Published Ahead of Print on June 22, 2017, as doi: /haematol Copyright 2017 Ferrata Storti Foundation.
|
|
|
- Ethel Thompson
- 5 years ago
- Views:
Transcription
 reveals a specific spectrum of molecular mutations with prognostic impact: a study on 123 patients and 27 genes by Manja")
1 Published Ahead of Print on June 22, 2017, as doi: /haematol Copyright 2017 Ferrata Storti Foundation. Molecular analysis of myelodysplastic syndrome with isolated del(5q) reveals a specific spectrum of molecular mutations with prognostic impact: a study on 123 patients and 27 genes by Manja Meggendorfer, Claudia Haferlach, Wolfgang Kern, and Torsten Haferlach Haematologica 2017 [Epub ahead of print] Citation: Meggendorfer M, Haferlach C, Kern W, and Haferlach T. Molecular analysis of myelodysplastic syndrome with isolated del(5q) reveals a specific spectrum of molecular mutations with prognostic impact: a study on 123 patients and 27 genes. Haematologica. 2017; 102:xxx doi: /haematol Publisher's Disclaimer. E-publishing ahead of print is increasingly important for the rapid dissemination of science. Haematologica is, therefore, E-publishing PDF files of an early version of manuscripts that have completed a regular peer review and have been accepted for publication. E-publishing of this PDF file has been approved by the authors. After having E-published Ahead of Print, manuscripts will then undergo technical and English editing, typesetting, proof correction and be presented for the authors' final approval; the final version of the manuscript will then appear in print on a regular issue of the journal. All legal disclaimers that apply to the journal also pertain to this production process.
2 Molecular analysis of myelodysplastic syndrome with isolated del(5q) reveals a specific spectrum of molecular mutations with prognostic impact: a study on 123 patients and 27 genes Manja Meggendorfer, Claudia Haferlach, Wolfgang Kern, Torsten Haferlach MLL Munich Leukemia Laboratory, Munich, Germany Running head: Mutation pattern of MDS with isolated del(5q) Corresponding Author: Dr. rer. nat. Manja Meggendorfer, PhD MLL Munich Leukemia Laboratory Max-Lebsche-Platz Munich, Germany T: F: manja.meggendorfer@mll.com Word count: 3825 Figures: 5 Tables: 0 Supplemental material: 1 Key words: Mutation analysis, MDS with isolated del(5q), molecular marker, prognostic impact 1
3 Abstract The only cytogenetic aberration defining a myelodysplastic syndrome subtype is the deletion of the long arm of chromosome 5, giving with morphological features the diagnosis of myelodysplastic syndrome with isolated del(5q). These patients show a good prognosis and respond to treatment such as lenalidomide, but some cases progress to acute myeloid leukemia. However, the molecular mutation pattern is rarely characterized. Therefore, we investigated a large cohort of 123 myelodysplastic syndrome patients with isolated del(5q) diagnosed following the World Health Organization classifications 2008 and 2016 by sequencing 27 genes. A great proportion of patients showed no or only one mutation. Only seven genes showed mutation frequencies >5% (SF3B1, DNMT3A, TP53, TET2, CSNK1A1, ASXL1, JAK2). However, the pattern of recurrently mutated genes was comparable to other myelodysplastic syndrome subtypes by comparison to a reference cohort, except of TP53 that was significantly more often mutated in myelodysplastic syndrome with isolated del(5q). As expected, SF3B1 was frequently mutated and correlated with ring sideroblasts, while JAK2 mutations correlated with elevated platelet counts. Surprisingly, SF3B1 mutations led to significantly worse prognosis within cases with isolated del(5q), but showed a comparable outcome to other myelodysplastic syndrome subtypes with SF3B1 mutation. However, addressing genetic stability in follow-up cases might suggest different genetic mechanisms for progression to secondary acute myeloid leukemia compared to overall myelodysplastic syndrome patients. 2
4 Introduction Myelodysplastic syndromes (MDS) are a heterogeneous group of clonal bone marrow neoplasms characterized by ineffective hematopoiesis, morphologic dysplasia and peripheral cytopenias. While the degree of dysplasia and blast percentage are disease classifying, the specific types of cytopenias have minor impact on MDS classification. The diagnosis of MDS is driven by the number of dysplastic cell lineages as well as blast counts <1% in the peripheral blood (pb) or <5% in the bone marrow (BM) or <19% in pb or BM for subtypes with excess blasts and at least one cytopenia. 1 The risk stratification for MDS patients is categorized according to the Revised International Prognostic Scoring System (IPSS-R), where beside morphological features cytogenetics plays a crucial role. Some cytogenetic aberrations can also define an MDS even in the absence of morphologic dysplasia. However, also following the new WHO 2016 classification again the only cytogenetic aberration defining a MDS subtype is the deletion of the long arm of chromosome 5 (del (5q)), giving the diagnosis of MDS with isolated del(5q). Overall, less than 50% of MDS patients show an aberrant karyotype, of which del(5q) is the most common aberration presenting in 10-20% of MDS patients. 2;3 In about 55% of patients with del(5q) this aberration appears as sole abnormality, in 17% with one additional aberration, while in another 28% del(5q) appears with two or more additional cytogenetic lesions, leading by definition to a complex karyotype. 4 This is shifted towards sole del(5q) (82%) when addressing only low and intermediate-1 risk MDS according to IPSS. 5 However, the WHO classification emphasizes that the main impact of cytogenetics is rather the prognostic than the classifying information. It was shown that MDS with isolated del(5q) shows a good prognosis, while MDS with del(5q) within a complex karyotype shows a poor prognosis. 2;4 In recent years the prognostic impact of additional aberrations was addressed, showing that the presence of only one aberration in addition to del(5) (excluding the abnormality -7 or del(7q)) had no adverse effect on prognosis. 6 Therefore, in the new WHO classification 2016 a diagnosis of MDS with isolated del(5q) allows the presence of one additional aberration excluding aberrations affecting chromosome 7. 1 Beside the good prognosis of these patients, a sensitivity for specific treatments such as lenalidomide was demonstrated. 7;8 Morphologically MDS with isolated del(5q) is defined by blast counts <1% in the pb and <5% in the BM, severe macrocytic anemia and frequent thrombocytosis. Patients with MDS with isolated del(5q) show a lower risk for progression to AML than other MDS. However, about 10% of these patients evolve to secondary AML. 4;9;10 Underlying pathobiological mechanisms are still under debate, while recent studies indicate that TP53 mutation as well as karyotype evolution predict disease progression. 11;12 3
5 Furthermore, the separation of MDS from reactive causes remains a challenge. In the recent years large data sets became available showing a limited number of genes to be mutated in patients with MDS % of patients show at least one mutation in one of the >100 addressed genes, supporting the clonal hematopoiesis of the disease and with that the diagnosis. 13;14 Even more, it was shown that the increasing number of gene mutations correlates with the disease outcome in MDS patients and addition of these data improves the existing risk stratifications. 13;14 Mutations in TP53 are overall associated with adverse outcome and an aggressive disease course in MDS. Furthermore, in MDS with isolated del(5q) a TP53 mutation seems to predict a poorer response to lenalidomide and a higher risk of transformation to AML. 11 Therefore, the respective mutation status should be addressed before treatment decisions are made as well as at diagnosis as recommended in the new WHO 2016 classification. 1 Therefore, the aim of the present study was to determine the frequency of mutations in a large cohort of 123 patients with MDS and isolated del(5q) with a 27 gene panel and combine clinical data and prognostic information. Methods Patients cohort We investigated 123 patients (35 male, 88 female, ratio: 1:2.5) having MDS with isolated del(5q), strictly classified according to WHO classification 2008 and added guidelines according to 2016 with respect to cytomorphology and cytogenetics (blast counts below 5% in the bone marrow and below 1% in the peripheral blood and 5q deletion sole or one additional aberration that is not affecting chromosome 7). 1 All patients samples were sent from different hematological centers to the MLL leukemia laboratory for diagnostic purposes between 2005 and The median age was 75 years (range: years). 119 patients showed an isolated del(5q) while 4 cases appeared with only one additional cytogenetic aberration (two patients with del(13q), one with del(9q) and one with a trisomy 8). Follow-up data were available in 111/123 cases with a median follow-up of 41 months. 112 cases of the present cohort were also included in the study by Heuser et al. 15 Mutation pattern and prognostic impact of MDS with del(5q) were compared to a MDS cohort of 944 patients representing all MDS subtypes /123 patients diagnosed with MDS with isolated del(5q) were already included in this recent study, resulting in a reference cohort of 905 patients after excluding these 39 cases. This reference cohort contained following MDS subtypes: 41 RA, 81 RARS, 27 RARS-T, 194 RCMD, 183 RCMD-RS, 191 RAEB-1 and 188 RAEB-2, diagnosed following WHO The median age was 73 years (range: years), the 4
6 male to female ratio was 1.7. Follow-up data in the reference cohort were available in 869 cases with a median follow-up of 62 months. All patients gave their consent for genetic analyses and the use of laboratory results for research purposes. The study adhered to the tenets of the Declaration of Helsinki and was approved by the laboratory s institutional review board. Cytomorphology Cytomorphology of bone marrow and/or peripheral blood samples was performed in all cases after May-Grünwald Giemsa staining, cytochemistry with myeloperoxidase (MPO), nonspecific esterase (NSE) and iron staining (Fe). 17 Cytogenetics and FISH Chromosome preparations and banding analysis of bone marrow and/or peripheral blood samples were performed for all 123 cases as previously described according to standard methods. 18 For classification of abnormalities and karyotypes, the ISCN guidelines (2016) were used. 19 Next generation sequencing All patients were analyzed by a myeloid gene panel containing ASXL1, BCOR, BRAF, CSNK1A1, CBL, DNMT3A, ETV6, EZH2, FLT3-TKD, GATA1, GATA2, IDH1, IDH2, JAK2, KIT, NRAS, KRAS, MPL, NPM1, PHF6, RUNX1, SF3B1, SRSF2, TET2, TP53, U2AF1 and WT1. The library of 26 genes was generated with the ThunderStorm (RainDance Technologies, Billerica, MA) and CSNK1A1 with the Access Array System (Fluidigm, San Francisco, CA). Both libraries were sequenced and demultiplexed on a MiSeq instrument (Illumina, San Diego, CA) as described previously. 20 The FASTQ files were further processed using the Sequence Pilot software version Build 510 (JSI Medical Systems, Ettenheim, Germany) for alignment and variant calling. Analysis parameters were set according to manufacturer s default recommendation. Validity of the somatic mutations was checked against the publicly accessible COSMIC v69 database ( and functional interpretation was performed using SIFT 1.03 ( PolyPhen 2.0 ( and MutationTaster 1.0 algorithms ( 21 Additionally, TP53 variants were verified using the IARC repository. 22 Single-nucleotide polymorphisms (SNP) were annotated according to the NCBI dbsnp ( Build 137) database. The detection limit for small nuclear variants was 3% variant allele frequency. Variants (n=9), not yet described in any public data base, were excluded from statistical analyses. 5
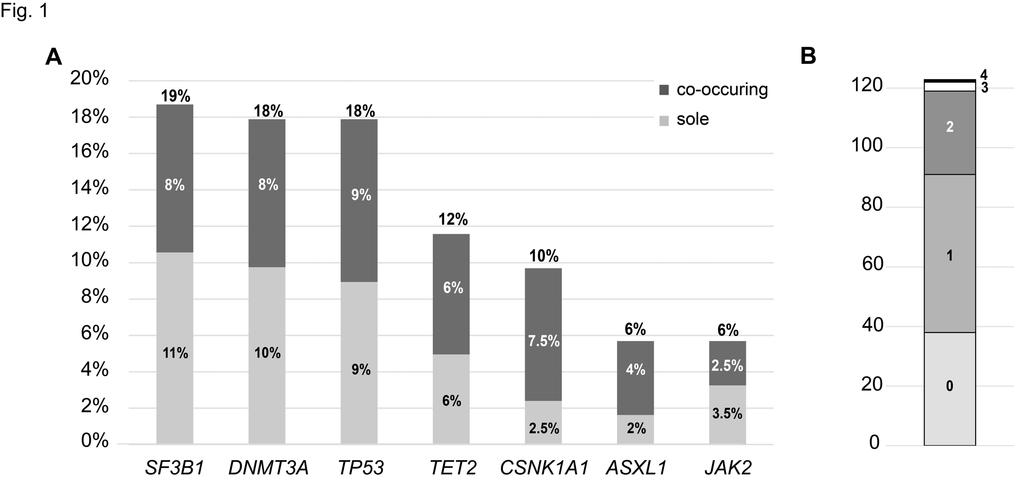
7 Statistical analysis Dichotomous variables were compared between different groups using the χ 2 -test and continuous variables by Student s T-test. Results were considered significant at p<0.05. Adjustment for multiple testing was not done. Statistical analyses were performed using SPSS version 19.0 (IBM Corporation, Armonk, NY); the reported p-values are two-sided. Survival curves were calculated for overall survival (OS) according to Kaplan-Meier and compared using the two-sided log rank test. OS was the time from diagnosis to death or last follow-up. Results Incidence of MDS with isolated del(5q) following the new WHO classification Following the recently revised 2016 version of the WHO classification for myeloid neoplasms one additional chromosomal aberration (other than aberration of chromosome 7) beside the deletion of the long arm of chromosome 5 still allows to make the diagnosis of MDS with isolated del(5q). 1 Therefore, we analyzed a well characterized MDS cohort for incidences of del(5q) and other diagnostic criteria leading to a diagnosis of MDS with isolated del(5q) /944 (9%) MDS patients carried a del(5q) either as sole abnormality or co-occurring with other lesions. 53/84 cases (63%) showed a sole del(5q), while only 5 cases (6%) appeared with one additional aberration and 26 (31%) showed a complex karyotype. 44/53 patients with isolated del(5q) fullfilled the diagnostic criteria of <1% blasts in the peripheral blood and <5% in the bone marrow. Furthermore, 4/5 cases with one additional lesion were also diagnosed as MDS with isolated del(5q), while the fifth case harbored a -7 as additional aberration. Therefore, 48 cases were diagnosed as MDS with isolated del(5q), whereof only 4/48 cases (8%) were grouped to these patients based on the new WHO classification, while the main group is still diagnosed by the criteria of the WHO 2008 classification. 1 Molecular genetic characterization of MDS with isolated del(5q) For a comprehensive molecular characterization we assembled a cohort of 123 patients diagnosed with MDS with isolated del(5q) and investigated 27 genes by mutation analyses. The most frequently mutated gene was SF3B1 (23/123; 19%), followed by DNMT3A (22/123; 18%), TP53 (22/123; 18%), TET2 (14/121; 12%), CSNK1A1 (12/123; 10%), ASXL1 and JAK2 (both 7/123; 6%) (Fig. 1A). All other analyzed genes showed mutation frequencies below 5%, with BRAF, ETV6, FLT3-TKD, GATA1, GATA2, IDH1, IDH2, NPM1, NRAS, PHF6 and WT1 showing no mutations at all. Nearly all mutations were heterozygous with median variant allele frequencies (VAF) for six of the most frequently mutated genes of 15 to 30% 6
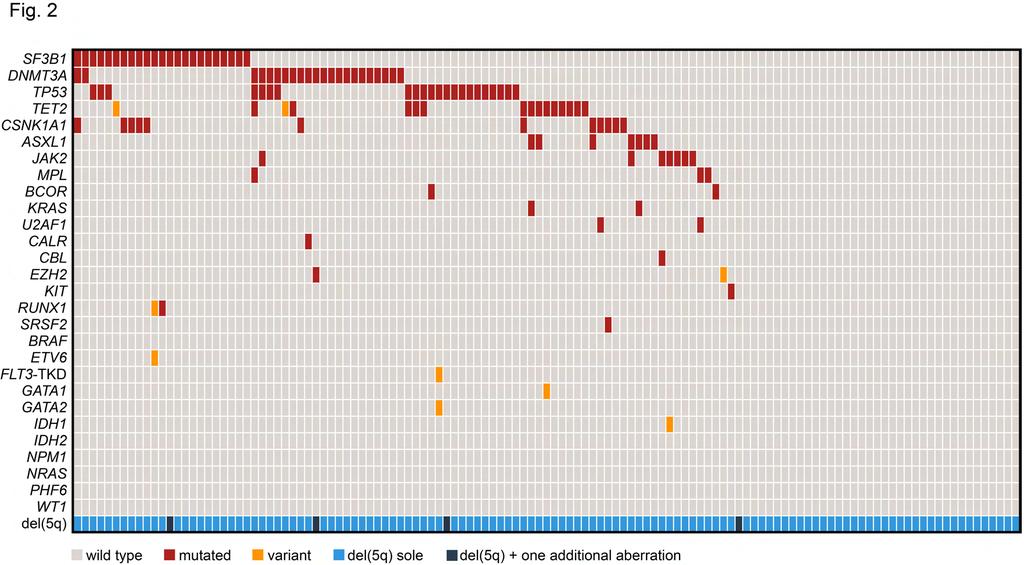
8 (range: 2 to 50% VAF). Solely CSNK1A1 showed VAF of 3-78%, mimicking a homozygous mutation status, caused by the location of CSNK1A1 on chromosome 5q in the commonly deleted region. Addressing the number of mutations per patient revealed a large number of patients with no mutation (38/123; 31%) or one mutation (53/123; 43%) in any of the 27 analyzed genes. 23% (28/123) of patients were mutated in two genes, while three and four mutations were detected in only 2% (3/123) and 1% (1/123) of patients, respectively (Fig. 1B). Looking at the co-occurrence of gene mutations resulted in a single association of CSNK1A1 and SF3B1 mutations. Only 16% of CSNK1A1 wild type cases showed a SF3B1 mutation (18/111), while 42% of CSNK1A1 mutated patients showed a co-occurring SF3B1 mutation (5/12; p=0.047). Although the most frequent gene mutations overlapped rarely and occurred frequently as sole mutations, they were not completely mutually exclusive (Fig. 1A and 2). Comparison of mutation frequencies in MDS with isolated del(5q) and other MDS subtypes For analyzing the differences in the mutation pattern of MDS with isolated del(5q) and all other MDS subtypes, we investigated the most frequently mutated genes in comparison to a reference cohort, represented by the previously published MDS cohort after excluding the respective diagnosed cases. 13 Comparing the mutation frequencies of the seven most frequently mutated genes in MDS with isolated del(5q) with all other MDS subtypes revealed that the respective six mutated genes were also ranked within the 15 most frequently mutated genes in all MDS subtypes (Fig. 3; CSNK1A1 was not addressed due to the missing data in the MDS reference cohort). Of note, TP53 mutations were significantly more often found in MDS with isolated del(5q) in comparison to all other MDS subtypes with a mutation frequency of 18% (22/123) compared to 6% in the MDS reference cohort (52/905; p<0.001). Clinical and morphological correlations Dividing the patients in groups defined by a bone marrow blast count of <2% and 2-5%, as described in the prognostic scoring system IPSS-R, we could not detect any correlation to the mutation number per patient. However, patients that had no mutation (n=38) were younger compared to patients with at least one mutation (n=85; 70 vs. 76 years, p=0.018). But there was no difference between these two patient groups in sex, white blood cell count, hemoglobin level or platelet count. Taking single gene mutations into account revealed that TP53 mutations correlated with higher age (78 vs. 73 years, p=0.038). All 22 patients with TP53 mutation were 67 years of age, with only 2 <70, but <80, 8 80 but <90, and even one patient in the group of 90 years of age. Addressing the correlation between percentages of ring sideroblasts (RS) and SF3B1 mutations showed that also in MDS with 7
9 isolated del(5q) these two parameters significantly correlate with a mean of 17% RS (range: 0-80%) in SF3B1 mutated patients and only 1% RS in SF3B1 wild type patients (wt; range: 0-12%, p=0.004). Furthermore, JAK2 mutations correlated with a platelet count > /µl (80% in JAK2 mutated vs. 12% in JAK2 wt, p=0.002). Prognostic impact of gene mutations Looking at prognostic relevance of gene mutations surprisingly showed that SF3B1 mutated patients (n=20 with follow-up data) had a significantly inferior outcome than SF3B1 wt patients (n=91; median overall survival (OS): 50 months vs. not reached, p=0.010; Fig. 4A). Furthermore, we analyzed the OS compared to the MDS reference cohort representing all other than isolated del(5q) MDS subtypes (n=869 with follow-up data). Overall the median OS was significantly favorable for patients with MDS with isolated del(5q) (62 months vs. not reached, p<0.001; Fig. 4B). To better characterize the not expected worse impact of SF3B1 mutations we analyzed both cohorts with respect to their SF3B1 mutation status as well as cytogenetics in terms of normal or aberrant karyotypes (Fig. 4C). SF3B1 mutations within a normal karyotype showed in MDS patients favorable outcomes (median OS: 93 months), however, this effect was reduced by an additional aberrant karyotype (median OS: 64 months). Therefore, SF3B1 mutated patients having aberrant karyotypes showed comparable outcomes (median OS: 50 vs. 64 months) irrespective of diagnoses with MDS with isolated del(5q) or any other subtype of MDS, while SF3B1 wt patients with isolated del(5q) had a favorable outcome compared to all other SF3B1 wt MDS patients (median OS: not reached vs. 49 months). However, we did not find a prognostic impact of TP53 mutations in our cohort (Supplemental figure 1; median OS was not reached in TP53 wt (n=92) and in TP53 mutated (n=19) patients; p=0.094). Molecular genetics during follow-up and progression to AML In 13 patients follow-up samples were available with a median time between two investigations of 22 months (range: 5-47 months, cases with less than 4 months between two investigations were excluded). In further 6/123 (5%) cases we could follow a progression to AML with a median transformation time to s-aml of 24 months (range: months). In these 19 cases with a follow-up sample mutation analyses were performed at follow-up, in 18/19 cases also cytogenetics was available. Overall, in 5/13 (38%) patients showing no transformation to AML no clonal evolution was detectable, neither in karyotype nor in mutation pattern, leaving 8/13 (62%) patients with clonal evolution. In 4/13 cases (31%) a change in cytogenetics occurred and in 7/13 patients (54%) additional gene mutations appeared, whereof in 3/13 patients clonal evolution occurred in both addressed instances. Looking at patients progressing to AML after MDS revealed a similar pattern with stability in 8
10 genetics with 3/5 cases (60%) showing no genetic evolution at all, 1/5 (20%) clonal evolution in cytogenetics and 2/6 (33%) change in the mutation pattern. Of note, none of the patients gained a mutation in TP53 or FLT3 during progression to AML. Addressing the gains of genetic lesions in the disease course showed no specific pattern. Cytogenetic gains included Y, del(11q), del(13q) and inv(3) and gained mutations affected ASXL1, BCOR, CSNK1A1, DNMT3A, IDH1, JAK2, RUNX1 and TET2. However, recurrent gains were limited to JAK2 (n=2) and RUNX1 (n=3), with two cases showing a gain of RUNX1 mutation progressing to AML and one progressing to MDS-RAEB-1. Furthermore, the variant allele frequencies of all gained mutations were <10% (median 4%, range: 3-7%), except of RUNX1 during transformation to AML, showing variant allele frequencies of 14 and 25%, respectively. An illustration of different types of clonal evolution is given in Figure 5. Discussion In the present study the molecular mutation pattern of a large cohort of 123 MDS patients with isolated del(5q) classified according to WHO classification 2008 and added guidelines according to 2016 was investigated. A great proportion of patients showed no or only one mutation in 27 analyzed genes, with only seven genes showing mutation frequencies >5% (SF3B1, DNMT3A, TP53, TET2, CSNK1A1, ASXL1, JAK2). Although in other studies more genes were investigated for mutation analyses, in overall MDS the median number of mutations is higher with three mutations per patient 13 or nearly half of the patients showing two or three mutations 14 in contrast to MDS with isolated del(5q). This indicates the specific and narrow spectrum of genetic lesion in this specific MDS subtype. However, the most frequently mutated genes were comparable to all other MDS subtypes investigated in a large MDS reference cohort. 13 The 15 most frequently mutated genes have also been identified by another large MDS study and by meta-analyses showing consistent data for the MDS mutation landscape. 14;23 Further, SF3B1 was frequently mutated and correlated with presence of ring sideroblasts going in line with previously published data in other MDS entities In contrast, TP53 was significantly more often mutated in MDS with isolated del(5q). In a number of studies mutations of TP53 were shown to occur in high-risk or therapy related MDS, MDS derived leukemia or within a complex karyotype Incidences of TP53 mutations in MDS with isolated del(5q) were found to be 5%, much lower than in other MDS subtypes. 12 However, in another previous study the incidence of TP53 mutations in low risk MDS with del(5q) was 18% investigated by back tracking TP53 mutated samples, already suggesting an previous under-estimation of TP53 subclonal mutations. 11 It was shown that 9
11 the TP53 mutation was already present at early stages of the disease and increased during disease course. 11 This is in line with the present data showing a TP53 mutation incidence of 18% with 7/22 cases having a variant allele frequency <10%. Surprisingly, SF3B1 mutations led to significantly worse OS, but showed finally a comparable outcome - still favorable - to all other MDS subtypes with SF3B1 mutation and an aberrant karyotype. Since a high frequency of MDS patients show a normal karyotype it was obvious to analyze the impact of karyotype information to SF3B1 mutation in overall MDS in our reference cohort. This demonstrated that also an accompanying altered karyotype reduces the favorable impact of SF3B1 mutation. Therefore, the highly favorable impact of SF3B1 mutation was limited to sole SF3B1 mutations without any additional lesion and might be an explanation why in MDS with isolated del(5q) the favorable impact is reduced and furthermore the overall good prognosis is not driven by SF3B1 mutations alone. However, this finding is in contrast to previous studies, showing that the prognostic effect of SF3B1 mutations is independent of variables that could coexist, like age, sex and cytogenetics. 24;26 In other studies, however, SF3B1 mutations did not keep independent prognostic significance in multivariate analyses or showed no prognostic impact at all, maybe indicating that MDS is representing a heterogeneous disease and should be rather analyzed in respective subgroups In MDS it was shown that transformation to s-aml is frequently accompanied by mutations in FLT3 and RAS genes and karyotype evolution In addition, RUNX1, GATA2 and CEBPA were identified by progression to s-aml, abrogating normal differentiation. 39 Furthermore, some genes have been identified to be affected by mutations as late events in MDS patients giving rise to a potential progression to AML, such as mutations in ASXL1, RUNX1, SRSF2, IDH2 or NRAS. 34;35;38 However, most of these genes were not identified to be affected in MDS with isolated del(5q) arguing for another progression mechanism than the one found in all other MDS patients. However, the recurrent gain of RUNX1 mutations in the disease course might indicate transformation to AML. In a comprehensive study of the mutation pattern in AML, some genes became obvious to be specific for s-aml, covering the spliceosomal genes as well as chromatin modifier. 38;39 The high incidence of SF3B1 mutations in MDS with isolated del(5q) would therefore reflect the MDS origin of the disease rather than the hint for disease progression. In previous studies mutations in TP53 and gain of cytogenetic aberrations were speculated to indicate disease progression and transformation to AML. 11;12 However, the clonal evolution was comparable in MDS with isolated del(5q) as described for overall MDS with a karyotype evolution in 34% and mutation pattern in 53% of MDS cases transforming to AML. 34 Even more, the clonal evolution appeared in the same manner in cases without progression to AML. Additionally, TP53 mutation were never gained during disease course, but the mutation burden increased (11% 10
12 to 75%) in the one case transforming to AML, while in follow-up cases without progression (n=2) the burden did not change. Therefore, one might suppose that in patients with clonal evolution clinical progress will be encountered, while the stable ones will stay stable also clinically. It was shown that clinical stability goes along with mutational stability, while developing new mutations resulted in AML progression in patients with MDS 5q- syndrome. 40 The previously published prognostic worse impact of TP53 mutations was not observed in the present cohort. Our patients were unselected and the median follow-up was 41 months. Thus, our cohort may include a larger proportion of patients earlier in their clinical course compared to cohorts enrolled in treatment studies. Therefore, the negative impact of TP53 mutations may become obvious in later stages of the disease course or even not before treatment needs to be started, that is not represented by the here presented collection of patients. Of note, 60% (61/101) of our patients were only under observation or received red blood cells or erythropoietin only. However, the presence of TP53 mutations already in early stages of the disease would therefore be in line with our data supported by the observed increase of clone size rather than the gain of TP53 mutation during disease course. 11 However, the case numbers were quite small for follow-up and need to be further proven in larger cohorts. In summary, MDS with isolated del(5q) show a very limited mutation spectrum of the recurrently mutated genes in comparison to all other MDS subtypes. However, the seven frequently mutated genes resemble the MDS mutation landscape with exception of TP53 mutations that are more often found in MDS with isolated del(5q). Therefore, progression to s-aml is rather driven by the prognostic worse impact of TP53 mutation in combination with del(5q) and potentially the gain of RUNX1 mutation than the otherwise identified accompanying mutations during MDS progression. The diagnostic and prognostic approach of MDS with isolated del(5q) should therefore include the mutation status of the seven most frequently mutated genes, including SF3B1 and TP53 and RUNX1 as potential progression marker, investigated with deep sequencing to catch all appearing mutations also subclonal ones with low variant allele frequencies. 11
13 Acknowledgment We thank all clinicians for sending samples to our laboratory for diagnostic purposes and for providing clinical information and follow-up data. In addition, we would like to thank all the coworkers at the MLL Munich Leukemia Laboratory for approaching together many aspects in the field of leukemia diagnostics and research. We also thank Karolína Perglerová for analyzing FLT3-ITD in the follow-up samples at MLL2 s.r.o., Prague, Czech Republic. Authorship contribution MM investigated molecular mutations, analyzed the data and wrote the manuscript. CH was responsible for cytogenetics. WK was involved in data analyses. TH was responsible for cytomorphologic analysis, was the principle investigator of the study. All authors read and contributed to the final version of the manuscript. Conflict of interest WK, CH, and TH declare part ownership of the MLL Munich Leukemia Laboratory. MM is employed by the MLL Munich Leukemia Laboratory. 12
14 References 1. Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia. Blood. 2016;127(20): Haase D, Germing U, Schanz J, et al. New insights into the prognostic impact of the karyotype in MDS and correlation with subtypes: evidence from a core dataset of 2124 patients. Blood. 2007;110(13): Bernasconi P, Klersy C, Boni M, et al. World Health Organization classification in combination with cytogenetic markers improves the prognostic stratification of patients with de novo primary myelodysplastic syndromes. Br J Haematol. 2007;137(3): Mallo M, Cervera J, Schanz J, et al. Impact of adjunct cytogenetic abnormalities for prognostic stratification in patients with myelodysplastic syndrome and deletion 5q. Leukemia. 2011;25(1): Germing U, Lauseker M, Hildebrandt B, et al. Survival, prognostic factors and rates of leukemic transformation in 381 untreated patients with MDS and del(5q): A multicenter study. Leukemia. 2012;26(6): Schanz J, Tuchler H, Sole F, et al. New Comprehensive Cytogenetic Scoring System for Primary Myelodysplastic Syndromes (MDS) and Oligoblastic Acute Myeloid Leukemia After MDS Derived From an International Database Merge. J Clin Oncol. 2012;30(8): Mallo M, del Rey M, Ibanez M, et al. Response to lenalidomide in myelodysplastic syndromes with del(5q): influence of cytogenetics and mutations. Br J Haematol. 2013;162(1): List AF, Dewald GW, Bennett J, et al. Lenalidomide in the myelodysplastic syndrome with chromosome 5q deletion. N Engl J Med. 2006;355(14): Giagounidis AA, Germing U, Haase S, et al. Clinical, morphological, cytogenetic, and prognostic features of patients with myelodysplastic syndromes and del(5q) including band q31. Leukemia. 2004;18(1): Side LE, Curtiss NP, Teel K, et al. RAS, FLT3, and TP53 mutations in therapy-related myeloid malignancies with abnormalities of chromosomes 5 and 7. Genes Chromosomes Cancer. 2004;39(3): Jadersten M, Saft L, Smith A, et al. TP53 mutations in low-risk myelodysplastic syndromes with del(5q) predict disease progression. J Clin Oncol. 2011;29(15): Fernandez-Mercado M, Burns A, Pellagatti A, et al. Targeted re-sequencing analysis of 25 genes commonly mutated in myeloid disorders in del(5q) myelodysplastic syndromes. Haematologica. 2013;98(12): Haferlach T, Nagata Y, Grossmann V, et al. Landscape of Genetic Lesions in 944 Patients with Myelodysplastic Syndromes. Leukemia. 2014;28(2): Papaemmanuil E, Gerstung M, Malcovati L, et al. Clinical and biological implications of driver mutations in myelodysplastic syndromes. Blood. 2013;122(22):
15 15. Heuser M, Meggendorfer M, Cruz MM, et al. Frequency and prognostic impact of casein kinase 1A1 mutations in MDS patients with deletion of chromosome 5q. Leukemia. 2015;29(9): Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, 4th ed. Lyon: International Agency for Research on Cancer (IARC), Löffler H, Rastetter J, Haferlach T. Atlas of Clinical Hematology, 6 ed. Heidelberg: Springer, Schoch C, Schnittger S, Bursch S, et al. Comparison of chromosome banding analysis, interphase- and hypermetaphase-fish, qualitative and quantitative PCR for diagnosis and for follow-up in chronic myeloid leukemia: a study on 350 cases. Leukemia. 2002;16(1): McGowan-Jordan J, Simons A, Schmid M. ISCN 2016: An International System for Human Cytogenomic Nomenclature. Basel, New York: Karger, Delic S, Rose D, Kern W, et al. Application of an NGS-based 28-gene panel in myeloproliferative neoplasms reveals distinct mutation patterns in essential thrombocythaemia, primary myelofibrosis and polycythaemia vera. Br J Haematol. 2016;175(3): Schwarz JM, Rodelsperger C, Schuelke M, Seelow D. MutationTaster evaluates disease-causing potential of sequence alterations. Nat Methods. 2010;7(8): Petitjean A, Mathe E, Kato S, et al. Impact of mutant p53 functional properties on TP53 mutation patterns and tumor phenotype: lessons from recent developments in the IARC TP53 database. Hum Mutat. 2007;28(6): Rose D, Kohlmann A, Nagata Y, et al. A robust molecular pattern for myelodysplastic syndromes in two independent cohorts investigated by next-generation sequencing can be revealed by comparative bioinformatic analyses. Br J Haematol. 2014;167(2): Papaemmanuil E, Cazzola M, Boultwood J, et al. Somatic SF3B1 mutation in myelodysplasia with ring sideroblasts. N Engl J Med. 2011;365(15): Yoshida K, Sanada M, Shiraishi Y, et al. Frequent pathway mutations of splicing machinery in myelodysplasia. Nature. 2011;478(7367): Malcovati L, Papaemmanuil E, Bowen DT, et al. Clinical significance of SF3B1 mutations in myelodysplastic syndromes and myelodysplastic/myeloproliferative neoplasms. Blood. 2011;118(24): Haferlach C, Dicker F, Herholz H, et al. Mutations of the TP53 gene in acute myeloid leukemia are strongly associated with a complex aberrant karyotype. Leukemia. 2008: Wong TN, Ramsingh G, Young AL, et al. Role of TP53 mutations in the origin and evolution of therapy-related acute myeloid leukaemia. Nature. 2015;518(7540): Bejar R, Stevenson K, Abdel-Wahab O, et al. Clinical effect of point mutations in myelodysplastic syndromes. N Engl J Med. 2011;364(26):
16 30. Patnaik MM, Lasho TL, Hodnefield JM, et al. SF3B1 mutations are prevalent in myelodysplastic syndromes with ring sideroblasts but do not hold independent prognostic value. Blood. 2012;119(2): Damm F, Thol F, Kosmider O, et al. SF3B1 mutations in myelodysplastic syndromes: clinical associations and prognostic implications. Leukemia. 2012;26(5): Thol F, Kade S, Schlarmann C, et al. Frequency and prognostic impact of mutations in SRSF2, U2AF1, and ZRSR2 in patients with myelodysplastic syndromes. Blood. 2012;119(15): Cazzola M, Rossi M, Malcovati L. Biologic and clinical significance of somatic mutations of SF3B1 in myeloid and lymphoid neoplasms. Blood. 2013;121(2): Meggendorfer M, de AA, Nadarajah N, et al. Karyotype evolution and acquisition of FLT3 or RAS pathway alterations drive progression of myelodysplastic syndrome to acute myeloid leukemia. Haematologica. 2015;100(12):e487-e Papaemmanuil E, Gerstung M, Bullinger L, et al. Genomic Classification and Prognosis in Acute Myeloid Leukemia. N Engl J Med. 2016;374(23): Takahashi K, Jabbour E, Wang X, et al. Dynamic acquisition of FLT3 or RAS alterations drive a subset of patients with lower risk MDS to secondary AML. Leukemia. 2013;27(10): Murphy DM, Bejar R, Stevenson K, et al. NRAS mutations with low allele burden have independent prognostic significance for patients with lower risk myelodysplastic syndromes. Leukemia. 2013;27(10): Sperling AS, Gibson CJ, Ebert BL. The genetics of myelodysplastic syndrome: from clonal haematopoiesis to secondary leukaemia. Nat Rev Cancer. 2017;17(1): Lindsley RC, Mar BG, Mazzola E, et al. Acute myeloid leukemia ontogeny is defined by distinct somatic mutations. Blood. 2015;125(9): Woll PS, Kjallquist U, Chowdhury O, et al. Myelodysplastic syndromes are propagated by rare and distinct human cancer stem cells in vivo. Cancer Cell. 2014;25(6):
17 Figure Legends Figure 1. Mutation frequencies and distributions. A) The frequencies of the seven most often mutated genes are given, as well as the appearance as sole abnormality. B) Illustration of the distribution of the number of mutations per patient. Figure 2. Molecular and cytogenetic characterization of patients with MDS with isolated del(5q). Illustration of all 123 samples, each column represents one patient. All 27 analyzed genes as well as occurrence of del(5q) as sole aberration or with one additional cytogenetic aberration are given for each patient. Light grey: wild type, red: mutated, orange: variant, light blue: del(5q) sole, dark blue: del(5q) and one additional lesion. Figure 3. Comparison of mutation frequencies between MDS with isolated del(5q) and all MDS subtypes. Mutation frequencies for MDS were taken from the previously published reference cohort. 13 The six most frequently mutated genes in MDS with isolated del(5q) are compared to the 14 most frequently mutated genes in the MDS reference cohort. CSNK1A1 and STAG2 (typed in grey) were not analyzed in the MDS reference cohort or MDS del(5q) cohort, respectively. Figure 4. Overall survival (OS) analyses. Case numbers, median OS and p-values are given. A) Prognostic impact of SF3B1 mutations in MDS with isolated del(5q). B) OS of MDS with isolated del(5q) in comparison to the MDS reference cohort. C) OS of SF3B1 mutation with additional cytogenetic aberrations in MDS with isolated del(5q) in comparison to the MDS reference cohort. Wt: wild type, n.r.: not reached, mo: months, NK: normal karyotype, AK: aberrant karyotype. Figure 5. The dynamic of variant allele frequency (VAF) and acquisition and loss of mutated genes as well as cytogenetic lesions at diagnosis and follow-up. VAF and clone size are indicated by height of the shapes. Cases evolving to s-aml are indicated by the red dashed time line, while follow-up without progression to s-aml is indicated by a black dashed time line. Disease course showing A) gain of gene mutations, B) loss of a gene mutation, C) cytogenetic evolution, and D) no significant chance in del(5q) clone size as well as gene mutation (VAF). In D) both cartoons represent three patients. For the third patient in the first row no cytogenetics was available at s-aml stage. 16
18
19

20
21

22
23 Supplement Molecular analysis of myelodysplastic syndrome with isolated del(5q) reveals a specific spectrum of molecular mutations with prognostic impact: a study on 123 patients and 27 genes M. Meggendorfer, C. Haferlach, W. Kern, T. Haferlach Supplemental Figure 1 Overall survival (OS) 100% 80% 60% 40% 20% 0% p=0.094 TP53 TP53 mut, n=18 median OS n.r. TP53 wt, n=93 median OS n.r years Supplemental figure 1. Overall survival (OS) analyses of TP53 mutation in MDS with isolated del(5q). Case numbers, median OS and p-value are given. Wt: wild type, mut: mutated, n.r.: not reached.
Supplemental Material. The new provisional WHO entity RUNX1 mutated AML shows specific genetics without prognostic influence of dysplasia
 Supplemental Material The new provisional WHO entity RUNX1 mutated AML shows specific genetics without prognostic influence of dysplasia Torsten Haferlach, 1 Anna Stengel, 1 Sandra Eckstein, 1 Karolína
Supplemental Material The new provisional WHO entity RUNX1 mutated AML shows specific genetics without prognostic influence of dysplasia Torsten Haferlach, 1 Anna Stengel, 1 Sandra Eckstein, 1 Karolína
Published Ahead of Print on April 14, 2016, as doi: /haematol Copyright 2016 Ferrata Storti Foundation.
 Published Ahead of Print on April 14, 2016, as doi:10.3324/haematol.2016.143214. Copyright 2016 Ferrata Storti Foundation. Immunohistochemical pattern of p53 is a measure of TP53 mutation burden and adverse
Published Ahead of Print on April 14, 2016, as doi:10.3324/haematol.2016.143214. Copyright 2016 Ferrata Storti Foundation. Immunohistochemical pattern of p53 is a measure of TP53 mutation burden and adverse
NOVEL APPROACHES IN THE CLASSIFICATION AND RISK ASSESSMENT OF PATIENTS WITH MYELODYSPLASTIC SYNDROMES-CLINICAL IMPLICATION
 ORIGINAL ARTICLES NOVEL APPROACHES IN THE CLASSIFICATION AND RISK ASSESSMENT OF PATIENTS WITH MYELODYSPLASTIC SYNDROMES-CLINICAL IMPLICATION Ilina Micheva 1, Rosen Rachev 1, Hinco Varbanov 1, Vladimir
ORIGINAL ARTICLES NOVEL APPROACHES IN THE CLASSIFICATION AND RISK ASSESSMENT OF PATIENTS WITH MYELODYSPLASTIC SYNDROMES-CLINICAL IMPLICATION Ilina Micheva 1, Rosen Rachev 1, Hinco Varbanov 1, Vladimir
Molecular profiling in confirming the diagnosis of early myelodysplastic syndrome
 Molecular profiling of early MDS Hematopathology - March 2016 Article Molecular profiling in confirming the diagnosis of early myelodysplastic syndrome Maya Thangavelu 1,*, Ryan Olson 2, Li Li 2, Wanlong
Molecular profiling of early MDS Hematopathology - March 2016 Article Molecular profiling in confirming the diagnosis of early myelodysplastic syndrome Maya Thangavelu 1,*, Ryan Olson 2, Li Li 2, Wanlong
Mutational Impact on Diagnostic and Prognostic Evaluation of MDS
 Mutational Impact on Diagnostic and Prognostic Evaluation of MDS Elsa Bernard, PhD Papaemmanuil Lab, Computational Oncology, MSKCC MDS Foundation ASH 2018 Symposium Disclosure Research funds provided by
Mutational Impact on Diagnostic and Prognostic Evaluation of MDS Elsa Bernard, PhD Papaemmanuil Lab, Computational Oncology, MSKCC MDS Foundation ASH 2018 Symposium Disclosure Research funds provided by
Changes to the 2016 WHO Classification for the Diagnosis of MDS
 Changes to the 2016 WHO Classification for the Diagnosis of MDS Welcome to Managing MDS. I am Dr. Ulrich Germing, and today, I will provide highlights from the 14th International Symposium on MDS in Valencia,
Changes to the 2016 WHO Classification for the Diagnosis of MDS Welcome to Managing MDS. I am Dr. Ulrich Germing, and today, I will provide highlights from the 14th International Symposium on MDS in Valencia,
Next Generation Sequencing in Haematological Malignancy: A European Perspective. Wolfgang Kern, Munich Leukemia Laboratory
 Next Generation Sequencing in Haematological Malignancy: A European Perspective Wolfgang Kern, Munich Leukemia Laboratory Diagnostic Methods Cytomorphology Cytogenetics Immunophenotype Histology FISH Molecular
Next Generation Sequencing in Haematological Malignancy: A European Perspective Wolfgang Kern, Munich Leukemia Laboratory Diagnostic Methods Cytomorphology Cytogenetics Immunophenotype Histology FISH Molecular
DISCLOSURE Luca Malcovati, MD. No financial relationships to disclose
 ICUS, CCUS and CHIP Luca Malcovati, MD Department of Molecular Medicine, University of Pavia Medical School, & Department of Hematology Oncology, IRCCS Policlinico S. Matteo Foundation, Pavia, Italy DISCLOSURE
ICUS, CCUS and CHIP Luca Malcovati, MD Department of Molecular Medicine, University of Pavia Medical School, & Department of Hematology Oncology, IRCCS Policlinico S. Matteo Foundation, Pavia, Italy DISCLOSURE
SUPPLEMENTARY INFORMATION
 Supplementary Information S1 Frequency of DNMT3A mutations in hematologic disorders and their associated clinical phenotypes. Disease Patient population Frequency (%) Associated Clinical Characteristics
Supplementary Information S1 Frequency of DNMT3A mutations in hematologic disorders and their associated clinical phenotypes. Disease Patient population Frequency (%) Associated Clinical Characteristics
Myelodysplastic syndromes
 Myelodysplastic syndromes Robert P Hasserjian Massachusetts General Hospital, Boston, MA Disclosure of Relevant Financial Relationships Dr. Hasserjian declares he has no conflict(s) of interest to disclose.
Myelodysplastic syndromes Robert P Hasserjian Massachusetts General Hospital, Boston, MA Disclosure of Relevant Financial Relationships Dr. Hasserjian declares he has no conflict(s) of interest to disclose.
Myelodysplastic syndrome is a highly heterogeneous hematopoietic
 SHORT COMMUNICATION Clinical Characteristics and Prognosis of 48 Patients with Mutations in Myelodysplastic Syndrome Yulu Tian #, Ruijuan Zhang #, Linhua Yang* Yang L. Clinical Characteristics and Prognosis
SHORT COMMUNICATION Clinical Characteristics and Prognosis of 48 Patients with Mutations in Myelodysplastic Syndrome Yulu Tian #, Ruijuan Zhang #, Linhua Yang* Yang L. Clinical Characteristics and Prognosis
Myelodysplastic syndromes and the new WHO 2016 classification
 Myelodysplastic syndromes and the new WHO 2016 classification 32nd General Annual Meeting of the Belgian Hematology Society 10-11 February 2017 Gregor Verhoef, Departement of Hematology, University Hospital
Myelodysplastic syndromes and the new WHO 2016 classification 32nd General Annual Meeting of the Belgian Hematology Society 10-11 February 2017 Gregor Verhoef, Departement of Hematology, University Hospital
Editorial Process: Submission:11/21/2017 Acceptance:06/19/2018
 DOI:10.22034/APJCP.2018.19.7.1825 RESEARCH ARTICLE Editorial Process: Submission:11/21/2017 Acceptance:06/19/2018 The Frequency of SF3B1 Mutations in Thai Patients with Myelodysplastic Syndrome Punchita
DOI:10.22034/APJCP.2018.19.7.1825 RESEARCH ARTICLE Editorial Process: Submission:11/21/2017 Acceptance:06/19/2018 The Frequency of SF3B1 Mutations in Thai Patients with Myelodysplastic Syndrome Punchita
Chronic Myelomonocytic Leukemia with molecular abnormalities SH
 Chronic Myelomonocytic Leukemia with molecular abnormalities SH2017-0351 Madhu P. Menon MD,PhD, Juan Gomez MD, Kedar V. Inamdar MD,PhD and Kristin Karner MD Madhu P Menon, MD, PhD Henry Ford Hospital Patient
Chronic Myelomonocytic Leukemia with molecular abnormalities SH2017-0351 Madhu P. Menon MD,PhD, Juan Gomez MD, Kedar V. Inamdar MD,PhD and Kristin Karner MD Madhu P Menon, MD, PhD Henry Ford Hospital Patient
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed
 MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
Examining Genetics and Genomics of Acute Myeloid Leukemia in 2017
 Examining Genetics and Genomics of Acute Myeloid Leukemia in 2017 Elli Papaemmanuil, PhD Memorial Sloan Kettering Cancer Center New York, New York, United States Today s Talk Cancer genome introduction
Examining Genetics and Genomics of Acute Myeloid Leukemia in 2017 Elli Papaemmanuil, PhD Memorial Sloan Kettering Cancer Center New York, New York, United States Today s Talk Cancer genome introduction
Management of Myelodysplastic Syndromes
 Management of Myelodysplastic Syndromes Peter L. Greenberg, MD Stanford Cancer Institute Myelodysplastic Syndromes: Clinical & Molecular Advances for Disease Classification and Prognostication MDSs: A
Management of Myelodysplastic Syndromes Peter L. Greenberg, MD Stanford Cancer Institute Myelodysplastic Syndromes: Clinical & Molecular Advances for Disease Classification and Prognostication MDSs: A
Concomitant WT1 mutations predicted poor prognosis in CEBPA double-mutated acute myeloid leukemia
 Concomitant WT1 mutations predicted poor prognosis in CEBPA double-mutated acute myeloid leukemia Feng-Ming Tien, Hsin-An Hou, Jih-Luh Tang, Yuan-Yeh Kuo, Chien-Yuan Chen, Cheng-Hong Tsai, Ming Yao, Chi-Cheng
Concomitant WT1 mutations predicted poor prognosis in CEBPA double-mutated acute myeloid leukemia Feng-Ming Tien, Hsin-An Hou, Jih-Luh Tang, Yuan-Yeh Kuo, Chien-Yuan Chen, Cheng-Hong Tsai, Ming Yao, Chi-Cheng
New treatment strategies in myelodysplastic syndromes and acute myeloid leukemia van der Helm, Lidia Henrieke
 University of Groningen New treatment strategies in myelodysplastic syndromes and acute myeloid leukemia van der Helm, Lidia Henrieke IMPORTANT NOTE: You are advised to consult the publisher's version
University of Groningen New treatment strategies in myelodysplastic syndromes and acute myeloid leukemia van der Helm, Lidia Henrieke IMPORTANT NOTE: You are advised to consult the publisher's version
Acute Myeloid Leukemia with RUNX1 and Several Co-mutations
 Case SH2017-0281 Acute Myeloid Leukemia with RUNX1 and Several Co-mutations James Bauer, MD, PhD David Yang, MD Erik Ranheim, MD, PhD Catherine Leith, MB, Bchir Clinical History Chief Complaint: 72 year
Case SH2017-0281 Acute Myeloid Leukemia with RUNX1 and Several Co-mutations James Bauer, MD, PhD David Yang, MD Erik Ranheim, MD, PhD Catherine Leith, MB, Bchir Clinical History Chief Complaint: 72 year
APPROACH TO MYELODYSPLASTIC SYNDROMES IN THE ERA OF PRECISION MEDICINE
 APPROACH TO MYELODYSPLASTIC SYNDROMES IN THE ERA OF PRECISION MEDICINE Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics Department of Hematopathology The University
APPROACH TO MYELODYSPLASTIC SYNDROMES IN THE ERA OF PRECISION MEDICINE Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics Department of Hematopathology The University
ACCME/Disclosures. History. Hematopathology Specialty Conference Case #4 4/13/2016
 Hematopathology Specialty Conference Case #4 Sherrie L. Perkins MD, PhD University of Utah ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose
Hematopathology Specialty Conference Case #4 Sherrie L. Perkins MD, PhD University of Utah ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose
Myelodysplastic syndromes Impact of Biology. Lionel Adès Hopital Saint Louis Groupe Francophone des SMD. Épidémiologie
 Myelodysplastic syndromes Impact of Biology Lionel Adès Hopital Saint Louis Groupe Francophone des SMD Épidémiologie Incidence : 3 à 6 / 100 000 hab. / An Prédomine chez les sujets âgés Augmentation de
Myelodysplastic syndromes Impact of Biology Lionel Adès Hopital Saint Louis Groupe Francophone des SMD Épidémiologie Incidence : 3 à 6 / 100 000 hab. / An Prédomine chez les sujets âgés Augmentation de
Acute leukemia and myelodysplastic syndromes
 11/01/2012 Post-ASH meeting 1 Acute leukemia and myelodysplastic syndromes Peter Vandenberghe Centrum Menselijke Erfelijkheid & Afdeling Hematologie, UZ Leuven 11/01/2012 Post-ASH meeting 2 1. Acute myeloid
11/01/2012 Post-ASH meeting 1 Acute leukemia and myelodysplastic syndromes Peter Vandenberghe Centrum Menselijke Erfelijkheid & Afdeling Hematologie, UZ Leuven 11/01/2012 Post-ASH meeting 2 1. Acute myeloid
SESSION 1 Reactive cytopenia and dysplasia
 SESSION 1 Reactive cytopenia and dysplasia Falko Fend, Tübingen & Alexandar Tzankov, Basel 1 Disclosure of speaker s interests (Potential) conflict of interest none Potentially relevant company relationships
SESSION 1 Reactive cytopenia and dysplasia Falko Fend, Tübingen & Alexandar Tzankov, Basel 1 Disclosure of speaker s interests (Potential) conflict of interest none Potentially relevant company relationships
Laboratory Service Report
 Specimen Type Peripheral blood CR PDF Report available at: https://test.mmlaccess.com/reports/c7028846-ih2xuglwpq.ashx Indication for Test DS CR Pathogenic utations Detected CR 1. JAK2: c.1849g>t;p.val617phe
Specimen Type Peripheral blood CR PDF Report available at: https://test.mmlaccess.com/reports/c7028846-ih2xuglwpq.ashx Indication for Test DS CR Pathogenic utations Detected CR 1. JAK2: c.1849g>t;p.val617phe
Better Prognosis for Patients With Del(7q) Than for Patients With Monosomy 7 in Myelodysplastic Syndrome
 Than for Patients With Monosomy 7 in Myelodysplastic Syndrome") Better Prognosis for Patients With Del(7q) Than for Patients With Monosomy 7 in Myelodysplastic Syndrome Iris Cordoba, MD 1 ; José R. González-Porras, MD 1 ; Benet Nomdedeu, MD 2 ; Elisa Luño, MD 3 ; Raquel
Better Prognosis for Patients With Del(7q) Than for Patients With Monosomy 7 in Myelodysplastic Syndrome Iris Cordoba, MD 1 ; José R. González-Porras, MD 1 ; Benet Nomdedeu, MD 2 ; Elisa Luño, MD 3 ; Raquel
Corporate Medical Policy. Policy Effective February 23, 2018
 Corporate Medical Policy Genetic Testing for FLT3, NPM1 and CEBPA Mutations in Acute File Name: Origination: Last CAP Review: Next CAP Review: Last Review: genetic_testing_for_flt3_npm1_and_cebpa_mutations_in_acute_myeloid_leukemia
Corporate Medical Policy Genetic Testing for FLT3, NPM1 and CEBPA Mutations in Acute File Name: Origination: Last CAP Review: Next CAP Review: Last Review: genetic_testing_for_flt3_npm1_and_cebpa_mutations_in_acute_myeloid_leukemia
Treatment of low risk MDS
 Treatment of low risk MDS Matteo G Della Porta Cancer Center IRCCS Humanitas Research Hospital & Humanitas University Rozzano Milano, Italy matteo.della_porta@hunimed.eu International Prognostic Scoring
Treatment of low risk MDS Matteo G Della Porta Cancer Center IRCCS Humanitas Research Hospital & Humanitas University Rozzano Milano, Italy matteo.della_porta@hunimed.eu International Prognostic Scoring
Myelodysplastic syndromes: revised WHO classification and distinction from non-neoplastic conditions
 Myelodysplastic syndromes: revised WHO classification and distinction from non-neoplastic conditions Robert P Hasserjian, MD Associate Professor Massachusetts General Hospital and Harvard Medical School
Myelodysplastic syndromes: revised WHO classification and distinction from non-neoplastic conditions Robert P Hasserjian, MD Associate Professor Massachusetts General Hospital and Harvard Medical School
Novità nelle MDS. Matteo G Della Porta. Cancer Center IRCCS Humanitas Research Hospital & Humanitas University Rozzano Milano, Italy
 Novità nelle MDS Matteo G Della Porta Cancer Center IRCCS Humanitas Research Hospital & Humanitas University Rozzano Milano, Italy matteo.della_porta@hunimed.eu Outline ARCH Predictive value of somatic
Novità nelle MDS Matteo G Della Porta Cancer Center IRCCS Humanitas Research Hospital & Humanitas University Rozzano Milano, Italy matteo.della_porta@hunimed.eu Outline ARCH Predictive value of somatic
Laboratory Service Report
 Client C7028846-DLP Rochester Rochester, N 55901 Specimen Type Peripheral blood CR PDF Report available at: https://test.mmlaccess.com/reports/c7028846-zwselwql7p.ashx Indication for Test DS CR Pathogenic
Client C7028846-DLP Rochester Rochester, N 55901 Specimen Type Peripheral blood CR PDF Report available at: https://test.mmlaccess.com/reports/c7028846-zwselwql7p.ashx Indication for Test DS CR Pathogenic
Please Silence Your Cell Phones. Thank You
 Please Silence Your Cell Phones Thank You Utility of NGS and Comprehensive Genomic Profiling in Hematopathology Practice Maria E. Arcila M.D. Memorial Sloan Kettering Cancer Center New York, NY Disclosure
Please Silence Your Cell Phones Thank You Utility of NGS and Comprehensive Genomic Profiling in Hematopathology Practice Maria E. Arcila M.D. Memorial Sloan Kettering Cancer Center New York, NY Disclosure
Introduction of an NGS gene panel into the Haemato-Oncology MPN service
 Introduction of an NGS gene panel into the Haemato-Oncology MPN service Dr. Anna Skowronska, Dr Jane Bryon, Dr Samuel Clokie, Dr Yvonne Wallis and Professor Mike Griffiths West Midlands Regional Genetics
Introduction of an NGS gene panel into the Haemato-Oncology MPN service Dr. Anna Skowronska, Dr Jane Bryon, Dr Samuel Clokie, Dr Yvonne Wallis and Professor Mike Griffiths West Midlands Regional Genetics
Clonal Cytopenia and Myeloid Neoplasms
 Clonal Cytopenia and Myeloid Neoplasms Luca Malcovati, MD Department of Molecular Medicine, University of Pavia Medical School, & Department of Hematology Oncology, IRCCS Policlinico S. Matteo Foundation,
Clonal Cytopenia and Myeloid Neoplasms Luca Malcovati, MD Department of Molecular Medicine, University of Pavia Medical School, & Department of Hematology Oncology, IRCCS Policlinico S. Matteo Foundation,
BHS Annual Meeting
 BHS Annual Meeting 2014 01.02.2014 Implementing next-generation deepsequencing assays in diagnostic algorithms in hematological malignancies Dr. Alexander Kohlmann Medical Need for Molecular Characterization
BHS Annual Meeting 2014 01.02.2014 Implementing next-generation deepsequencing assays in diagnostic algorithms in hematological malignancies Dr. Alexander Kohlmann Medical Need for Molecular Characterization
Illumina Trusight Myeloid Panel validation A R FHAN R A FIQ
 Illumina Trusight Myeloid Panel validation A R FHAN R A FIQ G E NETIC T E CHNOLOGIST MEDICAL G E NETICS, CARDIFF To Cover Background to the project Choice of panel Validation process Genes on panel, Protocol
Illumina Trusight Myeloid Panel validation A R FHAN R A FIQ G E NETIC T E CHNOLOGIST MEDICAL G E NETICS, CARDIFF To Cover Background to the project Choice of panel Validation process Genes on panel, Protocol
Juan Ma 1, Jennifer Dunlap 2, Lisong Shen 1, Guang Fan 2 1
 Juan Ma 1, Jennifer Dunlap 2, Lisong Shen 1, Guang Fan 2 1 Xin Hua Hospital, Shanghai, China 2 Oregon Health & Science University, Portland, OR, United States AML is a hematopoietic neoplasms characterized
Juan Ma 1, Jennifer Dunlap 2, Lisong Shen 1, Guang Fan 2 1 Xin Hua Hospital, Shanghai, China 2 Oregon Health & Science University, Portland, OR, United States AML is a hematopoietic neoplasms characterized
Blast transformation in chronic myelomonocytic leukemia: Risk factors, genetic features, survival, and treatment outcome
 RESEARCH ARTICLE Blast transformation in chronic myelomonocytic leukemia: Risk factors, genetic features, survival, and treatment outcome AJH Mrinal M. Patnaik, 1 Emnet A. Wassie, 1 Terra L. Lasho, 2 Curtis
RESEARCH ARTICLE Blast transformation in chronic myelomonocytic leukemia: Risk factors, genetic features, survival, and treatment outcome AJH Mrinal M. Patnaik, 1 Emnet A. Wassie, 1 Terra L. Lasho, 2 Curtis
Supplementary Appendix
 Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Patel JP, Gönen M, Figueroa ME, et al. Prognostic relevance
Supplementary Appendix This appendix has been provided by the authors to give readers additional information about their work. Supplement to: Patel JP, Gönen M, Figueroa ME, et al. Prognostic relevance
Myelodysplastic Syndromes. Post-ASH meeting 2014 Marie-Christiane Vekemans
 Myelodysplastic Syndromes Post-ASH meeting 2014 Marie-Christiane Vekemans Agenda New biological developments Risk assessment and prognostic factors New therapeutic options Agenda New biological developments
Myelodysplastic Syndromes Post-ASH meeting 2014 Marie-Christiane Vekemans Agenda New biological developments Risk assessment and prognostic factors New therapeutic options Agenda New biological developments
IV Simposio International Sao Paulo Nov Hematologic malignant diseases molecular information, present and future
 IV Simposio International Sao Paulo Nov 7 2012 Hematologic malignant diseases molecular information, present and future Dr. rer. nat. Alexander Kohlmann, MLL Munich Leukemia Laboratory Spectrum of Methods
IV Simposio International Sao Paulo Nov 7 2012 Hematologic malignant diseases molecular information, present and future Dr. rer. nat. Alexander Kohlmann, MLL Munich Leukemia Laboratory Spectrum of Methods
Response to azacitidine is independent of p53 expression in higher-risk myelodysplastic syndromes and secondary acute myeloid leukemia
 Published Ahead of Print on June 27, 2014, as doi:10.3324/haematol.2014.104760. Copyright 2014 Ferrata Storti Foundation. Response to azacitidine is independent of p53 expression in higher-risk myelodysplastic
Published Ahead of Print on June 27, 2014, as doi:10.3324/haematol.2014.104760. Copyright 2014 Ferrata Storti Foundation. Response to azacitidine is independent of p53 expression in higher-risk myelodysplastic
Table 1: biological tests in SMD
 Table 1: biological tests in SMD Tests Mandatory Recommended Under validation Morphology Marrow aspirate Marrow biopsy 1 Iron staining Quantification of dysplasia WHO 2008 Classification Cytogenetics Conventional
Table 1: biological tests in SMD Tests Mandatory Recommended Under validation Morphology Marrow aspirate Marrow biopsy 1 Iron staining Quantification of dysplasia WHO 2008 Classification Cytogenetics Conventional
Impact of Biomarkers in the Management of Patients with Acute Myeloid Leukemia
 Impact of Biomarkers in the Management of Patients with Acute Myeloid Leukemia Hartmut Döhner Medical Director, Department of Internal Medicine III Director, Comprehensive Cancer Center Ulm Ulm University,
Impact of Biomarkers in the Management of Patients with Acute Myeloid Leukemia Hartmut Döhner Medical Director, Department of Internal Medicine III Director, Comprehensive Cancer Center Ulm Ulm University,
When Cancer Looks Like Something Else: How Does Mutational Profiling Inform the Diagnosis of Myelodysplasia?
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Etiology. Definition MYELODYSPLASTIC SYNDROMES. De novo. Secondary MDS (10 years earlier than primary) transformation
 transformation") MYELODYSPLASTIC SYNDROMES Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics The University of Texas M.D. Anderson Cancer Center Houston, Texas No relevant COIs to
MYELODYSPLASTIC SYNDROMES Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics The University of Texas M.D. Anderson Cancer Center Houston, Texas No relevant COIs to
Molecular Genetic Testing to Predict Response to Therapy in MDS
 Molecular Genetic Testing to Predict Response to Therapy in MDS Rafael Bejar MD, PhD Bone Marrow Failure Disease Scientific Symposium Rockville, MD March 18 th, 2016 Overview Response Criteria Lenalidomide
Molecular Genetic Testing to Predict Response to Therapy in MDS Rafael Bejar MD, PhD Bone Marrow Failure Disease Scientific Symposium Rockville, MD March 18 th, 2016 Overview Response Criteria Lenalidomide
Next generation sequencing analysis - A UK perspective. Nicholas Lea
 Next generation sequencing analysis - A UK perspective Nicholas Lea King s HMDC LMH is part of an integrated pathology service at King s Haematological Malignancy Diagnostic Centre (HMDC) HMDC serves population
Next generation sequencing analysis - A UK perspective Nicholas Lea King s HMDC LMH is part of an integrated pathology service at King s Haematological Malignancy Diagnostic Centre (HMDC) HMDC serves population
New drugs in Acute Leukemia. Cristina Papayannidis, MD, PhD University of Bologna
 New drugs in Acute Leukemia Cristina Papayannidis, MD, PhD University of Bologna Challenges to targeted therapy in AML Multiple subtypes based upon mutations/cytogenetic aberrations No known uniform genomic
New drugs in Acute Leukemia Cristina Papayannidis, MD, PhD University of Bologna Challenges to targeted therapy in AML Multiple subtypes based upon mutations/cytogenetic aberrations No known uniform genomic
Emerging Treatment Options for Myelodysplastic Syndromes
 Emerging Treatment Options for Myelodysplastic Syndromes James K. Mangan, MD, PhD Assistant Professor of Clinical Medicine Abramson Cancer Center, University of Pennsylvania Please note that some of the
Emerging Treatment Options for Myelodysplastic Syndromes James K. Mangan, MD, PhD Assistant Professor of Clinical Medicine Abramson Cancer Center, University of Pennsylvania Please note that some of the
HEMATOLOGIC MALIGNANCIES BIOLOGY
 HEMATOLOGIC MALIGNANCIES BIOLOGY Failure of terminal differentiation Failure of differentiated cells to undergo apoptosis Failure to control growth Neoplastic stem cell FAILURE OF TERMINAL DIFFERENTIATION
HEMATOLOGIC MALIGNANCIES BIOLOGY Failure of terminal differentiation Failure of differentiated cells to undergo apoptosis Failure to control growth Neoplastic stem cell FAILURE OF TERMINAL DIFFERENTIATION
A prospective, multicenter European Registry for newly diagnosed patients with Myelodysplastic Syndromes of IPSS low and intermediate-1 subtypes.
 Protocol Synopsis Study Title A prospective, multicenter European Registry for newly diagnosed patients with Myelodysplastic Syndromes of IPSS low and intermediate-1 subtypes. Short Title European MDS
Protocol Synopsis Study Title A prospective, multicenter European Registry for newly diagnosed patients with Myelodysplastic Syndromes of IPSS low and intermediate-1 subtypes. Short Title European MDS
Prognostic models in myelodysplastic syndromes
 MYELODYSPLASTIC SYNDROMES:WHAT MAKES THERAPY EFFECTIVE? Prognostic models in myelodysplastic syndromes Rafael Bejar 1 1 Moores Cancer Center, Division of Hematology and Oncology, University of California,
MYELODYSPLASTIC SYNDROMES:WHAT MAKES THERAPY EFFECTIVE? Prognostic models in myelodysplastic syndromes Rafael Bejar 1 1 Moores Cancer Center, Division of Hematology and Oncology, University of California,
WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities
 WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities Robert W. McKenna, M.D. 1/2009 WHO Classification of Myeloid Neoplasms (4th Edition)--2008 Incorporates new information that
WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities Robert W. McKenna, M.D. 1/2009 WHO Classification of Myeloid Neoplasms (4th Edition)--2008 Incorporates new information that
WHO Update to Myeloproliferative Neoplasms
 WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
TET2 mutations were predictive of inferior prognosis in the presence of ASXL1 mutations in patients with chronic myelomonocytic leukemia
 Short Report TET2 mutations were predictive of inferior prognosis in the presence of ASXL1 mutations in patients with chronic myelomonocytic leukemia Yajuan Cui 1,2 *, Hongyan Tong 3 *, Xin Du 4 *, Bing
Short Report TET2 mutations were predictive of inferior prognosis in the presence of ASXL1 mutations in patients with chronic myelomonocytic leukemia Yajuan Cui 1,2 *, Hongyan Tong 3 *, Xin Du 4 *, Bing
Molecular Advances in Hematopathology
 Molecular Advances in Hematopathology HOW MOLECULAR METHODS HAVE CHANGED MY PRACTICE Objectives Understand the importance of cytogenetic/molecular studies in hematolymphoid diseases Know some of the important
Molecular Advances in Hematopathology HOW MOLECULAR METHODS HAVE CHANGED MY PRACTICE Objectives Understand the importance of cytogenetic/molecular studies in hematolymphoid diseases Know some of the important
Myelodysplastic syndromes post ASH Dominik Selleslag AZ Sint-Jan Brugge
 Myelodysplastic syndromes post ASH 2016 Dominik Selleslag AZ Sint-Jan Brugge Why did they put MDS at the end of the meeting? Possible explanations Least fascinating disease without progress? Poor speaker?
Myelodysplastic syndromes post ASH 2016 Dominik Selleslag AZ Sint-Jan Brugge Why did they put MDS at the end of the meeting? Possible explanations Least fascinating disease without progress? Poor speaker?
Reporting cytogenetics Can it make sense? Daniel Weisdorf MD University of Minnesota
 Reporting cytogenetics Can it make sense? Daniel Weisdorf MD University of Minnesota Reporting cytogenetics What is it? Terminology Clinical value What details are important Diagnostic Tools for Leukemia
Reporting cytogenetics Can it make sense? Daniel Weisdorf MD University of Minnesota Reporting cytogenetics What is it? Terminology Clinical value What details are important Diagnostic Tools for Leukemia
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls
 Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
June 11, Ella Noel, D.O., FACOI 1717 West Broadway Madison, WI
 June 11, 2018 Ella Noel, D.O., FACOI 1717 West Broadway Madison, WI 53713 policycomments@wpsic.com RE: Draft Local Coverage Determination: MolDX: MDS FISH (DL37772) Dear Dr. Noel Thank you for the opportunity
June 11, 2018 Ella Noel, D.O., FACOI 1717 West Broadway Madison, WI 53713 policycomments@wpsic.com RE: Draft Local Coverage Determination: MolDX: MDS FISH (DL37772) Dear Dr. Noel Thank you for the opportunity
Precision Medicine and Molecular Testing.
 Precision Medicine and Molecular Testing. David A. Sallman, MD Assistant Member Department of Malignant Hematology Moffitt Cancer Center david.sallman@moffitt.org Disclosures Research funding for Celgene
Precision Medicine and Molecular Testing. David A. Sallman, MD Assistant Member Department of Malignant Hematology Moffitt Cancer Center david.sallman@moffitt.org Disclosures Research funding for Celgene
Myelodysplastic syndromes in adults aged less than 50 years: Incidence and clinicopathological data
 JBUON 2014; 19(4): 999-1005 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Myelodysplastic syndromes in adults aged less than 50 years: Incidence
JBUON 2014; 19(4): 999-1005 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Myelodysplastic syndromes in adults aged less than 50 years: Incidence
Kevin Kelly, MD, Phd Acute Myeloid and Lymphoid Leukemias
 Kevin Kelly, MD, Phd Acute Myeloid and Lymphoid Leukemias Relevant financial relationships in the past twelve months by presenter or spouse/partner. Speakers bureau: Novartis, Janssen, Gilead, Bayer The
Kevin Kelly, MD, Phd Acute Myeloid and Lymphoid Leukemias Relevant financial relationships in the past twelve months by presenter or spouse/partner. Speakers bureau: Novartis, Janssen, Gilead, Bayer The
ASBMT MDS/MPN Update Sunil Abhyankar, MD
 ASBMT MDS/MPN Update Sunil Abhyankar, MD Professor of Medicine Medical Director, Pheresis and Cell Processing Division of Hematologic Malignancies and Cellular Therapeutics Department of Internal Medicine
ASBMT MDS/MPN Update Sunil Abhyankar, MD Professor of Medicine Medical Director, Pheresis and Cell Processing Division of Hematologic Malignancies and Cellular Therapeutics Department of Internal Medicine
Available online at
 Annals of Clinical & Laboratory Science, vol. 45, no. 5, 2015 Available online at www.annclinlabsci.org Bioinformatics Analysis to Determine Prognostic Mutations of 72 de novo Acute Myeloid Leukemia Cases
Annals of Clinical & Laboratory Science, vol. 45, no. 5, 2015 Available online at www.annclinlabsci.org Bioinformatics Analysis to Determine Prognostic Mutations of 72 de novo Acute Myeloid Leukemia Cases
MDS 101. What is bone marrow? Myelodysplastic Syndrome: Let s build a definition. Dysplastic? Syndrome? 5/22/2014. What does bone marrow do?
 101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
Update on the WHO Classification of Acute Myeloid Leukemia. Kaaren K. Reichard, MD Mayo Clinic Rochester
 Update on the WHO Classification of Acute Myeloid Leukemia Kaaren K. Reichard, MD Mayo Clinic Rochester reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Objectives Present a practical
Update on the WHO Classification of Acute Myeloid Leukemia Kaaren K. Reichard, MD Mayo Clinic Rochester reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Objectives Present a practical
Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms. Kaaren Reichard Mayo Clinic Rochester
 Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms Kaaren Reichard Mayo Clinic Rochester Reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Present
Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms Kaaren Reichard Mayo Clinic Rochester Reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Present
Molecular Pathology Evaluation Panel and Molecular Pathology Consortium Advice Note
 Molecular Pathology Evaluation Panel and Molecular Pathology Consortium Advice Note MPEP/MPC Advice Note 2016-02 June 2016 Test evaluated: Tumour Protein p53 (TP53) Molecular Pathology Evaluation Panel
Molecular Pathology Evaluation Panel and Molecular Pathology Consortium Advice Note MPEP/MPC Advice Note 2016-02 June 2016 Test evaluated: Tumour Protein p53 (TP53) Molecular Pathology Evaluation Panel
Partial tandem duplication of KMT2A (MLL) may predict a subset of myelodysplastic syndrome with unique characteristics and poor outcome
 may predict a subset of myelodysplastic syndrome with unique characteristics and poor outcome") Published Ahead of Print on January 19, 2018, as doi:10.3324/haematol.2017.185249. Copyright 2018 Ferrata Storti Foundation. Partial tandem duplication of KMT2A (MLL) may predict a subset of myelodysplastic
Published Ahead of Print on January 19, 2018, as doi:10.3324/haematol.2017.185249. Copyright 2018 Ferrata Storti Foundation. Partial tandem duplication of KMT2A (MLL) may predict a subset of myelodysplastic
Case Presentation No. 075
 Case Presentation No. 075 Session 4. Myelodysplastic Syndrome Cristina Montalvo, MD Baylor College of Medicine Houston, Texas 2007 Workshop of Society for Hematopathology and European Association for Haematopathology
Case Presentation No. 075 Session 4. Myelodysplastic Syndrome Cristina Montalvo, MD Baylor College of Medicine Houston, Texas 2007 Workshop of Society for Hematopathology and European Association for Haematopathology
Molecular Markers in Acute Leukemia. Dr Muhd Zanapiah Zakaria Hospital Ampang
 Molecular Markers in Acute Leukemia Dr Muhd Zanapiah Zakaria Hospital Ampang Molecular Markers Useful at diagnosis Classify groups and prognosis Development of more specific therapies Application of risk-adjusted
Molecular Markers in Acute Leukemia Dr Muhd Zanapiah Zakaria Hospital Ampang Molecular Markers Useful at diagnosis Classify groups and prognosis Development of more specific therapies Application of risk-adjusted
SWOG ONCOLOGY RESEARCH PROFESSIONAL (ORP) MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017
 MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017") LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
Chronic myelomonocytic leukemia. Lymphoma Tumor Board. May 26, 2017
 Chronic myelomonocytic leukemia Lymphoma Tumor Board May 26, 2017 Myeloproliferative Neoplasms CMML has an estimated incidence of less than 1 per 100,000 persons per year Myeloproliferative neoplasms (MPN)
Chronic myelomonocytic leukemia Lymphoma Tumor Board May 26, 2017 Myeloproliferative Neoplasms CMML has an estimated incidence of less than 1 per 100,000 persons per year Myeloproliferative neoplasms (MPN)
Myelodysplastic syndromes: 2018 update on diagnosis, risk-stratification and management
 Received: 2 October 2017 Accepted: 2 October 2017 DOI: 10.1002/ajh.24930 ANNUAL CLINICAL UPDATES IN HEMATOLOGICAL MALIGNANCIES Myelodysplastic syndromes: 2018 update on diagnosis, risk-stratification and
Received: 2 October 2017 Accepted: 2 October 2017 DOI: 10.1002/ajh.24930 ANNUAL CLINICAL UPDATES IN HEMATOLOGICAL MALIGNANCIES Myelodysplastic syndromes: 2018 update on diagnosis, risk-stratification and
Cost-Effective Strategies in the Workup of Hematologic Neoplasm. Karl S. Theil, Claudiu V. Cotta Cleveland Clinic
 Cost-Effective Strategies in the Workup of Hematologic Neoplasm Karl S. Theil, Claudiu V. Cotta Cleveland Clinic In the past 12 months, we have not had a significant financial interest or other relationship
Cost-Effective Strategies in the Workup of Hematologic Neoplasm Karl S. Theil, Claudiu V. Cotta Cleveland Clinic In the past 12 months, we have not had a significant financial interest or other relationship
INTRODUCTION TO CYTOGENETICS AND MOLECULAR TESTING IN MDS
 INTRODUCTION TO CYTOGENETICS AND MOLECULAR TESTING IN MDS Saturday, September 29, 2018 Cyrus C. Hsia, HBSc, MD, FRCPC Associate Professor of Medicine, Schulich School of Medicine and Dentistry, Western
INTRODUCTION TO CYTOGENETICS AND MOLECULAR TESTING IN MDS Saturday, September 29, 2018 Cyrus C. Hsia, HBSc, MD, FRCPC Associate Professor of Medicine, Schulich School of Medicine and Dentistry, Western
Emerging Treatment Options for Myelodysplastic Syndromes
 Emerging Treatment Options for Myelodysplastic Syndromes James K. Mangan, MD, PhD Assistant Professor of Clinical Medicine Abramson Cancer Center, University of Pennsylvania Please note that some of the
Emerging Treatment Options for Myelodysplastic Syndromes James K. Mangan, MD, PhD Assistant Professor of Clinical Medicine Abramson Cancer Center, University of Pennsylvania Please note that some of the
Case Report. Aisha Jamal 1, Nida Anwar 2, Saba Shahid 3, Shariq Ahmed 3, Tahir Shamsi 1*
 Merit Research Journal of Medicine and Medical Sciences (ISSN: 2354-323X) Vol. 5(4) pp. 192-196, April, 2017 Available online http://www.meritresearchjournals.org/mms/index.htm Copyright 2017 Merit Research
Merit Research Journal of Medicine and Medical Sciences (ISSN: 2354-323X) Vol. 5(4) pp. 192-196, April, 2017 Available online http://www.meritresearchjournals.org/mms/index.htm Copyright 2017 Merit Research
Blastic Plasmacytoid Dendritic Cell Neoplasm with DNMT3A and TET2 mutations (SH )
") Blastic Plasmacytoid Dendritic Cell Neoplasm with DNMT3A and TET2 mutations (SH2017-0314) Habibe Kurt, Joseph D. Khoury, Carlos E. Bueso-Ramos, Jeffrey L. Jorgensen, Guilin Tang, L. Jeffrey Medeiros, and
Blastic Plasmacytoid Dendritic Cell Neoplasm with DNMT3A and TET2 mutations (SH2017-0314) Habibe Kurt, Joseph D. Khoury, Carlos E. Bueso-Ramos, Jeffrey L. Jorgensen, Guilin Tang, L. Jeffrey Medeiros, and
Hematology Unit Lab 2 Review Material
 Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Changing AML Outcomes via Personalized Medicine: Transforming Cancer Management with Genetic Insight
 Changing AML Outcomes via Personalized Medicine: Transforming Cancer Management with Genetic Insight Co-Moderators: Rick Winneker, PhD, Senior Vice President, Research, Leukemia & Lymphoma Society Mike
Changing AML Outcomes via Personalized Medicine: Transforming Cancer Management with Genetic Insight Co-Moderators: Rick Winneker, PhD, Senior Vice President, Research, Leukemia & Lymphoma Society Mike
Mayo alliance prognostic system for mastocytosis: clinical and hybrid clinical-molecular models
 REGULAR ARTICLE Mayo alliance prognostic system for mastocytosis: clinical and hybrid clinical-molecular models Animesh Pardanani, 1 Sahrish Shah, 1 Francesco Mannelli, 2 Yoseph C. Elala, 1 Paola Guglielmelli,
REGULAR ARTICLE Mayo alliance prognostic system for mastocytosis: clinical and hybrid clinical-molecular models Animesh Pardanani, 1 Sahrish Shah, 1 Francesco Mannelli, 2 Yoseph C. Elala, 1 Paola Guglielmelli,
Characterization of MPL-mutated myeloid neoplasms: a review of 224 MPL+ cases
 Article Characterization of MPL-mutated myeloid neoplasms: a review of 224 MPL+ cases Keming Lin 1,*, Gang Xu 1, Jie-Gen Jiang 1, Mayuko Imai 1, Zhao Wu 1, Paris Petersen 1, Kim Janatpour 1, and Bashar
Article Characterization of MPL-mutated myeloid neoplasms: a review of 224 MPL+ cases Keming Lin 1,*, Gang Xu 1, Jie-Gen Jiang 1, Mayuko Imai 1, Zhao Wu 1, Paris Petersen 1, Kim Janatpour 1, and Bashar
AML: WHO classification, biology and prognosis. Dimitri Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen
 AML: WHO classification, biology and prognosis Dimitri Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen Acute myeloid leukemia Clonal expansion of undifferentiated myeloid precursors Impaired
AML: WHO classification, biology and prognosis Dimitri Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen Acute myeloid leukemia Clonal expansion of undifferentiated myeloid precursors Impaired
What is MDS? Epidemiology, Diagnosis, Classification & Risk Stratification
 What is MDS? Epidemiology, Diagnosis, Classification & Risk Stratification Rami Komrokji, MD Clinical Director Malignant Hematology Moffitt Cancer Center Normal Blood and Bone Marrow What is MDS Myelodysplastic
What is MDS? Epidemiology, Diagnosis, Classification & Risk Stratification Rami Komrokji, MD Clinical Director Malignant Hematology Moffitt Cancer Center Normal Blood and Bone Marrow What is MDS Myelodysplastic
CME/SAM. Mixed Phenotype Acute Leukemia
 AJCP / Original Article Mixed Phenotype Acute Leukemia A Study of 61 Cases Using World Health Organization and European Group for the Immunological Classification of Leukaemias Criteria Olga K. Weinberg,
AJCP / Original Article Mixed Phenotype Acute Leukemia A Study of 61 Cases Using World Health Organization and European Group for the Immunological Classification of Leukaemias Criteria Olga K. Weinberg,
Outline. Case Study 5/17/2010. Treating Lower-Risk Myelodysplastic Syndrome (MDS) Tapan M. Kadia, MD Department of Leukemia MD Anderson Cancer Center
 Tapan M. Kadia, MD Department of Leukemia MD Anderson Cancer Center") Treating Lower-Risk Myelodysplastic Syndrome (MDS) Tapan M. Kadia, MD Department of Leukemia MD Anderson Cancer Center Outline Case Study What is lower-risk MDS? Classification systems Prognosis Treatment
Treating Lower-Risk Myelodysplastic Syndrome (MDS) Tapan M. Kadia, MD Department of Leukemia MD Anderson Cancer Center Outline Case Study What is lower-risk MDS? Classification systems Prognosis Treatment
Session II: Summary. Robert P Hasserjian, MD Professor of Pathology Massachusetts General Hospital and Harvard Medical School
 Session II: Summary Robert P Hasserjian, MD Professor of Pathology Massachusetts General Hospital and Harvard Medical School Disclosure of speaker s interests (Prefix and Last Name) (Potential) conflict
Session II: Summary Robert P Hasserjian, MD Professor of Pathology Massachusetts General Hospital and Harvard Medical School Disclosure of speaker s interests (Prefix and Last Name) (Potential) conflict
NUP214-ABL1 Fusion: A Novel Discovery in Acute Myelomonocytic Leukemia
 Case 0094 NUP214-ABL1 Fusion: A Novel Discovery in Acute Myelomonocytic Leukemia Jessica Snider, MD Medical University of South Carolina Case Report - 64 year old Caucasian Male Past Medical History Osteoarthritis
Case 0094 NUP214-ABL1 Fusion: A Novel Discovery in Acute Myelomonocytic Leukemia Jessica Snider, MD Medical University of South Carolina Case Report - 64 year old Caucasian Male Past Medical History Osteoarthritis
All patients with FLT3 mutant AML should receive midostaurin-based induction therapy. Not so fast!
 All patients with FLT3 mutant AML should receive midostaurin-based induction therapy Not so fast! Harry P. Erba, M.D., Ph.D. Professor, Internal Medicine Director, Hematologic Malignancy Program University
All patients with FLT3 mutant AML should receive midostaurin-based induction therapy Not so fast! Harry P. Erba, M.D., Ph.D. Professor, Internal Medicine Director, Hematologic Malignancy Program University
Mixed Phenotype Acute Leukemias
 Mixed Phenotype Acute Leukemias CHEN GAO; AMY M. SANDS; JIANLAN SUN NORTH AMERICAN JOURNAL OF MEDICINE AND SCIENCE APR 2012 VOL 5 NO.2 INTRODUCTION Most cases of acute leukemia can be classified based
Mixed Phenotype Acute Leukemias CHEN GAO; AMY M. SANDS; JIANLAN SUN NORTH AMERICAN JOURNAL OF MEDICINE AND SCIENCE APR 2012 VOL 5 NO.2 INTRODUCTION Most cases of acute leukemia can be classified based
Acute Myeloid Leukemia Progress at last
 Acute Myeloid Leukemia Progress at last Bruno C. Medeiros, MD September 9, 217 Introduction Mechanisms of leukemogenesis Emerging therapies in AML Previously untreated AML Relapsed and refractory patients
Acute Myeloid Leukemia Progress at last Bruno C. Medeiros, MD September 9, 217 Introduction Mechanisms of leukemogenesis Emerging therapies in AML Previously untreated AML Relapsed and refractory patients
Classification and risk assessment in AML: integrating cytogenetics and molecular profiling
 ACUTE MYELOID LEUKEMIA: HOW CAN WE IMPROVE UPON STANDARD THERAPY? Classification and risk assessment in AML: integrating cytogenetics and molecular profiling Matahi Moarii and Elli Papaemmanuil Department
ACUTE MYELOID LEUKEMIA: HOW CAN WE IMPROVE UPON STANDARD THERAPY? Classification and risk assessment in AML: integrating cytogenetics and molecular profiling Matahi Moarii and Elli Papaemmanuil Department
Clonal Evolution of saml. Johnnie J. Orozco Hematology Fellows Conference May 11, 2012
 Clonal Evolution of saml Johnnie J. Orozco Hematology Fellows Conference May 11, 2012 CML: *bcr-abl and imatinib Melanoma: *braf and vemurafenib CRC: *k-ras and cetuximab Esophageal/Gastric: *Her-2/neu
Clonal Evolution of saml Johnnie J. Orozco Hematology Fellows Conference May 11, 2012 CML: *bcr-abl and imatinib Melanoma: *braf and vemurafenib CRC: *k-ras and cetuximab Esophageal/Gastric: *Her-2/neu
Hematology Measure #1: Myelodysplastic Syndrome (MDS) and Acute Leukemias: Baseline Cytogenetic Testing Performed on Bone Marrow
 and Acute Leukemias: Baseline Cytogenetic Testing Performed on Bone Marrow") Hematology Measure #1: Myelodysplastic Syndrome (MDS) and Acute Leukemias: Baseline Cytogenetic Testing Performed on Bone Marrow This measure may be used as an Accountability measure Clinical Performance
Hematology Measure #1: Myelodysplastic Syndrome (MDS) and Acute Leukemias: Baseline Cytogenetic Testing Performed on Bone Marrow This measure may be used as an Accountability measure Clinical Performance
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms. Curtis A. Hanson, MD
 Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
The Center for PERSONALIZED DIAGNOSTICS
 The Center for PERSONALIZED DIAGNOSTICS Precision Diagnostics for Personalized Medicine A joint initiative between The Department of Pathology and Laboratory Medicine & The Abramson Cancer Center The (CPD)
The Center for PERSONALIZED DIAGNOSTICS Precision Diagnostics for Personalized Medicine A joint initiative between The Department of Pathology and Laboratory Medicine & The Abramson Cancer Center The (CPD)