Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY
|
|
|
- Adele McKenzie
- 5 years ago
- Views:
Transcription



1 Carcinoma of Unknown Primary site (CUP) in HEAD & NECK SURGERY SEARCHING FOR THE PRIMARY? P r o f J P P r e t o r i u s H e a d : C l i n i c a l U n i t C r i t i c a l C a r e U n i v e r s i t y O f P r e t o r i a & S t e v e B i k o A c a d e m i c H o s p i t a l

2 YES! CUP in general has:.. Dismal prognosis! 7 th most common malignancy No primary site in 3 5% of patients with metastatic cancer 3 4 months mean survival <25% alive at 1 year <10% alive at 5 years Make up 15% of metastatic cervical lymph nodes Usually affect supraclavicular or lower jugular nodes Are usually adenocarcinoma CUP in Head & Neck has: SCC is most common 90% 10% of cases with metastatic SCC has no primary 1 3% of new cases of SCC annually present as CUP AdenoCA in upper neck Thyroid Salivary glands Parathyroid Metastases in upper & mid neck good prognosis on Rx
3 YES! CUP below the clavicles: CUP in Head & Neck: Generally incurable due to late presentation Represents distant metastases Brief longevity?chemotherapy Mx is directed at cure Locoregional disease Treat aggressively to prevent local recurrence To prevent primary emergence Imperative to find the primary
4 How to find the primary.comprehensive evaluation essential.to treat H & N CUP lesions optimally. Comprehensive history Extensive physical examination Appropriate imaging Full panendoscopy plus biopsies
5 The history E x p o s u r e t o etiological factors to carcinogens Occupational hazards C o u n t r y o f o r i g i n P r e v i o u s m a l i g n a n c i e s D e r m a t o l o g i c a l h i s t o r y A n y H & N s y m p t o m s pain, trismus, odynophagia, dysphagia, haemoptysis, hoarseness, epistaxis, nasal congestion, aspiration P a i n l e s s n e c k m a s s. w e e k s. m o n t h s
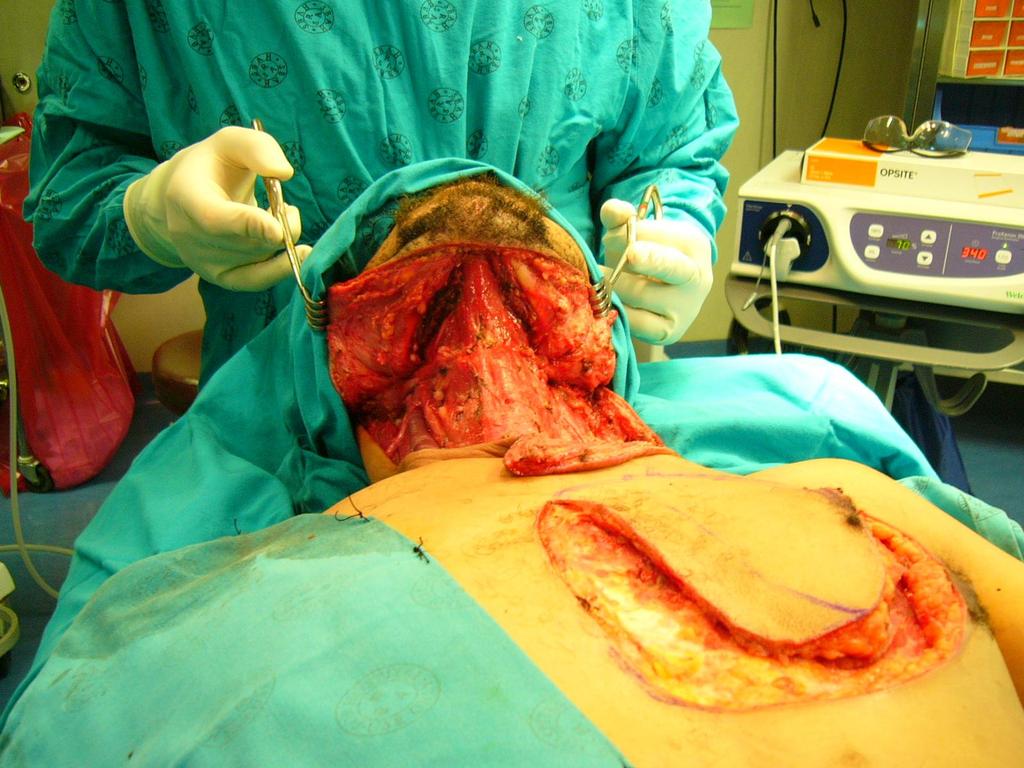
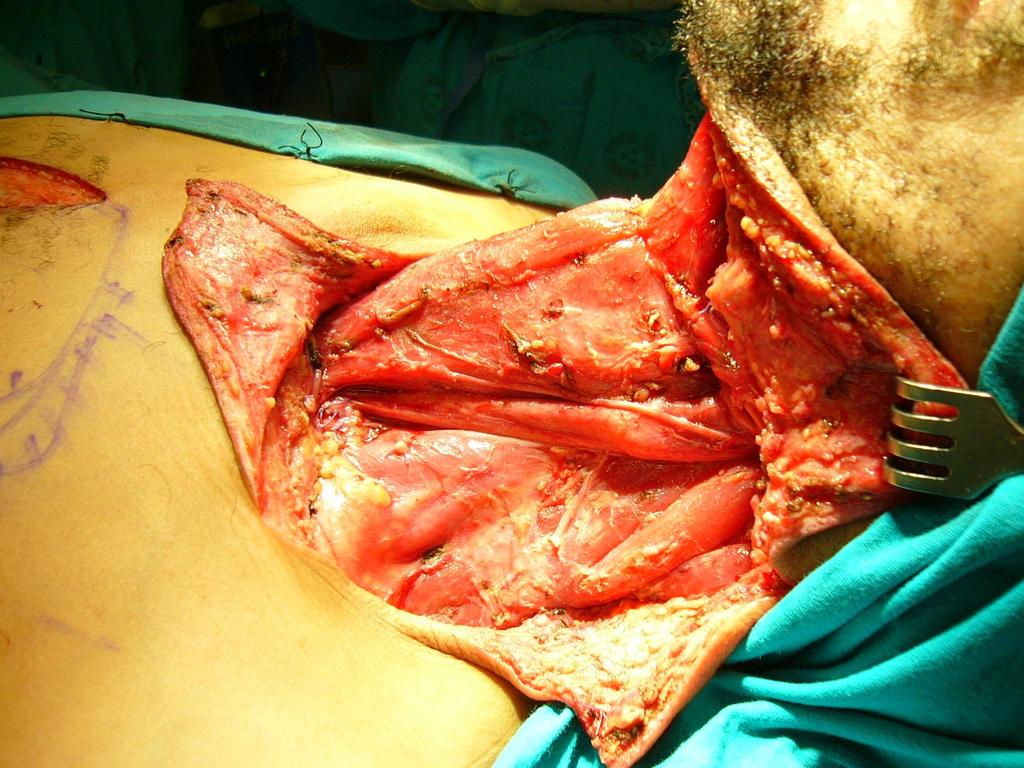
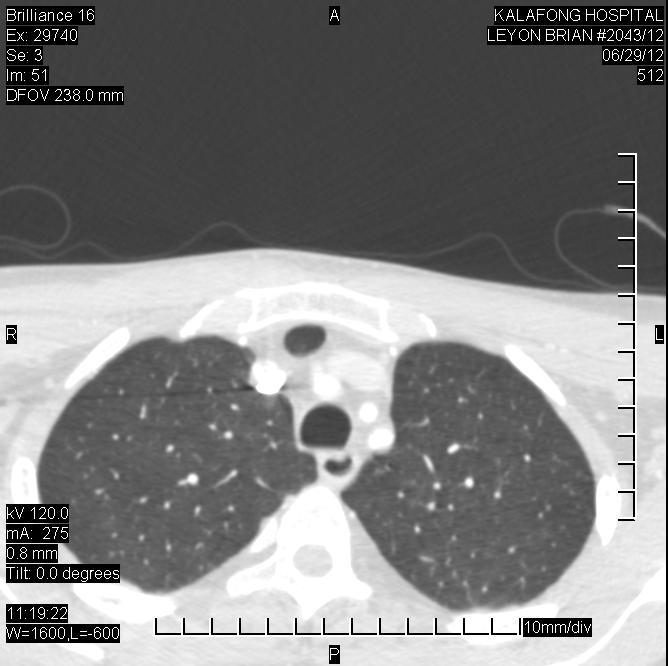
6 Case History 43 year old male Smokes 20 pack years, uses alcohol, good general condition HIV non-reactive 9/12 rapidly enlarging submental tumour Submental but slightly to the left, firm 15x15 cm mass. 3 Round, umbilicated areas of ulceration with central necrosis. Mass mobile. Floor of mouth clear. Rest of neck clinically non-significant nodes. CT-scan: ring enhancing mass in multiple cervical lymph nodes FNA: SCC Biopsy: poorly differentiated, infiltrating, keratinizing SCC TxN3Mo?CUP

7

8
9 The physical examination T h o r o u g h T o t a l H & N r e g i o n N e w s k i n l e s i o n s o r s c a r s C r a n i a l n e r v e s A L L a n a t o m i c a l s t r u c t u r e s Scalp, skin, ears, nose, nasal vestibules, salivary glands, oral cavity, oropharynx, nasopharynx, hypopharynx, larynx S u b m u c o s a l l e s i o n s. p a l p a t i o n E U A H i g h - y i e l d a n a t o m i c a l s i t e s B i o p s y s a m p l e s
10 DIFFERENTIAL DIAGNOSIS OF NECK MASSES 15% Inflammatory/Congenital Etiology in Adults (Excluding thyroid) 15% Benign 85% Neoplastic 15% Primary Lymphoma/Salivary 85% Malignant 15% From below the clavicles 85% Metastatic 85% Above the clavicles
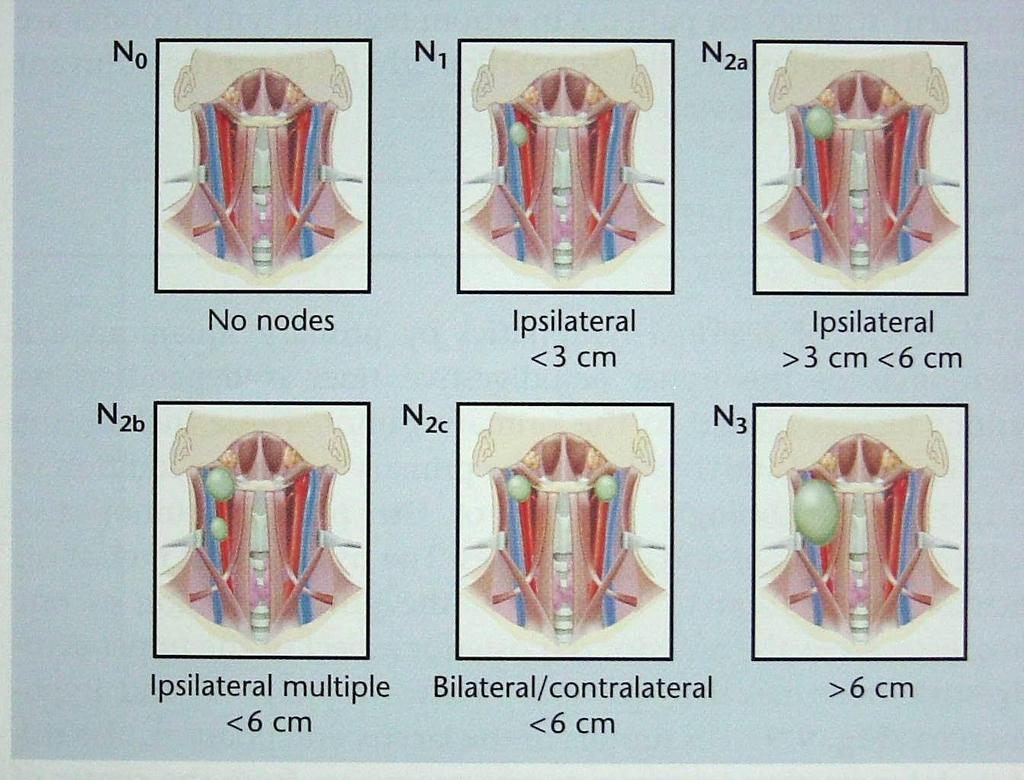
