Myelodysplastic Syndromes: WHO 2008
|
|
|
- Rosaline Griffith
- 5 years ago
- Views:
Transcription
 Weill Medical College of Cornell University New York, NY Congresso Nazionale SIE - Società Italiana di Ematologia - MIC")
1 Myelodysplastic Syndromes: WHO 2008 Attilio Orazi, M.D., FRCPath. (Engl.) Weill Medical College of Cornell University New York, NY Congresso Nazionale SIE - Società Italiana di Ematologia - MIC Milano Convention Centre. Milano Ottobre, 2009
2 MDS are clinically heterogeneous: Classification/Scoring Systems Based on morphologic differences including % blasts FAB 1976, 1982 FAB plus dysplasia (10% rule; uni vs. multi), and cytogenetics (5q-) IPSS 1997 WHO 2001 WHO 2008 WPSS 2007 Based on % blasts, karyotype, # of cytopenias Based on WHO classification and Transfusion Table courtesy of Dr. John Bennett
3 Myelodysplastic syndromes Key diagnostic points and updates
4 Guidelines: recommended levels for defining cytopenias: Hemoglobin <10 g/dl Neutrophil count <1.8 x10 9 /L Platelet count <100 x10 9 /L Values higher than these are not exclusionary of a diagnosis of MDS, if definitive morphologic and/or cytogenetic findings consistent with MDS are present
5 Morphologic Guidelines for the Diagnosis and Classification of MDS: Dyserythropoiesis, dysgranulopoiesis: >10% of cells on the BM aspirate smear Dysmegakaryopoiesis >10% of cells evaluated on 30 megakaryocytes at least (BM aspirate smear or biopsy) Ring sideroblasts (iron stain of aspirate) Blast percentage Correlate the findings with marrow biopsy


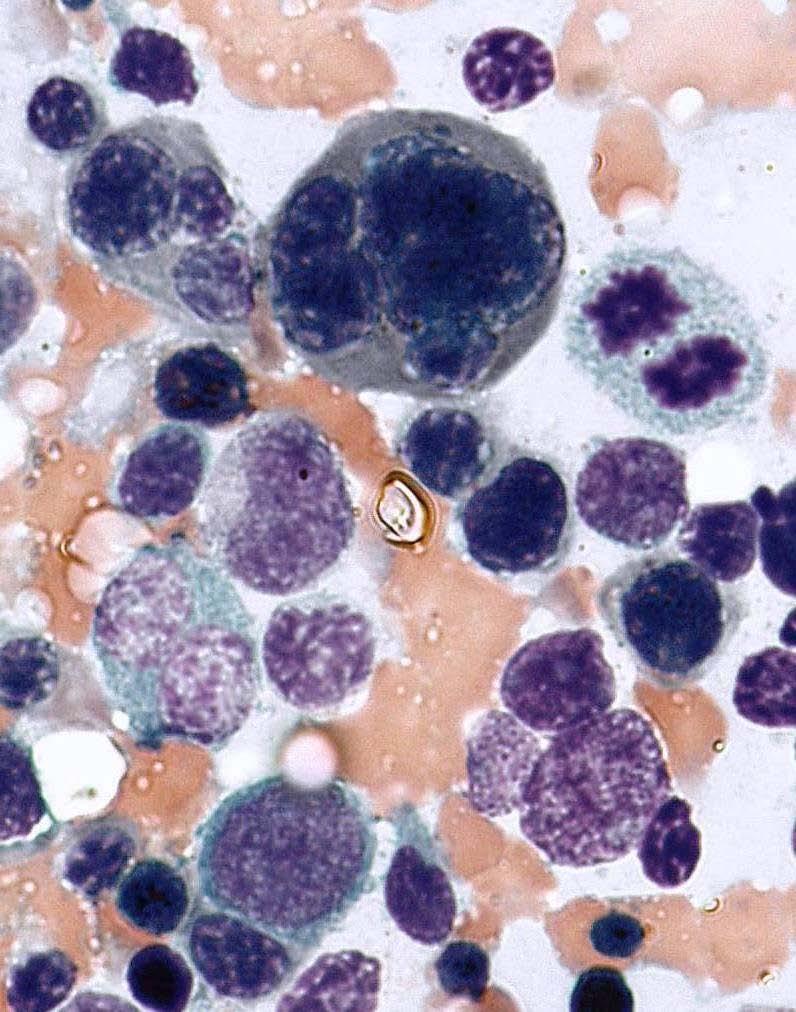
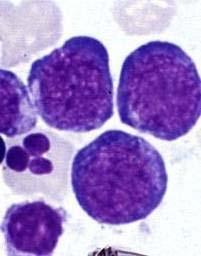
6 Erythroid precursors - multinucleation/asymmetrical nuclei and/or nuclear bridging




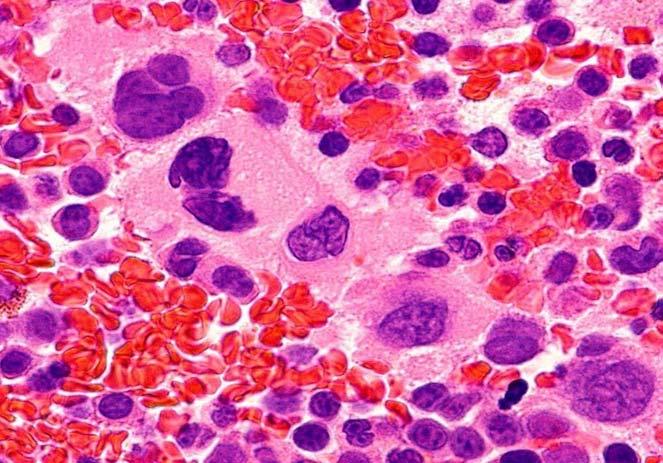
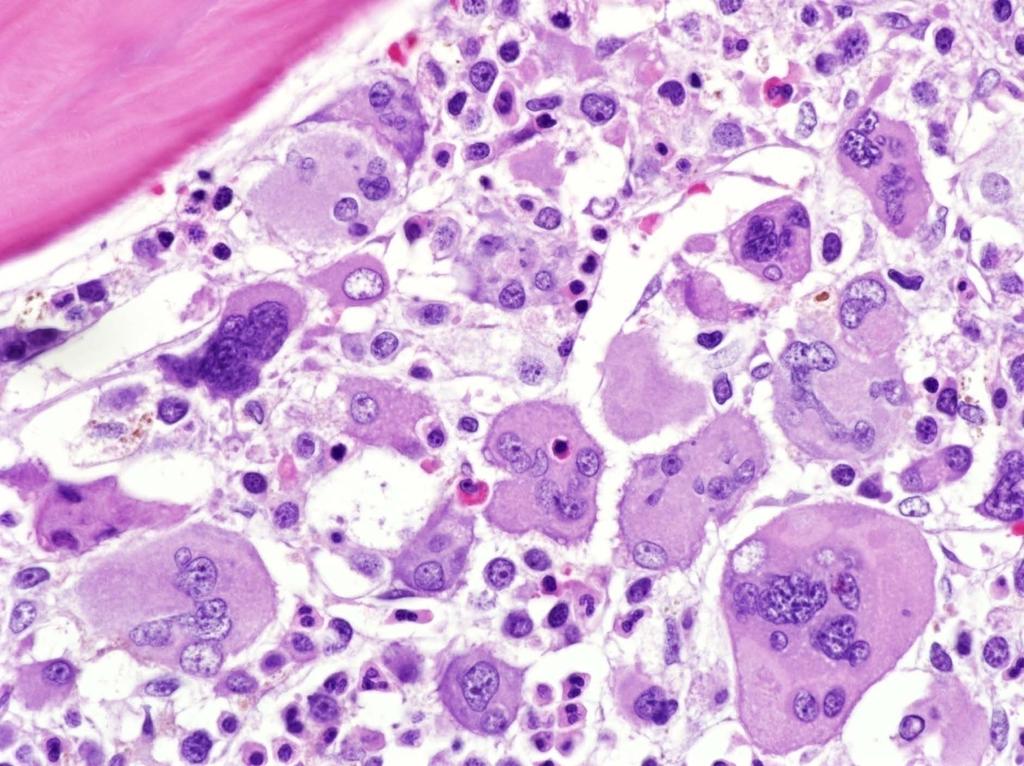
7 Granulocytes Pelger-Huet like nuclei, hypogranular cytoplasms Megakaryocytes Dwarf, non/ hypolobated forms including micromegakaryos

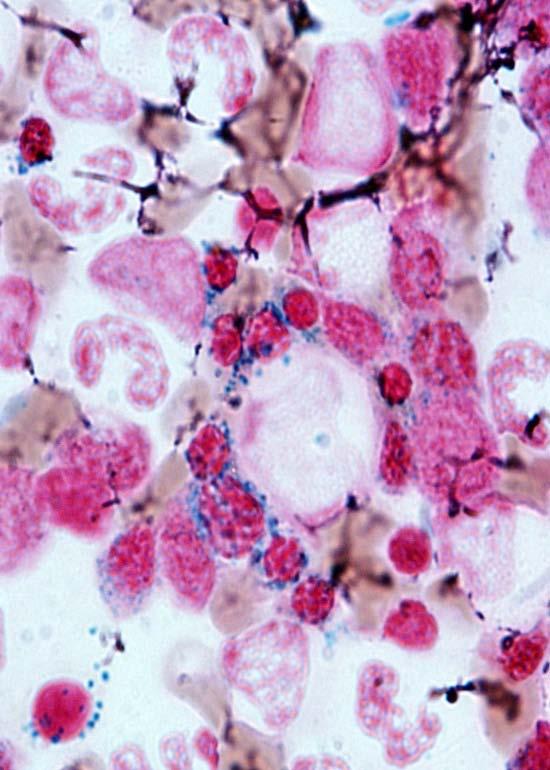
8 Definition of Ring Sideroblasts (updated from 3 rd Edition) > 15% erythroblasts with 1/3 or more of the nucleus encircled by >5 iron granules (was >10)



9 Blast Count PB 200 / BM 500 cell differential Cells counted as blasts include: - Myeloblasts - Monoblasts - Mk-blasts But not erythroblasts or promyelocytes! Mufti et al. Haematologica. 2008; 93:1712-7
10 The role of BM biopsy in MDS is better described in the 4 th edition Quality check for the adequacy of BM aspirate Provides information on stroma and cellularity (e.g. fibrosis, fatty marrow) Yields tissue for a number of studies: - immunohistochemistry - in-situ hybridization - molecular procedures (e.g. microdissection)

