Original article. Improved survival of cancer patients admitted to the ICU between 2002 and 2011 at a U.S. teaching hospital
|
|
|
- Martin Morgan
- 5 years ago
- Views:
Transcription
1 Original article Improved survival of cancer patients admitted to the ICU between 2002 and 2011 at a U.S. teaching hospital C.M. Sauer 1,2*, J. Dong 3, L.A. Celi 2, D. Ramazzotti 4 1 Department of Epidemiology, Harvard T.H. Chan School of Public Health, Boston, MA, United States 2 Institute for Medical Engineering and Science, Massachusetts Institute of Technology, Cambridge, MA, United States 3 Institute for Clinical Research and Health Policy Studies, Tufts Medical Center, Boston, MA, United States 4 Department of Pathology, Stanford University, Stanford, CA, United States *Corresponding author: Dr. Leo A. Celi Institute for Medical Engineering and Science Massachusetts Institute of Technology Deacon St, Cambridge, MA Tel: lceli@bidmc.harvard.edu 1
2 Abstract Background: Over the past decades, both critical care and cancer care have improved substantially. Due to increased cancer-specific survival [1], we hypothesized that both the number of cancer patients admitted to the ICU and overall survival have increased since the millennium change. Patients and methods: MIMIC-III, a freely accessible critical care database of Beth Israel Deaconess Medical Center, Boston, USA [2] was used to retrospectively study trends and outcomes of cancer patients admitted to the ICU between 2002 and Multiple logistic regression analysis was performed to adjust for confounders of 28-day and 1-year mortality. Results: Out of 41,468 unique ICU admissions, 1,100 hemato-oncologic, 3,953 oncologic and 49 patients with both a hematological and solid malignancy were analyzed. Hematological patients had higher critical illness scores than non-cancer patients, while oncologic patients had similar APACHE-III and SOFA-scores compared to non-cancer patients. In the univariate analysis, cancer was strongly associated with mortality (OR= 2.74, 95%CI: 2.56, 2.94). Over the 10-year study period, 28-day mortality of cancer patients decreased by 30%. This trend persisted after adjustment for covariates, with cancer patients having significantly higher mortality (OR=2.63, 95%CI: 2.38, 2.88). Between 2002 and 2011, both the adjusted odds of 28- day mortality and the adjusted odds of 1-year mortality for cancer patients decreased by 6% (95%CI: 4%, 9%). Having cancer was the strongest single predictor of 1-year mortality in the multivariate model (OR=4.47, 95%CI: 4.11, 4.84). Conclusion: Between 2002 and 2011, the number of cancer patients admitted to the ICU increased steadily and significantly, while longitudinal clinical severity scores remained overall unchanged. Although hematological and oncological patients had higher mortality rates than patients without cancer, both 28-day and 1-year mortality decreased significantly and faster than those of non-cancer patients over the 10-year study period. 2
3 Keywords: Intensive care, cancer, trends, survival, ICU 3
4 Key message: Admission of cancer patients doubled between Cancer patients had higher 28-day mortality rates than non-cancer patients (28.6% vs. 12.8%). While 28-day mortality rates of cancer patients decreased by 31%, clinical severity scores remained unchanged. After adjusting for confounders, there was an annual 6% decrease in the odds of dying at both 28-days and 1-year among cancer patients. 4
5 Background Cancer is a global public health concern and the second leading cause of death in the United States and most developed countries [3]. Despite a slight decrease in cancer incidence over the last two decades, cancer prevalence continues to increase due to improved treatment and earlier diagnosis [4]. Historically, advanced or end-stage oncological and hematological patients were, due to their limited prognosis, frequently not referred to intensive care units. Novel and more efficient antineoplastic treatments have resulted in prolonged progression-free and overall survival of oncological and hemato-oncological patients [3]. Consequently, a growing number of cancer patients is at risk of admission to intensive care units [1]. Concurrently, the average prognosis of oncological patients remains less than that of the general population, thereby frequently resulting in controversy whether an ICU admission is an appropriate medical choice [1]. While several studies have described the characteristics of oncological patients admitted to ICU, only two studies have investigated trends in hematological and oncological ICU admissions in the UK [5] and hematological patients in the Netherlands [6]. In both settings, the absolute number of oncologic patients admitted to intensive care units has increased. In the Netherlands, the odds of admission increased by an annualized 6% between 2004 and 2012, while the proportion of oncological patients admitted to British ICUs remained almost unchanged between 1997 and Of note, the Acute Physiology and Chronic Health Evaluation (APACHE-II) score for hematological patients at admission were the same in the Dutch and British cohorts (24 points). At the same time, both hospital (47% vs. 54%) and ICU mortality (34% vs. 41%) were approximately 7 percentage-points lower in the Dutch ICU cohort compared to the UK cohort, possibly indicating differences in referral pattern, aggressiveness of treatment or other patient characteristics. In both cohorts, hospital and ICU mortality for 5
6 hematological patients decreased, while mortality rates of oncological patients did not change. Regardless, the average prognosis of oncological patients remains less than that of the general population. For instance, hematological patients in the Netherlands had twice as high ICU mortality rates than patients without malignancy (34% vs. 17%). While prior studies have described oncological patient characteristics and outcomes in the U.S. [7], no published longitudinal analysis for trends in ICU mortality for the US is available. In the following, we therefore aim to describe trends in admission numbers and patient characteristics for cancer patients admitted to the ICU. Furthermore, we aim to establish if 28-day and 1-year mortality changed over the 10-year period, after adjusting for covariates. 6
7 Methods Patient information was extracted from a de-identified version of the MIMIC-III (v1.4) database using PostgreSQL (The PostgreSQL Global Development Group, MIMIC-III is an open-access ICU database jointly administered by the Massachusetts Institute of Technology and the Beth Israel Deaconess Medical Center [2]. The database comprises over 58,000 hospital admissions for 38,645 adults and 7,875 neonates, spanning from June October Year of admission is not available in this limited, de-identified dataset due to privacy concerns. Therefore, we obtained a supplementary dataset from the administrators. Previously established code from the MIMIC Code Repository was used to generate comorbidity scores and risk scores [8]. A waiver of consent that has previously been obtained from the Institutional Review Boards of BIDMC and MIT is applicable to these datasets. Cohort Selection All adult patients aged 18 years or older with a diagnosis of any cancer type as identified by ICD-9 codes (solid malignancies) and (neuroendocrine carcinomas) or (hematological malignancy) were included in this study. Patients with incomplete data on admission year, length of stay or severity of illness were excluded during data analysis. Since no complete annual data for 2001 and 2012 was available, all patients admitted in this period were excluded from the base population. If patients were admitted multiple times to the ICU, only their first admission was used for this analysis. Covariates Patient data on the following variables were extracted from the database: 7
8 Age at admission, gender, race, Elixhauser Comorbidity Index scores [9], vasopressor duration, ventilation duration, OASIS scores [10], SOFA scores [11], APACHE-III scores [12], renal replacement therapy, do not resuscitate order (DNR) at admission, ICU mortality, mortality (from the Social Security death records). SOFA scores were interpreted as being low (0-5), medium (6-10) and high risk ( 11 points), respectively. Duration of ventilation and duration of vasopressor use were converted from continuous to binary variables. Race was categorized into a white and non-white category. Cancer diagnoses were clustered according to ICD-9 codes into: Oral malignancies ( ), gastrointestinal ( ), respiratory and thoracic ( ), Connective tissue malignancy and others ( , ), genitourinary ( ), other solid malignancies ( , ), lymphoma ( , ), leukemia ( ), other hematologicalmalignancies ( , , ) and metastatic cancer ( , ). Outcomes The primary study outcomes were (a) trends in the number and relative frequency of oncological patients admitted to the ICU and (b) all-cause mortality within 28 days and 1 year after ICU admission. Secondary outcomes were (a) hospital and ICU length of stay, (b) changes in clinical severity scores and (c) predictors of mortality. Statistical Analysis All analyses were performed using the open-access software R (version 3.4.2, and the following packages: tableone, ggplot2, dplyr, MIMICbook, epitools, sjplot, MASS. For table 1, chi-square testing was performed for categorical variables (with continuity correction) and one-way ANOVA for parametric continuous variables. Multiple logistic regression was used to adjust for covariate levels in the longitudinal trend analysis for 28-day 8
