Strategies in the Management of Neuroendocrine Tumors. Dr. Jean Maroun Dr. Elena Tsvetkova
|
|
|
- Maurice White
- 6 years ago
- Views:
Transcription
1 Strategies in the Management of Neuroendocrine Tumors Dr. Jean Maroun Dr. Elena Tsvetkova 1

2 A ZORSE 2

3 Neuroendocrine Tumour Classification Neuroendocrine Tumours Carcinoid Tumours Pancreatic Neuroendocrine Tumours Functioning Non-functioning Functioning Non-functioning Symptomatic Asymptomatic 3


4 NET Incidence Is Increasing US SEER data show a 5-fold increase in the past 30 years Annual age-adjusted incidence 5.25/100,000 in 2004 versus 1.09/100,000 in 1973 SEER = Surveillance, Epidemiology and End Results. Adapted with permission from Yao JC, Hassan M, Phan A, et al. J Clin Oncol. 2008;26(18):
5 Increasing Incidence of NETs: Ontario Incidence of carcinoid tumours in Ontario, Rate per 1,000, Year Age-adjusted rates standardized to 1991 in rate per 1 million population by year of diagnosis. Ontario Cancer Registry,

6 NETs Are the Second Most Prevalent Type of GI Malignancy 2x more prevalent than pancreatic cancer ] ] 6
7 Carcinoid Tumours: Origin Bronchopulmonary system Carcinoid site 28% Digestive system Other Colon and rectum Colon, except appendix 9 Appendix 5 Rectum 14 Other 8% 64% 28.5 Small intestine Duodenum 3 Jejunum 2 Ileum 15 NOS Stomach Other 0.5 % 7
8 Functioning Tumours: Overview Secrete biologically active hormones Serotonin, vasoactive intestinal peptide, gastrin May present with vague abdominal symptoms, e.g., cramps, pain, diarrhea misdiagnosed as irritable bowel syndrome Flushing: a challenge at perimenopausal age Symptoms lead to diagnosis at an early stage when tumour small and resectable Result in Carcinoid Syndrome Elevated 5-HIAA levels lead to higher risk for carcinoid heart disease 8
9 Non-functioning tumours: overview Well-differentiated, slow-growing tumours that can go undetected 1/3 to 1/2 of all NETs Not associated with hormone hypersecretion incidental finding during surgery Histologic examination needed Tumours can produce mass effect Symptoms of intermittent intestinal entrapment due to mesenteric fibrosis can evolve into a functioning tumour Monitor mainly with cga 9
10 Pathology of Carcinoids: Ki67 Marker of cell proliferation Present in the nucleus during active phases of cell cycle, absent from resting cells Prognostic factor for survival and a marker of biologic behavior No well-established, validated cut-off points Testing should be done in all patients 10

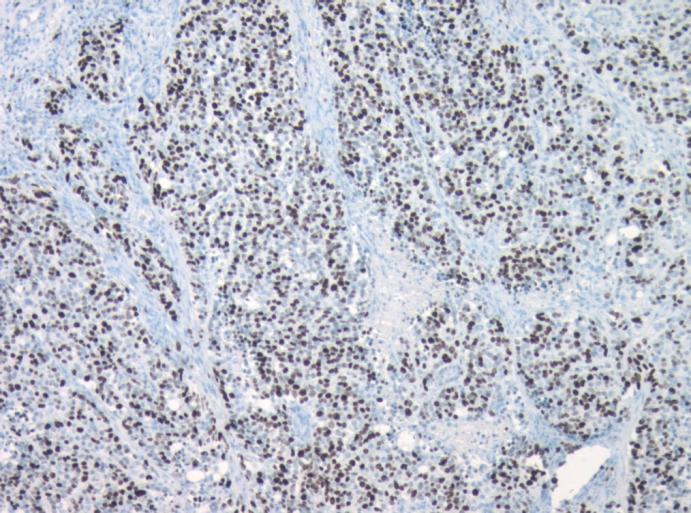
11 Pathology of Carcinoids: Ki67 11




12 WHO Classification Groups NETs by Diagnostic Factors Good Prognosis of Patients With NETs Poor WHO classification Well-differentiated neuroendocrine tumor Well-differentiated neuroendocrine carcinoma Poorly differentiated neuroendocrine carcinoma Biological behavior Low malignancy Low malignancy High malignancy Metastases + + Ki-67 index (%) <2 >2 >10 Infiltration, angioinvasion Tumor size cm >2 cm Any size >2 cm >3 cm 12

13 Survival Is Associated With Tumor Grade 13



14 Advanced TNM Stage Confers Worse Prognosis In localized NET, 5-year survival rates after resection range from 60 to 90% With regional lymph node involvement 5-year survival rates after surgery 50-75% Distant metastases decrease 5 year survival rate to 25-40% 14
15 Biochemical Markers: 5-HIAA 24 hour urine 5-HIAA ( metabolite of serotonin) Sensitivity 73%, specificity 100% Serotonin rich food affect accuracy 50% reduction from pre-treatment levels indicative of response Chronic elevation of 5-HIAA has been linked to carcinoid heart disease 5-HIAA= 5-hydroxyindoleacetic acid 15
16 Biochemical Markers: Chromogranin A Elevated in % of patients, irrespective of functional status Specificity 98.4%, sensitivity >62.9% Can be helpful when 5-HIAA is negative Other conditions cause increased CgA levels with falsepositive results Inflammatory conditions, renal insufficiency, type A gastritis, treatment with PPI Change over time may be more useful as CgA levels independent of symptoms Issues: availability and methods of determination 16


17 Chromogranin A (CgA) Serum CgA as an indication of tumor extent 5 year survival >5 liver met <5 liver met Lymph node met CgA measurements have become one of the most important parameters for NET diagnosis and monitoring 17
18 CgA Levels: Diagnostic and Prognostic Values Correlation between serum CgA level and Ø Tumor burden Ø Number of metastases Ø Symptoms Can indicate tumor activity in cases where imaging shows tumor volume is unchanged Independent predictor of survival data show Q-RT-PCR of CgA mrna can detect micrometastases currently undetectable with immunoassays 18
19 CgA: an Indicator of Disease Recurrence 10 CgA (nmol/l) CT neg US neg Octreoscan neg CT neg US neg PET neg US neg US shows liver metastases Interferon Months 19

20 Indium In-111 Pentetreotide (Octreoscan ) Detects and localizes primaries and metastases Octreoscan image Staging of NETs Patient follow-up to evaluate recurrence Selection of patients with metastatic disease for peptide receptor radionuclide therapy Highly sensitive for carcinoid tumours Similar specificity for functioning and nonfunctioning tumours 20
21 Constellation of Symptoms Can Make a Differential Diagnosis Difficult Nonspecific Symptoms Are Common to Multiple Diagnoses Menopause Functional Bowel Disease Food Allergy Neurosis NET Symptoms Sweating Flushing Diarrhea Intermittent abdominal pain Bronchoconstriction GI bleeding Cardiac disease Irritable Bowel Syndrome Alcoholism Asthma Thyrotoxicosis Anxiety Peptic Ulcer 21





