin A Analyte Information -1-2018-04-22 Chromogranin A Introduction Chromogranin A (CgA) is a 439-amino acid protein with a molecular weight of 48 to 60 kda, depending on glycosylation
This clinical study synopsis is provided in line with Boehringer Ingelheim s Policy on Transparency and Publication of Clinical Study Data.
 abcd Clinical Study for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the clinical
abcd Clinical Study for Public Disclosure This clinical study synopsis is provided in line with s Policy on Transparency and Publication of Clinical Study Data. The synopsis which is part of the clinical
PSMA Targeted radionuclide therapy in Prostate Cancer
 PSMA Targeted radionuclide therapy in Prostate Cancer Tawatchai Chaiwatanarat Division of Nuclear Medicine Department of Radiology Chulalongkorn University Bangkok, Thailand * cell si ze ~20 µm Radionuclide
PSMA Targeted radionuclide therapy in Prostate Cancer Tawatchai Chaiwatanarat Division of Nuclear Medicine Department of Radiology Chulalongkorn University Bangkok, Thailand * cell si ze ~20 µm Radionuclide
Evaluation and Management of Neuroendocrine Tumors
 Evaluation and Management of Neuroendocrine Tumors Jennifer Chan, MD, MPH Clinical Director, Program in Neuroendocrine and Carcinoid Tumors Dana-Farber/Brigham and Women's Cancer Center October 14, 2017
Evaluation and Management of Neuroendocrine Tumors Jennifer Chan, MD, MPH Clinical Director, Program in Neuroendocrine and Carcinoid Tumors Dana-Farber/Brigham and Women's Cancer Center October 14, 2017
Chapter 10. Summary, conclusions and future perspectives
 Chapter 10 Summary, conclusions and future perspectives 10.1 SUMMARY In this thesis, a new tumor imaging tracer in nuclear medicine is studied. This 123 tracer, L-3-[ I]Iodo-alpha-methyl-tyrosine (IMT),
Chapter 10 Summary, conclusions and future perspectives 10.1 SUMMARY In this thesis, a new tumor imaging tracer in nuclear medicine is studied. This 123 tracer, L-3-[ I]Iodo-alpha-methyl-tyrosine (IMT),
Surgical Therapy of GEP-NET: An Overview
 Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
CRITICAL ANALYSIS OF NEN GUIDELINES. G Pentheroudakis Associate Professsor of Oncology Medical School, University of Ioannina Chair, ESMO Guidelines
 CRITICAL ANALYSIS OF NEN GUIDELINES G Pentheroudakis Associate Professsor of Oncology Medical School, University of Ioannina Chair, ESMO Guidelines DISCLOSURES NO CONFLICTS OF INTEREST TO DECLARE UPDATED
CRITICAL ANALYSIS OF NEN GUIDELINES G Pentheroudakis Associate Professsor of Oncology Medical School, University of Ioannina Chair, ESMO Guidelines DISCLOSURES NO CONFLICTS OF INTEREST TO DECLARE UPDATED
Case Report Metastatic Insulinoma Managed with Radiolabeled Somatostatin Analog
 Case Reports in Endocrinology Volume 2013, Article ID 252159, 4 pages http://dx.doi.org/10.1155/2013/252159 Case Report Metastatic Insulinoma Managed with Radiolabeled Somatostatin Analog Ricardo Costa,
Case Reports in Endocrinology Volume 2013, Article ID 252159, 4 pages http://dx.doi.org/10.1155/2013/252159 Case Report Metastatic Insulinoma Managed with Radiolabeled Somatostatin Analog Ricardo Costa,
Nuclear Medicine in Australia. Shaun Jenkinson
 Nuclear Medicine in Australia Shaun Jenkinson Landmark Infrastructure for Australian Science OPAL Research Reactor Australian Synchrotron Camperdown Cyclotron Bragg Institute Centre for Accelerator Science
Nuclear Medicine in Australia Shaun Jenkinson Landmark Infrastructure for Australian Science OPAL Research Reactor Australian Synchrotron Camperdown Cyclotron Bragg Institute Centre for Accelerator Science
Dosimetry and radiobiology for Peptide Receptor Radionuclide Therapy
 Dosimetry and radiobiology for Peptide Receptor Radionuclide Therapy Short-ranged particle emitters for targeted radionuclide therapy require specific dosimetry and radiobiology Mark Konijnenberg Melodi
Dosimetry and radiobiology for Peptide Receptor Radionuclide Therapy Short-ranged particle emitters for targeted radionuclide therapy require specific dosimetry and radiobiology Mark Konijnenberg Melodi
MEDICAL POLICY SUBJECT: PEPTIDE RECEPTOR RADIONUCLIDE THERAPY (PRRT)
") MEDICAL POLICY SUBJECT: PEPTIDE RECEPTOR RADIONUCLIDE THERAPY (PRRT) POLICY NUMBER: 7.01.78 CATEGORY: Technology Assessment EFFECTIVE DATE: 06/21/07 REVISED DATE: 05/14/08, 04/16/09, 03/18/10, 03/17/11,
MEDICAL POLICY SUBJECT: PEPTIDE RECEPTOR RADIONUCLIDE THERAPY (PRRT) POLICY NUMBER: 7.01.78 CATEGORY: Technology Assessment EFFECTIVE DATE: 06/21/07 REVISED DATE: 05/14/08, 04/16/09, 03/18/10, 03/17/11,
Rodney J Hicks, MD, FRACP, FAAHMS, the Peter MaCallum Cancer Centre, Melbourne, Australia
 Journal of Nuclear Medicine, published on October 6, 2016 as doi:10.2967/jnumed.116.182188 Citius, Altius, Fortius An Olympian dream for Theranostics Rodney J Hicks, MD, FRACP, FAAHMS, the Peter MaCallum
