New Insights into the Biology of Atherosclerosis and Primary Prevention: Controversy and Consensus in the JUPITER Trial
|
|
|
- Randolph McDowell
- 5 years ago
- Views:
Transcription




1 Fundacion Fernandez-CruzXXVIII Leccion Memorial New Insights into the Biology of Atherosclerosis and Primary Prevention: Controversy and Consensus in the JUPITER Trial Paul M Ridker, MD, MPH Eugene Braunwald Professor of Medicine Director, Center for Cardiovascular Disease Prevention Brigham and Women s Hospital Harvard Medical School, Boston, MA USA Dr Ridker is listed as a co-inventor on patents held by the Brigham and Women s Hospital that relate to the use of inflammatory biomarkers in cardiovascular disease and diabetes.

2 Annals Int Med 1961;55:33-50

3 LDLC Levels in 136,905 Patients Hospitalized With CAD: LDLC (mg/dl) < 130 mg/dl > 160 mg/dl < 3.4 mmol/l >4.1 mmol/l Sachdeva et al, Am Heart J 2009;157:111-7.e2.

4 Pro-Inflammatory Pathways Pro-Inflammatory Risk Factors ICAM-1 Selectins, HSPs, etc. Primary Pro-Inflammatory Cytokines ( e.g., IL-1, TNF-a ) CRP SAA IL-6 Messenger Cytokine Liver Endothelium and other cells Circulation Circulation 1999;100:
5
6 Inflammation, hscrp, and Vascular Prevention Is there evidence that individuals with elevated levels of the inflammatory biomarker hscrp are at high vascular risk even when other risk factors are acceptable? Is there evidence that individuals identified at increased risk due to inflammation benefit from a therapy they otherwise would not have received? Is there evidence that reducing inflammation per se will reduce vascular events? Should our guidelines for vascular disease prevention change?
7 Relative Risk of MI Relative Risk of Stroke hscrp and Risk of Future MI and CVA in Apparently Healthy Men P Trend <0.001 P Trend < Quartile of hs-crp Quartile of hs-crp N Engl J Med 1997;336:
8 hscrp and Risks of Future MI: Analysis Stratified by Year of Follow-Up 2 Relative Risk (per quartile) Years of Study Follow-Up N Engl J Med 1997;336:973-9
9 hscrp, Aspirin, and Risks of Future Myocardial Infarction Relative Risk Myocardial Infarction 1 Placebo Aspirin Quartile of C-Reactive Protein N Engl J Med 1997;336:973-9
10 Risk Factors for Future Cardiovascular Events: WHS Lipoprotein(a) Homocysteine IL-6 TC LDLC sicam-1 SAA Apo B TC: HDLC hs-crp hs-crp + TC: HDLC Relative Risk of Future Cardiovascular Events N Engl J Med 2000;342:836-43
11 A Direct Comparison of LDL-C and hscrp in the Prediction of First Ever Cardiovascular Events Among 27,939 Women Total Cardiovascular Events MI, CABG, PTCA Ischemic Stroke Cardiovascular Death N Engl J Med 2002;347:
12 Relative Risk Relative Risk Relative Risk Relative Risk Markers of Inflammation in the Prediction of Cardiovascular Disease in Women High Medium Low Low Total Cholesterol Medium High High Medium Low Low Total Cholesterol Medium High High Medium Low Low Medium High High Medium Low Low Medium High Total Cholesterol Total Cholesterol NEJM. 2000;342:

13 Relative Risk Relative Risk Relative Risk Relative Risk Markers of Inflammation in the Prediction of Cardiovascular Disease in Women High Medium Low Low Total Cholesterol Medium High High Medium Low Low Total Cholesterol Medium High High Medium Low Low Medium High High Medium Low Low Medium High Total Cholesterol Total Cholesterol NEJM. 2000;342:

14 CRP, IL-6 and the Risk for Developing Type-2 Diabetes in the Women s Health Study Fully adjusted BMI-adjusted Crude Relative Risk IL Relative Risk hs-crp Quartile of IL Quartile of hs-crp Pradhan et al JAMA 2001; 286:327-34
15 CVD Event-Free Survival Probability hscrp, the Metabolic Syndrome, and Future Cardiovascular Events (N = 14,719) ATP III Metabolic Syndrome - No hscrp < hscrp > Years of Follow-Up ATP III Metabolic Syndrome - Yes Circulation 2003;107:391-7
16 Relative Risk of Future CV Events What are the environmental and genetic influences on CRP? < >20 low risk moderate risk high risk Circulation 2004;109: hscrp (mg/l)
17 hscrp and Coronary Heart Disease in a General Population of Japanese The Hisayama Study Arima H., et al, Arterioscler Thromb Vasc Biol. 2008;28:
18 Women s Genome Health Study GWAS for Plasma C-Reactive Protein Level Am J Hum Genet 2008;82:

19 < 1 mg/l 1 to 3 mg/l > 3 mg/l PHS 1997 WHS 2000 UK 2000 MONICA 2004 ARIC 2004 Iceland NHS 2004 HPFUS 2004 EPIC-N 2005 Strong 2005 Kuopio 2005 FHS CHS 2005 PIMA 2005 Fully Adjusted Relative Risk hscrp Adds Prognostic Information Beyond Traditional Risk Factors in All Major Cohorts Evaluated
20 AHA / CDC Scientific Statement Markers of Inflammation and Cardiovascular Disease: Applications to Clinical and Public Health Practice Circulation January 28, 2003 Measurement of hs-crp is an independent marker of risk and may be used at the discretion of the physician as part of global coronary risk assessment in adults without known cardiovascular disease. Weight of evidence favors use particularly among those judged at intermediate risk by global risk assessment. Circulation 2003; 107: CR-20
 in CRP = 1.63 (1.51-1.")
21 Cambridge Meta-Analysis : Emerging Risk Factors Collaboration CRP and risk of coronary heart disease, stroke, and total mortality 160,309 participants without a history of vascular disease, 54 prospective cohort studies, 1.31 million person-years of exposure, 27,769 fatal or nonfatal outcomes Risk ratio per 1-standard deviation increase (x3) in CRP = 1.63 ( ) after adjustment for age and gender, and 1.39 ( ) after additional adjustment for smoking, systolic blood pressure, diabetes, BMI, total cholesterol, HDL-cholesterol, and triglycerides. In these multivariable analyses, the RR for a 1-SD increase in CRP (1.39, ) was of similar magnitude as that of comparable analyses for non-hdlc (1.28, ) and systolic blood pressure (1.35, ). In serial measures obtained among 24,222 participants, the regression-dilution ratio for CRP, adjusted for age and gender, was 0.58 ( ) indicating year-to-year variability similar to that for systolic blood pressure (0.54, ), total cholesterol (0.59, ), and HDLC (0.74, ). Emerging Risk Factors Collaboration, Lancet 2009 (in press) CR-21
22 Cambridge Meta-Analysis : Emerging Risk Factors Collaboration CRP and risk of coronary heart disease, stroke, and total mortality 160,309 participants without a history of vascular disease, 54 prospective cohort studies, 1.31 million person-years of exposure, 27,769 fatal or nonfatal outcomes The current study has demonstrated that CRP levels are as consistent within individuals over several years as are total cholesterol and systolic blood pressure. In an analysis of 160,000 people without initial vascular disease, we have shown that under a wide range of circumstances CRP concentration has broadly loglinear associations with subsequent risk of coronary heart disease, ischemic stroke, and vascular death (and) the magnitude of these effects is comparable to that of other major established risk factors. Emerging Risk Factors Collaboration, Lancet 2009 (in press) CR-22
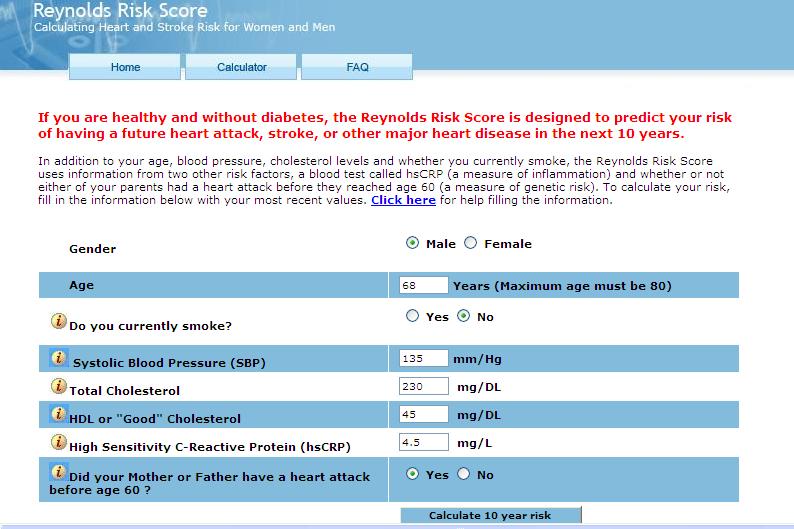
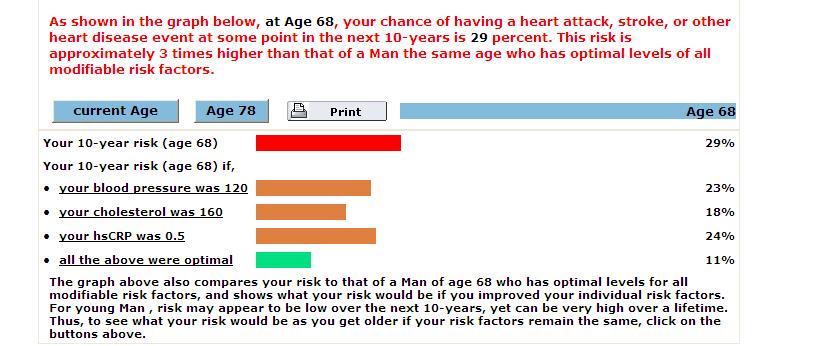
23 Framingham Risk Score Age Blood Pressure Diabetes Smoking Total cholesterol HDL cholesterol Reynolds Risk Score Age Blood Pressure Diabetes Smoking Total cholesterol HDL cholesterol hscrp Parental history of MI JAMA 2007;297:611-9 Circulation 2008
24

25 Reynolds Risk Score Example II Clinical Example: 72 year old non-diabetic woman, smoker, systolic BP 145 mm Hg, TC 216 mg/dl, HDLC 82 mg/dl, hscrp 7.7 mg/l, and a positive family history for MI. Predicted 10-year risk Framingham Covariates: Reynolds Covariates: 6.9 percent 23.2 percent
26 Inflammation, hscrp, and Vascular Prevention Is there evidence that individuals with elevated levels of the inflammatory biomarker hscrp are at high vascular risk even when other risk factors are acceptable? Is there evidence that individuals identified at increased risk due to inflammation benefit from a therapy they otherwise would not have received? Is there evidence that reducing inflammation per se will reduce vascular events? Should our guidelines for vascular disease prevention change?



27 Relative Risk Median hs-crp (mg/dl) Inflammation, Statin Therapy, and hscrp: Initial Observations 3 P Trend = % (P=0.004) 0.24 Placebo Pravastatin Pravastatin Placebo Pravastatin Placebo Inflammation Absent Inflammation Present 0.18 Baseline 5 Years Circulation. 1998;98: Circulation. 1999;100:
28 Cumulative Rate of Recurrent Myocardial Infarction or Coronary Death (percent) Clinical Relevance of Achieved LDL and Achieved CRP After Treatment with Statin Therapy LDLC>70 mg/dl LDLC<70 mg/dl hscrp>2 mg/l hscrp<2 mg/l NEJM 2005;352: Follow-Up (years)
29 Clinical Relevance of Achieved LDL and Achieved CRP After Treatment with Statin Therapy LDL > 70 mg/dl, CRP > 2 mg/l LDL > 70 mg/dl, CRP < 2 mg/l LDL < 70 mg/dl, CRP > 2 mg/l LDL < 70 mg/dl, CRP < 2 mg/l Follow-Up (Years) NEJM 2005;352:20-28.
30 Probability of Event-free Survival Primary Prevention : Whom Should We Treat? hscrp < 2 mg/l, LDL < 130 mg/dl hscrp < 2 mg/l, LDL > 130 mg/dl hscrp > 2 mg/l, LDL < 130 mg/dl 0.96 hscrp > 2 mg/l, LDL > 130 mg/dl Years of Follow-up N Engl J Med. 2002;347:
31 hscrp as a Method to Target Statin Therapy in Primary Prevention: AFCAPS/TexCAPS Study Group Statin Placebo NNT low LDLC / low hscrp low LDLC / high hscrp high LDLC / low hscrp high LDLC / high hscrp N Engl J Med 2001;344: Median LDLC = 150 mg/dl Median CRP = 2 mg/l
")

32 JUPITER Trial Design JUPITER Multi-National Randomized Double Blind Placebo Controlled Trial of Rosuvastatin in the Prevention of Cardiovascular Events Among Individuals With Low LDL and Elevated hscrp No Prior CVD or DM Men >50, Women >60 LDL <130 mg/dl hscrp >2 mg/l 4-week run-in Rosuvastatin 20 mg (N=8901) Placebo (N=8901) MI Stroke Unstable Angina CVD Death CABG/PTCA Argentina, Belgium, Brazil, Bulgaria, Canada, Chile, Colombia, Costa Rica, Denmark, El Salvador, Estonia, Germany, Israel, Mexico, Netherlands, Norway, Panama, Poland, Romania, Russia, South Africa, Switzerland, United Kingdom, Uruguay, United States, Venezuela

33 * JUPITER JUPITER Enrollment Sites 17,802 Patients Argentina Belgium Brazil Bulgaria Canada Chile Colombia Costa Rica Denmark El Salvador Estonia Germany Israel Mexico Netherlands Norway Panama Poland Romania Russia South Africa Switzerland UK USA Uruguay Venezuela
34 JUPITER Baseline Clinical Characteristics Rosuvastatin Placebo (N = 8901) (n = 8901) Age, years (IQR) 66.0 ( ) 66.0 ( ) Female, N (%) 3,426 (38.5) 3,375 (37.9) Ethnicity, N (%) Caucasian 6,358 (71.4) 6,325 (71.1) Black 1,100 (12.4) 1,124 (12.6) Hispanic 1,121 (12.6) 1,140 (12.8) Blood pressure, mm (IQR) Systolic 134 ( ) 134 ( ) Diastolic 80 (75-87) 80 (75-87) Smoker, N (%) 1,400 (15.7) 1,420 (16.0) Family History, N (%) 997 (11.2) 1,048 (11.8) Metabolic Syndrome, N (%) 3,652 (41.0) 3,723 (41.8) Aspirin Use, N (%) 1,481 (16.6) 1,477 (16.6) All values are median (interquartile range) or N (%)
35 JUPITER Baseline Blood Levels (median, interquartile range) Ridker et al NEJM 2008 Rosuvastatin Placebo (N = 8901) (n = 8901) hscrp, mg/l 4.2 ( ) 4.3 ( ) LDL, mg/dl 108 (94-119) 108 (94-119) mmol/l 2.8 ( ) 2.8 ( HDL, mg/dl 49 (40 60) 49 (40 60) mmol/l 1.27 ( ) 1.27 ( ) Triglycerides, mg/l 118 (85-169) 118 (86-169) mmol/l 1.33 ( ) 1.33 ( ) Total Cholesterol, mg/dl 186 ( ) 185 ( ) mmol/l 4.82 ( ) 4.79 ( ) Glucose, mg/dl 94 (87 102) 94 (88 102) mmol/l 5.22 ( ) 5.22 ( ) HbA1c, % 5.7 ( ) 5.7 ( ) All values are median (interquartile range) [ Mean LDL = 104 mg/dl (2.69 mmol/l)]
36 JUPITER Effects of rosuvastatin 20 mg on LDL, HDL, TG, and hscrp LDL (mg/dl) hscrp (mg/l) LDL decrease 50 percent at 12 months TG (mg/dl) HDL (mg/dl) 10 0 HDL increase 4 percent at 12 months hscrp decrease 37 percent at 12 months Months TG decrease 17 percent at 12 months Months
37 JUPITER Additional Aim: Evaluate Long Term Stability of hscrp Among those allocated to placebo and followed over five years, the intraclass correlation coefficient for hscrp repeated every 6 months was 0.56, very similar to that of LDL-C (0.60) and blood pressure (0.59). These data are consistent with multiple prior reports that the month-to-month, year-to-year, and even decade-to-decade variability of hscrp is comparable to that of cholesterol. Glynn et al Clin Chem 2009 CR-37
38 JUPITER Primary Trial Endpoint : MI, Stroke, UA/Revascularization, CV Death Cumulative Incidence HR 0.56, 95% CI P < NEJM 2008;359: Number Needed to Treat (NNT 5 ) = Placebo 251 / % Rosuvastatin 142 / 8901 Number at Risk Rosuvastatin Placebo Follow-up (years) 8,901 8,631 8,412 6,540 3,893 1,958 1, ,901 8,621 8,353 6,508 3,872 1,963 1,
39 JUPITER Fatal or Nonfatal Myocardial Infarction Cumulative Incidence NEJM 2008;359: HR 0.45, 95%CI P < Placebo - 55 % Rosuvastatin Follow-up Years
40 JUPITER Fatal or Nonfatal Stroke Cumulative Incidence NEJM 2008;359: HR 0.52, 95%CI P = Follow-up Years Placebo - 48 % Rosuvastatin
41 JUPITER Arterial Revascularization / Unstable Angina Cumulative Incidence NEJM 2008;359: HR 0.53, 95%CI P < Placebo (N = 143) - 47 % Rosuvastatin (N = 76) Number at Risk Rosuvastatin Placebo Follow-up (years) 8,901 8,640 8,426 6,550 3,905 1,966 1, ,901 8,641 8,390 6,542 3,895 1,977 1,
42 JUPITER Primary Endpoint Subgroup Analysis I NEJM 2008;359: Men Women Age < 65 Age > 65 Smoker Non-Smoker Caucasian Non-Caucasian USA/Canada Rest of World Hypertension No Hypertension All Participants N P for Interaction 11, ,801 8, ,261 2, ,975 12, ,117 6, ,761 10, ,586 17, Rosuvastatin Superior Rosuvastatin Inferior CR-42
43 JUPITER Primary Endpoint Subgroup Analysis II NEJM 2008;359: N P for Interaction Family HX of CHD No Family HX of CHD BMI < 25 kg/m 2 BMI kg/m BMI >30 kg/m Metabolic Syndrome No Metabolic Syndrome Framingham Risk < 10% Framingham Risk > 10% 2 2 2, ,684 4, ,009 6,675 7, ,296 8, ,895 hscrp > 2 mg/l Only 6,375 hscrp > 2 mg/l Only 6,375 All Participants 17, Rosuvastatin Superior Rosuvastatin Inferior CR-43
44 JUPITER Event Reduction at All Levels of Baseline LDLC < 130 mg/dl Baseline Levels N LDLC <100 mg/dl 6,269 LDLC <90 mg/dl 3,687 LDLC <80 mg/dl 2,033 LDLC <70 mg/dl 1,022 LDLC <60 mg/dl 511 All Participants 17, Rosuvastatin Better Rosuvastatin Worse
45 JUPITER Event Reduction at All Levels of Baseline hscrp > 2 mg/l Baseline hscrp N >10 _ mg/l 2,503 >9 _ mg/l >8 _ mg/l >7 _ mg/l >6 _ mg/l >5 _ mg/l >4 _ mg/l >3 _ mg/l >2 _ mg/l 3,071 3,839 4,723 5,897 7,425 9,726 12,939 17, Better Worse CR-45
46 JUPITER Event Reduction at All Levels of Baseline hscrp > 2 mg/l Baseline hscrp N >10 _ mg/l 2,503 >9 _ mg/l >8 _ mg/l >7 _ mg/l >6 _ mg/l >5 _ mg/l >4 _ mg/l >3 _ mg/l >2 _ mg/l 3,071 3,839 4,723 5,897 7,425 9,726 12,939 17, Better Worse Placebo Event Rate CR-46
47 JUPITER Secondary Endpoint All Cause Mortality HR 0.80, 95%CI P= 0.02 Cumulative Incidence NEJM 2008;359: Placebo 247 / % Rosuvastatin 198 / 8901 Number at Risk Rosuvastatin Placebo Follow-up (years) 8,901 8,847 8,787 6,999 4,312 2,268 1,602 1, ,901 8,852 8,775 6,987 4,319 2,295 1,614 1,
48 JUPITER Number Needed to Treat (5 year) Endpoint All Primary Endpoint 25 Primary Endpoint, Mortality 22 MI, Stroke, CABG/PTCA, Death 23 MI, Stroke, Death 31 Benchmarks: Statins for hyperlipidemia 5-year NNT Diuretics 5-year NNT Beta-blockers 5-year NNT Aspirin Men 5-year NNT Aspirin Women 5-year NNT
49 JUPITER Number Needed to Treat (5 year) Endpoint All FRS<10 FRS>10 Primary Endpoint Primary Endpoint, Mortality MI, Stroke, CABG/PTCA, Death MI, Stroke, Death Benchmarks: Statins for hyperlipidemia 5-year NNT Diuretics 5-year NNT Beta-blockers 5-year NNT Aspirin Men 5-year NNT Aspirin Women 5-year NNT
50 Estimated 5-Year NNT Values for the Primary Prevention of Cardiovascular Disease In Middle-Aged Populations


51 Inflammation and Thrombosis Thrombin Resting Endothelial Cell Activated Endothelial Cell Reactive Oxygen Species Resting Platelet Tissue Factor Procoagulant Resting Smooth Muscle Cell Activated Degranulating Platelet Activated Macrophage Pro-inflammatory Cytokines Proliferating Modulated Smooth Muscle Cell Pro-inflammatory Mediators (e.g., CD40L, RANTES, IL-6) Lipid mediators Of inflammation Croce K, Libby P. Intertwining of thrombosis and inflammation in atherosclerosis. Curr Opin Hematol. 2007;14:55-61

52 Venous Endothelium- transmission electron micrograph
53 JUPITER Total Venous Thromboembolism Cumulative Incidence HR 0.57, 95%CI P= Placebo 60 / % Rosuvastatin 34 / 8901 Number at Risk Rosuvastatin Placebo Follow-up (years) 8,901 8,648 8,447 6,575 3,927 1,986 1,376 1, ,901 8,652 8,417 6,574 3,943 2,012 1,
54 JUPITER Venous Thromboembolism Unprovoked vs Provoked Cumulative Incidence Cumulative Incidence Unprovoked Venous Thromboembolism Provoked Venous Thromboembolism HR 0.61, 95% CI P= Follow-up (years) Placebo Rosuvastatin HR 0.52, 95% CI P= Follow-up (years) Placebo Rosuvastatin Clear clinical benefit in the absence of any bleeding hazard (hemmorrhagic events : rosuvastatin 258, placebo 275, P=0.45)
55 JUPITER VTE + Primary Trial Endpoint + Total Mortality Cumulative Incidence HR 0.66, 95% CI P < Number Needed to Treat (NNT 5 ) = Placebo 483 / Fewer Events Rosuvastatin 320 / 8901 Number at Risk Rosuvastatin Placebo Follow-up (years) 8,901 8,624 8,400 6,525 3,880 1,951 1, ,901 8,612 8,338 6,486 3,854 1,949 1,
56 Inflammation, hscrp, and Vascular Prevention Is there evidence that individuals with elevated levels of the inflammatory biomarker hscrp are at high vascular risk even when other risk factors are acceptable? Is there evidence that individuals identified at increased risk due to inflammation benefit from a therapy they otherwise would not have received? Is there evidence that reducing inflammation per se will reduce vascular events? Should our guidelines for vascular disease prevention change?
57 JUPITER Achieved LDLC, Achieved hscrp, or Both? Is the benefit observed in the JUPITER trial associated with achieving a low level of LDLC, a low level of hscrp or both? Do we need to achieve the dual targets of low LDLC and low hscrp in order to maximize the benefit of statin therapy?
