6/5/2010. Renal vein invasion & Capsule Penetration (T3a) Adrenal Gland involvement (T4 vs. M1) Beyond Gerota s Fascia? (?T4).
|
|
|
- Clyde Abel Davis
- 5 years ago
- Views:
Transcription

 from recurrence stage (r) (m) for multiple primary tumors in same organ Added")
1 GU Cancer Staging: Updates and Challenging Areas 13 th Current Issues in Surgical Pathology San Francisco, CA June 5, 2010 Jeffry P. Simko, PhD, MD Associate Professor Departments of Urology and Anatomic Pathology AJCC Cancer Staging manual 7 th Edition Effective 1/1/2010 TNM Helpdesks: Staging Changes: General ptnmrglv ptn (Chapter 1) pmx eliminated, just ptn ( can have pm1) R category (margin status) still present, L,V categories dropped. R0= excised, R1= residual microscopic, R2 = macroscopic Special classifiers are clarified neoadjuvant stage (y) from recurrence stage (r) (m) for multiple primary tumors in same organ Added Prognostic Features (nonanatomic) e.g. Multigene signature for Breast. PSA for prostate Goal: Improve Staging Accuracy Kidney Renal vein invasion & Capsule Penetration (T3a) Adrenal Gland involvement (T4 vs. M1) Beyond Gerota s Fascia? (?T4). Bladder Tumors (renal pelvis, ureter, urethra) Invasion or not? (Tis/Ta vs. T1). Muscle invasion (T1 vs. T2) Beyond the bladder (T2 vs. T3 vs. T4) Prostate Gland Prostate Gland Bladder neck invasion (T3a or T4?). Capsule Penetration (T2 vs. T3a) 1
 Adrenal gland involvement Direct extension into adrenal = T4 Tumor deposit in adrenal = M1 Renal Vein involvement: Changed from T3b to T3a Node staging simplified (N0 vs.")
2 Kidney: Staging Changes T2 split T2a ( 7cm < T <= 10cm) vs. T2b ( > 10 cm) Adrenal gland involvement Direct extension into adrenal = T4 Tumor deposit in adrenal = M1 Renal Vein involvement: Changed from T3b to T3a Node staging simplified (N0 vs. N1) Kidney: Tumor type aids in staging Primary renal tumors are Expansile masses Pushing, compressing & crushing Cortex rather than medulla or pelvis Encapsulated or pseudo-encapsulated! exceptions = collecting duct & medullary CA Urothelial carcinomas are infiltrative (as are collecting duct & medullary CA) Replacing rather than pushing No capsule! Renal Pelvis or Medulla rather than Cortex? In situ vs. invasive tumor 2

3 3




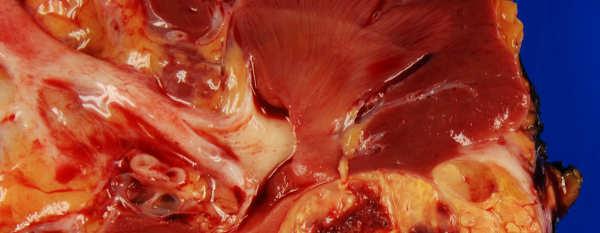
4 Problem area: Gross vessel invasion Tumor in any muscle-walled vessel T3a (Exception: Vena cava T3b or c) Gross Evaluation: Open renal vessels Microscopic confirmation: Trichrome and Elastin stains helpful 4
.")

. Fibrin vs.")
5 CD 31 Problem areas: Tumor thrombus Surgeon / imaging for staging (pt3a, b or c). Margin status: Tumor infiltrating at margin. (Patients disqualified from clinical trials) Histologic confirmation (thrombus type). Fibrin vs. xanthogranulomatous clot vs. tumor 5

 Penetration")
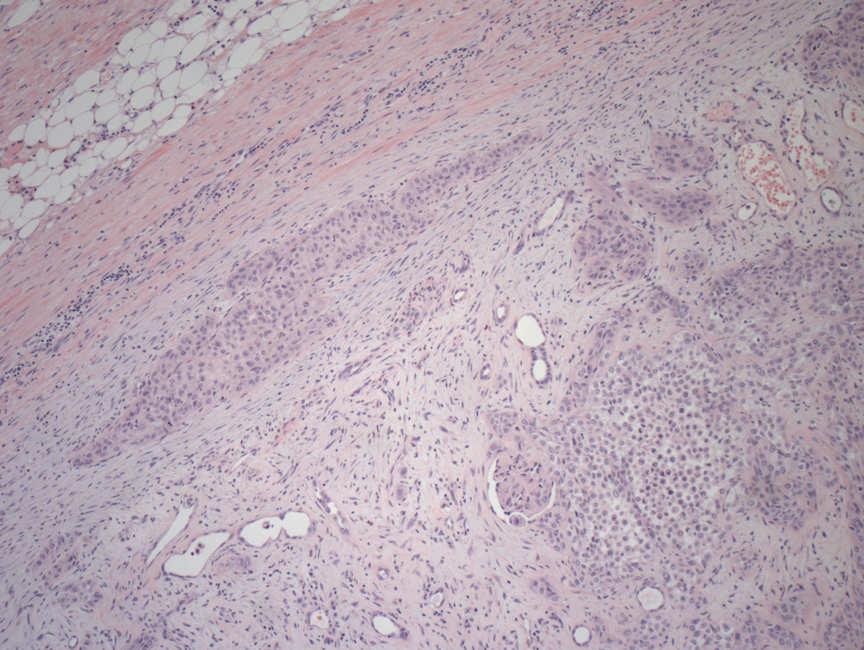
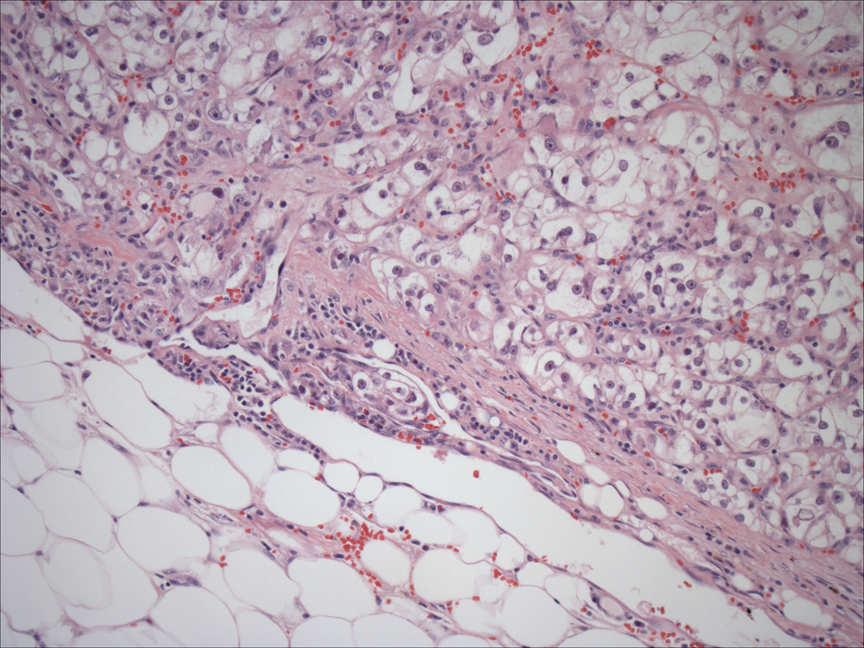
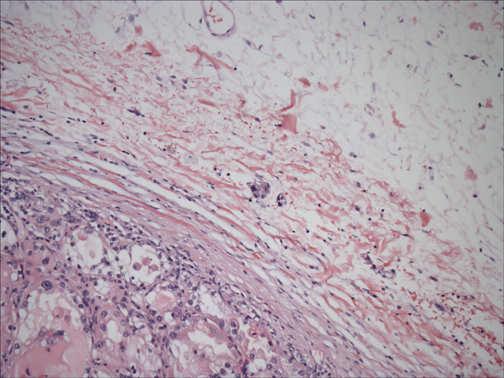
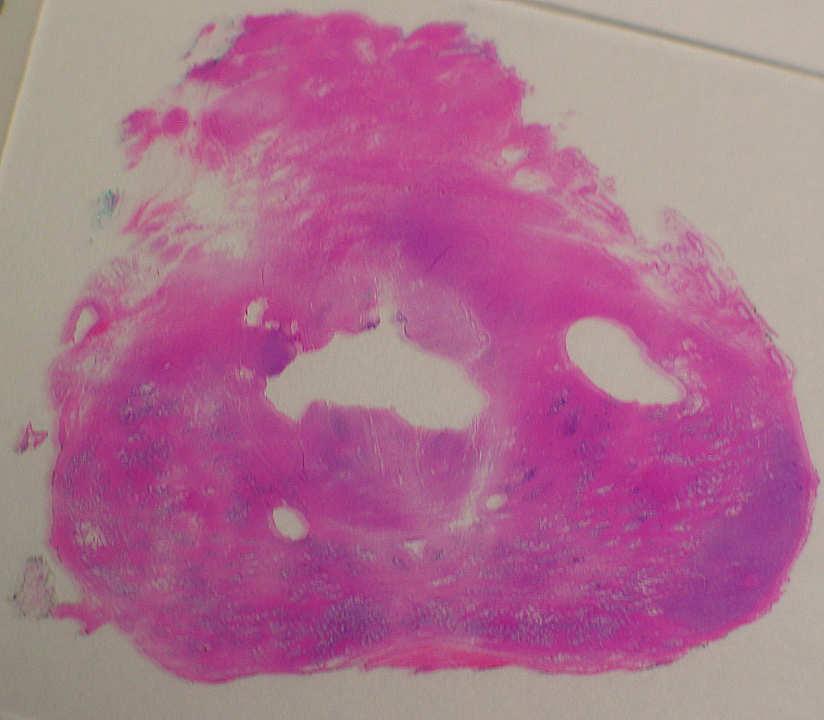
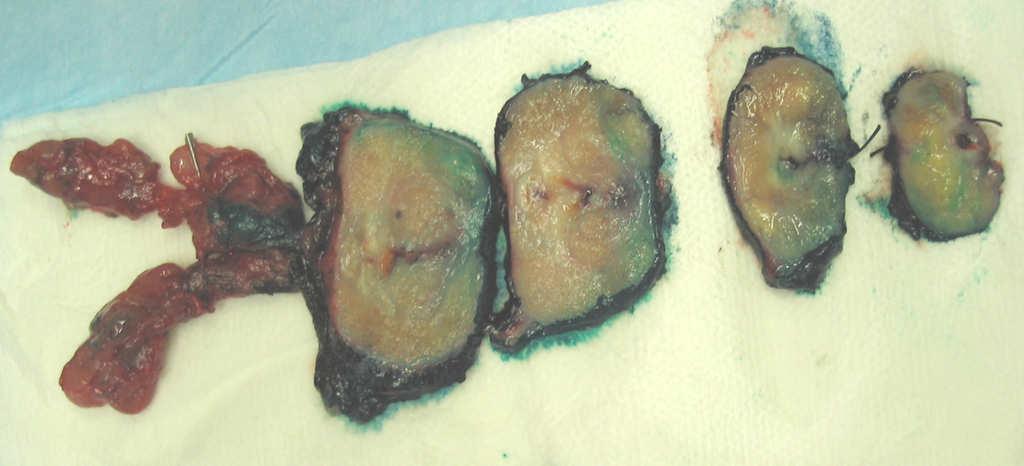
6 Problem area: Capsular Penetration (?pt3a) Problem area: Capsular Penetration 6