22 Nonspecific Symptoms Lead to a Delayed Diagnosis Presents to primary care Referred to multiple specialists Seen by gastroenterologist or other specialist who orders imaging Surgeon, pathologist perform biopsy or resection Vague abdominal symptoms May be diagnosed as IBS May be referred to specialists for evaluation when symptoms do not resolve Symptoms become worse or patient consults for another reason Diagnosis remains unclear A referral leads to a scan or patient scanned for another reason Liver metastasis or primary lesion is visualized May be an incidental finding Biopsy provides diagnosis of NET Patient is referred to surgical oncologist, medical oncologist, or endocrinologist Treatment depends on stage, histology, symptoms Estimated time to diagnosis: 5 to 7 years 22
23 Symptoms that Should Raise Index of Suspicion Cutaneous flushing ( in up to 94% of patients) begins as erythema of face and neck, may spread and is accompanied by a sensation of warmth May persist for minutes or hours Wheezing Asthma-like symptoms Chronic diarrhea (in up to 80% of patients) 2 to 30 watery stools/day, may be accompanied by abdominal pain, cramping Symptoms of right-sided heart failure Tricuspid valve regurgitation and pulmonic stenosis 23
24 Surgery Surgery of the primary tumour Mainstay of treatment, whatever the stage, when technically feasible Oncologic resection Even in the presence of non-resectable metastases, always resect primary Likely improves outcome Prophylactic cholecystectomy Surgery the only potentially curative treatment 24
25 Liver Metastases Surgical intervention can be palliative limited liver resection Resection may be combined with other ablation techniques Multiple liver metastases Debulking surgery, radio-frequency ablation, cryoablation, chemoembolization, medical therapy 25
26 Embolization of Liver Metastases Embolization/ or chemoembolization, can reduce symptoms and liver metastases Chemical response: 70 90% Tumour reduction: 30 50% Symptomatic response lasting months Mortality rate 7% Contraindications: complete portal vein obstruction, hepatic insufficiency, >50% of liver volume involved, ascites, tumours >7 cm, non-permissive vascular supply Complications: gallbladder necrosis, acute renal failure, pancreatitis, liver abscess 26
27 Medical Treatment: Principles Goals of carcinoid tumour management Symptom control Biochemical control Objective tumour control Improving quality of life Strategies differ for functioning and non-functioning tumours Alternative management Isotope therapy Addition of interferon and/or chemotherapy 27

28 Octreotide: A Somatostatin Analogue Octreotide D phe cys phe D trp Human somatostatin ala gly cys lys asn phe phe trp thr ol cys thr lys cys ser thr phe thr lys Amino acids essential for receptor binding Half life: 90 minutes Half life : 3 minutes 28

29 Medical Treatment: Somatostatin Analogues Can relieve symptoms and decrease hormone levels Use to prevent/treat carcinoid crises before, during and after procedures such as surgery and embolization Treatment likely to be lifelong 29
30 Safety: Adverse Events Hair loss Vomiting Nausea Steatorrhea Abdominal Pain Flatulence Diarrhea Loose stools th Injection 1st Injection Patients(%) 30
31 Somatostatin Analogues in Asymptomatic Carcinoid Tumours: Heated debate! Somatostatin analogues may have a role in tumour stabilization or regression, regardless of the secretory status of the tumour Treatment with somatostatin analogues should be considered for asymptomatic patients with elevated 5-HIAA (>70 mg/24 h) 31
32 Advantages of Sandostatin LAR Convenient once-monthly dosing Increased patient compliance Stable serum octreotide concentrations Sustained suppression of GH and IGF-1 Effective clinical improvement 32
33 Medical Treatment: Interferon-Alfa Inhibits Protein and hormone synthesis Angiogenesis Stimulates immune system Primary medical treatment for lowproliferating gastroenteropancreatic tumours Used as second-line therapy Combination with SSAs has additive and possible synergistic effects 33
34 Medical Treatment: Cytotoxic Treatment Tumours with high proliferative capacity (Ki67 >5 10%) Midgut tumours with low proliferation (Ki67 <2%) will not benefit Agents Single agents: limited benefit Combinations Streptozotocin + 5-FU + doxorubicin: response rate >50% Etoposide + cisplatin: 67% response rate in poorly differentiated NETs Standard endpoints are not always valid evaluations of benefits 34
35 Peptide Receptor Radionuclide Therapy Radionuclide attached to octreotide (binds to SSR 2 and 5) Molecule internalized and delivers radiation energy Radionuclides Indium 111 Yttrium 90 (less favorable) Lutetium 177 ( increasing importance) Results and tolerance differ with radionuclide Availability? Centres of expertise 35
36 Monitoring and Follow-up: Recommendations Symptomatic patient Follow-up depends on aggressiveness of disease In second and subsequent years, follow-up every 4 6 months are appropriate, with annual OctreoScan OctreoScan or MIBG if surgery, radiation or a change in treatment modality is considered Asymptomatic patient Watchful waiting Following complete resection, follow-up every year, with an annual evaluation of 5-HIAA, CgA and MIBG If any results positive, consider CT and OctreoScan 36
37 Carcinoid Heart Disease (40%) Associated with release of serotonin and other vasoactive substances Most common lesions Tricuspid regurgitation / stenosis pulmonary regurgitation / stenosis Right ventricular failure major cause of morbidity and mortality Commonly associated with chronic elevations of 5 HIAA 37

38 Carcinoid heart disease: pathology Pathology: Thickening of right heart valves due to formation of fibrotic plaques Affects valve function Leads to valve insufficiency, heart failure Involvement of left side of heart uncommon 38
39 Carcinoid Heart Disease: Recommendations Echocardiogram at diagnosis; annually if predisposed to carcinoid heart disease Patients with 5-HIAA levels of >50 mg/24 hours should be considered for octreotide therapy Cytoreductive surgery to reduce number of serotonin receptors Follow-up with a cardiologist, particularly those with any cardiac changes or elevated 5-HIAA Cardiac valve replacement may be indicated 39
40 Somatostatin Analogues: Asymptomatic Carcinoid Tumours: Answer to the debate! Somatostatin analogues may have a role in tumour stabilization or regression, regardless of the secretory status of the tumour 40

41 PROMID study objective and design To evaluate the antitumor effect of octreotide LAR Randomized, double-blind, placebo-controlled, Phase III 85 patients treated from a planned
42 Significantly increases TTP when hepatic tumor load 10% Patients with tumor load 10% Patients with tumor load >10% Octreotide LAR: 32 patients / 18 events Median TTP months Octreotide LAR: 10 patients / 8 events Median TTP months Proportion without progression Placebo: 32 patients / 31 events Median TTP 7.21 months Stratified log-rank test P<0.0001; HR=0.26 [95% CI: ] Proportion without progression Placebo: 11 patients / 10 events Median TTP 5.45 months Stratified log-rank test P=0.345; HR=0.64 [95% CI: Time (months) Time (months) Based on the ITT analysis 42
43 Prognostic factors for TTP Most favorable treatment outcome in: Hepatic tumor load <10% (P<0.0009) Resected primary (P<0.0104) Benefit of octreotide LAR versus placebo seen irrespective of Functioning or non-functioning NETs Elevated or non-elevated CgA 43

44 CLARINET CLARINET(Placebo Controlled study of Lanreotide Antiproliferative Response In Neuro-Endocrine Tumors)- 1 end point PFS; intestinal and pancreatic non-functional NET+ well controlled gastrinomas; Ki 3-10% in 22% pts 44

45 PROMID vs. CLARINET 45
46 Clinical Implications of PROMID / CLARINET Results A Significant achievement in the context of an uncommon tumor The use of LAR should be indicated in the following clinical settings: 1. Asymptomatic patients with progressive disease 2. Asymptomatic patients with stable disease particularly if 5 HIAA rising 3. As adjuvant therapy post resection? 46



47 Sunitinib Phase III Study: Randomized, Double-Blind Study Design (placebo-controlled) 47
48 RADIANT (progressive advanced PNET, Hx of carcinoid syndrome) 48

49 Ongoing Studies 49

50 What Does a Multi-Disciplinary Team Look Like? 50

 Capacity for clinical research Patient")
51 This is How a Multi-Disciplinary Team Should Look Like? Multiple HCPs involved in the Patient Journey through NET diagnosis and treatment Advance training on NET diagnosis and treatment for each HCP Patient management optimized through tumor board and/or NET treatment protocols Patient Gastr.Ent Support gp Endocr. NET Regional Referral Center NET Treatment Guidelines NET Tumor Board Radiology Dedicated medical education on NET (rounds) Capacity for clinical research Patient Outreach Initiatives & Support Utilization of latest Biomarker & Imaging techniques Disease Registry/Tumor Bank Nucl Med We Forgot the Nurses!! Tansplant Tumor Board Surgeon Oncologist Patholo 51