9 and 1-year mortality (categorical outcome). Model building was based on expert opinion including the most important confounders (C.M.S.& L.A.C.). An alpha-level of 0.05 was used as the cutoff value to reject the null hypotheses. Collinearity analyses were performed, hence only APACHE-III scores were included in the final model. We checked the final model for interaction terms, however did not find any interaction terms that were statistically significant after Bonferroni adjustment. Reproducibility Both the code for the SQL queries and data analysis will be made freely publicly available after acceptance of this article for publication. Due to privacy concerns, the re-identified data on year of admission will not be made publicly available. 9
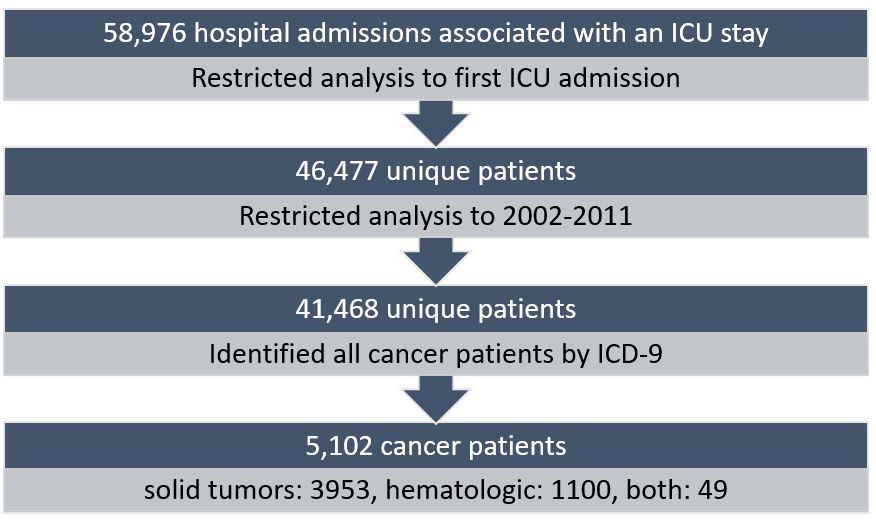
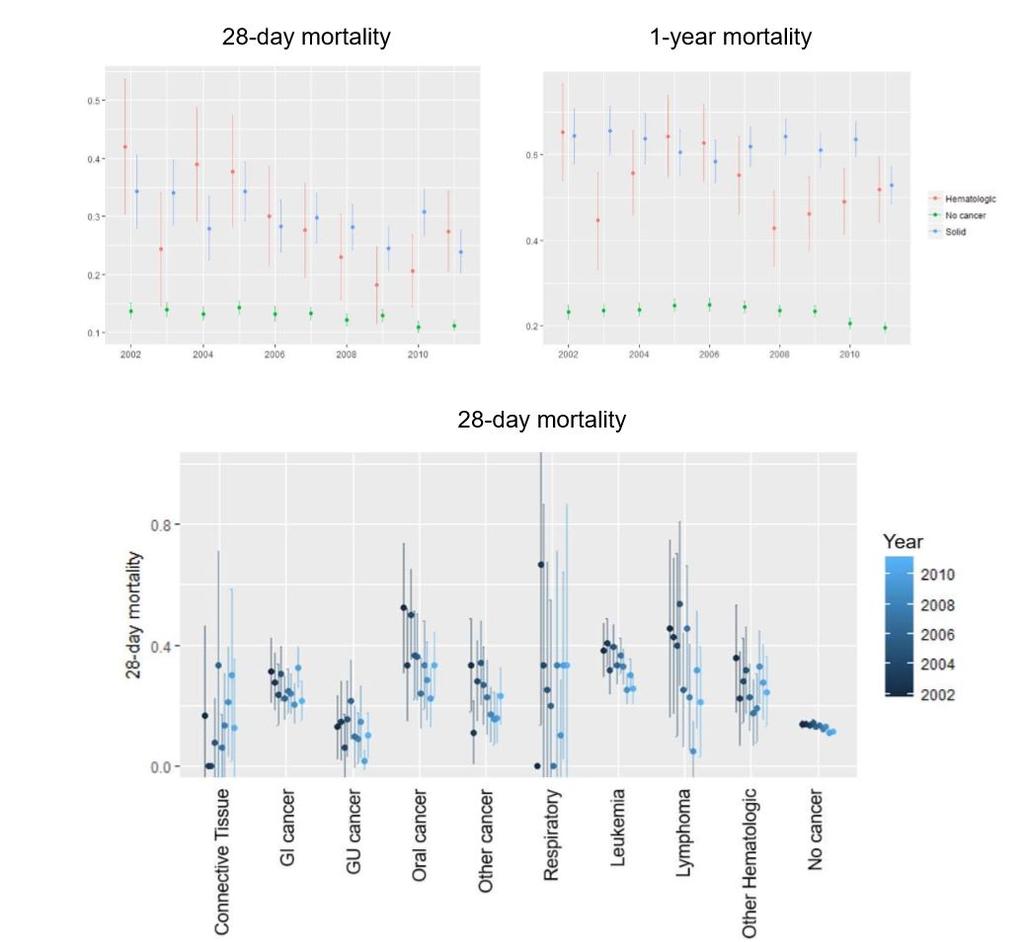
10 Results By restricting our analysis to the first ICU stay for each patient, a total unique patient cohort of 41,468 ICU admissions was obtained. Of these, 3953 had an oncologic malignancy, 1100 had a hematological malignancy and 49 patients had a diagnosis of both a hematological and solid malignancy (fig. 1). Baseline patient characteristics differed considerably between all subgroups (table 1). Hematological patients had highest mean clinical severity scores and a higher rate of DNR orders on admission (p<0.001), however were less likely to be ventilated or to receive vasopressors (p<0.001). Furthermore, mean length of ICU and hospital stay for hematological patients was significantly longer than that of non-cancer patients (p<0.001). Oncological patients had patient characteristics that were more similar to those of non-cancer patient, having comparable clinical severity scores and only slightly longer length of ICU and hospital stays. Of note, oncological patients less frequently received vasopressin and ventilation. Between 2002 and 2011, the overall number of patients admitted to the ICU increased from 3110 to Over the same period, the number of patients with cancer more than double from 285 to 678 (Suppl. table 1) and 28-day mortality of cancer patients decreased from 36.1% in 2002 to 24.8% in 2002 (p<0.001). Concurrently, use of vasopressors (p=0.002) and ventilation (p<0.001) decreased significantly, while clinical severity scores did not change significantly, and comorbidity scores increased from 16 to 20 (p<0.001). Between 2002 and 2011, both crude 28-day and 1-year mortality rates decreased (fig. 2). The highest mortality rates were measured in the oncology group, with 27.7% and 52.6% at 28 days and 1 year, respectively. Over the study period, the highest relative decrease in the odds of death at 28 days was recorded in the hematological group (-55%), followed by the oncologic (- 40%) and non-cancer patients (-20%). There was considerable variation in 28-day mortality rates depending on cancer subtype, with other oncological cancers (including neuroendocrine 10
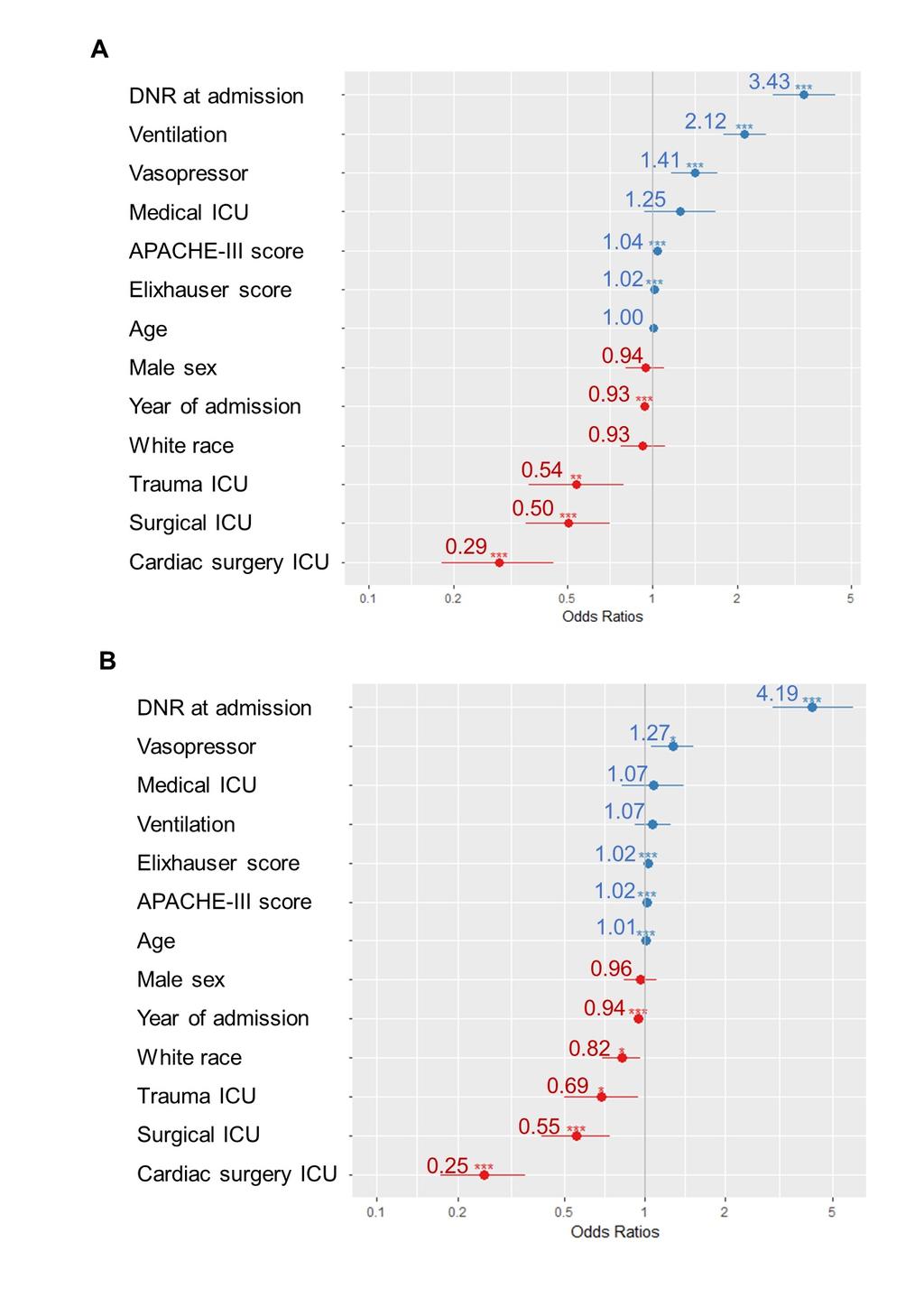
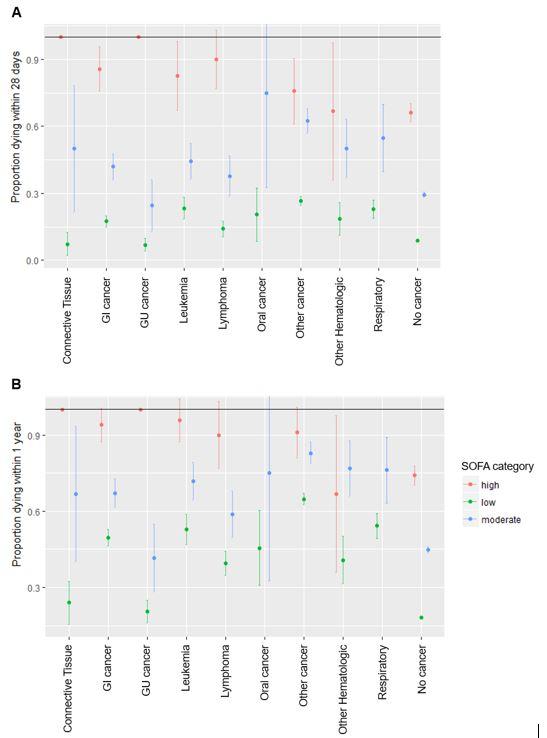
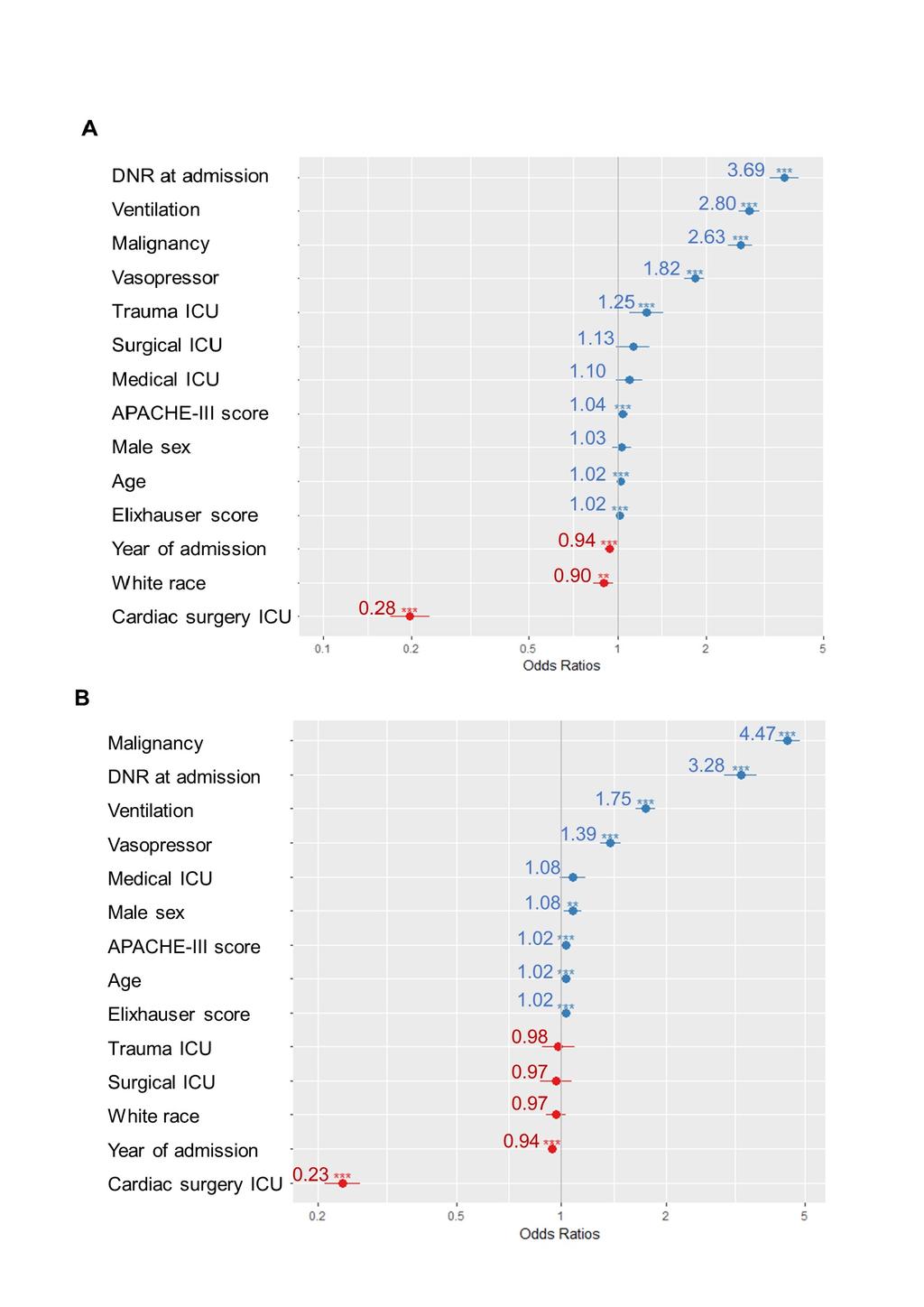
11 carcinomas) and cancer of the lip, oral cavity and pharynx having the highest mortality rate. Genitourinary and connective tissue (including breast) cancers had the lowest mortality rates of all malignancies. Mortality rates were closely associated with clinical severity scores across all cancer subtypes. Of note, patients with high SOFA-scores ( 11) and a connective tissue malignancy (including breast cancer, N=2) or genitourinary cancer (N=7) had a 100% probability of dying at 28-days. Similarly, patients with gastrointestinal cancer (N=49) or leukemia (N=23) and high SOFA-scores ( 11) had a close to 100% probability of dying within 1-year of ICU admission (Supp. Fig. 1). Multivariate logistic regression analysis confirmed the observed trends in mortality. For the whole ICU cohort, a do-not-resuscitate order at admission, any type of cancer and year of admission were the strongest predictors of both 28-day and 1-year mortality rates after adjustment for covariates (suppl. fig. 2). A DNR order was associated with a 3.69-times higher odds (95%CI: 3.30, 4.13) of death within 28 days of admission, and a malignancy with a 2.62 (95%CI: 2.38, 2.88) times higher odds of death. Notable differences between the intensive care units exists, with the cardiac surgery recovery unit being associated with the lowest odds of dying (0.2, 95%CI: 0.17, 0.23), while admission to a trauma surgical unit was associated with a 1.25 (95%CI: 1.10, 1.43) higher odds of death. Having any malignancy was the strongest single predictor of 1-year mortality after adjustment for covariates with an odds ratio of death of 4.47 (95%CI: 4.12, 4.85). The observed protective association between admittance to the cardiac surgery recovery unit persisted (OR= 0.23, 95%CI: 0.21, 0.26). The odds of death decreased by an annualized 6% (95%CI: 5%, 7%) each year. (suppl. fig. 2) Among cancer patients, a DNR order is the single most important factor associated with both 28-day and 1-year survival after adjustment for covariates (fig. 3). For 28-day survival, being ventilated (OR=2.12, 95%CI: 1.78, 2.52) or receiving vasopressors (OR=1.41, 95%CI: 1.16, 1.70) is strongly associated with worse outcome. Noteworthily, this association is weaker for 1-11
12 year survival, with vasopressor use (OR=1.27, 95%CI: 1.06, 1.52) being weakly associated and ventilation (OR=1.07, 95%CI: 0.91, 1.24) not being statistically significantly associated. Both Apache-III score and Elixhauser comorbidity score are important predictors of survival. Patients in the lowest Apache-III score quartile (score=31) have a 2.0-times higher odds of dying than patients in the 3 rd Apache-III score quartile (score=55). Similarly, patients in the lowest Elixhauser score quartile (score=10) have a 1.7-times higher odds of dying than patients in the 3 rd Elixhauser score quartile (score=28). Of note, white race is weakly associated with higher survival at 1-year (OR=0.82, 95%CI: 0.70, 0.97), but not with 28-day (OR=0.93, 95%CI: 0.77, 1.11). For both 28-day and 1-year survival, admission to a surgical, trauma surgical or cardiac surgery ICU is associated with a significantly decreased odds of death compared to admission to a medical ICU. Over the 10-year study period, both 28-day and 1-year mortality decreased at an annualized rate of 6%. Between 2002 and 2011, the odds of dying decreased by 49.2% (28-day mortality, 95%CI: 31%, 62%) and 44.7% (1-year mortality, 95%CI: 28%, 59%). Discussion This is one of the largest studies investigating trends in patient characteristics and outcomes of oncological patients admitted to the ICU worldwide, and the first study from the U.S. More than 58,000 ICU admissions were analyzed and 41,468 patients were included in the final analysis, among which were 1100 hematological and 3953 oncological patients. Cancer patients had comparable clinical severity scores compared to non-cancer patients, yet were more likely to die within 28 days (RR=2.23) and within 1 year (RR=2.58). Mortality rates decreased significantly over the study period (-7% annual decrease) for all patients, with cancer patients having a bigger decrease in mortality rates than non-cancer patients. 12