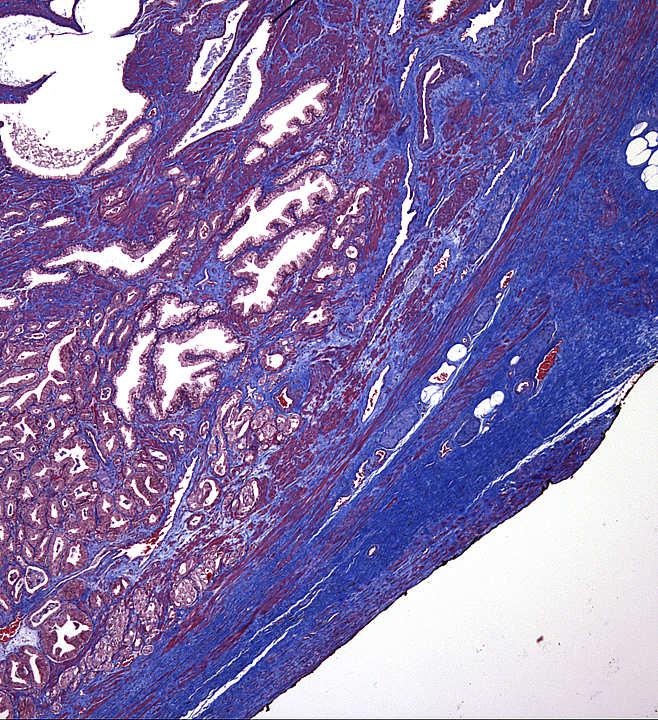
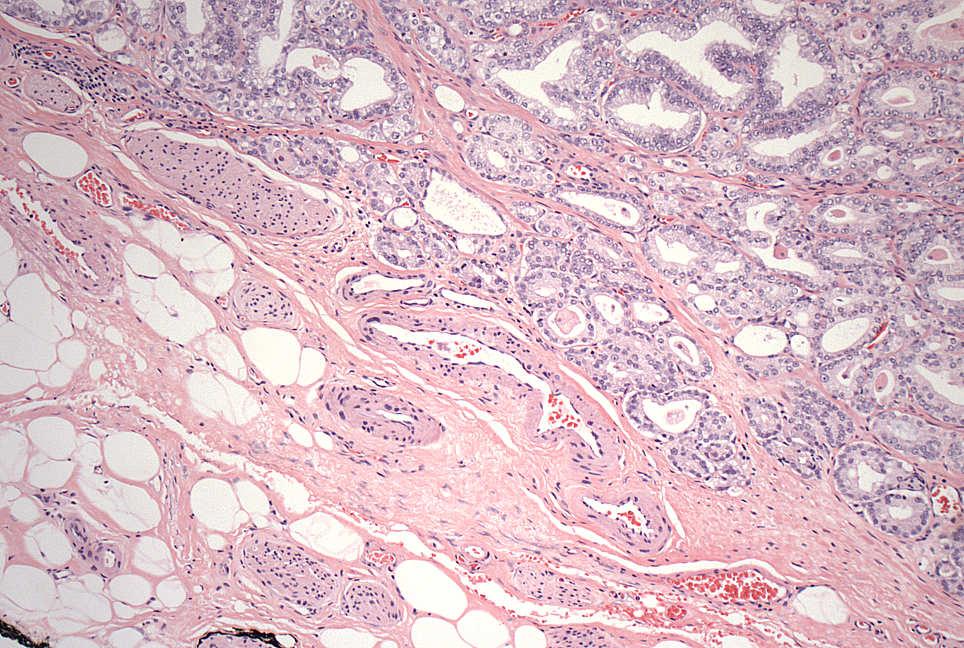
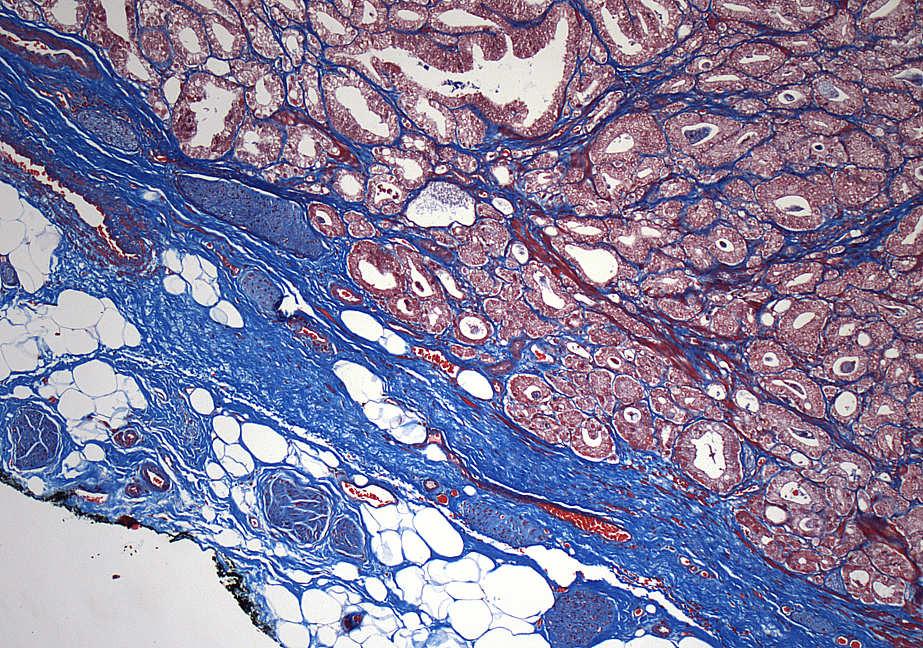
7 Capsular Penetration Problem area: Kidney Capsular Penetration Capsular Penetration Capsular Penetration Capsule: LET THE GROSS GUIDE YOU Fat mobile over tumor No fat invasion Fat falls off over tumor No fat invasion Take sections where fat adherent to kidney. Renal sinus involvement: more difficult Fat naturally immobile Take multiple sections Look for benign tubules in capsule wall? More likely vascular invasion? (Trichrome stain) 7