52 Multidisiplinary Treatment: Impact on Outcome Multidisciplinary treatment approach associated with improvement in patient outcomes Most individual physicians do not have specialized knowledge of NET due to low patient loads Optimal patient management is achieved through a multidisciplinary approach that takes advantage of multiple sources of expertise Diagnostic procedures should be critically reviewed to help establish consensus on the best evidence-based management Noticeable improvements in survival in the MRC setting THANK YOU 52
53 Treatment Algorithm Part I NET Locoregional Metastatic Resectable Unresectable Resectable Follow up Follow up NED Metaststic Recurrence Resectable Unresectable or metastic Resectable Low proliferative index Ki67 10% High proliferative index Ki67 > 10% Watchful observation Consider systemic chemotherapy NED: No evidence of disease Kocha W, et al. Submitted for publication
54 Treatment Algorithm Part II Liver only or Liver dominant Extrahepatic disease Early consideration of primary debulking in abdomen Stable disease Watchful observation Consider transplant Debulking measures (alone or in combination): Surgery RFA Hepatic arterial infusion Observation Debulking measures (alone or in combination): Surgery RFA Hepatic arterial infusion Medical management: Symptomatic treatment Somatostatin analogues Interferon Radiopeptide therapy Progression RFA: Radiofrequency ablation Kocha W, et al. Submitted for publication Clinical trials Chemotherapy/targeted therapy Refer to a centre of expertise 54
NET und NEC. Endoscopic and oncologic therapy
 NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
NET und NEC Endoscopic and oncologic therapy Classification well-differentiated NET - G1 and G2 - carcinoid poorly-differentiated NEC - G3 - like SCLC well differentiated NET G3 -> elevated proliferation
Neuroendocrine Tumors
 Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
Neuroendocrine Tumors Neuroendocrine tumors arise from cells that release a hormone in response to a signal from the nervous system. Neuro refers to the nervous system. Endocrine refers to the hormones.
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors
 Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
Gastrointestinal Neuroendocrine Tumors: A Closer Look at the Characteristics of These Diverse Tumors Jaume Capdevila, MD, PhD Vall d'hebron University Hospital Vall d'hebron Institute of Oncology (VHIO)
GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust
 GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust Introduction Carcinoid was old term, introduced in 1906 by German pathologist Cancinoma like More recent
GI CARCINOID Dr Mussawar Iqbal Consultant Oncologist Hull and East Yorkshire Hospitals NHS Trust Introduction Carcinoid was old term, introduced in 1906 by German pathologist Cancinoma like More recent
TRACTAMENT ONCOLÒGIC DELS TUMORS NEUROENDOCRINS METASTÀSICS
 TRACTAMENT ONCOLÒGIC DELS TUMORS NEUROENDOCRINS METASTÀSICS Jaume Capdevila Unitat de Tumors GI i Endocrins Hospital Universitari Vall d Hebron Barcelona Experts, acollidors i solidaris OUTLINE BACKGROUND
TRACTAMENT ONCOLÒGIC DELS TUMORS NEUROENDOCRINS METASTÀSICS Jaume Capdevila Unitat de Tumors GI i Endocrins Hospital Universitari Vall d Hebron Barcelona Experts, acollidors i solidaris OUTLINE BACKGROUND
NET εντέρου Τι νεότερο/ Νέες μελέτες. Μαντώ Νικολαΐδη παθολόγος-ογκολόγος ΜΗΤΕΡΑ
 NET εντέρου Τι νεότερο/ Νέες μελέτες Μαντώ Νικολαΐδη παθολόγος-ογκολόγος ΜΗΤΕΡΑ NET: A Diverse Group of Malignancies 1-3 Wide spectrum of malignancies arising in neuroendocrine cells throughout the body
NET εντέρου Τι νεότερο/ Νέες μελέτες Μαντώ Νικολαΐδη παθολόγος-ογκολόγος ΜΗΤΕΡΑ NET: A Diverse Group of Malignancies 1-3 Wide spectrum of malignancies arising in neuroendocrine cells throughout the body
Gastrinoma: Medical Management. Haley Gallup
 Gastrinoma: Medical Management Haley Gallup Also known as When to put your knife down Gastrinoma Definition and History Diagnosis Historic Management Sporadic vs MEN-1 Defining surgical candidates Nonsurgical
Gastrinoma: Medical Management Haley Gallup Also known as When to put your knife down Gastrinoma Definition and History Diagnosis Historic Management Sporadic vs MEN-1 Defining surgical candidates Nonsurgical
EXOCRINE: 93% Acinar Cells Duct Cells. ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others
 EXOCRINE: 93% Acinar Cells Duct Cells Digestive Enzymes Trypsin: Digests Proteins Lipases: Digests Fats Amylase: Digest Carbohydrates ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others Hormones Glucagon
EXOCRINE: 93% Acinar Cells Duct Cells Digestive Enzymes Trypsin: Digests Proteins Lipases: Digests Fats Amylase: Digest Carbohydrates ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others Hormones Glucagon
Color Codes Pathology and Genetics Medicine and Clinical Pathology Surgery Imaging
 Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
Saturday, November 5, 2005 8:30-10:30 a. m. Poorly Differentiated Endocrine Carcinomas Chairman: E. Van Cutsem, Leuven, Belgium 9:00-9:30 a. m. Working Group Sessions Pathology and Genetics Group leaders:
Diagnosing and monitoring NET
 Diagnosing and monitoring NET Inaccurate or delayed diagnosis of neuroendocrine tumors (NET) is common, because many NET are small and asymptomatic. 1 When symptoms are present, they are usually nonspecific
Diagnosing and monitoring NET Inaccurate or delayed diagnosis of neuroendocrine tumors (NET) is common, because many NET are small and asymptomatic. 1 When symptoms are present, they are usually nonspecific
MEDICAL MANAGEMENT OF METASTATIC GEP-NET
 MEDICAL MANAGEMENT OF METASTATIC GEP-NET Jeremy Kortmansky, MD Associate Professor of Clinical Medicine Yale Cancer Center DISCLOSURES: NONE Introduction Gastrointestinal and pancreatic neuroendocrine
MEDICAL MANAGEMENT OF METASTATIC GEP-NET Jeremy Kortmansky, MD Associate Professor of Clinical Medicine Yale Cancer Center DISCLOSURES: NONE Introduction Gastrointestinal and pancreatic neuroendocrine
Case Presentation. Marianne Ellen Pavel. Charité University Medicine Berlin. ESMO Preceptorship on GI Neuroendocrine Tumors
 Case Presentation Marianne Ellen Pavel Charité University Medicine Berlin ESMO Preceptorship on GI Neuroendocrine Tumors Session 3; Singapore November 2, 2012 06.11.2012 Medical History 46-year-old man
Case Presentation Marianne Ellen Pavel Charité University Medicine Berlin ESMO Preceptorship on GI Neuroendocrine Tumors Session 3; Singapore November 2, 2012 06.11.2012 Medical History 46-year-old man
FRANKLY SPEAKING ABOUT CANCER: NEUROENDOCRINE & CARCINOID TUMORS (NETS)
") FRANKLY SPEAKING ABOUT CANCER: NEUROENDOCRINE & CARCINOID TUMORS (NETS) Gilda s Club Quad Cities November 5 th, 2018 Joseph Dillon, MD Neuroendocrine Tumor Clinic University of Iowa Hospitals & Clinics
FRANKLY SPEAKING ABOUT CANCER: NEUROENDOCRINE & CARCINOID TUMORS (NETS) Gilda s Club Quad Cities November 5 th, 2018 Joseph Dillon, MD Neuroendocrine Tumor Clinic University of Iowa Hospitals & Clinics
Systemic Therapy for Gastroenteropancreatic (GEP) Neuroendocrine Tumors and Lung Carcinoid
 Neuroendocrine Tumors and Lung Carcinoid") Systemic Therapy for Gastroenteropancreatic (GEP) Neuroendocrine Tumors and Lung Carcinoid The Medical Oncology Perspective Nevena Damjanov, MD Associate professor Abramson Cancer Center of the University
Systemic Therapy for Gastroenteropancreatic (GEP) Neuroendocrine Tumors and Lung Carcinoid The Medical Oncology Perspective Nevena Damjanov, MD Associate professor Abramson Cancer Center of the University