11 The neck.all zones S y s t e m a t i c e x a m i n a t i o n S i z e a n d n u m b e r F i x a t i o n V i t a l s t r u c t u r e s U n i l a t e r a l. i p s i l a t e r a l p r i m a r y B i l a t e r a l. m i d l i n e p r i m a r y L y m p h a t i c d r a i n a g e p a t t e r n s A r e a o f p r i m a r y i n d i c a t e d b y l e v e l o f l y m p h nodes affected
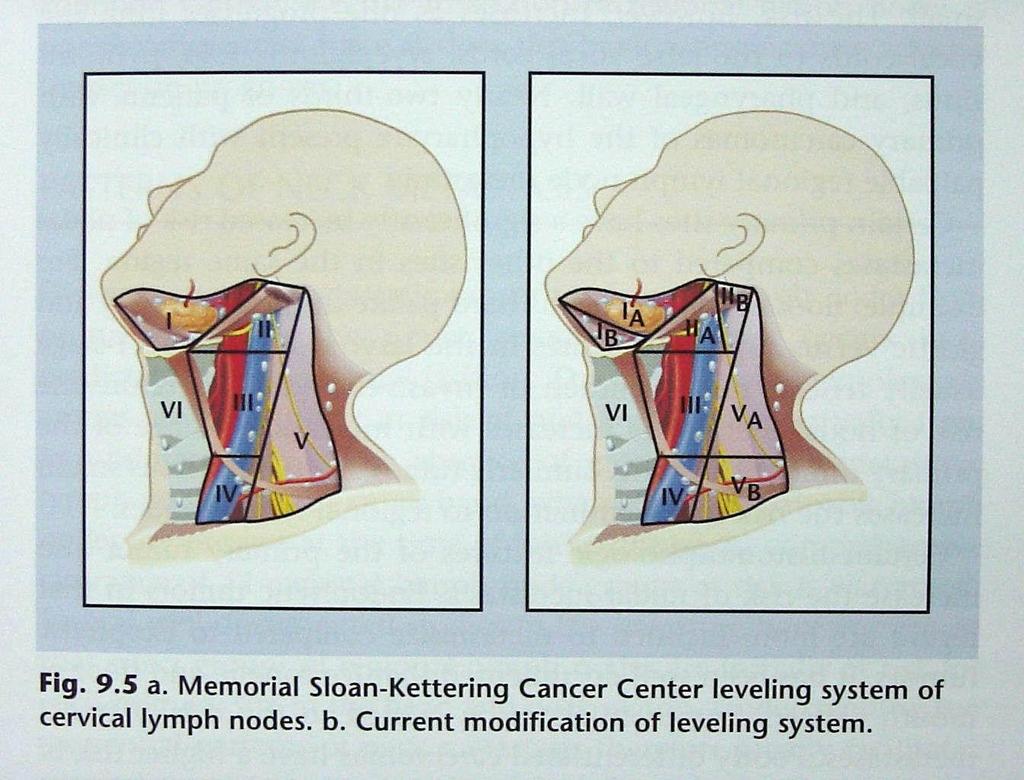
12 Regional lymph node groups draining a specific primary site as first echelon lymph nodes 20/03/2004
13 Imaging 1 st C T a n d / o r M R I w i t h c o n t r a s t 2 nd F D G - P E T o r i n t e g r a t e d P E T / C T Before panendoscopy Guide biopsies Avoid false positive FDG avidity after biopsies

14
15 Initial Dx FNA Tru-cut Histology report 1. FNA SCC 2. Tru-cut: poorly differentiated infiltrating keratinizing squamous cell carcinoma.. 3. After personal communication with pathologist..consider.?salivary gland primary Epidermoid Adenoid cystic Low grade polymorphous adenoca Plan: fresh tissue fore more immunohistochemical evaluations eg PAS, PAS-d, SMA 4. Perform panendoscopy
16 Panendoscopy D i r e c t i n s p e c t i o n a n d p a l p a t i o n F l e x i b l e f i b e r o p t i c e n d o s c o p y Sinuses, nasal cavity, nasopharynx, base of tongue, hypopharynx, larynx Directed biopsies of high-yield sites, suspicious areas, contact bleeding B i l a t e r a l t o n s i l l e c t o m y E s o p h a g o s c o p y
17 EUA Procedure: Panendoscopy Adenotonsillectomy Multiple biopsies Findings: Left base of tongue smooth, non-ulcerating mass extending to palatoglossal fold. Left tonsil superficial ulceration Adenoid tissue(minimal) in Nasopharynx Normal Right base of tongue Normal hypopharynx, pyriform fossae, post cricoid area, posterior pharyngeal wall Bimanual palpation of floor of mouth no clear submucous pathology Normal larynx and trachea up to the carina Normal oesophagus in its entirety
18 EUA Histology report Direct inspection Bimanual palpation Fibre optic endoscopy Esophagoscopy Multiple biopsies No evidence of epithelial dysplasia or of invasive malignancy in any of the sections examined of the 12 biopsies submitted. Tongue base L & R Tonsils L& R Adenoids
19 Newer Diagnostic Aids 1. H P V h u m a n p a p i l l o m a v i r u s : p o s i t i v e i n > 5 0 % o f o r o f a r y n g e a l S C C t u m o u r s vs n o n - o r o f a r y n g e a l t u m o u r s. 2. P 1 6 v a l u a b l e i m m u n o h i s t o c h e m i c a l a n a l y s i s t o i d e n t i f y H P V a s s o c i a t e d t u m o u r s. 3. E p s t e i n B a r r v i r u s s e n s i t i v e P C R m a r k e r f o r n a s o p h a r y n g e a l C A. 4. T i m e - r e s o l v e d l a s e r - i n d u c e d f l u o r e s c e n c e s p e c t r o s c o p y n o n i n v a s i v e, c a n d i s c r i m i n a t e b e t w e e n m a l i g n a n t a n d n o n - m a l i g n a n t t i s s u e. 5. I m m u n o h i s t o c h e m i c a l s t a i n i n g f o r k e r a t i n s, l e u k o c y t e c o m m o n a n t i g e n a n d S e x p r e s s e d i n m e l a n o m a 6. G e n e e x p r e s s i o n p r o f i l i n g t o i d e n t i f y s i t e o f o r i g i n o f a d e n o C A C U P l e s i o n s 7. E l e c t r o n m i c r o s c o p y H & N C U P : d e s m o s o m e s a n d t o n o f i l a m e n t s a r e c h a r a c t e r i s t i c o f S C C
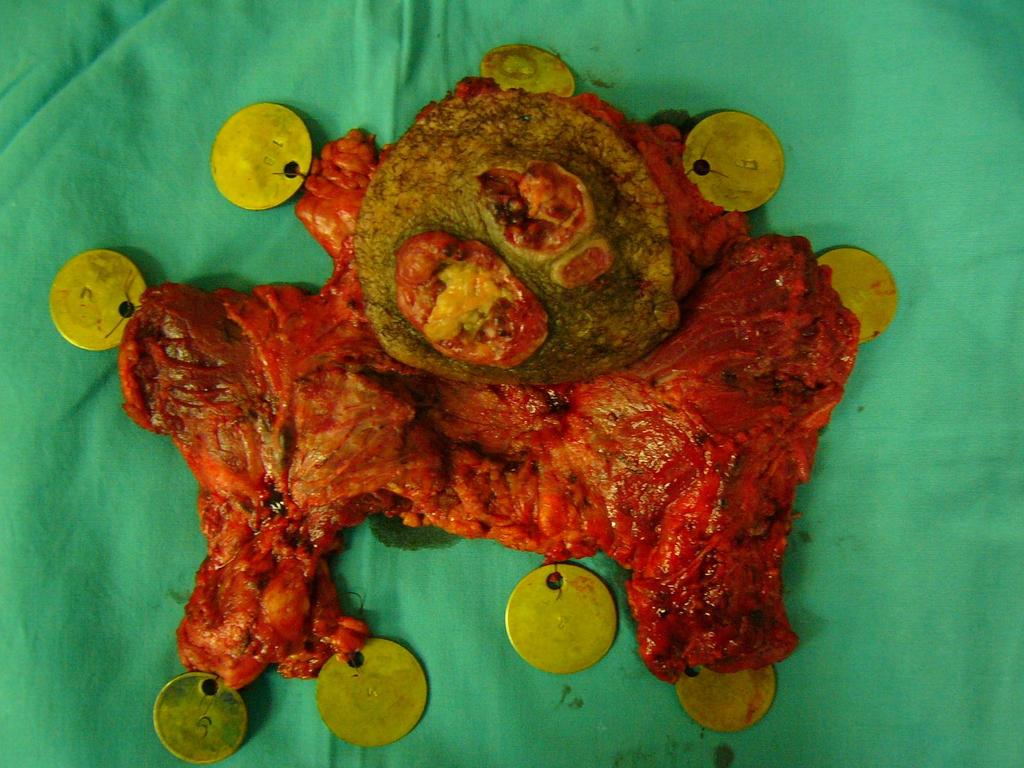
20 Final Pathological Information Personal communication with your pathologist! After more staining and re-evaluation, found: Intermediate cells Squamous or epidermoid cells Mucus-producing cells Final diagnosis: NOT A CUP LESION Mucoepidermoid CA high grade. From sublingual glands? Auclair and Brandwein classification assessing for: Nerve and blood vessel infiltration Cellular atypia >4 mitoses / 10x magnification Mucous cyst content Bone infiltration Necrosis
21 Treatment Options for H&N SCC CUP 1. N1 and N2a disease 2. Stage 2b or higher 3. Primary emergence from high yield sites 1. a)single modality RTx with IMRT technique to spare the mucosa b)formal neck dissection in selected cases 2. a)concurrent CTX-RTx with IMRT technique b)surgery reserved for persistent / recurrent disease after RTx c)formal Neck dissection and post op RTx with or without CTx is a second option 3. Radiation with/without CTx to minimize primary recurrence
22 Conclusion YES, search for the primary and treat aggressively. Locoregional control in H&N SCC CUP lesions: Two components: Controlling neck disease Preventing primary recurrence Prognosis determined by clinical stage at Dx Combination therapy best to contain neck recurrence + emergence of primary tumours SCC CUP overall survival comparable to that of patients with known primary 5 Year survival as high as 30-50%

23

24
25

26
27
28

29
30
31
32
33

34
35
36 20/03/2004
37 20/03/2004
38 CUP / CARCINOMA OF UNKNOWN PRIMARY ORIGIN Plan of Examination - patient presenting with a neck mass Skin scalp, face, ears, neck Nose inside Oral cavity -?EUA Salivary glands and Thyroid Arms, chest wall, breasts Abdomen and genitalia Transilluminate sinuses Panendoscopy - nasopharynx, larynx, oesophagus - biopsy primary / blind Lymph nodes - FNA or needle biopsy - Do not excise lymphnode primarily TB Lymphoma 20/03/2004
39 YES!!! CUP in general has:..dismal prognosis.. 7 th most common malignancy No primary site in 3 5% of patients with metastatic cancer 3 4 months mean survival <25% alive at 1 year <10% alive at 5 years Make up 15% of metastatic cervical lymph nodes Usually affect supraclavicular or lower jugular nodes Are usually adenocarcinoma
40 YES!!! CUP in Head & Neck has: 10% of cases with metastatic SCC has no primary 1 3% of new cases of SCC annually present as CUP Squamous cell cancer is the most likely histological finding (90%) in patients with: Cervical metastatic lymphadenopathy Adenocarcinoma Melanoma or even Anaplastic tumours may also be found
41 Markers
Management of Neck Metastasis from Unknown Primary
 Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
Management of Neck Metastasis from Unknown Primary.. Definition Histologic evidence of malignancy in the cervical lymph node (s) with no apparent primary site of original tumour Diagnosis after a thorough
FINE NEEDLE ASPIRATION OF ENLARGED LYMPH NODE: Metastatic squamous cell carcinoma
 Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Case Scenario 1 HNP: A 70 year old white male presents with dysphagia. The patient is a current smoker, current user of alcohol and is HPV positive. A CT of the Neck showed mass in the left pyriform sinus.
Chapter 13: Mass in the Neck. Raymond P. Wood II:
 Chapter 13: Mass in the Neck Raymond P. Wood II: In approaching the problem of a mass in the neck, one immediately encounters the fact that there are normally palpable masses in the neck (eg, almost all
Chapter 13: Mass in the Neck Raymond P. Wood II: In approaching the problem of a mass in the neck, one immediately encounters the fact that there are normally palpable masses in the neck (eg, almost all
The International Federation of Head and Neck Oncologic Societies. Current Concepts in Head and Neck Surgery and Oncology
 The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
The International Federation of Head and Neck Oncologic Societies Current Concepts in Head and Neck Surgery and Oncology www.ifhnos.net The International Federation of Head and Neck Oncologic Societies
Evaluation of Neck Mass. Disclosure. Learning Objectives 3/24/2014. Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ. Nothing to disclose
 Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
Evaluation of Neck Mass Karen T. Pitman MD, FACS Banner MDACC, Gilbert AZ Nothing to disclose Disclosure Learning Objectives 1. Describe a systematic method to evaluate a patient with a neck mass 2. Select
Cancers of unknown primary : Knowing the unknown. Prof. Ahmed Hossain Professor of Medicine SSMC
 Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Cancers of unknown primary : Knowing the unknown Prof. Ahmed Hossain Professor of Medicine SSMC Definition Cancers of unknown primary site (CUPs) Represent a heterogeneous group of metastatic tumours,
Objectives. Salivary Gland FNA: The Milan System. Role of Salivary Gland FNA 04/26/2018
 Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Salivary Gland FNA: The Milan System Dr. Jennifer Brainard Section Head Cytopathology Cleveland Clinic Objectives Introduce the Milan System for reporting salivary gland cytopathology Define cytologic
Management guideline for patients with differentiated thyroid cancer. Teeraporn Ratanaanekchai ENT, KKU 17 October 2007
 Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
Management guideline for patients with differentiated thyroid Teeraporn Ratanaanekchai ENT, KKU 17 October 2007 Incidence (Srinagarind Hospital, 2005, both sex) Site (all) cases % 1. Liver 1178 27 2. Lung
CERVICAL LYMPH NODES
 CERVICAL LYMPH NODES (ANATOMY & EXAMINATION) Hemant (DTCD 1 st YEAR) 1. Lymphatic Tissues: A Type of connective tissue that contains large numbers of lymphocytes. 2. Lymphatic Vessels: Are Tubes that assist
CERVICAL LYMPH NODES (ANATOMY & EXAMINATION) Hemant (DTCD 1 st YEAR) 1. Lymphatic Tissues: A Type of connective tissue that contains large numbers of lymphocytes. 2. Lymphatic Vessels: Are Tubes that assist
Dr Nick McIvor. Dr John Chaplin. Head & Neck Surgeon Auckland City Hospital Auckland. Auckland Head & Neck Surgeon Gillies Hospital Auckland
 Dr Nick McIvor Head & Neck Surgeon Auckland City Hospital Auckland Dr John Chaplin Auckland Head & Neck Surgeon Gillies Hospital Auckland 14:00-14:55 WS #148: Case Studies of Lumps in the Neck 15:05-16:00
Dr Nick McIvor Head & Neck Surgeon Auckland City Hospital Auckland Dr John Chaplin Auckland Head & Neck Surgeon Gillies Hospital Auckland 14:00-14:55 WS #148: Case Studies of Lumps in the Neck 15:05-16:00
Lecture 07. Lymphatic's of Head & Neck. By: Dr Farooq Amanullah Khan PMC
 Lecture 07 Lymphatic's of Head & Neck By: Dr Farooq Amanullah Khan PMC Dated: 28.11.2017 Lymphatic Vessels Of the 800 lymph nodes in the human body, 300 are in the Head & neck region. The lymphatic vessels
Lecture 07 Lymphatic's of Head & Neck By: Dr Farooq Amanullah Khan PMC Dated: 28.11.2017 Lymphatic Vessels Of the 800 lymph nodes in the human body, 300 are in the Head & neck region. The lymphatic vessels
Cervical Lymph Nodes
 Cervical Lymph Nodes Diana Gaitini, MD Unit of Ultrasound, Department of Medical Imaging Rambam Medical Center and Faculty of Medicine Technion, Israel Institute of Technology Haifa, Israel Learning Targets
Cervical Lymph Nodes Diana Gaitini, MD Unit of Ultrasound, Department of Medical Imaging Rambam Medical Center and Faculty of Medicine Technion, Israel Institute of Technology Haifa, Israel Learning Targets
Central Poorly Differentiated Adenocarcinoma of the Maxilla: Report of a Case
 Kobe J. Med. Sci., Vol. 49, No. 2, pp. 45-49, 2003 Central Poorly Differentiated Adenocarcinoma of the Maxilla: Report of a Case MASAHIRO UMEDA 1), SATOSHI YOKOO 1), YASUYUKI SHIBUYA 1), TAKAHIDE KOMORI
Kobe J. Med. Sci., Vol. 49, No. 2, pp. 45-49, 2003 Central Poorly Differentiated Adenocarcinoma of the Maxilla: Report of a Case MASAHIRO UMEDA 1), SATOSHI YOKOO 1), YASUYUKI SHIBUYA 1), TAKAHIDE KOMORI
Head & Neck Clinical Sub Group. Network Agreed Imaging Guidelines for UAT and Thyroid Cancer. Measure Nos: 11-1C-105i & 11-1C-106i
 Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Greater Manchester, Lancashire & South Cumbria Strategic Clinical Network & Senate Head & Neck Clinical Sub Group Network Agreed Imaging Guidelines for UAT and Thyroid Cancer Measure Nos: 11-1C-105i &
Salivary Glands 3/7/2017
 Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Salivary Glands 3/7/2017 Goals and objectives Focus on the entities unique to H&N Common board type facts Information for your future practice Salivary Glands Salivary Glands Major gland. Paratid. Submandibular.
Case Scenario. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Case Scenario 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of alcohol.
Cystic carcinoma of the neck
 Case Report Brunei Int Med J. 2010; 6 (1): 56-60 Cystic carcinoma of the neck Prathibha Parampalli SUBRHAMANYA, Ghazala KAFEEL, Hla OO, Pemasiri Upali TELISINGHE, Department of Pathology, RIPAS Hospital,
Case Report Brunei Int Med J. 2010; 6 (1): 56-60 Cystic carcinoma of the neck Prathibha Parampalli SUBRHAMANYA, Ghazala KAFEEL, Hla OO, Pemasiri Upali TELISINGHE, Department of Pathology, RIPAS Hospital,
Head and Neck Case 1 PATIENT HISTORY
 Head and Neck Case 1 PATIENT HISTORY Patient History May 7, 2007 Otolaryngology Head & Neck Subjective: Patient was recently seen by a dentist, who noted a roughness in his lower alveolus, and wanted to
Head and Neck Case 1 PATIENT HISTORY Patient History May 7, 2007 Otolaryngology Head & Neck Subjective: Patient was recently seen by a dentist, who noted a roughness in his lower alveolus, and wanted to
Case Scenario 1. 7/13/12 Anterior floor of mouth biopsy: Infiltrating squamous cell carcinoma, not completely excised.
 Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
Case Scenario 1 7/5/12 History A 51 year old white female presents with a sore area on the floor of her mouth. She claims the area has been sore for several months. She is a current smoker and user of
The many faces of extranodal lymphoma
 The many faces of extranodal lymphoma Frank Pameijer Departments of Radiology and Radiation Oncology University Medical Center Utrecht Special thanks to Ilona M Schmalfuss, MD University of Florida Gainesville,
The many faces of extranodal lymphoma Frank Pameijer Departments of Radiology and Radiation Oncology University Medical Center Utrecht Special thanks to Ilona M Schmalfuss, MD University of Florida Gainesville,
See the latest estimates for new cases of salivary gland cancers in the US and what research is currently being done.
 About Salivary Gland Cancer Overview and Types If you have been diagnosed with salivary gland cancer or are worried about it, you likely have a lot of questions. Learning some basics is a good place to
About Salivary Gland Cancer Overview and Types If you have been diagnosed with salivary gland cancer or are worried about it, you likely have a lot of questions. Learning some basics is a good place to
Salivary Gland Cytology
 Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Salivary Gland Cytology Diagnostic challenges and potential pitfalls Tarik M. Elsheikh, MD Professor and Medical Director Anatomic Pathology Cleveland Clinic FNA Salivary Gland Lesions Indications Distinguish
Management of unknown primary with neck node metastasis: Current evidence
 Management of unknown primary with neck node metastasis: Current evidence Dr. Pooja Nandwani Patel Associate Professor Dept. of Radiation Oncology GCRI, Ahmedabad Introduction- Approach to Topic What is
Management of unknown primary with neck node metastasis: Current evidence Dr. Pooja Nandwani Patel Associate Professor Dept. of Radiation Oncology GCRI, Ahmedabad Introduction- Approach to Topic What is
From GTV to CTV: A Critical Step Towards Cure. Kenneth Hu, MD Associate Professor New York University Langone Medical Center June 21, 2017
 From GTV to CTV: A Critical Step Towards Cure Kenneth Hu, MD Associate Professor New York University Langone Medical Center June 21, 2017 Head and Neck Cancer Model for Understanding CTV Expansion Radiation
From GTV to CTV: A Critical Step Towards Cure Kenneth Hu, MD Associate Professor New York University Langone Medical Center June 21, 2017 Head and Neck Cancer Model for Understanding CTV Expansion Radiation
Head and Neck Case Studies
 Head and Neck Case Studies John Chaplin & Nick McIvor www.headneck.co.nz Head and Neck lumps every lump must have a diagnosis Working diagnosis» +/- investigations Review» +/- investigations auckland head
Head and Neck Case Studies John Chaplin & Nick McIvor www.headneck.co.nz Head and Neck lumps every lump must have a diagnosis Working diagnosis» +/- investigations Review» +/- investigations auckland head
HPV and Head and Neck Cancer: What it means for you and your patients
 HPV and Head and Neck Cancer: What it means for you and your patients Financial Disclosure: None November 8, 2013 Steven J. Wang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery
HPV and Head and Neck Cancer: What it means for you and your patients Financial Disclosure: None November 8, 2013 Steven J. Wang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery
Catholic University of Louvain, St - Luc University Hospital Head and Neck Oncology Programme. Anatomopathology. Pathology 1 Sept.
 Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
Anatomopathology Pathology 1 Anatomopathology Biopsies Frozen section Surgical specimen Peculiarities for various tumor site References Pathology 2 Biopsies Minimum data, which should be given by the pathologist
Cervical Lymphadenopathy. Diagnosis and Management
 Cervical Lymphadenopathy Diagnosis and Management Case 1 Case 1: 6/12 hx of enlarging left level 2 neck mass no dysphonia, dysphagia, weight loss, stridor Ex smoker x 28 years 6-8 units of Ethanol weekly
Cervical Lymphadenopathy Diagnosis and Management Case 1 Case 1: 6/12 hx of enlarging left level 2 neck mass no dysphonia, dysphagia, weight loss, stridor Ex smoker x 28 years 6-8 units of Ethanol weekly
NASAL SEPTUM ADENOID CYSTIC CARCINOMA: A CASE REPORT
 NASAL SEPTUM ADENOID CYSTIC CARCINOMA: A CASE REPORT Shu-Yu Tai, 1 Chen-Yu Chien, 2 Chih-Feng Tai, 2,4 Wen-Rei Kuo, 2,4 Wan-Ting Huang, 3 and Ling-Feng Wang 2,4 Departments of 1 Family Medicine, 2 Otolaryngology
NASAL SEPTUM ADENOID CYSTIC CARCINOMA: A CASE REPORT Shu-Yu Tai, 1 Chen-Yu Chien, 2 Chih-Feng Tai, 2,4 Wen-Rei Kuo, 2,4 Wan-Ting Huang, 3 and Ling-Feng Wang 2,4 Departments of 1 Family Medicine, 2 Otolaryngology
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013
 EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
EVERYTHING YOU WANTED TO KNOW ABOUT. Robin Billet, MA, CTR, Head & Neck CTAP Member May 9, 2013 Head and Neck Coding and Staging Head and Neck Coding and Staging Anatomy & Primary Site Sequencing and MPH
Evaluation of Head and Neck Masses in Adults
 Evaluation of Head and Neck Masses in Adults Kristi Chang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery University of Iowa Hospitals and Clinics Annual Refresher Course for
Evaluation of Head and Neck Masses in Adults Kristi Chang, MD Associate Professor Department of Otolaryngology-Head and Neck Surgery University of Iowa Hospitals and Clinics Annual Refresher Course for
Case Scenario 1. Pathology: Specimen type: Incisional biopsy of the glottis Histology: Moderately differentiated squamous cell carcinoma
 Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 History A 52 year old male with a 20 pack year smoking history presented with about a 6 month history of persistent hoarseness. The patient had a squamous cell carcinoma of the lip removed
Case Scenario 1 Worksheet. Primary Site C44.4 Morphology 8743/3 Laterality 0 Stage/ Prognostic Factors
 CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
CASE SCENARIO 1 9/10/13 HISTORY: Patient is a 67-year-old white male and presents with lesion located 4-5cm above his right ear. The lesion has been present for years. No lymphadenopathy. 9/10/13 anterior
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu
 Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu Loma Linda University Medical Center June 12, 2007 CASE 1 76 year-old gentleman Status post right parotidectomy 1 year ago for a rare tumor
Los Angeles Society Of Pathologists Dr. Shobha Castelino Prabhu Loma Linda University Medical Center June 12, 2007 CASE 1 76 year-old gentleman Status post right parotidectomy 1 year ago for a rare tumor
My Journey into the World of Salivary Gland Sebaceous Neoplasms
 My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
My Journey into the World of Salivary Gland Sebaceous Neoplasms Douglas R. Gnepp Warren Alpert Medical School at Brown University Rhode Island Hospital Pathology Department Providence RI Asked to present
performed to help sway the clinician in what the appropriate diagnosis is, which can substantially alter the treatment of management.
 Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Hello, I am Maura Polansky at the University of Texas MD Anderson Cancer Center. I am a Physician Assistant in the Department of Gastrointestinal Medical Oncology and the Program Director for Physician
Head and Neck Squamous Subtypes
 1 Head and Neck Squamous Subtypes Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas HNSCC 5 th -6 th most common cancer 400,000/year 50% mortality Considerable
1 Head and Neck Squamous Subtypes Adel K. El-Naggar, M.D., Ph.D. The University of Texas MD Anderson Cancer Center, Houston, Texas HNSCC 5 th -6 th most common cancer 400,000/year 50% mortality Considerable
Case Scenario #1 Larynx
 Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
Case Scenario #1 Larynx 56 year old white female who presented with a 2 month history of hoarseness treated with antibiotics, but with no improvement. In the last 3 weeks, she has had a 15 lb weight loss,
AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY-
 -LIP & ORAL CAVITY-") TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
TX: primary tumor cannot be assessed T0: no evidence of primary tumor Tis: carcinoma in situ. T1: tumor is 2 cm or smaller AJCC Staging of Head & Neck Cancer (7 th edition, 2010) -LIP & ORAL CAVITY- T2:
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX
 QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
QUIZZES WITH ANSWERS FOR COLLECTING CANCER DATA: PHARYNX MP/H Quiz 1. A patient presented with a prior history of squamous cell carcinoma of the base of the tongue. The malignancy was originally diagnosed
CLINICAL MEDICATION POLICY
 CLINICAL MEDICATION POLICY Policy Name: Opdivo (nivolumab) injection Policy Number: Approved By: Medical Management, Clinical Pharmacy Products: Highmark Health Options Application: All participating hospitals
CLINICAL MEDICATION POLICY Policy Name: Opdivo (nivolumab) injection Policy Number: Approved By: Medical Management, Clinical Pharmacy Products: Highmark Health Options Application: All participating hospitals
What is head and neck cancer? How is head and neck cancer diagnosed and evaluated? How is head and neck cancer treated?
