Major Topic. Malignant Melanoma Plastic and Reconstructive Surgery R3 陸尊惠 /VS 吳瑞星
|
|
|
- Berniece Fitzgerald
- 5 years ago
- Views:
Transcription
1 Major Topic Malignant Melanoma Plastic and Reconstructive Surgery R3 陸尊惠 /VS 吳瑞星
2 Patient Data Name: OOO Age: 70 Gender: Male Date of admission: Day 1
3 Chief Complaint Black skin tumor at the back of the knee, noted for two months
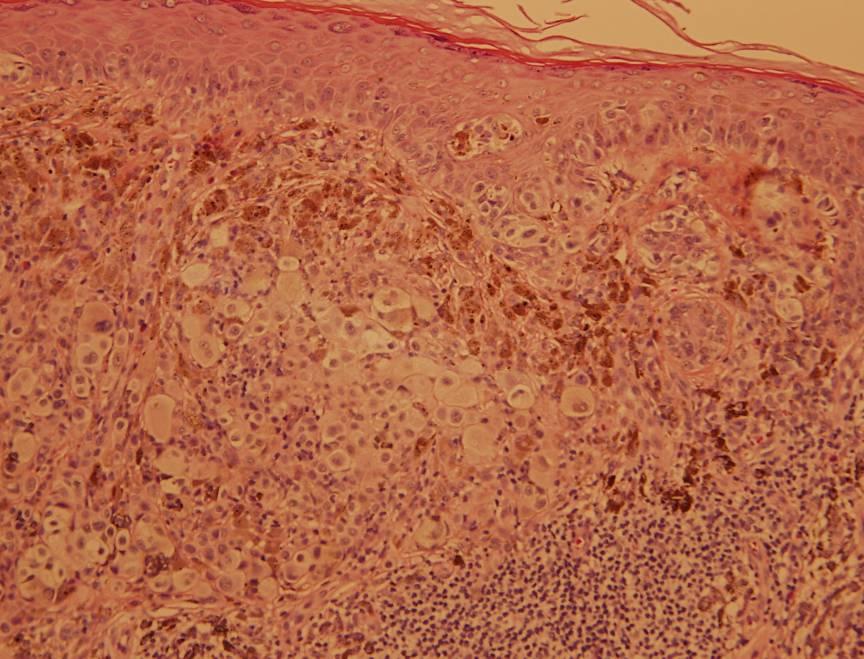
4 Present Illness Dark brown, blackish patch at the back of the right knee noted for 2 months No itching or bleeding, asymptomatic Visited our dermatology department Biopsy: Melanoma Proliferation of hyperchromatic atypical epithelioid neoplastic cells growing in nests in the epidermis and dermis Immunostain: positive for HMB-45 and MITF Tumor invades and expands the papillary dermis (Clark level III) and measures less than 1mm in thickness Ulceration, vascular space permeation and perineural invasion are not found
5 Past History Cardiac dysrhythmia, with regular OPD follow-up and medical control (Warfarin 4mg/day) No operation history Non-smoker, occasional social drinking No food or drug allergies
6 Physical Examination Conscious clear E4M6V5 Body height: 177cm, weight: 70kg Vital signs: BP 128/70, HR 64, RR 20, BT 36 HEENT: grossly normal, conjunctiva pink, sclera anicteric, pupils isocoric, neck supple, no LAP Chest: symmetric expansion, clear breathing,sound, regular heart beat, no murmur Abdomen: flat, soft, no tenderness, bowel sound normoactive, no flank knocking pain Extremities: freely movable, sutures at right popliteal region, wound clear, no palpable lymph nodes at inguinal region

7
8 Laboratory Data WBC: 5140/mm3, Seg 49.7%, Lym 38.3% Hb: 14.3 g/dl PLT: /mm3 GOT/GPT: 19/18 IU/L BUN/Cr: 15/1.1 mg/dl Na/K: 139/3.6 mmol/l PT: 14.9/11.9 sec aptt: 35.7/31.0 sec INR: 1.51
9 Positron Emission Tomography Scan Regionally increased radiotracer uptake in nasal cavity, oropharynx, colon, rectum and testes. The regional radiotracer uptake persisted in the delayed images acquired about 3 hours postinjection. The focal glucose hypermetabolism cannot be ascertained solely by FDG PET result. It may be due to normal physiological glucose metabolism and without clinical significance Otherwise, no other obvious abnormally increased radiotracer uptake is identified elsewhere in the body
10 Op Wide excision + elective lymph node dissection + split thickness skin graft 2.5cm surgical margin Intraoperative frozen section: Circumferential and basal margins free of malignancy

11

12
13 Pathology Skin, posterior knee, popliteal fossa, right, status post biopsy, wide excision for frozen section --- residual melanoma, Clark level III, 1mm in thickness, without ulceration Surgical margin, basal and circumferential --- free of malignancy Lymph node, inguinal area, right --- free of metastasis (0/11)
14
15 Discussion Malignant Melanoma
16 Introduction Malignant transformation of melanocyte Can occur anywhere melanocytes are present Most common tissue in which melanomas arise is the skin Incidence: varies widely, reflective of variation in genetic, phenotypic, and ultraviolet exposure risk factors US: 15 per 100,000 Australia: 45 per 100,000 China: <1 per 100,000
17 Risk Factors Exposure to UV radiation Intermittent, damaging exposure History of severe sunburn (blistering or pain for more than 2 days) confers a twofold increase in risk Chronic and occupational exposure confers less of a risk for melanoma, more of a risk for basal or squamous cell cancers Genetic predisposition Fair skin, blue eyes, red hair, easy freckling
18 Diagnosis Biopsy of a clinically suspicious lesion High-risk lesion (ABCDE Criteria) Asymmetry Border irregularity Color variegation Diameter >6mm Evolution 5% of melanomas are nonpigmented In earliest stages of development, most melanomas are <6mm in diameter Recent change or bleeding or itching: high risk
19 Workup Chest radiograph, serum lactic dehydrogenase (LDH) Head and neck primary lesion: head and neck CT or PET scan Clinically positive nodes in head or neck or groin: CT Distant metastasis: complete blood count, alkaline phosphatase, LDH, creatinine, CT of chest, abdomen, pelvis; MRI of brain; bone scan if symptomatic
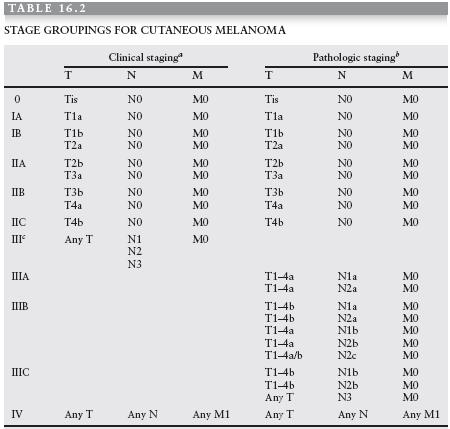
20 Staging Revised American Joint Committee on Cancer (AJCC) staging system published in August 2001 Major changes: T classification breakpoints of whole-integer thichness Tumor ulceration is included as a factor in the T classification and presence of ulceration upstages patients with stages I, II and III disease Clark level is now used only to subclassify T1 (<1mm) tumors Number of metastatic lymph nodes is prognostically significant Site of distant metastasis and presence of elevated LDH are used to subclassify M stage
21 5-Year Survival Rates Stage I: 92% Stage II: 68% Stage III: 45% Stage IV: 10%

22
23
24
25 Management Primary treatment for virtually all melanomas is surgical Wide excision of primary tumor Removal of regional lymph nodes that are involved or at high risk for involvement
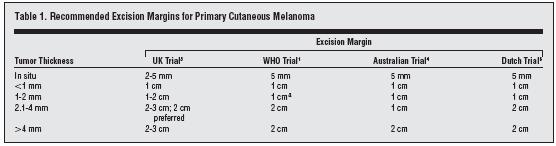
26 Wide Local Excision 5-cm standard margin (normal-appearing skin around the lesion, soft tissue down to, and including, muscle fascia) was the standard of care through most of 20 th century Late 1970s: series of retrospective reviews suggested narrower margins do not lead to significantly higher mortality or local recurrence rates
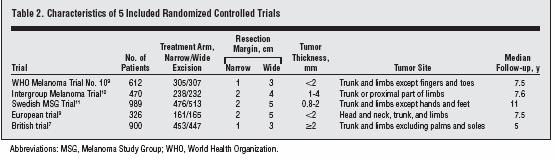
27 Archives of Surgery 2007 Excision Margins for Primary Cutaneous Melanoma: Updated Pooled Analysis of Randomized Controlled Trials Meta-analysis of 5 published prospective randomized trials evaluating the effect of width of excision margins on survival and recurrence
28
29
30 Results Total 3313 patients 1639 narrow excision 1674 wide excision 2220 had tumors less than 2mm None of the 5 trials demonstrated a survival advantage for wide excision margins Overall mortality was no significantly improved by performing wide excision margins No statistically significant difference in prevalence of locoregional recurrence between the two groups No statistically significant difference in incidence of local recurrence
31 WHO Melanoma Program Randomized patients with melanomas <2mm thick to receive wide local excision with 1 vs. 3 cm margin 612 patients, mean follow-up of 55 months No significant differences in disease-free survival, overall survival, or subsequent development of metastatic disease 3 patients developed local recurrence, all were in the 1- cm excision group and each had a primary lesion with a thickness > 1mm Authors concluded that for patients with primary lesions <1mm, a 1-cm margin excision is safe and effective
32 Intergroup Melanoma Trial Randomized patients with melanomas between 1 and 4 mm thick to receive excision with 2 vs. 4-cm margin 486 patients, median follow-up 6 years No significant difference in local recurrence, metastases, or 5-year survival Authors conclude that for 1 to 4mm thick melanoma patients, margin of excision could be safely reduced to 2 cm
33 British Trial Randomized 900 patients with melanomas >2mm to receive 1 vs. 3 cm margin wide excisions Median follow-up 60 months Significantly higher locoregional recurrence (37% vs. 32%) and disease-specific mortality (28% vs. 23%) in the group with narrower margins Limitations of study: most of the difference results from a higher nodal recurrence rate in the narrow margin group; there was no difference in local recurrence rate Overall survival was unaffected Authors conclude that to optimize disease-specific survival, use of a 1-cm margin should be avoided in patients with melanoma >2mm
34 There are no randomized trials to guide treatment standards for patients with thick melanomas (>4mm) A wider margin should be used unless it unduly increases morbidity Generally, a margin of 2 to 3cm is recommended for patients with melanomas >4mm in thickness
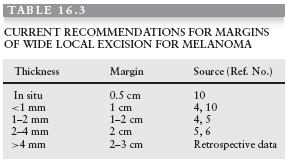
35 Current Recommendations
36 Lymphadenectomy Controversial Disagreement regarding excision of clinically uninvolved nodes Potential benefit of elective lymph node dissection is based on the dogma of sequential spread of metastatic disease to the regional lymph node prior to distant organs
37 Intergroup Melanoma Surgical Trial 740 patients randomized to receive ELND vs. observation, average follow-up of 7.4 years Patients with melanomas <1mm and >4mm were excluded from study There was no significant difference in survival There was significant survival advantage conferred by ELND in patients younger than 60 and for tumors between 1 and 2mm thick without ulceration Data suggest that there may be survival advantages for ELND in certain subgroups
38 Thank You
Cutaneous Melanoma: Epidemiology (USA) The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)
 The Sentinel Node in Head and Neck Melanoma. Cutaneous Melanoma: Epidemiology (USA)") The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
The Sentinel Node in Head and Neck Melanoma Cutaneous Melanoma: Epidemiology (USA) 6 th leading cause of cancer among men and women 68,720 new cases of invasive melanoma in 2009 8,650 deaths from melanoma
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
Melanoma: The Basics. What is a melanocyte?