11 Blast count is poorly reproducible particularly in thick paraffin sections. Clusters of blasts more specific.
.")

12 Blasts and blast clusters identification made easier by immunohistology (e.g. CD34, CD117). Micromegakaryocytes by CD61 or CD42b CD34 pos. cell clusters: 3-5 cells CD42b pos. dwarf- / micro- megs.
13 Flow cytometry to demonstrate an abnormal myeloid maturation (abnormalities in light scatter and antigenic expression) Cases with inconclusive morphologic and cytogenetic findings and >3 or more aberrant features by flow cytometry should be reevaluated over several months for definitive morphologic or cytogenetic evidence of MDS Utility of CD14/CD56 in CMML Substitution of blast % determined by flow cytometry for a visual blast count is discouraged
14 Interlaboratory variability issues: still work in progress Ogata K, et al. Diagnostic utility of flow cytometry in low-grade myelodysplastic syndromes: a prospective validation study. Haematologica Aug;94(8): Epub 2009 Jun 22. van de Loosdrecht AA et al. Standardization of flow cytometry in myelodysplastic syndromes: report from the first European LeukemiaNet working conference on flow cytometry in myelodysplastic syndromes. Haematologica Aug;94(8):
15 MDS: WHO 2008 Subtypes and changes
16 2008 WHO Classification of MDS Refractory Cytopenia with Unilineage Dysplasia (RCUD) Refractory Anemia (RA) Refractory Neutropenia (RN) Refractory Thrombocytopenia (RT) Refractory Anemia with Ring Sideroblasts (RARS) Refractory Cytopenia with Multilineage Dysplasia (RCMD) Refractory Anemia with Excess of Blasts (RAEB) Subtypes: RAEB - 1, RAEB 2 Myelodysplastic Syndrome with isolated del(5q) chrom. abnormality Myelodysplastic syndrome, Unclassifiable (MDS,U)
17 Refractory cytopenia with Mono-/bi-cytopenia 1 Dysplasia ( 10%) unilineage unilineage dysplasia No or <1% blasts 2,3 <5% blasts (RA, RN, RT) PB BM <15% ring sideroblasts Refractory anemia with Anemia Erythroid dysplasia only ring sideroblasts No blasts <5% blasts 15% ring sideroblasts Refractory cytopenia with Cytopenia(s) Dysplasia in 10% of the multilineage dysplasia No or <1% blasts 2,3 cells of two or more lineages <5% blasts < or >15% ring sideroblasts 1 Pancytopenia= MDS,u 2 If 1% blasts in PB (<5% blasts in BM)= MDS,u 3 If 2-4% blasts in PB (< 5% blasts in BM)= RAEB-1 [Note: Monocytes < /L; No Auer rods]
18 RAEB-1 PB Cytopenias <5% blasts* No Auer rods BM Uni- or multi-lineage dysplasia 5 9% blasts* No Auer rods *Also RAEB-1 if 2-4% PB blasts in cases of RCUD or RCMD with < 5% blasts in BM RAEB-2 Cytopenias 5 19% blasts Auer rods +/- Auer rods +/- Uni- or multi-lineage dysplasia 10 19% blasts MDS with isolated del(5q) Anemia, usually normal or mildly increased platelets Normal to increased megakaryocytes with hypolobated nuclei [Note: Monocytes < /L] No or <1% blasts <5% blasts No Auer rods No Auer rods
19 Diagnostic P.B. diagnostic algorithm algorithm for MDS: for P.B. MDS smear with BM (200 <5% cell blasts differential) (P.B. smear 200 cell differential) Step 1:Type of Cytopenia Mono-bicytopenia Pancytopenia Step 2: P.B. Blast Percentage Step 2: P.B. Blast Percentage No or <1% UD = RCUD UD = RARS * MD = RCMD * no blasts, > 15% RS 1%: MDS,u 2-4%: RAEB %: RAEB-2 No or <1% UD = MDS,u MD = RCMD
")
20 MDS with isolated 5q- Frequent erythroid hypoplasia Lenalidomide efficacy; potential leukemogenic effect A subset of patient with JAK2 mutation is mentioned (i.e. the so called proliferative variant)
 Thrombocytosis plus granulocytic proliferation in the BM and/or PB")
 Higher WBC (5.21 vs 4.45x10 9 /L; P=0.012) No difference in median HB (9.0 vs 8.")
21 Isolated 5q- associated with JAK2 mutation (6.2% of isolated 5q- cases) Thrombocytosis plus granulocytic proliferation in the BM and/or PB JAK2 positive cases had a trend towards: Higher platelet count (475 vs 250 x 10 9 /L; P=0.15) Higher WBC (5.21 vs 4.45x10 9 /L; P=0.012) No difference in median HB (9.0 vs 8.7 g/dl; P=0.272) Ingram et al: Leukemia 2006;20:
22 MDS, unclassifiable (3 settings) 1. Patients with refractory cytopenia with unilineage dysplasia (RCUD) or refractory cytopenia with multilineage dysplasia (RCMD) but with 1% blasts in the peripheral blood 2. Cases of MDS with unilineage dysplasia which are associated with pancytopenia. RCUD (in contrast with RCMD) only allows for a single cytopenia or bicytopenia
23 3. Persistent (6 mo.) cytopenia(s) lacking morphologic features of MDS, but with cytogenetic abnormalities presumptive for MDS* +8* -7 or del(7q) t(11;16)(q23;p13.3) -5 or del(5q) t(3;21)(q26.2;q22.1) del(20q)* -Y* i(17q) or t(17p) -13 or del(13q) del(11q) del(12p) or t(12p) del(9q) idic(x)(q13)) t(1;3)(p36.3;q21.2) t(2;11)(p21;q23) inv(3)(q21q26.2) t(6;9)(p23;q34) * As single cytogenetic abnormality, in the absence of morphologic findings, is insufficient evidence for MDS
24 Subtypes of MDS difficult to distinguish from other myeloid neoplasms (discussed in the 4 th edition) Hypoplastic MDS from acquired aplastic anemia MDS with fibrosis from other fibrotic myeloid neoplasms (e.g. PMF) MDS with > 50% erythroblasts from acute erythroid leukemia
 AA")


25 MDS, hypoplastic (Cellularity <30% in patients <70 years old, and <20% in >70 years old) AA CD34: h-mds vs. AA: p=.001 hypo-mds hypo-mds Maschek H,et al. Ann Hematol 1993; 66: Orazi et al. Am J Clin Pathol 1997; 107: Bennet & Orazi. Haematologica 2009; 94:264-8
26 Hypocellularity favors response to immunosuppressive therapy? Lim ZY, et al. Low IPSS score and bone marrow hypocellularity in MDS patients predict hematological responses to antithymocyte globulin. Leukemia. 2007;21: Sloand EM, et al. Factors* affecting response and survival in patients with myelodysplasia treated with immunosuppressive therapy. J Clin Oncol. 2008;26: Sloand EM. Hypocellular myelodysplasia. Hematol Oncol Clin North Am. 2009;23: Review. *Younger age & HLA-DR15 were the most significant factors favoring response to therapy

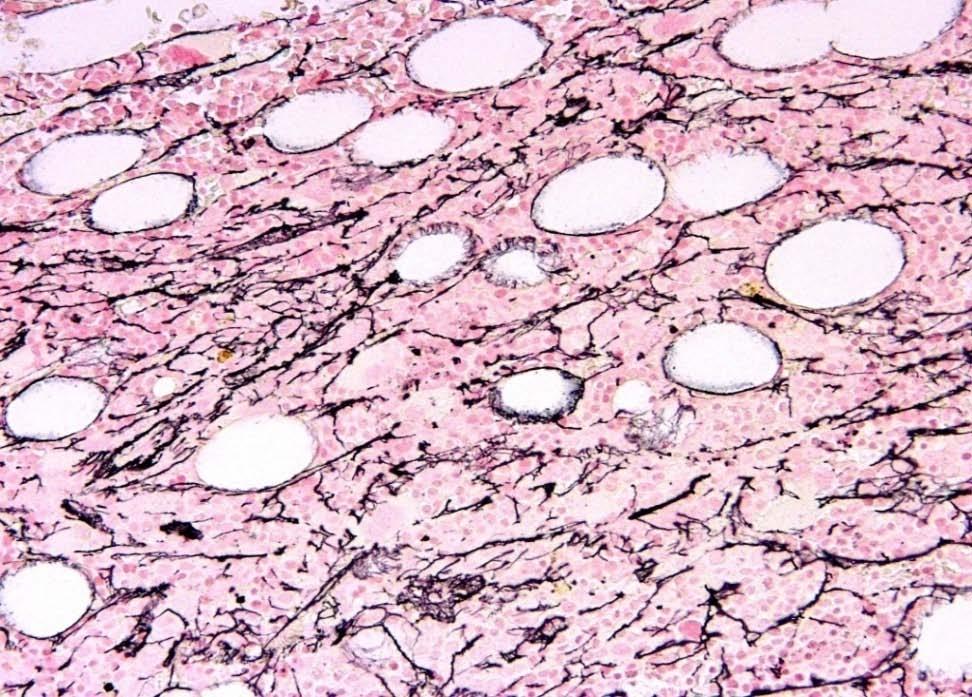
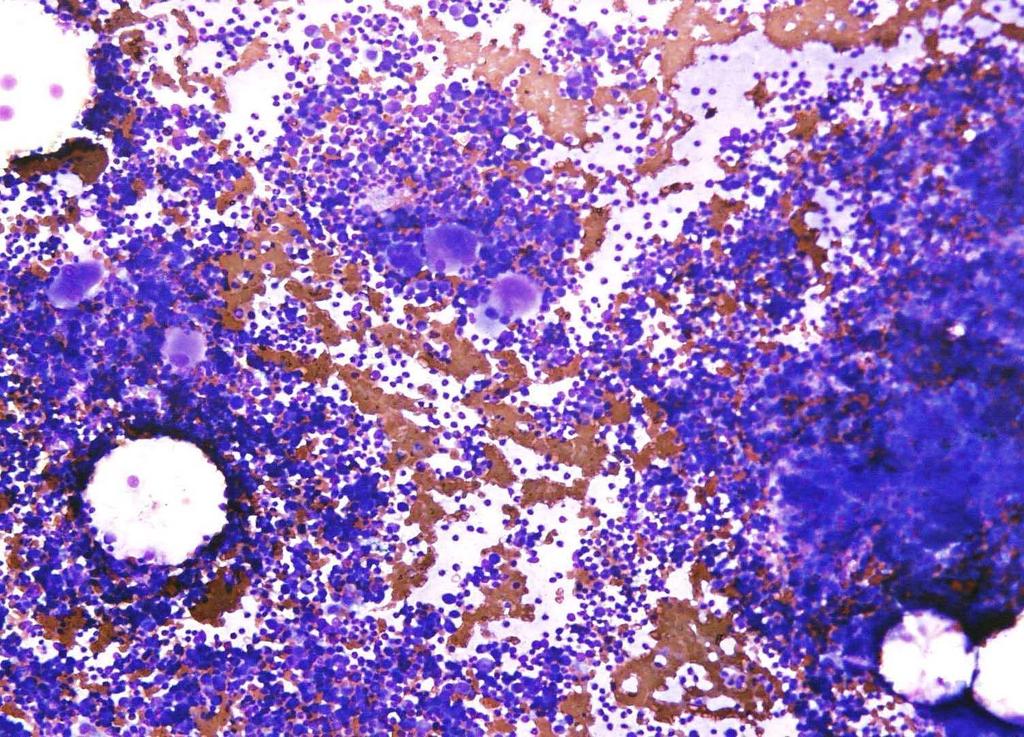
27 MDS with fibrosis (>2+ fibrosis)
28 100 II 80 % MDS fibrosis <2 Survival 60 I II I 40 p < MDS fibrosis > mo Lambertenghi-Deliliers G, Orazi A, Lucks R, et al.: Br J Haematol, 1991
29 Scott BL, et al. Marrow fibrosis as a risk factor for posttransplantation outcome in patients with advanced myelodysplastic syndrome or acute myeloid leukemia with multilineage dysplasia. Biol Blood Marrow Transplant 2007;13: Buesche G, et al. Marrow fibrosis predicts early fatal marrow failure in patients with myelodysplastic syndromes. Leukemia 2008; 22: Della Porta MG, et al. Clinical relevance of bone marrow fibrosis and CD34-positive cell clusters in primary myelodysplastic syndromes. J Clin Oncol 2009;27:754-62
30 Erythroid-rich MDS: when the erythroid cells are > 50% of all the nucleated cells A second count for the non-erythroid cells: AML, if the blasts are > 20% of the nonerythroid cells (erythroleukemia) MDS, if the blasts are less than 20% of the non-erythroid cells If MDS, then use the original blast % for further MDS subtyping
31 Myelodysplastic/Myeloproliferative Neoplasms (MDS/MPN) (Hematopoietic malignancies with hybrid features both of MDS and MPN) Chronic myelomonocytic leukemia (CMML) Atypical chronic myeloid leukemia* (acml) MDS/MPN, unclassified (MDS/MPN,u) Refractory anemia with ring sideroblasts and thrombocytosis (RARS-T) *BCR-ABL1 negative
32 Diagnosis of MDS/MPN: WHO requires to exclude In all cases the presence of Ph chromosome/bcr/abl1 fusion gene plus, in cases with eosinophilia PDGFR Alpha abnormalities PDGFR Beta abnormalities* *May resemble CMML or acml. Include cases formerly termed CMML with t(5;12)
 is not required if all other criteria")

33 CMML: definition Monocytes >1 x10 9 /L >10% of WBC Dysplasia (mono or multilineage) is not required if all other criteria are met and there is a cytogenetic abnormality or reactive causes are excluded and monocytosis has lasted for at least 3 months ANBE
 Abnormal monocytes More condensed chromatin, convoluted nuclei and more granulated Adapted from")
34 Monoblasts Promonocytes Monoblasts Large cells with abundant cytoplasm minimally vacuolated round nuclei with fine chromatin and nucleoli Promonocytes Irregular or folded nuclei, small indistinct nucleoli, fine chromatin and a more vacuolated and/or granular cytoplasm Abnormal monocytes (immature) Abnormal monocytes More condensed chromatin, convoluted nuclei and more granulated Adapted from WHO Classification of Tumors of Haematopoietic and Lymphoid Tissues. IARC: Lyon Fig.1-04 (p. 21).
35 RARS-T Its incidence is rare (underdiagnosed?) JAK2 positive in approx. 60% of cases MPL W515K/L (very rare) RARS-T has a worse outcome than ET Is controversial Wardrop D, Steensma DP. Is RARS-T a necessary or useful diagnostic category? Br J Haematol. 2009;144:809-17
36
37 BM Biopsy
38 RARS-T study (44 cases) Massachusetts General Hospital, Boston, MA 1 U. Mass Memorial Med. Center, Worcester, MA 2 Brigham and Women s Hospital, Boston, MA 3 Weill Cornell College of Medicine, New York, NY 4 Genzyme, Inc, New York, NY 5 Baystate Med. Center, Springfield, MA 5 Hasserjian RP 1, Soupir CP 1, Wang Sa A 2, Vergilio JoA 3, Orazi A 4, Dong H 5
39 Karyotype (40 patients) 31 (78%) had a normal karyotype 9 cases (22%) with abnormal karyotype which included: isolated +8 (4 cases) isolated del(20)(q11.2) (1 case) isolated Y (1 case) isolated del(11)(q23) (1 case) +1p,-6 (1 case) del(7)(q11.2)(1 case)
40 Morphology: comparative analysis of RARS-T, RARS and MPN RARS-T & RARS: have similar Erythroid hyperplasia Left shift erythrop. Dyserythropoiesis RARS-T & MPN both have: Megs. equally numerous Similarly large and pleomorphic Similarly variable fibrosis
 had")

41 Fibrosis in RARS-T 5 of 32 cases (16%) in our series 12 of 28 cases* (43%) had fibrosis: MF-1: 7 cases MF-2: 5 cases *Schmitt-Graeff AH, et al. Haematologica 2008
42 Morphology of JAK2 (-) vs. JAK2 (+) JAK2(+) cases had a significantly higher PLT and WBC counts, and a trend towards a higher HB level JAK2(+) cases had more prevalent large Megs often with staghorn or bulbous nuclear morphology while small and normal-sized Megs. were predominant in the JAK2(-) cases No differences in reticulin fibrosis and morphologic dysplasia in other lineages
43 Additional issues Prognosis Molecular pathogenesis
44 100 Overall survival of RARS-Tpatients Percent survival cases Time (months) The median follow-up for all patients was 59 months; at the time of study analysis (9/20/09), 26 patients had died..median survival for all pts. 74 months

45 Transformation to AML Our series: 4/27 (15%) cases with follow up Pich A, Godio L. RARS- T associated with JAK2V617F mutation transformed to AML with chromosomal evolution including monosomy 7. Leuk Res (2009). In press.