NEUROENDOCRINE CARCINOID TUMORS PANCREATIC NEUROENDOCRINE TUMORS
 University of Miami Jackson Memorial Hospital Role of the Surgeon in the Approach to Neuroendocrine tumors Dido Franceschi, MD Professor of Surgery University of Miami Karzinoide Siegfried Oberndorfer,
University of Miami Jackson Memorial Hospital Role of the Surgeon in the Approach to Neuroendocrine tumors Dido Franceschi, MD Professor of Surgery University of Miami Karzinoide Siegfried Oberndorfer,
An Overview of NETS. Richard R.P. Warner M.D
 An Overview of NETS Richard R.P. Warner M.D Diagnosis and Treatment Approaches Carcinoid (and other NETs) not as benign as originally described 13-50% of all carcinoids have distant metastases when first
An Overview of NETS Richard R.P. Warner M.D Diagnosis and Treatment Approaches Carcinoid (and other NETs) not as benign as originally described 13-50% of all carcinoids have distant metastases when first
To introduce the Interdisciplinary Neuroendocrine care team model at London Health Sciences Centre/London Regional Cancer Program
 To introduce the Interdisciplinary Neuroendocrine care team model at London Health Sciences Centre/London Regional Cancer Program To highlight the decision making process, treatment recommendations and
To introduce the Interdisciplinary Neuroendocrine care team model at London Health Sciences Centre/London Regional Cancer Program To highlight the decision making process, treatment recommendations and
Neuroendocrine Tumors
 Carcinoid tumours: origin Neuroendocrine Tumors THE A, B,C s Bronchopulmonary system Other 8% 28% Carcinoid site Digestive system 64% 2.3 28 28.5 Other Colon and rectum Small intestine Colon, except appendix
Carcinoid tumours: origin Neuroendocrine Tumors THE A, B,C s Bronchopulmonary system Other 8% 28% Carcinoid site Digestive system 64% 2.3 28 28.5 Other Colon and rectum Small intestine Colon, except appendix
PNET 3/7/2015. GI and Pancreatic NETs. The Postgraduate Course in Breast and Endocrine Surgery. Decision Tree. GI and Pancreatic NETs.
 GI and Pancreatic NETs The Postgraduate Course in Breast and Endocrine Surgery Disclosures Ipsen NET Advisory Board Marines Memorial Club and Hotel San Francisco, CA Eric K Nakakura San Francisco, CA March
GI and Pancreatic NETs The Postgraduate Course in Breast and Endocrine Surgery Disclosures Ipsen NET Advisory Board Marines Memorial Club and Hotel San Francisco, CA Eric K Nakakura San Francisco, CA March
Pathology testing and Neuroendocrine tumours (NETs)
") Pathology testing and Neuroendocrine tumours (NETs) NETs are probably far more common than we think. Most grow so slowly and produce such widely varied and non-specific symptoms, or no symptoms at all,
Pathology testing and Neuroendocrine tumours (NETs) NETs are probably far more common than we think. Most grow so slowly and produce such widely varied and non-specific symptoms, or no symptoms at all,
Hot of the press. Γρηγόριος Καλτσάς MD FRCP Καθηγητής Παθολογίας Ενδοκρινολογίας ΕΚΠΑ
 Hot of the press Γρηγόριος Καλτσάς MD FRCP Καθηγητής Παθολογίας Ενδοκρινολογίας ΕΚΠΑ Outline Diagnostic developments Histopathology Molecular Therapeutic developments Results on PRRT Telotristat in carcinoid
Hot of the press Γρηγόριος Καλτσάς MD FRCP Καθηγητής Παθολογίας Ενδοκρινολογίας ΕΚΠΑ Outline Diagnostic developments Histopathology Molecular Therapeutic developments Results on PRRT Telotristat in carcinoid
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL NEUROENDOCRINE GASTRO-ENTERO-PANCREATIC TUMOURS GI Site Group Neuroendocrine gastro-entero-pancreatic tumours Authors: Dr.
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GASTROINTESTINAL NEUROENDOCRINE GASTRO-ENTERO-PANCREATIC TUMOURS GI Site Group Neuroendocrine gastro-entero-pancreatic tumours Authors: Dr.
Community Case. Saeed Awan R5
 Community Case Saeed Awan R5 18 year old presents to ER with history of pain right lower quadrant for three days. Nauseated, denies vomiting and bowel movements normal and no urinary complaint. Admitted
Community Case Saeed Awan R5 18 year old presents to ER with history of pain right lower quadrant for three days. Nauseated, denies vomiting and bowel movements normal and no urinary complaint. Admitted
Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology
 Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology OUTLINE Molecular Rationale for the use of SSAs in
Jaume Capdevila, MD GI and Endocrine Tumor Unit Vall d Hebron University Hospital Developmental Therapeutics Unit Vall d Hebron Institute of Oncology OUTLINE Molecular Rationale for the use of SSAs in
Lu 177-Dotatate (Lutathera) Therapy Information
 Therapy Information") Lu 177-Dotatate (Lutathera) Therapy Information Information for Lu 177-dotatate therapy also known as Lutathera, for the treatment of metastatic midgut neuroendocrine tumor and other metastatic neuroendocrine
Lu 177-Dotatate (Lutathera) Therapy Information Information for Lu 177-dotatate therapy also known as Lutathera, for the treatment of metastatic midgut neuroendocrine tumor and other metastatic neuroendocrine
Toward More Aggressive Management of Neuroendocrine Tumors: Current and Future Perspectives
 Toward More Aggressive Management of Neuroendocrine Tumors: Current and Future Perspectives Moderator: Ashley Grossman, MD, FRCP Professor of Neuroendocrinology William Harvey Research Institute Barts
Toward More Aggressive Management of Neuroendocrine Tumors: Current and Future Perspectives Moderator: Ashley Grossman, MD, FRCP Professor of Neuroendocrinology William Harvey Research Institute Barts
Neuroendocrine Tumors: Just the Basics. George Fisher, MD PhD
 Neuroendocrine Tumors: Just the Basics George Fisher, MD PhD Topics that we will not discuss Some types of lung cancer: Small cell neuroendocrine lung cancer Large cell neuroendocrine lung cancer Some
Neuroendocrine Tumors: Just the Basics George Fisher, MD PhD Topics that we will not discuss Some types of lung cancer: Small cell neuroendocrine lung cancer Large cell neuroendocrine lung cancer Some
NEUROENDOCRINE TUMOURS Updated December 2015 by Dr. Doreen Ezeife (PGY-5 Medical Oncology Resident, University of Calgary)
") NEUROENDOCRINE TUMOURS Updated December 2015 by Dr. Doreen Ezeife (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Cynthia Card (Staff Medical Oncologist, University of Calgary)
NEUROENDOCRINE TUMOURS Updated December 2015 by Dr. Doreen Ezeife (PGY-5 Medical Oncology Resident, University of Calgary) Reviewed by Dr. Cynthia Card (Staff Medical Oncologist, University of Calgary)
Review of Gastrointestinal Carcinoid Tumors: Latest Therapies
 Review of Gastrointestinal Carcinoid Tumors: Latest Therapies Arvind Dasari, MD, MS Department of Gastrointestinal Medical Oncology The University of Texas MD Anderson Cancer Center Houston, TX, USA Neuroendocrine
Review of Gastrointestinal Carcinoid Tumors: Latest Therapies Arvind Dasari, MD, MS Department of Gastrointestinal Medical Oncology The University of Texas MD Anderson Cancer Center Houston, TX, USA Neuroendocrine
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary)
") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary) Staff Reviewers: Dr. Yoo Joung Ko (Medical Oncologist, Sunnybrook Odette Cancer
Management of Pancreatic Islet Cell Tumors
 Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