8 Capsular Penetration Capsular Penetration 8


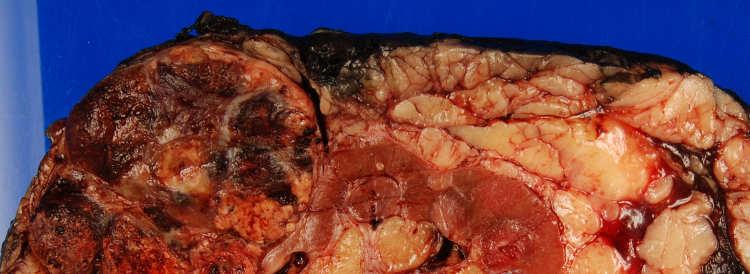
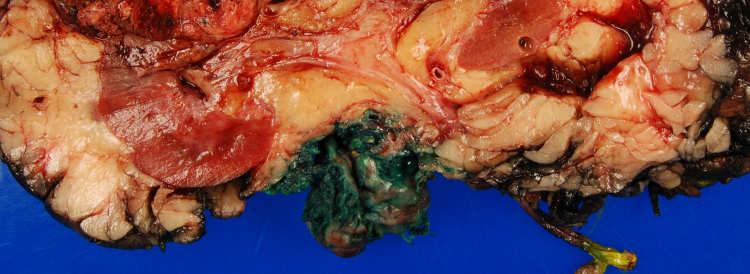
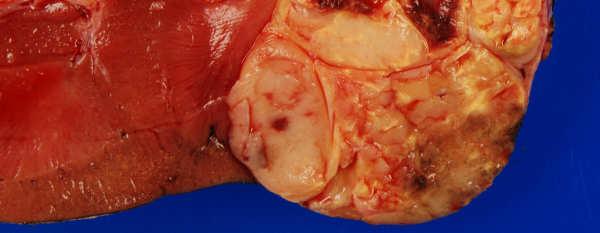
9 Problem area:? pt4 (Gerota s fascia) 9
 Gerota s Fascia Often the margin of a nephrectomy specimen Noticeable when removing kidney at autopsy Other organs in specimen?")

10 Problem area:? T4? (Through Gerota s fascia?) Gerota s Fascia Often the margin of a nephrectomy specimen Noticeable when removing kidney at autopsy Other organs in specimen? Likely T4. (Liver, spleen, pancreas, bowel, skeletal musc.) Surgeon can tell easier than pathologist! Problem area:? T4? (Adrenal gland invasion) Is it adrenal cortex or a renal tumor? Immunohistochemical stains CA IX in CCRCC; Melan-A, Inhibin in Adrenal PAX-2 and RCC Ag can be + in Adrenal CA! Direct extension pt4 Tumor deposit in Adrenal pm1 10




11 6/5/2010 Adrenal Inhibin IHC Cortical Rests: Melan-A Adrenal Cortical Rests Adrenal Cortical Rests in Kidney RCC Ag IHC 11


 from invasive")
12 Renal Pelvis, Ureters, Urethra NO staging changes Problem Area: Kidney / Renal pelvis Kidney involvement by Pelvic Urothelial CA Discriminate in situ (ptis) from invasive tumor (pt3)! 12



13 Kidney involvement by urothelial CA? Is tumor confined to tubules? Tis CIS colonizing tubules / glomeruli Expansion of native structures Adjacent stroma without tumor At most, small masses / apparent small sheets Tubule destruction? T3 Tumor around native structures Desmoplasia Large tumor cell sheets / masses Uninvolved structures surrounded by tumor 13
 N1: A single positive node, primary drainage N2: Two or more positive in primary drainage N3: Common iliac nodes involved M1: Other nodes involved (e.g. para-aortic) Near Future: Extranodal Extension?")
14 Urinary Bladder: Staging Changes T4a: Directly into prostate from bladder tumor Extra-nodal extension (bladder) 1.0 Disease-specific survival p<0.001 Nodal classification (Node location) N1: A single positive node, primary drainage N2: Two or more positive in primary drainage N3: Common iliac nodes involved M1: Other nodes involved (e.g. para-aortic) Near Future: Extranodal Extension? p<0.001 Without ENE (n=79) Without ENE (n=79) With ENE (n=80) With ENE (n=80) Years (R Seiler, et al., 99 th USCAP Meeting 2010, Wash. D.C., Abstract #975) (R Seiler, et al., 99 th USCAP Meeting 2010, Wash. D.C., Abstract #975) Problem Areas: Invasive vs. in situ (pta / ptis VS. pt1) Problem Area: Is there muscularis propria invasion?? Muscularis Propria Invasion (pt1b vs. T2) BIG differences in Rx for these diagnoses!!! Tis intravesicle Rx, T1 many options, T2 definitive Rx (cystectomy). Difficult and important area Many times cannot be certain Should always report if muscularis propria present or not. Should always report if smooth muscle involved by tumor and indicate type if possible Immunohistochemistry: Actin, smoothelin 14



15 Epstein, et al., Bladder Biopsy Interpretation, LWW 2004 Epstein, et al., Bladder Biopsy Interpretation, LWW 2004 Problem Area: Tumor in pericystic fat? (pt3) Fat can be present in Urinary bladder wall Tumor must be seen beyond muscle bundles to be certain T3a Epstein, et al., Bladder Biopsy Interpretation, LWW

?")


16 Problem Area: Tumor in pericystic fat? (T2b vs. T3)? T3a or T2b with LVI? Problem Area: Tumor in pericystic fat? Image of fat in smooth muscle 16
 In situ extension into prostate NOT T4!")
17 Problem Area: Bladder tumor into prostate (T4a)? In situ vs. invasive tumor? Bladder smooth muscle (T2) vs. directly into prostate / vagina smooth muscle (pt4a) In situ extension into prostate NOT T4!!! Grade bladder and prostate tumors separately Prostate T2 Bladder T2 17
 Direct into prostate stroma T4a Via in situ spread along urethra: Two tumors Via in situ spread along urethra: Two tumors Stage bladder tumor in urinary bladder")
18 Bladder stage T2 Bladder stage T4a Prostate stages Prostate Tis Bladder tumor into prostate gland (T4a vs. other) Direct into prostate stroma T4a Via in situ spread along urethra: Two tumors Via in situ spread along urethra: Two tumors Stage bladder tumor in urinary bladder Stage tumor in prostate separately (prostatic urethral tumor). 18

19 Prostate Gland: Staging Changes Direct extension of tumor into Urinary Bladder has been clarified Microscopic urinary bladder invasion T3a Macroscopic urinary bladder invasion T4 Prostate T3a 19

! Trichrome useful! Ohori, et. al, Mod Pathol (2004). Ohori, et. al, Mod Pathol (2004). 20")
20 Problem area: EPE (extra-prostatic extension) EPE Rules: NO capsule at apex Skeletal muscle invasion not helpful Just can report margin status Microscopic tumor in bladder musc = T3a Must see tumor in fat!?!?! Fat extremely rare in benign prostate Desmoplastic fibrosis? (subtle)! Trichrome useful! Ohori, et. al, Mod Pathol (2004). Ohori, et. al, Mod Pathol (2004). 20
.")


21 Ohori, et. al, Mod Pathol (2004). Evans, et. al, Am J Srug Pathol 32: (2008). Problem area: EPE Tumor in fat, T3a Tumor expanding the capsule Tumor in desmoplasia T3a? Why can t capsule be stretched and not penetrated? Can use trichrome to discriminate Smooth muscle between fat & Tumor T2 No smooth muscle between T3a Evans, et. al, Am J Srug Pathol 32: (2008). 21
22 22
23 Prostate: Surgical Margins Tumor touching ink margin +? Area of EPE or is it a cut into prostate? Length of positive margin, Gleason grade Tumor not on ink margin clear Report distance for EPE tumor. Do not report distance if T2 (might make comment if just a few fibroblasts from ink). Ohori, et. al, Mod Pathol (2004). Summary General changes (Chapter 1 of manual) TNM helpdesks on the web. Kidney (guidance from the gross) Vein invasion, fat invasion (special stains) Bladder (pelvis, ureters, urethra) unique issues at interface of all stages In situ vs. invasion of prostate (kidney). Prostate Bladder invasion, EPE, and margin status Ohori, et. al, Mod Pathol (2004). 23



24 That s all Folks!!!!! 24
TOPICS FOR DISCUSSION
 INTERNATIONAL SOCIETY OF UROLOGIC PATHOLOGY PATHOLOGIC STAGING OF SELECT UROLOGIC MALIGNANCIES Mahul B. Amin, MD Professor and Chairman Pathology and Laboratory Medicine Cedars-Sinai Medical Center Los
INTERNATIONAL SOCIETY OF UROLOGIC PATHOLOGY PATHOLOGIC STAGING OF SELECT UROLOGIC MALIGNANCIES Mahul B. Amin, MD Professor and Chairman Pathology and Laboratory Medicine Cedars-Sinai Medical Center Los
Bladder Case 1 SURGICAL PATHOLOGY REPORT. Procedure: Cystoscopy, transurethral resection of bladder tumor (TURBT)
") Bladder Case 1 February 17, 2007 Specimen (s) received: Bladder Tumor Pre-operative Diagnosis: Bladder Cancer Post operative Diagnosis: Bladder Cancer Procedure: Cystoscopy, transurethral resection of
Bladder Case 1 February 17, 2007 Specimen (s) received: Bladder Tumor Pre-operative Diagnosis: Bladder Cancer Post operative Diagnosis: Bladder Cancer Procedure: Cystoscopy, transurethral resection of
Kidney Case 1 SURGICAL PATHOLOGY REPORT
 Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
Kidney Case 1 Surgical Pathology Report February 9, 2007 Clinical History: This 45 year old woman was found to have a left renal mass. CT urography with reconstruction revealed a 2 cm medial mass which
I have no financial relationships to disclose. I WILL NOT include discussion of investigational or off-label use of a product in my presentation.
 Prostate t Cancer MR Report Disclosure Information Vikas Kundra, M.D, Ph.D. I have no financial relationships to disclose. I WILL NOT include discussion of investigational or off-label use of a g product
Prostate t Cancer MR Report Disclosure Information Vikas Kundra, M.D, Ph.D. I have no financial relationships to disclose. I WILL NOT include discussion of investigational or off-label use of a g product
UICC TNM 8 th Edition Errata
 UICC TNM 8 th Edition Errata ions are in italics Head and Neck Tumours Pages 20, p27, p34, p38, p41, and p49 ly pn2a Metastasis in a single ipsilateral lymph node, less than 3cm in greatest dimension with
UICC TNM 8 th Edition Errata ions are in italics Head and Neck Tumours Pages 20, p27, p34, p38, p41, and p49 ly pn2a Metastasis in a single ipsilateral lymph node, less than 3cm in greatest dimension with
Carcinoma of the Urinary Bladder Histopathology
 Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Urinary Bladder Histopathology Reporting Proforma (Radical & Partial Cystectomy, Cystoprostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Pathologic Assessment of Invasion in TUR Specimens. A. Lopez-Beltran. T1 (ct1)
") Pathologic Assessment of Invasion in TUR Specimens A. Lopez-Beltran T1 (ct1) 1 Prognostic factors for progression/invasive disease Ta,T1,CIS- NMIBC :TNM 2017 ESSENTIAL: Grade T stage CIS Number of lesions
Pathologic Assessment of Invasion in TUR Specimens A. Lopez-Beltran T1 (ct1) 1 Prognostic factors for progression/invasive disease Ta,T1,CIS- NMIBC :TNM 2017 ESSENTIAL: Grade T stage CIS Number of lesions
UICC TNM 8 th Edition Errata
 UICC TNM 8 th Edition Errata ions are in italics Page 28 Oropharynx p16 positive Pathological Stage II,T2 N2 M0 T3 N0,N1 M0 Stage II,T2 N2 M0 T3,T4 N0,N1 M0 Page 61 Oesophagus Adenocarcinoma Pathological
UICC TNM 8 th Edition Errata ions are in italics Page 28 Oropharynx p16 positive Pathological Stage II,T2 N2 M0 T3 N0,N1 M0 Stage II,T2 N2 M0 T3,T4 N0,N1 M0 Page 61 Oesophagus Adenocarcinoma Pathological
Update on staging colorectal carcinoma, the 8 th edition AJCC. General overview of staging. When is staging required? 11/1/2017
 Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Update on staging colorectal carcinoma, the 8 th edition AJCC Dale C. Snover, MD November 3, 2017 General overview of staging Reason for uniform staging Requirements to use AJCC manual and/or CAP protocols
Urinary Bladder, Ureter, and Renal Pelvis
 Urinary Bladder, Ureter, and Renal Pelvis Protocol applies to all carcinomas of the urinary bladder, ureter, and renal pelvis. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition Procedures
Urinary Bladder, Ureter, and Renal Pelvis Protocol applies to all carcinomas of the urinary bladder, ureter, and renal pelvis. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition Procedures
Prostate cancer staging and datasets: The Nitty-Gritty. What determines our pathological reports? 06/07/2018. Dan Berney Maastricht 2018
 Prostate cancer staging and datasets: The Nitty-Gritty What determines our pathological reports? Dan Berney Maastricht 2018 Biopsy reporting. How not to do it. The TNM 8 th edition. Changes good and bad
Prostate cancer staging and datasets: The Nitty-Gritty What determines our pathological reports? Dan Berney Maastricht 2018 Biopsy reporting. How not to do it. The TNM 8 th edition. Changes good and bad
Carcinoma of the Renal Pelvis and Ureter Histopathology
 Carcinoma of the Renal Pelvis and Ureter Histopathology Reporting Proforma (NEPHROURETERECTOMY AND URETERECTOMY) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
Carcinoma of the Renal Pelvis and Ureter Histopathology Reporting Proforma (NEPHROURETERECTOMY AND URETERECTOMY) Includes the International Collaboration on Cancer reporting dataset denoted by * Family
The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
 30 th Congress of the European Society of Pathology Tuesday, September 11, 2018 The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
30 th Congress of the European Society of Pathology Tuesday, September 11, 2018 The Depth of Tumor Invasion is Superior to 8 th AJCC/UICC Staging System to Predict Patients Outcome in Radical Cystectomy.
25 TH ICRO DEHRADUN STAGING OF GENITOURINARY MALIGNANCIES
 25 TH ICRO DEHRADUN STAGING OF GENITOURINARY MALIGNANCIES SPEAKER DR DEEPAK ABROL CLINICAL ONCOLOGIST JAND K HEALTH SERVICES CONSULTANT ONCOLOGIST MAHARISHI DAYANAND HOSPITAL AND MEDICAL RESEARCH CENTER
25 TH ICRO DEHRADUN STAGING OF GENITOURINARY MALIGNANCIES SPEAKER DR DEEPAK ABROL CLINICAL ONCOLOGIST JAND K HEALTH SERVICES CONSULTANT ONCOLOGIST MAHARISHI DAYANAND HOSPITAL AND MEDICAL RESEARCH CENTER
3/23/2017. Significant Changes in Prostate Cancer Classification, Grading, Staging and Reporting. Disclosure of Relevant Financial Relationships
 Disclosure of Relevant Financial Relationships Staging and Reporting of Prostate Cancer: Major Changes in 8 th Edition AJCC Staging and CAP Cancer Checklists USCAP requires that all planners (Education
Disclosure of Relevant Financial Relationships Staging and Reporting of Prostate Cancer: Major Changes in 8 th Edition AJCC Staging and CAP Cancer Checklists USCAP requires that all planners (Education
Definition of Synoptic Reporting
 Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
Definition of Synoptic Reporting The CAP has developed this list of specific features that define synoptic reporting formatting: 1. All required cancer data from an applicable cancer protocol that are
A215- Urinary bladder cancer tissues
 A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