 Melanoma: The Basics What is a melanocyte? A melanocyte is a normal cell, found in the skin, which produces melanin. Melanin is a black or dark brown pigment that is seen in the skin, hair, and parts of
Melanoma: The Basics What is a melanocyte? A melanocyte is a normal cell, found in the skin, which produces melanin. Melanin is a black or dark brown pigment that is seen in the skin, hair, and parts of
Clinical Pathological Conference. Malignant Melanoma of the Vulva
 Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
Clinical Pathological Conference Malignant Melanoma of the Vulva History F/48 Chinese Married Para 1 Presented in September 2004 Vulval mass for 2 months Associated with watery and blood stained discharge
World Articles of Ear, Nose and Throat Page 1
 World Articles of Ear, Nose and Throat ---------------------Page 1 Primary Malignant Melanoma of the Tongue: A Case Report Authors: Nanayakkara PR*, Arudchelvam JD** Ariyaratne JC*, Mendis K*, Jayasekera
World Articles of Ear, Nose and Throat ---------------------Page 1 Primary Malignant Melanoma of the Tongue: A Case Report Authors: Nanayakkara PR*, Arudchelvam JD** Ariyaratne JC*, Mendis K*, Jayasekera
WHAT DOES THE PATHOLOGY REPORT MEAN?
 Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Melanoma WHAT IS MELANOMA? Melanoma is a type of cancer that affects cells called melanocytes. These cells are found mainly in skin but also in the lining of other areas such as nose and rectum, and also
Mechanical versus bioprosthetic valve. Intern: Supervisor: VS
 Mechanical versus bioprosthetic valve Intern: Supervisor: VS Patient basic data ID: N102110716 Name: Age: 64 years old Sex: male Occupation: Admission date: 0960528 Chief complaint Exertional dyspnea for
Mechanical versus bioprosthetic valve Intern: Supervisor: VS Patient basic data ID: N102110716 Name: Age: 64 years old Sex: male Occupation: Admission date: 0960528 Chief complaint Exertional dyspnea for
Clinical characteristics
 Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Skin Cancer Fernando Vega, MD Seattle Healing Arts Clinical characteristics Precancerous lesions Common skin cancers ACTINIC KERATOSIS Precancerous skin lesions Actinic keratoses Dysplastic melanocytic
Dermatopathology: The tumor is composed of keratinocytes which show atypia, increase mitoses and abnormal mitoses.
 Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Squamous cell carcinoma (SCC): A common malignant tumor of keratinocytes arising in the epidermis, usually from a precancerous condition: 1- UV induced actinic keratosis, usually of low grade malignancy.
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Malignant Melanoma Early Stage. A guide for patients
 This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
This melanoma patient brochure is designed to help educate melanoma patients and their caregivers. It was developed under the guidance of Dr. Michael Smylie, Professor, Department of Oncology, University
Melanoma Case Scenario 1
 Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Melanoma Case Scenario 1 History and physical 11/5/16 Patient is a single, 48-year-old male in good health who presented to his primary physician for a yearly physical exam during which a 3.4 x 2.8 x 1.5
Skin Cancer. 5 Warning Signs. American Osteopathic College of Occupational and Preventive Medicine OMED 2012, San Diego, Monday, October 8, 2012 C-1
 Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Skin Cancer AMERICAN OSTEOPATHIC COLLEGE OF OCCUPATIONAL & PREVENTIVE MEDICINE OMED 2012 October 8, 2012 E. Robert Wanat II, D.O., M.P.H. Learning Objectives: Identify the 3 Basic Types of Skin Cancer
Corporate Medical Policy
 Corporate Medical Policy Gene Expression Profiling for Cutaneous Melanoma File Name: Origination: Last CAP Review: Next CAP Review: Last Review: gene_expression_profiling_for_cutaneous_melanoma 5/2018
Corporate Medical Policy Gene Expression Profiling for Cutaneous Melanoma File Name: Origination: Last CAP Review: Next CAP Review: Last Review: gene_expression_profiling_for_cutaneous_melanoma 5/2018
Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010
 Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010 Self Assessment Module on Nuclear Medicine and PET/CT Case Review FDG PET/CT IN LYMPHOMA AND MELANOMA Submitted
Los Angeles Radiological Society 62 nd Annual Midwinter Radiology Conference January 31, 2010 Self Assessment Module on Nuclear Medicine and PET/CT Case Review FDG PET/CT IN LYMPHOMA AND MELANOMA Submitted
An Overview of Melanoma. Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center
 An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
An Overview of Melanoma Harriet Kluger, M.D. Associate Professor Section of Medical Oncology Yale Cancer Center Melanoma Statistics Median age at presentation 45-55 55 years Incidence: 2003 54,200 cases
Technicians & Nurses Program
 ASCRS ASOA Symposium & Congress Technicians & Nurses Program May 6-10, 2016 New Orleans Evaluation and Treatment of Eyelid Malignancies Richard C. Allen MD PhD FACS Professor Section of Ophthalmology Dept.
ASCRS ASOA Symposium & Congress Technicians & Nurses Program May 6-10, 2016 New Orleans Evaluation and Treatment of Eyelid Malignancies Richard C. Allen MD PhD FACS Professor Section of Ophthalmology Dept.
1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter.
 Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
Melanoma. Lynn Schuchter, M.D. Associate Professor of Medicine Abramson Cancer Center of the University of Pennsylvania
 Melanoma Lynn Schuchter, M.D. Associate Professor of Medicine Abramson Cancer Center of the University of Pennsylvania WHAT IS MELANOMA? Melanoma is a type of skin cancer (a serious skin cancer because
Melanoma Lynn Schuchter, M.D. Associate Professor of Medicine Abramson Cancer Center of the University of Pennsylvania WHAT IS MELANOMA? Melanoma is a type of skin cancer (a serious skin cancer because
Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc
 1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
1 Benign versus Cancerous Lesions How to tell the difference FMF 2014 Christie Freeman MD, CCFP, DipPDerm, MSc Benign lesions Seborrheic Keratoses: Warty, stuck-on Genetics and birthdays Can start in late
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment. Justin Rivard MD, MSc, FRCSC September 21, 2018
 You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
You Are Going to Cut How Much Skin? Locoregional Surgical Treatment Justin Rivard MD, MSc, FRCSC September 21, 2018 Presenter Disclosure Faculty/Speaker: Justin Rivard Relationships with financial sponsors:
Melanoma Quality Reporting
 Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Melanoma Quality Reporting September 1, 2013 December 31, 2016 Laurence McCahill, MD Surgical Oncologist Metro Health Surgical Oncology Metro Health Professional Building 2122 Health Drive SW Wyoming,
Merkel Cell Carcinoma Case # 2
 DISCHARGE SUMMARY Admitted: 10/11/2010 Discharged: 10/13/2010 Merkel Cell Carcinoma Case # 2 Chief Compliant: A 79 year old lady status post tumor on the scalp excision and left neck likely dissection
DISCHARGE SUMMARY Admitted: 10/11/2010 Discharged: 10/13/2010 Merkel Cell Carcinoma Case # 2 Chief Compliant: A 79 year old lady status post tumor on the scalp excision and left neck likely dissection
FINE NEEDLE ASPIRATION OF ENLARGED LYMPH NODE: Metastatic squamous cell carcinoma
 Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Identifying Skin Cancer. Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018
 Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Identifying Skin Cancer Mary S. Stone MD Professor of Dermatology and Pathology University of Iowa Carver College of Medicine March, 2018 American Cancer Society web site Skin Cancer Melanoma Non-Melanoma
Clinical indications for positron emission tomography
 Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Clinical indications for positron emission tomography Oncology applications Brain and spinal cord Parotid Suspected tumour recurrence when anatomical imaging is difficult or equivocal and management will
Springer Healthcare. Staging and Diagnosing Cutaneous Melanoma. Concise Reference. Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone
 Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Concise Reference Staging and Diagnosing Cutaneous Melanoma Dirk Schadendorf, Corinna Kochs, Elisabeth Livingstone Extracted from Handbook of Cutaneous Melanoma: A Guide to Diagnosis and Treatment Published
Kentaro Tanaka, 1 Hiroki Mori, 1 Mutsumi Okazaki, 1 Aya Nishizawa, 2 and Hiroo Yokozeki Introduction. 2. Case Presentation
 Case Reports in Oncological Medicine Volume 2013, Article ID 259326, 4 pages http://dx.doi.org/10.1155/2013/259326 Case Report Long-Term Treatment Outcome after Only Popliteal Lymph Node Dissection for
Case Reports in Oncological Medicine Volume 2013, Article ID 259326, 4 pages http://dx.doi.org/10.1155/2013/259326 Case Report Long-Term Treatment Outcome after Only Popliteal Lymph Node Dissection for
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY
 IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
IT S FUNDAMENTAL MY DEAR WATSON! A SHERLOCKIAN APPROACH TO DERMATOLOGY Skin, Bones, and other Private Parts Symposium Dermatology Lectures by Debra Shelby, PhD, DNP, FNP-BC, FADNP, FAANP Debra Shelby,
Sentinel Lymph Node Biopsies in Cutaneous Melanoma: A systematic review of the literature. Sasha Jenkins
 Sentinel Lymph Node Biopsies in Cutaneous Melanoma: A systematic review of the literature By Sasha Jenkins A Master s Paper submitted to the faculty of the University of North Carolina at Chapel Hill in
Sentinel Lymph Node Biopsies in Cutaneous Melanoma: A systematic review of the literature By Sasha Jenkins A Master s Paper submitted to the faculty of the University of North Carolina at Chapel Hill in
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012
 Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
Skin Malignancies Non - Melanoma & Melanoma Marilyn Ng, MD Dept. of Surgery M&M Conference Downstate Medical Center July 19, 2012 Case Presentation 57 yo man with 3 month hx of a nonhealing < 1 cm right
Patient Information. Age: 8 y/o Sex: Female. Date of Admission: Date of Discharge:
 Patient Information Age: 8 y/o Sex: Female Date of Admission: 92-10-08 Date of Discharge: 92-10-18 Chief Complaint Severe admominal pain and vomiting with dysuria since last afternoon Present Illness Lower
Patient Information Age: 8 y/o Sex: Female Date of Admission: 92-10-08 Date of Discharge: 92-10-18 Chief Complaint Severe admominal pain and vomiting with dysuria since last afternoon Present Illness Lower
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR
 PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR Last Revision Date July 2015 1 Site Group: Gynecologic Cancer Vulvar Author: Dr. Stephane Laframboise 1. INTRODUCTION
PRINCESS MARGARET CANCER CENTRE CLINICAL PRACTICE GUIDELINES GYNECOLOGIC CANCER VULVAR Last Revision Date July 2015 1 Site Group: Gynecologic Cancer Vulvar Author: Dr. Stephane Laframboise 1. INTRODUCTION
BACK TO TABLE OF CONTENTS FOCUS ON MELANOMA Oncology Annual Report BAPTIST HEALTH LEXINGTON ONCOLOGY ANNUAL REPORT
 FOCUS ON MELANOMA 2014 Oncology Annual Report BAPTIST HEALTH LEXINGTON 1 2014 ONCOLOGY ANNUAL REPORT TABLE OF CONTENTS What is melanoma?...3 Who is at risk for melanoma?...3 What causes melanoma?...4 What
FOCUS ON MELANOMA 2014 Oncology Annual Report BAPTIST HEALTH LEXINGTON 1 2014 ONCOLOGY ANNUAL REPORT TABLE OF CONTENTS What is melanoma?...3 Who is at risk for melanoma?...3 What causes melanoma?...4 What
Subject ID: I N D # # U A * Consent Date: Day Month Year
 IND Study # Eligibility Checklist Pg 1 of 15 Instructions: Check the appropriate box for each Inclusion and Exclusion Criterion below. Each criterion must be marked and all protocol criteria have to be
IND Study # Eligibility Checklist Pg 1 of 15 Instructions: Check the appropriate box for each Inclusion and Exclusion Criterion below. Each criterion must be marked and all protocol criteria have to be
Management of Neck Metastasis from Unknown Primary
 Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Primary Cutaneous Melanoma Pathology Reporting Proforma DD MM YYYY. *Tumour site. *Specimen laterality. *Specimen type
 Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Primary Cutaneous Melanoma Pathology Reporting Proforma Includes the International Collaboration on Cancer reporting dataset denoted by * Family name Given name(s) Date of birth DD MM YYYY Sex Male Female
Glenn D. Goldman, MD. University of Vermont Medical Center. University of Vermont College of Medicine
 Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
Glenn D. Goldman, MD University of Vermont Medical Center University of Vermont College of Medicine Recognize and identify the main types of skin cancer and their precursors Identify and understand new
Index. Surg Oncol Clin N Am 16 (2007) Note: Page numbers of article titles are in boldface type.
 Note: Page numbers of article titles are in boldface type.") Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Surg Oncol Clin N Am 16 (2007) 465 469 Index Note: Page numbers of article titles are in boldface type. A Adjuvant therapy, preoperative for gastric cancer, staging and, 339 B Breast cancer, metabolic
Case Presentation and Discussion on GI Bleeding Nolan Ortega Aludino, M.D.
 Case Presentation and Discussion on GI Bleeding Nolan Ortega Aludino, M.D. General Data R.L. R.L. 4343 years old MaleMale PacoPaco Manila Chief Complaint Anal Anal bleeding History of Present Illness 3
Case Presentation and Discussion on GI Bleeding Nolan Ortega Aludino, M.D. General Data R.L. R.L. 4343 years old MaleMale PacoPaco Manila Chief Complaint Anal Anal bleeding History of Present Illness 3
Chief complaint. A mass at right chest
 Chief complaint A mass at right chest Present illness This 1-year-5-month-old girl had a mass at right side chest since one month ago. flat and not tender at first In the recent 2 days, the mass enlarged
Chief complaint A mass at right chest Present illness This 1-year-5-month-old girl had a mass at right side chest since one month ago. flat and not tender at first In the recent 2 days, the mass enlarged
MELANOMA. Some people are more likely to get a m Melanoma than others:
 MELANOMA This leaflet has been written to help you understand more about Melanoma. It tells you what is it, what causes it, what can be done about it, how it can be prevented, and where you can find out
MELANOMA This leaflet has been written to help you understand more about Melanoma. It tells you what is it, what causes it, what can be done about it, how it can be prevented, and where you can find out
Update on SLN and Melanoma: DECOG and MSLT-II. Gordon H. Hafner, MD, FACS
 Update on SLN and Melanoma: DECOG and MSLT-II Gordon H. Hafner, MD, FACS No disclosures The surgery of malignant disease is not the surgery of organs, it is of the lymphatic system. Lord Moynihan Lymph
Update on SLN and Melanoma: DECOG and MSLT-II Gordon H. Hafner, MD, FACS No disclosures The surgery of malignant disease is not the surgery of organs, it is of the lymphatic system. Lord Moynihan Lymph
Melanoma. Kaushik Mukherjee MD A. Scott Pearson MD
 Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Melanoma Kaushik Mukherjee MD A. Scott Pearson MD Disclosures You still have to study Not all inclusive No Western blots Extensive use of Google Image Search and Sabiston Melanoma Basics 8 th most common
Index. Note: Page numbers of article titles are in boldface type. A Age as factor in melanoma, Anorectal melanoma RT for, 1035
 Index Note: Page numbers of article titles are in boldface type. A Age as factor in melanoma, 947 948 Anorectal melanoma RT for, 1035 B Bacille Calmette-Guerin (BCG) in melanoma, 1008 BCG. See Bacille
Index Note: Page numbers of article titles are in boldface type. A Age as factor in melanoma, 947 948 Anorectal melanoma RT for, 1035 B Bacille Calmette-Guerin (BCG) in melanoma, 1008 BCG. See Bacille
North of Scotland Cancer Network Clinical Management Guideline for Malignant Melanoma
 Nth of Scotland Cancer Netwk Clinical Management Guideline f Malignant Melanoma Based on WOSCAN CMG with further consultation within NOSCAN UNCONTROLLED WHEN PRINTED Prepared by Approved by Issue date
Nth of Scotland Cancer Netwk Clinical Management Guideline f Malignant Melanoma Based on WOSCAN CMG with further consultation within NOSCAN UNCONTROLLED WHEN PRINTED Prepared by Approved by Issue date
Integumentary System
 Integumentary System The integumentary system is commonly known as the Skin Largest organ of human body 10% total body weight and would cover over 20 square feet Functions of Skin 1. Protection Barrier
Integumentary System The integumentary system is commonly known as the Skin Largest organ of human body 10% total body weight and would cover over 20 square feet Functions of Skin 1. Protection Barrier
PET in Rectal Carcinoma
 Case Report PET in Rectal Carcinoma Josefina Jofré M 1, Paulina Sierralta C 1, José Canessa G 1,2, Pamela Humeres A 3, Gabriel Castro M 4, Teresa Massardo V 1,4 1 Centro PET de Imágenes Moleculares, Hospital
Case Report PET in Rectal Carcinoma Josefina Jofré M 1, Paulina Sierralta C 1, José Canessa G 1,2, Pamela Humeres A 3, Gabriel Castro M 4, Teresa Massardo V 1,4 1 Centro PET de Imágenes Moleculares, Hospital
Da Costa was the first to coin the term. Marjolin s Ulcer: A Case Report and Literature Review. Case Report. Introduction
 E-Da Medical Journal 2016;3(2):24-28 Case Report Marjolin s Ulcer: A Case Report and Literature Review Yue-Chiu Su 1, Li-Ren Chang 2 Marjolin s ulcer is an aggressive cutaneous malignancy, which is common
E-Da Medical Journal 2016;3(2):24-28 Case Report Marjolin s Ulcer: A Case Report and Literature Review Yue-Chiu Su 1, Li-Ren Chang 2 Marjolin s ulcer is an aggressive cutaneous malignancy, which is common
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R
 Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Oncology General Principles L A U R I E S I M A R D B R E A S T S U R G I C A L O N C O L O G Y F E L L O W D E C E M B E R 2 0 1 2 Objectives Discuss Diagnostic and staging strategies in oncology Know
Case conference. Welcome Dr. Lawrence Tierney
 Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
Case conference Welcome Dr. Lawrence Tierney Case: 18 year-old male CC) hamatomesis, Fever and cough HPI) 1 st admission One month ago, he admitted to our hospital because of hematemesis. He had weight
General information about skin cancer
 Skin Cancer General information about skin cancer Key points Skin cancer is a disease in which malignant (cancer) cells form in the tissues of the skin. There are different types of cancer that start in
Skin Cancer General information about skin cancer Key points Skin cancer is a disease in which malignant (cancer) cells form in the tissues of the skin. There are different types of cancer that start in