 Scan for mobile link. Head and Neck Cancer Head and neck cancer is a group of cancers that start in the oral cavity, larynx, pharynx, salivary glands, nasal cavity or paranasal sinuses. They usually begin
Scan for mobile link. Head and Neck Cancer Head and neck cancer is a group of cancers that start in the oral cavity, larynx, pharynx, salivary glands, nasal cavity or paranasal sinuses. They usually begin
Case Scenario 1. Pathology report Specimen from mediastinoscopy Final Diagnosis : Metastatic small cell carcinoma with residual lymphatic tissue
 Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Case Scenario 1 Oncology Consult: Patient is a 51-year-old male with history of T4N3 squamous cell carcinoma of tonsil status post concurrent chemoradiation finished in October two years ago. He was hospitalized
Cancer in Estonia 2014
 Cancer in Estonia 2014 Estonian Cancer Registry (ECR) is a population-based registry that collects data on all cancer cases in Estonia. More information about ECR is available at the webpage of National
Cancer in Estonia 2014 Estonian Cancer Registry (ECR) is a population-based registry that collects data on all cancer cases in Estonia. More information about ECR is available at the webpage of National
Disclosures. HPV and Head and Neck Cancer NONE 5/8/2018
 Bill Lydiatt, MD EMBA Chair Department of Surgery Methodist Hospital Clinical Professor of Surgery Creighton University HPV and Head and Neck Cancer Disclosures NONE 1 OVERVIEW Traditional Head and Neck
Bill Lydiatt, MD EMBA Chair Department of Surgery Methodist Hospital Clinical Professor of Surgery Creighton University HPV and Head and Neck Cancer Disclosures NONE 1 OVERVIEW Traditional Head and Neck
Polymorphous Low-Grade. December 5 th, 2008
 Polymorphous Low-Grade Adenocarcinoma December 5 th, 2008 Epidemiology Represents 2 nd or 3 rd most common minor salivary gland malignancy (17-26%) 1 st mucoepidermoid carcinoma Rare in reported Asian
Polymorphous Low-Grade Adenocarcinoma December 5 th, 2008 Epidemiology Represents 2 nd or 3 rd most common minor salivary gland malignancy (17-26%) 1 st mucoepidermoid carcinoma Rare in reported Asian
Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S.
 Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S. Associate Professor Division of Head and Neck Surgery Department of Otolaryngology-Head and
Head and Neck Cancer in FA: Risks, Prevention, Screening, & Treatment Options David I. Kutler, M.D., F.A.C.S. Associate Professor Division of Head and Neck Surgery Department of Otolaryngology-Head and
Respiratory Interactive Session. Elaine Borg
 Respiratory Interactive Session Elaine Borg Case 1 Respiratory Cytology 55 year old gentleman Anterior mediastinal mass EBUS FNA Case 1 Respiratory Cytology 55 year old gentleman with anterior mediastinal
Respiratory Interactive Session Elaine Borg Case 1 Respiratory Cytology 55 year old gentleman Anterior mediastinal mass EBUS FNA Case 1 Respiratory Cytology 55 year old gentleman with anterior mediastinal
Head and Neck Cancer. What is head and neck cancer?
 Scan for mobile link. Head and Neck Cancer Head and neck cancer is a group of cancers that usually originate in the squamous cells that line the mouth, nose and throat. Typical symptoms include a persistent
Scan for mobile link. Head and Neck Cancer Head and neck cancer is a group of cancers that usually originate in the squamous cells that line the mouth, nose and throat. Typical symptoms include a persistent
SALIVARY GLAND DISEASES. Omar alnoubani MD,MRCS
 SALIVARY GLAND DISEASES Omar alnoubani MD,MRCS Salivary Glands Overview Parotid gland Sublingual gland Submandibular gland Salivary glands - Types 3 Major Salivary Glands Parotid Submandibular Sublingual
SALIVARY GLAND DISEASES Omar alnoubani MD,MRCS Salivary Glands Overview Parotid gland Sublingual gland Submandibular gland Salivary glands - Types 3 Major Salivary Glands Parotid Submandibular Sublingual
Physician to Physician AJCC 8 th Edition. Head and Neck. Summary of Changes. AJCC Cancer Staging Manual, 7 th Ed. Head and Neck Chapters
 Physician to Physician Head and Neck William M. Lydiatt, MD Chair of Surgery Nebraska Methodist Hospital Clinical Professor of Surgery, Creighton University Validating science. Improving patient care.
Physician to Physician Head and Neck William M. Lydiatt, MD Chair of Surgery Nebraska Methodist Hospital Clinical Professor of Surgery, Creighton University Validating science. Improving patient care.
Nasopharynx Cancer. 1 Feb Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar)
 Dr Peter Luk (Pathology Registrar)") Nasopharynx Cancer 1 Feb 2016 Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar) Expert Panels Prof Mo Mo Tin Prof Michael Boyer Dr Raewyn Campbell Prof
Nasopharynx Cancer 1 Feb 2016 Presenters: Dr Raghav Murali-Ganesh (Radiation Oncology Registrar) Dr Peter Luk (Pathology Registrar) Expert Panels Prof Mo Mo Tin Prof Michael Boyer Dr Raewyn Campbell Prof
Volumi di trattamento del cavo orale
 SIMPOSIO: Neoplasie del cavo orale Volumi di trattamento del cavo orale F. Miccichè ! DICHIARAZIONE Relatore: Francesco Miccichè Come da nuova regolamentazione della Commissione Nazionale per la Formazione
SIMPOSIO: Neoplasie del cavo orale Volumi di trattamento del cavo orale F. Miccichè ! DICHIARAZIONE Relatore: Francesco Miccichè Come da nuova regolamentazione della Commissione Nazionale per la Formazione
Head and Neck Pathology. Macroscopy and Dissection Dr Tim Bracey Consultant Pathologist (Derriford Hospital)
") Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey Consultant Pathologist (Derriford Hospital) Outline Introduction - importance of macro Lip, tongue and oropharynx Larynx Bony resections
Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey Consultant Pathologist (Derriford Hospital) Outline Introduction - importance of macro Lip, tongue and oropharynx Larynx Bony resections
Approach to Thyroid Nodules
 Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Approach to Thyroid Nodules Alice Y.Y. Cheng, MD, FRCPC Twitter: @AliceYYCheng Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted
Oral Cancer Dr Christine Goodall Consultant Oral Surgeon University of Glasgow Dental School
 Oral Cancer Dr Christine Goodall Consultant Oral Surgeon University of Glasgow Dental School christine.goodall@glasgow.ac.uk Locations Lip, mouth, oropharynx Tongue, floor of mouth, buccal mucosa, palate,
Oral Cancer Dr Christine Goodall Consultant Oral Surgeon University of Glasgow Dental School christine.goodall@glasgow.ac.uk Locations Lip, mouth, oropharynx Tongue, floor of mouth, buccal mucosa, palate,
Salivary Gland Imaging. Mary Scanlon MD FACR October 2016
 Salivary Gland Imaging Mary Scanlon MD FACR October 2016 Objectives Recognize normal and abnormal anatomy Discuss work up, management and differential diagnosis of commonly referred clinical scenarios
Salivary Gland Imaging Mary Scanlon MD FACR October 2016 Objectives Recognize normal and abnormal anatomy Discuss work up, management and differential diagnosis of commonly referred clinical scenarios
Dr. Muhammad Shamim. Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz University
 Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA). JMHPE (Nl & Eg) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz University Email: surgeon.shamim@gmail.com
Dr. Muhammad Shamim FCPS (Pak), FACS (USA), FICS (USA). JMHPE (Nl & Eg) Assistant Professor, Dept. of Surgery College of Medicine, Prince Sattam bin Abdulaziz University Email: surgeon.shamim@gmail.com
Presented By Shirley Jordan Seay PhD, RN, CTR
 Presented By Shirley Jordan Seay PhD, RN, CTR Objectives Discuss the unintended consequences of HPV infection. Identify cancers associated with HPV infection HPV Associated Cancers Cervix Vagina Vulva
Presented By Shirley Jordan Seay PhD, RN, CTR Objectives Discuss the unintended consequences of HPV infection. Identify cancers associated with HPV infection HPV Associated Cancers Cervix Vagina Vulva
Human Papillomavirus Testing in Head and Neck Carcinomas
 Human Papillomavirus Testing in Head and Neck Carcinomas Guideline from the College of American Pathologists Early Online Release Publication: Archives of Pathology & Laboratory Medicine 12/18/2017 Overview
Human Papillomavirus Testing in Head and Neck Carcinomas Guideline from the College of American Pathologists Early Online Release Publication: Archives of Pathology & Laboratory Medicine 12/18/2017 Overview
Head and Neck Cancer How to recognize it in your office
 Head and Neck Cancer How to recognize it in your office Peter M Hunt, MD, FACS Associates in ENT/Head & Neck Surgery Director CHI Memorial Head & Neck and Melanoma Centers of Excellence September 8, 2018
Head and Neck Cancer How to recognize it in your office Peter M Hunt, MD, FACS Associates in ENT/Head & Neck Surgery Director CHI Memorial Head & Neck and Melanoma Centers of Excellence September 8, 2018
NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36
 Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
Cancer of the upper aerodigestive e tract: assessment and management in people aged 16 and over NICE guideline Published: 10 February 2016 nice.org.uk/guidance/ng36 NICE 2018. All rights reserved. Subject
AJCC Cancer Staging 8 th edition. Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx
 and Hypopharynx Larynx") AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
AJCC Cancer Staging 8 th edition Lip and Oral Cavity Oropharynx (p16 -) and Hypopharynx Larynx AJCC 7 th edition Lip and Oral cavity Pharynx Larynx KEY CHANGES Skin of head and neck (Vermilion of the lip)
1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter.
 Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
Skin Cancer follow up guidelines If NEW serious diagnosis given: 1. Written information to patient /GP: fax ASAP to GP & offer copy of consultation letter. 2. Free prescription information details. 3.
What is ACC? (Adenoid Cystic Carcinoma)
") What is ACC? (Adenoid Cystic Carcinoma) 10-9-10 Where ACC Occurs ACC (Adenoid Cystic Carcinoma) is a rare and unique form of cancer that is known to be unpredictable in nature, with a typical growth pattern
What is ACC? (Adenoid Cystic Carcinoma) 10-9-10 Where ACC Occurs ACC (Adenoid Cystic Carcinoma) is a rare and unique form of cancer that is known to be unpredictable in nature, with a typical growth pattern
Salivary ultrasound. Dr T J Beale Royal National Throat Nose & Ear and UCLH Hospitals London UK
 Salivary ultrasound Dr T J Beale Royal National Throat Nose & Ear and UCLH Hospitals London UK Two main groups of patients with presenting symptoms of: Obstructive or chronic inflammatory symptoms (salivary
Salivary ultrasound Dr T J Beale Royal National Throat Nose & Ear and UCLH Hospitals London UK Two main groups of patients with presenting symptoms of: Obstructive or chronic inflammatory symptoms (salivary
Principles of Surgical Oncology. Winnie Achilles Tierklinik Hollabrunn Lastenstrasse Hollabrunn
 Principles of Surgical Oncology Winnie Achilles Tierklinik Hollabrunn Lastenstrasse 2 2020 Hollabrunn boexi@gmx.de The first surgery provides the best chance for a cure in an animal with a tumor Clinical
Principles of Surgical Oncology Winnie Achilles Tierklinik Hollabrunn Lastenstrasse 2 2020 Hollabrunn boexi@gmx.de The first surgery provides the best chance for a cure in an animal with a tumor Clinical
The importance of knowing the lymphatic spread patterns of head and neck cancer for accurate nodal staging on CT: A practical schematic guide
 The importance of knowing the lymphatic spread patterns of head and neck cancer for accurate nodal staging on CT: A practical schematic guide Alba L. Reyes Ortiz, MD Elena Capilla, MD. Lina Cruz Hernández,
The importance of knowing the lymphatic spread patterns of head and neck cancer for accurate nodal staging on CT: A practical schematic guide Alba L. Reyes Ortiz, MD Elena Capilla, MD. Lina Cruz Hernández,
Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey
 Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey Outline Introduction - importance of macro Lip, tongue and oropharynx Larynx Bony resections Salivary glands* will not be covered specifically
Head and Neck Pathology Macroscopy and Dissection Dr Tim Bracey Outline Introduction - importance of macro Lip, tongue and oropharynx Larynx Bony resections Salivary glands* will not be covered specifically
Head & Neck Contouring
 Head & Neck Contouring Presented by James Wheeler, MD Center for Cancer Care Goshen, IN 46526 September 12, 2014 Special Thanks to: Spencer Boulter, Director of Operations (AAMD) Adam Moore, RT(T), CMD
Head & Neck Contouring Presented by James Wheeler, MD Center for Cancer Care Goshen, IN 46526 September 12, 2014 Special Thanks to: Spencer Boulter, Director of Operations (AAMD) Adam Moore, RT(T), CMD
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS. Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1.
 RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
RADIO- AND RADIOCHEMOTHERAPY OF HEAD AND NECK TUMORS Zoltán Takácsi-Nagy PhD Department of Radiotherapy National Institute of Oncology, Budapest 1. 550 000 NEW PATIENTS/YEAR WITH HEAD AND NECK CANCER ALL
2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING
 2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Eight Groups are Revised for 2018 Head & Neck Colon (includes rectosigmoid and rectum for cases diagnosed 1/1/2018 forward) Lung (2018 Draft not yet
2018 SEER Solid Tumor Manual 2018 KCR SPRING TRAINING Eight Groups are Revised for 2018 Head & Neck Colon (includes rectosigmoid and rectum for cases diagnosed 1/1/2018 forward) Lung (2018 Draft not yet
Merkel Cell Carcinoma Case # 2
 DISCHARGE SUMMARY Admitted: 10/11/2010 Discharged: 10/13/2010 Merkel Cell Carcinoma Case # 2 Chief Compliant: A 79 year old lady status post tumor on the scalp excision and left neck likely dissection
DISCHARGE SUMMARY Admitted: 10/11/2010 Discharged: 10/13/2010 Merkel Cell Carcinoma Case # 2 Chief Compliant: A 79 year old lady status post tumor on the scalp excision and left neck likely dissection
CLINICAL PRESENTATION AND RADIOLOGY QUIZ QUESTION
 Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 4/30/2011 Radiology Quiz of the Week # 18 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Donald L. Renfrew, MD Radiology Associates of the Fox Valley, 333 N. Commercial Street, Suite 100, Neenah, WI 54956 4/30/2011 Radiology Quiz of the Week # 18 Page 1 CLINICAL PRESENTATION AND RADIOLOGY
Radiology Pathology Conference
 Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
Radiology Pathology Conference Sharlin Johnykutty,, MD, Cytopathology Fellow Sara Majewski, MD, Radiology Resident Friday, August 28, 2009 Presentation material is for education purposes only. All rights
The following images were all acquired using a CTI Biograph
 Positron Emission Tomography/ Computed Tomography Imaging of Head and Neck Tumors: An Atlas Michael M. Graham, MD, PhD, and Yusuf Menda, MD Department of Radiology, University of Iowa, Iowa City, IA. Address
Positron Emission Tomography/ Computed Tomography Imaging of Head and Neck Tumors: An Atlas Michael M. Graham, MD, PhD, and Yusuf Menda, MD Department of Radiology, University of Iowa, Iowa City, IA. Address
SEER Summary Stage Still Here!
 SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
SEER Summary Stage Still Here! CCRA NORTHERN REGION STAGING SYMPOSIUM SEPTEMBER 20, 2017 SEER Summary Stage Timeframe: includes all information available through completion of surgery(ies) in the first
Appendix 1: QIICR Iowa Head and Neck Clinical Data DICOM SR Template
 Appendix 1: QIICR Iowa Head and Neck Clinical Data DICOM SR Template Table of Content s Document Histor y TID QIICR_2000. Clinical Data Repor t TID QIICR_2002. Biops y TID QIICR_2003. Surgical Procedure
Appendix 1: QIICR Iowa Head and Neck Clinical Data DICOM SR Template Table of Content s Document Histor y TID QIICR_2000. Clinical Data Repor t TID QIICR_2002. Biops y TID QIICR_2003. Surgical Procedure
PET/CT Frequently Asked Questions
 PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
PET/CT Frequently Asked Questions General Q: Is FDG PET specific for cancer? A: No, it is a marker of metabolism. In general, any disease that causes increased metabolism can result in increased FDG uptake
6. Cervical Lymph Nodes and Unknown Primary Tumors of the Head and Neck
 1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
1 Terms of Use The cancer staging form is a specific document in the patient record; it is not a substitute for documentation of history, physical examination, and staging evaluation, or for documenting
Neck lumps in children
 Neck lumps in children Midline Lateral Midline neck lumps Thyroglossal cyst - 80% Dermoid cyst Submental lymph node Ectopic thyroid Some rare lesions Thyroglossal cyst Diagnosis: midline, usually overlying
Neck lumps in children Midline Lateral Midline neck lumps Thyroglossal cyst - 80% Dermoid cyst Submental lymph node Ectopic thyroid Some rare lesions Thyroglossal cyst Diagnosis: midline, usually overlying
Cytologic Evaluation of the Enlarged Neck Node: FNAC Utility in Metastatic Neck Disease
 ISPUB.COM The Internet Journal of Pathology Volume 6 Number 2 Cytologic Evaluation of the Enlarged Neck Node: FNAC Utility in Metastatic Neck Disease I Bagwan, S Kane, R Chinoy Citation I Bagwan, S Kane,
ISPUB.COM The Internet Journal of Pathology Volume 6 Number 2 Cytologic Evaluation of the Enlarged Neck Node: FNAC Utility in Metastatic Neck Disease I Bagwan, S Kane, R Chinoy Citation I Bagwan, S Kane,
4/22/2010. Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey.
 Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Management of Differentiated Thyroid Cancer: Head Neck Surgeon Perspective Hakan Korkmaz, MD Assoc. Prof. of Otolaryngology Ankara Dıșkapı Training Hospital-Turkey Thyroid gland Small endocrine gland:
Thyroid INTRODUCTION ANATOMY SUMMARY OF CHANGES
 AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
AJC 7/14/06 1:19 PM Page 67 Thyroid C73.9 Thyroid gland SUMMARY OF CHANGES Tumor staging (T) has been revised and the categories redefined. T4 is now divided into T4a and T4b. Nodal staging (N) has been
Shadow because the air
 Thyroid Ultrasound Thyroid US examination needs: 1. high frequency transducer 2. extended patient's neck 3. check all the neck area because the swelling could be in areas other than the thyroid such as
Thyroid Ultrasound Thyroid US examination needs: 1. high frequency transducer 2. extended patient's neck 3. check all the neck area because the swelling could be in areas other than the thyroid such as
Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies. Agenda
 Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Head & Neck Squamous Carcinoma: Artifacts, Challenges, and Controversies Jennifer L. Hunt, MD, MEd Aubrey J. Hough Jr, MD, Endowed Professor of Pathology Chair of Pathology and Laboratory Medicine University
Neck mass Evaluation & Management OTOLARYNGOLOGY, HEAD & NECK SURGICAL ONCOLOGY
 Neck mass Evaluation & Management MOHAMMED ALESSA MBBS,FRCSC ASSISTANT PROFESSOR CONSULTANT OTOLARYNGOLOGY, HEAD & NECK SURGICAL ONCOLOGY KSU, MEDICAL CITY & KKUH Objectives Obtain map overview in neck
Neck mass Evaluation & Management MOHAMMED ALESSA MBBS,FRCSC ASSISTANT PROFESSOR CONSULTANT OTOLARYNGOLOGY, HEAD & NECK SURGICAL ONCOLOGY KSU, MEDICAL CITY & KKUH Objectives Obtain map overview in neck
ANALYSIS OF SECONDARY NECK NODES IN MALIGNANCIES OF UPPER AERODIGESTIVE TRACT
 CIBTech Journal of Surgery ISSN: 39-3875 (Online) 03 Vol. () May-August, pp.-6/renukananda et al. ANALYSIS OF SECONDARY NECK NODES IN MALIGNANCIES OF UPPER AERODIGESTIVE TRACT Renukananda G.S., Santosh
CIBTech Journal of Surgery ISSN: 39-3875 (Online) 03 Vol. () May-August, pp.-6/renukananda et al. ANALYSIS OF SECONDARY NECK NODES IN MALIGNANCIES OF UPPER AERODIGESTIVE TRACT Renukananda G.S., Santosh
DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV
 DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV NEOPLASMS A) Epithelial I. Benign Pleomorphic adenoma( Mixed tumour) Adenolymphoma (Warthin s tumour) Oxyphil adenoma (Oncocytoma)
DISORDERS OF THE SALIVARY GLANDS Neoplasms Dr.M.Baskaran Selvapathy S IV NEOPLASMS A) Epithelial I. Benign Pleomorphic adenoma( Mixed tumour) Adenolymphoma (Warthin s tumour) Oxyphil adenoma (Oncocytoma)
Surgery in Head and neck cancers.principles. Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer
 Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
Surgery in Head and neck cancers.principles Dr Diptendra K Sarkar MS,DNB,FRCS Consultant surgeon,ipgmer Email:diptendrasarkar@yahoo.co.in HNC : common inclusives Challenges Anatomical preservation R0 Surgical
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital
 C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital Objectives Review basics of head and neck imaging Discuss our spatial approach
C. Douglas Phillips, MD FACR Director of Head and Neck Imaging Weill Cornell Medical Center NewYork Presbyterian Hospital Objectives Review basics of head and neck imaging Discuss our spatial approach
Head & Neck Staging. Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging
 AJCC 8 th Edition Staging Head & Neck Staging Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving
AJCC 8 th Edition Staging Head & Neck Staging Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving
Parotid Disease Case Discussions. Valerie Jefford November 28, 2002
 Parotid Disease Case Discussions Valerie Jefford November 28, 2002 Case 1 44 y.o. man referred with lump anterior to R ear. Q1 What do you want to know? no pain 2 years but bigger now Smoker Q2 What to
Parotid Disease Case Discussions Valerie Jefford November 28, 2002 Case 1 44 y.o. man referred with lump anterior to R ear. Q1 What do you want to know? no pain 2 years but bigger now Smoker Q2 What to
AJCC 8 th Edition Staging. Head & Neck Staging. Learning Objectives. This webinar is sponsored by. the Centers for Disease Control and Prevention.
 AJCC 8 th Edition Staging Head & Neck Staging Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving
AJCC 8 th Edition Staging Head & Neck Staging Donna M. Gress, RHIT, CTR Technical Editor, AJCC Cancer Staging Manual First Author, Chapter 1: Principles of Cancer Staging Validating science. Improving
64 y.o. F with CLL and leg tumour
 64 y.o. F with CLL and leg tumour Case History Excision with split-skin grafting Histology moderately differentiated squamous cell carcinoma with large areas of necrosis and brisk mitotic activity.
64 y.o. F with CLL and leg tumour Case History Excision with split-skin grafting Histology moderately differentiated squamous cell carcinoma with large areas of necrosis and brisk mitotic activity.
Case Scenario 1. 4/19/13 Bone Scan: No scintigraphic findings to suggest skeletal metastases.
 Case Scenario 1 3/8/13 H&P 68 YR W/M presents w/elevated PSA. Patient is a non-smoker, current alcohol use. Physical Exam: On digital rectal exam the sphincter tone is normal and there is a 1 cm nodule
Case Scenario 1 3/8/13 H&P 68 YR W/M presents w/elevated PSA. Patient is a non-smoker, current alcohol use. Physical Exam: On digital rectal exam the sphincter tone is normal and there is a 1 cm nodule
Evaluation and Management of Thyroid Nodules. Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada
 Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Evaluation and Management of Thyroid Nodules Nick Vernetti, MD, FACE Palm Medical Group Las Vegas, Nevada Disclosure Consulting Amgen Speaking Amgen Objectives Understand the significance of incidental
Pathology of Sarcoma ELEANOR CHEN, MD, PHD, ASSISTANT PROFESSOR DEPARTMENT OF PATHOLOGY UNIVERSITY OF WASHINGTON
 Pathology of Sarcoma ELEANOR CHEN, MD, PHD, ASSISTANT PROFESSOR DEPARTMENT OF PATHOLOGY UNIVERSITY OF WASHINGTON Presentation outline Background and epidemiology of sarcomas Sarcoma classification Sarcoma
Pathology of Sarcoma ELEANOR CHEN, MD, PHD, ASSISTANT PROFESSOR DEPARTMENT OF PATHOLOGY UNIVERSITY OF WASHINGTON Presentation outline Background and epidemiology of sarcomas Sarcoma classification Sarcoma
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules
 Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in
Take Home Quiz 1 Please complete the quiz below prior to the session. Use the Multiple Primary and Histology Rules Case 1 72 year old white female presents with a nodular thyroid. This was biopsied in