Hypertension in 2015: SPRINT-ing ahead of JNC-8. MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
|
|
|
- Laurence Fleming
- 5 years ago
- Views:
Transcription




1 Hypertension in 2015: SPRINT-ing ahead of JNC-8 MAJ Charles Magee, MD MPH FACP Director, WRNMMC Hypertension Clinic
2 Conflits of interest? None


3 Disclaimer The opinions contained herein are not to be considered as official or reflecting the views of the Department of the Army or Department of Defense
4 2015 A BIG year for hypertension Getting comfortable with JNC-8 (a SBP goal of 150?!?) SPRINT new SBP goal for 50+, non-diabetics? USPSTF adults 18+, out of office BP to confirm (Grade A recommendation) Goals Review where we were (JNC7) Identify where we are now (JNC8) See where are we going (SPRINT)
5
6 JNC7: Lancet 2002; 360:
7 60% and 50% decline in mortality from CVA and CAD, respectively, in 3 decades following 1972 Independent of gender, age, race, or socioeconomic status Correlates with improving societal awareness & HTN management JNC7: Lancet 2002; 360:

8 JNC7: from Circulation 1991;83:356-62

9 JNC7: from Hypertension 2001;37:869-74
10 Lifestyle Lifestyle Modification Weight reduction (goal BMI kg/m 2 ) DASH diet Dietary Na restriction (<2.4g/day) Physical activity (aerobic 30min >3x/week) Moderation of alcohol use Effect (SBP lowering) 5-20 mmhg/10 kg loss 8-14 mmhg 2-8 mmhg 4-9 mmhg 2-4 mmhg Tobacco cessation (36% mortality relative risk reduction) Arch Intern Med 1997;157: Hypertension 2000;35:544-9 NEJM 2001;344:3-10 Ann Intern Med 2001;135: Hypertension 2000;35: Hypertension 2000;35: Ann Intern Med 2002;136: Hypertension 2001;38: JAMA 2003;289: JAMA 2003;290: 86-97
11 Definitions Re-defined by JNC7 (unchanged in JNC8) Pre-hypertension: /80-89 Stage 1: / Stage 2: 160/ 100
12
13 JNC8 In adults with hypertension, does initiating antihypertensive pharmacologic therapy at specific BP thresholds improve health outcomes? In adults with hypertension, does treatment with antihypertensive pharmacologic therapy to a specified BP goal lead to improvements in health outcomes? In adults with hypertension, do various antihypertensive drugs or drug classes differ in comparative benefits and harms on specific health outcomes?
14 JNC8 The evidence review considered RCTs including the following health outcomes: -Overall mortality, CVD-related mortality or CKD-related mortality -Acute MI, heart failure, or stroke -Coronary revascularization or other revascularization -ESRD (resulting in HD or transplant), doubling of Cr or halving of GFR
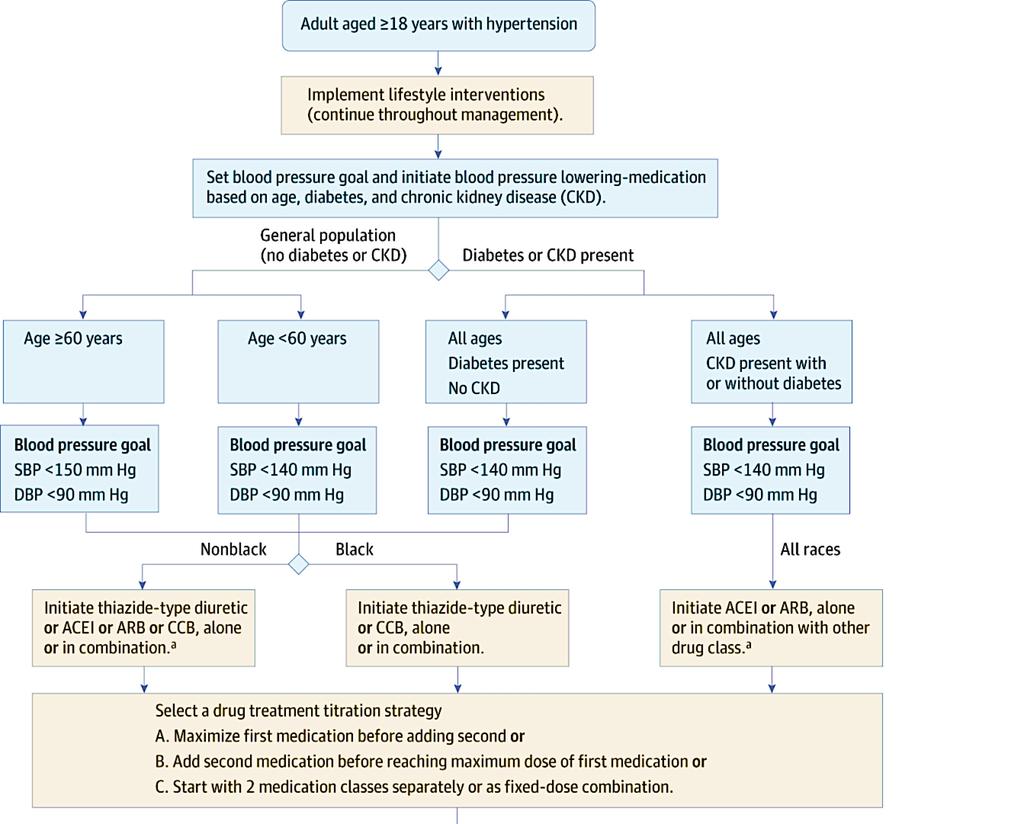
15 JNC8 Recommendations 1. General pop 60+, initiate tx at threshold 150/90 mmhg; & tx goal is below 150/90 mmhg (grade A) Corollary: do not adjust if already below and tolerating (grade E) 2. Gen pop <60, initiate tx at threshold DBP 90 mmhg; & tx goal is below DBP 90 mmhg Age (grade A) Age 18-29, (grade E) 3. Gen pop <60, initiate tx at threshold SBP 140 mmhg; & tx goal is below SBP 140 mmhg (grade E) 4. Ages 18+ w/ CKD, initiate tx to lower BP at 140/90 mmhg; & tx goal is below 140/90 mmhg (grade E) 5. Ages 18+ w/ DM, initiate tx to lower BP at 140/90 mmhg; & tx goal is below 140/90 mmhg (grade E)
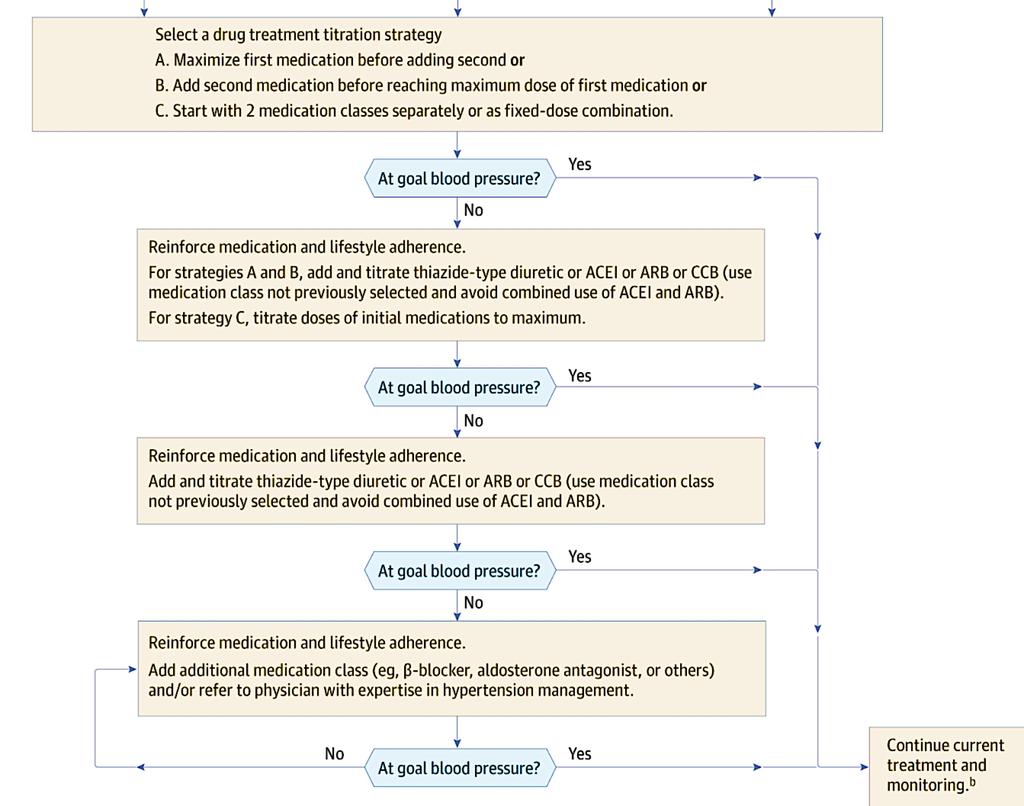
16 JNC8 Recommendations 6. Gen Nonblack pop (+/- DM), initial tx = thiazide diuretic, CCB, ACEI or ARB (grade B) 7. Gen black pop (+/- DM), initial tx = thiazide diuretic or CCB (grade B) with CKD, initial (or add-on) = ACEI or ARB to improve kidney outcomes (grade B) 9. If goal not achieved at 1 month, titrate up (increase initial drug dose), or add rx from Rec 6; repeat up to 3 meds; if not at goal, refer to specialist (grade E) *BB no longer recommended 1 st line; consider in Rec #9 with other therapeutic classes
17
18
19
20 JNC8 Strategies A Start one drug, titrate to max dose, then add 2 nd Ex: In patient with CKD, start with ACEI/ARB. Titrate to max dose at next visit in 1 month. If not at goal, add next agent, either thiazide diuretic or CCB and titrate up B Start one drug and add 2 nd before achieving max dose of initial drug Ex: In gen black patient, start with thiazide diuretic at starting dose. Add CCB before maximizing initial diuretic; titrate both up to maximum dosing before starting 3 rd agent C Begin 2 drugs at same time; consider combination pill. Consider if BP >160/100, or SBP >20 mmhg above goal or DBP >10 mmhg above goal Ex: Initiate or add two drugs or combination and if not at goal, add 3 rd agent and titrate up to maximum dose
21
22 Context Two days before the SPRINT trial release Meta-Analysis 19 RCTs of Intensive (mean 133/76 mmhg) vs Less-Intensive (mean 140/81mmHg) Significant reduction in RR: Major CV events (14%), MI (13%), stroke (22%), retinopathy (19%), and albuminuria (10%) Non-significant reduction in RR: total mortality (9%), CV-death (9%), HF (15%), ESRD (10%) Significant increase in hypotension (RR 2.68) Lancet Nov 7. [Epublication ahead of print]
23 SPRINT Design Unblinded RCT 9250 participants, age 50+, SBP 130+ mmhg, 1+ additional CVD risk factors Compliments ACCORD trial with non-dm population Early termination interpret with caution! N Engl J Med 2015;373:
24 Results Randomization effective Avg age 68 +/- 9, 64% male, 31% black, 28% CKD, FramRisk 20%,<50% statin use, CVD 17%, SBP 139 +/- 15 mmhg Excellent follow up Intensive mean SBP mmhg; ~3 meds (goal not achieved) Standard mean SBP mmhg; ~2 meds N Engl N Engl J Med J Med 2010;362: ;373:
25 Outcome Primary (Acute MI, ACS, CVA, CHF, death 2/2 CV cause) Secondary SPRINT Trial - Outcomes Intensive %/yr (N=4678) Standard %/yr (N=4683) HR Heart Failure Death, CV cause Death, any cause Primary outcome OR death (any cause) w/o CKD baseline (N=3332) (N=3345) NNT (NNH) >/= 30% reduction in egfr to < (37) NNT to prevent one [outcome] over 3.26 years Non-significant differences: Acute MI, ACS, CVA; composite, individual renal outcomes Subgroup analysis: Non-significantly favoring Intensive treatment for: No CKD (HR 0.70); age >75 (HR0.67); male (HR 0.72); nonblack (0.74); no known CVD (0.71); and SBP <132 mmhg N Engl J Med 2015;373:

26 SPRINT Outcomes N Engl J Med 2015;373: N Engl J Med 2010;362:
27 Outcome SPRINT Trial Adverse Effects Intensive no. of pts (%) (N=4678) Standard no. of pts (%) (N=4683) HR NNT (NNH) Serious adverse event only Hypotension 110 (2.4) 66 (1.4) 1.67 (107) Syncope 107 (2.3) 80 (1.7) 1.33 (173) Acute Kidney Injury 193 (4.1) 117 (2.5) 1.66 (62) ED visit or Serious adverse event Hypotension 158 (3.4) 93 (2.0) 1.7 (72) Syncope 163 (3.5) 113 (2.4) 1.44 (94) Electrolyte abnormality 177 (3.8) 129 (2.8) 1.38 (98) Acute Kidney Injury 204 (4.4) 120 (2.6) 1.71 (56) Serum Na <130 mmol/l 180 (3.8) 100 (2.1) 1.76 (59) Serum K <3.0 mmol/l 114 (2.4) 74 (1.6) 1.5 (117) Orthostatic Hypotension, asymptomatic 777 (16.6) 857 (18.3) N Engl J Med 2015;373:

28 SPRINT & STOP-IT 2
29 Conclusions JNC8 builds on JNC7 No changes to existing definitions Applies strongest available evidence; Sets evidence-based initiation thresholds & treatment goals conservative in nature If valid, SPRINT, modeled after ACCORD, suggests benefit with intensive therapy Asymmetric overlap with Lancet meta-analysis across CVD outcomes and mortality; Demonstrates important adverse effects with intensive therapy
30 Patient Scenario #1 Your next patient is an active, 56 year old black female with CKD and hypertension. She follows the news and has renewed concerns about her blood pressure. Her BP is 167/93. Labs reveal total cholesterol 174mg/dL, LDL 90mg/dL, HDL 60mg/ dl, and her Cr is 1.6 (GFR 43 ml/min/1.73m 2 ). She is currently untreated as she was without insurance for almost a decade. How do you advise the patient?
31 How do you advise the patient? JNC8 Age <60, + CKD Recs 2-4, 8 & 9 apply Initiate tx for >140/90 mmhg, treat to <140/90 mmhg Initiate with ACEI/ARB Consider combination with CCB or thiazide SPRINT Patient less similar to study (young, black, female, higher BP, no meds, lipids, overall risk) Unclear benefit driving SBP from 136 mmhg to 121 mmhg TAKE HOME: SPRINT trial was older, non-black male predominant, already near 140/90 and on medication at enrollment. Intensive treatment benefits and risk of harm may not generalize well to this patient.
32 Patient Scenario #2 68 year old male with hypertension, obesity and hyperlipidemia comes in for a routine physical. He is appreciably winded after a flight of stairs. His father died of an MI at age 60 and the patient quit smoking 3 years ago after his brother suffered a stroke. He s willing to do whatever it takes to lower his cardiovascular risk. He takes a high-intensity statin, chlorthalidone, and low dose aspirin. He started exercising 6 months ago and continues to focus on a DASH, low sodium diet. His BP is 138/84. His Cr is 1.2 (GFR >60 ml/min/1.73m 2 ) and hemoglobic A1c is 5.9%. How do you advise the patient?
33 How do you advise your patient? JNC8 Age >60, no CKD or DM Recs 1 & 6 apply Tx goal <150/90; advise to continue existing therapy as tolerated Lacking Strong evidence for clinical benefit to lower therapeutic goals SPRINT Increased CVD risk and potential increased mortality benefit w/ lower SBP goal of 120 mmhg. Recommend additional agents, discussing risk of significant hypotension, syncope, AKI, electrolytes TAKE HOME: SPRINT trial allows for evidenced-based shared-decision making to understand benefits and risks of more intensive therapy; this patient may be a candidate for intensive therapy.
34 Questions?
Management of Lipid Disorders and Hypertension: Implications of the New Guidelines
 Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
Management of Lipid Disorders and Hypertension Management of Lipid Disorders and Hypertension: Implications of the New Guidelines Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine
The Latest Generation of Clinical
 The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
The Latest Generation of Clinical Guidelines: HTN and HLD Dave Brackett Clinical Guideline Purpose Uniform approach Awareness of key details Diagnosis Treatment Monitoring Evidence based approach Inform
Hypertension JNC 8 (2014)
") Hypertension JNC 8 (2014) Renewed: February 2018 Updated: February 2015 Comparison of Seventh Joint National Committee (JNC 7) vs. Eighth Joint National Committee (JNC 8) Hypertension Guidelines Methodology
Hypertension JNC 8 (2014) Renewed: February 2018 Updated: February 2015 Comparison of Seventh Joint National Committee (JNC 7) vs. Eighth Joint National Committee (JNC 8) Hypertension Guidelines Methodology
JNC Evidence-Based Guidelines for the Management of High Blood Pressure in Adults
 JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
JNC 8 2014 Evidence-Based Guidelines for the Management of High Blood Pressure in Adults Table of Contents Why Do We Treat Hypertension? Blood Pressure Treatment Goals Initial Therapy Strength of Recommendation
Hypertension Management Controversies in the Elderly Patient
 Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Hypertension Management Controversies in the Elderly Patient Juan Bowen, MD Geriatric Update for the Primary Care Provider November 17, 2016 2016 MFMER slide-1 Disclosure No financial relationships No
Managing Hypertension in 2016
 Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Managing Hypertension in 2016: Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
Systolic Blood Pressure Intervention Trial (SPRINT)
") 09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
09:30-09:50 2016.4.15 Systolic Blood Pressure Intervention Trial (SPRINT) IN A NEPHROLOGIST S VIEW Sejoong Kim Seoul National University Bundang Hospital Current guidelines for BP control Lowering BP
Jared Moore, MD, FACP
 Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Hypertension 101 Jared Moore, MD, FACP Assistant Program Director, Internal Medicine Residency Clinical Assistant Professor of Internal Medicine Division of General Medicine The Ohio State University Wexner
Objectives. Describe results and implications of recent landmark hypertension trials
 Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
Hypertension Update Daniel Schwartz, MD Assistant Professor of Medicine Associate Medical Director of Heart Transplantation Temple University School of Medicine Disclosures I currently have no relationships
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure. No relevant financial relationships. Blood Pressure and Risk
 MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
MODERN MANAGEMENT OF HYPERTENSION Where Do We Draw the Line? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine baron@medicine.ucsf.edu
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Prevalence 29%; Blacks 33.5% About 72.5% treated; 53.5% uncontrolled (>140/90) Risk for poor control: Latinos, Blacks, age 18-44 and 80,
Disclosure. No relevant financial relationships. Placebo-Controlled Statin Trials
 PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
PREVENTING CARDIOVASCULAR DISEASE IN WOMEN: Current Guidelines for Hypertension, Lipids and Aspirin Disclosure Robert B. Baron, MD MS Professor and Associate Dean UCSF School of Medicine No relevant financial
Hypertension Update Clinical Controversies Regarding Age and Race
 Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
Hypertension Update Clinical Controversies Regarding Age and Race Allison Helmer, PharmD, BCACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 22, 2017 DISCLOSURE/CONFLICT
ADVANCES IN MANAGEMENT OF HYPERTENSION
 Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Advances in Management of Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Prevalence 29%; Blacks 33.5%
Treating Hypertension in 2018: What Makes the Most Sense Today?
 Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
Treating Hypertension in 2018: What Makes the Most Sense Today? Daniel Blanchard, MD Professor of Medicine UC San Diego Cardiovascular Center La Jolla, California 1 2 Speaker Disclosures Consultant and/or
New Lipid Guidelines. PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids.
 PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
PREVENTION OF CARDIOVASCULAR DISEASE IN WOMEN: Implications of the New Guidelines for Hypertension and Lipids Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Disclosure No relevant
DISCLOSURE PHARMACIST OBJECTIVES 9/30/2014 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES. I have nothing to disclose.
 JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
JNC 8: A REVIEW OF THE LONG-AWAITED/MUCH-ANTICIPATED HYPERTENSION GUIDELINES Tiffany Dickey, PharmD Assistant Professor, UAMS COP Clinical Pharmacy Specialist, Mercy Hospital Northwest AR DISCLOSURE I
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets
 New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
New Recommendations for the Treatment of Hypertension: From Population Salt Reduction to Personalized Treatment Targets Sidney C. Smith, Jr. MD, FACC, FAHA Professor of Medicine/Cardiology University of
Update in Cardiology Pharmacologic Management of Cardiovascular Risk. Christopher C. Roe, MSN, ACNP
 Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
Update in Cardiology Pharmacologic Management of Cardiovascular Risk Christopher C. Roe, MSN, ACNP Objectives 1. Verbalize understanding of new pharmacologic guidelines in the treatment of hypertension
DISCLOSURES OUTLINE OUTLINE 9/29/2014 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE
 ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
ANTI-HYPERTENSIVE MANAGEMENT OF CHRONIC KIDNEY DISEASE DISCLOSURES Editor-in-Chief- Nephrology- UpToDate- (Wolters Klewer) Richard J. Glassock, MD, MACP Geffen School of Medicine at UCLA 1 st Annual Internal
The New Hypertension Guidelines
 The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
The New Hypertension Guidelines Joseph Saseen, PharmD Professor and Vice Chair, Department of Clinical Pharmacy University of Colorado Anschutz Medical Campus Disclosure Joseph Saseen reports no conflicts
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014
 HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
HYPERTENSION GUIDELINES WHERE ARE WE IN 2014 Donald J. DiPette MD FACP Special Assistant to the Provost for Health Affairs Distinguished Health Sciences Professor University of South Carolina University
Hypertension targets: sorting out the confusion. Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town
 Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
Hypertension targets: sorting out the confusion Brian Rayner, Division of Nephrology and Hypertension, University of Cape Town Historical Perspective The most famous casualty of this approach was the
New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD
 New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD None Disclosures Objectives Understand trend in blood pressure clinical practice guidelines
New Hypertension Guidelines: Why the change? Neil Brummond, M.D. Avera Medical Group Internal Medicine Sioux Falls, SD None Disclosures Objectives Understand trend in blood pressure clinical practice guidelines
Preventing and Treating High Blood Pressure
 Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Preventing and Treating High Blood Pressure: Finding the Right Balance of Integrative and Pharmacologic Approaches Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Blood Pressure
Modern Management of Hypertension
 Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
Modern Management of Hypertension Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Current Status of Hypertension Prevalence
JNC 8 -Controversies. Sagren Naidoo Nephrologist CMJAH
 JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
JNC 8 -Controversies Sagren Naidoo Nephrologist CMJAH Joint National Committee (JNC) Panel appointed by the National Heart, Lung, and Blood Institute (NHLBI) First guidelines (JNC-1) published in 1977
2/9/2017. Financial Disclosures/Unapproved Use. Achieving Harmony in Blood Pressure Guidelines Around the Globe. Roger S. Blumenthal, MD.
 Achieving Harmony in Blood Pressure Guidelines Around the Globe Roger S. Blumenthal, MD The Kenneth Jay Pollin Professor of Cardiology Director, The Johns Hopkins Ciccarone Center for the Prevention Of
Achieving Harmony in Blood Pressure Guidelines Around the Globe Roger S. Blumenthal, MD The Kenneth Jay Pollin Professor of Cardiology Director, The Johns Hopkins Ciccarone Center for the Prevention Of
Diabetes and Hypertension
 Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Diabetes and Hypertension M.Nakhjvani,M.D Tehran University of Medical Sciences 20-8-96 Hypertension Common DM comorbidity Prevalence depends on diabetes type, age, BMI, ethnicity Major risk factor for
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, Financial Disclosures
 Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
Hypertension Guidelines: Are We Pressured to Change? Oregon Cardiovascular Symposium Portland, Oregon June 6, 2015 William C. Cushman, MD Professor, Preventive Medicine, Medicine, and Physiology University
OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA
 OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
OMED 17 OCTOBER 7-10 PHILADELPHIA, PENNSYLVANIA 29.5 Category 1-A CME credits anticipated ACOFP / AOA s 122 nd Annual Osteopathic Medical Conference & Exposition ACOFP - The Heart of the Matter - An Evidence
HYPERTENSION: UPDATE 2018
 HYPERTENSION: UPDATE 2018 From the Cardiologist point of view Richard C Padgett, MD I have no disclosures HYPERTENSION ALWAYS THE ELEPHANT IN THE EXAM ROOM BUT SOMETIMES IT CHARGES HTN IN US ~78 million
HYPERTENSION: UPDATE 2018 From the Cardiologist point of view Richard C Padgett, MD I have no disclosures HYPERTENSION ALWAYS THE ELEPHANT IN THE EXAM ROOM BUT SOMETIMES IT CHARGES HTN IN US ~78 million
Update in Hypertension
 Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Update in Hypertension Eliseo J. PérezP rez-stable MD Professor of Medicine DGIM, Department of Medicine UCSF 20 May 2008 Declaration of full disclosure: No conflict of interest (I have never been funded
Blood Pressure LIMBO How Low To Go?
 Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
Blood Pressure LIMBO How Low To Go? Joseph L. Kummer, MD, FACC Bryan Heart Spring Conference April 21 st, 2018 Hypertension Epidemiology Over a billion people have hypertension Major cause of morbidity
Modern Management of Hypertension: Where Do We Draw the Line?
 Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
Modern Management of Hypertension: Where Do We Draw the Line? Robert B. Baron MD Professor of Medicine Associate Dean for GME and CME Declaration of full disclosure: No conflict of interest Blood Pressure
4/4/17 HYPERTENSION TARGETS: WHAT DO WE DO NOW? SET THE STAGE BP IN CLINICAL TRIALS?
 HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
HYPERTENSION TARGETS: WHAT DO WE DO NOW? MICHAEL LEFEVRE, MD, MSPH PROFESSOR AND VICE CHAIR DEPARTMENT OF FAMILY AND COMMUNITY MEDICINE UNIVERSITY OF MISSOURI 4/4/17 DISCLOSURE: MEMBER OF THE JNC 8 PANEL
MANAGEMENT OF HYPERTENSION: TREATMENT THRESHOLDS AND MEDICATION SELECTION
 Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Management of Hypertension: Treatment Thresholds and Medication Selection Robert B. Baron, MD MS Professor and Associate Dean Declaration of full disclosure: No conflict of interest Presentation Goals
Hypertension Update. Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016
 Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
Mayo Clinic 90 th Annual Clinical Reviews November 2 nd and 16 th, 2016 Hypertension Update Vincent J. Canzanello, M.D. Consultant, Division of Nephrology and Hypertension Professor or Medicine College
Hypertension Update. Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy
 Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Update Sarah J. Payne, MS, PharmD, BCPS Assistant Professor, Department of Pharmacotherapy UNT System College of Pharmacy Introduction 1/3 of US adults have HTN More prevalent in non-hispanic
Hypertension Management: A Moving Target
 9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
9:45 :30am Hypertension Management: A Moving Target SPEAKER Karol Watson, MD, PhD, FACC Presenter Disclosure Information The following relationships exist related to this presentation: Karol E. Watson,
Using the New Hypertension Guidelines
 Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Using the New Hypertension Guidelines Kamal Henderson, MD Department of Cardiology, Preventive Medicine, University of North Carolina School of Medicine Kotchen TA. Historical trends and milestones in
Disclosures. Diabetes and Cardiovascular Risk Management. Learning Objectives. Atherosclerotic Cardiovascular Disease
 Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Disclosures Diabetes and Cardiovascular Risk Management Tony Hampton, MD, MBA Medical Director Advocate Aurora Operating System Advocate Aurora Healthcare Downers Grove, IL No conflicts or disclosures
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM
 Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
Todd S. Perlstein, MD FIFTH ANNUAL SYMPOSIUM Faculty Disclosure I have no financial interest to disclose No off-label use of medications will be discussed FIFTH ANNUAL SYMPOSIUM Recognize changes between
The earlier BP control the better cardiovascular outcome. Jin Oh Na Cardiovascular center Korea University Medical College
 The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
The earlier BP control the better cardiovascular outcome Jin Oh Na Cardiovascular center Korea University Medical College Index Introduction HOPE-3 Trial Sprint Study Summary Each 2 mmhg decrease in SBP
Hypertension. Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute
 Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Hypertension Does it Matter What Medications We Use? Nishant K. Sekaran, M.D. M.Sc. Intermountain Heart Institute Hypertension 2017 Classification BP Category Systolic Diastolic Normal 120 and 80 Elevated
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH)
") Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
Evolving Concepts on Hypertension: Implications of Three Guidelines (JNC 8 Panel, ESH/ESC, NICE/BSH) Sidney C. Smith, Jr. MD, FACC, FAHA, FESC Professor of Medicine/Cardiology University of North Carolina
We are delighted to have Dr. Roetzheim with us today to discuss Managing Hypertension in Older Adult Patients.
 Richard Roetzheim, MD, MSPH is Professor and Chair, Department of Family Medicine at the University of South Florida Morsani College of Medicine. Dr. Roetzheim has considerable experience leading NIH funded
Richard Roetzheim, MD, MSPH is Professor and Chair, Department of Family Medicine at the University of South Florida Morsani College of Medicine. Dr. Roetzheim has considerable experience leading NIH funded
Managing Hypertension in 2018
 MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
MANAGING HYPERTENSION IN 2018 How Do We Work With Conflicting Data and Conflicting Guidelines? Disclosure No relevant financial relationships Robert B. Baron, MD MS Professor and Associate Dean UCSF School
Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD?
 Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD? Suzanne Oparil, MD Distinguished Professor of Medicine, Professor of Cell, Developmental and Integrative Biology Director, Vascular
Hypertension and Diabetes Should we be SPRINTING or Reaching an ACCORD? Suzanne Oparil, MD Distinguished Professor of Medicine, Professor of Cell, Developmental and Integrative Biology Director, Vascular
What s In the New Hypertension Guidelines?
 American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
American College of Physicians Ohio/Air Force Chapters 2018 Scientific Meeting Columbus, OH October 5, 2018 What s In the New Hypertension Guidelines? Max C. Reif, MD, FACP Objectives: At the end of the
Hypertension Controversies: SPRINTing to New Goals
 Hypertension Controversies: SPRINTing to New Goals Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Lauren Wolfe, PharmD Primary Care Clinical Specialist Cleveland
Hypertension Controversies: SPRINTing to New Goals Diana Isaacs, PharmD, BCPS, BC-ADM, CDE Clinical Pharmacy Specialist Cleveland Clinic Lauren Wolfe, PharmD Primary Care Clinical Specialist Cleveland
Hypertension and Cardiovascular Disease
 Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
Hypertension and Cardiovascular Disease Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored, or transmitted in any form or by any means graphic,
HYPERTENSION MANAGEMENT IN ELDERLY POPULATIONS
 HYPERTENSION MANAGEMENT IN ELDERLY POPULATIONS Michael J. Scalese, PharmD, BCPS, CACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 14, 2018 DISCLOSURE/CONFLICT OF INTEREST
HYPERTENSION MANAGEMENT IN ELDERLY POPULATIONS Michael J. Scalese, PharmD, BCPS, CACP Assistant Clinical Professor Auburn University Harrison School of Pharmacy July 14, 2018 DISCLOSURE/CONFLICT OF INTEREST
Randomized Design of ALLHAT BP Trial
 Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
Outcomes in Hypertensive Black and Nonblack Patients Treated with Chlorthalidone, Amlodipine, and Lisinopril* *Wright JT, Dunn JK, Cutler JA et al. JAMA 2005:293:1595-1608. 42,418 High-risk hypertensive
ALLHAT. Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic
 1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
1 U.S. Department of Health and Human Services National Institutes of Health Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker
None. Disclosure: Relationships with Industry Conflicts of Interests. Learning Objectives: Participants will be able to:
 2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) James W. Shaw, MD Memorial Lecture
2014 Evidence-Based Guideline for the Management of High Blood Pressure in Adults: Report from the Panel Members Appointed to the Eighth Joint National Committee (JNC 8) James W. Shaw, MD Memorial Lecture
Diabetes Mellitus: A Cardiovascular Disease
 Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Diabetes Mellitus: A Cardiovascular Disease Nestoras Mathioudakis, M.D. Assistant Professor of Medicine Division of Endocrinology, Diabetes, & Metabolism September 30, 2013 1 The ABCs of cardiovascular
Antihypertensive Trial Design ALLHAT
 1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
1 U.S. Department of Health and Human Services Major Outcomes in High Risk Hypertensive Patients Randomized to Angiotensin-Converting Enzyme Inhibitor or Calcium Channel Blocker vs Diuretic National Institutes
Hypertension Update 2009
 Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Hypertension Update 2009 New Drugs, New Goals, New Approaches, New Lessons from Clinical Trials Timothy C Fagan, MD, FACP Professor Emeritus University of Arizona New Drugs Direct Renin Inhibitors Endothelin
Managing Hypertension in Diabetes Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park.
 Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
Managing Hypertension in Diabetes 2015 Sean Stewart, PharmD, BCPS, BCACP, CLS Internal Medicine Park Nicollet Clinic St Louis Park Case Scenario Mike M is a 59 year old man with type 2 diabetes managed
T. Suithichaiyakul Cardiomed Chula
 T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
T. Suithichaiyakul Cardiomed Chula The cardiovascular (CV) continuum: role of risk factors Endothelial Dysfunction Atherosclerosis and left ventricular hypertrophy Myocardial infarction & stroke Endothelial
Hypertension and the SPRINT Trial: Is Lower Better
 Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
Hypertension and the SPRINT Trial: Is Lower Better 8th Annual Orange County Symposium on Cardiovascular Disease Prevention Saturday, October 8, 2016 Keith C. Norris, MD, PhD, FASN Professor of Medicine,
New Hypertension Guideline Recommendations for Adults July 7, :45-9:30am
 Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Advances in Cardiovascular Disease 30 th Annual Convention and Reunion UERM-CMAA, Inc. Annual Convention and Scientific Meeting July 5-8, 2018 New Hypertension Guideline Recommendations for Adults July
Renal Denervation. by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School
 Renal Denervation by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School Disclosure Information ACOI Annual Meeting I have the following financial relationships to disclose:
Renal Denervation by Walead Latif, DO, MBA, CPE Assistant Clinical Professor Rutgers Medical School Disclosure Information ACOI Annual Meeting I have the following financial relationships to disclose:
Int. J. Pharm. Sci. Rev. Res., 36(1), January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences
, January February 2016; Article No. 06, Pages: JNC 8 versus JNC 7 Understanding the Evidences") Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Research Article JNC 8 versus JNC 7 Understanding the Evidences Anns Clara Joseph, Karthik MS, Sivasakthi R, Venkatanarayanan R, Sam Johnson Udaya Chander J* RVS College of Pharmaceutical Sciences, Coimbatore,
Management of Hypertension. M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine
 Division of Nephrology University of Missouri School of Medicine") Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Management of Hypertension M Misra MD MRCP (UK) Division of Nephrology University of Missouri School of Medicine Disturbing Trends in Hypertension HTN awareness, treatment and control rates are decreasing
Disclosures. Learning Objectives. Hypertension: a sprint to the finish Ontario Pharmacists Association 1
 Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Disclosures I have no current or past relationships with commercial entities I have received a speaker s fee from the Ontario Pharmacists Association for this learning activity Laura Tsang PharmD Sunnybrook
Hypertension diagnosis (see detail document) Diabetic. Target less than 130/80mmHg
 Diabetic. Target less than 130/80mmHg") Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Hypertension diagnosis (see detail document) Non-diabetic Diabetic Very elderly (older than 80 years) Target less than 140/90mmHg Target less than 130/80mmHg Consider SBP target less than 150mmHg Non-diabetic
Updates in Cardiovascular Recommendations for Diabetic Patients
 Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
Updates in Cardiovascular Recommendations for Diabetic Patients Chris Tawwater, Pharm.D., BCPS Clinical Pharmacist, Abilene Regional Medical Center Assistant Professor, Adult Medicine Division Pharmacotherapy
The Failing Heart in Primary Care
 The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
The Failing Heart in Primary Care Hamid Ikram How fares the Heart Failure Epidemic? 4357 patients, 57% women, mean age 74 years HFSA 2010 Practice Guideline (3.1) Heart Failure Prevention A careful and
Diversity and HTN: Approaches to optimal BP control in AfricanAmericans
 Diversity and HTN: Approaches to optimal BP control in AfricanAmericans Quinn Capers, IV, MD, FACC, FSCAI Assistant Professor of Medicine Associate Dean for Admissions Do Racial Differences Really Exist
Diversity and HTN: Approaches to optimal BP control in AfricanAmericans Quinn Capers, IV, MD, FACC, FSCAI Assistant Professor of Medicine Associate Dean for Admissions Do Racial Differences Really Exist
Blood Pressure Treatment Goals
 Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Blood Pressure Treatment Goals Kenneth Izuora, MD, MBA, FACE Associate Professor UNLV School of Medicine November 18, 2017 Learning Objectives Discuss the recent studies on treating hypertension Review
Outline. Outline CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
ALLHAT. ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status
 ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status 1 Introduction and Background Clinical trials have reported reduction in CV events with diuretics, CCBs, ACE inhibitors,
ALLHAT Antihypertensive Trial Results by Baseline Diabetic & Fasting Glucose Status 1 Introduction and Background Clinical trials have reported reduction in CV events with diuretics, CCBs, ACE inhibitors,
Reframe the Paradigm of Hypertension treatment Focus on Diabetes
 Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Reframe the Paradigm of Hypertension treatment Focus on Diabetes Paola Atallah, MD Lecturer of Clinical Medicine SGUMC EDL monthly meeting October 25,2016 Overview Physiopathology of hypertension Classification
Difficult to Treat Hypertension
 Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
Difficult to Treat Hypertension According to Goldilocks JNC 8 Blood Pressure Goals (2014) BP Goal 60 years old and greater*- systolic < 150 and diastolic < 90. (Grade A)** BP Goal 18-59 years old* diastolic
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005
 VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
VA/DoD Clinical Practice Guideline for the Diagnosis and Management of Hypertension - Pocket Guide Update 2004 Revision July 2005 1 Any adult in the health care system 2 Obtain blood pressure (BP) (Reliable,
Hypertension: 2016 Clinical Update
 PHASE Safety Net Community Benefit Hypertension: 2016 Clinical Update Presented by: Joseph Young, MD Hypertension Clinical Lead Kaiser Permanente Northern California October 6, 2016 Dr. Joseph Young Hypertension
PHASE Safety Net Community Benefit Hypertension: 2016 Clinical Update Presented by: Joseph Young, MD Hypertension Clinical Lead Kaiser Permanente Northern California October 6, 2016 Dr. Joseph Young Hypertension
Diabetes and Hypertension
 Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Diabetes and Hypertension William C. Cushman, MD, FAHA, FACP, FASH Chief, Preventive Medicine, Veterans Affairs Medical Center Professor, Preventive Medicine, Medicine, and Physiology University of Tennessee
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy. Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM
 Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
Highlights of the new blood pressure and cholesterol guidelines: A whole new philosophy Jeremy L. Johnson, PharmD, BCACP, CDE, BC-ADM OSHP 2014 Annual Meeting Oklahoma City, OK April 4, 2014 1 Objectives
CKD and risk management : NICE guideline
 CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
CKD and risk management : NICE guideline 2008-2014 Shahed Ahmed Consultant Nephrologist shahed.ahmed@rlbuht.nhs.uk Key points : Changing parameters of CKD and NICE guidance CKD and age related change of
Combination Therapy for Hypertension
 Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Combination Therapy for Hypertension Se-Joong Rim, MD Cardiology Division, Yonsei University College of Medicine, Seoul, Korea Goals of Therapy Reduce CVD and renal morbidity and mortality. Treat to BP
Egyptian Hypertension Guidelines
 Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Egyptian Hypertension Guidelines 2014 Egyptian Hypertension Guidelines Dalia R. ElRemissy, MD Lecturer of Cardiovascular Medicine Cairo University Why Egyptian Guidelines? Guidelines developed for rich
Placebo-Controlled Statin Trials Prevention Of CVD in Women"
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
The ABCs (A1C, BP and Cholesterol) of Diabetes
 of Diabetes") The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
The ABCs (A1C, BP and Cholesterol) of Diabetes Gregg Simonson, PhD Director, Professional Training and Consulting International Diabetes Center; Adjunct Assistant Professor, University of Minnesota Department
Drugs to Treat Type 2 DM Demonstrate Reductions in Major Adverse Cardiovascular Events
 Drugs to Treat Type 2 DM Demonstrate Reductions in Major Adverse Cardiovascular Events How does all this play out when it comes to treating patients with type 2 DM who have chronic kidney disease? Therapeutic
Drugs to Treat Type 2 DM Demonstrate Reductions in Major Adverse Cardiovascular Events How does all this play out when it comes to treating patients with type 2 DM who have chronic kidney disease? Therapeutic
Outline. Outline 10/14/2014 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW. Question 1: Which of these patients has CKD?
 CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
CHRONIC KIDNEY DISEASE UPDATE: WHAT THE GENERALIST NEEDS TO KNOW MICHAEL G. SHLIPAK, MD, MPH CHIEF-GENERAL INTERNAL MEDICINE, SAN FRANCISCO VA MEDICAL CENTER PROFESSOR OF MEDICINE, EPIDEMIOLOGY AND BIOSTATISTICS,
New Hypertension Guidelines. Kofi Osei, MD
 New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
New Hypertension Guidelines Kofi Osei, MD None Disclosures Objectives The new blood pressure definitions and cardiovascular risk The role to time and location in the diagnosis of hypertension Apply evidence-based
Evaluation and Management of Hypertension in Women. Vesna D. Garovic, M.D. Moscow, Russia, December 2016
 Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
Evaluation and Management of Hypertension in Women Vesna D. Garovic, M.D. Moscow, Russia, December 2016 2016 MFMER 3508058-1 Women are not small men There is nothing as powerful as an idea whose time has
Module 2. Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension
 Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Module 2 Global Cardiovascular Risk Assessment and Reduction in Women with Hypertension 1 Copyright 2017 by Sea Courses Inc. All rights reserved. No part of this document may be reproduced, copied, stored,
Hypertension (JNC-8)
") Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension (JNC-8) Southern California University of Health Sciences Physician Assistant Program Management and Treatment of Hypertension April 17, 2018, presented by Ezra Levy, Pharm.D.! The 8 th Joint
Hypertension: Update
 Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
Hypertension: Update Meenakshi A Bhalla MD,FACC Associate Professor of Medicine Director Preventive Cardiology Advanced Heart Failure and Transplant Cardiology University of Kentucky Faculty Disclosure
PHASE Preventing Heart Attacks & Strokes Everyday
 PHASE Preventing Heart Attacks & Strokes Everyday Welcome to the PHASE Learning Community! Joseph D. Young, MD Kaiser Permanente Northern California Jean Nudelman Kaiser Permanente Northern California
PHASE Preventing Heart Attacks & Strokes Everyday Welcome to the PHASE Learning Community! Joseph D. Young, MD Kaiser Permanente Northern California Jean Nudelman Kaiser Permanente Northern California
HYPERTENSION: ARE WE GOING TOO LOW?
 HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
HYPERTENSION: ARE WE GOING TOO LOW? George L. Bakris, M.D.,F.A.S.N.,F.A.S.H., F.A.H.A. Professor of Medicine Director, ASH Comprehensive Hypertension Center University of Chicago Medicine Chicago, IL USA
How do we diagnose hypertension today? Presentation Subtitle
 How do we diagnose hypertension today? Presentation Subtitle Renata Cífková Case 1 JM, a 64-year-old lady referred to our center because of undesirable effects of her antihypertensive medication Personal
How do we diagnose hypertension today? Presentation Subtitle Renata Cífková Case 1 JM, a 64-year-old lady referred to our center because of undesirable effects of her antihypertensive medication Personal
Placebo-Controlled Statin Trials MANAGEMENT OF HIGH BLOOD CHOLESTEROL MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES
 MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
MANAGEMENT OF HIGH BLOOD CHOLESTEROL: IMPLICATIONS OF THE NEW GUIDELINES Robert B. Baron MD MS Professor and Associate Dean UCSF School of Medicine Declaration of full disclosure: No conflict of interest
Tread Carefully Because you Tread on my Nephrons. Prescribing Hints in Renal Disease
 Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Tread Carefully Because you Tread on my Nephrons Prescribing Hints in Renal Disease David WP Lappin,, MB PhD FRCPI Clinical Lecturer in Medicine and Consultant Nephrologist and General Physician, Merlin
Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines. John Potter Professor Ageing & Stroke Medicine University of East Anglia
 Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines John Potter Professor Ageing & Stroke Medicine University of East Anglia Preventing Cardiovascular Disease Stroke Primary Prevention
Preventing Cardiovascular Disease Stroke Primary Prevention Guidelines John Potter Professor Ageing & Stroke Medicine University of East Anglia Preventing Cardiovascular Disease Stroke Primary Prevention
DEPARTMENT OF GENERAL MEDICINE WELCOMES
 DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global
DEPARTMENT OF GENERAL MEDICINE WELCOMES 1 Dr.Mohamed Omar Shariff, 2 nd Year Post Graduate, Department of General Medicine. DR.B.R.Ambedkar Medical College & Hospital. 2 INTRODUCTION Leading cause of global