Management of Pancreatic Islet Cell Tumors Ravi Dhanisetty, MD November 5, 2009 Morbidity and Mortality Conference Case Presentation 42 yr female with chronic abdominal pain. PMHx: Uterine fibroids Medications:
EXOCRINE: 93% Acinar Cells Duct Cells. ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others
 EXOCRINE: 93% Acinar Cells Duct Cells Digestive Enzymes Trypsin: Digests Proteins Lipases: Digests Fats Amylase: Digest Carbohydrates ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others Hormones Glucagon
EXOCRINE: 93% Acinar Cells Duct Cells Digestive Enzymes Trypsin: Digests Proteins Lipases: Digests Fats Amylase: Digest Carbohydrates ENDOCRINE: 5% Alpha Cells Beta Cells Delta Cells Others Hormones Glucagon
Your Medical Details and Treatment Tracker. About You
 This document is intended to help you keep a record of important details that you may need to share with healthcare professionals throughout your Living with Neuroendocrine Tumours (NETs) journey. Take
This document is intended to help you keep a record of important details that you may need to share with healthcare professionals throughout your Living with Neuroendocrine Tumours (NETs) journey. Take
WHAT TO EXPECT IN 2015? - Renuka Iyer, MD Associate Professor of Medicine, University at Buffalo Associate Professor of Oncology, Roswell Park Cancer
 WHAT TO EXPECT IN 2015? - Renuka Iyer, MD Associate Professor of Medicine, University at Buffalo Associate Professor of Oncology, Roswell Park Cancer Institute Overview Diagnosis: Gallium scan Biomarkers
WHAT TO EXPECT IN 2015? - Renuka Iyer, MD Associate Professor of Medicine, University at Buffalo Associate Professor of Oncology, Roswell Park Cancer Institute Overview Diagnosis: Gallium scan Biomarkers
Hepatic metastases of neuroendocrine tumors: treatment options and outcomes of local patients treated with radioembolization
 Hepatic metastases of neuroendocrine tumors: treatment options and outcomes of local patients treated with radioembolization JP King PGY2 May 22, 2015 Neuroendocrine Tumor (NET) WHO Classification Location
Hepatic metastases of neuroendocrine tumors: treatment options and outcomes of local patients treated with radioembolization JP King PGY2 May 22, 2015 Neuroendocrine Tumor (NET) WHO Classification Location
NICaN Pancreatic Neuroendocrine Tumour SACT protocols. 1.0 Dr M Eatock Final version issued
 Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Neuro-endocrine Tumours Dr Martin Eatock, Consultant Medical Oncologist & on behalf of the GI Oncologists Group,
Reference No: Title: Author(s) Systemic Anti-Cancer Therapy (SACT) Guidelines for Pancreatic Neuro-endocrine Tumours Dr Martin Eatock, Consultant Medical Oncologist & on behalf of the GI Oncologists Group,
Treatment algorithm Neuroendocrine tumours. Gregory Kaltsas Endocrine Unit, Department of Pathophysiology, University of Athens, Greece
 Treatment algorithm Neuroendocrine tumours Gregory Kaltsas Endocrine Unit, Department of Pathophysiology, University of Athens, Greece Outline Presenting a meaningful algorithm Means used to develop algorithm
Treatment algorithm Neuroendocrine tumours Gregory Kaltsas Endocrine Unit, Department of Pathophysiology, University of Athens, Greece Outline Presenting a meaningful algorithm Means used to develop algorithm
Octreotide LAR in neuroendocrine tumours a summary of the experience
 Endocrinology in oncology Review article Octreotide LAR in neuroendocrine tumours a summary of the experience Agnieszka Kolasińska-Ćwikła, MD, PhD Department of Chemotherapy, Oncology Clinic, Maria Sklodowska-Curie
Endocrinology in oncology Review article Octreotide LAR in neuroendocrine tumours a summary of the experience Agnieszka Kolasińska-Ćwikła, MD, PhD Department of Chemotherapy, Oncology Clinic, Maria Sklodowska-Curie
Pancreatic neuroendocrine cancer with liver metastases and multiple peritoneal metastases: report of one case
 Case Report Pancreatic neuroendocrine cancer with liver metastases and multiple peritoneal metastases: report of one case Yang Wang, Dongbing Zhao Department of Abdominal Surgery, Cancer Institute & Hospital,
Case Report Pancreatic neuroendocrine cancer with liver metastases and multiple peritoneal metastases: report of one case Yang Wang, Dongbing Zhao Department of Abdominal Surgery, Cancer Institute & Hospital,
Peptide Receptor Radionuclide Therapy using 177 Lu octreotate
 Peptide Receptor Radionuclide Therapy using 177 Lu octreotate BLR Kam, Erasmus Medical Centre, Rotterdam DJ Kwekkeboom, Erasmus Medical Centre, Rotterdam Legal aspects As 177 Lu-[DOTA 0 -Tyr 3 ]octreotate
Peptide Receptor Radionuclide Therapy using 177 Lu octreotate BLR Kam, Erasmus Medical Centre, Rotterdam DJ Kwekkeboom, Erasmus Medical Centre, Rotterdam Legal aspects As 177 Lu-[DOTA 0 -Tyr 3 ]octreotate
NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction
 NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Diagnostic & therapeutic
NeuroEndocrine Tumors Diagnostic and therapeutic challenges: introduction Prof Eric Van Cutsem, MD, PhD Gastroenterology/Digestive Oncology Leuven, Belgium Eric.VanCutsem@uzleuven.be Diagnostic & therapeutic
Neuroendocrine & Carcinoid Tumors
 Neuroendocrine & Carcinoid Tumors Acknowledgment This slide set was medically reviewed by Dr. Yi-Zarn Wang, DDS, PC, MD, FACS in August 2018. Workshop Overview Introductions What Are Neuroendocrine Tumors
Neuroendocrine & Carcinoid Tumors Acknowledgment This slide set was medically reviewed by Dr. Yi-Zarn Wang, DDS, PC, MD, FACS in August 2018. Workshop Overview Introductions What Are Neuroendocrine Tumors
Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms
 Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms Dr. Claudia LY WONG, Department of Surgery, Kwong Wah Hospital Joint Hospital Surgical Grand Round Presentation,
Management of an Appendiceal Mass - Approach to acute presentation of appendiceal neoplasms Dr. Claudia LY WONG, Department of Surgery, Kwong Wah Hospital Joint Hospital Surgical Grand Round Presentation,
Surgical Therapy of GEP-NET: An Overview
 Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Surgical Therapy of GEP-NET: An Overview Pierce K.H Chow MBBS, MMed, FRCSE, FAMS, PhD Professor, Duke-NUS Graduate School of Medicine Senior Consultant Surgeon, Singapore General Hospital Visiting Senior
Update on Surgical Management of NETs
 Update on Surgical Management of Neuroendocrine Tumors James R. Howe, M.D. Director, Surgical Oncology and Endocrine Surgery University of Iowa College of Medicine Distribution of NETs 2000-2004 27% ---
Update on Surgical Management of Neuroendocrine Tumors James R. Howe, M.D. Director, Surgical Oncology and Endocrine Surgery University of Iowa College of Medicine Distribution of NETs 2000-2004 27% ---
A) PUBLIC HEALTH B) PRESENTATION & DIAGNOSIS
 PUBLIC HEALTH B) PRESENTATION & DIAGNOSIS") Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary), April 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Centre, BC Cancer
Hepatocellular Carcinoma HCC Updated November 2015 by: Dr. Mohammed Alghamdi (Medical Oncology Fellow, University of Calgary), April 2017 by Dr. Jenny Ko (Medical Oncologist, Abbotsford Centre, BC Cancer
Imaging of Neuroendocrine Metastases
 Imaging of Neuroendocrine Metastases Aoife Kilcoyne, Shaunagh McDermott, Colin McCarthy,Manuel Patino, Dushyant Sahani, Michael Blake Abdominal Imaging Division Massachusetts General Hospital Disclosure
Imaging of Neuroendocrine Metastases Aoife Kilcoyne, Shaunagh McDermott, Colin McCarthy,Manuel Patino, Dushyant Sahani, Michael Blake Abdominal Imaging Division Massachusetts General Hospital Disclosure
Index. Surg Oncol Clin N Am 15 (2006) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 15 (2006) 681 685 Index Note: Page numbers of article titles are in boldface type. A Ablative therapy, for liver metastases in patients with neuroendocrine tumors, 517 with radioiodine
Surg Oncol Clin N Am 15 (2006) 681 685 Index Note: Page numbers of article titles are in boldface type. A Ablative therapy, for liver metastases in patients with neuroendocrine tumors, 517 with radioiodine
SIRT in the Management of Metastatic Neuroendocrine Tumors
 SIRT in the Management of Metastatic Neuroendocrine Tumors Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director,
SIRT in the Management of Metastatic Neuroendocrine Tumors Navesh K. Sharma, DO, PhD Assistant Professor, Departments of Radiation Oncology, Diagnostic Radiology and Nuclear Medicine Medical Director,
Neuroendocrine Tumours If you don t suspect it you can t detect it! Dr JWS Devar HPB Surgeon University of Witwatersrand E-AHPBA CHBAH & WDGMC
 Neuroendocrine Tumours If you don t suspect it you can t detect it! Dr JWS Devar HPB Surgeon University of Witwatersrand E-AHPBA CHBAH & WDGMC Case Study 43 yr old female with a history of a left mastectomy
Neuroendocrine Tumours If you don t suspect it you can t detect it! Dr JWS Devar HPB Surgeon University of Witwatersrand E-AHPBA CHBAH & WDGMC Case Study 43 yr old female with a history of a left mastectomy
Survivorship care of Neuroendocrine Tumours(NETs) from a Specialised Nursing Perspective
 from a Specialised Nursing Perspective") Survivorship care of Neuroendocrine Tumours(NETs) from a Specialised Nursing Perspective Avril Hull, Auckland District Health Board, New Zealand Kate Wakelin, Unicorn Foundation, Australia Philippa Davies,
Survivorship care of Neuroendocrine Tumours(NETs) from a Specialised Nursing Perspective Avril Hull, Auckland District Health Board, New Zealand Kate Wakelin, Unicorn Foundation, Australia Philippa Davies,
Hepatocellular Carcinoma: A major global health problem. David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center
 Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
Hepatocellular Carcinoma: A major global health problem David L. Wood, MD Interventional Radiology Banner Good Samaritan Medical Center Hepatocellular Carcinoma WORLDWIDE The #2 Cancer Killer Overall cancer
2015: Year in Review Results of Recent Trials
 2015: Year in Review Results of Recent Trials Pamela L. Kunz, MD Assistant Professor of Medicine / GI Oncology Director, Stanford NET Program Stanford University School of Medicine Disclosures Research
2015: Year in Review Results of Recent Trials Pamela L. Kunz, MD Assistant Professor of Medicine / GI Oncology Director, Stanford NET Program Stanford University School of Medicine Disclosures Research
Pancreas Quizzes c. Both A and B a. Directly into the blood stream (not using ducts)
") Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Pancreas Quizzes Quiz 1 1. The pancreas produces hormones. Which type of hormone producing organ is the pancreas? a. Endocrine b. Exocrine c. Both A and B d. Neither A or B 2. Endocrine indicates hormones
Grade 2 Ileum NET with liver and bone metastasis
 Grade 2 Ileum NET with liver and bone metastasis BERNARDO MARQUES ENDOCRINOLOGY DEPARTMENT PORTUGUESE INSTITUTE OF ONCOLOGY - COIMBRA April 2018, Lugano, Switzerland JPB, male, 67 years old April 2015
Grade 2 Ileum NET with liver and bone metastasis BERNARDO MARQUES ENDOCRINOLOGY DEPARTMENT PORTUGUESE INSTITUTE OF ONCOLOGY - COIMBRA April 2018, Lugano, Switzerland JPB, male, 67 years old April 2015
SCOPE TODAYS SESSION. Case 1: Case 2. Basic Theory Stuff: Heavy Stuff. Basic Questions. Basic Questions
 MONDAY TEACHING SCOPE TODAYS SESSION Case 1: Basic Questions Case 2 Basic Questions Basic Theory Stuff: AJCC TNM + Stage Group for Carcinoid of the Appendix Management of Carcinoid of the Appendix (NCCN)
MONDAY TEACHING SCOPE TODAYS SESSION Case 1: Basic Questions Case 2 Basic Questions Basic Theory Stuff: AJCC TNM + Stage Group for Carcinoid of the Appendix Management of Carcinoid of the Appendix (NCCN)
TUMORES NEUROENDOCRINOS. Miguel Navarro. Salamanca
 TUMORES NEUROENDOCRINOS Miguel Navarro. Salamanca Introduction to Neuroendocrine Tumours (NETs) NETs are relatively RARE At least 40 different entities are described arising in different organs. Different
TUMORES NEUROENDOCRINOS Miguel Navarro. Salamanca Introduction to Neuroendocrine Tumours (NETs) NETs are relatively RARE At least 40 different entities are described arising in different organs. Different
Cutting Edge Treatment of Neuroendocrine Tumors
 Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Cutting Edge Treatment of Neuroendocrine Tumors
 Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
Cutting Edge Treatment of Neuroendocrine Tumors Daneng Li, MD Assistant Clinical Professor Department of Medical Oncology & Therapeutics Research City of Hope Click to edit Master Presentation Date DISCLOSURE
SURGERY OF NETS. Iakovos N Nomikos MD FACS. Director and Chairman, Department of Surgery METAXA Memorial Cancer Hospital Piraeus Greece
 SURGERY OF NETS Iakovos N Nomikos MD FACS Director and Chairman, Department of Surgery METAXA Memorial Cancer Hospital Piraeus Greece Epidemiology 5-fold increase in occurrence of NETS over past 30 years
SURGERY OF NETS Iakovos N Nomikos MD FACS Director and Chairman, Department of Surgery METAXA Memorial Cancer Hospital Piraeus Greece Epidemiology 5-fold increase in occurrence of NETS over past 30 years
OPTIMISING OUTCOMES IN GASTROINTESTINAL NEUROENDOCRINE TUMOURS
 OPTIMISING OUTCOMES IN GASTROINTESTINAL NEUROENDOCRINE TUMOURS Dr Mairéad McNamara Senior lecturer, University of Manchester & Honorary Consultant in Medical Oncology, The Christie NHS Foundation Trust
OPTIMISING OUTCOMES IN GASTROINTESTINAL NEUROENDOCRINE TUMOURS Dr Mairéad McNamara Senior lecturer, University of Manchester & Honorary Consultant in Medical Oncology, The Christie NHS Foundation Trust
A VIPER IN THE COURTYARD L A I L A ABUZA I D, M D
 A VIPER IN THE COURTYARD L A I L A ABUZA I D, M D E N D O C R I N O L O G Y FELLOW NO DISCOLSURES OBJECTIVES: Recognize signs and symptoms of hyperthyroidism Develop a differential diagnosis for a patient
A VIPER IN THE COURTYARD L A I L A ABUZA I D, M D E N D O C R I N O L O G Y FELLOW NO DISCOLSURES OBJECTIVES: Recognize signs and symptoms of hyperthyroidism Develop a differential diagnosis for a patient
Staging & Current treatment of HCC
 Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Staging & Current treatment of HCC Dr.: Adel El Badrawy Badrawy; ; M.D. Staging & Current ttt of HCC Early stage HCC is typically silent. HCC is often advanced at first manifestation. The selective ttt
Sandostatin LAR. Sandostatin LAR (octreotide acetate) Description
 Description") Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.09 Subject: Sandostatin LAR Page: 1 of 5 Last Review Date: March 16, 2018 Sandostatin LAR Description
Federal Employee Program 1310 G Street, N.W. Washington, D.C. 20005 202.942.1000 Fax 202.942.1125 5.30.09 Subject: Sandostatin LAR Page: 1 of 5 Last Review Date: March 16, 2018 Sandostatin LAR Description
Hepatocellular Carcinoma: Diagnosis and Management
 Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Hepatocellular Carcinoma: Diagnosis and Management Nizar A. Mukhtar, MD Co-director, SMC Liver Tumor Board April 30, 2016 1 Objectives Review screening/surveillance guidelines Discuss diagnostic algorithm
Comprehensive treatment of a functional pancreatic neuroendocrine tumor with multifocal liver metastases
 Case Report Comprehensive treatment of a functional pancreatic neuroendocrine tumor with multifocal liver metastases Wei Wang 1,2,3 *, Sharvesh Raj Seeruttun 1,2,3 *, Cheng Fang 1,2,3, Zhiwei Zhou 1,2,3
Case Report Comprehensive treatment of a functional pancreatic neuroendocrine tumor with multifocal liver metastases Wei Wang 1,2,3 *, Sharvesh Raj Seeruttun 1,2,3 *, Cheng Fang 1,2,3, Zhiwei Zhou 1,2,3
Recent developments of oncology in neuroendocrine tumors (NETs)
") Recent developments of oncology in neuroendocrine tumors (NETs) Marc Peeters MD, PhD Coordinator Multidisciplinary Oncological Center Antwerpen (MOCA) Head of the Oncology Department UZA, Professor in
Recent developments of oncology in neuroendocrine tumors (NETs) Marc Peeters MD, PhD Coordinator Multidisciplinary Oncological Center Antwerpen (MOCA) Head of the Oncology Department UZA, Professor in
Selection of Appropriate Treatment
 Expert Review in Metastatic Gastroenteropancreatic Neuroendocrine Tumors (GEP-NETs): Selection of Appropriate Treatment Reference Slide Deck Neuroendocrine Tumors (NETs): A Diverse Group of Malignancies
Expert Review in Metastatic Gastroenteropancreatic Neuroendocrine Tumors (GEP-NETs): Selection of Appropriate Treatment Reference Slide Deck Neuroendocrine Tumors (NETs): A Diverse Group of Malignancies
Jose Ramos. Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma
 Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Role of Surgery in isolated hepatic metastasis from breast carcinoma, melanoma or sarcoma Jose Ramos University of the Witwatersrand Donald Gordon Medical Centre Evolution of liver resection Better understanding
Tumor markers. Chromogranin A. Analyte Information
 Tumor markers Chromogranin A Analyte Information -1-2018-04-22 Chromogranin A Introduction Chromogranin A (CgA) is a 439-amino acid protein with a molecular weight of 48 to 60 kda, depending on glycosylation
Tumor markers Chromogranin A Analyte Information -1-2018-04-22 Chromogranin A Introduction Chromogranin A (CgA) is a 439-amino acid protein with a molecular weight of 48 to 60 kda, depending on glycosylation
Hepatobiliary Malignancies Retrospective Study at Truman Medical Center
 Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
Hepatobiliary Malignancies 206-207 Retrospective Study at Truman Medical Center Brandon Weckbaugh MD, Prarthana Patel & Sheshadri Madhusudhana MD Introduction: Hepatobiliary malignancies are cancers which
Color Codes Pathology and Genetics Medicine and Clinical Pathology Surgery Imaging
 Friday, November 4, 2005 11:00-12:20 a. m. Pancreatic Tumors, Session 3 Chairman: D. O Toole, Clichy, France 11:20-11:50 a. m. Working Group Session Pathology and Genetics Group leaders: J. Y. Scoazec,
Friday, November 4, 2005 11:00-12:20 a. m. Pancreatic Tumors, Session 3 Chairman: D. O Toole, Clichy, France 11:20-11:50 a. m. Working Group Session Pathology and Genetics Group leaders: J. Y. Scoazec,
Nuevas alternativas en el manejo de TNE avanzados
 Nuevas alternativas en el manejo de TNE avanzados Jaume Capdevila Hospital Universitari Vall d Hebron Barcelona Coordinación científica: Dr. Fernando Rivera Hospital Universitario Marqués de Valdecilla,
Nuevas alternativas en el manejo de TNE avanzados Jaume Capdevila Hospital Universitari Vall d Hebron Barcelona Coordinación científica: Dr. Fernando Rivera Hospital Universitario Marqués de Valdecilla,
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options
 State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
State of the art management of Colorectal Liver Metastasis: an interplay of Chemotherapy and Surgical options Ioannis S. Hatzaras, MD, MPH, FACS Assistant Professor of Surgery Division of Surgical Oncology
Learning. A part of your guide to Neuroendocrine Tumours (NETs)
") Learning A part of your guide to Neuroendocrine Tumours (NETs) Your support guide This book will help you better understand NETs. It is however a reference only; you should always go to your doctor or
Learning A part of your guide to Neuroendocrine Tumours (NETs) Your support guide This book will help you better understand NETs. It is however a reference only; you should always go to your doctor or
Molecular Imaging Guided Therapy: The Perfect Storm. David M Schuster, MD Emory University Department of Radiology Atlanta, GA
 Molecular Imaging Guided Therapy: The Perfect Storm David M Schuster, MD Emory University Department of Radiology Atlanta, GA Talk can be found at radiology.emory.edu Let s start with a case 74 year
Molecular Imaging Guided Therapy: The Perfect Storm David M Schuster, MD Emory University Department of Radiology Atlanta, GA Talk can be found at radiology.emory.edu Let s start with a case 74 year
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
SMALL BOWEL ADENOCARCINOMA. Dr. C. Jeske
 SMALL BOWEL ADENOCARCINOMA Dr. C. Jeske Case presentation 54 year old female. Presents with OJ and weight loss. Abdominal examination only reveals a palpable gallbladder. ERCP reveals a circumferential
SMALL BOWEL ADENOCARCINOMA Dr. C. Jeske Case presentation 54 year old female. Presents with OJ and weight loss. Abdominal examination only reveals a palpable gallbladder. ERCP reveals a circumferential
Specialised Services Policy CP66: 68-gallium DOTA- peptide scanning for the Management of Neuroendocrine Tumours (NETs)
") Specialised Services Policy CP66: Management of Neuroendocrine Tumours (NETs) Document Author: Assistant Planner for Cancer and Blood Executive Lead: Director of Quality and Nursing Approved by: Management
Specialised Services Policy CP66: Management of Neuroendocrine Tumours (NETs) Document Author: Assistant Planner for Cancer and Blood Executive Lead: Director of Quality and Nursing Approved by: Management
Disclosure of Relevant Financial Relationships
 Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Disclosure of Relevant Financial Relationships USCAP requires that all faculty in a position to influence or control the content of CME disclose any relevant financial relationship WITH COMMERCIAL INTERESTS
Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide)
") GEP-NET Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide) 1 Histogenesis 16 different
GEP-NET Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas Oberndofer 1907 Illeal Serotonin Secreting Tumor Carcinoid (Karzinoide) 1 Histogenesis 16 different
Section Activity Activity Description Details Reference(s)
") Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with Renal Cell Carcinoma AA Cancer Centre Referrals Not routine pre-op referral indicated
Intended for use by Clinicians and Health Care Providers involved in the Management or Referral of adult patients with Renal Cell Carcinoma AA Cancer Centre Referrals Not routine pre-op referral indicated
CRITICAL ANALYSIS OF NEN GUIDELINES. G Pentheroudakis Associate Professsor of Oncology Medical School, University of Ioannina Chair, ESMO Guidelines
 CRITICAL ANALYSIS OF NEN GUIDELINES G Pentheroudakis Associate Professsor of Oncology Medical School, University of Ioannina Chair, ESMO Guidelines DISCLOSURES NO CONFLICTS OF INTEREST TO DECLARE UPDATED
CRITICAL ANALYSIS OF NEN GUIDELINES G Pentheroudakis Associate Professsor of Oncology Medical School, University of Ioannina Chair, ESMO Guidelines DISCLOSURES NO CONFLICTS OF INTEREST TO DECLARE UPDATED