Journal of Nuclear Medicine, published on October 6, 2016 as doi:10.2967/jnumed.116.182188 Citius, Altius, Fortius An Olympian dream for Theranostics Rodney J Hicks, MD, FRACP, FAAHMS, the Peter MaCallum
Development of New Treatment Modalities Oncolytic Viruses and Nanotechnique
 Development of New Treatment Modalities Oncolytic Viruses and Nanotechnique By Professor Kjell Öberg, M.D., Ph.D. Dept. of Endocrine Oncology, University Hospital, Uppsala, Sweden Nashville Oct. 2011 Hallmarks
Development of New Treatment Modalities Oncolytic Viruses and Nanotechnique By Professor Kjell Öberg, M.D., Ph.D. Dept. of Endocrine Oncology, University Hospital, Uppsala, Sweden Nashville Oct. 2011 Hallmarks
Update on Surgical Management of NETs
 Update on Surgical Management of Neuroendocrine Tumors James R. Howe, M.D. Director, Surgical Oncology and Endocrine Surgery University of Iowa College of Medicine Distribution of NETs 2000-2004 27% ---
Update on Surgical Management of Neuroendocrine Tumors James R. Howe, M.D. Director, Surgical Oncology and Endocrine Surgery University of Iowa College of Medicine Distribution of NETs 2000-2004 27% ---
SIRT in the Management of Metastatic Neuroendocrine Tumors
 SIRT in the Management of Metastatic Neuroendocrine Tumors Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director,
SIRT in the Management of Metastatic Neuroendocrine Tumors Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director,
Small-cell lung cancer (SCLC) accounts for 15% to 18% of
 accounts for 15% to 18% of") BRIEF REPORT Brief Report on the Use of Radiolabeled Somatostatin Analogs for the Diagnosis and Treatment of Metastatic Small-Cell Lung Cancer Patients Martina Sollini, MD,* Daniela Farioli, MS,* Armando
BRIEF REPORT Brief Report on the Use of Radiolabeled Somatostatin Analogs for the Diagnosis and Treatment of Metastatic Small-Cell Lung Cancer Patients Martina Sollini, MD,* Daniela Farioli, MS,* Armando
Understanding Biological Activity to Inform Drug Development
 National Cancer Policy Forum Understanding Biological Activity to Inform Drug Development December 12, 2016 Wolfgang Weber Molecular Imaging and Therapy Service Department of Radiology RECIST Response
National Cancer Policy Forum Understanding Biological Activity to Inform Drug Development December 12, 2016 Wolfgang Weber Molecular Imaging and Therapy Service Department of Radiology RECIST Response
Carcinoid Tumors: The Beginning and End. Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011
 Carcinoid Tumors: The Beginning and End Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011 1 st described by Oberndofer(1907) Karzinoide = cancer like Arise from
Carcinoid Tumors: The Beginning and End Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011 1 st described by Oberndofer(1907) Karzinoide = cancer like Arise from
Peking University School of Oncology, Beijing Cancer Hospital and Institute, Beijing, China
 Contrast Media & Molecular Imaging, Article ID 234389, 9 pages https://doi.org/1.1155/218/234389 Research Article Clinical and Prognostic Value of PET/CT Imaging with Combination of 68 Ga-DOTATATE and
Contrast Media & Molecular Imaging, Article ID 234389, 9 pages https://doi.org/1.1155/218/234389 Research Article Clinical and Prognostic Value of PET/CT Imaging with Combination of 68 Ga-DOTATATE and
LUTATHERA (lutetium Lu 177 dotatate) injection, for intravenous use Initial U.S. Approval: 2018
 injection, for intravenous use Initial U.S. Approval: 2018") HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use LUTATHERA safely and effectively. See full prescribing information for LUTATHERA. LUTATHERA (lutetium
HIGHLIGHTS OF PRESCRIBING INFORMATION These highlights do not include all the information needed to use LUTATHERA safely and effectively. See full prescribing information for LUTATHERA. LUTATHERA (lutetium
Neuroendocrine Tumours If you don t suspect it you can t detect it! Dr JWS Devar HPB Surgeon University of Witwatersrand E-AHPBA CHBAH & WDGMC
 Neuroendocrine Tumours If you don t suspect it you can t detect it! Dr JWS Devar HPB Surgeon University of Witwatersrand E-AHPBA CHBAH & WDGMC Case Study 43 yr old female with a history of a left mastectomy
Neuroendocrine Tumours If you don t suspect it you can t detect it! Dr JWS Devar HPB Surgeon University of Witwatersrand E-AHPBA CHBAH & WDGMC Case Study 43 yr old female with a history of a left mastectomy
Selection of Appropriate Treatment
 Expert Review in Metastatic Gastroenteropancreatic Neuroendocrine Tumors (GEP-NETs): Selection of Appropriate Treatment Reference Slide Deck Neuroendocrine Tumors (NETs): A Diverse Group of Malignancies
Expert Review in Metastatic Gastroenteropancreatic Neuroendocrine Tumors (GEP-NETs): Selection of Appropriate Treatment Reference Slide Deck Neuroendocrine Tumors (NETs): A Diverse Group of Malignancies