A215- Urinary bladder cancer tissues (formalin fixed) For research use only Specifications: No. of cases: 45 Tissue type: Urinary bladder cancer tissues No. of spots: 2 spots from each cancer case (90
Prognostic factors of genitourinary tumors: Do we have to care?
 Prognostic factors of genitourinary tumors: Do we have to care? Jae Y. Ro, MD, PhD Professor and Director of Surgical Pathology The Methodist Hospital, Weill Medical College of Cornell University, Houston,
Prognostic factors of genitourinary tumors: Do we have to care? Jae Y. Ro, MD, PhD Professor and Director of Surgical Pathology The Methodist Hospital, Weill Medical College of Cornell University, Houston,
Staging Challenges in Lower GI Cancers. Disclosure of Relevant Financial Relationships. AJCC 8 th edition and CAP protocol updates
 Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Staging Challenges in Lower GI Cancers Sanjay Kakar, MD University of California, San Francisco March 05, 2017 Disclosure of Relevant Financial Relationships USCAP requires that all planners (Education
Staging and Grading Last Updated Friday, 14 November 2008
 Staging and Grading Last Updated Friday, 14 November 2008 There is a staging graph below Blood in the urine is the most common indication that something is wrong. Often one will experience pain or difficulty
Staging and Grading Last Updated Friday, 14 November 2008 There is a staging graph below Blood in the urine is the most common indication that something is wrong. Often one will experience pain or difficulty
The pathology of bladder cancer
 1 The pathology of bladder cancer Charles Jameson Introduction Carcinoma of the bladder is the seventh most common cancer worldwide [1]. It comprises 3.2% of all cancers, with an estimated 260 000 new
1 The pathology of bladder cancer Charles Jameson Introduction Carcinoma of the bladder is the seventh most common cancer worldwide [1]. It comprises 3.2% of all cancers, with an estimated 260 000 new
Colorectal Cancer Structured Pathology Reporting Proforma DD MM YYYY
 Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Colorectal Cancer Structured Pathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.03). Family name Given name(s) Date of birth DD MM YYYY S1.02 Clinical details
Urology An introduction to cut up DR J R GOEPEL
 Urology An introduction to cut up DR J R GOEPEL Overview Principles Individual organs Small pieces Partial resections Whole organs Data recording and data sets Principles You are working for the patient
Urology An introduction to cut up DR J R GOEPEL Overview Principles Individual organs Small pieces Partial resections Whole organs Data recording and data sets Principles You are working for the patient
Staging for Residents, Nurses, and Multidisciplinary Health Care Team
 Staging for Residents, Nurses, and Multidisciplinary Health Care Team Donna M. Gress, RHIT, CTR Validating science. Improving patient care. Learning Objectives Introduce the concept and history of stage
Staging for Residents, Nurses, and Multidisciplinary Health Care Team Donna M. Gress, RHIT, CTR Validating science. Improving patient care. Learning Objectives Introduce the concept and history of stage
Urinary Bladder, Ureter, and Renal Pelvis
 Urinary Bladder, Ureter, and Renal Pelvis Protocol applies to all carcinomas of the urinary bladder, ureter, and renal pelvis. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition Procedures
Urinary Bladder, Ureter, and Renal Pelvis Protocol applies to all carcinomas of the urinary bladder, ureter, and renal pelvis. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition Procedures
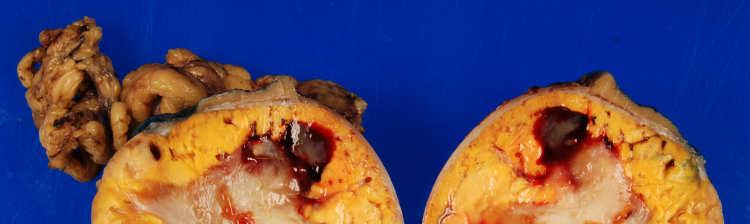
RENAL CELL CARCINOMA 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a Pseud
 GENITOURINARY PATHOLOGY Kathleen M. O Toole Toole, M.D. RENAL CELL CARCINOMA 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a
GENITOURINARY PATHOLOGY Kathleen M. O Toole Toole, M.D. RENAL CELL CARCINOMA 2 to 3% of All New Visceral Cancers Peak Incidence is 6th Decade M:F = 2:1 Grossly is a Bright Yellow, Necrotic Mass with a
3. Guidelines for Reporting Bladder Cancer, Prostate Cancer and Renal Tumours
 60 3. Guidelines for Reporting Bladder Cancer, Prostate Cancer and Renal Tumours Compilation and editing and of this volume: Prof. Chandu de Silva (Consultant Histopathologist) List of contributors Consultant
60 3. Guidelines for Reporting Bladder Cancer, Prostate Cancer and Renal Tumours Compilation and editing and of this volume: Prof. Chandu de Silva (Consultant Histopathologist) List of contributors Consultant
Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04
 Presentation Outline Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 General Information
Presentation Outline Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 General Information
Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04
 Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 1 Steven Peace, BS, CTR Susan Smith
Genitourinary Neoplasms Updated for 2012 Requirements and CSv02.04 X:\FCDS_PUB\wwwroot\downloads\Teleconfere nces\2013 FCDS Educational Webcast Series February 28, 2013 1 Steven Peace, BS, CTR Susan Smith
Collection of Recorded Radiotherapy Seminars
 IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
IAEA Human Health Campus Collection of Recorded Radiotherapy Seminars http://humanhealth.iaea.org Conservative Treatment of Invasive Bladder Cancer Luis Souhami, MD Professor Department of Radiation Oncology
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
You Want ME to Stage that Case???
 You Want ME to Stage that Case??? Jayne Holubowsky, CTR, Director, Virginia Cancer Registry 2 nd DelMarVa-DC Regional Conference October 11, 2018 What s New in the AJCC 8 th Edition Objectives Explain
You Want ME to Stage that Case??? Jayne Holubowsky, CTR, Director, Virginia Cancer Registry 2 nd DelMarVa-DC Regional Conference October 11, 2018 What s New in the AJCC 8 th Edition Objectives Explain
Coordinate Expression of Cytokeratins 7 and 20 in Prostate Adenocarcinoma and Bladder Urothelial Carcinoma
 Anatomic Pathology / CYTOKERATINS 7 AND 20 IN PROSTATE AND BLADDER CARCINOMAS Coordinate Expression of Cytokeratins 7 and 20 in Prostate Adenocarcinoma and Bladder Urothelial Carcinoma Nader H. Bassily,
Anatomic Pathology / CYTOKERATINS 7 AND 20 IN PROSTATE AND BLADDER CARCINOMAS Coordinate Expression of Cytokeratins 7 and 20 in Prostate Adenocarcinoma and Bladder Urothelial Carcinoma Nader H. Bassily,
Jesse K. McKenney, MD
 Jesse K. McKenney, MD Outline Microscopic anatomy of the urinary bladder Diagnosing invasion Subtle patterns (variants) of carcinoma Clinically important variants of carcinoma Microanatomy of Bladder Initial
Jesse K. McKenney, MD Outline Microscopic anatomy of the urinary bladder Diagnosing invasion Subtle patterns (variants) of carcinoma Clinically important variants of carcinoma Microanatomy of Bladder Initial
URINARY SYSTEM. These organs lie posterior or inferior to the. (membrane).
.") URINARY SYSTEM I. INTRODUCTION Each kidney is made up of about a million tiny tubules called nephrons. Each nephron individually filters the blood and makes urine and it does the job completely, from start
URINARY SYSTEM I. INTRODUCTION Each kidney is made up of about a million tiny tubules called nephrons. Each nephron individually filters the blood and makes urine and it does the job completely, from start
A Practicum Approach to CS: GU Prostate, Testis, Bladder, Kidney, Renal Pelvis. Jennifer Ruhl, RHIT, CCS, CTR Janet Stengel, RHIA, CTR
 A Practicum Approach to CS: GU Prostate, Testis, Bladder, Kidney, Renal Pelvis Jennifer Ruhl, RHIT, CCS, CTR Janet Stengel, RHIA, CTR Survey Questions and Answers 250 Responses 2 Question #1 A gentleman
A Practicum Approach to CS: GU Prostate, Testis, Bladder, Kidney, Renal Pelvis Jennifer Ruhl, RHIT, CCS, CTR Janet Stengel, RHIA, CTR Survey Questions and Answers 250 Responses 2 Question #1 A gentleman
INTRADUCTAL LESIONS OF THE PROSTATE. Jonathan I. Epstein
 INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
INTRADUCTAL LESIONS OF THE PROSTATE Jonathan I. Epstein Topics Prostatic intraepithelial neoplasia (PIN) Intraductal adenocarcinoma (IDC-P) Intraductal urothelial carcinoma Ductal adenocarcinoma High Prostatic
Male genital tract tumors. SiCA. Division of Urology, Department of Surgery, Faculty of Medicine Siriraj Hospital.
 Male genital tract tumors Division of Urology, Department of Surgery, Faculty of Medicine Siriraj Hospital. adenocarcinoma Prostate Cancer most common male cancer in western countries more detected in
Male genital tract tumors Division of Urology, Department of Surgery, Faculty of Medicine Siriraj Hospital. adenocarcinoma Prostate Cancer most common male cancer in western countries more detected in
CHAPTER 25 URINARY. Urinary system. Kidneys 2 Ureters 2 Urinary Bladder 1 Urethra 1. functions
 CHAPTER 25 URINARY Kidneys 2 Ureters 2 Urinary Bladder 1 Urethra 1 fluid waste elimination secretion of wastes control blood volume and BP control blood ph electrolyte levels RBC levels hormone production
CHAPTER 25 URINARY Kidneys 2 Ureters 2 Urinary Bladder 1 Urethra 1 fluid waste elimination secretion of wastes control blood volume and BP control blood ph electrolyte levels RBC levels hormone production
Comparative Analysis of Stage and Other Prognostic Factors Among Urethral, Ureteral, and Renal Pelvis Malignant Tumors
 Comparative Analysis of Stage and Other Prognostic Factors Among Urethral, Ureteral, and Renal Pelvis Malignant Tumors Presented to NAACCR Annual Conference 2012 Serban Negoita, MD, DrPH; Marsha Dunn,
Comparative Analysis of Stage and Other Prognostic Factors Among Urethral, Ureteral, and Renal Pelvis Malignant Tumors Presented to NAACCR Annual Conference 2012 Serban Negoita, MD, DrPH; Marsha Dunn,
Large blocks in prostate and bladder pathology
 Large blocks in prostate and bladder pathology Farkas Sükösd Department of Pathology, University of Szeged The history of the large block technique in radical prostatectomy and cystectomy The first large
Large blocks in prostate and bladder pathology Farkas Sükösd Department of Pathology, University of Szeged The history of the large block technique in radical prostatectomy and cystectomy The first large
5/8/2014. AJCC Stage Introduction and General Rules. Acknowledgements* Introduction. Melissa Pearson, CTR North Carolina Central Cancer Registry
 AJCC Stage Introduction and General Rules Linda Mulvihill Public Health Advisor NCRA Annual Meeting May 2014 National Center for Chronic Disease Prevention and Health Promotion Division of Cancer Prevention
AJCC Stage Introduction and General Rules Linda Mulvihill Public Health Advisor NCRA Annual Meeting May 2014 National Center for Chronic Disease Prevention and Health Promotion Division of Cancer Prevention
Urinary Bladder: WHO Classification and AJCC Staging Update 2017
 Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
Urinary Bladder: WHO Classification and AJCC Staging Update 2017 Houston Society of Clinical Pathologists 58 th Annual Spring Symposium Houston, TX April 8, 2017 Jesse K. McKenney, MD Classification
1/25/13 Right partial nephrectomy followed by completion right radical nephrectomy.
 History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
Protocol applies to specimens from patients with Wilms tumor (nephroblastoma) or other renal tumors of childhood.
 or other renal tumors of childhood.") Wilms Tumor Protocol applies to specimens from patients with Wilms tumor (nephroblastoma) or other renal tumors of childhood. Procedures Cytology (No Accompanying Checklist) Incisional Biopsy (Needle or
Wilms Tumor Protocol applies to specimens from patients with Wilms tumor (nephroblastoma) or other renal tumors of childhood. Procedures Cytology (No Accompanying Checklist) Incisional Biopsy (Needle or
S1.04 PRINCIPAL CLINICIAN G1.01 COMMENTS S2.01 SPECIMEN LABELLED AS G2.01 *SPECIMEN DIMENSIONS (PROSTATE) S2.03 *SEMINAL VESICLES
 S2.03 *SEMINAL VESICLES") Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Indigenous
Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Indigenous
Change Log V1.3- v1.4
 Change Log V1.3- v1.4 This document shows the changes that were made to the SSDI manual and the Grade manual for the SEER*RSA version 1.4 release on (Date TBD). SSDI Manual Section: General Instructions
Change Log V1.3- v1.4 This document shows the changes that were made to the SSDI manual and the Grade manual for the SEER*RSA version 1.4 release on (Date TBD). SSDI Manual Section: General Instructions
BLADDER CANCER EPIDEMIOLOGY
 BLADDER CANCER WHAT IS NEW AND CLINICALLY RELEVANT Canadian Geese - Geist Reservoir (my backyard), Indianapolis, USA BLADDER CANCER EPIDEMIOLOGY Urinary bladder 17,960 2% Urinary bladder 4,390 1.6% Siegel
BLADDER CANCER WHAT IS NEW AND CLINICALLY RELEVANT Canadian Geese - Geist Reservoir (my backyard), Indianapolis, USA BLADDER CANCER EPIDEMIOLOGY Urinary bladder 17,960 2% Urinary bladder 4,390 1.6% Siegel
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER
 GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
GUIDELINES ON NON-MUSCLE- INVASIVE BLADDER CANCER (Limited text update December 21) M. Babjuk, W. Oosterlinck, R. Sylvester, E. Kaasinen, A. Böhle, J. Palou, M. Rouprêt Eur Urol 211 Apr;59(4):584-94 Introduction
Attachment #2 Overview of Follow-up
 Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
46. Merkel Cell Carcinoma
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
C ORPUS UTERI C ARCINOMA STAGING FORM (Carcinosarcomas should be staged as carcinomas)
") C ORPUS UTERI C ARCINOMA STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery Tis * T1 I T1a IA NX N0 N1 N2
C ORPUS UTERI C ARCINOMA STAGING FORM CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery Tis * T1 I T1a IA NX N0 N1 N2
C ORPUS UTERI C ARCINOMA STAGING FORM (Carcinosarcomas should be staged as carcinomas)
") CLINICAL C ORPUS UTERI C ARCINOMA STAGING FORM PATHOLOGIC Extent of disease before S TAGE C ATEGORY D EFINITIONS Extent of disease through any treatment completion of definitive surgery y clinical staging
CLINICAL C ORPUS UTERI C ARCINOMA STAGING FORM PATHOLOGIC Extent of disease before S TAGE C ATEGORY D EFINITIONS Extent of disease through any treatment completion of definitive surgery y clinical staging
Urinary Anatomy. Lab 40. Kidneys. Nephrons. Renal Corpuscle
 Urinary Anatomy Lab 40. Urinary Anatomy and Kidney Dissection Kidneys: filters blood, produces urine Ureters: convey urine to bladder Bladder: holding tank Urethra: carries urine to the outside for elimination
Urinary Anatomy Lab 40. Urinary Anatomy and Kidney Dissection Kidneys: filters blood, produces urine Ureters: convey urine to bladder Bladder: holding tank Urethra: carries urine to the outside for elimination
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
A schematic of the rectal probe in contact with the prostate is show in this diagram.
 Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Hello. My name is William Osai. I am a nurse practitioner in the GU Medical Oncology Department at The University of Texas MD Anderson Cancer Center in Houston. Today s presentation is Part 2 of the Overview
Lecture 56 Kidney and Urinary System
 Lecture 56 Kidney and Urinary System The adrenal glands are located on the superomedial aspect of the kidney The right diagram shows a picture of the kidney with the abdominal walls and organs removed
Lecture 56 Kidney and Urinary System The adrenal glands are located on the superomedial aspect of the kidney The right diagram shows a picture of the kidney with the abdominal walls and organs removed
2018 Grade PEGGY ADAMO, RHIT, CTR OCTOBER 11, 2018
 1 2018 Grade PEGGY ADAMO, RHIT, CTR ADAMOM@MAIL.NIH.GOV OCTOBER 11, 2018 2 Acknowledgements Donna Hansen, CCR Jennifer Ruhl, NCI SEER Introduction 3 Histologic Type vs. Grade Credit: Dr. Kay Washington
1 2018 Grade PEGGY ADAMO, RHIT, CTR ADAMOM@MAIL.NIH.GOV OCTOBER 11, 2018 2 Acknowledgements Donna Hansen, CCR Jennifer Ruhl, NCI SEER Introduction 3 Histologic Type vs. Grade Credit: Dr. Kay Washington
Attachment #2 Overview of Follow-up
 Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
Attachment #2 Overview of Follow-up Provided below is a general overview of follow-up and this may vary based on specific patient or cancer characteristics. Of note, Labs and imaging can be performed closer
This form may provide more data elements than required for collection by standard setters such as NCI SEER, CDC NPCR, and CoC NCDB.
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Uterine Cervix. Protocol applies to all invasive carcinomas of the cervix.
 Uterine Cervix Protocol applies to all invasive carcinomas of the cervix. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition and FIGO 2001 Annual Report Procedures Cytology (No Accompanying
Uterine Cervix Protocol applies to all invasive carcinomas of the cervix. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6 th edition and FIGO 2001 Annual Report Procedures Cytology (No Accompanying
Urinary System Laboratory
 Urinary System Laboratory 1 Adrenal gland Organs of The Urinary System Renal artery and vein Kidney Ureter Urinary bladder Figure 26.1 2 Urethra Functions of the urinary system organs: Urethra expels urine
Urinary System Laboratory 1 Adrenal gland Organs of The Urinary System Renal artery and vein Kidney Ureter Urinary bladder Figure 26.1 2 Urethra Functions of the urinary system organs: Urethra expels urine
S1.04 Principal clinician. G1.01 Comments. G2.01 *Specimen dimensions (prostate) S2.02 *Seminal vesicles
 S2.02 *Seminal vesicles") Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
Prostate Cancer Histopathology Reporting Proforma (Radical Prostatectomy) Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Sex Male
3/23/2017. Disclaimer. Common Changes in TNM Staging. Overview. Overview. Understanding Terminology. Overview
 Common Changes in TNM Staging Understanding the General Rules of Cancer Staging Thomas P. Baker, MD FCAP March 5, 2017 Disclaimer The identification of specific products or scientific instrumentation is
Common Changes in TNM Staging Understanding the General Rules of Cancer Staging Thomas P. Baker, MD FCAP March 5, 2017 Disclaimer The identification of specific products or scientific instrumentation is
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER
 MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
MUSCLE-INVASIVE AND METASTATIC BLADDER CANCER (Text update March 2008) A. Stenzl (chairman), N.C. Cowan, M. De Santis, G. Jakse, M. Kuczyk, A.S. Merseburger, M.J. Ribal, A. Sherif, J.A. Witjes Introduction
Kidney Q&A 5/5/16 Q1: Can we please get that clarification sent with the presentation and Q&A? Also a start date for that clarification
 Kidney Q&A 5/5/16 Q1: Can we please get that clarification sent with the presentation and Q&A? Also a start date for that clarification A1: Yes. See below. I don't think it will have a start date. Clarification
Kidney Q&A 5/5/16 Q1: Can we please get that clarification sent with the presentation and Q&A? Also a start date for that clarification A1: Yes. See below. I don't think it will have a start date. Clarification
Case Scenario 1: Thyroid
 Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
Case Scenario 1: Thyroid History and Physical Patient is an otherwise healthy 80 year old female with the complaint of a neck mass first noticed two weeks ago. The mass has increased in size and is palpable.
URINARY SYSTEM ANATOMY PART
 URINARY SYSTEM ANATOMY PART 1 DANIL HAMMOUDI.MD Urinary System Composed of kidneys, ureters, urinary bladder, and urethra Eliminates nitrogenous wastes from the body Regulates water, electrolyte, and ph
URINARY SYSTEM ANATOMY PART 1 DANIL HAMMOUDI.MD Urinary System Composed of kidneys, ureters, urinary bladder, and urethra Eliminates nitrogenous wastes from the body Regulates water, electrolyte, and ph
URINARY SYSTEM ANATOMY
 URINARY SYSTEM ANATOMY Adapted from Human Anatomy & Physiology Marieb and Hoehn (9 th ed.) OVERVIEW Metabolism of nutrients by the body produces wastes that must be removed from the body. Although excretory
URINARY SYSTEM ANATOMY Adapted from Human Anatomy & Physiology Marieb and Hoehn (9 th ed.) OVERVIEW Metabolism of nutrients by the body produces wastes that must be removed from the body. Although excretory
NAACCR Webinar Series 1
 NAACCR 2009 2010 Webinar Series Collecting Cancer Data: Kidney 1 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes 3 NAACCR 2009 2010 Webinar
NAACCR 2009 2010 Webinar Series Collecting Cancer Data: Kidney 1 Questions Please use the Q&A panel to submit your questions Send questions to All Panelist 2 Fabulous Prizes 3 NAACCR 2009 2010 Webinar
Bio 322 Human Anatomy Objectives for the laboratory exercise Urinary System Filtration Reabsorption Secretion Concentration
 Bio 322 Human Anatomy Objectives for the laboratory exercise Urinary System Required reading before beginning this lab: Saladin, KS: Human Anatomy 5 th ed (2017) Chapter 25 For this lab you will use parts
Bio 322 Human Anatomy Objectives for the laboratory exercise Urinary System Required reading before beginning this lab: Saladin, KS: Human Anatomy 5 th ed (2017) Chapter 25 For this lab you will use parts
Question: If in a particular case, there is doubt about the correct T, N or M category, what do you do?
 Exercise 1 Question: If in a particular case, there is doubt about the correct T, N or M category, what do you do? : 1. I mention both categories that are in consideration, e.g. pt1-2 2. I classify as
Exercise 1 Question: If in a particular case, there is doubt about the correct T, N or M category, what do you do? : 1. I mention both categories that are in consideration, e.g. pt1-2 2. I classify as
Kidney, Bladder and Prostate Neoplasia. David Bingham MD
 Kidney, Bladder and Prostate Neoplasia David Bingham MD typical malignant cytology of bladder washings 1 benign 2 malignant typical malignant cytology of bladder washings b Bladder tumor Non invasive papillary
Kidney, Bladder and Prostate Neoplasia David Bingham MD typical malignant cytology of bladder washings 1 benign 2 malignant typical malignant cytology of bladder washings b Bladder tumor Non invasive papillary
CODING STAGE: TNM AND OTHER STAGING SYSTEMS. Liesbet Van Eycken Otto Visser
 CODING STAGE: TNM AND OTHER STAGING SYSTEMS Liesbet Van Eycken Otto Visser OVERVIEW PART I Introduction What is stage? Why stage? History and publications of TNM Classification Clinical and pathologic
CODING STAGE: TNM AND OTHER STAGING SYSTEMS Liesbet Van Eycken Otto Visser OVERVIEW PART I Introduction What is stage? Why stage? History and publications of TNM Classification Clinical and pathologic
Glossary of Terms Primary Urethral Cancer
 Patient Information English Glossary of Terms Primary Urethral Cancer Advanced cancer A tumour that grows into deeper layers of tissue, adjacent organs, or surrounding muscles. Anaesthesia (general, spinal,
Patient Information English Glossary of Terms Primary Urethral Cancer Advanced cancer A tumour that grows into deeper layers of tissue, adjacent organs, or surrounding muscles. Anaesthesia (general, spinal,
Appendix H 2018 FCDS Required Site Specific Data Items (SSDIs)
") Below is the short list of Site Specific Data Items (SSDI) Required by FCDS for 2018. The list may be subject to changes. FCDS requires only a subset of the 136 total SSDIs available to be reported as
Below is the short list of Site Specific Data Items (SSDI) Required by FCDS for 2018. The list may be subject to changes. FCDS requires only a subset of the 136 total SSDIs available to be reported as
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14
 Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
Greater Manchester and Cheshire HPB Unit Guidelines for the Assessment & Management of Hepatobiliary and Pancreatic Disease Chapter 14 Contents 14. Neuroendocrine Tumours 161 14.1. Diagnostic algorithm
STAGE CATEGORY DEFINITIONS
 CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c
CLINICAL Extent of disease before any treatment y clinical staging completed after neoadjuvant therapy but before subsequent surgery TX Tis Tis (DCIS) Tis (LCIS) Tis (Paget s) T1 T1mi T1a T1b T1c a b c
IMAGING GUIDELINES - COLORECTAL CANCER
 IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
IMAGING GUIDELINES - COLORECTAL CANCER DIAGNOSIS The majority of colorectal cancers are diagnosed on colonoscopy, with some being diagnosed on Ba enema, ultrasound or CT. STAGING CT chest, abdomen and
Urinary System VASTACCESS, INC.
 Urinary System www.vastaccess.com 2 Urinary Tract Kidney Ureter Urinary Bladder Urethra Prostate (male) Membranous (male) Spongy (male) 3 Kidney Relations Suprarenal (Adrenal) Glands Liver Duodenum Transverse
Urinary System www.vastaccess.com 2 Urinary Tract Kidney Ureter Urinary Bladder Urethra Prostate (male) Membranous (male) Spongy (male) 3 Kidney Relations Suprarenal (Adrenal) Glands Liver Duodenum Transverse
Urinary System. Chapter 17 7/19/11. Introduction
 7/19/11 Chapter 17 Urinary System Introduction A. The urinary system consists of two kidneys that filter the blood, two ureters, a urinary bladder, and a urethra to convey waste substances to the outside.
7/19/11 Chapter 17 Urinary System Introduction A. The urinary system consists of two kidneys that filter the blood, two ureters, a urinary bladder, and a urethra to convey waste substances to the outside.
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
The functional anatomy of the urinary system. Human Anatomy Department Dr. Anastasia Bendelic
 The functional anatomy of the urinary system Human Anatomy Department Dr. Anastasia Bendelic Plan Development of the kidneys and their abnormalities Development of the urinary ways and their abnormalities
The functional anatomy of the urinary system Human Anatomy Department Dr. Anastasia Bendelic Plan Development of the kidneys and their abnormalities Development of the urinary ways and their abnormalities
Gastric Cancer Histopathology Reporting Proforma
 Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
Gastric Cancer Histopathology Reporting Proforma Mandatory questions (i.e. protocol standards) are in bold (e.g. S1.01). S1.01 Identification Family name Given name(s) Date of birth Sex Male Female Intersex/indeterminate
UICC 8 th Edition Errata 25 th of May 2018
 UICC 8 th Edition Errata 25 th of May 2018 ions are in italics Head and Neck Tumours Page 19 Oral Cavity T2 T3 T4a Tumour 2 cm or less in greatest dimension and more than 5 mm but no more than 10 mm depth
UICC 8 th Edition Errata 25 th of May 2018 ions are in italics Head and Neck Tumours Page 19 Oral Cavity T2 T3 T4a Tumour 2 cm or less in greatest dimension and more than 5 mm but no more than 10 mm depth
Lab Activity 31. Anatomy of the Urinary System. Portland Community College BI 233
 Lab Activity 31 Anatomy of the Urinary System Portland Community College BI 233 Urinary System Organs Kidneys Urinary bladder: provides a temporary storage reservoir for urine Paired ureters: transport
Lab Activity 31 Anatomy of the Urinary System Portland Community College BI 233 Urinary System Organs Kidneys Urinary bladder: provides a temporary storage reservoir for urine Paired ureters: transport
Colon and Rectum. Protocol revision date: January 2005 Based on AJCC/UICC TNM, 6th edition
 Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Colon and Rectum Protocol applies to all invasive carcinomas of the colon and rectum. Carcinoid tumors, lymphomas, sarcomas, and tumors of the vermiform appendix are excluded. Protocol revision date: January
Interactive Staging Bee
 Interactive Staging Bee ROBIN BILLET, MA, CTR GA/SC REGIONAL CONFERENCE NOVEMBER 6, 2018? Clinical Staging includes any information obtained about the extent of cancer obtained before initiation of treatment
Interactive Staging Bee ROBIN BILLET, MA, CTR GA/SC REGIONAL CONFERENCE NOVEMBER 6, 2018? Clinical Staging includes any information obtained about the extent of cancer obtained before initiation of treatment
Immunohistochemistry and Bladder Tumours
 Immunohistochemistry and Bladder Tumours Dr. Andrew J. Evans MD PhD FRCPC Consultant in Genitourinary Pathology University Health Network Toronto, ON Objec ves Review markers of urothelial differen a on
Immunohistochemistry and Bladder Tumours Dr. Andrew J. Evans MD PhD FRCPC Consultant in Genitourinary Pathology University Health Network Toronto, ON Objec ves Review markers of urothelial differen a on
MCR: MANAGEMENT OF 2018 CHANGES. By: Maricarmen Traverso-Ortiz MPH, CGG, CTR
 MCR: MANAGEMENT OF 2018 CHANGES By: Maricarmen Traverso-Ortiz MPH, CGG, CTR LEARNING OBJECTIVES Discuss a summary of the new changes for 2018 Overview of how the Maryland Cancer Registry is managing and
MCR: MANAGEMENT OF 2018 CHANGES By: Maricarmen Traverso-Ortiz MPH, CGG, CTR LEARNING OBJECTIVES Discuss a summary of the new changes for 2018 Overview of how the Maryland Cancer Registry is managing and
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Ritu Nayar, MD Professor and Vice Chair of Pathology Northwestern University, Feinberg School of Medicine Chicago, IL
 Ritu Nayar, MD Professor and Vice Chair of Pathology Northwestern University, Feinberg School of Medicine Chicago, IL email: r-nayar@northwestern.edu Nothing to disclose College of American Pathologists
Ritu Nayar, MD Professor and Vice Chair of Pathology Northwestern University, Feinberg School of Medicine Chicago, IL email: r-nayar@northwestern.edu Nothing to disclose College of American Pathologists
5/21/2018. Prostate Adenocarcinoma vs. Urothelial Carcinoma. Common Differential Diagnoses in Urological Pathology. Jonathan I.
 Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
Common Differential Diagnoses in Urological Pathology Jonathan I. Epstein Prostate Adenocarcinoma vs. Urothelial Carcinoma 1 2 NKX3.1 NKX3.1 3 4 5 6 Proposed ISUP Recommendations Option to use PSA as a
AJCC Cancer Staging 8 th Edition. Prostate Chapter 58. Executive Committee, AJCC. Professor and Director, Duke Prostate Center
 AJCC Cancer Staging 8 th Edition Prostate Chapter 58 Judd W Moul, MD, FACS Executive Committee, AJCC Professor and Director, Duke Prostate Center Duke University Durham, North Carolina Validating science.
AJCC Cancer Staging 8 th Edition Prostate Chapter 58 Judd W Moul, MD, FACS Executive Committee, AJCC Professor and Director, Duke Prostate Center Duke University Durham, North Carolina Validating science.
Disclosures. Outline. What IS tumor budding?? Tumor Budding in Colorectal Carcinoma: What, Why, and How. I have nothing to disclose
 Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
Tumor Budding in Colorectal Carcinoma: What, Why, and How Disclosures I have nothing to disclose Soo-Jin Cho, MD, PhD Assistant Professor UCSF Dept of Pathology Current Issues in Anatomic Pathology 2017
SEER Summary Stage Still Here!
 SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
Procedures Needle Biopsy Transurethral Prostatic Resection Suprapubic or Retropubic Enucleation (Subtotal Prostatectomy) Radical Prostatectomy
 Radical Prostatectomy") Prostate Gland Protocol applies to invasive carcinomas of the prostate gland. Protocol web posting date: July 2006 Protocol effective date: April 2007 Based on AJCC/UICC TNM, 6 th edition Procedures Needle
Prostate Gland Protocol applies to invasive carcinomas of the prostate gland. Protocol web posting date: July 2006 Protocol effective date: April 2007 Based on AJCC/UICC TNM, 6 th edition Procedures Needle
*OPERATIVE PROCEDURE. Serum tumour markers within normal limits S1.04 PRINCIPAL CLINICIAN
 Neoplasia of the Testis - Orchidectomy Histopathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Indigenous
Neoplasia of the Testis - Orchidectomy Histopathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth Indigenous
Essentials of Clinical MR, 2 nd edition. 73. Urinary Bladder and Male Pelvis
 73. Urinary Bladder and Male Pelvis Urinary bladder carcinoma is best locally staged with MRI. It is important however to note that a thickened wall (> 5 mm) is a non-specific finding seen in an underfilled
73. Urinary Bladder and Male Pelvis Urinary bladder carcinoma is best locally staged with MRI. It is important however to note that a thickened wall (> 5 mm) is a non-specific finding seen in an underfilled