58 JUPITER Predicted vs Observed Benefit Based on Absolute LDL Reduction Proportional reduction in vascular event rate (95% CI) CTT JUPITER PREDICTED 20 TNT A-to-Z IDEAL PROVE-IT Mean LDL cholesterol difference between treatment groups (mmol/l)
59 JUPITER Predicted vs Observed Benefit Based on Absolute LDL Reduction Proportional reduction in vascular event rate (95% CI) JUPITER OBSERVED CTT JUPITER PREDICTED 20 TNT A-to-Z IDEAL PROVE-IT Mean LDL cholesterol difference between treatment groups (mmol/l)
60 JUPITER LDL reduction, hscrp reduction, or both? Lancet 2009;373: N Rate Placebo LDL>70mg/dL,hsCRP>2 mg/l LDL<70mg/dL,hsCRP>2 mg/l LDL>70mg/dL,hsCRP<2 mg/l LDL<70mg/dL,hsCRP<2 mg/l P < Placebo LDL>70mg/dL,hsCRP>1 mg/l LDL<70mg/dL,hsCRP>1 mg/l LDL>70mg/dL,hsCRP<1 mg/l LDL<70mg/dL,hsCRP<1 mg/l Full Adjusted Hazard Ratio 0.21, 95% CI , P < Rosuvastatin Better P < Rosuvastatin Worse
61 Clinical Importance of Achieving LDL-C < 70 mg/dl and hscrp < 2 mg/l Following Initiation of Statin Therapy LDL>70, hscrp>2 LDL<70, hscrp>2 LDL>70, hscrp<2 LDL<70, hscrp< Follow-up (days) PROVE IT TIMI 22 NEJM 2005;352: Follow-up (days) A to Z Circulation 2006;114:281-8
62 Can targeted Anti-Inflammatory Therapy Reduce Cardiovascular Risk? Aspirin / Statins Direct CRP inhibitors DMARDs/ MTX TNF / IL-6 Inhibitors IL-1 receptor antagonism 5-LO Inhibitors Leukotriene blockade CCR2/CCR5 Lp-PLA2 inhibition spla inhibition RNAi / anti-sense Immunization strategies

63
64 What is the impact of methotrexate, infliximab, and tocilizumab on lipid levels? TC Statins MTX Infliximab tocilizumab LDL HDL TG Chylo CRP
65 Methotrexate and Mortality in Patients with Rheumatoid Arthritis: Wichita Arthritis Study All Cause Mortality Cardiovascular Mortality Non-Cardiovascular Mortality Methotrexate Superior No DMARD Superior Choi et al, Lancet 2002;359:
66 LDM and CVD: Observational Evidence Cohort Group HR * (95 % CI) Endpoint Exposure Wichita RA 0.4 ( ) Total Mortality LDM Choi ( ) CV Mortality LDM 0.4 ( ) CV Mortality LDM < 15 mg/wk Netherlands RA 0.3 ( ) CVD LDM only van Helm ( ) CVD LDM + SSZ 0.2 ( ) CVD LDM + HCQ 0.2 ( ) CVD LDM + SSZ + HCQ Miami VA PsA 0.7 ( ) CVD LDM Pradanovich ( ) CVD LDM < 15 mg/wk RA 0.8 ( ) CVD LDM 0.6 ( ) CVD LDM < 15 mg/wk CORRONA RA 0.6 ( ) CVD LDM Solomon ( ) CVD TNF-inhibitor QUEST-RA RA 0.85 ( ) CVD LDM Narango ( ) MI LDM 0.89 ( ) Stroke LDM UK Norfolk RA, PsA 0.6 ( ) Total Mortality LDM ( ) CV Mortality LDM
67 Cardiovascular Inflammation Reduction Trial (CIRT) Stable CAD (post MI) On Statin, ACE/ARB, BB, ASA Persistent Elevation of hscrp (> 2 mg/l) Open Label Active Run-In VLDM 10 mg/wk Randomized VLDM 10 mg/wk + folate Randomized Placebo mg/wk + folate N = 3,500 N = 3,500 25% RRR, 3.0 year median f/u Nonfatal MI, Nonfatal Stroke, Cardiovascular Death
68 Inflammation, hscrp, and Vascular Prevention Is there evidence that individuals with elevated levels of the inflammatory biomarker hscrp are at high vascular risk even when other risk factors are acceptable? Is there evidence that individuals identified at increased risk due to inflammation benefit from a therapy they otherwise would not have received? Is there evidence that reducing inflammation per se will reduce vascular events? Should our guidelines for vascular disease prevention change?
69 WOSCOPS, AFCAPS, MEGA, ASCOT, JUPITER Can we use evidence to simplify guidelines for primary prevention? 1. Strong recommendations for diet, exercise, and smoking cessation for any patient with or at risk for cardiovascular disease. 2. If the patient is diabetic or has a very strong family history of premature atherothrombosis, strongly consider treatment with a statin if RRS or FRS > 5 % 3. If LDLC > 160, TC:HDLC > 5, or hscrp > 2, strongly consider treatment with a statin if RRS or FRS > 5 % 4. Beyond these recommendations, referral to lipid specialist or cardiologist for further evaluation.
70 2009 Canadian Cardiovascular Society (CCS) Guidelines for the Diagnosis and Treatment of Dyslipidemia and Prevention of Cardiovascular Disease in the Adult Primary Goal : LDLC High CAD, CVA, PVD <2mmol/L or 50% reduction Class I Most pts with Diabetes Level A FRS > 20 % RRS > 20 % Moderate FRS % <2mmol/L or 50 % reduction Class IIA RRS % Level A LDL > 3.5 mmol/l TC/HDLC > 5.0 hscrp > 2 in men >50 yr women > 60 yr Low FRS < 10 % <5mmol/L Class IIA Level A Secondary Targets : TC/HDLC < 4, non HDLC < 3.5 mol/l, hscrp < 2 mg/l, TG < 1.7 mol/l, ApoB/A<0.8 CR-75
71 JUPITER Primary Endpoint in Intermediate Risk Groups with hscrp >2 mg/l FRS (%) Rosuvastatin Placebo HR (95%CI) 5 10 % 32 (0.50) 59 (0.92) 0.55 ( ) % 74 (0.95) 145 (1.84) 0.51 ( ) None of these patients are currently eligible to receive statin therapy because, using traditional risk factors alone and calculating Framingham 10-year risk, they are less than 20 % AND they already have untreated LDL-C levels below the treatment target in primary prevention (ie < 130 mg/dl). However, they ALL have hscrp > 2 mg/l. CR-76
72 JUPITER Public Health Implications Exercise, diet, and smoking cessation remain the first interventions for those with elevated LDLC or hscrp. However, application of the simple screening and treatment strategy tested in the JUPITER trial over a five-year period could conservatively prevent more than 250,000 heart attacks, strokes, revascularization procedures, and cardiovascular deaths in the United States alone. Simplified guidelines that advocate combined lifestyle and pharmacologic therapy in those groups where trial evidence clearly supports a net benefit have the potential to greatly improve patient care and public health. With thanks to the 17,802 patients and the >1,000 physicians worldwide for their effort and commitment to the JUPITER trial program.
John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam
 Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Latest Insights from the JUPITER Study John J.P. Kastelein MD PhD Professor of Medicine Dept. of Vascular Medicine Academic Medial Center / University of Amsterdam Inflammation, hscrp, and Vascular Prevention
Therapeutic Implications of Vascular Inflammation: The Cardiovascular Inflammation Reduction Trials
 Therapeutic Implications of Vascular Inflammation: The Cardiovascular Inflammation Reduction Trials ESC Munich August 25, 2012 Paul M Ridker, MD Eugene Braunwald Professor of Medicine Harvard Medical School
Therapeutic Implications of Vascular Inflammation: The Cardiovascular Inflammation Reduction Trials ESC Munich August 25, 2012 Paul M Ridker, MD Eugene Braunwald Professor of Medicine Harvard Medical School
JUPITER NEJM Poll. Panel Discussion: Literature that Should Have an Impact on our Practice: The JUPITER Study
 Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Panel Discussion: Literature that Should Have an Impact on our Practice: The Study Kaiser COAST 11 th Annual Conference Maui, August 2009 Robert Blumberg, MD, FACC Ralph Brindis, MD, MPH, FACC Primary
Inflammation as A Target for Therapy. Focus on Residual Inflammatory Risk
 ESC Rome Monday August 29, 2016 Inflammation as A Target for Therapy Focus on Residual Inflammatory Risk Paul M Ridker, MD Eugene Braunwald Professor of Medicine Harvard Medical School Director, Center
ESC Rome Monday August 29, 2016 Inflammation as A Target for Therapy Focus on Residual Inflammatory Risk Paul M Ridker, MD Eugene Braunwald Professor of Medicine Harvard Medical School Director, Center
Expert Meeting on Large Simple Trials (LST s)
") Expert Meeting on Large Simple Trials (LST s) Clinical Trials Transformation Initiative Justification for the Use of statins in Prevention: an Intervention Trial Evaluating Rosuvastatin JUPITER Johannes
Expert Meeting on Large Simple Trials (LST s) Clinical Trials Transformation Initiative Justification for the Use of statins in Prevention: an Intervention Trial Evaluating Rosuvastatin JUPITER Johannes
Inflammation and and Heart Heart Disease in Women Inflammation and Heart Disease
 Inflammation and Heart Disease in Women Inflammation and Heart Disease What is the link between een inflammation and atherosclerotic disease? What is the role of biomarkers in predicting cardiovascular
Inflammation and Heart Disease in Women Inflammation and Heart Disease What is the link between een inflammation and atherosclerotic disease? What is the role of biomarkers in predicting cardiovascular
Reducing Inflammation to Reduce Cardiovascular Risk: The Canakinumab Anti-inflammatory Thrombosis Outcomes Study (CANTOS)
") New York City Cardiovascular Symposium December 10, 2017 Reducing Inflammation to Reduce Cardiovascular Risk: The Canakinumab Anti-inflammatory Thrombosis Outcomes Study (CANTOS) Paul M Ridker, MD, MPH
New York City Cardiovascular Symposium December 10, 2017 Reducing Inflammation to Reduce Cardiovascular Risk: The Canakinumab Anti-inflammatory Thrombosis Outcomes Study (CANTOS) Paul M Ridker, MD, MPH
