Myelodysplastic/Myeloproliferative Neoplasms (MDS/MPN) Updated
|
|
|
- Shon Brooks
- 6 years ago
- Views:
Transcription
1 Myelodysplastic/Myeloproliferative Neoplasms (MDS/MPN) Updated Attilio Orazi, MD, FRCPath. (Engl.) Professor of Pathology and Laboratory Medicine Weill Cornell Medical College/NYP Hospital New York, NY - USA
 payment Shareholder Other relationship, i.e. Company names")
2 Disclosure of speaker s interests (Attilio Orazi) (Potential) conflict of interest None Potentially relevant company relationships in connection with event Sponsorship or research funding Fee or other (financial) payment Shareholder Other relationship, i.e. Company names
3 MDS/MPN First introduced by the WHO 2001 (3 rd edition) Myeloid neoplasms characterized by proliferative features combined with evidence of partially ineffective hematopoiesis and (usually) dysplasia, simultaneously present at disease outset and persistent over time MDS/MPN have <20% blasts in PB and/or BM. They are negative for BCR/ABL1 and PDGFR-A,-B, FGFR1 or PCM1-JAK2 rearrangements Arber DA, Orazi A, Hasserjian RP et al. Blood 2016 Mughal TI, et al. Haematologica Orazi A, Germing U. Leukemia. 2008
4 Anemia (rarely normal Hb*) and dysplasia in one or more lineages, in combination with one or more of the following: Leucocytosis (WBC > 13 x10 9 /L)** Monocytosis (monocytes >1 x10 9 /L) Thrombocytosis (plts. >450 x10 9 /L) Splenomegaly associated with myeloproliferation*** *No erythrocytosis ** May have normal WBC but usually no absolute neutropenia (<1.8 x10 9 /L) *** The presence of splenomegaly or fibrosis alone is not a MPN-like qualifying feature
5 MDS/MPN: Entities Chronic myelomonocytic leukemia (CMML) Atypical chronic myeloid leukemia BCR-ABL1 negative (acml) MDS/MPN with ring sideroblasts and thrombocytosis (MDS/MPN-RS-T) MDS/MPN, unclassifiable (MDS/MPN,U) [Juvenile myelomonocytic leukemia (JMML)]
6 CMML
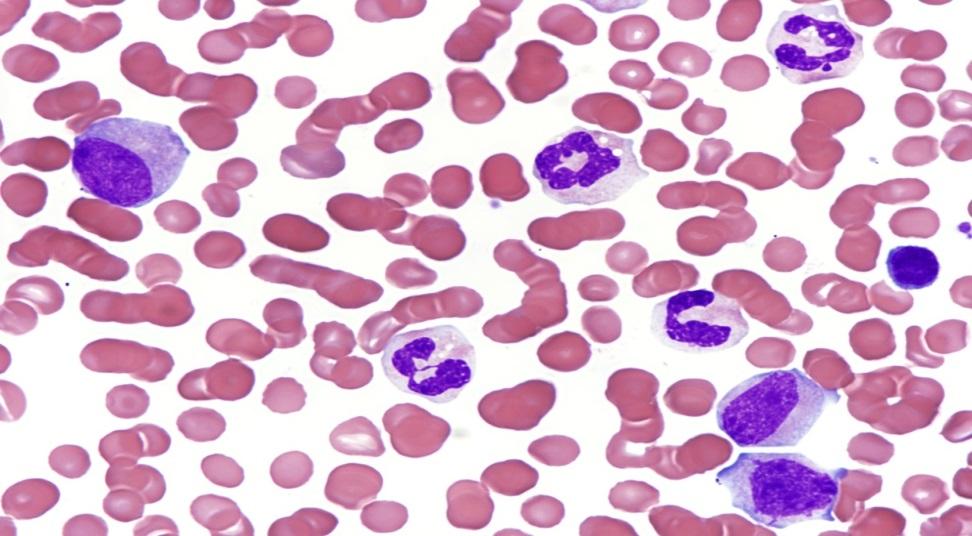
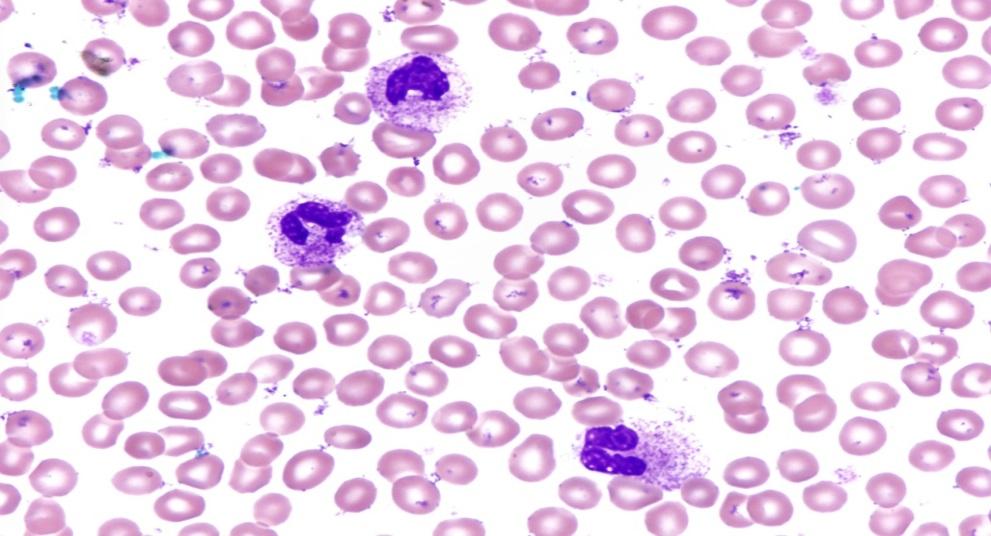
7 CMML: WHO definition A subtype of MDS/MPN which has monocytosis (PB) as its major defining feature Monocytosis > /L and > 10% of the WBC


8 Abnormal monocytes found in CMML
9 Flow cytometry Variable/abnormal antigenic expression in monocytes: Increased proportion of CD14 pos./cd16 neg. cells Aberrant phenotypes with two or more aberrant features, e.g. overexpression of CD56, aberrant expression of CD2 and/or decreased expression of CD14, CD64, HLA-DR, CD13, CD15, or CD36 Selimoglu-Buet D, et al. Blood. 2015;125: Xu Y, et al. Am J Clin Pathol. 2005;124: Lacronique-Gazaille C, et al. Haematologica. 2007;92:859-60
10 Normal karyotype (60%) If abnormal, overlaps MDS: +8, -7/del(7q), abn. chrom.12 complex Cytogenetics
11 Mutations of SRSF2, TET2, ASXL1; NPM1 One of the three above mutations can be identified in at least 90% of CMML cases; other mutations seen less frequently are SETBP1, RAS, RUNX1, CBL, and EZH2. They can be helpful diagnostic adjuncts in difficult cases, particularly given the frequently normal karyotype of CMML. Mughal TI, Haematologica Co-mutation of TET2 and SRSF2 is seen in about one-third of CMML cases and is a predictor of the diagnosis. Malcovati L, Blood ASXL1 is a predictor of aggressive disease behavior and has been incorporated into a prognostic scoring system alongside karyotype and clinicopathologic parameters. Itzykson R, J Clin Oncol NPM1 mutation is seen in a rare subset of CMML (3-5%) and appears to herald a worst prognosis. Peng J, Eur J Haematol. 2015
12 Bone Marrow Findings

13 Bone Marrow Hypercellular with high M:E ratio due to increased granulopoiesis (resembles CML); blasts usually <5% Typical morphologic dissociation between a granulocytic-rich BM and a monocytic-rich PB Monocytes are hard to see and to distinguish from myelocytes, metamyelocytes, and band forms Orazi et al: Mod Pathol 2006;19:


14 Esterase cytochemistry helps in confirming CMML CMML Mean: 13.4% CML Mean: 0.63% +0.7 P = Orazi et al: Mod Pathol 2006;19:

15 Bone Marrow Biopsy: myeloproliferative look
16 BM examination is always necessary AML-M4 and -M5b can simulate CMML in the PB CMML-1 in PB can have > 10% blasts in BM (CMML-2) or may be undergoing transformation to AML BM flow cytometry can help separating monocytes from blasts Karyotype e.g., 11q23 may suggest AML Monocytic proliferation can be more pronounced in BM than PB (seen in a subset of oligomonocytic CMML) Orazi A, Germing U. Leukemia 2008;22:
17 Immunohistochemistry in CMML Myeloid cells Granulocytes Monocytes Macrophages Plasmacytoid dendritic cells Blasts CD68, Lysozyme MPX, CD15, [CD56] CD14, CD68R, [CD56] CD163, CD68R CD303, CD123 CD34, CD117


18 CD68R/PG-M1 (high specificity for monocytes) Orazi et al: Mod Pathol 2006; 19:

19 CD14 (best marker for CMML in BMB) Qubaja M, et al. The detection of CD14 and CD16 in paraffin-embedded bone marrow biopsies is useful for the diagnosis of CMML. Virchows Arch. 2009;454:411-9.
 nodule CD123 PMs")

20 Mature plasmacytoid dendritic cell (PDC) nodule CD123 PMs nodules CMML (19%) CML 0 CD123 Orazi et al: Mod Pathol 2006
21 Mature plasmacytoid dendritic cells in myeloid neoplasms Clonal in nature, closely related to the associated myeloid neoplasm Immunophenotype CD303, CD123, CD14, CD43, CD4, CD68, CD68R, CD45RA, CD33 (weakly); CD2 and CD5 can also be positive Granzyme B pos.; TIA-1 and perforin neg. CD56 expression seen only in rare cases Low Mib-1 (Ki-67)
22 Prognostication
23 1. CMML dysplastic vs. MPN-like 2. Refined blast count for prognosis CMML dysplastic (WBC, <13 x10 9 /L) CMML proliferative (>13 x 10 9 /L); this subtype has more frequent RAS or JAK2 mutations and splenomegaly Ricci C, et al. Clin Cancer Res Schuler E, et al. Leuk Res Cervera N, et al. Am J Hematol CMML-0: <2% blasts in PB; <5% blasts in BM CMML-1: 2 4% blasts in PB; 5 9% blasts in BM CMML-2: 5 19% blasts in PB; 10 19% in BM, or when Auer rods are present irrespective of the blast count Storniolo AM, et al. Leukemia Onida,F, et al. Blood Schuler E, et al. Leuk Res. 2014
24 Prognosis and progression to AML Cytogenetic risk categories: high (complex and monosomal karyotypes) intermediate (all other abnormalities) low [normal, sole -Y and sole der (3q)] Median survivals of 3, 20 and 41 months, respectively Wassie EA, et al. Am J Hematol. 2014;89:1111-5
25 CMML with fibrosis
 fibrosis is seen in nearly 30% of these cases.")

, as well as for CMML cases lacking fibrosis. BM fibrosis was defined using the WHO semiquantitative MF grading system based on a 0-3 scale.")
 was compared with myeloproliferativetype (MPN-type; >13 x10 9 /L).")
. D reticulin stain showing MF-2 fibrosis. Table I. CMML MF-0 vs.")


 4.23 (0-16) 4.43 (0-10) 0.81 Mean BM Smear Monocytes (Range) 18 (3-48) 17 (2-69) 0.")
![79 Mean WBC [x 10 9 cells/ L] (Range) 17.2 (3.7-53.1) 30.7 (3-170) 0.06 Mean PB Blasts (%) (Range) 0.4 (0-8) 0.8 (0-3) 0.19 Mean Abs Mono [x 10 9 cells/ L](Range) 4.6 (0.6-22.](/docs-images/78/76956754/images/26-11.jpg "8) 10.7 (0.7-131.1) 0.17 Mean Hgb [g/ dl] (Range) 10.8 (5.0-14.9) 10.7 (6.4-15.0) 0.9 Mean MCV [fl] (Range) 91.0 (69-114) 91.2 (74-117) 0.")
![95 Mean Plt [x10 9 cells/ L] (Range) 113 (32-296) 90 (12-266) 0.2 Fig. 2. Kaplan-Meier analysis of disease progression.](/docs-images/78/76956754/images/26-12.jpg "CMML patients with MF 1 showed a shorter overall median time to disease progression by Kaplan-Meier survival analysis (45.8 months vs not reached; p=0.")
26 Click to edit BACKGROUND Chronic myelomonocytic leukemia (CMML) is a well characterized subtype of myelodysplastic/myeloproliferative neoplasms recognized by the WHO 2008 classification. Bone marrow (BM) fibrosis is seen in nearly 30% of these cases. Although BM fibrosis is an adverse prognostic marker in other myeloid neoplasms, particularly in MDS with fibrosis, no such information is available in relation to CMML. The aim of this study was to investigate the clinicopathological features Master text and prognosis correlates of CMML with fibrosis. MATERIALS & METHODS Pathology records of two institutions were searched styles for BM of untreated CMML patients with BM fibrosis over an 8 year period (from 4/2007 to 3/2015), as well as for CMML cases lacking fibrosis. BM fibrosis was defined using the WHO semiquantitative MF grading system based on a 0-3 scale. Second level Cases of CMML with at least MF-1 grade fibrosis Myelodysplastic-type CMML (MDS-type; <13 (MF>1: Third 30 level cases) were compared to CMML MF-0 (31 cases). Fourth level bulleted copy details x10» Fifth level 9 /L) was compared with myeloproliferativetype (MPN-type; >13 x10 9 /L). Progression was defined as either: (1) Progression from CMML-1 to CMML-2 or (2) Progression to AML. Petrova-Drus K et al. Mod Pathol 2016; 29:368A A C Fig. 1. BM biopsy of a patient with CMML and BM fibrosis. A,B,C (H&E). D reticulin stain showing MF-2 fibrosis. Table I. CMML MF-0 vs. MF >1: subtypes and clinical findings MF-0 (N=31) MF 1 (N=30) p Mean Age (Range) 70.0 (41-90) 66.3 (23-87) 0.2 M 19 61% 19 63% 0.86 F 12 39% 11 37% CMML Category % 28 93% % 1 33% CMML Type 0.52 MPN-type 14 45% 16 53% MDS-type 17 55% 14 47% Splenomegaly Y 11 35% 18 60% 0.04* N 20 65% 11 37% Median Time to Disease Progression Not Reached * Median overall survival (m) SCT Y 9 29% 10 33% 0.93 N 18 58% 19 63% NA 4 13% 1 3% Outcome Died of disease 8 26% 13 43% 0.35 No evidence of disease 14 45% 10 33% Lost to follow-up 9 29% 7 23% B D Table II. BM and PB findings in CMML MF-0 vs. MF >1 MF-0 (N=31) MF 1 (N=30) P Mean BM Cellularity (Range) 79 (40-100) 87 (40-100) 0.02* BM Megakaryocytes Increased 12 39% 21 70% 0.006* Decreased 3 10% 5 17% Adequate 16 51% 4 13% Mean BM Smear Blasts (Range) 4.23 (0-16) 4.43 (0-10) 0.81 Mean BM Smear Monocytes (Range) 18 (3-48) 17 (2-69) 0.79 Mean WBC [x 10 9 cells/ L] (Range) 17.2 ( ) 30.7 (3-170) 0.06 Mean PB Blasts (%) (Range) 0.4 (0-8) 0.8 (0-3) 0.19 Mean Abs Mono [x 10 9 cells/ L](Range) 4.6 ( ) 10.7 ( ) 0.17 Mean Hgb [g/ dl] (Range) 10.8 ( ) 10.7 ( ) 0.9 Mean MCV [fl] (Range) 91.0 (69-114) 91.2 (74-117) 0.95 Mean Plt [x10 9 cells/ L] (Range) 113 (32-296) 90 (12-266) 0.2 Fig. 2. Kaplan-Meier analysis of disease progression. CMML patients with MF 1 showed a shorter overall median time to disease progression by Kaplan-Meier survival analysis (45.8 months vs not reached; p=0.03, log rank test) compared to MF-0 patients. Progression Free Survival Kaplan-Meier analysis of progression by BM fibrosis MF 1 CONCLUSIONS Patients with CMML associated with BM fibrosis have higher marrow cellularity, increased megakaryopoiesis, more frequent splenomegaly and a significantly shorter median time to disease progression, when compared to those without BM fibrosis. Assessing BM fibrosis in CMML is important. MF=0 Months Similar to MDS, its presence identifies a distinct subgroup of CMML patients which may require a more aggressive treatment.
27 Oligomonocytic CMML


.")
28 70 year old male pt. with anemia and thrombocytopenia (PB) Hb 9.6, MCV 106 fl; WBC 5.7 x10 9 /L; monocytes 12% (0.7 x10 9 /L). Plts. 92 x10 9 /L


29 Bone marrow aspirate ANBE

30 Geyer JT et al. Mod Pathol 2015; 28:345 A
31 Diagnostic criteria for CMML (Update 2016) Persistent PB monocytosis > /L and > 10% of the WBC Not meeting WHO criteria for BCR-ABL1 pos. CML, PMF, PV or ET a No rearrangement of PDGFRA, PDGFRB, FGFR1, or PCM1-JAK2 Fewer than 20% blasts (include promonocytes) in the PB and BM Dysplasia in > 1 myeloid lineage(s). If absent, the diagnosis of CMML may still be made if the other requirements are met, and an acquired cytogenetic or molecular genetic abnormality b is detected, --or-- - the monocytosis has persisted for at least 3 months and all other causes of monocytosis have been excluded a Cases of MPN can be associated with monocytosis or they can develop it during the course of the disease. These cases may simulate CMML. In these rare instances, a previous documented history of MPN excludes CMML, while the presence of MPN features in the bone marrow and/or of MPN-associated mutations (JAK2, CALR or MPL) tend to support MPN with monocytosis rather than CMML. b The presence of mutations in genes often associated with CMML (e.g. TET2, SRSF2, ASXL1, SETBP1) in the proper clinical contest can be used to support a diagnosis. It should be noted however, that some of the mutations can be age related or be present in subclones. Therefore caution would have to be used in the interpretation of these genetic results. Adapted from Arber DA, Orazi A, Hasserjian RP et al. Blood, April 27, 2016
32 Atypical CML BCR-ABL1 neg. (acml)

33 acml has an abysmal prognosis Sa Wang et al. Blood. 2014; 123:
34 Peripheral blood smear in acml Note the severe dysgranulopoiesis and the abnormal chromatin clumping


35 Atypical chronic myeloid leukemia as defined in the WHO classification is a JAK2 V617F negative neoplasm Fend F, Horn T, Koch I, Vela T, Orazi A. Leuk Res. 2008;32:1931-5
36 acml: SETBP1 and ETNK1 mutation(s) in the absence of CSF3R mutation Piazza R, et al. Recurrent SETBP1 mutations in atypical chronic myeloid leukemia. Nat Genet. 2013;45: Gambacorti-Passerini CB, et al. Recurrent ETNK1 mutations in atypical chronic myeloid leukemia. Blood Oct 24. pii: blood [Epub ahead of print]. Elliott MA, Tefferi A. Chronic neutrophilic leukemia 2014: Update on diagnosis, molecular genetics, and management. Am J Hematol. 2014;89: (CSF3R: CNL only) Wang Sa, et al. Atypical chronic myeloid leukemia is clinically distinct from unclassifiable myelodysplastic/ myeloproliferative neoplasms. Blood. 2014;123: (acml: CSF3R neg.)
37 Differential diagnosis of acml acml vs. Chronic Neutrophilic Leukemia (CNL) acml vs. MPN-associated neutrophilia


38 acml vs. CNL
 CNL vs.")
 additional SETBP1 +/- (50%) SETBP1 (15-32%) ETNK1")
39 CNL Neutrophilia with no significant dysplasia (toxic granulations) CNL vs. acml acml Neutrophilia with immature myeloid cells and dysplasia CSF3R (90%) additional SETBP1 +/- (50%) SETBP1 (15-32%) ETNK1 (9%); in one third of these, coexists with SETBP1 ; CSF3R (<10%)
40 Diagnostic criteria for acml, BCR-ABL1 negative (update 2016) Leukocytosis /L due to neutrophilia Granulocytic precursors (promyelocytes, myelocytes and metamyelocytes) 10% of WBC Dysgranulopoiesis (may include abnormal chromatin clumping) No basophilia; basophils usually <2% of PB leukocytes; No monocytosis; monocytes <10% of PB leukocyte; Less than 20% blasts in the blood and bone marrow No BCR-ABL1, PDGFRA, PDGFRB or FGFR1, or PCM1-JAK2 No PMF, PV or ET* *Cases of MPN, particularly those in AP and/or in PV/ET myelofibrosis, if neutrophilic, may simulate acml A previous history of MPN, the presence of MPN features in the bone marrow tend to exclude a diagnosis of acml. MPN-associated mutations in JAK2, CALR or MPL tend also to exclude a diagnosis of acml. Conversely, a diagnosis of acml is supported by the presence of SETBP1 and/or ETNK1 mutations. The presence of a CSF3R mutation is uncommon in acml and if detected should prompt a careful morphologic review to exclude an alternative diagnosis of CNL or of other myeloid neoplasm.
41 MDS/MPN features in MPN Monocytosis Neutrophilia with dysplasia
42 Monocytosis in PMF and Polycythemia Vera Elliott MA, Verstovsek S, Dingli D, Schwager SM, Mesa RA, Li CY, Tefferi A. Monocytosis is an adverse prognostic factor for survival in younger patients with primary myelofibrosis. Leuk Res. 2007Nov;31(11): Barraco D et al. Am J Hematol Mar 28. doi: /ajh [Epub ahead of print]

 BMB 2010")

43 Monocytic progression of PMF 2010 PB Earlier (2002) BMB 2010 BMB Boiocchi L. et al. Mod Pathol. 2013;26:204-12


![; Karyotype: 46, XY [20]](/docs-images/78/76956754/images/44-2.jpg "Boiocchi et al. Mod Pathol.")
44 Polycythemia Vera with acml-like neutrophilic progression WBC > 25 x10 9 /L ; FISH for BCR-ABL1 neg.; Karyotype: 46, XY [20] Boiocchi et al. Mod Pathol. 2015;28:
45 The Overlaps Well defined and not so well defined entities


46 True gray zone between PMF and CMML Monocytosis > 1.0 x10 9 /L and ambiguous BM morphology


47 Molecularly an overlap syndrome Combination of mutations: MPL 44%; ASXL1 43%; EZH2 51%;, TET2 (2 frameshift mutations) 42% and 48%; SRSF2 46%; NRAS 25%. Chapman JR et al, Mod Pathol 2017, in press
48 Myeloid neoplasms associated with isolated isochromosome 17q
49 Myeloid neoplasms with isolated 17q Neutrophilia with monolobated forms In a proportion of the cases leukocytosis is CMML-like or acml like






50 Myeloid neoplasm with isolated 17q Courtesy of Dr. Carlos Bueso-Ramos, MD Anderson

51 MPN with isolated 17q Hypercellular BM with variable morphology e.g., pleomorphic megakaryocytes PMF-like have been reported (McClure RF et al. Br J Haematol, 1999)
52 MDS/MPN with isolated isochromosome 17q Its appropriate categorization is uncertain at this time Although a proportion of cases meet the criteria for CMML, acml, MPN-AP/BP, MDS or AML, others may be appropriately categorized as MDS/MPN-U High frequency of mutations in ASXL1, SETBP1, SRSF2, NRAS, TP53 Fioretos T, et al. Blood 1999; 94: McClure RF, et al. Br J Haematol 1999; 106: Kanagal-Shamanna R, et al. Cancer. 2012;118: Meggendorfer M, et al. Leukemia. 2016;30: Kanagal-Shamanna R, et al. Oncotarget. 2016;7:
53 The overlap syndrome promoted to full entity MDS/MPN-RS-T* *Formerly, Refractory Anemia with Ring Sideroblasts and Thrombocytosis (RARS-T)

 MPL W515K/L 5%; CALR rare")