13 Our findings confirm the previously reported decrease in mortality rates observed in the UK [5] and the Netherlands [13] since the millennium change. Interestingly, we observed unchanged clinical severity scores over time, while mortality rates decreased substantially between 2002 and While 28-day survival of oncological patients (71.1%) was comparable with 30-day survival in the Dutch cohort (73.1%), survival of hematological patients (72.3%) differed considerably from the Netherlands (55%). As expected, clinical severity scores were strong predictors of survival, as were the presence of any malignancy, a DNR order at admission, type of ICU, use of vasopressors or mechanical ventilation and comorbidities, thereby confirming earlier studies [5, 7, 14-18]. Of note, crude 1- year mortality rates for patients with high SOFA scores and gastrointestinal, genitourinary, connective tissue cancer, leukemia, lymphoma or other solid cancers were exceeding 90%. Mortality rates differed considerably between the ICU types and are possibly explained by different reasons for admission and long-term prognosis. The notable protective effect observed for cardiac surgical patients could be explained by selection bias, since primarily patients with a favorable oncologic diagnosis might undergoing surgery. In contrast, medical ICU patients might more likely be admitted due for reasons directly related with their underlying disease or treatment complications. Clinicians are frequently faced with the difficult decision whether patients with serious chronic conditions that limit their life expectancy should be admitted to the intensive care unit. This is particularly challenging for oncological patients, where long-term survival might more depend on their underlying malignancy than their acute health problem. Our findings together with previously published results [14, 16, 19, 20] suggests that elderly patients with high clinical severity scores, multiple comorbidities and certain cancer types do not sustain long-term survival regardless of intensive treatment. Concurrently, the presence of any malignancy alone 13
14 is an insufficient predictor of both 28-day and 1-year mortality and treatment decisions should not be based on oncological prognosis alone. Analysis of over 40,000 admitted patients, including more than 5,000 (hemato-)oncological patients allowed for precise and stratified analysis of patient characteristics, outcomes and predictive factors. Data was retrieved from clinical databases that were compiled at the time of treatment, thereby minimizing bias that may occur due to the retrospective study design. The high resolution of the clinical data is another advantage of this study. Furthermore, we had sufficient statistical power to detect annual changes in mortality of cancer patients. Major limitations of this study are a lack of important oncological predictive factors, including TNM classification, tumor size, histopathological features and clinical aggressiveness. Furthermore, no data was available on critically ill patients who were not admitted to the ICU and abstained. Preferably, additional information on oncological treatment, treatment type and time since administration of chemotherapy should be included in the analysis. In addition, data on rare cancers (including oral cancer and respiratory cancers) was sparse, thus not allowing for a more detailed subgroup analysis. Another disadvantage is that data was obtained from a single-center teaching hospital and generalizability of findings might therefore be limited. Future analyses should preferably include larger cohorts from different hospitals across the United States and contain more oncologic outcomes measures. Regardless of these shortcomings, the unchanged clinical severity scores over time and results of the multivariate logistic regression suggest that survival of oncologic patients has increased between and is not due to confounding by other variables or selection bias. It is tempting to speculate that the absolute and relative increase in cancer patients admitted to the ICU could be interpreted as a consequence of better oncological survival, rendering more patients at risk of ICU admission. The alternative, namely that the observed increase in oncological patient admissions is due to a more lenient ICU admission policy, is not supported 14
15 by unchanged clinical severity scores, increased comorbidity scores and another study showing a decrease in ICU utilization among cancer patients between [7]. Interestingly, 28- day mortality for both cancer and non-cancer patients decreased approx. equally on the multiplicative scale (-6% annually). At the same time, the absolute improvement in survival is larger for cancer patients, due to an approx. three times higher mortality rate at baseline. In this descriptive study, which should not be interpreted as a prognostic survival model, we recorded a steady and significant increase in the number and proportion of cancer patients admitted to the ICU, unchanged clinical severity scores, increased comorbidity score and a major decrease in mortality rates between 2002 and In our multivariate model for the whole ICU cohort, the presence of any malignancy was the single strongest predictor of 1-year survival of all ICU patients. Acknowledgements This manuscript has been produced as part of course HST.953 at the Massachusetts Institute of Technology, Cambridge, MA, USA. The authors gratefully acknowledge the support and feedback provided by T. Pollack, A. Johnson and J. Raffa. Funding The MIMIC database is funded by the National Institute of Health through the National Institute of Biomedical Imaging and Bioengineering [grant number R01 EB A1]. Disclosure 15
16 The authors have declared no conflicts of interest. Legend to the figures Figure 1: Overview of the cohort building process. Restriction to the years for which complete follow-up data is available decreased the cohort by 5,009 individuals. A total of 5,102 patients with cancer were identified, of which 3,953 had an ICD-9 code of a solid tumor, 1,100 of a hematological malignancy and 49 both a hematological and solid malignancy. Figure 2: Changes in 28-day mortality for (A) solid malignancies and (B) hematological malignancies over the 10-year period. There are notable differences in mortality between the subgroups, with cancers of the oral cavity/lip/pharynx and other primary origin having the highest mortality rates. Genitourinary (GU) and breast/connective tissue had the lowest mortality rates. GI: gastrointestinal cancer, Oral: cancer of the oral cavity/ lip/ pharynx Figure 3: Results of the multivariate regression model for (A) 28-day and (B) 1-year mortality among cancer patients. (A) DNR at admission (OR=3.4) was the strongest single predictor of 28-day mortality after adjusting for covariates. Any use of vasopressors or mechanical ventialtion was associated with worse 28-day outcomes. Year of admission was a strong predictive factor, with the odds of dying within 28-days decreasing by 7% every year. Elixhauser and Apache-III scores were singificantly associated with both 28-day and 1 year mortality, e.g. a 1 point increase in APACHE-III increasing the odds of dying within 28 days by 4%. Admission to a ICU other than the medical was associated with increased survival. (B) Notable differences between 28-day and 1-year survival are the weaker association between both vasopressor use and ventialtion with survival and a signficant assoication between white race and survival. 16
17 Legend to the tables Table 1: Overview of patient characteristics and outcomes. Patients with cancer had higher comorbidity scores, similar clinical severity scores, on average received less invasive treatment and had higher 28-day and 1-year mortality. All differences between the subgroups where overall statistically significant with p-values< DNR=Do not resuscitate, SOFA: Sepsis related organ failure assessment, OASIS: Oxford acute severity of illness score, APACHE-III: Acute physiology and chronic health evaluation score. If not indicated differently, values refer to the mean (Standard Deviation). 17
18 References 1. Jemal A, Ward EM, Johnson CJ et al. Annual Report to the Nation on the Status of Cancer, , Featuring Survival. J Natl Cancer Inst 2017; Johnson AEW, Pollard TJ, Shen L et al. MIMIC-III, a freely accessible critical care database. Scientific Data 2016; 3: Siegel RL, Miller KD, Jemal A. Cancer Statistics, CA Cancer J Clin 2017; 67: Miller KD, Siegel RL, Lin CC et al. Cancer treatment and survivorship statistics, CA Cancer J Clin 2016; 66: Ostermann M, Ferrando-Vivas P, Gore C et al. Characteristics and Outcome of Cancer Patients Admitted to the ICU in England, Wales, and Northern Ireland and National Trends Between 1997 and Crit Care Med 2017; 45: van Vliet M, Verburg IW, van den Boogaard M et al. Trends in admission prevalence, illness severity and survival of haematological patients treated in Dutch intensive care units. Intensive Care Med 2014; 40: Wallace SK, Rathi NK, Waller DK et al. Two Decades of ICU Utilization and Hospital Outcomes in a Comprehensive Cancer Center. Crit Care Med 2016; 44: Johnson AE, Stone DJ, Celi LA, Pollard TJ. The MIMIC Code Repository: enabling reproducibility in critical care research. J Am Med Inform Assoc 2018; 25: Moore BJ, White S, Washington R et al. Identifying Increased Risk of Readmission and In-hospital Mortality Using Hospital Administrative Data: The AHRQ Elixhauser Comorbidity Index. Med Care 2017; 55: Johnson AE, Kramer AA, Clifford GD. A new severity of illness scale using a subset of Acute Physiology And Chronic Health Evaluation data elements shows comparable predictive accuracy. Crit Care Med 2013; 41: Vincent JL, Moreno R, Takala J. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med 1996; Knaus WA, Wagner DP, Draper EA et al. The APACHE III prognostic system. Risk prediction of hospital mortality for critically ill hospitalized adults. Chest 1991; 100: Bos MM, Verburg IW, Dumaij I et al. Intensive care admission of cancer patients: a comparative analysis. Cancer Med 2015; 4: Rosolem MM, Rabello LS, Lisboa T et al. Critically ill patients with cancer and sepsis: clinical course and prognostic factors. J Crit Care 2012; 27: Azevedo LCP, Caruso P, Silva UVA et al. Outcomes for patients with cancer admitted to the ICU requiring ventilatory support: results from a prospective multicenter study. Chest 2014; 146: Soares M, Caruso P, Silva E et al. Characteristics and outcomes of patients with cancer requiring admission to intensive care units: a prospective multicenter study. Crit Care Med 2010; 38: Neuschwander A, Lemiale V, Darmon M et al. Noninvasive ventilation during acute respiratory distress syndrome in patients with cancer: Trends in use and outcome. Journal of Critical Care 2017; 38: Wigmore T, Farquhar-Smith P. Outcomes for Critically Ill Cancer Patients in the ICU: Current Trends and Prediction. Int Anesthesiol Clin 2016; 54: e Soares M, Salluh JI, Toscano L. Outcomes and prognostic factors in patients with head and neck cancer and severe acute illnesses. Intensive Care Med 2007; Demandt AMP, Geerse DA, Janssen BJP et al. The prognostic value of a trend in modified SOFA score for patients with hematological malignancies in the intensive care unit. Eur J Haematol 2017; 99:
19 Supplementary material Supplementary table 1: trends in cancer patient admission, characteristics and outcomes by year of admission. The number of oncological cases admitted to the ICU increased by 238% over the 10-year period. Clinical severity scores remained approximately unchanged, while use of vasopressors and ventilation decreased significantly. The mean Elixhauser comorbidity score increase steadily over the study period. Both 28-day and 1-year mortality decreased over time, with the 28-day mortality (-31%) decreasing faster than 1-year mortality (- 18%). Supplementary figure 1: (A) 28-days and (B) 1-year mortality rates by cancer type and SOFA-scores. SOFA scores were strongly associated with mortality across all cancer subtypes. Overall, cancer patients had worse outcomes compared to non-cancer patients with similar SOFA scores. Patients with high SOFA-scores ( 11) and a connective tissue malignancy (including breast cancer, N=2) and genitourinary cancer (N=7) had a 100% probability of dying at 28-days. Similarly, patients with gastrointestinal cancer (N=49) and leukemia (N=23) and high SOFA-scores ( 11) had a close to 100% probability of dying at 1-year. Supplementary figure 2: Results of the multivariate model for (A) 28-day and (B) 1-year mortality for the whole cohort. (A) After adjusting for other covariates, DNR at admission (OR=3.69) was the strongest predictor of 28-day mortality, followed by any use of mechanical ventilation and presence of any malignancy. Year of admission was a strong protective factor, with mortality rates decreaseing by 6% every year. With each year increase in age at admission, the odds of dying within 28 days and 1 year increased by 2%. A one point increase in APACHE- III scores was closer asscoiated with a higher increase in the odds of dying within 28 days (4%) than 1 year (2%). 19
20 Variables Without cancer Hematologic Malignancy Solid malignancy Hematologic and solid cancer Number of cases 36,366 1,100 3, Age at admission, years 63.8 (17.8) 65.3 (16.4) 65.8 (13. 6) 69.9 (12.7) DNR at admission (%) 1819 (6.0) 72 (8.2) 297 (9.5) 3 (7.7) White race (%) (71.7) 851 (77.4) 2979 (75.4) 39 (79.6) Length of stay ICU, days 4.59 (6.09) 5.38 (7.15) 4.19 (5.30) 4.00 (3.34) Length of stay Hospital, days 9.3 (8.7) 14.7 (15.2) 10.1 (8.3) 11.0 (10.0) Use of ventilation (%) (50.0) 470 (42.7) 1699 (43.0) 20 (40.8) Use of vasopressors (%) (34.2) 369 (33.5) 990 (25.0) 11 (22.4) Elixhauser score 8.8 (11.1) 17.6 (11.8) 19.4 (13.0) 23.9 (12.4) SOFA score 3.3 (2.5) 4.6 (3.0) 3.3 (2.7) 3.4 (2.9) APACHE-III score 42.0 (19.4) 50.4 (22.1) 44.5 (20.3) 46.7 (23.3) OASIS score 31.4 (9.0) 32.5 (9.0) 31.2 (9.5) 31.2 (9.9) 28-day Mortality (%) 4640 (12.8) 305 (27.7) 1143 (28.9) 13 (26.5) 1-year Mortality (%) 8378 (23.0) 579 (52.6) 2420 (61.2) 29 (59.2)
21
22
23
24 Variables p-value Number of Patients Age at admission, year (14.06) (14.92) (15.46) (13.92) (14.10) (13.85) (14.11) (13.94) (14.04) (14.12) White race (%) 169 (59.3) 247 (72.4) 252 (72.2) 323 (74.6) 385 (77.8) 433 (77.3) 495 (78.6) 526 (81.8) 528 (76.7) 511 (75.4) <0.001 Use of vasopressors (%) 89 (31.2) 106 (31.1) 115 (33.0) 130 (30.0) 138 (27.9) 145 (25.9) 165 (26.2) 154 (24.0) 177 (25.7) 151 (22.3) Use of ventilation (%) 133 (46.7) 171 (50.1) 164 (47.0) 224 (51.7) 218 (44.0) 233 (41.6) 243 (38.6) 280 (43.5) 288 (41.9) 235 (34.7) <0.001 Solid Malignancy (%) Hematologic Malignancy (%) 216 (75.8) 69 (24.2) 267 (78.3) 74 (21.7) 254 (72.8) 95 (27.2) 335 (77.4) 98 (22.6) 385 (77.8) 110 (22.2) 444 (79.3) 116 (20.7) 504 (80.0) 126 (20.0) 511 (79.5) 132 (20.5) 523 (76.0) 165 (24.0) 514 (75.8) 164 (24.2) Metastatic Cancer (%) 79 (27.7) 137 (40.2) 109 (31.2) 149 (34.4) 157 (31.7) 200 (35.7) 216 (34.3) 230 (35.8) 227 (33.0) 218 (32.2) Renal replacement therapy (%) 14 (4.9) 15 (4.4) 6 (1.7) 20 (4.6) 22 (4.4) 19 (3.4) 33 (5.2) 23 (3.6) 31 (4.5) 35 (5.2) Elixhauser Score (10.99) (11.69) (12.11) (12.75) (12.55) (12.74) (12.81) (12.88) (13.19) (13.71) <0.001 SOFA score 3.40 (2.95) 3.52 (2.71) 3.57 (2.79) 3.87 (2.93) 3.56 (2.81) 3.48 (2.81) 3.76 (2.87) 3.44 (2.48) 3.74 (2.80) 3.46 (2.77) APACHE-III score (23.77) (21.21) (20.45) (21.49) (21.87) (19.66) (22.80) (19.29) (21.19) (18.52) OASIS score (10.05) (9.82) (9.80) (9.42) (9.38) (8.94) (9.89) (9.12) (8.94) (9.37) ICU length of stay, days 5.34 (8.72) 5.32 (5.83) 5.40 (6.70) 4.97 (6.78) 4.89 (6.86) 4.03 (4.53) 4.20 (5.62) 3.97 (4.07) 4.30 (5.71) 3.67 (4.05) <0.001 Hospital length of stay, days (11.13) (10.48) (12.08) (9.58) (10.88) (9.80) (9.25) (12.04) (10.53) 9.91 (8.56) day Mortality 103 (36.1) 109 (32.0) 108 (30.9) 152 (35.1) 142 (28.7) 164 (29.3) 171 (27.1) 149 (23.2) 195 (28.3) 168 (24.8) < year Mortality 184 (64.6) 208 (61.0) 215 (61.6) 266 (61.4) 294 (59.4) 339 (60.5) 378 (60.0) 373 (58.0) 414 (60.2) 357 (52.7) 0.027
25
26
Supplementary Online Content
 Supplementary Online Content Gershengorn HB, Scales DC, Kramer A, Wunsch H. Association between overnight extubations and outcomes in the intensive care unit. JAMA Intern Med. Published online September
Supplementary Online Content Gershengorn HB, Scales DC, Kramer A, Wunsch H. Association between overnight extubations and outcomes in the intensive care unit. JAMA Intern Med. Published online September
The Artificial Intelligence Clinician learns optimal treatment strategies for sepsis in intensive care
 SUPPLEMENTARY INFORMATION Articles https://doi.org/10.1038/s41591-018-0213-5 In the format provided by the authors and unedited. The Artificial Intelligence Clinician learns optimal treatment strategies
SUPPLEMENTARY INFORMATION Articles https://doi.org/10.1038/s41591-018-0213-5 In the format provided by the authors and unedited. The Artificial Intelligence Clinician learns optimal treatment strategies
Outcome of critically ill patients with acute kidney injury using the akin criteria
 Outcome of critically ill patients with acute kidney injury using the akin criteria The MIT Faculty has made this article openly available. Please share how this access benefits you. Your story matters.
Outcome of critically ill patients with acute kidney injury using the akin criteria The MIT Faculty has made this article openly available. Please share how this access benefits you. Your story matters.
Risk factors and mortality of adults with lung cancer admitted to the intensive care unit
 Original Article Risk factors and mortality of adults with lung cancer admitted to the intensive care unit Chih-Cheng Lai 1#, Chung-Han Ho 2,3#, Chin-Ming Chen 4,5, Shyh-Ren Chiang 5,6, Chien-Ming Chao
Original Article Risk factors and mortality of adults with lung cancer admitted to the intensive care unit Chih-Cheng Lai 1#, Chung-Han Ho 2,3#, Chin-Ming Chen 4,5, Shyh-Ren Chiang 5,6, Chien-Ming Chao
Supplementary Online Content
 Supplementary Online Content Valley TS, Sjoding MW, Ryan AM, Iwashyna TJ, Cooke CR. Association of intensive care unit admission with mortality among older patients with pneumonia. JAMA. doi:10.1001/jama.2015.11068.
Supplementary Online Content Valley TS, Sjoding MW, Ryan AM, Iwashyna TJ, Cooke CR. Association of intensive care unit admission with mortality among older patients with pneumonia. JAMA. doi:10.1001/jama.2015.11068.
Empirical relationships among oliguria, creatinine, mortality, and renal replacement therapy in the critically ill
 Empirical relationships among oliguria, creatinine, mortality, and renal replacement therapy in the critically ill The MIT Faculty has made this article openly available. Please share how this access benefits
Empirical relationships among oliguria, creatinine, mortality, and renal replacement therapy in the critically ill The MIT Faculty has made this article openly available. Please share how this access benefits
Quality of End-of-Life Care in Patients with Hematologic Malignancies: A Retrospective Cohort Study
 Quality of End-of-Life Care in Patients with Hematologic Malignancies: A Retrospective Cohort Study David Hui, Neha Didwaniya, Marieberta Vidal, Seong Hoon Shin, Gary Chisholm, Joyce Roquemore, Eduardo
Quality of End-of-Life Care in Patients with Hematologic Malignancies: A Retrospective Cohort Study David Hui, Neha Didwaniya, Marieberta Vidal, Seong Hoon Shin, Gary Chisholm, Joyce Roquemore, Eduardo
Retrospective analysis of outcome of women with breast or gynaecological cancer in the intensive care unit
 RESEARCH Retrospective analysis of outcome of women with breast or gynaecological cancer in the intensive care unit Marlies Ostermann 1 Mario Raimundo 1,2 Anna Williams 1 Craig Whiteley 1 Richard Beale
RESEARCH Retrospective analysis of outcome of women with breast or gynaecological cancer in the intensive care unit Marlies Ostermann 1 Mario Raimundo 1,2 Anna Williams 1 Craig Whiteley 1 Richard Beale
Outcome of patients with hematologic malignancy admitted to the ICU
 Outcome of patients with hematologic malignancy admitted to the ICU Geeta Mehta MD, FRCPC Mount Sinai Hospital Toronto, Canada CCCF November 2, 2016 Disclosures Hematologic Malignancy Advances in diagnostics,
Outcome of patients with hematologic malignancy admitted to the ICU Geeta Mehta MD, FRCPC Mount Sinai Hospital Toronto, Canada CCCF November 2, 2016 Disclosures Hematologic Malignancy Advances in diagnostics,
Supplementary Online Content
 Supplementary Online Content Yunos NM, Bellomo R, Hegarty C, Story D, Ho L, Bailey M. Association between a chloride-liberal vs chloride-restrictive intravenous fluid administration strategy and kidney
Supplementary Online Content Yunos NM, Bellomo R, Hegarty C, Story D, Ho L, Bailey M. Association between a chloride-liberal vs chloride-restrictive intravenous fluid administration strategy and kidney
Impact of Screening Colonoscopy on Outcomes in Colon Cancer Surgery
 Impact of Screening Colonoscopy on Outcomes in Colon Cancer Surgery The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters. Citation
Impact of Screening Colonoscopy on Outcomes in Colon Cancer Surgery The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters. Citation
PEER REVIEW HISTORY ARTICLE DETAILS TITLE (PROVISIONAL)
") PEER REVIEW HISTORY BMJ Open publishes all reviews undertaken for accepted manuscripts. Reviewers are asked to complete a checklist review form (see an example) and are provided with free text boxes to
PEER REVIEW HISTORY BMJ Open publishes all reviews undertaken for accepted manuscripts. Reviewers are asked to complete a checklist review form (see an example) and are provided with free text boxes to
Supplementary Online Content
 Supplementary Online Content Toyoda N, Chikwe J, Itagaki S, Gelijns AC, Adams DH, Egorova N. Trends in infective endocarditis in California and New York State, 1998-2013. JAMA. doi:10.1001/jama.2017.4287
Supplementary Online Content Toyoda N, Chikwe J, Itagaki S, Gelijns AC, Adams DH, Egorova N. Trends in infective endocarditis in California and New York State, 1998-2013. JAMA. doi:10.1001/jama.2017.4287
Evaluation the Correlation between Ki67 and 5 Years Disease Free Survival of Breast Cancer Patients
 BIOSCIENCES BIOTECHNOLOGY RESEARCH ASIA, December 2015. Vol. 12(3), 2221-2225 Evaluation the Correlation between Ki67 and 5 Years Disease Free Survival of Breast Cancer Patients S.M. Hosseini¹, H. Shahbaziyan
BIOSCIENCES BIOTECHNOLOGY RESEARCH ASIA, December 2015. Vol. 12(3), 2221-2225 Evaluation the Correlation between Ki67 and 5 Years Disease Free Survival of Breast Cancer Patients S.M. Hosseini¹, H. Shahbaziyan
The Influence of Race and Ethnicity on End-of-Life Care in the Intensive Care Unit
 The Influence of Race and Ethnicity on End-of-Life Care in the Intensive Care Unit Sarah Muni, MD Department of Medicine Chair s Rounds November 10, 2009 Health Disparities Research Clinical appropriateness
The Influence of Race and Ethnicity on End-of-Life Care in the Intensive Care Unit Sarah Muni, MD Department of Medicine Chair s Rounds November 10, 2009 Health Disparities Research Clinical appropriateness
BIOSTATISTICAL METHODS
 BIOSTATISTICAL METHODS FOR TRANSLATIONAL & CLINICAL RESEARCH PROPENSITY SCORE Confounding Definition: A situation in which the effect or association between an exposure (a predictor or risk factor) and
BIOSTATISTICAL METHODS FOR TRANSLATIONAL & CLINICAL RESEARCH PROPENSITY SCORE Confounding Definition: A situation in which the effect or association between an exposure (a predictor or risk factor) and
Critical care resources are often provided to the too well and as well as. to the too sick. The former include the patients admitted to an ICU
 Literature Review Critical care resources are often provided to the too well and as well as to the too sick. The former include the patients admitted to an ICU following major elective surgery for overnight
Literature Review Critical care resources are often provided to the too well and as well as to the too sick. The former include the patients admitted to an ICU following major elective surgery for overnight
Ischemic Stroke in Critically Ill Patients with Malignancy
 Ischemic Stroke in Critically Ill Patients with Malignancy Jeong-Am Ryu 1, Oh Young Bang 2, Daesang Lee 1, Jinkyeong Park 1, Jeong Hoon Yang 1, Gee Young Suh 1, Joongbum Cho 1, Chi Ryang Chung 1, Chi-Min
Ischemic Stroke in Critically Ill Patients with Malignancy Jeong-Am Ryu 1, Oh Young Bang 2, Daesang Lee 1, Jinkyeong Park 1, Jeong Hoon Yang 1, Gee Young Suh 1, Joongbum Cho 1, Chi Ryang Chung 1, Chi-Min
Effect of post-intubation hypotension on outcomes in major trauma patients
 Effect of post-intubation hypotension on outcomes in major trauma patients Dr. Robert S. Green Professor, Emergency Medicine and Critical Care Dalhousie University Medical Director, Trauma Nova Scotia
Effect of post-intubation hypotension on outcomes in major trauma patients Dr. Robert S. Green Professor, Emergency Medicine and Critical Care Dalhousie University Medical Director, Trauma Nova Scotia
ELIZABETH CEDARS DR. KOREY HOOD Available September 29
 ELIZABETH CEDARS DR. KOREY HOOD Available September 29 Title and Investigators Optimizing Surgical Management of Thyroid Cancer: Using Surgeon-performed Ultrasound to Predict Extrathyroidal Extension of
ELIZABETH CEDARS DR. KOREY HOOD Available September 29 Title and Investigators Optimizing Surgical Management of Thyroid Cancer: Using Surgeon-performed Ultrasound to Predict Extrathyroidal Extension of
DATA ELEMENTS NEEDED FOR QUALITY ASSESSMENT COPYRIGHT NOTICE
 DATA ELEMENTS NEEDED FOR QUALITY ASSESSMENT COPYRIGHT NOTICE Washington University grants permission to use and reproduce the Data Elements Needed for Quality Assessment exactly as it appears in the PDF
DATA ELEMENTS NEEDED FOR QUALITY ASSESSMENT COPYRIGHT NOTICE Washington University grants permission to use and reproduce the Data Elements Needed for Quality Assessment exactly as it appears in the PDF
Association between Medical Costs and the ProVent Model in Patients Requiring Prolonged Mechanical Ventilation
 ORIGINAL ARTICLE https://doi.org/10.4046/trd.2018.0065 ISSN: 1738-3536(Print)/2005-6184(Online) Tuberc Respir Dis, Respir Dis 2019;82:166-172 Association between Medical Costs and the ProVent Model in
ORIGINAL ARTICLE https://doi.org/10.4046/trd.2018.0065 ISSN: 1738-3536(Print)/2005-6184(Online) Tuberc Respir Dis, Respir Dis 2019;82:166-172 Association between Medical Costs and the ProVent Model in
The Association between Renin-Angiotensin System Blockade, Premorbid Blood Pressure Control, and Acute Kidney Injury in Critically Ill Patients
 ICU AKI RAS A The Association between Renin-Angiotensin System Blockade, Premorbid Blood Pressure Control, and Acute Kidney Injury in Critically Ill Patients Acute Kidney Injury: AKI KDIGO ICU A 30 60%
ICU AKI RAS A The Association between Renin-Angiotensin System Blockade, Premorbid Blood Pressure Control, and Acute Kidney Injury in Critically Ill Patients Acute Kidney Injury: AKI KDIGO ICU A 30 60%
External Validation of the Acute Physiology and Chronic Health Evaluation II in Korean Intensive Care Units
 Original Article http://dx.doi.org/10.3349/ymj.2013.54.2.425 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 54(2):425-431, 2013 External Validation of the Acute Physiology and Chronic Health Evaluation
Original Article http://dx.doi.org/10.3349/ymj.2013.54.2.425 pissn: 0513-5796, eissn: 1976-2437 Yonsei Med J 54(2):425-431, 2013 External Validation of the Acute Physiology and Chronic Health Evaluation
Preoperative Biliary Drainage Among Patients With Resectable Hepatobiliary Malignancy: Does Technique Matter?
 Preoperative Biliary Drainage Among Patients With Resectable Hepatobiliary Malignancy: Does Technique Matter? Q. Lina Hu, MD; Jason B. Liu, MD, MS; Ryan J. Ellis, MD, MS; Jessica Y. Liu, MD, MS; Anthony
Preoperative Biliary Drainage Among Patients With Resectable Hepatobiliary Malignancy: Does Technique Matter? Q. Lina Hu, MD; Jason B. Liu, MD, MS; Ryan J. Ellis, MD, MS; Jessica Y. Liu, MD, MS; Anthony
Temporal Trends in Demographics and Overall Survival of Non Small-Cell Lung Cancer Patients at Moffitt Cancer Center From 1986 to 2008
 Special Report Temporal Trends in Demographics and Overall Survival of Non Small-Cell Lung Cancer Patients at Moffitt Cancer Center From 1986 to 2008 Matthew B. Schabath, PhD, Zachary J. Thompson, PhD,
Special Report Temporal Trends in Demographics and Overall Survival of Non Small-Cell Lung Cancer Patients at Moffitt Cancer Center From 1986 to 2008 Matthew B. Schabath, PhD, Zachary J. Thompson, PhD,
Admissions with severe sepsis in adult, general critical care units in England, Wales and Northern Ireland
 Admissions with severe sepsis in adult, general critical care units in England, Wales and Northern Ireland Question For all admissions to adult, general critical care units in the Case Mix Programme Database
Admissions with severe sepsis in adult, general critical care units in England, Wales and Northern Ireland Question For all admissions to adult, general critical care units in the Case Mix Programme Database
Outcome and prognostic factors of lung cancer patients admitted to the medical intensive care unit
 Eur Respir J 2008; 31: 47 53 DOI: 10.1183/09031936.00031607 CopyrightßERS Journals Ltd 2008 Outcome and prognostic factors of lung cancer patients admitted to the medical intensive care unit A.K. Adam*
Eur Respir J 2008; 31: 47 53 DOI: 10.1183/09031936.00031607 CopyrightßERS Journals Ltd 2008 Outcome and prognostic factors of lung cancer patients admitted to the medical intensive care unit A.K. Adam*
Antidepressant Use and Depressive Symptoms in Intensive Care Unit Survivors
 Antidepressant Use in ICU Survivors 1 Antidepressant Use and Depressive Symptoms in Intensive Care Unit Survivors Sophia Wang, MD, Chris Mosher, MD, Sujuan Gao, PhD, Kayla Kirk, MA, Sue Lasiter, PhD, RN,
Antidepressant Use in ICU Survivors 1 Antidepressant Use and Depressive Symptoms in Intensive Care Unit Survivors Sophia Wang, MD, Chris Mosher, MD, Sujuan Gao, PhD, Kayla Kirk, MA, Sue Lasiter, PhD, RN,
Hemodynamic Monitoring Using Switching Autoregressive Dynamics of Multivariate Vital Sign Time Series
 Hemodynamic Monitoring Using Switching Autoregressive Dynamics of Multivariate Vital Sign Time Series Li-Wei H. Lehman, MIT Shamim Nemati, Emory University Roger G. Mark, MIT Proceedings Title: Computing
Hemodynamic Monitoring Using Switching Autoregressive Dynamics of Multivariate Vital Sign Time Series Li-Wei H. Lehman, MIT Shamim Nemati, Emory University Roger G. Mark, MIT Proceedings Title: Computing
OHSU. Update in Sepsis
 Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
Update in Sepsis Jonathan Pak, MD June 1, 2017 Structure of Talk 1. Sepsis-3: The latest definition 2. Clinical Management - Is EGDT dead? - Surviving Sepsis Campaign Guidelines 3. A novel therapy: Vitamin
NIH Public Access Author Manuscript Comput Cardiol (2010). Author manuscript; available in PMC 2014 March 25.
. Author manuscript; available in PMC 2014 March 25.") NIH Public Access Author Manuscript Published in final edited form as: Comput Cardiol (2010). 2012 ; 39: 245 248. Predicting In-Hospital Mortality of ICU Patients: The PhysioNet/ Computing in Cardiology
NIH Public Access Author Manuscript Published in final edited form as: Comput Cardiol (2010). 2012 ; 39: 245 248. Predicting In-Hospital Mortality of ICU Patients: The PhysioNet/ Computing in Cardiology
Evaluation of Serum Lactate as Predictor of Morbidity and Mortality in Sepsis and Trauma Cases
 IOSR Journal of Pharmacy and Biological Sciences (IOSR-JPBS) e-issn:2278-38, p-issn:2319-7676. Volume 12, Issue 3 Ver. VII (May June 217), PP 1-5 www.iosrjournals.org Evaluation of Serum Lactate as Predictor
IOSR Journal of Pharmacy and Biological Sciences (IOSR-JPBS) e-issn:2278-38, p-issn:2319-7676. Volume 12, Issue 3 Ver. VII (May June 217), PP 1-5 www.iosrjournals.org Evaluation of Serum Lactate as Predictor
PERIOPERATIVE cardiopulmonary arrests are
 Predictors of Survival from Perioperative Cardiopulmonary Arrests A Retrospective Analysis of 2,524 Events from the Get With The Guidelines-Resuscitation Registry Satya Krishna Ramachandran, M.D., F.R.C.A.,*
Predictors of Survival from Perioperative Cardiopulmonary Arrests A Retrospective Analysis of 2,524 Events from the Get With The Guidelines-Resuscitation Registry Satya Krishna Ramachandran, M.D., F.R.C.A.,*
Risk of Fractures Following Cataract Surgery in Medicare Beneficiaries
 Risk of Fractures Following Cataract Surgery in Medicare Beneficiaries Victoria L. Tseng, MD, Fei Yu, PhD, Flora Lum, MD, Anne L. Coleman, MD, PhD JAMA. 2012;308(5):493-501 Background Visual impairment
Risk of Fractures Following Cataract Surgery in Medicare Beneficiaries Victoria L. Tseng, MD, Fei Yu, PhD, Flora Lum, MD, Anne L. Coleman, MD, PhD JAMA. 2012;308(5):493-501 Background Visual impairment
JAMA. 2016;315(8): doi: /jama
: doi: /jama") JAMA. 2016;315(8):801-810. doi:10.1001/jama.2016.0287 SEPSIS 3 life-threatening organ dysfunction caused by a dysregulated host response to infection organ dysfunction: an increase in the SOFA
JAMA. 2016;315(8):801-810. doi:10.1001/jama.2016.0287 SEPSIS 3 life-threatening organ dysfunction caused by a dysregulated host response to infection organ dysfunction: an increase in the SOFA
Lecture Outline. Biost 590: Statistical Consulting. Stages of Scientific Studies. Scientific Method
 Biost 590: Statistical Consulting Statistical Classification of Scientific Studies; Approach to Consulting Lecture Outline Statistical Classification of Scientific Studies Statistical Tasks Approach to
Biost 590: Statistical Consulting Statistical Classification of Scientific Studies; Approach to Consulting Lecture Outline Statistical Classification of Scientific Studies Statistical Tasks Approach to
PubH 7405: REGRESSION ANALYSIS. Propensity Score
 PubH 7405: REGRESSION ANALYSIS Propensity Score INTRODUCTION: There is a growing interest in using observational (or nonrandomized) studies to estimate the effects of treatments on outcomes. In observational
PubH 7405: REGRESSION ANALYSIS Propensity Score INTRODUCTION: There is a growing interest in using observational (or nonrandomized) studies to estimate the effects of treatments on outcomes. In observational
Comorbidity and intensive care outcome a multivariable analysis 2C01, 3C00
 The Intensive Care Society 2014 Original articles Comorbidity and intensive care outcome a multivariable analysis 2C01, 3C00 RI Docking, A Mackay, C Williams, J Lewsey, J Kinsella, MG Booth Decisions regarding
The Intensive Care Society 2014 Original articles Comorbidity and intensive care outcome a multivariable analysis 2C01, 3C00 RI Docking, A Mackay, C Williams, J Lewsey, J Kinsella, MG Booth Decisions regarding
Effect of ARDS Severity and Etiology on Short-Term Outcomes
 Effect of ARDS Severity and Etiology on Short-Term Outcomes Haitham El-Haddad MD, Hyejeong Jang MSc, Wei Chen PhD, and Ayman O Soubani MD BACKGROUND: We evaluated the outcome of subjects with ARDS in relation
Effect of ARDS Severity and Etiology on Short-Term Outcomes Haitham El-Haddad MD, Hyejeong Jang MSc, Wei Chen PhD, and Ayman O Soubani MD BACKGROUND: We evaluated the outcome of subjects with ARDS in relation
In each hospital-year, we calculated a 30-day unplanned. readmission rate among patients who survived at least 30 days
 Romley JA, Goldman DP, Sood N. US hospitals experienced substantial productivity growth during 2002 11. Health Aff (Millwood). 2015;34(3). Published online February 11, 2015. Appendix Adjusting hospital
Romley JA, Goldman DP, Sood N. US hospitals experienced substantial productivity growth during 2002 11. Health Aff (Millwood). 2015;34(3). Published online February 11, 2015. Appendix Adjusting hospital
Representation of Patients with Cardiovascular Disease in Pivotal Cancer. Clinical Trials
 Representation of Patients with Cardiovascular Disease in Pivotal Cancer Clinical Trials Running Title: Bonsu & Charles et al.; Cardiovascular Patients in Cancer Trials Janice Bonsu, MPH 1* ; Lawrence
Representation of Patients with Cardiovascular Disease in Pivotal Cancer Clinical Trials Running Title: Bonsu & Charles et al.; Cardiovascular Patients in Cancer Trials Janice Bonsu, MPH 1* ; Lawrence
Transfusion for the sickest ICU patients: Are there unanswered questions?
 Transfusion for the sickest ICU patients: Are there unanswered questions? Tim Walsh Professor of Critical Care Edinburgh University None Conflict of Interest Guidelines on the management of anaemia and
Transfusion for the sickest ICU patients: Are there unanswered questions? Tim Walsh Professor of Critical Care Edinburgh University None Conflict of Interest Guidelines on the management of anaemia and
THE CLINICAL course of severe
 ORIGINAL ARTICLE Improved Prediction of Outcome in Patients With Severe Acute Pancreatitis by the APACHE II Score at 48 Hours After Hospital Admission Compared With the at Admission Arif A. Khan, MD; Dilip
ORIGINAL ARTICLE Improved Prediction of Outcome in Patients With Severe Acute Pancreatitis by the APACHE II Score at 48 Hours After Hospital Admission Compared With the at Admission Arif A. Khan, MD; Dilip
Outcomes of Patients with Preoperative Weight Loss following Colorectal Surgery
 Outcomes of Patients with Preoperative Weight Loss following Colorectal Surgery Zhobin Moghadamyeghaneh MD 1, Michael J. Stamos MD 1 1 Department of Surgery, University of California, Irvine Nothing to
Outcomes of Patients with Preoperative Weight Loss following Colorectal Surgery Zhobin Moghadamyeghaneh MD 1, Michael J. Stamos MD 1 1 Department of Surgery, University of California, Irvine Nothing to
ICU Admission Improves Pneumonia Outcomes
 ICU Admission Improves Pneumonia Outcomes 1 Colin R. Cooke, MD, MSc, MS Assistant Professor of Medicine Pulmonary & Critical Care Medicine, Center for Healthcare Outcomes & Policy, Institute for Healthcare
ICU Admission Improves Pneumonia Outcomes 1 Colin R. Cooke, MD, MSc, MS Assistant Professor of Medicine Pulmonary & Critical Care Medicine, Center for Healthcare Outcomes & Policy, Institute for Healthcare
Stuart Murdoch Consultant Intensive Care St. James s University Hospital March 2010
 Stuart Murdoch Consultant Intensive Care St. James s University Hospital March 2010 Background- Critical Care Critical Care originated in Denmark with Polio epidemic 1950s respiratory support alone Rapid
Stuart Murdoch Consultant Intensive Care St. James s University Hospital March 2010 Background- Critical Care Critical Care originated in Denmark with Polio epidemic 1950s respiratory support alone Rapid
Hyperglycemia occurs frequently in critically ill patients.
 Mayo Clin Proc, December 2003, Vol 78 Hyperglycemia and Increased Hospital Mortality 1471 Original Article Association Between Hyperglycemia and Increased Hospital Mortality in a Heterogeneous Population
Mayo Clin Proc, December 2003, Vol 78 Hyperglycemia and Increased Hospital Mortality 1471 Original Article Association Between Hyperglycemia and Increased Hospital Mortality in a Heterogeneous Population
Aetiology versus Prediction - correct for Confounding? Friedo Dekker ERA-EDTA Registry / LUMC
 Aetiology versus Prediction - correct for Confounding? Friedo Dekker ERA-EDTA Registry / LUMC Aetiology Study effect of a risk factor on an outcome Consider potential confounding: other risk factor for
Aetiology versus Prediction - correct for Confounding? Friedo Dekker ERA-EDTA Registry / LUMC Aetiology Study effect of a risk factor on an outcome Consider potential confounding: other risk factor for
Surgical resection improves survival in pancreatic cancer patients without vascular invasion- a population based study
 Original article Annals of Gastroenterology (2013) 26, 346-352 Surgical resection improves survival in pancreatic cancer patients without vascular invasion- a population based study Subhankar Chakraborty
Original article Annals of Gastroenterology (2013) 26, 346-352 Surgical resection improves survival in pancreatic cancer patients without vascular invasion- a population based study Subhankar Chakraborty
Postoperative hypothermia and patient outcomes after elective cardiac surgery
 doi:10.1111/j.1365-2044.2011.06784.x ORIGINAL ARTICLE Postoperative hypothermia and patient outcomes after elective cardiac surgery D. Karalapillai, 1 D. Story, 2 G. K. Hart, 3,4 M. Bailey, 5 D. Pilcher,
doi:10.1111/j.1365-2044.2011.06784.x ORIGINAL ARTICLE Postoperative hypothermia and patient outcomes after elective cardiac surgery D. Karalapillai, 1 D. Story, 2 G. K. Hart, 3,4 M. Bailey, 5 D. Pilcher,
Roadmap for Developing and Validating Therapeutically Relevant Genomic Classifiers. Richard Simon, J Clin Oncol 23:
 Roadmap for Developing and Validating Therapeutically Relevant Genomic Classifiers. Richard Simon, J Clin Oncol 23:7332-7341 Presented by Deming Mi 7/25/2006 Major reasons for few prognostic factors to
Roadmap for Developing and Validating Therapeutically Relevant Genomic Classifiers. Richard Simon, J Clin Oncol 23:7332-7341 Presented by Deming Mi 7/25/2006 Major reasons for few prognostic factors to
A new measure of acute physiological derangement for patients with exacerbations of obstructive airways disease: The COPD and Asthma Physiology Score
 Respiratory Medicine (2007) 101, 1994 2002 A new measure of acute physiological derangement for patients with exacerbations of obstructive airways disease: The COPD and Asthma Physiology Score Martin J.