Experiences with interim trial monitoring, particularly with early stopped trials
 Experiences with interim trial monitoring, particularly with early stopped trials 1 Robert J Glynn, ScD Divisions of Preventive Medicine and Pharmacoepidemiology & Pharmacoeconomics, Brigham & Women s
Experiences with interim trial monitoring, particularly with early stopped trials 1 Robert J Glynn, ScD Divisions of Preventive Medicine and Pharmacoepidemiology & Pharmacoeconomics, Brigham & Women s
Beyond Framingham: Risk Assessment & Treatment for Primary Prevention
 Beyond Framingham: Risk Assessment & Treatment for Primary Prevention Ronald M. Goldenberg, MD, FRCPC, FACE Consultant Endocrinologist, North York General Hospital Medical Co-Director, LMC Endocrinology
Beyond Framingham: Risk Assessment & Treatment for Primary Prevention Ronald M. Goldenberg, MD, FRCPC, FACE Consultant Endocrinologist, North York General Hospital Medical Co-Director, LMC Endocrinology
New evidences in heart failure: the GISSI-HF trial. Aldo P Maggioni, MD ANMCO Research Center Firenze, Italy
 New evidences in heart failure: the GISSI-HF trial Aldo P Maggioni, MD ANMCO Research Center Firenze, Italy % Improving survival in chronic HF and LV systolic dysfunction: 1 year all-cause mortality 20
New evidences in heart failure: the GISSI-HF trial Aldo P Maggioni, MD ANMCO Research Center Firenze, Italy % Improving survival in chronic HF and LV systolic dysfunction: 1 year all-cause mortality 20
Subodh Verma, MD PhD FRCSC
 CIRT and CANTOS Targeting g Inflammation at in Atherosclerosis e s Subodh Verma, MD PhD FRCSC Cardiac Surgeon, St. Michael s Hospital Associate Professor, Surgery & Pharmacology Canada Research Chair in
CIRT and CANTOS Targeting g Inflammation at in Atherosclerosis e s Subodh Verma, MD PhD FRCSC Cardiac Surgeon, St. Michael s Hospital Associate Professor, Surgery & Pharmacology Canada Research Chair in
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009
 The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
The JUPITER trial: What does it tell us? Alice Y.Y. Cheng, MD, FRCPC January 24, 2009 Learning Objectives 1. Understand the role of statin therapy in the primary and secondary prevention of stroke 2. Explain
Keynote: Inflammation and Cardiovascular Risk: Emerging Complications for Clinical Practice
 Keynote: Inflammation and Cardiovascular Risk: Emerging Complications for Clinical Practice Dallas, TX December, 8 7: AM 8: AM Session 9: Keynote: Inflammation and Cardiovascular Risk: Emerging Implications
Keynote: Inflammation and Cardiovascular Risk: Emerging Complications for Clinical Practice Dallas, TX December, 8 7: AM 8: AM Session 9: Keynote: Inflammation and Cardiovascular Risk: Emerging Implications
Canakinumab Anti-Inflammatory Thrombosis Outcomes Study (CANTOS)
") Canakinumab Anti-Inflammatory Thrombosis Outcomes Study (CANTOS) Stable CAD (post MI) On Statin, ACE/ARB, BB, ASA Persistent Elevation of hscrp (> 2 mg/l) N = 10,061 39 Countries April 2011 - June 2017
Canakinumab Anti-Inflammatory Thrombosis Outcomes Study (CANTOS) Stable CAD (post MI) On Statin, ACE/ARB, BB, ASA Persistent Elevation of hscrp (> 2 mg/l) N = 10,061 39 Countries April 2011 - June 2017
Treatment of Cardiovascular Risk Factors. Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center
 Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
Treatment of Cardiovascular Risk Factors Kevin M Hayes D.O. F.A.C.C. First Coast Heart and Vascular Center Disclosures: None Objectives What do risk factors tell us What to check and when Does treatment
ATP IV: Predicting Guideline Updates
 Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Disclosures ATP IV: Predicting Guideline Updates Daniel M. Riche, Pharm.D., BCPS, CDE Speaker s Bureau Merck Janssen Boehringer-Ingelheim Learning Objectives Describe at least two evidence-based recommendations
Assessing Cardiovascular Risk to Optimally Stratify Low- and Moderate- Risk Patients. Copyright. Not for Sale or Commercial Distribution
 CLINICAL Viewpoint Assessing Cardiovascular Risk to Optimally Stratify Low- and Moderate- Risk Patients Copyright Not for Sale or Commercial Distribution By Ruth McPherson, MD, PhD, FRCPC Unauthorised
CLINICAL Viewpoint Assessing Cardiovascular Risk to Optimally Stratify Low- and Moderate- Risk Patients Copyright Not for Sale or Commercial Distribution By Ruth McPherson, MD, PhD, FRCPC Unauthorised
Inflammation and Atherothrombosis: Where have we been? Where Are We Going? Why Perform the CIRT and CANTOS Trials?
 Inflammation and Atherothrombosis: Where have we been? Where Are We Going? Why Perform the CIRT and CANTOS Trials? Paul M Ridker, MD Eugene Braunwald Professor of Medicine Harvard Medical School Director,
Inflammation and Atherothrombosis: Where have we been? Where Are We Going? Why Perform the CIRT and CANTOS Trials? Paul M Ridker, MD Eugene Braunwald Professor of Medicine Harvard Medical School Director,
Review of guidelines for management of dyslipidemia in diabetic patients
 2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
2012 international Conference on Diabetes and metabolism (ICDM) Review of guidelines for management of dyslipidemia in diabetic patients Nan Hee Kim, MD, PhD Department of Internal Medicine, Korea University
Inflammation, the Inflammasome and CAD Do Cardiologists need to know this? Jacques Genest MD
 Inflammation, the Inflammasome and CAD Do Cardiologists need to know this? Jacques Genest MD Cardiovascular Research Laboratories Research Institute of the McGill University Health Center Disclosure J.
Inflammation, the Inflammasome and CAD Do Cardiologists need to know this? Jacques Genest MD Cardiovascular Research Laboratories Research Institute of the McGill University Health Center Disclosure J.
Hyperlipidemia: Lowering the Bar on the Lipid Limbo. Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH
 Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
Mark slides Hyperlipidemia: Lowering the Bar on the Lipid Limbo Community Faculty Development Symposium March 13, 2004 Hugh Huizenga MD, MPH Hyperlipidemia is a common problem Nearly 50% of men in the
The Clinical Unmet need in the patient with Diabetes and ACS
 The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
The Clinical Unmet need in the patient with Diabetes and ACS Professor Kausik Ray (UK) BSc(hons), MBChB, MD, MPhil, FRCP (lon), FRCP (ed), FACC, FESC, FAHA Diabetes is a global public health challenge
Dyslipidaemia. Is there any new information? Dr. A.R.M. Saifuddin Ekram
 Dyslipidaemia Is there any new information? Dr. A.R.M. Saifuddin Ekram PhD,FACP,FCPS(Medicine) Professor(c.c.) & Head Department of Medicine Rajshahi Medical College Rajshahi-6000 New features of ATP III
Dyslipidaemia Is there any new information? Dr. A.R.M. Saifuddin Ekram PhD,FACP,FCPS(Medicine) Professor(c.c.) & Head Department of Medicine Rajshahi Medical College Rajshahi-6000 New features of ATP III
Do Women Benefit From Statins for Primary Prevention?: Controversy, Challenges and Consensus
 Do Women Benefit From Statins for Primary Prevention?: Controversy, Challenges and Consensus C. Noel Bairey Merz MD, FACC, FAHA Professor and Women s Guild Endowed Chair Director, Barbra Streisand Women
Do Women Benefit From Statins for Primary Prevention?: Controversy, Challenges and Consensus C. Noel Bairey Merz MD, FACC, FAHA Professor and Women s Guild Endowed Chair Director, Barbra Streisand Women
Dyslipidemia in the light of Current Guidelines - Do we change our Practice?
 Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
Dyslipidemia in the light of Current Guidelines - Do we change our Practice? Dato Dr. David Chew Soon Ping Senior Consultant Cardiologist Institut Jantung Negara Atherosclerotic Cardiovascular Disease
9/29/2015. Primary Prevention of Heart Disease: Objectives. Objectives. What works? What doesn t?
 Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
Primary Prevention of Heart Disease: What works? What doesn t? Samia Mora, MD, MHS Associate Professor, Harvard Medical School Associate Physician, Brigham and Women s Hospital October 2, 2015 Financial
This work is licensed under a Creative Commons Attribution-Noncommercial-Share Alike 3.0 License.
 University of Massachusetts Medical School escholarship@umms UMass Center for Clinical and Translational Science Research Retreat 2013 UMass Center for Clinical and Translational Science Research Retreat
University of Massachusetts Medical School escholarship@umms UMass Center for Clinical and Translational Science Research Retreat 2013 UMass Center for Clinical and Translational Science Research Retreat
How would you manage Ms. Gold
 How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
How would you manage Ms. Gold 32 yo Asian woman with dyslipidemia Current medications: Simvastatin 20mg QD Most recent lipid profile: TC = 246, TG = 100, LDL = 176, HDL = 50 What about Mr. Williams? 56
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline?