54 MDS/MPN-RS-T Combination of MDS-RS and MPN-like features clinically, morphologically and at molecular level May progress from RARS SF3B1 mutation (80% - similar to MDS-RS) JAK2 pos. in up to 60% (unclear prognostic role) MPL W515K/L 5%; CALR rare BCR/ABL1 neg. Karyotype variable Wang Sa, et al. Leukemia. 2006; Schmitt-Graeff AH, et al. Haematologica. 2008; Malcovati L, et al. Blood. 2009; Broséus J, et al. Leukemia. 2013
55 Diagnostic criteria for MDS/MPN-RS-T (update 2016) Anaemia associated with erythroid lineage dysplasia with or without multilineage dysplasia; 15% ring sideroblasts in BM; <1% blasts in PB and <5% blasts in BM Persistent thrombocytosis with platelet count 450 x 10 9 /L Presence of a SF3B1 mutation* No BCR-ABL1 fusion gene, or PDGFRA, PDGFRB, FGFR1, PCM1-JAK2; no (3;3)(q21;q26), inv(3)(q21q26) or del(5q)** No history of MPN, MDS (except MDS-RS), or other type MDS/MPN In the absence of SF3B1 mutation, no history of recent cytotoxic or growth factor therapy that could explain the myelodysplastic/ myeloproliferative features *A diagnosis of MDS/MPN-RS-T is strongly supported by the presence of SF3B1 mutation together with a mutation in JAK2 V617F, CALR or MPL genes **In a case which otherwise fulfills the diagnostic criteria for MDS with isolated del(5q) Adapted from Arber DA, Orazi A, Hasserjian RP et al. Blood, April 27, 2016
56 Mutational Analysis in MDS/MPN Useful in differential diagnosis: in establishing MDS/MPN-RS-T in separating acml from CNL in excluding MPN in supporting a highly suspected diagnosis (e.g. early phase disease not meeting all the diagnostic thresholds) Provide powerful prognostic info (several mutations are prognostically detrimental) Limited value for confirmation of clonality; analogy with MDS in relation to CHIP and CCUS (too few studies)
57 In conclusion Cytogenetics and molecular genetics are key diagnostic elements in some myeloid neoplasms. However, the MDS/MPNs are still clinicopathologically defined entities with specific diagnostic algorithms based on careful multiparametric integration Mutational analysis provides diagnostic support and helps in accurate prognostication Once the diagnostic role of genetic abnormalities is better clarified, a redefinition of disease boundaries (and a new Blue Book) will follow
58 Thank you for your attention!
Case Presentation. Attilio Orazi, MD
 Case Presentation Attilio Orazi, MD Weill Cornell Medical College/ NYP Hospital Department of Pathology and Laboratory Medicine New York, NY United States History 60 year old man presented with anemia
Case Presentation Attilio Orazi, MD Weill Cornell Medical College/ NYP Hospital Department of Pathology and Laboratory Medicine New York, NY United States History 60 year old man presented with anemia
Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms (MPN and MDS/MPN) Attilio Orazi, MD, FRCPath Weill Cornell Medical College/ NY Presbyterian Hospital, New York, NY USA EAHP EDUCATIONAL SESSION: Updated WHO classification
Myeloproliferative Neoplasms (MPN and MDS/MPN) Attilio Orazi, MD, FRCPath Weill Cornell Medical College/ NY Presbyterian Hospital, New York, NY USA EAHP EDUCATIONAL SESSION: Updated WHO classification
SH A CASE OF PERSISTANT NEUTROPHILIA: BCR-ABL
 SH2017-0124 A CASE OF PERSISTANT NEUTROPHILIA: BCR-ABL NEGATIVE John R Goodlad 1, Pedro Martin-Cabrera 2, Catherine Cargo 2 1. Department of Pathology, NHS Greater Glasgow & Clyde, QEUH, Glasgow 2. Haematological
SH2017-0124 A CASE OF PERSISTANT NEUTROPHILIA: BCR-ABL NEGATIVE John R Goodlad 1, Pedro Martin-Cabrera 2, Catherine Cargo 2 1. Department of Pathology, NHS Greater Glasgow & Clyde, QEUH, Glasgow 2. Haematological
Chronic Myelomonocytic Leukemia with molecular abnormalities SH
 Chronic Myelomonocytic Leukemia with molecular abnormalities SH2017-0351 Madhu P. Menon MD,PhD, Juan Gomez MD, Kedar V. Inamdar MD,PhD and Kristin Karner MD Madhu P Menon, MD, PhD Henry Ford Hospital Patient
Chronic Myelomonocytic Leukemia with molecular abnormalities SH2017-0351 Madhu P. Menon MD,PhD, Juan Gomez MD, Kedar V. Inamdar MD,PhD and Kristin Karner MD Madhu P Menon, MD, PhD Henry Ford Hospital Patient
WHO Update to Myeloproliferative Neoplasms
 WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
WHO Update to Myeloproliferative Neoplasms Archana M Agarwal, MD, Associate Professor of Pathology University of Utah Department of Pathology/ARUP Laboratories Myeloproliferative Neoplasms The categories
Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms. Kaaren Reichard Mayo Clinic Rochester
 Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms Kaaren Reichard Mayo Clinic Rochester Reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Present
Update on Myelodysplastic Syndromes and Myeloproliferative Neoplasms Kaaren Reichard Mayo Clinic Rochester Reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Present
Myelodysplastic syndromes: revised WHO classification and distinction from non-neoplastic conditions
 Myelodysplastic syndromes: revised WHO classification and distinction from non-neoplastic conditions Robert P Hasserjian, MD Associate Professor Massachusetts General Hospital and Harvard Medical School
Myelodysplastic syndromes: revised WHO classification and distinction from non-neoplastic conditions Robert P Hasserjian, MD Associate Professor Massachusetts General Hospital and Harvard Medical School
Juvenile Myelomonocytic Leukemia (JMML)
") Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
Juvenile Myelomonocytic Leukemia (JMML) JMML: Definition Monoclonal hematopoietic disorder of childhood characterized by proliferation of the granulocytic and monocytic lineages Erythroid and megakaryocytic
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms. Curtis A. Hanson, MD
 Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Opportunities for Optimal Testing in the Myeloproliferative Neoplasms Curtis A. Hanson, MD 2013 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2013 MFMER slide-2
Myelodysplastic Syndromes: WHO 2008
 Myelodysplastic Syndromes: WHO 2008 Attilio Orazi, M.D., FRCPath. (Engl.) Weill Medical College of Cornell University New York, NY Congresso Nazionale SIE - Società Italiana di Ematologia - MIC Milano
Myelodysplastic Syndromes: WHO 2008 Attilio Orazi, M.D., FRCPath. (Engl.) Weill Medical College of Cornell University New York, NY Congresso Nazionale SIE - Società Italiana di Ematologia - MIC Milano
Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms. Daniel A. Arber, MD Stanford University
 Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms Daniel A. Arber, MD Stanford University What is an integrated approach? What is an integrated approach? Incorporating all diagnostic
Integrated Diagnostic Approach to the Classification of Myeloid Neoplasms Daniel A. Arber, MD Stanford University What is an integrated approach? What is an integrated approach? Incorporating all diagnostic
Approaching myeloid neoplasms: diagnostic algorithms
 Approaching myeloid neoplasms: diagnostic algorithms Alexandar Tzankov Histopathology Pathology Content Integration of clinical and laboratory data Bone marrow evaluation approaching Myeloproliferative
Approaching myeloid neoplasms: diagnostic algorithms Alexandar Tzankov Histopathology Pathology Content Integration of clinical and laboratory data Bone marrow evaluation approaching Myeloproliferative
Heme 9 Myeloid neoplasms
 Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Heme 9 Myeloid neoplasms The minimum number of blasts to diagnose acute myeloid leukemia is 5% 10% 20% 50% 80% AML with the best prognosis is AML with recurrent cytogenetic abnormality AML with myelodysplasia
Session 4: Summary and Conclusions
 Session 4: Summary and Conclusions Total cases in Session 4 Myeloproliferative neoplasms 16 cases Oral #300 (CEL, NOS) Mastocytosis 2 cases Oral #156 (SM-AHN) Myeloid/lymphoid neoplasms with eosinophilia
Session 4: Summary and Conclusions Total cases in Session 4 Myeloproliferative neoplasms 16 cases Oral #300 (CEL, NOS) Mastocytosis 2 cases Oral #156 (SM-AHN) Myeloid/lymphoid neoplasms with eosinophilia
Myelodysplastic syndromes
 Myelodysplastic syndromes Robert P Hasserjian Massachusetts General Hospital, Boston, MA Disclosure of Relevant Financial Relationships Dr. Hasserjian declares he has no conflict(s) of interest to disclose.
Myelodysplastic syndromes Robert P Hasserjian Massachusetts General Hospital, Boston, MA Disclosure of Relevant Financial Relationships Dr. Hasserjian declares he has no conflict(s) of interest to disclose.
Disclosure BCR/ABL1-Negative Classical Myeloproliferative Neoplasms
 Disclosure BCR/ABL1-Negative Classical Myeloproliferative Neoplasms Sonam Prakash declares affiliation with Incyte Corporation: Advisor for Hematopathology Publications Steering Committee Sonam Prakash,
Disclosure BCR/ABL1-Negative Classical Myeloproliferative Neoplasms Sonam Prakash declares affiliation with Incyte Corporation: Advisor for Hematopathology Publications Steering Committee Sonam Prakash,