Surgical Issues in Melanoma
 Surgical Issues in Melanoma Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Director, Surgical Oncology Training Program Professor of Surgery John Wayne Cancer Institute Surgical
Surgical Issues in Melanoma Mark B. Faries, MD, FACS Director, Donald L. Morton Melanoma Research Program Director, Surgical Oncology Training Program Professor of Surgery John Wayne Cancer Institute Surgical
MELANOMA. 4 Fitzroy Square, London W1T 5HQ Tel: Fax: Registered Charity No.
 MELANOMA This leaflet had been written to help you understand more about melanoma. It tells you what it is, what causes it, what can be done about it, how it can be prevented, and where you can find out
MELANOMA This leaflet had been written to help you understand more about melanoma. It tells you what it is, what causes it, what can be done about it, how it can be prevented, and where you can find out
Imaging in gastric cancer
 Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
Imaging in gastric cancer Gastric cancer remains a deadly disease because of late diagnosis. Adenocarcinoma represents 90% of malignant tumors. Diagnosis is based on endoscopic examination with biopsies.
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER
 10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
10 MUSCLE - INVASIVE AND METASTATIC BLADDER CANCER Recommendations from the EAU Working Party on Muscle Invasive and Metastatic Bladder Cancer G. Jakse (chairman), F. Algaba, S. Fossa, A. Stenzl, C. Sternberg
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD
 Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
Updates on Melanoma: Are You Following the Latest Guidelines of Care? Jerry Brewer, MD Disclosure Statement Update on Melanoma Are You Following the Latest Guidelines of Care? I, Jerry D. Brewer, MD, do
Glenn D. Goldman, MD. Fletcher Allen Health Care. University of Vermont College of Medicine
 Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
Glenn D. Goldman, MD Fletcher Allen Health Care University of Vermont College of Medicine Recognize and identify the main types of skin cancer Understand how and why Mohs surgery is utilized for the treatment
STAGING, BIOPSY AND NATURAL HISTORY OF TUMORS SCOTT D WEINER MD
 STAGING, BIOPSY AND NATURAL HISTORY OF TUMORS SCOTT D WEINER MD WHAT DO YOU DO WHEN THIS SHOWS UP IN YOUR OFFICE? besides panicking KEY PRINCIPLE!!! Reactive zone is the edema, neovascularity and inflammation
STAGING, BIOPSY AND NATURAL HISTORY OF TUMORS SCOTT D WEINER MD WHAT DO YOU DO WHEN THIS SHOWS UP IN YOUR OFFICE? besides panicking KEY PRINCIPLE!!! Reactive zone is the edema, neovascularity and inflammation
Case Scenario 1. Discharge Summary
 Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
Case Scenario 1 Discharge Summary A 69-year-old woman was on vacation and noted that she was becoming jaundiced. Two months prior to leaving on that trip, she had had a workup that included an abdominal
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL
 A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
A PRACTICAL APPROACH TO ATYPICAL MELANOCYTIC LESIONS BIJAN HAGHIGHI M.D, DIRECTOR OF DERMATOPATHOLOGY, ST. JOSEPH HOSPITAL OBJECTIVES Discuss current trends and changing concepts in our understanding of
NAACCR Webinar Series 1
 Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Collecting Cancer Data: Melanoma 2013 2014 NAACCR Webinar Series April 3, 2014 Q&A Please submit all questions concerning webinar content through the Q&A panel. Reminder: If you have participants watching
Current Therapy of Cutaneous Melanoma
 CME Current Therapy of Cutaneous Melanoma Jeffrey D. Wagner, M.D., Michael S. Gordon, M.D., Tsu-Yi Chuang, M.D., and John J. Coleman, III, M.D. Indianapolis, Ind. Learning Objectives: After studying this
CME Current Therapy of Cutaneous Melanoma Jeffrey D. Wagner, M.D., Michael S. Gordon, M.D., Tsu-Yi Chuang, M.D., and John J. Coleman, III, M.D. Indianapolis, Ind. Learning Objectives: After studying this
Clinical Radiological Pathological Conference
 Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Clinical Radiological Pathological Conference CASE 1: A 59-year-old female Housekeeper Live in Phuket, Thailand Progressive dyspnea for 1 year Present illness 1 year PTA : She developed dyspnea on exertion
Skin Cancer - Non-Melanoma
 Skin Cancer - Non-Melanoma Introduction Each year, millions of people find out that they have skin cancer. Skin cancer is almost 100% curable if found early and treated right away. It is possible to prevent
Skin Cancer - Non-Melanoma Introduction Each year, millions of people find out that they have skin cancer. Skin cancer is almost 100% curable if found early and treated right away. It is possible to prevent
Dr Rosalie Stephens. Mr Richard Martin. Medical Oncologist Auckland City Hospital Auckland
 Dr Rosalie Stephens Medical Oncologist Auckland City Hospital Auckland Mr Richard Martin General Surgeon Melanoma Unit Team Waitemata District Health Board Auckland 8:30-9:25 WS #99: Interactive Case Studies
Dr Rosalie Stephens Medical Oncologist Auckland City Hospital Auckland Mr Richard Martin General Surgeon Melanoma Unit Team Waitemata District Health Board Auckland 8:30-9:25 WS #99: Interactive Case Studies
Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG
 Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG At tumor board, a surgeon insists that all level II melanomas are invasive since they have broken through the
Melanoma-Back to Basics I Thought I Knew Ya! Paul K. Shitabata, M.D. Dermatopathologist APMG At tumor board, a surgeon insists that all level II melanomas are invasive since they have broken through the
Esophageal Cancer Initially Thought to be Accompanied by a Solitary Metastasis to an Intrathoracic Paraaortic Lymph Node
 2012 66 5 417 421 Esophageal Cancer Initially Thought to be Accompanied by a Solitary Metastasis to an Intrathoracic Paraaortic Lymph Node a b* a a a a a a a b ʼ 418 Horio et al. Acta Med. Okayama Vol.