Interventional therapy for rectal neuroendocrine tumor with liver metastases: report of one case
 Case Report Interventional therapy for rectal neuroendocrine tumor with liver metastases: report of one case Lingxiao Liu 1 *, Xu Han 2 *, Wenhui Lou 2 1 Department of Interventional Radiology, 2 Department
Case Report Interventional therapy for rectal neuroendocrine tumor with liver metastases: report of one case Lingxiao Liu 1 *, Xu Han 2 *, Wenhui Lou 2 1 Department of Interventional Radiology, 2 Department
Factors Affecting Survival in Neuroendocrine Tumors: A 15-Year Single Center Experience
 RESEARCH ARTICLE Editorial Process: Submission:00/00/0000 Acceptance:00/00/0000 : A 15-Year Single Center Experience Abdullah Sakin 1 *, Makbule Tambas 2, Saban Secmeler 3, Orçun Can 3, Serdar Arici 3,
RESEARCH ARTICLE Editorial Process: Submission:00/00/0000 Acceptance:00/00/0000 : A 15-Year Single Center Experience Abdullah Sakin 1 *, Makbule Tambas 2, Saban Secmeler 3, Orçun Can 3, Serdar Arici 3,
Afternoon Session Cases
 Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
Afternoon Session Cases Case 1 19 year old woman Presented with abdominal pain to community hospital Mild incr WBC a14, 000, Hg normal, lipase 100 (normal to 75) US 5.2 x 3.7 x 4 cm mass in porta hepatis
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID
 ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
ENDOLUMINAL APPROACH FOR THE MANAGEMENT OF GASTROINTESTINAL CARCINOID Manoop S. Bhutani, MD, FASGE, FACG, FACP, AGAF, Doctor Honoris Causa Professor of Medicine Eminent Scientist of the Year 2008, World
Evaluation and Management of Neuroendocrine Tumors
 Evaluation and Management of Neuroendocrine Tumors Jennifer Chan, MD, MPH Clinical Director, Program in Neuroendocrine and Carcinoid Tumors Dana-Farber/Brigham and Women's Cancer Center October 14, 2017
Evaluation and Management of Neuroendocrine Tumors Jennifer Chan, MD, MPH Clinical Director, Program in Neuroendocrine and Carcinoid Tumors Dana-Farber/Brigham and Women's Cancer Center October 14, 2017
Surgery for NET Challenges and specific aspects
 Surgery for NET Challenges and specific aspects Raymond Aerts, MD Department of Abdominal Surgery and Liver Transplantation University Clinics Leuven ESMO Preceptorship on GI neuroendocrine tumours (NETs)
Surgery for NET Challenges and specific aspects Raymond Aerts, MD Department of Abdominal Surgery and Liver Transplantation University Clinics Leuven ESMO Preceptorship on GI neuroendocrine tumours (NETs)
Ruolo della interventistica per le secondarietà epatiche e di altre sedi
 Ruolo della interventistica per le secondarietà epatiche e di altre sedi Giancarlo Bizzarri Dipartimento di Diagnostica per Immagini e Radiologia Interventistica Ospedale Regina Apostolorum, Albano Laziale
Ruolo della interventistica per le secondarietà epatiche e di altre sedi Giancarlo Bizzarri Dipartimento di Diagnostica per Immagini e Radiologia Interventistica Ospedale Regina Apostolorum, Albano Laziale
Carcinoid Tumors: The Beginning and End. Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011
 Carcinoid Tumors: The Beginning and End Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011 1 st described by Oberndofer(1907) Karzinoide = cancer like Arise from
Carcinoid Tumors: The Beginning and End Surgical Oncology Update 2011 Chris Baliski MD, FRCS BC Cancer Agency, CSI October 21, 2011 1 st described by Oberndofer(1907) Karzinoide = cancer like Arise from
Surgical Management of Neuroendocrine Tumors of the Gut. Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School
 Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
Surgical Management of Neuroendocrine Tumors of the Gut Richard Hodin MD Professor of Surgery Massachusetts General Hospital Harvard Medical School Sites of GI Carcinoid Tumors Small intestine 44% Rectum
Treatment for early pancreatic cancer
 13 11 20 Information and support Treatment for pancreatic cancer Contents Treatment for early pancreatic cancer Surgery What to expect after surgery Neoadjuvant and adjuvant therapies Treatment for advanced
13 11 20 Information and support Treatment for pancreatic cancer Contents Treatment for early pancreatic cancer Surgery What to expect after surgery Neoadjuvant and adjuvant therapies Treatment for advanced
HEPATIC METASTASES. We can state 3 types of metastases depending on their treatment options:
 HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
HEPATIC METASTASES 1. Definition Metastasis means the spread of cancer. Cancerous cells can separate from the primary tumor and enter the bloodstream or the lymphatic system (the one that produces, stores,
Gallbladder Cancer. GI Practice Guideline. Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist)
 Barbara Fisher, MD, FRCPC (Radiation Oncologist)") Gallbladder Cancer GI Practice Guideline Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist) Approval Date: September 2006 This guideline is a statement of
Gallbladder Cancer GI Practice Guideline Michael Sanatani, MD, FRCPC (Medical Oncologist) Barbara Fisher, MD, FRCPC (Radiation Oncologist) Approval Date: September 2006 This guideline is a statement of
A case of persistent diarrhoea. Dr. Miles Levy, Dr. Jenny Prouten, Priya Jalota
 A case of persistent diarrhoea Dr. Miles Levy, Dr. Jenny Prouten, Priya Jalota Presentation 58 year old male with 3/12 history of persistent change in bowel habit following trip to India in January 2012
A case of persistent diarrhoea Dr. Miles Levy, Dr. Jenny Prouten, Priya Jalota Presentation 58 year old male with 3/12 history of persistent change in bowel habit following trip to India in January 2012
Liver Cancer (Hepatocellular Carcinoma or HCC) Overview
 Overview") Liver Cancer (Hepatocellular Carcinoma or HCC) Overview Recent advances in liver cancer care seek to address the rising incidence of liver cancer, which has steadily increased over the past three decades.
Liver Cancer (Hepatocellular Carcinoma or HCC) Overview Recent advances in liver cancer care seek to address the rising incidence of liver cancer, which has steadily increased over the past three decades.
Surveillance following treatment of primary ocular melanoma
 Surveillance following treatment of primary ocular melanoma Introduction 50% of UM patients relapse with predominantly liver metastases Risk of metastatic disease can be predicted relatively accurately
Surveillance following treatment of primary ocular melanoma Introduction 50% of UM patients relapse with predominantly liver metastases Risk of metastatic disease can be predicted relatively accurately
Patient Experience Survey
 Patient Experience Survey NET Patient Foundation Patient Experience Survey Objective: To understand the challenges faced by NET patients in reaching an appropriate diagnosis and then accessing the care
Patient Experience Survey NET Patient Foundation Patient Experience Survey Objective: To understand the challenges faced by NET patients in reaching an appropriate diagnosis and then accessing the care
Sometimes it takes a couple of years to find the right diagnoses. Norway, Medha Sharma and Asha Sundaran
 Sometimes it takes a couple of years to find the right diagnoses Norway, Medha Sharma and Asha Sundaran Male 54 years old. Personal history : healthy man with normal BMI. Very active. previous prolaps
Sometimes it takes a couple of years to find the right diagnoses Norway, Medha Sharma and Asha Sundaran Male 54 years old. Personal history : healthy man with normal BMI. Very active. previous prolaps