Disclosures for Ayalew Tefferi
 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
WHO Classification 7/2/2009
 Least Malignant Myeloproliferative Disorders Myelodysplastic Syndromes Most Malignant Acute Leukemia Classifying Hematopoietic Disorders French-American-British (FAB) World Health Organization (WHO) Thanks
Least Malignant Myeloproliferative Disorders Myelodysplastic Syndromes Most Malignant Acute Leukemia Classifying Hematopoietic Disorders French-American-British (FAB) World Health Organization (WHO) Thanks
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure
 Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
Beyond the CBC Report: Extended Laboratory Testing in the Evaluation for Hematologic Neoplasia Disclosure I am receiving an honorarium from Sysmex for today s presentation. 1 Determining the Etiology for
MDS/MPN: What it is and How it Should be Treated?
 MDS/MPN: What it is and How it Should be Treated? MDS MPN Rachel Salit, MD Assistant Member Fred Hutchinson Cancer Research Center rsalit@fredhutch.org MDS Founda>on Pa>ent & Family Forum: May 20, 2017
MDS/MPN: What it is and How it Should be Treated? MDS MPN Rachel Salit, MD Assistant Member Fred Hutchinson Cancer Research Center rsalit@fredhutch.org MDS Founda>on Pa>ent & Family Forum: May 20, 2017
WHO 2016/17 update on Myeloproliferative Neoplasms. Anna Ruskova Auckland City Hospital New Zealand
 WHO 2016/17 update on Myeloproliferative Neoplasms Anna Ruskova Auckland City Hospital New Zealand BLOOD, 19 MAY 2016 x VOLUME 127, NUMBER 20 2 2016/17 Classification of Myeloproliferative Neoplasms Chronic
WHO 2016/17 update on Myeloproliferative Neoplasms Anna Ruskova Auckland City Hospital New Zealand BLOOD, 19 MAY 2016 x VOLUME 127, NUMBER 20 2 2016/17 Classification of Myeloproliferative Neoplasms Chronic
Chronic Idiopathic Myelofibrosis (CIMF)
") Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
Chronic Idiopathic Myelofibrosis (CIMF) CIMF Synonyms Agnogenic myeloid metaplasia Myelosclerosis with myeloid metaplasia Chronic granulocytic-megakaryocytic myelosis CIMF Megakaryocytic proliferation
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD. Part 4 MYELOID NEOPLASMS
 HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
HENATOLYMPHOID SYSTEM THIRD YEAR MEDICAL STUDENTS- UNIVERSITY OF JORDAN AHMAD T. MANSOUR, MD Part 4 MYELOID NEOPLASMS Introduction: o Myeloid neoplasms are divided into three major categories: o Acute
Disclosures. I do not have anything to disclose. Shared Features of MPNs. Overview. Diagnosis and Molecular Monitoring in the
 Myeloproliferative Neoplasms: Diagnosis and Molecular Monitoring in the Target Therapy Era C. Cameron Yin, M.D., Ph.D. Department of Hematopathology UT MD Anderson Cancer Center Disclosures I do not have
Myeloproliferative Neoplasms: Diagnosis and Molecular Monitoring in the Target Therapy Era C. Cameron Yin, M.D., Ph.D. Department of Hematopathology UT MD Anderson Cancer Center Disclosures I do not have
Hematology Unit Lab 2 Review Material
 Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
Objectives Hematology Unit Lab 2 Review Material - 2018 Laboratory Instructors: 1. Assist students during lab session Students: 1. Review the introductory material 2. Study the case histories provided
74y old Female with chronic elevation of Platelet count. August 18, 2005 Faizi Ali, MD Hematopathology Fellow
 74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
74y old Female with chronic elevation of Platelet count August 18, 2005 Faizi Ali, MD Hematopathology Fellow Clinical History Patient is a 74y old otherwise healthy Caucasian female with no major complaint
Pathogenesis and management of CMML
 Pathogenesis and management of CMML Raphaël Itzykson, Hôpital Saint-Louis, Paris International Conference of the Korean Society of Hematology March 29th 2018 대한혈액학회 Korean Society of Hematology COI disclosure
Pathogenesis and management of CMML Raphaël Itzykson, Hôpital Saint-Louis, Paris International Conference of the Korean Society of Hematology March 29th 2018 대한혈액학회 Korean Society of Hematology COI disclosure
Myeloproliferative Neoplasms: Diagnosis and Molecular Monitoring in the Era of Target Therapy
 Myeloproliferative Neoplasms: Diagnosis and Molecular Monitoring in the Era of Target Therapy C. Cameron Yin, M.D., Ph.D. Department of Hematopathology UT MD Anderson Cancer Center Disclosures I do not
Myeloproliferative Neoplasms: Diagnosis and Molecular Monitoring in the Era of Target Therapy C. Cameron Yin, M.D., Ph.D. Department of Hematopathology UT MD Anderson Cancer Center Disclosures I do not
Myeloid neoplasms. Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories:
 Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Myeloid neoplasms Note: Early arrest in the blast cell or immature cell "we call it acute leukemia" Myoid neoplasm divided in to 3 major categories: 1. AML : Acute myeloid leukemia(stem cell with myeloid
Disclosures for Ayalew Tefferi
 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Myelodysplastic/Myeloproliferative Disorders. MDS/MPD Unclassified Provisional: CMML JMML acml RARS T. K. Foucar November 2007 SH/EAHP Workshop
 Myelodysplastic/Myeloproliferative Disorders CMML JMML acml MDS/MPD Unclassified Provisional: RARS T K. Foucar November 2007 SH/EAHP Workshop MDS/MPD: General Features Blood: Cytosis and cytopenia(s) Dysplasia
Myelodysplastic/Myeloproliferative Disorders CMML JMML acml MDS/MPD Unclassified Provisional: RARS T K. Foucar November 2007 SH/EAHP Workshop MDS/MPD: General Features Blood: Cytosis and cytopenia(s) Dysplasia
MDS/MPN MPN MDS. Discolosures. Advances in the Diagnosis of Myeloproliferative Neoplasms. Myeloproliferative neoplasms
 Discolosures Advances in the Diagnosis of Myeloproliferative Neoplasms Consulting income from Promedior, Inc. Robert P Hasserjian, MD Associate Professor Massachusetts General Hospital and Harvard Medical
Discolosures Advances in the Diagnosis of Myeloproliferative Neoplasms Consulting income from Promedior, Inc. Robert P Hasserjian, MD Associate Professor Massachusetts General Hospital and Harvard Medical
Myelodysplastic syndromes and the new WHO 2016 classification
 Myelodysplastic syndromes and the new WHO 2016 classification 32nd General Annual Meeting of the Belgian Hematology Society 10-11 February 2017 Gregor Verhoef, Departement of Hematology, University Hospital
Myelodysplastic syndromes and the new WHO 2016 classification 32nd General Annual Meeting of the Belgian Hematology Society 10-11 February 2017 Gregor Verhoef, Departement of Hematology, University Hospital
Disclosures. Myeloproliferative Neoplasms: A Case-Based Approach. Objectives. Myeloproliferative Neoplasms. Myeloproliferative Neoplasms
 Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
Myeloproliferative Neoplasms: A Case-Based Approach Disclosures No conflicts of interests regarding the topic being presented Adam M. Miller, MD PGY-4 Resident Physician Department of Pathology and Laboratory
MPN What's new in the morphological classification, grading of fibrosis and the impact of novel drugs
 MPN What's new in the morphological classification, grading of fibrosis and the impact of novel drugs Hans Michael Kvasnicka University of Frankfurt, Germany hans-michael.kvasnicka@kgu.de Disclosure of
MPN What's new in the morphological classification, grading of fibrosis and the impact of novel drugs Hans Michael Kvasnicka University of Frankfurt, Germany hans-michael.kvasnicka@kgu.de Disclosure of
9/25/2017. Disclosure. I have nothing to disclose. Young S. Kim MD Dept. of Pathology
 Disclosure MAST CELLNEOPLASM I have nothing to disclose. Young S. Kim MD Dept. of Pathology 1 Objectives What is mast cell lineage? Changes in updated WHO 2016 mastocytosis Issues of Mastocytosis CD30
Disclosure MAST CELLNEOPLASM I have nothing to disclose. Young S. Kim MD Dept. of Pathology 1 Objectives What is mast cell lineage? Changes in updated WHO 2016 mastocytosis Issues of Mastocytosis CD30
Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Neoplasms. Policy Specific Section:
 Medical Policy Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Type: Medical Necessity and Investigational / Experimental Policy Specific Section:
Medical Policy Allogeneic Hematopoietic Stem-Cell Transplantation for Myelodysplastic Syndromes and Myeloproliferative Type: Medical Necessity and Investigational / Experimental Policy Specific Section:
Refresher in Blood Cell Morphology. Tracy I. George, MD Professor of Pathology University of Utah
 Refresher in Blood Cell Morphology Tracy I. George, MD Professor of Pathology University of Utah No financial conflicts of interest Objectives Recognize non-neoplastic and neoplastic disorders in the peripheral
Refresher in Blood Cell Morphology Tracy I. George, MD Professor of Pathology University of Utah No financial conflicts of interest Objectives Recognize non-neoplastic and neoplastic disorders in the peripheral
SESSION 1 Reactive cytopenia and dysplasia
 SESSION 1 Reactive cytopenia and dysplasia Falko Fend, Tübingen & Alexandar Tzankov, Basel 1 Disclosure of speaker s interests (Potential) conflict of interest none Potentially relevant company relationships
SESSION 1 Reactive cytopenia and dysplasia Falko Fend, Tübingen & Alexandar Tzankov, Basel 1 Disclosure of speaker s interests (Potential) conflict of interest none Potentially relevant company relationships
ADx Bone Marrow Report. Patient Information Referring Physician Specimen Information
 ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
ADx Bone Marrow Report Patient Information Referring Physician Specimen Information Patient Name: Specimen: Bone Marrow Site: Left iliac Physician: Accession #: ID#: Reported: 08/19/2014 - CHRONIC MYELOGENOUS
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms
 & Myeloproliferative neoplasms") Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
Myelodysplastic syndrome (MDS) & Myeloproliferative neoplasms Myelodysplastic syndrome (MDS) A multipotent stem cell that can differentiate into any of the myeloid lineage cells (RBCs, granulocytes, megakaryocytes)
WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities
 WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities Robert W. McKenna, M.D. 1/2009 WHO Classification of Myeloid Neoplasms (4th Edition)--2008 Incorporates new information that
WHO Classification of Myeloid Neoplasms with Defined Molecular Abnormalities Robert W. McKenna, M.D. 1/2009 WHO Classification of Myeloid Neoplasms (4th Edition)--2008 Incorporates new information that
Changes to the 2016 WHO Classification for the Diagnosis of MDS
 Changes to the 2016 WHO Classification for the Diagnosis of MDS Welcome to Managing MDS. I am Dr. Ulrich Germing, and today, I will provide highlights from the 14th International Symposium on MDS in Valencia,
Changes to the 2016 WHO Classification for the Diagnosis of MDS Welcome to Managing MDS. I am Dr. Ulrich Germing, and today, I will provide highlights from the 14th International Symposium on MDS in Valencia,
NON-CLASSIC MYELOPROLIFERATIVE NEOPLASMS: ARE WE REALLY AWARE OF THESE RARE DISEASES IN DAILY PRACTICE?
 NON-CLASSIC MYELOPROLIFERATIVE NEOPLASMS: ARE WE REALLY AWARE OF THESE RARE DISEASES IN DAILY PRACTICE? *Serdal Korkmaz Department of Hematology, Kayseri Training and Research Hospital, Kayseri, Turkey
NON-CLASSIC MYELOPROLIFERATIVE NEOPLASMS: ARE WE REALLY AWARE OF THESE RARE DISEASES IN DAILY PRACTICE? *Serdal Korkmaz Department of Hematology, Kayseri Training and Research Hospital, Kayseri, Turkey
Hematopathology Case Study
 www.medfusionservices.com Hematopathology Case Study CV3515-14 JUNE Clinical Presentation: Clinical Information: A 42 year old male with history of chronic myelogenous leukemia (CML) presents with an elevated
www.medfusionservices.com Hematopathology Case Study CV3515-14 JUNE Clinical Presentation: Clinical Information: A 42 year old male with history of chronic myelogenous leukemia (CML) presents with an elevated
Disclosures for Ayalew Tefferi
 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Diagnostic Approach for Eosinophilia and Mastocytosis. Curtis A. Hanson, M.D.
 Diagnostic Approach for Eosinophilia and Mastocytosis Curtis A. Hanson, M.D. 2014 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2014 MFMER slide-2 Molecular Classification
Diagnostic Approach for Eosinophilia and Mastocytosis Curtis A. Hanson, M.D. 2014 MFMER slide-1 DISCLOSURES: Relevant Financial Relationship(s) None Off Label Usage None 2014 MFMER slide-2 Molecular Classification
MYELOPROLIFERATIVE NEOPLASMS
 9 : 2 MYELOPROLIFERATIVE NEOPLASMS Introduction William Dameshek in 1951 introduced the term Myeloproliferative disorders (MPD). This included polycythemia vera (PV), essential thrombocythemia (ET), primary
9 : 2 MYELOPROLIFERATIVE NEOPLASMS Introduction William Dameshek in 1951 introduced the term Myeloproliferative disorders (MPD). This included polycythemia vera (PV), essential thrombocythemia (ET), primary
New WHO Classification of Myeloproliferative Neoplasms
 New WHO Classification of Myeloproliferative Neoplasms Hans Michael Kvasnicka Senckenberg Institute of Pathology, University of Frankfurt, Germany hans-michael.kvasnicka@kgu.de Principles and rationale
New WHO Classification of Myeloproliferative Neoplasms Hans Michael Kvasnicka Senckenberg Institute of Pathology, University of Frankfurt, Germany hans-michael.kvasnicka@kgu.de Principles and rationale
Polycthemia Vera (Rubra)
") Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
Polycthemia Vera (Rubra) Polycthemia Vera (Rubra) Increased red cells Clonal Myeloid lineages also increased 2-13 cases per million Mean age: 60 years Sites of Involvement Bone marrow Peripheral blood
Update on the WHO Classification of Acute Myeloid Leukemia. Kaaren K. Reichard, MD Mayo Clinic Rochester
 Update on the WHO Classification of Acute Myeloid Leukemia Kaaren K. Reichard, MD Mayo Clinic Rochester reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Objectives Present a practical
Update on the WHO Classification of Acute Myeloid Leukemia Kaaren K. Reichard, MD Mayo Clinic Rochester reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Objectives Present a practical
Characterization of MPL-mutated myeloid neoplasms: a review of 224 MPL+ cases
 Article Characterization of MPL-mutated myeloid neoplasms: a review of 224 MPL+ cases Keming Lin 1,*, Gang Xu 1, Jie-Gen Jiang 1, Mayuko Imai 1, Zhao Wu 1, Paris Petersen 1, Kim Janatpour 1, and Bashar
Article Characterization of MPL-mutated myeloid neoplasms: a review of 224 MPL+ cases Keming Lin 1,*, Gang Xu 1, Jie-Gen Jiang 1, Mayuko Imai 1, Zhao Wu 1, Paris Petersen 1, Kim Janatpour 1, and Bashar
Chronic myelomonocytic leukemia. Lymphoma Tumor Board. May 26, 2017
 Chronic myelomonocytic leukemia Lymphoma Tumor Board May 26, 2017 Myeloproliferative Neoplasms CMML has an estimated incidence of less than 1 per 100,000 persons per year Myeloproliferative neoplasms (MPN)
Chronic myelomonocytic leukemia Lymphoma Tumor Board May 26, 2017 Myeloproliferative Neoplasms CMML has an estimated incidence of less than 1 per 100,000 persons per year Myeloproliferative neoplasms (MPN)
AML: WHO classification, biology and prognosis. Dimitri Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen
 AML: WHO classification, biology and prognosis Dimitri Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen Acute myeloid leukemia Clonal expansion of undifferentiated myeloid precursors Impaired
AML: WHO classification, biology and prognosis Dimitri Breems, MD, PhD Internist-Hematoloog Ziekenhuis Netwerk Antwerpen Acute myeloid leukemia Clonal expansion of undifferentiated myeloid precursors Impaired
Molecular techniques in a case of concurrent BCR-ABL1 positive CML and CMML
 reprinted from november 2014 pathology laboratory medicine laboratory management Molecular techniques in a case of concurrent BCR-ABL1 positive CML and CMML CAP TODAY and the Association for Molecular
reprinted from november 2014 pathology laboratory medicine laboratory management Molecular techniques in a case of concurrent BCR-ABL1 positive CML and CMML CAP TODAY and the Association for Molecular
Pathology. #11 Acute Leukemias. Farah Banyhany. Dr. Sohaib Al- Khatib 23/2/16
 35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
35 Pathology #11 Acute Leukemias Farah Banyhany Dr. Sohaib Al- Khatib 23/2/16 1 Salam First of all, this tafreegh is NOT as long as you may think. If you just focus while studying this, everything will
Hematology 101. Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD
 Hematology 101 Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD Hematocrits Plasma White cells Red cells Normal, Hemorrhage, IDA, Leukemia,
Hematology 101 Blanche P Alter, MD, MPH, FAAP Clinical Genetics Branch Division of Cancer Epidemiology and Genetics Bethesda, MD Hematocrits Plasma White cells Red cells Normal, Hemorrhage, IDA, Leukemia,
Blast transformation in chronic myelomonocytic leukemia: Risk factors, genetic features, survival, and treatment outcome
 RESEARCH ARTICLE Blast transformation in chronic myelomonocytic leukemia: Risk factors, genetic features, survival, and treatment outcome AJH Mrinal M. Patnaik, 1 Emnet A. Wassie, 1 Terra L. Lasho, 2 Curtis
RESEARCH ARTICLE Blast transformation in chronic myelomonocytic leukemia: Risk factors, genetic features, survival, and treatment outcome AJH Mrinal M. Patnaik, 1 Emnet A. Wassie, 1 Terra L. Lasho, 2 Curtis
Case Workshop of Society for Hematopathology and European Association for Haematopathology
 Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
Case 148 2007 Workshop of Society for Hematopathology and European Association for Haematopathology Robert P Hasserjian Department of Pathology Massachusetts General Hospital Boston, MA Clinical history
2 nd step do Bone Marrow Study If possible both the aspiration and
 Blood Malignancies-I Prof. Herman Hariman,SpPK a (KH). Ph.D.(U.K) Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. Clinpath, FK-USU First do the Full Blood Count Hb, WBCS, Platelets Morphology!! Such as blasts,
Blood Malignancies-I Prof. Herman Hariman,SpPK a (KH). Ph.D.(U.K) Prof. Dr. Adikoesoema Aman, SpPK (KH) Dept. Clinpath, FK-USU First do the Full Blood Count Hb, WBCS, Platelets Morphology!! Such as blasts,
Case Presentation No. 075
 Case Presentation No. 075 Session 4. Myelodysplastic Syndrome Cristina Montalvo, MD Baylor College of Medicine Houston, Texas 2007 Workshop of Society for Hematopathology and European Association for Haematopathology
Case Presentation No. 075 Session 4. Myelodysplastic Syndrome Cristina Montalvo, MD Baylor College of Medicine Houston, Texas 2007 Workshop of Society for Hematopathology and European Association for Haematopathology
Welcome to Master Class for Oncologists. Session 3: 9:15 AM - 10:00 AM
 Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
Welcome to Master Class for Oncologists Session 3: 9:15 AM - 10:00 AM Miami, FL December 18, 2009 Myeloproliferative Neoplasms: Bringing Order to Complexity and Achieving Optimal Outcomes Speaker: Andrew
Disclosures for Ayalew Tefferi
 Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
Disclosures for Ayalew Tefferi Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Janssen, Geron, Celgene, Sanofi-Aventis, Gilead Sciences, Incyte
SWOG ONCOLOGY RESEARCH PROFESSIONAL (ORP) MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017
 MANUAL LEUKEMIA FORMS CHAPTER 16A REVISED: DECEMBER 2017") LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
LEUKEMIA FORMS The guidelines and figures below are specific to Leukemia studies. The information in this manual does NOT represent a complete set of required forms for any leukemia study. Please refer
CASE 106. Pancytopenia in the setting of marrow hypoplasia, a PNH clone, and a DNMT3A mutation
 CASE 106 Pancytopenia in the setting of marrow hypoplasia, a PNH clone, and a DNMT3A mutation Gabriel C. Caponetti, MD University of Pennsylvania, US Clinical history 69, F peripheral neuropathy, refractory
CASE 106 Pancytopenia in the setting of marrow hypoplasia, a PNH clone, and a DNMT3A mutation Gabriel C. Caponetti, MD University of Pennsylvania, US Clinical history 69, F peripheral neuropathy, refractory
ACCME/Disclosures. History. Hematopathology Specialty Conference Case #4 4/13/2016
 Hematopathology Specialty Conference Case #4 Sherrie L. Perkins MD, PhD University of Utah ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose
Hematopathology Specialty Conference Case #4 Sherrie L. Perkins MD, PhD University of Utah ACCME/Disclosures The USCAP requires that anyone in a position to influence or control the content of CME disclose
SUPPLEMENTARY INFORMATION
 Supplementary Information S1 Frequency of DNMT3A mutations in hematologic disorders and their associated clinical phenotypes. Disease Patient population Frequency (%) Associated Clinical Characteristics
Supplementary Information S1 Frequency of DNMT3A mutations in hematologic disorders and their associated clinical phenotypes. Disease Patient population Frequency (%) Associated Clinical Characteristics
Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas. James J. Stark, MD, FACP
 Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS
Myeloproliferative Disorders: Diagnostic Enigmas, Therapeutic Dilemmas James J. Stark, MD, FACP Medical Director, Cancer Program and Palliative Care Maryview Medical Center Professor of Medicine, EVMS
Extramedullary precursor T-lymphoblastic transformation of CML at presentation
 Extramedullary precursor T-lymphoblastic transformation of CML at presentation Neerja Vajpayee, Constance Stein, Bernard Poeisz & Robert E. Hutchison Clinical History 30 year old man presented to the emergency
Extramedullary precursor T-lymphoblastic transformation of CML at presentation Neerja Vajpayee, Constance Stein, Bernard Poeisz & Robert E. Hutchison Clinical History 30 year old man presented to the emergency
Table 1: biological tests in SMD
 Table 1: biological tests in SMD Tests Mandatory Recommended Under validation Morphology Marrow aspirate Marrow biopsy 1 Iron staining Quantification of dysplasia WHO 2008 Classification Cytogenetics Conventional
Table 1: biological tests in SMD Tests Mandatory Recommended Under validation Morphology Marrow aspirate Marrow biopsy 1 Iron staining Quantification of dysplasia WHO 2008 Classification Cytogenetics Conventional
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed
 MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
MYELODYSPLASTIC SYNDROMES: A diagnosis often missed D R. EMMA W YPKEMA C O N S U LTA N T H A E M AT O L O G I S T L A N C E T L A B O R AT O R I E S THE MYELODYSPLASTIC SYNDROMES DEFINITION The Myelodysplastic
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls
 Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
Myelodysplastic Syndromes: Everyday Challenges and Pitfalls Kathryn Foucar, MD kfoucar@salud.unm.edu Henry Moon lecture May 2007 Outline Definition Conceptual overview; pathophysiologic mechanisms Incidence,
Disclosures for Angela Fleischman
 Disclosures for Angela Fleischman Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Sierra, Incyte None None None Incyte None Presentation includes
Disclosures for Angela Fleischman Principal investigator role Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board Sierra, Incyte None None None Incyte None Presentation includes
5/21/2018. Disclosures. Objectives. Normal blood cells production. Bone marrow failure syndromes. Story of DNA
 AML: Understanding your diagnosis and current and emerging treatments Nothing to disclose. Disclosures Mohammad Abu Zaid, MD Assistant Professor of Medicine Indiana University School of Medicine Indiana
AML: Understanding your diagnosis and current and emerging treatments Nothing to disclose. Disclosures Mohammad Abu Zaid, MD Assistant Professor of Medicine Indiana University School of Medicine Indiana
Conditions that mimic neoplasia in the bone marrow. Kaaren K. Reichard Mayo Clinic Rochester
 Conditions that mimic neoplasia in the bone marrow Kaaren K. Reichard Mayo Clinic Rochester reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Multiple conditions in
Conditions that mimic neoplasia in the bone marrow Kaaren K. Reichard Mayo Clinic Rochester reichard.kaaren@mayo.edu Nothing to disclose Conflict of Interest Learning Objectives Multiple conditions in
Prognostic models in PV and ET
 Prognostic models in PV and ET Francesco Passamonti Hematology, Varese, Italy Current risk stratification in PV and ET: statement from European LeukemiaNet consensus Age over 60 years Previuos thrombosis
Prognostic models in PV and ET Francesco Passamonti Hematology, Varese, Italy Current risk stratification in PV and ET: statement from European LeukemiaNet consensus Age over 60 years Previuos thrombosis
Evaluation of Bone Marrow Biopsies and Aspirates ANNA PORWIT DEPARTMENT OF PATHOLOGY, LUND UNIVERSITY
 Evaluation of Bone Marrow Biopsies and Aspirates ANNA PORWIT DEPARTMENT OF PATHOLOGY, LUND UNIVERSITY DISCLOSURES NONE Learning objectives To review the rules of BMA evaluation To review the main issues
Evaluation of Bone Marrow Biopsies and Aspirates ANNA PORWIT DEPARTMENT OF PATHOLOGY, LUND UNIVERSITY DISCLOSURES NONE Learning objectives To review the rules of BMA evaluation To review the main issues
[COMPREHENSIVE GENETIC ASSAY PANEL ON
 2014 SN GENELAB AND RESEARCH CENTER DR. SALIL VANIAWALA, PH.D [COMPREHENSIVE GENETIC ASSAY PANEL ON MYELOPROLIFERATIVE NEOPLASMS] SN Genelab presents one of the most comprehensive genetic assay panel for
2014 SN GENELAB AND RESEARCH CENTER DR. SALIL VANIAWALA, PH.D [COMPREHENSIVE GENETIC ASSAY PANEL ON MYELOPROLIFERATIVE NEOPLASMS] SN Genelab presents one of the most comprehensive genetic assay panel for
Session II: Summary. Robert P Hasserjian, MD Professor of Pathology Massachusetts General Hospital and Harvard Medical School
 Session II: Summary Robert P Hasserjian, MD Professor of Pathology Massachusetts General Hospital and Harvard Medical School Disclosure of speaker s interests (Prefix and Last Name) (Potential) conflict
Session II: Summary Robert P Hasserjian, MD Professor of Pathology Massachusetts General Hospital and Harvard Medical School Disclosure of speaker s interests (Prefix and Last Name) (Potential) conflict
Cost-Effective Strategies in the Workup of Hematologic Neoplasm. Karl S. Theil, Claudiu V. Cotta Cleveland Clinic
 Cost-Effective Strategies in the Workup of Hematologic Neoplasm Karl S. Theil, Claudiu V. Cotta Cleveland Clinic In the past 12 months, we have not had a significant financial interest or other relationship
Cost-Effective Strategies in the Workup of Hematologic Neoplasm Karl S. Theil, Claudiu V. Cotta Cleveland Clinic In the past 12 months, we have not had a significant financial interest or other relationship
JAK inhibitors in Phmyeloproliferative
 Disclosures for A Pardanani Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board TargeGen, Cytopia/YM BioSciences, PharmaMar None None None None None Presentation
Disclosures for A Pardanani Research Support/P.I. Employee Consultant Major Stockholder Speakers Bureau Scientific Advisory Board TargeGen, Cytopia/YM BioSciences, PharmaMar None None None None None Presentation
Disclosure: Objectives/Outline. Leukemia: Genealogy of Pathology Practice: Old Diseases New Expectations. Nothing to disclose.
 RC1 Leukemia: Genealogy of Pathology Practice: Old Diseases New Expectations RC2 Disclosure: Nothing to disclose Henry Moon Lecture: UCSF Annual Conference Kathryn Foucar, MD kfoucar@salud.unm.edu May
RC1 Leukemia: Genealogy of Pathology Practice: Old Diseases New Expectations RC2 Disclosure: Nothing to disclose Henry Moon Lecture: UCSF Annual Conference Kathryn Foucar, MD kfoucar@salud.unm.edu May
2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228
 2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228 Vishnu V. B Reddy, MD University of Alabama at Birmingham Birmingham, AL USA 11/03/07
2007 Workshop of Society for Hematopathology & European Association for Hematopathology Indianapolis, IN, USA Case # 228 Vishnu V. B Reddy, MD University of Alabama at Birmingham Birmingham, AL USA 11/03/07
Case #16: Diagnosis. T-Lymphoblastic lymphoma. But wait, there s more... A few weeks later the cytogenetics came back...
 Case #16: Diagnosis T-Lymphoblastic lymphoma But wait, there s more... A few weeks later the cytogenetics came back... 46,XY t(8;13)(p12;q12)[12] Image courtesy of Dr. Xinyan Lu Further Studies RT-PCR
Case #16: Diagnosis T-Lymphoblastic lymphoma But wait, there s more... A few weeks later the cytogenetics came back... 46,XY t(8;13)(p12;q12)[12] Image courtesy of Dr. Xinyan Lu Further Studies RT-PCR
HEMATOLOGIC MALIGNANCIES BIOLOGY
 HEMATOLOGIC MALIGNANCIES BIOLOGY Failure of terminal differentiation Failure of differentiated cells to undergo apoptosis Failure to control growth Neoplastic stem cell FAILURE OF TERMINAL DIFFERENTIATION
HEMATOLOGIC MALIGNANCIES BIOLOGY Failure of terminal differentiation Failure of differentiated cells to undergo apoptosis Failure to control growth Neoplastic stem cell FAILURE OF TERMINAL DIFFERENTIATION
Etiology. Definition MYELODYSPLASTIC SYNDROMES. De novo. Secondary MDS (10 years earlier than primary) transformation
 transformation") MYELODYSPLASTIC SYNDROMES Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics The University of Texas M.D. Anderson Cancer Center Houston, Texas No relevant COIs to
MYELODYSPLASTIC SYNDROMES Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics The University of Texas M.D. Anderson Cancer Center Houston, Texas No relevant COIs to
DISCLOSURE Luca Malcovati, MD. No financial relationships to disclose
 ICUS, CCUS and CHIP Luca Malcovati, MD Department of Molecular Medicine, University of Pavia Medical School, & Department of Hematology Oncology, IRCCS Policlinico S. Matteo Foundation, Pavia, Italy DISCLOSURE
ICUS, CCUS and CHIP Luca Malcovati, MD Department of Molecular Medicine, University of Pavia Medical School, & Department of Hematology Oncology, IRCCS Policlinico S. Matteo Foundation, Pavia, Italy DISCLOSURE
Combinations of morphology codes of haematological malignancies (HM) referring to the same tumour or to a potential transformation
 referring to the same tumour or to a potential transformation") Major subgroups according to the World Health Organisation (WHO) Classification Myeloproliferative neoplasms (MPN) Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB or
Major subgroups according to the World Health Organisation (WHO) Classification Myeloproliferative neoplasms (MPN) Myeloid and lymphoid neoplasms with eosinophilia and abnormalities of PDGFRA, PDGFRB or
APPROACH TO MYELODYSPLASTIC SYNDROMES IN THE ERA OF PRECISION MEDICINE
 APPROACH TO MYELODYSPLASTIC SYNDROMES IN THE ERA OF PRECISION MEDICINE Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics Department of Hematopathology The University
APPROACH TO MYELODYSPLASTIC SYNDROMES IN THE ERA OF PRECISION MEDICINE Rashmi Kanagal-Shamanna, MD Assistant Professor Hematopathology & Molecular Diagnostics Department of Hematopathology The University
Case #1. 65 yo man with no prior history presented with leukocytosis and circulating blasts: Bone marrow biopsy was performed
 Case #1 65 yo man with no prior history presented with leukocytosis and circulating blasts: WBC 187.4K/uL ; Hgb 10.0gm/dL; Platelet 68K/uL Neutrophil % 25.0% Lymphocyte % 38.0% Monocyte % 12.0% Metamyelocyte
Case #1 65 yo man with no prior history presented with leukocytosis and circulating blasts: WBC 187.4K/uL ; Hgb 10.0gm/dL; Platelet 68K/uL Neutrophil % 25.0% Lymphocyte % 38.0% Monocyte % 12.0% Metamyelocyte
Dong Wook Jekarl 1, Sang Bong Han 1, Myungshin Kim 1, Jihyang Lim 1, Eun-Jee Oh 1, Yonggoo Kim 1, Hee-Je Kim 2, Woo-Sung Min 2, Kyungja Han 1
 VOLUME 45 ㆍ NUMBER 1 ㆍ MARCH 2010 THE KOREAN JOURNAL OF HEMATOLOGY ORIGINAL ARTICLE JAK2 V617F mutation in myelodysplastic syndrome, myelodysplastic syndrome/myeloproliferative neoplasm, unclassifiable,
VOLUME 45 ㆍ NUMBER 1 ㆍ MARCH 2010 THE KOREAN JOURNAL OF HEMATOLOGY ORIGINAL ARTICLE JAK2 V617F mutation in myelodysplastic syndrome, myelodysplastic syndrome/myeloproliferative neoplasm, unclassifiable,
Leukemia and subsequent solid tumors among patients with myeloproliferative neoplasms
 Leukemia and subsequent solid tumors among patients with myeloproliferative neoplasms Tiziano Barbui (tbarbui@asst-pg23.it Hematology and Research Foundation,Ospedale Papa Giovanni XXIII, Bergamo Italy
Leukemia and subsequent solid tumors among patients with myeloproliferative neoplasms Tiziano Barbui (tbarbui@asst-pg23.it Hematology and Research Foundation,Ospedale Papa Giovanni XXIII, Bergamo Italy
Leukocytosis - Some Learning Points
 Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
Leukocytosis - Some Learning Points Koh Liang Piu Department of Hematology-Oncology National University Cancer Institute National University Health System Objectives of this talk: 1. To provide some useful
CHALLENGING CASES PRESENTATION
 CHALLENGING CASES PRESENTATION Michael C. Wiemann, MD, FACP Program Co-Chair and Vice President Indy Hematology Education President, Clinical St. John Providence Physician Network Detroit, Michigan 36
CHALLENGING CASES PRESENTATION Michael C. Wiemann, MD, FACP Program Co-Chair and Vice President Indy Hematology Education President, Clinical St. John Providence Physician Network Detroit, Michigan 36
June 11, Ella Noel, D.O., FACOI 1717 West Broadway Madison, WI
 June 11, 2018 Ella Noel, D.O., FACOI 1717 West Broadway Madison, WI 53713 policycomments@wpsic.com RE: Draft Local Coverage Determination: MolDX: MDS FISH (DL37772) Dear Dr. Noel Thank you for the opportunity
June 11, 2018 Ella Noel, D.O., FACOI 1717 West Broadway Madison, WI 53713 policycomments@wpsic.com RE: Draft Local Coverage Determination: MolDX: MDS FISH (DL37772) Dear Dr. Noel Thank you for the opportunity
20/20 PATHOLOGY REPORTS
 20/20 PATHOLOGY REPORTS Improving the Physician Experience. Enhancing the Patient Experience. We are LabTest Diagnostics. LabTest Diagnostics has a full-service laboratory with state-of-the-art equipment
20/20 PATHOLOGY REPORTS Improving the Physician Experience. Enhancing the Patient Experience. We are LabTest Diagnostics. LabTest Diagnostics has a full-service laboratory with state-of-the-art equipment
MDS 101. What is bone marrow? Myelodysplastic Syndrome: Let s build a definition. Dysplastic? Syndrome? 5/22/2014. What does bone marrow do?
 101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
101 May 17, 2014 Myelodysplastic Syndrome: Let s build a definition Myelo bone marrow Gail J. Roboz, M.D. Director, Leukemia Program Associate Professor of Medicine What is bone marrow? What does bone
Morfologia normale e patologica
 Morfologia normale e patologica Gina Zini Centro di Ricerca ReCAMH Dpt. Ematologia Università Cattolica S. Cuore - Roma EMATOLOGIA DI LABORATORIO: percorsi diagnostici e obiettivi clinici. Milano 11-12
Morfologia normale e patologica Gina Zini Centro di Ricerca ReCAMH Dpt. Ematologia Università Cattolica S. Cuore - Roma EMATOLOGIA DI LABORATORIO: percorsi diagnostici e obiettivi clinici. Milano 11-12
Myelodysplastic Syndrome Case 158
 Myelodysplastic Syndrome Case 158 Dong Chen MD PhD Division of Hematopathology Mayo Clinic Clinical History 86 year old man Persistent borderline anemia and thrombocytopenia. His past medical history was
Myelodysplastic Syndrome Case 158 Dong Chen MD PhD Division of Hematopathology Mayo Clinic Clinical History 86 year old man Persistent borderline anemia and thrombocytopenia. His past medical history was
Approach To Leucocytosis
 C H A P T E R 58 Approach To Leucocytosis Madhuchanda Kar, S Kartthik, Prantar Chakrabarti ABSTRACT Leukocytosis means elevation of WBC count for the patient s age. Leukocytosis might be because of lymphoid
C H A P T E R 58 Approach To Leucocytosis Madhuchanda Kar, S Kartthik, Prantar Chakrabarti ABSTRACT Leukocytosis means elevation of WBC count for the patient s age. Leukocytosis might be because of lymphoid