2012 66 5 417 421 Esophageal Cancer Initially Thought to be Accompanied by a Solitary Metastasis to an Intrathoracic Paraaortic Lymph Node a b* a a a a a a a b ʼ 418 Horio et al. Acta Med. Okayama Vol.
Guideline for the Management of Vulval Cancer
 Version History Guideline for the Management of Vulval Cancer Version Date Brief Summary of Change Issued 2.0 20.02.08 Endorsed by the Governance Committee 2.1 19.11.10 Circulated at NSSG meeting 2.2 13.04.11
Version History Guideline for the Management of Vulval Cancer Version Date Brief Summary of Change Issued 2.0 20.02.08 Endorsed by the Governance Committee 2.1 19.11.10 Circulated at NSSG meeting 2.2 13.04.11
1/25/13 Right partial nephrectomy followed by completion right radical nephrectomy.
 History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
History and Physical Case Scenario 1 45 year old white male presents with complaints of nausea, weight loss, and back pain. A CT of the chest, abdomen and pelvis was done on 12/8/12 that revealed a 12
Desmoplastic Melanoma R/O BCC. Clinical Information. 74 y.o. man with lesion on left side of neck r/o BCC
 R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
R/O BCC Sabine Kohler, M.D. Professor of Pathology and Dermatology Dermatopathology Service Stanford University School of Medicine Clinical Information 74 y.o. man with lesion on left side of neck r/o
11/21/13 CEA: 1.7 WNL
 Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Case Scenario 1 A 70 year-old white male presented to his primary care physician with a recent history of rectal bleeding. He was referred for imaging and a colonoscopy and was found to have adenocarcinoma.
Subject Index. Dry desquamation, see Skin reactions, radiotherapy
 Subject Index Actinic keratosis disseminated disease 42 surgical excision 42 AIDS, see Kaposi s sarcoma Amifostine, skin reaction prophylaxis 111 Basal cell carcinoma, superficial X-ray therapy Bowen s
Subject Index Actinic keratosis disseminated disease 42 surgical excision 42 AIDS, see Kaposi s sarcoma Amifostine, skin reaction prophylaxis 111 Basal cell carcinoma, superficial X-ray therapy Bowen s
Rebecca Vogel, PGY-4 March 5, 2012
 Rebecca Vogel, PGY-4 March 5, 2012 Historical Perspective Changes In The Staging System Studies That Started The Talk Where We Go From Here Cutaneous melanoma has become an increasingly growing problem,
Rebecca Vogel, PGY-4 March 5, 2012 Historical Perspective Changes In The Staging System Studies That Started The Talk Where We Go From Here Cutaneous melanoma has become an increasingly growing problem,
Directly Coded Summary Stage Melanoma
 Directly Coded Summary Stage Melanoma National Center for Chronic Disease Prevention and Health Promotion Division of Cancer Prevention and Control, National Program of Cancer Registries Directly Coded
Directly Coded Summary Stage Melanoma National Center for Chronic Disease Prevention and Health Promotion Division of Cancer Prevention and Control, National Program of Cancer Registries Directly Coded
Oral and Maxillofacial Surgery Department
 Oral and Maxillofacial Surgery Department This leaflet explains: Lentigo Maligna What are the aims of this leaflet? This leaflet has been written to help you understand more about lentigo maligna and melanoma
Oral and Maxillofacial Surgery Department This leaflet explains: Lentigo Maligna What are the aims of this leaflet? This leaflet has been written to help you understand more about lentigo maligna and melanoma
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses
 Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
Dermoscopy: Recognizing Top Five Common In- Office Diagnoses Vu A. Ngo, DO Department of Family Medicine and Dermatology Choctaw Nation Health Services Authority Learning Objectives Introduction to dermoscopy
Protocol applies to melanoma of cutaneous surfaces only.
 Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Melanoma of the Skin Protocol applies to melanoma of cutaneous surfaces only. Procedures Biopsy (No Accompanying Checklist) Excision Re-excision Protocol revision date: January 2005 Based on AJCC/UICC
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS
 Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
Exercise 15: CSv2 Data Item Coding Instructions ANSWERS CS Tumor Size Tumor size is the diameter of the tumor, not the depth or thickness of the tumor. Chest x-ray shows 3.5 cm mass; the pathology report
MELANOMA: HANDS-ON OR HANDS-OFF?
 MELANOMA: HANDS-ON OR HANDS-OFF? M SCHAMM MBChB (Pret), FCS (SA) Endocrine and Transplant Surgeon, Department of Surgery, University of the Witwatersrand; and Clinical Head Transplant Surgery, Charlotte
MELANOMA: HANDS-ON OR HANDS-OFF? M SCHAMM MBChB (Pret), FCS (SA) Endocrine and Transplant Surgeon, Department of Surgery, University of the Witwatersrand; and Clinical Head Transplant Surgery, Charlotte
PET/CT Frequently Asked Questions
 PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
Periocular Malignancies
 Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Periocular Malignancies Andrew Gurwood, O.D., F.A.A.O., Dipl. Marc Myers, O.D., F.A.A.O. Drs. Myers and Gurwood have no financial interests to disclose. Course Description Discussion of the most common
Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy
 American Academy of Dermatology 2018 Annual Meeting San Diego, CA, February 17, 2018 Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy Christopher Bichakjian,
American Academy of Dermatology 2018 Annual Meeting San Diego, CA, February 17, 2018 Translating Evidence into Practice: Primary Cutaneous Melanoma Guidelines. Sentinel Lymph Node Biopsy Christopher Bichakjian,
Krunal Amin 7/17/2010 Josh Cannon Topics in Biology
 SUMMER VENTURES UNC CHARLOTTE 2010 1 Malignant Melanoma Krunal Amin 7/17/2010 Josh Cannon Topics in Biology 2 Abstract Malignant melanoma is a cancer of melanocytes. It is caused by environmental (mainly
SUMMER VENTURES UNC CHARLOTTE 2010 1 Malignant Melanoma Krunal Amin 7/17/2010 Josh Cannon Topics in Biology 2 Abstract Malignant melanoma is a cancer of melanocytes. It is caused by environmental (mainly
ORAL MELANOMA Definition Epidemiology Clinical Presentation
 ORAL MELANOMA Definition Melanoma is a highly malignant neoplasia, arising from melanocytes, the cells that produce the brownish pigment melanin. Melanin is the determinant in skin colour and protects
ORAL MELANOMA Definition Melanoma is a highly malignant neoplasia, arising from melanocytes, the cells that produce the brownish pigment melanin. Melanin is the determinant in skin colour and protects
Melanoma. Exceptional healthcare, personally delivered
 Melanoma Exceptional healthcare, personally delivered What is Melanoma? Malignant Melanoma is a form of Skin Cancer which can start in a preexisting mole or normal looking skin. What causes Melanoma? Although
Melanoma Exceptional healthcare, personally delivered What is Melanoma? Malignant Melanoma is a form of Skin Cancer which can start in a preexisting mole or normal looking skin. What causes Melanoma? Although
Malignant tumors of melanocytes : Part 3. Deba P Sarma, MD., Omaha
 Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
Malignant tumors of melanocytes : Part 3 Deba P Sarma, MD., Omaha Let s go over one case of melanoma using the following worksheet. Of the various essential information that needs to be included in the
RECTAL CANCER CLINICAL CASE PRESENTATION
 RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
RECTAL CANCER CLINICAL CASE PRESENTATION Francesco Sclafani Medical Oncologist, Clinical Research Fellow The Royal Marsden NHS Foundation Trust, London, UK esmo.org Disclosure I have nothing to declare
Printed by Martina Huckova on 10/3/2011 3:04:54 PM. For personal use only. Not approved for distribution. Copyright 2011 National Comprehensive
 Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level
Table of Contents NCCN Categories of Evidence and Consensus Category 1: Based upon high-level evidence, there is uniform NCCN consensus that the intervention is appropriate. Category 2A: Based upon lower-level
CANCER. Mrs. Davis Health Education
 CANCER Mrs. Davis Health Education Cancer Terms: Tumors: Masses of useless tissue Benign: Non-cancerous Malignant: Cancerous Metastasis: Spread of cancer from the point where it originated to other parts
CANCER Mrs. Davis Health Education Cancer Terms: Tumors: Masses of useless tissue Benign: Non-cancerous Malignant: Cancerous Metastasis: Spread of cancer from the point where it originated to other parts
Epidemiology. Objectives 8/28/2017
 Case based Discussion of Head and Neck Melanoma: Review of Epidemiology, Risk Factors, Identification, Treatments and Prevention Jacqueline M. Doucette MS FNP-C Objectives Define and identify melanoma
Case based Discussion of Head and Neck Melanoma: Review of Epidemiology, Risk Factors, Identification, Treatments and Prevention Jacqueline M. Doucette MS FNP-C Objectives Define and identify melanoma
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY
 in HEAD & NECK SURGERY") Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f
MOHS MICROGRAPHIC SURGERY: AN OVERVIEW
 MOHS MICROGRAPHIC SURGERY: AN OVERVIEW SKIN CANCER: Skin cancer is far and away the most common malignant tumor found in humans. The most frequent types of skin cancer are basal cell carcinoma, squamous
MOHS MICROGRAPHIC SURGERY: AN OVERVIEW SKIN CANCER: Skin cancer is far and away the most common malignant tumor found in humans. The most frequent types of skin cancer are basal cell carcinoma, squamous
Quiz. b. 4 High grade c. 9 Unknown
 Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
Quiz 1. 10/11/12 CT scan abdomen/pelvis: Metastatic liver disease with probable primary colon malignancy. 10/17/12 Colonoscopy with polypectomy: Adenocarcinoma of sigmoid colon measuring at least 6 mm
SAMPLING OF POST NEPHRECTOMY CANCER CARE (5)
") SAMPLING OF POST NEPHRECTOMY CANCER CARE (5) Universally recognized post-nephrectomy cancer treatment. Sampling: National Comprehensive Cancer Network (NCCN) NCCN Clinical Practice Guidelines in Oncology
SAMPLING OF POST NEPHRECTOMY CANCER CARE (5) Universally recognized post-nephrectomy cancer treatment. Sampling: National Comprehensive Cancer Network (NCCN) NCCN Clinical Practice Guidelines in Oncology