Respiratory Medicine (2007) 101, 1994 2002 A new measure of acute physiological derangement for patients with exacerbations of obstructive airways disease: The COPD and Asthma Physiology Score Martin J.
Serum potassium levels and outcomes in critically ill patients in the medical intensive care unit
 Clinical Report Serum potassium levels and outcomes in critically ill patients in the medical intensive care unit Journal of International Medical Research 2018, Vol. 46(3) 1254 1262! The Author(s) 2018
Clinical Report Serum potassium levels and outcomes in critically ill patients in the medical intensive care unit Journal of International Medical Research 2018, Vol. 46(3) 1254 1262! The Author(s) 2018
NIH Public Access Author Manuscript Parkinsonism Relat Disord. Author manuscript; available in PMC 2009 August 1.
 NIH Public Access Author Manuscript Published in final edited form as: Parkinsonism Relat Disord. 2009 August ; 15(7): 535 538. doi:10.1016/j.parkreldis.2008.10.006. Embarrassment in Essential Tremor:
NIH Public Access Author Manuscript Published in final edited form as: Parkinsonism Relat Disord. 2009 August ; 15(7): 535 538. doi:10.1016/j.parkreldis.2008.10.006. Embarrassment in Essential Tremor:
NIH Public Access Author Manuscript Intensive Care Med. Author manuscript; available in PMC 2010 August 19.
 NIH Public Access Author Manuscript Published in final edited form as: Intensive Care Med. 2009 July ; 35(7): 1261 1264. doi:10.1007/s00134-009-1448-x. The significance of non-sustained hypotension in
NIH Public Access Author Manuscript Published in final edited form as: Intensive Care Med. 2009 July ; 35(7): 1261 1264. doi:10.1007/s00134-009-1448-x. The significance of non-sustained hypotension in
Updates on the Conflict of Postoperative Radiotherapy Impact on Survival of Young Women with Cancer Breast: A Retrospective Cohort Study
 International Journal of Medical Research & Health Sciences Available online at www.ijmrhs.com ISSN No: 2319-5886 International Journal of Medical Research & Health Sciences, 2017, 6(7): 14-18 I J M R
International Journal of Medical Research & Health Sciences Available online at www.ijmrhs.com ISSN No: 2319-5886 International Journal of Medical Research & Health Sciences, 2017, 6(7): 14-18 I J M R
European Journal of Internal Medicine
 European Journal of Internal Medicine 22 (2011) 57 61 Contents lists available at ScienceDirect European Journal of Internal Medicine journal homepage: www.elsevier.com/locate/ejim Original article Prognosis
European Journal of Internal Medicine 22 (2011) 57 61 Contents lists available at ScienceDirect European Journal of Internal Medicine journal homepage: www.elsevier.com/locate/ejim Original article Prognosis
Online Supplementary Appendix
 Online Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Lehman * LH, Saeed * M, Talmor D, Mark RG, and Malhotra
Online Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Lehman * LH, Saeed * M, Talmor D, Mark RG, and Malhotra
Patient Experience Research in Malignant Hematology: describing the lived experience of illness with acute myeloid leukemia
 Patient Experience Research in Malignant Hematology: describing the lived experience of illness with acute myeloid leukemia Thomas W. LeBlanc, MD, MA, MHS, FAAHPM Associate Professor of Medicine Division
Patient Experience Research in Malignant Hematology: describing the lived experience of illness with acute myeloid leukemia Thomas W. LeBlanc, MD, MA, MHS, FAAHPM Associate Professor of Medicine Division
Accuracy of endoscopic ultrasound staging for T2N0 esophageal cancer: a national cancer database analysis
 Review Article Accuracy of endoscopic ultrasound staging for T2N0 esophageal cancer: a national cancer database analysis Ravi Shridhar 1, Jamie Huston 2, Kenneth L. Meredith 2 1 Department of Radiation
Review Article Accuracy of endoscopic ultrasound staging for T2N0 esophageal cancer: a national cancer database analysis Ravi Shridhar 1, Jamie Huston 2, Kenneth L. Meredith 2 1 Department of Radiation
FACTORS ASSOCIATED WITH NEVUS VOLATILITY IN EARLY ADOLESCENCE
 FACTORS ASSOCIATED WITH NEVUS VOLATILITY IN EARLY ADOLESCENCE The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters Citation Oliveria,
FACTORS ASSOCIATED WITH NEVUS VOLATILITY IN EARLY ADOLESCENCE The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters Citation Oliveria,
Systemic Inflammatory Response Syndrome Criteria in Defining Severe Sepsis
 The new england journal of medicine original article Systemic Inflammatory Response Syndrome Criteria in Defining Severe Sepsis Kirsi-Maija Kaukonen, M.D., Ph.D., Michael Bailey, Ph.D., David Pilcher,
The new england journal of medicine original article Systemic Inflammatory Response Syndrome Criteria in Defining Severe Sepsis Kirsi-Maija Kaukonen, M.D., Ph.D., Michael Bailey, Ph.D., David Pilcher,
Risk Factors Predicting Mortality in Spinal Cord Injury in Nigeria
 Article ID: WMC00807 ISSN 2046690 Risk Factors Predicting Mortality in Spinal Cord Injury in Nigeria Corresponding Author: Dr. Ahidjo Kawu, Consultant Surgeon, Dept of Orthopaedics, UATH, Gwagwalada Abuja
Article ID: WMC00807 ISSN 2046690 Risk Factors Predicting Mortality in Spinal Cord Injury in Nigeria Corresponding Author: Dr. Ahidjo Kawu, Consultant Surgeon, Dept of Orthopaedics, UATH, Gwagwalada Abuja
Evidence-Based Medicine Journal Club. A Primer in Statistics, Study Design, and Epidemiology. August, 2013
 Evidence-Based Medicine Journal Club A Primer in Statistics, Study Design, and Epidemiology August, 2013 Rationale for EBM Conscientious, explicit, and judicious use Beyond clinical experience and physiologic
Evidence-Based Medicine Journal Club A Primer in Statistics, Study Design, and Epidemiology August, 2013 Rationale for EBM Conscientious, explicit, and judicious use Beyond clinical experience and physiologic
Predictors of Post-injury Mortality in Elderly Patients with Trauma: A Master's Thesis
 University of Massachusetts Medical School escholarship@umms GSBS Dissertations and Theses Graduate School of Biomedical Sciences 7-21-2016 Predictors of Post-injury Mortality in Elderly Patients with
University of Massachusetts Medical School escholarship@umms GSBS Dissertations and Theses Graduate School of Biomedical Sciences 7-21-2016 Predictors of Post-injury Mortality in Elderly Patients with
Study protocol v. 1.0 Systematic review of the Sequential Organ Failure Assessment score as a surrogate endpoint in randomized controlled trials
 Study protocol v. 1.0 Systematic review of the Sequential Organ Failure Assessment score as a surrogate endpoint in randomized controlled trials Harm Jan de Grooth, Jean Jacques Parienti, [to be determined],
Study protocol v. 1.0 Systematic review of the Sequential Organ Failure Assessment score as a surrogate endpoint in randomized controlled trials Harm Jan de Grooth, Jean Jacques Parienti, [to be determined],
OUTCOME PREDICTION IS IMportant
 CARING FOR THE CRITICALLY ILL PATIENT Serial Evaluation of the SOFA Score to Predict Outcome in Critically Ill Flavio Lopes Ferreira, MD Daliana Peres Bota, MD Annette Bross, MD Christian Mélot, MD, PhD,
CARING FOR THE CRITICALLY ILL PATIENT Serial Evaluation of the SOFA Score to Predict Outcome in Critically Ill Flavio Lopes Ferreira, MD Daliana Peres Bota, MD Annette Bross, MD Christian Mélot, MD, PhD,
Lecture Outline Biost 517 Applied Biostatistics I
 Lecture Outline Biost 517 Applied Biostatistics I Scott S. Emerson, M.D., Ph.D. Professor of Biostatistics University of Washington Lecture 2: Statistical Classification of Scientific Questions Types of
Lecture Outline Biost 517 Applied Biostatistics I Scott S. Emerson, M.D., Ph.D. Professor of Biostatistics University of Washington Lecture 2: Statistical Classification of Scientific Questions Types of
The Pennsylvania State University. The Graduate School. Department of Public Health Sciences
 The Pennsylvania State University The Graduate School Department of Public Health Sciences THE LENGTH OF STAY AND READMISSIONS IN MASTECTOMY PATIENTS A Thesis in Public Health Sciences by Susie Sun 2015
The Pennsylvania State University The Graduate School Department of Public Health Sciences THE LENGTH OF STAY AND READMISSIONS IN MASTECTOMY PATIENTS A Thesis in Public Health Sciences by Susie Sun 2015
Sepsis 3.0: The Impact on Quality Improvement Programs
 Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
Sepsis 3.0: The Impact on Quality Improvement Programs Mitchell M. Levy MD, MCCM Professor of Medicine Chief, Division of Pulmonary, Sleep, and Critical Care Warren Alpert Medical School of Brown University
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Chan PS, Nallamothu BK, Krumholz HM, et al. Long-term outcomes
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Chan PS, Nallamothu BK, Krumholz HM, et al. Long-term outcomes
Supplementary Online Content
 Supplementary Online Content Seymour CW, Liu V, Iwashyna TJ, et al. Assessment of clinical criteria for sepsis: for the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3).
Supplementary Online Content Seymour CW, Liu V, Iwashyna TJ, et al. Assessment of clinical criteria for sepsis: for the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3).
8.0 Parenteral Nutrition vs. Standard care May 2015
 8.0 Parenteral Nutrition vs. Standard care May 015 015 Recommendation: Based on 6 level studies, in critically ill patients with an intact gastrointestinal tract, we recommend that parenteral nutrition
8.0 Parenteral Nutrition vs. Standard care May 015 015 Recommendation: Based on 6 level studies, in critically ill patients with an intact gastrointestinal tract, we recommend that parenteral nutrition
Cover Page. The handle holds various files of this Leiden University dissertation
 Cover Page The handle http://hdl.handle.net/1887/22997 holds various files of this Leiden University dissertation Author: Wilden, Gwendolyn M. van der Title: The value of surgical treatment in abdominal
Cover Page The handle http://hdl.handle.net/1887/22997 holds various files of this Leiden University dissertation Author: Wilden, Gwendolyn M. van der Title: The value of surgical treatment in abdominal
MAKING THE NSQIP PARTICIPANT USE DATA FILE (PUF) WORK FOR YOU
 WORK FOR YOU") MAKING THE NSQIP PARTICIPANT USE DATA FILE (PUF) WORK FOR YOU Hani Tamim, PhD Clinical Research Institute Department of Internal Medicine American University of Beirut Medical Center Beirut - Lebanon Participant
MAKING THE NSQIP PARTICIPANT USE DATA FILE (PUF) WORK FOR YOU Hani Tamim, PhD Clinical Research Institute Department of Internal Medicine American University of Beirut Medical Center Beirut - Lebanon Participant
CLINICAL SCIENCE INTRODUCTION
 CLINICS 2008;63:343-50 CLINICAL SCIENCE Effects of early changes in organ dysfunctions on the outcomes of critically ill patients in need of renal replacement therapy Elizabeth Maccariello, Eduardo Rocha,
CLINICS 2008;63:343-50 CLINICAL SCIENCE Effects of early changes in organ dysfunctions on the outcomes of critically ill patients in need of renal replacement therapy Elizabeth Maccariello, Eduardo Rocha,
WHAT FACTORS INFLUENCE AN ANALYSIS OF HOSPITALIZATIONS AMONG DYING CANCER PATIENTS? AGGRESSIVE END-OF-LIFE CANCER CARE. Deesha Patel May 11, 2011
 WHAT FACTORS INFLUENCE HOSPITALIZATIONS AMONG DYING CANCER PATIENTS? AN ANALYSIS OF AGGRESSIVE END-OF-LIFE CANCER CARE. Deesha Patel May 11, 2011 WHAT IS AGGRESSIVE EOL CARE? Use of ineffective medical
WHAT FACTORS INFLUENCE HOSPITALIZATIONS AMONG DYING CANCER PATIENTS? AN ANALYSIS OF AGGRESSIVE END-OF-LIFE CANCER CARE. Deesha Patel May 11, 2011 WHAT IS AGGRESSIVE EOL CARE? Use of ineffective medical
Early-goal-directed therapy and protocolised treatment in septic shock
 CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
CAT reviews Early-goal-directed therapy and protocolised treatment in septic shock Journal of the Intensive Care Society 2015, Vol. 16(2) 164 168! The Intensive Care Society 2014 Reprints and permissions:
Journal Club American Journal of Respiratory and Critical Care Medicine. Zhang Junyi
 Journal Club 2018 American Journal of Respiratory and Critical Care Medicine Zhang Junyi 2018.11.23 Background Mechanical Ventilation A life-saving technique used worldwide 15 million patients annually
Journal Club 2018 American Journal of Respiratory and Critical Care Medicine Zhang Junyi 2018.11.23 Background Mechanical Ventilation A life-saving technique used worldwide 15 million patients annually
Hemodynamic monitoring using switching autoregressive dynamics of multivariate vital sign time series
 Hemodynamic monitoring using switching autoregressive dynamics of multivariate vital sign time series The MIT Faculty has made this article openly available. Please share how this access benefits you.
Hemodynamic monitoring using switching autoregressive dynamics of multivariate vital sign time series The MIT Faculty has made this article openly available. Please share how this access benefits you.
Transfusion & Mortality. Philippe Van der Linden MD, PhD
 Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
Transfusion & Mortality Philippe Van der Linden MD, PhD Conflict of Interest Disclosure In the past 5 years, I have received honoraria or travel support for consulting or lecturing from the following companies:
Aanvraag gegevens ten behoeve van wetenschappelijk onderzoek
 Aanvraag gegevens ten behoeve van wetenschappelijk onderzoek Registatie waarvan gegevens worden opgevraagd: NBCA Contactpersoon Nederland: Naam: Dr. A.C.M. van Bommel of Dr. H.A. Rakhorst Centrum/Ziekenhuis:
Aanvraag gegevens ten behoeve van wetenschappelijk onderzoek Registatie waarvan gegevens worden opgevraagd: NBCA Contactpersoon Nederland: Naam: Dr. A.C.M. van Bommel of Dr. H.A. Rakhorst Centrum/Ziekenhuis:
Chapter 17 Sensitivity Analysis and Model Validation
 Chapter 17 Sensitivity Analysis and Model Validation Justin D. Salciccioli, Yves Crutain, Matthieu Komorowski and Dominic C. Marshall Learning Objectives Appreciate that all models possess inherent limitations
Chapter 17 Sensitivity Analysis and Model Validation Justin D. Salciccioli, Yves Crutain, Matthieu Komorowski and Dominic C. Marshall Learning Objectives Appreciate that all models possess inherent limitations
Supplementary Online Content
 Supplementary Online Content Lee JS, Nsa W, Hausmann LRM, et al. Quality of care for elderly patients hospitalized for pneumonia in the United States, 2006 to 2010. JAMA Intern Med. Published online September
Supplementary Online Content Lee JS, Nsa W, Hausmann LRM, et al. Quality of care for elderly patients hospitalized for pneumonia in the United States, 2006 to 2010. JAMA Intern Med. Published online September
SEPTIC SHOCK PREDICTION FOR PATIENTS WITH MISSING DATA. Joyce C Ho, Cheng Lee, Joydeep Ghosh University of Texas at Austin
 SEPTIC SHOCK PREDICTION FOR PATIENTS WITH MISSING DATA Joyce C Ho, Cheng Lee, Joydeep Ghosh University of Texas at Austin WHAT IS SEPSIS AND SEPTIC SHOCK? Sepsis is a systemic inflammatory response to
SEPTIC SHOCK PREDICTION FOR PATIENTS WITH MISSING DATA Joyce C Ho, Cheng Lee, Joydeep Ghosh University of Texas at Austin WHAT IS SEPSIS AND SEPTIC SHOCK? Sepsis is a systemic inflammatory response to
Introduction. Original Article
 Korean J Crit Care Med 2017 November 32(4):340-346 / ISSN 2383-4870 (Print) ㆍ ISSN 2383-4889 (Online) Original Article Acute Physiology and Chronic Health Evaluation II Score and Sequential Organ Failure
Korean J Crit Care Med 2017 November 32(4):340-346 / ISSN 2383-4870 (Print) ㆍ ISSN 2383-4889 (Online) Original Article Acute Physiology and Chronic Health Evaluation II Score and Sequential Organ Failure
Anesthesiology and Intensive Care Department, University of Medicine and Pharmacology of Craiova, Romania 2
 Current Health Sciences Journal Vol. 40, No. 4, 2014 October December Original Paper The Predictive Value of Scores Used in Intensive Care Unit for Burn Patients Prognostic M. NOVAC 1, ALICE DRAGOESCU
Current Health Sciences Journal Vol. 40, No. 4, 2014 October December Original Paper The Predictive Value of Scores Used in Intensive Care Unit for Burn Patients Prognostic M. NOVAC 1, ALICE DRAGOESCU
Population based studies in Pancreatic Diseases. Satish Munigala
 Population based studies in Pancreatic Diseases Satish Munigala 1 Definition Population-based studies aim to answer research questions for defined populations 1 Generalizable to the whole population addressed
Population based studies in Pancreatic Diseases Satish Munigala 1 Definition Population-based studies aim to answer research questions for defined populations 1 Generalizable to the whole population addressed
The International CytoSorb-Registry
 The International CytoSorb-Registry Coordinating investigator Overall coordination Prof. Dr. Frank M. Brunkhorst. Jena University Hospital Financial support CytoSorbents Europe GmbH Ways to find truth
The International CytoSorb-Registry Coordinating investigator Overall coordination Prof. Dr. Frank M. Brunkhorst. Jena University Hospital Financial support CytoSorbents Europe GmbH Ways to find truth
FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME
 FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME Guillaume CARTEAUX, Teresa MILLÁN-GUILARTE, Nicolas DE PROST, Keyvan RAZAZI, Shariq ABID, Arnaud
FAILURE OF NONINVASIVE VENTILATION FOR DE NOVO ACUTE HYPOXEMIC RESPIRATORY FAILURE: ROLE OF TIDAL VOLUME Guillaume CARTEAUX, Teresa MILLÁN-GUILARTE, Nicolas DE PROST, Keyvan RAZAZI, Shariq ABID, Arnaud
Ammonia level at admission predicts in-hospital mortality for patients with alcoholic hepatitis
 Gastroenterology Report, 5(3), 2017, 232 236 doi: 10.1093/gastro/gow010 Advance Access Publication Date: 1 May 2016 Original article ORIGINAL ARTICLE Ammonia level at admission predicts in-hospital mortality
Gastroenterology Report, 5(3), 2017, 232 236 doi: 10.1093/gastro/gow010 Advance Access Publication Date: 1 May 2016 Original article ORIGINAL ARTICLE Ammonia level at admission predicts in-hospital mortality
Rapid Response Teams and End-of-Life Care. James Downar, MDCM, MHSc, FRCPC Critical Care and Palliative Care, University Health Network, Toronto
 Rapid Response Teams and End-of-Life Care James Downar, MDCM, MHSc, FRCPC Critical Care and Palliative Care, University Health Network, Toronto Conflicts of Interest To place your ad here, please call
Rapid Response Teams and End-of-Life Care James Downar, MDCM, MHSc, FRCPC Critical Care and Palliative Care, University Health Network, Toronto Conflicts of Interest To place your ad here, please call
Genetic Polymorphisms of Peptidase Inhibitor 3 (Elafin) Are. Associated with Acute Respiratory Distress Syndrome
 Are. Associated with Acute Respiratory Distress Syndrome") Genetic Polymorphisms of Peptidase Inhibitor 3 (Elafin) Are Associated with Acute Respiratory Distress Syndrome Paula Tejera 1, Zhaoxi Wang 1, Rihong Zhai 1, Li Su 1, Chau-Chyun Sheu 1, Deanne M. Taylor
Genetic Polymorphisms of Peptidase Inhibitor 3 (Elafin) Are Associated with Acute Respiratory Distress Syndrome Paula Tejera 1, Zhaoxi Wang 1, Rihong Zhai 1, Li Su 1, Chau-Chyun Sheu 1, Deanne M. Taylor
Supplementary Online Content
 Supplementary Online Content Holme Ø, Løberg M, Kalager M, et al. Effect of flexible sigmoidoscopy screening on colorectal cancer incidence and mortality: a randomized clinical trial. JAMA. doi:10.1001/jama.2014.8266
Supplementary Online Content Holme Ø, Løberg M, Kalager M, et al. Effect of flexible sigmoidoscopy screening on colorectal cancer incidence and mortality: a randomized clinical trial. JAMA. doi:10.1001/jama.2014.8266
Long-term outcomes of minor troponin elevations in the intensive care unit
 Anaesth Intensive Care 2014; 42: 356-364 Long-term outcomes of minor troponin elevations in the intensive care unit A. VELASQUEZ*, M. GHASSEMI, P. SZOLOVITS, S. PARK, J. OSORIO**, A. DEJAM, L. CELI Laboratory
Anaesth Intensive Care 2014; 42: 356-364 Long-term outcomes of minor troponin elevations in the intensive care unit A. VELASQUEZ*, M. GHASSEMI, P. SZOLOVITS, S. PARK, J. OSORIO**, A. DEJAM, L. CELI Laboratory
Disparities in the ICU: The Elderly? Shannon S. Carson, MD Associate Professor Pulmonary and Critical Care Medicine University of North Carolina
 Disparities in the ICU: The Elderly? Shannon S. Carson, MD Associate Professor Pulmonary and Critical Care Medicine University of North Carolina Critical Care Is Care of the Elderly 15,757 consecutive
Disparities in the ICU: The Elderly? Shannon S. Carson, MD Associate Professor Pulmonary and Critical Care Medicine University of North Carolina Critical Care Is Care of the Elderly 15,757 consecutive
JMSCR Vol 05 Issue 06 Page June 2017
 www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 83.27 ISSN (e)-2347-176x ISSN (p) 2455-45 DOI: https://dx.doi.org/.18535/jmscr/v5i6.1 A Study on Quick Sofa Score as a redictive
www.jmscr.igmpublication.org Impact Factor 5.84 Index Copernicus Value: 83.27 ISSN (e)-2347-176x ISSN (p) 2455-45 DOI: https://dx.doi.org/.18535/jmscr/v5i6.1 A Study on Quick Sofa Score as a redictive
Sepsis overview. Dr. Tsang Hin Hung MBBS FHKCP FRCP
 Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis
Sepsis overview Dr. Tsang Hin Hung MBBS FHKCP FRCP Epidemiology Sepsis, severe sepsis, septic shock Pathophysiology of sepsis Recent researches and advances From bench to bedside Sepsis bundle Severe sepsis