46 Prognostic role for JAK2 23 cases Schmitt-Graeff A et al. Haematologica 2008
47 Prognostic role for JAK2? Suggested by: Atallah E, et al. Leukemia. 2008; 22: Not confirmed by: Wang SA, et al. Leukemia. 2006;2 0: Raya JM, et al. Int J Hematol. 2008; 88: Hasserjian RP, et al. our current study
48 Molecular pathogenesis: Malcovati L, et al. Blood Aug 19. [Epub ahead of print] 19 RARS-T defined according to WHO 2008 Like in RARS, up-regulation of ALAS2 and downregulation of ABCB7 in CD34+ cells, i.e. RARS-T has distinctive sideroblastic features at the molecular level. X-chromosome inactivation shows that JAK2 pos. cells are only a fraction of clonal granulocytes 3 RARS pts. with low or normal plts. progressed to RARS-T (2/3 acquired JAK2). It may develop from RARS through the acquisition of somatic mutations of JAK2, MPL or other as-yet-unknown genes
49 Summary Morphology is still very important for diagnosis Perform always iron and reticulin stains Look out for monocytes in PB and BM and use cytochemistry and flow to confirm monocytosis Bone marrow biopsy supplemented by immunohistology (particularly useful in cases with fibrosis or fatty BM) Karyotype is mandatory. FISH may supplement BCR-ABL1 and, in cases with eosinophilia, PDGFR rearrangements Test for JAK2 when appropriate (e.g. RARS-T, 5q-)
50
Myelodysplastic syndromes
 Myelodysplastic syndromes Robert P Hasserjian Massachusetts General Hospital, Boston, MA Disclosure of Relevant Financial Relationships Dr. Hasserjian declares he has no conflict(s) of interest to disclose.
Myelodysplastic syndromes Robert P Hasserjian Massachusetts General Hospital, Boston, MA Disclosure of Relevant Financial Relationships Dr. Hasserjian declares he has no conflict(s) of interest to disclose.
Table 1: biological tests in SMD
 Table 1: biological tests in SMD Tests Mandatory Recommended Under validation Morphology Marrow aspirate Marrow biopsy 1 Iron staining Quantification of dysplasia WHO 2008 Classification Cytogenetics Conventional
Table 1: biological tests in SMD Tests Mandatory Recommended Under validation Morphology Marrow aspirate Marrow biopsy 1 Iron staining Quantification of dysplasia WHO 2008 Classification Cytogenetics Conventional
Myelodysplastic syndromes: revised WHO classification and distinction from non-neoplastic conditions
 Myelodysplastic syndromes: revised WHO classification and distinction from non-neoplastic conditions Robert P Hasserjian, MD Associate Professor Massachusetts General Hospital and Harvard Medical School
Myelodysplastic syndromes: revised WHO classification and distinction from non-neoplastic conditions Robert P Hasserjian, MD Associate Professor Massachusetts General Hospital and Harvard Medical School
Hematology Unit Lab 2 Review Material
 Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Case Presentation. Attilio Orazi, MD
 Case Presentation Attilio Orazi, MD Weill Cornell Medical College/ NYP Hospital Department of Pathology and Laboratory Medicine New York, NY United States History 60 year old man presented with anemia
Case Presentation Attilio Orazi, MD Weill Cornell Medical College/ NYP Hospital Department of Pathology and Laboratory Medicine New York, NY United States History 60 year old man presented with anemia
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls
 Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
ACCME/Disclosures. History. Hematopathology Specialty Conference Case #4 4/13/2016
 Hematopathology Specialty Conference Case #4 Sherrie L. Perkins MD, PhD University of Utah ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose
Hematopathology Specialty Conference Case #4 Sherrie L. Perkins MD, PhD University of Utah ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose
Juvenile Myelomonocytic Leukemia (JMML)
") Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
Participants Identification No. % Evaluation. Mitotic figure Educational Erythrocyte precursor, abnormal 1 0.
 Cell Identification Mitotic figure 212 99.5 Educational Erythrocyte precursor, abnormal BMD-02 The arrowed cell is a mitotic figure. It was correctly identified by 99.5% of the participants. A cell containing
Cell Identification Mitotic figure 212 99.5 Educational Erythrocyte precursor, abnormal BMD-02 The arrowed cell is a mitotic figure. It was correctly identified by 99.5% of the participants. A cell containing
What is MDS? Epidemiology, Diagnosis, Classification & Risk Stratification
 What is MDS? Epidemiology, Diagnosis, Classification & Risk Stratification Rami Komrokji, MD Clinical Director Malignant Hematology Moffitt Cancer Center Normal Blood and Bone Marrow What is MDS Myelodysplastic
What is MDS? Epidemiology, Diagnosis, Classification & Risk Stratification Rami Komrokji, MD Clinical Director Malignant Hematology Moffitt Cancer Center Normal Blood and Bone Marrow What is MDS Myelodysplastic
Hematology 101. Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD
 Hematology 101 Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD Hematocrits Plasma White cells Red cells Normal, Hemorrhage, IDA, Leukemia,
Hematology 101 Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD Hematocrits Plasma White cells Red cells Normal, Hemorrhage, IDA, Leukemia,
Myelodysplastic syndromes and the new WHO 2016 classification
 Myelodysplastic syndromes and the new WHO 2016 classification 32nd General Annual Meeting of the Belgian Hematology Society 10-11 February 2017 Gregor Verhoef, Departement of Hematology, University Hospital
Myelodysplastic syndromes and the new WHO 2016 classification 32nd General Annual Meeting of the Belgian Hematology Society 10-11 February 2017 Gregor Verhoef, Departement of Hematology, University Hospital
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed
 MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
Myelodysplastic/Myeloproliferative Neoplasms (MDS/MPN) Updated
 Updated") Myelodysplastic/Myeloproliferative Neoplasms (MDS/MPN) Updated Attilio Orazi, MD, FRCPath. (Engl.) Professor of Pathology and Laboratory Medicine Weill Cornell Medical College/NYP Hospital New York, NY
Myelodysplastic/Myeloproliferative Neoplasms (MDS/MPN) Updated Attilio Orazi, MD, FRCPath. (Engl.) Professor of Pathology and Laboratory Medicine Weill Cornell Medical College/NYP Hospital New York, NY
Myelodysplastic Syndromes: Hematopathology. Analysis of SHIP1 as a potential biomarker of Disease Progression
 Myelodysplastic Syndromes: Hematopathology. Analysis of SHIP1 as a potential biomarker of Disease Progression Carlos E. Bueso-Ramos, M.D., Ph.D Department of Hematopathology The University of Texas M.
Myelodysplastic Syndromes: Hematopathology. Analysis of SHIP1 as a potential biomarker of Disease Progression Carlos E. Bueso-Ramos, M.D., Ph.D Department of Hematopathology The University of Texas M.
ADx Bone Marrow Report. Patient Information Referring Physician Specimen Information
 ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms. Curtis A. Hanson, MD
 Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
WHO Classification 7/2/2009
 Least Malignant Myeloproliferative Disorders Myelodysplastic Syndromes Most Malignant Acute Leukemia Classifying Hematopoietic Disorders French-American-British (FAB) World Health Organization (WHO) Thanks
Least Malignant Myeloproliferative Disorders Myelodysplastic Syndromes Most Malignant Acute Leukemia Classifying Hematopoietic Disorders French-American-British (FAB) World Health Organization (WHO) Thanks
Myelodysplastic Syndromes
 Myelodysplastic Syndromes Attilio Orazi, MD, FRCPath, 1 and Magdalena B. Czader, MD, PhD 2 Key Words: Myelodysplastic syndrome; Refractory cytopenia with unilineage dysplasia; Refractory anemia with ring
Myelodysplastic Syndromes Attilio Orazi, MD, FRCPath, 1 and Magdalena B. Czader, MD, PhD 2 Key Words: Myelodysplastic syndrome; Refractory cytopenia with unilineage dysplasia; Refractory anemia with ring
Evaluation of Bone Marrow Biopsies and Aspirates ANNA PORWIT DEPARTMENT OF PATHOLOGY, LUND UNIVERSITY
 Evaluation of Bone Marrow Biopsies and Aspirates ANNA PORWIT DEPARTMENT OF PATHOLOGY, LUND UNIVERSITY DISCLOSURES NONE Learning objectives To review the rules of BMA evaluation To review the main issues
Evaluation of Bone Marrow Biopsies and Aspirates ANNA PORWIT DEPARTMENT OF PATHOLOGY, LUND UNIVERSITY DISCLOSURES NONE Learning objectives To review the rules of BMA evaluation To review the main issues
MYELODYSPLASTIC SYNDROMES
 MYELODYSPLASTIC SYNDROMES Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra university hospital, Isfahan university of medical sciences Key Features ESSENTIALS OF DIAGNOSIS Cytopenias
MYELODYSPLASTIC SYNDROMES Babak Tamizi Far MD. Assistant professor of internal medicine Al-zahra university hospital, Isfahan university of medical sciences Key Features ESSENTIALS OF DIAGNOSIS Cytopenias
Etiology. Definition MYELODYSPLASTIC SYNDROMES. De novo. Secondary MDS (10 years earlier than primary) transformation
 transformation") MYELODYSPLASTIC SYNDROMES Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics The University of Texas M.D. Anderson Cancer Center Houston, Texas No relevant COIs to
MYELODYSPLASTIC SYNDROMES Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics The University of Texas M.D. Anderson Cancer Center Houston, Texas No relevant COIs to
Changes to the 2016 WHO Classification for the Diagnosis of MDS
 Changes to the 2016 WHO Classification for the Diagnosis of MDS Welcome to Managing MDS. I am Dr. Ulrich Germing, and today, I will provide highlights from the 14th International Symposium on MDS in Valencia,
Changes to the 2016 WHO Classification for the Diagnosis of MDS Welcome to Managing MDS. I am Dr. Ulrich Germing, and today, I will provide highlights from the 14th International Symposium on MDS in Valencia,
WHO Update to Myeloproliferative Neoplasms
 WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
Myelodysplastic scoring system with flow cytometry. G Detry B Husson
 Myelodysplastic scoring system with flow cytometry G Detry B Husson Myelodysplastic syndroms Clonal haematopoietic stem cell disease characterized by dysplasia in one or more of the myeloid cell lines
Myelodysplastic scoring system with flow cytometry G Detry B Husson Myelodysplastic syndroms Clonal haematopoietic stem cell disease characterized by dysplasia in one or more of the myeloid cell lines
Morfologia normale e patologica
 Morfologia normale e patologica Gina Zini Centro di Ricerca ReCAMH Dpt. Ematologia Università Cattolica S. Cuore - Roma EMATOLOGIA DI LABORATORIO: percorsi diagnostici e obiettivi clinici. Milano 11-12
Morfologia normale e patologica Gina Zini Centro di Ricerca ReCAMH Dpt. Ematologia Università Cattolica S. Cuore - Roma EMATOLOGIA DI LABORATORIO: percorsi diagnostici e obiettivi clinici. Milano 11-12
June 11, Ella Noel, D.O., FACOI 1717 West Broadway Madison, WI
 June 11, 2018 Ella Noel, D.O., FACOI 1717 West Broadway Madison, WI 53713 policycomments@wpsic.com RE: Draft Local Coverage Determination: MolDX: MDS FISH (DL37772) Dear Dr. Noel Thank you for the opportunity
June 11, 2018 Ella Noel, D.O., FACOI 1717 West Broadway Madison, WI 53713 policycomments@wpsic.com RE: Draft Local Coverage Determination: MolDX: MDS FISH (DL37772) Dear Dr. Noel Thank you for the opportunity
RAEB-2 2 Transforming to Acute Erythroleukemia Case # 165
 RAEB-2 2 Transforming to Acute Erythroleukemia Case # 165 Sebastian J. Sasu, M.D. UCLA Medical Center, Hematopathology Los Angeles, CA and Saint John s s Health Center Santa Monica, CA Clinical History
RAEB-2 2 Transforming to Acute Erythroleukemia Case # 165 Sebastian J. Sasu, M.D. UCLA Medical Center, Hematopathology Los Angeles, CA and Saint John s s Health Center Santa Monica, CA Clinical History
APPROACH TO MYELODYSPLASTIC SYNDROMES IN THE ERA OF PRECISION MEDICINE
 APPROACH TO MYELODYSPLASTIC SYNDROMES IN THE ERA OF PRECISION MEDICINE Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics Department of Hematopathology The University
APPROACH TO MYELODYSPLASTIC SYNDROMES IN THE ERA OF PRECISION MEDICINE Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics Department of Hematopathology The University
Case Presentation No. 075
 Case Presentation No. 075 Session 4. Myelodysplastic Syndrome Cristina Montalvo, MD Baylor College of Medicine Houston, Texas 2007 Workshop of Society for Hematopathology and European Association for Haematopathology
Case Presentation No. 075 Session 4. Myelodysplastic Syndrome Cristina Montalvo, MD Baylor College of Medicine Houston, Texas 2007 Workshop of Society for Hematopathology and European Association for Haematopathology
Participants Identification No. % Evaluation. Mitotic figure Educational Erythrocyte precursor, abnormal/
 Cell Identification BMD-09 Participants Identification No. % Evaluation Mitotic figure 233 96.7 Educational Erythrocyte precursor, abnormal/ 4 1.7 Educational dysplastic nuclear features Erythrocyte precursor
Cell Identification BMD-09 Participants Identification No. % Evaluation Mitotic figure 233 96.7 Educational Erythrocyte precursor, abnormal/ 4 1.7 Educational dysplastic nuclear features Erythrocyte precursor
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure
 Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
SH A CASE OF PERSISTANT NEUTROPHILIA: BCR-ABL
 SH2017-0124 A CASE OF PERSISTANT NEUTROPHILIA: BCR-ABL NEGATIVE John R Goodlad 1, Pedro Martin-Cabrera 2, Catherine Cargo 2 1. Department of Pathology, NHS Greater Glasgow & Clyde, QEUH, Glasgow 2. Haematological
SH2017-0124 A CASE OF PERSISTANT NEUTROPHILIA: BCR-ABL NEGATIVE John R Goodlad 1, Pedro Martin-Cabrera 2, Catherine Cargo 2 1. Department of Pathology, NHS Greater Glasgow & Clyde, QEUH, Glasgow 2. Haematological
Chronic Myelomonocytic Leukemia with molecular abnormalities SH
 Chronic Myelomonocytic Leukemia with molecular abnormalities SH2017-0351 Madhu P. Menon MD,PhD, Juan Gomez MD, Kedar V. Inamdar MD,PhD and Kristin Karner MD Madhu P Menon, MD, PhD Henry Ford Hospital Patient
Chronic Myelomonocytic Leukemia with molecular abnormalities SH2017-0351 Madhu P. Menon MD,PhD, Juan Gomez MD, Kedar V. Inamdar MD,PhD and Kristin Karner MD Madhu P Menon, MD, PhD Henry Ford Hospital Patient
Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms. Kaaren Reichard Mayo Clinic Rochester
 Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms Kaaren Reichard Mayo Clinic Rochester Reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Present
Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms Kaaren Reichard Mayo Clinic Rochester Reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Present
Myelodysplastic Syndrome Case 158
 Myelodysplastic Syndrome Case 158 Dong Chen MD PhD Division of Hematopathology Mayo Clinic Clinical History 86 year old man Persistent borderline anemia and thrombocytopenia. His past medical history was
Myelodysplastic Syndrome Case 158 Dong Chen MD PhD Division of Hematopathology Mayo Clinic Clinical History 86 year old man Persistent borderline anemia and thrombocytopenia. His past medical history was
CHALLENGING CASES PRESENTATION
 CHALLENGING CASES PRESENTATION Michael C. Wiemann, MD, FACP Program Co-Chair and Vice President Indy Hematology Education President, Clinical St. John Providence Physician Network Detroit, Michigan 36
CHALLENGING CASES PRESENTATION Michael C. Wiemann, MD, FACP Program Co-Chair and Vice President Indy Hematology Education President, Clinical St. John Providence Physician Network Detroit, Michigan 36
Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms (MPN and MDS/MPN) Attilio Orazi, MD, FRCPath Weill Cornell Medical College/ NY Presbyterian Hospital, New York, NY USA EAHP EDUCATIONAL SESSION: Updated WHO classification
Myeloproliferative Neoplasms (MPN and MDS/MPN) Attilio Orazi, MD, FRCPath Weill Cornell Medical College/ NY Presbyterian Hospital, New York, NY USA EAHP EDUCATIONAL SESSION: Updated WHO classification
Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Neoplasms. Policy Specific Section:
 Medical Policy Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Type: Medical Necessity and Investigational / Experimental Policy Specific Section:
Medical Policy Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Type: Medical Necessity and Investigational / Experimental Policy Specific Section:
Treatment of low risk MDS
 Treatment of low risk MDS Matteo G Della Porta Cancer Center IRCCS Humanitas Research Hospital & Humanitas University Rozzano Milano, Italy matteo.della_porta@hunimed.eu International Prognostic Scoring
Treatment of low risk MDS Matteo G Della Porta Cancer Center IRCCS Humanitas Research Hospital & Humanitas University Rozzano Milano, Italy matteo.della_porta@hunimed.eu International Prognostic Scoring
Heme 9 Myeloid neoplasms
 Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Acute Myeloid Leukemia with Recurrent Cytogenetic Abnormalities
 Acute Myeloid Leukemia with Recurrent Cytogenetic Abnormalities Acute Myeloid Leukemia with recurrent cytogenetic Abnormalities -t(8;21)(q22;q22)(aml/eto) -inv(16) or t(16;16) -t(15;17) -11q23 Acute Myeloid
Acute Myeloid Leukemia with Recurrent Cytogenetic Abnormalities Acute Myeloid Leukemia with recurrent cytogenetic Abnormalities -t(8;21)(q22;q22)(aml/eto) -inv(16) or t(16;16) -t(15;17) -11q23 Acute Myeloid
Case Workshop of Society for Hematopathology and European Association for Haematopathology
 Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
Approaching myeloid neoplasms: diagnostic algorithms
 Approaching myeloid neoplasms: diagnostic algorithms Alexandar Tzankov Histopathology Pathology Content Integration of clinical and laboratory data Bone marrow evaluation approaching Myeloproliferative
Approaching myeloid neoplasms: diagnostic algorithms Alexandar Tzankov Histopathology Pathology Content Integration of clinical and laboratory data Bone marrow evaluation approaching Myeloproliferative
Outline. Case Study 5/17/2010. Treating Lower-Risk Myelodysplastic Syndrome (MDS) Tapan M. Kadia, MD Department of Leukemia MD Anderson Cancer Center
 Tapan M. Kadia, MD Department of Leukemia MD Anderson Cancer Center") Treating Lower-Risk Myelodysplastic Syndrome (MDS) Tapan M. Kadia, MD Department of Leukemia MD Anderson Cancer Center Outline Case Study What is lower-risk MDS? Classification systems Prognosis Treatment
Treating Lower-Risk Myelodysplastic Syndrome (MDS) Tapan M. Kadia, MD Department of Leukemia MD Anderson Cancer Center Outline Case Study What is lower-risk MDS? Classification systems Prognosis Treatment
2013 AAIM Pathology Workshop
 2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
2013 AAIM Pathology Workshop John Schmieg, M.D., Ph.D. None Disclosures 1 Pathology Workshop Objectives Define the general philosophy of reviewing pathology reports Review the various components of Bone
2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228
 2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228 Vishnu V. B Reddy, MD University of Alabama at Birmingham Birmingham, AL USA 11/03/07
2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228 Vishnu V. B Reddy, MD University of Alabama at Birmingham Birmingham, AL USA 11/03/07
Leukaemia Section Review
 Atlas of Genetics and Cytogenetics in Oncology and Haematology OPEN ACCESS JOURNAL AT INIST-CNRS Leukaemia Section Review Classification of myelodysplasic syndromes Georges Flandrin Laboratoire d'hématologie,
Atlas of Genetics and Cytogenetics in Oncology and Haematology OPEN ACCESS JOURNAL AT INIST-CNRS Leukaemia Section Review Classification of myelodysplasic syndromes Georges Flandrin Laboratoire d'hématologie,
The International Working Group on Morphology of MDS (IWGM-MDS)
") The International Working Group on Morphology of MDS (IWGM-MDS) Barbara J. Bain, St Mary s Hospital Imperial College, London, UK John M. Bennett, University of Rochester, NY, USA Richard Brunning, University
The International Working Group on Morphology of MDS (IWGM-MDS) Barbara J. Bain, St Mary s Hospital Imperial College, London, UK John M. Bennett, University of Rochester, NY, USA Richard Brunning, University
Flow Cytomety Immunophenotyping For Myelodysplastic Syndromes. Sa A.Wang, MD Dept. of Hematopathology UT MD Anderson Cancer Center Houston, TX
 Flow Cytomety Immunophenotyping For Myelodysplastic Syndromes Sa A.Wang, MD Dept. of Hematopathology UT MD Anderson Cancer Center Houston, TX Myelodysplastic Syndromes Definition: A group of heterogeneous
Flow Cytomety Immunophenotyping For Myelodysplastic Syndromes Sa A.Wang, MD Dept. of Hematopathology UT MD Anderson Cancer Center Houston, TX Myelodysplastic Syndromes Definition: A group of heterogeneous
Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms. Daniel A. Arber, MD Stanford University
 Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms Daniel A. Arber, MD Stanford University What is an integrated approach? What is an integrated approach? Incorporating all diagnostic
Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms Daniel A. Arber, MD Stanford University What is an integrated approach? What is an integrated approach? Incorporating all diagnostic
2 nd step do Bone Marrow Study If possible both the aspiration and
 Blood Malignancies-I Prof. Herman Hariman,SpPK a (KH). Ph.D.(U.K) Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. Clinpath, FK-USU First do the Full Blood Count Hb, WBCS, Platelets Morphology!! Such as blasts,
Blood Malignancies-I Prof. Herman Hariman,SpPK a (KH). Ph.D.(U.K) Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. Clinpath, FK-USU First do the Full Blood Count Hb, WBCS, Platelets Morphology!! Such as blasts,
NOVEL APPROACHES IN THE CLASSIFICATION AND RISK ASSESSMENT OF PATIENTS WITH MYELODYSPLASTIC SYNDROMES-CLINICAL IMPLICATION
 ORIGINAL ARTICLES NOVEL APPROACHES IN THE CLASSIFICATION AND RISK ASSESSMENT OF PATIENTS WITH MYELODYSPLASTIC SYNDROMES-CLINICAL IMPLICATION Ilina Micheva 1, Rosen Rachev 1, Hinco Varbanov 1, Vladimir
ORIGINAL ARTICLES NOVEL APPROACHES IN THE CLASSIFICATION AND RISK ASSESSMENT OF PATIENTS WITH MYELODYSPLASTIC SYNDROMES-CLINICAL IMPLICATION Ilina Micheva 1, Rosen Rachev 1, Hinco Varbanov 1, Vladimir
Pathology. #11 Acute Leukemias. Farah Banyhany. Dr. Sohaib Al- Khatib 23/2/16
 35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
Update on the WHO Classification of Acute Myeloid Leukemia. Kaaren K. Reichard, MD Mayo Clinic Rochester
 Update on the WHO Classification of Acute Myeloid Leukemia Kaaren K. Reichard, MD Mayo Clinic Rochester reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Objectives Present a practical
Update on the WHO Classification of Acute Myeloid Leukemia Kaaren K. Reichard, MD Mayo Clinic Rochester reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Objectives Present a practical
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD. Part 4 MYELOID NEOPLASMS
 HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
MDS 101. What is bone marrow? Myelodysplastic Syndrome: Let s build a definition. Dysplastic? Syndrome? 5/22/2014. What does bone marrow do?
 101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
Dong Wook Jekarl 1, Sang Bong Han 1, Myungshin Kim 1, Jihyang Lim 1, Eun-Jee Oh 1, Yonggoo Kim 1, Hee-Je Kim 2, Woo-Sung Min 2, Kyungja Han 1
 VOLUME 45 ㆍ NUMBER 1 ㆍ MARCH 2010 THE KOREAN JOURNAL OF HEMATOLOGY ORIGINAL ARTICLE JAK2 V617F mutation in myelodysplastic syndrome, myelodysplastic syndrome/myeloproliferative neoplasm, unclassifiable,
VOLUME 45 ㆍ NUMBER 1 ㆍ MARCH 2010 THE KOREAN JOURNAL OF HEMATOLOGY ORIGINAL ARTICLE JAK2 V617F mutation in myelodysplastic syndrome, myelodysplastic syndrome/myeloproliferative neoplasm, unclassifiable,
Myeloid neoplasms. Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories:
 Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities
 WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities Robert W. McKenna, M.D. 1/2009 WHO Classification of Myeloid Neoplasms (4th Edition)--2008 Incorporates new information that
WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities Robert W. McKenna, M.D. 1/2009 WHO Classification of Myeloid Neoplasms (4th Edition)--2008 Incorporates new information that
Myelodysplastic/Myeloproliferative Disorders. MDS/MPD Unclassified Provisional: CMML JMML acml RARS T. K. Foucar November 2007 SH/EAHP Workshop
 Myelodysplastic/Myeloproliferative Disorders CMML JMML acml MDS/MPD Unclassified Provisional: RARS T K. Foucar November 2007 SH/EAHP Workshop MDS/MPD: General Features Blood: Cytosis and cytopenia(s) Dysplasia
Myelodysplastic/Myeloproliferative Disorders CMML JMML acml MDS/MPD Unclassified Provisional: RARS T K. Foucar November 2007 SH/EAHP Workshop MDS/MPD: General Features Blood: Cytosis and cytopenia(s) Dysplasia
Myelodysplastic Syndrome: Let s build a definition
 1 MDS: Diagnosis and Treatment Update Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine Weill Medical College of Cornell University The New York Presbyterian Hospital Myelodysplastic
1 MDS: Diagnosis and Treatment Update Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine Weill Medical College of Cornell University The New York Presbyterian Hospital Myelodysplastic
MYELODYSPLASTIC SYNDROME. Vivienne Fairley Clinical Nurse Specialist Sheffield
 MYELODYSPLASTIC SYNDROME Vivienne Fairley Clinical Nurse Specialist Sheffield MDS INCIDENCE 1/100,000/YEAR 3,250/YEAR MEDIAN AGE 70 MDS HYPO OR HYPERCELLULAR BONE MARROW BLOOD CYTOPENIAS (EARLY STAGES
MYELODYSPLASTIC SYNDROME Vivienne Fairley Clinical Nurse Specialist Sheffield MDS INCIDENCE 1/100,000/YEAR 3,250/YEAR MEDIAN AGE 70 MDS HYPO OR HYPERCELLULAR BONE MARROW BLOOD CYTOPENIAS (EARLY STAGES
Bone marrow histopathology in Ph - CMPDs. - the new WHO classification - Juergen Thiele Cologne, Germany
 Bone marrow histopathology in Ph - CMPDs - the new WHO classification - Juergen Thiele Cologne, Germany Current issues in MPNs concerning morphology 1.Prodromal stages of disease 2.Impact of histopathology
Bone marrow histopathology in Ph - CMPDs - the new WHO classification - Juergen Thiele Cologne, Germany Current issues in MPNs concerning morphology 1.Prodromal stages of disease 2.Impact of histopathology
AML: WHO classification, biology and prognosis. Dimitri Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen
 AML: WHO classification, biology and prognosis Dimitri Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen Acute myeloid leukemia Clonal expansion of undifferentiated myeloid precursors Impaired
AML: WHO classification, biology and prognosis Dimitri Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen Acute myeloid leukemia Clonal expansion of undifferentiated myeloid precursors Impaired
Border between aplastic anemia and myelodysplastic syndrome
 Int J Hematol (2013) 97:558 563 DOI 10.1007/s12185-013-1324-x PROGRESS IN HEMATOLOGY Advances in the management of acquired aplastic anemia (AA) Border between aplastic anemia and myelodysplastic syndrome
Int J Hematol (2013) 97:558 563 DOI 10.1007/s12185-013-1324-x PROGRESS IN HEMATOLOGY Advances in the management of acquired aplastic anemia (AA) Border between aplastic anemia and myelodysplastic syndrome
The Role of JAK2 Mutations in RARS and Other MDS
 MYELODYSPLASTIC SYNDROMES The Role of JAK2 Mutations in RARS and Other MDS Eva Hellström-Lindberg 1 and Mario Cazzola 2 1 Karolinska Institutet, Stockholm, Sweden; 2 University of Pavia and Fondazione
MYELODYSPLASTIC SYNDROMES The Role of JAK2 Mutations in RARS and Other MDS Eva Hellström-Lindberg 1 and Mario Cazzola 2 1 Karolinska Institutet, Stockholm, Sweden; 2 University of Pavia and Fondazione
Impact of Comorbidity on Quality of Life and Clinical Outcomes in MDS
 Current Therapeutic and Biologic Advances in MDS A Symposium of The MDS Foundation ASH 2014 Impact of Comorbidity on Quality of Life and Clinical Outcomes in MDS Peter Valent Medical University of Vienna
Current Therapeutic and Biologic Advances in MDS A Symposium of The MDS Foundation ASH 2014 Impact of Comorbidity on Quality of Life and Clinical Outcomes in MDS Peter Valent Medical University of Vienna
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED
 Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Done By : WESSEN ADNAN BUTHAINAH AL-MASAEED Acute Myeloid Leukemia Firstly we ll start with this introduction then enter the title of the lecture, so be ready and let s begin by the name of Allah : We
Hematopathology Case Study
 www.medfusionservices.com Hematopathology Case Study CV3515-14 JUNE Clinical Presentation: Clinical Information: A 42 year old male with history of chronic myelogenous leukemia (CML) presents with an elevated
www.medfusionservices.com Hematopathology Case Study CV3515-14 JUNE Clinical Presentation: Clinical Information: A 42 year old male with history of chronic myelogenous leukemia (CML) presents with an elevated
74y old Female with chronic elevation of Platelet count. August 18, 2005 Faizi Ali, MD Hematopathology Fellow
 74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
Myelodysplastic syndromes in adults aged less than 50 years: Incidence and clinicopathological data
 JBUON 2014; 19(4): 999-1005 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Myelodysplastic syndromes in adults aged less than 50 years: Incidence
JBUON 2014; 19(4): 999-1005 ISSN: 1107-0625, online ISSN: 2241-6293 www.jbuon.com E-mail: editorial_office@jbuon.com ORIGINAL ARTICLE Myelodysplastic syndromes in adults aged less than 50 years: Incidence
Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas. James J. Stark, MD, FACP
 Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS
Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS
SWOG ONCOLOGY RESEARCH PROFESSIONAL (ORP) MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017
 MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017") LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
About Myelodysplastic Syndromes
 About Myelodysplastic Syndromes Overview and Types If you have been diagnosed with a myelodysplastic syndrome or are worried about it, you likely have a lot of questions. Learning some basics is a good
About Myelodysplastic Syndromes Overview and Types If you have been diagnosed with a myelodysplastic syndrome or are worried about it, you likely have a lot of questions. Learning some basics is a good
Myelodysplastic Syndromes Myeloproliferative Disorders
 Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
Myelodysplastic Syndromes Myeloproliferative Disorders Myelodysplastic Syndromes characterized by maturation defects that are associated with ineffective hematopoiesis and a high risk of transformation
Network Guidance Document. Oncological treatment of Haematology. Myelodysplastic Syndromes (MDS) Final. Status: November 2012.
 Final. Status: November 2012.") Network Guidance Document Oncological treatment of Haematology Myelodysplastic Syndromes (MDS) Status: Final Expiry Date: November 2012 Version Number: 1 Publication Date: November 2010 Page 1 of 14T:\DOG
Network Guidance Document Oncological treatment of Haematology Myelodysplastic Syndromes (MDS) Status: Final Expiry Date: November 2012 Version Number: 1 Publication Date: November 2010 Page 1 of 14T:\DOG
FLOW CYTOMETRIC ANALYSIS OF NORMAL BONE MARROW
 XI International Conference Hematopoiesis Immunology Budapest, June 6-7, 2014 FLO CYTOMETRIC ANALYSIS OF NORMAL BONE MARRO Bruno Brando and Arianna Gatti Hematology Laboratory and Transfusion Center Legnano
XI International Conference Hematopoiesis Immunology Budapest, June 6-7, 2014 FLO CYTOMETRIC ANALYSIS OF NORMAL BONE MARRO Bruno Brando and Arianna Gatti Hematology Laboratory and Transfusion Center Legnano
Aplastic Anemia & MDS International Foundation Talk. Definition. Introduction 4/20/2012. April 2012 H. Phillip Koeffler, M.D.
 Aplastic Anemia & MDS International Foundation Talk April 2012 H. Phillip Koeffler, M.D. Definition Myelo Greek prefix; marrow Dysplasia abnormal morphology Can affect: RBCs WBCs Plts Introduction 1949:
Aplastic Anemia & MDS International Foundation Talk April 2012 H. Phillip Koeffler, M.D. Definition Myelo Greek prefix; marrow Dysplasia abnormal morphology Can affect: RBCs WBCs Plts Introduction 1949:
HEMATOLOGIC MALIGNANCIES BIOLOGY
 HEMATOLOGIC MALIGNANCIES BIOLOGY Failure of terminal differentiation Failure of differentiated cells to undergo apoptosis Failure to control growth Neoplastic stem cell FAILURE OF TERMINAL DIFFERENTIATION
HEMATOLOGIC MALIGNANCIES BIOLOGY Failure of terminal differentiation Failure of differentiated cells to undergo apoptosis Failure to control growth Neoplastic stem cell FAILURE OF TERMINAL DIFFERENTIATION
Blood Cell Identification: 2011-B Mailing: Acute Myeloid Leukemia (AML)
") Please Note: To view the Figures and Images contained within this education activity in color, access the electronic version of the reading. CASE HISTORY This peripheral blood smear is from a 51-year-old
Please Note: To view the Figures and Images contained within this education activity in color, access the electronic version of the reading. CASE HISTORY This peripheral blood smear is from a 51-year-old
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and
 Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
Group of malignant disorders of the hematopoietic tissues characteristically associated with increased numbers of white cells in the bone marrow and / or peripheral blood Classified based on cell type
Disclosures. Myeloproliferative Neoplasms: A Case-Based Approach. Objectives. Myeloproliferative Neoplasms. Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
CD34 positive dysplastic giant platelets masquerading as blasts on flow cytometry
 CD34+ Giant Platelets Hematopathology - September 2016 Case Study CD34 positive dysplastic giant platelets masquerading as blasts on flow cytometry Anmaar Abdul-Nabi 1,*, Yvette Reese 2, Susan Treese 2,
CD34+ Giant Platelets Hematopathology - September 2016 Case Study CD34 positive dysplastic giant platelets masquerading as blasts on flow cytometry Anmaar Abdul-Nabi 1,*, Yvette Reese 2, Susan Treese 2,
MYELOPROLIFERATIVE DISEASE. Dr Mere Kende MBBS (UPNG), MMED (Path),MAACB, MACTM, MACRRM (Aus) Lecturer-SMHS UPNG
, MMED (Path),MAACB, MACTM, MACRRM (Aus) Lecturer-SMHS UPNG") MYELOPROLIFERATIVE DISEASE Dr Mere Kende MBBS (UPNG), MMED (Path),MAACB, MACTM, MACRRM (Aus) Lecturer-SMHS UPNG Myeloproliferative Diseases Essential to diagnosis Acquired clonal abnormalities of the hematopoietic
MYELOPROLIFERATIVE DISEASE Dr Mere Kende MBBS (UPNG), MMED (Path),MAACB, MACTM, MACRRM (Aus) Lecturer-SMHS UPNG Myeloproliferative Diseases Essential to diagnosis Acquired clonal abnormalities of the hematopoietic
MDS - Diagnosis and Treatments. Dr Helen Enright, Adelaide and Meath Hospital Dr Catherine Flynn, St James Hospital
 MDS - Diagnosis and Treatments Dr Helen Enright, Adelaide and Meath Hospital Dr Catherine Flynn, St James Hospital Overview What is myelodysplasia? Symptoms Diagnosis and prognosis Myelodysplasia therapy
MDS - Diagnosis and Treatments Dr Helen Enright, Adelaide and Meath Hospital Dr Catherine Flynn, St James Hospital Overview What is myelodysplasia? Symptoms Diagnosis and prognosis Myelodysplasia therapy
MDS: Who gets it and how is it diagnosed?
 MDS: Who gets it and how is it diagnosed? October 16, 2010 Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine Weill Medical College of Cornell University The New York Presbyterian
MDS: Who gets it and how is it diagnosed? October 16, 2010 Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine Weill Medical College of Cornell University The New York Presbyterian
Myelodysplastic Syndromes (MDS) FAQs for Nurses
 FAQs for Nurses") Myelodysplastic Syndromes (MDS) FAQs for Nurses Find answers to the most commonly asked questions about MDS from nurses and patients. This content meets the Oncology Nursing Society guidelines for quality
Myelodysplastic Syndromes (MDS) FAQs for Nurses Find answers to the most commonly asked questions about MDS from nurses and patients. This content meets the Oncology Nursing Society guidelines for quality
MYELODYSPLASTIC SYNDROMES WITH MONOCYTIC COMPONENT: HEMATOLOGIC AND CYTOGENETIC CHARACTERIZATION
 original paper Haematologica 1997; 82:25-30 Advances in the Cytobiology of Leukemias* MYELODYSPLASTIC SYNDROMES WITH MONOCYTIC COMPONENT: HEMATOLOGIC AND CYTOGENETIC CHARACTERIZATION GIAN MATTEO RIGOLIN,
original paper Haematologica 1997; 82:25-30 Advances in the Cytobiology of Leukemias* MYELODYSPLASTIC SYNDROMES WITH MONOCYTIC COMPONENT: HEMATOLOGIC AND CYTOGENETIC CHARACTERIZATION GIAN MATTEO RIGOLIN,
2007 Workshop of SH/EAHP. Session 5 Therapy-related myeloid neoplasms
 2007 Workshop of SH/EAHP Session 5 Therapy-related myeloid neoplasms Classification: Key issues MDS vs. AML-M6 MDS vs. MDS/MPD Genetically defined entities Relevance of morphologic classification Clinical
2007 Workshop of SH/EAHP Session 5 Therapy-related myeloid neoplasms Classification: Key issues MDS vs. AML-M6 MDS vs. MDS/MPD Genetically defined entities Relevance of morphologic classification Clinical
Case Report Blasts-more than meets the eye: evaluation of post-induction day 21 bone marrow in CBFB rearranged acute leukemia
 Int J Clin Exp Pathol 2014;7(7):4498-4502 www.ijcep.com /ISSN:1936-2625/IJCEP0000851 Case Report Blasts-more than meets the eye: evaluation of post-induction day 21 bone marrow in CBFB rearranged acute
Int J Clin Exp Pathol 2014;7(7):4498-4502 www.ijcep.com /ISSN:1936-2625/IJCEP0000851 Case Report Blasts-more than meets the eye: evaluation of post-induction day 21 bone marrow in CBFB rearranged acute
Characteristics of the four subtypes of myelodysplastic/myeloproliferative neoplasms
 1332 Characteristics of the four subtypes of myelodysplastic/myeloproliferative neoplasms HUANLING WU 1*, SHUQUAN BIAN 2*, JINGXUE CHU 3, XIAOYAN ZHONG 4, HUI SUN 1, BINGCHANG ZHANG 1 and ZHIMING LU 5
1332 Characteristics of the four subtypes of myelodysplastic/myeloproliferative neoplasms HUANLING WU 1*, SHUQUAN BIAN 2*, JINGXUE CHU 3, XIAOYAN ZHONG 4, HUI SUN 1, BINGCHANG ZHANG 1 and ZHIMING LU 5
Molecular techniques in a case of concurrent BCR-ABL1 positive CML and CMML
 reprinted from november 2014 pathology laboratory medicine laboratory management Molecular techniques in a case of concurrent BCR-ABL1 positive CML and CMML CAP TODAY and the Association for Molecular
reprinted from november 2014 pathology laboratory medicine laboratory management Molecular techniques in a case of concurrent BCR-ABL1 positive CML and CMML CAP TODAY and the Association for Molecular
23/10/2017. Analysis of bone marrow for MDSrelated. Approach used at Hematopathology, Lund
 Approach used at Hematopathology, Lund Analysis of bone marrow for MDSrelated aberrancies According to International/ELN Flow Cytometry Working Group (IMDSFlow) Anna Porwit Lund, Sweden 1. new patients
Approach used at Hematopathology, Lund Analysis of bone marrow for MDSrelated aberrancies According to International/ELN Flow Cytometry Working Group (IMDSFlow) Anna Porwit Lund, Sweden 1. new patients
CASE REPORT Myelodysplastic syndrome with fibrosis and complex karyotype arising in a patient with essential thrombocythaemia
 Malaysian J Pathol 2018; 40(2) : 191 197 CASE REPORT Myelodysplastic syndrome with fibrosis and complex karyotype arising in a patient with essential thrombocythaemia Nor Ainiza MANSOR 1, Nurasyikin YUSOF
Malaysian J Pathol 2018; 40(2) : 191 197 CASE REPORT Myelodysplastic syndrome with fibrosis and complex karyotype arising in a patient with essential thrombocythaemia Nor Ainiza MANSOR 1, Nurasyikin YUSOF
Disclosure BCR/ABL1-Negative Classical Myeloproliferative Neoplasms
 Disclosure BCR/ABL1-Negative Classical Myeloproliferative Neoplasms Sonam Prakash declares affiliation with Incyte Corporation: Advisor for Hematopathology Publications Steering Committee Sonam Prakash,
Disclosure BCR/ABL1-Negative Classical Myeloproliferative Neoplasms Sonam Prakash declares affiliation with Incyte Corporation: Advisor for Hematopathology Publications Steering Committee Sonam Prakash,
Histopathology in the diagnosis of high-risk myelodysplastic syndromes
 Journal of clinical and experimental hematopathology Vol. 58 No.2, 51-60, 2018 JC lin EH xp ematopathol Review Article Histopathology in the diagnosis of high-risk myelodysplastic syndromes Hidekazu Kayano
Journal of clinical and experimental hematopathology Vol. 58 No.2, 51-60, 2018 JC lin EH xp ematopathol Review Article Histopathology in the diagnosis of high-risk myelodysplastic syndromes Hidekazu Kayano
myelodysplastic syndrome MDS MDS MDS
 myelodysplastic syndrome MDS MDS 15 10 3 2004 15 MDS 400 2 65 61 70 MDS MDS 1 1 2 3 3 4 1 4 2 3 4 MDS 1982 Bennett French- American-BritishFAB 1 2 WHO 1999 3 2001 4 2002 Vardiman MDS 5 2WHO FAB refractory
myelodysplastic syndrome MDS MDS 15 10 3 2004 15 MDS 400 2 65 61 70 MDS MDS 1 1 2 3 3 4 1 4 2 3 4 MDS 1982 Bennett French- American-BritishFAB 1 2 WHO 1999 3 2001 4 2002 Vardiman MDS 5 2WHO FAB refractory
Published Ahead of Print on January 14, 2009, as doi: /haematol Copyright 2009 Ferrata Storti Foundation.
 Published Ahead of Print on January 14, 2009, as doi:10.3324/haematol.13755. Copyright 2009 Ferrata Storti Foundation. DECISION MAKING AND PROBLEM SOLVING Diagnostic criteria to distinguish hypocellular
Published Ahead of Print on January 14, 2009, as doi:10.3324/haematol.13755. Copyright 2009 Ferrata Storti Foundation. DECISION MAKING AND PROBLEM SOLVING Diagnostic criteria to distinguish hypocellular
When Cancer Looks Like Something Else: How Does Mutational Profiling Inform the Diagnosis of Myelodysplasia?
 Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including
Transcript Details This is a transcript of a continuing medical education (CME) activity accessible on the ReachMD network. Additional media formats for the activity and full activity details (including