 What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
What have We Learned in Dyslipidemia Management Since the Publication of the 2013 ACC/AHA Guideline? Salim S. Virani, MD, PhD, FACC, FAHA Associate Professor, Section of Cardiovascular Research Baylor
Genetics of Arterial and Venous Thrombosis: Clinical Aspects and a Look to the Future
 Genetics of Arterial and Venous Thrombosis: Clinical Aspects and a Look to the Future Paul M Ridker, MD Eugene Braunwald Professor of Medicine Harvard Medical School Director, Center for Cardiovascular
Genetics of Arterial and Venous Thrombosis: Clinical Aspects and a Look to the Future Paul M Ridker, MD Eugene Braunwald Professor of Medicine Harvard Medical School Director, Center for Cardiovascular
Disclosures. Objectives. Cardiovascular Risk. Patient Case. JUPITER: The final frontier in statin utilization or an idea from outer space?
 Disclosures JUPITER: The final frontier in statin utilization or an idea from outer space? Kathy E. Komperda, PharmD, BCPS Midwestern University Chicago College of Pharmacy kkompe@midwestern.edu 4/25/09
Disclosures JUPITER: The final frontier in statin utilization or an idea from outer space? Kathy E. Komperda, PharmD, BCPS Midwestern University Chicago College of Pharmacy kkompe@midwestern.edu 4/25/09
Case Presentation. Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer
 Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Case Presentation Rafael Bitzur The Bert W Strassburger Lipid Center Sheba Medical Center Tel Hashomer Case Presentation 50 YO man NSTEMI treated with PCI 1 month ago Medical History: Obesity: BMI 32,
Fasting or non fasting?
 Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Vascular harmony Robert Chilton Professor of Medicine University of Texas Health Science Center Director of Cardiac Catheterization labs Director of clinical proteomics Which is best to measure Lower continues
Val-MARC: Valsartan-Managing Blood Pressure Aggressively and Evaluating Reductions in hs-crp
 Página 1 de 5 Return to Medscape coverage of: American Society of Hypertension 21st Annual Scientific Meeting and Exposition Val-MARC: Valsartan-Managing Blood Pressure Aggressively and Evaluating Reductions
Página 1 de 5 Return to Medscape coverage of: American Society of Hypertension 21st Annual Scientific Meeting and Exposition Val-MARC: Valsartan-Managing Blood Pressure Aggressively and Evaluating Reductions
LDL cholesterol and cardiovascular outcomes?
 LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
LDL cholesterol and cardiovascular outcomes? Prof Kausik Ray, BSc (hons), MBChB, FRCP, MD, MPhil (Cantab), FACC, FESC Professor of Cardiovascular Disease Prevention St Georges University of London Honorary
Environmental. Vascular / Tissue. Metabolics
 Global Risk Reduction--WINS Picking Mom and Dad-2016 Environmental Vascular / Tissue Metabolics Stop smoking-1b Physical activity-1b Weight control-1b Chelation therapy-3c Influenza vaccination-1b Blood
Global Risk Reduction--WINS Picking Mom and Dad-2016 Environmental Vascular / Tissue Metabolics Stop smoking-1b Physical activity-1b Weight control-1b Chelation therapy-3c Influenza vaccination-1b Blood
Preventing Cardiovascular Disease With Lipid Management: Matching Therapy to Risk
 PREVENTING CARDIOVASCULAR DISEASE WITH LIPID MANAGEMENT : MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict
PREVENTING CARDIOVASCULAR DISEASE WITH LIPID MANAGEMENT : MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
How to Reduce Residual Risk in Primary Prevention
 How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
How to Reduce Residual Risk in Primary Prevention Helene Glassberg, MD Assistant Professor of Medicine Section of Cardiology Hospital of the University of Pennsylvania Philadelphia, PA USA Patients with
STABILITY Stabilization of Atherosclerotic plaque By Initiation of darapladib TherapY. Harvey D White on behalf of The STABILITY Investigators
 STABILITY Stabilization of Atherosclerotic plaque By Initiation of darapladib TherapY Harvey D White on behalf of The STABILITY Investigators Lipoprotein- associated Phospholipase A 2 (Lp-PLA 2 ) activity:
STABILITY Stabilization of Atherosclerotic plaque By Initiation of darapladib TherapY Harvey D White on behalf of The STABILITY Investigators Lipoprotein- associated Phospholipase A 2 (Lp-PLA 2 ) activity:
Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence
 Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence Karen E. Aspry, M.D., M.S., ABCL, FACC Assistant Professor of Medicine (Clinical) Alpert Medical School of Brown University
Statins for Cardiovascular Disease Prevention in Women: Review of the Evidence Karen E. Aspry, M.D., M.S., ABCL, FACC Assistant Professor of Medicine (Clinical) Alpert Medical School of Brown University
Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes?
 Late Breaking Clinical Trial Session at AHA 2017 Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes? The REAL-CAD Study in 13,054 Patients With Stable Coronary Artery Disease Takeshi
Late Breaking Clinical Trial Session at AHA 2017 Does High-Intensity Pitavastatin Therapy Further Improve Clinical Outcomes? The REAL-CAD Study in 13,054 Patients With Stable Coronary Artery Disease Takeshi
journal of medicine The new england Rosuvastatin to Prevent Vascular Events in Men and Women with Elevated C-Reactive Protein Abstract
 The new england journal of medicine established in 1812 november 20, 2008 vol. 359 no. 21 to Prevent Vascular Events in Men and Women with Elevated C-Reactive Protein Paul M Ridker, M.D., Eleanor Danielson,
The new england journal of medicine established in 1812 november 20, 2008 vol. 359 no. 21 to Prevent Vascular Events in Men and Women with Elevated C-Reactive Protein Paul M Ridker, M.D., Eleanor Danielson,
The Framingham Coronary Heart Disease Risk Score
 Plasma Concentration of C-Reactive Protein and the Calculated Framingham Coronary Heart Disease Risk Score Michelle A. Albert, MD, MPH; Robert J. Glynn, PhD; Paul M Ridker, MD, MPH Background Although
Plasma Concentration of C-Reactive Protein and the Calculated Framingham Coronary Heart Disease Risk Score Michelle A. Albert, MD, MPH; Robert J. Glynn, PhD; Paul M Ridker, MD, MPH Background Although
The Clinical Debates
 The Clinical Debates Speakers: Round 2: Statins for Primary Prevention of Cardiovascular Disease Matthew Cantrell, PharmD, BCPS, is a 2000 graduate of Mt. Mercy College and 2005 graduate from the University
The Clinical Debates Speakers: Round 2: Statins for Primary Prevention of Cardiovascular Disease Matthew Cantrell, PharmD, BCPS, is a 2000 graduate of Mt. Mercy College and 2005 graduate from the University
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway
 Terje R.Pedersen Oslo University Hospital Oslo, Norway") Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
Should we prescribe aspirin and statins to all subjects over 65? (Or even all over 55?) Terje R.Pedersen Oslo University Hospital Oslo, Norway The Polypill A strategy to reduce cardiovascular disease by
4/7/ The stats on heart disease. + Deaths & Age-Adjusted Death Rates for
 + Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
+ Update on Lipid Management Stacey Gardiner, MD Assistant Professor Division of Cardiovascular Medicine Medical College of Wisconsin + The stats on heart disease Over the past 10 years for which statistics
Landmark Clinical Trials.
 Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Landmark Clinical Trials 1 Learning Objectives Discuss clinical trials and their role in lipid and lipoprotein treatment in cardiovascular prevention. Review the clinical trials of lipid-altering drug
Ischemic Heart and Cerebrovascular Disease. Harold E. Lebovitz, MD, FACE Kathmandu November 2010
 Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
Ischemic Heart and Cerebrovascular Disease Harold E. Lebovitz, MD, FACE Kathmandu November 2010 Relationships Between Diabetes and Ischemic Heart Disease Risk of Cardiovascular Disease in Different Categories
CVD risk assessment using risk scores in primary and secondary prevention
 CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
CVD risk assessment using risk scores in primary and secondary prevention Raul D. Santos MD, PhD Heart Institute-InCor University of Sao Paulo Brazil Disclosure Honoraria for consulting and speaker activities
No relevant financial relationships
 MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
MANAGEMENT OF LIPID DISORDERS Balancing Benefits and harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial relationships baron@medicine.ucsf.edu
1. Which one of the following patients does not need to be screened for hyperlipidemia:
 Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
Questions: 1. Which one of the following patients does not need to be screened for hyperlipidemia: a) Diabetes mellitus b) Hypertension c) Family history of premature coronary disease (first degree relatives:
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough?
 New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
New ACC/AHA Guidelines on Lipids: Are PCSK9 Inhibitors Poised for a Breakthrough? Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of North Carolina at Chapel Hill Immediate
Should we treat everybody over 60 years with a statin? Comprehensive primary prevention in practice
 Should we treat everybody over 60 years with a statin? Comprehensive primary prevention in practice Pathogenesis of atherosclerosis A decades-long disease course Inflammation Selectins ICAM IL M-CSF CRP
Should we treat everybody over 60 years with a statin? Comprehensive primary prevention in practice Pathogenesis of atherosclerosis A decades-long disease course Inflammation Selectins ICAM IL M-CSF CRP
Eugene Barrett M.D., Ph.D. University of Virginia 6/18/2007. Diagnosis and what is it Glucose Tolerance Categories FPG
 Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Diabetes Mellitus: Update 7 What is the unifying basis of this vascular disease? Eugene J. Barrett, MD, PhD Professor of Internal Medicine and Pediatrics Director, Diabetes Center and GCRC Health System
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
The 10 th International & 15 th National Congress on Quality Improvement in Clinical Laboratories
 The 10 th International & 15 th National Congress on Quality Improvement in Clinical Laboratories Cardiac biomarkers in atherosclerosis Najma Asadi MD-APCP Ross and Colleagues in 1973: Response to Injury
The 10 th International & 15 th National Congress on Quality Improvement in Clinical Laboratories Cardiac biomarkers in atherosclerosis Najma Asadi MD-APCP Ross and Colleagues in 1973: Response to Injury
ROLE OF INFLAMMATION IN HYPERTENSION. Dr Barasa FA Physician Cardiologist Eldoret
 ROLE OF INFLAMMATION IN HYPERTENSION Dr Barasa FA Physician Cardiologist Eldoret Outline Inflammation in CVDs the evidence Basic Science in Cardiovascular inflammation: The Main players Inflammation as
ROLE OF INFLAMMATION IN HYPERTENSION Dr Barasa FA Physician Cardiologist Eldoret Outline Inflammation in CVDs the evidence Basic Science in Cardiovascular inflammation: The Main players Inflammation as
Lessons from Recent Atherosclerosis Trials
 Lessons from Recent Atherosclerosis Trials Han, Ki Hoon MD PhD Asan Medical Center Seoul, Korea Change of concept Primary vs. secondary prevention Low risk vs. High risk High Risk CHD and equivalents CHD
Lessons from Recent Atherosclerosis Trials Han, Ki Hoon MD PhD Asan Medical Center Seoul, Korea Change of concept Primary vs. secondary prevention Low risk vs. High risk High Risk CHD and equivalents CHD
Dyslipidemia in women: Who should be treated and how?
 Dyslipidemia in women: Who should be treated and how? Lale Tokgozoglu, MD, FACC, FESC Professor of Cardiology Hacettepe University Faculty of Medicine Ankara, Turkey. Cause of Death in Women: European
Dyslipidemia in women: Who should be treated and how? Lale Tokgozoglu, MD, FACC, FESC Professor of Cardiology Hacettepe University Faculty of Medicine Ankara, Turkey. Cause of Death in Women: European
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines
 Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
Update on Lipid Management in Cardiovascular Disease: How to Understand and Implement the New ACC/AHA Guidelines Paul Mahoney, MD Sentara Cardiology Specialists Lipid Management in Cardiovascular Disease
The Metabolic Syndrome: Is It A Valid Concept? YES
 The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
The Metabolic Syndrome: Is It A Valid Concept? YES Congress on Diabetes and Cardiometabolic Health Boston, MA April 23, 2013 Edward S Horton, MD Joslin Diabetes Center Harvard Medical School Boston, MA
Sanjay Kaul, MD, FACC, FAHA Division of Cardiology Cedars-Sinai Medical Center Los Angeles, California
 Targeting Inflammation in Atherosclerosis: Has CANTOS Nailed It? Controversies and Advances in the Treatment of Cardiovascular Disease The Seventeenth in the Series Beverly Hills, November 16, 2017 Sanjay
Targeting Inflammation in Atherosclerosis: Has CANTOS Nailed It? Controversies and Advances in the Treatment of Cardiovascular Disease The Seventeenth in the Series Beverly Hills, November 16, 2017 Sanjay
Placebo-Controlled Statin Trials EXPLAINING THE DECREASE IN DEATHS FROM CHD! PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN EXPLAINING THE DECREASE IN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Lipid is evolving. Dyslipidemia Vascular disease. Statin. Beyond 관동의대제일병원 내과박정배
 Lipid is evolving Dyslipidemia Vascular disease Statin Beyond 관동의대제일병원 내과박정배 A Dyslipidemia 와혈관질환, 그연결고리는? & 약 80% 가 체내에서생성 약 20% 가 음식물에서흡수 Quantity of cholesterol in the body Bile acids 배설 동맥경화증의위험요인
Lipid is evolving Dyslipidemia Vascular disease Statin Beyond 관동의대제일병원 내과박정배 A Dyslipidemia 와혈관질환, 그연결고리는? & 약 80% 가 체내에서생성 약 20% 가 음식물에서흡수 Quantity of cholesterol in the body Bile acids 배설 동맥경화증의위험요인
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest EXPLAINING THE DECREASE
Introduction. Objective. Critical Questions Addressed
 Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Introduction Objective To provide a strong evidence-based foundation for the treatment of cholesterol for the primary and secondary prevention of ASCVD in women and men Critical Questions Addressed CQ1:
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
MANAGEMENT OF HYPERLIPIDEMIA AND CARDIOVASCULAR RISK IN WOMEN: Balancing Benefits and Harms Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Decline in CV-Mortality
 Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Lipids id 2013 What s Changed? Christopher Granger, MD Disclosure Research contracts: AstraZeneca, GSK, Merck, Sanofi- Aventis, BMS, Pfizer, The Medicines Company, Medtronic Foundation, and Boehringer
Andrew Cohen, MD and Neil S. Skolnik, MD INTRODUCTION
 2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
2 Hyperlipidemia Andrew Cohen, MD and Neil S. Skolnik, MD CONTENTS INTRODUCTION RISK CATEGORIES AND TARGET LDL-CHOLESTEROL TREATMENT OF LDL-CHOLESTEROL SPECIAL CONSIDERATIONS OLDER AND YOUNGER ADULTS ADDITIONAL
Joslin Diabetes Center Advances in Diabetes and Thyroid Disease 2013 Consensus and Controversy in Diabetic Dyslipidemia
 Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
Consensus and Controversy in Diabetes and Dyslipidemia Om P. Ganda MD Director, Lipid Clinic Joslin diabetes Center Boston, MA, USA CVD Outcomes in DM vs non- DM 102 Prospective studies; 698, 782 people,
Welcome! Mark May 14, Sat!
 Welcome! Mark May 14, Sat! Do We Have All Answers with Statins In Treating Patients with Hyperlipidemia? Kwang Kon Koh, MD, PhD, FACC, FAHA Cardiology, Gil Heart Center, Gachon Medical School, Incheon,
Welcome! Mark May 14, Sat! Do We Have All Answers with Statins In Treating Patients with Hyperlipidemia? Kwang Kon Koh, MD, PhD, FACC, FAHA Cardiology, Gil Heart Center, Gachon Medical School, Incheon,
Is Lower Better for LDL or is there a Sweet Spot
 Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
Is Lower Better for LDL or is there a Sweet Spot ALAN S BROWN MD, FACC FNLA FAHA FASPC DIRECTOR, DIVISION OF CARDIOLOGY ADVOCATE LUTHERAN GENERAL HOSPITAL, PARK RIDGE, ILLINOIS DIRECTOR OF CARDIOLOGY,
9/18/2017 DISCLOSURES. Consultant: RubiconMD. Research: Amgen, NHLBI OUTLINE OBJECTIVES. Review current CV risk assessment tools.
 UW MEDICINE UW MEDICINE UCSF ASIAN TITLE HEALTH OR EVENT SYMPOSIUM 2017 DISCLOSURES Consultant: RubiconMD ESTIMATING CV RISK IN ASIAN AMERICANS AND PREVENTION OF CVD Research: Amgen, NHLBI EUGENE YANG,
UW MEDICINE UW MEDICINE UCSF ASIAN TITLE HEALTH OR EVENT SYMPOSIUM 2017 DISCLOSURES Consultant: RubiconMD ESTIMATING CV RISK IN ASIAN AMERICANS AND PREVENTION OF CVD Research: Amgen, NHLBI EUGENE YANG,
Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode Island Cardiology Center
 Primary and Secondary Prevention of Coronary Artery Disease: What is the role of non statin drugs (fenofibrates, fish oil, niacin, folate and vitamins)? Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode
Primary and Secondary Prevention of Coronary Artery Disease: What is the role of non statin drugs (fenofibrates, fish oil, niacin, folate and vitamins)? Janet B. Long, MSN, ACNP, CLS, FAHA, FNLA Rhode
Weintraub, W et al NEJM March Khot, UN et al, JAMA 2003
 Global risk hscrp Should not be included in a Global Cardiovascular Risk Assessment. Jodi Tinkel, MD Assistant Professor Director of Cardiac Rehabilitation Associate Program Director, Cardiovascular Medicine
Global risk hscrp Should not be included in a Global Cardiovascular Risk Assessment. Jodi Tinkel, MD Assistant Professor Director of Cardiac Rehabilitation Associate Program Director, Cardiovascular Medicine
Contemporary management of Dyslipidemia
 Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Contemporary management of Dyslipidemia Todd Anderson Feb 2018 Disclosure Statement Within the past two years: I have not had an affiliation (financial or otherwise) with a commercial organization that
Placebo-Controlled Statin Trials
 PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
PREVENTION OF CHD WITH LIPID MANAGEMENT AND ASPIRIN: MATCHING TREATMENT TO RISK Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of
The Diabetes Link to Heart Disease
 The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
The Diabetes Link to Heart Disease Anthony Abe DeSantis, MD September 18, 2015 University of WA Division of Metabolism, Endocrinology and Nutrition Oswald Toosweet Case #1 68 yo M with T2DM Diagnosed DM
Statins and endothelium function
 Statins and endothelium function Matthias Endres Berlin, Germany Klinik und Poliklinik für Neurologie Conflict of interest: research grant from AstraZeneca from prevention to acute therapy... Pleiotropic
Statins and endothelium function Matthias Endres Berlin, Germany Klinik und Poliklinik für Neurologie Conflict of interest: research grant from AstraZeneca from prevention to acute therapy... Pleiotropic
Macrovascular Disease in Diabetes
 Macrovascular Disease in Diabetes William R. Hiatt, MD Professor of Medicine/Cardiology University of Colorado School of Medicine President, CPC Clinical Research Conflicts CPC Clinical Research (University-based
Macrovascular Disease in Diabetes William R. Hiatt, MD Professor of Medicine/Cardiology University of Colorado School of Medicine President, CPC Clinical Research Conflicts CPC Clinical Research (University-based
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient
 Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Update on Dyslipidemia and Recent Data on Treating the Statin Intolerant Patient Steven E. Nissen MD Chairman, Department of Cardiovascular Medicine Cleveland Clinic Disclosure Consulting: Many pharmaceutical
Low-density lipoprotein as the key factor in atherogenesis too high, too long, or both
 Low-density lipoprotein as the key factor in atherogenesis too high, too long, or both Lluís Masana Vascular Medicine and Metabolism Unit. Sant Joan University Hospital. IISPV. CIBERDEM Rovira i Virgili
Low-density lipoprotein as the key factor in atherogenesis too high, too long, or both Lluís Masana Vascular Medicine and Metabolism Unit. Sant Joan University Hospital. IISPV. CIBERDEM Rovira i Virgili
Medscape: What do we currently know about the role of CRP as a prognostic marker for primary prevention?
 To Print: Click your browser's PRINT button. NOTE: To view the article with Web enhancements, go to: http://www.medscape.com/viewarticle/500108 Expert Interview C-Reactive Protein -- Inflammatory Marker
To Print: Click your browser's PRINT button. NOTE: To view the article with Web enhancements, go to: http://www.medscape.com/viewarticle/500108 Expert Interview C-Reactive Protein -- Inflammatory Marker
Prospective Natural-History Study of Coronary Atherosclerosis
 Introduction Review of literature from April 2010 to present Concentrated on clinical studies Categories: Atherosclerosis, Lipids, Diabetes and CVD Risk Medical Therapy Statins really could there be anything
Introduction Review of literature from April 2010 to present Concentrated on clinical studies Categories: Atherosclerosis, Lipids, Diabetes and CVD Risk Medical Therapy Statins really could there be anything
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center
 Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
Branko N Huisa M.D. Assistant Professor of Neurology UNM Stroke Center THE END! CHANGABLE Blood pressure Diabetes Mellitus Hyperlipidemia Atrial fibrillation Nicotine Drug abuse Life style NOT CHANGABLE
PAR-1 Antagonist: What Do Clinical Trials Teach Us?
 Prevention of Atherothrombotic Events: What s the New Evidence? PAR-1 Antagonist: What Do Clinical Trials Teach Us? David A. Morrow, MD, MPH Director, Levine Cardiac Intensive Care Unit Senior Investigator,
Prevention of Atherothrombotic Events: What s the New Evidence? PAR-1 Antagonist: What Do Clinical Trials Teach Us? David A. Morrow, MD, MPH Director, Levine Cardiac Intensive Care Unit Senior Investigator,
CVD Risk Assessment. Lipid Management in Women: Lessons Learned. Conflict of Interest Disclosure
 Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
Lipid Management in Women: Lessons Learned Conflict of Interest Disclosure Emma A. Meagher, MD has no conflicts to disclose Emma A. Meagher, MD Associate Professor, Medicine and Pharmacology University
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona,
 Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Marshall Tulloch-Reid, MD, MPhil, DSc, FACE Epidemiology Research Unit Tropical Medicine Research Institute The University of the West Indies, Mona, Jamaica At the end of this presentation the participant
Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic Conflits of interest? None Disclaimer The opinions contained herein are not to be considered
Is it an era for statin for life?
 Is it an era for statin for life? Mohamed Abdel Ghany Professor of Cardiology Cairo University Cardiovascular Disease (CVD) is the leading global cause of death 1 Dyslipidemia as a main Risk Factor for
Is it an era for statin for life? Mohamed Abdel Ghany Professor of Cardiology Cairo University Cardiovascular Disease (CVD) is the leading global cause of death 1 Dyslipidemia as a main Risk Factor for
Modern Lipid Management:
 Modern Lipid Management: New Drugs, New Targets, New Hope Kirk U. Knowlton, M.D Director of Cardiovascular Research Co Chief of Cardiology Why lower LDL C in those without evidence of CAD (primary prevention)
Modern Lipid Management: New Drugs, New Targets, New Hope Kirk U. Knowlton, M.D Director of Cardiovascular Research Co Chief of Cardiology Why lower LDL C in those without evidence of CAD (primary prevention)
In-Ho Chae. Seoul National University College of Medicine
 The Earlier, The Better: Quantum Progress in ACS In-Ho Chae Seoul National University College of Medicine Quantum Leap in Statin Landmark Trials in ACS patients Randomized Controlled Studies of Lipid-Lowering
The Earlier, The Better: Quantum Progress in ACS In-Ho Chae Seoul National University College of Medicine Quantum Leap in Statin Landmark Trials in ACS patients Randomized Controlled Studies of Lipid-Lowering
Weigh the benefit of statin treatment: LDL & Beyond
 Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
Weigh the benefit of statin treatment: LDL & Beyond Duk-Woo Park, MD, PhD Heart Institute, University of Ulsan College of Medicine, Asan Medical, Seoul, Korea FOURIER Further cardiovascular OUtcomes Research
Preventing coronary artery disease: Cholesterol or inflammation?
 Preventing coronary artery disease: Cholesterol or inflammation? Alexis Baass MD, MSc, FRCPC, DABCL, FNLA Medical Biochemist and Lipidologist MUHC Clinical Researcher and Lipidologist IRCM Disclaimers
Preventing coronary artery disease: Cholesterol or inflammation? Alexis Baass MD, MSc, FRCPC, DABCL, FNLA Medical Biochemist and Lipidologist MUHC Clinical Researcher and Lipidologist IRCM Disclaimers
Tailored Statin Treatment for Type 2 Diabetes. Han, Ki Hoon Asan Medical Center University of Ulsan
 Tailored Statin Treatment for Type 2 Diabetes Han, Ki Hoon Asan Medical Center University of Ulsan 1 Cardiovascular disease ; No1. death (2001) respiratory tract infection Other NCD S HIV/AIDS deaths during
Tailored Statin Treatment for Type 2 Diabetes Han, Ki Hoon Asan Medical Center University of Ulsan 1 Cardiovascular disease ; No1. death (2001) respiratory tract infection Other NCD S HIV/AIDS deaths during
JAMA. 2011;305(24): Nora A. Kalagi, MSc
: Nora A. Kalagi, MSc") JAMA. 2011;305(24):2556-2564 By Nora A. Kalagi, MSc Cardiovascular disease (CVD) is the number one cause of mortality and morbidity world wide Reducing high blood cholesterol which is a risk factor for
JAMA. 2011;305(24):2556-2564 By Nora A. Kalagi, MSc Cardiovascular disease (CVD) is the number one cause of mortality and morbidity world wide Reducing high blood cholesterol which is a risk factor for
SESSION 3 11 AM 12:30 PM
 SESSION 3 11 AM 12:30 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
SESSION 3 11 AM 12:30 PM for the Primary Prevention of Cardiovascular Disease: A Personalized Approach SPEAKER Samia Mora MD, MHS Presenter Disclosure Information The following relationships exist related
Modifying atherosclerosis in cardiometabolic disease: targeting inflammation!
 Modifying atherosclerosis in cardiometabolic disease: targeting inflammation Peter Libby Brigham & Women s Hospital Harvard Medical School Primary Care Congress for Cardiometabolic Health Boston April
Modifying atherosclerosis in cardiometabolic disease: targeting inflammation Peter Libby Brigham & Women s Hospital Harvard Medical School Primary Care Congress for Cardiometabolic Health Boston April
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform