Nodal staging of colorectal cancer, TNM and practical issues
|
|
|
- Virgil Gordon
- 5 years ago
- Views:
Transcription



1 Nodal staging of colorectal cancer, TNM and practical issues Gábor Cserni 1. Bács-Kiskun County Teaching Hospital, Kecskemét 2. University of Szeged, Szeged

2 Different staging systems: A,B,C,(D) Same letters sometimes different meaning Cserni G. J Clin Pathol 2003;56:327
3 Primary tumor: (c)t & pt (TNM7, 2010-) T & pt TX: Not assessable (to be minimized) T0: No tumor Tis: carcinoma in situ: intraepithelial tumor or involving the lamina propria (intramucosal) T1: Tumor invading into submucosa. T2: Tumor invading into muscularis propria. T3: Tumor invading through the muscularis propria into pericolorectal tissues. T4a: Tumor penetrating through visceral peritoneum.* T4b: Tumor invading into adjacent organs or structures* (through the peritoneum or over the m. propria for retro- or infraperitoneal localizations) (opposite meanings in TNM5) * Still reverted in RCPath reporting proforma using TNM5, accessed 1 May 2017
4 Implementation delayed In order to ensure that the cancer care community has the necessary infrastructure in place for documenting 8th Edition stage, the AJCC Executive Committee, in dialogue with the National Cancer Institute (NCI-SEER), Centers for Disease Control and Prevention (CDC), the College of American Pathologists (CAP), the National Comprehensive Cancer Network (NCCN, the National Cancer Data Base (NCDB), and the Commission on Cancer (CoC), made the decision to delay the implementation of the 8th Edition Cancer Staging System to January 1, Cancer-Staging-System.aspx
5 Primary tumor: (c)t & pt (TNM8, 2018-) T & pt TX: Not assessable (to be minimized) T0: No tumor Tis: carcinoma in situ tumor involving the lamina propria (intramucosal carcinoma) only. (Intraepithelial carcinoma = HG dysplasia ptis) T1: Tumor invading into submucosa. T2: Tumor invading into muscularis propria. T3: Tumor invading through the muscularis propria. T4a: Tumor demonstrating serosal involvement. T4b: Tumor invading into adjacent organs or structures (through the peritoneum or over the m. propria for retro- or infraperitoneal localizations)
6 pt3: pt3a ( 5 mm from the muscularis propria) & pt3b (> 5 mm from the muscularis propria) Bori R et al. Pathol Oncol Res 2009;15: pt3a tumors have a better prognostic profile than pt3b. These are not TNM categories recognized in the AJCC staging books, but are mentioned in the TNM Supplement (since 1993). Merkel S et al. Int J Colorectal Dis 2001;16:
7 pt4a peritoneal involvement (TNM8) Direct tumor extension With perforation in which the tumor cells are continuous with the serosal surface through inflammation No pt4a category for non peritonealized areas (e.g. posterior ascending colon) <1mm from serosal surface and accompanied by serosal reaction; if multiple levels exclude serosal surface involvement pt3
8 pt4a peritoneal involvement Shepherd N et al. Gastroenterology 1997 (Gloucester) 1. Lack of peritoneal involvement 2. Fibrin and inflammatory exsudate on the peritoneum with tumor cells beneath the peritoneum, but not on it (TNM: pt3) 3. Tumor propagation on the peritoneal surface 4. Ulceration and apparently free tumor cells floating on the peritoneal surface (especially in crevices)

9 Category 3 & 4 had worse survival Shepherd N et al. Gastroenterology 1997
pt1 (y)pt2")
10 Assessment of peritoneal involvement Higher pt4 ratio as a result of more precise pathological work-up Percentage of pt1-4 categories 0,9 0,8 0,7 0,6 0,5 0,4 0,3 0,2 0, n = (y)pt1 (y)pt2 (y)pt3 pt4
11 Lymph nodes: pn (TNM7) pnx: Not assessable (eg: removed earlier / not removed / no LNs identified) pn0: No regional LN metastasis (including isolated tumor cell clusters) pn1: Metastasis to 1-3 regional LNs pn1mi Micrometastasis (>0.2 mm and/or >200 cells, but none > 2.0 mm) pn1a Metastasis to 1 LN (>2 mm) pn1b Metastasis to 2-3 LN (at least one metastasis >2 mm) pn1c Tumor deposit(s) (TD) in the subserosa, mesocolon, pericolic, perirectal tissues, without LN structure, if there is no LN metastasis pn2: Metastasis to 4 or more regional LNs pn2a Metastasis to 4-6 LNs (at least one metastasis >2 mm) pn2b Metastasis to 7 or more LNs (at least one metastasis >2 mm)
12 LNs (TNM8) At least 12 Number of nodes correlates with survival Micrometastasis (may be designated as pn1mi, but it is better to consider them standard positive nodes) pn0(i+) (<0.2 mm) worse prognosis than pn0

13 Theory and practice

")
14 Is this a lymph node? (1) (x10-x20)

")
15 Is this a lymph node? (2) (x10-x20)

16 Is this a lymph node metastasis? (1) x 2
17 Is this a lymph node metastasis? (1) x 2

 x 35")
18 Is this a lymph node metastasis? (1) x 35
 x 2.")
19 Is this a lymph node metastasis? (2) x 2.5

20 Is this a lymph node metastasis? (2) x 10 (central part)
 x 1.")
21 Is this a lymph node metastasis? (2) x 1.5
 x 25 Smooth muscle, elastic")
22 Is this a lymph node metastasis? (2) x 25 Smooth muscle, elastic fibers
23 Is this a lymph node? (3) (x 3)
 (x")
24 Is this a lymph node? (3) (x 10)
 (x 5)")
25 Is this a lymph node? (4) (x 5)
 (x 4.")
26 Is this a lymph node? (4) (x 4.5) (Orcein-H)

 (SMA -")
27 Is this a lymph node? (4) (x 4 x 4.5) (SMA - H-caldesmon)
 (x")
28 Is this a lymph node? (5) (x 10)

")
29 Is this a lymph node? (5) (x 10 x 40) Orcein



30 X4 X40 Is this a LN metastasis? (3) x20 x20
31 Primary vs Metastasis Rectosigmoid colon pt1 here, but pt2 elsewhere pn1b (2/10)
32 Primary vs Metastasis Rectosigmoid colon pt1 here, but pt2 elsewhere pn1b (?) CDX2





33 Primary vs Metastasis Rectosigmoid colon pt1 here, but pt2 elsewhere pn1 (?) NO pt2 pn0 & Occult prostatic cancer M1 PSAP CDX2

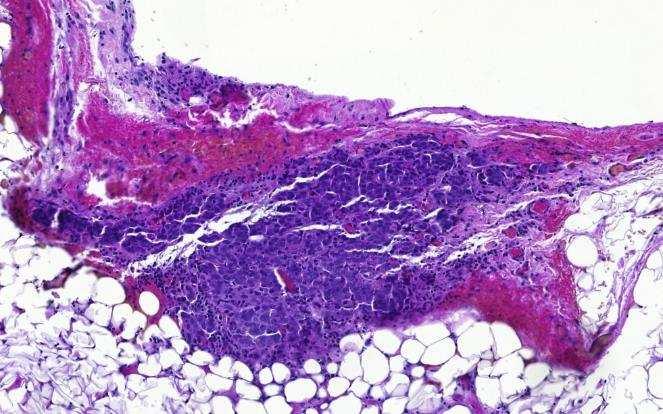
34 Is this a LN metastasis? (4)

35 Is this a LN metastasis? (4)
")
36 No cells, just mucin (negative) ypn0

37 Halving / Slicing larger LNs
38 LNs vs TDs (tumor deposits) Lymph nodes have the following features: capsule, subcapsular sinus, lymphoid tissue, often with follicles, sometimes perinodal lymphoid tissue as well; they may have smooth muscle in their capsule very rarely, it seems, they may have even elastic fibres in the capsule
39 Tumor deposits Of 400 pts with pt3 N+M0 colon ca 18% had tumor deposits (TD)(TNM5, 1998) TD: adenocarcinoma within adipose or fibrous tissue but not associated with a LN Grossly palpated lesions, generally submitted as LN Goldstein NS, Turner JR. Cancer 2000
40 Tumor deposits Independent factors associated with shorter DFS: Any TDs (independent of size) Increasing number of TDs Increasing number of involved LNs Grade TDs proved to be perivascular (large vessels), intravascular and/or perineural tumor foci Goldstein NS, Turner JR. Cancer 2000
41 Lymph node metastasis vs TD Tumor nodule lacking elements of a LN TNM5 >3 mm: LN metastasis pn 3 mm: discontinuous tumor spread pt TNM6 Regular outline: LN metastasis pn irregular outline: venous invasion: V1


42 Lymph node metastasis vs TD V1 orcein stain V1
43 Lymph node metastasis vs TD Tumor nodule lacking elements of a LN TNM7 Can be: discontinuous tumor spread, completely destroyed LN (N1/2), venous invasion (V1/2), If destroyed LN: pn category Discontinuous spread, venous invasion (V1/2) TD (pn1c, if no LN metastasis, for T1-2 tumors) TD and V1 on the basis of the orcein (elastica) stain
44 TD (TNM8) No elements of a LN Not venous invasion (V1, V2), not lymphovascular (small vessel) involvement (L1), not perineural involvement (Pn1) If there is no LN metastasis: pn1c If there is a LN metastasis: this should not be added to the number of metastatic nodes
45 The suggested number of LNs to be assessed for a reliable pn0 6 Hernanz F et al. Dis Colon Rectum 1994;37: Caplin S et al. Cancer 1998;83: Mainprize KS et al. J Clin Pathol 1998;51: Cserni G. J Clin Pathol 2002;55: Maurel J et al. Cancer 1998;82: Cianchi F et al. World J Surg 2002;26: TNM Supplement 3rd Ed 13 Scott KWM et al. Br J Surg 1989;76: Wong JH et al. J Clin Oncol 1999;17: Tepper JE et al. J Clin Oncol 2001;19: Cserni G et al. Pathol Oncol Res 1999;5: Goldstein NS. Am J Surg Pathol 2002;26: Greco P et al. Virchows Arch 2006;449:
46 How many LNs? As many as possible! T3N0M0 CRC from the SEER database year OS 0.8 a survival estimate b c 10-year OS number of nodes examined Cserni G, et al. Is there a minimum number of lymph nodes that should be histologically assessed for a reliable nodal staging of T3N0M0 colorectal carcinomas? J Surg Oncol 2002; 81:63-69.
47 Distribution of pn categories at BKMK (y)pn2 pnx More (y)pn2 pnx (y)pn0 (y)pn0 (y)pn1 (y)pn Mean (SD): 9 (6) Median: 8 Range: 0-31 Number of LNs assessed 2006 (2016) 19 (11) 13 (6)
48 Distance from the tumour as qualitative feature D C B A B C D Tumour cm 2 cm 2 cm 3 cm 3 cm 100 cases of CRC Mean: 17 LN / case Cserni G, et al. Distance of lymph nodes from the tumor, an important feature in colorectal cancer specimens. Arch Pathol Lab Med 2001; 125:


49 An example C A C A B B B C No fraction D in this specific case
50 Results 53 pn1 or pn2 All but 1 staged correctly as pn+ on the basis of LNs from fraction A All staged correctly on the basis of A and B (3 cms from the tumor in each direction SUGGESTION: LNs from below the tumor and its 3 cm-wide perimetry should be evaluated for reliable staging. Look for further LNs if <7, or if pn1 with 3 LNs +! Cserni G, et al. Arch Pathol Lab Med 2001; 125:
51 Further testing 762 further CRCs studied - sections A & B (3cm) vs C & D (>3cm) till end 2008 Only 4/369 N+ cases had metastasis in a LN from segment CD without having metastasis in the AB segment. 14 further cases would have been wrongly classified as pn1 instead of pn2 This error rate is LOWER than the FNR of lymphatic mapping Cserni G et al. J Clin Pathol 2011
 3 false negative cases (3.")
 The aim would be a more reliable and improved staging")
52 Sentinel nodes and lymphatic mapping in CRCs 85/86 successfull SN identifications 29 N+ cases; 15 only SN+ (7 only micrometastatic; 2 only IHC) 3 false negative cases (3.6% FNR as reported % FNR as I understand it) The aim would be a more reliable and improved staging (detailed pathology of SLNs). Saha S et al. Ann Surg Oncol 2000;7:120-4.

53 Unexpected lymph drainage Lymphatic mapping studies have demonstrated that direct drainage may occur from a tumor site to apical or even paraaortic LNs. Merrie AE, et al. Dis Colon Rectum 2001;44: This LN proved to be the only positive LN resected with the colon, but was outside the margins of a standard right hemicolectomy, the operation usually performed for a primary carcinoma at the given location. Tsioulias GJ, et al. Arch Surg 2000;135: Same case reported in 2 papers Bilchik AJ, et al. J Clin Oncol 2001;19: The only positive (only CK+) / 18 LN
54 Less success in other series (11-50 pts, mean 24 pts / series) False negative rates (false negatives / all positives) & upstaging rates: 1/3 (33%) & NA Evangelista W et al. Tumori 2002;88: /3 (33%) & 2/13 (15%) Tsoulias GJ et al. Am Surg 2002;68: /13 (38%) & NA Cserni G et al. Pathol Oncol Res 1999; 5: /7 (43%) & 2/16 (13%) Merrie AE et al. Dis Colon Rectum 2001;44: /7 (29%) & 2/20 (10%) Fitzgerald TL et al. J Surg Oncol 2002;80: /3 (33%) & NA Esser S et al. Dis Colon Rectum 2001;44: /8 (25%) & NA Kitagawa Y et al. Surg Clin North Am 2000;80: /20 (60%) & 2/15 (13%) Joosten JJA et al. Br J Surg 1999;86:482-6.
55 Lymphatic mapping in CRC Meta-analysis van der PAS MH et al, Lancet Oncol mapping procedures (2961 colon, 806 rectum) Mean weighted identification rate: 94% (95%CI: 92-95%) Pooled sensitivity: 76% (95%CI: 72-80%) being independent of pt category and tumor localisation To be considered for cn0 M0 patients, as there is about 15% upstaging; prognostic importance?
56 Distant Metastasis: M (TNM7) Mx: Not defined pm0: There is no such category M0: No metastasis present M1(pM1): Metastasis present pm1a Metastasis in 1 organ or site (>0.2 mm) pm1b Metastasis in >1 organ or site or the peritoneum
57 Distant Metastasis: M (TNM8) Mx: Not defined pm0: There is no such category M0: No metastasis present M1(pM1): Metastasis present pm1a Metastasis in 1 organ or site e.g. liver, lung, ovary, non-regional lymh node(s) pm1b Metastasis in >1 organ or site pm1c Metastasis to the peritoneum +/- other organ involvement
58 Final recapitulating case (TNM8) - 81-year-old female with bowel obstruction - emergency operation: coecal dilation and necrosis, tumor of descending colon, total colectomy specimen

59 Primary tumour x0.8 pt Ulcerated luminal surface Serosal surface

60 Primary tumour x5 pt

61 Primary tumour x40 pt X40
62 Primary tumour ptx pt0 ptis pt1 pt2 pt3 pt4a pt4b
63 Primary tumour ptx pt0 ptis pt1 pt2 pt3 pt4a pt4b
64
65 Primary tumour x1 pt Ulcerated luminal surface Serosal surface
 Serosal")
66 Primary tumour: pt (x4) Serosal crevice
67 Primary tumour: pt (x10)
68 Primary tumour: pt (x20)



69 Primary tumour: pt (x40)
70 Final recapitulating case Primary tumour ptx pt0 ptis pt1 pt2 pt3 pt4a pt4b
71 Final recapitulating case Primary tumour ptx pt0 ptis pt1 pt2 pt3 pt4a pt4b
72 Primary tumour: (histological type) x1
73 Primary tumour: (histological type) x1



74 Primary tumour: (histological type) x1 ca 3-4:1



75 Lymph nodes (gross n=13 from the 3 cm perit region) 10 negative LNs + 3
76 Lymph nodes (gross n=13 from the 3 cm perit region) 10 negative LNs + 2 TDs + 1 LN met: 1/11 LN + 2TDs
77 Final recapitulating case Tumour + Nodes ptx - pnx pt0 - pn0 ptis - pn1a pt1 - pn1b pt2 - pn1c pt3 - pn2a pt4a - pn2b pt4b
78 Final recapitulating case Tumour + Nodes ptx - pnx pt0 - pn0 ptis - pn1a pt1 - pn1b pt2 - pn1c pt3 - pn2a pt4a - pn2b pt4b Because TDs do not count, if you have an LN met.
79 Omentum (x0.8)
80 Omentum x5


81 Omentum x20 (micropapillary component) x5
82 Final recapitulating case Tumour + Nodes + Metastasis ptx - pnx - Mx pt0 - pn0 - M0 ptis - pn1a - pm0 pt1 - pn1b - (p)m1a pt2 - pn1c - (p)m1b pt3 - pn2a - (p)m1c pt4a - pn2b pt4b
83 Final recapitulating case Tumour + Nodes + Metastasis ptx - pnx - Mx pt0 - pn0 - M0 ptis - pn1a - pm0 pt1 - pn1b - pm1a pt2 - pn1c - pm1b pt3 - pn2a - pm1c pt4a - pn2b pt4b The omentum supports peritoneal carcinosis, this can be a pm category.
84 Final recapitulating case T + N + M ptx - pnx - Mx pt0 - pn0 - M0 ptis - pn1a - pm0 pt1 - pn1b - pm1a pt2 - pn1c - pm1b pt3 - pn2a - pm1c pt4a - pn2b pt4b STAGE IV.C

85

:")

86 CK7 CDX2 CA125 CK20 (not shown): in both areas
87 CK7 CDX2


88 CK7 CDX2
89 Final recapitulating case T + N + M ptx - pnx - Mx pt0 - pn0 - M0 ptis - pn1a - pm0 pt1 - pn1b - (p)m1a pt2 - pn1c - (p)m1b pt3 - pn2a - (p)m1c pt4a - pn2b cannot be determined pt4b w/o additional means & rpt3a rpn1 ovarian serous carcinoma

90 Id. Markó Károly: Visegrád 1826
Update on staging colorectal carcinoma, the 8 th edition AJCC. General overview of staging. When is staging required? 11/1/2017
 Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
LOINC. Clinical information. RCPA code. Record if different to report header Operating surgeon name and contact details. Absent.
 Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Complete as narrative or use the structured format below 55752-0 17.02.28593 Clinical information 22027-7 17.02.30001 Record if different to report header Operating surgeon name and contact details 52101004
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Staging Challenges in Lower GI Cancers. Disclosure of Relevant Financial Relationships. AJCC 8 th edition and CAP protocol updates
 Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Definition of Synoptic Reporting
 Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
A916: rectum: adenocarcinoma
 General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
General facts of colorectal cancer The colon has cecum, ascending, transverse, descending and sigmoid colon sections. Cancer can start in any of the r sections or in the rectum. The wall of each of these
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
Greater Manchester & Cheshire Guidelines for Pathology Reporting for Oesophageal and Gastric Malignancy Authors: Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments 1.1 Cancer reporting: Biopsies
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors
 Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors Frédéric Bibeau, MD, PhD Pathology department Biopathology unit Institut du Cancer de Montpellier France Quality
Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors Frédéric Bibeau, MD, PhD Pathology department Biopathology unit Institut du Cancer de Montpellier France Quality
IMAGING GUIDELINES - COLORECTAL CANCER
 IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
Seventh Edition Staging 2017 Colorectum. Overview. This webinar is sponsored by. the Centers for Disease Control and Prevention.
 Seventh Edition Staging 2017 Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express
Seventh Edition Staging 2017 Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. No materials in this presentation may be repurposed in print or online without the express
AJCC Cancer Staging 8 th Edition
 AJCC Cancer Staging 8 th Edition Colon and Rectal Cancer Staging Update Webinar George J Chang, MD, MS Deputy Chair, Department of Surgical Oncology Chief, Colon and Rectal Surgery Professor of Surgical
AJCC Cancer Staging 8 th Edition Colon and Rectal Cancer Staging Update Webinar George J Chang, MD, MS Deputy Chair, Department of Surgical Oncology Chief, Colon and Rectal Surgery Professor of Surgical
AJCC 7 th Edition Staging Disease Site Webinar Colorectum
 AJCC 7 th Edition Staging Disease Site Webinar Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310
AJCC 7 th Edition Staging Disease Site Webinar Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310
7 th Edition Staging. AJCC 7 th Edition Staging. Disease Site Webinar. Colorectum. Overview. This webinar is sponsored by
 AJCC 7 th Edition Staging Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers
AJCC 7 th Edition Staging Colorectum Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers
Small Intestine. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition
 Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Small Intestine Protocol applies to all invasive carcinomas of the small intestine, including those with focal endocrine differentiation. Excludes carcinoid tumors, lymphomas, and stromal tumors (sarcomas).
Descriptor Definition Author s notes TNM descriptors Required only if applicable; select all that apply multiple foci of invasive carcinoma
 S5.01 The tumour stage and stage grouping must be recorded to the extent possible, based on the AJCC Cancer Staging Manual (7 th Edition). 11 (See Tables S5.01a and S5.01b below.) Table S5.01a AJCC breast
S5.01 The tumour stage and stage grouping must be recorded to the extent possible, based on the AJCC Cancer Staging Manual (7 th Edition). 11 (See Tables S5.01a and S5.01b below.) Table S5.01a AJCC breast
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Staging AJCC eighth edition. Duncan McLeod Westmead Hospital, NSW
 Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
Gastric Cancer Staging AJCC eighth edition Duncan McLeod Westmead Hospital, NSW Summary of changes New clinical stage prognostic groups, ctnm Postneoadjuvant therapy pathologic stage groupings, yptnm -
NUMERATOR: Reports that include the pt category, the pn category and the histologic grade
 Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
NUMERATOR: Reports that include the pt category, the pn category and the histologic grade
 Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Quality ID #100 (NQF 0392): Colorectal Cancer Resection Pathology Reporting: pt Category (Primary Tumor) and pn Category (Regional Lymph Nodes) with Histologic Grade National Quality Strategy Domain: Effective
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Rectal Cancer Cookbook Update. A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux
 Rectal Cancer Cookbook Update A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux Prof Dr A Jouret-Mourin, Department of Pathology, UCL, St Luc, Brussels
Rectal Cancer Cookbook Update A. JOURET-MOURIN with the collaboration of A Hoorens,P Demetter, G De Hertogh,C Cuvelier and C Sempoux Prof Dr A Jouret-Mourin, Department of Pathology, UCL, St Luc, Brussels
Neoplasms of the Colon and of the Rectum
 Neoplasms of the Colon and of the Rectum 2 0 1 5-2 0 1 6 F C D S E D U C A T I O N A L W E B C A S T S E R I E S S T E V E N P E A C E, B S, C T R F E B R U A R Y 1 8, 2 0 1 6 2016 Focus o Anatomy o SS
Neoplasms of the Colon and of the Rectum 2 0 1 5-2 0 1 6 F C D S E D U C A T I O N A L W E B C A S T S E R I E S S T E V E N P E A C E, B S, C T R F E B R U A R Y 1 8, 2 0 1 6 2016 Focus o Anatomy o SS
46. Merkel Cell Carcinoma
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
SEER EOD AND SUMMARY STAGE ABSTRACTORS TRAINING
 SEER EOD AND SUMMARY STAGE ABSTRACTORS TRAINING OVERVIEW What is SEER EOD Ambiguous Terminology General Guidelines EOD Primary Tumor EOD Regional Nodes EOD Mets Site Specific Data Items (SSDI) SEER Summary
SEER EOD AND SUMMARY STAGE ABSTRACTORS TRAINING OVERVIEW What is SEER EOD Ambiguous Terminology General Guidelines EOD Primary Tumor EOD Regional Nodes EOD Mets Site Specific Data Items (SSDI) SEER Summary
LUNG STAGING FORM LATERALITY: LEFT RIGHT BILATERAL
 LUNG STAGING FORM LATERALITY: LEFT RIGHT BILATERAL ( ) Tx Primary tumor cannot be assessed, or tumor proven by the presence of malignant cells in sputum or bronchial washings but not visualized by imaging
LUNG STAGING FORM LATERALITY: LEFT RIGHT BILATERAL ( ) Tx Primary tumor cannot be assessed, or tumor proven by the presence of malignant cells in sputum or bronchial washings but not visualized by imaging
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
ACRIN 6666 Therapeutic Surgery Form
 S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
S1 ACRIN 6666 Therapeutic Surgery Form 6666 Instructions: Complete a separate S1 form for each separate area of each breast excised with the intent to treat a cancer (e.g. each lumpectomy or mastectomy).
Staging for Residents, Nurses, and Multidisciplinary Health Care Team
 Staging for Residents, Nurses, and Multidisciplinary Health Care Team Donna M. Gress, RHIT, CTR Validating science. Improving patient care. Learning Objectives Introduce the concept and history of stage
Staging for Residents, Nurses, and Multidisciplinary Health Care Team Donna M. Gress, RHIT, CTR Validating science. Improving patient care. Learning Objectives Introduce the concept and history of stage
Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ]
![Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ]](/thumbs/82/86264030.jpg "Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ]") Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ] CS Tumor Size 000 No mass/tumor found 001-988 001-988 millimeters (code exact size in millimeters) 989 989 millimeters or larger 990 Microscopic
Collaborative Stage for TNM 7 - Revised 06/30/2008 [ Schema ] CS Tumor Size 000 No mass/tumor found 001-988 001-988 millimeters (code exact size in millimeters) 989 989 millimeters or larger 990 Microscopic
University of Groningen. Lymph node staging in colon cancer Kelder, Wendy
 University of Groningen Lymph node staging in colon cancer Kelder, Wendy IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the
University of Groningen Lymph node staging in colon cancer Kelder, Wendy IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the
Peritoneal Involvement in Stage II Colon Cancer
 Anatomic Pathology / PERITONEAL INVOLVEMENT IN STAGE II COLON CANCER Peritoneal Involvement in Stage II Colon Cancer A.M. Lennon, MB, MRCPI, H.E. Mulcahy, MD, MRCPI, J.M.P. Hyland, MCh, FRCS, FRCSI, C.
Anatomic Pathology / PERITONEAL INVOLVEMENT IN STAGE II COLON CANCER Peritoneal Involvement in Stage II Colon Cancer A.M. Lennon, MB, MRCPI, H.E. Mulcahy, MD, MRCPI, J.M.P. Hyland, MCh, FRCS, FRCSI, C.
Handling & Grossing of Colo-rectal Specimens for Tumours. for Medical Officers in Pathology
 Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Handling & Grossing of Colo-rectal Specimens for Tumours for Medical Officers in Pathology Dr Gayana Mahendra Department of Pathology Faculty of Medicine University of Kelaniya Your Role in handling colorectal
Diagnostic Difficulties Encountered Among Colorectal Polyps
 Diagnostic Difficulties Encountered Among Colorectal Polyps Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Cornell Medical
Diagnostic Difficulties Encountered Among Colorectal Polyps Rhonda K. Yantiss, M.D. Professor of Pathology and Laboratory Medicine Department of Pathology and Laboratory Medicine Weill Cornell Medical
PROTOCOL SENTINEL NODE BIOPSY (NON OPERATIVE) BREAST CANCER - PATHOLOGY ASSESSMENT
 BREAST CANCER - PATHOLOGY ASSESSMENT") PROTOCOL SENTINEL NODE BIOPSY (NON OPERATIVE) BREAST CANCER - PATHOLOGY ASSESSMENT Author: Dr Sally Ann Hales On behalf of the Breast and pathology CNGs Written: March 2005 Reviewed by CNG: June 2009 &
PROTOCOL SENTINEL NODE BIOPSY (NON OPERATIVE) BREAST CANCER - PATHOLOGY ASSESSMENT Author: Dr Sally Ann Hales On behalf of the Breast and pathology CNGs Written: March 2005 Reviewed by CNG: June 2009 &
Question: If in a particular case, there is doubt about the correct T, N or M category, what do you do?
 Exercise 1 Question: If in a particular case, there is doubt about the correct T, N or M category, what do you do? : 1. I mention both categories that are in consideration, e.g. pt1-2 2. I classify as
Exercise 1 Question: If in a particular case, there is doubt about the correct T, N or M category, what do you do? : 1. I mention both categories that are in consideration, e.g. pt1-2 2. I classify as
Wendy L Frankel. Chair and Distinguished Professor
 1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
1 Wendy L Frankel Chair and Distinguished Professor Case 1 59 y/o woman Abdominal pain No personal or family history of cancer History of colon polyps Colonoscopy Polypoid rectosigmoid mass Biopsy 3 4
Alison Douglass Gillian Lieberman, MD. November. Colon Cancer. Alison Douglass, Harvard Medical School Year III Gillian Lieberman, MD
 November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
November Colon Cancer Alison Douglass, Harvard Medical School Year III Our Patient Mr. K. is a 67 year old man with no prior medical problems other than hemorrhoids which have caused occasional rectal
WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER?
 CANCER STAGING TNM and prognosis in CRC WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER? Alessandro Lugli, MD Institute of Pathology University of Bern Switzerland Maastricht, June 19
CANCER STAGING TNM and prognosis in CRC WHAT SHOULD WE DO WITH TUMOUR BUDDING IN EARLY COLORECTAL CANCER? Alessandro Lugli, MD Institute of Pathology University of Bern Switzerland Maastricht, June 19
Interactive Staging Bee
 Interactive Staging Bee ROBIN BILLET, MA, CTR GA/SC REGIONAL CONFERENCE NOVEMBER 6, 2018? Clinical Staging includes any information obtained about the extent of cancer obtained before initiation of treatment
Interactive Staging Bee ROBIN BILLET, MA, CTR GA/SC REGIONAL CONFERENCE NOVEMBER 6, 2018? Clinical Staging includes any information obtained about the extent of cancer obtained before initiation of treatment
The Voyage to Direct Coding of AJCC TNM & Stage... Jayne Holubowsky, CTR DelMarVa-DC Educational Meeting Annapolis, MD October 8, 2015.
 The Voyage to Direct Coding of AJCC TNM & Stage... Jayne Holubowsky, CTR DelMarVa-DC Educational Meeting Annapolis, MD October 8, 2015 outline Evolution General Rules Site-specific Rules How well do you
The Voyage to Direct Coding of AJCC TNM & Stage... Jayne Holubowsky, CTR DelMarVa-DC Educational Meeting Annapolis, MD October 8, 2015 outline Evolution General Rules Site-specific Rules How well do you
STAGE CATEGORY DEFINITIONS
 CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c
CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
The Rodger C. Haggitt Memorial Lecture
 The Rodger C. Haggitt Memorial Lecture I got an email on 4/22/14 from Hala El Zamaity inviting me to give this lecture and giving me this topic: The ever changing TNM classification and its implication
The Rodger C. Haggitt Memorial Lecture I got an email on 4/22/14 from Hala El Zamaity inviting me to give this lecture and giving me this topic: The ever changing TNM classification and its implication
47. Melanoma of the Skin
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Effect of Tumor Deposits on Overall Survival in Colorectal Cancer Patients with Regional Lymph Node Metastases
 J Rural Med 2014; 9(1): 20 26 Original article Effect of Tumor Deposits on Overall Survival in Colorectal Cancer Patients with Regional Lymph Node Metastases Eiichi Yabata, Masaru Udagawa and Hiroyuki
J Rural Med 2014; 9(1): 20 26 Original article Effect of Tumor Deposits on Overall Survival in Colorectal Cancer Patients with Regional Lymph Node Metastases Eiichi Yabata, Masaru Udagawa and Hiroyuki
Ritu Nayar, MD Professor and Vice Chair of Pathology Northwestern University, Feinberg School of Medicine Chicago, IL
 Ritu Nayar, MD Professor and Vice Chair of Pathology Northwestern University, Feinberg School of Medicine Chicago, IL email: r-nayar@northwestern.edu Nothing to disclose College of American Pathologists
Ritu Nayar, MD Professor and Vice Chair of Pathology Northwestern University, Feinberg School of Medicine Chicago, IL email: r-nayar@northwestern.edu Nothing to disclose College of American Pathologists
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015
: Imaging Guidelines September 2015") Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
Colorectal Pathway Board (Clinical Subgroup): Imaging Guidelines September 2015 1 Contents Page No. 1. Objective 3 2. Imaging Techniques 3 3. Staging of Colorectal Cancer 5 4. Radiological Reporting 6
Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma. Michael T. Tetzlaff MD, PhD
 Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational and Molecular Pathology
Update on 8 th Edition Cutaneous AJCC Staging of Primary Cutaneous Melanoma Michael T. Tetzlaff MD, PhD Associate Professor Departments of Pathology (Dermatopathology) and Translational and Molecular Pathology
Clinical, Pathologic and Molecular Updates
 Colorectal Cancer: Clinical, Pathologic and Molecular Updates Joanna A. Gibson, M.D./Ph.D. Yale University School of Medicine/Yale New Haven Hospital, Department of Pathology Gastrointestinal, Pancreaticobiliary
Colorectal Cancer: Clinical, Pathologic and Molecular Updates Joanna A. Gibson, M.D./Ph.D. Yale University School of Medicine/Yale New Haven Hospital, Department of Pathology Gastrointestinal, Pancreaticobiliary
8. The polyp in the illustration can be described as (circle all that apply) a. Exophytic b. Pedunculated c. Sessile d. Frank
 a. Exophytic b. Pedunculated c. Sessile d. Frank") Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
Quiz 1 Overview 1. Beginning with the cecum, which is the correct sequence of colon subsites? a. Cecum, ascending, splenic flexure, transverse, hepatic flexure, descending, sigmoid. b. Cecum, ascending,
6/5/2010. Renal vein invasion & Capsule Penetration (T3a) Adrenal Gland involvement (T4 vs. M1) Beyond Gerota s Fascia? (?T4).
 Adrenal Gland involvement (T4 vs. M1) Beyond Gerota s Fascia? (?T4).") GU Cancer Staging: Updates and Challenging Areas 13 th Current Issues in Surgical Pathology San Francisco, CA June 5, 2010 Jeffry P. Simko, PhD, MD Associate Professor Departments of Urology and Anatomic
GU Cancer Staging: Updates and Challenging Areas 13 th Current Issues in Surgical Pathology San Francisco, CA June 5, 2010 Jeffry P. Simko, PhD, MD Associate Professor Departments of Urology and Anatomic
5/8/2014. AJCC Stage Introduction and General Rules. Acknowledgements* Introduction. Melissa Pearson, CTR North Carolina Central Cancer Registry
 AJCC Stage Introduction and General Rules Linda Mulvihill Public Health Advisor NCRA Annual Meeting May 2014 National Center for Chronic Disease Prevention and Health Promotion Division of Cancer Prevention
AJCC Stage Introduction and General Rules Linda Mulvihill Public Health Advisor NCRA Annual Meeting May 2014 National Center for Chronic Disease Prevention and Health Promotion Division of Cancer Prevention
2014/2015 FCDS Educational Webcast Series
 2014/2015 FCDS Educational Webcast Series February 19, 2015 Steven Peace, CTR 2015 Update; Background, Anatomy, Risk Factors, Screening Guidelines, MPH Rules Review AJCC TNM 7 th ed, SS2000, CSv02.05 and
2014/2015 FCDS Educational Webcast Series February 19, 2015 Steven Peace, CTR 2015 Update; Background, Anatomy, Risk Factors, Screening Guidelines, MPH Rules Review AJCC TNM 7 th ed, SS2000, CSv02.05 and
COMPARATIVE ANALYSIS OF COLON AND RECTAL CANCERS IN SENTINEL LYMPH NODE MAPPING
 Trakia Journal of Sciences, Vol. 5, No. 1, pp 10-14, 2007 Copyright 2007 Trakia University Available online at: http://www.uni-sz.bg ISSN 1312-1723 Original Contribution COMPARATIVE ANALYSIS OF COLON AND
Trakia Journal of Sciences, Vol. 5, No. 1, pp 10-14, 2007 Copyright 2007 Trakia University Available online at: http://www.uni-sz.bg ISSN 1312-1723 Original Contribution COMPARATIVE ANALYSIS OF COLON AND
A215- Urinary bladder cancer tissues
 A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
Local staging of colon cancer: the current role of CT
 Local staging of colon cancer: the current role of CT Poster No.: C-2699 Congress: ECR 2018 Type: Authors: Keywords: DOI: Educational Exhibit A. P. Pissarra, R. R. Domingues Madaleno, C. Sanches, L. Curvo-
Local staging of colon cancer: the current role of CT Poster No.: C-2699 Congress: ECR 2018 Type: Authors: Keywords: DOI: Educational Exhibit A. P. Pissarra, R. R. Domingues Madaleno, C. Sanches, L. Curvo-
Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas.
 Protocol applies to all carcinomas of the exocrine pancreas.") Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist)
Pancreas (Exocrine) Protocol applies to all carcinomas of the exocrine pancreas. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist)
Colon and Rectum 5/1/14
 Collecting Cancer Data: Colon and Rectum 2013 2014 NAACCR Webinar Series May 1, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
Collecting Cancer Data: Colon and Rectum 2013 2014 NAACCR Webinar Series May 1, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants
The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
 30 th Congress of the European Society of Pathology Tuesday, September 11, 2018 The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
30 th Congress of the European Society of Pathology Tuesday, September 11, 2018 The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors
 Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors Pr Frédéric Bibeau, MD, PhD Head, Pathology department CHU de Caen, Normandy University, France ESMO preceptorship,
Early colorectal cancer Quality and rules for a good pathology report Histoprognostic factors Pr Frédéric Bibeau, MD, PhD Head, Pathology department CHU de Caen, Normandy University, France ESMO preceptorship,
Protocol for the Examination of Specimens From Patients With Invasive Carcinoma of the Breast
 Protocol for the Examination of Specimens From Patients With Invasive Carcinoma of the Breast Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
Protocol for the Examination of Specimens From Patients With Invasive Carcinoma of the Breast Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy
 Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
Greater Manchester & Cheshire Guidelines for Pathology Reporting of Oesophageal and Gastric Malignancy Authors: Dr Stephen Hayes, Dr David Bisset, Dr Gordon Armstrong, Dr Sue Pritchard 1. General Comments
Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum
 Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum Well-differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. Based on AJCC/UICC
Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum Well-differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. Based on AJCC/UICC
Protocol for the Examination of Specimens from Patients with Primary Carcinoma of the Colon and Rectum
 Protocol for the Examination of Specimens from Patients with Primary Carcinoma of the Colon and Rectum Well-differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. This modified NB
Protocol for the Examination of Specimens from Patients with Primary Carcinoma of the Colon and Rectum Well-differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. This modified NB
Completing the Puzzle AJCC TNM Staging Breast. Nicole Catlett, CTR 2017 Kentucky Cancer Registry Fall Conference, September 21 & 22, 2017
 Completing the Puzzle AJCC TNM Staging Breast Nicole Catlett, CTR 2017 Kentucky Cancer Registry Fall Conference, September 21 & 22, 2017 OBJECTIVES Understanding of Breast TNM staging Identify clinical
Completing the Puzzle AJCC TNM Staging Breast Nicole Catlett, CTR 2017 Kentucky Cancer Registry Fall Conference, September 21 & 22, 2017 OBJECTIVES Understanding of Breast TNM staging Identify clinical
Carcinoma of the Urinary Bladder Histopathology
 Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
12/7/2011. The reporting of colorectal cancer pathology: recent advances. Colorectal cancer resection specimens
 The reporting of colorectal cancer pathology: recent advances Professor Neil A Shepherd President, British Division of the IAP IAP-AD, Beirut, Lebanon 1 December 2011 Colorectal cancer resection specimens
The reporting of colorectal cancer pathology: recent advances Professor Neil A Shepherd President, British Division of the IAP IAP-AD, Beirut, Lebanon 1 December 2011 Colorectal cancer resection specimens
Procedures Needle Biopsy Transurethral Prostatic Resection Suprapubic or Retropubic Enucleation (Subtotal Prostatectomy) Radical Prostatectomy
 Radical Prostatectomy") Prostate Gland Protocol applies to invasive carcinomas of the prostate gland. Protocol web posting date: July 2006 Protocol effective date: April 2007 Based on AJCC/UICC TNM, 6 th edition Procedures Needle
Prostate Gland Protocol applies to invasive carcinomas of the prostate gland. Protocol web posting date: July 2006 Protocol effective date: April 2007 Based on AJCC/UICC TNM, 6 th edition Procedures Needle
Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum
 Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum Well-differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. Based on AJCC/UICC
Protocol for the Examination of Specimens From Patients With Primary Carcinoma of the Colon and Rectum Well-differentiated neuroendocrine neoplasms (carcinoid tumors) are not included. Based on AJCC/UICC
Michael T. Tetzlaff MD, PhD
 Update on American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma Emphasis on concise and accurate reporting of primary and metastatic melanoma for effective risk stratification
Update on American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma Emphasis on concise and accurate reporting of primary and metastatic melanoma for effective risk stratification
M etastasis to regional lymph nodes (LNs) is
 is") 327 REVIEW Nodal staging of colorectal carcinomas and sentinel nodes G Cserni... This review surveys the staging systems used for the classification of colorectal carcinomas, including the TNM system,
327 REVIEW Nodal staging of colorectal carcinomas and sentinel nodes G Cserni... This review surveys the staging systems used for the classification of colorectal carcinomas, including the TNM system,
The pathology of bladder cancer
 1 The pathology of bladder cancer Charles Jameson Introduction Carcinoma of the bladder is the seventh most common cancer worldwide [1]. It comprises 3.2% of all cancers, with an estimated 260 000 new
1 The pathology of bladder cancer Charles Jameson Introduction Carcinoma of the bladder is the seventh most common cancer worldwide [1]. It comprises 3.2% of all cancers, with an estimated 260 000 new
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS
 COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
COLLECTING CANCER DATA: STOMACH AND ESOPHAGUS 2017 2018 NAACCR WEBINAR SERIES Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Urinary Bladder, Ureter, and Renal Pelvis
 Urinary Bladder, Ureter, and Renal Pelvis Protocol applies to all carcinomas of the urinary bladder, ureter, and renal pelvis. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition Procedures
Urinary Bladder, Ureter, and Renal Pelvis Protocol applies to all carcinomas of the urinary bladder, ureter, and renal pelvis. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition Procedures
Surgical Issues in Melanoma
 Surgical Issues in Melanoma Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Director, Surgical Oncology Training Program Professor of Surgery John Wayne Cancer Institute Surgical
Surgical Issues in Melanoma Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Director, Surgical Oncology Training Program Professor of Surgery John Wayne Cancer Institute Surgical
Controversies in Breast Pathology ELENA PROVENZANO ADDENBROOKES HOSPITAL, CAMBRIDGE
 Controversies in Breast Pathology ELENA PROVENZANO ADDENBROOKES HOSPITAL, CAMBRIDGE Neoadjuvant Chemotherapy Indications: Management of locally advanced invasive breast cancers including inflammatory breast
Controversies in Breast Pathology ELENA PROVENZANO ADDENBROOKES HOSPITAL, CAMBRIDGE Neoadjuvant Chemotherapy Indications: Management of locally advanced invasive breast cancers including inflammatory breast
S1.04 Principal clinician. G1.01 Comments. G2.01 *Specimen dimensions (prostate) S2.02 *Seminal vesicles
 S2.02 *Seminal vesicles") Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
Uterine Cervix. Protocol applies to all invasive carcinomas of the cervix.
 Uterine Cervix Protocol applies to all invasive carcinomas of the cervix. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition and FIGO 2001 Annual Report Procedures Cytology (No Accompanying
Uterine Cervix Protocol applies to all invasive carcinomas of the cervix. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition and FIGO 2001 Annual Report Procedures Cytology (No Accompanying
Chapter 2 Staging of Breast Cancer
 Chapter 2 Staging of Breast Cancer Zeynep Ozsaran and Senem Demirci Alanyalı 2.1 Introduction Five decades ago, Denoix et al. proposed classification system (tumor node metastasis [TNM]) based on the dissemination
Chapter 2 Staging of Breast Cancer Zeynep Ozsaran and Senem Demirci Alanyalı 2.1 Introduction Five decades ago, Denoix et al. proposed classification system (tumor node metastasis [TNM]) based on the dissemination
Registrar s Guide to Chapter 1, AJCC Seventh Edition. Overview. Learning Objectives. Describe intent and purpose of AJCC staging
 Registrar s Guide to Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers for Disease Control
Registrar s Guide to Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement Number DP13-1310 from The Centers for Disease Control
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
3/23/2017. Disclosure of Relevant Financial Relationships. Pathologic Staging Updates in Breast Cancer. Pathologic Staging Updates Breast Cancer
 Pathologic Staging Updates in Breast Cancer Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME
Pathologic Staging Updates in Breast Cancer Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education Committee) in a position to influence or control the content of CME
Retinoblastoma. Protocol applies to retinoblastoma only.
 Retinoblastoma Protocol applies to retinoblastoma only. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist) Biopsy (No Accompanying
Retinoblastoma Protocol applies to retinoblastoma only. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition Procedures Cytology (No Accompanying Checklist) Biopsy (No Accompanying
Overview. Collecting Cancer Data: Colon 11/5/2009. Collecting Cancer Data: NAACCR Webinar Series 1. Agenda NAACCR WEBINAR SERIES
 Collecting Cancer Data: Colon 11/5/2009 Collecting Cancer Data: Colon/Rectum/Appendix NAACCR 2009 2010 WEBINAR SERIES Agenda Overview Treatment MP/H Rules CSv2 2 Overview Colon/Rectum/Appendix 2009 2010
Collecting Cancer Data: Colon 11/5/2009 Collecting Cancer Data: Colon/Rectum/Appendix NAACCR 2009 2010 WEBINAR SERIES Agenda Overview Treatment MP/H Rules CSv2 2 Overview Colon/Rectum/Appendix 2009 2010
UICC 8 th Edition Errata 25 th of May 2018
 UICC 8 th Edition Errata 25 th of May 2018 ions are in italics Head and Neck Tumours Page 19 Oral Cavity T2 T3 T4a Tumour 2 cm or less in greatest dimension and more than 5 mm but no more than 10 mm depth
UICC 8 th Edition Errata 25 th of May 2018 ions are in italics Head and Neck Tumours Page 19 Oral Cavity T2 T3 T4a Tumour 2 cm or less in greatest dimension and more than 5 mm but no more than 10 mm depth
UICC TNM 8 th Edition Errata
 UICC TNM 8 th Edition Errata ions are in italics Head and Neck Tumours Pages 20, p27, p34, p38, p41, and p49 ly pn2a Metastasis in a single ipsilateral lymph node, less than 3cm in greatest dimension with
UICC TNM 8 th Edition Errata ions are in italics Head and Neck Tumours Pages 20, p27, p34, p38, p41, and p49 ly pn2a Metastasis in a single ipsilateral lymph node, less than 3cm in greatest dimension with
Michael T. Tetzlaff MD, PhD
 American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
American Joint Cancer Committee (AJCC) staging system for primary cutaneous melanoma (8 th Edition) and principles of sentinel lymph node evaluation Emphasis on concise and accurate reporting of primary
Disclosures. Outline. What IS tumor budding?? Tumor Budding in Colorectal Carcinoma: What, Why, and How. I have nothing to disclose
 Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
The tumor-node-metastasis (TNM) system is
 system is") LUNG CARCINOMA STAGING PROBLEMS Philip T. Cagle, MD a,b, * KEYWORDS Lung Carcinoma Staging Tumor-node-metastasis TNM system ABSTRACT The tumor-node-metastasis (TNM) system is the most commonly used staging
LUNG CARCINOMA STAGING PROBLEMS Philip T. Cagle, MD a,b, * KEYWORDS Lung Carcinoma Staging Tumor-node-metastasis TNM system ABSTRACT The tumor-node-metastasis (TNM) system is the most commonly used staging
SEER Summary Stage Still Here!
 SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
How much colon should be resected?
 Colon Cancer Surgical Standard of Care and Operative Techniques Madhulika G. Varma MD Professor and Chief Section of Colorectal Surgery University of California, San Francisco How much colon should be
Colon Cancer Surgical Standard of Care and Operative Techniques Madhulika G. Varma MD Professor and Chief Section of Colorectal Surgery University of California, San Francisco How much colon should be
malignant polyp Daily Challenges in Digestive Endoscopy for Endoscopists and Endoscopy Nurses BSGIE Annual Meeting 18/09/2014 Mechelen
 Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Plan Incidental finding of a malignant polyp 1. What is a polyp malignant? 2. Role of the pathologist and the endoscopist 3. Quantitative and qualitative risk assessment 4. How to decide what to do? Hubert
Protocol for the Examination of Specimens From Patients With Merkel Cell Carcinoma of the Skin
 Protocol for the Examination of Specimens From Patients With Merkel Cell Carcinoma of the Skin Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
Protocol for the Examination of Specimens From Patients With Merkel Cell Carcinoma of the Skin Version: Protocol Posting Date: June 2017 Includes ptnm requirements from the 8 th Edition, AJCC Staging Manual
Explaining Blanks and X, Ambiguous Terminology and Support for AJCC Staging
 Explaining Blanks and X, Ambiguous Terminology and Support for AJCC Staging Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement
Explaining Blanks and X, Ambiguous Terminology and Support for AJCC Staging Donna M. Gress, RHIT, CTR Validating science. Improving patient care. This presentation was supported by the Cooperative Agreement
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm